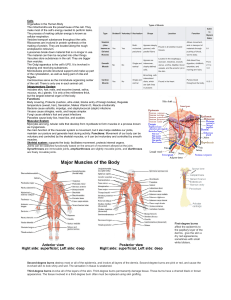
PSORIASIS Diagnosis & Management Maria Lourdes B. Galima WHAT IS PSORIASIS? – Inflammatory and hyperplastic disease of skin – Characterized by erythema and elevated scaly plaques – Chronic, relapsing condition – Course of disease often unpredictable 2 WHAT IS PSORIASIS? • A noncontagious common skin condition that causes rapid skin cell reproduction resulting in red, dry patches of thickened skin. • Commonly affects the skin of the elbows, knees, and scalp. EPIDEMIOLOGY • Prevalence equal in males and females • Estimated incidence: ~ 60 per 100,000 per year3 4 WHO CAN GET PSORIASIS? • Psoriasis is seen worldwide, in all races, and both sexes, in approximately 125 million people. • Ranked among the top 20 dermatologic cases seen every year at the University of the Philippines-Philippine General Hospital Dermatology Clinic, with 10 new Psoriasis cases seen each day WHO CAN GET PSORIASIS? • Others have very severe psoriasis where virtually their entire body is fully covered with thick, red, scaly skin. • Psoriasis is considered a non-curable, longterm (chronic) skin condition. • It has a variable course, periodically improving and worsening. COMMON SITES AFFECTED BY PSORIASIS • Can affect any part of the body – typically scalp, elbow, knees and sacrum1 • Extent of disease varies 7 WHAT CAUSES PSORIASIS? • Cause of psoriasis remains unknown. • Combination of risk factors, including genetic predisposition and environmental factors. GENETIC INFLUENCE 9 • Evidence suggests strong genetic association – Studies of monozygotic twins show concordance for psoriasis (e.g. 64% in a Danish Study) – Multiple susceptibility loci have been identified • Disease expression – likely result of genetic and environmental factors WHAT CAUSES PSORIASIS? • Common to be found in members of the same family. • The immune system is thought to play a major role. COMMON TRIGGER FACTORS FOR PSORIASIS • • • • • • • Infections (e.g. streptococcal, viral) Skin trauma (Koebner phenomenon) Psychological stress Drugs (e.g. lithium, beta blockers) Sunburn Metabolic factors (e.g. calcium deficiency) Hormonal factors (e.g. pregnancy) 11 PSORIASIS IS A T-CELL MEDIATED, AUTOIMMUNE DISEASE • Current hypothesis: – Unknown skin antigens stimulate immune response • Antigen-specific memory T-cells are primary mediators – Leads to impaired differentiation and hyperproliferation of keratinocytes 12 WHAT DOES PSORIASIS LOOK LIKE? • Typically looks like red or pink areas of thickened, raised, and dry skin. • Affects areas over the elbows, knees, and scalp. • Any body area may be involved. • More common in areas of trauma, repeated rubbing, use, or abrasions. WHAT DOES PSORIASIS LOOK LIKE? • It may be small flattened bumps, large thick plaques of raised skin, red patches, and mildly dry pink skin to big flakes of dry skin that flake off. • Covered by white, silvery scales CHARACTERISTIC LESION OF PSORIASIS • Sharply demarcated erythematous plaque with micaceous silvery white scale • Histopathology – Thickening of the epidermis – Tortuous and dilated blood vessels – Inflammatory infiltrate primarily of lymphocytes TYPES OF PSORIASIS • • • • Chronic plaque Guttate Flexural Erythrodermic 16 • Pustular – Localized and generalized • Local forms – Palmoplantar – Scalp – Nail (psoriatic onychodystrophy) PSORIASIS VULGARIS • Psoriasis vulgaris is the medical name for the most common form of psoriasis ("vulgaris" means common). • About 80% of people with psoriasis have this type. PSORIASIS VULGARIS • Also called plaque psoriasis because of the characteristic plaques on the skin: – well-defined patches of red raised skin that can appear on any area of skin, although the knees, elbows, scalp, trunk, and nails are the most common locations. PSORIASIS VULGARIS • The flaky silvery white buildup on top of the plaques is called scale; - it is composed of dead skin cells. - This scale comes loose and sheds constantly from the plaques. 