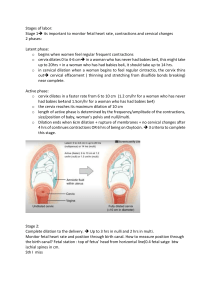
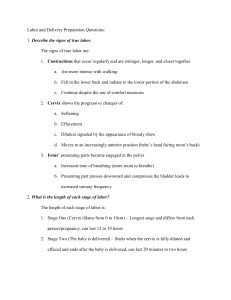
NCM 107: Care of Mother, Child, Adolescent (Well-Client) DEFINITION OF TERMS 1. Labor - - A series of events by which uterine contraction and abdominal pressure expel a fetus and placenta from the uterus Begins within 37–42 weeks ➔ Considered the term age of pregnancy Primipara: 14–16 hours Multipara: 6–8 hours However, this could be longer. Recently, research suggests that this could be longer. 2. Episiotomy - - - - - A surgical incision made at the opening of the vagina during childbirth to aid a difficult delivery and prevent rupture of tissues 2 kinds of Episiotomy: A. Midline – lesser chance of bleeding, less painful B. Mediolateral – less risk of greater laceration Allows the accommodation of the fetal head In the perineum, as the mother is delivering her child, if the doctor sees that the fetal head needs some assistance in being delivered, the doctor or obstetrician may opt to make a small cut at the perineal area In order to facilitate the delivery of the fetus and at the same time prevent further injury One of the duties of a student nurse is to support the perineum using the hands and a towel so that as the mother delivers the child, the perineal incision or the episiotomy won’t tear all the way down. ➔ Support the perineal area in order to prevent that from further lacerating Each kind of episiotomy have their pros and cons but in the end, it will be the obstetrician who will decide which one is the more appropriate incision for the mother. MODULE 3F: INTRA-NATAL CARE 3. Duration - Length of a uterine contraction How long a contraction lasts 4. Intensity - Strength of a uterine contraction 5. Frequency - Measured from the beginning of one contraction to the beginning of the next As labor increases, the frequency also increases 6. Increment - Building-up phase of the contraction 7. Acrement - Peak of the contraction 8. Decrement - Letting down phase of the contraction Interval - Space between two contractions The Augmentation of Labor and Induction of Labor procedures help initiate or at least strengthen labor. 9. Augmentation of Labor - - Assisting labor that has spontaneously started but is not effective or strong enough As the mother approaches true labor, there may be times wherein her labor contractions are not strong enough or not effective enough and that could cause her to be prolonged in a certain stage In order to enhance that labor, the obstetrician can administer oxytocin through IV fluids Other way to augment the labor is through amniotomy ➔ Artificial rupture of membranes during labor ➔ The mother would experience bursting of the bag of waters. Sometimes, it doesn’t happen spontaneously during labor so the YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) doctor can actually induce that using forceps in order to rupture the bag of waters so that labor can be triggered ➔ In that case if that is the reason why she requires CS, there is a chance that in her following delivery, she would still need to undergo CS ➔ But there are also some mothers whose reason may not be the shape of the pelvis but other reasons and maybe this mother would want to try vaginal birth instead. So, instead of going to vaginal birth directly, the mother would still have to undergo through trial of labor wherein the obstetrician will observe and assess if the mother is ready for a normal spontaneous vaginal delivery. 10. Induction of Labor - - - Applicable when the mother is already of term age. Around 37-40 weeks of gestation but has not yet initiated labor yet. The mother has not felt any contractions. Labor started artificially It can be inducted through oxytocin or amniotomy as well. But amniotomy is the most common. Labor that is started by the obstetrician rather than the mother’s body itself 11. Dysfunctional Labor - Prolonged labor due to the sluggishness of contractions Indication of augmentation of labor THEORIES OF LABOR Progesterone levels will decrease slightly during the later weeks of pregnancy especially as the mother approaches labor and delivery. - 12. Eutocia - Normal labor 13. Dystocia - Difficult labor How Does Labor Start? LABOR - 14. Amniotomy - Artificial rupture of membranes during labor 15. Trial of Labor - - - Full acronym is TOLAC (Trial of Labor after Cesarean Delivery) An attempt labor to determine whether labor will progress normally especially for women who have experienced cesarean section For women post-cesarean section Ideally, if the mother has experienced cesarean section in her previous delivery, she would ideally still be in cesarean section in the following delivery