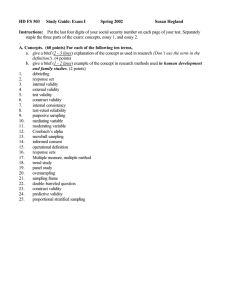
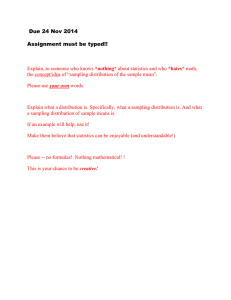
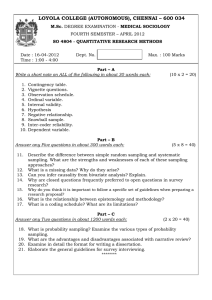
American University of Antigua College of Medicine Epidemiology & Biostatistics 1 Preclinical Science October 2023 Juan Manuel Lozano, MD, MSc Division of Medical and Population Health Sciences Educations and Research Herbert Wertheim College of Medicine, Florida International University Populations and Samples Juan Manuel Lozano, MD, MSc Division of Medical and Population Health Sciences Research Department of Medical Education Herbert Wertheim College of Medicine Florida International University Objectives Goal RU1.EB1.5 Understand advanced concepts in populations and samples in health research: inference, generalizability, and other errors in research. 1Q Given a clinical or research scenario, graph or table, students should be able to: RU1.EB1.5.1 Describe the main differences between probabilistic and nonprobabilistic sampling methods in descriptive and analytical studies. RU1.EB1.5.2 Contrast the most common sampling methods used in epidemiological health research in terms of inference (generalizability) RU1.EB1.5.3 Describe the main sources of error in the selection of samples: random error (chance) and systematic error (bias) RU1.EB1.5.4 Correlate validity with eligibility criteria, sampling methods, and the generation of systematic and random errors. All subjects in a population: o can rarely be studied. o do not need to be studied. o should not be studied. We can work on a sample of those subjects (from the population) by design and then generalize to the population (inference). Samples in health research Samples in health research Target or reference population: group to which the researcher intends to generalize findings. e.g., all children with learning disabilities in the US. Accessible population: portion of the target population that has a chance of being selected. e.g., children with learning disabilities in Miami's school system. Sample: subset of the accessible population that is selected. e.g., children with learning disabilities who attended school X and Y at a given date. Characteristics of a good sample 1. Representative of the target population: More easily achieved using probabilistic sampling methods. Particularly critical for descriptive studies like surveys. Main sources of bias: Voluntary bias. Nonresponse. 2. Adequate size: Large enough to control random sources of error. Not too large (avoid wasting resources). Steps for acquiring study subjects 1. Selection criteria: characteristics of the target population that serve the research question well. Inclusion: requirements to get subjects in. Exclusion: reasons to leave subjects out. 2. Sampling: selecting a subset of individuals from the accessible population. Selection criteria Inclusion: requirements to get in the study (relevant for research question, efficient for the study): Demographic (age, gender, etc.). Clinical (specific condition, severity, comorbidities, etc.). Geographic: place and setting. Temporal: time frame of the study. Exclusion criteria: subset of those who fulfill the inclusion criteria that need to be excluded because: Need to control some confounders. High likelihood of being lost to follow-up. Inability to provide good data. High risk of potential side effects. Table 3.1 Designing Selection Criteria for a Clinical Trial of Low Dose Testosterone to Enhance Libido in Menopause Design Feature Example Inclusion Specifying populations relevant to the research question and efficient for study: criteria (be specific) Demographic characteristics White women 50 to 60 years old Clinical characteristics Good general health Has a sexual partner Geographic characteristics Patients attending clinic at the investigator's hospital Temporal characteristics Between January 1 and December 31 of specified year Exclusion Specifying subsets of the population that will not be studied because of: criteria (be parsimonious) High likelihood of being lost to follow-up Alcoholic or plan to move out of state Inability to provide good data Disoriented or have a language barrier* High risk of possible adverse effects History of myocardial infarction or stroke *Alternatives to exclusion (when these subgroups are important to the research question) would be collecting nonverbal data or using bilingual staff and questionnaires. Probability (random): Driven by probabilistic methods (like a raffle). Participants have a known (but not necessarily equal) probability of being selected. Non-Probability: Driven by nonprobabilistic methods (“cherry picking”). Types of samples (some) Probability (random): Simple Systematic Stratified Proportional Disproportional Cluster Multistage Non-Probability: Convenience Purposive Quota Snowball Types of samples (some) Simple random sampling Each member of the population has an equal probability of being chosen. Requires having a list of all members of the population. Random selections can be made: Drawing slips of paper from a bag. Using a table of random numbers. Using a computer. Systematic random sampling Requires having a list of all members of the population. Steps: 1. Obtain the sampling interval dividing the number in the population by the number of individuals to be selected (figure: 12 / 4 = every 3rd individual). 