Motion Rest cfions
Linda C. Monroe,MPT, OCS
SUMl\IARY
OF INFORMATION
lntroduction
Typesof Motion
Patternsof Motion Restriction
TissuesThat Can RestrictMotiorr
PathologiesThat Can CauseMotion Restrictions
Assessmentof Motion Restrictions
COVERED
Treatment Approachesfor Motion
Restrictions
The Role ofPhysical Agents in the Treatment of
Motion Restrictions
Clinical CaseStudies
Chapter Review
OBJECTIVES
Uyon comyletionof this cha2zter,
the readerwill beable to:
1 . Define different b?es of motion.
6. Selectand apply appropriatemethods to
2 . Describedifferent patternsof motion
determinethe structuresand
restrictions.
pathologiescontributing to motion
3 . Identify tissuestl.ratcan restrict motion.
restrictions.
Discusspathologiesthat can contribute to
7. When presentedwith a clinical caseinvolving a
motion restrictions.
motion restriction, evaluatethe clinical findings,
5 . Selectand apply appropriatetools and methods
proposetreatment goals,and identi$zpossible
to quantify and qualify motion restrictions.
interventions.
ltl
lt2
5 . .Ilotiot
Re strittions
INTRODUCTION
This chapter discussesmotion between body segments and the factorsthat can restrict such motion.
The amountof motionthat occurswhen onesegment
oI the body moves in relationto an adjacentsegment is known as rangeof motiox(ROM).1When a
segment of the body moves through its. available
ROM, all tissuesin that region, including the bones,
strucligaments,tendons.intraarticular
ioint capsule,
tur"r. mrr.les, nerves,fascia,and skin may be
affected.When all of thesetissuesfunction normally,
ful1, normal ROM can be achieved;however, dysfunction of any of these tissuesmay contribute to a
restriction of the avai.lableROM. Many patients in
rehabilitationseekmedicaltreatmentwith an impairment of restricted ROM. To restore motion most
effectively,the therapist must understandboth the
factorsthat influencenormal motion and the factors
thatmay contrjbuteto motionrestrictions.'
fhe impairment of restricted motioh may contribute directly or indirecdy to patient functional
limitation and disability.3-6lor example, restricted
shoulderROM may stop an individual from raising
the arm aboveshoulderheightandmay preventhim
or her from performing a job that involvesoverhead
lifting, This impairment may also contribute indirecdy b further pathology by causingimpingement
of the rotatorcuff tendons,resultingin pain.weakoflifting capaciry.
ness,andadditionalLimitation
ROM is generaliyiimpathology,
absence
of
In the
of anatomior
approximation
ited by the lengthening
of the sott
flexibility
and
The
integrity
cal structures.T
joint,
and
relationshape
and
the
a
tissuessurrounding
o[
amount
the
affect
structures.
ship of the articular
it
joint
midrange,
is
at
a
When
motion that can occur.
a
small
o[
application
with
the
cangenerallybe moved
force.This is becausethe collagenfibersin the connective tissuesurounding the joint are in a relaxedstate,
loosely oriented in vadous directions, and only
sparselvcross-linkedwith other fibers,allowingthem
t; dist;nd readily.As *re joint approachesterminal
motion, the collagenfibersbegin to align in the direction of the stressandstartto straightenMotion ceases
at the normal terminal range when the fibers have
achievedtheir maximum alignmentor when soft or
bony tissuesapproximate.Ior example,ankle dorsiflexion normally ceaseswhen *re fibers of the calf
muscles have achieved maximum alignment and
the musclesarefully extended,whereaselbow flexion
normally ceaseswhen the soft tissuesof the anterior
arm aonroximate with the soft tissuesof the antedor
foreanl, and elbow extensionceaseswhen the olecranon processof the ulna approximateswith the
olecranonfossaofthe humerus(Fig.5-1)
The normal ROM for all human joints has been
measuredand documented;howeveqthesemeasures
vary wirh the individual'sage,sex,and health stawith age
Rang"of -otion generallydecreases
tur.B-10
and is qreaterin women than in men, althoughthese
differeicesvary with differentmotions andjoints and
are not consistentfor all individuals.ll-l9Becauseof
this variabiliry normal ROM is generallydetermined
bv comparisonwith the motion of the contralateral
limb, if'available, rather than by comparisonwith
notmative data. A motion is considered to be
restrictedwhen it is less than that availablefor the
samesegmenton the contralateralside of the same
individual. When a normal contralateralside is not
available-as occurs,for example,with the spinemotion is consideredto be restrictedwhen it is less
than normal for the individual'sageand sex.
OFMOTION
TYPES
Motion
ActiveandPassive
The motion of body segmentscan be classifiedas
ei,theractiveor yassiveActive motion is the movement producedby contractionof the musclescrossing
a joini. Assessmentof activeROM can provide information about an individual's functional abilities'
Active motionmay be restrictedby muscleweakness,
abnormal muscle tone, Pain originating trom the
musculotendinousunit or other local structures,an
inability or unwillingness of the subject to follow
directions,or as the result of restrictionsin passive
ROM.20
Passivemotion is movementproducedentirely by
an externalforce without voluntary muscle contraction by *re subiect.The externalforce may be produced by gravity, a machine,another individual, or
another'pirt of the subiect'sown bodyl Passive
motion may be restdctedby shorteningof the soft tissues,edema,adhesion,mechanicalblock, spinal disc
neuraltension.
or adverse
herniarion,
ROM is greaterthannormalactive
Normalpassive
ROM when motion is limited by *re distention or
aooroximation of soft tissue, but both types of
-otio.r ut" equalwhen motion is limited by approxiof passive
a fewdegrees
mationofbone.Forexample,
One c PATHOLOGY AND PATIENTPROBLEMS
113
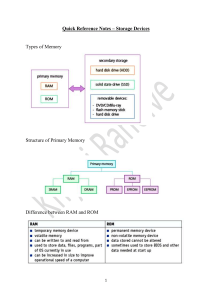
' gure5-1. A, Ankle dorsiflexion limited by solt tissuedistension.B, Elbow flexion limited by soft tissueapproxima'-:n. C, Elbow extensionlimited by bone approximation.
