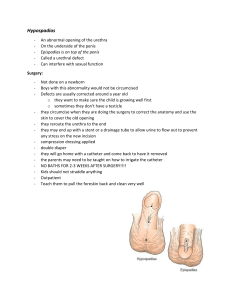
1 Comprehensive Final Review Aging Ethno-geriatrics: Is used to describe the specialty area of providing culturally competent care to ethnic elders • Nurse should attend to primary needs first, ensuring that the pt is pain free and does not need to urinate • All assistive devices should be in place Older Adult Women • Are alone (spouse has often already died) therefore they are at more risks b/c they are home alone • They have a limited source of income so they may have high out of pocket costs Cognitively Impaired Older • Use memory aids for medication and appointment purposes, orientation, use of judgment, emotional Adults state Rural Older Adults • Limited access to healthcare, transportation • RN must clearly define the lifestyle values and practices of rural life Homeless Older Adults • Have low income, reduced cognitive capacity and often live alone Frail Older Adults • Quite often have disability, multiple chronic illnesses, and the presence of geriatric syndromes • Assess important nutritional indicators: SCALES • S: Sadness or mood change • C: Cholesterol, high • A: Albumin, Low • L: Loss or gain of weight • E: Eating problems • S: Shopping and food preparation problems Chronically Ill Older Adults • Have complications with ADLs and IADLs End Of Life Physical Manifestations Sensory Changes Circulatory and Respiratory Changes Loss of Muscle Tone • • • • • • • • • • Blurred vision Decreased pain and touch perception. Blink reflex is eventually lost Sense of touch decreases in the lower extremities first then upper. Hearing is the last sense to remain intact. Decreased oxygenation and circulation causes HR to weaken and slow; reducing BP progressively The Death Rattle occurs because of mouth breathing and mucus in throat Cheyne-Stokes occurs: alternating periods of apnea and deep, rapid breathing Sluggish functional abilities Facial muscles lose tone, causing the jaw to sag 2 Brain Death • • • • Difficulty speaking Gag reflex is lost Constipation, distention and nausea Cerebral cortex stops functioning or is irreversibly destroyed Types of Grief Definition: Grief is the emotional and behavioral response to loss. It is an emotional reaction that is necessary to maintain quality in both emotional and physical well-being Pathologic • Can manifest as chronic grief when the intensity doesn’t wane after the first year. • “Bogged Down” Conflicted • Bereaved person has not resolved ambivalent feelings toward the deceased Absent • Bereaved person appears to be coping and carrying on a s if nothing has happened Maladaptive or Dysfunctional • Prolonged, unresolved, or disruptive • May be related to a real loss or a perceived loss • Feelings and behaviors may become exaggerated and disruptive Adaptive • Helpful or that assists the person in accepting the reality of death • Healthy response Preoperative Care Teaching • Pt has the right to know what to expect and how to participate effectively during the surgical experience • Have balance between telling so little that the pt is unprepared, and explaining so much that the patient is overwhelmed • Explain to patient what they will see, hear, smell and feel during the surgery: cold, bright lights, lots of unfamiliar sounds • Explain pt will go to the OR and wake up in the PACU General Surgery Information • Teach Deep breathing, coughing and moving postop • Make sure to teach rationale for above activities • Explain if the pt will have tubes, drains, monitoring devices, or special equipment and explain what they are for Ambulatory Surgery • Teaching normally done in the DR’s office prior to admission Information • Include time to arrive (1-2hrs before scheduled) • Include day of information: pt registration, parking, what to wear, what to bring, and the need to have a responsible person for transportation after surgery • NPO and explain rationale: to decrease risk for aspiration and to decrease the risk of post op N/V Day of Surgery Preparation Nursing Role • • Preoperative Medications • • • • • • • • • • • • • Transportation to the OR • • • • • • 3 Final pre op teaching, assessment and communication of pertinent findings, and ensuring that all pre op preparation orders have been completed and that records and reports are present and complete to accompany the pt to the OR Verify presence of signed operative consent, laboratory data, H&P, record of any consultations, baseline vital signs, and RN notes complete to that point Pt is wearing hospital gown with no underclothes (depends on surgery) No cosmetics b/c observation of skin colour will be important Remove nail polish: can interfere with pulse ox ID band is present on wrist as well as allergy band if any Can tape wedding ring to the finger Remove all glasses and hearing aids Be sure pt has used the rest room Benzodiazepines and Barbiturates: used for sedative and amnestic properties • Midazolam (Versed): Reduce anxiety • Diazepam (Valium): Induce Sedation • Lorazepam (Ativan): Induce amnesia Anticholinergics: Reduce secretions • Atropine: Decrease oral and respiratory secretions • Glycopyrrolate: Prevent Bradycardia Narcotics: decrease intraoperative anesthetic requirements and to decrease pain • Morphine: Relieve discomfort • Meperidine (Demerol): Relieve pain Antiemetics: Given to decrease N/V • Metoclopramide (Reglan): Increase gastric emptying Eyedrops: pt will require multiple sets of Eyedrops administered at 5 minute intervals Most pt’s will be advised to take routine cardiac, antihypertensive and asthma medications on the day of surgery PO meds should be given 60-90 minutes before the pt goes to the OR IM and SC injections should be given 30-60 minutes before arrival at the OR If I/P: transferred to OR in bed If O/P: taken to OR by cart or wheelchair RN needs to ensure safety during transportation Instructed family where to wait Postoperative Care Nursing Assessment • Record time of pt’s return to unit • Note last dose and type of apin control 4 • • • • • • • • • • • • Take baseline vital signs Assess airway and breath sounds Assess neurologic status including LOC and movement of extremities Assess wound, dressing, drainage tubes Note type and amt of drainage Assess colour and appearance of skin Assess urinary status Note time of voiding Note presence of catheter and total output Check for bladder distention or urge to void Note catheter patency Assess pain and discomfort • • • • • • • • • • • • • Postanesthesia Discharge Criteria • • • • • • Pt awake (or baseline) VS stable No excess bleeding or drainage No respiratory depression Oxygen saturation >90% Report given Note current pain intensity Position for airway maintenance, comfort, safety (bed in low position, side rails up) Check IV infusion Note type of solution Note amt of fluid remaining Note flow rate Check integrity of insertion site and size of catheter Attach call light within reach and orient pt to use of call light Ensure that emesis basin and tissues are available Determine emotional condition and support Check for presence of family member or significant other Orient pt and family to immediate environment Check and carry out post op orders Ambulatory Surgery Discharge Criteria • • • • • • • All PACU discharge criteria met NO IV narcotics for last 30 minutes Minimal N/V Voided (if appropriate to surgical procedure/orders) Able to ambulate if age appropriate and not contraindicated Responsible adult present to accompany pt D/C instructions given and understood Cancer • Group of more than 200 diseases characterized by uncontrolled and unregulated growth of cells. • Occurs in persons of all ages and ethnicities • Cancer incidence and death rate higher in African Americans than in whites Prevention and Detection • Reduce or avoid exposure to known or suspected carcinogens and cancer-promoting agents, including cigarette smoke and sun exposure • Eat a balanced diet that includes vegetables (green, yellow, and orange), fresh fruits, whole grains, and adequate amts of fiber, and reduce the amt of fat and preservatives, including smoked and saltcured meats • Participate in a regular exercise regimen • Obtain adequate, consistent periods of rest (at least 6-8 hrs per night) • Have a health examination on a regular basis that includes a health history, physical, and specific diagnostic rests for common cancers in accordance with American Cancer Society • • • • • Surgery Radiation • • • • • • • • • • • • • • • • • • 5 Eliminate, reduce, or change the perceptions of stressors and enhance the ability to effectively cope with stressors Enjoy consistent periods of relaxation and leisure Know the seven warnings signs of cancer: CAUTION • C: Change in bowel or bladder habits • A: A sore that doesn’t heal • U: Unusual bleeding or discharge from any body orifice • T: Thickening or a lump in the breast or elsewhere • I: Indigestion or difficulty in swallowing • O: Obvious change in a wart of mole • N: Nagging cough or hoarseness Learn and practice self-examinations Seek immediate medical care if you notice a change in what is normal for you and if cancer is suspected. Early detection of cancer has a positive impact on prognosis Cure and Control Oldest form of treatment Try to remove all cancerous tissue Can be used as supportive measures: Insertion of feeding tubes and Colostomy Palliative: Debulking of tumor to relieve pain or pressure, Colostomy for relief of a bowel obstruction, Laminectomy for relief of a spinal cord compression Rehabilitative: Breast reconstruction after mastectomy Is the emission and distribution of energy through space or a material medium Energy produced by radiation, when absorbed into tissue, produces ionization and excitation Local energy is sufficient to break chemical bonds in DNA, which leads to a biologic effect Brachytherapy: Consists of implantation or insertion of radioactive materials directly into the tumor or in close proximity to the tumor. Commonly used for tumors of the head and neck and GYN tumors. The pt is radioactive during the time the source is in place. Maintain distance, time and shielding are used when caring for the person with an implant. Must wear a film badge Fatigue is common side effect: normally begins in the 3rd or 4th week of treatment Maintain nutritional status Keep pt active: walking programs Bone marrow suppression Decrease in salivary flow: lose taste Soft, nonirritating high-protein and high-caloric foods should be offered frequently throughout the day Encourage nutritional supplements Weigh pt at least twice each week 6 Chemotherapy • • • • • • • • • • • • • Administer prophylactic antiemetics 1hr before treatment Eating a light meal before treatment may help reduce post nausea feeling Permanent cessation of menses occurs in 95% of women less than 40 yrs of age Offer advice on harvesting of sperm or ova Nitrogen Mustard: Chemical warfare agent used to treat Acute Leukemia Alkylating Agents: Damage DNA by causing breaks in the double strand helix, Nitrogen Mustard, Cytoxan Antimetabolites: Interfere with synthesis of DNA by mimicking certain essential cellular metabolites that cell incorporates into synthesis of DNA; cells die immediately, MTX, 5-FU Antitumor Antibiotics Plant Alkaloids Nitrosoureas Corticosteroids Hormone Therapy Leukemia General term used to describe a group of malignant disorders affecting the blood and blood forming tissues of the bone marrow, lymph system, and spleen Etiology and Pathophysiology • NO single causative agent • Result from genetic and environment influences • Increased incidence of leukemia in radiologists, person living near nuclear bomb test sites or clear reactor accidents, survivors of the bombing of Nagasaki and Hiroshima, and persons previously treated with radiation or Chemo. Classifications • Can be done based on acute versus chronic and on the type of WBC involved • Acute: characterized by the clonal proliferation of immature hematopoietic cells. Develops from malignant transformation of a single type of immature hematopoietic cell, followed by cellular replication and expansion of that malignant clone • Chronic: involve more mature forms of WBC, and the disease onset is more gradual • AML: • ¼ of all leukemia’s, but about 85% of acute leukemia’s • Onset abrupt and dramatic • Serious infections and abnormal bleeding from the onset of the disease • Uncontrolled proliferation of myeloblasts • Hyperplasia of the bone marrow and spleen • ALL: • Most common type of leukemia in children • 15% of acute leukemia’s in adults 7 • • • Clinical Manifestations Diagnostic Studies Collaborative Care Nursing Management Immature lymphocytes proliferate in the bone marrow Fever at the time of diagnoses S&S’s may appear abruptly with bleeding or fever, or may be insidious with progressive weakness, fatigue, and bleeding tendencies CNS manifestations Leukemic meningitis • • • CML: • Caused by excessive development of mature neoplastic granulocytes in the bone marrow • Granulocytes move into the peripheral blood in massive numbers and ultimately infiltrate the liver and spleen • Philadelphia Chromosome • Chronic stable phase followed by a more acute aggressive phase • CLL: • Production and accumulation of functionally inactive but long lived, mature appearing lymphocytes • B cell is involved • The lymphocytes infiltrate the bone marrow, spleen and liver • Lymph node enlargement • Infection • Hairy Cell Leukemia: • 2% of all adult leukemias • Seen in male pt’s over 40 • Chronic disease of lymphoproliferation predominantly involving B lymphocytes that infiltrate the bone marrow and spleen • Cells have a hairy appearance • Splenomegaly common finding • Problems are caused by bone marrow failure and the formation of leukemic infiltrates • As the dx progresses, fewer normal blood cells are produced • Leukemic cells infiltrate the pt’s organs, leading to problems such as splenomegaly, hepatomegaly, lymphadenopathy, bone pain, meningeal irritation, and oral lesions • Peripheral blood evaluation • Bone marrow examination • Goal of remission • Chemo • Bone marrow and stem cell transplantation • Explain and teach pt about treatments, drugs and side effects. 