2. The starting point is selected at random (figure: among individuals 1 to 3; No. 2). 3. Use the sampling interval to choose consecutively from the population. Stratified random sampling Population Strata Proportional Disproportional 1. Divide the population into subgroups (strata) according to some characteristics (sex, race). 2. Take a random sample from each strata, which can be: Proportional (strata distributed as in the populations), or Disproportional (overrepresenting some strata in the sample) Cluster random sampling The population is divided in natural groups (clusters) of individuals (states, cities, hospitals, blocks, etc.). Steps: 1. Obtain the list of clusters. 2. Select some clusters at random. Convenience / nonprobability sampling Subjects are chosen because they meet the selection criteria and are easily accessible to the investigator. The most common form of nonprobability sample. Some variations: 1. Consecutive sample: recruits all participants who meet the selection criteria as they become available. 2. Volunteer / self-selection. Surveys that track behaviors that can lead to poor health in students grades 9 to 12. Administered every other year. Some of the health-related behaviors and experiences monitored are: Student demographics: sex, sexual identity, race and ethnicity, and grade. Youth health behaviors and conditions: sexual, injury and violence, bullying, diet and physical activity, obesity, and mental health, including suicide. Substance use behaviors: electronic vapor product and tobacco product use, alcohol use, and other drug use. Student experiences: parental monitoring, school connectedness, unstable housing, and exposure to community violence. YRBSS Sampling, Weighting, and Response Rates National Survey Target population: all public and private school students in grades 9–12 in the 50 states and the District of Columbia. Three-stage, cluster sample design to obtain a nationally representative sample of U.S. students in grades 9–12: 1. Primary sampling units (PSUs) consisting of large sized counties or groups of smaller, adjacent counties. 2. Schools (both public and private) are selected from PSUs with probability proportional to school enrollment size. 3. Classes (one or two) selected randomly in each chosen school and in each of grades 9–12. Average sample size of 14,517 and average school, student, and overall response rates of 78%, 86%, and 71%, respectively. Activity 1. Selection and sampling in an RCT In the report of an RCT, identifying: 1. The selection (inclusion, exclusion) criteria. 2. The sampling method. Participants Eligible patients were English speaking adults 18 years or older who were awaiting elective upper abdominal surgery that required general anaesthesia, a minimum overnight hospital stay, and a 5 cm or longer incision above, or extending above, the umbilicus, and who attended an outpatient preadmission assessment clinic. Participants were recruited at three tertiary public hospitals in Australia and New Zealand from June 2013 to August 2015. We excluded patients if they were current hospital inpatients, required organ transplants, required abdominal hernia repairs, were unable to ambulate for more than one minute, and were unable to participate in a single physiotherapy preoperative session within six weeks of surgery. Site investigators screened preadmission clinics daily and invited eligible patients to participate in the trial. Written informed consent was gained before randomisation. Results From June 2013 to August 2015, we assessed 504 patients listed for elective upper abdominal surgery for eligibility. Of these, 441 met the inclusion criteria and were randomly assigned to receive either an information booklet (n=219; control) or preoperative physiotherapy (n=222; intervention). Nine (2%) patients were withdrawn from the trial, leaving 432 (98%) included for primary analysis (fig 1). Fig 1. Flow of patients through trial. Inclusion criteria In this trial a) Demographic • Adults aged ≥ 18 y. characteristics • English speaking. • Within 6 w of elective major upper abdominal surg. b) Clinical characteristics • Minimum overnight hospital stay. • Incision ≥ 5 cm above / extending above umbilicus. • Attended outpatient preadmission assessment c) Geographical 3 tertiary public hospitals in Australia / New Zealand. characteristics d) Temporal June 2013 to August 2015. characteristics Exclusion criteria In this trial • • • Current hospital inpatients. Required organ transplant or abdominal hernia repair. Unable to ambulate > 1. f) High risk of • lost to followup Unable to participate in a single physiotherapy session within 6 w of surgery. g) Inability to • provide good • data Unable to understand English Cognitive impairment e) Control for confounders h) High risk of side effects NA The investigators used the inclusion and exclusion criteria to select the sample of patients