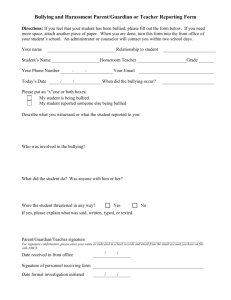
Community Mental Health Journal (2022) 58:689–700 https://doi.org/10.1007/s10597-021-00873-y ORIGINAL PAPER Factors Related to Immigrant/Nonimmigrant Children’s Experience of Being Bullied: An Analysis Using the Multiple Disadvantage Model Tyrone C. Cheng1 · Celia C. Lo2 Received: 30 January 2021 / Accepted: 2 July 2021 / Published online: 14 July 2021 © The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature 2021 Abstract Applying the multiple disadvantage model, a study of children in the United States examined experiences of being bullied in terms of 5 factors: social disorganization, social structural factors, social relationships, mental health and access to care, and acculturation. The study was a secondary data analysis of 19,882 immigrant and non-immigrant children, using data from the 2018 National Survey of Children’s Health. Logistic regression results show children’s likelihood of being bullied to be associated positively with racial discrimination; child mental health problem (either attention deficit/hyperactivity disorder, depression, anxiety, behavioral/conduct problem, or Tourette Syndrome); family substance use; being female; being age 6–10; being age 11–13; and parent education level. Likelihood of being bullied was associated negatively with safe neighborhood; being Black; being Asian; family cohesiveness; neighbor support; parent mental health; being a first- or second-generation immigrant; and parent age. The results imply the usefulness of interventions promoting racial harmony and family support. Keywords Bullying victimization · Racial discrimination · Mental health · Family support · Acculturation Introduction Bullying is aggression repeatedly displayed by a perpetrator who has a power advantage over a victim, who is unable to self-defend against the repeated aggression (Gladden et al., 2014; Shea et al., 2016). Research results have suggested that, in the United States, 10.6% to 28.0% of children are victims of bullying at school (Lim & Hoot, 2015; U.S. Department of Education, 2011). Moreover, one study reported that 18.3% to 54% of immigrant children in the U.S. experience bullying at school (Shea et al., 2016). Two others, however, found no association between immigrant status and bullying victimization among children (Abada et al., 2008; Lim & Hoot, 2015). Among American children with mental health problems, moreover, 35% to 47% report experiencing bullying victimization (Jackson et al., 2019). * Tyrone C. Cheng ccheng@sw.ua.edu; tyronecheng@yahoo.com Celia C. Lo clo@twu.edu 1 School of Social Work, University of Alabama, Little Hall, Tuscaloosa, AL 35401, USA 2 Department of Sociology, Texas Woman’s University, CFO 306, P. O. Box 425887, Denton, TX 76204, USA It remains important to continue to try to identify factors perhaps involved in being bullied, among immigrant and nonimmigrant children alike. Literature Review Investigating potential factors in children’s experience of bullying victimization, the present research used the multiple disadvantage model, which proposes that socioeconomic disadvantages and associated distress affect family and peer relationships negatively. The model has been applied in explaining racial disparities in victimization (Lo et al., 2013, 2015; Cheng & Lo, 2015). In this study, the multiple disadvantage model was employed in testing roles played by five socioeconomic disadvantages in children’s experience of bullying victimization. The five were social disorganization, social structural factors, social relationships, mental health and access to care, and substance use (see Fig. 1). Prior studies with children in the general population have indicated a link between bullying victimization and social disorganization, which may include residing in an unkempt, crime-ridden, unsafe neighborhood that exposes children to a subculture reliant on intimidation (Cook et al., 2010; Espelage et al., 2000; Holt et al., 2014). Socially 13 Vol.:(0123456789) 690 Community Mental Health Journal (2022) 58:689–700 Social Disorganizaon --Rundown neighborhood --Unsafe neighborhood --Racial discriminaon Social Structural Factors --Race/ethnicity --Socio-economic status --Gender & age as controls Mental Health– Related Factors --Child/parent mental health --Access to care Acculturaon Parental substance use Child being bullied Social Relaonships --Family support --Social support --Single-parent family Fig. 1 The multiple disadvantage model explaining children’s experience of being bullied (The figure was adopted from Cheng, Tyrone C., and Li, Q. (2017). Adolescent delinquency in child welfare sys- tem: A multiple disadvantage model. Children and Youth Service Review, 73, 205-212) disorganized neighborhoods often number immigrant families among their residents (Sidhu & Song, 2019; Yoshikawa & Kalil, 2011), which led the present researchers to speculate that living in a neighborhood that is rundown and unsafe from criminal perpetrators is linked to immigrant children’s experience of bully victimization. Moreover, the multiple disadvantage model holds that structural racism continually frustrates persons of minority ethnicity (Lo et al., 2013). Thus race/ethnicity and racism are social structural factors that may figure importantly in children’s experience of bully victimization. Perhaps not surprisingly, the literature indicates that racially discriminatory comments are often made by those perpetrating bullying (Koo et al., 2012; Mendez et al., 2016; Seaton et al., 2013; Walton, 2018; Wang et al., 2020). Some studies have found American children of Latino and Asian ethnicity to be bullied less often at school compared to White children (Koo et al., 2012; Peguero, 2009; U.S. Department of Education, 2011; Wang et al., 2020). One, however, found the rate of bullying among White children to be lower than that among their peers of minority ethnicity (Mendez et al., 2016), while two more studies observed no significant difference in bullying victimization between these groups (Holt et al., 2014; Hong et al., 2020). Like ethnicity, gender may affect childhood experience of bullying victimization. At least three investigations have concluded that male respondents reported experiencing more bullying than female respondents did (Holt et al., 2014; Hong et al., 2020; Wang et al., 2020). In contrast, a different study found just the opposite (Merrill & Hanson, 2016), and yet another found girls who had immigrated from Asian nations experienced more bullying than did White nonimmigrant boys (Koo et al., 2012). Additionally, three published studies indicate younger children are more often bullied than older ones (Cappadocia et al., 2012; Holt et al., 2014; U.S. Department of Education, 2011). Social structural factors describing their parents also appear to figure in children’s experience of being bullied. Specifically, parents’ education, employment status, and income have been implicated in victimization. One American study showed that having relatively