Final FRCA
300 SBAs
Final FRCA
300 SBAs
Kariem El-Boghdadly MBBS BSc (Hons) FRCA
Specialist Registrar in Anaesthesia,
South East School of Anaesthesia, London, UK
Imran Ahmad MBBS FRCA
Consultant Anaesthetist,
Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Honorary Senior Lecturer,
King’s College London, UK
Training Programme Director
Anaesthesia South London (ASL), London, UK
London • Philadelphia • Panama City • New Delhi
© 2015 JP Medical Ltd.
Published by JP Medical Ltd
83 Victoria Street, London, SW1H 0HW, UK
Tel: +44 (0)20 3170 8910
Fax: +44 (0)20 3008 6180
Email: info@jpmedpub.com
Web: www.jpmedpub.com
The rights of Kariem El-Boghdadly and Imran Ahmad to be identified as editors of this work have
been asserted by them in accordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any
form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as
permitted by the UK Copyright, Designs and Patents Act 1988, without the prior permission in
writing of the publishers. Permissions may be sought directly from JP Medical Ltd at the address
printed above.
All brand names and product names used in this book are trade names, service marks, trademarks
or registered trademarks of their respective owners. The publisher is not associated with any
product or vendor mentioned in this book.
Medical knowledge and practice change constantly. This book is designed to provide accurate,
authoritative information about the subject matter in question. However readers are advised
to check the most current information available on procedures included and check information
from the manufacturer of each product to be administered, to verify the recommended dose,
formula, method and duration of administration, adverse effects and contraindications. It is the
responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher
nor the editors assume any liability for any injury and/or damage to persons or property arising
from or related to use of material in this book.
This book is sold on the understanding that the publisher is not engaged in providing professional
medical services. If such advice or services are required, the services of a competent medical
professional should be sought.
Every effort has been made where necessary to contact holders of copyright to obtain permission
to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be
pleased to make the necessary arrangements at the first opportunity.
ISBN: 978-1-909836-18-1
British Library Cataloguing in Publication Data
A catalogue record for this book is available from the British Library
Library of Congress Cataloging in Publication Data
A catalog record for this book is available from the Library of Congress
Commissioning Editor:
Editorial Assistant:
Design:
Steffan Clements
Sophie Woolven
Designers Collective Ltd
Copy-edited, typeset, printed and bound in India.
Preface
Recent pass rates for the Final FRCA written examination have fallen by around 25%, a significant
drop that suggests candidates require more practice ahead of the exam. There are few single best
answer (SBA) revision books or past papers currently available for the Final FRCA. Recognising this
problem and following on from our experience of writing Primary FRCA: 450 MTFs and SBAs, we
decided to write this book of 300 practice SBAs.
The written element of the Final FRCA consists of a 3-hour short answer question (SAQ) section
of 12 compulsory questions and a multiple choice question (MCQ) section. This comprises 90
MCQs to be completed in 3 hours; 60 multiple-true-false (MTF) questions and 30 SBA questions
(the latter introduced in September 2010). The content of the exam is aligned to the intermediate
training CCT curriculum, with variable weighting applied to different aspects of the curriculum.
The 30 question SBA section generally includes 20 questions in clinical anaesthesia, 5 in intensive
care medicine and 5 in pain management. The SBAs are often seen as the most challenging
section of the MCQ paper, because they test the application of knowledge in the clinical setting, as
opposed to the MTFs which test factual recall.
Each SBA question consists of a clinical scenario (the ‘stem’), and a direct ‘lead-in’ question,
followed by five answer options. One of these is the ideal response, although all options are
possible solutions. Four marks are awarded for each correct answer and no marks are lost for an
incorrect answer, therefore a total of 120 marks is possible. Due to the heavy relative weighting of
the SBAs, they are an important aspect of the written examination, and it is crucial that candidates
practise as much possible in order to answer them correctly.
The 10 papers of 30 SBAs in this book cover every aspect of the Final FRCA syllabus. We have
included 20 clinical anaesthesia, 5 intensive care medicine and 5 pain management questions in
each paper to reflect the exam. Each question is up-to-date at the time of writing and reflects the
standard and type of question that candidates will encounter.
Failing to pass the Final FRCA is both expensive and upsetting, so it is prudent to be well
prepared. It requires candidates to have an in-depth knowledge spanning the syllabus, and to
have practised their examination technique. We believe this book provides candidates with both
the knowledge and the technique, and that it will help candidates succeed in the Final FRCA SBA
exam.
Kariem El-Boghdadly
Imran Ahmad
January 2015
v
Contents
Preface
Contributors
v
ix
Chapter 1 Mock Paper 1
Questions
Answers
1
1
12
Chapter 2 Mock Paper 2
Questions
Answers
41
41
51
Chapter 3 Mock Paper 3
Questions
Answers
81
81
92
Chapter 4 Mock Paper 4
Questions
Answers
121
121
131
Chapter 5 Mock Paper 5
Questions
Answers
159
159
170
Chapter 6 Mock Paper 6
Questions
Answers
203
203
214
Chapter 7 Mock Paper 7
Questions
Answers
247
247
258
Chapter 8 Mock Paper 8
Questions
Answers
287
287
297
vii
viii
Chapter 9 Mock Paper 9
Questions
Answers
327
327
337
Chapter 10 Mock Paper 10
Questions
Answers
365
365
375
Index
405
Contributors
Dr Jonathan Aron MBBS BSc MRCP FRCA, Specialist Registrar in Anaesthetics and Intensive Care
Medicine, South East School of Anaesthesia, London, UK
Dr Sheela Badiger MB/BChir MA FRCA, Specialist Registrar in Anaesthetics, South East School of
Anaesthesia, London, UK
Dr Jonathan Ball MRCP EDIC FCCP FFICM MSc MD, Consultant and Honorary Senior Lecturer in
General and Neuro Intensive Care, St George’s Hospital and Medical School, London, UK
Dr Toby Dixson BSc (Hons) AlBiol MBBS FRCA, Specialist Registrar in Anaesthetics and Intensive
Care Medicine, South East School of Anaesthesia, London, UK
Dr Dragos Dragnea MBBS FRCA, Specialist Registrar in Anaesthetics, South East School of Anaesthesia, London, UK
Dr Heng Gan MRCPCH FRCA, Specialist Registrar in Anaesthetics, South East School of Anaesthesia, London, UK
Dr Akhil Gupta MBBS BSc FRCA, Specialist Registrar in Anaesthetics, South East School of Anaesthesia, London, UK
Dr Martin John MBBS BSc(Hons) MRCP FRCA, Specialist Registrar in Anaesthetics, South East
School of Anaesthesia, London, UK
Dr Mubeen Khan MBBS DA FCPS DNB FRCA, Consultant Anaesthetist, King’s College Hospital NHS
Foundation Trust, London, UK
Dr Desire N Onwochei MBBS BSc (Hons) FRCA, Specialist Registrar in Anaesthetics, South East
School of Anaesthesia, London, UK
Dr David Pang MBChB FRCA FFPMRCA, Consultant in Pain Medicine, St Thomas’ Hospital NHS
Trust, London, UK
Dr Shital Patel MBBS BSc MRCP FRCA, Specialist Registrar in Anaesthetics, South East School of
Anaesthesia, London, UK
Dr Isabelle Reed MBChB FRCA, Specialist Registrar in Anaesthetics, South East School of Anaesthesia, London, UK
Dr Ramai Santhirapala MBBS BSc (Hons) FRCA FFICM, Specialist Registrar in Anaesthetics and
Intensive Care Medicine, South East School of Anaesthesia, London, UK
Dr Husham Al-shather MBChB ICO FRCA EDRA, Specialist Registrar in Anaesthetics, South East
School of Anaesthesia, London, UK
Dr Michael Shaw BSc (Hons) MBChB (Hons) FRCA, Specialist Registrar in Anaesthetics, South East
School of Anaesthesia, London, UK
Dr Philippa Webb MBBS MSc FRCA, Locum Consultant Neuroanaesthetist, St George’s Hospital,
London, UK
ix
Chapter 1
Mock Paper 1
Questions
1. You are called to anaesthetise a claustrophobic patient who requires an MRI scan.
The patient has a cervical fixation device in place to stabilise a recent C-spine
fracture, and the neurosurgeons have requested that it remains in situ until after
the scan results.
Which of the following factors would most likely mean that an MRI scan is
contraindicated?
A
B
C
D
E
The provision of a standard anaesthetic machine in the MRI suite
The patient having a permanent pacemaker (PPM) in situ
The patient recalling that he has a foreign body in his eye
The provision of standard infusion pumps in the MRI suite
A Halo device for cervical stabilisation
2. A 77-year-old man arrived in the intensive care unit 2 hours ago following coronary
artery bypass grafting (CABG). He has a background of interstitial lung disease
and hypertension. He is intubated, ventilated and sedated and on a noradrenaline
infusion at 0.05 μg/kg/min. Atrial pacing wires are in situ. You are called to see him
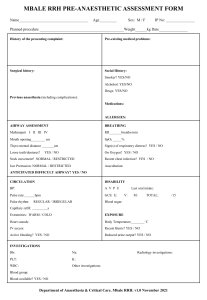
as the nurse looking after him thinks the ECG has changed. His blood pressure is
110/80 mmHg and the cardiac index reading on the PiCCO is 1.5 L/min/m2. The
readings an hour ago were 130/80 and 2.4 L/min/m2 respectively. His 12-lead ECG
is shown in Figure 1.1.
What is the most appropriate course of action?
A
B
C
D
E
1 mg intravenous metoprolol
300 mg amiodarone over 30 minutes
Synchronised DC cardioversion with 100J
Atrial pacing at 100 beats per minute
250 µg intravenous digoxin
2
Chapter 1
I
aVR
V1
V4
II
aVL
V2
V5
III
aVF
V3
V6
II
Figure 1.1: 12-lead ECG.
3. You are scheduled to anaesthetise an 80 kg man for aortic valve replacement. He is
73 years old and reports a rash upon administration of penicillin. His skin swab is
positive for methicillin-resistant Staphylococcus aureus (MRSA) colonisation.
Which of the following antibiotic regimens is most appropriate for the patient?
A
B
C
D
E
Flucloxacillin 2 g, gentamicin 120 mg
Vancomycin 1.5 g, gentamicin 400 mg
Cefuroxime 1.5g, metronidazole 750 mg
Co-amoxiclav 1.2 g, linezolid 600 mg
Clindamycin 900 mg, ciprofloxacin 400 mg
4. A 76 year old woman who is spontaneously breathing through a temporary double
lumen cuffed tracheostomy tube following a laryngectomy becomes acutely
breathless. Help is on its way but despite application of high-flow oxygen, her
oxygen saturations are 82% with a respiratory rate of 40 breaths per minute.
What is the most appropriate next step in her airway management?
A
B
C
D
E
Deflate the tracheostomy tube cuff
Remove the inner cannula
Hand ventilate through the tracheostomy tube
Position the patient upright
Remove the tracheostomy tube
5. A 28-year-old woman has an Achilles tendon repair under general anaesthesia as
a day case. She has a BMI of 32 kg/m2 and is taking the oral contraceptive pill. She
will need a below knee plaster cast for 6–8 weeks postoperatively.
Questions
What is the best form of venous thromboembolism prophylaxis for her?
A
B
Advice on mobilisation and fluid intake
Graduated compression stockings and pneumatic compression device on day
of surgery
C Graduated compression stockings post discharge for 7 days
D Single dose low molecular weight heparin on day of surgery
E Extended course of low molecular weight heparin post discharge
6. A 65-year-old woman is scheduled for an extended abdominal hysterectomy. She
is not on any anticoagulants but 2 years ago she developed a blood clot following
a total hip replacement. At that time her treatment injections caused a wound
haematoma, and she was put on a ‘blood thinning’ infusion for several days. At the
end of the treatment she remembers having investigations for low platelets in her
blood. These results are unavailable.
For immediate perioperative prophylaxis this time the best treatment would be:
A
B
C
D
E
A heparin infusion started 6 hours following surgery if bleeding is controlled
Treatment dose low-molecular-weight heparin (LMWH) injection once daily
Fondaparinux injection once daily
Low-dose aspirin orally throughout the perioperative period
A danaparoid infusion
7. A 21-year-old woman is undergoing a Le Fort I transverse osteotomy to correct
her maxillary retrusion. A nasal tube is used and anaesthesia is maintained by
propofol and remifentanil infusions. During the down-fracture, her pulse rate falls
to 29 bpm and her blood pressure reads 70/30 mmHg. Her oxygen saturation, end
tidal CO2 and airway pressures remain unchanged.
What is the most likely cause of her haemodynamic compromise?
A
B
C
D
E
Haemorrhage
Venous air embolus
Endotracheal tube damage
Trigeminocardiac reflex
Remifentanil
8. A 64-year-old man with no previous cardiac or respiratory morbidity is attending
for his second treatment of electroconvulsive therapy (ECT). After his previous
treatment, he had a supraventricular tachycardia with a peak blood pressure
of 198/105 mmHg, which resolved spontaneously within 5 minutes. For his
anaesthetic he had received propofol 90 mg and suxamethonium 40 mg.
What is the most appropriate course of action for this second treatment?
A
B
C
D
E
Perform procedure with defibrillation pads on his chest
Pre-medicate with oral atenolol
Use intravenous esmolol during procedure
Use remifentanil infusion during procedure
Use sublingual nifedipine during procedure
3
4
Chapter 1
9. You are called to see a 65-year-old patient in the surgical ward 3 days following an
elective abdominal aortic aneurysm repair. A thoracic epidural catheter is in situ.
He is febrile and complains of back pain and lower limb weakness.
What would be the most appropriate next step?
A
B
Stop the epidural infusion and contact the neurosurgeon
Stop the epidural infusion, do regular neurological observations and monitor
the epidural catheter site
C Arrange an urgent MRI scan and inform the neurosurgeon
D Stop the epidural infusion and start empirical antibiotics
E Remove the epidural catheter and do a full neurological examination
10. A 70 kg, 36-year-old man is scheduled for foot surgery under a regional anaesthetic
approach.
Which of the following needles would you use to perform a lateral popliteal nerve
block?
A
B
C
D
E
50 mm length, short bevel peripheral nerve block needle
50 mm length, long bevel peripheral nerve block needle
150 mm length, short bevel peripheral nerve block needle
100 mm length, short bevel peripheral nerve block needle
100 mm length, long bevel peripheral nerve block needle
11. A 28-year-old pedestrian struck by a bus presents to the emergency department.
In hospital, he has had a primary survey which reveals an obvious head injury; he
also appears to have a fracture to his right arm. His chest appears clear and a FAST
scan of the abdomen is negative. Because he had been confused, the emergency
medicine registrar has asked you to sedate him for a CT scan of his head. On
examination, he grimaces and groans to a deep painful stimulus, but does not
open his eyes. He flexes his left arm and leg.
The safest option for CT scan would be to:
A
Titrate small doses of propofol to effect with continuous monitoring including
waveform capnography
B Refuse to give sedative drugs on account of his depressed conscious state, but
accompany him to the scanner
C Perform a rapid sequence induction (RSI) with propofol and suxamethonium
1.5 mg/kg, and transfer with a propofol infusion
D Perform a modified RSI with 1.5 mg/kg suxamethonium, after 2 µg/kg fentanyl
and propofol and manual in-line stabilisation of the cervical spine
E Fit a Miami J collar and blocks and then perform a modified RSI with 1 mg/kg
rocuronium and 3 mg/kg ketamine.
12. A 19-year-old man presents to a district general hospital emergency department
8 hours after suffering a penetrating injury to his anterior chest. He has a Glasgow
Questions
coma scale (GCS) of 15, heart rate of 105 beats per minute, blood pressure of 95/50
(MAP 65) mmHg, saturations of 99% on oxygen and a haemoglobin of 105 g/L.
Transthoracic echocardiogram shows a haemopericardium for which he requires
transfer to a nearby cardiothoracic centre for exploration.
What pre-transfer intervention is most appropriate?
A
B
C
D
E
Needle pericardiocentesis
Intubation and ventilation
Insertion of a pulmonary artery catheter for cardiac output monitoring
Insertion of invasive arterial and central venous catheter
Transfusion of 2 units packed red cells
13. A 62-year-old man who sustained an isolated non-penetrating chest injury
resulting in lung contusions and rib fractures is on the intensive care unit
intubated and ventilated. He has deteriorated over the past 72 hours and now has
a Po2:Fio2 ratio (PFR) of 50 mmHg with a Fio2 of 1.0 and a positive end-expiratory
pressure (PEEP) of 5 cmH2O. The investigations suggest he has developed Acute
Respiratory Distress Syndrome (ARDS).
The most important first intervention is:
A
Furosemide bolus of 40 mg intravenously and commence an infusion aiming
for a negative fluid balance
B Administer a neuromuscular blocking agent
C Perform a recruitment manoeuvre and incrementally increase the PEEP to
above 14 cmH2O
D Adjust the ventilator settings to ensure tidal volumes of 6 mL/kg and a peak
pressure of less than 30 cmH2O
E Prone the patient
14. A 26-year-old woman with a past medical history of self-harm was found
unconscious at home with empty alcohol and amitriptyline bottles on the
floor. These had been ingested within half an hour. On arrival to the emergency
department her Glasgow coma scale (GCS) was 5 (E1, V1, M3). She was
intubated for airway protection. The patient subsequently developed a blood
pressure of 80/60 mmHg associated with a heart rate of 150 beats per min, a QRS
width of 100 msec and multiple ventricular ectopic beats.
The next most important intervention is:
A
B
Nasogastric tube insertion and administration of activated charcoal
Intravenous crystalloid bolus of 20 mL/kg followed by a noradrenaline infusion
to maintain blood pressure
C 500 ml intravenous sodium bicarbonate 1.26% for treatment of a broadened
QRS complex
D Lignocaine 2 mg/kg for the management of ventricular ectopic beats
E Lipid emulsion 20% 1.5 mL/kg for intravascular sequestration of tricyclic drug
5
6
Chapter 1
15. A 28-year-old woman presents with progressive and ascending motor weakness.
She reports a recent history of coryzal symptoms.
The following would be an early indicator of the requirement for intubation:
A
B
C
D
E
Respiratory rate > 35 breaths per minute
Pao2 < 8 kPa
Paco2 > 6.5 kPa
Vital capacity < 15 mL/kg
Absence of bulbar weakness
16. A 70 kg elderly man, awaiting an elective transurethral resection of prostate
(TURP), is admitted to the intensive care unit (ITU) with urosepsis. His average
urine output over 12 hours is 28 mL/hour.
His ITU admission and pre-admission clinic biochemistry profile are shown in
Table 1.1.
Table 1.1 Pre-admission and ITU admission biochemistry profile
Pre-admission clinic
Admission
Urea (mmol/L)
6.2
11.2
Creatinine (μmol/L)
83
132
Na+
131
129
4.5
5.1
(mmol/L)
K+ (mmol/L)
According to the RIFLE criteria, which stage of acute kidney injury does this man
fulfill?
A
B
C
D
E
Risk
Injury
Failure
Loss
End-stage renal disease
17. A 41-year-old man has been invasively mechanically ventilated for three days due
to pancreatitis. He develops pyrexia and increasing oxygen requirements. He is
noted to have new left lower zone infiltrates on chest X-ray.
Which of the following organisms is most likely to be the cause of his
deterioration?
A
B
C
D
E
Escherichia coli
Methicillin sensitive Staphylococcus aureus (MSSA)
Pseudomonas
Acinetobacter
Vancomycin resistant enterococci (VRE)
Questions
18. A 32-year-old primigravid patient with a body mass index (BMI) of 55 is on the
labour ward. It is 10 pm; she is currently 7 cm dilated and requesting an epidural.
The baby is in the occiput posterior (OP) position. You are unable to palpate her
spinous processes. On your third attempt, with difficulty, you perform a lumbar
epidural at L3/4 and accidentally cause a dural tap.
What is the best line of management in this situation?
A
B
C
Repeat your attempt at an adjacent lumbar level and use a smaller test dose
Request help from a colleague to attempt the epidural
Use the ultrasound to help locate the depth of the epidural space before reattempting
D Abandon your attempt and institute a remifentanil PCA
E Site a spinal catheter, inform midwife and perform subsequent top-ups
yourself
19. You are fast bleeped to the emergency department (ED) where a 22-year-old
woman who is 28/40 pregnant has presented with a history of seizures for the
past 45 minutes. A wedge has been placed under the right side of the patient
and large bore intravenous access has been secured. Her blood pressure is
180/110 mmHg, heart rate 154 beats per minute, respiratory rate 24 breaths per
minute and an arterial blood gas sample reveals a pH of 7.2 with an elevated
lactate. The obstetric registrar is present and suspects this is an eclamptic fit. 4 g
of intravenous magnesium sulphate (MgSO4) has been given over 5 minutes and
anti-hypertensive medication has been started. The patient is still fitting.
What should the next stages of management be?
A
Secure airway with endotracheal tube (ETT) and perform emergency
Caesarean section in the ED
B Commence MgSO4 infusion at 1 g/hour, secure airway with ETT and perform
emergency Caesarean in the ED
C Commence MgSO4 infusion at 1 g/hour, give a further 2 g MgSO4 bolus, secure
airway with ETT and continue supportive management
D Give a further 2 g MgSO4 bolus and if no response administer phenytoin 15 mg/
kg
E Commence MgSO4 infusion at 1 g/hour, give a further 2 g MgSO4 bolus, secure
airway with ETT and perform emergency Caesarean section in the ED
20. A 5-day-old boy presents to a local emergency department with a 2-day history
of increasing respiratory distress. He is lethargic with a heart rate of 184 beats
per minute, a respiratory rate of 68 breaths per minute, a blood pressure of
66/32 mmHg, capillary refill time of 6 seconds, Spo2 96% on air on the right hand,
but unrecordable from the other limbs. His axillary temperature is 36.1°C, but his
extremities are mottled and feel cool to touch. The chest sounds clear and the heart
sounds seem normal with weakly palpable femoral pulses. He was given a bolus
of 10 mL/kg of 0.9% saline and broad-spectrum intravenous antibiotics. A rapid
sequence induction was performed, and the patient intubated and ventilated.
7
8
Chapter 1
The most appropriate next step in his management is:
A
Start prostaglandin E2 intravenous infusion and refer to tertiary centre for
possible coarctation of the aorta
B Arrange for an urgent chest X-ray
C Insert a nasogastric tube to decompress the stomach to aid ventilation
D Perform arterial blood gas analysis
E Keep the infant warm with radiant heater
21. A 20 kg 5-year-old child was brought to the emergency department of a district
general hospital with 15% burns from scalding to neck, chest, abdomen and right
upper limb having already received 20 mL/kg (400 mL) Hartmann's and 20 µg/
kg intravenous (IV) morphine for analgesia. It is 4 hours since the time of injury.
On examination, the child appears comfortable, with a heart rate of 110 beats
per minute, blood pressure of 124/82 mmHg, a respiratory rate of 22 breaths per
minute and Spo2 of 99% on air.
The next most appropriate step in the management of this patient for the next 4
hours is:
A
B
IV Hartmann’s at 110 mL/hour. Refer to tertiary centre for further management
IV Hartmann’s at 110 mL/hour. Admit for further observation and
management
C IV Hartmann’s at 75 mL/hour. Refer to tertiary centre for further management
D Intubate and ventilate. IV Hartmann’s at 110 mL/hour. Refer to tertiary centre
for further management
E Give IV antibiotic prophylaxis. IV Hartmann’s at 110 mL/hour. Admit for
further observation and management
22. A 57-year-old woman presents with a history of severe facial pain that occurs in
sudden episodes of a few minutes and only affect her right cheek. It starts with a
sharp ’electric shock‘ which then becomes an ache before it abruptly disappears.
Treatment with carbamazepine was commenced at 100 mg b.d. this week, and this
has provided only modest relief.
The most appropriate next step in her treatment is:
A
B
C
D
E
Increase dose of carbamazepine
Microvascular decompression
Add amitriptyline
Add lamotrigine
Cognitive-behavioural therapy
23. You are presented with a 43-year-old woman who had a mastectomy 7 years ago,
followed by neoadjuvant radiothearpy and chemotherapy for left sided breast
cancer. She is currently taking hormonal therapy and has had pain over the left
chest wall for the past 2 years.
Questions
Which of the following is most correct regarding this patient’s chest wall pain?
A
B
C
D
E
Urgent referral for investigation of recurrence is needed
Phantom pain is rare in post-mastectomy patients
Long-term opioids should be commenced
Brachial plexus pathology is the likely cause
The pain will usually respond to anticonvulsants
24. A 46-year-old right-handed violinist presents with a 3-month history of
worsening severe pain in his right wrist, which commenced suddenly after a long
performance in a concert. He has noticed the painful wrist going pale and cold
at times, and swelling occasionally. Sometimes it sweats, and it has become stiff
and difficult to use. It appears smaller than his left hand, and the nails of his right
fingers have become brittle and discoloured. He admits to being very distressed
and anxious as he is no longer able to perform. Treatment with paracetamol and
amitriptyline has been commenced.
The most appropriate next step in his management is:
A
B
C
D
E
Pregabalin 75 mg b.d.
Acupuncture
Patient education and psychological support
Application of 5% lignocaine patches
Mirror therapy
25. A 30-year-old woman with chronic lower back pain is assessed in an outpatient
clinic. She tells you that her pain has improved with exercise and local heat
application, but when she thinks about the pain it seems to get worse.
Regarding this gate theory of pain, which of the following is most accurate?
A
B
It applies mostly to nociceptive pain
It is the basis of how transcutaneous electrical nerve stimulation (TENS)
machines work
C A supraspinal input is required
D Inhibition occurs via Aδ fibres
E This theory does not apply to children
26. A 73-year-old woman with metastatic breast cancer presents with a 4-month
history of severe pain in her back, upper arms and legs. She has been on increasing
doses of modified release oral morphine and paracetamol, and while this
combination provides her some relief, she is troubled by drowsiness, pruritus,
and constipation. At times she feels this is more distressing than her initial pain.