for the study. Which of the following sampling methods was used in this trial? A. Simple random. B. Systematic random. C. Stratified random. D. Cluster random. E. Non-random (convenience). You have up to 12 minutes Inclusion criteria In this trial a) Demographic • Adults aged ≥ 18 y. characteristics • English speaking. • Within 6 w of elective major upper abdominal surg. b) Clinical characteristics • Minimum overnight hospital stay. • Incision ≥ 5 cm above / extending above umbilicus. • Attended outpatient preadmission assessment c) Geographical 3 tertiary public hospitals in Australia / New Zealand. characteristics d) Temporal June 2013 to August 2015. characteristics Exclusion criteria In this trial • • • Current hospital inpatients. Required organ transplant or abdominal hernia repair. Unable to ambulate > 1. f) High risk of • lost to followup Unable to participate in a single physiotherapy session within 6 w of surgery. g) Inability to • provide good • data Unable to understand English Cognitive impairment e) Control for confounders h) High risk of side effects NA The investigators used the inclusion and exclusion criteria to select the sample of patients for the study. Which of the following sampling methods was used in this trial? A. Simple random. B. Systematic random. C. Stratified random. D. Cluster random. E. Non-random (convenience). Patients aged ≥ 18 y within 6 w of elective major upper abdominal surgery Target population Eligible patients in three hospitals in Australia / New Zealand from June 2013 to August 2015 Accessible population Intended Sample Actual sample Fig 1. Flow of patients through trial Major problems with samples 1. Systematic error (bias): the sample does not represent the target population: Inadequate selection criteria. Low response rate. 2. Random error: the sample size does not provide good precision in the estimate obtained in the study: Insufficient number of participants. Random error is unavoidable, but can be reduced to adequate levels. Large samples do not solve issues with bias. Common objectives in health research Objective Test of Sampling? hypotheses? Most often 1. To describe (descriptive studies): No • The frequency / distribution of a probabilistic problem or finding 2. To compare (analytical studies): • • • • Causality: exposed vs. non exposed Interventions: treated vs. untreated Diagnosis: a test vs. a “gold standard” Prognosis: exposed vs. non exposed Yes (always) Most often convenience Take home messages Most health research is based on the study of samples. Advantage: efficiency: examining a subset of subjects reduces cost, time and effort. Disadvantage: error may be introduced if the sample: not represent the target population (findings may not generalize). Is not large enough (poor precision on estimates). Does The appropriate sample depends on the research question: Descriptive: Random sample is usually more appropriate. Analytical: Convenience sample is more often used. Take home messages Nonprobability (convenience) samples are used more often in clinical research because of the difficulties in obtaining true access to populations; patients are recruited as they become available, making true random selection impossible. Researchers must be aware of the limitations inherent to any sampling method and should try to incorporate elements of random sampling whenever possible. “Sampling, like life, is a compromise.” Measurement Juan Manuel Lozano, MD, MSc Division of Medical and Population Health Sciences Research Department of Medical Education Herbert Wertheim College of Medicine Florida International University Objectives Goal RU1.EB1.6 Identify the main conceptual elements of measurement: variables and the relationship with sources of error in health research Given a clinical or research scenario, graph or table, students should be able to: RU1.EB1.6.1 Describe the roles of descriptive, independent, dependent, and confounding variables in health research. RU1.EB1.6.2 Identify the type of variables in a given study. RU1.EB1.6.3 Correlate the four different measurement scales (NOIR: nominal, ordinal, interval, ratio) with health research variables. RU1.EB1.6.4 Determine the measurement scales used for the variables in a study after reading a methods section in published research. RU1.EB1.6.5 Define internal validity, external validity, and reliability as they relate to measurement of variables in research. Variable “Anything that is measured or manipulated in a study” (Norman GR. Statistics. BC Decker Inc., 2003) “Any attribute, phenomenon or event that can have different values. Any amount that varies” (Last JM. A Dictionary of Epidemiology. Oxford University Press, 2001) “A concept, or factor, that can have more than one value” (Portney LG. Foundations of Clinical Research. Prentice-Hall, Inc., 2000) How can we classify research variables? By the role that they play in the research question By the measurement scale Analytical research = assessing associations Association: the quantity of a variable varies with the quantity of one or more other variables. Positive or Direct Negative