,::kle dorsiflexion motion are available beyond the
.::rit of active motion because the limiting tissues are
- astic and may be extended by an external force that
i greater than that of the active muscles when at ter:::inal active ROM. A few degrees of additional pas,. .'e elbow flexion are availabie beyond the limit of
.:,ive range because the limiting ris'ues are com::essible by an external force greater than that of the
::iive muscles in that position and because the
::proximating muscles may be less bulky when
,"laxed. This additional passive ROM may protect
,iint structures by absorbing external forces during
::rivities, particularly those performed at or close to
-- .-A ^t ,.ri,'" ."^."
Physiological
andAccessory
Molion
:rysiological motion is the motion of one segment of
::re body relative to another segment. For example,
:nysiological knee extension is the straightening of
-:reknee *rat occurs when the leg moves away from
re thigh. Accessory motion is the motion that occurs
: . ' w e e n t h e ' o i n r , u r f a c e sd u r i n g n o r m a lp h y s o l o g i r l m o t i o n . T14 24 3F o re x a m p J ea. n c e r i ogr l i oi n g o f t } e
tibia on the femur is the accessorymotron that occurs
d u r i n g p h y s i o l o g i c akl n e e e x r e n s i o nr l i g . 5 - 2 ) .
Accessorymotions may be intraarticular,as in the
prior example of anterior tibial gliding during knee
extension,or extraarticular,aswith the upward rotation of lhe scapula during physiological shoulder
flexion (Iig. 5-3). Accessorymotions cannot be performed actively in isolation from their associated
physiologicalmovement;howeveSthey may be performed passivelyin isolation from their associated
physiologicaimovement.
Normal accessorymotion is required Ior normal
active and passivejoint motion to occur.The direction of normal accessorymotion depends on the
shape of the articular surfacesand the direction of
physiologicalmotion. Concavejoint surfacesrequire
accessoryglidingto be availablein the directionof the
associatedphysiological motion of the segment,
whereasconvexjoint surfacesrequireaccessorygiiding to be availablein the opposite direction of the
associatedphysiologicalmotion of the segment.2llor
example, the tibial plateau, which has a concave
surface at the knee, glides anteriorly during knee
extensionwhenthe tibia is moving anteriorly,and the
ll4
Figure5-2. Accessoryanterior
gliding of the tibia on the
femur during physiological
kneeextension.
Figure5-3. Extraarticular accessory motior\ which is the
upward rotation of the scapula
that accompaniesshoulder flexton.
5 . Motion Restictions
Femur
O$e . PATHOLOGY AND PATIENT PROBLMS
:emoralcondyles,which have convexsurfacesat the
<nee,glide posteriorly during knee extensionwhen
--nefemur is moving anteriorly.
PATTERNS
OFMOTION
RESTRICTION
Capsular
andNoncapsular
Patterns
ofMotion
Restriction
l1le restrictionof motion at a joint canbe classifiedas
:aving either a caysularor a noncaVsular
pattern. A
:apsularpattem of restrictionis the specificcombina:on of motion lossthat is causedby shorteningof the
'oint capsulesurroundinga joint. Eachsynovialjoint
ras a unique capsularpattern of restriction.Capsular
rattems generally include restrictionsof motion in
::rultipledirections.Ior example,the capsularpattern
:or the glenohumeral joint involves restriction of
3xternal rotation, abduction, internal rotation, and
lexion to progressivelysmaller degrees.Capsular
f,attemsof restrictionmay be causedby the effusion,
ibrosis, or inflammation commonly associatedwith
legenerativejoint disease,arthritis, immobilization,
fnd acutetrauma.
A noncapsularpattern of restdctionis a combina:on of motion loss that doesnot follow the capsular
eattem.A noncapsularpattem of motion lossmay be
:ausedby ligamentousadhesion,an internalderange:rrent,or an extraarticularlesion.ligamentous adhe,ionwill limitmotion in the directions*lat stretchthe
adheredligament. For example,an adhesionof the
:alofibularligament after an ankle sprainwill restrict
:nkle inversion because this motion olaces the
:dheredligamenton srretch;however,thjs adhesion
'.vill not alter the motion of the ankle in other direc:ons. Internal derangement,the displacement of
.oose fragmentswithin a joint, will generallylimit
:rrotiononly in the directionthat compresses
the frag:nent. Ior example,a cartilagefragmentin the knee
-,villgenerallylimit knee extensionbut will not limit
klee flexion. Extraarticularlesions,such as muscle
adhesions,hematomas, cysts, or inflamed bursae,
nay limit motion in the directionof either stretchor
.ompression,dependingon the nature of the lesion.
For example,adhesionof the quadricepsmuscle to
-rheshaftof the femurwill limit stretchinsof the mus;le, while a poplicealcyst will limit compression
of
-J-re
popliteal area.Both of these lesionswill restrict
irotion in the noncapsularpattern of restrictedknee
Jexion.with fulJ.painless
kneeexrension.
115
TISSUES
THAT
CANRESTRICT
MOTION
Contractile
andNoncontractile
Tissues
Any of the musculoskeietaltissuesin the area of a
motion restrictionmay contributeto that restriction.
Thesetissuesaremostreadilyclassifiedascontractile
or
notlcontractile
flable 5-1). Contractile tissue is composedof the musculotendinousunit, which includes
*re muscle,the muscuiotendinousjunction, the tendon, and the tendon's interfacewith bone. Skeletal
muscleis consideredto be contractilebecauseit can
contractby forming cross-bridges
of the myosin proteins with the actin proteins within its fibers.24
Tendonsand their attachmentsto boneareconsidered
contractilebecausecontractingmusclesapply tension
direcdyto thesestructures.When a muscleconftacts,
it appliestensionto its tendons,causingthe bonesto
which it is attachedand the surroundins tissuesto
movethroughtheavailable
accjveROM. *hen all the
componentsof the musculotendinousunit and the
noncontractiletissuesare functioning normall, the
availableactiveROM will be within normal limits for
the ageand sexofthe subject.Injury or dysfunctionof
contractiletissuegenerallyresultsin a restrictionof
active ROM in *re direction of movement oroduced
by contraction of the m usculotendinousunit.
