Health Assessment
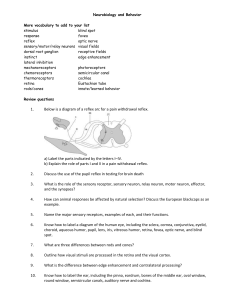
ANATOMY: SPECIAL SENSES | SENSE OF HEARING | EARS
HEARING
Sense of hearing and equilibrium
MECHANORECEPTORS
-
Detect sound waves (touch & hearing)
OUTER EAR
PINNA | AURICLE
-
The only visible part of the ear with its special helical shape
EXTERNAL AUDITORY CANAL | EXTERNAL ACOUSTIC MEATUS
-
A tube running from the outer ear to the middle ear
TYMPANIC MEMBRANE
-
Thin, cone-shaped membrane that separates the external ear from the middle ear
MIDDLE EAR
1|Health assessment
TYMPANIC CAVITY
-
An air chamber
It contains a chain of movable bones which transmits the vibrations of the tympanic membrane
across the cavity to the middle ear
MASTOID ANTRUM | TYMPANIC ANTRUM
-
An airspace in the petrous portion of the temporal bone
AUDITORY TUBE | EUSTACHIAN TUBE
-
Equalizes the pressure between the outer and inner ear
EQUALIZES THE PRESSURE BETWEEEN THE INNER EAR AND THE ATMOSPHERE
Methods we use when we feel pressure inside our ear: swallowing yawning, and chewing
(happens here)
AUDITORY OSSICLES
1.
2.
3.
MALLEUS | HAMMES
Transmits sound vibrations from the eardrums to the incus
INCUS | ANVIL
The middle bone; connects to the malleus and to the stapes
STAPES | STIRRUP
Transmits sound vibrations from the incus to the oval window
It connects middle ear to the inner ear
INNER EAR
COCHLEA
-
Receives sounds in the form of vibrations
Transforms vibrations of the cochlear liquids and associated structures into a neural signals
Organ of hearing
VESTIBULE
1.
2.
Detect changes in gravity and linear accelerations
Responsible in balance
Contains utricle and saccule
UTRICLE
Changes in velocity when traveling (horizontal & vertical)
SACCULE
Acceleration & Deceleration
2|Health assessment
A. OVAL WINDOW | VESTIBULAR WINDOW
Transmits the vibrations to the inner ear
B. ROUND WINDOW | COCHLOEAR WINDOW
SEMICIRCULAR CANALS (ANTERIOR, POSTERIOR, LATERAL)
-
Helps maintain balance when turning spinning, or tumbling
Fluid filled tubes in your inner ear that helps you keep your balance
FLUIDS IN THE EAR
1.
2.
-
Help in transmission of the sound
Are separated from each other
Chemically different
PERILYMPH
Fluid outside
ENDOLYMPH
Fluid inside
NOTES:
FLUID
-
The flow of fluid in the ear counter flows the movement of our body to maintain balance
CERUMINOUS GLANDS
-
Produces earwax
EARWAX | CERUMEN
-
Helps keep the skin in the ear canal soft
Keeps the bugs out
CUPULA
-
Hair-like structure
It helps the movement of the fluid; Endolymph
VESTIBULOCOCHLEAR NERVE VII
-
VESTIBULAR – maintain balance
COCHLEAR – auditory sense
3|Health assessment
SENSE OF HEARING
-
Last sense that is last to leave the body when you die
First to return when you wake up
AUDITORY PATHWAY
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
AURICLE
EXTERNAL AUDITORY CANAL
TYMPANIC MEMBRANE
AUDITORY OSSICLE
COCHLEAR FLUID is disturbed
Ripple disturbs hair cells in the ORGAN OF CONTI/COCHLEA
COCHLEAR NERVE
BRAIN STEM
THALAMUS
AUDITORY NERVE OF TEMPORAL LOBE
ASSESING THE EAR/HEARING
Position
-
Alignment of pinna with the corner of the eye and within 10 degree angle of vertical position
INFANTS
-
Inspection:
Top of the pinna should match on imaginary line extending from the corner of the eye to the occiput
Should be positioned 10 degrees of vertical
New born: hasn’t yet developed the cartilage that will give shape and firmness of shape of the
external ear
Folded/misshape ears are normal for infants
-
Skin Conditions:
Smooth without nodules
Colour pink
Consistent with the patient’s facial colour
Intact on the skin with no lesions
-
To Assess:
To assess gross hearing, ring a bell from behind the infant or;
Have the parent call the child’s name to check for a response
If there is response to the sound the infant may open eyes wider
3 -4 months of age, the child will turn head toward the sound
There are many variations in size and shape of the ear
-
4|Health assessment
-
Palpation:
Palpate the external ear;
Normal: non tender auricle, tragus
Mastoid process for;
Normal: no tenderness, warm to touch, mastoid process easily palpated
Tenderness, temperature, oedema
Deviations
-
Hypoplastic ear
Can be genetic
-
Ear tag
The infant’s external part of the ear are the first areas to develop inside a pregnant mother
Associated with loss of hearing in babies
It may indicate that the internal ear didn’t form correctly inside
5|Health assessment
-
Lop ear
Can be treated – treatment: ear moulding
-
TINITUS
is the perception of noise or ringing in the ears
it's a symptom of an underlying condition, such as age-related hearing loss, ear injury or a circulatory
system disorder
At risk:
seniors / older adults
military personnel
musicians
construction workers
-
TESTS
Whisper Test
-
to assess high-frequency hearing
have the patient occlude one ear
go out of the patient’s sight, at distance of 1-2 ft. , whisper
ask the patient to repeat the phrase
the patient should be able to repeat the phrases correctly
Conductive Hearing Loss
-
is the result of interrupted transmission of sounds through the external and middle structure of the ear
a tear/obstruction in tympanic membrane
Sensorineural Hearing Loss
-
damage to the inner ear, auditory ear, hearing centre in the brain (cochlea)
Mixed Hearing Loss
-
combination of conduction and sensorineural hearing loss
6|Health assessment
-
external to inner ear
-
OTOSCOPY
an examination that involves looking into the ear with an instrument called an otoscope (or auriscope)
performed in order to examine the 'external auditory canal' – the tunnel that leads from the outer ear
(pinna) to the eardrum
-
WEBER TEST
Ernst Heinrich Weber
Using a tuning fork
Quick screen test for hearing
When holding a vibrating tuning fork, always hold the fork by its base preferable as low as possible
Generally performed first and assess for lateralization of sound or whether sound is heard louder in one
ear
Normal: sound is heard equally in both ears (WEBER NEGATIVE)
Deviation: sound is better in impaired ear, including a bone-conductive hearing loss
sound is heard better in ear without a problem indicating a sensorineural disturbance (WEBER
POSITIVE)
If the result is WEBER NEGATIVE no need to perform additional test
-
7|Health assessment
RINNE TEST
In the event of sound lateralization perform Rinne Test
Helps to determine in what area have deviation
Sound lateralizes to the ear with a conductive hearing loss
Masking effect of air conduction has been lost
Expected: sound is heard by both air conduction and bone conduction, air conducted sound can
mask the bone conducted sound
Bone Conductive Deficit: ossicles respond to the direct stimulation of the vibrations and not any sound
that is transmitted by air conduction
Ear with Conductive Hearing Loss: does not receive any air conduction sound to ask or dilute bone
conduction and sound is lateralized to that ear
Compare air conduction to bone conduction
Normal: air conduction of sound is generally louder and heard twice as long as bone conduction
ACBC 2:1
Thus if the patient heard the sound by bone conduction for 8 seconds, sound should be heard by air
conduction by 16 seconds
Ask whether the patient now hears the sound, sound conducted by air is heard more readily
Normal: AC>BC
Deviation: BC>AC or BC = AC – indicates a conduction hearing loss
GENERALLY:
-
8|Health assessment
9|Health assessment
ANATOMY: EYE
SUPERIOR RECTUS
MUSCLES OF THE EYE
Rolls eyeballs upward
INFERIOR RECTUS
Rolls eyeballs downward
MEDIAL RECTUS
Rolls eyeballs medially
LATERAL RECTUS
Rolls eyeballs laterally
SUPERIOR OBLIQUE
Rolls eyeballs on axis
INFERIOR OBLIQUE
Rolls eyeballs on axis
3 LAYERS OF THE EYE
1. SCLERA
2. CHOROID
3. RETINA
Hardest part
Serves as an
attachment
Highly pigmented
Contains lots of blood
vessels | Vascular
Avascular / no blood
Photoreceptors and very fragile
Helps maintain
shape
Outermost layer
Middle layer
Innermost layer
RODs – acts night-time, detects colour (black,
white, and gray), functions in peripheral vision
CONEs – acts daytime, detects various/all
colours, functions best in bright light
3 types of CONES (BLUE: 16%) (GREEN: 10%)
(RED: 74%)
10 | H e a l t h a s s e s s m e n t
LACRIMAL GLAND
-
Produces tears
FOVEA CONTRALIS
-
Small central pit composed of closely packed cones in the eye
Located in the center of the macula lutea of the eye
MEIBOMIAN GLAND
-
Produce and oily substance that keeps the eyes moist
CONJUNCTIVA
-
Mucous membrane, lines the inner surface of the eyelids
Transparent, coral pink, may visible small vessels
CORNEA
-
Avascular
Most exposes and transparent
Nothing protects cornea
Protective window for which the light passes
-
Makes the constriction and dilation of pupils
Iris muscle
CIRCULAR MUSCLE – when contracts it constricts the pupil (parasympathetic)
RADIAL MUSCLE – when contracts it dilate the pupil (sympathetic)
IRIS
PUPIL
-
Protective reflex
Prevents excessively bright light from damaging the delicate photoreceptor
11 | H e a l t h a s s e s s m e n t
-
-
ACCOMODATION PUPILLARY EFFECT – pupil constrict to increase depth of focus of the eye by blocking
the light
PUPILLARY LIGHT REFLEX – the reflex of the eye to the brightness or dimness of the light
CORNEAL LIGHT REFLEX
asymmetrical placement of the corneal light reflex indicates that the eye are not in the proper
alignment
can be due to strabismus
generally caused by weakness or paralysis of eye muscle
LENS
-
Avascular like the cornea
65% water
35% protein
To focus light rays on the retina by accommodation
Distant object – the lens flattens
Near object – the lens gets rounder and thicker
MACULA LUTEA OR FUVEA
-
Contains very high concentration of cones
CILLARY BODY
-
Controls the shape of the lens (cilliary muscle)
Cillary epithelium – produces aqueous humor
Vitreous humor – produced in the non-pigmented portion of the cillary body
AQUEOUS HUMOR
-
Help with the movement of the eye
Anterior
Nourishing the cornea and the lens by supplying nutrition such as amino acids and glucose, the
aqueous humour will: Maintain intraocular pressure.
VITREOUS HUMOR
-
Fillers of the eyeball behind the lens
Posterior
NORMAL INTRAOCULAR PRESSURE (IOP)
-
Ranges from - 12 – 21 mm Hg
CANAL OF SCHLEMM
-
Circular canal lying in the substance of the schlerocorneal junction of the eye and;
Draining the aqueous humor from the anterior chamber
Aqueous humor circulation.
12 | H e a l t h a s s e s s m e n t
VISUAL PATHWAY
1.
2.
3.
4.
5.
6.
7.
8.
LIGHT
CORNEA
PUPIL
CLEAR LENS
RETINA
RODS & CONES
OPTIC NERVE
BRAIN
AQUEOUS HUMOR CIRCULATION
1.
2.
3.
4.
