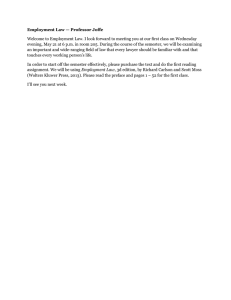
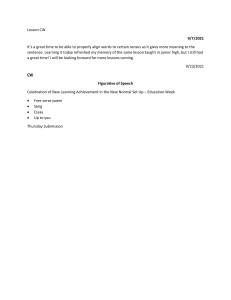
Chapter 36 Nursing Care of the Child with an Alteration in Comfort–Pain Assessment and Management Pain Management in Children Copyright © 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins Pain Transmission in the Nervous System #1 Transduction o Nociceptors (specialized nerve cell endings) are activated when exposed to noxious stimuli Mechanical, chemical, or thermal Transmission o Stimuli are converted to electrical impulses and relayed to spinal cord and brain by afferent nerve fibers and unmyelinated small C fibers o Neurotransmitters facilitate transmission process to the brain Copyright © 2021 Wolters Kluwer • All Rights Reserved Pain Transmission in the Nervous System #2 Perception o Nerve fibers divide in the dorsal horn of the spinal cord, cross to the opposite side, and rise upward to the thalamus o Thalamus quickly sends a message to somatosensory cortex of the brain where impulse is interpreted as pain A-delta fibers lead to sharp, stabbing, local pain C fibers lead to diffuse, dull, burning or aching pain Pain threshold is the point where a person feels the lowest intensity of painful stimulus Copyright © 2021 Wolters Kluwer • All Rights Reserved Pain Transmission in the Nervous System #3 Modulation o Neuromodulators modulate the pain sensation Naturally occurring examples include serotonin, endorphins, enkephalins, and dynorphins Pharmacologic treatments can interrupt or modulate the perception of pain o Pain sensation can be modified peripherally (at the site) or centrally (in the brain) Copyright © 2021 Wolters Kluwer • All Rights Reserved Physiology of Pain Copyright © 2021 Wolters Kluwer • All Rights Reserved Question #1 Is the following statement true or false? The nurse accurately explains to a child’s parents that the point at which a person feels the highest intensity of a painful stimulus is termed the pain threshold. Copyright © 2021 Wolters Kluwer • All Rights Reserved Answer to Question #1 False. The point at which a person feels the lowest intensity of a painful stimulus is termed the pain threshold. Rationale: In addition to sending a message to the cerebral cortex, the thalamus also sends a message to the limbic system, where the sensation is interpreted emotionally, and to the brain stem centers, where autonomic nervous system responses begin. Copyright © 2021 Wolters Kluwer • All Rights Reserved Classifications of Pain Duration o Acute or chronic Etiology o Nociceptive or neuropathic Source/location o Somatic or visceral Copyright © 2021 Wolters Kluwer • All Rights Reserved Factors Influencing Pain Age Gender Cognitive level Temperament Previous pain experiences Family and cultural background Situational factors Copyright © 2021 Wolters Kluwer • All Rights Reserved Myths and Misconceptions About Children and Pain Newborns don’t feel pain Exposure to pain at an early age has little or no effect later Infants and small children have little memory of pain Intensity of the child’s reaction to pain indicates intensity of pain A child who is sleeping or playing is not in pain Children are truthful when asked if they are in pain Children learn to adapt to pain and painful procedures Children experience more adverse effects of narcotic analgesics than adults do Children are more prone to addiction to narcotic analgesics Not true! (Adapted from The Hospital for Sick Children. (2005). Myths vs facts of children’s pain. Retrieved June 16, 2020, from https://s3.amazonaws.com/rdcms-iasp/files/production/public/Content/ContentFolders/GlobalYearAgainstPain2/ 20052006PaininChildren/pdfist.pdf) Copyright © 2021 Wolters Kluwer • All Rights Reserved Indicators of Pain in Infants Behavioral o Facial expressions, body movements, crying, increased irritability, refusal to move injured body part, interrupted sleep Physiologic o Changes in heart rate, respiratory rate, oxygen saturation levels, vagal tone, plantar or palmar sweating Copyright © 2021 Wolters Kluwer • All Rights Reserved Using Age-Appropriate Language to Assess Pain in Older Children Toddlers