Additionally, she is on warfarin for atrial fibrillation.
The most appropriate next step in her management would be:
A
Add diclofenac
9
10
Chapter 1
B
C
D
E
Reduce the dose of morphine
Add naloxone
Opioid rotation
Prescribe a laxative
27. A 35-year-old man has been admitted to the intensive care unit with a 55% total
body surface area (BSA) burn. He is intubated and has been resuscitated as per the
Parkland formula.
Which of the following statements is correct?
A
Should temperature spike above 38°C, take blood cultures and start broad
spectrum antibiotics
B Enteral nutrition should be started as soon as possible
C Steroids are indicated as there is greater than 40% BSA burns
D Fluid resuscitation should be continued according to the Parkland formula
even if polyuria develops
E If fluid management is optimal generalised oedema is unlikely to develop
28. A hypertensive 68-year-old man on amlodipine is undergoing an elective
abdominal aortic aneurysm repair. At the end of the operation the surgeon is
prepared to release the infrarenal aortic cross-clamp.
Which of the following interventions would mitigate the ensuing hypotension?
A
Starting an infusion of noradrenaline at 0.5 µg/kg/min after cross-clamp
release
B Starting an infusion of dobutamine at 5 µg/kg/min after the cross-clamp
release
C Rapid infusion of 500 mL of colloid during cross-clamp release
D Tilting the table in reverse Trendelenburg position
E Optimising the intravascular volume during aortic cross-clamping
29. A 74-year-old man is brought to the emergency department with palpitations. He
has a heart rate of 156 beats per minute and atrial fibrillation on his ECG.
Which one of the following would not warrant immediate direct current
cardioversion?
A.
B.
C.
D.
E.
Blood pressure of 84/30 mmHg
GCS of 12/15
Bi-basal creptitations and tachypnea
Sweating with cold clammy hands
T wave inversion in lead aVR
30. A 3-year-old boy suffers from dry and scaly skin, oral thrush, dandruff and dry hair,
as well as poor vision in the dark. On examination he has xerosis and Bitot’s spots.
Questions
The most likely deficiency is:
A
B
C
D
E
Vitamin A
Vitamin D
Vitamin C
Vitamin B12
Vitamin K
11
Chapter 1
Answers
1.C The patient recalling that he has a foreign
body in his eye
Magnetic resonance imaging (MRI) scans are often utilised for investigating the
central nervous system as they provide images that show improved distinction
between tissue types compared with computed tomography (CT) scans.
MRI scanning takes advantage of the fact that atomic nuclei within tissues naturally
spin, generating their own small magnetic field. By applying a larger external field to
a tissue, these spinning nuclei align with the field which has been applied. A second
external field is then pulsed in a perpendicular fashion causing some nuclei to be
pulled to an angle. This incorporates nuclear energy absorption, and they begin to
wobble or precess – a term used to describe rotation around an axis different to that
of original spin. Precession results in tissues producing rotational magnetic fields,
the amplitude and specific frequency of which can be detected and used to form
an image. As the nuclei return to their previous positions between pulses, they emit
the energy they previously absorbed at the same frequency. The rate of their return
depends on the elemental content of the nucleus (e.g. hydrogen or phosphorous)
in addition to the molecule of which it is a part (e.g. water or fat). Different tissue
types therefore return at different rates. By using a combination of magnetic field
gradients and pulse configurations, detailed cross-sectional views can be obtained.
MRI scanners raise a number of safety concerns with regards to equipment. As the
magnetic field is constantly present, anything containing ferromagnetic material
will be attracted to it, turning them into projectiles. The field strength is measured
in Tesla (T) and Gauss (G). 1T=10,000G. MRI scanners for medical imaging are usually
1.5T but sometimes 3T. The strength declines with distance from the magnet and
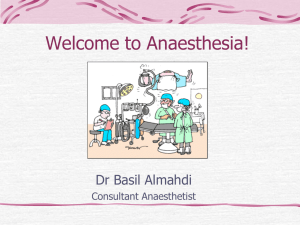
contours are marked in Gauss lines on the floor of the MRI suite (Figure 1.2).
Figure 1.2 Representation of
the 5 Gauss line around an MRI
scanner
Control
room
5 Gauss line
12
Magnet
Beyond the 5G line no ferromagnetic material should ever be taken. This includes
many items of equipment and implanted devices. Another concern with regards to
equipment is the effect of radiofrequency energy resonating with material causing
the dispersion of energy as heat. Patients can therefore suffer burns from any
conductive material with which they are in contact.
Answers
As a result of the above, all equipment is classified according to the hazard it
poses under certain conditions such as magnetic field strength or in view of
radiofrequency absorption. MR safe equipment can be used in all MR settings,
MR conditional in specified environments, and MR unsafe in none of the
aforementioned situations.
Monitoring in the MRI suite is essential and has evolved accordingly. MR compatible
monitoring is standard, with many units using telemetric equipment to avoid any
induced currents in long cables. MR compatible anaesthetic machines and infusion
pumps are available; however standard equipment can be used with extensions to
beyond the 5G line. The anaesthetic machine must be securely fixed to the wall and
the pumps attached to their extensions through a port into the control room.
Pacemakers and implanted cardiac defibrillators are at risk of malfunctioning or
displacing and so were, until recently, a strict contraindication to having an MRI.
Technology has, however, advanced and there are now some MR-compatible models.
There are also MR strategies and guidelines that have been described to limit risk in
the event that an MRI is absolutely necessary for a patient with a standard device.
Cervical fixators, such as the halo device, vary in their classification. Some are MR
safe and this, or the hazard of any other item, can be easily checked by referring to a
list on www.MRIsafety.com.
Foreign bodies in the eye have the potential to migrate and cause bleeding into the
vitreous, therefore contraindicating an MRI scan.
Reddy U, White MJ, Wilson SR. Anaesthesia for magnetic resonance imaging. Contin Educ Anaesth Crit
Care Pain 2012; 12(3):140–44.
Association of Anaesthetists of Great Britain and Ireland. Safety in magnetic resonance units: an update.
Anaesthesia 2010; 65:766–70.
2. C Synchronised DC cardioversion with 100J
The ECG shows atrial flutter. Up to 40% of coronary artery bypass grafting (CABG)
patients will develop postoperative atrial fibrillation or flutter. The majority of
these dysrhythmias occur within 48-hours and may be recurrent. Presence of atrial
fibrillation or flutter is associated with an increase in hospital mortality as well as
other complications including stroke.
Risk factors for the development of atrial fibrillation or flutter include:
•
•
•
•
•
Atrial injury during cannulation
Ischaemia
Prolonged cardiopulmonary bypass time
Use of post operative catecholamines
Hypokalaemia and hypomagnesaemia
Although accompanied with reasonable haemodynamics, there is a clear fall in
cardiac index (and hence output) as measured by the PiCCO. Atrial flutter may
change to atrial fibrillation and rate control is rarely an option. Restoration of
sinus rhythm should be the aim in this circumstance and this is best achieved with
synchronised DC cardioversion.
13
14
Chapter 1
Although amiodarone is frequently used for atrial flutter, data concerning its
use in this setting is surprisingly lacking. When using amiodarone, cardioversion
may take hours rather than minutes. Another reason to avoid amiodarone in this
circumstance would be the history of interstitial lung disease, which is a risk factor
for exacerbation of any lung fibrosis that may be caused by amiodarone.
Rate controlling agents such as metoprolol and digoxin would not be optimal
treatment here.
Atrial pacing is a viable option but would usually be performed at a rate 10–15 bpm
higher than the atrial flutter rate. If the ventricular rate rises to match the atrial rate,
the pacemaker frequency can then be reduced (i.e. the rhythm is entrained) to an
acceptable rate. This may lead to conversion to sinus rhythm (or atrial fibrillation!).
Given this patient is already sedated and ventilated, it is quicker and more effective
to perform DC cardioversion.
As well as addressing strategies for cardioversion, it is also imperative that other
contributing factors for the development of any dysrhythmias are addressed:
•
•
•
•
Hypoxaemia
Hypercarbia
Electrolyte disturbances
Other causes of myocardial ischaemia e.g. graft failure
European Society of Cardiology. Guidelines for the management of atrial fibrillation. Eur Heart J 2010;
31:2369–429.
3. B Vancomycin 1.5 g, gentamicin 400 mg
Common pathogens in cardiac surgery are Staphylococcus aureus and
Staphylococcus epidermidis. In addition, this man has evidence of methicillin-resistant
staphylococcus aureus (MRSA) colonisation, so any prophylactic antibiotics must
cover this organism (vancomycin or linezolid). Most centres also administer some
gram negative cover such as an aminoglycoside (gentamicin at 5 mg/kg) or a
fluoroquinolone (ciprofloxacin).
Although the skin reaction reported after penicillin may not be significant, it is
prudent to avoid penicillins thus flucloxacillin and co-amoxiclav should be avoided.
Vancomycin 1.5 g with gentamicin 400 mg provides gram-positive (including MRSA)
and gram-negative cover and is the correct regimen for this patient. The dose of
vancomycin is 15 mg/kg and should be given as an infusion. The combination of
cefuroxime and metronidazole does not have MRSA cover and although clindamycin
with ciprofloxacin gives good gram positive, gram negative and MRSA cover, the use
of untargeted ciprofloxacin is often discouraged due to the speed by which plasmid
mediated resistance can occur.
Other elements of perioperative care that may reduce the incidence of surgical site
infection include patient warming, tight glycaemic control, hair removal and the
sterility of instruments and the surgical field.
Bratzler DW, Dellinger EP, Olsen KM, et al. 2013 Clinical practice guidelines for antimicrobial prophylaxis in
surgery. Surg Infect 2013; 14(1):73.
Answers
4. B Remove the inner cannula
Tracheostomy airway emergencies can lead to significant morbidity and mortality
if not managed correctly. Laryngectomy patients do not have an upper airway so
crucially cannot be intubated or oxygenated orally. They are unlikely to obstruct
when lying flat so sitting them more upright is not the immediate airway priority. In
this scenario following a call for help and application of oxygen, the tracheostomy
tube patency needs to be assessed as a priority.
With double lumen tracheostomy tubes, the initial step is to remove the inner
tube which will clear any secretions if these are causing a blockage. Following
inner tube removal, passage of a suction catheter should be attempted to confirm
airway patency and also help clear any further secretions within the tracheostomy
tube. If the suction catheter fails to pass, deflation of the tracheostomy tube cuff
may improve airflow if the tracheostomy tube is partially displaced. If the clinical
condition fails to improve following cuff deflation, the tracheostomy tube may be
completely blocked or displaced, preventing the patient to breathe around the tube
adequately and should therefore be removed. Attempting hand ventilation through
a tracheostomy tube to confirm airway patency is hazardous, since significant
surgical emphysema can ensue in the presence of tube displacement making
subsequent airway management more difficult. Figure 1.3 provides a graphical
suggestion for the steps to be taken in the assessment of tracheostomy tube
patency in post-laryngectomy patients.
Figure 1.3 Suggested steps in
assessing tracheostomy tube
patency in post-laryngectomy
patients
Patient does not have an upper airway in
continuity with the lungs.
Remove inner tube (if present)
Attempt passing a suction catheter
If unsuccessful
Deflate the cuff
Look, listen, feel at the tube
If patient
deteriorates
Remove tube
15
16
Chapter 1
Therefore, this patient requires removal of the inner cannula for further assessment
and management of the cause of her respiratory distress.
McGrath BA, Bates L, Atkinson D, Moore JA. Multidisciplinary guidelines for the management of
tracheostomy and laryngectomy airway emergencies. Anaesthesia 2012; 67(9):1025–41.
Regan K, Hunt K. Tracheostomy management. Contin Educ Anaesth Crit Care Pain 2008; 8(1):31–35.
5.E Extended course of low molecular weight
heparin post discharge
The risk of venous thromboembolic disease (VTE) after a day surgery procedure
is lower than after in-patient procedures as surgery is generally less invasive and
mobilisation is earlier. However, more complex and longer procedures in higher risk
patients are increasingly being performed in this setting. The 2010 National Institute
for Health and Care Excellence (NICE) guidelines for the prevention of VTE includes
day surgery as a specific cohort of patients and recommends that mechanical
prophylaxis should be used if one or more risk factors are present. Pharmacological
prophylaxis should be added depending on ‘patient factors and clinical judgement’.
• Surgical procedure with a total anaesthetic and surgical time of more than 90
minutes, or 60 minutes if the surgery involves the pelvis or lower limb
• Acute surgical admission with inflammatory or intra-abdominal condition
• Expected significant reduction in mobility
• One or more of the risk factors below:
–– Active cancer or cancer treatment
–– Age over 60 years
–– Critical care admission
–– Dehydration
–– Known thrombophilia
–– Obesity (body mass index [BMI] over 30 kg/m2)
–– One or more significant medical comorbidities (for example: heart disease,
metabolic, endocrine or respiratory pathologies, acute infectious diseases,
inflammatory conditions)
–– Personal history or first-degree relative with a history of VTE
–– Use of hormone replacement therapy
–– Use of oestrogen-containing contraceptive therapy
–– Varicose veins with phlebitis
Pharmacological prophylaxis should be continued for 5–7 days if significantly
reduced mobility is expected. This patient has three risk factors and extended
pharmacological prophylaxis is indicated. In addition she will have a lower limb
plaster cast, where NICE recommends that prophylaxis should be continued until the
cast is removed after discussion with the patient and evaluation of risks and benefits.
The exact duration will vary between centres.
National Institute for Health and Care Excellence (NICE). Venous thromboembolism – reducing the risk. CG
no 92. London: NICE, 2010.
British Association of Day Surgery (BADS). Organisational issues in pre operative assessment for day
surgery. London: BADS, 2010.
Answers
6. E A danaparoid infusion
Venous thromboembolism (VTE), is of major clinical significance given that up
to a quarter of inpatients with risk factors may be affected, albeit subclinically.
Candidates will be familiar with the risk factors for VTE (see above) but also should
be comfortable with the drug treatment strategies available and their complications.
Mechanical methods
Anti-embolism stockings or thromboembolic deterrent stockings (TEDS), are
graded to provide increased compression from distal to proximal. They are effective
at promoting venous return and increasing the speed of blood flow, but not
suitable for all patients, such as those with arteriopathy. Intermittent calf and thigh
compression devices produce pressures of approximately 40 mmHg 10 times per
minute to emulate the limb muscle pump.
Heparins
Unfractionated heparin is a naturally occurring antithrombin binder. This inhibits
factor Xa and thrombin and in higher doses also has an antiplatelet function.
Low-molecular-weight heparin (LMWH) is more effective than subcutaneous
heparin, has a lower risk of bleeding, and less anti-platelet effects. It is more
convenient with once daily administration, but is less controllable than a heparin
infusion, and accumulates in renal failure. It will not usually affect the activated
partial thromboplastin time (aPTT), which is a useful monitor of unfractionated
heparinisation.
Warfarin
Warfarin has the advantage of being given orally, and has similar risks of bleeding as
LMWH. It can be monitored using the international normalised ratio (INR).
Fondaparinux
Fondaparinux is a synthetic saccharide which emulates the structure of the
heparin anti-thrombin binding site. It indirectly inhibits factor Xa, and is given by
subcutaneous daily injection. It is more effective at preventing VTE than LMWH,
but also at producing bleeding. The half-life is long, and the drug-free time before
neuraxial block is thus 36 hours. It has a lower incidence of HIT, and has been used as
a LMWH substitute in this condition.
Others
Lepirudin is a hirudin derivative made as a recombinant protein in yeast, whose main
use is in heparin-induced thrombocytopenia (HIT). It directly inhibits thrombin and due
to its short half-life is administered by a continuous infusion and is monitored with the
aPTT. Due to manufacturer cessation of production in April 2012, lepirudin is no longer
available in the UK. Notably, this withdrawal was not due to any safety concerns.
Danaparoid is a heparinoid that inhibits factor Xa, and can be used in patients with
HIT. There is a need for close monitoring as some HIT cross reactivity does occur. It
has now replaced the use of lepirudin in the management of HIT in the UK due to
the aforementioned withdrawal.
17
18
Chapter 1
Dabigatran is an orally administered direct thrombin inhibitor licensed for VTE
prophylaxis after surgery. It does not require monitoring but also lacks any method
to reverse the anticoagulant effect.
Rivaroxaban is a direct oral inhibitor of factor Xa that is becoming more common.
Previously only for postoperative VTE prophylaxis, it is now being used in atrial
fibrillation and in Europe as an adjunct to aspirin and clopidogrel in acute coronary
syndromes.
The likely diagnosis in the above patient is an episode of heparin-induced
thrombocytopenia (HIT). HIT is an immune-mediated IgG response to an
immunogenic component of heparin, leading to thrombocytopenia. This occurs in
around 3% of patients as a consequence of treatment with unfractionated heparin,
and less-so at a rate of 0.1–1% with LMWH preparations. Paradoxically, the risk of
thrombosis is increased to 50% at this time, so alternate forms of anticoagulation
are needed. Platelet counts should be monitored from day 4 – 14, which is the risk
period for antibody formation.
Although the diagnosis is not absolutely confirmed, the question forces you to
respond and treat in the safest way possible. If HIT is a possibility then a heparin
infusion should be avoided, as should LMWH, as this can also precipitate the
condition. In addition, the dose of LMWH is probably too high, given that she is no
longer on anticoagulant treatment. Aspirin may or may not be indicated for this
patient in terms of primary cardiovascular prophylaxis, but does not have any role
in thromboprophylaxis. Of the two HIT-safe options, fondaparinux and danaparoid,
only danaparoid has no association with HIT. Fondaparinux has a very low rate of
giving rise to HIT and is sometimes used off-license as a treatment. However, in
this scenario the long half-life makes fondaparinux irreversible and uncontrollable
in the immediate postoperative phase. From day 2 onwards, without bleeding,
fondaparinux would represent a good choice for prophylaxis with adequate
monitoring of platelets.
Barker RC, Marval P. Venous thromboembolism: risks and prevention. Contin Educ Anaesth Crit Care Pain
2011; 11(1):18–23.
7. D Trigeminocardiac reflex
The horizontal Le Fort I osteotomy is a common procedure used to correct maxillary
deformities and knowledge of the surgical technique and relevant anatomy is
useful in recognising and treating complications. Surgery involves an intraoral
incision and the formation of a transverse maxillary osteotomy that extends to the
pterygomaxillary junction. The maxilla is then separated from the upper face along
this osteotomy plane by a down-fracture and fully mobilised to aid surgery.
Bleeding is a recognised complication during the down-fracture since the bony midface receives a rich blood supply and is in close proximity to an extensive venous
plexus. The blood vessels most likely to be injured during the down-fracture are the
pterygoid vessels, palatine and alveolar arteries, or on rare occasions the internal
carotid. In order to visualise the source of bleeding and achieve haemostasis,
completion of the down-fracture is often required. It is unusual for an acute
haemorrhage to present with a severe bradycardia as described in the above case.
Answers
Venous air emboli can occur during any head and neck surgery where open veins
are exposed to the atmosphere. However, end-tidal carbon dioxide levels would
be expected to fall as a result of an increase in physiological dead space and
intrapulmonary shunting which is not observed in the above case.
A nasal endotracheal tube is usually the airway of choice when correcting for
maxillary retrusion, since the jaw is frequently closed and wired to ensure normal
alignment of the upper and lower teeth. During the osteotomy and down fracture,
the nasal tube may be damaged resulting in impaired gas exchange and secondary
haemodynamic compromise. In such a situation, the airway (which is now likely to
be difficult) needs to be re-established. This scenario is unlikely in the above case
since the oxygen saturations, end tidal carbon dioxide levels and airway pressures
remain unchanged.
The Le Fort I osteotomy can also cause nerve damage and pressure effects to cranial
nerves II-VII due to their proximity to the surgical field. A recognised complication of
the maxillary down-fracture in particular is the generation of the trigeminocardiac
reflex. This reflex occurs as a result of pressure on the cranial nerve V (trigeminal
nerve) initiating a vagal reflex causing a severe bradycardia which may even
progress to asystole. Cessation of the down-fracture and return of the jaw to its
original position can increase the heart rate, as can administration of anticholinergic
drugs. The isolated bradycardia and hypotension in relation to the down-fracture in
the above scenario makes this reflex the most likely cause.
Remifentanil use in maxillofacial surgery is increasing in popularity due to its
favourable pharmacokinetic profile and its useful contribution to deliberate
hypotension. Severe bradycardia and hypotension are recognised complications of
remifentanil use, however the temporal relationship between the down-fracture and
the bradycardia in the above case make the trigeminal reflex more likely.
Beck J, Johnston K. Anaesthesia for cosmetic and functional maxillofacial surgery. Contin Educ Anaesth
Crit Care Pain 2013 doi:10.1093/bjaceaccp/mkt027.
Miloro M, Kolokythas A. Management of complications in oral and maxillofacial surgery. 1st Ed. New
York:John Wiley & Sons Inc, 2012.
8. C Use intravenous esmolol during procedure
During electroconvulsive therapy (ECT) an electrical current is applied to the brain
via transcutaneous electrodes to induce a generalised therapeutic seizure lasting
between 10–120 seconds. There is a biphasic physiological response. The seizure
causes an immediate direct stimulation of the vagal parasympathetic outflow, which
can lead to transient bradycardia and hypotension, and rarely asystole.
Premedication with an anticholinergic agent is often used to attenuate this effect.
This is followed by a more prominent catecholamine mediated sympathetic
response, which peaks 3–5 minutes after therapy, causing a tachycardia, and
hypertension and may give rise to tachyarrhythmias.
This sympathetic response can be attenuated using a variety of agents. Beta blockers
have been shown to be the most effective in controlling both heart rate and mean
arterial pressure. Due to the risk of initial bradycardia short acting agents such as
19
20
Chapter 1
esmolol or labetalol given just prior or during the procedure may avoid accentuating
the parasympathetic response compared to longer acting agents. Esmolol is
preferred as it reduces the peak systolic blood pressure more than labetalol while
labetalol may be associated with a shorter seizure duration.
Calcium channel blockers can also be effective to control arterial pressures but reflex
tachycardia may occur with nifedipine. Remifentanil has been shown to reduce
both the heart rate and blood pressure and does not have an effect on seizure
duration, though use of an infusion may not be available or suitable for these short
procedures.
Uppal V, Dourish J, Macfarlane A. Anaesthesia for electroconvulsive therapy. Contin Educ Anaesth Crit Care
Pain 2010; 10(6):192–197.
9.C Arrange an urgent MRI scan and inform the
neurosurgeon
There are many benefits for neuroaxial drug delivery. However, we need to balance
the advantages against the risk of complications such as infection, nerve damage
and haematoma.
In the third National Audit Project (NAP 3) report, the incidence of epidural abscess
after central neuraxial block (CNB) was quoted as 2.1 in 100,000. Although this is
considerably lower than previous studies, epidural abscess is still a very serious
complication of CNB and can lead to permanent neurological damage. In the above
scenario, the patient has signs and symptoms of an established epidural abscess that
needs decompression immediately.
We should recognise patients at increase risk of spinal infection before commencing
the CNB, with risk factors including:
•
•
•
•
•
•
•
Immune compromised patients
Patient with local or systemic infection
Long-term vascular access
Long duration of epidural catheterisation
Difficult CNB or a bloody tap after epidural
Prolonged hospital stay
Disruption of the spinal column, e.g. surgery or trauma
Following epidural catheter insertion, catheter site checks and regular temperature
monitoring are very important to recognise epidural abscess.
The classical presentation of epidural abscess is of pyrexia, back pain and progressive
abnormal neurology of the lower half of the body. However, 1 in 4 patients have
no back pain. Therefore, a high index of suspicion is required to diagnose epidural
abscess.
Advice from neurosurgeons, neurologists, radiologists and microbiologists are
needed early in established epidural abscess.
The most important action when we suspect epidural abscess is to organise MRI
with gadolinium. This will help to decide whether open or percutaneous drainage
should be used.
Answers
In this example, arranging an MRI scan and informing the neurosurgeons are the
first and most important steps to perform because early diagnosis and surgical
decompression is needed. Although option E is correct, it is time consuming and
delays the diagnosis. Once muscle weakness is present, only 20% patients regain full
function, even after surgery.
A full infection screen including blood cultures is mandatory if an epidural abscess
is suspected. At the same time, it is essential to remove the epidural catheter, as well
as stop the epidural infusion, and send the catheter tip for culture and sensitivity.
As solely stopping the infusion is inadequate, options A, B and D are insufficient
management options.
The most common microorganism found in spinal infection is Staphylococcus. Initial
antibiotic therapy should be empirical and then modified depending on the culture
and sensitivity results, while treatment must be guided by microbiological input.
Intravenous antibiotics are required initially for 2–4 weeks, followed by a prolonged
course of oral antibiotics. Regularly checking of inflammatory markers, back pain
and neurology should be used to monitor the response to antibiotics.
Royal College of Anaesthetists. Major complications of central neuraxial blocks in the United Kingdom:
the 3rd National Audit Project (NAP3) of the Royal College of Anaesthetists, 2009. Br J Anaesth 2009;
102(2):179–90.
Simpson KH, Al-Makadma YS. Epidural drug delivery and spinal Infection. Contin Educ Anaesth Crit Care
Pain 2007; 7(4):112–15.
Gosavi C, Bland D, Poddar R, Horst C. Epidural abscess complicating insertion of epidural catheters. Br J
Anaesth 2004; 92:294–95.
10. D 100 mm length, short bevel peripheral nerve block
needle
When performing nerve blocks, the length of the block needle is an essential
consideration. Longer needles might have potential tissue damage if advanced
further than needed, while the shorter needle may not be long enough to reach the
nerve.