8 • • • • • • Laryngectomy Removing structures above the true cords-false vocal cords and epiglottis High risk of aspiration Requires temporary tracheostomy Voice is preserved unless they have a total laryngectomy Teach Supraglottic Swallow • Take deep breath to aerate lungs • Perform Valsalva maneuver to approximate cords • Place food in mouth and swallow. Some food will enter airway and remain on top of closed vocal cords • Cough to remove food form top of vocal cords • Swallow so food is moved from top of vocal cords • Breathe after cough swallow sequence to prevent aspiration of food collected on top of vocal cords Requires frequent suctioning after surgery Cataracts • An opacity within the crystalline lens • May be in one or both eyes • Third leading cause of preventable blindness • Cataract removal is the most common surgical procedure Etiology and Pathophysiology • May be caused by blunt or penetrating trauma, congenital factors such as maternal rubella, radiation or UV light exposure, corticosteroids and ocular inflammation • Diabetes • Altered metabolic processes within the lens cause an accumulation of water and alterations in the lens fiber structure Clinical Manifestations • Decrease in vision, abnormal colour perception and glare • Visual decline is gradual Diagnostic Studies • Visual acuity measurement • Ophthalmoscopy (direct and indirect) • Slit lamp microscopy • Glare testing • Keratometry and A-scan ultrasound • Visual field perimetry Collaborative Care Nonsurgical • Change prescription of glasses • Strong reading glasses or magnifiers • Increased lighting 9 Nursing Management • Lifestyle adjustment • Reassurance Acute Care: Surgical Therapy • Preoperative • Mydriatic, cycloplegic agents • Nonsteroidal anti-inflammatory drugs • Topical antibiotics • Antianxiety medications • Surgery • Removal of lens • Phacoemulsification • Extracapsular extraction • Correction of surgical aphakia • Intraocular lens implantation (most frequent type of correction) • Contact lens • Postoperative • Topical antibiotics • Topical corticosteroids or other anti-inflammatory agents • Mild analgesia • Eye shield and activity as preferred by patient’s surgeon • Wear sunglasses, • Avoid extraneous or unnecessary radiation • Maintain appropriate intake of antioxidant vitamins-C and E • Good nutrition • When giving topical medications for pupil dilation before surgery pt’s with dark irides may need a larger dose • Photophobia is common • Use dark glasses • When administering mydriatics use punctual occlusion • Teach there may be scratchiness in the operative eye • If there is intense pain call MD-may be a sign of hemorrhage, infection or increased IOP • Surgery is only few hrs long • Eye remains patched for 24hrs and many pt’s have good vision in their unoperated eye After Eye Surgery Teaching 10 • • • • • • Teach pt and family proper hygiene and eye care techniques to ensure that medications, dressings, and surgical wound are not contaminated during necessary eye care Teach pt and family about signs and symptoms of infection and when and how to report those to allow early recognition and tx of possible infection Instruct pt to comply with postop restrictions on head positioning, bending, coughing, and Valsalva maneuver to optimize visual outcomes and prevent IOP Instruct pt to instill eye medications using aseptic techniques and to comply with prescribed eye medication routine to prevent infection Instruct pt to monitor pain and take prescribed medication for pain as directed and to report pain not relieved by prescribed medications Instruct pt of the importance of continued follow up as recommended to maximize potential visual outcomes Glaucoma • • Is a group of disorders Characterized by: • Increased IOP and the consequences of elevated pressure • Optic nerve atrophy • Peripheral visual field loss • Directly related to the balance or imbalance of fluid • Second leading cause of permanent blindness in the US • Leading cause of blindness among AA Etiology and Pathophysiology • Improper balance between the rate of aqueous production and aqueous reabsorption • Primary: the outflow of aqueous humor is decreased in the trabecular meshwork. The drainage channels become clogged • Secondary: inflammatory reasons that block the meshwork-trauma, intraocular or periorbital neoplasms, iris neovascularization Clinical Manifestations • POAG: develops slowly without symptoms-no pain or pressure, don’t notice the visual loss until peripheral vision has been severely compromised • Eventually the pt gets tunnel vision • Acute angle closure: sudden, excruciating pain in or around the eye, N/V • See halos around lights • Blurred vision • Ocular redness • Corneal edema-gives the cornea a frosted appearance Diagnostic Studies • Visual acuity measurement • Tonometry • Ophthalmoscopy • Slit lamp microscopy • Gonioscopy 11 Collaborative Care Nursing Management • Visual field perimetry • Fundus photography Ambulatory/Home Care for Open-Angle • Drug therapy • B adrenergic blockers • Alpha adrenergic agonists • Cholinergic agents • Carbonic andhydrase inhibitors • Surgical Therapy • Argon laser trabeculoplasty • Cyclocryotherapy destruction of ciliary body Acute Care Angle-Closure Glaucoma • Topical cholinergic agent • Hyperosmotic agent • Laser peripheral iridotomy • Surgical iridectomy • Teach risk factors • Have eye test every 2-4 yrs fo persons between 40-64 and every 1-2 yrs for 65 and older • AA in every age category should have examinations more often Acute Interventions • Darkening the environment • Applying cool compresses to the pt’s forehead • Providing quiet and private space Ambulatory and Home Care • Encouragement of following medication regimen • Provide information about the purpose, frequency and technique for administration of prescribed agents • Provide written copy Gerontologic Considerations • Older pt’s may experience an additive effect if a systemic b adrenergic blocking drug is also being taken • Alpha adrenergic agonists can cause tachycardia or HTN Meniere’s Disease • Characterized by symptoms caused by inner ear disease, including episodic vertigo, tinnitus, fluctuating sensorineural hearing loss, and aural fullness 12 • • Duration of attacks may be hours or days, and may occur several times a year Autonomic symptoms include pallor, sweating, nausea, and vomiting Diagnostic Studies • Audiometic studies, including speech discrimination, tone decay • Vestibular tests, including caloric test, postional test • Electronystagmography • Neurologic Examination • Glycerol test Collaborative Care Acute Care • Sedative (Diazepam) • Anticholinergic (Atropine) • Vasodilators • Antihistamine (Benadryl) Surgical Therapy • Endolymphatic Shunt • Vestibular Nerve section • Labyrinthotomy • Labyrinthectomy Ambulatory/Home Care • Diuretics • Antihistamines • Vasodilators • Antiseizure drugs • Vitamins • Diazepam • Low salt diet • Restriction of caffeine, nicotine, and alcohol Nursing Management • During acute attack keep pt in quiet, darkened room in a comfortable position • Teach to avoid sudden head movement or position changes • Fluorescent or flickering lights or watching television may exacerbate symptoms and should be avoided • Provide emesis basin • Keep side rails up and bed in low position to minimize falling • Monitor I&O’s GERD Etiology and Pathophysiology • Syndrome 13 • • Clinical Manifestations Complications Diagnostic Studies Collaborative Care No one single cause Defenses of the lower esophagus are overwhelmed by the reflux of stomach acidic contents into the esophagus • Predisposing conditions -hiatal hernia, incompetent LES, decreased esophageal clearance resulting from impaired esophageal motility and decreased gastric emptying • Heartburn-relieved with milk, alkaline substances or water • Wheezing, coughing, and dyspnea • Hoarseness, sore throat and sense of a lump in the throat and coking • Hot, bitter, or sour liquid taste • Esophagitis • Barrett’s esophagus • Precancerous lesion • Replacement of the normal squamous epithelium of the esophagus with columnar epithelium • Bronchospasm • Laryngospasm • Cricopharyngeal spasm • Pneumonia RT aspiration • Barium swallow-see if there protrusion of the upper part of the stomach • Endoscopy-see competence of the LES and extent of inflammation, scarring and strictures • Esophageal manometric studies-measure pressure in the esophagus and LES • Radionuclide tests-detect reflux of gastric contents and the rate of esophageal clearance • High dose proton pump inhibitor treatment used as a first step in the diagnosis of GERD Lifestyle Modifications: • Diet and drugs • Stop smoking Nutritional Therapy: • Avoid fatty foods, chocolate, peppermint, coffee, and tea • Avoid milk at night b/c milk increases gastric acid secretion • Eat small frequent meals • Don’t eat late • Fluids should be taken between meals to reduce gastric distention • Avoid tomatoes and orange juice-acidic Drug Therapy: • Antacids • Antisecretory agents • H2 receptor blockers • Proton pump inhibitors 14 Nursing Management Gerontologic Considerations • • • • • • Prokinetic drug therapy • Cholinergic drugs Surgical Therapy: • Nissen fundoplication • Toupet fundoplication • Hill gastropexy • Belsey fundoplication Endoscopic Therapy: • Stretta device • Teach to avoid factors that cause reflux • HOB is elevated • Don’t lay down 2-3 hrs after eating • Eat high protein, low fat diet • Eat small frequent meals • Loss weight • Peptic Ulcer Disease Condition characterized by erosion of the GI mucosa resulting from the digestive action of HCL acid and pepsin Types: acute, chronic Acute: associated with superficial erosion and minimal inflammation; short duration and resolves quickly when the cause is identified and removed Chronic: one of long duration, eroding through the muscular wall with the formation of fibrous tissue, present continuously for many months or intermittently throughout the person’s lifetime; at least four times as common as acute erosion Gastric and duodenal ulcers also defined as peptic ulcers Gastric Ulcers Lesion • Location of lesion • Gastric secretion Incidence • • • • • Superficial; smooth margins; round, oval or cone shaped Predominantly atrium, also in body and fundus of stomach Normal to decreased Greater in women Peak age 50-60 yr More common in persons of lower socioeconomic status and in unskilled laborers Increased with smoking, drug, and alcohol use Duodenal Ulcers • • • • • • • Penetrating (associated with deformity of duodenal bulb form healing of recurrent ulcers) First 1-2 cm of duodenum Increased Greater in men, but increasing in women, especially postmenopausal Peak age 35 to 45 yr Associated with psychologic stress Increased with smoking, drug, and alcohol use 15 • • Clinical Manifestations • • • Increase with incompetent pyloric sphincter and bile reflux Increased with stress ulcers after severe burns, head trauma, and major surgery Burning or gaseous pressure in high left epigastrium and back and upper abdomen Pain 1-2 hr after meals; if penetrating ulcer, aggravation of discomfort with food Occasional n/v, weight loss • • • • Recurrence rate Complications • • High Hemorrhage, perforation, outlet obstruction, intractability • • Associated with other diseases (COPD, pancreatic disease, hyperparathyroidism, Zollinger-Ellison syndrome, chronic renal failure) Burning, cramping, pressure like pain across midepigastrium and upper abdomen; back pain with posterior ulcers Pain 2-4 hours after meals and midmorning, midafternoon, middle of night, periodic and episodic Pain relief with antacids and food; occasional nausea and vomiting High Hemorrhage, perforation, obstruction Gastric Surgery Complications Dumping syndrome • • • Postprandial hypoglycemia • • • • • • • • • • • • Dumping syndrome is the direct result of surgical removal of a large portion of the stomach and the