Dysfunction of contractiletissue may also result in
pain or weaknesson resistedtestingof the musculotendinousunit. For example,a tear in the anteriortibialis muscleor tendon can restrictactivedorsiflexion
at the ankleandreducethe forcegeneratedby resisted
testing of ankle dorsiflexion,but this lesion is not
Contractile tfusue
Noncontraatile tissue
Muscle
Skin
Musculotendinousjunction Ligament
Tendon
Bursa
Tendinousinterface
with bone
Capsule
Articular cartilage
Intervertebraldisc
Peripheralnerve
Dura mater
5 . Moriofl Resttictiotts
ll6
likely to alter passiveplantar flexion, dorsiflexion,
ROM, or activeplantarflexion strength.
A11tissuesthat are not componentsof the musculotendinous unit are considered noncontractile.
Noncontractiletissuesincludeskin, fascia,scartissue,
ligamenqbursa,capsule,articularcanilage,bone,intervertebraldisc,newe, and dura mater When the noncontractiletissuesin an areaare functioningnormally,
the passiveROM of the segmentsin that areawill be
within normallimits. Injury or dysfunctionof noncontractile tissue can causea restrictionof the passive
in question
ROM o[ the johcs in rheareaof the cissue
oI actjveROM.2s
to restriction
andmayalsocontribure
The direction,degree,andnatureof the motion restriction dependson the type of noncontractiietissue
involved,the type of tissuedysfunction,andthe severiqyof involvement.Forexample,adhesivecapsulitisof
*re shoulder,which involvesshorteningof the glenohumeraljoint capsuleand elimination of the inferior
axiliaryfold, will restrictbothpassiveandactiveshoul(Iig. 5-4).
derROM in a capsularpattem26-31
THATGANCAUSE
MOTION
PATHOLOGIES
RESTRICTIONS
Contracture
Motion may be restrictedif any of the soft tissue
structuresin an area have become shortened.Such
may
soft tissue shortening,known as a contracturet
noncontractile
tissues.32,33
A
occur in contractileor
resuitcontracturemay be causedby immobilization
ing from external splinting provided by a cast or
splint, for example.Contracturesare also causedby
imbalanceof musclepower resultingfrom weakness,
ascouldbe causedby poliomyelitisor from spasticity
from central, nervous system (CNS) damage, for
It has been proposedthat immobilizaexample.33,34
tion results in contracturebecauseit allows anomalouscross-linksto form betweencollagenfibers and
it causesfluid to be lost from fibrous connectivetissue,includingtendon,capsule,ligament,and fascia.34
36 Anomalous crosslinks can developwhen tissues
remain stationarybecause,in the absenceof normal
stressand motion, fibersremainin contactwith each
otherfor prolongedperiodsand startto adhereat their
points of interception.Thesecross-linksmay prevent
normalalignmentof the collagenfiberswhenmotion is
attempted.They also increasethe stressrequiredto
stretchthe tissue,limit tissueextension,and resultin
contracture(Iig. 5-5).Iluid losscanalsoimpair norrnal
fiber gliding,causingcollagenfibrilsto haveclosercontactandlimitins tissueextension.32
The risk of contractureformauon rn responsero
immobilization is increasedwhen the tissuehas been
injuredbecausescartissue,which is formedduringthe
proliferationphaseofhealing,tendsto havepoor fiber
alignmentand a high degreeof cross-linkingbenveen
,:'.:ii.:'.,.\\
', \
,:.,. } . ' . . . ' . , ]
1.',:
i.:..;.,.;;;,;,'t
r 1 1:.:.,.,.; f.r-.:. .,_
,"/
l\.'::,r,ll
'.':i
L\
li
J,/ \'::,1.'tl\
Normal inferiorjoint
capsule
HUmerus
Figure5-4. Joint capsuleshorteningand adhesionrestricting shoulder rangeof motion.
One . PATHOLOGY AND PATIENTPROBLEMS
CollagenFibersat Resl
withCrosslinks
NormalCollagen
Fibersat Rest
I
t
I
I
I
+
5-5. Normal collagenfibersandcollagenflberswith
Figure
cross-links.(FromWoo SL,Matthews [{ AkesonWH et
to immobility.Correlative
aLConnective
tissueresponse
study of biomechanicalmeasurementsof normal and
Mayimmobilized rabbrtktrces,Anhitls andRheumatism,
permission
of
197
5.
This
material
is
used
by
78(3):262,
June
of JohnWiley & Sons,Inc.)
Wiley-Liss,
Inc.,a subsidiary
its fibers.Restrictionof motion after an irlury may be
further aggravatedif a concurrentproblem, such as
sepsisor ongoing trauma, amplifies the inflammatory
scarring.33
responseand causesexcessive
A persistentshort€ningof a musclethat is resistant
A muscle
to stretchis known as a musclecofltracture.
contracturecanbe causedby prolongedmusclespasm,
guarding, muscle imbalance, muscle disease, or
ischemicmusclenecrosis,and by immobilization.33A
musclecontracturemay limit both activeand passive
motion of the joint(s)that the musclecrossesand can
also cause deformity of the joint(s) normally cont'^ll.J
hv thp mr,vle
Edema
Normally,a joint capsulecontainsfluid but is not fully
distended.This allows the capsuleto fold or distend
tt7
when the joint moves, altering its size and shape
as required for movement through fuI1 ROM. If
excessivefluid forms inside a joint capsule,a condition known as ixtraatticularedema,the joint capsule
becomesmore distended,limiting i* folding and further distention and potentially restrictingbo*r passive and activejoint motion in a capsularpattem.For
example,intraarticularedema in the knee will producethe capsularpattern of knee flexion being more
limited than kneeextension.
Accumulation of fluid outside of the ioint, a
condition known as extraarticularedema,may also
restdctactiveand passivemotion by causingsoft tissue approximation to occur earlier in the range.
Extraarticularedema generallyrestrictsmotion in a
noncapsularpattem. Ior example,edemain the calf
musclemay resffict knee flexion ROM while having
no effecton kneeextensionROM.
Adhesion
Adhesion is the abnormal joining of parts to each
Adhesionmay occurbetvveendifferenttypes
other.37
of tissue for various reasonsand ftequendy causes
restriction of motion. During ttre healing process,
scartissuecan adhereto surroundingstructures,and
fibrofatty tissue may proliferate inside joints and
adherebetweeninftaarticularstructuresas it matures
into scartissue.38
Prolongedjoint immobilizatioq even
in the absenceof local injury can also causethe synovial membrane sunounding the joint to adhereto the
cartilageinside the joint. Adhesionscan affect both the
quality and the quantity of joint motion. For example,
with adhesivecapsulitis,not only doesthe joint capsuleshorten,it alsoadheresto the slmovialmembrane.
