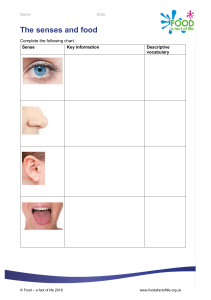
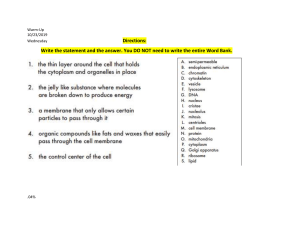
Chapter 24 Conditions in the Newborn Related to Gestational Age, Size, Injury, and Pain Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Preterm Infants ❖ Approximately 11.6% of babies are born before 37 weeks every year in the United States. ❖ Of those babies, 3.4% are born before 34 weeks. ❖ Preterm babies face many challenges including: o Respiratory distress syndrome (RDS) o Intraventricular hemorrhage (IVH) ❖ Risks for prematurity are many and include: o Infection o Fetal anomalies o Preeclampsia/eclampsia “Connor”-26 wks.-<11oz Copyright © 2019 Wolters Kluwer • All Rights Reserved Preterm Infants: Terminology #1 AGA SGA LGA Growth Copyright © 2019 Wolters Kluwer • All Rights Reserved Late Preterm Infants ❖ Infants born from 34-0/7 to 36-6/7 weeks are considered late preterm. ❖ Although their size may appear to be term, late preterm infants have higher morbidity and mortality due to immaturity. ❖ Late preterm infants are at high risk for: o Hypothermia o Hypoglycemia o Respiratory distress o Jaundice o Feeding difficulties ❖ Late preterm infants may appear to be feeding appropriately but have difficulties related to the inability to coordinate sucking, swallowing, and breathing. Copyright © 2019 Wolters Kluwer • All Rights Reserved Postterm Infants ❖ Postterm infants are born beyond 42 weeks of gestation. ❖ Postterm infants may be macrosomic or small for gestational age (SGA) because of the aging placenta. ❖ Complications for postterm infants include: o Birth injuries o Oligohydramnios o Low Apgar scores o Cerebral palsy ❖ Meconium aspiration ❖ Almost leather-like, dry, cracked skin, insignificant vernix caseosa. Copyright © 2019 Wolters Kluwer • All Rights Reserved Small or Large for Gestational Age (SGA or LGA) Infants ❖ SGA infants may be normal based on ethnicity or the height and weight of the parents or it could be due to environmental or pathologic genetic reasons. o At risk for hypoglycemia, polycythemia (resulting from hypoxia in utero), or hypocalcemia (potentially caused by perinatal asphyxia, hypoparathyroidism, or maternal diabetes). ❖ LGA infants are at high risk for birth injury, perinatal asphyxia, and hypoglycemia. o Common in infants of mothers with obesity, diabetes, and excessive weight gain in pregnancy. Copyright © 2019 Wolters Kluwer • All Rights Reserved Birth Injuries #1 ❖ Newborns should be assessed for birth injuries such as: o Bruising – generally self-limiting but may contribute to hyperbilirubinemia. o Lacerations—may be obtained during a cesarean or operative vaginal delivery. May be serious enough to require plastic surgery. o Fractures—most common is a clavicle fracture and generally heals spontaneously. o Subconjunctival hemorrhage—looks alarming (ocular bleed) but are very common in neonates and resolve spontaneously within 2 weeks. Copyright © 2019 Wolters Kluwer • All Rights Reserved Birth Injuries #2 ❖ Brachial plexus injury – typically unilateral nerve damage from stretching and traction on the brachial plexus. May heal without treatment. ❖ Facial nerve trauma – due to prolonged pressure against maternal pelvis or forceps delivery. There are reduced movement on the side of the injury, may heal in a few hours or may take months. Facial nerve trauma may cause feeding difficulties. ❖ Spinal cord injury – rare but may be caused by forceps or vaginal breech delivery. Prognosis depends on the location and severity of the injury. Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Pain ❖ Infants admitted to the NICU experience an average of 5 to 15 painful procedures every day. ❖ Pain should be treated anticipately when possible. ❖ Pain management for neonates include: o Breastfeeding o Nonnutritive sucking (pacifier) o Skin-to-skin contact o Oral sucrose o Topical anesthesia o Acetaminophen or opioid analgesics o Nerve block with lidocaine Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Pain Assessment Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #3 A preterm infant is scheduled to have a new peripheral IV line inserted. How might the nurse best address pain related to this procedure? A. Observe the infant for signs of pain during the procedure. B. Understand that neonates do not experience pain. C. Swaddle the infant and provide a pacifier before the procedure. D. Administer opioid analgesics prior to the procedure. Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Intensive Care Equipment #1 ❖ The neonatal intensive care unit (NICU) can be stressful. ❖ Nasogastric tubes are used for feeding and for gastric suction. ❖ An umbilical artery catheter: placed in the umbilical stump to one of the two umbilical arteries and into the aorta. Used to monitor arterial blood glasses. ❖ An umbilical vein catheter : placed into the umbilical stump to the ductus venosus and into the inferior vena cava. Used for fluid and medication administration and can be used for blood pressure monitoring. https://youtu.be/G0oPnF3IqK4 ❖ Both are rarely left in place more than 1 week. Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Intensive Care Equipment #2 ❖ Peripherally inserted central line (PICC) is used when intermediateterm intravenous (IV) access is required. ❖ Nasal canula (NC) are available in different sizes and allows for visualization of the baby’s face. ❖ Continuous positive airway pressure (CPAP) is useful for infants unable to obtain adequate oxygenation by nasal canula alone. ❖ An endotracheal tube (ET) is placed by intubation through the infant's mouth. The ET tube is then attached to a ventilator. ❖ An oxygen hood is for infants who do not need supplemental oxygen pressure. If the infant is removed from the hood (for example, during a feeding) oxygen should be supplied by NC. Copyright © 2019 Wolters Kluwer • All Rights Reserved Chapter 25 Acquired Conditions and Congenital Abnormalities in the Newborn Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Hyperbilirubinemia in the Newborn ❖ Hyperbilirubinemia is a bilirubin serum >5 ml/dL. ❖ Bilirubin comes from the breakdown of red blood cells (unconjugated). Is bound to albumin and transferred to liver for conjugation. o conjugated will be excreted normally ( becomes water soluble), excreted poop and pee. o unconjugated bilirubin remains in the blood stream to cause the jaundice. Can deposit in the brain tissue causing damage (kernicterus) intellectual deficit, death. ❖ Jaundice is from head to toe (progressive) ❖ Hyperbilirubinemia is common in newborns and is known as physiologic jaundice but can also be pathologic . Copyright © 2019 Wolters Kluwer • All Rights Reserved Physiologic Jaundice #1 ❖ physiologic (after 24 hrs. of live) results from: o Newborn's shortened red blood cell lifespan and breakdown of fetal RBC’s o Live immaturity ❖ pathologic jaundice (within 24 hrs. of live) results form an underlying disease. o Caused by a blood group incompatibility (ABO), infections, or RBC disorders. ❖ To prevent complications, the nurse should carefully assess infant feeding and ensure frequent feedings. Copyright © 2019 Wolters Kluwer • All Rights Reserved Pathologic Jaundice #2 Copyright © 2019 Wolters Kluwer • All Rights Reserved Jaundice: Assessments ❖ A assess all infants after birth for jaundice by visual inspection every 8 to 12 hours. ❖ Expects yellowish tint to skin, sclera and mucous membranes ❖ Check mom and baby blood type. ❖ Direct Coombs test is a blood test to check for hemolytic disease of newborn (determine the cause). o Done on the baby’s cord blood to detect antibody coated RH positive red blood cells. ❖ Screen infants by transcutaneous bilirubin (TcB) measurements. Results are often confirmed by total serum bilirubin (TSB) measurements. ❖ Preterm infants are at higher risk for pathologic jaundice. Copyright © 2019 Wolters Kluwer • All Rights Reserved Copyright © 2019 Wolters Kluwer • All Rights Reserved Jaundice: Treatments ❖ The goal of treating hyperbilirubinemia is to avoid kernicterus o Fatty portion of bilirubin attaches the brain basal ganglia. o Causes neurological damage. o Can cause Cerebral Palsy baby o Occurs if Bili is > 20ml/dl ❖ Phototherapy used in hospital or home, exposes the infant's skin to a particular wavelength of light. This exposure converts the bilirubin to a water-soluble form that can be excreted in bile or urine. o Phototherapy blankets o Single or double banks. ❖ Copyright © 2019 Wolters Kluwer • All Rights Reserved Jaundice: Treatments ❖ Nurses monitor the infant’s temperature, serum bilirubin, hydration status, and exposure time during phototherapy. ❖ Cover the eyes, avoid lotions, minimal clothing (diapers only) ❖ Phototherapy Side Effects: diarrhea, increased insensible water loss, skin rash, and transient bronzing of the skin . ❖ Exchange transfusion effectively removes bilirubin from the circulation but is expensive, requires clinical expertise, and is rarely used. