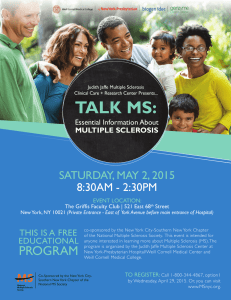
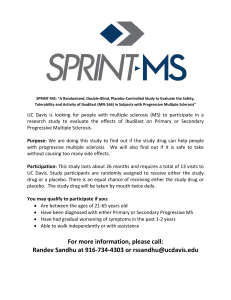
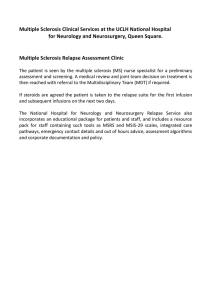
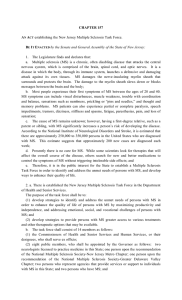
REVIEWS Mechanisms of neurodegeneration and axonal dysfunction in multiple sclerosis Manuel A. Friese, Benjamin Schattling and Lars Fugger Abstract | Multiple sclerosis (MS) is the most frequent chronic inflammatory disease of the CNS, and imposes major burdens on young lives. Great progress has been made in understanding and moderating the acute inflammatory components of MS, but the pathophysiological mechanisms of the concomitant neurodegeneration—which causes irreversible disability—are still not understood. Chronic inflammatory processes that continuously disturb neuroaxonal homeostasis drive neurodegeneration, so the clinical outcome probably depends on the balance of stressor load (inflammation) and any remaining capacity for neuronal self-protection. Hence, suitable drugs that promote the latter state are sorely needed. With the aim of identifying potential novel therapeutic targets in MS, we review research on the pathological mechanisms of neuroaxonal dysfunction and injury, such as altered ion channel activity, and the endogenous neuroprotective pathways that counteract oxidative stress and mitochondrial dysfunction. We focus on mechanisms inherent to neurons and their axons, which are separable from those acting on inflammatory responses and might, therefore, represent bona fide neuroprotective drug targets with the capability to halt MS progression. Friese, M. A. et al. Nat. Rev. Neurol. 10, 225–238 (2014); published online 18 March 2014; doi:10.1038/nrneurol.2014.37 Introduction Zentrum für Molekulare Neurobiologie Hamburg, Universitätsklinikum Hamburg-Eppendorf, Falkenried 94, D‑20251 Hamburg, Germany (M.A.F., B.S.). Nuffield Department of Clinical Neurosciences and Medical Research Council Human Immunology Unit, Weatherall Institute of Molecular Medicine, John Radcliffe Hospital, University of Oxford, Oxford OX3 9DS, UK (L.F.). Correspondence to: M.A.F. manuel.friese@ zmnh.uni-hamburg.de Multiple sclerosis (MS) is a disseminated, chronic, inflam­ matory demyelinating disease of the CNS with progres­ sive neuroaxonal degeneration. The disease nearly always starts before the age of 40 years, afflicts approximately three females per one male, and is a major cause of dis­ ability.1 MS is considered to be an autoimmune disease, initiated by T cells targeting self antigens in the CNS in genetically susceptible individuals. The first lesions are typically focal areas of demyelination in the white matter, known as plaques. Depending on the locations of these plaques, the resulting clinical neurological manifest­ ations are notoriously variable, and usually result from immune cell invasion across the blood–brain barrier. This process eventually leads to continuous activation of CNS-homing and CNS-resident innate immune cells (macrophages and microglia) in the brain parenchyma, with ensuing demyelination and neurodegeneration.1,2 However, we still do not fully understand the relation­ ships between the inflammatory lesions, demyelination, and the neuro­degenerative changes that correlate best with clinical disability. Although demyelination with loss of trophic support from oligodendrocytes clearly contrib­ utes to axonal degeneration,3,4 axonal and neuronal injury also occurs without demyelination.5–10 Since modulation of peripheral inflammatory responses or demyelination seems to be insufficient to inhibit neuronal loss, we aim to identify potential novel therapeutic targets in MS by reviewing work on patho­ logical mechanisms of neuroaxonal dysfunction and Competing interests The authors declare no competing interests. injury, which have the potential to be translated into druggable approaches. In particular, we point to evi­ dence that axonal and neuronal impairment are early and independent contributors to the progression of MS, and assess pathophysiological mechanisms of intrinsic neurodegeneration, which could occur under chronic inflammatory insults. Early and continuous neurodegeneration Clinical evidence In most patients, MS starts with a relapsing–remitting course (RRMS), with subacute episodes of neurologi­ cal symptoms that subside spontaneously to apparently normal baseline function. After 15–25 years, however, the relapses typically shift into inexorably progressive neurodegeneration, which is termed secondary progres­ sive MS (SPMS; Figure 1a).11 10–15% of patients enter this neurodegenerative phase directly from the onset of clinical disease—a condition known as primary pro­ gressive MS (PPMS). While the length of the relapsing–­ remitting phase varies greatly, both the inevitability and the rate of neurological decline are highly consistent, regardless of the preceding disease course and severity.1,12 These clinical observations have led to the sugges­ tion that the underlying neurodegeneration depends on the patient’s age and not on the number of relapses or inflammation. Notably, it transpires that neither the risk of entering the secondary progressive phase nor the latency of entering progression is related to total relapse number during the relapsing–remitting phase (Figure 1b).13,14 This dissociation between relapses and progression implies that relapses might not be a valid NATURE REVIEWS | NEUROLOGY VOLUME 10 | APRIL 2014 | 225 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Key points ■■ Neuronal and axonal degeneration in multiple sclerosis (MS) is a slow process initiated by acute lymphocytic inflammation, and subsequently driven by chronically smouldering, diffuse parenchymal myeloid and meningeal lymphocytic inflammation ■■ Oxidative stress, mitochondrial injury and subsequent ion channel dysfunction secondary to chronic inflammation seem to have a constant impact on neurons and axons, leading to their demise during progressive MS ■■ Several ion channels show compensatory changes in response to the inflammatory stimulus by altering their relative distribution in the neuron—a process that eventually becomes maladaptive and perpetuates neuroaxonal injury ■■ Several neuroprotective pathways have been identified in MS, but these pathways become overridden, resulting in neuronal degeneration that is probably mediated by the initiation of apoptosis and Wallerian degeneration ■■ The balance between continuous inflammatory stressors and intrinsic buffering mechanisms depends partly on age, sex and genetic factors, which eventually determine the clinical course of MS ■■ In an animal model of MS, few molecular targets with proven neuroprotective properties that are separable from their impact on inflammatory responses have been identified; these molecules include CyPD, ASIC1 and TRPM4 surrogate outcome measure for the late disability of MS. In support of this notion are the minimal—or at least unknown—long-term effects on disability or rate of clini­cal progression of current disease-modifying treat­ ments initiated early during clinically isolated syndrome (CIS) or RRMS. 15–17 Nevertheless, once progression starts, no current drug has been found to affect its rate. These findings have led to the hypothesis that MS is a two-stage disease, starting with an inflammatory phase and later entering a supposedly distinct neurodegenera­ tive phase. However, advances in imaging and neuro­ pathology in early MS are making it increasingly clear that neurodegeneration starts directly at onset of disease, so is already apparent by the time of clinical diagnosis, and that the transition from RRMS to SPMS is likely to Paraclinical evidence from MRI and biomarkers Several classic MRI modalities detecting hypointense T1 ‘black holes’, cortical lesions and atrophy of the brain and spinal cord, as well as novel analytical methods, provide data that correlate with clinical disability, and have been used to show that neurodegeneration is often already evident at the time of diagnosis (Figure 2). 18 Cerebral and spinal cord atrophy has proved to be the most important marker of neurodegeneration, and can be detected in patients with CIS, as well as at the earliest stages of RRMS.19,20 Various studies have demonstrated that this atrophy also affects the grey matter, again from the ­earliest stages of disease.19 Unmyelinated CNS axons are uniquely accessible in the retinal nerve fibre layer (RNFL), and optical coher­ ence tomography (OCT) now allows their measure­ ment at micrometre resolution, offering the potential to monitor neurodegeneration in a novel and simple way. Indeed, in patients with MS who have no prior clinical history of optic neuritis, the estimated annual thinning of the RNFL is approximately 2 μm, compared with 0.2 μm per year in disease-free controls (Figure 3a,b).18,21 Independent evidence for ongoing neurodegeneration has come from biomarker studies measuring different neuron-specific and axon-specific proteins in cerebro­ spinal fluid (CSF). The most robust marker to date seems to be the concentration of neurofilament heavy chain in the CSF, which correlates with the extent of disability. Indeed, levels of the protein are already significantly increased in patients with CIS.22 Neurofilament light chains have shown similarly increased CSF levels at all stages of MS; in patients with RRMS, the levels decreased after treatment with natalizumab.23 b 100 1–2 2–4 ≥5 80 80 RRMS SPMS 60 50% RR 40 Median time to SP = 15 years 20 0 10 60 40 20 50% SP 0 Patient survival (%) Patients converting to SPMS (%) a 100 be the point at which the compensatory bypassing of neuronal injury exceeds its capacity. 0 20 30 40 50 0 Disease duration (years) 10 20 30 40 50 Time (years) Figure 1 | Clinical correlates of neurodegeneration in MS. a | Rate of conversion to SPMS. In a population-based series of 806 patients with RRMS with 28-year follow up, median time to conversion to SPMS (defined as at least 1 year of deterioration) was 15 years, shown here as a cumulative percentage in a Kaplan–Meier analysis. b | In the same cohort as in part a, patients with RRMS reached onset of progression within a similar time frame, regardless of categorization as having low (1–2), intermediate (3–4) or high (≥5) total number of relapses. Data are depicted as Kaplan–Meier survival curves. Estimated mean times from disease onset to Disability Status Scale 6 (requiring aid for walking) were similar between the groups: 1–2 relapses, 15.6 mean years; 3–4 relapses, 15.7 mean years; ≥ 5 relapses, 15.9 mean years. Abbreviations: MS, multiple sclerosis; RR, relapsing–remitting; SP, secondary progressive. Part a adapted by permission from BMJ Publishing Group Limited. J. Neurol. Neurosurg. Psychiatry, Scalfari, A. et al. 85, 67–75 © 2013. Part b by permission of Oxford University Press: Scalfari, A. et al. The natural history of multiple sclerosis: a geographically based study 10: relapses and long-term disability. Brain 133 (Pt 7) (2010), 1914–1929. 226 | APRIL 2014 | VOLUME 10 www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Figure 2 | Radiological correlates of neurodegeneration in multiple sclerosis. Black holes on T1-weighted spin-echo MRI in multiple sclerosis represent severe tissue destruction, including axonal and neuronal loss (boxes). Sequential T1-weighted spin-echo MRI scans, obtained at 2‑month intervals, show evolution of black holes from a new lesion, starting with a new gadolinium-enhancing (bright) lesion that represents an active inflammatory process with a breakdown of the blood–brain barrier, evolving into hypointense non-contrast-enhanced images at all subsequent time points. Permission obtained from Nature Publishing Group © Barkhof, F. et al. Nat. Rev. Neurol. 