This lirrli* motion andreduces,or evenobliterates,the
space between the cartilage and the sl,novial membrane, thus blocking normal synovial fluid nutrition
that can
and causingarticular cartilage^d-egeneration
alterthe qualityof joint motion.rr
Mechanical
Block
Motion canbe mechanicallyblockedby bone or ftagments of articularcartilage,or by tearsin intraarticular discs or menisci. Degenerativejoint diseaseor
malunion of bony segmentsfollowing fracturehealing frequendy resultsin a bony block that restricts
joint motion in one or more directions (Fig 5-Q
This is becausethese pathologies cause bone to
tta
5 . Motiofl Restictioqs
length of the spinal column without interuption of
transmission.au
Adverseneuraltensionis the presence
of abnormal responsesproduced from peripheral
nervous system structures when their ROM and
stretch capabilitiesare tested.arAdverseneural tension may resulcfrom majoror minor nerveinjury or
may be causedindirecdy by extraneuraladhesions
that result in tethering of the nerve to surrounding
structures.Nerve injury may be the result of trauma
due to friction, compression,or stretch.It may alsobe
causedby disease,ischemia,inflammation, or a disFigure5-6. Osteophytesblocking metatarsophalangeal ruption in the axonaltransportsystem.42
]schemiacan
extenston.
pressure
extravascular
fluid, blood,
be causedby
ftom
discmaterial,or soft tissueswith decreased
mobiliqy.
joints.
hypertrophy in or around the
Loosebodiesor
Adverseneural tensionis most commonly due to
fragmentsof articular cartilage,causedby avascular restriction of nerve motion. A number of structural
necrosisor ffauma,canalsoalterthe mechanicsof the
features predispose nerve motion to restriction.
joint, causing"lockingoin variouspositions,pain,and
Nerve motion is commonly restrictedwhere nerves
pass through tunnels, as, for example, where *re
other dysfunctions.33
Tearsin intraarticularfibrocarti
laginous discs and menisci caused by high-force median nerve passesthrough the carpal tunnel or
traumaticinjury or by repetitivelow-force straingenwhere the spinal nervespassthrough the interuerteerallyblock motion in one directiononly.
bral foramina.Peripheralnewe motionis alsolikely to
be restrictedat points where the nervesbranch;for
example,where the ulnar nerve splits at the hook of
DiscHerniation
Spinal
the hammateorwhere the sciaticnervesplitsinto the
pironeal and tibial nervesin the fiigh. Placeswhere
Spinaldischerniationmay resultin direct blockageof
sninal motion if a portion of *re discal material
the systemis relativelyfixed arealsopoints of vulnerbecomestrapped in i facet joint or if the disc comability; for example,at the duramater at L4 or where
pressesa spinal nerve root where it passesthrough
the common oeronealnerve oassesthe head of the
the vertebralforamen. Other pathologiesassociated fibula. The system is also ielatively fixed where
with spinal disc hemiation, including inflammation,
nervesare closeto unyieldinginterfaces;for example,
hyp€ftrophic changes,decreaseddisc height, and
where the cordsof the brachialplexuspassover the
pain, may further limit spinal motion. Inflammation
first rib or the greateroccipitalnerve passesthrough
*re fasciain the posteriorskull.al
about the spinalfacetjoint or herniatedsegmentcan
limit motion by narrowing the vertebralforamenand
compressingthe nerveroot. Hypertrophicchangesat
Weakness
the vertebral margins and facet joints, as well as
decreaseddischeight, alsonarow the vertebralforaWhen musclesare too weak to seneratethe force
men, making the nerve root more vulnerable to
requiredro move a segmenL
of the body throughits
compression.Painmay limitmotion by causinginvolnormal ROM. activeROM will be restricted.
untary musclespasmsor by causing*re individual to
weakness may be the result of contractile
restrictmovementsvoluntarily.
changessuch as atrophy or injury poor
along the motor nerves,or poor synaptic
sion at the neuromuscularjunction.
Osleophytes
Adverse
Neural
Tension
Under normal circumstances,the nervous system,
including *re spinal cord and the peripheralnerves,
must adapt to both mechanicaland physiological
stresses.39
lor example,during forward flexion of the
trunk, the newoussystemmust adaptto the increased
0therFactors
Motion restrictions may also be causedby
other factors, including pain, psychological
and tone.Painmay restrictactjveor passive
O,te . PATHOLOGYAND PATIENTPROBLEMS
dependingon whether contractileor noncontractile
sffucturesare the sourceof the pain. Psychological
factorssuchasfeat poormotivatior! or poor compr€hension are most likely to causerestriction of only
active ROM. Tone abnormalities,particularlyhypotonia or flaccidity, may also impair the control of
activemusclecontractionsand may thus limit active
ROM.
ASSESSMENT
OFMOTION
RESTRICTIONS
When a patient seeksmedical treatment for complaints of limited motion. an examination of the
mobility of all the structuresin the areaof the restriction, including the joints, muscles,intra- and exffaarticular structures. and newes. should be made.
Evaluationof all these findings is required to determine the pathophysiology underlying the motion
restrictioq identify the tissues limiting motioq and
assessthe severity and irritability of the dysfunction.€ This comolete examination and evaluation
will direct treatment to the appropriatestructure(s)
and will facilitate selectionof the optimal intervention to meet goals.Ongoing assessment
of outcomes
is required to modify treatment appropriately in
responseto changesin the dysfunction. This will
accelerateand optimize progresstoward the treatment goals.22,23'42
A variety of tools and methodsare
availablefor quantitativeand qualitative assessment
of motion andmotion restrictions.
Measures
0uantitative
Goniometers,tape measures,and various types of
inclinometersare commonly usedin the clinical setting for quantitativeassessment
of ROM. Thesetools
provide objective and moderately reliable measures
of ROM. and are oracticaland convenientfor clinical
use. Radiographs,photographs,electrogoniometers,
flexometers,and plumb linesmay be usedto increase
the accuracyand reliability of ROM measurement.