CILLIARY BODY
POSTERIOR CHAMBER OF THE EYE
ANTERIOR CHAMBER OF THE EYE
CANAL OF SCHLEMM
ASSESSING THE EYES
PALPEBRAL FISSURES
-
Length : Endocanthion to Exocanthion
the elliptic space between the medial and lateral canthi of the two open lids
In adults, this measures about 10mm vertically and 30mm horizontally.
13 | H e a l t h a s s e s s m e n t
EYELIDS
-
Overlaps the superior area of / part of the iris and approximate completely with the lower lids when
close.
INFANTS
First week after birth and up to 3 months, baby can focus only on objects and people that are
close up, about 10 – 12 inches from her face
Four to six months when the baby is able to see colour and perceive depth
Baby is able to develop the ability to focus on objects/people – 6 months
8 months – infants can now almost see to the level of an adult with regards to clarity and depth
perception, and able to recognize faces
Infants do not have tears until – 3 months
By 6 months, average infant’s vision is already 20/20
*Binocular fixation pattern
DEVIATIONS
Infantile Esotropia
A form of ocular motility disorder where there is an inward turning of one or both eyes, commonly
referred to as crossed eyes.
It occurs during the first 6 months of life in an otherwise neurologically normal child.
Periorbital area – Periorbital Oedema
a term for swelling around the eyes
Purpura
discoloration - around the eye
Ptosis
Droopy eyelid caused by more serious conditions such as stroke, brain tumour, or cancer of the
nerves or muscle
Uneven opening of the eyes
Lid Lag
static situation in which the upper eyelid is higher than normal with the globe in downgaze
most often a sign of thyroid eye disease, but may also occur with cicatricial changes to the eyelid
or congenital ptosis
Hordeolum/Sty
Most often caused by staphylococcus bacteria
Usually lived around the surface of the eyelid without causing any harm
When a gland becomes clogged with dead skin cells or old oil, these can become trapped and
cause infection
Found on the sides of the eye
Chalazion
14 | H e a l t h a s s e s s m e n t
-
Found at the middle
Caused by non-infectious meibomian gland occlusion, whereas a hordeolum usually caused by
infection
Conjunctivitis
Aka sore eyes
Subconjunctival haemorrhage
bleeding underneath the conjunctiva
the conjunctiva contains many small, fragile blood vessels that are easily ruptured or broken
when this happens, blood leaks into the space between the conjunctiva and sclera
Foreign Object
something that enters the eye from outside the body
Pterygium
Growth of the conjunctiva that occurs the white part of your eye over the cornea
Shape : wedge shape
CAUSE: unknown, too much sun/UV exposure
Jaundice Sclera
The conjunctiva of the eye are one of the first tissues to change color as bilirubin levels rise in
jaundice.
This is sometimes referred to as scleral icterus.
The sclera themselves are not "icteric" (stained with bile pigment), however, but rather the
conjunctival membranes that overlie them.
CAUSE: High bilirubin levels
Red Sclera
caused by dilation of tiny blood vessels that are located between the sclera and the overlying
clear conjunctiva of the eye
usually are caused by allergy, eye fatigue, over-wearing contact lenses or common eye infections
such as pink eye (conjunctivitis)
-
Strabismus
one eye looks directly at the object you are viewing, while the other eye is misaligned
inward (esotropia, "crossed eyes" or "cross-eyed")
outward (exotropia or "wall-eyed")
upward (hypertropia)
downward (hypotropia)
TESTS
SNELLEN’S CHART
15 | H e a l t h a s s e s s m e n t
-
-
Children are tested with snellen letter chart (ages 7 – 8 years old)
To assess the quality of the eyesight of the patient
Expected visual activity is 20/20
Numerator – indicating distance from the chart, it is constant
Denominator – representing the distance a person with normal vision could see and interpret
symbol
Its score is recorded L 20/40
The patient is 20ft from the eye chart and reads with the left eye at 20ft what the “normal” eye
visualizes at 40ft
The patient visual acuity is determined by what line the patient can read correctly
FIXATION TEST
Used to screen vision in children 6 months to 2½ years and for those children up to 3 years cannot
be tested with picture eye *
Used : Penlight & colourful object (RED)
Cover one eye and hold the light 1 ½ ft. away from the child
Move the light/toy from midline, side-to-side
Normally the child will track the light or toy with both eyes
It fails when he objects
-
TESTING VISUAL FIELDS
Measure peripheral vision
50 – Upward field
90 – Temporal field
60 – Nasal Field
70 – Downward field
Considered a neurological rather than ocular
It assesses the integrity of the optic nerve and its appropriate pathways
Deviation: homonymous hemianopia
-
16 | H e a l t h a s s e s s m e n t
-
HIRSCHBERG TEST
Muscle strength and position of the eye can also be determined
The light reflex should be in the same position bilaterally
DEVIATION: Strabismus
-
PUPILLARY ASSESSMENT
To assess pupillary size in a darkened room, illuminate the face from below. Slowly move the light up
to the patient's eye level and check the pupillary response
-
ACCOMODATION OF PUPIL
The normal pupillary response is constriction of the pupils and convergence of the eyes
PUPILLARY ASSESSMENT
Fixed, pinpoint pupils:
Indicate PONS involvement or the use of opiates/drugs
CN III – Oculomotor – constriction of the eye – Originates from the midbrain
-
-
Tumour, Clotted blood, Oedema, Aneurysm
Compression of the nerve may result in dilation on the side of the lesion or the area affected
Cataract
17 | H e a l t h a s s e s s m e n t
-
The lens are affected
Number 1 cause is AGING
-
Arcus Senilis
Cause: lipid/cholesterol (those who are fat or obese) deposits in the periphery of the cornea stromal
layer
ADDITIONAL/S
PERRLA
-
Normal Pupil size: 3-5 mm
Response to light
Brisk, sluggish, non-reactive or fixed
Normally constrict when exposed directly to light
Consensual response
Have at least 10 seconds interval between assessment of each eye
-
Older adults
Visual acuity decreases
the eye ages and become more opaque and loses elasticity
peripheral vision diminishes
eyeball may appear sunken
Less absorption of vitamin B12 in the ileum which may result in PALE CONJUNCTIVA
ASSESSING THE FACE & SKULL AND NECK
FACE
2 Structures of the face that are important in assessing for symmetry
1. Nasolabial Folds
2. Palpebral Fissures
HEAD AND NECK
18 | H e a l t h a s s e s s m e n t
-
Framework of the head is the skull
Normal size of the skull (infant) ranges from 32-38 with an average of 34 – 55-57 in adult
All of the facial bones are immovable except for mandible
The face also consist of many muscles that produce facial movements and expressions
NECK
-
Composed of muscles, ligaments, and the cervical vertebrae
Hyoid bone, several blood vessels, larynx, trachea, thyroid gland
LYMPH NODES OF THE HEAD AND NECK
-
Lymph nodes produces lymphocytes and antibodies as defence against invasion by foreign
substances
Size and shape of lymph nodes vary ; but are buried deep in the connective tissue
Normally lymph nodes are either not palpable or they may feel like small beads
Order in assessing the lymph nodes
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Pre-auricular
Post auricular
Occipital
Submental
Submandibular
Jugulodigastric/tonsilar
Superficial cervical
Deep cervical
Posterior cervical
Supraclavicular
-
DEVIATIONS
Acromegaly
Enlargement of the facial features (nose,eyes) and the hands and feet
-
Microcephaly
Small head
-
Anencephaly
No brain
-
Hydrocephalus
Abnormal enlargement of the head
-
Cushing’s Syndrome
May present with a moon shaped face with reddened cheeks and increased facial hair
-
Scleroderma
Tightened-face with thinning facial skin
Autoimmune disease
Unknown cause
19 | H e a l t h a s s e s s m e n t
-
Bell’s Palsy
Paralysis of the facial nerve (7)
Symptoms may include twitching, weakness, paralysis, drooping eyelid and corner of the mouth,
drooling
-
Hyperthyroidism
Enlarged thyroid gland (goiter)
-
Exopthalmus
Bulging of the eye
-
Jugular Vein Distention
ccurs when the pressure inside the vena cava increases and appears as a bulge running down the
right side of a person's neck
-
NVE
Pressure in the right side of the heart is high
Normal Characteristics of the Thyroid Gland
Smooth surface
Firm consistency
Nontender to gentle pressure
-
Bruit sound
-
An indicator of thyroid hyperplasia
Best heard with the bell of a stethoscope
A soft, pulsatile, whooshing, blowing sound
This bruit is not present normally
PHYSICAL EXAMINATION
Inspection
-
It is a visual examination
This examination must be systematic to assess colour, body shape, wounds, facial expression, motor
behaviours and some area to be examined
Palpation
-
Used to validate your inspection
It is an examination using the sense of touch. The pads of the fingers are used because the
concentration of nerve endings are highly sensitive to tactile discrimination
Light Palpation
Deep Palpation
Percussion
20 | H e a l t h a s s e s s m e n t
-
The examiner places one hand on the patient and then taps a finger on that hand, with the index
finger of the other hand
It can determine the position, size, and consistency of an internal organ
Based on the auditory and tactile perception, the notes heard can be categorized as follows:
• Tympanic
• Hyperresonant (pneumothorax)
• Normal resonance/ Resonant
• Impaired resonance (mass, consolidation)
• Dull (consolidation)
• Stony dull (pleural effusion)
Auscultation
-
Technical term for listening to the internal sounds of the body, usually using a stethoscope; based on
the Latin verb auscultare "to listen"
To auscultate heart, lungs, abdomen
Palpation
-
PRINCIPLES
Have short nails
Warm your hands prior to placing them on the patient
Encourage the patient to breathe normally throughout the palpation
If pain is experienced during the palpation, discontinue the palpation immediately
Inform the patient what you are going to do and why it is necessary
-
TYPES OF PALPATIONS
Light Palpation
-
Light pressure is applied by placing the fingers together and depressing the skin and underlying
structures about ½ inch (1cm)
Used to check the muscle and tenderness
Deep Palpation
-
It is used/done with caution because pressure can damage internal organs
Depresses the skin 2cm or deeper
Hooking Technique
-
To know the size of the liver
21 | H e a l t h a s s e s s m e n t
Fingertips
-
used for localized pulsations
Thrills
-
is felt from light palpation over the chest wall
-
is a slight movement – a palpable vibration due to strong heart murmur (like a purring cat)
Lifts
Heaves
-
is more vigorous movement than the lift, a vibratory sensation felt on the skin overlying an area of
turbulence
-
Percussion
Used to determine the size and shape of internal organs by establishing their border
The detect the presence of air, fluid, enlargement of organ
BONE – flat sound
Lungs / PRESENCE OF AIR – resonance
22 | H e a l t h a s s e s s m e n t
ORGANS / WATER – dull
ABDOMEN – tympanitic
-
Auscultation
the action of listening to sounds from the heart, lungs, or other organs, typically with a stethoscope, as
a part of medical diagnosis
Diaphragm
-
breathe sounds
bowel sounds
normal heart sounds
-
murmur
bruit
Bell
# Most used position when auscultating are – sitting position and supine
23 | H e a l t h a s s e s s m e n t
Instruments used in physical examination
BASIC
-
Stethoscope
Opthalmoscope
Dermatoscope
Otoscope
Tape measure
Reflex hammer
Monofilament
Tuning fork
STANDARD PRECAUSIONS
Nosocomial Infection
-
Infection acquired during hospitalization
Hand Washing / Hand Hygiene
-
Before and after physical contact with each patient
After inadvertent contact (blood, body fluids, secretions, excretions)
After handling any equipment w/ body fluids
Before and after gloving
Gloves
-
Use when you’re going to be in contact with;
Blood and Body Fluids
Excretions and Secretions
And any contaminated things
Gown
-
Wear in doing any procedure to protect yourself
24 | H e a l t h a s s e s s m e n t
Linen / Laundry
-
Are placed in a private room and linens from patients with infectious disease/s are separated
SKIN ASSESSMENT
SKIN: FUNCTIONS
1.
