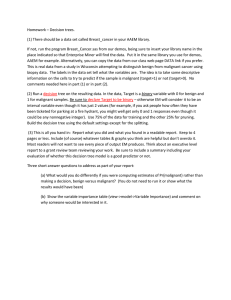
Benign tumors • Chondroma (gross + microscopic) • Osteochondroma(gross + microscopic) Malignant tumors • Osteosarcoma(gross + microscopic) Locally malignant tumors • Giant cell tumor (microscopic ) Chondroma of Hand Tumour mass with well formed capsule Left hand (Adult) Specimen: Comment : Cut surface : (mass) Sum: single Site: at region of metacarpal bones destroying and replacing them ??????????? Shape: oval- well circumscribed- encapsulated Size: 8x6 cm Cut surface: myxomatous degeneration (Honey comb appearance) Diagnosis : chondroma Chondroma Capsule Thin vascular fibrous tissue septa Lobules of mature cartilage Back to Slide Nature: BENIGN MESENCHYMAL TUMOR of cartilage Diseases of bone: Chondroma Mature bland chondrocyte Homogenous blue chondroid matrix Capsule Back to Slide Lacunae (appears as a clear space) Organ : Cartlagenous mass Diagnosis : Chondroma Nature of the lesion : Benign tumor—mesenchymal (cartilagenous ) Important patholgical findings : 1. encapsulated lesion 2. Lobules of mature cartilage 3. Thin vascular fibrous tissue septa Osteochondroma x-ray/ mushroom appearance Osteochondroma Piece of flat bone Cancellous bone Cartilaginous cap Calcification Cartilage exophytic oval bony swelling (mushroom appearance) Osteochondroma foci of calcifications A stalk & head of the tumour is formed of woven bone with a bone marrow cavity continuous with that of bone covered by a cartilagenous cap Specimen: Comment : Irregular bony tumor mass Cut surface : (mass – focal lesion) Sum: single Shape: mushrom shaped covered by cartilagenous cap Size: 5x4 cm Consistency: hard Diagnosis : Osteochondroma Cartilagenous exostosis Osteochondroma microscopic • Bone trabeculae covered by linear hyaline cartilage NEXT? Osteosarcoma x ray • Sun ray appearance: perpendical rays of sclerotic bone to bone cortex • Codmanns triangle: at the angle of elevated periosteum from bone cortex Osteosarcoma • Specimen: lower part of femur • An ill defined mass infiltrating medulla and bone cortex causing pathological fracture. Cut section shows Hemorrhage, necrosis, cystic degeneration Specimen: Comment : Lower part of femur Cut surface : focal lesion (mass) Sum: single Site: arising from the Metaphysis Shape: irregular infiltrating and destroying surrounding tissue, head,and bone marrow,…. Size:…..x……cm Colour: greyish white with areas of hemorrhage and necrosis Consistency: Fleshy Diagnosis : Osteosarcoma Intramedullary Production osteoid of Malignant osteoid Malignant osteobalasts Bone and soft tissue pathology.Andrew Horvai Mitotic activity Organ : Diagnosis : Bone mass Osteosarcoma Nature of the lesion : Metaphyseal malignant tumor (osteoid producing) Important patholgical findings : 1. Malignant osteoblasts. 2. Malignant osteoid. 3. Hemorrhage and necrosis. ” Giant Cell Tumor Clinical keynotes: •Usually young adults •Commonly epiphysis of lower end of femur and radius, upper end of tibia and humerus •The mass is Radiolucent mass in lower femur traversed by thin sclerotic lines giving soap bubble appearance. with thinned cortex Giant Cell Tumor Nature of this lesion: locally malignant bone tumor of unknown cell of origin Giant Cell Tumor Mononuclear stromal cells: - NEOPLASTIC -Plump, oval cells with scanty cytoplasm and large vesicular nuclei with prominent nucleoli Multinucleated large osteoclast-like giant cells: -DIAGNOSTIC -Evenly distributed -Numerous,contain up to 100 End of muscloskeletal Skin Benign Malignant • Squamous cell papilloma • Squamous cell carcinoma • Basal cell carcinoma • Malignant melanoma Squamous cell papilloma Squamous cell papilloma Identification: •Papillary surface with broad base or papillary structure •Stratified Squamous epithelium covering Squamous cell papilloma Hyperkeratosis Papillomatosis Acanthosis Squamous cell papilloma Hyperkeratosis Acanthosis acanthosis Squamous cell papilloma Papillomatosis Vascular onnective tissue core Acanthosis Hyperkeratosis Organ : Skin mass Diagnosis : Squamous cell papilloma Nature of the lesion : Benign tumor—surface epithelial Important patholgical findings : 1. Papillary growth 2. Stratified squamous epithelial lining showing: a) Hyperkeratosis (increased keratin) b) Acanthosis (increased prickle cell layer) c)Papillomatosis (elongated dermal papillae) 3. Branching fibrovascular connective tissue core Malignant Tumors Back to Slide Squamous cell carcinoma Ulcer on the face with raised everted edges, necrotic floor Back to Slide Nuclear ccc of malignancy 1. 