The ideal needle length for peripheral nerve blocks is:
• 25 mm – Interscalene
• 50 mm – Cervical plexus, supraclavicular, axillary, femoral and popliteal ('posterior
approach')
• 100 mm – Infraclavicular, paravertebral, lumbar plexus, sciatic (‘posterior
approach’) and popliteal (‘lateral approach’)
• 150 mm – Sciatic (‘anterior approach’)
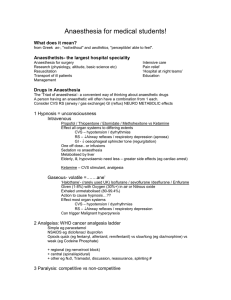
There are two types of nerve block needles: cutting tip needle and pencil point tip
needle (see Figure 1.4).
Cutting tip needles might be long bevel (15°) or short bevel (30–45°). Long bevel
needles are more likely to cause nerve damage by causing sharp nerve penetration.
Although the nerve damage caused by a short bevel needle is less frequent, the
damage will be more severe.
21
22
Chapter 1
Figure 1.4 Different needle
tips. (a) Cutting tip, short bevel
needle. (b) Cutting tip, long
bevel needle. (c) Pencil point
needle.
a
b
c
Pencil point needles are believed to penetrate tissue rather than cut through it, thus
providing an improved feel of anatomical layers through which they pass. It is not
clear whether a pencil point needle or a short bevel needle is safer to use.
The most frequently used needle in the current practice is the short bevel one. It
offers more resistance as it passes through the tissue planes, provides better tactile
feedback than long bevel needles and is less likely to cause nerve damage. Thus in
this clinical scenario, the most appropriate needle for a lateral approach popliteal
nerve block is a 100 mm, short bevel needle.
Jeng CL, Torrillo TM, Rosenblatt MA. Complications of peripheral nerve block. Br J Anaesth 2010; 105(suppl
1):i97–i107.
Hadzic A. Textbook in Regional Anaesthesia and Acute Pain Management. 1st ed. Columbus, OH: McGrawHill Medical, 2006.
11 D Perform a modified RSI with 1.5 mg/kg
suxamethonium, after 2 µg/kg fentanyl and propofol and
manual in-line stabilisation of the cervical spine
This question relates to the management of the patient with traumatic brain
injury (TBI). TBI is a major cause of morbidity and mortality in young patients, with
over 10% of injuries falling in the moderate to severe category. The principles of
management are those relevant to all neurosurgical emergencies and neurotrauma
patients.
Initial assessment and resuscitation
Should be along the familiar treatment algorithm of ABCDE, but with treatment and
stabilisation of each problem simultaneously as the assessment continues.
Answers
Haemodynamics
Even one episode of hypotension has been shown to double mortality. The aim is to
maintain cerebral perfusion pressure (CPP), in the face of raised intracranial pressure
(ICP) as CPP = MAP – ICP. International targets differ slightly, but a widespread MAP
target is 90 mmHg. Fluid resuscitation to normovalaemia would be the logical first
step, with vasopressors following if required. Crystalloid is best, with some evidence
of harm with albumin colloid. Hypotonic dextrose solutions must be avoided (unless
hypoglycaemic), as they contribute to tissue oedema.
Airway/ventilation
Intubation is indicated for a deterioration in Glasgow coma scale (GCS), or a GCS
of < 8, or if there is a failure of the patient's protective reflexes. Any disturbance
in oxygenation or ventilation leading to hypoxia or hypercapnia is likewise a
mandatory indication as hypoxic episodes are shown to worsen prognosis.
Hypercapnia will increase cerebral blood flow (CBF) and thus ICP, so must be
controlled; similarly a patient hyperventilating to hypocapnia must move to
controlled ventilation as they will compromise their cerebral perfusion. Other
indications include those that may compromise the airway if not dealt with, such as
bilateral mandibular fractures, oral bleeding, or seizures. Targets again differ, but a
Pao2 of > 10 kPa and a Paco2 in the normal range of 4.5–5 kPa are assumed to be safe.
Managing ICP
Outside of a neurosurgical centre, intracranial hypertension is either a presumptive
diagnosis, or made when so severe as to bring about herniation and associated
pupillary unresponsiveness. Where facilities exist for monitoring, the level at which
treatment should begin, is > 20–25 mmHg.
Hyperosomolar fluids such as mannitol and 3% saline draw fluid from the
intracellular space back into the interstitium and vasculature. Fewer complications
are seen with hypertonic saline and doses depend on the concentrations available,
but 3 ml/kg of 3% or 2 mL/kg of 5% are reasonable, titrated to a serum sodium of
< 155 mmol/L.
Hyperventilation has been shown to compromise cerebral perfusion, and is thus
reserved for severe cases resistant to other treatments. A temporary course of
hyperventilation titrated to a Paco2 of 4–4.5 kPa may be used.
Hypothermia reduces ICP and cerebral metabolic rate of oxygen (CMRO2), and is
used in neurosurgical centres for this reason. The target temperature, and duration
to achieve benefit are not known, as no benefit has yet been reliably shown. Most
would ensure mild hypothermia (35°C), and ensure prevention of fevers, which are
known to be harmful.
Adequate sedation (reducing CMRO2) and muscle relaxation preventing coughing
and associated rises in ICP is essential. This is extrapolated using barbiturates for
burst suppression in some cases of raised ICP, but is associated with significant
hypotension.
In the above patient, the GCS is E1 V2 M3 = 6/15, and, in the context of a head
injury this represents an indication for intubation. The patient meets the criteria for
23
24
Chapter 1
immediate CT scanning, and the need for imaging in this patient also mandates
securing of the airway prior to the scan.
This is a dangerous mechanism of injury, and the C-spine is compromised until
proven otherwise. Therefore C-spine control is needed for intubation and scanning.
Clearing this clinically is no longer possible due to the conscious level. Even if the
GCS were 15, with a distracting fractured arm, one cannot clear the neck confidently
without imaging.
The final discriminator here is choice of drugs used. The priority is rapid control of
the airway with muscle relaxation, whilst preventing either hypertension, (and raised
CBF and therefore increased ICP), or hypotension (with a fall in cerebral perfusion
pressure). Most would achieve the former by adjunctive use of an opioid, and the
latter with cautious use of induction agent. Ketamine has recently been shown to
have no effect on increasing ICP, contrary to traditional teaching, but the dosing
of 3 mg/kg is high, and a dosing of 1.5–2 mg/kg is likely sufficient. Similarly, for
muscle relaxation, classical teaching has urged against suxamethonium because of a
transient rise in ICP. However, the rise is small and for the most part offset by the fall
in perfusion pressure caused by co-administration of induction agents. Therefore the
most appropriate course of action in this patient would be to perform an RSI with
fentanyl, suxamethonium and propofol and manual in-line cervical stabilisation.
Dinsmore J. Traumatic brain injury: an evidence based review of management. Contin Educ Anaesth Crit
Care Pain 2013; 13(6):189–95.
12. D Insertion of invasive arterial and central venous
catheter
This patient requires transfer for specialist surgical services. Although not in extremis
his condition may become compromised during transfer and adequate resuscitation
and pre-transfer planning are essential.
Motion artefact may make non-invasive blood pressure (NIBP) readings unreliable
and continuous invasive arterial blood pressure (ABP) monitoring in these situations
is more appropriate. Central venous catheters provide a reliable form of intravenous
access and allows for the use of inotropic or vasopressor support should the need
arise during transfer.
The use of a pulmonary artery catheter and cardiac output measurements by
thermodilution is not practical during transfer and will not contribute to this
patient’s management.
Intubation and ventilation monitored with continuous capnography should occur
pre-transfer in patients in whom the airway or ventilation may be compromised,
neither of which are a concern in this case. Pericardial clots may prevent adequate
pericardial drainage and blood may further accumulate. Pericardiocentesis in a noncardiac centre without immediate surgical support should be carefully considered,
and may unnecessarily delay transfer. It is indicated in patients with significant
haemodynamic compromise, although a haemodynamically unstable patient with a
penetrating chest wound likely warrant a thoracotomy. Aggressive fluid resuscitation
in patients with penetrating injuries should be cautious and goals should be to
Answers
maintain an adequate filling pressure, heart rate and contractility. Blood should
be cross-matched and available to administer in the ambulance if required, and
tranexamic acid would be an appropriate adjunct in this circumstance.
Association of Anaesthetists of Great Britain and Ireland. Interhospital transfer. AAGBI Safety Guideline.
London: AAGBI, 2009.
Intensive Care Society (ICS). Guidelines for the transport of the critically ill adult. London: ICS, 2002.
13. C Perform a recruitment manoeuvre and incrementally
increase the PEEP to above 14 cmH2O
Acute respiratory distress syndrome (ARDS) was first described in 1967 by
Ashbaugh et al to describe tachypnoea, pulmonary infiltrates, decreased pulmonary
compliance, atelectatic lungs with alveolar oedema and hyaline membranes on
pathological examination.
The first formalised diagnostic criteria were created by the American-European
Consensus Conference (AECC) in 1994 and have since evolved. This included:
•
•
•
•
An acute clinical course
Bilateral infiltrates on the chest radiograph
No atrial enlargement or left ventricular failure
A severity classification dependent on the Pao2/Fio2 ratio (PFR)
–– ARDS was classified as a PFR < 200 mmHg
–– Acute lung injury (ALI) was classified as a PFR of > 200 < 300 mmHg
In 2012 the Berlin definition by the AECC superseded the original classification:
Respiratory failure now needs to occur within a week of a known initiating process.
Heart failure no longer needs to be excluded but must not fully explain the patients
respiratory failure. Acute lung injury no longer exists, and grades of severity of ARDS
has replaced the older classification (Table 1.2). The new definition offers better
predictive information for duration of treatment and the mortality.
This patient has severe ARDS as defined by his PFR and is at risk of dying from
hypoxia. There is an escalation protocol on how to manage such a patient, starting
with simple manoeuvres and ending with desperate measures:
1. Recruitment manoeuvres to improve oxygenation. There are several methods,
which are detailed by Lapinsk and Mehta. Most involve a transient increase in
PEEP and peak ventilator pressures, which can be performed using a manual
technique or the ventilator.
Table 1.2 ARDS classification of severity
Classification of ARDS severity
(mmHg)
Mortality (%)
Length of mechanical
ventilation (days)
Mild (PFR < 300)
27% (CI 24–30)
5
Moderate (PFR 100–200)
32% (CI 29–34)
7
Severe (PFR < 100)
45% (CI 42–48)
9
25
26
Chapter 1
2. ARDSNet ventilator strategy which includes an appropriately high maintenance
PEEP > 14 mmHg with tidal volumes of less than 6 mL/kg and peak pressures of
less than 30 cmH2O.
3. Other ventilator settings such as reverse inspiratory: expiratory (I:E) time ratios
may be beneficial.
4. Fluid balance management is key for more long-term management. Recent
evidence suggests that avoiding a positive fluid balance increases ventilator-free
days and may reduce mortality.
5. Prone positioning has recently been shown to improve oxygenation, improve
28-day and 90-day mortality and is not associated with an increase in
complications if performed properly. It should be commenced early in the
disease process and for a minimum of 17–24 hours per day.
10. Extracorporeal membrane oxygenation (ECMO) is becoming increasingly used
for refractory respiratory failure in a select cohort of patients with reversible
conditions, however caries a significant risk of haemorrhage. It can only be
carried out in regional centres.
Two therapies investigated previously include steroid administration and oscillation
ventilation. Both these interventions do not improve outcome, and in the case of
oscillation may infer risk if used by a centre without significant experience. Therefore
they are no longer recommended treatment options for ARDS.
In summary, at present the only interventions for ARDS that infer a mortality benefit
is ARDSNet ventilator strategy, fluid balance managing and most recently prone
ventilation. In the above scenario the patient was not on an optimum ventilator
setting. Recruitment manoeuvres would be the most important first intervention
followed by maintenance of recruitment with appropriate ventilator settings.
Mackay A. Acute lung injury and acute respiratory distress syndrome. Contin Educ Anaesth Crit Care Pain
2009; 9(5):152–56.
Lapinsk S, Mehta S. Bench-to-bedside review: recruitment and recruiting maneuvers. Crit Care 2005;
9(1):60–65.
14. B Intravenous crystalloid bolus of 20 mL/kg followed by a
noradrenaline infusion to maintain blood pressure
Tricyclic antidepressants (TCA) are a class of drug used to treat depression, chronic
pain syndromes and attention deficit disorder in children. Amitriptyline is the most
commonly used in clinical practice. Overdose occurs at all ages including accidental
overdose. TCAs are some of the most frequently overdosed medications and
contribute to up to 300 deaths per annum in the UK.
Cardiovascular collapse is due to a sodium channel ‘stabilising effect’ due to
blockade of fast sodium channels in the myocardial conduction system. This leads
to an increase in QRS duration initially and may progress to decreased myocardial
excitability, bradycardia and asytole. In addition a dose-dependent decrease in
myocardial contractility occurs due to noradrenaline (NA) and serotonin re-uptake
inhibition. Alpha-1 adrenergic receptor blockade causes profound vasodilatation,
which leads to distributive shock.
Answers
Altered mental state resulting in confusion or agitation may be as a result of central
anti-histaminic and anti-cholinergic activity. Increasing central nervous system levels
of noradrenaline and serotonin reduces the seizure threshold.
The management of the patient described above should include an ABC approach
to protect the airway. All options are viable:
1. Once the airway is protected, if ingestion is within an hour of presentation
activated charcoal may be considered but this will only prevent further
gastrointestinal absorption and not impact the current emergent problem of
hypotension and may in fact worsen it.
2. Fluid and vasopressors are the most important initial management. This will
counteract the distributive shock component as described above. This may be
sufficient to improve mean arterial pressure resulting in a decrease in heart rate.
3. The high sodium load found in sodium bicarbonate stabilises the myocardium
and may prevent arrhythmias. It is indicated if the QRS width is over 100 msecs.
An alternative treatment is hypertonic saline if no metabolic acidosis is present.
Increasing plasma pH also has the effect of increasing drug protein binding,
which can be achieved by hyperventilation.
4. Amiodarone and other class 1a and 1c anti-arrhythmic agents should be avoided
as they increase the cardiac action potential. Both lignocaine and magnesium
have been used for arrhythmia management in TCA overdose.
5. There are case reports that lipid emulsion has been used successfully in cardiac
arrest secondary to TCA overdose by sequestering plasma drug and reducing
the active concentration. If used, this should follow the same protocol as for
local anaesthetic toxicity.
A multi-faceted approach is required however the initial management should focus
on airway control, volume expansion and management of vasoplegia before moving
onto more complex treatment options.
Body R, Bartram T, Azam F, Mackway-Jones K. Guideline for the management of tricyclic antidepressant
overdose. Emerg Med J 2011; 28(4):347–68.
Ward C. Oral poisoning: an update. Contin Educ Anaesth Crit Care Pain 2010; 10(1):6–11.
15. D Vital capacity < 15 mL/kg
The symptoms of progressive and ascending motor weakness with the antecedent
history of a viral infection suggest Guillain–Barré syndrome. Guillain–Barré is a
collection of diseases that result from acute inflammatory demyelination leading
to the hallmark signs of ascending muscle weakness and areflexia. Sensory and
autonomic function can also be affected by Guillain–Barré.
The pathophysiology of Guillain–Barré appears to be an immune mediated reaction
to a prior infection, commonly upper respiratory tract infections or Campylobacter
jejuni. Autoantibodies (such as antiganglioside autoantibodies) initiate either a
cascade of myelin destruction or axonal damage; the latter results from C. jejuni
infection with a worse prognosis.
Early detection of the need for intubation is imperative as rapid deterioration
can ensue. Indications for intubation predominantly include respiratory failure
27
28
Chapter 1
secondary to muscle weakness or the presence of bulbar symptoms necessitating
airway protection.
Whilst clinical signs of respiratory failure such as tachypnoea, hypoxia and
hypercapnia will strongly suggest the requirement for intubation, these are relatively
late signs. Serial vital capacity (VC) measurements should be taken and management
in a critical care area should be considered when VC < 20 mL/kg. Intubation should
be carefully considered when measurements fall below 15 mL/kg in the presence
of bulbar symptoms or rapidly progressive disease. Rapid sequence induction is
recommended due to the raised aspiration risk. In addition to full AAGBI monitoring,
invasive arterial blood pressure monitoring should be instituted, particularly in the
presence of autonomic instability. Due to reports of an exaggerated hyperkalaemic
response, depolarising muscle relaxants should be avoided.
Critical care management should include consideration of immunotherapy in liaison
with specialist teams. Intravenous immunoglobulin or plasma exchange is the
mainstay of current management, while steroids do not appear to have a role.
Richards KJC, Cohen AT. Guillain‐Barré syndrome. BJA CEPD Reviews.2003;3(2):46–49.
Yuki N, Hartung HP. Guillain–Barré syndrome. N Engl J Med 2012; 366(24):2294–304.
16. B Injury
Acute kidney injury (AKI) describes an abrupt decline in renal function. A number of
classification systems have been devised to further the definition and staging of AKI.
Three in common use are the RIFLE criteria (2004), AKIN criteria (2009) and KDIGO
(2012). All three rely on a defined creatinine rise with or without criteria for urine
output. There is an increasing recognition that serum creatinine may not detect early
AKI and the role of renal injury biomarkers, such as neutrophil gelatinase-associated
lipocalin (NGAL), is under investigation.
Of the three criteria to describe AKI, none have shown clinical superiority, although
the AKIN criteria are more sensitive. The question uses the RIFLE criteria as this is
commonly referred to in UK practice. According to RIFLE, AKI is subdivided into five
progressive stages based on creatinine rise and urine output. Further information
regarding the AKIN criteria can be found in question 10.13.
The patient described in the question has doubled his creatinine from baseline
and his urine output has been less than 0.5 mL/kg/hr (35 mL/hour) for 12 hours. He
therefore fulfills the RIFLE ‘injury’ criteria (Table 1.3).
Table 1.3 RIFLE criteria
Creatinine increase
Urine output
Risk
x 1.5
< 0.5 mL/kg/hr for > 6 hours
Injury
x2
< 0.5 mL/kg/hr for > 12 hours
Failure
x3
< 0.3 mL/kg/hr for > 24 hours
Loss
Complete loss of kidney function for > 4 weeks
End-stage
Complete loss of kidney function for > 3 months
Answers
The morbidity and associated mortality from AKI is high both within and outside
the critical care environment. Prevention, early recognition (using criteria) and
good adherence to the principles of management should be a part of routine care.
The principles of management include treating the underlying cause, optimising
renal perfusion, withholding nephrotoxic agents and, where appropriate, renal
replacement therapy.
The clinical importance of AKI has lead to a recent National Institute for Health
and Care Excellence (NICE) guideline and the London Acute Kidney Injury Network
releasing an ‘AKI bundle.’
National Institute for Health and Care Excellence. Acute Kidney Injury (CG169). 2013. London: National
Institute for Health and Care Excellence. Available from: http://guidance.nice.org.uk/CG169
London Acute Kidney Injury Network. Acute Kidney Injury Bundle. 2013. Available from: http://www.
londonaki.net/news/downloads/AKI_bundle-GSTH.pdf
17. B Methicillin sensitive Staphylococcus aureus (MSSA)
The case described has features consistent with the development of pneumonia
during the provision of invasive mechanical ventilation (MV). Ventilator-associated
pneumonia (VAP) has traditionally been defined as tracheobronchitis or pneumonia
occurring more than 48 hours after initiation of MV. This definition relies on a
high index of suspicion with confirmation based on clinical, radiological and
microbiological evidence. The definition of VAI remains a controversial area. A recent
Society of Critical Care Medicine (SCCM) guideline has suggested that VAP may not
require a positive microbiological diagnosis.
Clinical scoring systems, such as the Clinical Pulmonary Infection Score (CPIS), can
help to objectify the diagnosis of VAP. CPIS is based on temperature, white cell
count, appearance of tracheal secretions, new infiltrates on chest radiology and
oxygenation indices. A score of greater than 6 is suggestive of VAP. However the
validity of this score has been questioned.
The most commonly associated causative organisms tend to relate to the timing of the
infection from the onset of MV. In the case described here, the onset is early (< 5 days)
and as such is most commonly associated with MSSA and Haemophilus influenzae. The
commonest bacterial pathogens in late onset VAP (> 5 days) are aerobic gram negative
bacilli (AGNB) such as Klebsiella, Pseudomonas, Enterobacter and Acinetobacter. Drug
resistant microbes such as methicillin-resistant Staphylococcus aureus (MRSA) and
vancomycin-resistant Enterococci (VRE) are also causative organisms for late onset
VAP. The value of bronchoalveolar lavage (BAL) over and above blind endotracheal
aspiration is keenly debated.
The management of VAP is supportive with continuous microbiological
surveillance and antimicrobial therapy based on local policies in combination with
microbiological advice. The prevention of VAP is the focus of a Department of Health
(DoH) High Impact Intervention Care bundle. This document outlines six key areas of
recommended good practice:
• Elevation of the head of the bed to 30–45° (though trials of supine and even head
down positioning are currently in progress)
29
30
Chapter 1
• Daily sedation level assessment (though many would advocate mandatory daily
cessation for which there is a strong evidence base)
• Oral hygiene with chlorhexidine 6 hourly and tooth brushing 12 hourly
• Subglottic aspiration in patients expected to be intubated for > 72 hours (complex
and controversial evidence for this intervention)
• Tracheal cuff pressure measured 4 hourly and maintained between 20–30 cmH2O
• Stress ulcer prophylaxis prescribed only in high risk patients according to local
protocols and reviewed daily (though this contradicts the earlier DoH, ‘Ventilator
care bundle’)
Kalanuria AA, Zai W, Mirski M. Ventilator-associated pneumonia in the ICU. Crit Care. 2014;18(2):208.
Department of Health. High impact intervention care bundle to reduce ventilation-association
pneumonia. London: Department of Health, 2010.
18. E Site a spinal catheter, inform midwife and perform
subsequent top-ups yourself
Accidental dural puncture (ADP) is a well-known complication of epidural
anaesthesia, being said to occur in 0.2–4% of cases. Parturients are at risk due to
difficulty in positioning and being ‘moving targets’. In this case, there is the added
risk of multiple attempts at insertion and a high body mass index (BMI). This case
is typical of a pressurised situation on labour ward and the clinical setting must be
taken into account when deciding how to manage the ADP.
Repeating the attempt is a potential option but is not the best line of management
due to the difficulty of finding the space with multiple attempts already having been
undertaken.
The chance of a colleague being available to assist at this time is slim, as opposed
to during a day shift. Although this is a possibility, a colleague may also find this
epidural difficult to perform, and there may be a significant delay before they can
attend to help.
Ultrasound can help to locate the depth, but even with optimum conditions, this will
be difficult in a lady of this size, especially if you are unfamiliar with this technique.
Finding the ultrasound machine and the correct probe may also prove challenging
in the clinical circumstances.
A remifentanil PCA is a potential alternative, but in this situation, the lady has a high
risk of needing further intervention due to the position of the baby. Therefore, a
spinal catheter is the best option. To reduce the risks of neurological damage, no
more than 3 cm is left inside the subarachnoid space. The catheter must be clearly
labelled as intrathecal, and both the midwife and mother must be informed. Top-ups
must be given only by the anaesthetist. A suggested regime may be 2.5 mL of low
dose mixture (0.1% levobupivacaine + 2 μg/mL fentanyl) every 2–4 hours. This can
also be used if the patient goes on to need any operative intervention. There is also
some evidence that introducing a spinal catheter may reduce the incidence of post
dural puncture headache.
Sharpe P. Accidental dural puncture in obstetrics. BJA CEPD Reviews 2001; 1(3):81–84.
Palmer CM. Continuous spinal anesthesia and analgesia in obstetrics. Anesth Analg 2010;111(6):1476-9.
Answers
19. C Commence MgSO4 infusion at 1 g/hour, give a further
2 g MgSO4 bolus, secure airway with ETT and continue
supportive management
Pre-eclampsia is one of the causes of maternal death and since it is well managed,
it is not often that patients present with eclamptic seizures. The MAGPIE Trial
demonstrated that MgSO4 significantly reduces the risk of eclampsia and this
is standard management in these cases. The initial dose of MgSO4 is 4 g over
5–10 minutes followed by an infusion at 1 g/hour for 24 hours post-partum. Any
subsequent seizures may be treated with a further bolus of 2 g MgSO4. Phenytoin
and diazepam have no place in the management of eclampsia.
Every effort should be made to stabilise the mother (e.g. correct hypoxia, control
blood pressure and stop seizures) before undertaking a Caesarean section, as this is
a risky procedure to undertake whilst the mother is unstable. Also, the emergency
department is a dirty environment therefore the risk of postoperative infection
is high. There is unlikely to be diathermy available and the patient may bleed
significantly, which is a risk due to the disorders of coagulation that can occur in
eclampsia. Furthermore, the baby is only 28/40 and a course of steroid treatment
would help lung maturation if delivery were expected to be undertaken. It may be
better for the baby to undergo in utero recovery from hypoxia and hypercarbia.
If the mother were to arrest in the emergency department then an emergency
Caesarean section would be necessary.
National Institute for Health and Care Excellence Clinical Guideline. Hypertension in pregnancy: the
management of hypertensive disorders during pregnancy. August 2010 (revised reprint January 2011)
Hart E, Coley S. The diagnosis and management of pre-eclampsia. BJA CEPD Rev 2003; 3(2): 38–42.
The Magpie Trial Collaborative Group. Do women with pre-eclampsia, and their babies, benefit from
magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet 2002; 359:1877–90.
Munro P. Management of eclampsia in the accident and emergency department. J Accid Emerg Med 2000;
17(1):7–11.
20. A Start prostaglandin E2 intravenous infusion and refer
to tertiary centre for possible coarctation of the aorta
Stabilisation of critically ill neonates, as with all paediatric patients, should
prioritise securing the airway, then establishing breathing and maintaining
adequate circulation. Endotracheal intubation and fluid resuscitation are usually
required in critically ill neonates and these procedures, if indicated, should
not be delayed while waiting for diagnostic evaluation. Establishing optimal
ventilation and oxygenation is often sufficient to improve both respiratory and
cardiac insufficiency; however, continued IV fluids and resuscitation may be
required in the gravely ill neonate. An initial bolus of 10 mL/kg of isotonic fluid
(0.9% saline) should be given if necessary. Sepsis is one of the most common
causes of critical illness in the neonate and prompt empirical treatment with
antibiotics is almost always indicated. If the history and physical examination
suggest a possible cardiac diagnosis, a continuous infusion of prostaglandin E2
(Prostin, PGE2, 0.01–0.1 μg/kg/min) should be promptly initiated and paediatric
cardiology consulted.