less educated parents elevated children’s likelihood of being bullied (Hong et al., 2020); in turn, a Canadian study observed no link between parents’ education and children’s bullying victimization (Abada et al., 2008). Additionally, at least two prior studies report that children in low-income families are relatively likely to be bullied, compared to higher-income peers (Hong et al., 2020; Mendez et al., 2016), although two others report no link of parents’ income to children’s experience of bullying (Abada et al., 2008; U.S. Department of Education, 2011). Poverty is a disadvantage affecting many immigrant children (Chaudry et al., 2010; Gulbas et al., 2016; Sidhu & Song, 2019), since immigrant parents often face underemployment and the resulting financial hardships. Stressed by these things, immigrant parents may often be unable to attend fully to children’s development and concerns (Shea et al., 2016; Yoshikawa & Kalil, 2011). While there is scant published literature on relationships among immigrant children’s experience of bullying and their parents’ education, employment status, and income, the authors of the present study speculate that strong negative links may exist, for immigrant and nonimmigrant children alike. When parents and children face multiple socioeconomic disadvantages, supportive social relationships can alleviate the distress of that experience. Parents with strong social networks tend to demonstrate effective parenting (McConnell 13 Community Mental Health Journal (2022) 58:689–700 et al., 2011); for immigrant children, support from parents and family, as well as peers, seem to reduce risk of being bullied (DeJonckheere et al., 2017; Gulbas et al., 2016), and the same link has been observed in studies of children generally (Abada et al., 2008; Cook et al., 2010; Hong et al., 2020). A study of children in Canada found those in single-parent families were more likely to be bullied than other families (Abada et al., 2008). The finding implies the important role of spousal support in minimizing children’s experience of bullying victimization. Interestingly, one study in the literature shows that immigrant children derive social support from relationships with healthcare providers who understand and respect norms of the children’s native cultures (Sidhu & Song, 2019). Another study, however, observed no significant relationship between immigrant children’s bullying victimization and the degree or quality of communication established between parents and these children’s healthcare providers (Wong et al., 2017). The present research reflects the simple speculation that, for immigrant and nonimmigrant children, experience of bullying victimization may be associated positively with single-parent family and associated negatively with supportive social relationships, including family relationships. As already noted, children’s rates of bullying victimization may be even higher in the presence of a mental disorder. Such disorders in children are fostered by socioeconomic disadvantages. In children, the disorders attention deficit/ hyperactivity (ADHD), depression, generalized anxiety, autism, pervasive developmental disorder (PDD), and Tourette syndrome are all linked to relatively higher odds of being bullied (Abada et al., 2008; Cappadocia et al., 2012; Charania et al., 2019; Crawford & Manassis, 2011; DeJonckheere et al., 2017; Jawaid et al., 2012; Mayes et al., 2015; Pontillo et al., 2019; Simmons & Antshel, 2021; Yockey et al., 2019; Zinner et al., 2012). Furthermore, parents dealing with their own mental health problems may be unable to provide their children with supportive parenting (Waylen & Stewart-Brown, 2010); among children who are bullied, links have been observed between that experience and their own mental health problems (Abada et al., 2008; Cappadocia et al., 2012; Merrill & Hanson, 2016; Ong et al., 2021) as well as their parents’ mental health problems (Cappadocia et al., 2012). One study reported that immigrant children with mental health problems were more likely to be bullied than not (DeJonckheere et al., 2017). Bullying victimization among children may be related to their parents’ use of substances. One investigation found less than 13% of mothers with depression to seek professional care (Cheng & Lo, 2016) (Woolhouse et al., 2009), and parents who go without such care probably are likelier than parents who do get treatment to self-medicate with alcohol and/or drugs. Such use of substances, of course, tends to further impair both mental health and parenting competence. At 691 least one published study reports a link between children’s experience of being bullied and their parents’ alcohol use (Eiden et al., 2010). One socioeconomic disadvantage commonly affecting American families is the lack of insurance. Lack of health coverage can affect children’s mental health, with uninsured children reported more likely to have a mental health problem, versus insured children (Akobirshoev et al., 2017; Ong et al., 2021). The literature presents mixed findings concerning a relationship between possession of health insurance by an immigrant child’s parent and that child’s use of mental health services. Two studies of immigrant children of Latino ethnicity found those children to be relatively unlikely, compared to other children, to be covered by a health insurance policy (Carson et al., 2011; Flores & Vega, 1998), although two additional studies did not observe this association to characterize immigrant children of Latino or Asian ethnicity (Finno-Velasquez et al., 2016; Spencer et al., 2010). The present researchers speculated that, for immigrant and nonimmigrant children alike, experience of bullying victimization is associated in a negative direction with family possession of health insurance. Facilitating use of the multiple disadvantage model to assess immigrant children’s bullying victimization likelihood, the present researchers explored immigrant children’s acculturation. Specifically, they examined acculturation’s relationship to victimization. Through the process of acculturation, immigrants adjust to and/or are changed by some culture beyond their native culture (Zea et al., 2003). Findings in the literature indicate that first-generation immigrant children report fewer mental health problems, versus second-generation ones, due to a tendency among the first generation to suppress one’s mental health needs to promote maintenance of ethnic identity (Pumariega & Rothe, 2010). In contrast, second-generation immigrant children are caught between the old culture and the new (Pumariega & Rothe, 2010), which can present certain challenges to mental health (Pumariega et al., 2005). According to one study of distinct ethnic groups, differences in patterns of bullying victimization are generational. First- and second-generation immigrant children of Latino ethnicity were found less likely to be bullied, compared to the third generation; and first- and second-generation immigrant children of Asian