The mother would need to undergo cesarean delivery due to various reasons and one of that is the shape of her pelvis is not wide enough or not conducive enough for labor and delivery MODULE 3F: INTRA-NATAL CARE This is actually due to various factors and one of the theorized factors is actually due to the increase of estrogen and also the increase in prostaglandins. - Series of events by which uterine contractions and abdominal pressure expel a fetus and placenta from uterus Normally begins between 37 and 42 weeks of pregnancy Many factors known to be responsible for the initiation of spontaneous labor: 1. Uterine muscle stretching resulting in release of prostaglandins • As the fetus continues to grow, it also continues to expand the uterus • One of the theories in labor that is the uterus expands to a certain size, the body recognizes it as the fetus being ready to be delivered therefore resulting in the release of prostaglandins in the uterine area YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) 2. Cervical pressure • Fetus pressing on the cervix stimulates the release of oxytocin from the posterior pituitary gland • As the fetus becomes bigger, the fetal head presses into the cervix so the fetus pressing the cervix can stimulate the release of oxytocin from the posterior pituitary gland • Oxytocin is also known as labor hormone Oxytocin stimulation + Prostaglandins - Oxytocin stimulation works together with prostaglandins to initiate contractions - Together, they are very much observed during the initiation of true labor or labor itself 3. Estrogen – Progesterone Ratio • Progesterone withdrawal: Increasing estrogen in relation to progesterone can trigger or initiate labor • Throughout pregnancy, we have there a stable ratio or sustained level of estrogen and progesterone, particularly progesterone. It’s actually the high levels of progesterone that prevents the initiation of uterine contractions. • Near the end of the pregnancy, what happens is progesterone, the pregnancy hormone, decreases. In this case, there is an increasing level of estrogen and that these two have an inverse relationship. • As the estrogen increases, especially due to the secretion of prostaglandins, progesterone will reduce or decrease. Or rather the prostaglandins will overpower the effects of progesterone, therefore leading to labor and delivery. 4. Placental Degeneration • Placenta is thought to have a set age • So, if the placenta reaches around 37 to 40 weeks of age, the placenta starts to degenerate because it has reached the peak of maturity and therefore could lead to labor and delivery MODULE 3F: INTRA-NATAL CARE 5. Rising Fetal Cortisol Levels • Reduction of progesterone and increase in prostaglandins • In the fetal area or the fetal side of the pregnancy, the fetus will experience secretion of rising fetal cortisol levels • The fetal cortisol levels can stimulate the increase of prostaglandins in the mother which will also inhibit or reduce progesterone 6. Fetal Membrane prostaglandin production • The fetal membrane also continues to secrete prostaglandins leading to labor and delivery PREPARATION FOR LABOR - Where we observe the signs and symptoms of a mother who is about to go through labor and delivery Preliminary Signs of Labor - - Subtle signs or symptoms Days or hours before labor begins. NOTE: These signs don’t occur on the same day during delivery. They could occur as early as days away from the labor It is important that you, especially when you are conducting your health teaching, it’s important to inform the mother of these signs, especially the first-time mother so that they will not panic and instead, they will have a better experience in preparing themselves for the upcoming labor and delivery 1. Lightening - - Sinking of fetal head into the true pelvis Changes in abdominal contours (“Decreasing” fundal height) Causes relief from diaphragmatic pressure ➔ Encourage deep breathing exercises for the mother in preparation for the labor and delivery There’s a chance if you take your Leopold’s maneuver again, you might notice a decrease in the fundal height. So, do not panic if you observe that. YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) ➔ That just means that the baby is sinking into 3. Excess energy the true pelvis or descended - Burst of adrenaline to provide energy for labor ➔ Because of this, there is lesser pressure in - The mother’s body actually recognizes that the the lungs and also in the abdominal area mother’s about to go and give birth. So, the - At the same time, the relief from the body also prepares by supplementing the diaphragmatic pressure and also from