are likely to understand words such as “owie” or “boo-boo” Preschoolers may need to be coaxed to discuss their pain as they feel it is something to be expected School-age children can usually report type, location, and severity because of their well-developed language skills Teens concern about body image and fear of losing control may result in denying pain or refusing medication Copyright © 2021 Wolters Kluwer • All Rights Reserved Question #2 Is the following statement true or false? The nurse assessing pain in children is correct in stating that the school-age child is usually able to communicate the type, location, and severity of pain. Copyright © 2021 Wolters Kluwer • All Rights Reserved Answer to Question #2 True. The school-age child is usually able to communicate the type, location, and severity of pain. Rationale: Children older than the age of 8 years can use specific words, such as sharp as a knife, burning, or pulling, to describe their pain. However, they may deny pain in an attempt to appear brave or to avoid further pain related to a procedure or intervention. Copyright © 2021 Wolters Kluwer • All Rights Reserved Factors Affecting Children’s Responses to Pain Type of pain Extent of pain Age/developmental level Cultural/family norms surrounding expression of pain Copyright © 2021 Wolters Kluwer • All Rights Reserved Key Principles of Pain Assessment (QUESTT) Question the child Use a reliable and valid pain scale Evaluate the child’s behavior and physiologic changes to establish a baseline and determine the effectiveness of the intervention Secure the parent’s involvement Take the cause of pain into account when intervening Take action Copyright © 2021 Wolters Kluwer • All Rights Reserved Health History Data Related to Pain Assessment Location, quality, severity, and onset of the pain, as well as the circumstances in which the child experiences the pain. Conditions, if any, that preceded the onset of pain and conditions that followed the onset of pain Any measures that increase or decrease the pain Any associated symptoms, such as weight loss, fever, vomiting, or diarrhea, that may indicate a current illness Any recent trauma, including any interventions that were used in an attempt to relieve the pain Copyright © 2021 Wolters Kluwer • All Rights Reserved Pediatric Pain Assessment Tools FACES pain rating scale (ages 3+, emoticon-like faces) Oucher pain rating scale (ages 3+, actual photos of children, must know number values) Poker chip tool ( ages 3+, uses 1 to 4 poker chips to describe pain) Visual analog and numeric scales (ages 5+, scales of 0–10) Adolescent pediatric pain tool (ages 8 to 15, measures pain location, intensity, and quality) Copyright © 2021 Wolters Kluwer • All Rights Reserved FACES Pain Rating Scale (Source: Wong-Baker FACES Foundation 2019. Wong-Baker FACES® Pain Rating Scale. Retrieved June 9, 2020 with permission from http://www.WongBakerFACES.org) Copyright © 2021 Wolters Kluwer • All Rights Reserved Question #3 The nurse is assessing the pain of a 3-year-old child. Which of the following pain assessment scales would be most appropriate? a. Visual analog scale b. Visual numeric scale c. Word-graphic rating scale d. FACES pain rating scale Copyright © 2021 Wolters Kluwer • All Rights Reserved Answer to Question #3 d. FACES pain rating scale. The FACES pain rating scale would be most appropriate for a 3-year-old. Rationale: The FACES pain rating scale is a self-report tool that can be used by children as young as 3 or 4 years of age. The word-graphic rating scale is useful for children between 4 and 17 years old. The visual analog scale can be used with children 7 years or older. The numeric scale can be used with children 8 years or older. Copyright © 2021 Wolters Kluwer • All Rights Reserved Pediatric Physiologic and Behavioral Pain Assessment Tools Premature Infant Pain Profile Neonatal Infant Pain Scale Riley Infant Pain Scale Pain Observation Scale for Young Children CRIES Scale for Neonatal Postoperative Pain Assessment FLACC Behavioral Scale for Postoperative pain in Young Children Copyright © 2021 Wolters