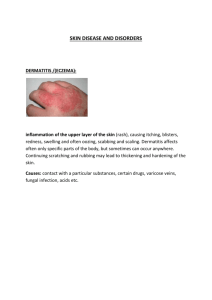
Skin Infections: Furuncles, Carbuncles, Folliculitis, Impetigo
advertisement

Furunclosis/Boils/ A furuncle (i.e, boil) is an acute inflammation arising deep in one or more hair follicles and spreading into the surrounding dermis. It is a deeper form of folliculitis. Furunculosis refers to multiple or recurrent lesions. Is a localized, painful, deep seated, red, hot, very tender, inflammatory peri follicular abscess. Common microorganism: staphylococcus aureus It occurs at all age Furunclosis/Boils/…cont. Most common on persons who are carriers of staphylococcus, contact with oils or grease, diabetes, poor habits of personal hygiene, immunosuppression, alcoholism, obese, malnutrition, etc The lesion begins in the opening of hair follicle or sebaceous gland prevalent in areas subjected to irritation, pressure, friction, and excessive perspiration: back of the neck, face, buttocks, thighs, perineum, breasts, axilla, nose, genitallia, etc Furunclosis cont’d Sign and symptom Hard nodule initially then fluctuant abscess with centrally yellow pustule, then ruptures in to an ulcer It can be isolated single lesion or few multiple lesion Hotness and pain at the site May start as a small, red, raised, painful pimple. Frequently, the infection progresses and involves the skin and subcutaneous fatty tissue, causing tenderness, pain, and surrounding cellulitis. N.B. The area of redness and induration represents an effort of the body to keep the infection localized. Furunclosis (Boils) Furunclosis cont’d Diagnosis Gram stain of the pus Culture and sensitivity test of blood/pus Furunclosis cont’d Treatment Warm compresses to sooth and hasten maturation and drainage of the lesion Warn patient not to squeeze or incise the lesion Incision and drainage when it is fluctuant Systemic antibiotics (cloxacillin, erythromycin, etc) Rest especially for genital areas. For the sever pain codien, morphine Carbuncles (multiple furuncles) A carbuncle is an abscess of the skin and subcutaneous tissue that represents an extension of a furuncle that has invaded several follicles and is large and deep seated. Is an aggregation of interconnected furuncles that drain through multiple openings in the skin. Carbuncles appear most commonly in areas where the skin is thick and inelastic. Exposure to grease and oil increase the risk. Microorganism mostly involved is staphylococcus aureus Carbuncles cont’d more likely to occur in patients with underlying systemic diseases, such as diabetes or hematologic malignancies, and in those receiving immunosuppressive therapy for other diseases. more prevalent in hot climates, especially on skin beneath occlusive clothing. the extensive inflammation frequently prevents a complete walling off of the infection; absorption may occur, resulting in high fever, pain, leukocytosis, and even extension of the infection to the bloodstream. Carbuncles cont’d Sign and symptom Sites are back of the neck, shoulder, buttock, outer aspect of the thigh and over the hip joints. Develop slowly than furuncle They can reach the size of an egg/small orange. Fever, chills, extreme pain, malaise. Because of the large size of the lesion and its delayed drainage the patient is much sicker. Carbuncles (multiple furuncles) Carbuncles cont’d Diagnosis Gram stain, and culture of the pus/blood Leucocytosis (12,000-20,000 mm3) normal 4,00010,000mm3 Treatment The same as furunclosis, plus Avoid friction and irritation from tight clothing. In treating staphylococcal infections, it is important not to rupture or destroy the protective wall of induration that localizes the infection. The boil or pimple should never be squeezed. Oral cloxacillin, dicloxacillin, and flucloxacillin are firstline medications. Cephalosporins and erythromycin are also effective. Nursing Management Intravenous fluids, and fever reduction are indicated for patients who are very ill or suffering with toxicity. Bed rest is advised for patients who have boils on the perineum or in the anal region, When the pus has localized and is fluctuant, a small incision with a scalpel can speed resolution by relieving the tension and ensuring direct evacuation of the pus and slough. The patient is instructed to keep the draining lesion covered with a dressing. Management cont’d Warm, moist compresses increase vascularization and hasten resolution of the furuncle or carbuncle. The surrounding skin may be cleaned gently with antibacterial soap, and an anti- bacterial ointment may be applied. Nursing personnel should carefully follow isolation precautions to avoid becoming carriers of staphylococci. Disposable gloves are worn when caring for these patients. Folliculitis Folliculitis: is an inflammation of the hair follicle caused by bacterial or fungal origin that arises within the hair follicles. Folliculitis commonly affects the beard area of men who shave and women’s legs. Other areas include the axillae, trunk, and buttocks. Sign and symptom Lesions may be superficial or deep; single or multiple papules or pustules appear close to the hair follicles. Folliculitis Management Warm compress to