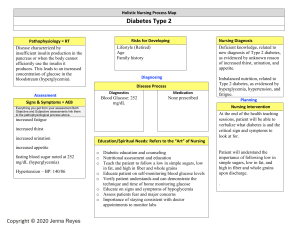
N204 Advanced Pathophysiology 1st Semester A.Y. 2023-2024 Case Analysis No. 5 Care of Clients with Alterations in Nutrition, Metabolism, and Endocrine Function NAME: Jason Anthony I. Alberto, RN DATE: December 3, 2023 Program: Master of Arts in Nursing Major: Adult Health Nursing CASE SCENARIO T.G. is a 67-year-old patient, diagnosed with a 3-year history of type 2 diabetes. Prior to diagnosis, his history indicated a fasting blood glucose value of 113–125 mg/dl. He also had past episodes of nocturia associated with large rice meals and desserts. At the time of initial diagnosis, he was advised to lose weight, but no further action was taken. T.G.’s parents both had type 2 diabetes, but states that he does not understand why he has diabetes since he never eats a lot of sugar. Instead, his usual meals include 2 cups of rice and a viand, usually pork or beef. His favorite breakfast is 4 slices of white bread with margarine spread. He stopped smoking more than 5 years ago, especially when cigarette prices become higher than usual. T.G. presents with recent weight gain, right leg pain, a non-healing wound in his right foot. He had been started on Gliclazide 30 mg once a day, but had stopped taking it because of dizziness, often accompanied by sweating and a feeling of mild agitation in the late afternoon. T.G. also takes Atorvastatin 10 mg daily, for hypercholesterolemia (elevated LDL cholesterol, low HDL cholesterol, and elevated triglycerides). The laboratory results that T.G. brought indicate that his hemoglobin A1c has never been <8%. His blood pressure has been measured at 150/70, 148/92, and 166/88 mmHg on separate occasions during the past year at the nearby health center. 1 Physical examination findings: • • • • • • • • Weight: 181 lbs; height: 5′4′′ Capillary blood glucose (random): 176 mg/dl VS: BP 150/90 mmHg; PR 88 bpm; RR 20 cpm; T 36.8 C Corrective lenses, pupils equal and reactive to light and accommodation Lungs: bilateral clear breath sounds Heart: Rate and rhythm regular, no murmurs or gallops No carotid bruits; Left lower extremity - popliteal and dorsalis pedis pulses 2+ Right lower extremity - popliteal and dorsalis pedis pulses 1+, right foot pale and cool to touch, diminished vibratory sense, absent ankle reflexes Laboratory tests revealed the following results: • • • • • Glucose (fasting): 167 mg/dl; HbA1C: 8.1% Creatinine: 1.8 mg/dl; Blood urea nitrogen: 25 mg/dl Sodium: 141 mg/dl; Potassium: 5.0 mg/dl Lipid profile: Total cholesterol: 222 mg/dl; HDL cholesterol: 48 mg/dl; LDL cholesterol: 114 mg/dl; Triglycerides: 177 mg/dl Urine microalbumin: 45 mg The patient was ordered for admission. The latest orders are as follows: 2 Diabetes Mellitus Diabetes mellitus is the collective term for heterogeneous metabolic disorders whose main finding is chronic hyperglycemia. The cause is either a disturbed insulin secretion or a disturbed insulin effect or usually both. (ECED, 2019) The condition is also brought about by metabolic syndrome which is an umbrella term used to described a set of clinical and diagnostic manifestations that increases the risk for comorbidities such as diabetes, stroke and heart diseases. (NIH, 2022) Criteria for identifying if an individual has metabolic syndrome includes various factors. First, is a large waistline with >45 inches in men and >35 inches in women as this may imply that there is an accumulation of adipose tissue in around the viscera called “visceral fat” that is stubborn and cannot be removed easily. Another one is hypertension which is a silent killer and causes a myriad of cardiovascular damage and may also lead to developing plaques in the arteries hence, atherosclerosis. Elevated low density lipoprotein (LDL) and decreased high density lipoprotein (HDL) can also affect in the development of metabolic syndrome because high LDL’s correspond to greater chance of forming fat plaques and low HDL’s further increase the risk of atherosclerosis as its function is to remove the LDL. Increased amounts of Triglycerides in the blood which can cause additional rise in LDL’s. Lastly, elevated blood glucose levels is associated with metabolic syndrome as it can lead increased blood viscosity and increased risk for blood clotting which is detrimental and can cause stroke and heart attack. Classifications of Diabetes Mellitus According to the standards of medical care of diabetes from the American Diabetes Association (ADA) in 2022, In classifying diabetes, there have been evolving definitions and parameter how to classify diabetes. Type 1 Diabetes Mellitus (T1DM) was