31
32
Chapter 1
Coarctation of the aorta is a congenital narrowing of the descending thoracic aorta
at or near the connection of the ductus arteriosus. It is the sixth most common
congenital heart disease, constituting 8% of heart anomalies. The most dramatic
presentation of aortic coarctation occurs in the neonate who is dependent on a
patent ductus arteriosus (PDA) for blood flow to the distal aorta. After a relatively
asymptomatic period of days to weeks, the PDA will close and immediately limit
blood flow distal to the coarctation. The ensuing left ventricular failure and systemic
hypoperfusion manifest as respiratory distress, cold and pale lower extremities,
markedly decreased or absent pulses, metabolic and respiratory acidosis.
Kim UO, Brousseau DC, Konduri G. Evaluation and management of the critically ill neonate in the
emergency department. Clin Pediatr Emerg Med 2008; 9:140–148.
Landsman IS, Davis P J. Aortic coarctation: anesthetic considerations. Semin Cardiothor Vasc Anesth 2001;
5:91–97.
21. A IV Hartmann’s at 110 mL/hour. Refer to tertiary centre
for further management
Burns are a common cause of injury in children. Most burns occur at home, usually in
the kitchen and bathroom. The aetiology changes with age; younger children suffer
more scalds, older children more flame burns.
The anaesthetist’s roles include resuscitation, analgesia, sedation, anaesthesia and
intensive care management of these patients. Adequate early fluid resuscitation
maintains organ perfusion and controls the extent of the burn injury itself. Early
excision and covering of non-viable skin reduces morbidity, mortality, and the extent
of inflammatory response. Adequate pain management is an obligation and may
help to alleviate psychological sequelae.
Resuscitation fluid volumes are calculated using the Parkland formula: for the
first 24 hours after the burn, give 4 mL/kg per % body surface area (BSA) burn of
crystalloid, half of this volume should be delivered in the first 8 hours post-burn, the
other half in the next 16 hours. In this case:
4 mL x 15 kg x 20% = 1200 mL over 24 hours
Since 400 mL has already been given in the first 4 hours, only 200 mL should be given
in the next 4 hours, i.e. 50 mL/hour.
Maintenance fluid is calculated using the 4/2/1 rule:
• 4 mL/kg/hour for the first 10 kg body weight
• 2 mL/kg/hour for the next 10 kg body weight
• 1 mL/kg/hour for each kg body weight above 20 kg
For this 20 kg child, this works out to 60 mL/hour.
Therefore resuscitation (50 mL/hour) and maintenance fluid (60 mL/hour) together
is 110 mL/hour. Glucose containing intravenous fluids are not generally indicated
though may be required for infants when early feeding cannot be established.
Specialist services are required for full-thickness burns exceeding 5% of BSA,
partial thickness exceeding 10% BSA, inhalation burns or burns to the airway, face,
Answers
hands, feet, and perineum. Antibiotics are indicated only in suspected or confirmed
infection, not for prophylaxis.
Fenlon S, Nene S. Burns in children. Contin Educ Anaesth Crit Care Pain 2007;7:76–80.
22. A Increase dose of carbamazepine
This patient has trigeminal neuralgia.
Trigeminal neuralgia (TN), also known as tic douloureux, is a condition characterised
by paroxysmal episodes of intense, severe, lancinating facial pain. A typical episode
lasts seconds to minutes, and starts and ends abruptly. The pain itself is often
described as feeling like “electric shocks” or “stabbing”, and almost always affects just
one side of the face, frequently the right. Triggers are usually trivial and may include
washing the face, chewing food, brushing teeth, vibrations, or exposure to wind.
In particular, the maxillary and/or mandibular distributions of the trigeminal nerve
are most commonly affected. Attacks vary significantly in frequency, and may range
from just one or two, to several hundred per day.
Over time, TN follows a relapsing and remitting course. A relapse may last days or
months, and remission may be as long as several years.
Occurring more commonly in females, the peak incidence of TN is in the fifth and
sixth decades of life.
In approximately 80% of cases, there is compression of the trigeminal ganglion,
most commonly due to an aberrant arterial or venous loop. Other causes may
include multiple sclerosis, Chiari malformation, tumours such as schwannomas or
meningiomas, or pontine lesions.
Diagnosis is purely clinical. Differential diagnoses include post-herpetic neuralgia,
temporomandibular joint dysfunction, migraine, cluster headaches, and atypical
facial pain.
Magnetic resonance imaging (MRI) may be helpful to exclude other causes of pain if
the diagnosis is less obvious. It is the most sensitive test available for the diagnosis
of multiple sclerosis, and useful in visualising the posterior fossa where tumours
associated with TN such as schwannomas and meningiomas are found.
While TN may go into remission spontaneously, the symptoms are usually severe
enough to warrant treatment. Treatment options may be medical or surgical.
The drug of choice is carbamazepine. It is thought to be so effective that lack of
response, some authors suggest, should prompt reconsideration of the diagnosis.
It’s keto-derivative, oxcarbazepine, can be used with equal effect and with fewer
unwanted effects. Treatment should be commenced at a low dose, and then
gradually increased every 3–7 days until a dose suitable to that patient is found.
Carbamazepine, for example, is started at 100 mg b.d. and may need to be increased
to 200 mg q.d.s. Alternatives such as lamotrigine or baclofen may be tried if
carbamazepine or oxcarbazepine are contra-indicated or poorly tolerated.
Surgical options include microvascular decompression, rhizotomy, and stereotactic
radiosurgery, but due to the invasive nature of these interventions, they are reserved
33
34
Chapter 1
for refractory cases. In this patient, therefore, the most appropriate intervention at
this stage would be to increase the dose of carbamazepine appropriately.
Zakrzewska JM, Linskey ME. Trigeminal neuralgia. Br Med J 2014; 348:g474.
National Institute for Health and Care Excellence (NICE). Trigeminal neuralgia. Clinical Knowledge
Summary (CKS). London: NICE, 2013.
23. E The pain will usually respond to anticonvulsants
Chronic post-surgical pain (CPSP) is an increasingly common phenomenon and
its exact aetiology is unknown. Most of these pains are benign and local cancer
recurrence is unlikely at 2 years. The nature of the pain is mixed neuropathic and
nociceptive but phantom pain can occur in 22–64% of post-mastectomy patients
and it is appropriate to use anticonvulsants such as gabapentin to treat such pain.
The use of long-term opioids is not recommended as tolerance usually develops
and long-term hormonal and immune suppression is increasingly recognised.
Although brachial plexopathy can cause chest wall pain, these patients often have
arm symptoms rather than pure chest wall pain. Also, brachial plexopathy is usually
only found if the cancer has recurred, while the 2-year history would make it unlikely
in this circumstance. Therefore the most appropriate statement is that this patient's
pain will probably respond to anticonvulsants.
Alves Nogueira Fabro E, Bergmann A, do Amaral E Silva B, et al. Post-mastectomy pain syndrome:
incidence and risks. Breast 2012; 21(3):321–5.
24. C Patient education and psychological support
This patient has developed symptoms and signs of complex regional pain syndrome
(CRPS) type 1.
CRPS is a chronic, debilitating and painful condition. It is uncommon and usually
develops following an injury, but may occur spontaneously. It affects one or more
limbs and typically demonstrates a collection of symptoms and signs described as
sensory, vasomotor, sudomotor, trophic and inflammatory. The presentation varies
from mild and self-limiting to a chronic and disabling disease process.
Diagnosis is clinical. In 1994, the International Association for the Study of Pain (IASP)
established a definition, but the latest definition came from Budapest in 2004.
The Budapest criteria classify symptoms and signs into four broad categories
(Table 1.4).
According to the Budapest criteria, all of the following must be met in order to make
a diagnosis of CRPS:
•
•
•
•
The patient has continuing pain which is disproportionate to the inciting event
The patient has at least one sign in two or more categories
The patient has at least one symptom in three or more categories
No other diagnosis can better explain the signs and symptoms
CRPS can be academically classified as being type 1 (not associated with major
nerve damage) or type 2 (associated with major nerve damage), but this does not
influence subsequent management or prognosis.
Answers
Table 1.4 The Budapest criteria diagnostic categories
Category
Sign
(detected clinically)
Symptom
(patient complaint)
Sensory
Allodynia, hyperalgesia
Hyperalgesia
Vasomotor
Changes/asymmetry in skin colour
Temperature asymmetry > 1oC
Changes/asymmetry in skin colour
or temperature
Sudomotor/oedema
Sweating asymmetry
Oedema
Sweating asymmetry
Oedema
Motor/trophic
Decreased range of motion
Weakness, stiffness, tremor
Motor dysfunction
Hair/skin/nail changes
Aetiology is uncertain and thought to be multifactorial, as no one single theory
fully explains the condition. Current hypotheses include an inflammatory process,
or altered neurological function. There may be an association between the use of
angiotensin converting enzyme (ACE) inhibitors and the development of CRPS.
Regarding treatment, there is a lack of robust evidence for CRPS and most
recommendations are derived and extrapolated from those for other neuropathic
pain conditions. Early treatment may help prevent the development of some of the
longer term sequelae of severe CRPS.
There are four equally important aspects to treatment (see Table 1.5).
In this scenario, the patient must first be educated about the condition and fully
involved in decisions regarding his subsequent management. This will establish
whether he will benefit from treatments such as mirror therapy, motor imagery or
CBT. Physiotherapy and occupational therapy are both recommended early.
Table 1.5 Treatment options in CRPS
Area of treatment
Description
Example
Patient information/education
Support self-management
Ensure patient understands
condition, and be involved in
making informed decisions
about their treatment options
Information leaflets
Sufficient time spent with
patient and family
Allow questions
Physical and vocational rehabilitation
General physiotherapy/occupational therapy
Specialised PT/OT
Stretching, weight bearing, fine
motor exercises
Mirror therapy
Graded motor imagery
Pain relief methods
Medical or procedural options
Medical: amitriptyline, pregabalin, 5% lignocaine patches,
ketamine, steroids
Spinal cord stimulation, intravenous regional blocks
Psychological interventions
Both patient and family benefit
from psychotherapy, significant
psychological burden of CRPS
Cognitive behavioural therapy
(CBT)
35
36
Chapter 1
Pharmacologically, there is a lack of evidence for the benefits of anti-neuropathic
agents. Amitriptyline is the first line agent of choice for neuropathic pain in general,
followed by pregabalin. Additionally, there is still limited evidence to support early
use of acupuncture in the treatment of CRPS patients.
Ganty P, Chawla R. Complex regional pain syndrome: recent updates. Contin Educ Anaesth Crit Care Pain
2013; 14(2):79–84.
Turner-Stokes L, Goebel A. Complex regional pain syndrome in adults: concise guidance (on behalf of the
Guideline Development Group of the Royal College of Physicians). Clin Med 2011; 11:596–600.
25. B It is the basis of how transcutaneous electrical nerve
stimulation (TENS) machines work
The gate theory of pain was proposed by Wall and Melzack in 1967. They stated that
pain synapses are affected by other neural inputs and inhibitory signals may prevent
nociceptive impulses passing to the central nervous system. This applies to all pain
and is the basis of how transcutaneous electrical nerve stimulation (TENS) and spinal
cord stimulation work. It does not explain all pain phenomena, and other theories
such as the neuromatrix theory exist. This hypothesizes that the brain has a map of
the body and disruption of peripheral input may be represented as pain.
Supraspinal input is not always required and an example is the use of localised heat
and light touch causing Aβ fibres impulses to inhibit pain (see Figure 1.5).
C fibres
–
Inhibitory
interneuron
+
–
+
secondary
neuron
To forebrain
Figure 1.5 The gate theory of
pain. Activation of Aα or Aβ
fibres may activate inhibitory
interneurones that reduce
transmission of primary
nociceptive transmission
by C fibres to the forebrain.
Activation of these Aα/Aβ fibres
is the principle of TENS, rubbing
painful areas, or local heat
application.
Αα/Αβ fibres
Aδ have thin, myelinated axons that are responsible for the transmission of thermal
and pressure signals as well as mediating fast pain signals.
The gate theory of pain applies to both adults and children.
Lynch L, Simpson KH. Transcutaneous electrical nerve stimulation and acute pain. BJA CEPD Reviews 2002;
2(2):49–52.
26. B Reduce the dose of morphine
Pain is a common symptom amongst those suffering with malignant disease, and its
management can be challenging. Aetiology of pain in cancer is multifactorial, and
causes may include:
Answers
•
•
•
•
•
•
Mass effect of the tumour
Effect of treatment, e.g. radiotherapy, chemotherapy
Paraneoplastic syndromes
Conditions associated with the disease process, e.g. osteoporosis, hypercalcaemia
Pre-existing pain from other chronic conditions
Combination of any of the above
Table 1.6 summarises some of the strategies that may be employed in controlling
pain.
Opioids are very effective in management of cancer-related pain in general. To begin
with, most patients are started on longer acting oral opioids to treat background
pain, supplemented with additional doses to treat breakthrough pain. Oral
morphine is a suitable agent for most patients, but different people may display an
unpredictably different benefit-side-effect profile with different opioids.
Table 1.6 Strategies for pain control
Method of pain
control
Examples
Pharmacological
WHO analgesic ladder is a guide, but sometimes patients may need to
start with strong opioids in the early stages of treatment
Adjuvant medications such as ketamine
Anti-neuropathic agents such as amitriptyline, pregabalin
Steroids reduce oedema and inflammation around tumour growth, hence
reducing local mass effects
Bisphosphonates for bone pain from osteoporosis or metastases
Antispasmodics
Oncological
Chemotherapy
Radiotherapy
Hormonal therapy, e.g. tamoxifen
Immunotherapy, e.g. Herceptin
Surgical
Treatment of gastrointestinal obstruction
Reduction and treatment of pathological fractures
Curative surgery
CSF shunt procedures
Psychological
Grief counselling
Cognitive behavioural therapy
Relaxation techniques
Pain management programmes
Complementary
Therapies
Acupuncture
Reflexology
Herbal remedies
Interventional
techniques
Spinal cord stimulation
In general, a low dose oral preparation is commenced. The dose is then increased by
30–50% gradually over intervals of 2–3 days until adequate control of symptoms is
achieved. If using morphine as an example, an appropriate dose for breakthrough
pain would be 1/6 of the total daily morphine requirement.
37
38
Chapter 1
It is not uncommon to use parenteral routes to administer opioids. In palliative care
settings, opioids are frequently administered subcutaneously by syringe driver.
Those on very large doses of oral morphine (> 60 mg per 24 hours) may benefit from
a fentanyl patch.
Long-term opioid use is associated with significant unwanted effects. These include
dependence, tolerance, drowsiness, constipation, nausea, vomiting, pruritus, urinary
retention and respiratory depression. Sometimes, patients may report a paradoxical
worsening of their pain. This is a phenomenon known as opioid-induced hyperalgesia.
Unwanted side effects will usually settle as tolerance develops. However, at times they
may be more distressing than the pain itself, as in this scenario.
If adverse effects of opioids cause the patient notable distress or discomfort they
warrant specific treatment. The reversal agent naloxone has an extremely short
plasma half-life, and while it is useful for acute opioid poisoning, it has no role in
a chronic setting. In the first instance, the dose of opioid should be reduced, but
other adjuvant analgesia should be prescribed, e.g. paracetamol or ketamine.
Anti-pruritic drugs, laxatives, and other medication for symptom relief may be
considered. Failing this, opioid rotation may be attempted. This is a method by
which one opioid is substituted for an equipotent dose of another (e.g. oxycodone
for morphine).
Prescribing a laxative is not the best option here as it only tackles constipation,
rather than treating the problem of unwanted effects as a whole.
Scott-Warren J, Bhaskar A. Cancer pain management – Part 1: General principles. Contin Educ Anaesth Crit
Care Pain 2014, doi: 10.1093/bjaceaccp/mkt070.
Ripamonti CI, Bandieri E, Roila F. Management of cancer pain: ESMO. Ann Oncol 2012; 23(suppl 7):vii39–
vii154.
27. B Enteral nutrition should be started as soon as possible
Following a significant burns injury, the resultant increase in basal metabolic rate is
proportional to the size of the burn and is thought to peak at 7–10 days. Early enteral
nutrition is essential and has been shown to improve survival. Good nutritional
support minimises protein breakdown, improves wound healing and reduces
infective complications. A high protein and carbohydrate diet is required.
Patients with severe burns reset their baseline temperature to 38.5°C. It is therefore
important to prevent hypothermia by ensuring ambient room temperature is kept
between 28–32°C as well as all the usual warming measures. There is no evidence
for prophylactic antibiotics in patients with burns. Diagnosis of sepsis in these
patients is difficult as the burn itself results in a systemic inflammatory response
syndrome (SIRS) that mimics sepsis. It is important to be vigilant to the presence of
infection as this represents a significant source of morbidity and mortality in major
burns. To reduce resistance, antibiotics should only be started following positive
cultures or when there is a high index of clinical suspicion. Skin grafting, aseptic
dressing changes and patient isolation are all measures that reduce the risk of
infection.
Prophylactic steroids are not indicated in the routine management of burns patients.
Answers
The Parkland formula (volume to be infused in first 24 hours = 4 mL/kg/% body
surface area burn) is merely a guide to fluid resuscitation in burns and will almost
always need to be adjusted. Too much fluid can be as detrimental as too little. The
complications of over resuscitation include abdominal compartment syndrome, the
need for fasciotomies to prevent extremity necrosis and pulmonary oedema. The
resultant SIRS leads to increase capillary permeability, so even if fluid management is
optimal there will still be a degree of oedema.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3): 118–122.
28. E Optimising the intravascular volume during aortic
cross-clamping
Hypotension following the application of aortic cross-clamp is a significant
intra-operative event. The most effective interventions that can minimise this
haemodynamic instability include optimal fluid resuscitation during the pre-release
phase and gradual release of the aortic cross-clamp by the surgeon.
Although they have a role, vasoconstrictors and inotropes are not as effective
if initiated following aortic cross-clamp release. Hypoperfusion to the lower
limbs leads to anaerobic metabolism, metabolic acidosis and hyperkalaemia.
This in turn reduces the sensitivity of adrenergic receptors in the affected areas.
If used, vasoconstrictors will increase the systemic vascular resistance causing
vasoconstriction in the upper limbs, potentially diverting the blood away from the
central compartment and thereby compromising cardiac output.
Administration of fluids is less effective in the post-release phase, and a 500 mL
colloid bolus during the release of the cross-clamp is often insufficient resuscitation.
Tilting the table head up would only decreased the left-ventricular preload and
cause hypotension. Therefore, carefully optimising the patients intravascular
status throughout the operation is the safest method to mitigate the predictable
hypotension following aortic cross-clamping.
Gelman S. The pathophysiology of aortic cross-clamping and unclamping. Anesthesiology 1995; 82:1026–
60.
29. E T wave inversion in lead aVR
Arrhythmias may occur preceding a myocardial infarction or may lead to ventricular
fibrillation, thus it is necessary to identify them and treat them without a delay.
As with any other medical emergency there needs to be an ABCDE approach. A 12lead ECG would differentiate between broad QRS complex and narrow QRS complex
tachyarrhythmias.
It is important to look for features suggesting clinical instability in view of the
arrhythmia. In the presence of such adverse features it is necessary to perform direct
current cardioversion in attempt to restore sinus rhythm. These features include:
• Shock: hypotension (systolic pressure <90mmHg), pallor, cold clammy extremities,
sweating, confusion or impaired consciousness
39
40
Chapter 1
• Syncope: transient unconsciousness due to compromised cerebral blood flow
• Myocardial ischaemia: clinical features of chest pain or ECG changes suggesting
the same
• Heart failure: pulmonary oedema and raised jugular venous pressure (with or
without peripheral oedema or enlarged liver)
T wave inversion in aVR is normal ECG morphology, and therefore not an adverse
feature necessitating urgent intervention.
Resuscitation Council (UK). Peri-arrest arrhythmias. In: Advanced Life Support, 6th ed. London:
Resuscitation Council (UK), 2010.
30. A Vitamin A
This patient presents with clinical features suggesting vitamin A deficiency. Vitamin
A is an essential nutrient whose deficiency leads to eye and skin manifestations.
It is found as retinol and beta-carotene in the diet. Retinol comes from animal
sources like liver, fish and eggs whereas beta-carotene is found in fruits and green
vegetables. Peak incidence for vitamin A deficiency occurs in children aged 2-5 years
due to poor nutrition .
Skin effects are seen as repeated skin infections, acne and dry skin. It can also lead to
thrush and dry hair.
Vitamin A deficiency leads to dry conjunctivae (xerosis) and night blindness. Small,
raised, grey plaques are found in the interpalpebral conjunctivae called Bitot’s spots.
Corneal ulceration and perforation may occur in extreme cases.
Treatment is by administering retinol palmitate intramuscularly or beta-carotene
orally.
Collier J, Longmore M, Scally P. Oxford Handbook of Clinical Specialties, 7th ed. Oxford: Oxford University
Press, 2007.
Chapter 2
Mock Paper 2
Questions
1. 5 days ago a 25-year-old woman suffered a traumatic brain injury. Despite a
normal CT, she demonstrated bilateral motor posturing. She therefore had an
intracranial pressure (ICP) bolt inserted shortly after admission in order to
monitor her ICP. You begin your morning review by analysing her ICP waveform.
Which of the following would concern you most acutely?
A
B
C
D
E
Lundberg A waves
A flat trace
A baseline value of 20 mmHg
Lundberg B waves
The most prominent upstroke being the P2 (tidal) wave
2. You are called to the emergency department to assist with a 20-year-old man
who presented following a grand-mal seizure. He has begun fitting again and his
conscious level has remained below baseline for 30 minutes. He has a history of
epilepsy and has not been taking his usual medication since his prescription ran
out 1 week ago. He is otherwise well.
Which of the following is the most appropriate immediate action?
A
B
Intubate the patient to protect his airway and optimise ventilation
Check his blood glucose and treat any hypoglycaemia with intravenous
dextrose
C Take blood for full blood count, electrolytes, urea, creatinine, liver function
tests and anti-epileptic medication levels
D Administer his anti-epileptic medication intravenously
E Apply pulse oximetry, blood pressure and ECG monitoring
3. You are asked to pre-assess a 68-year-old man for elective open umbilical hernia
repair. He suffers from exertional angina (three flights of stairs) and had coronary
angiography 6 months ago, which showed right coronary and circumflex artery
disease. He had a myocardial infarction 2 years ago. His symptoms have been
stable over the past year and he is currently taking bisoprolol 2.5 mg once a day
(o.d.), aspirin 75 mg o.d. and ramipril 2.5 mg o.d. His creatinine is 120 μmol/L. He is
not diabetic and has not had a stroke. He is independent and performs all his own
housework.
42
Chapter 2
Which of the following is the most appropriate next step in this patient’s
management?
A
Schedule the patient for surgery. Cease the ramipril 24 hours preoperatively.
Continue the aspirin
B Schedule the patient for surgery. Cease the bisoprolol 2 days preoperatively.
C Obtain non-invasive stress testing
D Refer for repeat coronary angiogram
E Refer for coronary artery bypass surgery
4. A healthy 30-year-old man due for an appendicectomy is undergoing a rapid
sequence induction. After full pre-oxygenation and administration of thiopentone
and suxamethonium, three attempts at intubation have failed with an unexpected
grade III Cormack & Lehane laryngoscopy view. His oxygen saturations are 92%
and full cricoid pressure is being applied.
What action is most appropriate in this situation?
A
B
C
D
C
Reattempt intubation using a different laryngoscope
Reattempt intubation whilst reducing the cricoid pressure
Attempt insertion of a supraglottic airway device
Postpone surgery and awaken the patient
Attempt cannula cricothyroidotomy
5. An 80-year-old woman, admitted with pneumonia 14 days ago, suffers an episode
of large haematemesis requiring endoscopic investigation. You anaesthetise
her and secure her airway uneventfully with a size 7.5 endotracheal tube
(ETT) secured at 24 cm to the teeth. Oxygen saturations are 99% (Fio₂ 0.4). The
gastroenterologist then extends her head. At this point she becomes progressively
hypoxic and chest wall movement becomes limited to the right side.
What is the most likely reason for her desaturation?
A
B
C
D
E
Aspiration of gastric contents
Bronchospasm
Sputum plugging of a bronchus
Pneumothorax
Endobronchial intubation
6. A 56-year-old man is taken to the intensive care unit following a laparotomy a
week ago for bowel obstruction. He is hypertensive, has a body mass index (BMI)
of 42, and has had an ileus for the last 7 days. His abdomen is tender and tensely
distended. There are no signs of sepsis, but he has worsening renal function
and a poor urine output, despite a very positive fluid balance. He had become
increasingly breathless with type II respiratory failure, and after a failed trial of
non-invasive ventilation, is now mechanically ventilated. His ventilator pressures
are worsening and his base excess and lactate are increasing.
Which of the following is the most correct regarding this patient?
Questions
A
A measurement of intra-abdominal pressure is most safely performed with an
intraperitoneal catheter and pressure transducer
B An intravesical measurement is performed at the end of inspiration
C Abdominal compartment syndrome may provoke a cardiac arrest at
laparotomy
D An abdominal pressure of 24 mmHg can be considered normal
E The only effective treatment is re-laparotomy leaving the abdomen open with a
Bogota bag
7. A 60-year-old man awaiting surgical resection for his tracheal carcinoma presents
to the emergency department with worsening dyspnoea. As part of his pulmonary
function tests, a bedside flow-volume loop (spirogram) is ordered.