Theseadditionaltools areoften usedfor researchpurposesbut are not availablein most clinical settings.
The different tools provide different information
about the available or demonstratedROM. Most
tools,includinggoniometers,inclinometers,and electrogoniometers,provide measuresof the angle, or
changein angle, between body segments,whereas
other tools, such as the tape measure,provide measuresof the changein lengthof bodysegments.aa
l19
Measures
0ualitative
techniquessuchassoft tissue
Qualitativeassessment
palpatiorSaccessorymotion testing,and end-feelprovide valuableinformation about motion restrictions
that canhelp to guidetreaunent.Soft tissuepalpation
may be usedto assessthe mobility of skin or scartissue,local tendemess,the presenceof musclespasm,
skin temperature,and the quality of edema.It is also
usedto identify bony landmarksbefore quantitative
measurementof ROM.
TestMethods
andRationale
Active, resisted,passive,and accessorymotion, and
neuraltensiontestingcanbe usedto determinewhich
tissuesare restrictingmotion and the nature of ttre
pathologiescontributingto a motion restriction.
Activerangeof motion
Active ROM is testedby askingthe subjectto move the
desiredsegmentto its limit in a given direction.The
subjectis askedto reportany s)'mptomsor sensations,
such as pain or tingling, experiencedduring this activity. The maximum motion is measuted,and the quality
or coordination of the motion and any associated
symptoms are noted. Testing of active ROM yields
' information regardingthe subjecCsability and willingnessto move functionally and is generally most useful
for assessingthe integrity of contractile structures.
The following questionsshould be noted when
testingactiveROM:
1. Is the ROM symmetrical, normal, restricted,or
excessive?
2. Whatis *re quality of the availablemotion?
3. Are any signs or symptoms associatedwith the
motion?
Resisted
muscle
testing
Resistedmuscle testing is performed by having the
subjectcontracthis or her muscleagainsta resistance
strong enough to prevent movement.45,46
Resisted
muscletestsprovide information about the ability of
a muscleto produceforce.This information may help
detemine whether contractileor noncontractiletissuesare the sourceof a motion resffictionsincemuscleweaknessis commonly the causeof a lossof active
ROM.47
Cyriax25has identified four possibleresponsesto
resisted muscle testing and has proposed interpretations for each of these responses(able 5-2).
5 . Motiot Restrictiotts
120
Interpretation
1. Strongand painless
No apparentpathologyof contractileor neryoustissue
2. Strongand painful
trAinorlesionof musculotendinousunit
3. Weak and painless
Completeruptureofthe musculotendinousunit
Neurologicallesion
4. Weak and painful
Partialdisruptionof the musculotendinousunit
Inhibitionby pain due to pathologysuchasinflammation,
f',.r"'" ^' -.^-1,.Concurrentneurologicaldeficit
lromCynaxJ: Textboab
of Orthoyedic
Medicine,ed 6, Baltimore,1975,Williams & Wilkins.
When the force is strong and there is no pain with
testing,this indicatesno pathology of contractileor
nervoustissues.When the force is strongbut pain is
producedwith testing,this usuallyindicatesa minor
structurallesionof the musculotendinousunit. When
the force is weak and there is no pain with testing,
this indicates a complete rupture of the musculotendinous unit or a neurologicaldeficit. When the
force is weak but pain is producedwith testing,this
indicatesa minor structurallesion o[ the musculotendinousunit with a concurent neuroloeicaldeficit
or inhibition of conffacdon resultinglrom pain
causedby pathology such as inflammation, fracture,
or neoplasm.
Passive
rangeof motion
PassiveROM is assessedby the tester moving the
segment to its limit in a given direction. During
passive ROM testing, the quantity of available
motion is measured,and the quality of motion and
symptoms associatedwith motion and the end-feel
are noted. End-feelis the quality of the resistanceat
the limit of passivemotion felt by the clinician.An
end-feelmay be normal (physiological)or abnormal
(pathological).A normal end-feelexistswhen passive
ROM is full and the normal anatomyof the joint stops
movement. Certain end-feelsare notmal for some
joints but may be pathological at other joints or
at abnomal points in the range.Other end-feelsare
abnormal if felt at any point in the motion of any
joint. Normal and abnormalend-feelsfor most joints
arelistedinTable 5-3.20,42'47
PassiveROM is normally
limited by stretchingof soft tissuesor by the opposition of soft tissuesor bone and may be restrictedasa
result of soft tissue contracture,mechanicalblock,
or edema.The amount of passivemotion available
and *re quality of the end-feel can assist in the
determination of tlre structures at fault and the
nature of the pathologiescontributingto the motion
resffiction.4/
Combining the findings of active
range of motion assessment, resrsted
muscle testing, and passive range of
motion
Combining the findings of active ROM, resisted
muscle testing, and passive ROM can assist in
differentiatingbewveenrestrictionsoI motion caused
by contractile and nonconffactile structures. For
example, if active elbow flexion is restricted, the
elbow flexors are weak and passiveelbow flexion
rangeis normal, then the structureslimiting motion
are most likely to be contractile. In contrast, if
both active and passive elbow flexion ROM are
restrictedand the strengthofthe elbow flexorsis normal, then noncontractile tissues are proba
involved. Other combinations of abnormality may
indicate muscle substitution durine active ROM
testing, psychologicalfactors limiting motion,
use of poor testing technique, or pain inhibi
musclecontraction(lable 5-4).To definitelyimpli
a particular pathology or a particular stuucturq
the findings of thesenoninvasivetests may need to
be correlatedwith the findinss of other
pf 5-3 Descriptions and Examplesof Different Types of End-Feels
Type
Description
Exarnples
Comments
Hard
Abrupt halt to movement
when two hard surfaces
meet
Normal: elbow extension
Abnormal:resuitof malunion
fractureorheterotoPic
ossification
May be normal or abnormal
Firm
Leathery firm resistance
when rangeis limited by
joint capsule
Normal: shoulderrotation
Abnormal:resultofadhesive
capsulitis
May be nomal or abnormal
Soft
Gradualonsetofresistance
when softtissue
approximatesorwhen
rangeis limited by length
of muscle
Approximation:kneeflexion
Musclelength:cervicalside
bending
May be normal or abnormal,
dependingon tissuebulk
andmusclelength
Empry
Movement stoppedby
subjectprior to tester's
feelingresjstance
Passiveshoulderabduction
stoppedby subjectdue to
pain
Always abnormal
Spasm
Movementstoppedabrupdy
by reflexmuscle
contraction
?assiveankledorsiflexionin
subiectwith spasticitydue to
uppermotor neuronlesion
Active trunk fl€xion in subiect
with acutelow backinjLrry
Always abnormal
Springyblock
Reboundfelt and seenat end
ofrange
Causedby loosebody or
displacedmeniscus
Always abnormal
Boggy
Resistance
by fluid
Kneejoint effusion
Always abnormal
Extended
No resistancefeltwithin
the normal rangeexpected
for t-hepanicularjornt
Jointinstabiliryorhypermobility
Always abnormal
ed 3, New York, 1991,
lrom Cote L, CrutcherMD: The basalganglia.In KandelERuSchwartzJH,fessellTM, eds:P/wiVlesofNeuralSciexce,
:Lsevier.