ethnicity were found more likely to be bullied, compared to the third generation (Peguero, 2009). This suggests that acculturation process can be a challenge or problem for a specific generation of immigrant children. How completely an immigrant has become acculturated is indicated by, among other things, the proficiency demonstrated with the dominant language (Celenk & Van de Vijver, 2011; Guerrero et al., 2015; Lakey, 2003). Just 43% of Asian immigrants in one U.S. study demonstrated proficiency with English (Ragavan et al., 2018), while less than 39% of Latino 13 692 children examined in a different study demonstrated such proficiency (Santiago et al., 2014). In yet another study, children’s experience of being bullied was found to exhibit an association in negative direction with speaking English at home (Yu et al., 2003). Hypothesis The reviewed literature provided only a small number of U.S. studies of immigrant children focusing on factors in their bullying victimization experience. The present study hypothesized that such victimization would be associated with measures of children’s (a) social disorganization (e.g., maintenance of neighborhood, safety of neighborhood, racism in community), (b) social structural factors (e.g., race/ ethnicity, parent’s education, parent’s employment, family income), (c) social relationships (e.g., family support, social support, single-mother household), (d) mental health and access to care (e.g., child/parent mental health, substance use by family members, possession of health insurance), and (e) acculturation (e.g., first/second/third-generation, English spoken at home). Method Sample This secondary data analysis of a nationally representative sample of 19,882 children was extracted from a public-use data set, the 2018 National Survey of Children’s Health (NSCH). Between June 2018 and January 2019, NSCH researchers interviewed 30,530 children and their caregivers, gathering information on health status, insurance coverage, social relationships, family relationships, and neighborhood characteristics (Child & Adolescent Health Measurement Initiative, 2020). The present sample was limited to children age 6–17 years who lived with their biological parents and/ or stepparents, some of whom had immigrated to the U.S. As a secondary data analysis, the present research received exempted approval from the institutional review board of the university. Measures This study’s dichotomous (yes/no) outcome variable, being bullied, indicated if a child had been bullied, picked on, or excluded by others at least once in the 12 months preceding interview. The study employed six groups of explanatory variables: social disorganization, social structural factors, social relationships, mental health and access to care, acculturation, and demographic characteristics (see Table 1). The social disorganization group comprised three variables. 13 Community Mental Health Journal (2022) 58:689–700 Rundown neighborhood (yes/no) denoted whether a parent described the neighborhood of residence as (a) “litter or garbage on street or sidewalk,” (b) “poorly kept or rundown housing,” or (c) “vandalism such as broken windows or graffiti.” The safe neighborhood variable described how safe the neighborhood of residence was for the child, using a range of responses: 4 (definitely agree), 3 (somewhat agree), 2 (somewhat disagree), and 1 (definitely disagree). Finally, racial discrimination (yes/no) indicated whether a parent had reported a child was at some point treated or judged by a member of the community solely on the basis of race/ ethnicity. Three measures constituted the social structural factors. A child’s race/ethnicity was described using the dummy variables White (the reference), Black, Hispanic, Asian, and other race/ethnicity. Nine numbered categories were used to describe parent’s educational attainment: 1 (8th grade or below), 2 (9–12th grade), 3 (graduated high school or GED), 4 (vocational school), 5 (some college), 6 (associate degree), 7 (undergraduate degree), 8 (master’s degree), 9 (doctoral or professional degree). The dichotomous measure employed parent indicated each parent who had been a paid employee during 50 of the 52 weeks preceding the interview. Last, family income-to-poverty ratio gave the percentage of federal poverty level represented by the income of a child’s family; measures of this ratio were part of the original NSCH data set. Six explanatory variables made up the variables group assessing social relationships. Single mother (yes/no) indicated a child’s caretaker was the female parent, who was a single parent. Family cohesiveness was measured as the combined score from two survey items that elicited information about how a family responded to problems they faced, using the levels “the family talks together about what to do” and “the family has strengths to draw on.” Each item was measured via the following 4-point scale: 1 (none of the time), 2 (some of the time), 3 (most of the time), and 4 (all the time). Higher combined scores implied stronger family cohesiveness. The Cronbach’s alpha for the two items was .81. As well, family support (yes/no) indicated whether a parent received emotional support from a spouse/partner, other family members, or friends. Similarly, professional support (yes/no) indicated whether a parent received emotional support from a counselor or health care provider, and peer/religious group support (yes/no) indicated whether a parent received emotional support from a group of peers or a religious group. Finally, neighbor support was the total score from three survey items asking parents how much they agreed that adults in their neighborhoods (a) know where to get help, (b) watch out for each other’s children, and (c) provide help to others. Responses for each item ranged from 4 to 1, as follows: 4 (definitely agree), 3 (somewhat agree), 2 (somewhat disagree), and 1 (definitely disagree). Higher Community Mental Health Journal (2022) 58:689–700 Table 1 Descriptive statistics of children (n = 19,882) 693 Percent Outcome variable Being bullied (yes) (no) Social disorganization factors Rundown neighborhood (yes) (no) Safe neighborhood Racial discrimination (yes) (no) Social structural factors White Black Hispanic Asian Other race/ethnicity Parent educational attainment Employed parent (yes) (no) Family income-to-poverty ratio (%) Social relationships Single mother (yes) (no) Family cohesiveness Family support (yes) (no) Professional support (yes) (no) Peer/religious group support (yes) (no) Neighbor support Mental health and access to care ADHD (yes) (no) Depression (yes) (no) Anxiety (yes) (no) Behavioral/conduct problem (yes) (no) Autism spectrum disorder/pervasive developmental disorder (yes) (no) Tourette syndrome (yes) (no) Other mental health problem/condition (yes) (no) Parent mental health Family mental health problem (yes) (no) Family substance use (yes) (no) Mean Range sd 50.6 49.4 20.5 79.5 4.0 96.0 71.7 5.8 11.6 4.8 7.1 78.5 21.5 14.6 85.4 80.3 19.7 