5, 256–266 (2009). Neuropathological evidence Historically, the white matter plaques, with primary demyelin­ation and astrocytic scarring, dominated think­ ing on MS pathology, and degeneration of neurons and their axons was overlooked.24 However, early involvement of axons is now accepted; indeed, their loss is the best cor­ relate of the irreversible neurological disability in MS.25 Acute axon injury is commonly found in white matter inflammatory plaques in early RRMS, but is less evident in chronic inactive lesions and normal-appearing white matter (NAWM; Figure 3c,d). Although NAWM is defined as macroscopically normal and microscopically normally myelinated, most samples actually show significantly decreased densities of axons.5–9 This finding might partly be explained by Wallerian degeneration, which occurs after transections have separated distal axon segments from their cell bodies.26 However, diffuse axon injury in NAWM is not associated with white matter plaques, but correlates instead with diffusely scattered inflammation throughout the CNS. Therefore, this process seems to be partially independent of demyelination.5–10 Imaging and neuropathological studies have rediscov­ ered extensive grey matter pathology in MS, often with demyelinated cortical plaques and transected axons, apoptotic neurons,27 and reduced neuronal density with atrophy.24,28 The grey matter lesions are usually wide­ spread and random, include the deep grey matter, and show intense microglial and immune cell infiltration.29 Chronic grey matter lesions, however, tend to have less immune cell infiltration than do chronic white matter lesions. 24 Pathological evidence indicates very early involvement of the cortex, sometimes even before any white matter lesions are found in brain biopsies29 and, since cortical lesions are seen particularly in SPMS and PPMS, they could be important pathological cor­ relates of the irreversible disability.7,30 Supporting this idea, cortical grey matter lesions with widespread neuro­ nal loss are associated with diffuse meningeal inflam­ mation that is, in turn, closely correlated with the rate of clinical progression in SPMS and PPMS, suggest­ ing that soluble factors produced by the inflammatory cells in the subarachnoid compartment have a crucial role in neurodegeneration.31,32 Taken together, these findings imply that neuro­ degeneration in MS is at least partially independent of demyelination, and is a slow process initiated by acute lymphocytic inflammation and subsequently driven by chronically smouldering, diffuse parenchymal myeloid and meningeal lymphocytic inflammation. According to this model, inflammation can drive neurodegeneration at any stage of the disease. Genetic evidence The suggestion that inflammation is causally linked to neurodegeneration has recently been supported by a cor­ relation between meningeal inflammation and the extent of small-fibre axonal loss in the lumbar spinal cord. This phenomenon can, however, only be detected in indi­ viduals who are positive for HLA-DRB1*15,33 the most important genetic risk factor for MS.34 To date, almost all genome-wide association studies (GWAS) have com­ pared MS patients with healthy controls, thereby focusing on initiating events rather than on severity and, thus, the neurodegenerative pathways involved in MS progres­ sion.34 Only three GWAS have focused on MS sever­ ity, 35–37 and showed no consistent associ­ations with any of the genes known to predispose to MS onset,37 although GRIN2A, which encodes the NR2A subunit of N‑methyl‑d-aspartate (NMDA)-type glutamate recep­ tors, showed an association in two of the three studies.35,37 Moreover, MS patients with allelic variants in a gene network that led to higher glutamate levels in the brain showed greater brain atrophy over 1 year of follow-up in comparison to patients who did not carry these risk alleles.38 Clearly, these data need to be replicated in larger studies, which might identify other interesting candidate genes that are associated with MS severity. Although the above-delineated studies provide mostly phenomenological and correlative evidence, they have prompted hypothesis-driven molecular studies, which have provided partial insights into the inflammationinduced neurodegenerative and compensatory neuro­ protective pathways, which we will describe in the next section. Molecular pathways of neurodegeneration Inflammation in the CNS leads to innumerable molecu­ lar changes (Figure 4). Immune cells secrete neurotoxic products—including reactive oxygen species (ROS), glutamate, cytokines and chemokines—that direct the evolution of immune responses and also alter cellular metabolism in neurons and their axons. The short-term effects of these immune cell products are important for tissue defence and resolution; however, in the long-term, they evoke intrinsic stress responses and activate other homeostatic processes. Dissecting these pathways in MS is very difficult because of the complexity of the disease, the limited access to the target tissue, and the clinical and genetic heterogeneity of the condition. Not surprisingly, most of our current knowledge about neurodegeneration in MS originates from experi­ mental autoimmune encephalomyelitis (EAE), the animal model of MS, which mimics many clinical and NATURE REVIEWS | NEUROLOGY VOLUME 10 | APRIL 2014 | 227 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Box 1, and have thereby identified proven neuroaxonal mechanisms of injury or protection during chronic CNS inflammation in vivo (Figure 5, Table 1, Supplementary Table 1 online). Moreover, we have included selected studies that have a compelling rationale but do not yet comply with these criteria and, therefore, need further investigations to demonstrate neuroprotective properties. a Thickness (μm) b 200 100 0 0 T 120 150 180 210 240 N I T Position on retinal map Pathologically thinned RNFL Normal RNFL thickness RNFL thickness in optic neuritis Borderline RNFL thickness 30 60 S 90 0 1 2 Axons (%) d 100 c 0 0 * 50 0 1 * 1 2 NAWM 2 * Lesion Figure 3 | Pathological correlates of neurodegeneration in MS. a | RNFL thickness (red and yellow area indicated by arrow), assessed by optical coherence tomography, provides an estimate of the extent of neurodegeneration. Retinogram shows imaged layers of a normal retina. b | Blue line indicates RNFL thickness in an eye affected by optic neuritis, superimposed over normative data for an age-matched control. c | Representative axonal changes in acute MS lesions. Normal appearance of axons (stage 0; top), focal swellings (stage 1; middle) or fragmentation (stage 2; bottom) in Bielschowsky silver impregnation. d | Axonal injury is also prevalent in NAWM, but stages 1 and 2 are much more frequently detected in acute MS lesions. Asterisks indicate significant differences between NAWM and lesions. Abbreviations: I, inferior sector; MS, multiple sclerosis; N, nasal sector; NAWM, normal-appearing white matter; RNFL, retinal nerve fibre layer; S, superior sector; T, temporal sector. Permission for parts a and b obtained from Nature Publishing Group © Barkhof, F. et al. Nat. Rev. Neurol. 5, 256–266 (2009). Permission for parts c and d obtained from Nature Publishing Group © Nikic, I. et al. Nat. Med. 17, 495–499 (2011). neuropathological features of the disease.39 To identify truly neurodegenerative pathways in MS or EAE, one must be aware of indirect effects of inflammatory pro­ cesses, which could account for several reports of ‘neuro­ degeneration’ or ‘neuroprotection’. Since it is difficult to predict whether in vitro experiments mimicking only part of the inflammatory environment will translate into the same pathophysiological correlate in EAE or MS, we will primarily discuss in vivo studies that have provided novel conceptual insights into oxidative stress, mito­chondrial dysfunction and altered ion channel activ­ ity. These studies fulfil the strict quality criteria listed in 228 | APRIL 2014 | VOLUME 10 Oxidative stress Neuropathological studies have implicated activated macro­phages and microglia in driving ongoing neuro­ degeneration. Given that active neurodegenerative processes in RRMS and SPMS correlate closely with inflammation,5 great interest has been expressed in the neurotoxic products released by such innate immune cells. ROS and reactive nitrogen species (RNS) such as nitric oxide (NO) are produced by macrophages and micro­glia in MS and EAE lesions, and their oxidation products correlate with inflammation.40–42 Moreover, neurons with intense cytoplasmic accumulation of oxi­ dized phospho­lipids and DNA strand breaks are abun­ dant in active cortical MS lesions, implying that oxidative damage is highly prevalent.43 Besides being a by-product of cellular respiration, ROS can be synthesized specifically in activated macrophages and microglia by enzymes including myeloperoxidase, xanthine and NADPH oxidases (NOX). 44,45 Activated microglia in both active and slowly expanding lesions show upregulation of NOX2 subunits, and also of NOX1 and NOX organizer 1.45 The importance of NOX2 in oxidative tissue damage is supported by the milder EAE course in mice that were deficient in gp91phox, which encodes a NOX2 subunit, although neither neuroaxonal degeneration nor the extent of inflammatory infiltrates was assessed. 46 NO donors have also been shown to cause reversible conduction block in axons and to drive neuronal degeneration in rat spinal cords.47 An in vivo imaging study revealed that application of oxygen and nitrogen donors to the spinal cords of healthy mice was sufficient to induce EAE-like axonal injury in the absence of demyelin­ation.42 In turn, scavengers that reduced levels of ROS and RNS in EAE mice were able to attenuate focal axonal degeneration without altering the numbers of immune cells in acute EAE lesions. Iron accumulation in the physiologically ageing human brain and in patients with MS can further amplify ROSand-RNS-mediated injury 48 by generating toxic react­ ants, as experimentally shown in spinal cord injury.49 In the CNS, iron is stored in oligodendrocytes, and injury of these cells during MS releases Fe2+ into the extra­ cellular space, where it is taken up by activated macro­ phages and microglia.50,51 In turn, the macrophages and microglia degenerate,52 thereby further contributing to Fe2+ accumu­lation in the extracellular space and also in axons.48 Eventually, this process might contribute to oxi­ dative neuronal damage.53 Importantly, this iron accumu­ lation correlates with early axonal injury, and is particular prominent in active lesions of patients with acute MS and short disease duration.48 In chronic MS, however, a sig­ nificant decrease in iron levels is observed in the NAWM, www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Reactive oxygen species Chronic CNS inflammation Reactive nitrogen species Oxidative stress Hypoxia Mitochondrial damage and dysfunction Cytokines Demyelination Glutamate Ca2+ influx Ion channel redistribution Energy deficiency Ion imbalance 2+ Ca /Na+ overload Activation of degrading enzymes Oncotic cell swelling Neuroaxonal damage by apoptosis and necrosis Figure 4 | Cascades leading to inflammation-induced neuroaxonal injury. The scheme illustrates the prevailing hypothetical sequence of events eventually leading to neuroaxonal