AKI Developing Critical Thinking Through Understanding Pathophysiology
advertisement

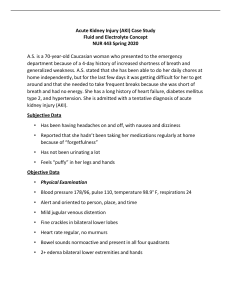
Developing Critical Thinking Through Understanding Pathophysiology Write Worksheet Topic: Acute Kidney Injury 1. Define and describe in your OWN WORDS, the pathophysiology of the primary problem of your patient: Acute kidney injury is where there is sudden onset of reduced renal function. It can lead to electrolyte imbalances, HTN, acid-base disorders, and anemia. 2. How would you explain and teach your patient about the pathophysiology of this medical problem using non-medical terminology? AKI is an abrupt onset- within 48 hours- where their kidneys are not working well. It can lead to high blood pressure, electrolyte imbalances, and low blood counts. 3. What body system(s) are directly impacted by this disease and how are those systems affected? Body System(s): How Body System(s) is Affected: Kindeys ABN renal lab values Low urine output, changes in urinary composition Decreased filtration- GFR, increased BUN, Creatinine Electrolytes High potassium, high phosphorus, low calcium, acidosis Blood Anemia, lack of adequate erythropoiesis Hemodynamics HTN Fluid imbalances Weight gain 4. PRIORITY nursing assessments with this disease? (refer to body system that is most affected). What assessment findings may be abnormal as a result of this illness? Priority Assessments: Expected Abnormal Assessments: Urine output oliguria- less than 500ml/day Non oliguria- greater than 500m/day Anuria- less than 50ml/day Weight and Fluid volume status Increased weight , edema, Assess for s/s of fluid volume excess, keep accurate I&O, and daily weights Lab values High potassium, high phosphorus, low calcium, acidosis Low HGB/HCT, high serum osmolality, increased urine specific gravity, sediment may be present, urine sodium Blood Pressure may be elevated Neuro Watch for hypertension Watch for confusion as toxins build up in their bloodstream Obtain blood and urine cultures as needed fever and infections can increase metabolic and catabolic rate Skin may be dry, scaley, susceptible to breakdown due to edema Respiratory/Lung sounds can be short of breath with fluid overload, increased resp rate 5. What lab tests are altered by this problem? How are those lab tests affected? Does the altered lab test affect any physical assessment findings? Abnormal Lab Tests: How Lab Tests Affected: Does it Impact Assessment? Urine tests helpful in diagnosing etiology Urine sodium, osmolality, and specific gravity distinguish AKI from ATN Patient may need IVFs Patient may need dialysis Pre-renal- increased Post renal- varies ATN- 250-300 Fractional excretion of Na+ (FENa) Pre-renal- <1% Post-renal- >1% ATN- >1% (often >3%) Bun/Creat ratio Fractional excretion of BUN and Pre-renal- >20:1 creatinine distinguish prerenal AKI and Post-renal- 10:1 to 15:1 ATN or postrenal AKI ATN- 10:1 to 15:1 Sedimentation Distinguish AKI from ATN Helps distinguish pre-renal AKI from and ATN and or post renal AKI Patient may need IVFs Patient may need dialysis Pre-renal- normal , few casts Post-renal- normal may be crystals ATN- granular casts, yubular epithelial cells Helps distinguish pre-renal AKI from and ATN and or post renal AKI GFR decreased Patient may need IVFs Patient may need dialysis GFR 6. What medications are most commonly used to manage this problem? Consider the medications you might use, how it works, and why you are using it…. Medications: Mechanism of Action (Own Words): administer IV fluid therapy diuretics – sodium polystyrene – IV medications (dextrose, insulin, potassium, and calcium) – sodium bicarbonate – Rehydrates kidneys and patient Encourages urine output This medication is used to treat a high level of potassium in your blood. Calcium gluconate for hyperkalemia Insulin and glucose can shift potassium into the cells Helpful after contrast medium, cardiac surgery, or liver transplant can reduce the incidence of AKI. It’s a base substance that helps kidney not get worse Manages HTN CCB along with renin angiotensin aldosterone inhibitors 7. Are there any surgical, procedural, or diagnostic interventions for each topic that are important to note? If there are, list 1 or 2 below and why they are used. Renal ultrasonography- R/O obstruction CT and MRI- Evaluate for masses, vascular disorders and filling defects Renal angiography- Evaluate for renal artery stenosis Renal biopsy- Diagnosis, prognosis, and therapy evaluation continuous renal replacement therapy – better for a slower treatment when patient is not HDS enough to tolerate HD. CRRT differs from hemodialysis and peritoneal dialysis in that it is intended to be utilized for 24 hours or longer, continuous and slower (removing fluid at a much slower pace than traditional hemodialysis or peritoneal dialysis) which is better for hemodynamically unstable patients. For this reason, CRRT is usually administered in the critical care units. hemodialysis- good for HDS patients with long term dialysis needs peritoneal dialysis- good for home dialysis and less acute/unstable cases ______________________________________________________________________________________________ On Your Own Time: Consider the Clinical Judgement Measurement Model and try to order your knowledge and understanding of this disease process: Recognize Cues Evaluate outcomes Analyze Cues Take Action Generate Solutions Prioritize Hypotheses