25.1 74.9 30.3 69.7 3.7 1–4 .6 6.1 1–9 1.9 292.9 50–400 122.0 6.8 2–8 1.3 10.0 3–12 1.9 4.1 1–5 .9 12.6 87.4 6.7 93.3 14.0 86.0 9.1 90.9 3.3 96.7 0.3 99.7 0.4 99.6 9.5 90.5 9.9 90.1 13 694 Community Mental Health Journal (2022) 58:689–700 Table 1 (continued) Percent Insured (yes) (no) Acculturation 1st-generation immigrant family 2nd-generation immigrant family 3rd-generation immigrant family English spoken at home (yes) (no) Demographic characteristics Girl Boy Child age: 6 to 10 years Child age: 11 to 13 years Child age: 14 to 17 years Parent age (years) Mean Range sd 95.8 4.2 2.1 15.5 82.4 93.2 6.8 47.5 52.5 34.2 24.6 41.2 44.0 18–75 7.5 sd standard deviation total scores suggested stronger networks of supportive neighbors. These three survey items yielded a Cronbach’s alpha of .80. The fourth group of explanatory variables represented mental health and access to care. Seven dichotomous variables were used to indicate whether a doctor had ever diagnosed the child respondent with ADHD, depression, anxiety, behavioral/conduct problem, autism spectrum disorder/ pervasive developmental disorder, Tourette syndrome, and other mental health problem/condition. In contrast, parent mental health was a self-reported measure using a 5-point response scale: 1 (poor), 2 (fair), 3 (good), 4 (very good), and 5 (excellent). Family mental health problem denoted dichotomously whether a child ever lived with a mentally ill, suicidal, or severely depressed individual. Family substance use, also dichotomous, indicated if a child ever lived with an individual who used alcohol or drugs problematically. The yes/no variable insured described a child’s access to health care in terms of the family’s possession of health insurance coverage. Three explanatory variables measured the acculturation of a family in the study. Two dichotomous dummy variables were allowed to indicate what stage of the acculturation process characterized child and parent. A first-generation immigrant family included a child born outside the U.S. plus at least one parent born outside U.S. A second-generation immigrant family included a child born in the U.S. plus at least one parent born outside U.S. The reference for these two variables was third-generation family, in which the child and both parents were born within U.S. borders. Additionally, the dichotomous variable English spoken at home stated whether a family largely used English as their language at home. (The measure was an indicator of a family’s 13 English-language proficiency.) Finally, three demographic variables provided controls during modeling: parent age (in years), girl (versus boy), and child age, indicated using three age ranges: 6–10 years, 11–13 years, and 14–17 years (the reference). Data Analysis Since the present study used a binary outcome variable, STATA logistic regression was employed to conduct linearized variance estimations with robust standard errors. Sampling weights provided by NSCH researchers were, furthermore, applied. No multicollinearity problems among employed explanatory variables were suggested by the conducted preliminary analyses of tolerance statistics (.62 or higher) and correlations (− .41 ≤ r ≤ .45). Results Sightly over half (50.6%) of child respondents in this analysis of data gathered in 2018 were reportedly bullied at some point during the period under study (see Table 1). Just 20.5% of the children resided in rundown neighborhoods, and on average their parents “somewhat agreed” that the neighborhood of residence was safe for the child, their average score being 3.7. Parent respondents reported just 4.0% of child respondents had experienced racial discrimination. Child respondent race/ethnicity broke down as follows: White, 71.7%; Black, 5.8%; Hispanic, 11.6%; Asian, 4.8%; other race/ethnicity, 7.1%. On average, parent’s education level was 6.1 (associate degree). More than three-fourths of parent respondents (78.5%) were employed, and average Community Mental Health Journal (2022) 58:689–700 family income-to-poverty ratio for the sample was 292.9% (of 400.0% possible). In the present study, single mothers represented 14.6% of the caregivers of the sample’s 19,882 child respondents. Average score for family cohesiveness across the sample was 6.8 (of 8.0 possible), and for neighbor support was 10.0 (of 12.0 possible). Among the parent respondents, cited sources of emotional support broke down as follows: 80.3% reported deriving it from family members and/or friends; 25.1% from counselors and/or other health providers; 30.3% from members of a formal group of peers and/or a religious group. Among child respondents in the present sample, a physician’s diagnosis of ADHD described 12.6% of them; of depression described 6.7% of them; of anxiety described 14.0% of them; of a behavioral/conduct problem described 9.1%; of autism spectrum disorder/pervasive developmental disorder described 3.3%; of Tourette syndrome described 0.3%; and of other mental health problem/condition described 0.4%. Parent respondents had, on average, a score of 4.1 for mental health, or very good. Just under one in ten child respondents in the sample (9.5%) had lived with a family member suffering from a mental disorder, while slightly more (9.9%) had lived with a family member who used one or more substances problematically. The large majority of child respondents, 95.8%, were covered by a health insurance policy of some sort. Members of first-generation immigrant families made up 2.1% of the present sample; second-generation immigrant families made up 15.5%, and third-generation families made up 82.4%. English was the language primarily spoken in the homes of 93.2% of families in the present sample. The average age of a parent respondent in the sample was 44 years. Concerning age of child respondents, 34.2% were 6–10 years old; 24.6% were 11–13 years old; and 41.2% were 14–17 years old. Girls constituted 47.5% of the child sample. Results of multivariate analysis confirmed the hypothesized model to differ significantly from the null model (Wald’s χ2 = 810.25, p < .01; see Table 2). Children’s likelihood of being bullied was reduced, in this study, by residence in a safe neighborhood (OR 0.84; p < .01). It was increased, in turn, by experience of racial discrimination (OR 2.43; p < .01). Residence in a rundown neighborhood showed no association with children’s likelihood of being bullied. In the present study, child respondents who were Black were less likely to be bullied than those who were White (OR .45; p < .01). Similarly, child respondents who were of Asian ethnicity were less likely to be bullied than White counterparts (OR .56; p < .01). No significant differences in likelihood of bullying victimization were observed between White child respondents and those of either Hispanic or other race/ethnicity. As well, no significant association with 695 bullying likelihood was found for family income-to-poverty ratio or for parent employment status. This study did find an association in positive direction