19 PSORIATIC PLAQUE SEVERITY OF DISEASE • Three Cardinal Signs of Psoriatic Lesions – Plaque elevation – Erythema – Scale • Body Surface Area CHRONIC PLAQUE PSORIASIS • Most Common Variant • Plaques may be as large as 20 cm • Symmetrical disease • Sites of Predilection – Elbows – Knees – Presacrum – Scalp – Hands and Feet CHRONIC PLAQUE PSORIASIS 23 CHRONIC PLAQUE PSORIASIS CHRONIC PLAQUE PSORIASIS • May be widespread – up to 90% BSA • Genitalia involved in up to 30% of patients • Most patients have nail changes – Nail pitting – “Oil Spots” – Involvement of the entire nail bed • Onychodystrophy • Loss of nail plate WIDESPREAD CHRONIC PLAQUE PSORIASIS 26 WIDESPREAD CHRONIC PSORIASIS 27 CHRONIC PSORIASIS SYMPTOMS OF CHRONIC PLAQUE PSORIASIS • • • • Pruritus Pain Excessive heat loss Patient Complaints – – – – Unsightliness of the lesions Low self-esteem Feelings of being socially outcast Excessive scale CHRONIC PLAQUE PSORIASIS 30 CHRONIC PLAQUE PSORIASIS 31 CHRONIC PLAQUE PSORIASIS 32 GUTTATE PSORIASIS • Guttate psoriasis is a type of psoriasis that looks like small, salmon-pink drops on the skin. • The word guttate is derived from the Latin word gutta, meaning drop. • Usually there is a fine scale on the droplike lesion that is much finer than the scales in plaque psoriasis. GUTTATE PSORIASIS – Numerous and small lesions – ~ 1 cm diameter – Pink with less scale than plaque psoriasis – Commonly found on trunk and proximal limbs – Typically seen in individuals < 30 years – Often preceded by an upper respiratory tract streptococcal infection 34 GUTTATE PSORIASIS • The trigger to the disease is often a preceding streptococcal (bacterial) infection. • The eruption of the lesions on the skin usually happens about two to three weeks after the person has strep throat. • Characterized by numerous 0.5 to 1.5 cm papules and plaques • Most common form in children GUTTATE PSORIASIS INVERSE/FLEXURAL PSORIASIS – Lesions in skin folds – Particularly groin, gluteal cleft, axillae and submammary regions – Often minimal or absent scaling – May cause diagnostic difficulty when genital or perianal region is affected in isolation 37 INVERSE/FLEXURAL PSORIASIS • Inverse/Flexural psoriasis consists of bright red, smooth (not scaly) patches found in the folds of the skin. • The most common areas are under the breasts, in the armpits, near the genitals, under the buttocks, or in abdominal folds. INVERSE/FLEXURAL PSORIASIS • These irritated and inflamed areas are aggravated by the sweat and skin rubbing together in the folds. • Yeast overgrowth, common in skin folds, may trigger the skin lesions of psoriasis. INVERSE/FLEXURAL PSORIASIS 40 LIFE–THREATENING FORMS OF PSORIASIS • Generalized Pustular Psoriasis • Erythrodermic Psoriasis 41 PUSTULAR PSORIASIS • Pustular psoriasis is an uncommon form of psoriasis. • People with pustular psoriasis have clearly defined, raised bumps on the skin that are filled with pus (pustules). • The skin under and around these bumps is reddish. GENERALIZED PUSTULAR PSORIASIS • Unusual manifestation of psoriasis • Can have a gradual or an acute onset • Characterized by waves of pustules on erythematous skin often after short episodes of fever of 39˚ to 40˚C • Weight loss • Muscle Weakness • Hypocalcemia • Leukocytosis • Elevated ESR GENERALIZED PUSTULAR PSORIASIS • Cause is obscure • Triggering Factors – Infection – Pregnancy – Lithium – Hypocalcemia secondary to hypoalbuminemia – Irritant contact dermatitis – Withdrawal of glucocorticosteroids, primarily systemic GENERALIZED