the mother with a burst of adrenaline especially abdomen, this may cause feelings of nausea. So, during delivery to provide energy for labor be mindful of that. At least you could explain it to the mother 4. Backache Primiparas: Approximately 10-14 days before labor Multiparas: On the day of labor/after the beginning of true labor 2. Slight weight loss - - 1-3 lbs. ➔ Due to the decreasing levels of progesterone which leads to increased fluid excretion, one of the effects of decreasing progesterone, which then leads to increased urine production Not the loss of fat but rather the loss of fluid Progesterone level decreases Increased fluid excretion Increased urine production - - - 5. Cervical Ripening - MODULE 3F: INTRA-NATAL CARE One of the most common complaints of mothers who are experiencing labor and delivery Onset of true labor contractions Intermittent, stronger than usual backache Labor contractions begin in the back Why backache? ➔ There’s the pressure because of the weight distribution and also more significantly is the location of your uterus ➔ In anatomy and physiology, the location of your uterus is retroperitoneal. So, the pain is actually strongest at the back and then it sweeps throughout the abdomen. When a nurse or a student nurse is assigned to perform labor watch, what you can do is to provide back rubs. ➔ Not too deep pressure just back rubs in order to relieve the pressure and also provide for relief from pain Cervix feels very soft upon palpation during internal examination ➔ In internal examination, what happens is the obstetrician will be inserting 2 of her fingers into the birth canal to both assess the cervical dilation and also the effacement ➔ The mother will be placed in a lithotomy position “Butter soft” (usual assessment finding) Goodell’s sign – earlobe consistency of cervix throughout pregnancy Marks the beginning of true labor Refers to the steady thinning of the cervix YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) waters has already been ruptured, amniotic fluid still continues to be produced until delivery. ➔ At least there’s still some fluid that is buffering the baby and also ensuring that the baby will be delivered properly 6. Rupture of Membranes - - - - - Sudden gush or scanty, slow seeping of clear fluid from the vagina Early rupture of membranes helps fetal head descent and engagement (engaged into the true pelvis) ➔ Therefore, the rupture of the bag of waters could lead to enhanced cervical dilation and labor progression Amniotic fluid continues to be produced until delivery of the membranes after the birth of the child Risks to need to watch out for ➔ Intrauterine Infection – labor does not before spontaneously by 24h ◼ You need to observe for maternal or intrauterine infection ➔ Umbilical Cord prolapse ◼ What happens is the umbilical cord of the baby may be pushed downwards and instead of the presenting head, that is really directly presenting into the cervix, you might find there an umbilical cord. ◼ This is very dangerous for the baby. ◼ You need to watch out for this as well. Amniotic fluid is colloquially known as bag of water. In movies, the pregnant mothers would say, “my water broke” ➔ This is actually the rupture of the bag of water Maybe, you may encounter some mothers who may be concerned especially if they early rupture of membranes. They may be concerned if the delivery is “dry”. ➔ One health teaching to give them is that it’s not possible because even if the bag of MODULE 3F: INTRA-NATAL CARE 7. Show - Internal cervical mucus plug has been released “Bloody Show” – blood from cervical capillaries mixed with mucus plug As the mother approaches true labor, her cervix will get rid of the mucus plug. The picture is what she may find in her pads. Sometimes it may be bloody Assure the mother that this is a normal finding because as the cervical mucus plug detaches from the cervix, some of the capillaries of the cervix will also rupture and will induce a slight bleeding. The blood from these capillaries may be mixed with the mucus plug. Therefore, leading to a bloody show. 8. Uterine Contractions - Braxton Hicks YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) ➔ Known as the trial contractions ➔ Can start Last week or days before labor begins ➔ May be extremely strong for the mother (but the frequency varies or there is no change in strength) - ➔ Localized mostly in the abdomen ◼ It does not radiate from the back or towards the legs ➔ Triggered due to decreasing progesterone levels ➔ Primigravid mothers may not be able to distinguish between Braxton Hicks and true contractions ◼ Assure them and also give them adequate health