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #1 A 39-week infant had a tachycardic fetal heart rate (FHR) baseline and persistent variable decelerations during labor. The infant has a cephalohematoma from a vacuum-assisted delivery and is exclusively formula feeding. Which of the following predisposes the infant to hyperbilirubinemia? A. Tachycardic FHR baseline B. Variable decelerations in labor C. A cephalohematoma D. Exclusive formula feeding Copyright © 2019 Wolters Kluwer • All Rights Reserved Cold Stress ❖ Occurs with uncontrolled hypothermia when blood vessels constrict to conserve heat. The metabolic rate increases as does oxygen consumption. ❖ Prolonged cold stress can lead to o respiratory distress, acidosis, hypoglycemia, and reopening or failure to close of the ductus arteriosus. ❖ Treatment o Monitor for skin pallor with mottling and cyanotic trunk, tachypnea o Warm slowly over a period of 2-4 hrs. o Give o2 Copyright © 2019 Wolters Kluwer • All Rights Reserved Hypoglycemia ❖ Hypoglycemia in the newborn is defined as a blood sugar less than 40 mg/dl. ❖ Symptoms: o Hypotonic, lethargy, Tremors, o Irritability, Seizures o Temperature instability o Poor feeding, Vomiting ❖ Monitor as per facility protocol. ❖ Infants with mild hypoglycemia should have early feedings ❖ Give Iv dextrose for a symptomatic newborn or TPN Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #2 A nurse is caring for a newborn who is 4 hr. old and has a bedside glucometer reading of 68 mg/ dL. The newborn’s mother has type 2 diabetes mellitus. Which of the following actions should the nurse take? A. Obtain a blood sample for a serum glucose level B. Feed the newborn immediately C. Administer 30 mL of dextrose solution IV D. Reassess the blood glucose level prior to the next feeding Copyright © 2019 Wolters Kluwer • All Rights Reserved Respiratory Distress Syndrome (RDS) and Apnea ❖ (RDS) is the respiratory condition most associated with prematurity. o Is caused by surfactant insufficiency, immature lungs, regardless of newborn birth weight. o Symptoms include tachypnea, nasal flaring, expiratory grunting, retractions, cyanosis, and pallor. o Treated with assisted ventilation, surfactant, and supportive therapy. ❖ Apnea is common and significant if : breathing stops for more than 20 seconds or with either a Heart Rate less than 70 to 80 bpm or oxygen saturation below 80% to 85%. Copyright © 2019 Wolters Kluwer • All Rights Reserved Respiratory Distress Syndrome (RDS) # 2 ❖ Conditions causing RDS include: o Bronchopulmonary dysplasia (BPD) causes the lungs are stiff and noncompliant requiring treatment complication of artificial respiratory support. o Persistent Pulmonary Hypertension of the Neonate (PPHN)is a left to right shunting and hypoxia, underdeveloped or abnormal pulmonary vascular, or lung disease. o Transient tachypnea of the newborn (TTN) form of pulmonary edema resulting from failure to clear fluid from the lungs o Meconium Aspiration Syndrome (MAS); aspiration of meconium in the fetal lungs resulting in airway obstruction, inflammation and chemical irritation, infection, and inactivation of surfactant. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #3 ❖ A neonatal intensive care nurse monitors patients for what signs of respiratory distress syndrome? A. Nasal flaring B. Expiratory grunting C. Use of accessory muscles to breathe D. All of the above Copyright © 2019 Wolters Kluwer • All Rights Reserved Retinopathy of Prematurity (ROP) ❖ (ROP) is a leading cause of blindness in children in the United States. o caused by abnormal vascular growth of the blood vessels of the retina in infants born prematurely. o Linked to resuscitation method ❖ Complications associated with oxygen administration to the newborn can cause mild to severe eye and vision problems ❖ Keep target oxygenation to no more than 90%. ❖ Eval Ophthalmology Pediatrician before 30 wks Copyright © 2019 Wolters Kluwer • All Rights Reserved Patent ductus arteriosus (PDA). ❖ A common cardiovascular issue. ❖ Occurs when the ductus arteriosus reopens after birth due to neonatal hypoxia or when the it does not close after birth. • Extra blood gets pumped from the body artery (aorta) into the lung (pulmonary) arteries. ❖ Signs and symptoms: o Systolic murmur o Ventricular dilation o Cyanosis ❖ Treatment include diuretics, ibuprofen or indomethacin. ECHO, cardiac counseling . ❖ Infants who do not respond to medications may need surgery. Copyright © 2019 Wolters Kluwer • All Rights Reserved Intraventricular hemorrhage (IVH) ❖ Bleeding in or around ventricles of the brain and s one of the most common and dangerous causes of brain injury. ❖ Treatment incudes supportive care such as o avoiding hyper- or hypotension, o providing adequate oxygen and nutrition, o and treat seizures to avoid alterations in cerebral blood flow. o Minimal TOUCH Copyright © 2019 Wolters Kluwer • All Rights Reserved Necrotizing Enterocolitis (NEC) ❖ (NEC) is ischemic necrosis of the intestines and a gastrointestinal emergency. ❖ Most infants with NEC appear healthy. Predominantly in preterm infants. ❖ The first sign of a problem is typically a feeding intolerance. ❖ Other signs of NEC include: Abdominal distension, discoloration, loops • • Hypotension • Temperature instability • Respiratory failure • Vomiting, bloody stools ❖ Treatment includes antibiotics, laboratory monitoring (CBC, electrolytes, BUN, creatinine, and acid base studies), radiographic monitoring every 6 to 12 hours (monitors progression), and bowel resection surgery. ❖ Put newborn NPO , give TPN and connect to a low suction gastric decompression. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #4 ❖ Necrotizing enterocolitis (NEC) is an inflammatory disease of the gastrointestinal mucosa. The signs of NEC are nonspecific. Some generalized signs include : A. hypertonia, tachycardia, and metabolic alkalosis B. abdominal distension, temperature in stability, and grossly bloody stools. C. hypertension, absence of apnea, and ruddy skin color D. scaphoid abdomen , no residual with feedings Coleman and increase urinary output. Copyright © 2019 Wolters Kluwer • All Rights Reserved Maternal Substance Abuse: Neonatal Abstinence Syndrome ❖ Urine toxicology serum will confirm the drug the newborn was exposed to. ❖ Provide a quiet environment, swaddle ,small feedings, avoid eye contact (cocaine),cluster care, initiate seizure precautions. ❖ The goal of treatment is to reduce symptoms. Infants are given opioids and then weaned from them after they are stable for 24 hours. Copyright © 2019 Wolters Kluwer • All Rights Reserved Maternal Substance Abuse: Signs of NAS* (projectile) Interventions: Swaddle, put baby in a flexed position, minimum stimuli Discharge planning includes an evaluation of the home environment and maternal substance abuse treatment. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question # 5 ❖ A newborn has been diagnosed with NAS. The nurse is planning to contact the provider regarding the newborn's status. Which of the following prescriptions should the nurse anticipate? Select the 3 interventions the nurse should anticipate. A. Encourage the birthing parent to breastfeed. B. Swaddle the newborn. C. Initiate seizure precautions D. Administer naloxone for NAS scores greater than 24. E. Administer oral morphine. Copyright © 2019 Wolters Kluwer • All Rights Reserved Maternal Substance Abuse: Fetal Alcohol Spectrum Disorder ❖ Exposure to alcohol in utero is the number one cause of preventable birth defects and developmental disabilities. o Prenatal exposure can result in fetal alcohol spectrum disorder (FASD), which expresses as a wide range of physical, mental, and cognitive issues. o CNS Teratogen. ❖ Care considerations: Include: social work, occupational, physical and speech therapy. , ❖ In both NAS and FAS Allow extra time for feeding. Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Infections ❖ May be acquired in utero or during or after birth. ❖ Newborns have an immature immune system, making them susceptible to infections having severe consequences from infection. ❖ Maternal immunoglobulin (antibodies) G (IgG) is transferred to the fetus via the placenta after 32 weeks. ❖ Neonatal sepsis is the presence of a bacterium (E. coli), fungus, or virus in the blood as confirmed by blood culture and manifested by systemic signs of infection. o Risk factors for neonatal sepsis include chorioamnionitis, maternal temperature greater than 100.4˚F, delivery prior to 37 weeks, or an Apgar score of 6 or less. o Sepsis is treated with antibiotics. Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Infections :Guidelines and Evaluation Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Infections: Group B Streptococcus (GBS) #1 ❖ GBS bacterial infection . o Can cause sepsis, pneumonia, RDS, or meningitis, with most displaying symptoms within 24 hours after birth. o Fist sign unstable temp. ❖ Risk factors for early-onset GBS disease include: o Delivery less than 37 weeks o Premature rupture of membranes >18 hours prior to delivery o Chorioamnionitis o GBS in urine in current pregnancy ❖ Treatment: ALL status- X2 antibiotics at least 4 hours prior to delivery ( IV-PCN- G, Ampicillin or Cefazolin, and Clindamycin or Vancomycin in allergies to PCN) Copyright © 2019 Wolters Kluwer • All Rights Reserved Neonatal Infections: Group B Streptococcus #2 ❖ Late-onset GBS is less likely to exhibit signs of shock than early-onset GBS. ❖ Late-onset GBS symptoms may include: o Fever o Cellulitis o Irritability o Lethargic with poor feeding o Grunting o Tachypnea o Apnea o Nuchal rigidity o Seizure Copyright © 2019 Wolters Kluwer • All Rights Reserved Other Sources of Neonatal Infections #1 ❖ Congenital syphilis is transmitted vertically from mother to fetus and can result in stillbirth, prematurity, or hydrops fetalis. o Symptoms of congenital syphilis vary widely and is identified with a blood test or an evaluation of cerebrospinal fluid for (VDRL). Treatment is with Penicillin G. ❖ Gonorrhea neonatorum (newborn conjunctivitis) was once a leading cause of blindness and is now routinely treated with an antibiotic eye ointment (Erythromycin) at the time of birth. ❖ Chlamydia can cause conjunctivitis or pneumonia. Often transmitted through a vaginal birth but may pass the membranes or the placenta. Treated with oral antibiotic and antibiotic eye ointment( Erythromycin) at the time of birth. ❖ Herpes is most common when vaginally delivered by a mother experiencing a herpes outbreak. May cause sepsis. Treatment is antiviral medication © 2019 Kluwer • All Rights Reserved (Acyclovir) therapy forCopyright 14 to 21Wolters days. Other Sources of Neonatal Infections #2 ❖ Toxoplasmosis is caused by a common protozoan parasite found in cat feces, contaminated soil, and undercooked meat. o may cause anemia, seizure activity, calcifications in the brain, thrombocytopenia, or jaundice. Diagnosed with blood test or CSF evaluation. ❖ Infants born to hepatitis B positive mothers are treated with HBsAG after birth and receive the first dose of Hep B vaccine within 12 hours ❖ HIV occurs during the intrapartum period. o o o Prophylactic treatment of infants with ART is begun 6 to 12 hours after delivery until 18 month of age. Breastfeeding is contraindicated for HIV-positive mothers*. During vaginal delivery do not use instruments. As early in life as possible, HIV-exposed infants and children should receive all vaccines under the Expanded Programme for Immunization (EPI), including Haemophilus influenzae type B and pneumococcal vaccine. Copyright © 2019 Wolters Kluwer • All Rights Reserved Other Sources of Neonatal Infections #3* ❖ Congenital Cytomegalovirus is a leading cause of nonhereditary hearing loss and other long-term neurodevelopmental disabilities. Trasmission Treatment includes IV antiviral medications. ❖ Congenital rubella syndrome is rare in countries with high immunization rates. Symptoms include hearing loss, cataracts, and jaundice. ❖ Neonatal varicella is dangerous if the infection occurs within the first 5 days of life. Treated with acyclovir as soon as possible. ❖ Candidiasis is a common cause of late onset neonatal sepsis due to invasive colonization. Diagnosed by blood culture and treated with antifungal medication and by removing any medical hardware such as IV lines or urinary catheters immediately. ❖ Zika is transmitted sexually or by mosquito bite and transmitted prenatally to a fetus. Associated with microcephaly, craniofacial disproportion, and hearing loss. There is no specific treatment. ❖ USE GLOVES until first bath, and bathe before skin-to-skin contact. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Heart Disease #1 Structure anomalies of the heart include: Risk factors include: ❑ Family history ❖ Transposition of great arteries ❖ Double outlet right ventricle ❖ Ventricular septal defect ❖ Tetralogy of Fallot ❖ Atrioventricular septum defect ❖ Coarctation of the aorta ❖ Atrial septum defect ❑ Certain genetic syndromes ❑ Prematurity ❑ Certain in utero infections ❑ Use of assisted reproductive technology Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Symptoms of Heart Disease ❖ Defects may be identified prior to birth. ❖ Symptoms of heart defects can be subtle and possibly missed during assessment. ❖ Symptoms of defects after birth include: o Cyanosis o Tachypnea o Pulmonary edema o Cardiogenic shock ❖ Some infants will appear normal at birth and begin to decompensate as the ductus arteriosus closes. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Heart Disease Screening Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Neurologic Abnormalities #1 ❖ Anencephaly: cranial anterior neural tube failing to close post conception. at day 25 ❖ Encephalocele: Brain or meninges protrude through a skull defect called a cranium bifidum. ❖ Spina bifida: Incomplete closure of the vertebra surrounding the spinal cord. Results from the spinal neural tube failing to close by 28 days after fertilization. https://youtu.be/bLnYzCcTEEA ❖ Adequate levels of folic acid (400 mcg daily) prior to conception may help prevent neural tube defects. ❖ Risk factors include: o Family history o Obesity o Elevated temperature in the first trimester of pregnancy (e.g., a sauna, fever, or hot tub) Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Neurologic Abnormalities #2 Figure 25.10. Spina bifida. (A) Normal spine. (B) Spina bifida occulta. (C) Spina bifida with meningocele. (D) Spina bifida with myelomeningocele (most common) Occulta: neural tissue is not exposed, and the skin remains intact Meningocele. Skin intact, the meninges (the membrane surrounding the spinal cord) protrudes through the opening in the spine. The nervous system remains undamaged, Myelomeningocele. Both the meninges and the nerve tissue come through the opening in the spine, resulting in damage to both. complete paralysis and absence of sensation. fecal and urinary function compromise. Cover the area with sterile gauze (non-adherent dressing( and normal saline. Place the baby in prone position until tranfer to surgically repair. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question # 6 ❖ A baby was born 2 hours ago by Cesarean section. The newborn has a myelomeningocele with the sac intact and has been placed in an incubator. Select all that apply regarding this condition: A. Potential risk for infection B. The sac should be kept moist with normal saline C. Keep the baby in prone position D. Complications of hydrocephalus E. Prenatal test screen is alpha-Fetoprotein(AFP) Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Orofacial Cleft ❖ An orofacial cleft is a cleft lip with or without a cleft palate or a cleft palate without a cleft lip. o may be caused by a genetic syndrome, maternal exposure to certain teratogens, smoking, diabetes, or obesity. o surgery are usually performed at 3 months, cleft palates at 6 months of age. ❖ With this defect the sucking ability most likely be compromised because they cannot create suction to extract milk. A special bottle and nipple may be used. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Gastrointestinal Anomalies Often immediately apparent on routine prenatal screening or at the time of birth; but may become apparent over time. ❖ A tracheoesophageal fistula (TEF) is an abnormal passage joining the trachea and the esophagus. • Excess secretions, choking, drooling, and respiratory distress. Require surgery. • Hirschsprung disease is a disorder of the nerves of the colon (absence) causing a functional obstruction. • abdominal distention, vomiting of bile, and failure to pass meconium within the first 48 hours of life. Confirmed by biopsy, barium enema, and imaging. Require surgery. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Gastrointestinal Anomalies #3 ❖An omphalocele is an opening of the abdominal wall at the level of the umbilical cord that contains abdominal contents contained in a membrane. ❖Gastroschisis is an abdominal wall defect associated with bowel herniation with no containing membrane. ❖In the delivery room, is wrapped in a sterile dressing with Normal Saline to prevent heat and fluid loss. ❖Multiple surgeries may be required. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Respiratory Anomalies ❖ A congenital diaphragmatic hernia is a condition in which the abdominal contents herniate through the diaphragm into the chest. ❖ Signs and symptoms include: o Respiratory distress consistent with the degree of herniation. o Development of persistent pulmonary hypertension in the neonate. o Breath sounds may be diminished or absent. o Heart sounds may be displaced. ❖ Diagnosis in the neonate is done by chest x-ray. ❖ Perinatal intrauterine repair may be attempted. ❖ Postnatal management includes stabilization followed by immediate surgical repair. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Genitourinary Anomalies #1 ❖ Hypospadias is the malplacement of the urethra on the ventral aspect of the penis. ❖ Epispadias is abnormal placement of the urethra on the dorsal aspect of the penis. ❖ Risk factors include maternal diabetes, advanced maternal age, and placental insufficiency. o It is important not to circumcise these infants because the foreskin may be needed for surgical repair. ❖ Ambiguous genitalia, Undescended testicles, hydrocele. Copyright © 2019 Wolters Kluwer • All Rights Reserved Congenital Anomalies: Musculoskeletal Anomalies ❖ Hip dysplasia may be evident at birth or become evident during infancy or childhood. o May occur as part of a syndrome but often an isolated occurrence. o The goal of treatment is to facilitate the alignment of the acetabulum and the femoral head. Is generally not initiated until after 4 weeks of age to allow time for spontaneous resolution. o The most common intervention when treatment is deemed necessary is a Pavlik harness, which limits adduction and extension while stabilizing the hip. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #4 A nurse uses pulse oximetry to screen for critical congenital heart defects (CCHD). What is the best rationale for this screening test? A. Screening for congenital heart defects should only be done if a heart defect is suspected. B. Congenital heart defect screenings should only be used for infants with tachycardia or bradycardia. C. Infants with a congenital heart defects are always diagnosed via prenatal ultrasounds. D. An infant with a congenital heart defect may appear well but then decompensate after discharge. Copyright © 2019 Wolters Kluwer • All Rights Reserved Chapter 26 Wellness and Health Promotion https://youtu.be/-UsuqWkfbQY Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Cervical Cancer Screening #1 https://youtu.be/UwyzCg57dlA ❖ Detects precancerous screening as well as early disease when it can still be managed. ❖ Done primarily with the collection of a small number of cervical cells called the Pap test (Pap smear). ❖ Two types of HPV are responsible for most cervical cancers ( types 16 and 18) and genital warts. ❖ When teaching about pelvic exams and Pap smear, advise clients: ▪ Do not douche 24 hours before exam/test (can interfere with accuracy of Pap smear) ▪ Avoid intercourse ▪ Avoid using feminine hygiene products or spermicidal agents immediately before ▪ Specimens should not be obtained during menstruation Copyright © 2019 Wolters Kluwer • All Rights Reserved Cervical Cancer Screening #2 ➢ Recommendations for screening include: ▪ First screening at the age of 21 regardless of sexual activity. ▪ Subsequent screening every 3 years until age 30. ▪ After age 30, women should receive a Pap test and HPV testing every 5 years until age 65. Or a Pap test alone every 3 years. ➢ Screening may end at age 65, ▪ provided the woman is not at increased risk for cervical cancer, has had two negative co-tests or three negative Pap tests, and no history of high-grade abnormalities. ➢ Pelvic examination should be done yearly. ➢ If test is abnormal colposcopy is performed to further examine the cervix o Risk : Multiple sexual partners o Administer HPV vaccine. Copyright © 2019 Wolters Kluwer • All Rights Reserved Breast Cancer Routine Screening ❖ The American College of Obstetricians and Gynecologists (ACOG) recommends the following breast cancer screening guidelines for women of average risk: ✓ Mammograms every 1 to 2 years between the ages of 40 and 49 years based on shared decision making (SDM) between the patient and provider ✓ Every 1 to 2 years between the ages of 50 to 75. ✓ After age 75, women should have mammograms based on SDM. ✓ Should receive a clinical breast exam (CBE) every 1 to 3 years between the age of 29 and 39 and annually after . Copyright © 2019 Wolters Kluwer • All Rights Reserved Breast Cancer Breast Examination ❖ Many organizations do not recommend Clinical Breast Examinations or Breast Self-examination because of lack of efficacy. ❖ Of the breast cancers discovered by women (rather than mammograms), most women identified changes during her routine (e.g., dressing, showering, etc.) and not by self-examination. ❖ Therefore, current recommendations are for women to develop breast awareness or familiarity will her own breasts to be able to indicate changes that might be breast cancer. Copyright © 2019 Wolters Kluwer • All Rights Reserved Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #1 ❖ A client has come to the clinic for an annual check up and expresses concern about developing breast cancer. Which factors in the client's history would the nurse discuss as possibly placing this client at risk for breast cancer? Select all that apply. A. Family history of breast, ovarian, or peritoneal cancer B. Use of aluminum chlorohydrate antiperspirant C. Dense breasts D. Never given birth E. Positive BRCA1 and BRCA2 gene mutations Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #2 Which statement made by a patient requires further education by the nurse? A. “Because I have no risk factors for breast cancer, I do not need a mammogram until I am at least 40.” B. “It is important for me to have awareness of what is normal for my breasts.” C. “Since I am 52, I should schedule a mammogram every 1 to 2 years.” D. “I should do monthly self breast examinations.” E. I must be aware of what is normal for my breasts” Copyright © 2019 Wolters Kluwer • All Rights Reserved Heart disease ❖ The term heart disease refers to several types of heart conditions, including coronary artery disease and heart attack. o *According to CDC databased on February 21, 2022, Heart disease is the leading cause of death for women in the United States, killing 314,186 women in 2020—or about 1 in every 5 female deaths. o Women are much more likely to have atypical heart attack symptoms. ▪ Classic chest or absent, women are much more likely to get symptoms such as indigestion, abdominal pain, shortness of breath, neck and back pain, sweating, light-headness. Copyright © 2019 Wolters Kluwer • All Rights Reserved Intimate Partner Violence (IPV) Screening ❖ IPV is any actual or threatened psychological, sexual, or physical harm of one current or past partner by the other. Increases during pregnancy. ❖ Victims of IPV may be of any gender identity, age, socioeconomic class, ethnicity, or sexual preference. They are often reluctant to disclose IPV for shame, guilt, or fear. Have a few friends ,low self steam, low academic achievement, lots of problem with partner, can be using alcohol and drugs. ❖ May present with: o bruises in different phases, frequency of injuries (face, head, neck), reported history of the injury inconsistent with the presenting problem, depression, anxiety, or substance abuse ❖ Abuser extremely controller, jealous, possessive, don’t leave her side, blame partner for everything. ❖ All women are screened by a paper or computer questionnaire and by engaging in an open-ended questions. o Regardless of method, the partner of the patient must not be present during the screening. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #3 ❖ A nurse is working in a local community health care facility where she frequently encounters victims of abuse. For which signs should the nurse assess to find out if a client is a victim of abuse? Select all that apply. A. injuries on the face, head, and neck B. reported history of the injury inconsistent with the presenting problem C. frequent STIs D. mental health problems such as depression, anxiety, or substance abuse E. partner of suspected victim relaxed and not overly worried Copyright © 2019 Wolters Kluwer • All Rights Reserved Sexual Assault and Human Trafficking ❖ Sexual violence is unwanted sexual experiences, sexual contact, and sexual coercion. ❖ Nurses are mandated reporters, and it is the responsibility of the nurse to know the reporting requirements in his or her state. ❖ After an assault, individuals are tested for sexually transmitted infections, pregnancy, Hep B, HIV. ❖ Offer: o prophylactic treatment for STIs o postcoital contraceptive therapy. o sexual assault counseling. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #4 The nurse is caring for a client who adheres to a vegan diet. Which micronutrient does the nurse recommend for this client? A. The client needs to take supplemental folic acid and iron. B. The client needs more protein and fat. C. Additional calcium is needed in the vegan diet. D. client needs to include a B vitamin supplement. Copyright © 2019 Wolters Kluwer • All Rights Reserved Physical Activity #1 ❖ Current physical activity guidelines recommend ❖ 2.5 hours moderate-intensity aerobic activity per week o E.g., walking briskly (3 miles per hour or faster), water aerobics, slow bicycling, doubles tennis, ballroom dancing, and general gardening) ❖ 0R 1 hour and 15 minutes of vigorous-intensity aerobic activity per week. o E.g., swimming laps, jogging, aerobic dancing. Copyright © 2019 Wolters Kluwer • All Rights Reserved Screening for Sexually Transmitted Infections (STIs) #1 ❖ Screening for STIs is based on risk in accordance with sexual activity and sex. ❖ Screening guidelines include: o Chlamydia and gonorrhea: ▪ Annually for all sexually active women under 25 years. ▪ Women 25 or older with new sex partners, more than one sex partner, or a sex partner with known STI. ▪ Pregnant women o Syphilis: ▪ Pregnant women at the first visit ▪ At least annually for men who have sex with men Copyright © 2019 Wolters Kluwer • All Rights Reserved Screening for Sexually Transmitted Infections #2 ❖ Human immunodeficiency virus (HIV): o All adolescents o Pregnant women at their first visit o Annually for men who have sex with men ❖ Hepatitis B virus: o All pregnant women at their first visit o Past and current drug users ❖ Hepatitis C virus: o All pregnant women with current or past injection drug use, an unregulated tattoo, or long-term hemodialysis. o Past and current drug users o Individuals who test positive for HIV Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #3 Which of the following patients is a priority for sexually transmitted infection screening? A. A woman 6 weeks pregnant during her initial prenatal visit B. A 17-year-old sexually active male C. A 24-year-old woman being seen for an annual gynecologic exam D. All of the above Copyright © 2019 Wolters Kluwer • All Rights Reserved Osteoporosis ❖ Loss of bone mass. After the age of 35 decreased. ❖ Diagnosed; DXA scan- T-scores > or equal to -2.5 ❖ Sign and symptoms: o Back pain, loss of height, stooping posture ❖ Risk: thin, Caucasian, chronic or current smoker, 3 or more drinks/day, lack of exercise, corticosteroids, BMI >20 ❖ Medication Bisphosphonates. E.g., Fosamax (Alendronate) inhibits the process through which the body breaks down bone tissue. o Side effects: Musculoskeletal pain, GI irritation and ulcers. ▪ Take in the morning, sitting or standing, upright for 30 min, before breakfast with 8 ounces of water. No coffee or juice. Copyright © 2019 Wolters Kluwer • All Rights Reserved Chapter 27 Common Gynecologic Conditions Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Endometriosis ❖ Is the presence of endometrial tissue outside the uterus. Lesion usually in peritoneal area or reproductive organs that cause pain. ❖ Symptoms include dysmenorrhea, dyspareunia, infertility, pelvic mass, pelvic pain/cramping. ❖ The cause hormonal changes (Estrogen and Progesterone). inflammation of the endometrium, hereditary, immunologic defects. ❖ Treatment: NSAIDs, combined oral contraceptive, or Medroxyprogesterone (MPA), Danazol , GnRH agonist (Lupron).Category X • laparoscopy for definitive diagnosis and removal of endometrial lesions (electrocautery) or Hysterectomy. ❖ Nurses should provide information on likely outcomes Fi of treatment options. Copyright © 2019 Wolters Kluwer • All Rights Reserved Endometriosis #2 Copyright © 2019 Wolters Kluwer • All Rights Reserved Pelvic Prolapse ❖ Pelvic organs are held in place by a combination of connective tissue and the muscles of the pelvic floor. Hormonal changes makes those muscle weak and pelvic organs descend into the vagina o May involve prolapse of the bladder (cystocele), rectum (rectocele), bowel (enterocele), or uterus. ❖ Risk for pelvic floor prolapse include: o Multiple births o The use of forceps to assist delivery o Perineal tears during delivery o Episiotomy during birth Copyright © 2019 Wolters Kluwer • All Rights Reserved Pelvic Prolapse: Classifications by Stage Figure 27.12. Types of pelvic organ prolapse. (A) No prolapse. (B) Cystocele. (C) Rectocele. (D) Enterocele. (E) Uterine prolapse. Copyright © 2019 Wolters Kluwer • All Rights Reserved Pelvic Prolapse: Symptoms and Treatment ❖ Signs and symptoms may include: o Vaginal pressure o Pelvic pain o Bulge at the opening of the vagina o Problems with defecation urination. Stress incontinence. or o Painful intercourse. ❖ Treatment may include vaginal pessaries (silicone ring) to assist with pelvic organ support, physical therapy, or surgery, when the women experiences distressing symptoms. • https://youtu.be/_pXG815daDs Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #1 Which of the following statements is false? A. Risks for pelvic prolapse include obesity and having a baby. B. Symptoms include vaginal pressure and pelvic pain. C. Treatment is indicated when the woman experiences distressing symptoms. D. Treatment always involves surgery. Copyright © 2019 Wolters Kluwer • All Rights Reserved Menopause PMS-https://youtu.be/ZtrynEEffMw ❖ Natural menopause is when a woman has not menstruated for a full 12 months in the absence of any other reason. Typically occurs around age 51 or 52. ❖ The time prior to menopause is referred to as perimenopause and typically lasts around 4 years. ❖ Perimenopause and Menopause symptoms : hot flashes, night sweats, increased anxiety, depression, insomnia, sporadic ovulation, mood swings, increased abdominal fat, dry, thinning skin, and increased waist size. ❖ Best indicator : High FSH ,and Estrogen levels drop, vaginal mucosa becomes progressively dry and less elastic (vaginal Atrophy) Use OTC moisturizing ,lubricants. ❖ Estrogen replacement therapy is no longer recommended for symptoms due to the risk for cardiovascular disease and osteoporosis. ❖ Postmenopausal bleeding is highly suspicious of endometrial cancer. Copyright © 2019 Wolters Kluwer • All Rights Reserved Polycystic Ovarian Syndrome (PCOS) ❖ The most common endocrine disorder that causes infertility in women. ❖ Usually appears in Childbearing age. Cyst in ovaries . ❖ Is associated with obesity, hyperinsulinemia, Increase estrogen, testosterone, LH, decrease FSH, Dyslipidemia, Sleep apnea, anovulation, amenorrhea, hirsutism, acne, virilization, oily skin. ❖ Long terms RISK : Hypertension and cardiovascular disease and metabolic syndrome. ❖ Patients may ovulate intermittently. Should use contraception if they do not want to get pregnant. o If pregnancy is an immediate goal: Clomiphene citrate (Clomid), ART ❖ Treatment: • Metformin (Glucophage) to improve insulin sensitivity and utilization. • Spironolactone (Aldactone) or Eflornithine to decrease symptoms such as excessive hair growth and acne. Copyright © 2019 Wolters Kluwer • All Rights Reserved PCOS Diagnostic Criteria for Adolescents Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #2 The nurse counsels a patient recently diagnosed with polycystic ovarian syndrome. Which of the following should be included in the patient education: A. The need to use reliable birth control B. The importance of annual testing for STIs C. Lifestyle behaviors to manage urinary incontinence D. Self-care measures for secondary dysmenorrhea Copyright © 2019 Wolters Kluwer • All Rights Reserved Gynecologic Cancers ❖ Uterine, cervical, ovarian (“silent killer’), vaginal, and vulvar. ❖ Diagnoses: Biopsy ❖ Risk : Multiple sexual partners ❖ Symptoms: Vaginal discharge, watery, pink brown and foul smelling, leaking urine and feces from the vagina, abnormal vaginal bleeding between periods, intercourse or menopause, painful sex, loss of appetite, fatigue, pelvic pain. ❖ The prognosis depends on the type and stage. ❖ Treatment includes total hysterectomy(TA-remove uterus and cervix), with bilateral salpingo-oophorectomy(both ovaries)(TAH,BSO), surgical removal of the cancerous tissue ,chemotherapy and radiation as needed. ❖ Advise woman (TAH,BSO) will cause premature menopause. ❖ All cancers are staged based on the TNM staging system. Copyright © 2019 Wolters Kluwer • All Rights Reserved Breast Cancer #1 ❖ Approximately 1 in 8 women will be diagnosed with breast cancer during their lifetime. Major risk nulliparas. ❖ A majority of breast cancers are discovered by mammogram and diagnosed by needle biopsy of the core lesion. ❖ Prognostic factors depend on factors such as tumor stage, gene expression, circulating tumor cells, age, race, and smoking status. ❖ Treatment may include: o Surgery (lumpectomy, radical mastectomy, modified radical mastectomy, simple mastectomy) o Chemotherapy, Radiation therapy, Hormone therapy Copyright © 2019 Wolters Kluwer • All Rights Reserved Breast Cancer #2 ❖ Symptoms to report: o New lump in the breast or underarm (armpit). o Redness, irritation, dimpling ,thickening, swelling or enlarge pores