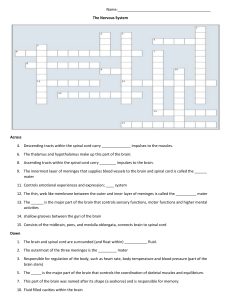
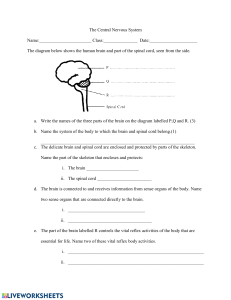
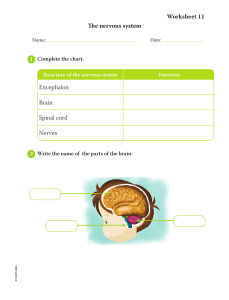
Spinal cord Dr.Jagadeesh Topic outcomes Topic outcomes: 3.1Describe the extent, size and coverings of spinal cord. 3.2 Define and distinguish the spinal segments. 3.3 Describe the internal structure : grey horns, group of neurons and white matter location of ascending and descending tracts. matter -columns, 3.4 Discuss the grey matter and white matter of spinal cord. 3.5 Describe the arteries and veins of spinal cord. 3.6 Explain the congenital anomalies of spinal cord. Introduction Spinal cord is the caudal part of central nervous system. Cylindrical in shape. 45 cm in length in adults. Average diameter 1cm Occupies upper two thirds of vertebral column. Extent: Beginning – foramen magnum/upper border of C1 vertebra. Termination – lower border of L1. External structure Coverings(Meninges) & spaces Covered by 3 meninges: • Dura mater • Archnoid mater • Pia mater Spaces: Outer to dura mater- extra dural space. Deep to dura mater- subdural space. Between the arachnoid & pia mater - subarachnoid space. Dura mater The dura mater is a dense, strong, fibrous membrane that encloses the spinal cord and the cauda equina. It is continuous above through the foramen magnum with the meningeal layer of dura covering the brain. Inferiorly, it terminates at the level of the lower border of the second sacral (S2) vertebra. The dural sheath lies loosely in the vertebral canal and is separated from the wall of the canal by the extradural space,which contains loose areolar tissue and the internal vertebral venous plexus. The dura mater extends along each nerve root and becomes continuous with the connective tissue surrounding each spinal nerve (epineurium). Arachnoid mater The arachnoid mater is a delicate impermeable membrane that covers the spinal cord and lies between the pia mater internally and dura mater externally. It is separated from the pia mater by a wide space, the subarachnoid space, which is filled with cerebrospinal fluid. The arachnoid mater is continuous above through the foramen magnum with the arachnoid covering the brain. Inferiorly, it ends at the level of the lower border of the second sacral vertebra. The arachnoid mater continues along the spinal nerve roots, forming small lateral extensions of the subarachnoid space. Pia mater & pial modifications The pia mater, a vascular membrane that closely covers the spinal cord and continues below the spinal cord as filum terminale which ends at the level of 1st coccygeal vertebra. Pia is thickened on either side between the nerve roots to form ligamentum denticulatum(21 pairs) which passes laterally to adhere to the arachnoid and dura so that the spinal cord is suspended in the middle of the dural sheath. Pia mater is thickened in the anterior median fissure to form median longitudanal band called linea splendens. Pial modifications: are filum terminale, ligamentum denticulatum, linea splendens Spinal cord enlargements Two enlargements: 1. Cervical enlargement - C3 to T2 spinal segments - Nerve supply to upper limb. 2. Lumbar enlargement - L1 to S3 spinal segments-Nerve supply to lower limb. Conus medullaris • Conical lower ending of the spinal cord is conus medullaris • Central canal is dilated to form terminal ventricle. Cauda equina • The bundle of nerve fibres arising from the conus medullaris is called cauda equina (tail of horse). Fissure and sulci • Anterior median fissure. • Posterior median sulcus. • Anterior lateral sulcus. • Posterior lateral sulcus. Spinal nerve roots • Dorsal root (DR) • Ventral root (VR) • Spinal ganglion (SG) or dorsal root ganglion • Spinal nerve ( SN) 31 pairs (8+12+5+5+1). Spinal nerve roots & Spinal nerve • Dorsal root has a ganglion made up of pseudounipolar cells. • With two processes - peripheral process is a dendrite. Central process is an axon. • Dorsal root Joins with the ventral root to form spinal nerve. • Spinal nerve divides into 2 rami - dorsal ramus & ventral ramus Spinal segments 31 spinal segments: • 8 Cervical (C) • 12 Thoracic (T) • 5 Lumbar (L) • 5 