or Inverse Role of variables in analytical research Independent Dependent Confounding “The CRASH trial (corticosteroid randomisation after significant head injury) is a large, international, randomised placebo-controlled trial of the effect of early administration of 48 h infusion of methylprednisolone on risk of death and disability after head injury.” Independent variable Also called: Explanatory Exposure Experimental Manipulated Predictor Causal “The CRASH trial (corticosteroid randomisation after significant head injury) is a large, international, randomised placebo-controlled trial of the effect of early administration of 48 h infusion of methylprednisolone on risk of death and disability after head injury.” Dependent variable Also called: Outcome Endpoint Response Explained “The CRASH trial (corticosteroid randomisation after significant head injury) is a large, international, randomised placebo-controlled trial of the effect of early administration of 48 h infusion of methylprednisolone on risk of death and disability after head injury.” Confounding variable Also called: Confounder Extraneous Intervening Controlled Role of variables in analytical research Independent Dependent Confounding “The CRASH trial (corticosteroid randomisation after significant head injury) is a large, international, randomised placebo-controlled trial of the effect of early administration of 48 h infusion of methylprednisolone on risk of death and disability after head injury.” Activity 2. Variables in an RCT In the report of an RCT, identifying the following variables: 1. Independent or exposure. 2. Main dependent or main outcome(s). 3. Some confounders. OBJECTIVE To assess the efficacy of a single preoperative physiotherapy session to reduce postoperative pulmonary complications (PPCs) after upper abdominal surgery. INTERVENTIONS Preoperatively, participants received an information booklet (control) or an additional 30-minute physiotherapy education and breathing exercise training session (intervention). Education focused on PPCs and their prevention through early ambulation and self-directed breathing exercises to be initiated immediately on regaining consciousness after surgery Postoperatively, all participants received standardised early ambulation, and no additional respiratory physiotherapy was provided. MAIN OUTCOME MEASURES The primary outcome was a PPC within 14 postoperative hospital days assessed daily using the Melbourne group score. Secondary outcomes were hospital acquired pneumonia, length of hospital stay, utilisation of intensive care unit services, and hospital costs. Patient reported health related quality of life, physical function, and post-discharge complications were measured at six weeks, and all cause mortality was measured to 12 months. Role of variables in the trial Independent Dependent Preoperative management Booklet + Education Session (E) vs Booklet only (C) Having a PPCs within 14 days Yes or No Confounders Age Gender BMI ASA physical health status Comorbidities Smoking Type of surgery Etc…. Up to 6 minutes (≈ 2 min / question) Role of variables in the trial Independent Dependent Preoperative management Booklet + Education Session (E) vs Booklet only (C) Having a PPCs within 14 days Yes or No Confounders Age Gender BMI ASA physical health status Comorbidities Smoking Type of surgery Etc…. How can we classify research variables? By the role that they play in the research question By the measurement scale One mnemonic N O I R Nominal Ordinal Interval Ratio Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • Temperature (oC, oF) • Time • Age • Weight • Blood pressure Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • Temperature (oC, oF) • Time • Age • Weight • Blood pressure Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • Temperature (oC, oF) • Time • Age • Weight • Blood pressure Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • Temperature (oC, oF) • Time • Age • Weight • Blood pressure Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • Temperature (oC, oF) • Time • Age • Weight • Blood pressure Scale Qualitative (categorical) Quantitative Sub scale Nominal: values fit into categories with no hierarchy Ordinal: values fit into categories with implicit hierarchy Discrete: measure in integers, limited number Interval: Zero is arbitrary (i.e., it is not “0”), can have fractions Ratio: Zero is not arbitrary (it is “0”), can have fractions Examples • Sex • Blood type • Type of cancer • Cancer staging • Apgar or Glasgow Coma scores • • • • Number of pregnancies Number of treatments Temperature (oC, oF) Time • Age • Weight • Blood pressure And why is this important? Because it allows: 1. To decide how to collect the data 2. To decide how to analyze the data Birth weight in 100 neonates admitted to NICU in five hospitals Case Hospital Gender Birth weight (g) LBW (<2500 g) 1 A Fem 2800 No 2 B Mal 3200 No 3 C Mal 2300 Yes 4 D Fem 2950 No 5 E Fem 1800 Yes 6 E Mal 2700 No 7 D Mal 1500 Yes 100 B Fem 3800 No Statistical tests (just a few) Measurement scale Statistical measures or tests Descriptive Comparative Categorical (nominal, ordinal) Proportions, percentages Continuous (interval, ratio) t-test, analysis of variance Mean / standard deviation, median / range, (ANOVA), linear regression mode Chi square, Fisher, MannWhitney U, MantelHaenszel, survival analysis, RR, OR, etc. Activity 3. Variables in an RCT In the report of an RCT, identifying the measurement scale (nominal, ordinal, interval, ratio) for variables: Table 1 | Baseline demographic and clinical characteristics of the study population. Values are numbers (percentages) unless stated otherwise Characteristics Preoperative physiotherapy (n=218) Information booklet (n=214) Median (IQR) age (years) 63.4 (51.5-71.9) 67.5 (56.3-75.3) Mean (SD) body mass index 28.5 (5.9) (6.2) Body mass index >35 25 (12) 30 (14) ASA physical health status: 1-2 150 (69) (58) 3-4 67 (31) 90 (42) Recent chest infection 12 (6) 5 (2) Smoking status: Never smoked 76 (35) 71 (33) Former smoker 93 (43) 86 (40) Current smoker 49 (21) 57 (27) Mean (SD) average pack year 18.1 (23.7) 20.6 (24.7) Comorbidities: Respiratory disease 42 (19) 55 (26) Diabetes mellitus 33 (15) 41 (19) Cancer 148 (68) 148 (69) Cardiac disease 26 (12) 34 (16) Surgical category and procedure: Colorectal 108 (50) 101 (47) Hepatobiliary / upper GI 49 (22) 59 (28) Renal / urology / other 61 (28) 54 (24) Scale Sub scale Qualitative Nominal: values fit into categories (categorical) with no natural order Examples • BMI > 35 (Y, N) • Recent chest infection (Y, N) • Comorbidities (respiratory, DM, cancer, heart) • Surgical category & procedure (colorectal, hepatobiliary, renal) Ordinal: values fit into categories with • ASA physical health status (1-2, 3-4) natural order • Smoking status (never, former, current) Quantitative Interval: zero is arbitrary (it is not “0”), can have decimals and negative values Ratio: zero is not arbitrary (it is “0”), can have decimals but not negative values • None that we can identify in Table 1 • Age • BMI • (Tobacco) Pack years Scale Sub scale Qualitative Nominal: values fit into categories (categorical) with no natural order Examples • BMI > 35 (Y, N) • Recent chest infection (Y, N) • Comorbidities (respiratory, DM, cancer, heart) • Surgical category & procedure (colorectal, hepatobiliary, renal) Ordinal: values fit into categories with • ASA physical health status (1-2, 3-4) natural order • Smoking status (never, former, current) Quantitative Interval: zero is arbitrary (it is not “0”), can have decimals and negative values Ratio: zero is not arbitrary (it is “0”), can have decimals but not negative values • None that we can identify in Table 1 • Age • BMI • (Tobacco) Pack years Take home messages Variable: anything that is measured or controlled for in clinical measurements or in health research. Role of variables in comparative research: Independent (exposure or intervention) Dependent (outcome, endpoint) Confounders Measurement scales - NOIR: Determine how to collect and analyze data Validity “How well the measurement represents the phenomenon of interest” (Hulley SB. Designing Clinical Research. Lippincott Williams & Williams, 2001) “The results of a measurement correspond to the true state of the phenomenon being measured” (Fletcher RH. Clinical Epidemiology. Lippincott Williams & Williams, 2005) “The value of the parameter that is the object of measurement is estimated with little error” (Rothman KJ. Modern Epidemiology. Wolters Kluwer, 2008) What is validity? Validity: A reflection of the truth When the measurement tool or the research report (or study) reflects the truth Reliability (a related but different concept): Consistency in reporting in repeated measurements (several observations, different observers) Reproducibility, although not necessarily the truth Examples of health measurements Clinical: Body weight, measured with a scale Severity of head trauma, measured with the Glasgow Coma Score Health research: Proportion of FIU community members that endorse the ban for tobacco in the university (measured in a survey) Risk of death after head injury when steroids are used (measured in a randomized controlled trial) Types of validity in studies Internal: the study measured correctly what it was supposed to measure in the study sample (the study subjects) External: the findings of the study can be generalized to subjects who did not participate in the study Consequence: internal validity is required before considering external validity Internal validity “Degree to which the results of the study are correct for the sample of participants being studied”. Fletcher et al, Clinical Epidemiology Depends largely on the procedures of the study and how rigorously it is performed. It is not a "yes or no" concept. Instead, we consider how confident we can be with the findings of a study, based on whether it avoids errors that may make the findings questionable. External validity “Degree to which the results of the study hold true in other settings. Another term is generalizability”. Fletcher et al, Clinical Epidemiology Depends largely on the how similar individuals in other settings are as compared to those included in the