pyloric sphincter Reduce the reservoir capacity of the stomach Dumping syndrome more commonly experienced after a Billroth II procedure, can occur after any gastric reconstruction and vagotomy Associated with meals having a hyperosmolar composition Stomach no longer has control over the amount of gastric chime entering the small intestine Onset of sx occurs at the end of a meal or within 15 to 30 minutes after eating Feelings of weakness, sweating, palpitations, and dizziness; sx r/t sudden decrease in plasma volume Pt c/o abdominal cramps, borborygmi, and urge to defecate Manifestations lasts for no longer than an hour pc Variant of dumping syndrome Result of uncontrolled gastric emptying of a bolus of fluid high in carbs into the small intestine Bolus of concentrated carbs results in hyperglycemia and release of excessive amounts of insulin into the circulation Secondary hypoglycemia occurs Sx occurs about 2 hours after meals Symptoms: sweating, weakness, mental confusion, palpitations, tachycardia, and anxiety Bile reflux gastritis • • • • • • • • • 16 Gastric surgery that involves the pylorus, either reconstruction or removal can result in reflux alkaline gastritis Prolonged contact of bile, especially bile salts causes damage to gastric mucosa Peptic ulcer may recur after surgical tx Sx associated with reflux alkaline gastritis are continuous epigastric distress that increases after meals Vomiting relieves it temporarily Administration of cholestyramine (Questran) ac or pc Aluminum hydroxide antacids also tx Billroth I Gastroduodenostomy Partial gastrectomy with removal of the distal two thirds of the stomach and anastomosis of the gastric stump to the duodenum • Billroth II Gastrojejunostomy Partial gastrectomy with removal of the distal two thirds of the stomach and anastomosis of the gastric stump to the jejunum • Preferred because the duodenum is bypassed • Prevent recurrence of duodenal ulcers • Dumping syndrome experienced more commonly In both procedures the antrum and pylorus are removed • • Ostomies • Surgical procedure in which an opening is made to allow the passage of intestinal contents from the bowel to an incision or stoma • Fecal matter is diverted through the stoma to the outside of the abdominal wall Ileostomy • Opening from the ileum through the abdominal wall • Conventional or Brooke Ileostomy • Commonly used for ulcerative colitits, Crohn’s dx and familial polyposis Cecostomy • Opening between the cecum and the abdominal wall • Both cecostomies and ascending colostomies are uncommon • Usually temporary and most often used for fecal diversion before surgery or for palliation Colostomy • Opening between the colon and the abdominal wall • Proximal end of the colon is sutured to the skin • Temporary colostomy is usually performed to protect and end to end anastomosis after a bowel resection or is an emergency measure following bowel obstruction, abdominal trauma, or a perforated diverticulum • Temporary colostomies are usually located in the transverse colon • Loop colostomy and double barrel colostomy are most commonly performed as temporary colostomies, but they may be permanent 17 Ascending Colostomy Transverse Colostomy Stool Consistency • Semiliquid • Fluid Requirement Bowel Regulation • • Increased No Pouch and skin barriers Irrigation • Indications for surgery Ileostomy • Formed • • • Semiliquid to Semiformed Possibly increased Uncommon • • • • Yes • Yes • • Yes • No • No • • No • Perforating diverticulitis in lower colon Trauma Inoperable tumors of colon, rectum, or pelvis Rectovaginal fistula • Same as for ascending Birth Defect • No change Yes (if there is a history of a regular bowel pattern Dependent on regulation Possible Q24-48hr (If patient meets criteria) Cancer of the rectum or rectosigmoidal area Perfoating diverticulum Trauma Liquid to Semiliquid Increased No • • • Ulcerative colitis Crohn’s disease Diseased or injured colon Birth defect Familial polyposis Trauma Cancer • • • • Sigmoid Colostomy • • • • • • • Parkinson’s Disease Disease of the basal ganglia characterized by a slowing down in the initiation and execution of movement (bradykinesia), increased muscle tone (rigidity), tremor at rest, and impaired postural reflexes. Etiology and Pathophysiology • Increases with age. Peak onset in the 60’s • Onset before 50 is likely related to a genetic defect • Encephalitis lethargica, or type A encephalitis, has been associated with the onset of parkinsonism • Parkinson like symptoms has occurred after intoxication with carbon monoxide and manganese. • Degeneration of the dopamine-producing neurons in the substantia nigra of the midbrain which in turn disrupts the normal balance between dopamine and Ach in the basal ganglia. Clinical Manifestations • Gradual and insidious • May involve only one side of the body • Early signs: tremor, slight limp, or a decreased arm swing • Late signs: shuffling, propulsive gait with arms flexed and loss of postural reflexes • Slight change in speech Tremor: • 1st, only patient notices it 18 Complications Diagnostic Studies Collaborative Care • Can affect handwriting • More prominent at rest • Aggravated by emotional stress or increased concentration • “Pill rolling” • Can involve the diaphragm, tongue, lips, and jaw. Rigidity: • 2nd sign • Jerky • “Cogwheel Rigidity” • Caused by sustained muscle contraction and consequently elicits a complaitn of muscle soreness; feeling tired and achy; or pain in the head, upper body, spine, or legs. • Slowness of movement b/c it inhibits the alternating of contraction and relaxation in opposing muscle groups Bradykinesia: • Loss of automatic movements • Blinking of the eyelids, swinging of the facial and hand movements, and minor movement of postural adjustment • Swallowing may become difficult • Malnutrition or aspiration • Pneumonia, UTI’s, skin breakdown • Gait slows and turning is difficult • Constipation, ankle edema, contractures due to decreased mobility • Orthostatic hypotension-falls • Seborrhea (increased oily secretion of the sebaceous glands of the skin) • Dandruff • Excessive sweating • Conjunctivitis • Difficulty reading • Insomnia • Incontinence • depression • Based solely on history and the clinical features • Diagnoses is based on 2 out of 3 clinical signs (tremor, rigidity, bradykinesia) • Aimed at reliving symptoms Drug therapy: • Correcting imbalance of neurotransmitters with in the CNS • Levodopa 19 • • Nursing Management Sinemet Anticholinergic drugs-act by decreasing the activity of Ach, providing balance between cholinergic and dopaminergic actions. • Antihistamines-used to manage tremors • Amantadine-promotes the release of DA from neurons • Selegiline-monoamine oxidase inhibitor used in combination with Sinemet Surgical therapy: • Aimed at relieving symptoms and usually used in patients who are unresponsive to drug therapy or who have developed severe motor complications • 3 categories: 1. Ablation (Destruction): • Involves stereotactic ablation of areas in the thalamus, globus palidus, and subthalamic nucleus 2. Deep Brain Stimulation: • Involves placing an electrode in either the thalamus, globus pallidus, or subthalamic nucleus and connecting it to a generator placed in the upper chest • Device is programmed to deliver a specific current to the targeted brain location • Can be adjusted to control symptoms better and is reversible 3. Transplantation: • Fetal neural tissue into the basal ganglia is designed to provide DA-producing cells in the brains • Still in the experimental stages Nutritional Therapy: • Easily chewed and soft foods • Adequate roughage and fruit to avoid constipation • Cut food into bite sized portions • Serve warm • Eat 6 small meals/day • Provide ample time for eating • Some patient’s advised to limit protein intake in the evening b/c absorption of levodopa can be impaired by protein ingestion • Promotion of physical exercise • Well balanced diet • Teach maintenance of good health, encouragement of independence, and avoidance of complications such as contractures • Teach think about stepping over imaginary lines on the floor, drop rice kernels and step over them, rock from side to side, lift the toes when stepping, take one step backward and two steps forward 20 • • • • Assess for Levodopa overdose Use slip-on shoes and Velcro hook-and-loop fasteners or zippers on clothing, instead of buttons and hooks Use elevated toilet seat Multiple Sclerosis Chronic, progressive, degenerative disorder of the CNS characterized by disseminated demyelination of nerve fibers of the brain and spinal cord • Disease of young-middle age adults • Onset normally between 15-50 • Women more affected then men Etiology and Pathophysiology • Cause is unknown • Research suggests viral infections, immunologic, and genetic factors and is perpetuated as a result of intrinsic factors • Characterized by chronic inflammation, demyelination, and gliosis in the CNS Clinical Manifestations • Insidious and gradual, with vague symptoms that occur intermittently over months or years • May not be diagnosed until long after the onset of the first symptom • Motor, sensory, cerebellar, and emotional problems • Weakness or paralysis of the limbs, trunk, head • Scanning speech • Spasticity of the muscles • Numbness and tingling • Patchy blindness, blurred vision, vertigo, tinnitus, decreased hearing, and chronic neuropathic pain • Lhermitte’s Phenomenon • Transient sensory symptom • Electric shock radiating down the spine or into the limbs with flexion of the neck • Nystagmus • Ataxia • Dysarthria • Dysphagia • Constipation • Spastic bladder-lesion aboce the second sacral nerve, which cuts off suprasegmental inhibiting influences on bladder contractility • Sexual dysfunction-decreased libido, painful intercourse, decreased vaginal lubrication Diagnostic Studies • Based on history, clinical manifestations, and the presence of multiple lesions over time • CSF-show an increase in oligoclonal immunoglobulin G, increased lymphocytes and monocytes 21 Collaborative Care Nursing Management Drug Therapy: • Corticosteroids• Immunomodulators-Betaseron, Interferon • Immunosuppressants- Axathioprine, methotrexate, Cytoxan • Cholinergics • Anticholinergics • Muscle relaxants Surgical Therapy: • Thalamotomy (unmanageable tremor) • Neurectomy (unmanageable Spasticity) • Rhizotomy (unmanageable Spasticity) • Cordotomy (unmanageable Spasticity) Nutritional Therapy: • Megavitamin therapy (Vit B & C) • Diet consisting of low fat and gluten free food and raw vegetables • High protein diet with supplementary vitamins • Increase roughage to relieve constipation • Exacerbations are triggered by infection, trauma, immunization, delivery after pregnancy, stress, and change in climate • Prevent major complications of immobility such as UTIs, pressure ulcers and respiratory infections • Teach avoid fatigue, extreme heat and cold and exposure to infection • Teach to achieve a good balance of exercise and rest • Eat nutritious and well balanced meals • Increase fiber to decrease constipation Myasthenia Gravis • Autoimmune disease of the neuromuscular junction characterized by the fluctuating weakness of certain skeletal muscle groups • Can occur at any age but most commonly between 10-65 • Peak age in women 20-30 • 3 times more common in women, but at older ages both sexes are equally affected Etiology and Pathophysiology • Caused by autoimmune process in which antibodies attack Ach receptors, resulting in a decreased number of Ach receptor sites at the neuromuscular junction. This prevents Ach molecules from attaching and stimulating muscle contraction. Clinical manifestations and Complications • Fluctuating weakness of skeletal muscle • Strength usually restored after a period of rest • Muscles most often involved are the muscles that move the eyes and eyelids, chewing, swallowing, speaking and breathing 22 • • • • Facial mobility and expression can be impaired Voice fades after a long conversation No sensory loss, reflexes are normal, and muscle atrophy is rare Exacerbations can be precipitated by emotional stress, pregnancy, menses, secondary illness, trauma, temperature extremes, and hypokalemia • Myasthenic Crisis-acute exacerbation of muscle weakness triggered by infection, surgery, emotional distress, or overdose of or inadequate drugs • History and Physical examination • EMG- may show a decrementing response to repeated stimulation of the hand muscles, indicative of muscle fatigue • Tensilon Test-reveals improved muscle contractility after intravenous injection of the anticholinesterase agent edrophonium chloride • ACh receptor antibodies Drug Therapy: • Anticholinesterase agents • Corticosteroids • Immunosuppressive agents Surgery: • Thymectomy Plasmapheresis: • Indicated for patients in crisis or in preparation for surgery when corticosteroids must be avoided • Maintaining adequate ventilation • Continuing drug therapy • Watching for side effects of therapy • Balanced diet with food that can be chewed and swallowed