Sacral (S) • 1 Coccygeal (Co) Spinal segments Relation of the spinal segments to vertebral spines: • • • • • Cervical segments: - 1(C4 at C3) Upper thoracic: - 2 Lower thoracic: - 3 (T12 at T9). L 1 & L 2: at 10th thoracic spine. L 3 & L 4: at 11th thoracic spine. • L 5: at 12 th thoracic spine. • Sacral and coccygeal: L 1 lumbar spine. Spinal segments Internal structure Internal structure of Spinal cord Inner grey matter & outer white matter. Distribution of cell bodies in the grey matter. White matter has tracts & fibres. Internal structure of Spinal cord Grey matter On cross section, the grey matter is seen as an H-shaped pillar with anterior and posterior grey columns, or horns, united by a thin grey commissure containing the small central canal. A small lateral grey column or horn is present in the thoracic and upper lumbar segments of the cord. The amount of grey matter present at any given level of the spinal cord is related to the amount of muscle innervated at that level. Thus, grey matter is greatest in the cervical and lumbosacral enlargements of the cord, which innervate the muscles of the upper and lower limbs. Grey matter As in other regions of the central nervous system, the grey matter of the spinal cord consists of a mixture of nerve cell bodies and their processes, neuroglia, and blood vessels. The nerve cells are multipolar, and the neuroglia forms an intricate network around the nerve cell bodies and their neurites. Nerve cell groups in the Anterior grey column: Most nerve cells are large and multipolar, and their axons pass out in the anterior roots of the spinal nerves as alpha efferents, which innervate skeletal muscles. The smaller nerve cells are also multipolar, and the axons of many of these pass out in the anterior roots of the spinal nerves as gamma efferents, which innervate the intrafusal muscle fibers of neuromuscular spindles. The nerve cells of the anterior grey column may be divided into three groups : medial, central, lateral. 1. Medial group innervates the skeletal muscles of the neck and trunk, including the intercostal and abdominal musculature. 2. Central group innervate the diaphragm (phrenic nucleus), sternocleidomastoid and trapezius muscles (accessory nucleus). 3. Lateral group is present in the cervical and lumbosacral segments, innervates the skeletal muscles of the limbs. Grey matter Nerve cell groups in the Posterior grey column: Four nerve cell groups : two group that extend throughout the length of the cord & two group that are restricted to the thoracic and lumbar segments. 1. Substantia gelatinosa group - situated at the apex of the posterior grey column. Receives afferent fibers concerned with pain, temperature, and touch from the posterior root. 2. Nucleus proprius- situated anterior to the substantia gelatinosa. Receives fibers associated with the senses of position and movement (proprioception), two-point discrimination, and vibration. 3. Nucleus dorsalis (Clarke's column) - situated at the base of the posterior grey column and associated with proprioceptive endings (neuromuscular spindles and tendon spindles). 4. Visceral afferent nucleus - situated lateral to the nucleus dorsalis; it is associated with receiving visceral afferent information. Nucleus dorsalis and visceral afferent nucleus is absent in cervical and sacral region Grey matter Nerve cell groups in the Lateral grey column: The intermediolateral group of cells form the small lateral grey column, extends from the first thoracic to the second or third lumbar segment of the spinal cord. The cells are relatively small & give rise to preganglionic sympathetic fibers. Grey matter: REXED’S classification Lamina I – IV corresponds to dorsal horn head. Lamina V corresponds to neck. Lamina VI corresponds to base of dorsal horn. Lamina VII- corresponds to intermediate area. Lamina VIII & IX occupies the ventral horn Lamina X is the grey matter surrounding the central canal. White matter Funiculus or white columns: Anterior column Posterior column Lateral column. The columns contains ascending & descending tracts. Sources of nerve fibres of white matter