study. Again, it is not a "yes or no" concept. Instead, we consider how confident we can be that the findings of a study apply to others. All target participants of interest Activity 4. Describing a health situation Goal: to measure the frequency (%) of Covid-19 vaccination at FIU. Target population: FIU community of ≈ 55,000 people comprising students, employees and faculty members. Study: observational - descriptive (survey). Activity 4. Describing a health situation Goal: to measure the frequency (%) of Covid-19 vaccination at FIU. Participants: stratified random sample of 100 HWCOM members (students, employees, faculty). Methods: Observational descriptive (survey). Self-administered questionnaire completed anonymously online. The questionnaire has been validated and used in many similar studies. 100% response rate. Main finding: vaccination frequency 85% (95% precision: 77% to 91%). Conclusion: 85% of FIU community members are vaccinated. 4A. How do you feel about the internal validity of the study? 1. 2. 3. 4. 5. I have very serious concerns about it. I have some concerns about it. I don’t know how we feel about it. I feel somewhat confident about it. I am very confident about it. 4B. How do you team feel about the external validity of the study (i.e., do the findings apply to FIU overall)? 1. 2. 3. 4. 5. I have very serious concerns about it. I have some concerns about it. I don’t know how we feel about it. I feel somewhat confident about it. I am very confident about it. 4C. Studies that have serious methodological issues and therefore low internal validity can, however, have good external validity. 1. True. 2. False. 3. I don’t know. Up to 9 minutes (≈ 3 min / question) 4A. How do you feel about the internal validity of the study? 1. 2. 3. 4. 5. I have very serious concerns about it. I have some concerns about it. I don’t know how we feel about it. I feel somewhat confident about it. I am very confident about it. All target participants of interest 4B. How do you team feel about the external validity of the study (i.e., do the findings apply to FIU overall)? 1. 2. 3. 4. 5. I have very serious concerns about it. I have some concerns about it. I don’t know how we feel about it. I feel somewhat confident about it. I am very confident about it. All target participants of interest 4C. Studies that have serious methodological issues and therefore low internal validity can, however, have good external validity. 1. True. 2. False. 3. I don’t know. Describing a situation Goal: to measure the frequency of opinions (favorable or oppositional) towards the FIU “Free Tobacco Smoke” policy Population: FIU community (≈45,000 people) Study: observational descriptive Take home messages Validity in research: Internal: are the findings correct for the sample of participants studied? External: do the results of the study hold true in other settings? Sources of error: Bias: findings deviate systematically from the truth. Random: findings are distributed above and below the truth. Not mutually exclusive; rather, their effects are cumulative. More about both in future sessions. Random error (chance) Health research is almost always conducted studying samples Even appropriate sampling techniques entail the chance of random error Describing a situation Goal: to measure the frequency of opinions (favorable or oppositional) towards the FIU “Free Tobacco Smoke” policy Population: FIU community (≈55,000 people) Study: observational descriptive Describing a situation Survey in a random sample (n = 500) from the whole FIU community Study sample FIU community 0.65 (≈65%) endorsement Population and multiple samples Population % = ? Sample 1 = 65% Sample 2 = 60% Sample 3 = 70% Sample 4 = 72% Sample 5 = 61% Sample n = n% Why???? Random (albeit representative) samples of equal size produce different estimates of the population parameter What is the cause of this variation? Each sample is different (i.e., composed by different subjects) = each gives different results Chance determines the composition of each sample Therefore, chance is the cause of the variability in the estimates from different samples There is (at least in theory) one way to eliminate random error; what is it? Population % = ? Sample 1 = 65% Sample 2 = 60% Sample 3 = 70% Sample 4 = 72% Sample 5 = 61% Sample n = n% Is it possible to eliminate random error? Very rarely: including all subjects from the population in the sample Thus, random error is almost always present in clinical and health research If so, what can be done? Can be minimized by design (sample size calculation) Can be measured by statistical techniques (by calculating p values and confidence intervals) Take home message: potential explanations for research findings 1. The study findings do not represent the truth: Bias: systematic errors lead to study findings that do not represent the truth Control measures: good design and conduct Chance: random error leads to study findings that do not represent the truth Control measures: random error cannot be eliminated; it can be minimized and quantified 2. The study findings represent the truth