classically know as insulin dependent diabetes and Juvenile DM while Type 2 Diabetes Mellitus (T2DM) was formerly known as non-insulin dependent diabetes. While those definitions have been widely used, advancements in diagnosing diabetes has further reached and discovered other types that does not limit to T1DM and T2DM. Type 1 DM is caused by either a genetic predisposition to diabetes or other direct causes characterized by insulin deficiency which while Type 2 DM can also be genetic but predominantly lifestyle-related and the key mechanism is insulin resistance. At some point, insulin resistance can lead to actual damage to the beta cells making them insulin requiring. Other types of diabetes 3 include specific types of DM related to diseases of the exocrine pancreas, drug-induced DM and even monogenic diabetes syndromes. Gestational diabetes mellitus (GDM), is a diseases that only spans across pregnancy specifically during second and third trimester and it is theoretically characterized by the production of human placental lactogen from the placenta and is a known insulin antagonist causing insulin resistance hence, GDM. Risk Factors Patient TG is a known case of Type 2 Diabetes Mellitus. Familial or genetic predisposition plays a role in developing Type 2 DM and according to ADA (2022), the diagnosis of Type 2 DM is not solely based on lifestyle but the decreased beta cell function that is carried out by the genes of parental DNA to the offspring which is not as observable versus type 1 DM but type 2 DM has shown to be manifested in those families with familial history of Obesity. Obesity on the other hand, is also part of the risk factors because Patient TG’s BMI is 31.1 kg/m2 and obesity is a major contributor due to increased visceral fat which causes insulin resistance. Patient TG’s age of 67 years old indicated advancing age which is a risk factor for DM as aging signifies a decline in the beta cells causing decreased insulin sensitivity and production. Unhealthy diet and sedentary lifestyle are a direct contributor to developing type 2 diabetes since these behaviors may lead to obesity. Hypercholesterolemia and hypertension are a known dyad that causes insulin resistance as well as atherosclerosis in which when not managed can cause serious complications from diabetes. Social Determinants The development of type 2 diabetes (T2DM) can also be determined by social determinants and other related risk factors. Globally, the incidence and prevalence of T2DM are found to vary widely depending on ethnicity and geographical region with Japanese, Hispanics and Native Americans having the highest risks (Galicia-Garcia et. al., 2020). It has shown higher incidence risk in the Asian population especially those living in low- to middle income group. It highest incidence belong to those who are in the African descent. Sex has shown almost equal affectation to T2DM being pre-dominantly female specifically African Women. The unusual, disturbed and reduced sleep is associated with glucose intolerance (Ismail, Materwala, & Kaabi, 2021) Sleep quality and quantity has been deemed to have an impact with diabetes. Among working professionals, fatigue and tiredness causes increased stress leading to increased production of cortisol which is a glucocorticoid that triggers increase in plasma glucose in stressed states. Psychiatric 4 disorders mainly, depression is associated with multiple health condition which includes diabetes. The elevated sympathetic response cause an increase in catecholamines leading to inflammation, stress and eventually, insulin resistance. Age While it is known that type 2 diabetes is commonly seen in older patients, younger age groups also comprise the population of people with T2DM. In is said according to Porth (2023) that T2DM usually onset in people after the age of 30 while in McCance (2018), specific age groups are mentioned with people aged 18-44 years old with four percent (4%) incidence, 45 to 64-year-old adults with 17% affectation and majority being greater that 65 years old at 25.2%. Generally, an aged individual poses a higher risk of developing type 2 diabetes however, with the discovery other specific types of diabetes, the ADA (2022) has inferred that while the olden knowledge divides T1DM and T2DM related to its age, in today’s age both types can onset in all age groups as the development of insulin deficiency and insulin resistance span across all walks of life. Environment and genetics both play a role in developing diabetes hence, diagnostics and therapeutics shall vary depending on whether the patient has acquired