teaching ➔ You know that this is not yet true labor because the contractions is relieved by rest, activity, or repositioning True Labor ➔ Begin at the back and sweeps forward across abdomen and possibly legs ➔ Gradually increases in frequency and intensity ➔ Painful, wavelike, building and receding ➔ Not relieved by rest ◼ It constantly increases ➔ Uterus becomes hard on palpation, indentation with fingers is not possible ◼ When you try to palpate the fundus, it is hard and indentation cannot be done 3 Main Signs: - ➔ Because knowing this will help us create the nursing care plan of a mother who is undergoing labor and delivery ➔ It is really important not to just focus on the physiologic aspects but also focus on the psyche of the mother, assist her as she experiences her uterine contractions, etc… ➔ All of these components has to be good in order to ensure both the survival of the mother and the baby PASSAGE - - PASSENGER - Rupture of membranes Show or the bloody show Uterine contractions COMPONENTS OF THE BIRTHING PROCESS Successful labor depends on the 4 concepts or components: passage, passenger, powers, and psyche - A problem in one of these can significantly impact the progression of labor Why do we need to review this again and again? MODULE 3F: INTRA-NATAL CARE Mother’s pelvis Route a fetus must travel from the uterus through the cervix Fetopelvic disproportion – commonly caused by the insufficient pelvic structure ➔ One problem involving this factor ➔ In some examinations, the fetal head may be a bit too big for the pelvis ➔ If that’s the case, it is really not the fetal head that is too big but rather the uterus is not really conducive for labor and delivery Shape of Pelvis • Gynecoid (maternal pelvis) • Android • Anthropoid • Platypelloid Refers to the fetus and its ability to move through the passage Affected by the following fetal features • Fetal skull • Fetal Presentation (Cephalic) • Fetal Lie (Longitudinal) • Fetal Attitude • Fetal Position • Fetal Station POWER or POWERS - Uterine contractions Phases • Increment – building up phase (longest) • Acrement or Acme – peak of contraction YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) • Decrement – letting down phase - Characteristics • Duration ◼ Beginning of increment to end of decrement ◼ Early labor: 30 seconds ◼ Late labor: 60-90 seconds • Frequency ◼ Beginning of one contraction to the beginning of the next ◼ Early labor: 5-30 mins apart ◼ Late labor: 2-3 mins apart or even lesser • Intensity ◼ Measured through palpation itself or through insertion of intrauterine catheter • • • ◼ Can also contribute to the knowledge of the mother Past experiences Accomplishment of pregnancy tasks Feeling of control over situation STAGES OF LABOR FIRST STAGE OF LABOR - - From onset of true labor contractions until full cervical dilation Average – 12 hours • Primipara: 6-18 hours • Multipara: 2-10 hours Recent research suggests that normal labor can take longer Three Phases: 1. Latent Phase - PSYCHE - Maternal psychological state Feelings that the mother brings to the labor Apprehension, fear, wonder, excitement Factors affecting psychological readiness • Presences of support system ◼ Very crucial according to studies. ◼ The mother is able to undergo effective delivery with the presence of her partner or support system ◼ In the local setting, our institutions don’t allow the partner to be physically there for the mother. So, in lieu of the partner, we, nurses, get to be their support system ◼ We need to keep the family and the partner updated • Degree of preparation from the mother’s side • Childbirth education classes MODULE 3F: INTRA-NATAL CARE Begins at onset of regularly perceived uterine contractions - Ends when rapid cervical dilatation begins - Cervical dilation: 0-3 cm - Mild and short contractions • 20-40 seconds • May be irregular Longer for women with “nonripe” cervix - Primipara: around 6 hours - Multipara: 4 ½ hours Nursing Care: Pain Management ❖ Analgesia may be given but if given too early, it may prolong the stage ❖ Assist mother to prepare psychologically ❖ Teach controlled and deep breathing exercises ❖ Encourage activity, ambulation, and other non – pharmacotherapeutic measures ❖ Offer clear liquids or ice chips Involve partner, family, or support person ❖ Provide calm environment Psychological Maternal Responses - Anticipation - Excitement - Apprehension YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) 2. Active Phase - More rapid cervical dilatation (4-7 cm) Uncomfortable phase for the mother Stronger contractions (40-60 seconds every 3-5 minutes) - Bloody show and spontaneous rupture of membranes