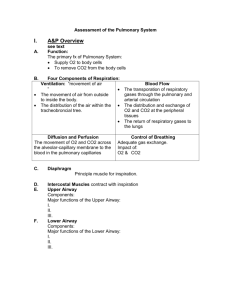
Health Assessment THORACIC AND LUNGS ASSESSMENT 2/23/23 BY MARK B SAMSON & MARJ SIBAYAN LEARNING OBJECTIVES On completion of this topic, the students will be able to: 1. Describe the structures and functions of the thorax and lungs 2. Describe the factors involve in inspiration and expiration 3. Differentiate oxygen transport, ventilation and respiration and gas exchange 4. Discriminate between normal and adventitious sounds 5. Use techniques of examination appropriate for determining the normal and abnormal findings. 2/23/23 THORAX AND LUNGS 2/23/23 2/23/23 2/23/23 VERTICAL LINES 2/23/23 2/23/23 2/23/23 LOBES 2/23/23 2/23/23 2/23/23 PLEURAL MEMBRANES 2/23/23 2/23/23 MECHANICS OF BREATHING 2/23/23 2/23/23 COLLECTING SUBJECTIVE DATA: THE NURSING HEALTH HISTORY 2/23/23 HISTORY OF PRESENT HEALTH CONCERN QUESTION Difficulty of Breathing • Experience difficulty breathing RATIONALE • Indicates a number of health problems most of which related to respiratory system • Other symptoms • Provide clues to other to the underlying problems • DOB when resting or doing activities • For aging person – changes in lungs • DOB when sleeping • Orthopnea may be associated with heart failure • Snore or apnea episode when sleeping • May account for fatigue or excessive tiredness, depression, etc. 2/23/23 Question Chest pain • Chest pain and associated other symptoms Cough • When and how often Rationale • Pain-sensitive nerve endings are located in the parietal pleura, thoracic muscles and tracheobronchial tree • Continuous coughs are usually associated with acute infection • Presence of sputum, color, amount, increased or decreased recently, odor • Non-productive are often associated with upper respiratory irritations or early CHF. • White – common colds, viral infections or bronchitis • Yellow or green – bacterial infection • Wheezing when coughing • Indicates of narrowing of the airways due to spasm or obstruction Gastrointestinal symptoms • Heartburn, frequent hiccups, chronic coughs • Studies have shown that patients with asthma often have GERD 2/23/23 PAST HEALTH HISTORY Question Rationale • Respiratory problems • Increase the risk for recurrence • Thoracic surgery, biopsy, or trauma • May alter the appearance of the thorax and cause changes in respiratory sounds • Diagnosed with allergies • Allergic responses are manifested with respiratory symptoms • CXR, TB skin test, influenza immunization • Useful for comparison with current findings and give information • Travel to high-risk areas for SARS • May have exposed the client to SARS 2/23/23 FAMILY HISTORY Question Rationale • Lung disease in the family • lung cancer is thought to be partially based on genetic, other respiratory diseases may increase the risk • Members in the family in the home smoke • Risk for emphysema or lung cancer later in life • Other pulmonary illnesses/disorders in the family • Tend to run in families 2/23/23 Question LIFESTYLE AND HEALTH Rationale PRACTICES • Cigarettes or other tobacco smoking • High risk to develop lung cancer and other smoking-related respiratory problems • Environmental, second-hand smoker • Increased incidence of certain respiratory conditions • Difficulty performing usual daily activities. Describe. • Respiratory problems can negatively affect person’s ability to perform the usual ADL. • Stress • Manifestation of stress • Treatment or medication for breathing problems • Could be attributed to adverse reaction • Herbal medicines or alternative therapies to manage colds or respiratory problems • To check for side effects or adverse interaction with prescribed medications 2/23/23 RISK FACTORS – LUNG CANCER 2/23/23 COLLECTING OBJECTIVE DATA: PHYSICAL EXAMINATION 2/23/23 GENERAL ASSESSMENT Assessment Procedure Normal Findings Abnormal Findings Inspect for nasal flaring and pursed lip breathing Nasal flaring is not observed. Normally the diaphragm and the external intercostal muscles do most of the work of breathing. This is evidence by outward expansion of the abdomen and lower ribs on inspiration and return to resting position on expiration. Nasal flaring is seen with labored respirations. Pursed lip breathing may be seen in asthma, emphysema or CHF Observe color of face, lips, and chest. Does not use accessory muscle but the diaphragm muscle as evidence of expansion of lower chest during inspiration. Trapezius are used to facilitate inspiration in cases of acute and chronic airway obstruction Inspect color and shape of nails. Pink tones should be seen in the nailbeds. There is normally a 160-degree angle between the nail base and the skin. Pale or cyanosis nails may indicate hypoxia. Early clubbing can occur from hypoxia. 