h
g
5-4 Combining the Findings of Active Rangeof Motion, ResistedMuscle Testing, and
PassiveRange of Motion Assessment
Active range
of motion
Resisted
testing
Passive range
ofmotion
Int€rpretation
Normal
Normal
Normal
No pathologyrestrictingmotion
Normal
Normal
Abnomal
Pathologybeyondterminalactiverangeof motion
Poortestingtechniquefor passiverangeof motion
Normal
Abnormal
Abnormal
Poortestingtechniqueforpassiverangeofmotion
Strengthat least3/5butless*ran 5/5
Normal
Abnormal
Normal
Strengthat least3/5 butless*Ian 5/5
Abnormal
Normal
Abnormal
Nonconffactiletissuerestrictingmotion
Abnormal
Abnormal
Normal
Contractiletissueiniury resuictingmotion
Abnormal
Normal
Normal
Poorrestingtechniquesforactive rangeof motion or
psychologicalfactorslimiting activerangeof motion
Abnormal
Abnormal
Abnormal
Conuactileandnoncontractiletissuesrest ctinSmotion
122
5 . Motiofl Restrictiofts
proceduressuch as radiographicimaging, diagnostic
injection, arthroscopic exploration, and blood
tests.
motion
Passive
accessory
Passiveaccessorymotion is testedusing joint mobiThe clinician can
lization treatrnent techniques.s,13
to
assess
the motion
use thesetreatmenttechniques
joint
surfaces and the extensibility of maior
of
ligamentsand portions of the joint capsule.During
accessorymotion testing the clinician notes qualitatively if the motion felt is greatertharl lessthar5 or
similar to the normal accessorymotion expectedfor
that joint in that planein the particularindividual and
Ac."ttory
if pain is produced with testing.22,4e-50
motion testing may provide information about joint
mechanicsnot availablefrom other tests.Ior example, a reduction of accessorygliding of the glenohumeral joint when passive shoulder tlexion is
normal may indicatethat glenohumeraljoint motion
is resfticted,and the motion of the scapulothoracic
joint is excessive.
Musclelength
Muscle length is tested by passively positioning
muscle attachmentsas far apart as possibieto elongate the muscle in the direction opposite to its
action.4sThe testing of muscle length by this technique will producevalid resultsonly if pathology of
the noncontractilestructuresor muscletone doesnot
limit jointmotion. When testingthe lengthof muscles
that crossonly one joint, the passiveROM available
at that joint will indicatethe length of the muscle.Ior
example, the length of the soleus muscle can be
assessedby measurement of passive dorsiflexion
ROM at the ankle.To test the length of a musclethat
crossestwo or more joints, the musclemust first be
elongatedacrossone o[ the joints and then that joint
must be held in that position while the muscle is
elongatedas far as possible acrossthe other joint
that it crosses.4s
The oassiveROM availableat the
joint
wiil
indicate the length of the muscle.
second
the
length
of the gasrocnemiusmuscle
For example,
can be tested by first elongatingit acrossthe knee,
by placingthe knee in full extension,and then measuring the amount of passivedorsiflexionavailableat
the ankle. It is essentialthat multijoint musclesbe
fully extendedacrossone joint before measurement
at the other ioint to obtain a valid test of muscle
length.
Adverseneuraltension
Adverseneuraltensionis usuallytestedby passively
placing neural structuresin their position of maximum length.Evaluationis basedon comparisonwith
the contralateralside, comparisonwith norms, and
of the symptomsproducedin the position
assessment
maximum
length.
of
Adverse neural tension tests include the passive
straight leg raise (PSLR"Lasegue'ssign), prone knee
bend, passiveneck flexion, and upper limb tension
tests.The PSLRis the most commonly used neural
tension test and is intended to test for adverseneural tensionin the sciaticnerve.
Becauseadverseneuial tensiontestsmay alsoprovoke s;rmptoms in the presence of pathologies
associatedwith the muscles or joints, it is recommended that maneuversthat apply tension to the
nervoussystembutdo not additionallystressthe muscles or joints be used to differentiatethe sourceof
symptoms with this ty?e of test. Ior example,the
PSLRtest can provoke symptomsin the presenceof
pathologiesassociated
with the hamstringmusclesor
the sacroiliac,iliofemoral,orlumbarspinalfacetjoints.
Therefore at the onset of s)'rnptomswith this test,
additionaltensioncan be appliedto the nervoussystem by passivelydorsiflexingthe ankleto increasethe
tension on the sciaticnerve distally or by passively
flexing the neck to tighten the dura proximally. If these
maneuversincreasethe patient'ss;'rnptoms,adverse
neuraltensionratherthan joint or musclepat'hologyis
probablythe causeof symptoms.al
toRange
of
andPrecautions
Contraindications
Techniques
Motion
when
Rangeof motion techniquesarecontraindicated
motion of a part may disrupt *re healing process.
However, some controlledmotion within the range,
speed,and toleranceof the patientmay be beneficial
during the acute recovery stageor immediately following acute tearc, ftactures,and surgery Limited,
controlled motion is recommendedto reduce the
severity of adhesion,contracture,decreasedcirculation, and loss of strength associatedwith complete
immobilization.33,aT
123
O e. PATHOLOGY AND PATIENTPROBLEMS
Contraindications
techniquesare con-Lctiveand passiveassessment
=aindicated:
1 In the region of a dislocation or an unhealed
fracture.