degeneration in multiple sclerosis. Chronic CNS inflammation lies at the root of deregulation of neuronal and axonal metabolism. The cascade culminates in the hallmarks of inflammation-induced neurodegeneration described in this Review. corresponding with disease duration,48 questioning a direct role for iron accumulation in MS progression with advancing age. Moreover, iron is important for several cellular processes and homeo­stasis in the CNS, sound­ ing a note of caution regarding the use of iron-chelating therapies in patients with MS. Fe2+ accumulation in the CNS of EAE animals is scarce,54 so its pathogenic role during inflammation-induced neurodegeneration remains e­ nigmatic and difficult to test. Intrinsic and extrinsic oxidants are major stressors in cell physiology, and dynamic cellular programmes have evolved to moderate their long-term deleterious effects. One such programme is orchestrated by nuclear factor erythroid 2‑related factor 2 (NRF2), a transcrip­ tion factor that induces such antioxidant enzymes as heme oxygenase 1 (HMOX1), which scavenge free radi­ cals and remove damaged proteins.55 HMOX1 levels are increased in MS lesions56 and in the CNS of EAE mice,57 and are also found to be elevated in the CSF of patients with MS.58 Exacerbation of EAE in both Nrf2 and Hmox1 knockout mice underscores the therapeutic potential of Box 1 | Criteria verifying direct neurodegeneration or neuroprotection in EAE Very few studies on defined molecules allow direct inference regarding neurodegeneration or neuroprotection; that is, direct injury or preservation of axons and neurons without altering the accompanying CNS inflammation in vivo. Since many tested molecules are expressed in both CNS-resident cells and the immune system, studies on these molecules and their pathways reporting neurodegenerative or neuroprotective processes in the context of EAE must fulfil at least one of the following criteria to verify their direct neuronal involvement: ■■ Reports of altered neuroaxonal damage with unchanged CNS inflammation during the disease. However, due to the difficulties of analysing the entire EAErelevant immune cell functions, and the possibility that reduced (neuronal) tissue damage results in an attenuated reactive inflammatory response, further measures must be taken to prove a direct neuronal phenotype by interfering with defined molecular pathways ■■ Generation of tissue-specific (conditional) transgenic animals with exclusive expression or deletion of the respective molecule in neurons ■■ Bone marrow chimaeric animals, which harbour an immune system that is replaced by haematopoietic stem cells of a different genotype, resulting in mice with a wild-type immune system and genetically altered CNS-resident cells. However, the caveat remains that CNS-resident immune cells, such as microglial cells, are not replaced by this procedure ■■ A further valid approach to decipher immune and neurobiological effects is adoptive transfer EAE experiments, whereby the animals are passively immunized by ex vivo-activated, CNS-specific T cells from appropriate donor animals Abbreviation: EAE, experimental autoimmune encephalomyelitis. enhancing these antioxidant pathways, 57,59 but both of these knockout mice show elevated immune responses in the EAE model, thereby preventing imputation of their enhanced neuronal injury to a compromised neuronal antioxidative response.57,59 Notably, in mice, Nrf2 is induced in neurons by the drug dimethyl fumarate (DMF).60 This effect has been proposed to contribute to an attenuated EAE disease course in DMF-treated mice, and might, therefore, partly underlie the beneficial effects of this drug in patients with MS.60 No differences were reported in immune cell infiltration for DMF-treated versus control mice, but the assessments were performed 74 days after EAE induc­ tion, by which time most of the inflammatory responses have already subsided from the CNS. Other studies have reported that DMF induces Hmox1 in dendritic cells, resulting in an anti-inflammatory phenotype of den­ dritic cells and, subsequently, T cells, but this agent also inhibits macrophage infiltration.61,62 This finding might explain, at least in part, the ameliorated EAE course in DMF-treated animals. The hypothesis that antioxidative pathways protect neurons from inflammatory-mediated oxidative stress is attractive, but whether these pathways are enhanced in neurons is not yet known, and experimental data are lacking to support the idea that neuronal NRF2 induction by DMF results in neuroprotection in CNS inflammation in vivo. However, given that mitochondrial dysfunction is a major component in MS pathophysiology (Box 2), and mitochondria have long been known to be particu­ larly vulnerable to damage from prolonged exposure to oxidants,63 the concept of ROS-and-RNS-mediated neurodegeneration in chronic CNS ­inflammation is particularly appealing. Mitochondrial dysfunction and energy deficit According to one hypothesis, damage to mitochon­ dria is the main cause of tissue injury in MS (Box 2).64 Mitochondria are derived from aerobic bacteria that infiltrated proto-eukaryotes around 109 years ago, and they still have a separate genome and synthesize ATP by oxidative phosphorylation (OXPHOS). Normal cellular respiration yields ROS as by-products that require detoxi­ fication. Lacking protective histones, mitochondrial DNA (mtDNA) can rapidly accumulate mutations when ROS levels are increased, which can eventually compromise NATURE REVIEWS | NEUROLOGY VOLUME 10 | APRIL 2014 | 229 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS b Glu Microglia Glu Monocyte Myelin GluR NOS Lymphocyte H+ Glu H+ H+ VGCC ASIC1 Ca2+ Na+/K+ATPase NCX Ca2+ Ca2+ Ca2+ Ca2+ Ca2+ Axon Neuron Nav1.2 Nav1.6 TRPM4 Nav1.8 Na+ Reverse Na+ Na+ Cell swelling ATP Calpain Oligodendrocyte Blood vessel Axon Myelin Neuron a Axon c Demyelination ROS OXPHOS CyPD Mutated mtDNA Dying back mtPTP Presynaptic neuron Necrosis ATP Apoptosis DR4/5 CD200R CD200 WldS Resveratrol Bcl-2 Neuroaxonal injury H+ Glu NO CB1R ROS Cannabinoids Cytokines Figure 5 | Neuronal injury and counteracting pathways in chronic CNS inflammation. Chronic inflammation in multiple sclerosis is primarily driven by activated parenchymal macrophages and microglia, and meningeal lymphocytes. a | Inflammatory ROS and NO production leads to mtPTP opening, accumulation of mtDNA mutations and oxidized and misfolded proteins, and necrosis. Compromised mitochondria disturb OXPHOS, leading to further ROS elevation and decreased ATP production. Apoptosis is induced partly by DR4/5 engagement. b | Excess extracellular Glu activates Glu receptors, leading to neuroaxonal Ca2+ influx. Membrane depolarization activates VGCC and increases Nav activity. ASIC1 contributes to further Ca2+ influx, and ASIC1 and TRPM4 potentiate Na+ influx. Reduced ATP levels lower Na+/K+-ATPase activity, resulting in reverse operation of NCX and fatally increasing intracellular Ca2+ and Na+ levels. Continuously elevated Ca2+ activates degradative enzymes and NOS. These processes lead to neuronal apoptosis and necrosis. c | Excitotoxicity associated with Ca2+ and Na+ overload is counterbalanced by prosurvival gene expression, cannabinoid system activity, and inhibition of Wallerian degeneration. Continuous inflammation overrides these buffering systems, resulting in substantial neuroaxonal damage. Abbreviations: ASIC1, acid-sensing ion channel 1; CyPD, cyclophilin D; DR4/5, death receptor 4 and 5; Glu, glutamate; mtDNA, mitochondrial DNA; mtPTP, mitochondrial permeability transition pore; Nav, voltage-gated sodium channel; NCX, Na+/Ca2+-exchanger; NO, nitric oxide; NOS, NO synthase; OXPHOS, oxidative phosphorylation; ROS, reactive oxygen species; TRPM4, transient receptor potential cation channel subfamily M member 4; VGCC, voltage-gated calcium channels. OXPHOS efficiency.65 Both excessive ROS production and mitochondrial deficiency normally seem to increase with age.63 ROS-inflicted mtDNA mutations compromise OXPHOS, initiating a vicious circle that results in mito­ chondrial collapse with consequent reductions in cellular fitness (Figure 5a).65 This effect is further mimicked in mice66 and humans67 with mutations in mtDNA polymer­ ase, which accumulate excessive mtDNA mutations and exhibit signs of premature ageing of a type that can also be detected in the brains of patients with MS. As transport in axons is highly energy-demanding, these structures are extremely sensitive to fluctuations in energy supply; indeed, compromised mitochondrial trans­ port is an early change in inflammatory EAE lesions,42 230 | APRIL 2014 | VOLUME 10 possibly mediated by translocation of histone deacetylase 1 from the nucleus to the axoplasm, where it hinders kinesin motor protein functions.68 Resveratrol attenuates neuronal damage in optic neuritis during EAE without affecting the inflammatory infiltrate in the optic nerve;69 it protects by indirectly activating sirtuin 1 (SIRT1), a NAD+-dependent deacetylase that promotes mitochondrial function.70 In addition to excessive ROS, mitochondrial damage or death can be triggered by the mitochondrial per­meability transition (MPT), which depends on the matrix protein cyclophilin D (CyPD). MPT leads to instantaneous col­ lapse of the mitochondrial trans­membrane potential, equilibration of ionic gradients, and cessation of OXPHOS with subsequent necrosis. EAE is milder in Cypd-deficient www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Table 1 | Genetic evidence: molecules mediating neurodegeneration or neuroprotection in EAE Gene modulation* Outcome Evidence for neurospecific effect Reference BCL2 overexpression under NSE promoter Reduction in clinical impairment; reduced axonal damage Overexpression of human BCL2 only in neurons (NSE promotor); no differences in T‑cell proliferation and ‘delayed-type hypersensitivity’ Offen et al. (2000)129 Asic1–/– Reduction in clinical impairment; reduced neuroaxonal damage No significant difference in immune cell infiltrate; adoptive transfer EAE Friese et al. (2007)72 Cnr1–/– (CB1) Reduction in clinical impairment on cannabinoid treatment (is dependent on CB1 in neurons) Conditional knockout in neurons (nestin promotor) and T cells (Lck promotor) Maresz et al. (2007)139 Trpm4–/– Reduction in clinical impairment; reduced neuroaxonal damage No significant differences in immune cell infiltrate, T‑cell activation or cytokine production; bone marrow transplantation Schattling et al. (2012)94 Ppid–/– (CyPD) Reduction in clinical impairment; reduced neuroaxonal damage No significant differences in immune cell infiltrate and antigen-specific T‑cell proliferation Forte et al. (2007)71 Expression of the fusion protein Wlds Reduction in clinical impairment; reduced neuroaxonal damage No significant differences in the area of inflammation and T‑cell infiltration Kaneko et al. (2006)140 Reduction in clinical impairment; reduced demyelination and neuroaxonal damage; reduced microglia activation by neuronal inhibition No significant differences in T‑cell proliferation, cytokine production and ‘delayed-type hypersensitivity’ Chitnis et al. (2007)131 Scn10a–/– (Nav1.8) Reduction in clinical impairment Immune cell effects were not tested, but Nav1.8 is probably not expressed in immune cells Shields et al. (2012)91 Scn2b–/– Reduction in lethality and clinical impairment; reduced neuroaxonal damage No significant differences in immune cell infiltrate, T‑cell proliferation and cytokine release O’Malley et