2.
3.
4.
5.
6.
7.
8.
Regulates body temperature.
Prevents loss of essential body fluids, and penetration of toxic substances.
Protection of the body from harmful effects of the sun and radiation.
Excretes toxic substances with sweat.
Mechanical support.
Immunological function mediated by Langerhans cells.
Sensory organ for touch, heat, cold, socio-sexual and emotional sensations.
Vitamin D synthesis from its precursors under the effect of sunlight and introversion of steroids.
Infants and Children
Have very smooth skin – lack of exposure to environmental variables
Subcutaneous is poorly developed thus predisposing infants to hypothermia
Vernix Caseosa
-
Cheese-like substance (sebum)
For the skin not to be easily macerated
Creamy substance on newborn’s skin and has anti-microbial and moisturizing qualities that
help protect them in their new environment
25 | H e a l t h a s s e s s m e n t
Lanugo
-
The baby’s body (esp. shoulders and back) are covered with fine silky hair
(if present) it disappear 10 – 15 days
Apocrine Glands
-
Do not function at this age resulting in odourless perspiration
Makes the skin with a less oily texture
-
Begins to function about 4 weeks
Merocrine is a term used to classify exocrine glands and their secretions in the study of
histology. A cell is classified as merocrine if the secretions of that cell are excreted via
exocytosis from secretory cells into an epithelial-walled duct or ducts and thence onto a bodily
surface or into the lumen
Merocrine
Eccrine Glands
-
Perspiration – present after 1 hour (after birth)
INSPECTION
Skin Colour
Erythema – reddening of the skin
Cyanosis – bluing
Pallor – paling of the skin
Jaundice – yellowing of the skin
Skin Uniformity
Skin’s generally uniform except in
areas exposed to the sun and
areas prone to friction (armpit,
groins, etc.)
Areas with lighter pigmentation
(esp. noticeable in dark skinned
people) – palms, lips, nail beds
Deviations – Abnormal
HYPERPIGMENTATION
-
Abnormal distribution of melanin
Freckles, birthmarks, Mongolian blue spots – etc
26 | H e a l t h a s s e s s m e n t
Cutis Marmorata
-
Skin has a pinkish blue mottled or marbled appearance when subjected to cold temperature
It loses when exposed to warm temperature / normal temperature again (Rewarming)
Senile Lentigines
-
spots that appears when you get old (hyperpigmentation)
Freckles
-
Indication of sun damage
When the skin produces more melanin pigmentation (UV RAYS)
Light brown spots (face, neck, and shoulders)
More prominent to Caucasians
Addison’s Disease
27 | H e a l t h a s s e s s m e n t
-
Also known as primary adrenal insufficiency, result from the insufficient production of these two
hormones, cortisol and aldosterone. Major symptoms include fatigue, gastrointestinal
abnormalities, and changes in skin colour (pigmentation).
HYPOPIGMENTATION
-
Pallor
Partial or complete absence of melanin
Vitiligo
-
Destruction of melanocytes in the area (most prominent in Africans)
Albinism
-
Complete or partial lack of melanin
A congenital disorder
(white) skin, hair, and eyes
Associated with a number of vision defects; photophobia, nystagmus, amblyopia)
They are more prone to sunburn and skin cancer
28 | H e a l t h a s s e s s m e n t
Physiological Jaundice
-
-
-
RBC / Hemoglobin in the blood is divided to HEME and GLOBIN, HEME is divided into BILIVERDIN
and ****** which are then converted to BILURUBIN. BILIRUBIN is collected by the liver, since the
new born or infants (physiological jaundice) have undeveloped/not fully developed LIVER,
since they don’t have fully developed liver they don’t have the capability to collect the
unneeded BILIRUBIN, which then causes the yellowing of the skin of the new born / infant
(JAUNDICE)
Yellowing of the skin, sclera and mucous membranes
Occurs at 3rd – 4th day of life – normal
Reaches its maximal intensity (3-6 days)
Subside (10 days – 2 weeks)
Jaundice occurring in the first 24 hours of life is abnormal –
PALPATION
Temperature
The skin should be warm (to touch) and the temperature should be equal bilaterally
Hypothermia
-
Generalized or localized coolness
May cause immobilized extremity
Happens when limb is in cast
Hyperthermia
-
High temperature
When you have; fever, infection, trauma
-
Skin Turgor
Ability of the skin to change shape and return to normal after pinching (turgor)
A sign commonly used by health workers to assess fluid loss of dehydration
29 | H e a l t h a s s e s s m e n t
Edema
-
Swelling
abnormal accumulation of fluid in certain tissues within the body
Edema happens when your small blood vessels leak fluid into nearby tissues
INSPECTION | PALPATION
Lesions
-
Uses inspection and palpations to describe skin lesions;
Colour, elevation, size, location
Pedunculated Lesions
-
small wound that have its own blood vessels
Shape or Pattern
Annular Lesions
-
The term “annular” stems from the Latin word “annulus,” meaning ringed
The lesions appear as circular or ovoid macules or patches with an erythematous periphery
and central clearing.
30 | H e a l t h a s s e s s m e n t
Confluent Lesions
Linear Lesions
-
Size
Size in centimetres : use ruler to measure
-
Location and Distribution
Any exudate – note any color
Palpate lesions
Gently scrape a scale to see if it comes off, or if it bleeds when the scale comes off
Do the lesions blanching
**Tumbler Test
-
Used to check if the lesion is pressed a glass and non-blanchable it could be; Erythema, herpes
zoster, etc.
Herpes Zoster or Shingles – highly infectious
31 | H e a l t h a s s e s s m e n t
Macule
-
Flat, cannot be palpated, skin colour may change (brown, white, tan, purple, red)
Note the colour
Less than 1cm with circumscribed border
-
Bigger than macule
More than 1cm and may have an irregular border
Freckles, flat moles, petechiae, rubella, vitiligo
-
Small, containing solid mass, elevated
Have circumscribed border and are less than 0.5cm
-
Small flat (small little deviation)
Coming together
-
Small red spots - are tiny, circular, non-raised patches that appear on the skin or in a mucous
or serous membrane.
They occur as the result of bleeding under the skin
-
Ex. Meningitis, snake bites
Purplish spots
Patches
Papule
Plaque
Petechiae
Purpura
Ecchymosis
-
Hemorraghic blotching due to pooling of blood under the skin or mucous membrane
Comedone
-
Increased in sebaceous gland activity, creates increase oiliness
Common skin problem of adolescence (7-8)
Peak (14-16 in girls, 16-19 in boys)
-
Puss-filled vesicle or bulla
Pustule
Wheals/Hives
-
Ex. Allergies, urticarial, insect bites
Elevated mass with transient borders that is often irregular
Size and color vary
-
Characterized by elevated lesions caused by local edema
Urticarial
Acrochordons
32 | H e a l t h a s s e s s m e n t
-
Skin tags
Common in areas where there is skin friction
Neck, axilla cheeks and trunk
-
They feel like large peas under the surface of the skin.
-
extremely common as people get older
Some common benign tumors include: Warts (skin tumor resulting from a virus) Seborrheic
keratoses (growths on the skin ranging from light skin color to dark brown)
-
small, fluid-filled sacs that can appear on your skin
The fluid inside these vesicles may be clear, white, yellow, or mixed with blood
-
fluid-filled sac or lesion that appears when fluid is trapped under a thin layer of your skin
It's a type of blister
-
Cysts are noncancerous, closed pockets of tissue that can be filled with fluid, pus, or other
material.
can develop as a result of infection, clogging of sebaceous glands (oil glands), or around
foreign bodies, such as earrings
Nodule
Tumour
Vesicles
Bulla
Cyst
-
Cherry Angioma
-
Hair
-
Red moles
They're usually found on people aged 30 and older
The collection of small blood vessels inside a cherry angioma give them a reddish appearance
Color – texture (fine, straight, curly, kinky)
In young, should be shiny
Oiliness is natural (not excessive)
Note for any scalp lesions;
Lice, loss of hair (alopecia)- autoimmune disease
33 | H e a l t h a s s e s s m e n t
Nails
-
Inspect and palpate the nails
Blanching
Shape
Curvature (Convex, 160 c)
ADULT/AGED
-
drier skin and less perspiration
thinning and nuttering epidermis
risk for injury
greying of hair
nail growth slows down
the toenails; thicker, hard, brittle and yellowing appearance
ASSESSING THE HEART AND NECK VESSELS
-
When beginning the examination, the ideal location to stand is on the right side
INSPECTION
-
General Appearance
Skin Colour
Skin; warm to touch
Homogenous in colouring
Without significant moisture
34 | H e a l t h a s s e s s m e n t
-
-
-
Capillary Refill
The capillary nail refill test is a quick test done on the nail beds. It is used to monitor dehydration and
the amount of blood flow to tissue.
Heaves or Lifts
A parasternal heave (or lift) is a precordial impulse that may be felt (palpated) in patients with cardiac
or respiratory disease. Precordial impulses are visible or palpable pulsations of the chest wall, which
originate on the heart or the great vessels.
Pulsations (apical) – left ventricle on the 5th ICS, left MCL
Jugular Venous Pulsation / Distention
< is connected to superior vena cava
**NVE – Neck Vein Engorgement
Deviations
Skin Pallor & Cyanosis
-
May suggest poor tissue perfusion
Skin Diaphoresis
-
May result from SNS stimulation as a result of diminished cardiac output
Cyanosis
-
Best seen in the lips, earlobes, mucous membranes, or where the skin is thin
Hands and Fingernails
-
-
Schamroth’s Test
Detects fingers clubbing
Normal: small diamond-shaped “window” is typically apparent between the nail beds
Deviation: increased convexity
< loss of normal – 165 degrees between the nail bed and cuticle
< may indicate endocarditis or a classic indicator of Cyanotic Congenital Heart Disease (CCHD)
<< CCHD – cardiac malformations that commonly affect the atrial or ventricular walls, heart valves,
or large blood vessels
<< Endocarditis – inflammation of the heart’s inner lining (endocardium)
< TB, Chronic Hypoxia, Liver Cirrhosis, IBD
Anterior Chest
For visible pulsations or movements
Apical impulse / apex beat / Point of Maximal Impulse (PMI)
< Location: 5th ICS, left MCL
Generally not observed in healthy individuals (unless the patient is thin)
35 | H e a l t h a s s e s s m e n t
-
-
Internal Jugular Vein & External Jugular Vein
IJV_bigger_anteriori EJV_posterior
Normal: pressure on the left side of the heart is always higher than the right
Deviation: Jugular Vein Distention (JVD)
< occurs when the pressure inside the vena cava increases and appears as a bulge down the right
side of a person’s neck
< sign of increases Central Venous Pressure (CVP)
<< CVP – measurement of the pressure inside the vena cava
Indicates how much blood is flowing back into your heart and how well your heart can move that
blood into your lungs and the rest of your body
Occurs when CVP increases above a normal/healthy level
Can be caused by Right-sided heart failure
<often occurs due to left-sided heart failure, when the weakened and/or stiff left ventricle loses power
to efficiently pump blood to the rest of the body. As a result, fluid is forced back through the lungs,
weakening the heart's right side, causing right-sided heart failure
(READ MORE) LINK: https://www.healthline.com/health/jvd
-
JUGULAR VEIN ASSESSMENT
1. Examine position
Head of bed elevated at 45 degree angle
Head turned to right
-
2. Identify top of venous pulsation in neck (JVP)
Jugular Venous Pulsations are inward
Contrast with outward Carotid Artery pulsations
-
3. Identify the sternal angle (Angle of Louis)
Located at superior edge or notch of Sternum
-
4. Measure distance between top of pulsation and Sternum
Measured in centimetres
PRECORDIUM
-
Book – anterior chest area that overlies the heart and great vessels
The region or the thorax immediately in front of the heart
Front of the chest wall over the heart
36 | H e a l t h a s s e s s m e n t
PALPATION
-
Patient should be in supine position
Be on his/her right side to gain easy access to the apex of the precordium
Pulsation
Heaves
Thrills
Displacement of the apex beat is often associated with ventricular enlargement / cardiomegaly
< abnormal enlargement of the heart
THRILLS
Palpable murmurs – vibratory sensations
Felt from light palpation over the chest wall
Deviation: loud heart murmur – caused by an incompetent heart valve
LIFTS
A slight movement
HEAVES
More vigorous movement
Sustained forceful thrusting of the ventricle during systole
Palpable lifting sensation under the sternum and anterior chest left sternal border suggest a central
precordial heave associated with RVH
< Right Ventricular Hypertrophy – affecting right ventricle – right side of the heart is enlarged
Caused by either congenital heart conditions or high blood pressure in the lungs / pulmonary
hypertension
****MUST TO KNOW****
Left Lateral Decubitus Position (LLDP)
-
Patient is lying on his/her left side
To bring the heart (nearer) to the chest wall to listen/feel for the sounds/vibrations better
Tissue Perfusion
-
Flow of blood
**a parasternal heave or lift is a precordial impulse that may be felt (palpated) in patients with cardiac or
respiratory disease
**Precordial impulse are visible or palpable pulsations of the chest wall, which originate on the heart or the
great vessel
2nd Part Palpations
-
Peripheral Pulses – rate, rhythm, quality
Thrills, Heaves, Lifts
Apex Beat (PMI) – Point of Maximal Impulse
Aortic Pulsation
< Deviation: 6th ICS – Posterior Axillary Line
< Runs from the heart, down to the centre of the chest, and into the abdomen
37 | H e a l t h a s s e s s m e n t
Abdominal Aortic Aneurism (AAA)
< occurs in the part of the abdomen
< Thoracic Aortic Aneurism – occur in the part of the aorta located in the chest area
-
-
-
Capillary Refill Time (CRT)
Refers to the amount of time it takes for capillary circulation to return to the fingertips after capillary
circulation is obliterated
A common indicator of peripheral tissue perfusion
Normal: less than 3 seconds / position above heart level / pinch/blanch finger nails, in older adults –
it can be longer than 3 seconds, in neonates – pressure is exerted in the sternum for 5 seconds
SIGNIFICANCE
Prolonged CRT is suggestive of hypoperfusion and/or dehydration
< decreased blood flow through an organ cerebral hypoperfusion
(may cause pallor?)