Afferent fibres from dorsal root ganglion cells. Long ascending fibres from cells of spinal cord to supraspinal levels. Long descending fibres from supra spinal sources to the spinal cord cells. Efferent fibres from anterior and lateral grey column cells which pass into ventral roots of spinal nerves. Fibres making intra-segmental and inter-segmental connections within the cord. Sources of nerve fibres of white matter Tract Tract is a collection of nerve fibres within central nervous system connecting two masse of grey matter. Tract is a collection of nerve fibres having the same origin, course and termination. Tracts may be ascending or descending. Tracts are named after the masses of grey matter connected by them. E.g. – corticospinal tract, spinothalamic tract. Tracts are sometimes referred to as fasciculi or leminisci . Anterior funiculus Ascending tract: Anterior/ventral spinothalamic tract. Descending tracts: Anterior/ventral corticospinal Vestibulospinal Tectospinal Reticulospinal Lateral funiculus Ascending tracts: Descending tracts: Posterior spinocerebellar Anterior spinocerebellar Lateral spinothalamic Spinotectal Dorsolateral (tract of Lissauer) Lateral corticospinal Rubrospinal Lateral reticulospinal Olivospinal Descending autonomic fibres Posterior funiculus Ascending tracts: Medial part - Fasciculus gracilis. Lateral part - Fasciculus cuneatus. Descending tract: Septomarginal. Spinal cord tracts - Overall Descending tracts Descending tracts Begins in the cortical or subcortical areas and descends down to spinal cord. Controls motor activities, achieved by the interconnections between the major motor components of the nervous system. Divided into: - Pyramidal tract(corticospinal tract). - Extrapyramidal tracts. Major Descending tracts origin & function Tracts Origin Functions Corticospinal Lateral & anterior Motor cortex of cerebrum Controls voluntary movements Rubrospinal Red nucleus of midbrain Facilitatory influence of flexor tone Reticulospinal Medial & Lateral Reticular formation voluntary movements and muscle tone Tectospinal Superior colliculus Spinovisual reflexes Vestibulospinal Medial & Lateral Lateral vestibular nucleus Controls body equilibrium Olivospinal Inferior olivary nucleus Controls motor tone Pyramidal tract - Corticospinal tract Originates in the motor cortex. Pass through genu of the internal capsule, crus cerebri, pons, pyramids of medulla. Decussates and descends in the lateral column of the spinal cordlateral cortricospinal tract. 10% does not cross and descends in the anterior column of the spinal cord and form anterior corticospinal tract. They relay in the anterior horn cells of the spinal cord. These anterior horn cells project directly to muscle and control muscular contraction. Pyramidal tract - Corticospinal tract Pyramidal tract - Corticospinal tract Upper motor lesion- hemiplegia: • Loss of motor power – paralysis. • Increased muscle tone – spasticity. • Increased reflexes» Exaggerated knee jerk » Babinski’s positive • No wasting of muscles. Lower motor lesion – Poliomyelitis: • Loss of motor power- paralysis. • Loss of muscle tone. • Loss of reflexes. • Wasting of muscles. Corticobulbar tract Fibres originate in the region of sensorimotor cortex. Pass through posterior limb of internal capsule & middle portion of crus cerebri to the cranial nerve nuclei in the brain stem. Projects through cranial nerves to areas of supply for motor functions. Extrapyramidal tracts- Vestibulospinal tract Two components: Lateral vestibulospinal – arise from lateral vestibular nucleus in the brain stem and course downward, uncrossed, in the anterior funiculus of the spinal cord. Medial vestibulospinal – arise from medial vestibular nucleus in the brain stem and descend within the cervical spinal cord,with both crossed & uncrossed, in the anterior funiculus of the spinal cord to terminate at cervical levels. Function - provide excitatory input to extensor muscles. Extrapyramidal tracts- Rubrospinal tract Arises from the red nucleus of midbrain. Cross in the midbrain and descends in the pons, medulla and in the lateral column of the spinal