2. 3. 4. 5. Large nuclei-increased N/C ratio Pleomorphism(different shapes) Hyperchromatism (dark)chromatin clumping Prominent nucleoli. Mitotic figures Back to Slide Squamous cell carcinoma Stratified Squamous epithelium Ulcer Hair follicle Sebaceous gland Groups of malignant squamous epithelial cells Epithelial Pearl (cell nest) Back to Slide Squamous cell carcinoma Stratified Squamous epithelium malignant squamous epithelial cells Well differentiated squamous cell carcinoma Back to Slide Cell nest Squamous cell carcinoma Stratified Squamous epithelium Cell nest Ulcer Well differentiated squamous cell carcinoma Back to Slide Squamous cell carcinoma Ulcer Epithelial pearl T Moderately differentiated squamous cell carcinoma Back to Slide Organ : Diagnosis : Skin mass Squamous cell carcinoma Nature of the lesion : MALIGNANT EPITHELIAL TUMOR (surface epithelial) Important patholgical findings : 1. Surface Ulcer and Infiltration of the wall by a malignant tumor 2. Tumor cells architecture: nests formed of malignant cells+ central keratin pearls (laminated eosinphillic)+ invade basement membrane to permeate underlying connective tissue 3. Tumor cells morphology: polygonal with eosinophillic cytoplasm and have hyperchromatic, irregular, pleomorphic, large nuclei with increased N/C ratio, prominent nucleoli & atypical mitosis Basal cell carcinoma Large rodent ulcer with a rolled , inverted beaded edge on the medial canthus and right side of the nose Ulcer at left side of nose Back to Slide Basal cell carcinoma Identification skin Ulcer Peripheral nuclear palisading masses of malignant basaloid epithelial cells Peripheral palisading Back to Slide Basal cell carcinoma T Back to Slide Basal cell carcinoma Skin Ulcer masses of malignant basaloid epithelial cells Back to Slide Basal cell carcinoma Nuclear palisading Masses of malignant basaloid cells Fibrous stroma with inflammatory cells Back to Slide Basal cell carcinoma Neoplastic masses with palisading Malignant basaloid epithelial cells (darkly stained) Back to Slide Basal cell carcinoma Inner polygonal cells Outer columnar cells arranged in a palisade manner Cells show scanty cytoplasm & large oval hyper chromatic nuclei Back to Slide Organ : Diagnosis : Skin mass Basal cell carcinoma Nature of the lesion : MALIGNANT EPITHELIAL TUMOR (surface epithelial) Important patholgical findings : 1. Surface Ulcer and Infiltration of the wall by a malignant tumor 2. Tumor cells architecture: The dermis is infiltrated by masses and nests of darkly stained blue malignant basaloid cells. • Tumor cells morphology: a. the outer layer of cells is formed of columnar cells arranged in a palisade manner. b. The inner cells are polygonal. c. The malignant cells have scanty cytoplasm and large oval hyperchromatic nuclei. 3. The masses are separated by fibrous stroma infiltrated by inflammatory cells . Malignant Melanoma Malignant Melanoma identification Malignant melanocytes N.E. Ulcer Anorectal junction Groups of Malignant melanocytes Infiltrating Single malignant melanocytes Malignant Melanoma T Malignant Melanoma T Malignant Melanoma Squamous epithelium T Malignant Melanoma T Malignant Melanoma Malignant cells with melanin pigment Organ : (Skin//Anorectal) mass Diagnosis : Malignant melanoma Nature of the lesion : MALIGNANT EPITHELIAL TUMOR (Melanocytes) Important patholgical findings : Subepithelial tissue is infiltrated by masses of malignant cells. 1. These cells are epithelioid or spindle in shape 2. The malignant cells have scanty cytoplasm and large oval hyperchromatic nuclei. 3. Brown melanin pigment is seen both in the cytoplasm of the malignant cells and also extracellular 4. Stroma is scanty with areas of hemorrhage and necrosis. THANK YOU