of the breast. (Peau d’orange) o Pulling in of the nipple or discharge other than breast milk, including blood. o Any change in the size or the shape of the breast. Copyright © 2019 Wolters Kluwer • All Rights Reserved Breast Cancer #3 ❖ After surgery asses wound for healing. ❖ Side Effects from chemo and radiation: o Diarrhea, mouth ulcers, weight loss, nausea, vomiting. o Ask to drink more fluids, Gatorade, eat small frequent meals, cook meals very well, plenty of rest. Antidiarrheal medications, baby wipes, o Check for skin changes on the area of radiation. ❖ Teach: Post mastectomy arm exercises to prevent lymphedema. ❖ Women with fibrocystic breast are not at increase for breast cancer. Copyright © 2019 Wolters Kluwer • All Rights Reserved Chapter 28 Infections https://youtu.be/BOksgV3g9Bo Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Urinary Tract Infections (UTIs) ❖ https://www.cdc.gov/std/default.htm ❖ The result of bacteria (often Escherichia coli) ascending into the urethra, bladder, and kidneys (pyelonephritis). ❖ Cystitis most common form limited to the bladder ❖ Symptoms urinary frequency, urgency, a sensation of incomplete emptying, pain with urination, and sometimes hematuria. ❖ Point-of-care urinalysis may be used .Values specific to UTI are leukocytes, nitrites, and blood. ❖ A urine culture must be done in a laboratory ❖ Elderly presentation unusual of UTI: confusion, disorientation, agitation (mental status changes), falling. Copyright © 2019 Wolters Kluwer • All Rights Reserved Urinary Tract Infections: Treatments ❖ Often resolve without treatment or may need antibiotics. o Trimethoprim/sulfamethoxazole (Bactrim), Nitrofurantoin ❖ If antibiotics, patients should be taught to finish their course of antibiotics even if they feel better. ❖ Phenazopyridine (Pyridium) urinary analgesic that can manage symptoms related to cystitis, but it does not cure the UTI. o Teach do not take more than 2 days it can mask UTI symptoms o changes urine color to bright orange, which can be alarming. ❖ Complications: Pyelonephritis: UTI that has ascended into the kidneys. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #1 A patient calls the clinic with complaints of fever, back pain, urinary frequency, and urinary urgency. The nurse suspects the provider will do which of the following? A. Recommend the patient stay home and drink a lot of water. B. Recommend the patient come to the clinic to be evaluated for pyelonephritis. C. Diagnose the patient with a urinary tract infection and call in a prescription. D. Recommend the patient take phenazopyridine for 2 days and call back if symptoms persist. Copyright © 2019 Wolters Kluwer • All Rights Reserved Vaginosis ❖ Any abnormality of vaginal discharge. ❖ Bacterial vaginosis (BV) is associated with higher-than-normal pH in the vagina that allows certain bacteria to become dominant. Not an STI. Only females are affected. ❖ Conditions that raise the pH include pregnancy, intercourse, and tampons. having multiple sex partners, vaginal douching. ❖ Signs and symptoms of BV include fishy vaginal odor and thin white/gray vaginal discharge. Clue" cells are seen on wetmount preparation. ❖ Often resolves spontaneously but may be treated with Clindamycin, oral Metronidazole or vaginal cream. Copyright © 2019 Wolters Kluwer • All Rights Reserved Vaginitis ❖ Means inflammation of the mucosa of the vagina. ❖ Candida vulvovaginitis, also known as yeast infection. Causative organism is Candida albicans. No STI o Associated with use of antibiotics, restrictive clothing, underwear made with artificial fibers, and glucose intolerance. It may occasionally be shared sexually. ❖ Women may report a thick, cottage cheese-like vaginal discharge and/or acute vaginal dryness, itchiness. Examination findings include inflamed tissue of the vulva. o Men rash or excoriation of the skin of the penis, possible pruritus. ❖ Treatment: Monistat (OTC) or topical -azoles fluconazole, miconazole Intravaginal . Male generally no treatment is necessary. ❖ Women with recurrent yeast infections should be assessed for diabetes. Copyright © 2019 Wolters Kluwer • All Rights Reserved Vaginitis 2 Copyright © 2019 Wolters Kluwer • All Rights Reserved Vaginitis: Trichomoniasis ❖ A sexually transmitted form of vaginitis caused by Trichomonas vaginalis. ❖ Trichomoniasis is the most common asymptomatic nonviral STI. ❖ Signs and symptoms include a thin, yellow-green, frothy vaginal or urethral Malodorous discharge , vaginal or vulvar erythema, dyspareunia, pelvic pain, dysuria, urinary frequency, and offschedule bleeding. Some women, however, are asymptomatic. ❖ Findings include cervical bleeding on contact, cervical petechiae, and vaginal or vulvar erythema ❖ If untreated, may lead to pelvic inflammatory disease (PID). ❖ Trichomoniasis may be treated with a single dose of Metronidazole. ❖ Sexual partners must be treated as well to avoid reinfection. Copyright © 2019 Wolters Kluwer • All Rights Reserved Trichomoniasis Copyright © 2019 Wolters Kluwer • All Rights Reserved Chlamydia ❖ Most commonly diagnosed bacterial STI in the States. ❖ Often asymptomatic. Most common symptoms are dysuria and frequency of urination. Men may experience urethritis, females may experience cervicitis, PID ❖ Can scar fallopian tubes, cause infertility, ectopic pregnancy, postpartum endometritis, PROM. Pneumonia in babies and conjunctivitis. ❖ Diagnosed by urinalysis or swab sampling to culture. ❖ Treatment includes Azithromycin or Doxycycline. ❖ Sexual partners should also be treated. ❖ Retesting should be done 3 months after treatment. ❖ The law mandates reporting Copyright © 2019 Wolters Kluwer • All Rights Reserved Gonorrhea ❖ Bacterial STI may cause infertility, ectopic pregnancy, and pelvic pain. ❖ Symptoms are similar to chlamydia. o Locally enlarged lymph nodes ❖ Because most people are asymptomatic, routine screening is recommended. ❖ First-line treatment often single dose of ceftriaxone and azithromycin, or doxycycline. Although some strains are antibiotic resistant. ❖ Sexual partners should also be treated. ❖ The law mandates reporting . Copyright © 2019 Wolters Kluwer • All Rights Reserved Gonorrhea Copyright © 2019 Wolters Kluwer • All Rights Reserved Syphilis ❖ STI occurs in 4 stages: o Primary: May present as single, painless chancre, multiple or uncomfortable lesions where the point of entry was. o Secondary : Individual may have a rash, fever. Weight loss. o Latent: Asymptomatic period that may last for years. o Tertiary: May affect multiple organ systems including brain, nerves, and joints. ❖ Blood tests: Venereal disease research laboratory (VDRL)(RPR) serum ❖ Penicillin G is the treatment of choice single dose. Treat both partners. Doxycycline or tetracycline if allergy to PCN. ❖ The law mandates reporting Copyright © 2019 Wolters Kluwer • All Rights Reserved Syphilis Copyright © 2019 Wolters Kluwer • All Rights Reserved HPV ❖ Most common STI ❖ Presents with wart-like lesions that are soft, moist, or flesh colored and appear on the vulva and cervix, and inside and surrounding the vagina and anus. ❖ Two types of HPV are responsible for the majority of cervical cancers ( types 16 and 18) ❖ HPV vaccination: Gardasil or Gardasil 9 for 9 to 26 years old, (before having sex0, ideally at age 11, both sexes, 3 doses. ❖ Dx; warts: based on appearance, based on Pap: colposcopy or biopsy. ❖ Treatment : For genital warts ,apply creams Imiquimod, podofilox (Condylox). ❖ Lesion are contagious. ❖ Even after warts are removed the HPV infection remains. Copyright © 2019 Wolters Kluwer • All Rights Reserved HPV Copyright © 2019 Wolters Kluwer • All Rights Reserved Pelvic Inflammatory Disease (PID) ❖ Inflammation of upper female genital tract. ❖ Causative agents: o Chlamydia, trichomoniasis and Neisseria gonorrhoeae. ❖ Infertility may occur due to post- infection. ❖ More common-sexually active women younger than 25 years. ❖ Risk factors – multiple partners, IUD, regular douching. ❖ Symptoms: ❖ Women may be asymptomatic or o Severe abdominal, uterine, and ovarian pain and tenderness fever ,elevated WBC ❖ Treatment o o Antibiotics, analgesic Sexual partner. Copyright © 2019 Wolters Kluwer • All Rights Reserved Toxic Shock Syndrome (TSS) ❖ Primarily a disease of women at or near menses, or during the postpartum period, but it can happen to anyone exposed to the bacteria. ❖ Causative organism is a toxin released by a strain of Staphylococcus aureus. ❖ Related to the use of superabsorbent tampons, contraceptive devices - cervical cap or diaphragm during menses. ❖ Signs and Symptoms: abnormally hypotension, flu-like symptom, rashes especially on the palms and bottoms of the feet, peeling skin, and seizures. ❖ Treatment- antibiotics, low blood pressure medication, other supportive care. ❖ Instruct the patient to change tampons