In adults prolonged CRT is also suggestive to CHF and/or PVD
< CHF Congestive Heart Failure – failure of heart to pump blood with normal efficiency
Heart is unable to provide adequate blood flow to other organs, such as the brain, liver, and kidneys
< PVD Peripheral Vascular Disease – blood circulation disorder that causes the blood vessles outside
the heart to narrow, block, or spasm
< Peripheral Artery Disease (PAD) – common cause ATHEROSCLEROSIS
<< gradual process in which a fatty material builds up inside the arteries
Less common cause: blood clots, injury to the limbs
PERCUSSION
-
To estimate heart size
AUSCULTATION
-
Blood Pressure
Carotid Bruit
Heart Sounds
Normal: no sound should be heard
Essential that auscultation of heart sounds be done in a quiet environment as possible
Avoid a cold stethoscope on an exposed skin
-
Auscultate the CAROTID ARTERY for the presence of bruit
< supplies the brain with blood
<< RIGHT COMMON CAROTID ARTERY – originates from brachiocephalic trunk the left from the aortic
arch in the thorax
Presence of bruit indicates atherosclerosis plaque, build up on the interior lumen
-
38 | H e a l t h a s s e s s m e n t
< means a clogged/plagued/ presence of clotted blood
<< Thrombus – causes stroke, clogged artery/vein
<< Embolus – the clotted blood travels through the blood vessels
There would be a presence of a bruit sound when there is/are – fats, blood clot
PENUMBRA - Occlusion of the MCA with irreversibly affected or dead tissue in black and tissue at
risk or penumbra in red.
CARDIAC OUTPUT
-
Amount of blood ejected by the heart in 1 minute
5-8 litres per minute
20% of the blood goes to the brain
STROKE VOLUME
-
Amount of blood ejected by the valves/heart per contraction
FORMULA:
CO = SV x HR/PR
SV – constant: 70cc
CONDUCTION SYSTEM OF THE HEART
Step 1: Pacemaker Impulse Generation
The first step of cardiac conduction is impulse generation. The sinoatrial (SA) node (also referred to as the
pacemaker of the heart) contracts, generating nerve impulses that travel throughout the heart wall. This
causes both atria to contract. The SA node is located in the upper wall of the right atrium. It is composed of
nodal tissue that has characteristics of both muscle and nervous tissue.
Step 2: AV Node Impulse Conduction
The atrioventricular (AV) node lies on the right side of the partition that divides the atria, near the bottom of
the right atrium. When the impulses from the SA node reach the AV node, they are delayed for about a tenth
of a second. This delay allows atria to contract and empty their contents into the ventricles prior to ventricle
contraction.
Step 3: AV Bundle Impulse Conduction
The impulses are then sent down the atrioventricular bundle. This bundle of fibers branches off into two bundles
and the impulses are carried down the center of the heart to the left and right ventricles.
Step 4: Purkinje Fibres Impulse Conduction
39 | H e a l t h a s s e s s m e n t
At the base of the heart, the atrioventricular bundles start to divide further into Purkinje fibers. When the
impulses reach these fibers they trigger the muscle fibers in the ventricles to contract. The right ventricle sends
blood to the lungs via the pulmonary artery. The left ventricle pumps blood to the aorta.
Cardiac Conduction and the Cardiac Cycle
Cardiac conduction is the driving force behind the cardiac cycle. This cycle is the sequence of events that
occur when the heart beats. During the diastole phase of the cardiac cycle, the atria and ventricles are
relaxed and blood flows into the atria and ventricles. In the systole phase, the ventricles contract sending
blood to the rest of the body.
Cardiac Conduction System Disorders
Disorders of the heart's conduction system can cause problems with the heart's ability to function effectively.
These problems are typically the result of a blockage that diminishes the rate of speed at which impulses are
conducted. Should this blockage occur in one of the two atrioventricular bundle branches that lead to the
ventricles, one ventricle may contract more slowly than the other. Individuals with bundle branch block
typically don't experience any symptoms, but this issue can be detected with an electrocardiogram (ECG).
A more serious condition, known as heart block, involves the impairment or blockage of electrical signal
transmissions between the heart's atria and ventricles. Heart block electrical disorders range from first to third
degree and are accompanied by symptoms ranging from light-headedness and dizziness to palpitations and
irregular heartbeats.
DIASTOLE s2
During ventricular diastole, the AV valves are open and the ventricles are relaxed. This causes
higher pressure in the atria than in the ventricles. Therefore, blood rushes through the atria into the
ventricles. This early, rapid, passive filling is called early or protodiastolic filling. This is followed by a
period of slow passive filing. Finally, near the end of ventricular diastole, the atria contract and
complete emptying blood out of the upper chambers by propelling it into the ventricles. This final
active filling phase is called preystole, atrial systole, or sometimes the “atrial kick”. This action raises
left ventricular pressure.
SYSTOLE s1
The filling phases during diastole result in large amount of blood in the ventricles, causing the
pressure in the ventricles to be higher than in the atria. This causes the AV valves (mitral and
tricuspid) to shut. Closure of the AV valves produces the first heart sound (s1), which is the
beginning of systole. This valve closure also prevents blood from flowing backward (a process
known as regurgitation) in the atria during ventricular contraction. At this point in systole, all four
valves are closed and the ventricles contract (isometric contraction). There is now high pressure
inside the ventricles, causing the aortic valve to open on the right side of the heart. Blood is ejected
rapidly through these valves. With ventricular emptying the ventricular pressure falls and the
semilunar valves close. This closure produces the second heart sound (s2), which signals the end
of systole. After closure of the semilunar valves, the ventricles relax. Atrial pressure is now higher
than the ventricular pressure, causing the AV valves to open and diastolic filling to begin again.
ABNORMAL HEART SOUND s3
Normally diastole is silent
DEVIATION: when ventricular filling creates vibration \
40 | H e a l t h a s s e s s m e n t
-
Resistant to filling during the early rapid filling phase
Occurs immediately after s2
Low pitched, quiet sound – difficult to hear
Cause: Myocardium is RIGID
When present in adults, s3 is considered pathological indicating decreased ventricular
compliance
May be produced by either the right or left side of the heart and is often initial of heart failure
ANATOMY OF RESPIRATORY SYSTEM
LUNGS
Have a lower and upper compartment
3 lobes on the right, 2 lobes in the left
Diaphragm
Major muscle for respiration
Separates the thoracic from the abdominal region
INHALATION – down
EXHALATION – up
Rests on the lobe of the liver
-
UPPER RESPIRATORY
o Passageway for respiration
o Moistens incoming air
o Receptors for smell
Nose
Nasopharynx
Oropharynx
Laryngopharynx
Larynx (voice box)
41 | H e a l t h a s s e s s m e n t
NOSTRILS
Filters the air we breathe and the debris from the air
NASAL CAVITY
-
The nasal cavity is a hollow space within the nose and skull that is lined with hairs and mucus
membrane.
The function of the nasal cavity is to warm, moisturize, and filter air entering the body before it
reaches the lungs.
TURBINATE
-
o
o
o
These structures are responsible for warming, humidifying, and filtering the air we
breathe.
Normally there are three turbinates including the superior (upper), middle, and inferior
(lower) turbinates.
Pulmonary Ventilation
Internal and External Respiration
Cleanse the airs, warms the air, moisture
PHARYNX
o Is also called the throat.
o Is the passageway for both air and food and forms a resonating chamber for speech sounds
o It serves as both a connection between the mouth and the digestive tract and as a
connection between the nose and respiratory system.
o It is divided into three portions:
o Nasopharynx – It has 4 openings in its walls: the 2 internal nares and 2 openings that lead to
the auditory or Eustachian tubes.
o Oropharynx – It has only 1 opening called Fauces which connects to the mouth; It is a common
passageway for both food and air.
o Laryngopharynx/Hypopharynx
–
Connects
with
the
esophagus
posteriorly and with the larynx anteriorly.
LARYNX
o Is also called the Voice box.
o It connects the pharynx to the trachea.
o Thyroid
Cartilage
–
It
is
the
largest
piece
in
the
larynx.
also known as the Adam’s apple which is larger in males than in females.
o Epiglottis – Allows food to go down to the oesophagus; It closes the trachea.
o Vestibular Folds/ False Vocal Cords.
o Vocal Folds/ True Vocal Cords.
EPIGLOTTIS
SUPRAEPIGLOTTIS – GLOTTIS (VOCAL CHORDS) – SUBGLOTTIS
Closes the trachea for the food and water to enter the oesophagus
TRACHEA
It
is
42 | H e a l t h a s s e s s m e n t
o
o
o
Is also referred to as the windpipe.
It is the passageway for air.
Goblet Cells – Produces mucus and the Ciliated Cells provide the same protection against
dust particles.
ANATOMY OF THE LUNGS
o PLEURAL MEMBRANE – It encloses and protects each lung.
o PARIETAL PLEURA – It is the outer layer that attaches the lung to the wall of the thoracic
cavity.
o VISCERAL PLEURA – It is the inner layer which covers the lungs.
o PLEURAL CAVITY – Is the space between the parietal and visceral pleura which contains
pleural cavity.
o PLEURAL CAVITY – It is a pleural fluid that prevents friction between the two membranes and
allows them to slide past each other during breathing, as the lungs and thorax change
shape.
