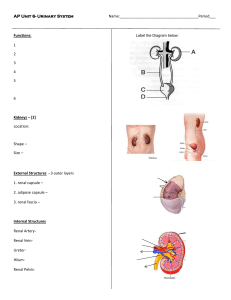
Essentials of Human Anatomy & Physiology Unit 12: The Urinary System Organs of the Urinary system Kidneys (2) Ureters (2) Urinary bladder (1) Urethra (1) Location of the Kidneys Dimensions Reddish-brown, bean shaped 12cm long, 6cm wide, 3cm thick High on posterior abdominal wall at the level of T12 to L3- superior lumbar region Retroperitoneal & against the dorsal body wall The right kidney is slightly lower than the left ,convex laterally Attached to ureters, renal blood vessels, and nerves at renal hilus (medial indention) Atop each kidney is an adrenal gland Coverings of the Kidneys Adipose capsule Surrounds the kidney Provides protection to the kidney Helps keep the kidney in its correct location against muscles of posterior trunk wall Ptosis-kidneys drop to a lower position due to rapid fat loss, creating problems with the ureters. Ptosis can lead to hydronephrosis, a condition where urine backs up the ureters and exerts pressure on the kidney tissue. Renal capsule Surrounds each kidney Regions of the Kidney Three regions of kidneys Renal cortex – outer region, forms an outer shell Renal columns – extensions of cortex- material inward Renal medulla – inside the cortex, contains medullary (renal) pyramids Medullary pyramids – triangular regions of tissue in the medulla, appear striated Renal pelvis – inner collecting tube, divides into major and minor calyces Calyces – cup-shaped structures enclosing the tips of the pyramids that collect and funnel urine towards the renal pelvis Functions of the Urinary System Elimination of waste products filtering gallons of fluid from the bloodstream every day creating “filtrate” “filtrate” includes: metabolic wastes, ionic salts, toxins, drugs Maintenance of blood Red blood cell production- by producing hormone erythropoietin to stimulate RBC production in bone marrow Blood pressure (vessel size)- by producing renin which causes vasoconstriction Blood volume (water balance)- ADH released from Anterior Pituitary targets the kidney to limit water loss when blood pressure decreases or changes in blood composition Blood composition (electrolyte balance)- water follows salt; aldosterone reclaims sodium to the blood Blood pH- regulates H+ ions and HCO3- ions Blood Flow in the Kidneys Rich blood supply to filter blood and adjust blood composition ~¼ of blood supply passes through the kidneys each minute Blood enters the kidneys under extremely high pressure Renal artery arises from abdominal aorta, divides into Segmental artery at hilus Inside renal pelvis, Segmental artery divides into Lobar artery, which branch into Interlobar artery travelling thru the renal column to reach the renal cortex At the medulla-cortex junction, the Interlobar artery curves over the medullary pyramids as the Arcuate artery. Small Interlobular arterioles branch off of the Arcuate artery and move away from the renal cortex and into the Nephron of the kidney Blood Flow in the Kidneys The final branches of the interlobular arteries are called afferent arterioles. Afferent arterioles lead to the glomerulus, a network of capillaries that are involved in filtration. Leading away from the glomerulus, blood less filtrate travels through the efferent arterioles and into the peritubular capillaries. From there, blood moves through similar veins that parallel the arteries at their respective locations. Nephrons The structural and functional units of the kidneys Over 1 million Responsible for forming urine Consist of renal corpuscle and renal tubule Renal corpuscle composed of a knot of capillaries called the Glomerulus (a.k.a. Bowman’s Capsule) Renal tubule- enlarged, closed, cup-shaped end giving rise to the PCT, dLOH, aLOH, DCT, and CD. Glomerulus A specialized capillary bed fed and drained by arterioles. Glomerular capillaries filter fluid from the blood into the renal tubule GC is attached to arterioles on both sides in order to maintain high pressure Large afferent arteriole-arises from interlobular artery (feeder vessel); large in diameter, high resistance vessels that force fluid & solutes (filtrate) out of the blood into the glomerular capsule. 