What will be the most likely appearance of his flow-volume loop?
A
B
C
D
E
Flattening of the inspiratory limb only
Flattening of the expiratory limb only
Flattening of both the inspiratory and expiratory limbs
Saw-tooth pattern in both the inspiratory and expiratory limbs
Normal appearance of both inspiratory and expiratory limbs
8. A 32-year-old woman was recently diagnosed with brainstem death following
a subarachnoid haemorrhage. She was initially hypertensive, then developed
polyuria and gradually became hypotensive. The patient has received 30 mL/kg of
crystalloid boluses.
What is the next pharmacological intervention needed to restore the patient's
blood pressure?
A
B
C
D
E
Dopamine
Adrenaline
Vasopressin
Noradrenaline
Further bolus of colloid
9. You have been asked to see a 32-year-old patient in recovery following a retrograde
intramedullary femoral nailing. He works as a builder and fell from a ladder
sustaining bilateral femoral fractures. The plan is to fix the other leg in the next few
days. He is desaturating to 88% on oxygen via facemask and is confused, and one of
the recovery staff has also noticed a petechial rash on the patient’s neck.
In diagnosis and treatment of the likely condition, which of the following tests is
most important?
A
B
C
D
E
Arterial blood gas analysis
Bronchoscopic alveolar lavage (BAL) for macrophages
Trial of methylprednisolone for 48 hours
A CT of the chest
Urine microscopy for lipid droplets
43
44
Chapter 2
10. A 50-year old woman for elective hand surgery is to have an ultrasound guided
axillary brachial plexus block.
Which of the following would be the most appropriate ultrasound probe to use?
A
B
C
D
E
Curved array probe
Linear array probe
Low frequency (2–5 MHz) probe
Phased array probe
Hockey stick footprint probe
11. A 38-year-old man has sustained a stab wound in the left flank following an
altercation. In the emergency department he is awake and has saturations of 99%
on room air, a respiratory rate of 25 breaths per minute, a heart rate of 110 beats
per minute and a blood pressure of 85/40 mmHg. Initial resuscitation has started
with intravenous access and blood samples taken. Any other injuries have been
excluded apart from a dry puncture wound to the left flank associated with mild
abdominal tenderness and no peritonism.
What is the next step in the ongoing resuscitation of this patient?
A
B
C
D
E
A fluid bolus of 10 ml/kg of colloid
A fluid bolus of 10 ml/kg of crystalloid
No fluid bolus
Insert an arterial line
Admit the patient to the emergency department observation ward
12. A 55-year-old woman with a 1-month history of headaches presents with a
severe headache followed by a collapse. In the emergency department of a large
teaching hospital her Glasgow coma scale (GCS) was 3 and she was intubated
and ventilated appropriately. A CT scan demonstrated a large subarachnoid
haemorrhage (SAH) with blood in the intraventricular system and dilated lateral
ventricles. A CT angiogram demonstrated a large posterior communicating artery
aneurysm. Her pupillary response to light is sluggish.
The most beneficial intervention in this patient would be:
A
Immediate transfer to neurosurgical theatre for an extraventricular drain
(EVD)
B Immediate transfer to neurosurgical theatre for insertion of an intracranial bolt
monitor
C Immediate transfer to the intensive care unit for medical stabilisation before
embolisation of the aneurysm
D Administration of hypertonic saline and mannitol
E Administration of intravenous phenytoin
13. A 52-year-old man is admitted to the emergency department one hour ago with
worsening shortness of breath, fevers and productive sputum. His observations
include a temperature of 38°C, Spo2 95% on high-flow oxygen, blood pressure
88/49 mmHg, heart rate 126 beats per minute and respiratory rate 28 breaths per
minute. His arterial blood gas is below (Table 2.1):
Questions
Table 2.1 Arterial blood gas test results
Parameter
Result
Fio2
0.4
pH
7.21
Paco2
4.8 kPa
Pao2
11.4 kPa
Base excess
–5.6 mmol/L
–)
Bicarbonate concentration (HCO3
20.6 mmol/L
Potassium concentration (K+)
4.8 mmol/L
+
Sodium concentration (Na )
138 mmol/L
Lactate
4.6 mmol/L
Blood cultures have been taken and a dose of co-amoxiclav and clarithromycin has
been administered.
The most appropriate next step would be:
A
B
C
D
E
Intubation and ventilation
Central venous access and noradrenaline
Central venous access and measurement of Scv–o2
Non-invasive ventilation
30 mL/kg crystalloid bolus
14. An 18-year-old woman presents to the intensive care unit with diabetic
ketoacidosis (DKA) for which she has had multiple admissions in the past. On
examination her heart rate is 110 beats per minute and her blood pressure is
100/60 mmHg. Her Glasgow coma scale (GCS) is 14 (E3, V5, M6). Her laboratory
glucose was 39 mmol/L and the arterial blood gas demonstrated the following
(Table 2.2):
Current treatment is an insulin infusion of 5 units/hour and 500 mL of intravenous
Hartmann’s solution being administered over 4 hours.
Table 2.2 Arterial blood gas test results
Parameter
Result
pH
6.9
Pao2
14.1 kPa
Paco2
2.1 kPa
Bicarbonate concentration (HCO3–)
3.4 mmol/L
Lactate
2.2 mmol/L
Potassium concentration (K+)
4.6 mmol/L
45
46
Chapter 2
How would you alter her treatment on admission to the ICU?
A
B
Reduce the rate of insulin when her blood sugar drops below 30 mmol/L
Increase the insulin infusion by 1 unit/hr if the bicarbonate concentration
remains 3 mmol/L after 1 hour
C Change the intravenous fluid from Hartmann’s solution to 0.9% sodium
chloride and add potassium 20 mmol to be given over 4 hours
D Give a fluid bolus of 500 mL of crystalloid to assess cardiovascular and
metabolic response
E Start an infusion of bicarbonate 1.26% 100 mL/hour to correct the acidosis
until the blood ketone level reduces as a result of insulin therapy
15. A 76-year-old patient is admitted to the postoperative care unit (POCU) following
a prolonged and difficult laparotomy for ischaemic bowel. She underwent an
extended right hemicolectomy, associated bowel oedema was noted. Her intraabdominal pressure (IAP) is monitored due to her risk of abdominal compartment
syndrome (ACS).
Which of the following would define abdominal compartment syndrome in this
patient:
A
B
C
D
E
IAP > 12 mmHg with new organ dysfunction
IAP > 16 mmHg with new organ dysfunction
IAP > 20 mmHg with new organ dysfunction
IAP > 25 mmHg with new organ dysfunction
IAP > 30 mmHg with new organ dysfunction
16. A 24-year-old asthmatic presents to the emergency department with wheeze,
shortness of breath and a peak flow which is 20% of his usual. He has had two
courses of steroids in the past year and has been hospitalised twice for acute
asthma. The medical team has asked you to review him as they are worried he is
tiring and not responding to initial treatment.
Which feature is most likely to suggest that this is the case?
A
B
C
D
E
pH of 7.32
Oxygen saturations of 88% on air
Unable to complete sentences with single breath
Responding to voice on the AVPU score
No improvement despite optimum therapy including a salbutamol infusion
17. A 37-year-old woman with a past history of asthma is 38/40 pregnant and
undergoing a category 2 Caesarean section for pre-eclampsia. The baby and
placenta have been delivered, 5 IU of syntocinon has been given and a syntocinon
infusion commenced. The estimated blood loss so far is 800 ml and the obstetric
registrar informs you “the uterus is still floppy”.
Which of the following is the best drug to use next?
Questions
A
B
C
D
E
5 IU syntocinon intravenously
5/500 syntometrine intravenously
250 μg carboprost intramuscularly
1 mg misoprostol rectally
Atosiban 6.75 mg intravenously
18. A 6-year-old, 24 kg boy is seen in the emergency department having fallen on his
right arm. An X-ray confirmed a closed displaced fracture of the right distal radius.
There is no neurovascular compromise to the right hand. He was given 2.4 mg of
oral morphine for pain. The surgeon wants to perform an urgent manipulation
under anaesthesia with percutaneous wiring. The boy last ate 9 hours ago and the
fall occurred 7 hours ago.
The immediate anaesthetic management should be:
A
Proceed immediately with surgery with routine induction of general
anaesthesia
B Proceed immediately with surgery under general anaesthesia following a rapid
sequence induction and intubation
C Delay general anaesthesia and surgery by a further 4 hours, and then perform a
rapid sequence induction and intubation
D Delay general anaesthesia and surgery by further 12 hours, and then proceed
as an elective case
E Proceed with surgery under an axillary brachial plexus block
19. A 9-year-old 30 kg girl has woken up in the anaesthetic recovery area after an
emergency open appendicectomy. She is in distress and complaining of pain
over the surgical site. Intraoperatively she was given 50 μg of fentanyl, 450 mg of
paracetamol, and 15 mg of ketorolac all intravenously. A right-sided transverse
abdominal plane block was performed using 20 mL of 0.25% bupivacaine. Her
most recent set of clinical observations are:
•
•
•
•
Heart rate 128 beats per minute
Respiratory rate 22 breaths per minute
Blood pressure 122/82 mmHg
Spo2 99% on air
The most appropriate management is:
A
B
C
D
E
Midazolam 20 μg/kg intravenous bolus to treat emergence delirium
Propofol 0.5 mg/kg intravenous bolus to treat emergence delirium
Fluid bolus of 20 ml/kg 0.9% NaCl to treat hypovolaemia
Morphine 50 μg/kg intravenous bolus for analgesia
Morphine 20 μg/kg/hour intravenous infusion for analgesia
20. A 6-month-old 7 kg boy is scheduled for an elective orchidopexy for undescended
testis. He was intubated successfully following an uneventful intravenous
induction. A caudal block was performed with 7 ml of bupivacaine 0.25%. The
ECG showed occasional ventricular premature beats immediately after the caudal
47
48
Chapter 2
block was performed. Shortly after that, the ECG showed a regular broad complex
tachycardia at 160 beats per minute. You notice the end tidal CO2 trace becomes
flat despite good bilateral chest movement. There are no palpable pulses.
Your immediate first action is:
A
B
Announce cardiac arrest, call for help, and start chest compressions
Give 1.5 mL/kg of 20% lipid emulsion as an intravenous bolus over 1 minute,
followed by an infusion of 15 mL/kg/hour
C Request for the cardiac defibrillator and deliver a DC shock of 4 J/kg
D Request the local anaesthetic toxicity box
E Give 0.1 mL/kg of 1:10,000 epinephrine intravenously
21. A 6-year-old girl is admitted with acute appendicitis. After uncomplicated surgery
she is noted to be in discomfort and crying.
In the assessment this child’s pain, which of the following is most correct:
A
B
C
The FLACC scale is for 1 month and above
Self-reporting is reliable over the age of 10
The visual analogue scale (VAS) can be used in patients aged 12 years and
above
D Physiological measures such as heart rate can be used alone
E The Wong-Baker FACES pain scale consist of 5 hand drawn faces
22. A 45 kg, 83-year-old woman with dementia and chronic kidney disease is admitted
with a right fractured neck of femur following a fall. She is in severe pain, is
confused and agitated. She has been given regular paracetamol, and is booked for
a dynamic hip screw.
Which of the following is the best method to provide her with adequate analgesia
intra- and postoperatively?
A
B
C
D
E
Fascia liaca block
Femoral nerve block
Spinal anaesthesia
Codeine phosphate
Intravenous morphine
23. A 61-year-old woman presents with worsening left sided chest pain over the last
3 months. She describes an intense burning sensation over the T5 distribution,
which began after an episode of shingles 4 months ago. The pain gets worse
through the day, and especially during the night when it disturbs her sleep. It may
be triggered by cold wind blowing over the painful part, or her clothes rubbing
against it. She has been taking co-codamol with only modest effect.
Which of the following is the most appropriate next step in her management?
A
B
Lignocaine patch
Oral morphine sulphate
Questions
C Topical capsaicin
D Gabapentin
E Thoracic sympathectomy
24. A 45-year-old man has undergone multiple spinal surgeries in the past and has
been on 80 mg daily of slow release morphine for the past year. He is asking for an
increase in his medication.
Which of the following most appropriately describes this patient’s opioid therapy?
A
B
C
D
E
There is no upper limit on the efficacy of opioids
Respiratory depression is a significant risk at this dose
Hyperalgesia may develop with increasing dosage
Constipation is usually resolved after 1 year
Levels of serum adrenocorticotrophic hormone (ACTH) may be increased
25. A 31-year-old woman with a history of acute intermittent porphyria presents with
severe abdominal pain. She is tachycardic, hypertensive and vomiting. A diagnosis
of small bowel obstruction is made and she is to go to theatre for a laparotomy.
Which of the following is the best option for her postoperative analgesia?
A
B
C
D
E
Epidural with levobupivacaine and fentanyl
Titrated intravenous ketamine
Intravenous morphine
Oxycodone
Wound infiltration of 0.25% levobupivacaine
26. A 32-year-old man is undergoing emergency surgery under general anaesthesia for
a penetrating eye injury. During the procedure, the surgeon palpates the globe and
tells you that the intraocular pressure (IOP) is too high.
Which of the following measures is least likely to reduce the IOP?
A
B
C
D
E
Adequate muscle relaxation
Trendelenburg positioning
Increasing minute ventilation
Intravenous acetazolamide
Intravenous mannitol bolus
27. A 71-year-old man is undergoing a bilateral ilio-femoral bypass graft with the aid
of a cell salvage device. The surgeons have completed the right ilio-femoral bypass
and are preparing to begin operating on the left side when you notice that the
blood returned to the patient from the cell salvage device is 1,900 mL.
After sending a clotting sample to the lab, what is the most appropriate next step in
the management of this patient’s blood loss?
A
B
Await the lab results and treat the coagulation accordingly
Request cryoprecipitate and platelets from the blood bank
49
50
Chapter 2
C Administer a 1 g bolus of tranexamic acid intavenously
D Use hypotensive anaesthesia to decrease further blood loss
E Check the patients activated clotting time (ACT)
28. A 67-year-old man is admitted to the emergency department with a sudden
onset of severe chest pain and breathlessness. His ECG shows ST elevation in the
following leads: I, aVL and V2–V6.
Which of the following is the most likely affected blood vessel?
A
B
C
D
E
Left anterior descending artery
Right coronary artery
Left circumflex artery
Left coronary artery
Posterior descending artery
29. A 7-year-old boy presents following a head injury by falling from a height of
3 metres. On assessing his neurological status he opens his eyes to a painful
stimulus, cries to pain and withdraws from a painful stimulus.
Which score on the paediatric Glasgow coma scale best represents the findings?
A
B
C
D
E
Eyes 2 Verbal 3 Motor 4
Eyes 1 Verbal 2 Motor 4
Eyes 2 Verbal 2 Motor 3
Eyes 3 Verbal 3 Motor 4
Eyes 2 Verbal 4 Motor 4
30. You are called to urgently assess a 54-year-old man in outpatient clinic who has
acutely deteriorated following administration of oral antibiotics. On assessment
his heart rate is 145 beats per minute, blood pressure is 74/36 mmHg and
saturations are 93% on 6 L/minute of oxygen via Hudson mask. He is wheezy and
has a generalised rash all over his body.
Which of the following would be the most appropriate pharmacological
intervention for the patient?
A
B
C
D
E
intravenous adrenaline 3 mg bolus
intravenous adrenaline 0.5 mL of 1:1000
intramuscular adrenaline 1 mL of 1:1000
intramuscular adrenaline 0.5 mL of 1:1000
intramuscular adrenaline 0.5 mL of 1:10000
Answers
Answers
1. A Lundberg A waves
An intracranial pressure (ICP) bolt is a solid, intra-parenchymal catheter containing
either a fibreoptic sensor or a micro strain gauge in its tip. It can be inserted under
local anaesthetic and extends up to 20 mm intracranially, thereby allowing the
transduction of intracranial pressure in that region of brain tissue. The value is
usually displayed as a number but can also be translated into a graphical display of
the waveform.
The ICP waveform is a reflection of the intracranial arterial pulsation and
subsequently has recognisable characteristics (Figure 2.1).
Arterial blood pressure
Figure 2.1 Intracranial pressure
and arterial pressure waveforms.
Intracranial pressure
Time
P1
P2
P3
Time
The ICP waveform has 3 identifiable peaks. The first (P1) coincides with the upstroke
of the arterial pressure trace, is a result of choroidal pulsation and is known as the
‘percussive’ wave. It is succeeded by a second ‘tidal’ wave (P2) which ends at the
point of the arterial dicrotic notch, following which, the final or ‘dicrotic’ wave occurs
(P3). The size of P2 is an inversely proportional reflection of brain compliance.
Therefore with decreased compliance its amplitude is increased such that it is more
prominent than P1 and P3 (Figure 2.2).
The waveform can also be analysed over a period of time. Lundberg described
trends in waveform analysis and ascribed the letters A, B and C to the trends as
follows.
• Lundberg A waves: Large plateau waves persisting for 5–10 minutes. These are
always pathological and warn of impending herniation
• Lundberg B waves: Fluctuations in ICP that occur with a frequency of 0.5–2
waves per minute. They are thought to be associated with ICP instability and/
51
Chapter 2
Intracranial pressure
Figure 2.2 Intracranial pressure
waveform in a non-compliant
brain
P1
P2
P3
Time
or vasospasm due to their correlation with increased flow velocity results from
middle cerebral artery transcranial doppler studies
• Lundberg C waves: Fluctuations in ICP at a frequency of 4–8 waves per minute.
These are considered normal in some patients and thought to correspond to the
respiratory and cardiac cycles (Figure 2.3)
The advantages of an ICP bolt include ease of insertion, that does not require
transfer to the operating theatre, and output that is neither altered by patient
position nor susceptible to damping. The disadvantages are that it only reflects
regional pressure changes and once inserted, cannot be recalibrated. Therefore if the
bolt has been in-situ for several days, a degree of drift must be taken into account
and subsequently they often need replacing if required for longer than 5 days.
The most acutely worrying characteristic in the above scenario would be the
presence of Lundberg A waves. Lundberg B waves would be a matter for concern
but not as pressing. A baseline value of 20 mmHg may represent the true ICP
value but at 5 days could also incorporate an element of drift in calibration. When
interpreting a flat trace the possibility of displacement or kinking of the transducer
must be considered in the first instance.
Nathanson M, Moppett I, Wiles M. Neuroanaesthesia. Oxford Specialist Handbooks in Anaesthesia, 1st Ed.
Oxford: Oxford University Press, 2011.
Pahl C. Traumatic Brain Injury: Outcome and Pathphysiology. Anaesthesia uk [Internet].2007.
Ross MJ, McLellan SJ, Andrews PJD. Depth of intraparenchymal brain monitoring devices in neurosurgical
intensive care. J Intens Care Soc 2010; 11(4):250–52.
Intracranial pressure (mmHg)
52
Figure 2.3 Intracranial pressure
waveform demonstrating
Lundberg A waves.
40
10
0
10
20
30
40
Time
(minutes)
Answers
2.E Apply pulse oximetry, blood pressure and ECG
monitoring
Seizure activity that persists without return of conscious level to baseline for 30
minutes is defined as status epilepticus and is a medical emergency. Status can
occur with any classification of seizure but the generalised form is that which is
most commonly observed. Rapid assessment and swift management is required to
minimise the complications of unremitting neuronal discharge. If status persists,
compensation in blood flow to meet increased metabolic demand begins to fail,
leading to insufficient cerebral perfusion. Cerebral tissue damage follows. Cardiac
arrhythmias, pulmonary hypertension, pulmonary oedema, global metabolic
disturbances and rhabdomyolysis may also ensue.
All of the options should be performed as soon as possible, and ideally in parallel.
National Institute for Health and Care Excellence (NICE) UK guidelines specify that
airway securement should be implemented immediately but in order to perform this
safely, it is mandatory to have standard monitoring in situ.
Gratrix AP, Enright SM. Epilepsy in anaesthesia and intensive care. Contin Educ Anaesth Crit Care Pain
2005; 5 (4): 118–21.
The National Institute for Health and Care Excellence (NICE). UK guidelines for management of convulsive
status epilepticus. London: NICE. Guideline CG137, 2012.
3.A Schedule the patient for surgery. Cease the ramipril
24 hours preoperatively. Continue the aspirin
The European Society of Cardiology (ESC) has produced guidelines and a step-wise
pathway for the assessment of cardiac patients for non-cardiac surgery. The patient
presented has stable coronary artery disease and scores 2 (for previous myocardial
infarction and proposed intraperitoneal surgery) on the revised cardiac risk index
(also known as the Lee Index). This gives an approximate risk of cardiac death or
non-fatal myocardial infarction of 2.4% (95% CI 1.3–3.5%). The factors included on
this risk index include:
•
•
•
•
•
•
History of ischaemic heart disease
History of congestive heart failure
History of cerebrovascular disease
History of diabetes requiring preoperative insulin use
Chronic kidney disease (serum creatinine > 170 μmol/L)
Undergoing major surgery (suprainguinal vascular, intraperitoneal or
intrathoracic)
The ESC guidelines for non-invasive testing (stress echo, exercise testing) use a
slightly amended version of the above risk scale (with prior myocardial infarction
being assigned a separate point) and recommend that patients with three or more
of the clinical factors listed below are referred for further assessment of myocardial
perfusion and function preoperatively.
• Angina
• Prior myocardial infarction
• Heart failure
53
54
Chapter 2
• Stroke/transient ischaemic attack
• Renal dysfunction with serum creatinine > 170 μmol/L
• Diabetes requiring insulin therapy
In patients with extensive stress-induced ischaemia, referral for coronary
revascularisation may be indicated. The method of achieving this will depend on the
potential benefit of the procedure (percutaneous coronary intervention vs coronary
artery bypass grafting) against the risk of the procedure.
Pre-operative diagnostic angiography is indicated in those patients with:
• Acute ST elevation myocardial infarction (STEMI)
• Non-STEMI (NSTEMI) and unstable angina
• Angina not controlled with medical therapy
It may also be considered in stable patients undergoing high-risk surgery. Referral
for any procedure must take into account the risk to the patient as well as the
potential benefit. In this situation, the patient is relatively low-risk and has had a
reasonably recent angiogram; it is therefore unlikely that a repeat angiography
justifies the risk.
In patients already established on beta-blockers, these should be continued
throughout the perioperative period. Although a topic of some debate, usual
practice is to omit ACE-inhibitors 24 hours before surgery due to an increased risk of
intraoperative hypotension. Aspirin should be continued unless there are concerns
regarding haemostasis during surgery (certain neurosurgical procedures, for
example).
The use of biomarkers including Brain Natriuretic Peptide (BNP) is under evaluation
and may be of some use in the risk stratification of cardiac patients.
Kristensen SD, Knuuti J, Saraste A, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular
assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment
and management of the European Society of Cardiology (ESC) and the European Society of
Anaesthesiology (ESA). Eur J Anaesthesiol 2014; 31:517-573.
4. D Postpone surgery and awaken the patient
The management of an unanticipated difficult intubation during a rapid sequence
induction can often be a challenging experience for the anaesthetist and clear
guidelines by the Difficult Airway Society have been developed to help keep
patients safe should this occur. During routine inductions, four initial intubation
attempts are allowed, however this is reduced to three in the rapid sequence
scenario. Patients receiving a rapid sequence induction have an increased risk
of regurgitation so their risk of aspirating during repeated attempts at tracheal
intubation is higher. Furthermore, the short half-life of suxamethonium will also
increase the risk of laryngospasm and difficult laryngoscopy should repeated
intubation attempts be made when neuromuscular function is recovering.
The safest action in the above scenario is to postpone surgery and awaken the
patient.
The first attempt at laryngoscopy should always be performed with the patient
in the optimum intubating position after full pre-oxygenation. If intubation is
unsuccessful, then reducing the cricoid pressure, using introducers or an alternative
Answers
laryngoscope can all improve the success rate. However these changes need to be
performed within the allocated initial three attempts.
The use of laryngeal mask airways do have a role during rapid sequence inductions,
but should only be used after a failed initial intubation plan and failed face mask
oxygenation whilst waiting for the patient to awaken. Failure of oxygenation is
defined as oxygen saturations of < 90% whilst receiving 100% oxygen.
Only in a ‘cannot intubate and cannot ventilate’ scenario with increasing hypoxemia
should a cannula or surgical cricothyroidotomy be performed (Figure 2.4).
Plan A
Initial tracheal
intubation plan
• Pre-oxygenate, apply cricoid pressure, optimise patient position, external
laryngeal manipulation by laryngoscopist.
• If poor view: reduce cricoid force, use bougie and/or alternative
laryngoscope.
• Not more than three attempts maintaining oxygenation with facemask,
cricoid pressure and anaesthesia.
FAILED INTUBATION
• Use face mask, 1 or 2 person mask technique (with oral +/– nasal airway)
to maintain oxygenation and ventilation.
• Reduce cricoid force if ventilation difficult.
Plan C
Maintain
oxygenation
and awaken
Plan D
Rescue "can't
intubate
can't ventilate"
techniques
IF FAILED FACE MASK OXYGENATION ( SpO2 < 90%, FIO2 1.0)
• LMA insertion (reduce cricoid during insertion) and attempt ventilation
FAILED VENTILATION AND OXYGENATION
• Cannula cricothyroidotomy
• Surgical cricothyroidotomy
Figure 2.4 Unanticipated difficult tracheal intubation during rapid sequence induction of anaesthesia in
the non-obstetric adult patient
Henderson J, Popat M, Latto I, Pearce A. Difficult Airway Society guidelines for management of the
unanticipated difficult intubation. Anaesthesia 2004; 59(7):675–94.
5. E Endobronchial intubation
When intubating a patient it is imperative that tube position is assessed clinically.
It is important to bear in mind that change in patient position for a procedure may
cause the endotracheal tube (ETT) to migrate. This lady’s ETT is originally placed at a
55
56
Chapter 2
depth most likely to be too great for a female patient. Extending her head probably
resulted in confirming endobronchial intubation.