THE BRONCHI AND THE BRONCHIAL TREE
BRONCHI
1.
o
o
Passageway of air
Has goblet cells that produce mucus
Contains mucus that traps foreign bodies
The trachea terminates in the chest by dividing into a:
Right Primary Bronchus – Goes to the right lung.
Left Primary Bronchus – Goes to the left lung.
2. On entering the lungs, the primary bronchi divide to form smaller bronchi called the:
o Secondary or Lobar Bronchi – The right lung has 3 lobes and the left lung has 2 lobes.
3. The secondary bronchi continue to branch forming even smaller bronchi called:
o Tertiary or Segmental Bronchi
4. And tertiary bronchi divide into smaller branches called:
o Bronchioles
43 | H e a l t h a s s e s s m e n t
5. Bronchioles finally branch into smaller tubes called:
o Terminal Bronchioles
THE ALVEOLI
The actual exchange of respiratory gases between the lungs and the blood occurs by
diffusion across the ALVEOLI and the walls of the capillary network that surrounds it.
ALVEOLAR-CAPILLARY MEMBRANE – The membrane through which the respiratory gases move.
-
The blood–air barrier in the gas exchanging region of the lungs. It exists to prevent air bubbles from
forming in the blood, and from blood entering the alveoli.
SURFACTANT
o Is a fluid that coats the surface of the membrane inside each alveolus.
o It helps reduce surface tension (the force of attraction between water molecules) of the fluid.
o Breaks the bond of water molecules
o Helps prevent alveoli from collapsing or sticking shut as air moves in and out during breathing.
o It is produced by Alveolar Type 2 Cells.
o During inspiration, when alveoli expand, the molecules move apart.
o During expiration when lungs shortened, molecules move together and become
concentrated thus surface tension is reduced.
RESPIRATION PROCESS
Carbon Dioxide
-
Product of metabolism
Metabolism – use of carbohydrates, proteins, glucose, etc. of the body
RBC carries the OXYGEN and CARBON DIOXIDE and brings it to the lungs
Breathing In (Inhalation)
a.
b.
c.
d.
e.
When you breathe in, or inhale, your diaphragm contracts (tightens) and moves downward. This
increases the space in your chest cavity, into which your lungs expand. The intercostal muscles
between your ribs also help enlarge the chest cavity. They contract to pull your rib cage both upward
and outward when you inhale.
As your lungs expand, air is sucked in through your nose or mouth. The air travels down your windpipe
and into your lungs. After passing through your bronchial tubes, the air finally reaches and enters the
alveoli (air sacs).
Through the very thin walls of the alveoli, oxygen from the air passes to the surrounding capillaries (blood
vessels). A red blood cell protein called hemoglobin (HEE-muh-glow-bin) helps move oxygen from the
air sacs to the blood.
At the same time, carbon dioxide moves from the capillaries into the air sacs. The gas has traveled in
the bloodstream from the right side of the heart through the pulmonary artery.
Oxygen-rich blood from the lungs is carried through a network of capillaries to the pulmonary vein. This
vein delivers the oxygen-rich blood to the left side of the heart. The left side of the heart pumps the
blood to the rest of the body. There, the oxygen in the blood moves from blood vessels into surrounding
tissues.
44 | H e a l t h a s s e s s m e n t
Breathing Out (Exhalation)
A. When you breathe out, or exhale, your diaphragm relaxes and moves upward into the chest cavity.
The intercostal muscles between the ribs also relax to reduce the space in the chest cavity.
B. As the space in the chest cavity gets smaller, air rich in carbon dioxide is forced out of your lungs and
windpipe, and then out of your nose or mouth.
ASSESSING THE LUNGS AND THORAX
ASSESS
SHAPE AND CONFIGURATION
-
Thorax is oval, its AP Diameter is half its transverse diameter
FACIAL EXPRESSION
-
Should be relaxed
LEVEL OF CONSCIOUSNESS
-
Should be alert and cooperative
Brain cells are affected by lack of oxygen
SKIN COLOR AND CONDITION
-
Lips and nail beds are free from pallor and cyanosis
QUALITY OF RESPIRATION
-
Automatic, effortless, regular and even, produces no noise
Chest expands symmetrically
INSPECT
COLOR
-
Lesions (scars, stretch marks), use of accessory muscle, over prominence of the ribs (
may indicate respiratory problems)
-
Nares
Bulges
Asymmetry
SYMMETRY
AP DIAMETER and TRANSVERSE DIAMETER
45 | H e a l t h a s s e s s m e n t
-
Anterioposterior Diameter – side
Should be half the size of the transverse diameter
The anteroposterior diameter should be less than the transverse diameter. The ratio of
anteroposterior to transverse diameter is from 1:2 to 5:7. AP = transverse diameter, or
“barrel chest.” Ribs are horizontal, chest appears as if held in continuous inspiration.
-
AP Diameter is more than half the transverse
AGED
TAKE THE RESPIRATORY RATE
-
NORMAL – 12-20 RR ADULT | 30-60 RR INFANT
SPINAL ALIGNMENT
-
Impedes the space of the lung/s
Kyphosis - is an abnormally excessive convex curvature of the spine as it occurs in the
thoracic and sacral regions – KUBA
Lordosis - is defined as an excessive inward curve of the spine, It differs from the spine's
normal curves at the cervical, thoracic, and lumbar regions, which are, to a degree,
either kyphotic (near the neck) or lordotic (closer to the low back) – LIYAD
Scoliosis - is a medical condition in which a person's spine has a sideways curve. The
curve is usually "S"- or "C"-shaped
PALPATE
-
Warm your hands before palpating or percussing
When palpating and percussing ask the patient to cross arms and bow head, to see
the spinal column better
No tenderness, masses, bulges, pulsation
LANDMARKS
Anterior Axillary Line
Midclavicular Line
Midsternal Line
46 | H e a l t h a s s e s s m e n t
Accessory Muscles
-
Trapezius
Scalene Muscle
Respiratory Excursion
-
Thumbs on the xiphoid process and fingers on the 10th ribs
Exhale and inhale – distance between the thumbs should be (5 – 10 cm)
If obese – pinch the skin
-
vibratory tremors that can be felt through the chest by palpation
ask the patient to say “99”, “blue moon”, “tres, tres”
palpated using the balls of hand or the ulnar side of the hand
PLEURAL EFFUSION
accumulation of water in the pleural cavity between visceral pleura and parietal
pleura
Fremitus
-
Diaphragmatic Excursion
-
movement of the thoracic diaphragm during breathing
3 – 5 cm distance
Checking the diaphragm muscle
Measuring the contraction of the muscle
Resonance and dullness
DEVIATIONS
ATELECTASIS
-
Collapsed lungs or closure of a lung resulting in reduced or absent gas exchange.
It may affect part or all of a lung.
47 | H e a l t h a s s e s s m e n t
-
It is usually unilateral. It is a condition where the alveoli are deflated down to little or no
volume, as distinct from pulmonary consolidation, in which they are filled with liquid.
-
Swelling (inflammation) of the tissue in one or both lungs. It's usually caused by a
bacterial infection. At the end of the breathing tubes in your lungs
PNEUMONIA
POSTOPERATIVE GUARDING
-
shallow breathing due to pain
-
Difficulty and noisy breathing
Increased RR
Use of accessory muscle
Nasal Flaring
PECTUS CARINATUM
-
Pigeon chest
breastbone protrudes outward abnormally
PECTUS EXCAVATUM
-
funnel chest
sternum and rib cage are shaped abnormally
these can be familial
most common in boys than girls
interferes with the functions of the lungs
-
is normal with infants
deviations in adult
MAIN CAUSE: SMOKING
Too much accumulation of air
COPD
Pneumothorax – not with barrel chest
EMPHYSEMA – Alveoli is destroyed
Barrel Chest
Accessory Muscles
-
Trapezius
Scalene
Sternocleidomastoid
-
Note any tenderness, superficial lumps or masses
Note skin mobility and turgor, temperature and moisture
PERCUSSION
48 | H e a l t h a s s e s s m e n t
o
o
o
o
o
intercostal spaces
liver located at the 5th rib to 10th rib
intercostal margin
Resonance – presence of air
Hyperesonance – too
Dull – organ (Liver – right, Heart – middle)
Tympanitic - stomach
Flat – bones
Common Characteristics of New Born
-
Nose breather
30-53 or 40-60 breathes per minute
Irregular breathing
-
THORAX – rounded, diameter from the front is equal, barrel chest
AP Diameter is equal to the transverse diameter
30 – 36 cm is the newborn chest, 2 cm smaller that the head circumference
Ribs and xiphoid process are prominent
Chest wall is thin
85% water
6 years old, AP Diameter has decreased in proportion to the Transverse Diameter 1:2
ratio
Tend to breathe normally as with the adult
BREATH SOUNDS
49 | H e a l t h a s s e s s m e n t
-
BRONCHIAL
BRONCHOVESICULAR
VESICULAR
AUSCULTATION
Using a stethoscope, the doctor may hear normal breathing sounds, decreased or absent breath sounds,
and abnormal breath sounds.
Absent or decreased sounds can mean:
Air or fluid in or around the lungs (such as pneumonia, heart failure, and pleural effusion)
Increased thickness of the chest wall
Over-inflation of a part of the lungs (emphysema can cause this)
Reduced airflow to part of the lungs
There are several types of abnormal breath sounds. The 4 most common are:
Rales. Small clicking, bubbling, or rattling sounds in the lungs. They are heard when a person breathes in
(inhales). They are believed to occur when air opens closed air spaces. Rales can be further described as
moist, dry, fine, and coarse.
Rhonchi. Sounds that resemble snoring. They occur when air is blocked or air flow becomes rough through
the large airways.
50 | H e a l t h a s s e s s m e n t
Stridor. Wheeze-like sound heard when a person breathes. Usually it is due to a blockage of airflow in the
windpipe (trachea) or in the back of the throat.
Wheezing. High-pitched sounds produced by narrowed airways. Wheezing and other abnormal sounds can
sometimes be heard without a stethoscope.