al. (2009)83 *Affected proteins are given in brackets, where relevant. Abbreviation: EAE, experimental autoimmune encephalomyelitis. mice, and axon damage is decreased despite unaffected immune cell infiltration.71 Furthermore, neurons lacking CyPD are more resistant to damage mediated by ROS and RNS.71 Eventually, because of impaired mitochondrial OXPHOS and MPT, the high demands for neuroaxonal ATP can no longer be met, and chronic hypoxia ensues. This shortfall has been one of the prevailing explana­ tions for neurodegeneration in MS,64 and is supported by hypoxic gene expression signatures, including induc­ tion of hypoxia-inducible factor‑1α (HIF‑1α) in EAE.72 In addition, some studies in the brains of patients with MS have revealed nuclear translocation of HIF‑1α that indicates its activation,73,74 which would promote tissue oxygenation and glucose delivery. Box 2 | Mitochondrial damage in multiple sclerosis Chronic inflammation leads to increased local levels of reactive oxygen species and reactive nitrogen species, increasing the risk of mitochondrial damage. Remarkably, mitochondria from the motor cortex of patients with MS show abnormal reductions in nuclear DNA-encoded complex I and III activities.141 Moreover, mitochondrial DNA (mtDNA) gradually accumulates deletions in neurons in the grey matter of patients with secondary progressive MS (SPMS) compared with age-matched controls.142 These deletions are not limited to cortical lesions, but are found throughout the grey matter—and primarily in layer VI—in SPMS. Layer VI consists mainly of motor neurons, and borders on the subcortical white matter, suggesting involvement of white matter processes such as production of toxic agents by macrophages and microglia within active white matter lesions.142 Additional loss of the mtDNA-encoded catalytic subunits of complex IV might be incurred, especially in demyelinated axons in active and chronic active lesions with high densities of macrophages and microglia.107,143 On the other hand, total mitochondrial content and complex IV activity can be increased in apparently undamaged but demyelinated axons in chronic inactive lesions, probably in response to increased energy needs,107 and might even normalize in remyelinating axons.144 Given that mitochondria are key regulators of cell survival and death, a detailed understanding of specific damaging pathways seems to be central in designing strategies to halt inflammation-induced neuroaxonal failure. Moreover, as the newest calculations of energy consumption by cortical neurons show that 75% of total neural energy is used for ionic equilibrium during infor­ mation processing,75 ion channel malfunction seems to be central during the energy shortfall, as we will now discuss. Ion channel dysfunction Both energy imbalance and demyelination during chronic CNS inflammation lead to activation, dysfunction and maldistribution of several ion channels (Supplementary Table 1 online), evoking downstream mechanisms that mostly converge on Ca2+ overload (Figure 5b). This over­ load seems to be the key instigator of neurotoxicity, initi­ ating a vicious circle by activating degradative enzymes, compromising mitochondrial function and impairing axonal transport, all of which results in a further increase in Ca2+ levels. Sodium MRI has revealed increased Na+ concentrations within MS lesions, NAWM and grey matter, which were particularly pronounced in patients with SPMS,76 providing evidence for ion dysregulation in progressive MS. Sodium channels Concentration of Na+ channels at nodes of Ranvier allows accelerated ‘saltatory’ conduction from node to node by myelinated fibres. When it enters the axon, Na+ is rapidly exchanged for extracellular K + by Na+/K+-ATPase at the internodal axolemma.77 This ongoing ion exchange is important for axonal polarization, which in turn is NATURE REVIEWS | NEUROLOGY VOLUME 10 | APRIL 2014 | 231 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS needed for transmission of action potentials, but con­ sumes large amounts of neuronal energy, leading to the assumption that excessive Na+ influx results in aggravated energy run down.75 These observations have also resulted in the concept that demyelination not only exposes axon segments to extrinsic stressors, but also vastly increases the energy demand for signal conduction, as Na+ channels spread along the denuded axolemma.78 However, it has now been shown that action potentials consume much less energy 79,80 than was previously thought.81 Therefore, Na+ influx-related energy run down remains speculative, as there is a low correlation between the membrane area and the predicted energy consumption of a neuron.75 Another postulate is that the Na +/Ca 2+ exchanger (NCX) operates in reverse when Na+ levels rise in axons, thereby increasing intracellular Ca2+ levels. This sug­ gestion is supported by colocalization of voltage-gated Na+ channel (Nav)1.2, Nav1.6 and NCX subunits along demyelin­ated axons in MS plaques78 and EAE lesions,82 as well as by the beneficial effects of gene knockouts and Nav/NCX blockers in EAE. Deficiency of the Navmodulating β2 subunit (Scn2b) prevents Nav1.6 upregula­ tion in EAE lesions and reduces both axon degeneration and clinical scores.83 Moreover, the class I antiarrhyth­ mic flec­ainide,84,85 Na+-channel antagonistic anticonvul­ sants86–88 and the α‑aminoamide derivative safinamide85 all reduce axon injury and neurological disability in mice. Importantly, peripheral immune cell compositions and T‑cell responses in Scn2b-deficient mice were compar­able to those in wild-type mice.83 Immune cell infiltration into the CNS in EAE mice was not quantified, however, so the possibility remains that channel modulation, as recorded with the antagonists used to date, are actually acting as immunosuppressants on Nav-expressing macro­phages and microglia89—a notion that is supported by the acute EAE exacerbations and increases in inflammation on their withdrawal.85,86 Similarly, the anti­convulsant lamo­ trigine proved ineffective in SPMS, with no effect on cer­ ebral volume over 24 months. Indeed, this drug caused transient early volume losses, suggesting water shifts or ‘pseudoatrophy’, again implying anti-inflammatory rather than neuroprotective effects.90 Nav1.8 has a more definitive role in cerebellar dys­ function in MS. Normally restricted to the PNS, this channel is ectopically expressed in cerebellar Purkinje neurons in patients with MS and mice with EAE. In mice, Nav1.8 overexpression clearly disrupts coordi­ nated motor behaviours; both treatment with a Nav1.8selective blocker and deficiency of the Scn10a gene, which encodes Nav1.8, moderate EAE and alter Purkinje neuron firing.91 These findings provide further evidence for a distinct inflammation-induced ion channelopathy, and suggest possible therapeutic options for treating ­cerebellar dysfunction in MS. Nonselective cation channels The transient receptor potential (TRP) superfamily of ion channels enables individual cells to sense thermal and chemical changes in their local environment.92 These channel properties allow neurons also to sense 232 | APRIL 2014 | VOLUME 10 and respond to inflammation. Most of the TRP proteins are nonselective cation channels, although member four of the melastatin-like TRP subfamily (TRPM4) consti­ tutes an exception by just gating monovalent cations, thereby being impermeable for Ca2+.93 As detailed above, increased intracellular Ca2+ levels and ATP depletion due to mitochondrial dysfunction are two major patho­ physiological alterations in neurons during chronic CNS inflammation. Of note, the opening behaviour of TRPM4 is altered by these two conditions: it can be acti­ vated by increasing intracellular Ca2+ levels but can also be blocked by high cytosolic ATP levels.93 A study published in 2012 showed that genetic or pharma­c ological inactivation of TRPM4 resulted in reduced axonal and neuronal degeneration and amelior­ated clinical EAE disease scores.94 Importantly, the neuro­nal protection in Trpm4-deficient mice arose without alterations in lesion or immune cell numbers, antigen-specific T‑cell proliferation, cytokine profiles or demyelination. The neuron-specific effect was further validated by the generation of bone marrow chimaeric mice and by in vitro studies. Importantly, TRPM4 is expressed in neuronal somata in mouse and humans, but is redistributed into axons during chronic inflammation in MS and EAE, and colocalizes with the axonal injury marker amyloid precursor protein (APP). Neuronal damage probably occurs through TRPM4-dependent neuronal ion influx with subsequent oncotic cell ­swelling on intracellular Ca2+ stimulation.94 Potassium channels Since K+ channels regulate synaptic transmission and neuronal excitability, alterations in expression or acti­ vation, particularly of voltage-gated K+ (Kv) channels, could possibly affect these functions. Congruously, 4‑aminopyridine, a nonspecific blocker of Kv channels, is currently in use to improve the mobility of patients with MS.95 Alterations in the neuronal expression pat­ terns of Kv1.2, Kv1.4 and Kv2.1 have been found during chronic CNS inflammation, and could underlie the ben­ eficial effects of this therapy.96 Furthermore, selective pharmacological blockade of Kv1.1, which is expressed on neurons and astrocytes, attenuates the clinical EAE phenotype and reduces brain damage, without affect­ ing peripheral T‑cell activation. 97 CNS immune cell ­infiltration was not quantified in this study. The various members of the two-pore-domain K+ channel family are expressed in different body cells and, by giving rise to leak K+ currents, control excitability. TWIKrelated acid-sensitive potassium channel 1 (TASK1) is neuronally expressed and, due to its physicochemical modulation (by pH and pO2, for example), it might alter electrical excitability during chronic CNS inflamma­ tion.98 In support of this idea, gene deletion or pharma­ cological blockade of TASK1 ameliorates the EAE disease course, although inactivation of the channel also leads to repression of inflammatory responses, thereby hamper­ ing any conclusions regarding neuroprotective proper­ ties.99,100 Therefore, whether K+ channel blockers harbour ­neuroprotective properties in the strictest sense is unclear. www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Calcium channels Several parallel sources contribute to neuroaxonal Ca2+ overloading; namely, entry through voltage-gated Ca2+ channels (VGCCs), release from intracellular stores, and other cation channels, among which glutamate-gated receptors have a prominent role. Depolarization of neurons and axons after substantial cation influx will activate VGCCs, which might thereby contribute to Ca2+ influx. Blocking of L‑type VGCCs with bepridil or nitrendipine significantly moderated EAE, and reduced inflammation and axon pathology.101 In nor­ mally myelinated axons, N‑type VGCCs are ubiquitously expressed on nerve terminals and play an important part in neurotransmitter release, but are absent from the internodal axolemma.102 By contrast, prominent axonal accumu­lation of the pore-forming subunit of N‑type VGCC was reported in demyelinated axons and axonal swellings in MS and EAE lesions, and integration into the axonal membrane in EAE lesions has been shown.103 The maldistribution of VGCCs into demyelinated axons might result in a pathological influx of Ca2+, contributing to axonal demise. Supporting a role for these channels in axonal degeneration, specific