one over the other. Assessment Data Assessment Data According to Gordon’s Functional Health Patterns FUNCTIONAL PATTERN Health Perception/Health Management Objective Subjective o Compliance with o Patient’s inability to maintenance make an effort to medications such as lose weight shows a Gliclazide lack and Atorvastatin o Both of health- seeking behaviour parents are known to have been diagnosed with Type 2 Diabetes Nutritional-Metabolic o Elevated FBS – 167 mg/dL o RBS – 176 mg/dL o HbA1c of 8.1% o Usually eats 2 cups of rice and a viand o Favorite breakfast is 4 slices of white 5 o Hyperlipidaemia bread o Urine margarine and Microalbuminuria – 45 mg/dL – o Creatinine 1.8 mg/dL o BUN – 25 mg/dL o BMI – 31.1 kg/m2 o Elevated BP SBP 148-166 mmHg DBP 70-90 mmHg Elimination o Low Serum Sodium o Episodes of (141 md/dL) related increased urination to excess urination at night (nocturia) leading to electrolyte loss Activity-Exercise o Patient’s inability to N/A make an effort to lose weight may indicate that he has a sedentary lifestyle Cognitive-Perceptual o Patient has o (+) Sweating experienced accompanied dizziness and mild agitation due to side agitation related to effects side diabetic medications effects of of by anti- Gliclazide o Right foot is pale and cool to touch with diminished vibratory sense and absent ankle reflexes 6 Sleep-Rest o Sleep deprivation N/A may arise related to episodes of nocturia Self-Perception/Self- o Presence of non- Concept o Inability to healing wound in his understand onset of right foot diabetes o Weight gain that has progressed and misconception that to diabetes Obesity is only related with sugar consumption. Role-Relationship N/A N/A Sexuality-Reproductive N/A N/A Coping-Stress Tolerance N/A N/A Values-Belief N/A N/A Diagnostic and Laboratory Laboratory Test Normal Values Glycosylated Hemoglobin 5.7% - 6.4% Significance Identifies compliance for (HbA1c) the last Increased 3-6 months. glycosylated hemoglobin indicates elevated glucose in the bloodstream and attaches to hemoglobin in the circulation. Fasting Plasma Glucose Less than 100 mg/dL Signifies glucose control for (FPG) over 8-10 hours of fasting. Elevated FPG may infer that there is poor glucose reuptake after a meal that sustains through the course fasting 7 Random Plasma Glucose >200 mg/dL Done on casual events to (RPG) identify on-the-spot blood glucose. Results may differ and does not diagnose or rule out diabetes and must be done together with other tests Oral Glucose Tolerance <140 mg/dL Consumption of anhydrous Tests glucose powder in water (orange or cola flavor) with 2Hr blood glucose test. Elevated glucose indicates poor level glucose control. Values are based on ADA Guidelines 2022 Other Related Diagnostic and Laboratory Tests Laboratory Tests Complete Blood Count Significance Increased leukocytes may indicate possible infection problems and increased hematocrit may be related to dehydration secondary to osmotic diuresis Kidney Function Tests (BUN/Creatinine) Diabetes can cause microvascular complications to the renal vessels causing decline in kidney function which can be seen when there is an increase in nitrogenous waste and creatinine in the blood Urinalysis with Ketones Presence of glucose in the urine signifies increased glucose vs renal threshold causing the excess glucose to be excreted through urination. Increased protein in the urine can be related to protein wasting from gluconeogenesis which passes through the renal tubules and exits the 8 body through voiding. It is also possible that ketones may be detected in the urine and can cause serious complication specifically, DKA. Lipid Profile In the presence of increased visceral fat, low density lipoproteins and triglycerides will also increase and cause insulin resistance Serum C-Peptide This blood test can differentiate insulin deficiency over insulin resistance as it shows the by-product of insulin produced in almost same amounts. Low to nonexistent C-Peptide may indicate insulin deficiency and normal C-Peptide indicates a person has insulin but is experiencing resistance. Islet Cell Antibodies Islet cell antibodies are markers that exist which indicates presence of damage to beta cells. This signifies if a patient has or is developing Type 1 Diabetes as damage to beta cells is permanent. Anti-GAD (Glutamic Acid Carboxylase) Serological Antibodies markers like Anti-GAD presents as a reliable diagnostic test to identify if an individual is insulin dependent and is related with having neurological diseases involving muscle rigidity and spasms 9 International Diagnostic Criteria FASTING