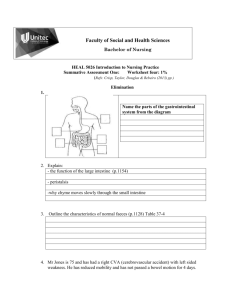
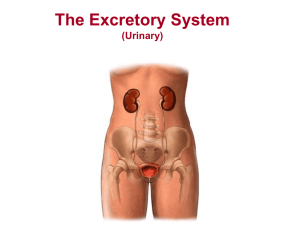
At the end of the session, students will be able to: Define Urinary tract infection Explain the causes Identify the clinical manifestations seen in different age groups Explain the treatment Define the glomerulonephritis Identify the clinical manifestations and treatment Define nephrotic syndrome Explain the pathophysiology Identify the clinical manifestations Explain the nursing care and therapeutic management Define inguinal hernia Identify clinical manifestation and treatment Define hydrocele and identify the therapeutic management Define undescended testes and identify the clinical manifestation Discuss the therapeutic management of this condition Define hypospadias and identify the therapeutic management Define epispadias and identify the therapeutic management UTI is a clinical condition that may involve lower urinary tract and upper urinary tract UTI is applied to presence of a significant number of micro-organisms anywhere within the urinary tract except to distal 1/3 of urethra Urinary tract infections (UTI) is common in the pediatric age group Early recognition and prompt treatment of UTI are important to prevent progression of infection • To pyelonephritis or urosepsis and • To avoid late sequelae such as renal scarring or renal failure. UTI generally begins in the bladder due to ascending infection from perineal contaminants, usually bowel flora such as Escherichia coli. In neonates, infection of the urinary tract is assumed to be due to hematogenous rather than ascending infection. This etiology may explain the nonspecific symptoms associated with UTI in these patients. Infants and young children with UTI may present with few specific symptoms. Older pediatric patients are more likely to have symptoms and findings Newborn and children below 2 Resemble GI disorders: failure to thrive, feeding problems, vomiting, diarrhea, abdominal distention and jaundice Newborns may have fever, hypothermia or sepsis. Frequent or infrequent voiding, constant squirming and irritability, strong smelling urine, and abnormal stream. Children more than 2 years of age: Enuresis, or daytime incontinence – toilet trained children Fever Strong or foul smelling urine Increased frequency or urination, dysuria or urgency Abdominal May pain have hematuria Antibiotic therapy Prophylactic antibiotic for recurrent UTI Ultrasound Voiding Cystogram: It is the inflammation of the tiny filters in the kidney (glomeruli) Most cases are post infectious: pneumococcal, streptococcal and viral infections Presumed as a result from immune complex formation and glomerular disposition Impairment of selective filtering properties of the kidney leading to a decreased GFR Molecules normally not filtered such as constituents of the blood, pass into the urine and are excreted Oliguria Periorbital Oedema (worse in the morning) Loss of appetite Dark coloured urine Antecedent streptococcal infection Hypertension Circulatory congestion Haematuria Proteinuria Decreased urine output Hypertensive encephalopathy Acute cardiac de-compensation Acute renal failure Maintenance of fluid balance Vital signs, body weight and I/O Management of hypertension Loop diuretics Calcium channel blockers Beta blockers Nutrition Depends on stage / edema Sodium intake is limited Potassium intake is restricted during oliguria Antibiotics Variety of disease processes where there is direct attack on the kidney or secondary the previously damaged glomeruli Treatment Some of underlying disease form of CGN treated with corticosteroids and cytotoxic agents In case of renal failure: dialysis and renal transplantation Defined as massive proteinuria, hypoalbunemia, hyperlipidemia and oedema Increased glomerular permeability to plasma protein resulting in massive protein loss Minimal change nephrotic syndrome; most common form of primary disease Secondary nephrotic syndrome: associated with another disease Congenital nephrotic syndrome: hereditary form The glomerular membrane becomes permeable to protein specially albumin, which leak through the membrane and is lost in urine (hyperalbuminuria) Reduces serum albumin – Hypoalbuminemia Increased hepatic synthesis of protein and lipids – hyperlipidemia Fluid accumulate in the interstitial spaces (edema) and body cavities e.g. ascites Sudden weight gain Puffiness of the face especially around the eyes Generalized oedema (anasarca) Skin pallor, changes in nail colour Rapid weight gain Labial or scrotal swelling Decreased urine output Evaluate a child who exhibits the following for the possibility of nephrotic syndrome: Periorbital, Weight gonadal or lower extremity edema. gain greater than that expected based on previous pattern. Decreased Pallor urinary output. fatigue. History Clinical manifestations Urinalysis Total serum protein Renal biopsy General measures Diet Corticosteroid therapy Immunosuppressant Prevention Family therapy of infection support and home care Most cases of minimal change disease eventually remit permanently. Inguinal hernia is when persistence of all parts or part of processus vaginalis during the 8th month of gestation. The upper part of processus vaginalis does not atrophy. Therefore abdominal fluid or abdominal structure can be forced into it creating a palpable bulge or mass A painless inguinal swelling that disappears during period of rest or is reduced by gentle compression. Appears when infant cries or strains. In older children: it appears when strains, coughs or stands for a long time. Symptoms appears when abdominal content or loop of intestines become partially obstructed – irritability, tenderness, anorexia, abdominal distention, difficulty defecation. Prompt elective surgery Nursing care Pre-operative and post operative care for general abdominal surgeries It is the presence of fluid in the processus vaginalis and or result of same developmental defect as in inguinal hernia It can be Non-communicating Communicating Prompt elective surgery Nursing care Pre-operative and post operative care for general abdominal surgeries It is failure of one or both testes to descend normally through the inguinal canal into the scrotum Therapeutic management If the testes do not descend between 1 an 2 years of age orchiopexy is performed Urethral opening is located below the glans penis or any where along ventral surface of the penile shaft Surgical correction of the deformity Objectives are Enhance child’s ability to void in standing position Improve physical appearance of genitalia Preserve a sexually adequate organ Usually presented with bladder exstrophy In epispadiasis there is failure of urinary canalization and urethral opening seen on dorsal surface of penile shaft Preservation Attainment Adequate of renal function of urinary control reconstructive repair Prevention of UTI Preservation of maximum external genitalia with continence and sexual function