2/23/23 POSTERIOR THORAX (INSPECTION) Assessment Procedure Normal Findings Abnormal Findings Inspect configuration Scapulae are symmetric and non-protruding. Shoulders and scapulae at equal horizontal position. Spinous processes appear straight, and thorax appears symmetric with ribs sloping downward at approximately a 45-degree angle in relation to the spine. • Spinous processes that deviate laterally in the thoracic area may indicate scoliosis. • Ribs appearing horizontal at an angle greater than 45 degrees with spinal column resulted to barrel chest. Observe use of accessory muscles Does not use accessory muscle but the diaphragm muscle as evidence of expansion of lower chest during inspiration. Trapezius are used to facilitate inspiration in cases of acute and chronic airway obstruction Inspect the client’s positioning Client should be silting up and relaxed, breathing easily Client leans forward and uses arms to support weight and lift chest to increase breathing capacity (COPD). 2/23/23 Assessment Procedure POSTERIOR THORAX Normal Findings Abnormal Findings (PALPATION) Palpate for tenderness and sensation No tenderness, pain or unusual sensations. Temperature should be equal bilaterally. Tender or painful areas may indicate inflamed fibrous connective tissues. Pain from ICS may be from inflamed pleurae. Pain on ribs is symptom of fractured ribs. Palpate surface characteristics Skin and subcutaneous tissue are free of lesions and masses To be evaluated further by a physician Palpate for fremitus Fremitus is symmetric and easily identified in the upper regions of the lungs Unequal is usually the result of consolidation or bronchial obstruction, air trapping in emphysema, pleural effusion, or pneumothorax 2/23/23 POSTERIOR THORAX (PALPATION) Assessment Procedure Assess chest expansion Normal Findings Client takes a deep breath, examiner’s thumb should move 5-10 cm apart symmetrically Abnormal Findings Unequal – severe atelectasis, pneumonia, chest trauma, or pneumothorax 2/23/23 POSTERIOR THORAX (PERCUSSION) Assessment Procedure Normal Findings Abnormal Findings Percuss for tone Resonance is the percussion tone over normal lung tissue. Hyperresonance in cases of trapped air such as in emphysema or pneumothorax. Percuss for diaphragmatic excursion Excursion should be Descent may be limited equally bilaterally and by atelectasis of the measure 3-5 cm in adults lower lobes or by emphysema in which diaphragmatic movement and air trapping are minimal. 2/23/23 POSTERIOR THORAX (AUSCULTATION Assessment Procedure Normal Findings Abnormal Findings Auscultate for breath sounds Normal breath sounds Diminished or absent sounds indicate that little or no air is moving in and out of the lung area. Auscultate for adventitious sound No adventitious sounds Adventitious sounds Auscultate voice sounds. Bronchopony Voice transmission is soft, muffled, and indistinct The words are easily understood and louder over areas of increased density. Egophony Voice transmission will be soft and muffled but the letter “E” should be distinguishable Over areas of consolidation or compression, the sound is louder and sounds like “A” Whispered Pectoriloquy Transmission of sound is very faint and muffled. It may be inaudible. Over areas of consolidation or compression, the sound is transmitted clearly and distinctly. 