easily • Semisolid foods • Teaching to focus on the importance of following the medical regimen, potential adverse reactions to specific drugs, planning activities of daily living to avoid fatigue, the availability of community resources, and the complications of the disease and therapy and what to do about them. Diagnostic Studies Collaborative Care Nursing Management Guillian-Barre Syndrome Etiology and Pathophysiology • • • • Acute Rapidly progressing Potentially fatal form of polyneuritis Affects the PNS and results in loss of myelin and edema and inflammation of the affected nerves, causing 23 Clinical Manifestations Diagnostic Studies Collaborative Care Nursing Management a loss of neurotransmission to the periphery • Affects both genders • Etiology is unknown, but is believed to be a cell mediated immunologic reaction directed at the peripheral nerves • Often preceded by immune system stimulation from a viral infection, trauma, surgery, viral immunizations, HIV, or lymphoproliferative neoplasm’s • Campylobacter jejuni • Heterogeneous • Symptoms usually develop 1-3 weeks after an upper respiratory or GI infection • Weakness of the lower extremities occurs over hrs to days to weeks, usually peaking about the 14th day • Distal muscles are more severely affected • Numbness and tingling in the extremities • Reduced muscle tone and lack of reflexes are common and persistent symptoms • Pain, worse are night • Respiratory or UTIs may occur • immobility • diagnosis based on patients history and clinical signs • CSF is normal or has a low protein but after 7-10 days shows and elevated protein level to 700mg/dl • EMG and nerve conduction studies-show sever abnormalities • Supportive care • Ventilatory support during the acute phase • Plasma exchange used in the first two weeks IB of high dose Sandoglobulin-need to be well hydrated and have adequate renal function • After 3 weeks of disease onset, plasma exchange and immunoglobulin therapies have little value Nutritional Therapy: • Difficulty swallowing b/c of cranial nerve involvement-place patient in upright position and flexing the head forward during feedings • TPN • Monitor body weight, albumin, and calorie counts regularly • Support body symptoms until the patient recovers • Monitor ABGs • Suctioning • Urinary retention is common for a few days • Intermittent catheterization preferred to avoid UTIs • PT • Passive ROM • Artificial tears frequently during the day 24 • • • • • • Inspect eyes for presence of eyelashes Check for gag reflex Note drooling and other secretions which may be indicative of an inadequate gag reflex B/C of delayed gastric emptying, residual volumes of the feedings should be assessed at regular intervals or before feedings Monitor fluid and electrolyte balances Begin bowel program b/c constipation is a common problem Amyotrophic Lateral Sclerosis • • • • • • • • • • • Rare progressive neurologic disorder Loss of motor neurons Usually leads to death within 2-6 yrs after diagnosis Onset between 40-70 yrs old More common in men For unknown reasons motor neurons in the brainstem and spinal cord gradually degenerate Symptoms-weakness in the legs Death is from respiratory infection secondary to compromised respiratory function No cure Riluzole slows the progression • It decreases the amount of glutamate in the brain Support the patients cognitive and emotional functions by facilitating communication, reducing risk of aspiration, decreasing pain secondary to muscle weakness, decreasing risk of injury related to falls, providing divisional activities such as reading and human companionship, and helping the person and family with advance are planning and anticipatory grieving related to loss of motor function and death Seizure Disorders and Epilepsy Seizures • Paroxysmal, uncontrolled electrical discharge of neurons in the brain that interrupts normal function • Often symptoms of underlying diseases • May occur spontaneously without any apparent cause Epilepsy • Person has spontaneously recurring seizures caused by a chronic underlying condition • Higher in underdeveloped countries • Rates are higher during the first year of life, decline during childhood and adolescence, plateau in middle age, and rise sharply again among the elderly Etiology and Pathophysiology • Most common cause during first 6 months of life are severe birth injury, congenital defects involving the CNS, infections, and inborn errors of metabolism 25 • Clinical Manifestations Generalized Seizures Partial Seizures Pt’s between 2-20yrs old the primary causative factors are birth injury, infection, trauma, and genetic factors • Between 20-30yrs old usually occurs as the result of structural lesions, such as trauma, brian tumors, or vascular disease • After 50 the cause are cerebrovascular lesions and metastatic brain tumors • ¾ of all seizure disorder cases can’t be attributed to a specific cause and are considered idiopathic • Preferred method of classifying recurring seizures is the International Classification System • Seizures are divided into Generalized and Partial Seizures • Phases: • Prodromal-with signs or activity which precede a seizure • Aural-Sensory warning • Ictal-full seizure • Postictal-period of recovery after the seizure • Characterized by bilateral synchronous epileptic discharges in the brain from the onset of the seizure • No warning or aura • Pt loses consciousness for a few seconds to several minutes Tonic Clonic Seizures • Most common generalized seizure • Loss of consciousness and falling to the ground • Followed by stiffening of the body for 10-20 seconds and subsequent jerking of the extremitites for another 30-40 seconds • Cyanosis, excessive salivation, tongue or cheek biting and incontinence may accompany the seizure • In postictal phase the pt usually has muscle soreness, is very tired, and may sleep for several hrs • Pt has no memory of the seizure Typical Absence Seizures • Usually occurs only in kids • May cease as kid grows older • Brief staring spell that lasts only a few seconds • Often unnoticed • When untreated, may occur up to 100 times a day • Can often be precipitated by hyperventilation and flashing lights Atypical Absence Seizures • Staring spell accompanied by other signs and symptoms, including brief warnings, peculiar behaviour during the seizure, or confusion after the seizre • Being in specific region of the cortex • May be confined to one side of the brain and may spread to other parts of the brain 26 • • Complications Diagnostic Studies Collaborative Care Nursing Management Todd’s paralysis (focal weakness) Involves lip smacking and automatisms (repetitive movements that may not be appropriate)-picking at clothing, fumbling with objects, or walking away Physical • Status Epilepticus • State of continuous seizure activity or a condition in which seizures recur in rapid succession without return to consciousness between seizures • Most serious complication of epilepsy and is a neurologic emergency • Neurons become exhausted and cease to function • Permanent brain damage may result • Death from head injury • Drowning in the bathtub Psychosocial • Associated with supernatural powers • Possession by the devil • Insanity • May experience employment discrimination • Driving laws • Birth and development history • Significant illnesses and injuries • Family History • Febrile seizures • Comprehensive neurologic assessment • Precipiating factors • Antecendent events • Seizure description • CBC, UA, LYTES, CREA, fasting blood glucose • Lumbar puncture • CT, MRI, MRA, MRS, PET scans • EEG • Antiseizure drugs • Surgery • Vagal nerve stimulation • Psychosocial counseling • Wear helmets • Maintain proper diet • Adequate rest 27 • • • • • Exercise When seizure occurs observe and record all details of the event-onset, course and nature of the seizure (LOC, tongue bitting, automatisms, stiffening, jerking, total lack of muscle tone), body parts involved, presence of autonomic signs, such as dilated pupils, excessive salivation, altered breathing, cyanosis, flushing, diaphoresis, incontinence During the seizure maintain airway-supporting the head, turning the pt to the side, loosening constrictive clothing, easing the pt to the floor Don’t restrain the pt DON”T PLACE THINGS IN THE MOUTH Mastectomy • Removal of breast and auxiliary lymph nodes, • Preserves the pectorals major muscle. • Selected if the tumor is too large to excise with good margins and attain a reasonable cosmetic result. • Reconstructive surgery can be performed immediately following the mastectomy or delayed until post op recovery (6 months) • The most common site of recurrence of breast cancer is at the surgical site Follow Up Care • The woman must be followed up for the rest of her life at regular intervals. • Examinations every 6months for 2 years then annually thereafter. • Most continue BSE monthly on both breast or remaining breast and mastectomy site. • Most common site of recurrence is surgical site. Post Mastectomy Pain Syndrome • S/S- chest and upper arm pain, tingling down the arm, numbness, shooting/pricking pain, and unbearable itching that persist beyond the normal 3 month healing time. • Rx- NSAIDS, antidepressants, topical lidocaine patches, guided imagery training, physical therapy to prevent “frozen shoulder” syndrome R/t dec. movement, and psychologic counseling. Prostate Cancer Pathophysiology • • • • • • • • Androgen-dependent adenocarcinoma The majority of tumors occur in the outer aspect of the prostate gland Usually slow growing Spreads by three routes: direct extension, lymph system, bloodstream Spread by direct extension involves the seminal vesicles, urethral mucosa, bladder wall, and external sphincter The cancer later spreads through the lymphatic system to the regional lymph nodes The veins from the prostate seem to be the mode of spread to the pelvic bones, head of the femur, lower lumbar spine, and lungs Age, ethnicity, and family history are 3 nonmodifiable risk factors 28 Clinical Manifestations Collaborative Care Health Promotion • • • • • • • The incidence of prostate cancer rises markedly after age 50 AA have the highest incidence of prostate cancer of any ethnic group A high-fat diet is thought to be associated with an increased risk of prostate cancer Occupational exposure to chemicals may be associated with higher prostate cancer risk A history of BPH is not a risk factor Usually asymptomatic in the early stages Eventually, the patient may experience dysuria, hesitancy, dribbling, frequency, urgency, hematuria, nocturia, retention, interruption of urinary system, and inability to urinate • Pain in the lumbosacral area that radiates down to the hips or legs, when coupled with urinary symptoms, may indicate metastasis • The tumor can spread to pelvic lymph nodes, bones, bladder, lungs, and liver. • Once the tumor has spread to distant sites, the major problem becomes the management of pain • As the cancer spreads to the bones, pain becomes severe, especially in the back and legs because of compression of the spinal cord and destruction of bone • Early-stage prostate cancer is a curable disease in the majority of men • Collaborative care depends on the stage of cancer and overall health of patient Stage A (clinically unrecognized) • Watchful waiting with annual PSA and DRE • Radical prostatectomy • Radiation therapy (external beam, brachytherapy) Stage B (clinically intracapsular) • Radical prostatectomy • Radiation therapy Stage C (clinically extracapsular, localized to periprostatic area) • Radical prostatectomy • Radiation therapy • Hormone therapy • Orchiectomy Stage D (metastatic disease) • Hormone therapy • Orchiectomy • Chemotherapy • Radiation therapy to metastatic bone areas Prognosis is very unfavorable • Encourage patients to have annual prostate screening (PSA and DRE) starting at age 50 or younger if risk factors are present • Acute Intervention Ambulatory/Home Care • • • • • • • 29 AA men and other men with family history of prostate cancer should have annual PSA and DRE beginning at age 45 Provide sensitive, caring support for patient and family to help cope with diagnosis of cancer Preoperative and postoperative phases of radical prostatectomy are similar to procedures for BPH If patient is discharged with an indwelling catheter in place, the patient must be taught appropriate catheter care Instruct patient to clean urethral meatus with soap and water once a day, maintain high fluid intake, keep collecting bag lower than bladder at all times, keep catheter securely anchored to inner thigh or abdomen, and report any signs of bladder infections such as bladder spasms, fever, or hematuria If urinary incontinence is a problem, patients should be encourage to practice pelvic floor muscle exercises (Kegel exercises) at every urination and throughout day Continuous practice during the 4 to 6 week healing process improves success rate Management of pain is one of the most important aspects of nursing care for patients with stage D