PLASMA GLUCOSE Greater than or Equal to 126mg/dL (7.0 mmol/L) 2-Hr Post Prandial Glucose Greater than or Equal to 200 mg/dL (11.1 mmol/L) during OGTT HbA1C Greater than or Equal to 6.5% (48 mmol/mol) In patients with classic Random Plasma Glucose of >200 mg/dL (11.1 symptoms of hyperglycemia or mmol/L) hyperglycemic crisis Values are based on ADA Guidelines 2022 and CDCP 2019 Other Co-Morbidities of Patient TG Co-morbidity OBESITY BMI – 31.1 kg/m2 Hyperlipidemia Mechanism Obesity causes increased adipose tissue along the visceral area (Visceral Fat) together with increased lipoproteins and triglycerides. The increased visceral fat Total Cholesterol – 222 mg/dL HDL – 48 mg/dL LDL – 114 mg/dL and cholesterol can cause an endocrine effect causing increase in adipokines, cytokines and free fatty acids. The cascade of these enzymes synthesizes insulin resistance and metabolic memory which contributes to developing type 2 diabetes. Hypertension Hypertension elevates the sympathetic nervous system activity leading to a decrease in the body’s glucose uptake. (Ismail, Materwala & Kaabi, 2021) Elevated blood pressure heightens the sympathetic nervous system leading impaired vasodilation to activity of muscles which consequently, the reuptake 10 of glucose decrease that leads to development of Type 2 DM. Complications of Diabetes Mellitus Diabetes when not managed well can lead to chronic hyperglycemia which damages the body in various ways. One of the chief injuries arising from hyperglycemia is injury to vasculature, which is classified as either small vascular injury or injury to the large blood vessels of the body (Fowler, 2011). Microvascular Complication Mechanism Retinopathy The most common microvascular complication. Caused by hemorrhage and microaneurysms in the small vasculature of the retina leading to retinal edema which compromises vision and can lead to blindness. Neuropathy Decline in nerve function caused by multiple inflammatory response (polyol pathway, oxidative stress) related to hyperglycemia that reduced blood supply to nerves. Nephropathy Leading cause of renal failure globally (ADA, 2022). microalbuminuria Precedes from accompanied urine by increased glucose threshold more than the renal capacity causing damage to renal tubules and glomerulus. Macrovascular Complication Mechanism Stroke The central pathological mechanism in Coronary Artery Disease and Heart Failure macrovascular disease is the process of Peripheral Vascular Disease atherosclerosis, which leads to narrowing of arterial walls throughout the body. 11 Atherosclerosis is thought to result from chronic inflammation and injury to the arterial wall in the peripheral or coronary vascular system. In response to endothelial injury and inflammation, oxidized lipids from LDL particles accumulate in the endothelial wall of arteries (Fowler, 2011). In the progression of these mechanisms, Stroke, CAD and PVD can arise. Other Complications Diabetic Ketoacidosis (DKA) Mechanism In the presence of severe hyperglycemia (>300mg/dL) and the impaired compensatory mechanisms are done to produce more glucose as protein and lipids are broken down. In turn, ketones are produced and accumulate in the blood causing metabolic acidosis. Delayed management can be detrimental which can cause coma and even death. Hyperglycemic Hyperosmolar Non-ketotic Syndrome (HHNS) Hyperglycemia in levels higher than 500md/dL, serum osmolarity triggers severe osmotic diuresis leading to dehydration. This can also lead to diabetic coma. 12 Nursing Diagnosis o Risk for Unstable Blood Glucose – Related to poor glycaemic control secondary to insulin resistance hence, development of Type 2 DM o Impaired Tissue Perfusion/Risk for Impaired Skin integrity – Due to poor glucose control causing damage to endothelial vessel wall which decreases blood supply to Patient TG’s right lower extremity o Deficient Fluid Volume – Increased blood sugar can cause increased serum osmolarity thereby causing osmotic diuresis leading to increased thirst and dehydration o Risk for Infection – Presence of decreased right lower extremity circulation may lead to the development of infection specifically, DM Foot. o Ineffective Health Maintenance – As evidenced by non-compliance to intake of Gliclazide for glucose control due to the side effects experienced by the patient. o Imbalanced Nutrition More than Body Requirements/ Deficient Knowledge – As evidenced by patient’s daily intake of large rice meals and desserts as well as patient’s expression of confusion as to why he acquired diabetes despite the claim that he never eats a lot of sugar. 13