?. Immediatelyfollowing surgrcalproceduresto tendons,ligaments,muscle,joint capsule,or skin.
F
(,
z
uJ
Precautions
Caution should be obsewed when performing
active or passiveROM techniqueswhen motion to
-Jrepart might aggravatethe condition. This may
SCCUr:
1. When there is an infection or an inflammatory
processin or aroundthe joint.
2. In patientstaking pain medicationwho may not
be ableto respondappropriately.
3. In the presenceof osteoporosisor any condition
that causesboneftagiliry.
4. With hypermobile joints or joints prone to subluxation.
5. In painful conditionswhere the techniquesmight
reinforcethe severityof the symptoms.
6. In patientswith hemophilia.
7. In the regionof a hematoma.
8. lf bonyankylosisis suspected
9. Immediatelyafter an injury where therehasbeen
a disruptionof soft tissue.
10. In the presenceof myositis ossificans.
In additioq neural tension testing should be per[ormedwith cautionin the presenceof inflammatory
conditions;spinal cord symptoms; tumors; signs of
nerveroot compression;unrelentingnight pain; neurologicalsymptomssuchasweakness,reflexchanges,
or lossof sensationlrecentparesthesiaor anestltesial
al a2 Detailed
and reflex sympathericdystrophy.3q
contraindicationsand precautionsfor each specific
neuraltensiontest areprovidedin other textsdevoted
to the assessmentand treatrnent of adverseneural
rension.4l
APPROACHES
FOR
MOTION
TREATMENT
RESTRICTIONS
Stretching
Currendy,most noninvasiveinteruentionsfor reestablishing soft tissue ROM involve sffetching.Clinical
TIME
z
o
a
z
ut
TIME
Figure5-7. The relationshipsof time, tension, and length
during creepand stressrelaxation.
and experimentalevidencedemonstratesthat stretching can increasemotion; however, the results may
not be consistentand the recommendedprotocols
vary51 When a stretch is applied to connectivetissues,within the elastic limit, over time the tissues
may demonstratecreep,stressrelaxation,and plastic
deformation.S2Creep is transient lengthening or
deformation with the application of a fixed load.
is a decreasein the amount of force
Stress-relaxation
required over time to hold a given length (Fig.5-7).
Creepand stressrelaxationcan occurin soft tissuein
a short time and are thought to be dependenton
Plastic
the viscous components of the tissue.53'55
124
I
I
|
|
||
I
I FE
z
5 . Motiott Rcsttictiohs
-
t
|
|
Ptastic
deformarion
Etasric
deformation
|
'...--
I AA
| :ffiiix:?;:il:t"',5fi".fi:.1T
I
ut
|
|
|
|
I
|
|
|
t
Load
on
t
Load
or
I
I
|
|
|
appliedfor a proiongedtime to causeplasticdeforma_
tjon. The Jengthof-timenecessary
ro determinerhac
no furcherROM gainsarepossibleis nor known and ]
is probablydepe"ndent
on rhe specificpoLhologyor j
p at h o l o g i ecsau s i n gr h er e srr i c t i o a
n n di L s d u r a t i oLnr . j
additionLotime.the forcedirectionandspeedof the I
,
TIME
rnre
|
I
I
I
I
rissueor cau,inghypermobiliry.
I
Many srretchingLechniques
ro increasesoft tis_ |
sue lengrbhave beendescribed.
The mosLcommon I
of
stretching
are
passive
sLrerching.pro. I
to"r
prioceptive neuromuscular facilitation (PNI), and I
ballistic stretching(Table5-5). To perform a passive I
Fisure
5-8.plastic
deformation
versus
elastic
deformation.*[:'f';:"
deformation is the,elongationproducedunder loading drat remainsafter the load is removed (Iig. 5-8).
After plastic deformation,tissuewill have a permanent increasein length. A controlledstretchmust be
,L.-:.l"i:l' :Hi:"Ir:l.i
o;iljt?:,.T
I
j,,H:l::f
jil"""/fi
:il:',",'#d:,*
;i?;,';:r
stretch. External devices such as progressiueend I
range splints, serial casts,or dynamiclplint, -"y I
also-beusedto stretchtissuepassively.aithough opti- |
mal parametersfor passivelyttr"t.Ling
tO
""tt
I
p u-u t*"rofsrerching
I
Metbod
Description
Examples
Comments
l
Limb held passivelyin a
positionin which the subject
Manualpassivestretching
Progressive
end range
Painperceptionis a factor,
Resultsin no motor learning
Passive
reeis
amird
stretch
2. Proprioceptive Activemusclecontraction
ojlllTlior,",-,
conffact-relax
I
I
I
ol'::#ff:H;TJ;n*"
I
rr."quir",tn" u..i.turL1tJr
I
n
i"".fi:f;:?'"'
ffiim;f ffi*'" l$[iil1l**""0,,o.
_fl"d#]'proric
3 Banistic ^'::?"H:*:'ffi';:TI:'i$:
^:il,:':::'*::Ji*""r"'?::::T*;'i*:"," I
subject's available range of
this may increase f.^^.-^
motion
tightness
by activJtri!
I
|
I
[#:'f,Ti;l]:
I
-nu"cres
I
1yril5".1,'"1;'i:,?""",?'":;t1::if,1,?"i.:f;1:TJ:'#ifrli'#x"J
rec.sor oneoou-or nvo tJ :eco-Opass.ve
\tiptche5on arWe doritliexto-ta-gpo! -nouon.Josf
26:2
| 4-Dl - |(r9_
.
+BandyWD, kion JM, BrigglerM: The effeci of time and frequencyof staticstretchingon
flexibility of rhe hamstringmuscles.pl,,s 1r
77:1090-1096,1997.
I
I
One c PAIHOLOGY AND PATIENT PROBLEMS
lathological tissueshave not been established,it is
generally recommended that low-load, prolonged
iorces be applied to minimize the risk of adverse
effects.
Manipulation of a joint while the subjectis anes-Jretizedalso involves passivestretchingof the soft
dssuesto increaseROM. Manipulation under anesihesiacan producea rapid increasein ROM because
high forcesthat would otherwisebe painful or cause
musclesto spasmmay be applied.Thesehigh forces
may cause greater increasesin soft tissue length
andmay tear adhesionsto increasemotion; however,
-fie risk of damaging structures or exacerbating
inflammation may be greaterwith such techniques
-.han with stretching while the subject is fully
conscious.