PUSTULAR PSORIASIS PUSTULAR PSORIASIS • Pustular psoriasis may cause large portions of the skin to redden. • The skin changes that occur before, during, or after an episode of pustular psoriasis can be similar to those of regular psoriasis. PUSTULAR PSORIASIS ERYTHRODERMIC PSORIASIS • This is the least common type of psoriasis and can be quite serious. • A very large area of the body, if not most of the body, is bright red and inflamed. • The body can appear to be covered in a peeling red rash. The rash usually itches or burns. ERYTHRODERMIC PSORIASIS • Classic lesion is lost • Entire skin surface becomes markedly erythematous with desquamative scaling. • Often only clues to underlying psoriasis are the nail changes and usually facial sparing ERYTHRODERMIC PSORIASIS • Triggering Factors – Systemic Infection – Withdrawal of high potency topical or oral steroids – Withdrawal of Methotrexate – Phototoxicity – Irritant contact dermatitis ERYTHRODERMIC PSORIASIS ERYTHRODERMIC PSORIASIS PSORIASIS OF THE SCALP • The scalp may have fine, dry, scaly skin or have heavily crusted plaque areas. • The plaque can flake off or peel off in crusted clumps. • Sometimes psoriasis of the scalp is confused with seborrheic dermatitis. • A key difference is that in seborrheic dermatitis, the scales are greasy looking, not dry. SCALP PSORIASIS – Varies from minor scaling with erythema to thick hyperkeratotic plaques – May extend beyond hairline1,2 – Patient scratching may produce asymmetric plaques 54 PSORIATIC ARTHRITIS • Psoriatic arthritis is a specific condition in which a person has both psoriasis and arthritis. PSORIATIC ARTHRITIS • Rarely, a person can have psoriatic arthritis without having skin psoriasis. • Arthritis can precede the psoriasis by months or years, or present after years of psoriasis. CAN PSORIASIS AFFECT ONLY NAILS? • More commonly, the nail symptoms accompany the skin and arthritis symptoms. • Nails affected by psoriasis can have small pinpoint pits or large yellowish separations of the nail plate called "oil spots." CAN PSORIASIS AFFECT ONLY NAILS? • Nail psoriasis is typically very difficult to treat, but it can respond to medications taken internally to treat psoriasis or psoriatic arthritis. PSORIASIS OF THE NAIL • potent topical steroids applied at the nail-base cuticle, • injection of steroids at the nail-base cuticle, and • oral or systemic medications PSORIASIS OF THE NAIL NAIL PSORIASIS NAIL PSORIASIS NAIL PSORIASIS NAIL PSORIASIS PALMOPLANTAR PSORIASIS – Can be hyperkeratotic or pustular – May mimic dermatitis – look for psoriatic manifestations elsewhere to aid diagnosis – Possibly aggravated by trauma IS PSORIASIS CURABLE? • Psoriasis is not currently curable. • However, it can go into remission and show no signs of disease. IS PSORIASIS CONTAGIOUS? • You cannot catch it from anyone, and you cannot pass it to anyone else via skin-to-skin contact. • You can directly touch someone with psoriasis every day and never develop the skin condition. FACTORS THAT MAY TRIGGER PSORIASIS. • Injury to the skin: - Injury to the skin has been associated with plaque psoriasis. - For example, a skin infection, skin inflammation, or even excessive scratching can trigger psoriasis. • Sunlight: - Most people generally consider sunlight to be beneficial for their psoriasis. However, a small minority find that strong sunlight aggravates their symptoms. -A bad sunburn may worsen psoriasis. FACTORS THAT MAY TRIGGER PSORIASIS • Streptococcal infections: - Some evidence suggests that streptococcal infections may cause a type of plaque psoriasis. - These bacterial infections have been shown to cause guttate psoriasis, a type of psoriasis that looks like small red drops on the skin. • HIV: - Psoriasis