ALVEOLAR HYPOXIA
-
Less oxygen in lungs
-
Surround the airways in wheezing
-
Prone to kyphosis – because of osteoporosis and changes in cartilage
Respiratory muscle strength declines after age 50 and continues to decrease into the
70s
Small airways, lose their cartilaginous support and elastic recoil; as a result, they tend
to close, particularly in basal or dependent portions of the lungs
CILIA in the airways decreases in number and are less effective in removing mucus
Greater risk for pulmonary infections
Smooth Muscles
AGED
-
ASSESSING THE NOSE AND MOUTH
NOSE
-
Centre of the face
The colour should be consistent with the face
51 | H e a l t h a s s e s s m e n t
-
Has plenty of arteries
Nasal Septum – should be in the midline
BREATHING
-
Infants are nose breathers
Audible effort to breathe
Inability to such is an indicator of obstruction
NASAL CAVITY
-
Moist
Dark pink
Turbinate
-
Pulmonary ventilation
Cleanse the air, warms the air, moisture
Inferior and middle turbinate should be the same colour in the surrounding area
Sinuses
-
Produce mucus to moisturize the inside of the nose
Protects from pollutants, microorganisms
Allow for voice resonance
Adds moisture to any air that is inhaled
Mucous
-
Traps foreign bodies
Humidifies the air we breathe
DEVIATIONS
Nasal Flaring
-
indicates difficulty in breathing, commonly seen in children and infants (normal)
Epistaxis
-
nose bleed
Dyspnoea
-
difficulty in breathing
52 | H e a l t h a s s e s s m e n t
Dysphagia
-
difficulty in swallowing
MOUTH
Tongue
-
light pink with light coating, smooth and moist
rough surface due to presence of papillae
moves the food
identify the object in the mouth
should protrude midline, if not there can be weakness or paralysis
NORMAL – light pink with light coating, no cracks, ulcers, or teeth marks
surface: rough (presence of papillae), smooth and moist, surrounded by anterior and lateral teeth
ABNORMAL – pallor, cyanosis, redness
VENTRAL TONGUE – should glisten – and a network of small vessel
Frenulum
-
Is midline,
Should allow tongue to reach the roof of the mouth
Uvula
-
Midline, in between the tonsils
Cone shaped
Large amounts of thin saliva produced by the uvula serves to keep the throat well lubricated
Functions in speech as well
Should lean towards the area with deviation
Soft Palate
-
Soft palate and uvula Move together to close off the nasopharynx and prevent food from entering
the nasal cavity
NORMAL - Smooth, mobile
Pharynx
-
Fluid and food passageway
Epiglottis
53 | H e a l t h a s s e s s m e n t
-
A flap in the throat that keeps food from entering the windpipe and the lungs
Buccal Mucosa
-
NORMAL – Pink and moist
inside lining of the cheeks and floor of the mouth and is part of the lining mucosa
DEVIATIONS
Exudative Tonsillitis
-
accumulation of pus between the tonsil and its capsule
Ankyloglossia
-
Tongue-tie
congenital oral anomaly that may decrease mobility of the tongue tip and is caused by an unusually
short, thick lingual frenulum
may interfere with breast feeding in infants
Oral Leukoplakia
-
HIV positive patient
Fungus
Pernicious Anaemia
-
a condition in which the body can't make enough healthy red blood cells because it doesn't have
enough vitamin B12
caused by autoimmune destruction of gastric parietal cells
The appearance of the tongue in vitamin B12 deficiency is described as "beefy" or "fiery red and sore"
Macrocytic – vitamin B-12 and folate deficiencies can be treated and cured with diet and
supplements
Microcytic –
White Coating
-
Dehydration or poor hygiene, bad oral care
Common with patients in the ICU
Yellowing of tongue
-
Liver or gallbladder problems
Digestive system disorder
Vagus Paralysis
-
Failure of the soft palate to rise symmetrically
Uvula will deviate towards the affected side
PARESIS
-
Weakness
PLEGIA
-
Paralysis of the nerve or muscle
54 | H e a l t h a s s e s s m e n t
ASSESSMENT
-
Elevation of the soft palate
When you say ‘ah’ the movement of the soft palate upwards
PALPATION
Gums, Teeth, Tongue
-
Should feel firm, no soft areas, no tenderness
LIPS
Mentolabial Suculus
-
Is a permanent crease between the inner lip and the chin, which plays a significant role in movement
of the lower lip and in facial
NORMAL – vertically and horizontally symmetrical, both are at rest and with movement
Vermillion Border
-
Should be well defined without any evidence of cracking, swelling, and lesions
INSPECTION
-
Lips should be – PINK to RED
Vertically and horizontally symmetrical
DEVIATIONS
Chapped Lips
55 | H e a l t h a s s e s s m e n t
-
Bad oral hygiene
Dehydration
Pale Lips
-
Anemia
Dehydration
Dry, Craked Lips
-
Dehydration
Overexposure to cold temperature
Cold Sores
-
STD
Herpes simplex
Syphilis
Cheilosis | Cheilitis
-
Scaling, painful fissures
painful inflammation and cracking of the corners of the mouth
sometimes occurs on only one side of the mouth, but usually involves both sides
Vitamin B12 deficiency
Aphthous Stomatitis
-
benign and non-contagious mouth ulcers
Oral Cancer
-
which includes cancers of the lips, tongue, cheeks, floor of the mouth, hard and soft palate, sinuses,
and pharynx (throat), can be life threatening if not diagnosed and treated early
White Patches – Leukoplakia
Red/White Patches – Erythroleukoplakia
Red Patches – Erthryplakia
Addison’s Disease
-
Hormonal Imbalance
Halitosis
-
Bad breath
Xerostomia
-
dry mouth resulting from reduced or absent saliva flow
decrease in saliva production occurs with age, the gums may get thinner and begin to recede
TEETH
56 | H e a l t h a s s e s s m e n t
-
good oral care will increase, production of saliva, contains antibodies, kills the bacteria in the mouth
and cleanses the mouth
Front teeth – pointed and sharp, for biting and tearing
Back Teeth – flat, for crushing and grinding
Children - Infant
Deciduous Teeth
-
begin to erupt by 6 months
by 2 years all 20 teeth should be present
begins to be lost around 6 years of age
by ages 14-15 they are replaced with 32 permanent teeth (same as with the adults)
TETRACYCLINE and DOXYCYLINE
-
should not be administered with children below 8 years old
cause tooth discoloration in the infant by affecting enamel development
-
AGED
Decrease in saliva production occurs with age, causes (XEROSTOMIA)
Tooth Enamel
-
tends to weak away with aging, making the teeth vulnerable to damage and decay
DEVIATIONS
Cavities
-
Poor oral hygiene
Bottled water does not have fluoride added so the individual may be missing
GUMS
-
NORMAL – healthy gums are pink in colour, firm, margins of the gums should be tight and well defined
NOT NORAML – red, swollen and have tendency to bleed or even have pus
most fragile part of the body
Gingival Hyperplasia
-
Swollen gums, oedematous
57 | H e a l t h a s s e s s m e n t
-
Sodium Dilantin (medication given to patients with seizure) – may cause this deviation – side effect
Gingivitis
-
Red and puffy gums that bleeds easily
Common type of periodontal disease
Often resolves with oral hygiene
Malocclusion
-
Affect the chewing efficiency as well as the choice of foods
This has potential to result in malnutrition and gastric alterations
-
OLDER ADULTS
Nasal hair becomes coarser, stiffer and more visible
Air filtration may not be as effective
Reduction in the sense of smell, reduction of olfactory nerve fibres
Loss of sense of taste due to loss of papillae
Reduction of saliva
Gradual loss of teeth, drift causing malocclusion, affects the chewing efficiency and choice of foods
-
ASSESSING THE PERIPHERAL VASCULAR SYSTEM
HEMOGLOBIN in RBC brings oxygen
Ischemia
an inadequate blood supply to an organ or part of the body, especially the heart muscles
Albumin
Responsible for maintaining the osmotic pressure
helps keep fluid in your bloodstream so it doesn't leak into other tissues
also carries various substances throughout your body, including hormones, vitamins, and enzymes
MADE BY THE LIVER
Diffusion
Movement of solute, or particles from a greater to lower concentrated solution
Osmosis
Movement of water molecules from lesser to greater concentrated solution
Oedema
There is inflammation
Increased capillary permeability
Capillary membrane
are very thin blood vessels
They bring nutrients and oxygen to tissues and remove waste products
They have thin walls/single layer – so that exchange of substances will be easy (oxygen,
electrolytes, nutrients)
58 | H e a l t h a s s e s s m e n t
5 CARDINALS OF MANIFESTATION
1. REDNESS
2. PAIN
3. WARM TO TOUCH
4. LOSS OF FUNCTION
5. OEDEMA/SWELLING
>> If there is a tissue injury caused by an inflammation (cut, fall, trauma, incision, injury) – SNS will be stimulated
– it will stimulate adrenal glands in the adrenal medulla to release CATECOLOMINES – EPINEPHRINE (increases
Cardiac Rate – more than 100) and NOREPINEPHRINE (increase Blood Pressure 120/80 – arteries constrict)
CHEMICAL MEDIATORS will be released due to tissue injury;
CHEMICAL MEDIATORS
-
Will be released if there is tissue injury
-
Increases capillary permeability
Pores in the capillary membrane becomes bigger;
Intravascular space decreases, Albumin goes out, there will be swelling/oedema because the
water comes out to the interstitial space/third space from the intravascular space.
Histamine – (more) When we come into contact with an allergen, such as pollen or animal dander,
histamine is released by the body to the site of contact | vasodilator
Brings more blood to the injured site which causes the skin to be warm to touch | causes
redness/rubor
Injured site such as; surgery, appendectomy, incision
Bradykinin - an inflammatory mediator | a peptide that causes blood vessels to dilate (enlarge), and
therefore causes blood pressure to fall
Prostaglandin – one of the more potent mediators that cause increased blood flow, chemotaxis
(chemical signals that summon white blood cells), and subsequent dysfunction of tissues and organs
Serotonin - increases vascular permeability, dilates capillaries, and causes contraction of nonvascular
smooth muscle
{VEINS: clotted blood – gives redness in colour – warm to touch}
59 | H e a l t h a s s e s s m e n t
{ARTERY: lipids – gives pallor in colour – cold to touch}
WALLS OF THE BLOOD VESSELS
1. Tunica Adventitia
2. Tunica Media
3. Tunica Intima
ARTERY
-
Blood vessels that carry oxygenated, nutrient-rich blood from the heart to the capillaries
Arterial network is a high-pressure system
Blood is propelled under pressure from the left ventricle of the heart
There is high pressure, arterial wall must be thick and strong; the arterial walls also contain elastic fibres
so that they can stretch
COLOUR CHANGE TEST
-
Arterial occlusion
Elevate the leg 12 inches above the client’s <3
NORMAL: it will return to its normal pinkish colour; 15 seconds – veins | 10 seconds or less – artery
**IF occlusion has been shown in developing, there will likely be;
muscle atrophy
skin atrophy
loss of hair growth
BUERGER TEST
-
Arterial insufficiency
This test can be carried out to further demonstrate poor lower limb perfusion.
1. Ensure the patient is positioned supine
60 | H e a l t h a s s e s s m e n t
-
2. Standing at the bottom of the bed, raise both of the patient’s feet to 45º for 2-3 mins:
Observe for pallor – emptying of the superficial veins
If a limb develops pallor, note at what angle this occurs e.g. 20º (known as Buerger’s angle)
A healthy leg’s toes should remain pink, even at 90º
A Buerger’s angle of less than 20º indicates severe limb ischaemia
3. Once the time limit has been reached, ask patient to place their legs over the side of the bed:
- Observe for a reactive hyperaemia – this is where the leg first returns to its normal pink colour, then becomes
red in colour – this is due to arteriolar dilatation (an attempt to remove built up metabolic waste)
VEINS
-
Blood vessels that carry deoxygenated, nutrient-depleted, waste laden blood from the tissues back
to the heart
The vein contain nearly 70% of the body’s volume
Mechanisms
1st - Contains VALVES – permit blood to pass through them on the way to the heart and prevent blood
from returning through them in the opposite direction.
2nd – muscular contraction
3rd – creation of a pressure gradient through the act of breathing – inspiration decreases intrathoracic
pressure while increasing abdominal pressure, thus producing pressure gradient
Deep Veins
Iliac vein
Femoral vein
Popliteal vein
Tibial vein
Superficial Veins
Greater Saphenous Vein
Lesser Saphenous Vein
INSPECTION
SKIN COLOUR
-
There should be no localized colour changes
SKIN
-
Should be mobile and elastic and able to be pinched
Extremities should be bilaterally equal in size
Veins should not be visible on the surface or through the skin
If any veins are visible, elevate the lower extremities; if veins and valves are not compromised ?