prostate cancer BPH • BPH is an enlargement of the prostate gland resulting from an increase in the number of epithelia cells and stromal tissue. • It is the most common problem of the adult male reproductive system. • Prostate hyperplasia does not predispose to the development of prostate cancer. • BPH develops in the inner part of the prostate. • This enlargement gradually compresses the urethra, eventually leading to partial or complete obstruction. • It is the compression of the urethra that ultimately leads to the development of clinical symptoms. • There is no direct relationship between the size of the prostate and degree of obstruction. • It is the location of the enlargement that is most significant in the development of obstructive symptoms. Risk factors • Family history • Environment • Diet • Higher risk for BPH has been found in association with a diet high in zinc, butter, and margarine. Health Promotion • The cause of BPH is largely attributed to the aging process; the focus of health promotion is on early detection and treatment • A yearly medical history and DRE for men over 50 yrs of age is recommended to provide early detection of prostate problems • Ingestion of alcohol and caffeine tends to increase prostatic symptoms because the diuretic effect of these substances increases bladder distention • Compounds found in common cough and cold remedies such as pseudoephedrine and phenylephrine often worsen the symptoms of BPH Acute Intervention 30 • The patient with obstructive symptoms should be advised to urinate every 2 to 3 hours and when first feeling the urge to minimize urinary stasis and acute urinary retention • Fluid intake should be maintained at a normal level to avoid dehydration or fluid overload; restricting fluid intake increases the chances of infection • If the patient increases fluid intake too rapidly, bladder distention can develop because of prostatic obstruction Preoperative • Urinary drainage must be restored before surgery; a urethral catheter such as a Coude (curvedtip) catheter may be needed to restore drainage • Antibiotics are usually administered before any invasive procedure; any infection of the urinary tract must be treated before surgery • Restoring urine drainage and encouraging a high fluid intake (2 to 3 L/day) are also helpful in managing infection • The patient needs to know how the surgery may affect sexual functioning • Inform patient that the ejaculate may be decreased in amount or totally absent • Retrograde ejaculation results in some degree Postoperative • The main complications following surgery are hemorrhage, bladder spasms, urinary incontinence, and infection • Patient will have standard catheter or a triple lumen catheter • Bladder irrigation is done to remove clotted blood from bladder and ensure drainage of urine • If the bladder is manually irrigated, 50 mL of irrigating solution should be instilled and then withdrawn with a syringe to remove clots that may be in the bladder and catheter • With continuous bladder irrigation (CBI), irrigating solution is continuously infused and drained from the bladder; the rate of infusion is based on the color of drainage • Ideally the urine drainage should be light pink without clots • The secretions that accumulate around the meatus can be cleansed daily with soap and water • Blood clots are expected for the first 24 to 36 hrs after surgery • Postoperative hemorrhage may occur from displacement of the catheter, dislodging a large clot, or increases in abdominal pressure • Traction on catheter may be applied to provide counterpressure (tamponade) on bleeding site in prostate, thereby decreasing bleeding • Instruct patient not to urinate around catheter because this increases the likelihood of spasm • If bladder spasms develop, check catheter for clots • The catheter is often removed 2 to 4 days after surgery • The patient should urinate within 6 hrs after catheter removal • Sphincter tone can be strengthened by Kegel exercises 10 to 20 times per hour while awake Ambulatory/Home Care 31 • Patient should be encouraged to practice starting and stopping the stream several times during urination to facilitate learning the pelvic floor exercises • In some instances, control of urine may never be fully regained • The patient can also be instructed to use a penile clamp, condom catheter, or incontinence pads or briefs to avoid embarrassment from dribbling Dietary intervention and stool softeners are important to prevent patient from straining while having bowel movements • Instructions include: 1. caring for indwelling catheter if one is left in place 2. managing urinary incontinence 3. maintaining oral fluids between 2 to 3 L/day\ 4. observing for S/S of UTI and wound infection 5. preventing constipation 6. avoiding heavy lifting (more than 10 lb) 7. refraining from driving or intercourse after surgery as directed by physician • Many men experience retrograde ejaculation because of trauma to internal sphincter; semen is discharged into bladder at orgasm and may produce cloudy urine when patient urinates after orgasm • Although some patients experience concerns regarding change in sexual function, this is not a universal concern; many men are comfortable with such changes and view them as appropriate for their age • The bladder may take up to 2 months to return to normal capacity • Instruct patient to drink at least 2 L of fluid/day and urinate every 2 to 3 hrs to flush urinary tract Advise patient to continue to have a yearly DRE if he has had any procedure other than complete removal of the prostate TREATMENT Transurethral resection of the prostate (TURP) DESCRIPTION - - Open prostatectomy - Use of excision and cauterization to remove prostate tissue cytoscopically Considered the most effective treatment of BPH Surgery of choice for men with large prostates ADVANTAGES - - DISADVANTAGES Best long-term relief of prostatic obstruction Erectile dysfunction unlikely - Bleeding Retrograde ejaculation Complete visualization of prostate and surrounding tissue - ED Bleeding Postoperative pain 32 - Transurethral incision of the prostate (TUIP) Transurethral microwave thermotherapy (TUMT) Transurethral needle ablation of the prostate (TUNA) Involves external incision with three possible approaches (retropubic, perineal, suprapubic) - Involves making transurethral slits or incisions into prostatic tissue to relieve obstruction - Effective for men with relatively little prostatic involvement Use of microwave radiating heat to produce coagulative necrosis of the prostate - Usually only indicated if prostate gland is very large - Risk of infection - Outpatient procedure Minimal complications Good for high risk patients No ED or retrograde ejaculation - Considered temporary solution to obstructive problem Urinary catheter needed after procedure - Low-wave radiofrequency used to heat the prostate causing necrosis - Outpatient procedure Short procedure ED and retrograde ejaculation are rare Short outpatient procedure ED and retrograde ejaculation are rare Precise delivery of heat to desired area Very little pain experienced by patient Short procedure Minimal bleeding Fast recovery time Very effective - - - Laser Prostatectomy Transurethral electrovaporization of prostate (TUVP) Urethral Stents - Procedure uses a laser beam to cut or destroy part of the prostate - Different techniques available: visual laser ablation of prostate, contact laser technique, interstitial laser coagulation Electrosurgical vaporization and desiccation are used together to destroy prostatic tissue Insertion of self-expandable metallic stent into urethra where enlarged area of prostate occurs - - Minimal risks Minimal bleeding and sloughing Safe and effective Low risk - - - Potential for damage to surrounding tissue Urinary catheter needed after procedure Urinary retention common Irritative voiding symptoms Hematuria - Postprocedure catheterization (up to 7 days) needed because of edema and urinary retention Delayed sloughing of tissue Takes several weeks to reach optimal effect Retrograde ejaculation - Retrograde ejaculation Intermittent hematuria - Stent may move Long-term experience is limited - 33 • • PNEUMONIA Acute inflammation of the lung parenchyma caused by a microbial agent Leading cause of death from an infectious disease in the U.S Etiology • Normal Defense Mechanisms • Factors Predisposing to Pneumonia ◊ Defense mechanisms become incompetent or are overwhelmed or overwhelmed by the virulence or quantity of infections agents ◊ Decreased consciousness depresses the cough, which may allow aspiration of Oropharyngeal contents into the lungs ◊ Tracheal intubation ◊ air pollution, cigarette smoking, viral upper respiratory infections, and normal Changes of aging ◊ Malnutrition ◊ Bed rest and prolonged immobility ◊ Chronic diseases • Acquistion of Organisms 1. Aspiration from the nasopharynx or oropharynx 2. Inhalation of microbes present in the air 3. Hematogenous spread from a primary infection elsewhere in the body Pathophysiology • Pneumococcal pneumonia is the most common cause of bacterial pneumonia • 4 characteristic stages of the disease process: 1. Congestion: outpouring of fluid into the alveoli→ organisms multiply in the serous fluid, and the infection is spread 2. Red hepatization: massive dilation of the capillaries, and alveoli are filled w/organisms, neutrophils, RBCs and fibrin 3. Gray hepatization: blood flow decreases, and leukocyte and fibrin consolidate in the affected part of the lung 4. Resolution Clinical Manifestations • CAP: fever, chills, cough productive of purulent sputum, and pleuritic chest pain, • Elderly or debilitated pt: confusion or stupor (possibly related to hypoxia) • Dullness to precussion, increased fremitus, bronchial breath sounds, and crackles, may be found • Gradual onset of dry cough, headache, myalgias, sore throat, N&V and diarrhea Complications • Pleurisy: inflammation of the pleura • Pleural effusion • Atelectasis: collapsed, airless alveoli. Clear w/effective coughing and deep breathing • Delayed resolution from persistent infection and is seen on x-ray as residual consolidation. 34 • • • Diagnostic Studies • • • • • • • Collaborative Care • • • • • • • • • • • Lung abscess Empyema: accumulation of purulent exudates in the pleural cavity. Requires antibiotic therapy and drainage of the exudates by a chest tube or open surgical drainage Pericarditis: from spread of the infecting organism from an infected pleura or via hematogenous route to the pericardium Arthritis: from systemic spread of the organism. Meningitis Endocarditis: organism attack the endocardium and the valves of the heart History and physical examination Chest x-ray: shows a typical pattern characteristic of the infecting organism and is an invaluable adjunct in the diagnosis of pneumonia. Gram stain of sputum: provides info on the predominant causative organism. Sputum culture and sensitivity test: if drug resistant pathogen or organism not covered by empiric therapy Pulse Oximetry or ABGs CBC, differential, and routine blood chemistries Blood cultures Prompt Rx w/ the appropriate antibiotic almost always cures bacterial and mycoplasma pneumonia Oxygen therapy for hypoxemia Analgesics to relieve chest pain Antipyretics for significantly elevated temp During acute febrile phase, pt’s activity should be restricted, and rest should be encouraged and planned Influenza vaccine is considered a mainstay of prevention and is recommended annually for use in the individual considered to be at risk Pneumococcal Vaccine 1. Has chronic illnesses such as lung and heart disease and DM 2. Recovering from a severe illness 3. In a long term care facility ◊ Revaccination is recommended every 5 years for immunosuppressed individuals Drug Therapy ◊ Main problem problems are the development of resistant strains of organisms and the pt’s hypersensitivity or allergic reaction to certain antibiotics ◊ Empiric Rx w/broad spectrum antibiotics ◊ Category 1: either azithromycin (Zinthromax) or clarithromycin (Biaxin) ◊ Doxycycline (Vibramycin) recommended for pt who is allergic to marolides, but is not reliably active against pneumococcus organisms 35 • Nursing Management • • Types of Pneumonia • • ◊ Clinical response evaluated by factors such as change in fever, sputum purulence, leukocytosis, oxygenation or x-ray patterns Nutritional Therapy ◊ fluid intake of at least 3 L per day ◊ At least 1500 cals per day to provide energy for the increased metabolic processes ◊ Small, frequent meals are better tolerated Health Promotion ◊ practice good health habits, such as proper diet and hygiene, adequate rest, and regular exercise ◊ avoid exposure to URI ◊ Pts w/altered consciousness place them in positions (side-lying, upright) that will prevent or minimize the risk of aspiration ◊ turn and reposition pt q2h ◊ Avoid overmedication w/narcotics or sedatives, which can cause a depressed cough reflex and accumulation of fluid in lungs ◊ Practice strict medical asepsis and