between parent education and children’s likelihood of being bullied (OR 1.05, p < .05). Furthermore, children’s likelihood of being bullied was diminished by family cohesiveness (OR .89, p < .01) and by neighbor support (OR .95, p < .01), although such likelihood was not found to be significantly associated with parent emotional support from family, health providers, or peer/religious groups. Concerning mental health, this study found the likelihood of being bullied to be associated (in positive direction) with child’s diagnosis with ADHD (OR 1.46, p < .01), depression (OR 1.95, p < .01), anxiety (OR 1.70, p < .01), behavioral/ conduct problem (OR 1.70, p < .01), or Tourette syndrome (OR 2.29, p < .01), and also with family substance use (OR 1.27, p < .05). Likelihood of being bullied showed association in negative direction with parent mental health (OR .88, p < .01). No link between likelihood of being bullied and possessing health insurance was observed here. In addition, compared to children in third-generation families, those in first-generation families (OR .58, p < .05) and second-generation families (OR .65, p < .01) were less likely to be bullied (although speaking English in the family home showed no association with bullying likelihood). Finally, likelihood of being bullied was associated in positive direction with being a girl (OR 1.33, p < .01), with being 6–10 years old (OR 3.05, p < .01), and with being 11–13 years old (OR 2.17, p < .01); while an observed association between bullying likelihood and parent age lay in a negative direction (OR .98, p < .01). Discussion This secondary data analysis of data gathered in 2018 yielded results showing one-half of its child respondents to have been bullied. This percentage is 4.8 times greater than one calculated in a small study of children attending a U.S. inner-city school (Lim & Hoot, 2015), and 1.7 times greater than one calculated by a national study (U.S. Department of Education, 2011). Closer examination of measures for child respondents in the present sample whose families were firstor second-generation immigrant families showed that children had experienced bullying victimization in the following by-race/ethnicity percentages: White, 45.1%; Hispanic, 35.3%; Black, 32.6%; Asian, 24.8%; and other race/ethnicity, 43.5%. Bullying victimization affected clearly substantial percentages of immigrant child respondents in this study. The findings partially support the present hypothesis, that children’s experience of being bullied is associated with children’s social disorganization (e.g., maintenance of neighborhood, safety of neighborhood, racism in community), social 13 696 Table 2 Logistic regression results on children being bullied (n = 19,882) Community Mental Health Journal (2022) 58:689–700 Variables OR Social disorganization factors Rundown neighborhood (no) Safe neighborhood Racial discrimination (no) Social structural factors Black (white) Hispanic (white) Asian (white) Other race/ethnicity (white) Parent educational attainment Employed parent (no) Family income-to-poverty ratio Social relationships Single mother (no) Family cohesiveness Family support (no) Professional support (no) Peer/religious group support (no) Neighbor support Mental health and access to care ADHD (no) Depression (no) Anxiety (no) Behavioral/conduct problem (no) Autism spectrum disorder/pervasive developmental disorder (no) Tourette syndrome (no) Other mental health problem/condition (no) Parent mental health Family mental health problem (no) Family substance use (no) Insured (no) Acculturation 1st-generation immigrant family (3rd-generation) 2nd-generation immigrant family (3rd-generation) English spoken at home (no) Demographic characteristics Girl (boy) Child age: 6 to 10 years (age: 14 to 17 years) Child age: 11 to 13 years (age: 14 to 17 years) Parent age Wald’s χ2 = RSE 95% CI 1.06 .84** 2.43** .08 .05 .38 .91–1.24 .74–.95 1.79–3.30 .45** .83 .56** .83 1.05* 1.07 1.00 .06 .09 .10 .09 .02 .08 .00 .34–.60 .68–1.02 .40–.78 .67–1.03 1.01–1.08 .92–1.24 .99–1.00 1.04 .89** .92 1.11 1.11 .95** .09 .02 .08 .07 .07 .02 .88–1.23 .85–.93 .79–1.08 .97–1.26 .98–1.26 .92–.99 1.46** 1.95** 1.70** 1.70** 1.39 .15 .29 .15 .24 .27 1.19–1.79 1.46–2.61 1.40–2.06 1.29–2.25 .94–2.04 2.29** 1.09 .88** 1.22 1.27* 1.21 .85 .61 .03 .13 .12 .18 1.11–4.76 .36–3.27 .81–.95 .99–1.49 1.05–1.53 .90–1.63 .58* .65** 1.37 .15 .07 .25 .35–.96 .52–.81 .95–1.96 1.33** 3.05** 2.17** .98** 810.25** .07 .22 .15 .00 1.19–1.48 2.65–3.52 1.90–2.49 .98–.99 Reference groups are in parentheses OR odds-ratios, RSE robust standard errors, CI confidence-interval **p < .01; *p < .05 structural factors (e.g., race/ethnicity, parent’s education, parent’s employment, family income), social relationships (e.g., family support, social support, single-mother household), mental health and access to care (e.g., child/parent 13 mental health, substance use by family members, possession of health insurance), and acculturation (e.g., first/second/ third-generation, English spoken at home). The study found residence in an unsafe neighborhood raised the likelihood a Community Mental Health Journal (2022) 58:689–700 child was bullied, which supports prior results (Cook et al., 2010; Espelage et al., 2000; Holt et al., 2014). A strong predictor of bullying victimization was children’s experience of racial discrimination. It raised such likelihood by 143% in this study, consistent with earlier findings (Koo et al., 2012; Mendez et al., 2016; Seaton et al., 2013; Walton, 2018; Wang et al., 2020). (The 2018 survey item assessing racial discrimination did not limit the environment in which the discrimination had occurred. That is, respondents were not asked about discrimination specifically in school or during gatherings of peers or similar. Discrimination, then, could have been targeted at the child respondents by any individual in the general community.) It certainly appears that socially disorganized neighborhoods and racism loom large in the question of which children are most likely to experience bullying victimization. Like some earlier studies, the present study found ethnic Asian children to be less likely than White children to experience bullying (Koo et al., 2012; Peguero, 2009; U.S. Department of Education, 2011; Wang et al., 2020). It also found Black children to be less likely than White children to be bullied. It did not observe any association between family income and children’s likelihood of being bullied, which supported certain prior findings (Abada et al., 2008; U.S. Department of Education, 2011). In contrast, some of this study’s findings on parent education and bullying likelihood contradicted earlier research. Namely, for the present sample of 6- to 17-year-olds, likelihood of bullying victimization was elevated when parent education level was relatively high. But when Hong et al. (2020) studied a sample of only 6- to 11-year-olds from the NSCH 2016 data set (not 2018), they found a negative association. The present study