Aspiration of gastric contents would most likely result in right-sided
decompensation or, in this scenario, be evident from viewing the oral cavity. She
may have plugged off her left bronchus, although her saturations are surprisingly
robust for a patient with the amount of sputum that would be present for such
an event. Bronchospasm and pneumothorax may occur independently or as a
consequence of endobronchial intubation.
Sitzwohl C, Langheinrich A, Schober A, et al. Endobronchial intubation detected by insertion depth of
endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial. BMJ
2010;341:c5943doi:10.1136/bmj.c5943.
6C Abdominal compartment syndrome may provoke a
cardiac arrest at laparotomy
The management of abdominal hypertension and compartment syndrome can
be imagined in a similar way to elevated intracranial pressure. Thus the initial
management relies on the maintenance of abdominal perfusion pressure (APP),
which is mean arterial pressure (MAP) minus intra-abdominal pressure (IAP).
Maintenance of an APP > 60 mmHg has been shown to improve outcome in a
condition with an untreated mortality otherwise approaching 100%.
Definitions and measurement
Normal IAP is in the region of 5–7 mmHg in the critical care setting, and this is
increased by presence of intra-abdominal fluid or collections, upright position, and
mechanical ventilation. Intra-abdominal hypertension is diagnosed with a pressure
persisting above 12 mmHg, and this is termed compartment syndrome when the
pressure is consistently above 20 mmHg with new organ failure.
Measurement can be direct, using an intraperitoneal needle or catheter and
transducer system, or indirect via intra-vesical, intra-gastric, intrauterine or rectal
routes. The commonest route is the bladder, which can make use of a normal Foley
catheter and gives usable results with lower risk than direct methods. The process
involves connecting a transducer to a three-way tap, which measures the pressure of
25 mL of sterile saline instilled into an empty bladder, after the catheter is clamped.
Readings should be taken at end-expiration and one minute following instillation
of the saline to allow for bladder relaxation. The patient should have a relaxed
abdominal wall, and not be coughing straining.
Systemic pathological effects
Elevated intra-abdominal pressure has wide-ranging systemic effects; high
abdominal pressure produces collapsing of the vasculature. On the venous side,
this gives rise to reductions in venous return and reduced stroke volume. Arteriolar
compression gives an increased systemic vascular resistance (SVR) and afterload.
The combined effects are those of reduced cardiac output that can rapidly spiral to
produce gut ischaemia.
Answers
Respiratory features are those of respiratory failure due to atelectasis, collapse and
shunt. There is a reduction in chest wall compliance and diaphragmatic excursion.
In ventilated patients the increased pressures required to maintain oxygenation and
ventilation can compromise cardiac output further.
Renal function is impaired as a combined result of reduced cardiac output and a
reduction in filtration gradient (FG). The filtration gradient is the pressure difference
across the glomerulus, and is therefore the difference between the perfusion
pressure and the pressure in the proximal tubule. Raised IAP compresses the
collapsible renal outflow tracts and collecting systems, such that tubular pressure
rises, thereby lowering FG. Thus a high IAP both reduces the APP and raises the
tubular pressure all of which reduce the FG required to drive filtration.
High IAPs also increase intracranial pressure (ICP). This occurs by a combination of
high intrathoracic pressure and reduced venous return, and ventilatory difficulties
and the consequences for arterial carbon dioxide tension. The combination of
pre-existing intracranial hypertension and abdominal compartment syndrome is
particularly dangerous and may mandate surgical abdominal decompression to
lower ICP.
Management
Non-surgical management is directed toward the joint aims of lowering intraabdominal pressure and maintaining APP with careful fluid resuscitation to
normovolaemia followed by vasopressor support if required. Over enthusiastic fluid
therapy may contribute to gut oedema and further compromise tissue perfusion.
Pressure in the abdomen may be lowered by reducing the volumes of the contents,
with nasogastric tubes, endoscopic evacuation or invasive drainage of gas or fluid.
In addition, in the ventilated patient consideration can be given to optimal sedation
and muscle relaxation to reduce straining and asynchrony.
Surgical management involves laparotomy and decompression. The abdomen
is then left open and covered with a temporary closure of a Bogota bag or
vacuum dressing. It remains important to measure abdominal pressure even after
decompression, as 25% of patients with a Bogota bag go on to develop secondary
hypertension. Serious caution should be exercised at laparotomy for raised IAP as
profound haemodynamic instability may ensue as a consequence of abdominal
reperfusion alongside a sudden fall in SVR. This can be massive and of sufficient
magnitude to bring about cardiac arrest.
As described above, indirect methods of measurement reduce the risks of
complications associated with needle or catheter techniques. Measurement
takes place at the end of expiration. A pressure of 24 mmHg is more than double
the cut-off for hypertension, and within the range of compartment syndrome, if
sustained. Management strategies are discussed above, with non-surgical options
also available. Laparotomy is indeed a risk factor for cardiac arrest given the massive
physiological changes that occur in this situation.
Berry N, Fletcher S. Abdominal compartment syndrome. Contin Educ Anaesth Crit Care Pain 2012; 12
(3):110–116.
57
58
Chapter 2
7. C Flattening of both the inspiratory and expiratory limbs
A flow-volume loop is a plot of flow rate (y-axis) against lung volume (x-axis) during
maximal forced inspiration and expiration. The contour of this loop can aid in
localising upper airway obstructions and assessing their functional impact.
Upper airway obstructions are classified as either intrathoracic or extrathoracic
depending on whether they are present within or outside the thoracic inlet
respectively. In addition, they are also described as either variable or fixed
depending on whether the airway lesion calibre changes during the respiratory
cycle.
For variable extrathoracic obstructions (such as vocal cord paralysis), the flow
volume loop classically displays a flattened inspiratory and normal expiratory limb.
This is because during inspiration, the transmural pressure is negative as a result of
a subatmospheric intraluminal pressure and an atmospheric extraluminal pressure.
Consequently, the extrathoracic portion of the upper airway will have a tendency
to collapse during inspiration resulting in reduced airflow in the presence of an
obstructing lesion. During expiration, the intraluminal pressure surpasses the
pressure surrounding the airway thus reducing the obstruction.
Flow volume loops in the presence of variable intrathoracic obstructions (such as
bronchogenic cysts) classically display a flattened expiratory and normal inspiratory
limb. Flow limitation is encountered during expiration because at this phase of the
respiratory cycle, the pleural pressures exceed the airway pressures exacerbating
the obstruction. During inspiration, the pleural pressures are negative relative to the
intrathoracic airways thereby creating no restriction to airflow.
Fixed upper airway obstructions are characterised by a constant degree of
airflow limitation during the whole respiratory cycle as they limit the influence of
transmural pressures on airway diameter. They can be extrathoracic (large goitres) or
intrathoracic (large tracheal tumours) and their flow loops display flattening of both
the inspiratory and expiratory limbs. The above case is an example of a fixed airway
obstruction.
A saw-tooth pattern describes small oscillations which can be observed
throughout the inspiratory and expiratory limbs of the flow volume loops
as a consequence of either equipment artifact, neuromuscular disease or
pedunculated tumours (Figure 2.5).
Answers
Normal flow – volume loop
Inspiration Expiration
(L/min)
(L/min)
Flow
Extrathoracic variable
obstruction
Inspiration Expiration
(L/min)
(L/min)
Flow
+
+
+
+
Volume
Intrathoracic variable
obstruction
Intrathoracic fixed
obstruction
Extrathoracic fixed
obstruction
+
+
+
+
+
+
+
+
+
+
+
+
–
–
–
–
–
–
–
–
–
–
–
–
Volume
–
–
–
–
Figure 2.5 Flow-volume loops with different configurations of extrathoracic and intrathoracic
obstructions.
Nethercott D, Strang T, Krysiak P. Airway stents: anaesthetic implications. Contin Educ Anaesth Crit Care
Pain 2010; 10(2):53–8.
Rendleman N. Quinn S. The answer is blowing in the wind: a pedunculated tumour with saw tooth flowvolume loop. J Laryngol Otol 1998; 112(10):973–5.
8. C Vasopressin
Brainstem herniation causes relative hypotension and bradycardia after an initial
period of hypertension due to catecholamine release. This is due to loss of autonomic
control of vasomotor tone and loss of vagal tone. Treating episodes of hypotension
with adrenergic vasoactive drugs exacerbates end-organ ischaemia and they are
contraindicated in a potential organ donor. Vasopressin is the agent of choice to
treat hypotension and maintain vascular tone following brainstem herniation as it
improves organ perfusion and corrects the polyuric component of diabetes insipidus
caused by hypothalamic ischaemia. Fluid boluses are useful to maintain euvolaemia,
but over filling patients also risks detrimental outcomes to organs.
Gordon JK. Physiological changes after brain stem death and management of heart-beating donor. Contin
Educ Anaesth Crit Care Pain 2012; 12(5):225–29.
59
60
Chapter 2
9. A An arterial blood gas analysis
Fat embolism indicates the presence of fat within the pulmonary or peripheral
circulation, often without symptoms. Fat embolism syndrome is the clinical
consequences of fat embolism occurring in some patients and has a quoted
mortality of between 5–15%. The commonest implicated fractures are the closed
fractures of the long bones and pelvis. The greater the number of fractures, the
higher the incidence. A third of patients with bilateral femoral fractures go on to
develop the syndrome.
Presentation and diagnosis
The syndrome most often presents at 1–3 days. There are a variety of sets of
published diagnostic criteria, but all have in common either an arterial blood gas
(ABG) or clinical features of profound type I respiratory failure. Clinically, the two
other major tenets are neurological dysfunction, most commonly acute confusion,
and the classical petechial rash. The rash may be a late sign and only present in 60%
of cases.
Blood indices most often reflect a marked anaemia with thrombocytopenia. Other
features such as fat in sputum, urine and alveolar macrophages may support the
diagnosis, but equally do not correlate well with the severity of the syndrome.
Pathophysiology
Two main theories exist. In the mechanical theory, physical disruption forces adipose
marrow into the venous system and bones with high marrow content are indeed
most associated with the syndrome. However, studies have directly demonstrated
embolic load in patients during orthopaedic surgery who have not progressed to
develop the clinical syndrome. The mechanical theory also does not explain why,
despite the fact that embolism is greatest around the time of injury, occurrence of
the syndrome peaks at 24–72 hours.
The biochemical theory ascribes toxicity to the hydrolytic degradation of neutral
marrow fat to free fatty acids. These free acids are shown to be able to induce acute
lung injury in animal models. C-reactive protein may also have a role in abnormal
lipid metabolism in these patients.
Treatment
The treatment is essentially supportive with good oxygenation and ventilation in an
intensive care environment if indicated. Correction of blood indices may be needed.
Prevention is with operative fixation after early immobilisation, and some operative
techniques exist to reduce intraosseous pressure during drilling or reaming to
reduce the embolic load.
Some advocate steroid prophylaxis with methylprednisolone for those patients at
highest risk, with some evidence to support this. There is no evidence to support the
use of steroids as a treatment however. Aspirin may speed recovery of platelets and
possibly lung injury.
In this question, the stem highlights the diagnosis of fat embolism syndrome, which
most candidates are likely to discern. The real question relates to the most helpful test,
Answers
in both diagnosis and treatment, which requires a more extensive understanding of
the disease. Special investigations which have been used to assist in the diagnosis do
include bronchoscopic alveolar lavage (BAL) for lipid-laden macrophages, and urine
microscopy for lipid, but may not add much over clinical examination particularly
given that the patient presents with the tell-tale petechial rash. CT and CXR findings
may be variable, and unlike in prevention, there is no beneficial role for steroids in
treatment. The ABG will, however both assist in diagnosis (Pao2 is in all diagnostic
criteria) and help the clinician decide on level of respiratory support required.
Gupta A, Reilly CS. Fat embolism. Contin Educ Anaesth Crit Care Pain 2007; 7(5):148–51.
Khanna G, Cernovsky J. Bone cement and the Implications for anaesthesia. Contin Educ Anaesth Crit Care
Pain 2012; 12(4): 213–16.
10. B Linear array probe
The use of ultrasound is well established in regional anesthesia and pain medicine.
Ultrasound guided nerve blocks offer potential benefits over landmark technique
including reduced complications and increased success rates.
The diagnostic ultrasound in current medical practice is usually in the range of 1–20
megahertz (mHz).
The ultrasound probe contains a large number of transducers in the form of
piezoelectric crystals. The piezoelectric transducer converts an electrical charge into
an ultrasound wave. The produced ultrasound wave then propagates into the tissues
and is either scattered or reflected back onto the probe. The reflected wave the
piezoelectric crystal again, creating an electrical signal that can be processed and
interpreted by the ultrasound machine to produce an image.
The probe transducers are activated in turn so that the probe is always discharging
or receiving signals when operating. Ultrasound probes may have different shapes:
Linear array probes: High frequency (6–13 MHz) probes where the piezoelectric
crystals are arranged in a line along the surface. They provide the best axial
resolution, however the higher the frequency the more attenuation therefore these
probes have poor penetration. A rectangular ultrasound image is produced and they
are best used for performing superficial blocks like interscalene, supraclavicular and
axillary blocks.
Curved array probes: Low frequency (2–5 MHz) probes where the crystals are
arranged along a curved surface. They provide lower resolution images when
compared with linear probes. However, they have better penetration and allow
visualisation of deeper structures. Curved array probes are best used for performing
deep blocks such as sciatic nerve and infraclavicular brachial plexus blocks. These
probes produce wide sector-shaped images with a curved upper and lower edge.
Phased array probes: Piezoelectric crystals are fired in phases to produce a sectorshaped image on the monitor with an expanding field of view. These probes are
mainly used for echocardiography.
Hockey stick footprint probes: Also called J-shaped probes. These are a type of
linear array transducer that are small in size and therefore ideally used in areas where
space is limited or in paediatric patients.
61
62
Chapter 2
As mentioned, higher frequency linear probes are better for more superficial blocks and
lower frequency curved probes are better for deeper blocks. Thus in this clinical scenario,
the most appropriate ultrasound transducer is the linear high frequency probe.
Carty S, Nicholls B. Ultrasound-guided regional anaesthesia. Contin Educ Anaesth Crit Care Pain 2007; 7(1):
20-24.
Marhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia. Br J Anaesth 2005; 94(1): 7–17.
11. C No fluid bolus
This patient has sustained a penetrating abdominal trauma and displays signs of at
least class 2 haemorrhagic shock according to ATLS guidelines (see Table 2.3). Initial
fluid resuscitation uses the principle of permissive hypotension with the emphasis
on early surgery in order to stop the bleeding. The debate regarding choice of fluids
rages on, but the definitive management of these patients is crucial. It is therefore
currently accepted that the optimal intervention is to refrain from fluid boluses as
long as the patient is conscious and thus perfusing his vital organs. Insertion of an
arterial line is not part of the initial resuscitation, but may be required once operative
management is to be undertaken. Conservative treatment and observation might
be appropriate in certain abdominal injuries, but in a haemodynamically unstable
patient early surgery is indicated.
Table 2.3 Classes of haemorrhagic shock according to ATLS guidelines
Class 1
Class 2
Class 3
Class 4
% Blood loss
< 15%
15–30%
30–40%
> 40%
Respiratory rate
(breaths per
minute)
14–20
20–30
30–40
> 35
Heart rate (beats
per minute)
< 100
> 100
> 120
> 140
Blood pressure
Normal
Normal
Decreased
Decreased
Pulse pressure
Normal or increased
Decreased
Decreased
Decreased
Mental status
Slightly anxious
Mildly anxious
Anxious, confused
Confused,
lethargic
Dutton R. Fluid management for trauma: where are we now? Cont Educ Anaesth Crit Care Pain 2006;
6(4):166–67.
12. A Immediate transfer to neurosurgical theatre for an
extra-ventricular drain (EVD)
The normal intracranial pressure (ICP) in the horizontal position is 7–10 mmHg and
the normal waveform mirrors the arterial trace but consists of three peaks (P1-3),
which reflect cardiac contraction, brain compliance (the pressure wave reflected
from the rigid skull) and aortic valve closure respectively (Figure 2.6).
Answers
Figure 2.6 The intracranial
pressure waveform in a normal
brain and a non-compliant
brain with increased intracranial
pressure.
P2
P1
Pressure (mmHg)
40
P1
20
0
P2
P3
Non-compliant brain
tissue result in a
decreased P1
P3
(Increased intracranial
pressure)
(Normal)
1
Time (second)
2
3
An ICP > 15 mmHg is considered pathological, and in head injured patients,
levels > 20 mmHg are usually treated. The Brain Trauma Foundation publishes
clinical guidelines regarding ICP monitoring and actively managing intracranial
hypertension is associated with improved survival.
This patient should initially be managed with an ABC approach, controlling the
airway, ventilating appropriately to maintain Pao2> 10 kPa and PaCO2 at around
4.5 kPa while maintaining mean arterial blood pressure to optimise cerebral
perfusion pressure (CPP). Other key interventions include ensuring cerebral venous
drainage (by avoiding internal jugular vein central lines, endotracheal tube ties and
maintaining a 30° head-up position), ensure normoglycaemia, normothermia and
avoiding seizure activity.
The important information given to you in the vignette is that she presented to a
teaching hospital (which you may assume has neurosurgical services). Therefore
it suggests that the first 3 options may be most appropriate. The others may be
important if you are awaiting transfer to a neurosurgical centre. In this case a large
subarachnoid haemorrhage (SAH) with dilated ventricles and sluggish pupillary
response to light is suggestive of obstructive hydrocephalus. Thus the intracranial
pressure may be assumed to be high and will only increase without intervention.
As you are assuming there is a neurosurgical service in the teaching hospital, your
answer will recommend involving the neurosurgeon as soon as possible. Intracranial
monitoring will allow you to titrate the therapies to a measured end-point, which
reduces mortality. The options are:
• Extra-ventricular drain (EVD): this is the gold standard, which involves a drain
placed directly into the lateral ventricles via the frontal lobe and is therefore
the most invasive. It allows monitoring of the ICP and waveform morphology,
therapeutic draining of CSF to reduce the ICP and administration of intra-thecal
drugs if required. The complications include bleeding into the frontal lobe and
infection (rate 1–5%). Blockage may occur necessitating a revision.
• Intra-parenchymal monitors are almost as accurate with lower complication rates.
However no therapeutic interventions can be performed with it.
63
64
Chapter 2
• The sub-dural bolt is least invasive, has the least complications but is also the least
accurate and is used for monitoring only, not therapeutic intervention.
Hyper-osmotic treatments are most useful for management of space-occupying
mass lesions including an intra cranial blood clot. It may also be used as a rescue
measure in this scenario to buy time if there is clinical evidence of impending
cerebral herniation. Phenytoin is usually administered after the second witnessed
seizure. Nimodipine should be given as early as possible via a nasogastric tube to
prevent vasospasm.
Therefore the most important intervention is inserting a device for monitoring and
intervention, which allows you to optimise the medical management appropriately.
Management of the aneurysm is undertaken once the ICP has been controlled
and the aneurysm is secured, forced hypertensive treatment can begin to prevent
cerebral infarction related to vasospasm. The other measures may be used to buy
time prior to an EVD insertion if it is not immediately available.
Pattinson K, Wynne-Jones G, Imray CHE. Monitoring intracranial pressure, perfusion and metabolism.
Contin Educ Anaesth Crit Care Pain 2005; 5(4):130–33.
Brain Trauma Foundation. Guidelines for the Management of Severe Traumatic Brain Injury. New York:
Brain Trauma Foundation, 2007; S45–65.
13. E 30 mL/kg crystalloid bolus
Sepsis is the commonest reason for a patient to be admitted to a critical care unit
and therefore the 2012 Surviving Sepsis Guidelines is essential revision. The bundle
of care now mandates:
To be completed within 3 hours
1.
2.
3.
4.
Measure lactate level
Obtain blood cultures prior to administration of antibiotics
Administer broad-spectrum antibiotics
Administer 30 mL/kg crystalloid for hypotension or lactate ≥4 mmol/L
To be completed within 6 hours
5. Apply vasopressors (for hypotension that does not respond to initial fluid
resuscitation) to maintain a mean arterial pressure (MAP) ≥ 65 mmHg
6. In the event of persistent arterial hypotension despite volume resuscitation
(septic shock) or initial lactate ≥ 4 mmol/L (36 mg/dL):
• Measure central venous pressure (CVP)
• Measure central venous oxygen saturation (Scv–o2)
7. Re-measure lactate if initial lactate was elevated
This patient has recently been admitted to the emergency department with severe
sepsis probably secondary to pneumonia, though the current history is inadequate
to exclude other causes. He has had antibiotics within one hour following blood
cultures. This is optimal care as for each hour delay in antibiotic administration there
is a 7.6% increase in mortality from sepsis.
This patient has distributive shock based on cardiovascular parameters and a raised
lactate, therefore immediate fluid resuscitation should be commenced as per the
Answers
Surviving Sepsis Guidelines above. 30 mL/kg should be given in the next two hours.
If hypotension persists despite this fluid resuscitation, then noradrenaline should be
–o , MAP and CVP. The lactate level should be re-evaluated.
considered titrated to Scv
2
This patient has evidence of a raised alveolar-arterial gradient representing a
probable diffusion defect and ventilation/perfusion mismatch with shunting.
However clinically his predominant problem is hypoperfusion and shock so should
be fluid resuscitated in the first instance. Currently he does not have an indication for
non-invasive ventilation (NIV) or intubation and ventilation.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: International guidelines for
management of severe sepsis and septic shock. Crit Care Med 2013;41:580–637.
14. B Increase the insulin infusion by 1 unit/hour if the
bicarbonate concentration remains 3 mmol/L after 1 hour
Diabetic ketoacidosis (DKA) is an endocrine emergency that presents in diabetic
patients who do not produce endogenous insulin. Relative or absolute lack of insulin
(endogenous or exogenous) results in a triad of hyperglycaemia, a ketotic state and
acidaemia. Eleven percent of Type 1 diabetics presented with DKA in 2004–2009.
Mortality is still 2%, most commonly attributable to cerebral oedema.
Glucose forces renal diuresis and results in profound hypovolaemia. The patient
presents with a metabolic acidosis (often partially compensated by a monumental
minute ventilation) with a large anion gap due to unmeasured blood ketones.
Blood ketones can now be measured at the bedside and indicate severity of disease
and response to treatment. The patient is often potassium-deplete which may not
be immediately obvious from initial lab results as a high level of acidosis causes
intracellular potassium ions to migrate into the plasma. As acidosis resolves and
potassium once again returns to the intracellular space, the plasma potassium
concentration decreases rapidly.
Management of DKA in critical care areas focuses on the following issues:
• Fluid management including resuscitation and replacement of ongoing losses
• Blood glucose control and providing glucose once the blood glucose drops below
15 mmol/L
• Acidosis and electrolyte management (in particular potassium maintained
between 4 and 5 mmol/L)
• Insulin administration and titration
• Septic screening and appropriate antibiotics
• Thromboprophylaxis
• Monitoring for complications including cerebral oedema, sepsis, hypokalaemia,
ischaemic cardiac events, acute kidney injury (AKI) and acute respiratory distress
syndrome
• Management of psycho-social issues
• Involving of specialist teams for ongoing management
The management of DKA has undergone a recent change in 2011 and guidelines
have been published by Diabetes UK. The sliding scale is no longer incorporated and
titrating insulin to biochemical markers is the primary objective. To summarise some
of the new recommendations:
65
66
Chapter 2
A ‘fixed rate’ infusion of 0.1 units/kg insulin should be administered. The rate is no
longer adjusted solely according to blood sugar levels, but to blood ketone levels or
bicarbonate levels. Aims of treatment are:
• A reduction of 0.5 mmol/L/hour blood ketone concentration
• An increase of 3 mmol/L/hour of venous bicarbonate concentration
• A reduction of 3 mmol/L/hour of blood glucose concentration
If this is being met then the current insulin infusion is to be unaltered regardless
of current blood glucose levels. If treatment goals are not being met the infusion
should be increased by 1 unit/hour.
1. DKA protocol should be terminated once pH> 7.3, venous plasma bicarbonate
above 18 mmol/L and blood ketones < 0.3 mmol/L
2. If the patient is on long-acting insulin this should be continued simultaneously.
In the above clinical scenario, answer B is the most appropriate option that follows
the suggested guidelines. The other options are also viable, but:
• Option A is following the ‘old’ sliding scale regime, which is used on ICUs for
diabetics and non-diabetics alike (the difference between these groups should be
distinguished as the pathology and resulting disease is very different);
• Option C may be performed if you wanted to add potassium but that may not be
needed yet;
• Option D is possible but the patient is not hypotensive and lactate is not
significantly raised;
• Option E may be indicated in shock unresponsive to inotropes or if the metabolic
acidosis is in part caused by AKI, however administrating intravenous bicarbonate
masks one of the biological markers of treatment responsiveness.
It is important to be aware of new guidelines and understand the difference
between managing DKA (providing insulin and glucose to reduce ketosis) and
maintaining normoglyaemia in unwell-adults due to a hormonal stress response.
Savage MW, Dhatariya KK, Kilvert A, et al. Guideline for the management of diabetic ketoacidosis. Joint
British Diabetes Societies. Diabet Med 2011; 28:508–15.
15. C IAP > 20 mmHg with new organ dysfunction
This elderly patient is at high risk of developing intra-abdominal complications
following a complex laparotomy. Monitoring her intra-abdominal pressure (IAP)
provides additional information to her clinical status.
IAP can be measured using direct or indirect methods. A direct method would be to
leave a catheter or needle within the abdomen at the end of the laparotomy.
Indirect methods are the commonest measurement technique in the UK. This
involves the intravesical method via a bladder catheter; working on the principle
that intravesical pressure is a surrogate for intra-abdominal pressure. One technique
involves introducing sterile saline into the bladder and clamping the catheter
distally. A wide bore needle or cannula is introduced into the bladder catheter via
the culture port and connected to a pressure transduction system. The system
is zeroed at the level of the symphysis pubis. In order to provide an accurate
Answers
measurement, the reading should be taken in the supine patient at the end of
expiration. The measurement should be repeated four hourly.