LESIONS
-
Petechiae – smaller, tiny red spots | dengue
Ecchymosis – medical term for bruises
Purpura – bigger, purplish colour | snake bites, venous insufficiency
61 | H e a l t h a s s e s s m e n t
HAIR DISTRIBUTION
-
Should be equally distributed bilaterally
DEVIATIONS
DEEP VEIN THROMBOSIS
- a blood clot that forms in a vein deep in the body
- Most deep vein clots occur in the lower leg or thigh
- If the vein swells, the condition is called thrombophlebitis
- A deep vein thrombosis can break loose (called
EMBOLUS) and cause a serious problem in the lung, called
a pulmonary embolism (patient can die after 1 hour)
Valves are not closing completely or incompetent
Veins will be distended
EARLY SIGNS: accumulation of blood – causes-redness
UNILATERAL SWELLING
VARICOSITY
-
Valves incompetent – allowing blood to backflow distending the vein – increasing the pressure –
pushing the blood outside the interstitial space/third space – haemoglobin will be released and
become haemosiderin – which causes discoloration
TESTS
TRENDELENBURG TEST
-
-
To perform this test, elevate the patient’s leg until all of the congested superficial veins collapse (to
drain blood | elevate 90 degrees) | Elevate the leg, put tourniquet between femoral and popliteal
vein (to temporarily stop blood flow)
Apply direct pressure to occlude the superficial veins below the point of suspected reflux from the
deep system into the superficial varicosity.
With the occlusion still in place, have the patient stand. If the distal varicosity remains empty or fills
slowly, quickly remove the occluding hand or tourniquet
*** Tourniquet is applied to prevent 1. Backflow of blood, 2. To temporarily stop the blood flow
NORMAL: slow filling of blood due to competent valves
62 | H e a l t h a s s e s s m e n t
ABNORMAL: incompetent valves allows rapid venous filling causing rubor
Deep Vein – if there is engorgement in the vein before releasing the tourniquet within 5 seconds
Superficial Vein – rapid filling of blood after removing the tourniquet within 30 seconds causing rubor
CAPILLARY REFILL TEST
-
2 seconds is normal – prolonged in PVD
ALLEN TEST
-
Assesses for the;
COMPETENCY
PATENCY
ADEQUATE collateral circulation of blood supply
63 | H e a l t h a s s e s s m e n t
1.
2.
3.
PALPATION
RATE
RYTHYM
QUALITY
RADIAL & DORSALIS PEDIS ARTERY
-
Two most distal pulses
Palpate using the 1st and 2nd fingers or finger pads
-
AMPLITUDE
Quality pulse is the measurement of the force of left ventricular contraction that produces the pulse
wave
Contraction of the heart is slow
Integrity of the arterial wall will also have effect on the quality of the pulse wave
-
The pulse quality is measured on a +3 scale
+3 = full/bounding pulse
+2 = expected
+1 = diminished/barely
0 = absent pulse
ASSESSING THE BRAIN AND NERVES
INFANTS
-
-
The nervous system begins to form within the first 3 weeks of fetal development
At birth, the nervous system is quite immature
There is still no BBB (astrocyte) *develops 5-6 years
Responses by the newborn are primarily primitive reflexes that are present – should subside while
growing up, if not, it indicates an abnormality
Reflexes
The disappearance of these reflexes is a measurement of nervous system maturation
Persistence of these reflexes – indication of CNS dysfunction
Observe the child’s gait – the child just beginning to walk will have a wide-based gait
64 | H e a l t h a s s e s s m e n t
-
By 4 years of age the child should be able to balance on one foot for about 5 seconds and by age 5
should be able to balance for 8-10 seconds
-
Tonic Neck Reflex
Appears at birth
Disappear – 5-7 mos.
Fencing Reflex
-
Babinski Reflex
Normal up to 2 years
-
Rooting Reflex
Disappear: 4 mos.
-
Landau Reflex
Horizontal prone position
Appears 6 mos. and hypotonicity (low tone) indicates motor system deficit
Appears 3 mos. after birth – last up to 12-24 mos. of age
-
Moro Reflex
Consists of rapid abduction and extension of arms with the opening of hands
The arms then come together as in embrace
Any sudden movement of the neck initiates the reflex
Elicit by pulling the baby half-way to a sitting position
Disappear: 4-6 mos.
-
Grasp Reflex | Palmar Grasp Reflex
Appear – at birth
Disappear – 8-10 mos.
-
Sucking Reflex
Probably one of the most important reflex – paired with rooting reflex – secretes for a food source
INSPECTION
1. LEVEL OF CONSCIOUSNESS (LOC)
Awareness is determined by the patient’s orientation to a person, place and time
PERSON – who the patient is and recognition of other individuals
PLACE – where located at this time
TIME – day, month, and year
Early manifestation, agitation, drowsy, confusion – probably caused by a lung problem – lack of blood
supply (oxygenated) to the brain
ASSESSING:
Observe the patient’s ability to follow commands
Ask the patient to squeeze the examiner’s two fingers
65 | H e a l t h a s s e s s m e n t
NORMAL FINDINGS
-
Awake, alert, and responds appropriately to verbal and environmental stimuli
Should be able to follow a simple command and grasp the examiner’s finger
-
When conducting a neurological exam, cranial nerve assessment is the first component of the exam
-
Testing CN III (Oculomotor) is the MOST important – because it is an indicator of brain function
The remaining 11 CNs are not generally tested unless there is a specific reason to do so
GLASGOW COMA SCALE (GCS)
-
Assesses the LOC
CRANIAL NERVES
66 | H e a l t h a s s e s s m e n t
-
Brainstem – consists of most the cranial nerves
The 12 pairs of CNS are part of the peripheral nervous system
Can be sensory and/or motor (function)
CLASSIFICATIONS
SENSORY CRANIAL NERVES – contain only afferent (sensory) fibres
CN 1 OLFACTORY
CN 2 OPTIC
CN 8 VESTIBULOCOCHLEAR
MOTOR CRANIAL NERVES – contain only efferent (motor) fibres
CN 3 OCULOMOTOR
CN 4 TROCHLEAR
CN 6 ABDUCENS
CN 11 ACCESSORY
CN 12 HYPOGLOSSAL
MIXED CRANIAL NERVES – contain both sensory and motor fibres
CN 5 TRIGEMINAL
CN 7 FACIAL
CN 9 GLOSSOPHARYNGEAL
CN 10 VAGUS
LINK:
https://teachmeanatomy.info/head/cranialnerves/summary/?fbclid=IwAR3PzR4ixfyNnJmkvH7STgBpkG8gx0tJpRwjbKpwQTc-HjuQLzmbAguWgp8
LINK: https://www.kenhub.com/en/library/anatomy/the-12-cranial-nerves
CRANIAL NERVE 1 OLFACTORY NERVE
-
SENSORY/AFFERENT - innervates the olfactory mucosa within the nasal cavity
ORIGIN: CEREBRUM
FUNCTION: Responsible for the sense of smell
Smell is an important component of the appreciation of tasks
Loss of sense of smell – as a result of
TRAUMA
INFECTION
AGING
Do not test routinely
Test with:
REPORT OF LOSS OF SMELL
HEAD TRAUMA
SUSPECTED INTRACRANIAL PRESSURE (ICP)
First: assess patency by occluding one nostril at a time and asking the person to sniff – with the person’s
eyes closed
67 | H e a l t h a s s e s s m e n t
-
Use familiar smells, conveniently obtainable and non-noxious smells; coffee, toothpaste orange,
peppermint.
*Alcohol wipes smell are familiar and are easy to find but are irritating
Normally, a person can identify an odour on each side of the nose
Sense of smell normally decreased bilaterally with aging
Any asymmetry is an indication of an abnormality
CRANIAL NERVE 2 OPTIC NERVE
-
SENSORY/AFFERENT - innervates the retina of the eye and brings visual information to the brain
ORIGIN: CEREBRUM
Test Visual Acuity: Snellen’s Chart for distant vision, newspaper/magazine for near vision
Test Visual Fields: Confrontation
CRANIAL NERVE 3 OCULOMOTOR
-
MOTOR/EFFERENT - both a somatic and visceral efferent motor nerve
ORIGIN: MIDBRAIN-PONTINE JUNCTION
FUNCTION: Helps in moving eyeballs in different direction
TEST: Six Cardinal Movements of the Eye
TEST: Pupillary Light Reflex
Shine a direct light or the pupil – Pupillary constriction
**Symptoms of Nerve Damage
Double Vision – diplopia, the affected eye turns outward when the unaffected eye looks straight
ahead
Ptosis – eyelid droop
Pupil may be dilated
Affected eye can move only to the middle when looking inward and cannot look upward and
downward
CRANIAL NERVE 4 TROCHLEAR NERVE
-
MOTOR/EFFERENT
ORIGIN: posterior side of the MIDBRAIN
It has the longest intracranial length of all the cranial nerves.
Superior oblique muscle – eye
TEST: Six Cardinal Movements of the Eye
CRANIAL NERVE 5 TRIGEMINAL NERVE
-
SENSORY & MOTOR / AFFERENT & EFFERENT
ORIGIN: PONS
3 Branches/Divisions
OPTHALMIC (CN V1) - leaves through the superior orbital fissure
MAXILLARY (CN V2) - through the foramen rotundum
MANDIBULAR (CN V3) - exits via the foramen ovale
68 | H e a l t h a s s e s s m e n t
-
Temporal and masseter muscles are examined by palpating the muscles and attempts to resist the
jaw by applying pressure
Testing pain, thermal, and other sensations in the area supplied by the trigeminal nerve
TEST: The Corneal Reflex test – wisp of cotton (Normal: smooth, transparent, involuntary blinking)
CRANIAL NERVE 6 ABDUCENS
-
MOTOR/EFFERENT
ORIGIN: PONTINE-MEDULLA JUNCTION - originates from the brainstem and exits the skull via the superior
orbital fissure
FUNCTION: lateral eye movements (lateral rectus muscle) – abducts the eye; thus the name abducens
Test for Convergence (far and near object)
DEVIATION: Strabismus
CRANIAL NERVE 7 FACIAL NERVE
-
-
SENSORY & MOTOR / AFFERENT & EFFERENT
ORIGIN: PONTINE-MEDULLA JUNCTION
FUNCTION: Once the facial nerve reaches the face it enables many functions, such as facial
expression, secretion of glands and taste sensation.
Motor – note mobility and facial symmetry as the person responds to these requests;
FROWNING
SMILING
Sensory – test only when you suspect facial nerve injury
When indicated, test sense of taste – salt, lemon,
TEST: Inspect for NASOLABIAL FOLDS AND PALPEBRAL FISSURES
DEVIATION: Inability to close eyelid, Drooping of mouth
CRANIAL NERVE 8 VESTIBULOCOCHLEAR
-
SENSORY/AFFERENT - comprised of two parts: the vestibular nerve and the cochlear nerve.
ORIGIN: PONTINE-MEDULLA JUNCTION
FUNCTION: The cochlear component enables hearing, while the vestibular part mediates balance
and motion.
TESTS: Whisper test, Rinne Test, Balance and Hearing
CRANIAL NERVE 9 GLOSSOPHARYNGEAL
-
SENSORY & MOTOR / AFFERENT & EFFERENT
MEDULLA OBLONGATA - It originates from the brainstem and leaves the skull through the jugular
foramen.
FUNCTION: It enables swallowing, salivation, and taste sensation, as well as visceral and general
sensation in the oral cavity.
TEST: Perform – Gag Reflex Test (observe: soft palate & uvula)
DEVIATION: Nerve damage – dysphagia
69 | H e a l t h a s s e s s m e n t
CRANIAL NERVE 10 VAGUS
-
-
SENSORY & MOTOR / AFFERENT & EFFERENT
ORIGIN: MEDULLA OBLONGATA - It originates from multiple nuclei in the brainstem, and exits the skull
through the jugular foramen.
It is the longest cranial nerve and the only one to leave the head and neck region.
The vagus nerve travels into the thoracic and abdominal cavities, providing parasympathetic supply
to visceral organs.
FUNCTION: The vagus nerve controls a large number of functions, including gland secretion, peristalsis,
phonation, taste, visceral and general sensation of the head, thorax and abdomen.