2/23/23 ANTERIOR THORAX (INSPECTION) Assessment Procedure Normal Findings Abnormal Findings Inspect for shape and configuration The anteroposterior diameter is less than the transverse diameter Anteroposterior equals transverse diameter, resulting in barrel chest Inspect position of the sternum Positioned at midline and straight Pectus excavatum, pectus carinatum Ribs slope downward with symmetric intercostal spaces. Barrel chest configuration results in a more horizontal position of the ribs Labored and noisy breathing •Inspect intercostal space • Respirations are relaxed, effortless, and quiet • No retractions or bulging of ICS • Retraction – increased inspiratory effort Bulging – emphysema and asthma Observe for use of accessory muscle Not seen with normal respiratory effort Used to facilitate inspiration Inspect slope of the ribs 2/23/23 ANTERIOR THORAX (PALPATION) Assessment Procedure Normal Findings Abnormal Findings Palpate for tenderness, sensation and surface masses No tenderness or pain Tenderness over thoracic muscles can result from exercising Palpate for fremitus Fremitus is symmetric and easily identified in the upper region of lungs. Diminished vibrations even with loud spoken voice Palpate anterior chest expansion Thumbs move outward in a symmetric fashion from the midline Unequal chest expansion 2/23/23 ANTERIOR THORAX (PERCUSSION) Assessment Procedure Percuss for tone Normal Findings Resonance Abnormal Findings Hyperresonance 2/23/23 ANTERIOR THORAX (AUSCULTATION) Assessment Procedure Auscultate for anterior breath sounds, adventitious sounds, and voice sounds Normal Findings Depict locations for normal breath sounds Abnormal Findings •Adventitious sounds 2/23/23 TECHNIQUES OF EXAMINATION Tool for Assessment §IPPA 2/23/23 POSITION OF THE CLIENT Posterior thorax and lungs § Sitting position with client’s arm folded across the chest with hands resting on the opposite shoulder 2/23/23 POSITION OF THE CLIENT Anterior thorax and lungs § Supine 2/23/23 GENERAL INSPECTION • Inspect the client’s posture 2/23/23 GENERAL INSPECTION Funnel chest Pigeon chest 2/23/23 Barrel chest GENERAL INSPECTION 2/23/23 GENERAL INSPECTION Scoliosis 2/23/23 Kyphosis GENERAL INSPECTION Lordosis 2/23/23 GENERAL INSPECTION Use of Accesory Muscle 2/23/23 Check respiration rate, depth and rhythm • Eupnea Observe color of the face,lips and chest. Inspect color of the nails • Tachypnea • Bradypnea • Apnea 2/23/23 POSTERIOR THORAX (INSPECTION) Inspect for posterior and lateral views 2/23/23 POSTERIOR THORAX (INSPECTION) 2/23/23 2/23/23 POSTERIOR THORAX (PALPATION) • Identify for tender areas, presence of pain 2/23/23 POSTERIOR THORAX (PALPATION) 2/23/23 POSTERIOR THORAX (PALPATION) Chest Expansion • Place your thumb at about the level of the 10th ribs • Ask the patient to inhale deeply 2/23/23 POSTERIOR THORAX (PALPATION) Tactile Fremitus • Use bony part of the palm or ulnar side of the hand • Ask the patient to repeat the words ninety-nine 2/23/23 2/23/23 2/23/23 2/23/23 POSTERIOR THORAX (PERCUSSION) 2/23/23 POSTERIOR THORAX (PERCUSSION) 2/23/23 POSTERIOR THORAX (PERCUSSION) • Identify the percussion notes and the area where it is heard 2/23/23 POSTERIOR THORAX (PERCUSSION) • Percuss using the ladder pattern 2/23/23 POSTERIOR THORAX (PERCUSSION) Diagphragmatic Excursion 2/23/23 2/23/23 POSTERIOR THORAX (AUSCULATATION) • Auscultate for vesicular sound, bronchovesicular sound and bronchial sound • Listen with the diaphragm of the stethoscope after instructing the patient to breath deeply through an open mouth • Note the intensity of the breath sounds 2/23/23 POSTERIOR THORAX (AUSCULATATION • Auscultate for bronchovesicular and vesicular breath sounds posteriorly 2/23/23 ANTERIOR THORAX (INSPECTION) • Check for deformities and asymmetry • Check for abnormal retraction of the lower interspaces during inspiration 2/23/23 ANTERIOR THORAX (PALPATION) • Identify of tender areas, mass and presence of pain 2/23/23 ANTERIOR THORAX (PALPATION) Chest Expansion • Place the thumbs along the costal margin, hands along the lateral rib cage • Instruct the patient to take some deep breathing 2/23/23 ANTERIOR THORAX (PALPATION) Tactile Fremitus • Compare both sides of the chest, using the ball or ulnar surface of your hand. 2/23/23 2/23/23 2/23/23 ANTERIOR THORAX (PERCUSSION) 2/23/23 ANTERIOR THORAX (AUSCULTATION) 2/23/23 ANTERIOR THORAX (AUSCULTATION) • Auscultate for vesicular sound, bronchovesicular sound and bronchial sound • Listen with the diaphragm of the stethoscope after instructing the patient to breath deeply through an open mouth • Note the intensity of the breath sounds 2/23/23 ANTERIOR THORAX (AUSCULTATION) 2/23/23 ANTERIOR THORAX (AUSCULTATION) • Review normal and adventitious breath sounds in the video 2/23/23 2/23/23 2/23/23