may occur - Primipara: around 3 hours - Multipara: around 2 hours Nursing Care ❖ Frequent perineal care ❖ Encourage mothers to keep active and assume most comfortable position except flat on back ❖ Pain management ❖ Anticipate mood swings and difficulty in coping (offer support) ❖ Continue to involve family and partner ❖ Positioning • Upright • Left side lying 3. Transition Phase - Cervical Dilatation (8-10 cm) Contractions reach peak of intensity Longer contractions (60-70 seconds every 2-3 minutes) - Full cervical dilatation and effacement - ROM may occur at full cervical dilation - Strong urge to push Nursing Care: ❖ Mothers may experience intense discomfort, nausea and vomiting, feeling of loss of control, anxiety, panic, or irritability ❖ Help direct maternal focus to birthing of baby ❖ Provide support ❖ Stay with the mother at all times SECOND STAGE OF LABOR - - Exhaustion Nursing Care: ❖ ❖ ❖ ❖ ❖ Assist with second stage pushing Prepare birthing area Assist mother in birthing position Be ready to assist in episiotomy Prepare for and assist with delivery Mother may feel: - Uncontrollable urge to push Nausea and vomiting (due to decrease in abdominal pressure) Cardinal Movements of Labor 1. Fetal Engagement, Descent, and Flexions 2. Internal Rotation - Of the fetal head at the internal perineum - Aligns fetal head in the most optimum position for descent (widest part at widest inlet area) - Perineum may appear bulging and tense - Anus may be everted; stool may be expelled - Crowning – fetal scalp visible at the opening of the vagina 3. Extension - Delivery of the head - Compression of presenting parts 4. External Rotation - Head rotates to being the anterior shoulders into the best line with the pelvis - Slight upward flexion needed to deliver posterior shoulder - Watch for: Shoulder dystocia in macrosomic babies 5. Expulsion of the baby - The baby is considered born once the entire body is already delivered and exposed to the extrauterine life Complete cervical dilatation to delivery of the neonate Lasts 2-60 minutes Primipara: 40 mins average Multipara: 20 mins average Fetus moved along the birth canal by the mechanisms of labor Psychological Maternal Responses: - Focus from discomfort to active pushing MODULE 3F: INTRA-NATAL CARE YUSON, DREA NCM 107: Care of Mother, Child, Adolescent (Well-Client) THIRD STAGE OF LABOR - Fourth Degree Begins with the birth of the infant and ends with the delivery of the placenta (1-30 mins) Entire perineum, rectal sphincter, and some of the mucous membrane of the rectum Two Phases: Signs: ➢ ➢ ➢ ➢ ➢ 1. Placental Separation Placenta detaches from the uterine wall Lengthening of the umbilical cord Sudden gush of vaginal blood Placenta is visible at the vaginal opening Uterus contracts and feels firm Presentations: Schultze and Duncan 2. Placental Expulsion Placenta is delivered through natural bearing down or gentle pressure on the contracted uterine fundus (Crede’s Maneuver) - No pressure on noncontracted uterus – can cause uterine eversion and massive hemorrhage - Excessive hemorrhage with poor contraction – administer Hemabate or Methergine (Check BP before administration) - Note time of placental delivery - Inspect intactness of placenta - Inspect for placental remains (leads to uncontracted uterus and bleeding) Psychological Maternal Responses: - Concern for neonate’s condition - Discomfort from uterine contractions before placental expulsion Nursing Care: ❖ Assist with the delivery of the placenta ❖ Assist with episiorrhaphy ❖ Administer oxytocin as ordered (IV) ❖ Introduce neonate to the parents and allow breastfeeding - Classification of Perineal Lacerations Classification Description of Involvement First Degree Vaginal mucous membrane and skin of the perineum to the fourchette Second Degree Vagina, perineal skin, fascia, levator ani muscle, and perineal body Third Degree Entire perineum, extending to reach the external sphincter of the rectum MODULE 3F: INTRA-NATAL CARE FOURTH STAGE OF LABOR - Time immediately after placental delivery First hour after delivery (recovery period) Beginning of the postpartum period Postpartum period: 6 weeks High risk for hemorrhage Psychological Maternal Responses: - Attention towards neonate Adjusting to maternal role Nursing Care: ❖ Primary activity is stabilizing the status of the neonate and helping neonate get acclimated to extrauterine life ❖ Focus on maternal-neonatal bonding ❖ Obtain vital signs every 15 mins for the first hour ❖ Assess lochia, consistency and position of the fundus, episiotomy site ❖ Be prepared to initiate emergency procedures if mother’s or child’s condition do not stabilize YUSON, DREA