cord. Synapses in the ventral horn interneurons of the spinal cord. Controls motor tone. Extrapyramidal tracts- Reticulospinal tract Arises in the reticular formation of the brain stem. Descends in both the ventral and lateral white columns. Both crossed and uncrossed descending fibres are present. Terminate on dorsal grey column neurons may modify transmission of sensation of body, egpain. Extrapyramidal tracts- Tectospinal tract Arises from superior colliculus of the midbrain. Decussates & passes through contralateral anterior white column. Relay in ventral grey interneurons. Function causes sudden movement of head in response to visual or auditory stimuli. Descending autonomic tracts Arising from the hypothalamus and brain stem. Project to preganglionic sympathetic neurons in the thoracolumbar segments spinal cord. To preganglionic parasympathetic neurons in sacral segments. Modulate autonomic functions. Medial longitudinal fasciculus Arises from vestibular nuclei in the brain stem. Descends run close to and intermingles tectospinal tract. Terminates in the ventral grey interneurons of the cervical segments of the spinal cord. Function coordinates head and eye movements. Ascending tracts Ascending tracts Ascending tracts are seen in spinal cord & brain stem. They are multineuronal pathways by which afferent impulses arising from various parts of the body are conveyed to different parts of the brain. Usually three set of neuron: - First order neuron - Second order neuron - Third order neuron. First order neurons- dorsal root ganglia Each neuron in dorsal root ganglion gives off a peripheral process & a central process. The peripheral processes of the neurons form the afferent fibres of peripheral nerves. They end in relation to sensory end organs situated in various tissues. The central processes of these neurons enter the spinal cord through the dorsal nerve roots. Second order neurons Having entered the spinal cord the central processes as a rule, terminate by synapsing with cells in spinal grey matter. Some of them may run upwards in the white matter of the cord to form ascending tracts. The majority of ascending tracts are however formed by axons of cells in spinal grey matter. These are second order neurons. Third order sensory neurons In the case of pathways that convey sensory information to the cerebral cortex the second order neurons end by synapsing with neurons in the thalamus. Third order sensory neurons located in the thalamus carry the sensations to the cerebral cortex. Major Ascending tracts & their functions Anterior spinothalamic –Simple touch and pressure. Lateral spinothalamic – Pain & temperature Fasciculus gracilis & Fasciculus cuneatus - Proprioceptiive impulses, vibration sense, fine touch, tactile localization & discrimination Anterior spinocerebellar -Proprioceptive impulses. Posterior spinocerebellar -Proprioceptive impulses. Spinotectal & spino olivary - Spinovisual reflexes. Dorsolateral tract -pain & temperature Spinothalamic tracts Anterior spinothalamic tract- ascend in the anterior funiculus and ascend to the medulla. Fibres of lateral spinothalamic tract enter the lateral funiculus. Merges with the medial lemniscus. Ascend through medulla, pons and midbrain (spinal lemniscus) End ultimately in the thalamus. End in the thalamus (VPL nucleus). Anterior spinothalamic tract Lateral spinothalamic tract Spinoreticular tract Begin from the spinal neurons mainly in lamina VII. Fibres are partly crossed & partly uncrossed. Fibres ascend in the ventrolateral part of the spinal cord, intermingling with spinothalamic tracts. They end in the reticular formation of the medulla & pons. Probably carries the pain. Spino-olivary tract Is also a crossed tract. It lies at the junction of the anterior & lateral funiculi of the spinal cord. The fibres of the tract end in accessory olivary nuclei. May carry exteroceptive impulses. Spino mesencephalic tract A number of tracts travel from spinal cord to different areas in the midbrain.They are collectively referred to as spinomesencephalic tracts. Spinotectal tract – connect spinal cord to the superior