typically worsens after an individual has been infected with HIV. However, psoriasis often becomes less active in advanced HIV infection. FACTORS THAT MAY TRIGGER PSORIASIS • Drugs: A number of medications have been shown to aggravate psoriasis. Some examples are as follows: – Lithium: Drug that may be used to treat depression – Beta-blockers: Drugs that may be used to treat high blood pressure – Antimalarials: Drugs used to treat malaria – NSAIDs: Drugs, such as ibuprofen (Motrin and Advil) or naproxen (Aleve), used to reduce inflammation FACTORS THAT MAY TRIGGER PSORIASIS • Emotional stress: - Many people see an increase in their psoriasis when emotional stress is increased. • Smoking: - Cigarette smokers have an increased risk of chronic plaque psoriasis. • Alcohol: - Alcohol is considered a risk factor for psoriasis, particularly in young to middle-aged males. FACTORS THAT MAY TRIGGER PSORIASIS • Hormone changes: - The severity of psoriasis may fluctuate with hormonal changes. - Disease frequency peaks during puberty and menopause. - A pregnant woman's symptoms are more likely to improve than worsen, if any changes occur at all. - In contrast, symptoms are more likely to flare in the postpartum period, if any changes occur at all. DIAGNOSING PSORIASIS • Other dermatological disorders can resemble psoriasis • Diagnosed clinically according to appearance, distribution, history of lesions and family history • Important to consider non-cutaneous complications 73 DIFFERENTIAL DIAGNOSIS • Localised patches/plaques – Tinea – Eczema – Superficial basal cell carcinoma and Bowen’s disease – Seborrhoeic dermatitis – Cutaneous T-cell lymphoma (mycosis fungoides) • Guttate – Pityriasis rosea – Drug eruption – Secondary syphilis • Flexural – – – – Tinea Eczema Candidiasis Seborrhoeic dermatitis • Erythrodermic – – – – – Eczema Cutaneous T-cell lymphoma Pityriasis rubra pilaris Lichen planus Drug • Palmoplantar – Tinea CAN I PASS PSORIASIS ON TO MY CHILDREN? • Yes, it is possible. • Psoriasis may be inherited from parents to their children or other ancestors. • It does tend to run in some families, and a family history is helpful in making the diagnosis. MEDICAL TREATMENT – TOPICAL AGENTS • Medications applied directly to the skin are the first course of treatment options. • The main topical treatments are corticosteroids (cortisone like creams, gels, liquids, sprays, or ointments), vitamin D-3 derivatives, coal tar, anthralin, or retinoids. MEDICAL TREATMENT – TOPICAL AGENTS • Because each drug has specific adverse effects or loses potency over time, it is common to rotate them. • Sometimes topical preparations are combined together. - For example, keratolytics (substances used to break down scales or excess skin cells) are often added to these preparations. MEDICAL TREATMENT – TOPICAL AGENTS • Some preparations should never be mixed together because they interfere with each other. - For example, salicylic acid inactivates calcipotriene cream or ointment (a form of vitamin D-3). • On the other hand, drugs such as anthralin (tree bark extract) may require the addition of salicylic acid to work effectively. MEDICAL TREATMENT – PHOTOTHERAPY (LIGHT THERAPY) • The ultraviolet (UV) light from the sun slows the production of skin cells and reduces inflammation. • If psoriasis is widespread, as defined by more patches than can easily be counted, then artificial light therapy may be used. • Resistance to topical treatment is another indication for light therapy. MEDICAL TREATMENT – PHOTOTHERAPY (LIGHT THERAPY) • Proper facilities are required for the two main forms of light therapy. • Medical light sources use particular wavelengths of light. • Sunlamps and tanning booths are usually not acceptable as substitutes