99% of the filtrate will be reclaimed by the renal tubule cells and returned to the blood in the peritubular capillary beds(blood vessels surrounding renal tubule) . Narrow efferent arteriole-merges to become the interlobular vein; draining vessel. Glomerulus Glomerular capillaries are covered with podocytes from the inner (visceral) layer of the glomerular capsule. Podocytes have long, branching processes called pedicels that intertwine with one another and cling to the glomerular capillaries. Filtration slits between the pedicels form a porous membrane around the glomerular capillaries. The glomerular capillaries sit within a glomerular capsule (Bowman’s capsule) Expansion of renal tubule Receives filtered fluid Renal tubule coils into the PCT, then the dLOH, aLOH, DCT and finally, the CD. Along the PCT, much of the filtrate is reclaimed Renal Tubule Glomerular (Bowman’s) capsule enlarged beginning of renal tubule Proximal convoluted tubule- lumen surface (surface exposed to filtrate) is covered with dense microvilli to increase surface area. The descending limb of the nephron Loop of Henle The ascending limb of the nephron coils tightly again into the distal convoluted tubule Many DCT’s merge in renal cortex to form a collecting duct Collecting ducts not a part of nephron Collecting ducts receive urine from nephrons and deliver it to the major calyx and renal pelvis. CD run downward through the medullary pyramids, giving them their striped appearance. Blood Supply of a Nephron Peritubular capillary Efferent arteriole braches into a second capillary bed Blood under low pressure Capillaries adapted for reabsorption instead of filtration. Attached to a venule and eventually lead to the interlobular veins to drain blood from the glomerulus Cling close to the renal tubule where they receive solutes and water from the renal tubule cells as these substances from the filtrate are reabsorbed into the blood. Juxtaglomerular apparatus At origin of the DCT it contacts afferent and efferent arterioles Epithelial cells of DCT narrow and densely packed, called macula densa Together with smooth muscle cells, comprise the juxtaglomerular apparatus Control renin secretion & indirectly, aldosterone secretion Types of Nephrons Cortical nephrons Located entirely in the cortex Includes most nephrons Juxtamedullary nephrons Found at the boundary of the cortex and medulla and their LOH dip deep into the medulla. Urine Formation Processes Filtration- Water & solutes smaller than proteins are forced through the capillary walls and pores (of the glomerulus) into the renal tubule (Bowman’s capsule). Reabsorption- Water, glucose, amino acids & needed ions are transported out of the filtrate into the peritubular capillary cells and then enter the capillary blood. Secretion- Hydrogen ions, Potassium ions, creatinine & drugs are removed from the peritubular capillaries (blood) and secreted by the peritubular capillary cells into the filtrate. Filtration Beginning step of urine formation Occurs at the glomerulus, nonselective passive process Water and solutes smaller than proteins are forced through capillary walls of the glomerulus, which act as a filter. Fenestrations – (openings in glomerular walls) make glomerulus more permeable than other arterioles. Podocytes cover capillaries, make membrane impermeable to plasma proteins. Blood cells cannot pass out to the capillaries; filtrate is essentially blood plasma w/o blood proteins, blood cells. Filtrate is collected in the glomerular (Bowman’s) capsule and leaves via the renal tubule Filtration pressure Hydrostatic pressure of blood forces substances through capillary wall. Net filtration pressure normally always positive Hydrostatic pressure of blood is greater than the hydrostatic pressure of the glomerulus capsule and the osmotic pressure of glomerulus plasma If arterial blood pressure falls dramatically, the glomerular hydrostatic pressure falls below level needed for filtration. The epithelial cells of renal tubules lack nutrients and cells die. Can lead to renal failure. Filtration rate Rate of filtration is directly proportional to net filtration pressure. Regulation of filtration rate Rate typically constant; may need to increase or decrease to maintain homeostasis 1. Sympathetic nervous system reflexes Respond to drops in blood pressure and blood volume As pressure drops, sympathetic nerves cause vasoconstriction of afferent arterioles. Decreases rate of filtration Less urine produced, water is conserved As pressure rises, sympathetic nerves cause vasoconstriction of efferent arterioles. Increases rate of filtration More urine produced, water is removed Filtration rate 2. Renin production by JGA Renin is an enzyme controlling filtration rate Juxtaglomerular cells secrete renin in response to 3 stimuli Sympathetic stimulation (fast response) Specialized pressure receptors in afferent arterioles sense decrease in blood pressure Macula densa senses decrease in chloride, potassium, and sodium ions reaching distal tubule Released renin reacts with angiotensinogen in bloodstream to form angiotensin I which is converted into angiotensin II by the angiotensin I converting enzyme, ACE Angiotensin II acts to vasoconstrict efferent arteriole Blood backs up into glomerulus, increasing pressure and maintains filtration rate Angiotension II also stimulates secretion of aldosterone from adrenal glands Stimulates tubular reabsorption of sodium & H2O follows Reabsorption The composition of urine is different than the composition of glomerular filtrate. Tubular reabsorption returns substances to the internal environment of the blood by moving substances through the renal tubule walls into the peritubular capillaries (99%) Some water, ions, glucose, amino acids Some reabsorption is passive = water osmosis = small ions diffusion Most is active using protein carriers by active transport Most reabsorption occurs in the proximal convoluted tubule, where microvilli cells act as transporters, taking up needed substances from the filtrate and absorbing them into the peritubular capillary blood. Substances that remain in the renal tubule become more concentrated as water is reabsorbed from the filtrate. Reabsorption – sodium and water The sodium potassium pump reabsorbs 70% of sodium ions in the PCT. The positive sodium ions attract negative ions across the membrane as well Water reabsorption occurs passively across the membrane to areas of high solute concentration Therefore, more sodium reabsorption = more water reabsorption Active transport of sodium ions occurs along remainder of nephron and collecting duct Almost all sodium ions and water are reabsorbed. Materials Not Reabsorbed Nitrogenous waste products Urea – formed by liver; end product of protein breakdown when amino acids are used to produce energy Uric acid – released when nucleic acids are metabolized Creatinine – associated with creatine metabolism in muscle tissue Excess water Secretion – Reabsorption in Reverse Some materials move from the peritubular capillaries into the renal tubules to be eliminated in urine. Example: Hydrogen ions; potassium ions Creatinine Drugs; penicillin; histamine Process is important for getting rid of substances not already in the filtrate or for controlling pH. Materials left in the renal tubule move toward the ureter Formation of Urine Summary: • glomerular filtration of materials from blood plasma •Reabsorption of substances, including glucose; water, sodium •Secretion of substances, including penicillin, histamine, hydrogen and potassium ions Maintaining Water Balance Normal amount of water in the human body Young adult females – 50% Young adult males – 60% Babies – 75% Old age – 45% Water is necessary for many body functions and levels must be maintained Distribution of Body Fluid Intracellular fluid (inside cells) Extracellular fluid (outside cells) Interstitial fluid Blood plasma The Link Between Water and Salt Changes in electrolyte balance causes water to move from one compartment to another Alters blood volume and blood pressure (think of aldosterone) Can impair the activity of cells (swelling/edema) Water intake must equal water output Sources for water intake/output: Intake: Ingested foods and fluids, Water produced from metabolic processes (glycolysis) Output: Vaporization out of the lungs, Lost in perspiration, Leaves the body in the feces, Urine production Dilute vs. Concentrated Urine Dilute urine is produced if water intake is excessive Less urine (concentrated) is produced if large amounts of water are lost Proper concentrations of various electrolytes must be present Regulation of Water and Electrolyte Reabsorption Regulation is primarily by hormones Antidiuretic hormone (ADH) prevents excessive water loss in urine Neurons in the hypothalamus produce ADH, which are released by the anterior pituitary gland in response to a decrease in blood volume or water concentration ADH increases the water permeability of the distal convoluted tubule epithelium to the peritubular capillaries Decreases volume of urine, increasing concentration of solutes Negative feedback control Aldosterone regulates sodium ion content of extracellular fluid Triggered by the renin-angiotensin mechanism Stimulates the DCT to reabsorb sodium and excrete potassium Cells in the kidneys