colliculus. It is a crossed tract. It carries impulses like pain & temperature, that regulate reflex movements of the head & eyes in response to stimulation of some parts of the body. Some reach pretectal nuclei or some reticular formation of midbrain. Spinocerebellar tracts Carry proprioceptive impulses arising in muscle spindles, Golgi tendon organs and other receptors in cerebellum. First order neurons of this pathway are located in dorsal nerve root ganglia. Central process of these neurons end in the spinal grey matter. Second order neurons are arranged in a number of groups. Dorsal spinocerebellar uncrossed– remains ipsilateral lying in the lateral funiculus. Ascends to the medulla become incorporated into the inferior cerbellar peduncle and reach cerbellum. Spinocerebellar tracts Blood supply of spinal cord Arterial supply The spinal cord receives its arterial supply from three small arteries. Two posterior spinal arteries and one anterior spinal artery. These longitudinally running arteries are reinforced by small segmental arteries that arise from arteries outside the vertebral column and enter the vertebral canal through the intervertebral foramina. Anterior and posterior spinal arteries anastomose on the surface of the cord and send branches into the substance of the white and grey matter. Arterial supply Anterior spinal artery: The anterior spinal artery is formed by the union of two arteries, each of which arises from the vertebral artery inside the skull. The anterior spinal artery then descends on the anterior surface of the spinal cord within the anterior median fissure. Branches from the anterior spinal artery supply the anterior two-thirds of the spinal cord. Arterial supply Posterior spinal arteries: The posterior spinal arteries arise either directly from the vertebral arteries inside the skull or indirectly from the posterior inferior cerebellar arteries. They descend on the posterior surface of the spinal cord close to the posterior nerve roots and gives off branches that enter the substance of the cord. The posterior spinal arteries supply the posterior one-third of the spinal cord. Arterial supply Segmental spinal arteries: At each intervertebral foramen, posterior and anterior spinal arteries are reinforced by small segmental arteries on both sides. The arteries are branches of deep cervical, intercostal, and lumbar arteries. Segmental artery enters the vertebral canal, gives rise to anterior and posterior radicular arteries that accompany the anterior and posterior nerve roots to the spinal cord. Additional feeder arteries enter the vertebral canal.One large feeder artery, the great anterior medullary artery of Adamkiewicz, arises from the aorta a major source of blood to the lower twothirds of the spinal cord. Arterial supply Venous drainage Through internal vertebral venous plexus. 6 longitudinal spinal veins. They communicate superiorly within the skull with the veins of the brain and the venous sinuses and drain through intervertebral foramina into: - Vertebral veins in the neck. - Azygos vein in the thorax. - Lumbar veins in the lumbar region. - Lateral sacral veins in the sacral region. Clinical importance Lumbar puncture Lumbar puncture: Obtaining the CSF from the lumbar cistern for diagnostic purposes. Done between L3 and L4 vertebrae. Layers that the spinal needle traverse are: 1. Skin 2. Superficial fascia 3. Supraspinous ligament 4. Interspinous ligament 5. Ligamentum flavum 6. Epidural space containing the internal vertebral venous plexus 7. Dura mater 8. Arachnoid mater. Spinal cord anomalies - Spina bifida occulta • Congenital absence of spinous process and lamina of vertebra. • No visible meninges or neural tissue. • Often incidental finding. Spinal cord anomalies - Spina bifida cystica Meningocele : • Congenital defect in vertebral arches with cystic distension of meninges. • No abnormality of neural tissue. Spinal cord anomalies - Spina bifida cystica Meningomyelocele: • Congenital defect in vertebral arches with cystic distension of meninges. • With structural or functional abnormality of spinal cord or cauda equina. Thank You