blockade of N‑type VGCCs by use of ω‑conotoxin GVIA decreased axon and myelin degeneration in an optic neur­itis model.104 However, as with many other reports, it remains uncertain whether the treatment was acting primarily on neurons and axons or on immune cells, as substantially reduced macrophage–­ microglial inflammation was detected in the treatment groups,101,104 precluding an interpretation with regard to neuroprotective properties. Locations of intracellular or intra-axonal stores of Ca2+ include the endoplasmic reticulum and mitochondria. Both of these organelles seem to contribute to neuronal Ca 2+ overload with subsequent neuroaxonal injury in vitro105 but, other than indirect evidence for mitochon­ drial Ca2+ release,71 neither has been shown to operate in vivo during CNS inflammation. Glutamate is the main excitatory neurotransmitter in the CNS. Its concentration is tightly regulated by several mechanisms, including metabolic and transport pathways. Alterations in glutamate levels, which result in excessive neuronal signalling, could lead to Ca2+-mediated excito­ toxicity,106 which is implicated by GWAS in patients with MS, as specified above.40,42 On glutamate stimulation, Ca2+ enters mainly through ionotropic glutamate recep­ tors, and several factors, such as cell type, developmen­ tal stage and the relative contributions of synaptic versus extrasynaptic receptor activation, determine whether prosurvival or death pathways are activated.106 Reduced mitochondrial complex IV activity can further augment glutamate-­mediated axon injury 107 and, in turn, glutamate and abnormal NMDA receptor function contribute to ­dysfunctional mitochondrial activity in EAE.108 Glutamate levels are elevated in the CSF109 and brains38 of patients with MS, apparently deriving from dying neurons and secretion by activated immune cells.110 Concomitantly, various cell types show upregulation of the ionotropic NMDA, AMPA (α-amino‑3-hydroxy‑5methyl‑4-isoxazole propionic acid) and kainate receptors in MS lesions.111 Moreover, disposal of glutamate prob­ ably declines, as expression of its transporters is decreased in the CNS of patients with MS112 and EAE mice.113,114 Indeed, inhibition of NMDA and AMPA receptors improves the outcome of EAE,115–121 and limits neuro­ degeneration also by preserving dendritic spines.120 Some of these antagonists conferred clinical benefits without affecting peripheral T‑lymphocyte activation,115,116,121 but monocyte–­microglial infiltration was substantially reduced by glutamate receptor inhibition.121 Mice that were genetically deficient for the enzyme d‑aspartate oxidase released increased amounts of d‑aspartate and NMDA in the CNS.108 These mice showed no difference in EAE severity in comparison to wild-type mice, but did exhibit accelerated disease progression. Therefore, the question of whether inhibitors of ionotropic glutamate receptors indeed act specifically as neuroprotectants remains enig­ matic, and further studies with conditional transgenic animals, bone marrow chimaeras or adoptive transfer EAE are needed to decipher the precise ­contribution of glutamate receptors to direct neurodegeneration. Chronic inflammation is also associated with a rise in extracellular proton concentrations—another indepen­ dent stressor that activates a distinct class of cation chan­ nels, the acid-sensing ion channels (ASICs). These channels belong to the degenerin/epithelial Na+ channel (DEG/ENaC) family, are sensitive to amiloride, and are present in peripheral and central neurons. 122 ASIC1a seems to be essential for acid-activated currents in mouse neurons, where it may heteromerize with ASIC2a. Besides acid­osis, ASIC1a is activated by lactate, arachidonic acid and decreased extracellular Ca2+, which are all features of chronic inflammation.122 Interestingly, the pH drops from around 7.4 to around 6.5 in inflammatory CNS lesions.72 Although its main function is to gate Na+ cur­ rents, ASIC1a can also allow Ca2+ entry during acidosis.123 Notably, neuro­axonal degeneration is reduced—without affecting the lymphocytic or myeloid inflammatory ­infiltrates—­in Asic1a-deficient mice and during treat­ ment with amiloride in several EAE models and neuro­ nal cultures.72,124 Importantly, like VGCC and TRPM4, ASIC1 is found particularly in injured axons, and colocal­ izes with the axonal injury marker APP, in both EAE and active MS lesions.124 However, mice deficient in ASIC2 are not protected against EAE (M. A. Friese and L. Fugger, unpublished data), so ASIC1 seems the more promis­ ing therapeutic target for strategies to protect neurons in MS. Supporting this idea, in a pilot study, patients with PPMS showed a reduction in whole-brain volume loss during amiloride treatment, ­compared with their own pre-treatment phase.125 Downstream of the Ca2+ overload in neuronal somata and axons are Ca2+-dependent proteases such as cal­ pains, which degrade axon components. Inhibition of these proteases improved clinical scores in a chronic EAE model.126 Although calpain expression was also increased in immune and glial cells during EAE,127 upregulation of these proteases in neurons correlated most closely with the extent of axonal degeneration in acute EAE.128 However, calpain inhibitors also significantly reduced inflammatory NATURE REVIEWS | NEUROLOGY VOLUME 10 | APRIL 2014 | 233 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS Box 3 | Exploring neurotrophins as neuroprotectants The few soluble neuroprotectants that have been identified include ciliary neurotrophic factor (CNTF145) and brain-derived neurotrophic factor (BDNF146). BDNF belongs to the family of neurotrophins and is secreted primarily by neurons and glia. The wide-ranging actions of these factors are important for the development and maintenance of the nervous system. A single nucleotide polymorphism in the human BDNF gene converts valine to methionine at codon 66 (Val66Met). The BDNFMet protein shows altered dendritic trafficking and synaptic localization, and has a substantially reduced propensity to activity-dependent release.147 Given that the Val66Met polymorphism has been selected for during evolution,148 and in view of its association with changes in brain structure, network and function in healthy humans and several neurological and psychiatric disorders, it might have an important modifying influence on health and disease.147 In patients with multiple sclerosis (MS), the BDNFMet genotype is associated with preservation of grey matter volume, and correlates inversely with autoimmune-induced lesions.149,150 BDNF has, therefore, been tested as a potential neuroprotectant.151 BDNF is produced mainly by CNS-resident cells, but infiltrating immune cells can also secrete BDNF in MS.152,153 Mice with Bdnf gene deletions in either astrocytes or immune cells show enhanced experimental autoimmune encephalomyelitis (EAE) and axon loss,146 and CNS-derived BDNF seems to mediate axonal protection in EAE, as demonstrated by experiments with bone marrow chimaeras.154 However, BDNF can be a double-edged sword, depending on its levels and the availability of its receptors and target cells. Acting directly on neurons, it mediates neuroprotection and neuroregeneration; however, it also induces neurodegeneration after engaging with the TrkB receptor on astrocytes. 155 Therefore, the use of BDNF in MS demands caution. Two novel therapeutics, alemtuzumab156 and laquinimod,157 increase BDNF secretion by peripheral immune cells, and whether this action renders these drugs neuroprotective should emerge from their forthcoming use in MS. Box 4 | Cannabinoids and erythropoietin as neuroprotectants Cannabinoids have been tested as neuroprotectants to counteract inflammatory stressors (Figure 5c). CB1 receptors bind several different endocannabinoids that are released locally on demand. These receptors are involved in controlling excitotoxicity,158 and experimental autoimmune encephalomyelitis (EAE) is more severe in Cb1-deficient mice than in controls, with greater neurodegeneration and increased tumour necrosis factor-mediated excitotoxicity.159,160 In mice with cell-type-specific knockouts, cannabinoid treatment-mediated neuroprotection was shown to depend on CB1 expressed by neurons rather than by T cells.139 This neuroprotective effect is further supported by the fact that low, nonimmunosuppressive doses of cannabinoid receptor agonists can ameliorate axonal loss and disability in EAE.161 Disappointingly, in a randomized, double-blind, placebo-controlled study, the cannabinoid receptor agonist Δ9-tetrahydrocannabinol showed no efficacy with regard to disability progression over a 36-month period in patients with primary or secondary progressive multiple sclerosis.162 Erythropoietin (EPO) shows more promising clinical signals. EPO and its receptor are widely expressed in the nervous system and are upregulated after injury. Since peripherally administered EPO crosses the blood–brain barrier and can stimulate neurogenesis and neuronal differentiation, it is proposed to be a potent neuroprotectant. Furthermore, EPO has antiapoptotic, antioxidant and antiinflammatory properties.163 Prompted by the beneficial effects of EPO derivatives on inflammatory responses and neurodegeneration in the EAE model,164 a randomized phase II trial was initiated in which patients with optic neuritis received recombinant human EPO or placebo daily for 3 days as an add-on therapy to methylprednisolone.165 The EPO-treated patients showed a significant decrease in retinal nerve fibre layer thinning after 16 weeks. Since long-term treatment of EPO is associated with severe adverse effects, such as thromboembolic events and oncogenic potential, the neuroprotective properties might be further explored in long-term treatments with novel EPO derivatives and mimetics, which engage the tissue-protective effects of EPO without activating haematopoietic and coagulation pathways.163 234 | APRIL 2014 | VOLUME 10 infiltrates, thereby precluding any firm conclusions regarding their potential neuroprotective activities.126 Adaptive changes in ion channels On the basis of the evidence presented above, ion channel dysregulation seems to be central to the process of neuronal and axonal demise during MS. However, it also transpires that several ion channels show adap­ tive changes to the inflammatory stimulus by altering their relative distribution in the neuron. Nav,78 VGCC,103 TRPM494 and ASIC1a124 ion channels relocalize from the somata and dendrites in healthy individuals to axons in MS and EAE. Although these channels contribute to axonal degeneration, it seems likely that their axonal distribution represents an initially beneficial counter­ measure to preserve conductance and axonal integrity. Understanding this change in distribution, as well as the sequence of pathological ion channel activation and the relative contributions of the different channels to MS‑related neurodegeneration, might open up new possibilities for therapeutic intervention. While ion channels represent promising targets mostly for generating inhibitory drug compounds, hopes have also been ascribed to endogenous soluble factors that are physiologically produced by CNS or immune cells to counteract neurodegeneration. These factors include neuro­t rophins (Box 3), as well as cannabinoids and erythropoietin (Box 4), which have already been tested in ­clinical trials in MS. Apoptosis and Wallerian degeneration Eventually, most of the above-described neurodegenera­ tive