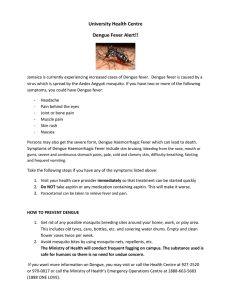
DENGUE HEMORRHAGIC FEVER Dengue Fever Classic dengue fever, or “break bone fever,” is characterized by acute onset of high fever 3–14 days after the bite of an infected mosquito. A dengue epidemic requires the presence of o The vector mosquito (usually Aedes aegypti). o The dengue virus. o A large number of susceptible human hosts. The main medical complications of classic dengue fever are febrile seizures and dehydration. Some patients with dengue fever go on to develop dengue hemorrhagic fever (DHF), a severe and sometimes fatal form of the disease. Dengue Hemorrhagic Fever Overview DHF is primarily a disease of children under the age of 15 years, although it may also occur in adults. It is characterized by sudden onset of fever, which usually lasts for 2 to 7 days, and a variety of nonspecific signs and symptoms. Just so You Know: The first known epidemic of DHF occurred in Manila, Philippines, in 1953 to 1954, but within 20 years the disease in epidemic form had spread throughout Southeast Asia; by the mid-1970s, DHF had become a leading cause of hospitalization and death among children in the region. DHF is currently defined by the following four World Health Organization (WHO) criteria: o Fever or recent history of fever lasting 2–7 days. o Any hemorrhagic manifestation. o Thrombocytopenia (platelet count of <100,000/mm3) o Evidence of increased vascular permeability Manifestations Warning signs of DHF include severe abdominal pain, persistent vomiting, marked change in temperature (from fever to hypothermia), hemorrhagic manifestations, or change in mental status (irritability, confusion, or obtundation). The most common hemorrhagic manifestations are mild and include a positive tourniquet test, skin hemorrhages (petechiae, hematomas), epistaxis (nose bleed), gingival bleeding (gum bleed), and microscopic hematuria. More serious types of hemorrhage include vaginal bleeding, hematemesis, melena, and intracranial bleeding. Despite the name, the critical feature that distinguishes DHF from dengue fever is not hemorrhaging, but rather plasma leakage resulting from increased vascular permeability. Evidence of plasma leakage due to increased vascular permeability consists of at least one of the following: o o o o An elevated hematocrit ≥20% above the population mean hematocrit for age and sex. A decline in hematocrit after volume-replacement treatment of ≥20% of the baseline hematocrit. Presence of pleural effusion or ascites detected by radiography or other imaging method. Hypoproteinemia or hypoalbuminemia as determined by laboratory test. What to Look for When You Evaluate Patients for DHF EVALUATE the patient’s heart rate, capillary refill, skin color and temperature, peripheral pulse volume, pulse pressure, and blood pressure. A drop in systolic blood pressure is usually the last sign and appears only when the patient is in shock. LOOK FOR evidence of bleeding on the skin and at other sites. LOOK FOR evidence of increased capillary permeability (e.g., pleural effusions, ascites, hemoconcentration). MEASURE and ask about urine output. Clinical Management Stress the need to maintain adequate hydration. Monitor your patients’ hydration status during the febrile phase of illness. Educate patients and parents about the signs of dehydration and have them monitor their urine output. Teach about assessment of possible bleeding (such as Melena). Warn patients to avoid aspirin and other nonsteroidal, anti-inflammatory medications because they increase the risk of hemorrhage. Successful management of DHF and DSS includes judicious and timely IV fluid replacement therapy with isotonic solutions Assess hemodynamic status frequently by checking the patient’s heart rate, capillary refill, pulse pressure, blood pressure, and urine output Monitoring for warning signs of severe dengue and initiating early appropriate treatment are key to preventing complications such as prolonged shock and metabolic acidosis. References: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC88892/#B1, Dengue hemorrhagic fever, diagnosis, treatment and control. Geneva, Switzerland: World Health Organization; 1986 Dietz V, Gubler D J, Ortiz S, Kuno G, Casta-Velez A, Sather G E, Gomez I, Vergne E. The 1986 dengue and dengue hemorrhagic fever epidemic in Puerto Rico: epidemiologic and clinical observations. P R Health Sci J. 1996;15:201– 210. [PubMed] [Google Scholar] CHIKUNGUNYA Overview Chikungunya is a viral disease transmitted to humans through the bites of mosquitoes infected with the chikungunya virus. It was first described during an outbreak in southern Tanzania in 1952 and has now been identified in nearly 40 countries in Asia, Africa, Europe and, most recently, the Americas The word comes from the African Makonde language and means "bent over in pain." Chikungunya virus is an alphavirus that belongs to the Togaviridae family usually transmitted by the bite of the Aedes aegypti mosquito and Aedes albopictus mosquito. A person can only have chikungunya once, then develop antibodies that will protect people. According to the evidence available so far, there would be immunity for life. Cases of death from chikungunya are very rare and are almost always related to other existing health problems. Mothers who have chikungunya during pregnancy do not transmit the virus to their babies. However, there are documented cases of mother-to-child transmission when the mother has fever in the days immediately prior to delivery or during delivery. Manifestations Symptoms usually begin 4 to 8 days after a mosquito bite but can appear anywhere from 2 to 12 days. The most common symptom is an abrupt onset of fever, often accompanied by joint pain. Other symptoms include muscle pain, headache, nausea, fatigue, and rash. Severe joint pain usually lasts a few days but can persist for months or even years. Serious complications are uncommon, but atypical severe cases can cause long-term symptoms and even death, especially in older people. Clinical Management There is no vaccine or antiviral drug treatment for chikungunya. Treatment is focused on relieving the symptoms. Improve the body temperature. Eliminate excess clothing and covers; give antipyretic medications as prescribed; perform tepid sponge bath, and modify cooling measures based on the patient’s physical response. Restore adequate amount of fluid volume. Assess skin turgor and oral mucous membranes for signs of dehydration; assess color and amount of urine and report urine output less than 30 ml/hr for 2 consecutive hours; urge the patient to drink the prescribed amount of fluid, and administer parenteral fluids as prescribed. Relief from pain. Acknowledge reports of pain immediately; provide rest periods to promote relief, sleep, and relaxation; and provide analgesics as ordered, evaluating the effectiveness and inspecting for any signs and symptoms of adverse effects. For prevention, use insect repellent; wear long-sleeved shirts and pants; and stay in places with air conditioning or that use window and door screens when visiting a place with known cases of the disease. Summary Chikungunya fever is a self-remitting febrile viral illness that has been associated with frequent outbreaks in tropical countries of Africa and Southeast Asia. Chikungunya virus is transmitted to humans through day-biting mosquitoes that belong to the Aedes genus. Numerous Chikungunya epidemics have been reported in several countries in Southern and Southeast Asia. Chikungunya virus is an alphavirus that belongs to the Togaviridae family. Symptoms usually begin 3–7 days after being bitten by an infected mosquito, and these include fever, arthralgia, cutaneous manifestations, and neurological manifestation There is no specific antiviral therapy for chikungunya virus infection. References: Centers for Disease Control and Prevention. https://www.cdc.gov/chikungunya/index.html (2019, Sept 19). Chikungunya. Retrieved from Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Vector-Borne Diseases (DVBD) Natesan, S.K. (2019, Aug 1). Chikungunya virus. Retrieved from https://emedicine.medscape.com/article/2225687overview