showed an association in negative direction between likelihood of being bullied and the variables family cohesiveness and neighbor support (Hong et al., 2020). On the other hand, likelihood of being bullied had no association with emotional support from family, professionals, and peer/religious groups. These results imply that children are protected when cohesiveness with family and neighbors are strong. Like some prior ones, the present study showed increased likelihood of bullying victimization among children diagnosed with ADHD, depression, anxiety, behavioral/conduct problem, or Tourette syndrome (Abada et al., 2008; Cappadocia et al., 2012; Charania et al., 2019; Crawford & Manassis, 2011; DeJonckheere et al., 2017; Mayes et al., 2015; Pontillo et al., 2019; Simmons & Antshel 2021; Yockey et al., 2019; Zinner et al., 2012). Tourette syndrome, however, yielded the strongest odds-ratio or association with likelihood of being bullied. In addition, unlike a study with a psychiatric sample of children (Mayes et al., 2015), the present study did not link diagnoses of autism spectrum disorder and pervasive 697 developmental disorder to children’s experience of being bullied. The present study did suggest that bullying victimization was relatively likely among children of parents with poor mental health (Cappadocia et al., 2012) or a substance use problem (Eiden et al., 2010), compared to other children. So, child mental health problems along with nonsupportive parenting arising from parent mental health problems are disadvantageous where likelihood of bullying is concerned. Moreover, it must be remembered that mental health problems in children may be among the adverse consequences of bullying victimization. The present results indicated no association between children’s being covered by a health insurance policy and their likelihood of being bullied; it is probably the case that many bullied children seek no help from professionals to address mental health problems triggered by victimization. Concerning acculturation and bullying victimization, the present findings support at least one prior study of Latino immigrant children in finding that children belonging to first- and second-generation immigrant families had a lower likelihood of being bullied versus children belonging to third-generation families (Peguero, 2009). However, development of some interaction terms during additional analysis led the present study to contradict other published results. The interaction term linking ethnic Asian child and first-generation immigrant family showed a negative association with likelihood of being bullied (OR .14, p < .01), unlike the positive association shown by a national study of ­10th-graders from some two decades ago (Peguero, 2009). This means that, in the present study, first-generation Asian immigrant children were less likely to be bullied than were second- and third-generation ethnic Asian children. This study found the percentage of first-generation child respondents of all ethnicities who were bullied was 28.4%; of all second-generation child respondents was 37.3%; and 36.2% of children from these two generations were bullied. The majority of children in this study who belonged to first- and second-generation immigrant families were not bullied. Still, the study’s finding of a strong link between bullying victimization and racial discrimination suggests that many immigrant children witness race-based bullying; that fact may discourage or at least complicate their efforts towards acculturation. This study with children 6–17 years old found no association between child bullying victimization and speaking of English at home. In that, it differs from 1997 research with a nationally representative sample of children 12–17 years old (Yu et al., 2003). Acculturation-related results from the present study suggest immigrant children are unlikely to be bullied early on in the acculturation process. This is due in part to their tendency to feel alienated by and even withdraw from mainstream culture (Chaudry et al., 2010; Pumariega & Rothe, 2010). As children’s acculturation 13 698 significantly progresses, they may become more likely to experience bullying victimization (Peguero, 2009). Consistent with prior research, the present study found younger (under age 14) children were more likely than older (14 and up) ones to be bullied (Cappadocia et al., 2012; Holt et al., 2014; U.S. Department of Education, 2011). Present findings were also consistent with the literature in showing an association in positive direction between being a girl and being bullied (Merrill & Hanson, 2016). Conclusion Examination of 2018 data from a nationally representative sample of 6- to 17-year-old immigrant and nonimmigrant children, using the multiple disadvantage model, identified key factors in U.S. children’s bullying victimization. Perhaps most important is the results’ implication that intervention can be of most benefit to bullied children who have been discriminated against because of their race/ethnicity. Social policies that, inadvertently or not, tend to perpetuate prejudice and discrimination should certainly be reevaluated, and perhaps abolished. Social service professionals who work with families are responsible to raise clients’ awareness of bullying and its adverse effects on child mental health. The present study was constrained by two limitations. First, the study used measures of child and parent factors which NSCH provided but which did not represent clinical evaluations or standardized scales. Examples are the measures for rundown neighborhood, safe neighborhood, social-emotional supports, and mental health. Generalizing any results that involved such proxy measure requires caution. Second, less than 18% of children in the present sample belonged to first- or second-generation immigrant families. That fact limits the study’s illustration of acculturation. Future research might use longitudinal data to explore bullying of children. Such an analysis could prove particularly helpful for understanding bullying victimization within a child-development context. For better understanding any relationship of bullying victimization to the acculturation process, future research might focus exclusively on first- and second-generation immigrant families, looking specifically at the country of origin and at length of residence in the U.S. Also, researchers should consider examining relationships between children’s bullying victimization and their own specific health-related behaviors (e.g., substance use, aggression). Of course, to obtain the full picture of bullying among children will require studying respondents who both suffer and perpetrate bullying. 