relieve pain Clean with antibacterial soap Topical antibiotic ointment Systemic antibiotics for recurrent cases The only entirely effective treatment is to avoid shaving. Other treatments include using special lotions or antibiotics or using a hand brush to dislodge the hairs mechanically. Management cont’d If the patient must remove facial hair, a depilatory cream or electric razor may be more appropriate than a straight razor. Impetigo Impetigo is a common superficial skin bacterial infection. Is an acute, contagious, rapidly spreading cutaneous infection Causative agents are staphylococcus aureus or a Bhemolytic streptococcus or both Bullous impetigo, a more deep-seated infection of the skin caused by S. aureus Impetigo cont’d Is characterized by the formation of bullae (i.e, large, fluid-filled blisters) from original vesicles. The bullae rupture, leaving raw, red areas. The exposed areas of the body, face, hands, neck, and extremities are most frequently involved. It is particularly common among children living in poor hygienic conditions. Impetigo cont’d It often follows pediculosis capitis (head lice), scabies (itch mites), herpes simplex, insect bites, poison ivy, or eczema. Chronic health problems, poor hygiene, and malnutrition may predispose an adult to impetigo. Some people have been identified as asymptomatic carriers of S. aureus, usually in the nasal passages. Sign and Symptom Superficial pustules or blisters which becomes oozing with yellow crusts Blisters break easily and form golden crusts If the scalp is involved, the hair is matted, which distinguishes the condition from ringworm. Diagnosis Clinical Culture and sensitivity Impetigo Medical Management Reduces contagious spread, treats deep infection, and prevents acute glomerulonephritis (i.e, kidney infection), In nonbullous impetigo, benzathine penicillin or oral penicillin may be prescribed. Bullous impetigo is treated with a penicillinase-resistant penicillin (eg, cloxacillin, dicloxacillin). In penicillin-allergic patients, erythromycin is an effective alternative. Topical antibacterial therapy (eg, mupirocin) may be pre scribed when the disease is limited to a small area. Management KMNO4 bath or wet dressing-in mild forms GV paint-in mild forms Prevent spreading by not sharing towels and ointment Change clothes, towels and sheets frequently Cut finger nails short to minimize damage to lesion and to prevent autoinoculation from scratching Don’t use Vaseline (use aqueous creams instead) Nursing Management The nurse instructs the patient and family members to bathe at least once daily with bactericidal soap. Cleanliness and good hygiene practices help prevent the spread of the lesions from one skin area to another and from one person to another. Each person should have a separate towel and wash cloth, because impetigo is a contagious disorder. KMNO4 bath or wet dressing-in mild forms GV paint-in mild forms Prevent spreading by not sharing towels and ointment Change clothes, towels and sheets frequently Cut finger nails short to minimize damage to lesion and to prevent autoinoculation from scratching Don’t use Vaseline (use aqueous creams instead) Fungal skin disorder Dermatophytosis (Mycosis) Is a fungal infection of the skin, hair and nails Types a. Tinea pedis (Athlete’s foot) Is itchy, whitish scaling lesions and inflammation of the superficial skin of the feet and inter-digital spaces of the toes It is especially prevalent in those who use communal showers or swimming pools Often seen in people wearing rubber boots/shoes Tinea pedis (Athlete’s foot) Clinical Manifestations Tinea pedis may appear as an acute or chronic infection on the soles of the feet or between the toes. The toenail may also be involved. Lymphangitis and cellulitis occur occasionally when bacterial superinfection occurs. Sometimes, a mixed infection involving fungi, bacteria, and yeast occurs. Management Keep the space in between the toes dry : after washing, expose to air, Gv paint, wear cotton socks, don’t wear shoe that are too tight/hot, changing socks daily prevents reinfection. Imidazole cream/ whitfield’s ointment twice daily until symptoms disappear for a total of 4 weeks Treat secondary bacterial infection if present Expose to the air Avoid wearing too hot shoe Tinea corporis (Tinea circinata) A fungal infection that affects the trunk, legs, arms/neck, excluding the beard area, feet, hands and groin Is fungal infection of the skin most common on the exposed surfaces of the body. Sites are face, arms and shoulders. Lesions are round and scaling at the periphery with a tendency to central healing Intensive itching is there Frequent causes of tinea corporis is the presence of an infected pet in the home. Tinea corporis (Tinea circinata) Management Imidazole cream/whitfield’s ointment twice daily for a minimum of 4 weeks Continue treatment until one week, after symptoms have cleared Multiple, widespread lesions may be treated systematically Griseofulvin 500mg once daily for 2-6 wks (1015mg/kg) Ketoconazole 200mg once/twice daily x 2-4wks When there is sever itching antihistamines /mild steroids can be added