and hypothalamus are active monitors Maintaining Water and Electrolyte Balance Maintaining Acid-Base Balance in Blood Blood pH must remain between 7.35 and 7.45 to maintain homeostasis Alkalosis – pH above 7.45 Acidosis – pH below 7.35 Most acid-base balance is maintained by the kidneys Excrete bicarbonate ions if needed Conserve / generate new bicarbonate ions if needed Excrete hydrogen ions if needed Conserve / generate new hydrogen ions if needed Regulation of these ions results in a urine pH range of 4.5 to 8.0 Acidic urine: protein-rich diet, starvation, diabetes Basic urine: bacterial infections, vegetarian diet Characteristics of Urine Used for Medical Diagnosis Colored somewhat yellow due to the pigment urochrome (from the destruction of hemoglobin/bilirubin byproduct) and solutes Sterile Slightly aromatic Normal pH of around 6 Specific gravity of 1.001 to 1.035 Urine composition Composition differs considerably based upon diet, metabolic activity, urine output. ~95% water, contains urea and uric acid, electrolytes and amino acids (trace amount) Volume produced ranges from 0.6-2.5 liters per day (1.8L average). Depends on fluid intake, body and ambient air temperature, humidity, respiratory rate, emotional state Output of 50-60ml per hour normal, less than 30ml per hour may indicate kidney failure Ureters Slender tubes attaching the kidney to the bladder 10-12” long & ¼” diameter Superior end is continuous with the renal pelvis of the kidney Mucosal lining is continuous with that lining the renal pelvis and the bladder below. Enter the posterior aspect of the bladder at a slight angle Runs behind the peritoneum Peristalsis aids gravity in urine transport from the kidneys to the bladder. Smooth muscle layers in the ureter walls contract to propel urine. There is a valve-like fold of bladder mucosa that flap over the ureter openings to prevent backflow. Renal calculi= calculus means little stone; result of precipitated uric acid salts created by bacterial infections, urinary retention, and alkaline urine. Lithotripsy or surgery are common treatments. Urinary Bladder Smooth, collapsible, muscular sac Temporarily stores urine Located retroperitoneally in the pelvis posterior to the pubic symphysis. Urinary Bladder Trigone – three openings Two from the ureters (ureteral orifices) One to the urethra (internal urethral orifice) which drains the bladder. Common site for bacterial infections In males, prostate gland surrounds the neck of the bladder where it empties into the urethra. Urinary Bladder Wall Three layers of smooth muscle (detrusor muscle) Mucosa made of transitional epithelium Walls are thick and folded in an empty bladder 2-3” long Bladder can expand significantly without increasing internal pressure As it fills, the bladder rises superiorly in the abdominal cavity becoming firm and pear shaped. A moderately full bladder can hold ~500mL (1 pint) of urine. A full bladder can stretch to hold more than twice that amount. Urethra Thin-walled tube that carries urine from the bladder to the outside of the body by peristalsis Release of urine is controlled by two sphincters Internal urethral sphincter (involuntary) – a thickening of smooth muscle at the bladder-urethra jxn. keeps urethra closed when urine is not being passed. External urethral sphincter (voluntary) -skeletal muscle that controls urine as the urethra passes through the pelvic floor. Urethra Gender Differences Length Females – 3–4 cm (1-1.5 inches) Males – 20 cm (7-8 inches) Location Females – along wall of the vagina Males – through the prostate and penis Function Females – only carries urine Males – carries urine and is a passageway for sperm cells Urethra Gender Differences Females: •Feces can enter urethral opening causing •Uretritis-inflammation of the urethra •Pyelitis or pyelonephritis-inflammation of the kidneys •Urinary tract infections-bacterial infection •Dysuria •Urgency •Frequency •Fever •Cloudy urine •Bloody urine Males: •Prostatic, membranous and spongy (penile) urethrae •Enlargement of the prostate gland causes urinary retention •can be corrected with a catheter Micturition (Voiding) Both sphincter muscles must open to allow voiding The internal urethral sphincter is relaxed after stretching of the bladder ~200mL Activation is from an impulse sent to the spinal cord and then back via the pelvic nerves The external urethral sphincter must be voluntarily relaxed Incontinence-inability to control micturition Retention-inability to micturate