Normal IAP is 5–7 mmHg. The World Society of the Abdominal Compartment
Syndrome (WSACS) classifies intra-abdominal hypertension as a sustained IAP
> 12 mmHg. Abdominal compartment syndrome is a sustained IAP > 20 mmHg with
new organ dysfunction, hence making option C correct.
Risk factors can be subdivided into:
• Intraluminal such as gastroparesis, ileus or pseudo-obstruction
• Extraluminal such as ascites or pelvic tumours
• Decreased abdominal wall compliance such as abdominal surgery with fascial
closure, obesity, abdominal burns or trauma
• Capillary leak or excessive fluid resuscitation such as pancreatitis, sepsis or
massive transfusion
This patient is at high risk due to the risk of ileus, risk of capillary leak from a
systemic inflammatory response syndrome and reduced abdominal wall compliance
following a laparotomy.
The principle of management is to optimise abdominal perfusion pressure. The
strategies used broadly fall into medical and surgical categories.
Medical management involves:
• IAP monitoring if risk factors are present
• Draining abdominal fluid collections such as ascites or abscesses
• Reducing intraluminal contents; nasogastric and rectal decompression and the
cautious use of prokinetics
• Improving abdominal wall compliance such as sedation and analgesia with
possible neuromuscular blockade and removal of constrictive dressings or
escharotomy
• Maintain oxygen delivery with the use of fluid challenges and cardiovascular
support. Excessive fluid administration should be avoided and diuretics may have
a role
The main surgical option is decompression via a laparostomy with delayed closure.
Close liaison with the surgical team is mandated in the management of high-risk
patients, such as this case, and thresholds ascertained which alert the teams to
consider a surgical option.
Berry N, Fletcher S. Abdominal compartment syndrome. Contin Educ Anaesth Crit Care Pain 2012;
12(3):110–117.
16. D Responding to voice on the AVPU score
Asthma is characterised by reversible airways obstruction due to bronchial smooth
muscle contraction, airway inflammation and increased airway secretion production.
Chronic management focuses on a step-wise approach to therapy escalation aiming
for minimal requirement for rescue therapy. Around 1400 people a year still die from
asthma despite improvements in chronic management.
67
68
Chapter 2
Table 2.4 Characteristics of asthma severity
Characteristic
Acute severe
Life threatening
Near fatal
Peak Flow (% best)
33–50%
< 33%
Unable
Sentences
Cannot complete
1–2 words
Nil
Respiratory rate (/min)
> 25
< 10
Requires ventilation
Pao2
> 8 kPa
< 8 kPa
< 8 kPa
Spo2
> 92%
< 92%
< 92%
Paco2
Low
Normal
High
Chest sounds
Wheeze
Silent chest
No ventilation
Consciousness
Alert
Somnolence
Unconsciousness
The definition of the severity of an acute attack can be summarised below (Table 2.4):
The first decision as the anesthetist or intensivist is which category your patient
falls into as this dictates immediate management. The time delay from decision-tointubate to actually intubating with all the drugs, equipment and help you need may
be significant and thus it is best to prepare early.
The next decision is whether the patient is on optimum therapy, which for lifethreatening asthma should be:
• Oxygen-driven salbutamol nebulisers 5 mg continuously (allocate someone to
monitor and change over the nebuliser when finished). Its worth noting however
if there is little respiratory effort the inhaled drug will just move in and out of
conducting airways and not reach the desired site of action
• Magnesium 2 g intravenous infusion over 20 minutes
• Steroid therapy: either oral prednisolone 40 mg or hydrocortisone 200 mg
intravenous
• Intravenous fluids as the patient may become profoundly dehydrated with
a sustained high respiratory rate being treated with non-humidified oxygen
therapy
• Salbutamol infusion 5–20 μg/min titrated to effect
• Aminophylline 5 mg/kg loading dose over 20 minutes (if not on oral theophylline)
followed by 0.5 mg/kg/min
• Adrenaline infusion is an option but the patient is more likely to require an
anaesthetic before this stage is reached
In the case above the most concerning feature is the drowsiness. Patients with
asthma have a high adrenergic response (otherwise known as fear) and should
be alert. You are not told what treatment the patient is on already. A pH of 7.32 is
worrying if it is a respiratory acidosis but both dehydration and salbutamol therapy
can cause metabolic acidosis, which if being appropriately compensated for, is less
worrying. Similarly this patient should be on oxygen as part of their treatment and
Answers
their oxygen saturations should be judged when receiving appropriate therapy. It
is helpful to quantify the ability to speak with the number of words used: obviously
unable to utter one word is more worrying than reciting the daily adventures of
one’s cat and pausing for breath. Response to treatment is important and if no
improvement is being made, a decision to ‘electively’ intubate may be made.
It is therefore crucial to look at the complete clinical picture and use good judgment
in the management of acute asthma. Alteration in consciousness is an ominous sign
and should be treated very seriously.
D Stanley, W Tunnicliffe. Management of life-threatening asthma in adults. Contin Educ Anaesth Crit Care
Pain 2008; 8(3):95–99.
British Thoracic Society (BTS)/SIGN. Guideline on the management of asthma. London: British Thoracic
Society, 2012.
17. A 5 IU Syntocinon IV
This woman is on her way to a post partum haemorrhage (PPH), which is the loss of
500 ml blood after vaginal delivery or 1000 mL after Caesarean section. She requires
urgent control of the bleeding. In this case the cause is an atonic uterus, hence
uterotonics are needed.
A further dose of syntocinon is the ideal choice in this situation. It is a synthetic
oxytocin analogue that acts on oxytocin receptors in the uterus to increase uterine
contractions. Its side effects include hypotension, fluid retention and tachycardia.
For these reasons it should be given slowly, and some advocate diluting prior to
administration, especially in pre-eclamptic patients.
Ergometrine is an ergot alkaloid that acts on serotonergic receptors in the uterus.
Syntometrine contains 5IU of syntocinon and 500 µg of ergometrine. Although the
syntocinon would help in this situation, this lady is pre-eclamptic and there is a risk
the ergometrine could exacerbate hypertension. Other side effects of ergometrine
include, nausea and vomiting.
Carboprost is a prostaglandin F2α analogue and also stimulates uterine contractions.
Side effects include hypotension, diarrhoea, nausea and bronchospasm; hence, it is
avoided in asthmatic patients.
Misoprostol is a prostaglandin E1 analogue that is usually given rectally. Although
it can also be given orally and by direct myometrial injection, the rectal route has
fewer side effects. In this case, the operation is still ongoing and rectal misoprostol,
even if given intraoperatively, will take a while to work. It can be used at the end of
the procedure. Its side effects include nausea, vomiting, diarrhoea and pyrexia.
Atosiban is a tocolytic drug that antagonises oxytocin at its uterine receptors. It is
used in preterm labour and has no application in this situation.
Al-Foudri H, Kevelighan E, Catling S. CEMACH 2003–5 saving mothers’ lives: lessons for anaesthetists.
Contin Educ Anaesth Crit Care Pain 2010; 10(3): 81–87.
69
70
Chapter 2
18. B Proceed immediately with surgery under general
anaesthesia following a rapid sequence induction and
intubation
The gastric volume in an injured patient is related to the interval between the
last meal and the time of injury. Thus, this injured child should be considered as
a patient with a full stomach. In addition, opioids further decrease gastric transit.
A routine induction of general anaesthesia is not appropriate in a child with a full
stomach. There is insufficient evidence to conclude that prolonging fasting time
pre-procedure decreases the incidence of adverse outcomes, therefore there is little
benefit in delaying surgery. Performing an axillary block is a reasonable option, but
would not be feasible in a 6-year old child without sedation or general anaesthesia.
Thus immediate surgery under general anaesthesia is the most appropriate
anaesthetic management in this clinical scenario.
Smith I, Kranke P, Murat I, et al. Perioperative Fasting in Adults and Children: Guidelines from the European
Society of Anaesthesiology. Eur J Anaesthesiol 2011; 28(8):556–69.
19. D Morphine 50 μg/kg intravenous bolus for analgesia
Postoperative pain and emergence delirium (ED) present similarly and may
overlap. ED is more likely to occur in children between 2 and 5 years of age,
patients undergoing painful procedures under volatile anaesthetics and after a
rapid emergence. Co-induction with fentanyl or midazolam reduces the risk of ED.
Midazolam and propofol can be used to treat ED.
Pain as a cause of this patient’s distress should be considered first and most likely,
particularly since the patient’s main complain was pain. The patient’s tachycardia
and hypertension are consistent with pain, not hypovalaemia. Starting a morphine
infusion without a loading dose would take several hours for plasma levels to reach
a therapeutic concentration. Therefore, a morphine intravenous bolus is the most
appropriate management in this case, and may be repeated and titrated to effect.
Reduque LL, Verghese ST. Paediatric emergency delirium. Contin Educ Anaesth Crit Care Pain 2012;
13:39–41.
Haidon J, Cunliffe M. Analgesia for neonates. Contin Educ Anaesth Crit Care Pain 2010; 10:123–27.
20. A Announce cardiac arrest, call for help, and start chest
compressions
This is a pulseless ventricular tachycardia (VT) cardiac arrest. The immediate first
action should be to call for help and start chest compressions. As per paediatric
life support guidelines, pulseless VT is a shockable rhythm, and 4 J/kg of DC shock
should be delivered as soon as the cardiac defibrillator is available and set up, and
epinephrine given as soon as available. The most likely cause of the cardiac arrest in
this patient is local anaesthetic toxicity.
The young infant is at increased risk of amide local anaesthetic toxicity. The usual
early warning signs and symptoms are not exhibited, and the first sign of toxicity
may be a grand mal convulsion, apnoea or arrhythmia. Raised cerebral blood flow
Answers
will increase delivery of local anaesthetic to the brain. The blood–brain barrier is not
well developed in the neonate while decreased plasma protein binding and reduced
hepatic clearance result in increased free drug availability.
Treatment of local anaesthetic toxicity should include cessation of drug
administration, measures to ensure a clear airway, artificial ventilation with oxygen
100%, external cardiac massage if necessary, and administration of 20% lipid
emulsion (Intralipid). Intralipid is an emulsion in water of soybean oil, predominantly
neutral triglycerides, made isotonic with glycerin. In blood, these fat droplets form a
lipid compartment, separate from the plasma aqueous phase, into which a lipophilic
substance such as bupivacaine might dissolve.
The Association of Anaesthetists of Great Britain and Ireland (AAGBI). Safety Guideline, Management of
Severe Local Anaesthetic Toxicity, London: AAGBI, 2010.
Resuscitation Council UK. Paediatric Advanced Life Support. London: Resuscitation Council (UK), 2010.
Patil K. Use of intralipid for local anesthetic toxicity in neonates. Paediatric Anaesthesia, 2011; 21 :1268–69.
21. C The visual analogue scale (VAS) can be used in patients
aged 12 years and above
There are a number of pain assessment systems that can be applied to paediatric
patients. The FLACC (Face, Legs, Arms, Cry, Consolability) scale is for children aged 1
year and above but it can be occasionally be used from 2 months (Table 2.5). Each
of the five criteria can have a score between 0 and 2, with a maximum score of 10. A
score of 0 represents no pain.
Self-reporting is suitable for over 5 years of age but this is not always exact and some
authors recommend 7 as the starting point. It is the most accurate assessment when
correctly used.
The visual analogue scale (VAS) can be use in patients aged 8 years and above but it
is recommended for patients over 12 years of age as it is more reliable.
Table 2.5 The FLACC scale
Criteria
Score 0
Score 1
Score 2
Face
No particular expression or smile
Occasional grimace or frown,
withdrawn, uninterested
Frequent to constant
quivering chin, clenched
jaw
Legs
Normal position or
relaxed
Uneasy, restless, tense
Kicking or legs drawn up
Activity
Lying quietly, normal
position, moves easily
Squirming, shifting, back and
forth, tense
Arched, rigid or jerking
Cry
No cry (awake or
asleep)
Moans or whimpers; occasional
complaint
Crying steadily, screams
or sobs, frequent complaints
Content, relaxed
Reassured by occasional touching, hugging or being talked to,
distractible
Difficult to console or
comfort
Consolability
71
72
Chapter 2
Although physiological markers have been used in some pain scales its use is always
in the context of other signs, thus isolated physiological markers are inaccurate and
not recommended for use for pain assessment.
The Wong-Baker FACES pain rating scale is comprises 6 hand drawn faces ranging
from a happy face (0) to a crying face (10) that represent pain intensity. A change of
one face at a time is considered clinically significant.
Bandstra NF, Chambers CT. Pain assessment in children. In: Brevik H, Campbell W, Nicholas MK (eds)
Clinical Pain Management Practice and Procedures, 2nd edn. London: Hodder Arnold, 2008: 447–461.
22. A Fascia Iliaca block
Hip fractures are extremely painful. Typically, pain may be constant, or only on
moving the joint, and this can limit the care that these patients receive on the
ward, such as restricting nursing care, or transferring from trolley to bed. In the
postoperative period, persistent pain may delay mobility and recovery, leading to a
prolonged hospital stay, and increased risk of complications.
Analgesia should be administered as soon as possible after the patient presents
to hospital, and initially this may be with a dose of opioid. However, use of opioids
and non-steroidal anti-inflammatory drugs (NSAIDs) should be minimised where
possible in this cohort of patients. Opioids increase the risk of postoperative
confusion, and many patients who present with femoral neck fractures have
comorbidities including renal impairment. This can lead to opioid accumulation and
toxicity. NSAIDs increase the risk of further renal impairment.
Regular paracetamol is safe and very effective when used in combination with other
analgesics. The addition to regional anaesthesia has been demonstrated to reduce
opioid requirements. Increasingly, simple nerve blocks can be administered in the
emergency department by trained staff, and this can improve the entire patient
experience, with less pain on transferring and moving, and reduced requirement for
sedative analgesia.
Adequate blockade of the femoral nerve, obturator nerve, and the lateral cutaneous
nerve of the thigh would be sufficient for preoperative, intraoperative as well as
postoperative analgesia. A fascia iliaca block can achieve this.
In this scenario, the patient is known to have chronic kidney disease (CKD), dementia
and is confused. This should defer your choice away from NSAIDs and opioids.
Answers
The choice between the blocks should lead you to choose the fascia iliac block. A
femoral nerve block would not anaesthetise the lateral cutaneous nerve of the thigh,
which supplies sensation to the incision site. Additionally, a spinal anaesthetic has
not been shown to provide longer lasting analgesia than a peripheral nerve block.
Many would therefore advocate performing a spinal anaesthetic for intraoperative
management, as well as a fascia iliaca block for postoperative analgesia.
Maxwell L, White S. Anaesthetic management of patients with hip fractures: an update. Cont Educ
Anaesth Crit Care Pain 2013; 13(5):179–183.
Scottish Intercollegiate Guidelines Network (SIGN). Management of hip fracture in older people. National
CG No. 111. Edinburgh: Scottish Intercollegiate Guidelines Network, 2009.
23. D Gabapentin
‘Shingles’, also known as herpes zoster, is caused by reactivation of the varicella
zoster virus (VZV), a virus in the same family as the herpes simplex virus
(Alphaherpesvirinae). Herpes zoster and herpes simplex are, however, independent
diseases. After causing its primary infection (chickenpox) the VZV lies dormant in
a sensory ganglion, until it is given such conditions when it can re-emerge. The
clinical manifestation of this re-emergence is called shingles. The most common
cause is immunosuppression, which may be due to malignancy, acquired syndromes
including HIV, or immunosuppressive medication such as steroids.
On reactivation, VZV causes pain and a characteristic rash, limited to the dermatomal
distribution of the dorsal root ganglion in which it lies. In this scenario the dorsal
root ganglion affected is T5. Some patients may describe a painful prodrome,
followed by development of skin lesions. The associated pain can be intense, severe
and neuropathic in character. Classically described as throbbing or burning, it is
worse as the day progresses and maximal at night. Associated sleep disturbances
are common, and it may subsequently lead to depression, fatigue and concentration
difficulties. The commonest site of pain is in the thoracic dermatomes, but it
may also affect the ophthalmic division of the trigeminal nerve, making it a key
differential diagnosis for trigeminal neuralgia.
In the majority of patients, pain is acute, lasting less than 30 days, or subacute,
lasting less than 120 days. In some patients, however, it lasts more than 3 months
after skin lesions have healed, and this is described as post-herpetic neuralgia
(PHN).
PHN may last several years and can be severe and debilitating. Risk factors include
increasing age, female gender, presence of a prodrome, more severe pain in the
acute phase, and a more intense rash, as well as psychosocial factors such as higher
anxiety levels.
Management of PHN can be challenging. Patients should be well educated about
their condition, and given appropriate support and counselling. Psychological
therapies such as cognitive behavioural therapy may be of benefit.
In terms of pharmacological management, recommended first line agents include
gabapentinoids (gabapentin, pregabalin) or tricyclic antidepressants (amitriptyline,
nortriptyline). Lignocaine patches have been used and are recommended but robust
evidence for their benefit is lacking. Opioids help reduce severity of the pain but
73
74
Chapter 2
long-term use is associated with several unwanted effects, and topical capsaicin has
been used successfully for PHN, but may be painful to apply.
In this scenario, each of the options is possible, but the first line agent, and hence
the most appropriate next step, would be gabapentin. Subsequently, other options
can be explored, depending on the patient’s response.
Gupta R, Smith PF. Post-herpetic neuralgia. Cont Educ Anaesth Crit Care Pain 2012; 12(4):181–85.
24. C Hyperalgesia may develop with increasing dosage
Opioid-induced hyperalgesia occurs when pain is uncontrolled despite increasing
use of long-term oioids.
The use of opioids has commonly been described without a ceiling in cancer pain
and palliative care, but in this clinical picture is inappropriate. The use of opioids in
non-cancer pain is becoming recognised as ineffective and potentially harmful due
to its suppression of the immune and hormonal systems. Opioids can act directly on
the hypothalamo-pituitary axis to reduce gonadotrophin releasing hormone (GnRH),
luteinizing hormone (LH) as well as gonadal testosterone. Opioids also reduce
adrenocorticotrophic hormone (ACTH) and cortisol with long-term use.
Respiratory depression is not observed at stable doses of opioids administered longterm.
The constipating effects of opioids are long-term and do not resolve unless the
opioids are withdrawn.
Seyfreid O, Hester J. Opioids and endocrine dysfunction. Br J Pain 2012; 6(1):17–24.
25. C Intravenous morphine
The expression ‘porphyria’ encompasses a collection of inherited disorders of haem
synthesis. Haem is a key constituent of haemoglobin and an example of a naturally
occurring porphyrin. Its synthetic pathway consists of a series of enzyme-dependent
steps. Genetic mutation causing a deficit of a particular enzyme in this pathway
results in accumulation of the intermediate substrates that rely on it for their
metabolism.
The primary step in the haem synthetic pathway is the combination of glycine and
succinyl CoA to form the compound 5-aminolevulinic acid (5-ALA) by the action of
ALA synthase. Deficiency of any enzyme downstream from this step will cause the
accumulation of 5-ALA. In all acute porphyrias, 5-ALA levels are elevated. Whether
this itself is the cause of the clinical manifestations of acute porphyria is unclear.
In any form of acute porphyria, an acute neurovisceral crisis may be triggered by
anything that increases the demand for haem, including infection, dehydration,
starvation and drugs. The key presenting features are abdominal pain, neurological
symptoms and tachycardia. As these are rather non-specific presentations, diagnosis
is often made late. In this scenario, it is not a surgical condition causing the patient’s
pain, but this may additionally trigger a porphyric crisis.
Answers
A number of drugs used in common anaesthetic practice may be unsafe for use
in patients with porphyria. The majority are, in fact, safe, and the Table 2.6 below
summarises drugs that are either known to be dangerous or those which are yet
unclassified for use in porphyric patients.
Table 2.6 Safety of different drug classes for use in porphyria.
Class of drug
Unsafe
Intravenous induction agents
Thipentone ketamine
Inhalational anaesthetic agents
Sevoflurane
Local anaesthetic agents
Unclassified
Levobupivacaine ropivacaine
Analgesics
Oxycodone diclofenac
Mefanamic acid pentazocine
Vasopressors
Ephedrine
Metaraminol vasopressin
Antibiotics
Erythromycin rifampicin
Morphine is a safe, effective, titratable drug that can be used in porphyria, and
would be the drug of choice here. The patient is tachycardic with small bowel
obstruction, and likely to be hypovolaemic. This would preclude the use of an
epidural. Levobupivacaine has indeterminate safety profile so should be avoided
and relying on local infiltration of the surgical wound would not provide lasting
analgesia. Oxydone and ketamine are unsafe.
Findley H, Philips A, Cole D, Nair A. Porphyrias: implications for anaesthesia, critical care, and pain
medicine. Contin Educ Anaesth Crit Care Pain 2011; 12(3): 128–133.
26. B Trendelenburg positioning
During surgery for penetrating eye injury, control of intraocular pressure (IOP)
is important to prevent expulsion of the contents of the orbit. Episcleral venous
pressure, which is influenced by central venous pressure (CVP), is the most important
factor determining IOP acutely; hence measures to prevent venous congestion
must be employed. Such measures include taping, not tying, the endotracheal tube,
keeping the head in the neutral position, reverse Trendelenburg positioning and
avoiding coughing by ensuring adequate muscle relaxation. Hypercarbia can lead to
an increase in IOP; hence increasing the minute ventilation will reduce CO2 and help
to reduce IOP.
Both acetazolamide and mannitol can be used to reduce IOP in the acute setting.
Acetazolamide is a carbonic anhydrase inhibitor that reduces the production of
aqueous humour, while mannitol dehydrates the eye by its action as an osmotic
diuretic. Both have systemic effects that must be taken into account when
administered, such as electrolyte disturbance and dehydration.
Trendelenburg positioning is the correct answer, as the head down position will
reduce venous drainage from the orbit and cause an increase in CVP and therefore
the IOP.
Murgatroyd H, Bembridge J. Intraocular pressure. Contin Educ Anaesth Crit Care Pain 2008; 8(3):100–103.
75
76
Chapter 2
27. B Request cryoprecipitate and platelets from the blood
bank
Cell salvage is the process of utilising a patients own blood retrieved from the
surgical field to produce autologously transfused blood by filtering and washing it.
Cell salvage therefore returns red cells and reduces the requirement for allogenic
transfusions, with the following indications:
• Expected blood loss of > 20% blood volume or > 1 litre
• Operations with an expected blood transfusion requirement
• Pro-haemorrhagic states
• Preoperative anaemia
• Rare blood groups
• Patients with rare blood antibodies
• Patient refusal for allogenic blood transfusion
As cell salvage only returns red blood cells, other blood products such as plasma,
inflammatory mediators and, importantly platelets and clotting factors, are therefore
discarded. Patients receiving more than 2 litres of autologous red cells are at a
significant risk of developing coagulopathy.
In this clinical scenario, the patient is likely to require coagulopathic support, due to
anticipated further bleeding, in the form of platelets and cryoprecipitate.
Tranexamic acid is useful in reducing on-going bleeding as an antifibrinolytic, but
it will not prevent the massive blood loss coagulopathy expected. Hypotensive
anaesthesia is not a recommended anaesthetic technique in vascular surgery
and carries a significant hazard of complications in high-risk patients undergoing
vascular intervention. Point of care measurement of activated clotting time (ACT)
guides intraoperative heparin therapy, but will not assist in the treatment of massive
haemorrhage coagulopathy. Finally, waiting for laboratory blood results will merely
delay the required intervention of administering clotting products in a timely
manner. Thus, requesting clotting products is the most appropriate step at this point
as it prepares the anaesthetist for the ensuing coagulopathy.
Kuppurao L, Wee M. Perioperative cell salvage. Contin Educ Anaesth Crit Care Pain 2010; 10 (4):104–108.
28. D Left coronary artery
Sudden occlusion of major coronary arteries is the most common cause of
myocardial infarction (MI). The area of myocardial ischaemia depends on the
coronary circulation. Early recognition of acute coronary obstruction and quick
reperfusion is essential for good outcome after MI.
A good anatomical knowledge is essential for successful MI management (Figure 2.7).
The blood to the heart is mainly supplied by two main coronary arteries (CAs), the
right coronary artery (RCA) and the left coronary artery (LCA).
The RCA arises form the right anterior aortic sinus. It mainly supplies blood to the
right side of the heart. However, the RCA also gives twigs to the right atrium and left
ventricle (LV).
Answers
Figure 2.7 Coronary circulation.
Aortic arch
Left
coronary artery
LPA
SVC
RPA
Left
circumflex artery
LA
RA
Right
coronary
artery
Right
marginal
artery
RV
LV
Left anterior
descending
artery
Left marginal
artery
Diagonal
arteries
Posterior
descending artery
The RCA travels along the right atrioventricular (AV) groove on its way to the crux
of the heart. It gives off the right marginal artery, which descends along the acute
margin of the heart and gives off branches to both sides of right ventricle. The RCA
continues on the diaphragmatic surface of the heart along the posterior longitudinal
sulcus to continue to the apex of the heart as the posterior descending artery (PDA).
The PDA supplies the inferior and the posterior walls of the left ventricle (LV), the
ventricular septum and part of the papillary muscles.
The LCA arises from the left anterior aortic sinus. It supplies blood to the left side
of the heart and it is larger than RCA. It usually runs for 1–25 mm as the left main
coronary artery before bifurcating into left anterior descending artery (LAD) and left
circumflex artery (LCX).
The LAD runs in the interventricular groove along the anterior surface of the heart.
It gives off diagonal branches (supply the anterolateral surface) and septal branches
(supply the interventricular septum) on its way toward the apex of the heart.
The LCX primarily supplies the lateral wall of the heart. It runs along the left
atrioventricular groove, reaching as far as the posterior longitudinal sulcus. It gives 1
to 3 marginal branches, which supply the lateral free wall of the LV.