for medical light sources. ULTRAVIOLET B (UV-B) • Usually combined with one or more topical treatments and is extremely effective for treating moderate to severe plaque psoriasis. • UV-B is light with wavelengths of 290-320 nanometers (nm), shorter than the range of visible light (visible light ranges from 400-700 nm). • The major drawbacks of this therapy are the time commitment required for treatments and the accessibility of UV-B equipment. PUVA • Is the therapy that combines a psoralen drug (taken by mouth) with ultraviolet A (UV-A) light therapy (UV-A is light with wavelengths of 320-400 nm). • Psoralen drugs make the skin more sensitive to light and the sun. • More than 85% of patients report relief of disease symptoms with 20-30 treatments. • Therapy is usually given two to three times per week on an outpatient basis, with maintenance treatments every two to four weeks until remission. ADVERSE EFFECTS OF PUVA THERAPY • Adverse effects of PUVA therapy include nausea, itching, and burning. • Long-term complications include increased risks of sensitivity to the sun, sunburn, skin cancer, and cataracts. • Protective glasses must be worn during and after treatment to prevent cataracts. • PUVA therapy is not used for children younger than 12 years of age. TREATMENT: LASER THERAPY • This lets doctors aim the treatment at affected areas without exposing healthy skin. TREATMENT: LASER THERAPY 85 • Laser therapy may have fewer side effects and a smaller risk of skin cancer compared to traditional phototherapy. • It also appears to deliver results with fewer treatments. NATURAL REMEDIES FOR PSORIASIS • Natural alternatives include aloe, tea tree oil, and oatmeal baths to soothe itchy skin. • Although alcohol has been linked to psoriasis, experts are skeptical about special diets that claim to treat psoriasis. • There's no convincing evidence that they work 86 CLIMATOTHERAPY • For decades, people have claimed that visiting the Dead Sea in Israel is a powerful treatment for psoriasis. • The sun and water, which is 10 times saltier than the ocean, are believed to be a healing combination. CLIMATOTHERAPY 88 • It may sound like a myth, but scientific evidence suggests this form of climatotherapy works. • In studies, 80% to 90% of patients improved after visiting the Dead Sea. • Almost half saw their rash disappear for the next several months. STRESS REDUCTION • Relaxation techniques may help control flareups. • Anything that helps you relax, whether it's yoga, deep breathing, or a long walk, may help ease your symptoms. SOCIAL SUPPORT • Isolation can lead to stress and depression, which tend to make symptoms worse. • Experts recommend staying connected to the people you trust. SYSTEMIC AGENTS (DRUGS TAKEN WITHIN THE BODY) • These drugs are often started for psoriasis after both topical treatment and phototherapy have failed. • These agents are potent drugs given by mouth or injection and block inflammation which can slow the growth of skin cells in psoriasis. • Examples include methotrexate (Rheumatrex, Trexall), adalimumab (Humira), and infliximab (Remicade). • Systemic agents may also be considered for psoriatic arthritis. • People whose disease is disabling because of physical, psychological, social, or economic reasons may also be considered for systemic treatment. WHAT IS THE LONG-TERM PROGNOSIS IN PATIENTS WITH PSORIASIS? • Overall, the prognosis for most patients with psoriasis is good. • Many newer medications have led to excellent results." • There have been a few studies showing a possible association of psoriasis and other medical conditions, including obesity and heart disease. LOCALIZED PATCHES/PLAQUES 94 – Tinea corporis1 • Affects body • Lacks symmetrical lesions • Presence of peripheral