frequently. Copyright © 2019 Wolters Kluwer • All Rights Reserved Herpes Simplex Virus ❖ Transmitted by skin-to-skin contact, usually of the mucosa. No cure. ❖ HSV 1 and HSV 2 ❖ Presents with small red bumps with blisters or open sores in the area where the virus enters the body. Cervix, vagina or outer peritoneal area. Results in inflammation and pain. ❖ Flu-like symptoms may develop or asymptomatic. Itching or burning genital ,anus area. ❖ Treated with Acyclovir. Oral analgesics, cool compresses that has peppermint. ❖ Outbreaks are triggered by emotional stress, use of corticosteroids, sexual intercourse. ➢ Abstain from sex while the lesions resolve. ➢ Good handwashing technique. Copyright © 2019 Wolters Kluwer • All Rights Reserved Herpes Simplex Virus Copyright © 2019 Wolters Kluwer • All Rights Reserved Hepatitis B ❖ Primary modes of Hepatitis B transmission are perinatally, unprotected sex, and IV drug use. ❖ may be asymptomatic or include symptoms ❖ People with hepatitis B are at risk for cirrhosis, liver failure, liver cancer, and death. ❖ Vaccination is the most effective means of avoiding hepatitis B infection. o hepatitis B recombinant vaccine o Provided in 3 doses, first dose at birth, with the second dose 1 month after the first and the third dose 6 months after the first. ❖ Risk factors include having multiple sex partners, engaging in unprotected anal intercourse, and having a history of other STIs. Copyright © 2019 Wolters Kluwer • All Rights Reserved Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) ❖ HIV retrovirus attacks and destroys T Lymphocytes. ❖ Symtoms: fever, fatigue, anemia, diarrhea and weight loss. ❖ Risk: contaminated blood products, IV drug use, and having unprotected intercourse. ❖ Dx: Antibody screening (EIA), Confirm Western Blot. o Rapid antibody (blood and urine) for client in labor o Screen for STI if seeking treatment o Obtain viral load levels ad CD4 cell counts through pregnancy ❖ Treatment :ART( antiretroviral therapy) PO ❖ Has profound implications for the fetus if infected woman is pregnant. Know treatment in pregnancy/Labor/ postpartum!! ❖ The law mandates reporting. ❖ If vaginal deliver do not use instruments can mixed with baby's blood. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #2 The nurse plays a vital role in screening patients for a possible HIV infection. What questions below could the nurse ask to help identify a patient who is at risk for HIV? Select all that apply: A. “How often do you use alcohol or drugs?” B. “Have you recently experienced an abusive relationship?” C. “If you are sexually active, do you or your partner use protection?” D. “In the past month, have you felt sad or unable to get out of bed?” E. “Have you ever been treated for a sexually transmitted infection?” F. “Do you ever experience intrusive or unwanted thoughts?” Copyright © 2019 Wolters Kluwer • All Rights Reserved Chapter 29 Family Planning Copyright © 2015 Wolters Kluwer Health | Lippincott Williams & Wilkins Family Planning ❖ Family Planning -https://youtu.be/IEffOROmkbQ ❖ Family planning includes any educational, social, or health care interventions that allow people to plan reproduction. ❖ Family planning includes contraception, abortion, and subfertility or infertility care. ❖ Nurses participating in family planning o must be respectful of patient choice and careful not to interject his or her own biases. o must establish realistic outcomes for the patient o must be sensitive to the couple's religious, cultural, and moral beliefs. Copyright © 2019 Wolters Kluwer • All Rights Reserved Contraception ❖ The goal of contraception is to prevent unwanted or mistimed pregnancy. (specially with teenagers). ❖ Major types of contraception include: o Long-acting reversible contraception (LARC) o Combined oral contraceptives (COCs) o Progestin only pills (POPs) o Hormonal patches o Hormonal vaginal rings o Barrier methods o Spermicide o Natural family planning (NFP) o Withdrawal o Contraceptive injections o Sterilization Copyright © 2019 Wolters Kluwer • All Rights Reserved Contraception Considerations ❖ The most effective methods of birth control are bilateral tubal ligation (BTL), vasectomy, and methods of LARC (contraceptive implants and intrauterine contraception). ❖ Contraception decisions involve evaluating family planning goals. ❖ A contraceptive method is only as good as the patient’s adherence to and continued, consistent use of the method once adopted. ❖ When counseling nurses must consider the efficacy of the method and the future childbearing plans. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: COCs ❖ Relief of menstrual symptoms, lessened cramps, decreased flow, improved cycle regularity. ❖ Contain 21 hormone-containing pills followed by 7 placebo pills or packaging is 84 hormone pills followed by 7 placebo pills (known as extended cycling) ❖ Works by increasing viscosity of cervical mucus, suppressing ovulation, and thinning the uterine lining. ❖ Contraindications for birth control containing estrogen include migraine with aura, history of DVT, hypertension, >35 y/old, diabetic retinopathy. ❖ Side effects: weight gain, depression ,breakthrough bleeding (specially with teenagers), and thromboembolism. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: POPs ❖ Progestin-only pills (POPs) contain only progestin (artificial form of progestin). ❖ Safe for breastfeeding mothers. ❖ All 28 pills in a pack contain progestin (no placebo pills). ❖ Must be taken within a 3-hour window every day to be effective. ❖ Primary side effect is a less regular period and more breakthrough bleeding, clots ❖ Patients on OCP reporting chest pain and SOB should go to the Emergency room. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Vaginal Ring ❖ Contraceptive rings are flexible silicone rings impregnated with estrogen and progestin. ❖ The woman places the ring inside her vagina for 3 weeks, removes it for a week to create a withdrawal bleed, and then replaces it with a new ring. E.g, NuvaRing. ❖ Ring can be removed for intercourse and left out for up to 3 hours per day. ❖ The ring can be dislodged during a bowel movement. The nurse should teach the patient to check placement of the ring. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Contraceptive Patch ❖ A contraceptive patch contains estrogen and progestin and is applied weekly for 3 weeks. Followed by a patch-free week, which will cause a withdrawal bleed. ❖ The patch should be applied on the upper back, upper arm, upper buttock, or lower abdomen, but not on the breast. ❖ The woman should rotate the cite weekly to avoid skin irritation. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Emergency Contraception ❖ Emergency contraception (EC) “morning-after pill”. o Levonorgestrel (PlanB): ▪ Available over the counter or by prescription and is most effective when taken within 72 hours of unprotective intercourse. ▪ Works by preventing ovulation and does not affect an established pregnancy. o Ulipristal (Ella): ▪ Available by prescription only. May be used within 120 hours of unprotected intercourse. ▪ Works as a progestin blocker and may affect an existing pregnancy. ❖ Side effects: nausea, vomiting, headache, and irregular bleeding. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Contraceptive Injection * ❖ Medroxyprogesterone acetate (brand name: Provera) is a progestin-only injection given every 13 weeks until pregnancy is desired. ❖ Start DMPA within 7 days of the start of her last menstrual cycle. Breastfeeding clients start 6 weeks postpartum. ❖ Concerns include weight gain. Decreased bone mineral density. Maintain adequate intake of calcium or increase it and weight bearing exercises. ❖ Not a good choice for patients that wants to get pregnant within 3 months. ❖ Benefits include less frequent or scant menses. ❖ Do not massage the site, decreased absorption. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Contraceptive Implant ❖ A 4-cm rod of nonestrogen etonogestrel is inserted under the skin of the inner upper arm. E.g., Implanon and Nexplanon. ❖ Approved for use for 3 years, contraceptive implant works by creating changes to cervical mucus and to fallopian tube motility that impede fertilization. Also suppresses follicle maturation and ovulation. ❖ A BMI greater than 30 may make contraceptive implants less effective. ❖ Unscheduled bleeding is a common side effect. ❖ A majority of women ovulate within a month of removal. Copyright © 2019 Wolters Kluwer • All Rights Reserved Hormone-Containing Birth Control: Intrauterine Contraception #1 ❖ (IUCs or IUDs) are T-shaped plastic devices inserted into the uterus. Releases chemical substance that damage the sperm. ❖ The copper IUD may last 10 years. E.g., ParaGard. Does not contain hormones. ❖ The progestin IUD may last 5 years. E.g., Skyla, Liletta, Mirena. ❖ Sign a consent ❖ Perform a pregnancy test. ❖ Perform a U/S if pregnancy is suspected after insertion. ❖ Contraception can be reverse immediately. ❖ Can cause irregular menstrual bleeding. ❖ Require the collection of cultures for sexually transmitted infections prior to placement. Copyright © 2019 Wolters Kluwer • All Rights Reserved Intrauterine Contraception #2 ❖ Women should report new acute cramping, bleeding, late period, fever, unusual bleeding, pain with intercourse. ❖ Not longer recommended to check for string placement monthly to verify placement. ❖ With IUC placement, women are screened for STIs. ❖ Contraindicated in women with menorrhagia ❖ Risk for bacterila vaginosis , PID, uterine perforation or uterine expulsion. Copyright © 2019 Wolters Kluwer • All Rights Reserved Barrier Methods of Birth Control: Condoms ❖ Male condoms are generally less effective as contraceptives but the best protection against STIs (other than abstinence). ❖ A new condom should be used with each episode of oral, rectal, or vaginal sex with a partner whose STI status is unknown. ❖ The condom should be applied prior to genital contact, on an erect penis ,leaving a space at the tip for sperm reservoir. ❖ Condoms should be removed and discarded immediately after ejaculation. ❖ Latex and polyurethane protect against STI , but made of natural skin no. Copyright © 2019 Wolters Kluwer • All Rights Reserved Barrier Methods of Birth Control: Diaphragm ❖ The diaphragm is a flexible saucer that is placed into the vagina to cover the cervix and area around it. It does not protect against STIs. ❖ Fit should be checked if the woman gives birth, has a miscarriage or abortion, or gains or loses more than 10 pounds. ❖ Should be replaced every 2 years. ❖ Avoid if latex allergy. ❖ Used with spermicidal cream or gel. Copyright © 2019 Wolters Kluwer • All Rights Reserved Barrier Methods of Birth Control: Contraceptive Sponge ❖ A contraceptive sponge is a 2-inch round, spermicideinfused, foam disk that fits over the cervix, and is available over the counter. Protect the sperm form entering the vagina. ❖ One size fits all. ❖ Prior to insertion, the woman wets the sponge and inserts it with her fingers into the top of her vagina. ❖ May be placed up to 24 hours before sexual intercourse but should stay in no more than 30 hours. ❖ Risk for TSS if left in the vagina. Copyright © 2019 Wolters Kluwer • All Rights Reserved Natural Family Planning (NFP) ❖ Abstinence: The most effective contraception method. ❖ Calendar: track menstrual cycle to determine time of ovulation. Avoid intercourse on days 8-19 of the cycle and record menstrual cycles 6-8 months to determine fertile days. ❖ Basal Body Temperature (BBT):Symptom base method. a slight dip temperature just before ovulation, then rises sharply and thinning cervical mucus). o Teach to take temperature before getting out of bed in the morning . o avoid intercourse when temperature rise and for at least three days after. Copyright © 2019 Wolters Kluwer • All Rights Reserved Natural Family Planning (NFP) 2 ❖ Billings or cervical mucous method. o At time of ovulation mucous is clear and stretchy (spinnbarkeit) amiable to sperm. ❖ Withdrawal or coitus interruptus: o Be aware ejaculatory fluid can leak form the penis prior to ejaculation. It contain sperm. o Free, safe and acceptable where religious beliefs prohibit other methods. o Highest risk for unintended pregnancy. Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #1 A couple plans to try for a baby after they get married in 3 months. Based on their situation, what method of birth control might be best for them? A. A progestin intrauterine device B. A Depo Provera injection C. Condoms D. None of the above Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #2 A patient is interested in emergency contraception due to unprotected intercourse that occurred 1 week ago. What is the best response by the nurse? A. “Levonorgestrel (Plan B) can be use now as emergency contraception.” B. “Emergency contraception is only available after a sexual assault.” C. “Emergency contraception should be taken within 72 to 120 hours to be effective.” D. “A progestin intrauterine device may be inserted at this time for emergency contraception.” Copyright © 2019 Wolters Kluwer • All Rights Reserved Sterilization ❖ Bilateral Tubal Ligation (BTL) may involve the cauterization, suturing, clamping, or removal of a portion the fallopian tubes. (Normal ovulation continues). ❖ Surgical, permanent procedure with general or spinal anesthesia. ❖ Vasectomy is the safest means of permanent sterilization and the most cost-effective. Involve clamping, cutting and sealing the vas deferens to prevent the release of sperm. Local anesthesia. o Does not produce immediate sterility. Takes about 6–8 weeks. o Resume sexual intercourse in about 1 week. o Use a birth control method until a negative sperm reports occur. o Does not protect against STIs Copyright © 2019 Wolters Kluwer • All Rights Reserved Abortion #1 ❖ Abortion is the spontaneous or elective termination of pregnancy before 20 weeks’ gestation ❖ Abortions are referred to as o Induced medical or surgical termination of pregnancy before fetal viability ▪ Medical abortions : 200 mg of Mifepristone (RU-486) followed by 800 μg of Misoprostol 6 hours later. ✓ Complications :prolonged bleeding and incomplete abortion. ✓ Monitor vital signs, pain, and bleeding, for at least 30 minutes after the procedure. ▪ Surgical :is typically done by uterine aspiration and is also called dilation and curettage (D&C). Copyright © 2019 Wolters Kluwer • All Rights Reserved Abortion #2 ❖ Elective: termination of pregnancy before fetal viability at the request of the woman ❖ Therapeutic: termination of pregnancy for serious maternal medical indications or serious fetal anomalies. ❖ Spontaneous: (SAB) abortion occurring without medical or mechanical means, also called miscarriage. o The majority (80%) occur in the first 12 weeks of gestation and are termed early abortion, and more than half of those are a result of chromosomal abnormalities. ❖ Women who are Rh negative should be given Rh o (D) immune globulin ❖ Nurses who participate in abortion care should know state laws Copyright © 2019 Wolters Kluwer • All Rights Reserved Fertility ❖ Infertility is defined as lack of conception despite unprotected sex for at least 1 year (6 months if the woman is over 35 years old). ❖ Some couples may need information about ovulation and timing intercourse. ❖ Infertility may be related to male factors or female factors. The cause is determined after tests are done. ❖ Overweight or underweight women may be counseled to lose or gain weight to induce ovulation. ❖ Test: Hysterosalpingogram. Do not perform in patients allergic to selfish. ❖ Patients may experience anger at others who have babies, feelings of failure because they cannot make a baby and guilt of one partner because unable to give the other a baby. Copyright © 2019 Wolters Kluwer • All Rights Reserved Fertility: Evaluation Prolonged heat exposure is a gonadotoxin. Several medications such as calcium channel blockers can influence sperm production. Copyright © 2019 Wolters Kluwer • All Rights Reserved Fertility: Clomid ❖ Clomiphene citrate (Clomid) is a selective estrogen receptor modulator and common first-line medication to induce ovulation. ❖ Usually is started 5 days after the start of menses. ❖ Ovarian hyperstimulation syndrome (OHSS) may occur: o ovarian enlargement, severe GI symptoms, abdominal swelling/ pain, shortness of breath, pleural effusions, decreased urination. o Seek medical care if these symptoms develop. ❖ The risk of multiple gestation increase. ❖ Side effect: breast pain or tenderness, nausea, vomiting, flushing. Copyright © 2019 Wolters Kluwer • All Rights Reserved Artificial Reproductive Technology (ART) ❖ ART is used to treat infertility. ❖ Intrauterine insemination: sperm is prepared and then introduced in the uterus at the time of ovulation. ❖ In Vitro Fertilization (IVF) fertilized eggs with sperm in the laboratory will be transferred into the woman uterus ❖ Gamete intrafallopian tube: gametes injected into fallopian tubes via laparoscopy after being placed together in a catheter. ❖ Donor oocyte or Donor embryo, ❖ Gestational carrier, ❖ Surrogate mother, ❖ Therapeutic donor insemination. ❖ Risk for eptopic and multiple pregnancies Copyright © 2019 Wolters Kluwer • All Rights Reserved Question #3 Which of the following would a provider diagnose with infertility? A. A 37-year-old woman trying to get pregnant for 7 months B. A 24-year-old woman trying to get pregnant for 11 months C. A 30-year-old woman trying to get pregnant for 6 months D. A 34-year-old woman trying to get pregnant for 10 months E. None of the above Copyright © 2019 Wolters Kluwer • All Rights Reserved