Proprioceptive neuromuscular facilitation techniques for muscle stretching inhibit contraction of
rhe musclebeins stretchedand facilitate contraction
This is achievedby having the
o[ its opponent.5o
subject actively contract and then voluntarily
relaxthe musclesto be stretchedbefore the applicacion of the stretching force. PNF techniqueshave
the advantageover other stretching techniquesof
rncluding a motor leaming component ftom the
repeatedactive muscle contractionslhowever, their
use is frequendy limited by the requirement that
a skilled individual help the patient perform the
techruque.
Ballisticstretchingis a techniquein which the subiect performsshort, bouncingmovementsat the end
of the availablerange.Although somepeopleattempt
to sffetch in this manner, ballistic stretchingis not
generally used or recommended,becauseit may
increasetissue tightness by activating the sketch
reflex.5/
Motion
The formation of conffactures is a time-related
processthat may be inhibiredby motion.3sMotjon
can inhibit contractureformation by physically disrupting the adhesions between gross structures
and/or by limiting intermolecular cross-linking.
Active or passive motion also stretches tissues,
promotes *reir lubrication, and may also alter their
metabolic activiqy,s4Becauseactive ROM may be
125
contraindicatedduring early stagesof healing,particularly when contractile tissue is damaged,passive
motion may be usedto limit conEactureformation at
this stage.For example,continuouspassivemotion
(CPM) can be used to prevent motion loss after
joint trauma or surgery.In addition to inhibiting the
formation of contractures and adhesions, CPM
has been shown to acceleratehealing, improve the
orientation of collagen fibers, and inhibit edema
formation.5s-61
Surgery
Although the noninvasiveapproachesof stretching
and motion frequently resolve or prevent motion
restrictions,in some casesthese approachesare not
effective and surgery may be required to optimize
motion. Surgery will be necessaryif motion is
restrictedby a mechanicalblock, particularly if the
mechanicalblock is bony. In such cases,the surgical
procedureremovessome or all of the tissueblocking
motion. Surgerymay also be required'if stretching
techniquescannotlengthena contractuleadequately
due
or if the functionallengthofa tendonis decreased
procedures
to hypertoniciqy.For example,Z-plasry
arefrequentlyperformedto lengthentheAchillestendon in children with limited dorsiflexioncausedby
congenitalplantar flexion contracturesor by hypertonicity of the plantarflexor muscles.Z-plasty is generally preformedwhen it canbe expectedto permit a
more functional sait than is achievedwith noninvasive techniques alone.9 Surgical procedures to
increase ROM are also frequently performed in
adults. For example, surgical releasemay be performed to restoremotion limited by a Dupuytren's
contracture,and tenotomy may be performedwhen
tendonlengthlimits motion. Surgerymayalsobe performed to releaseadhesionsand lengthenscarsthat
have formed after prolonged immobilization. Ior
example, patients with extensivebums who have
received limited medical intewention frequently
develop contractures that cannot be stretched
sufficiendy to allow fuIl function and therefore
require surgicalrelease.Surgeryis more commonly
requiredto releaseadhesionsthat form after injury if
by prolongedinflammationor
scarringis exaggerated
infection.
126
5 . Motiott Restrictiotts
OFPHYSICAL
AGENTS
INTHE
THEROLE
TREATMENT
OFMOTION
RESTBICTIONS
Although physical agents alone are generally not
sufficient to revelse or prevent motion restdctions,
they may be used as adjuncts to the treatment
of such impairments. Physical agents combined
with other appropriate treatment can enhance
the functional recovery associatedwith regaining
normal motion. Physicalagents are generally used
as componentsof the treatment of motion restrictions becausethey can increasesoft tissueextensibility, control inflammation, contuolpain, and facilitate
moUon.
Extensibility
Increase
SoftTissue
Physicalagentsthat increasetissuetemperaturemay
be used as componentsof the treatment of motion
resftictionbecausethey canincreasesofttissueextensibiliry thereby decreasingthe force required to
increasetissuelengthand decreasingthe risk of injury
during the stretching procedure.62'64
Applying physical agentsto soft tissuebefore prolongedstretching
can alter the viscoelasticityof the fibers, allowing
66 To achievethe
plastic deFormationto occur.65
maximum benefit from the use of physical agents
that increase soft tissue extensibility, agents that
increasesuperficialtissuetemperature,such as those
describedin Chanter6. shouldbe usedbeforestretching superficialtiisues, whereas agentsthat increase
deep tissue temperature, such as ultrasound and
diathermy,shouldbe usedbeforestretchingdeepsoft
tissues.
Control
lnflammation
andAdhesion
Formation
A numberof physicalagents,panicularlycryotherapy
and certain types of electricalcurrents,are thought
to control inflammation and its associatedsigns
Controlling
and symptoms after tissue injury.6z,6e
inflammation may help to prevent the development
of motion restrictions by limiting the formation
of edema during the acute inflammatory stage
and thereby limiting the degreeof immobilization.
Controlling the severity and duration of inflammation alsolimits the durationand extentof the proliferative responseand may thus limit the formation of
adhesionsduring tissuehealing.
PainDuring
Stretching
Control
Many physical agents, including thermotherapy,
cryotherapy,and electricalcurrents,can help to control pain. This effect may assistin the treatment of
motion restrictionsbecause,if pain is well controlled,
tissuesmay be stretchedfor a longer period, which
may increasetissuelength more effectively.If pain is
controlled,motion may also be initiated soonerafter
inlury limiting the lossof motion causedby immobi
lization.
Motion
Facilitate
Somephysicalagentsfacilitatemotion and thus assist
in tlle treatment of motion restrictions. Electrical
stimulation of the motor nervesof imervated muscles or direct electrical stimulation of denervated
muscle can make muscles contract, These muscle
contractionsmay complementmotion producedby
normal physiological contractionsor substitute for
such conffactionsif the subject does not or cannot
move independently. Water may also facilitate
motion since it provides buoyancy to an immersed
body to assistwith motion againstgravity.The buoyancy of water may prove particularly beneficialin
assisting patients with active ROM restrictions
causedby contractiletissueweakness.