pathways, combined with a lack of neuroprotective support, result in a common final pathway of neuronal and axonal demise, most probably mediated by the initi­ ation of apoptosis and Wallerian degeneration (Figure 5c). DNA fragmentation reflecting activation of the apoptotic signalling cascade in neurons is frequently detected in MS lesions in areas of active demyelination and tissue injury, but also to a lesser extent in the demyelinated lesion centre, inactive cortical MS lesions and NAWM.27,43 Supporting evidence for the importance of apoptosis in inflammation-induced neuronal cell death has come from mice overexpressing the antiapoptotic protein B‑cell lymphoma‑2 (Bcl‑2) speci­fically in neurons.129 In com­ parison with control mice, the transgenic mice displayed attenuated EAE severity and reduced axonal loss without exhibiting changes in immune response. Moreover, the cytokine TRAIL, a member of the tumour necrosis factor–nerve growth factor receptor superfamily that is secreted by various immune cells, can induce caspasedependent apoptosis in neurons on binding to the death receptors DR4 and DR5.130 Wallerian degeneration—an active process that is sim­ ilar to apoptosis—seems to drive axonal loss in patients with MS26 and EAE mice.131 This dying-back process can be attenuated in mice by the expression of the fusion protein ‘Wallerian degeneration slow’ (Wlds). Wlds mice, which carry a triplication of the fusion gene Ube4b/ Nmnat, show reduced neuroaxonal damage as well as www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS ameliorated clinical impairment in EAE. Although this neuronal protection occurs without changes in immune cell infiltration, T‑cell proliferation or cytokine produc­ tion, Wlds mice display decreased levels of microglial and macrophage activation in EAE lesions.131 Indeed, this type of immune modulation seems to be directly con­ trolled by neuronal cells. Neurons of Wlds mice express increased amounts of the non-signalling glycoprotein CD200, which inactivates monocytes by binding to the CD200 receptor,131 thereby providing a protection mechanism by which neurons are able to control the extent of CNS inflammation. Conclusions and future prospects Descriptive and correlative clinical, paraclinical and neuro­pathological studies (Figures 1–3) indicate that inflammation can cause white matter axon transection as well as cortical and subcortical neuronal injury, even from the onset of MS. Inflammation is composed of several relentless stressors—such as electrons, protons or ­oxidants—that disturb complex interconnected neuro­ axonal metabolic pathways,132 to which mitochondrial damage and glutamate metabolism seem to be central. These events lead to energy deficits and Ca2+ overload. Neurons and axons respond to these continuing inflam­ matory challenges via compensatory induction of protec­ tive pathways. However, several additional maladaptive changes, most notably ion channel redistrib­ution along inflamed axons, seem to accelerate degener­ation. Although these alterations might have transient functional benefits, ­prolonged changes seem to be deleterious (Figure 4). The balance between these continuous stressors and intrinsic buffering mechanisms depends partly on age, sex and genetic factors, which eventually determine the clinical course. An obvious therapeutic goal is to enhance any compensatory mechanisms and inhibit maladaptive changes that perpetuate the stressor load. However, inhibition of adaptive changes is fraught with difficulties; for example, inhibition of Na+ channels has resulted in initial worsening of paresis (as these channels seem to secure conduc­tion along demyelinated axons), but might provide long-term neuroprotection.90 Equally, 1. 2. 3. 4. 5. 6. Compston, A. & Coles, A. Multiple sclerosis. Lancet 372, 1502–1517 (2008). Weiner, H. L. A shift from adaptive to innate immunity: a potential mechanism of disease progression in multiple sclerosis. J. Neurol. 255 (Suppl. 1), 3–11 (2008). Funfschilling, U. et al. Glycolytic oligodendrocytes maintain myelin and long-term axonal integrity. Nature 485, 517–521 (2012). Lee, Y. et al. Oligodendroglia metabolically support axons and contribute to neurodegeneration. Nature 487, 443–448 (2012). Frischer, J. M. et al. The relation between inflammation and neurodegeneration in multiple sclerosis brains. Brain 132, 1175–1189 (2009). Kornek, B. et al. Multiple sclerosis and chronic autoimmune encephalomyelitis: a comparative quantitative study of axonal injury in active, inactive, and remyelinated lesions. Am. J. Pathol. 157, 267–276 (2000). targeting of g­ lutamate c­ hannels is associated with severe adverse effects.133 So far, few molecular targets have been identified with proven neuroprotective properties that are sepa­ rable from their impact on inflammatory responses. Attractive approaches would be to inhibit ROS produc­ tion or CyPD, ASIC1 or TRPM4 activity, or to explore the tissue-protective effects of erythro­poietin (Figure 5, Table 1, Supplementary Table 1 online). Several of these targets are currently under investigation for drug develop­ ment. By contrast, no pharmacological agents are avail­ able that might be capable of inducing neuronal pathways that increase tolerance towards inflammatory stressors. Physical exertion has been shown to increase resist­ ance to degenerative disorders of ageing.134 Some crosssectional studies report positive associations between aerobic fitness and grey matter density in trained versus untrained patients with MS,135 and a randomized trial has demonstrated a link between physical fitness and improved cognition in patients with progressive MS.136 These findings are corroborated by the attenuation of EAE with exercise and the consequent protection of axons with enhancement of neuronal plasticity.137 Equally, exer­ cise potently rescues the premature ageing phenotype of mice with mutations in mtDNA p ­ olymerase by inducing mitochondrial biogenesis.138 Overall, the current dearth of treatment options for the progressive phases of MS highlights the pressing need for better understanding of neurodegenerative pathways and protective mechanisms. Review criteria The cited articles in this Review were identified by a search of the PubMed database, and were retrieved as full-text articles. Search terms used were “multiple sclerosis”, “neurodegeneration”, “axonal degeneration”, “neuropathology”, “genetics”, “MRI”, “progression”, “ion channels”, “oxidative injury”, “mitochondria”, “microglia”, “inflammation”, “neuroprotection” and “neurotrophins”, alone or in combination without limits on publication date or language. We further analysed reference lists of key papers to identify additional papers and cross-references. 7. Kutzelnigg, A. et al. Cortical demyelination and diffuse white matter injury in multiple sclerosis. Brain 128, 2705–2712 (2005). 8. DeLuca, G. C., Ebers, G. C. & Esiri, M. M. Axonal loss in multiple sclerosis: a pathological survey of the corticospinal and sensory tracts. Brain 127, 1009–1018 (2004). 9. Bitsch, A., Schuchardt, J., Bunkowski, S., Kuhlmann, T. & Bruck, W. Acute axonal injury in multiple sclerosis. Correlation with demyelination and inflammation. Brain 123, 1174–1183 (2000). 10. DeLuca, G. C., Williams, K., Evangelou, N., Ebers, G. C. & Esiri, M. M. The contribution of demyelination to axonal loss in multiple sclerosis. Brain 129, 1507–1516 (2006). 11. Scalfari, A., Neuhaus, A., Daumer, M., Muraro, P. A. & Ebers, G. C. Onset of secondary progressive phase and long-term evolution of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 85, 67–75 (2014). NATURE REVIEWS | NEUROLOGY 12. Confavreux, C., Vukusic, S., Moreau, T. & Adeleine, P. Relapses and progression of disability in multiple sclerosis. N. Engl. J. Med. 343, 1430–1438 (2000). 13. Scalfari, A. et al. The natural history of multiple sclerosis: a geographically based study 10: relapses and long-term disability. Brain 133, 1914–1929 (2010). 14. Scalfari, A. et al. Early relapses, onset of progression, and late outcome in multiple sclerosis. JAMA Neurol. 70, 214–222 (2013). 15. Kappos, L. et al. Long-term effect of early treatment with interferon beta-1b after a first clinical event suggestive of multiple sclerosis: 5‑year active treatment extension of the phase 3 BENEFIT trial. Lancet Neurol. 8, 987–997 (2009). 16. Shirani, A. et al. Association between use of interferon beta and progression of disability in patients with relapsing–remitting multiple sclerosis. JAMA 308, 247–256 (2012). VOLUME 10 | APRIL 2014 | 235 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS 17. Haghikia, A., Hohlfeld, R., Gold, R. & Fugger, L. Therapies for multiple sclerosis: translational achievements and outstanding needs. Trends Mol. Med. 19, 309––319 (2013). 18. Barkhof, F., Calabresi, P. A., Miller, D. H. & Reingold, S. C. Imaging outcomes for neuroprotection and repair in multiple sclerosis trials. Nat. Rev. Neurol. 5, 256–266 (2009). 19. Chard, D. T. et al. Brain atrophy in clinically early relapsing–remitting multiple sclerosis. Brain 125, 327–337 (2002). 20. Miller, D. H., Barkhof, F., Frank, J. A., Parker, G. J. & Thompson, A. J. Measurement of atrophy in multiple sclerosis: pathological basis, methodological aspects and clinical relevance. Brain 125, 1676–1695 (2002). 21. Petzold, A. et al. Optical coherence tomography in multiple sclerosis: a systematic review and metaanalysis. Lancet Neurol. 9, 921–932 (2010). 22. Kuhle, J. et al. Neurofilament heavy chain in CSF correlates with relapses and disability in multiple sclerosis. Neurology 76, 1206–1213 (2011). 23. Gunnarsson, M. et al. Axonal damage in relapsing multiple sclerosis is markedly reduced by natalizumab. Ann. Neurol. 69, 83–89 (2011). 24. Popescu, B. F. & Lucchinetti, C. F. Pathology of demyelinating diseases. Annu. Rev. Pathol. 7, 185–217 (2012). 25. Bjartmar, C., Kidd, G., Mörk, S., Rudick, R. & Trapp, B. D. Neurological disability correlates with spinal cord axonal loss and reduced N‑acetyl aspartate in chronic multiple sclerosis patients. Ann. Neurol. 48, 893–901 (2000). 26. Dziedzic, T. et al. Wallerian degeneration: a major component of early axonal pathology in multiple sclerosis. Brain Pathol. 20, 976–985 (2010). 27. Peterson, J. W., Bö, L., Mörk, S., Chang, A. & Trapp, B. D. Transected neurites, apoptotic neurons, and reduced inflammation in cortical multiple sclerosis lesions. Ann. Neurol. 50, 389–400 (2001). 28. Vercellino, M. et al. Grey matter pathology in multiple sclerosis. J. Neuropathol. Exp. Neurol. 64, 1101–1107 (2005). 29. Lucchinetti, C. F. et al. Inflammatory cortical demyelination in early multiple sclerosis. N. Engl. J. Med. 365, 2188–2197 (2011). 30. Kutzelnigg, A. et al. Widespread demyelination in the cerebellar cortex in multiple sclerosis. Brain Pathol. 17, 38–44 (2007). 31. Choi, S. R. et al. Meningeal inflammation plays a role in the pathology of primary progressive multiple sclerosis. Brain 135, 2925–2937 (2012). 32. Howell, O. W. et al. Meningeal inflammation is widespread and linked to cortical pathology in multiple sclerosis. Brain 134, 2755–2771 (2011). 33. DeLuca, G. C. et al. Casting light on multiple sclerosis heterogeneity: the role of HLA-DRB1 on spinal cord pathology. Brain 136, 1025–1034 (2013). 34. The International Multiple Sclerosis Genetics Consortium. Risk alleles for multiple sclerosis identified by a genomewide study. N. Engl. J. Med. 357, 851–862 (2007). 35. Baranzini, S. E. et al. Genome-wide association analysis of susceptibility and clinical phenotype in multiple sclerosis. Hum. Mol. Genet. 