13 Community Mental Health Journal (2022) 58:689–700 Author Contributions All authors contributed to the study conception, design, material preparation, data collection and analysis. All authors read and approved the final manuscript. Funding The authors did not receive funding support from any organization for the submitted work. Declarations Conflict of interest The authors declare that they have no conflict of interest. References Abada, T., Hou, F., & Ram, B. (2008). The effects of harassment and victimization on self-rated health and mental health among Canadian adolescents. Social Science & Medicine, 67(4), 557–567. https://doi.org/10.1016/j.socscimed.2008.04.006 Akobirshoev, I., Bowser, D., Parish, S. L., Thomas, C., & Bachman, S. S. (2017). Does parental health mediate the relationship between parental Uninsurance and insured Children’s Health Outcomes? Evidence from a US National Survey. Health & Social Work, 42(2), E68–E76. https://doi.org/10.1093/hsw/hlx003 Cappadocia, M. C., Weiss, J. A., & Pepler, D. (2012). Bullying experiences among children and youth with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(2), 266–277. https://doi.org/10.1007/s10803-011-1241-x Carson, N. J., Stewart, M., Lin, J. Y., & Alegria, M. (2011). Use and quality of mental health services for Haitian youth. Ethnicity & Health, 16(6), 567–582. https://doi.org/10.1080/13557858.2011. 586024 Celenk, O., & Van de Vijver, F. J. R. (2011). Assessment of acculturation: Issues and overview of measures. Online Readings in Psychology and Culture, 8(1), 10. Charania, S. N., Danielson, M., Bitsko, R., Claussen, A., & LeburnHarris, L. A. (2019). Bullying victimization and perpetration among children with Tourette’s disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 58(10), S187–S187. https://doi.org/10.1016/j.jaac.2019.08.143 Chaudry, A., Capps, R., Pedroza, J. M., Castañeda, R. M., Santos, R., & Scott, M. M. (2010). Facing our future: Children in the aftermath of immigration enforcement. The Urban Institute. Cheng, T. C., & Lo, C. C. (2015). Racial disparities in intimate partner violence and in seeking help with mental health. Journal of Interpersonal Violence, 30(18), 3283–3307. Cheng, T. C., & Lo, C. C. (2016). Racial disparities in children’s health: A longitudinal analysis of mothers based on the multiple disadvantage model. Journal of Community Health, 41(4), 753–760. Child and Adolescent Health Measurement Initiative. (2020). 2018 National Survey of Children’s Health: SPSS Codebook for Data Users (Data Resource Center for Child and Adolescent). U.S. Department of Health and Human Services. Cook, C. R., Williams, K. R., Guerra, N. G., Kim, T. E., & Sadek, S. (2010). Predictors of Bullying and Victimization in Childhood and Adolescence: A Meta-analytic Investigation. School Psychology Quarterly, 25(2), 65–83. https://doi.org/10.1037/a0020149 Crawford, A. M., & Manassis, K. (2011). Anxiety, social skills, friendship quality, and peer victimization: An integrated model. Journal of Anxiety Disorders, 25(7), 924–931. https://doi.org/10.1016/j. janxdis.2011.05.005 DeJonckheere, M. J., Vaughn, L. M., & Jacquez, F. (2017). Latino immigrant youth living in a nontraditional Migration City: A social-ecological examination of the complexities of stress and Community Mental Health Journal (2022) 58:689–700 resilience. Urban Education, 52(3), 399–426. https://doi.org/10. 1177/0042085914549360 Eiden, R. D., Ostrov, J. M., Colder, C. R., Leonard, K. E., Edwards, E. P., & Orrange-Torchia, T. (2010). Parent alcohol problems and peer bullying and victimization: Child gender and toddler attachment security as moderators. Journal of Clinical Child and Adolescent Psychology, 39(3), 341–350. https://doi.org/10.1080/ 15374411003691768 Espelage, D. L., Bosworth, K., & Simon, T. R. (2000). Examining the social context of bullying behaviors in early adolescence. Journal of Counseling and Development, 78(3), 326–333. https://doi.org/ 10.1002/j.1556-6676.2000.tb01914.x Finno-Velasquez, M., Cardoso, J. B., Dettlaff, A. J., & Hurlburt, M. S. (2016). Effects of parent immigration status on mental health service use among latino children referred to child welfare. Psychiatric Services, 67(2), 192–198. https://doi.org/10.1176/appi. ps.201400444 Flores, G., & Vega, L. R. (1998). Barriers to health care access for Latino children: A review. Family Medicine, 30(3), 196–205. Gladden, R. M., Vivolo-Kantor, A. M., Hamburger, M. E., & Lumpkin, C. D. (2014). Bullying surveillance among youths: Uniform definitions for public health and recommended data elements, version 1.0. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, U.S. Department of Education. Guerrero, A. D., Ponce, N. A., & Chung, P. J. (2015). Obesogenic dietary practices of Latino and Asian subgroups of children in California: An analysis of the California Health Interview Survey, 2007–2012. American Journal of Public Health, 105(8), E105– E112. https://doi.org/10.2105/ajph.2015.302618 Gulbas, L. E., Zayas, L. H., Yoon, H., Szlyk, H., Aguilar-Gaxiola, S., & Natera, G. (2016). Deportation experiences and depression among US citizen-children with undocumented Mexican parents. Child Care Health and Development, 42(2), 220–230. https://doi.org/ 10.1111/cch.12307 Holt, T. J., Turner, M. G., & Exum, M. L. (2014). The impact of self control and neighborhood disorder on bullying victimization. Journal of Criminal Justice, 42(4), 347–355. https://doi.org/10. 1016/j.jcrimjus.2014.04.004 Hong, J. S., Song, E. J., Peguero, A. A., Wu, C. F., & Schmaeman, A. C. (2020). Can family and neighborhood cohesiveness buffer the association between family economic hardship and children’s peer victimization? Families in Society-the Journal of Contemporary Social Services, 101(3), 382–394. https://doi.org/10.1177/10443 89419895853 Jackson, D. B., Vaughn, M. G., & Kremer, K. P. (2019). Bully victimization and child and adolescent health: New evidence from the 2016 NSCH. Annals of Epidemiology, 29, 60–66. https://doi.org/ 10.1016/j.annepidem.2018.09.004 Jawaid, A., Riby, D. M., Owens, J., White, S. W., Tarar, T., & Schulz, P. E. (2012). “Too withdrawn” or “too friendly”: Considering social vulnerability in two neuro-developmental disorders. Journal of Intellectual Disability Research, 56(4), 335–350. https://doi.org/ 10.1111/j.1365-2788.2011.01452.x Koo, D., Peguero, A., & Shekarkhar, Z. (2012). The “model minority” victim: Immigration, gender, and Asian American vulnerabilities to violence at School. Journal of Ethnicity in Criminal Justice, 10(2), 129–147. https://doi.org/10.1080/15377938.2011.609405 Lakey, P. N. (2003). Acculturation: A review of the literature. Intercultural Communication Studies, 7(2), 103–118. Lim, S. J. J., & Hoot, J. L. (2015). Bullying in an increasingly diverse school population: A socio-ecological model analysis. School Psychology International, 36(3), 268–282. https://doi.org/10.1177/ 0143034315571158 Lo, C. C., Howell, R. J., & Cheng, T. C. (2013). Explaining black-white differences in homicide victimization. Aggression and Violent Behavior, 18, 125–134. 