adherence to infection control Ambulatory and Home Care ◊ reassure that complete recovery is possible ◊ Emphasize the need to take all of the prescribed drug and to return for follow up ◊ Drug-drug and the food-drug interactions should be taught ◊ Deep breathing exercises should be practiced for 6-8wks Community-Acquired Pneumonia (CAP) ◊ lower respiratory tract infection of the lung parenchyma w/onset in the community or during the first 2 days of hospitalization ◊ Highest in the winter months ◊ Smoking is an important risk factor ◊ S.pneumoniae ◊ Category 1: outpatients w/no hist of cardiopulmonary disease, no modifying factors ◊ Category 2: Outpatients w/cardiopulmonary disease and/or modifying factors ◊ Category 3: inpatients, not admitted to ICU ◊ Category 4: ICU admitted pts ◊ Modifying risk factors: age > 65, alcoholism, multiple medical comorbidities, and immunosuppressive disease Hospital Acquired Pneumonia ◊ occurring 48 hrs or longer after hospital admission and not incubating at the time of hospitalization 36 ◊ Has the highest morbidity and mortality rates of any nosocomial infection ◊ predisposing factors: immunosuppressive therapy, general debility and endotracheal intubations ◊ Group 1: pts w/o unusual risk factors who have mild to moderate HAP w/onset at any time during hospitalization or severe HAP of early onset ◊ Group 2: pts w/specific risk factors who have mild to moderate HAP occurring any time during hospitalization ◊ Group 3: Pts w/sever HAP either of early onset w/specific risk factors or of late onset • Fungal Pneumonia • Aspiration Pneumonia ◊ sequelae occurring from abnormal entry of secretions or substances into the lower airway • Opportunistic Pneumonia ◊ Pneumocystis carinii ◊ Rx trimethoprim-sulfamethoxazole (Bactrim) ◊ Risks: severe protein cal malnutrition, immune defiencies, transplants treated w/immunosuppressive drugs, chemo, radiation and corticosteroids • • • • TUBERCULOSIS Infectious disease cause by Mycobacterium tuberculosis Involves lungs, but also larynx, kidneys, bones, adrenal glands, lymph nodes, and meninges Kills more pple worldwide than any other infectious disease Seen disproportionately in poor, underserved and minorities • Homeless pple, residents of inner city neighborhoods, foreign born persons, older adults, institutions, injection drug users, socioeconomically disadvantaged, and medically underserved of all races are at risk Etiology and Patho • Usually spread from person to person via airborne droplets • Repeated, close, prolonged exposure to infected person • Can’t be spread by fomites • When bacilli inhaled→ pass down bronchial system and implant on respiratory bronchioles or alveoli→ multiply w/no initial resistance from host→ spred through lymphatic channels to regional lymph node and via thoracic duct to circulating blood while cellular immune response is being activated • Lower lungs initial site of bacterial implantation • Table 27-7 Clinical Manifestations • Usually free of symptoms in early stages • Systemic: fatigue, malaise, anorexia, weight loss, low grade fever, night sweats 37 • Complications Diagnostic Studies Collaborative Care Pulmonary manifestation: cough that becomes frequent and produces mucoid or mucopurulent sputum, chest pain • Chills, flulike symptoms, pleuritic pain, and productive cough • Military TB ◊ blood invasion and spread to all body organs Pleural Effusion and Empyema ◊ fluid accumulation in pleural area ◊ Pus in the lungs Tuberculosis Pneumonia ◊ tubercle bacilli discharged from the liquefied necrotic lesion into the lung or lymph nodes • Other organ involvement • Tuberculin Skin testing ◊ positive reaction occurs 2-12 wks after the initial infection, corresponding to time needed to mount an immune response ◊ PPD used primarily to detect the delayed hypersensitivity response ◊ positive reaction indicates the presence of tuberculosis infection, BUT does not show whether the infection is dormant or active • Chest x-ray ◊ Important, but it’s not possible to make a diagnosis of TB solely on the basis of this ◊ This is b/c other diseases can mimic the x-ray appearance of TB • Bacteriologic Studies ◊ essential for establishing a dx ◊ usually the 1st bacteriologic evidence of the presence of tubercle bacilli ◊ 3 consecutive sputum specimens collected on diff days are obtained and sent for smear and culture ◊ most accurate means of dx is a culture technique ◊ Disadvantage: may take 6-8wks for mycobacterium to grow ◊ Nucleic acid amplification (NAA): rapid diagnostic test. Results available in few hrs. • Mainstay is drug therapy • Drug Therapy ◊Active disease 38 Nursing Management • • • • ▪ Rx consists of combination of at lest four drugs ▪ 5 primary drugs used are INH, rifampin (rifamate), pyrazinamide, streptomycin, and ethambutol (myambutol) ▪ Pts on antiretroviral drugs for HIV can’t take rifampin b/c it can impair the effectiveness of antiretroviral drugs ▪ Table 27-10: Regimen options ▪ Follow up care to ensure adherence to the Rx regimen ▪ Noncompliance is a major factor ▪ Critical to teach pts about the S.E of the drugs and when to seek prompt medical attention ▪ Major S.E. of INH, rifampin and pyrazinamide is hepatitis ▪ Monitor liver function test ◊ Latent tuberculosis infection ▪ occures when an individual becomes infected w/M.tuberculosis but doesn’t become acutely ill ▪ INH generally used ▪ qd for 6-9 months ▪ Indications for Rx: Table 27-11 ◊ Vaccine ▪ bacilli Calmette-Guerin ▪ efficacy not clear Assess for productive cough, night sweats, afternoon temp elevation, weight loss, pleuritc chest pain, and crackles over apices of lungs Health Promotion ◊ selective screening programs in known risk groups ◊ Chest x-ray for a person w/positive tuberculin skin test to assess presence of TB ◊ Identify contacts of individual to be assessed for possibility of infection Acute Intervention ◊ In hospital: 1. placed on respiratory isolation 2. receive four drug regimen and 3. receive an immediate medical workup ◊ negative pressure isolation room ◊ Pt should be taught ot cover nose and mouth w/tissue every time he/she coughs, sneezes or produces sputum ◊ Tissues should be thrown in a paper bag and disposed of w/trash, burned or flush down the toilet Ambulatory and Home Care ◊ develop a therapeutic, consistent relationship w/ each pt 39 ◊ notify public health department if drug compliance is questionable ◊ reassure TB can be cured if the prescribe regimen is followed ASTHMA • Chronic Inflammatory disorder of the airways in which inflammation causes varying degrees of obstruction in the airways • Inflammation causes recurrent episodes of wheezing, breathlessness, chest tightness and cough, particularly at night and early morning • African Americans have a higher hospitalization rate and mortality rate from asthma than whites Triggers of Asthma Attack Allergens ◊ Pollen, house dust mite, animal danders, perfumes etc ◊ Attach to IgE receptors on mast cells→ mast cell degranulation at second exposure • Exercise ◊ after vigorous exercise ◊ bronchospasm, SOB, cough and wheezing ◊ perform warm up of stretching for 2-3 mins before exercise ◊ Inhale meds 10-20 mins before exercise • Respiratory Infections ◊ most common participating factor ◊ avoid pple w/colds or flu and get yearly influenza vaccinations ◊ Avoid taking OTC cold remedies unless approved by Dr • Nose and Sinus Problems ◊ Allergic rhinitis: can be seasonal or perennial ◊ Nasal polyps • Drugs and Food Additives ◊ NSAIDs ◊ foods, beverages and flavorings containing salicylic acid ◊ β adrenergic blockers: prevent bronchodilation ◊ ACE inhibitors produces cough ◊ Tartarazine (yellow dye #5), vitamins and sodium metabisulfite (food preservative in fruits, beer and wine) • GERD • Emotional Stress Patho • Hallmarks are airway inflammation and non-specific hyperirritability or hyperresponsiveness • Reduction in airway diameter and an increase in airway resistance related to mucosal inflammation, constriction of bronchial smooth muscle, and excess production of mucus • Clinical Manifestations • • • • Complications • • • • 40 Bronchial smooth muscle hypertrophy, basement membrane thickening, mucous glad hypertrophy, thick and tenacious sputum, hyperinflation, and air trapping in the alveoli leading to increased work of breathing Characteristic clinical manifestations are wheezing, cough, dyspnea, and chest tightness after exposure to precipitating factor or trigger Wheezing unreliable sign to gauge te severity of an attack Severely diminished breath sounds “Silent chest” ominous sign indicating severe obstruction and impending respiratory failure Restlessness, increased anxiety, inappropriate behavior, increased pulse and BP, and pulsus paradoxus (drop in systolic during the inspiratory cycle >10 mm hg) Resp rate increased (>30 bpm) w/use of accessory muscles Hyperresonance in lungs and inspiratory or expiratory wheezing upon auscultation Classification of asthma Table 28-2 Status Asthmaticus ◊ severe, life threatening asthma attack that is refractory to usual Rx and places pt at risk for developing respiratory failure ◊ Causes: viral illness, ingestions of aspirin or other NSAIDs, emotional stress, increase in environmental pollutants or other allergens exposure, abrupt discontinuation of drug therapy, abuse of Diagnostic Studies Collaborative Care aerosol med, and ingestion of β adrenergic blockers ◊ CM similar to asthma, but are more severe and prolonged ◊ extreme anxiety, fear of suffocation, severely increased work of breathing and daphoresis are Common ◊ HTN, sinus tachycardia and ventricular arrhythmias may occur ◊ Complications: pneumothorax, pneumomediastinum, acute cor pulmonale w/ right ventricular failure and severe respiratory muscle fatigue ◊ Death usually the result of respiratory arrest or cardiac failure • History and Physical assessment • Pulmonary function studies including response to bronchodilator therapy • Peak expiratory flow monitoring • Chest x-ray • Measurement of ABGs or oximetry • Allergy test testing • Blood level of esinophils and IgE • Education for an active partnership w/patients remains the cornerstone of asthma management and should be carried out by health care providers Mild Intermittent and Persistent Asthma ◊ avoid triggers of acute attacks and premedicate before exercising 41 ◊ Mild: use inhaled β adrenergic agonists, cromolyn (Intal) or nedocromil (Tilade) before exercising or Drug Therapy when anticipating exposure to allerges ◊ Moderate: regular or maintainence use of inhaled anti-inflammatory meds. Corticosetriods, cromolyn and nedocromil ◊ Persistent: inhaled or oral corticosteroids, β2 adrenergic agonists and theophylline Acute Asthma Episode ◊ O2 therapy started immediately, monitored by pulse ox ◊ Initial therapy: inhaled β2 adrenergic agonists administered by MDI. Every 20mins to 4 hrs ◊ Corticosteriods if initial response insufficient Status Asthmaticus ◊ focuses on correcting hypoxemia and improving ventilation ◊ typical MDI use is 2-6 puffs every 5-20mins ◊ Continous monitoring critical ◊ inhaled β2 adrenergic drugs or anticholinergic agents ◊ IV aminophylline and corticosteriods ◊ O2 by mask or nasal prongs ◊ IV fluids ◊ IV magnesium ◊ heliox therapy Antiinflammatory Drugs ◊ Corticosteroids: most potent and effective anti-inflammatory med currently available. Suppress inflammatory response ▪ block the late phase response and subsequent bronchial hyperresponsiveness ▪ Onset action approximately 3-6hrs after oral admin ▪ oropharyngeal candidiasis, hoarseness and dry cough are local adverse effects caused by inhalation of corticosteroids ▪ insomnia, heartburn, mood swings, blurry vision, headache, increased appetite and weight gain are side effects of oral corticosteroids ◊ Cromolyn and nedocromil: inhibit the immediate response from exercise and allergens and prevent the late phase response ◊ Leukotrene modifiers: interfere with the synthesis or block the action of leukotrienes Bronchodilators: 3 classes ◊ β adrenergic agonist: short term relief and choice Rx for acute exacerbations of asthma ▪ Onset w/in mins and effective for 4-8 hrs ▪ If used often may produce tremors, anxiety, tachycardia, palpitations, and nausea ◊ Methylxanthines: bronchodilation, which is useful in the early phase response ◊ Anticholinergic drugs: inhibit only the component of bronchoconstriction related to the 42 Nursing Management parasympathetic nervous system ▪ used in combination with other bronchodilators ▪ onset is slower than β2 adrenergic agonists, peaking at 1 hr and lasting longer, usually up to 4-6 hrs. ◊ Monoclonal antibody of IgE: Omalizumab (Xolair) decreases circulating free IgE levels ▪ prevents IgE from attaching to mast cells, thus preventing the release of chemical mediators ▪ Used to treat patients who have been inadequately controlled with inhaled corticosteroids Patient Teaching related to drug therapy ◊ Info about med should include the name, dosage, method of admin and schedule ◊ Major factors determining success in asthma