Kluwer • All Rights Reserved Pain Management Guide for Children Individualize interventions based on the amount of pain experienced and the child’s characteristics, such as developmental level, temperament, previous pain experience, and coping strategies Use nonpharmacologic and pharmacologic approaches to ease or eliminate the pain Teach the child and family about pain-relief interventions and techniques and discuss with the child and family expectations of pain management Copyright © 2021 Wolters Kluwer • All Rights Reserved Techniques for Pain Management Nonpharmacologic o Relaxation, distraction, guided imagery, massage Pharmacologic o Analgesics, patient-controlled analgesia, local analgesia, epidural analgesia, conscious sedation Copyright © 2021 Wolters Kluwer • All Rights Reserved Behavioral-Cognitive Pain Management Strategies Relaxation Distraction Imagery Biofeedback Thought stopping Positive self-talk Copyright © 2021 Wolters Kluwer • All Rights Reserved Biophysical Interventions for Pain Management Nonnutritive sucking with sucrose (infants or toddlers) Heat and cold applications Massage and pressure Copyright © 2021 Wolters Kluwer • All Rights Reserved Factors Affecting the Choice of Pharmacologic Interventions for Pain Drug being administered The child’s status The type, intensity, and location of the pain Any factors that may be influencing the child’s pain Copyright © 2021 Wolters Kluwer • All Rights Reserved Medications Used for Pain Management Analgesics o Nonopioid and opioids Adjuvant o Benzodiazepines o Anticonvulsants Anesthetics Preferred routes o Oral, rectal, intravenous, topical, or local nerve block routes o Epidural administration and moderate sedation also can be used Copyright © 2021 Wolters Kluwer • All Rights Reserved Nurse’s Role in Pharmacologic Pain Management Adhering to the rights of medication administration Knowledge about the drug’s pharmacokinetics and pharmacodynamics Assessment is crucial and ongoing o Monitor physiologic parameters level of consciousness vital signs oxygen saturation levels urinary output monitor for signs of adverse effects (respiratory depression) o Assess the child’s and parents’ emotional status o Teach the child and parent’s about the drug Copyright © 2021 Wolters Kluwer • All Rights Reserved Common Adverse Events Associated With Use of Opioid Medications Constipation Pruritus Nausea and vomiting Copyright © 2021 Wolters Kluwer • All Rights Reserved Required Interventions When a Child Is Receiving Moderate (Conscious) Sedation Moderate sedation is a medically controlled state of depressed consciousness Ensuring that emergency equipment is readily available Maintaining a patent airway Monitoring the child’s level of consciousness and responsiveness Assessing the child’s vital signs (especially pulse rate, heart rate, blood pressure, and respiratory rate) Monitoring oxygen saturation levels Copyright © 2021 Wolters Kluwer • All Rights Reserved Nurse’s Role in Managing ProcedureRelated Pain Use topical anesthetic at site of a skin or vessel puncture Use nonpharmacologic strategies for pain relief Prepare child/family ahead of time about the procedure Use therapeutic hugging to secure the child Use the smallest-gauge needle possible Use intermittent infusion device or PICC for multiple samples Opt for venipuncture in newborns instead of heel sticks if large amount needed Use kangaroo care for newborns before and after heel stick Provide nonnutritive sucking before the procedure Copyright © 2021 Wolters Kluwer • All Rights Reserved Nurse’s Role in Managing Chronic Pain Similar to that for the child experiencing acute pain or procedurerelated pain Assessment of the child’s pain is key o Onset, duration, intensity, and location of pain o Alleviating or exacerbating factors o Impact on child’s daily life o Effect on child and family’s stress level o Methods used to alleviate pain (including home remedies or alternative therapies) o Physical examination Multiple nonpharmacologic and pharmacologic strategies combined to provide pain relief Copyright © 2021 Wolters Kluwer • All Rights Reserved