699 Lo, C. C., Howell, R. J., & Cheng, T. C. (2015). Racial disparities in age at time of homicide victimization: A test of the multiple disadvantage model. Journal of Interpersonal Violence, 30(1), 152–167. Mayes, S. D., Calhoun, S. L., Baweja, R., & Mahr, F. (2015). Maternal ratings of bullying and victimization: Differences in frequencies between psychiatric diagnoses in a large sample of children. Psychological Reports, 116(3), 710–722. https://doi.org/10.2466/16. PR0.116k30w8 McConnell, D., Breitkreuz, R., & Savage, A. (2011). From financial hardship to child difficulties: Main and moderating effects of perceived social support. Child Care Health and Development, 37(5), 679–691. https://d oi.o rg/1 0.1 111/j.1 365-2 214.2 010. 01185.x Mendez, J. J., Bauman, S., Sulkowski, M. L., Davis, S., & Nixon, C. (2016). Racially-focused peer victimization: Prevalence, psychosocial impacts, and the influence of coping strategies. Psychology of Violence, 6(1), 103–111. https://doi.org/10.1037/a0038161 Merrill, R. M., & Hanson, C. L. (2016). Risk and protective factors associated with being bullied on school property compared with cyberbullied. BMC Public Health. https://doi.org/10.1186/ s12889-016-2833-3 Ong, M. S., Lakoma, M., Bhosrekar, S. G., Hickok, J., McLean, L., Murphy, M., et al. (2021). Risk factors for suicide attempt in children, adolescents, and young adults hospitalized for mental health disorders. Child and Adolescent Mental Health. https://doi.org/ 10.1111/camh.12400 Peguero, A. A. (2009). Victimizing the children of immigrants Latino and Asian American student victimization. Youth & Society, 41(2), 186–208. https://doi.org/10.1177/0044118x09333646 Pontillo, M., Tata, M. C., Averna, R., Demaria, F., Gargiullo, P., Guerrera, S., et al. (2019). Peer victimization and onset of Social anxiety disorder in children and adolescents. Brain Sciences. https:// doi.org/10.3390/brainsci9060132 Pumariega, A. J., & Rothe, E. (2010). Leaving no children or families outside: The challenges of immigration. American Journal of Orthopsychiatry, 80(4), 505–515. https://doi.org/10.1111/j. 1939-0025.2010.01053.x Pumariega, A. J., Rothe, E., & Pumariega, J. B. (2005). Mental health of immigrants and refugees. Community Mental Health Journal, 41(5), 581–597. https://doi.org/10.1007/s10597-005-6363-1 Ragavan, M. I., Li, W. D., Elwy, A. R., Cowden, J. D., & Bair-Merritt, M. (2018). Chinese, vietnamese, and Asian Indian parents’ perspectives about well-child visits: A qualitative analysis. Academic Pediatrics, 18(6), 628–635. https://doi.org/10.1016/j.acap.2017. 11.003 Santiago, C. D., Gudino, O. G., Baweja, S., & Nadeem, E. (2014). Academic achievement among immigrant and US-born Latino adolescents: Associations with cultural, family, and acculturation factors. Journal of Community Psychology, 42(6), 735–747. https://doi.org/10.1002/jcop.21649 Seaton, E. K., Neblett, E. W., Cole, D. J., & Prinstein, M. J. (2013). Perceived discrimination and peer victimization among African American and Latino Youth. Journal of Youth and Adolescence, 42(3), 342–350. https://doi.org/10.1007/s10964-012-9848-6 Shea, M., Wang, C. X., Shi, W. N., Gonzalez, V., & Espelage, D. (2016). Parents and teachers’ perspectives on School Bullying Among Elementary School-Aged Asian and Latino Immigrant Children. Asian American Journal of Psychology, 7(2), 83–96. https://doi.org/10.1037/aap0000047 Sidhu, S. S., & Song, S. J. (2019). Growing up with an undocumented parent in America: Psychosocial adversity in domestically residing immigrant children. Journal of the American Academy of Child and Adolescent Psychiatry, 58(10), 933–935. https://doi. org/10.1016/j.jaac.2019.05.032 13 700 Simmons, J. A., & Antshel, K. M. (2021). Bullying and depression in Youth with ADHD: A systematic review. Child & Youth Care Forum. https://doi.org/10.1007/s10566-020-09586-x Spencer, M. S., Chen, J. A., Gee, G. C., Fabian, C. G., & Takeuchi, D. T. (2010). Discrimination and mental health-related service use in a National Study of Asian Americans. American Journal of Public Health, 100(12), 2410–2417. https://doi.org/10.2105/ ajph.2009.176321 U.S. Department of Education. (2011). Student reports of bullying and cyber-bullying: Results from the 2009 School Crime Supplement to the National Crime Victimization Survey. U.S. Department of Education. Walton, L. M. (2018). The effects of “bias based bullying” (BBB) on health, education, and cognitive-social-emotional outcomes in children with minority backgrounds: Proposed comprehensive public health intervention solutions. Journal of Immigrant and Minority Health, 20(2), 492–496. https://doi.org/10.1007/ s10903-017-0547-y Wang, K., Chen, Y., Zhang, J., & Oudekerk, B. A. (2020). Indicators of school crime and safety: 2019 (NCES 2020-063/NCJ 254485). Washington, DC: National Center for Education Statistics, U.S. Department of Education, and Bureau of Justice Statistics, Office of Justice Programs, U.S. Department of Justice. Waylen, A., & Stewart-Brown, S. (2010). Factors influencing parenting in early childhood: A prospective longitudinal study focusing on change. Child Care Health and Development, 36(2), 198–207. https://doi.org/10.1111/j.1365-2214.2009.01037.x Wong, M. S., Showell, N. N., Bleich, S. N., Gudzune, K. A., & Chan, K. S. (2017). The association between parent-reported provider communication quality and child obesity status: Variation by parent obesity and child race/ethnicity. Patient Education and Counseling, 100(8), 1588–1597. https://doi.org/10.1016/j.pec. 2017.03.015 13 Community Mental Health Journal (2022) 58:689–700 Woolhouse, H., Brown, S., Krastev, A., Perlen, S., & Gunn, J. (2009). Seeking help for anxiety and depression after childbirth: Results of the Maternal Health Study. Archives of Womens Mental Health, 12(2), 75–83. https://doi.org/10.1007/s00737-009-0049-6 Yockey, R. A., King, K. A., & Vidourek, R. A. (2019). School factors and anxiety disorder among Hispanic youth: Results from the 2016 US National Survey on Children’s Health. School Psychology International, 40(4), 403–415. https://doi.org/10.1177/ 0143034319849621 Yoshikawa, H., & Kalil, A. (2011). The effects of parental undocumented status on the developmental contexts of young children in immigrant families. Child Development Perspectives, 5(4), 291–297. https://doi.org/10.1111/j.1750-8606.2011.00204.x Yu, S. M., Huang, Z. J., Schwalberg, R. H., Overpeck, M., & Kogan, M. D. (2003). Acculturation and the health and well-being of US immigrant adolescents. Journal of Adolescent Health, 33(6), 479–488. https://doi.org/10.1016/s1054-139x(03)00210-6 Zea, M. C., Asner-Self, K. K., Birman, D., & Buki, L. P. (2003). The Abbreviated Multidimensional Acculturation Scale: Empirical validation with two latino/latina samples. Cultural Diversity & Ethnic Minority Psychology, 9(2), 107–126. https://doi.org/10. 1037/1099-9809.9.2.107 Zinner, S. H., Conelea, C. A., Glew, G. M., Woods, D. W., & Budman, C. L. (2012). Peer victimization in youth with tourette syndrome and other chronic tic disorders. Child Psychiatry & Human Development, 43(1), 124–136. https://doi.org/10.1007/ s10578-011-0249-y Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Community Mental Health Journal is a copyright of Springer, 2022. All Rights Reserved.