scale and central clearing Tinea coporis Psoriasis LOCALIZED PATCHES/PLAQUES 95 – Discoid eczema1 • Individualised patches more pruritic than psoriasis • Lack silvery scale • Less vivid colour than psoriasis Discoid eczema Psoriasis LOCALISED PATCHES/PLAQUES 96 – Superficial basal cell carcinoma/Bowen’s disease1,2 • Asymmetrical lesions, either single or few in number • Perform biopsy if lesions resistant to topical psoriasis treatment, or to confirm diagnosis Bowen’s disease Psoriasis LOCALISED PATCHES/PLAQUES – Seborrhoeic dermatitis • Characterized by yellowish scaling and erythema1 – Localized to many of the same areas as psoriasis • Diffuse scaling differs from sharply defined psoriasis plaques2 • Affects furrows of face (facial psoriasis is generally restricted to hairline)1 Dermatitis Psoriasis 97 LOCALIZED PATCHES/PLAQUES 98 – Cutaneous T-cell lymphoma (mycosis fungoides) • Red, discoid lesions1 • Asymmetrical and less scaly than psoriasis1 • Lesions may present with fine atrophy and be resistant to antipsoriatic therapy2 • Biopsy to confirm diagnosis Mycosis fungoides Psoriasis 1. Fry L. An atlas of psoriasis. Spain: Taylor & Francis, 2004. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. GUTTATE PSORIASIS 99 – Pityriasis rosea1 • Difficult to distinguish from acute guttate psoriasis • Presents first as single large patch, progresses to a truncal rash of multiple red scaly plaques (‘Christmas tree’ distribution) • Resolves over 8–12 weeks < Psoriasis ^ Pityriasis rosea 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. GUTTATE PSORIASIS 100 – Secondary syphilis • Search for characteristic primary syphilitic lesion, lymphadenopathy, and lesions of face, palm and soles1 • Conduct serology and skin biopsies to confirm1,2 < Psoriasis ^ Secondary syphilis 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. FLEXURAL PSORIASIS 101 – Tinea cruris1 • Affects groin area • Characterized by central clearing with advancing edge • Non-silvery lesion with fine scale, particularly at periphery • Lesion frequently extends more on left side < Psoriasis ^ Tinea cruris 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. FLEXURAL PSORIASIS 102 – Atopic eczema1,2 • Often associated with asthma and hay fever • Lacks classic psoriatic nail involvement and sharply demarcated scaly plaques < Psoriasis 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. Fischer, G. How to treat: atopic dermatitis. Australian Doctor. 16 April 2010: 29–36. ^ Atopic eczema FLEXURAL PSORIASIS – Candidiasis1,2 • Characteristic peripheral pustules and scaling differ to psoriasis • Yeast cultures are diagnostic – Seborrhoeic dermatitis2 Flexural psoriasis 1. Van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 2. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 103 PALMOPLANTAR PSORIASIS 104 – Tinea manum1 • Ringworm of hands • Fine powdery scale, particularly involving palms and palmar creases • Usually asymmetrical Tinea corporis 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. Psoriasis PALMOPLANTAR PSORIASIS – Hand and foot eczema • Hyperkeratotic forms difficult to distinguish from psoriasis1,2 • Biopsies can assist diagnosis1 • Look for history of atopy, a lack of psoriasis elsewhere on body, and evidence of eczema elsewhere on skin1 Eczema Psoriasis 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 2. van de Kerkhof P, ed. Textbook of psoriasis. 2nd ed. Melbourne: Blackwell Publishing, 2003. 105 PALMOPLANTAR PSORIASIS – Pompholyx of palms and soles (dishydrotic eczema)1 • Presents as clear vesicles – contrast to white/yellow pustules in pustular psoriasis • Accompanied by intense pruritus Eczema Psoriasis 1. Menter A et al. Fast facts: psoriasis. 2nd ed. Oxford: Health Press, 2004. 106