18, 767–778 (2009). 36. Brynedal, B. et al. MGAT5 alters the severity of multiple sclerosis. J. Neuroimmunol. 220, 120–124 (2010). 37. International Multiple Sclerosis Genetics Consortium. Genome-wide association study of severity in multiple sclerosis. Genes Immun. 12, 615–625 (2011). 236 | APRIL 2014 | VOLUME 10 38. Baranzini, S. E. et al. Genetic variation influences glutamate concentrations in brains of patients with multiple sclerosis. Brain 133, 2603–2611 (2010). 39. Friese, M. A. et al. The value of animal models for drug development in multiple sclerosis. Brain 129, 1940–1952 (2006). 40. Haider, L. et al. Oxidative damage in multiple sclerosis lesions. Brain 134, 1914–1924 (2011). 41. Zeis, T. et al. Molecular changes in white matter adjacent to an active demyelinating lesion in early multiple sclerosis. Brain Pathol. 19, 459–466 (2009). 42. Nikic, I. et al. A reversible form of axon damage in experimental autoimmune encephalomyelitis and multiple sclerosis. Nat. Med. 17, 495–499 (2011). 43. Fischer, M. T. et al. Disease-specific molecular events in cortical multiple sclerosis lesions. Brain 136, 1799–1815 (2013). 44. Gray, E., Thomas, T. L., Betmouni, S., Scolding, N. & Love, S. Elevated activity and microglial expression of myeloperoxidase in demyelinated cerebral cortex in multiple sclerosis. Brain Pathol. 18, 86–95 (2008). 45. Fischer, M. T. et al. NADPH oxidase expression in active multiple sclerosis lesions in relation to oxidative tissue damage and mitochondrial injury. Brain 135, 886–899 (2012). 46. Li, S., Vana, A. C., Ribeiro, R. & Zhang, Y. Distinct role of nitric oxide and peroxynitrite in mediating oligodendrocyte toxicity in culture and in experimental autoimmune encephalomyelitis. Neuroscience 184, 107–119 (2011). 47. Smith, K. J., Kapoor, R., Hall, S. M. & Davies, M. Electrically active axons degenerate when exposed to nitric oxide. Ann. Neurol. 49, 470–476 (2001). 48. Hametner, S. et al. Iron and neurodegeneration in the multiple sclerosis brain. Ann. Neurol. 74, 846–861 (2013). 49. Rathore, K. I. et al. Ceruloplasmin protects injured spinal cord from iron-mediated oxidative damage. J. Neurosci. 28, 12736–12747 (2008). 50. Craelius, W., Migdal, M. W., Luessenhop, C. P., Sugar, A. & Mihalakis, I. Iron deposits surrounding multiple sclerosis plaques. Arch. Pathol. Lab. Med. 106, 397–399 (1982). 51. Bagnato, F. et al. Tracking iron in multiple sclerosis: a combined imaging and histopathological study at 7 Tesla. Brain 134, 3602–3615 (2011). 52. Lopes, K. O., Sparks, D. L. & Streit, W. J. Microglial dystrophy in the aged and Alzheimer’s disease brain is associated with ferritin immunoreactivity. Glia 56, 1048–1060 (2008). 53. Lassmann, H., van Horssen, J. & Mahad, D. Progressive multiple sclerosis: pathology and pathogenesis. Nat. Rev. Neurol. 8, 647–656 (2012). 54. Nathoo, N. et al. Susceptibility-weighted imaging in the experimental autoimmune encephalomyelitis model of multiple sclerosis indicates elevated deoxyhemoglobin, iron deposition and demyelination. Mult. Scler. 19, 721–731 (2013). 55. Kensler, T. W., Wakabayashi, N. & Biswal, S. Cell survival responses to environmental stresses via the Keap1–Nrf2–ARE pathway. Annu. Rev. Pharmacol. Toxicol. 47, 89–116 (2007). 56. van Horssen, J. et al. Severe oxidative damage in multiple sclerosis lesions coincides with enhanced antioxidant enzyme expression. Free Radic. Biol. Med. 45, 1729–1737 (2008). 57. Chora, A. A. et al. Heme oxygenase‑1 and carbon monoxide suppress autoimmune neuroinflammation. J. Clin. Invest. 117, 438–447 (2007). 58. Pennisi, G. et al. Redox regulation of cellular stress response in multiple sclerosis. Biochem. Pharmacol. 82, 1490–1499 (2011). 59. Johnson, D. A., Amirahmadi, S., Ward, C., Fabry, Z. & Johnson, J. A. The absence of the proantioxidant transcription factor Nrf2 exacerbates experimental autoimmune encephalomyelitis. Toxicol. Sci. 114, 237–246 (2010). 60. Linker, R. A. et al. Fumaric acid esters exert neuroprotective effects in neuroinflammation via activation of the Nrf2 antioxidant pathway. Brain 134, 678–692 (2011). 61. Ghoreschi, K. et al. Fumarates improve psoriasis and multiple sclerosis by inducing type II dendritic cells. J. Exp. Med. 208, 2291–2303 (2011). 62. Schilling, S., Goelz, S., Linker, R., Luehder, F. & Gold, R. Fumaric acid esters are effective in chronic experimental autoimmune encephalomyelitis and suppress macrophage infiltration. Clin. Exp. Immunol. 145, 101–107 (2006). 63. Lin, M. T. & Beal, M. F. Mitochondrial dysfunction and oxidative stress in neurodegenerative diseases. Nature 443, 787–795 (2006). 64. Trapp, B. D. & Stys, P. K. Virtual hypoxia and chronic necrosis of demyelinated axons in multiple sclerosis. Lancet Neurol. 8, 280–291 (2009). 65. Wallace, D. C., Fan, W. & Procaccio, V. Mitochondrial energetics and therapeutics. Annu. Rev. Pathol. 5, 297–348 (2010). 66. Trifunovic, A. et al. Premature ageing in mice expressing defective mitochondrial DNA polymerase. Nature 429, 417–423 (2004). 67. Echaniz-Laguna, A. et al. POLG1 variations presenting as multiple sclerosis. Arch. Neurol. 67, 1140–1143 (2010). 68. Kim, J. Y. et al. HDAC1 nuclear export induced by pathological conditions is essential for the onset of axonal damage. Nat. Neurosci. 13, 180–189 (2010). 69. Shindler, K. S. et al. Oral resveratrol reduces neuronal damage in a model of multiple sclerosis. J. Neuroophthalmol. 30, 328–339 (2010). 70. Park, S. J. et al. Resveratrol ameliorates agingrelated metabolic phenotypes by inhibiting cAMP phosphodiesterases. Cell 148, 421–433 (2012). 71. Forte, M. et al. Cyclophilin D inactivation protects axons in experimental autoimmune encephalomyelitis, an animal model of multiple sclerosis. Proc. Natl Acad. Sci. USA 104, 7558–7563 (2007). 72. Friese, M. A. et al. Acid-sensing ion channel‑1 contributes to axonal degeneration in autoimmune inflammation of the central nervous system. Nat. Med. 13, 1483–1489 (2007). 73. Aboul-Enein, F. et al. Preferential loss of myelinassociated glycoprotein reflects hypoxia-like white matter damage in stroke and inflammatory brain diseases. J. Neuropathol. Exp. Neurol. 62, 25–33 (2003). 74. Graumann, U., Reynolds, R., Steck, A. J. & Schaeren-Wiemers, N. Molecular changes in normal appearing white matter in multiple sclerosis are characteristic of neuroprotective mechanisms against hypoxic insult. Brain Pathol. 13, 554–573 (2003). 75. Howarth, C., Gleeson, P. & Attwell, D. Updated energy budgets for neural computation in the neocortex and cerebellum. J. Cereb. Blood Flow Metab. 32, 1222–1232 (2012). 76. Paling, D. et al. Sodium accumulation is associated with disability and a progressive course in multiple sclerosis. Brain 136, 2305–2317 (2013). www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS 77. Young, E. A. et al. Imaging correlates of decreased axonal Na+/K+ ATPase in chronic multiple sclerosis lesions. Ann. Neurol. 63, 428–435 (2008). 78. Craner, M. J. et al. Molecular changes in neurons in multiple sclerosis: altered axonal expression of Nav1.2 and Nav1.6 sodium channels and Na+/ Ca2+ exchanger. Proc. Natl Acad. Sci. USA 101, 8168–8173 (2004). 79. Alle, H., Roth, A. & Geiger, J. R. Energy-efficient action potentials in hippocampal mossy fibers. Science 325, 1405–1408 (2009). 80. Carter, B. C. & Bean, B. P. Sodium entry during action potentials of mammalian neurons: incomplete inactivation and reduced metabolic efficiency in fast-spiking neurons. Neuron 64, 898–909 (2009). 81. Hodgkin, A. The optimum density of sodium channels in an unmyelinated nerve. Philos. Trans. R. Soc. Lond. B Biol. Sci. 270, 297–300 (1975). 82. Craner, M. J., Hains, B. C., Lo, A. C., Black, J. A. & Waxman, S. G. Co-localization of sodium channel Nav1.6 and the sodium-calcium exchanger at sites of axonal injury in the spinal cord in EAE. Brain 127, 294–303 (2004). 83. O’Malley, H. A., Shreiner, A. B., Chen, G. H., Huffnagle, G. B. & Isom, L. L. Loss of Na+ channel β2 subunits is neuroprotective in a mouse model of multiple sclerosis. Mol. Cell. Neurosci. 40, 143–155 (2009). 84. Bechtold, D. A., Kapoor, R. & Smith, K. J. Axonal protection using flecainide in experimental autoimmune encephalomyelitis. Ann. Neurol. 55, 607–616 (2004). 85. Morsali, D. et al. Safinamide and flecainide protect axons and reduce microglial activation in models of multiple sclerosis. Brain 136, 1067–1082 (2013). 86. Black, J. A., Liu, S., Carrithers, M., Carrithers, L. M. & Waxman, S. G. Exacerbation of experimental autoimmune encephalomyelitis after withdrawal of phenytoin and carbamazepine. Ann. Neurol. 62, 21–33 (2007). 87. Lo, A. C., Saab, C. Y., Black, J. A. & Waxman, S. G. Phenytoin protects spinal cord axons and preserves axonal conduction and neurological function in a model of neuroinflammation in vivo. J. Neurophysiol. 90, 3566–3571 (2003). 88. Bechtold, D. A. et al. Axonal protection achieved in a model of multiple sclerosis using lamotrigine. J. Neurol. 253, 1542–1551 (2006). 89. Craner, M. J. et al. Sodium channels contribute to microglia/macrophage activation and function in EAE and MS. Glia 49, 220–229 (2005). 90. Kapoor, R. et al. Lamotrigine for neuroprotection in secondary progressive multiple sclerosis: a randomised, double-blind, placebo-controlled, parallel-group trial. Lancet Neurol. 9, 681–688 (2010). 91. Shields, S. D. et al. A channelopathy contributes to cerebellar dysfunction in a model of multiple sclerosis. Ann. Neurol. 71, 186–194 (2012). 92. Moran, M. M., McAlexander, M. A., Biro, T. & Szallasi, A. Transient receptor potential channels as therapeutic targets. Nat. Rev. Drug Discov. 10, 601–620 (2011). 93. Guinamard, R., Demion, M. & Launay, P. Physiological roles of the TRPM4 channel extracted from background currents. Physiology (Bethesda) 25, 155–164 (2010). 94. Schattling, B. et al. TRPM4 cation channel mediates axonal and neuronal degeneration in experimental autoimmune encephalomyelitis and multiple sclerosis. Nat. Med. 18, 1805–1811 (2012). 95. Dunn, J. & Blight, A. Dalfampridine: a brief review of its mechanism of action and efficacy as a treatment to improve walking in patients with multiple sclerosis. Curr. Med. Res. Opin. 27, 1415–1423 (2011). 96. Jukkola, P. I., Lovett-Racke, A. E., Zamvil, S. S. & Gu, C. K+ channel alterations in the progression of experimental autoimmune encephalomyelitis. Neurobiol. Dis. 47, 280–293 (2012). 97. Beraud, E. et al. Block of neural Kv1.1 potassium channels for neuroinflammatory disease therapy. Ann. Neurol. 60, 586–596 (2006). 98. Mathie, A. & Veale, E. L. Therapeutic potential of neuronal two-pore domain potassium-channel modulators. Curr. Opin. Investig. Drugs 8, 555–562 (2007). 99. Bittner, S. et al. TASK1 modulates inflammation and neurodegeneration in autoimmune inflammation of the central nervous system. Brain 132, 2501–2516 (2009). 100. Bittner, S. et al. The TASK1 channel inhibitor A293 shows efficacy in a mouse model of multiple sclerosis. Exp. Neurol. 238, 149–155 (2012). 101. Brand-Schieber, E. & Werner, P. Calcium channel blockers ameliorate disease in a mouse model of multiple sclerosis. Exp. Neurol. 189, 5–9 (2004). 102. Waxman, S. G. & Ritchie, J. M. Molecular dissection of the myelinated axon. Ann. Neurol. 33, 121–136 (1993). 103. Kornek, B. et al. Distribution of a calcium channel subunit in dystrophic axons in multiple sclerosis and experimental autoimmune encephalomyelitis. Brain 124, 1114–1124 (2001). 104. Gadjanski, I. et al. Role of N‑type voltagedependent calcium channels in autoimmune optic neuritis. Ann. Neurol. 