management is the correct administration of drugs ◊ Inhalation is preferred b/c a lower dose is needed and systemic effects are reduced ◊ It is important to explain to the pt the importance and purpose of taking the long term therapy regularly, emphasizing the maximum improvement may take more than 1 week Nonprescription combination drugs ◊ Usually combos of a bronchodilator, an expectorant and a sedative ◊ Generally should be avoided ◊ Some dangers of these drugs: ▪ Epinephrine, found in Primatene spray, acts only for short time and may increase the pt’s HR and BP. Not recommended for use ▪ Teophylline, taken with other xanthines including caffeine, has an additive effect. Side effects include CNS and cardiovascular effects, vomiting, nausea and anorexia ▪ A combo of ephedrine and theophylline causes synergistic stimulation of CNS and cardio system. Side effects include nervousness, heart palpitations and arrhythmias, tremors, insomnia and increases BP • Health Promotion ◊ Pt should be taught to identify and avoid known personal triggers for asthma and irritants ◊ use dust covers on mattresses can significantly reduce exposure to dust mites ◊ dress properly w/carves or using a mask to reduce the risk if cold air can’t be avoided ◊ aspirin and NSAIDs should be avoided ◊ encouraged to maintain a fluid intake of 2-3 L per day, good nutrition and adequate rest • Acute intervention ◊ monitor respiratory and cardiovascular systems ◊ administer O2, bronchodilators, chest physiotherapy, and meds and ongoing pt monitoring ◊ encourage slow breathing using pursed lips for prolonged exhalation during acute attack • Ambulatory and Home Care ◊ good nutrition and physical exercise are important 43 ◊ Involve family in the management plan ◊ emphasize the importance of monitoring PEFR daily because asthma tends to worsen gradually over time ◊ Counseling may be indicated to help pt and family ◊ Relaxation therapy may help pt relax respiratory muscles and decrease the respiratory rate • • • EMPHSEMA AND CHRONIC BRONCHITIS COPD is a disease state characterized by the presence of airflow obstruction caused by chronic bronchitis or emphysema Chronic bronchitis is the presence of chronic productive cough for 3 months in each of 2 successive years in a pt Emphysema is a abnormal enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and w/o obvious fibrosis Etiology • Cigarette Smoking ◊ major risk factor ◊ remains the most preventable cause of premature death in U.S ◊ smoke causes hyperplasia of cell, which results in increased mucous production ◊ reduces O2 carrying capacity • Infection ◊ impair normal defense mechanisms, making the bronchioles and alveoli more susceptible to injury • Heredity ◊ α1-Antitrypsin (AAT) deficiency is the only known genetic abnormality that leads to COPD • Aging ◊ results from changes in the lung structure, thoracic cage and respiratory muscles Patho • Emphysema ◊ hyperinflation of alveoli ◊ destruction of alveolar walls ◊ destruction of alveolar capillary walls ◊ narrowed, tortuous, small airways ◊ loss of lung elasticity ◊ 2 major types 1. Centrilobular: area of involvement is the central part of the lobule. Respiratory bronchioles enlarge→ wall are destroyed→ bronchioles become confluent. Often associated w/ chronic bronchitis 2. Panlobular: distention and destruction of the whole lobule. Usually found in pple w/AAT deficiency • Chronic Bronchitis ◊ hyperplasia of mucous-secreting glands in the trachea and bronchi ◊ increase in goblet cells ◊ disappearance of cilia 44 Clinical Manifestations • • Complications • • • • Diagnostic Studies • • • • • • • • • ◊ chronic inflammatory changes and narrowing of small airways ◊ altered function of alveolar macrophages, leading to increase bronchial infections ◊ alveolar structure and capillaries are normal ◊ chronic inflammation is the primary pathologic mechanism Emphysema ◊ dyspnea is an early symptom ◊ barrel chest ◊ Hypoxemia maybe be present (exercise) and hypercapnia develops later in the disease ◊ Underweight ◊ protein calorie malnutrition Chronic Bronchitis ◊ frequent, productive cough during most winter months is the earliest symptom ◊ Bronchospasms at the end of paroxysms of coughing ◊ normal weight or heavyset, w/ ruddy appeareance ◊ hypoxemia and hypercapnia result from hypoventilation cause by increased airway resistance ◊ bluish-red colored skin from polycythemia and cyanosis ◊ Hgb 20 g/dl or more Comparison of both Table 28-15 Cor Pulmonale ◊ hypertrophy of the right side of the heart resulting from pulmonary HTN ◊ distended neck veins, hepatomegaly ◊ Management: continuous low-flow O2, dietary salt restriction Acute Exacerbations of Chronic Bronchitis ◊ CM: worsened cough, hemoptysis, wheezing, increased SOB, and changes in the amount, color, consistency or viscosity of the sputum ◊ Rx w/antibiotics, corticosteroids, humidification, and postural drainage Acute Respiratory Failure ◊ Respiratory tract infection or acute bronchitis most common PUD and GERD Pneumonia To determine the major disease component of COPD, severity of the disease and the impact of disease on the pt’s quality of life H&P examination Pulmonary function tests Chest x-ray ABGs ECG Exercise testing w/oximetry 45 Collaborative Care • • • • • • • • • • Nursing Management • Echocardiogram or cardiac nuclear scans Primary goals are to 1) improve ventilation, 2) promote secretion removal, 3) prevent complications, 4) promote pt comfort and participation in care, and 5) improve quality of life as much as possible Have influenza vaccine yearly and pneumococcal vaccine every 5 yrs Most common antibiotics are amoxicillin, amoxicillin w/clavulanate, cipro, erythromycin and trimethoprim-sufamethoxazole (Bactrim) Smoking Cessation ◊ most significant factor in slowing the progression of the disease Drug Therapy ◊ Bronchodilator therapy ◊ Cortiosteriods O2 Therapy Surgical Therapy for COPD ◊ lung volume reduction surgery: decreases airway obstruction ◊ lung transplantation Respiratory Therapy ◊ PURSED-LIP BREATHING Purpose is to prolong exhalation and prevent bronchiolar collapse and air trapping • Breath in slow through nose • Purse lips as if drinking through a straw • Breath out slowly and evenly through pursed-lips • Inhale through nose 2—3 sec • Exhale more slowly for 4-6 sec – O2 sats Nutritional Therapy ◊ Difficult to maintain – especially acute care ◊ Frequent small meals ◊ Vitamins ◊ Monitor electrolytes and albumin levels ◊ H&H, decrease salt intake ◊ Allow extra time for eating ◊ Adequate fluids Health Promotion ◊ Counseling and treatment should be offered o Clear and truthful information o Assistance to attend a program o Quit date o Means to get nicotine patches o Reassurance that quitting is difficult and may require multiple attempts 46 • Ambulatory and Home Care ◊ SLEEP AND REST ▪Check O2 sat levels - >90% ▪Elevate the HOB ▪Clear secretions prior to sleep ▪May need an increase in O2 during sleep ◊ Pt should be encouraged to walk 15-20 mins a day w/gradual increases DVT Clinical Manifestations Risk factors Complications Diagnostic Studies Collaborative Care • May have no symptoms or have unilateral leg edema, extremity pain, warm skin, erythema and a systemic temp greater than 100.4 F • Positive Homans’ sign but is unreliable • Involvement of inferior vena cava: lower extremities may be edematous and cyanotic • Involvement of superior vena cava: upper extremities, neck, back and face • Venous Stasis: obesity, CHF, Prolonged immobility, Stroke etc • Endothelial Damage: abd and pelvic surgery, hst of dvt, IV drug abuse, Indwelling femoral vein catheter etc. • Hypercoagulability of Blood: Cigarette smoking, dehydration or malnutrition, sepsis, Antithrombin III deficiency • Pulmonary embolism: life threatening • Chronic venous insufficiency: from valvular destruction, allowing retrograde flow of venous blood • Phlegmasia cerulean dolens: swollen, blue, painful leg. Rare complication • Blood Lab Studies: platelet count, bleeding time, INR, APTT, D-dimer • Noninvasive Venous studies: venous Doppler evaluation, Duplex scanning • Venogram • Lung Scan • Pulmonary Angiogram • Spiral CT scan Prevention and prophylaxis: ◊ early mobilization ◊ If on bed rest instruct pt to change position, dorsiflex their feet, and rotate their ankles q2-4h ◊ Elastic compression stocking ◊ Intermittent compression devices (ICDs): for hospitalized pts at moderate, high risk for DVT and PE Nonpharmacologic Therapy: ◊ elevation of the affected extremity about the level of heart ◊ Warm compresses 47 Nursing Management Drug Therapy: ◊ Anticoagulants: heparin, LMWHs, hirudin derivatives, and coumarin compunds Surgical Therapy ◊ Venous Thrombectomy ◊ Inferior vena cava interruption • Acute Intervention ◊ closely observe for indication of bleeding when receiving anticoagulants ◊ Assess urine for gross or microscopic hematuria ◊ Review w/pt any meds currently being taken that my interfere w/anticoagulant therapy ◊ Monitor PTT, INR, Hgb, Hct and platelet levels • Ambulatory and Home Care ◊ evaluate the pt’s psychologic response ◊ discharge teaching should focus on elimination of modifiable risk factors for DVT, importance of compression stockings, monitoring of lab values, med instruction and guidelines for follow up ◊ Avoid prolonged standing or sitting in the motionless, leg dependent position ◊ Teach pt and family S&S of PE ◊ Well balanced diet is important b/c Ca and Vit E play active roles in the clotting mechanism ◊ Proper hydration HIV/AIDS Transmission –Viral load – number of HIV particles in the blood –Fragile virus – contact with infected body fluids • Blood, semen, vaginal secretions, and breast milk –Transmission occurs through • Sex, blood exposure & perinatal –Not transmitted through any casual contact –High viral load first 2-6 months after infection and then in later stages –Health care workers at low risk –Most common mode of transmission is sexual contact with an infected person –Greatest risk for exposure of HCW is through puncture (needle-sticks) wounds – 0.3%-0.4% –Higher the patients viral load the greater the risk –Deep puncture wounds and hollow-bore needles with visible blood –Children – perinatal transmission Pathophysiology –HIV affects human cells with CD4 receptors on their surfaces • Lymphocytes, monocytes, macrophages, astrocytes and oligodendrocytes 48 Clinical Manifestations Chronic HIV Infection Diagnostic Studies Drug Therapy • HIV immune dysfunction caused by damage to and destruction of CD4 T-cells –Normal CD4 T cells per microliter of blood – 800-1200 –Normal life span of a CD4 T-cell is 100 days - HIV – 2 days –Immune problems begin to occur when CD4 levels drop below 500 –Seroconversion – Development of HIV-specific antibodies –Flu-like symptoms – fever, sore throat, swollen glands, headache, malaise, nausea, etc. –Acute Retroviral Syndrome – 1-3 weeks following initial exposure (includes sx such as fever, swollen lymph glands, sore throat, nausea, malaise, muscle pain, diarrhea, headache, rash) –Early – CD4 count is >500, VL is low (can be asymptomatic, but can have fatigtue, low grade fever, headaches, night sweats and PGL) –Intermediate – CD4 count drops to 200-500, VL is high • Common infection – Candida (oral thrush) (leukoplakia) –Late – diagnosis of AIDS after meeting CDC specific criteria – Table 14-1 on page 268 • CD4 T cells < 200 • Development of OIs (fungal, bacterial, viral, protozoal infections) –Detection of HIV-specific antibodies • Best test but 2 month lag time for positives –Table 14-3 on page 271 (HIV antibody test screening process) • EIA is done to detect serum antibodies that attach to HIV antigens • If EIA is positive, the test is repeated • If continuously positive, then take Western blot test or IFA • Western Blot uses purifies HIV antigens electrophoresed gels • IFA is used to identify HIV infected cells w/a fluorescent light • Blood that is reactive in all 1st 3 tests is reported as HIV+ –Disease progression is followed with CD4+-T cell counts –EIA, Western Blot (most common, definitive), IFA –Goals of therapy: • Dec HIV-RNA levels to 50 copies or less • Maintain or raise CD4 levels to > 200 • Delay HIV related opportunistic infections –Education and strict adherence to the protocol is imperative – resistance can happen rapidly –Nucleoside Reverse Transcriptase Inhibitors (NRTI’s) • Mechanism of axn: inserts a bit of protein into the developing HIV DNA chain, blocking further development of the chain and leaving the strand of HIV DNA incomplete 49 Nursing Management Nursing Interventions • AZT, Retrovir • SE: N&V, anemia, leucopenia, myopathy, fatigue, headache –Nonucleoside Reverse Transcriptase Inhibitors (NNRTI’s) • Mechanism of axn: combines w/reverse transcriptase enzyme to block the process needed to convert HIV RNA into HIV DNA • Viramune • SE: rash, stevens-johnson syndrome, hepatitis, inc transaminase levels –Nucleotide Reverse Transcriptase Inhibitors • Mechanism of axn: inhibit action of reverse trancrioptase • Viread • SE: N&V, vaginal irritation, renal impairment –Protease Inhibitors (PI’s) • Mechanism of axn: prevent the protease enzyme from cutting HIV proteins into the proper lengths needed to allow viable virons to assemble and bud out from the cell membrane • Viracept, indinavir • SE: Diarrhea, Nausea, Flatulence, nephritis, kidney stones –Fusion Inhibitors • Mechanism of axn: prevent binding of HIV to cells, thus preventing the entry of HIV into healthy cells • Fuzeon • SE: skin irritation at injection site, fatigue, nausea, neuropathy –Review pages 272 and 273 including the tables –Assessment of risk factors • Four major questions 1. Ever had an blood transfusion? If so before 85? 