CRANIAL NERVE 11 ACCESSORY
-
MOTOR/EFFERENT
ORIGIN: MEDULLA OBLONGATA - originating from the brainstem and spinal cord
FUNCTION: Acting to enable phonation and movements of the head and shoulders.
CRANIAL NERVE 12 HYPOGLOSSAL
-
-
MOTOR/EFFERENT
ORIGIN: MEDULLA OBLONGATA Anterior to the olive
FUNCTION: Its function is to enable tongue movements.
extremely important for smooth daily functioning of every person, as it plays a significant role in
important mouth functions such as speech and swallowing
PROPRIOCEPTION
Unconscious perception of movement and spatial orientation arising from stimuli within the body
In humans, these stimuli are detected by nerves within the body itself, as well as the semicircular canals
TESTS
CEREBELLAR EXAMINATION
-
Assess motor activity by the patient’s ability for muscle movement and coordination
Should run the test in smooth, rapid, accurate, straight line and coordinated movement
FINGER-TO-NOSE TEST
HANDFLIP TEST
THUMB-TO-FINGER TEST
HEEL-TO-SHIN TEST
ALTERED MOTOR RESPONSE
-
Uncoordinated actions, misses touching the nose/body part several times
DEVIATIONS
DYSDIADOCHOKINESIS
70 | H e a l t h a s s e s s m e n t
-
Inability to perform rapidly alternation movements (may be an indication of multiple sclerosis)
DYSMETRIA
Inability to perform point to point movements by over-or-under projection of the fingers
Lose of motor strength or proprioception
May indicate – Cerebellar lesions
SENSORY
SUPERFICIAL POINT
-
With the patient’s eyes closed, touch the patient’s skin lightly with sharp and dull points of a; bent
paper clip, pen, broken tongue blade
Before testing, it is helpful to touch the patient on both sides
LIGHT TOUCH
-
Use; cotton ball, cotton tip swab
Wait 2 seconds between each touch
Instruct the patient to indicate where the sensation is felt
BALANCE AND EQUILIBRIUM (CN 8 AND CEREBELLUM)
ROMBERG TEST
-
-
-
Patient should stand with his/her feet together and arms at the side
Instruct the patient to close eyes (approx. 30 secs.)
Observe the patient’s ability to maintain upright position
Patient may demonstrate slight swaying back and forth, without the danger of falling
Expected: patient is able to maintain balance and equilibrium within 30 seconds
POSITIVE ROMBERG indicates the possibility of;
CEREBELLAR ATAXIA
Cerebellum becomes inflamed or damaged
Cerebellum: responsible for controlling gait and muscle coordination
Ataxia: lack of fine motor or voluntary movements
VESTIBULAR DYSFUNCTION
SENSORY LOSS
CEREBELLAR LESIONS
In some instances, the patient will lose balance with the eyes closed but be able to regain balance
when the eyes are opened (cerebellar lesions)
TANDEM GAIT
71 | H e a l t h a s s e s s m e n t
-
A gait (method of walking or running) where the toes of the back foot touch the heel of the front foot
each step
Ask the person to walk a straight line in a heel-to-toe fashion
This decreases the base of support and will accentuate any problem with coordination
NORMALLY the person can walk straight and stay balanced
Methods – STATIC BALANCE
-
REFLEXES
Subconscious actions and reactions that are vital defense mechanisms of the nervous system.
-
Initiates immediate response to alert and protect the patient
-
REFLEX ARC
-
Neural pathway that controls the action reflex
A reflex, or reflex action, is an involuntary and nearly instantaneous movement in response to a
stimulus.
A reflex is made possible by neural pathways called reflex arcs which can act on an impulse before
that impulse reaches the brain.
DEEP TENDON REFLEXES
-
Monosynaptic spinal segmental reflexes
Easily assessed by tapping the tendon
-
BICEP REFLEX
Antecubital fossa
TRICEPS REFLEX
72 | H e a l t h a s s e s s m e n t
-
-
-
-
Identify the triceps tendon, a discrete, broad structure that can be palpated (and often seen) as it
extends across the elbow to the body of the muscle, located on the back of the upper arm.
BRACHIORADIALIS REFLEX
Identify the triceps tendon, a discrete, broad structure that can be palpated (and often seen) as it
extends across the elbow to the body of the muscle, located on the back of the upper arm.
PATELLAR REFLEX
LOCATION: Just below the kneecap
Striking – will/should cause
contraction of the quadriceps muscle – extension of the lower leg
ACHILLES REFLEX
LOCATION: Directly behind the ankle
Striking Achilles tendon causes contraction of gastrocnemius muscle – resulting in plantar flexion of the
foot
DEVIATION: lack of reflex – indicates – neuropathy (lower motor neuron)
SUPERFICIAL TENDON REFLEXES
-
-
-
-
Any withdrawal reflex elicited by noxious or tactile stimulation of the skin, cornea, or mucous
membrane, including the corneal, pharyngeal, and cremasteric reflexes.
PLANTAR REFLEX
plantar flexion of the foot when the ankle is grasped firmly and the lateral border of the sole is stroked
or scratched from the heel toward the toes
The reflex can take one of two forms.
In healthy adults, the plantar reflex causes a downward response of the hallux (flexion).
DEVIATION: dorsiflexion of the great toe with or without forming BABINSKI-POSITIVE (this is normal to
children under 2y/o)
ABDOMINAL REFLEX
A superficial neurological reflex stimulated by stroking of the abdomen around the umbilicus.
It can be helpful in determining the level of a CNS lesion.
CREMASTERIC REFLEX
A superficial reflex found in human males that is elicited when the inner part of the thigh is stroked.
Stroking of the skin causes the cremaster muscle to contract and pull up the ipsilateral testicle toward
the inguinal canal.
DEVIATION: TESTICULAR TORSION - It happens when the spermatic cord, which provides blood flow to
the testicle, rotates and becomes twisted.
The twisting cuts off the testicle's blood supply and causes sudden pain and swelling.
OLDER ADULTS
-
Have less blood supply (20% - ages 60^)
73 | H e a l t h a s s e s s m e n t
-
-
Gradual atrophy of the brain occurs due to the loss of neurons in the brain and spinal cord
By 80 years of age, brain has lost 15% of its weight
Speed of nerve conduction decreases – causing the reaction time of the elderly to decrease
Decreased in the speed of learning and processing information
There is an increased delay at the synapses, resulting in a slower traveling time for an impulse
This may result in a diminished sense of smell and taste as well as decreased sensation of pain and
touch
These,, therefore are the probable reason why older adults/aged are prone to Alzheimer’s
There is an overall loss of muscle bulk that reduces muscle strength
GATE CONTROL THEORY
-
Open Gate -> T-cell -> brings the stimulus to the brain -> the brain (hypothalamus) will interpret it to
pain
SG – Substantia Gelatinosa
-
a collection of cells in the gray area (dorsal horns) of the spinal cord
found at all levels of the cord
it receives direct input from the dorsal (sensory) nerve roots, especially those fibers from pain and
thermoreceptors
WHAT OPENS THE GATE
-
Lack of sleep
Stressful lifestyle
Fear and anxiety about pain
Depression
Physical activity / tired
Mentally focusing on pain
Hypoglycemia (Normal: 80/100 mg/dl of blood)
Serotonin and Endorphin deficit
Consumption of nutrients that increase inflammation (such as fried and oily foods)
74 | H e a l t h a s s e s s m e n t
WHAT CLOSES THE GATE
-
Relaxation
Exercise
Medications (Pain relievers, Opioids – Morphin, Demerol)
Distractions from pain
Positive Thoughts
Endorphin
Avoiding nutrients that increases inflammation (such as fried and oily foods)
Acupuncture
Serotonin (consumption of food rich in serotonin such as banana)
Adequate sleep
PAIN
Transmission
-
Impulses from afferent – CNS – Neurons – Spinal Cord –
Thalamus – relay station for sensory input –
Midbrain – signals cortex to raise awareness of the stimuli
PAIN TOLERANCE
-
Amount and duration of pain a person can stand before seeking relief
Can vary between different individuals in the same situations
-
TOLERANCE
A state of adaptation in which exposure to a drug induces charges that result in a decrease in
one or more of the drug’s effects over time
PAIN THRESHOLD
-
Point at which each person recognizes pain
Tends to be the same among healthy persons
INCREASE TOLERANCE
-
Alcohol
Drugs
Hypnosis
Strong beliefs
Distractions
Rubbing
DECREASE TOLERANCE
-
Fatigue
75 | H e a l t h a s s e s s m e n t
-
Anger
Boredom
Anxiety
Stress
Depression
** Anxiety and Stress can stimulate or inhibit urination and may provoke urgency and frequency
** Schwann Cells = PNS Oligodendrocytes = CNS
= MYELIN SHEATH
Specific Types of Pain
-
REFFERED PAIN
Discomfort
Perceived in a general area of the body but not in the exact site where an organ is anatomically
located
-
VISCERAL PAIN
Arises from internal organs that are diseased or injured
Usually accompanied by ANS symptoms
Sharp or dull, aching cramping pain
-
-
SOMATIC PAIN
(e. g a hot stove) Pain may originate in the skin tissues
SUPERFICIAL PAIN
Sharp, pricking, burning
DEEP SOMATIC PAIN
Muscles or bones, sharp, dull and aching
-
NEUROPATHIC PAIN
Caused by damage to the CNS or Peripheral nerves
Damage: vertebrae – causes pressure to the root nerve causing pain
Damage; to myelin sheath – damaged by our own antibody / autoimmune
PHANTON PAIN
-
ENDORPHINS
-
Endogenous chemicals that act like opioids to inhibit pain impulses in the spinal cord and brain
They degrade too quickly
TYPES OF PAIN
ACUTE
-
Tachy – increased bp
Associated with SNS
CHRONIC
-
No changes in Vital Signs
Assessment of chronic pain should focus on impact of the pain and on patients’ function and daily
activities
76 | H e a l t h a s s e s s m e n t
**DANGERS OF UNRELIEVED PAIN
-
Pain causes shallow breathing and cough suppression -> prevention of pulmonary secretions ->
pneumonia
-
may delay the return of normal gastric and bowel function
Peristalsis – inhibited
Suppress the immune system and heighten susceptibility to illness
PAIN
CHRONIC PAIN
-
Lowers the pain threshold as a result of the depletion of SEROTONIN and ENDORPHIN
DRUG THERAPHY
Non-Opioid Analgesics
-
First line therapy for mild to moderate pain
Do not produce tolerance or physical or psychological dependence
Works primarily at the site of injury rather than the CNS
They do not have antipyretic effect
Opioid Analgesics
-
Given when pain is moderate in intensity (PS: 7-10)
Also for mild but persistent pain
Non-Pharmacologic Methods of Pain Management
-
-
-
Massage. A lot of people find relief from gentle massage, and some hospice agencies have
volunteers who are trained in massage therapy. Several studies have found that massage is
effective in relieving pain and other symptoms for people with serious illness.
Relaxation techniques. Guided imagery, hypnosis, biofeedback, breathing techniques, and
gentle movement such as tai chi. Relaxation techniques are often very effective, particularly when
a patient -- or a caregiver -- is feeling anxious.
Acupuncture. Several studies have found that acupuncture can be helpful in relieving pain for
people with serious illnesses such as cancer.
Physical therapy. If a person has been active before and is now confined to bed, even just moving
the hands and feet a little bit can help.
Pet therapy. If you have bouts of pain that last 5, 10, or 15 minutes, trying to find something pleasant
-- like petting an animal's soft fur -- to distract and relax yourself can be helpful.
Gel packs. These are simple packs that can be warmed or chilled and used to ease localized pain.
PAIN DICRIMINATION – eyes closed
77 | H e a l t h a s s e s s m e n t