66, 81–93 (2009). 105. Stirling, D. P. & Stys, P. K. Mechanisms of axonal injury: internodal nanocomplexes and calcium deregulation. Trends Mol. Med. 16, 160–170 (2010). 106. Hardingham, G. E. & Bading, H. Synaptic versus extrasynaptic NMDA receptor signalling: implications for neurodegenerative disorders. Nat. Rev. Neurosci. 11, 682–696 (2010). 107. Mahad, D. J. et al. Mitochondrial changes within axons in multiple sclerosis. Brain 132, 1161–1174 (2009). 108. Grasselli, G. et al. Abnormal NMDA receptor function exacerbates experimental autoimmune encephalomyelitis. Br. J. Pharmacol. 168, 502–517 (2013). 109. Sarchielli, P., Greco, L., Floridi, A. & Gallai, V. Excitatory amino acids and multiple sclerosis: evidence from cerebrospinal fluid. Arch. Neurol. 60, 1082–1088 (2003). 110. Piani, D., Frei, K., Do, K. Q., Cuenod, M. & Fontana, A. Murine brain macrophages induced NMDA receptor mediated neurotoxicity in vitro by secreting glutamate. Neurosci. Lett. 133, 159–162 (1991). 111. Newcombe, J. et al. Glutamate receptor expression in multiple sclerosis lesions. Brain Pathol. 18, 52–61 (2008). 112. Vercellino, M. et al. Altered glutamate reuptake in relapsing-remitting and secondary progressive multiple sclerosis cortex: correlation with microglia infiltration, demyelination, and neuronal and synaptic damage. J. Neuropathol. Exp. Neurol. 66, 732–739 (2007). 113. Hardin-Pouzet, H. et al. Glutamate metabolism is down-regulated in astrocytes during experimental allergic encephalomyelitis. Glia 20, 79–85 (1997). 114. Ohgoh, M. et al. Altered expression of glutamate transporters in experimental autoimmune encephalomyelitis. J. Neuroimmunol. 125, 170–178 (2002). NATURE REVIEWS | NEUROLOGY 115. Pitt, D., Werner, P. & Raine, C. S. Glutamate excitotoxicity in a model of multiple sclerosis. Nat. Med. 6, 67–70 (2000). 116. Smith, T., Groom, A., Zhu, B. & Turski, L. Autoimmune encephalomyelitis ameliorated by AMPA antagonists. Nat. Med. 6, 62–66 (2000). 117. Kanwar, J. R., Kanwar, R. K. & Krissansen, G. W. Simultaneous neuroprotection and blockade of inflammation reverses autoimmune encephalomyelitis. Brain 127, 1313–1331 (2004). 118. Paul, C. & Bolton, C. Modulation of blood–brain barrier dysfunction and neurological deficits during acute experimental allergic encephalomyelitis by the N‑methyl‑d-aspartate receptor antagonist memantine. J. Pharmacol. Exp. Ther. 302, 50–57 (2002). 119. Wallstrom, E. et al. Memantine abrogates neurological deficits, but not CNS inflammation, in Lewis rat experimental autoimmune encephalomyelitis. J. Neurol. Sci. 137, 89–96 (1996). 120. Centonze, D. et al. Inflammation triggers synaptic alteration and degeneration in experimental autoimmune encephalomyelitis. J. Neurosci. 29, 3442–3452 (2009). 121. Basso, A. S. et al. Reversal of axonal loss and disability in a mouse model of progressive multiple sclerosis. J. Clin. Invest. 118, 1532–1543 (2008). 122. Wemmie, J. A., Taugher, R. J. & Kreple, C. J. Acid-sensing ion channels in pain and disease. Nat. Rev. Neurosci. 14, 461–471 (2013). 123. Yermolaieva, O., Leonard, A. S., Schnizler, M. K., Abboud, F. M. & Welsh, M. J. Extracellular acidosis increases neuronal cell calcium by activating acid-sensing ion channel 1a. Proc. Natl Acad. Sci. USA 101, 6752–6757 (2004). 124. Vergo, S. et al. Acid-sensing ion channel 1 is involved in both axonal injury and demyelination in multiple sclerosis and its animal model. Brain 134, 571–584 (2011). 125. Arun, T. et al. Targeting ASIC1 in primary progressive multiple sclerosis: evidence of neuroprotection with amiloride. Brain 136, 106–115 (2013). 126. Hassen, G. W., Feliberti, J., Kesner, L., Stracher, A. & Mokhtarian, F. Prevention of axonal injury using calpain inhibitor in chronic progressive experimental autoimmune encephalomyelitis. Brain Res. 1236, 206–215 (2008). 127. Shields, D. C., Tyor, W. R., Deibler, G. E., Hogan, E. L. & Banik, N. L. Increased calpain expression in activated glial and inflammatory cells in experimental allergic encephalomyelitis. Proc. Natl Acad. Sci. USA 95, 5768–5772 (1998). 128. Guyton, M. K. et al. Upregulation of calpain correlates with increased neurodegeneration in acute experimental auto-immune encephalomyelitis. J. Neurosci. Res. 81, 53–61 (2005). 129. Offen, D. et al. Mice overexpressing Bcl‑2 in their neurons are resistant to myelin oligodendrocyte glycoprotein (MOG)-induced experimental autoimmune encephalomyelitis (EAE). J. Mol. Neurosci. 15, 167–176 (2000). 130. Aktas, O. et al. Neuronal damage in autoimmune neuroinflammation mediated by the death ligand TRAIL. Neuron 46, 421–432 (2005). 131. Chitnis, T. et al. Elevated neuronal expression of CD200 protects Wlds mice from inflammationmediated neurodegeneration. Am. J. Pathol. 170, 1695–1712 (2007). 132. Saxena, S. & Caroni, P. Selective neuronal vulnerability in neurodegenerative diseases: from stressor thresholds to degeneration. Neuron 71, 35–48 (2011). VOLUME 10 | APRIL 2014 | 237 © 2014 Macmillan Publishers Limited. All rights reserved REVIEWS 133. Kemp, J. A. & McKernan, R. M. NMDA receptor pathways as drug targets. Nat. Neurosci. 5 (Suppl.), 1039–1042 (2002). 134. Stranahan, A. M. & Mattson, M. P. Recruiting adaptive cellular stress responses for successful brain ageing. Nat. Rev. Neurosci. 13, 209–216 (2012). 135. Prakash, R. S., Snook, E. M., Motl, R. W. & Kramer, A. F. Aerobic fitness is associated with gray matter volume and white matter integrity in multiple sclerosis. Brain Res. 1341, 41–51 (2010). 136. Briken, S. et al. Effects of exercise on fitness and cognition in progressive MS: a randomized, controlled pilot trial. Mult. Scler. http:// dx.doi.org/10.1177/1352458513507358. 137. Rossi, S. et al. Exercise attenuates the clinical, synaptic and dendritic abnormalities of experimental autoimmune encephalomyelitis. Neurobiol. Dis. 36, 51–59 (2009). 138. Safdar, A. et al. Endurance exercise rescues progeroid aging and induces systemic mitochondrial rejuvenation in mtDNA mutator mice. Proc. Natl Acad. Sci. USA 108, 4135–4140 (2011). 139. Maresz, K. et al. Direct suppression of CNS autoimmune inflammation via the cannabinoid receptor CB1 on neurons and CB2 on autoreactive T cells. Nat. Med. 13, 492–497 (2007). 140. Kaneko, S. et al. Protecting axonal degeneration by increasing nicotinamide adenine dinucleotide levels in experimental autoimmune encephalomyelitis models. J. Neurosci. 26, 9794–9804 (2006). 141. Dutta, R. et al. Mitochondrial dysfunction as a cause of axonal degeneration in multiple sclerosis patients. Ann. Neurol. 59, 478–489 (2006). 142. Campbell, G. R. et al. Mitochondrial DNA deletions and neurodegeneration in multiple sclerosis. Ann. Neurol. 69, 481–492 (2011). 143. Mahad, D., Ziabreva, I., Lassmann, H. & Turnbull, D. Mitochondrial defects in acute multiple sclerosis lesions. Brain 131, 1722–1735 (2008). 144. Zambonin, J. L. et al. Increased mitochondrial content in remyelinated axons: implications for multiple sclerosis. Brain 134, 1901–1913 (2011). 145. Linker, R. A. et al. CNTF is a major protective factor in demyelinating CNS disease: a neurotrophic cytokine as modulator in 238 | APRIL 2014 | VOLUME 10 neuroinflammation. Nat. Med. 8, 620–624 (2002). 146. Linker, R. A. et al. Functional role of brain-derived neurotrophic factor in neuroprotective autoimmunity: therapeutic implications in a model of multiple sclerosis. Brain 133, 2248–2263 (2010). 147. Lu, B., Nagappan, G., Guan, X., Nathan, P. J. & Wren, P. BDNF-based synaptic repair as a disease-modifying strategy for neurodegenerative diseases. Nat. Rev. Neurosci. 14, 401–416 (2013). 148. Petryshen, T. L. et al. Population genetic study of the brain-derived neurotrophic factor (BDNF) gene. Mol. Psychiatry 15, 810–815 (2010). 149. Zivadinov, R. et al. Preservation of gray matter volume in multiple sclerosis patients with the Met allele of the rs6265 (Val66Met) SNP of brain-derived neurotrophic factor. Hum. Mol. Genet. 16, 2659–2668 (2007). 150. Ramasamy, D. P. et al. Effect of Met66 allele of the BDNF rs6265 SNP on regional gray matter volumes in patients with multiple sclerosis: a voxel-based morphometry study. Pathophysiology 18, 53–60 (2011). 151. Nagahara, A. H. & Tuszynski, M. H. Potential therapeutic uses of BDNF in neurological and psychiatric disorders. Nat. Rev. Drug Discov. 10, 209–219 (2011). 152. Stadelmann, C. et al. BDNF and gp145trkB in multiple sclerosis brain lesions: neuroprotective interactions between immune and neuronal cells? Brain 125, 75–85 (2002). 153. Kerschensteiner, M. et al. Activated human T cells, B cells, and monocytes produce brainderived neurotrophic factor in vitro and in inflammatory brain lesions: a neuroprotective role of inflammation? J. Exp. Med. 189, 865–870 (1999). 154. Lee, D. H. et al. Central nervous system rather than immune cell-derived BDNF mediates axonal protective effects early in autoimmune demyelination. Acta Neuropathol. 123, 247–258 (2012). 155. Colombo, E. et al. Stimulation of the neurotrophin receptor TrkB on astrocytes drives nitric oxide production and neurodegeneration. J. Exp. Med. 209, 521–535 (2012). 156. Jones, J. L. et al. Improvement in disability after alemtuzumab treatment of multiple sclerosis is associated with neuroprotective autoimmunity. Brain 133, 2232–2247 (2010). 157. Thone, J. et al. Modulation of autoimmune demyelination by laquinimod via induction of brain-derived neurotrophic factor. Am. J. Pathol. 180, 267–274 (2012). 158. Marsicano, G. et al. CB1 cannabinoid receptors and on-demand defense against excitotoxicity. Science 302, 84–88 (2003). 159. Pryce, G. et al. Cannabinoids inhibit neurodegeneration in models of multiple sclerosis. Brain 126, 2191–2202 (2003). 160. Rossi, S. et al. Cannabinoid CB1 receptors regulate neuronal TNF‑α effects in experimental autoimmune encephalomyelitis. Brain Behav. Immun. 25, 1242–1248 (2011). 161. Croxford, J. L. et al. Cannabinoid-mediated neuroprotection, not immunosuppression, may be more relevant to multiple sclerosis. J. Neuroimmunol. 193, 120–129 (2008). 162. Zajicek, J. et al. Effect of dronabinol on progression in progressive multiple sclerosis (CUPID): a randomised, placebo-controlled trial. Lancet Neurol. 12, 857–865 (2013). 163. Broxmeyer, H. E. Erythropoietin: multiple targets, actions, and modifying influences for biological and clinical consideration. J. Exp. Med. 210, 205–208 (2013). 164. Li, W. et al. Beneficial effect of erythropoietin on experimental allergic encephalomyelitis. Ann. Neurol. 56, 767–777 (2004). 165. Suhs, K. W. et al. A randomized, double-blind, phase 2 study of erythropoietin in optic neuritis. Ann. Neurol. 72, 199–210 (2012). Acknowledgements M.A.F. is supported by the Deutsche Forschungsgemeinschaft Emmy Noether-Programme (FR1720/3‑1), Gemeinnützige Hertie-Stiftung (1.01.1/11/003 and P1130075), Werner Otto Stiftung (1/81), Forschungs- und Wissenschaftsstiftung Hamburg, Boehringer Ingelheim Stiftung Exploration Grant and BMBF Biopharma (NEU2 programme). L.F. is supported by the Wellcome Trust, the Medical Research Council, the Lundbeck Foundation and the Naomi Bransom Foundation. Author contributions M.A.F. researched most of the data and drafted the article with substantial contributions from B.S. and L.F. All authors contributed to discussion of the content, reviewing, and editing of the manuscript before submission. Supplementary information is linked to the online version of the paper at www.nature.com/nrneurol. www.nature.com/nrneurol © 2014 Macmillan Publishers Limited. All rights reserved