2. Ever shared needles, syringes or other injecting equipment 3. Ever had a sexual experience? 4. Ever had and STD? –Nursing Diagnosis – dictated by multiple variables: stage, presence of specific etiologic probs, and social factors –Planning – affects entire holistic person (social, economic, emotional, spiritual, and physical) –Assist with the following: • • • Adhere to drug therapy Promote healthy lifestyle Prevent opportunistic disease 50 Implementation Complications • Protect others from the disease • Maintain, develop healthy support systems • Activity, productivity • Acceptance of disease , illness, disability, death – spirituality –Health promotion – prevent disease –Prevention of HIV infection – preventable –Safe sex –Risk related to drug use –Risk associated with perinatal transmission –Risk at work – post-exposure prophylaxis shown to significantly reduce risk –Pneumocystis carinii pneumonia (fungus) –Cryptococcal meningitis (yeast) • Stiff nect • Sensitivity to light • Ataxia • Flu symptons –Mycobacterium avium complex • Causes GI problems (diarrhea, abd pain) • Spleen and lymph nodes • Bone marrow –Kaposi Sarcoma • Neoplastic lesions on skin and oral mucosa –Cytomegalovirus • Esophagitis • Colitis • Pneumonia • Rentinitis (leads to blindness) HYPERTENSION • • • • • Sustained elevation of BP SBP > 140. DBP > 90. Diagnosis requires elevated readings on 3 occasions over several weeks AAs, Puerto Ricans, Cubans, and Mexican Americans – highest incidence. 51 • AAs –highest incidence, develop at younger age, AA women particularly high, more aggressive with more end-organ damage, higher mortality, AAs in SE US higher incidence, AAs produce less renin = ↓ response to ACE inhibitors (stops conversion of Ang I to Ang II) Mechanisms involved in • BP= CO x SVR (Systemic Vascular Resistance) regulating BP • CO= Stroke volume x HR for 1 minute (Total blood flow through the systemic ciculation per minute) • SVR= force opposing the movt of blood within the blood vessels. • Sympathetic nervous system - Inc SNS activity= Inc HR and Contractility, Vasoconstriction in peripheral arterioles, releases renin from kidneys. - Baroreceptors (nerve cells): senses changes in BP, and transmitted to vasomotor centers in the brainstem. - Norepinephrine activates receptors located in SA node, myocardium, and vascular smooth muscle which cause inc contractions (inotropic) and inc HR (chronotropic) and inc speed of conduction. • Baroreceptors are specialized nerve cells loc in the carotid arteries and when stimulated by an Inc in BP, sends impulses to the vasomotor center in the brainstem. A fall in BP sensed by baroreceptors causes an activation of SNS. • Vascular endothelium is a single layer that lines the blood vessels. Endothelin which is prodeuced by endothelial cells is a potent vasoconstrictor. • Renal system. The kidneys contribute to BP regulation by controlling sodium excretion and ECF volume. Na retention- Water Retention- inc ECF voume - Inc venous return to the heart- Inc SV- Inc BP- Inc CO. The renin-angiotensin system plays an imp role as well. •Endocrine system.Stimulation of the SNS results in release of Epinephrine along with the norepinephrine by adrenal medulla. An inc in blood sodium stimulates the release of ADH. ADH increase the ECF volume, elevates BP. Classifications •Primary hypertension (95% of all cases): cause is uknown but some contributing factors include: inc SNS ativity, Inc Na retaining hormones, inc sodium intake, DM, and elevated allcohol intake. o 50 million people in US. o Prevalence increases with age. o Incidence higher in African-Americans. o Develops at earlier age in African-Americans. o African-Americans have higher mortality rate at every level of HTN. o More prevalent in less educated. o More men than women until age 55. o 55 to 75 equal (men and women). o Over 75 more women o RISK FACTORS. ▪ Heredity. ▪ H20 and Na+ retention. (The more salt, the greater the circulating volume in IVS) 52 Complications ▪ Altered Renin-Angiotensin System. ▪ Stress. ▪ Increased SNS. (Fight or Flight response going on all the time) ▪ Insulin resistance and hyperinsulinemia. ▪ Endothelial cell dysfunction. o MANIFESTATIONS ▪ Usually asymptomatic (silent killer). ▪ Symptoms signify either secondary causes or effects of sustained elevated BP on endorgans. • CAD. (Major risk factor) • LVH. High BP increse heart worload leading to LVH can lead to Heart Failure • Cerebrovascular disease. Atherosclerosis is the most common cause • Peripheral vascular disease. • Renal insufficiency. •Secondary hypertension (<5% adults; > 80% in children; specific cause). • Causes. 1. Coarctation of the aorta. 2. Renal disease. 3. Endocrine disorders. 4. Neurological disorders. 5. Sleep apnea. 6. Medications. 7. Pregnancy. • Clinical findings. 1. Unprovoked hypokalemia. 2. Abdominal bruit. 3. Variable pressures with Hx of tachycardia, sweating and tremor. 4. Family history of renal disease. • Asymptomatic until severe. • Symptoms secondary to pressure in target organs • Increased workload of the heart can possibly cause CHF 53 Diagnostic studies Collaborative Care •CAD. •LVH. •CHF. •CV disease. (Atherosclerosis is the most common ause of CVD) •PVD.( a classic sx of PVD: intermittent claudication -muscle pain)) •Nephrosclerosis. HTN is one of the leading causes of end stage renal disease. Renal dysfuncn is the direct result of ischemia caused by narrowed lumen of BV. •Retinal damage. Only plac ein body where the vessels can be directly visualized, it proides imp info about the severity and duration of the HTN. • H&P. • UA. • BUN, serum creatinine.= renal involvement • Serum electrolytes, esp. K+. checks for hyperaldosteronism (secondary HTN0 • Blood glucose. (DX of DM) • Serum cholesterol & triglycerides. • Uric acid. • EKG. (provides baselines info about cardiac status; heart and lungs are married) • Echocardiogram. (size and structure of the heart) • Eye Exam. • Assess BP several months before initiating TX (must have 3 consistent readings) • Decide to TX based on overall CV risk. • Lifestyle modifications foundation for TX. • TX primary & systolic HTN up to age 85. • LIFESTYLE MODIFICATIONS (takes at least 3 months) • Dietary changes: restrict Na, caffeine, reduce cholesterol and saturated fats, maintain dietary intake of K, Ca, Mg and restrict calories if overweight • Limitation of alcohol intake.(Excessive alcohol consumption is the most frequent cause of secondary HTN) • Regular physical activity. (30 mins or more of physical activity QD) • Avoidance of tobacco (smoking & chewing). • Modify ETOH intake. • Stress management. • DRUG THERAPY • GOAL: BP < 135/85, young adults, mild HTN. • <140/90, older adults with elevated SBP & DBP. • <140, older adults with ISH. • 2 main actions of meds- 54 1. Reduction of systemic vascular resistance. 2. Reduction of volume of circulating blood. • Diuretics: promote water and NA excretion (Lasix) • Adrenergic (sympathetic) inhibitors: Decrease fight or flight responses; inhibit norepinephrine release. • Vasodilators: Decrease BP by relaxing smooth muscle. • Angiotensen inhibitors: prevents conversion on Ang I to Ang II • Calcium channel blockers: Inc Na excretion, prevents movt of Ca into cells. • All patients with stages 2 or 3 not controlled by lifestyle changes. • Causes for Lack of Response - Nonadherence to Therapy (cost of med, dementua, inconvenient dosing, lack of involvement, instructions not clear) - Drug Related Causes (dosages too low, rapid inactivation, drug interaxns, inapprop combinations) - Associated Conditions (inc obesity, alcohol intake more than 1 oz/day) - Secondary HTN (renal insuff, primary aldosteronism) - Volume Overload (Inadequate diuretic therapy, excess Na intake, fluid retention from red BP) - Preogressive renal damage - PseudoHTN • SIDE EFFECTS • Hyperuricemia, hyperglycemia, hypokalemia-thiazide & loop diuretics. • Hyperkalemia-potassium-sparing diuretics and ACE inhibitors. • Impotence with many diuretics. • Orthostatic hypotension & sexual dysfunction-adrenergic inhibiting agents. • Tachycardia & orthostatic hypotension-vasodilators & angiotensen inhibitors. 55 Classification/Drugs to Know Nursing Management Gerontologic Considerations • • • • • Thiazide diuretics: Inhibit NaCl reabsorption, Inc excretion Na and Cl, Dec in ECF Loop diuretics: Inc excretion Na and Cl Potassium-sparing diuretics: Reduce K and Na exchange, Inhibit the Na retaining and K excreting effects. Centrally-Acting Adrenergic Antagonists: Reduces sympathetic outflow from CNS. Peripherally-Acting Adrenergic Antagonists: Prevents peripheral release of norepinephrine, resulting in vasodilation, lowers CO and SBP more than DBP. • Alpha Blockers: Block adrenergic effects producinf peripheral vasodilation (Dec SVR and BP) • Beta Blockers: Reduced BP by antagonizing B-adrenergic effects. Dec CO . Dec renin secretion by kidneys. • Combined Alpha/Beta Blockers: Produce peripheral vasodilation, Dec HR, Red CO, SVR and BP • Ganglionic Blockers: Interrupts adrenergic control of arteries. • Direct Vasodilators: Reduces SVR and BP by direct arterial vasodilation • ACE Inhibitors: Inhibit angiotensin converting enzyme, reduce conversion of Ang I to Ang II, prevent vasoconstriction. • Angiotensen II Receptor Blockers: Prevent action of angiotensin II and produce vasodilation and Inc salt and H2O excretion • Calcium Channel Blockers: Block movt of extracellular calcium into cells causing vasodilation and dec SVR. •Achieve and maintain desired BP. •Understand, accept, and implement therapeutic plan. •Experience minimal or no unpleasant side effects of therapy. •Be confident of ability to manage and cope with this condition •Health Promotion • Primary Prevention. • Lifestyle modifications. • Diet rich in fruits, vegetables, low-fat dairy foods, reduced saturated and total fats, reduced sodium chloride. • Screening programs: Cholesterol, BP, Etc.. • Appropriate Technique for Measuring Blood Pressure: Too tight, falsely high/ Too loose, falsely low • Review Table 32-13 on Page 794- Teaching Guide • Ambulatory and Home Care • Assist the patient in reducing BP. • Assist with complying with TX plan. • Patient and family education. • Detection & reporting adverse effects of TX • Compliance assessment and enhancement. • Evaluating therapeutic effectiveness • >50% US pop 65 & older. 56 Isolated Systolic Hypertension Pseudohypertension Hypertensive Urgency Hypertensive Emergency Hypertensive Crisis • Age-related physical changes. • Loss of tissue elasticity. • Increased collagen content-stiff myocardium. • Increases peripheral vascular resistance. • Decreased beta/adrenergic receptor sensitivity. • Blunting of baroreceptor reflexes: in kidneys and crotid arteries • Decreased renal function. •Decreased renin response to Na+ & H2O depletion • Sustained elevation of SBP>160 & DBP<90. • Borderline -SBP 140-159 & DPB <90. • More common in elderly. • More prevalent in women & Blacks. • Caused by loss of elasticity from atherosclerosis. • Can occur with sclerosis of the large arteries • Suspect if • arteries feel rigid, or • when few retinal or cardiac signs present. • Use Osler’s maneuver to differentiate. • Must use intra-arterial catheter to accurately measure if pseudohypertension is present. • Develops over days to weeks. • Severely elevated BP without end-organ damage. •Ususlly do not require IV meds can be managed with oral alone. • Develops over hours to days. • Acute target organ damage, esp. CNS. • Hypertensive encephalopathy. • Intracranial or subarachnoid hemorrhage. • Acute left ventricular failure with pulmonary edema. • MI. • Renal failure. • Dissecting aortic aneurysm. •NEED IV drugs and oral drugs • Severe, abrupt elevation. • DBP of 120 to 130 mm Hg. • Rate of rise more important than absolute value. • It is classified by degree of organ damage and the rapidity in which the BP must be lowered. • It is important to determine cause after crisis is resolved to make sure further crisi dont occur. 57 • Clinical Manifestations • HA. • Nausea. • Vomiting. • Seizures. • Confusion. • Stupor. • Coma. • Blurred vision and transient blindness. • Renal insufficiency. • Nursing and Collaborative management • Mean arterial pressure used instead of BP. • Hospitalization. • IV medications. • EKG monitoring. • Urinary output monitoring. • Neurological monitoring