The coronary artery dominance is determined by the artery that gives the posterior
descending artery. In most of patient (85%), the RCA gives off the PDA and the
coronary circulation can be identified as right-dominant. In a left-dominant
circulation, the PDA is given off by the LCX (15% of cases).
A 12-lead electrocardiogram (ECG) looks at the heart from different angles.
The changes seen in the ECG leads adjacent to the ischaemic area usually reflect the
areas of the coronary arteries occluded (Table 2.7).
In this clinical scenario, the patient has acute occlusion of the left coronary artery
(anterolateral V2-V6, I and aVL). This lesion results in rapid deterioration of the
77
78
Chapter 2
Table 2.7 ECG changes seen depending on infarcted areas or coronary arteries involved
Area infarcted
Leads adjacent
Artery involved
Septal
V1–V2
LAD
Anterior
V2, V3 and V4
LAD
Anteroseptal
V1–V4
LAD
Lateral
I, aVL and V5–V6
LCX
Anterolateral
V2–V6, I and aVL
LCA (LAD + LCX)
Inferior
II, III and aVF
RCA
Posterior
Reciprocal changes V1–V3
RCA
patient condition because it usually leads to entire LV infarction. These patients have
a poor prognosis if not treated immediately.
Thejanandan CS, Reddy D, Rajasekhar D, Vanajakshamma V. Electrocardiographic localization of infarct
related coronary artery in acute ST elevation myocardial infarction. J Clin Sci Res 2013;2:151–60.
29. A Eyes 2 Verbal 3 Motor 4
In order to assess the conscious levels of infants and children a modified Glasgow
coma scale (GCS) has been devised. The eye opening response is graded similarly to
the standard GCS. The modifications are for the motor and verbal response.
Eye opening response
4- Spontaneous
3- Verbal
2- Pain
1- None
Verbal response
5- Age appropriate
4- Irritable and cries
3- Cries to pain
2- Moans to pain
1- None
Motor response
6- Spontaneous movement
5- Withdraws to touch
4- Withdraws to pain
3- Abnormal flexion
Answers
2- Extensor response
1- None
Using this scoring system, this patient scores: eyes 2; verbal 3; motor 4 giving a
paediatric GCS of 9/15.
The current guidelines recommend that a CT scan is indicated if GCS < 12 and
intracranial pressure monitoring is required if GCS is between 3-8, both of which
would be necessary in this case.
Cullen PM. Paediatric trauma. Contin Educ Anaesth Crit Care Pain 2012; 12(3):158–161.
30. D intramuscular adrenaline 0.5 mL of 1:1000
This scenario most likely represents an anaphylactic reaction to the intravenous
cefuroxime administered to the patient. Adrenaline (epinephrine) is the most
appropriate drug for management of anaphylaxis. The α-adrenoceptor agonistic
effect reverses peripheral vasodilatation and oedema, whereas the β-adrenoceptor
agonistic effect increases cardiac output, dilates bronchial airways and attenuates
the IgE-mediated reaction by acting on β-adrenoceptors on mast cells. The
intramuscular route is most appropriate for adrenaline as:
• ECG monitoring is not immediately available (patient being on a ward)
• There is a greater margin of safety required in a suspected case of anaphylaxis
Repeated intramuscular dose can be administered according to patient response,
with an initial dose of 0.5 mL of 1:1000 (500 mcg) adrenaline.
The intravenous route is recommended in certain specific conditions:
• The administrator has vast experience of using this route for adrenaline
administration excluding cardiac arrest scenarios
• The patient is under full monitoring (ECG, BP, pulse oximetry)
• There is no doubt regarding the diagnosis
The dose for intravenous administration for treatment of anaphylaxis is 0.5 mL of
1:10,000 (500 mcg) adrenaline.
Resuscitation Council (UK). Emergency treatment of anaphylactic reactions. London: Resuscitation Council
(UK), 2008.
79
Chapter 3
Mock Paper 3
Questions
1. You are asked to anaesthetise a 40-year-old man for an elective brain tumour
resection. He has a Glasgow coma score (GCS) of 15/15 and his CT shows minimal
midline shift.
Which volatile-based anaesthetic is least likely to detrimentally affect his
intracranial pressure?
A
B
C
D
E
Desflurane
Isoflurane
Nitrous oxide and sevoflurane
Sevoflurane
Halothane
2. A 76-year-old man has been admitted following coronary artery bypass grafting.
He has severe left ventricular dysfunction postoperatively and failed to wean from
cardiopulmonary bypass necessitating intra-aortic balloon pump insertion.
Concerning the expected haemodynamic effects of a correctly sited and timed
intra-aortic balloon pump, which of the following is the most appropriate answer?
A
Increased aortic systolic pressure, increased left ventricular end-diastolic
pressure
B Reduced aortic systolic pressure, increased preload
C Increased coronary blood flow, reduced aortic diastolic pressure
D Increased left ventricular volume, increased coronary blood flow
E Reduced preload, reduced left ventricular wall tension
3. You are anaesthetising a patient for a right pneumonectomy. You have successfully
inserted a left-sided double lumen tube (DLT) and the patient is taken into the
operating room and placed in the right lateral position. Initial ventilator settings
are intermittent positive pressure ventilation (IPPV) with a tidal volume of 600 mL
and Fio2 1.0. Shortly after clamping the catheter mount and deflating the right lung
the patient rapidly desaturates to 88%. The peak pressure alarm on the ventilator
sounds.
82
Chapter 3
What is the first appropriate course of action?
A
B
C
D
E
Deflate the bronchial cuff
Apply 5 cm H2O CPAP
Check the position of the tube with a fibrescope
Administer 5 L/minute oxygen to the deflated lung
Advance the DLT 2 cm
4. A 70-year-old woman is receiving laser therapy to vocal cord polyps. Her grade
1 intubation with a laser-resistant cuffed tube filled with methylene blue was
uneventful and she is being ventilated with 2% sevoflurane and 50% oxygen.
Suddenly the surgeon notices flames and methylene blue around the endotracheal
tube so stops lasering and floods the site with saline.
What is the most appropriate next step in managing her airway?
A
B
C
D
E
Reduce the Fio2 and perform bronchoalveolar lavage
Stop the flow of all airway gases and remove the endotracheal tube
Reduce the Fio2 and pack wet swabs around the endotracheal cuff
Reduce the Fio2 and perform a tracheostomy
Reduce the Fio2 and inspect the endotracheal tube lumen via fibrescope
5. A 27-year-old man with type 1 diabetes is listed for day case shoulder arthroscopy
under general anaesthesia. He is listed first on an afternoon list and will take an
early breakfast on the morning of surgery. He takes Novomix 30 twice a day after
his morning and evening meals. His HbA1c measured last month was 53 mmol/
mol (7%).
What is the most appropriate advice for his insulin adjustment on the day of
surgery?
A
B
C
D
E
Take usual morning dose, and usual insulin with evening meal
Halve usual morning dose, take usual insulin with evening meal
Omit usual morning dose, take normal insulin with evening meal
Halve usual morning dose, halve evening dose
Omit usual morning dose, halve evening dose
6. A 25-year-old woman is having a hysteroscopic myomectomy for infertility under
general anaesthesia. The procedure has been prolonged and the irrigation bags
have been changed several times. On screen you can see some blood and bubbles
in the uterine cavity. She is positioned in the lithotomy position and is slightly
head down. You suddenly notice a stepwise decrement in end-tidal waveform
capnography, the patient desaturates and there is new T wave inversion on her
ECG.
Which of the following is the most appropriate immediate management?
A
Call for help, ask the surgeon to stop. Place the patient flat. Give a fluid
challenge and high-flow oxygen.
Questions
B
Call for help, ask the surgeon to flood the uterus with irrigation. Place the
patient flat. Give a fluid challenge and high-flow oxygen.
C Call for help, ask the surgeon to externally compress the uterus. Place the
patient lateral. Give a fluid challenge and high-flow oxygen.
D Call for help, ask the surgeon to empty the uterus. Place the patient head up.
Give a fluid challenge and high-flow oxygen.
E Call for help. Steepen the head down to insert a central venous line into the right
internal jugular vein, pass it into the right atrium and attempt to aspirate air.
7. A 68-year-old man undergoing vocal cord surgery is receiving high frequency jet
ventilation via a subglottic catheter with the following standard settings: Fio2 0.9,
driving pressure 2 atmospheres, frequency 150 min-1, inspiratory time 50%. Blood
gas analysis shows a respiratory acidosis and clinically there is no evidence of air
trapping.
Which action is most likely to improve the respiratory acidosis?
A
B
C
D
E
Increasing the driving pressure
Increasing the ventilator frequency
Increasing the inspiratory time
Increasing the Fio2
Increasing the expiratory time
8. A patient 10 days post coronary artery bypass grafting requires an MRI brain scan
for neurological deterioration.
Which of the following is most likely to be a safety hazard during the scan?
A
B
C
D
E
History of a total hip replacement
Presence of sternal wires
Use of an endotracheal tube with metallic spring in the pilot balloon
Epicardial pacing wires
Invasive arterial blood pressure transducer
9. A 27-year-old woman is to have femoral nerve block with the aid of nerve
stimulator.
What is the most important feature of an electrical peripheral nerve stimulator?
A
B
C
D
E
Short pulse duration
Stimulation frequency of 2 Hz
Constant current generator
Negative stimulation polarity
Actual current digital display
10. You have been called to site an epidural for a 32-year-old term primigravida
patient. She is now 3 cm dilated with slow progress and very distressed with each
contraction. While you are placing the Tuohy needle in the epidural space, you see
an obvious flow of clear fluid through the needle.
83
84
Chapter 3
What would be the most appropriate next course of action?
A
B
Pull the needle out and arrange alternative analgesia
Inject 10 mL of normal saline into the subarachnoid space to prevent postdural puncture headache (PDPH) and then re-site the epidural catheter in
another interspace
C Remove the needle and re-site the epidural catheter in another interspace. Tell
the midwife to use 10 mL of epidural mixture for each top-up
D Thread the epidural catheter through the punctured dural hole and use it as
intrathecal catheter. Make sure only an anaesthetist gives every top-up dose
E Pull the needle out and call the consultant on call to perform a blood patch to
prevent PDPH
11. You have been called to an acute medical ward to help manage a man who has
become distressed and angry with the medical management of a relative, and is
now behaving violently toward one of the ward staff. When you arrive the situation
is heated, security and porter staff are already in attendance. The sister tells you
and the on call psychiatrist that the man is unreasonable and needs to be sedated
for safety.
How do you proceed?
A
B
Offer the man a dose of oral lorazepam
Attempt to assess his capacity, and discuss with your consultant. Defer
immediate management to the security staff and police
C Give intramuscular lorazepam and haloperidol
D Give a dose of intramuscular ketamine and transfer to a monitored environment
E Organise the security staff to restrain the man, and give intramuscular lorazepam
12. A 24-year-old 60 kg woman has been injured in a house fire. She has sustained
40% full thickness lower limb and abdominal burns. Her burns were sustained at
11 pm. She is intubated in the emergency department for suspected inhalational
injury and resuscitated with 2 litres of crystalloid in total. At 3 am she is ready for
transfer to the regional burns unit that is 4 hours away.
What is the most appropriate fluid regime during transfer?
A
B
C
D
E
Colloid solution, at 500 mL/hour
Compound sodium lactate, at 500 mL/hour
0.9% sodium chloride, at 500 mL/hour
Colloid solution, at 700 mL/hour
Compound sodium lactate, at 700 mL/hour
13. A previously well 28-year-old man presents to the emergency department with
a 48-hour history of feeling generally unwell and complains of polyuria and
abdominal pain.
His arterial blood gas on room air is shown in Table 3.1.
His biochemistry profile is shown in Table 3.2.
Questions
Table 3.1 Arterial blood gas results
Parameter
Result
pH
7.18
Paco2
3.4 kPa
Pao2
14.2 kPa
Base excess
–8.8 mmol/L
–)
Bicarbonate concentration (HCO3
19.7 mmol/L
Lactate
1.8 mmol/L
+
Sodium concentration (Na )
136 mmol/L
Chloride concentration (Cl–)
102 mmol/L
+
Potassium concentration (K )
5.9 mmol/L
Table 3.2 Biochemistry profile
Parameter
Result
Urea
10.7 mmol/L
Creatinine
124 μmol/L
K+
5.8 mmol/L
+
Na
137 mmol/L
Which of the following is the most likely diagnosis?
A
B
C
D
E
Renal tubular acidosis
Severe sepsis
Pancreatitis
Addison’s disease
Diabetic ketoacidosis
14. A 64-year-old man with a background of hypertension and ischaemic heart
disease is being managed for septic shock. The patient has pyelonephritis
and gram negative sepsis that is being treated with sensitive antibiotics. The
management includes a positive fluid balance for the last 24 hours of 5.5 liters and
a noradrenaline infusion currently administered at 0.8 μg/kg/min maintaining
a mean arterial blood pressure (MAP) of 55 mmHg. The ventilation parameters
are deteriorating and he is now receiving an Fio2 of 0.6. His latest haemodynamic
monitoring studies from a minimally invasive device are:
• Cardiac output index (CI) L/min/m2 (NR 3–5) – 1.94
• Intra-thoracic blood volume index (ITBVI) mL/m2 (NR 850–1000) – 650
• Systemic vascular resistance index (SVRI) (NR 1970–2390 ) – 3854
• Extra-vascular lung water index (EVLWI) (mL/kg) (NR 3–7) – 14
85
86
Chapter 3
What is the most appropriate next course of action?
A
B
C
D
E
Fluid bolus of 500 mL crystalloid and repeat studies
Increase the noradrenaline to increase MAP to 70 mmHg
Add dobutamine at 2.5 μg/kg/min
Order an urgent transthoracic echo and send cardiac troponin measurement
Commence urgent haemofiltration aiming to reduce pulmonary interstitial
fluid
15. A 17-year-old man is admitted to the critical care unit having ingested 11 g of
paracetamol 18 hours ago. An N-acetylcysteine infusion has been started and
bloods are awaited.
His blood pressure is 80/43 mmHg following one litre of Hartmann’s solution,
with a heart rate of 118 beats per minute. He is agitated and full neurological
examination is difficult. On 100% oxygen his Spo2 is 92%, with a respiratory rate of
42 breaths per minute.
An arterial blood gas is shown in Table 3.3.
Table 3.3 Arterial blood gas results
Parameter
Result
Fio2
1.0
pH
6.9
Paco2
2.8 kPa
Pao2
18 kPa
Base excess
–13.2 mmol/L
–)
Bicarbonate concentration (HCO3
12 mmol/L
Lactate
10.8 mmol/L
The next most appropriate intervention in his management would be:
A
B
C
D
E
Central venous catheter and start noradrenaline
Intubation and ventilation
Urgent transfer to a liver specialist intensive care unit
CT head
Placement of a urinary catheter
16. A 28-year-old woman presents to the emergency department with pleuritic chest
pain, shortness of breath and dizziness shortly after disembarking a flight from
South East Asia. Her respiratory rate is 45 breaths per minute, her blood pressure
is 70/40 mmHg and heart rate is 160 beats per minute. Admission to the high
dependency unit is requested for cardiovascular support.
Which piece of information would most influence your choice to administer
thrombolysis?
Questions
A
B
C
D
E
Currently on anticoagulation
Information from a CT pulmonary angiography
Information from a bedside transthoracic echo
A history of being 20 weeks pregnant
A history of peptic ulcer disease
17. A 46-year-old man is sedated and intubated for respiratory failure secondary to
community acquired pneumonia. He is known to have recurrent admissions with
pneumonia. Your junior colleague sustains a needlestick injury whilst inserting an
arterial line, is anxious and would like you to test this patient for HIV.
With regards to HIV testing in this patient, the best course of action is:
A
B
C
D
E
Request consent from the next of kin
Test the patient for HIV
Do not test this patient for HIV because you suspect he is low risk
Do not test this patient for HIV as it is unethical
Wait until the patient has capacity and gain consent from the patient for HIV
testing
18. A 25-year-old woman is undergoing a category 1 lower segment Caesarean
section (LSCS) for fetal bradycardia. You perform a rapid sequence induction with
thiopentone 500 mg and suxamethonium 100 mg but are unable to intubate after
three attempts. The patient is desaturating and you are unable to ventilate with
a face mask and Guedel airway or with a laryngeal mask airway, despite cricoid
pressure being reduced and then released. You successfully perform a needle
cricothyroid puncture and an ENT surgeon has been informed and is on their way.
The fetal heart rate remains at 60 bpm.
What is the next appropriate step?
A
B
C
D
E
Continue oxygenation and proceed with emergency LSCS
Delay LSCS until ENT have performed surgical tracheostomy
Once ENT arrive, perform surgical tracheostomy and LSCS at the same time
Abandon LSCS and continue oxygenation until patient wakes up
Continue oxygenation until patient wakes up and then perform a spinal
anaesthetic
19. A 30-year-old woman who is 32/40 pregnant is undergoing an open
appendicectomy under general anaesthesia. She had a rapid sequence induction
with thiopentone 500 mg and suxamethonium 100 mg and was maintained on
sevoflurane in oxygen and air. At the end of the procedure, in the recovery room,
the patient complains of abdominal discomfort. The midwife from labour ward
performs a cardiotocograph (CTG), which suggests the patient is going into
preterm labour.
87
88
Chapter 3
Which of the following is the least likely cause of her preterm labour?
A
B
C
D
E
Third trimester pregnancy
Acute appendicitis
Surgical manipulation of the uterus
Sevoflurane
Maternal pyrexia
20. A 4-month-old 4.5-kg boy is on your elective day case surgical list for bilateral
inguinal hernia repair. He was born at 27 weeks gestation and his current corrected
gestational age is 44 weeks. The patient was ventilated for 10 days and was oxygen
dependent for 6 weeks. He was discharged home 3 weeks previously, but represented last week with an apparently obstructed hernia that was reduced by the
on-call surgeon. He is on iron and folic acid for anaemia of prematurity.
The most appropriate anaesthetic management would be:
A
Proceed with day case surgery under general anaesthesia supplemented with
regional anaesthesia
B Proceed with day case surgery under regional anaesthesia supplemented with
minimal intravenous sedation
C Postpone surgery until 60 weeks gestational age
D Postpone surgery until 52 weeks gestational age
E Proceed with surgery under general anaesthesia supplemented with regional
anaesthesia and admit postoperatively for apnoea monitoring
21. A 16 kg 4-year-old girl with diabetic ketoacidosis (DKA) is given 40 mL/kg of
0.9% saline for resuscitation and 85 mL/hour of 0.45% saline with 5% glucose
as replacement and maintenance fluid. An insulin infusion was commenced at
0.1 unit/kg/hour after an initial bolus dose of 0.1 unit/kg.
2 hours later she has become drowsy with a blood glucose of 11 mmol/l. She
appears lethargic and somnolent, and responds to voice. Her heart rate is 96 beats
per minute, blood pressure is 128/68 mmHg and respiratory rate is 38 breaths per
minute.
The most likely cause of her reduced level of consciousness is:
A
B
C
D
E
Cerebral oedema
Meningitis
Hypokalaemia
Dehydration
Exhaustion
22. A 65-year-old man was scheduled for a below knee amputation for peripheral
vascular disease. He is currently on 10 mg morphine sulphate twice daily for
analgesia.
What would be the most appropriate pre-medication to reduce the risk of
development of chronic pain?
Questions
A
B
C
D
E
Morphine sulphate 15 mg
Gabapentin 900 mg
Amitriptyline 25 mg
Ketamine 20 mg
Epidural analgesia 24 hours preoperatively
23. A 34-year-old woman presents with a 3-month history of poor sleep, fatigue, and
worsening widespread muscular pain. On examination, she is extremely tender on
finger palpation of several muscle groups and a diagnosis of fibromyalgia is made.
Regarding management of her symptoms, which of the following is the most
appropriate first step?
A
B
C
D
E
Trigger point injection
Morphine
Amitriptyline
Ibuprofen
Gabapentin
24. A 3-year-old boy presents for circumcision. He is previously fit and well, and
weighs approximately 10 kg. You decide to give him intravenous paracetamol
intraoperatively.
Which of the following is the correct dose?
A
B
C
D
E
150 mg
200 mg
75 mg
100 mg
500 mg
25. A 49-year-old diabetic man with peripheral vascular disease presents for right
below knee amputation. He has been in severe pain in his right leg for several
months and no oral analgesia has provided any relief. An epidural is to be
commenced preoperatively and continued into the postoperative period.
Which of the following factors increase his risk of developing chronic post surgical
pain?
A
B
C
D
E
Severe preoperative pain
Increasing age
Male gender
Use of an epidural
Diabetes mellitus
26. A 30-year-old man has sustained a partial brachial plexus injury to his left arm.
He describes constant, sharp pain with spontaneous burning and shock-like
symptoms. Light touch elicits painful episodes and there are constant tingling
sensations.
89
90
Chapter 3
Which of these statements about pain classifications would apply?
A
Neuropathic pain requires a disease or lesion of the somatosensory system to
be present
B Dysaesthesias are not always unpleasant
C Paraesthesia is usually painful
D Complex regional pain syndrome results from serious trauma
E Hyperalgesia is pain from a non-painful stimuli
27. A 33-year-old man is brought to the emergency department with an 18% body
surface area (BSA) burn.
Regarding fluid resuscitation, what is the most appropriate statement?
A
The Parkland formula should not be used as he is an adult with < 20% BSA
burn
B 4 mL/kg/% burn predicts the fluid required in the first 24 hours. Half the fluid
should be given in the first 8 hours and the remaining half over the next 16
hours from presentation to hospital
C Fluid requirement should be calculated as per the Baxter formula: 4 mL/kg/%
burn. Half the fluid should be given in the first 8 hours and the remaining half
over the next 16 hours from the time of burn
D Fluid requirement should be calculated as per the modified Brooke formula:
2 mL/kg/% burn
E Fluid requirement should be calculated as per the Parkland formula. Half
should be given as colloid and the other half as crystalloid to reduced the
complications of massive fluid resuscitation
28. During the initial surgical dissection of an aortic abdominal aneurysm, the
surgeon warns you that he needs to apply the aortic cross-clamp above the
coeliac arteries, following which the patient undergoes significant haemodynamic
changes.
What are the changes in left ventricle preload and afterload that are caused by the
aortic cross-clamp?
A
B
C
D
E
Increased preload, increased afterload
Decrease preload, increased preload
No change in preload or afterload
No change in preload, increased afterload
Increased preload, decreased afterload
29. A 45-year-old chronic alcoholic in the emergency department was found lying
unconscious on the floor of his flat amidst claims that he was not contactable for
almost 48 hours. On arrival his Glasgow coma scale (GCS) is 8, (eyes 1; verbal
3; motor 4). His has a heart rate of 104 beats per minute and a blood pressure of
80/60 mmHg. His blood gas shows severe metabolic acidosis and hyperkalaemia.
His urine output in the last hour has been 5 mL and is brown in colour.
Questions
The most appropriate investigation would be:
A
B
C
D
E
Creatinine kinase
Urininary haem
Myoglobinuria
Blood urea
Alkaline phosphatase
30. A malnourished 93-year-old man with dementia complains of lethargy,
breathlessness, myalgia and bone pain, and has petechiae, bleeding gums and
gingivitis.
Which of the following nutritional deficiencies would most likely be attributed to
this clinical condition:
A
B
C
D
E
Ascorbic acid
Iron
Thiamine
Vitamin A
Vitamin D
91
Chapter 3
Answers
1. D Sevoflurane
All volatile agents have the potential to cause cerebral vasodilation and affect
cerebral blood flow (CBF) autoregulation. The resulting increased cerebral blood
volume ultimately leads to an increased intracranial pressure (ICP) – an effect more
pronounced in cases where the ICP is already raised or there is evidence of midline
shift.
Cerebral blood flow is dependent on a number of mechanisms:
•
•
•
•
•
Autoregulation
Cerebral metabolism coupling
Biochemical reactivity
The autonomic nervous system
Flow dynamics
All volatile anaesthetics inhibit the autoregulation of cerebral blood flow which is
normally maintained over the range of perfusion pressures from approximately 50 –
150 mmHg (Figure 3.1).
Figure 3.1 Graph demonstrating
the autoregulation of cerebral
blood flow (mL/100g/min) at
cerebral perfusion pressures
between 50 and 150 mmHg in
normal individuals.
100
Cerebral blood flow
(mL/100g/min)
92
50
0
50
100
150
Cerebral perfusion pressures (mmHg)
By causing vasodilation, volatile agents obtund the myogenic reaction of the arterial
smooth muscle when exposed to increased pressure, thereby preventing the control
of blood flow. There is a range of effect across the different agents as listed below.
Halothane
Isoflurane and desflurane
Sevoflurane (minimal effect ≤ MAC 1.5)
decreasing potency
Nitrous oxide disturbs autoregulation in a similar fashion when used in isolation
and with other volatiles. Autoregulation remains intact, however, when it is used
alongside propofol, but the increased risk of expansion of any air introduced into the
cranium during surgery, leads most anaesthetists to avoid its use.
Answers
All volatiles reduce the cerebral metabolic rate as cerebral activity decreases.
Normally this would be associated with a reduction in blood flow but, if the
vasodilatory actions of volatiles are taken into account, the balance can be tipped
towards increased flow. This is known as cerebral flow-metabolism uncoupling and is
seen at higher concentrations of volatile anaesthetic in the order of potency as seen
above.
Biochemical reactivity of cerebral vasculature has been demonstrated with regards
to the cerebrospinal fluid (CSF) pH, secondary to arterial concentration of carbon
dioxide (Paco₂), and oxygen (Pao₂) (Figure 3.2).
Cerebral blood flow
(mL/100g/min)
100
CO2
50
0
Figure 3.2 Graph demonstrating
the changes in cerebral blood
flow (mL/100g/min) against
arterial partial pressures of CO2
and O2 (kPa).
O2
5
10
PaGas (kPa)
15
20
Reactivity to carbon dioxide is marginally affected by volatile anaesthetics.
Subsequently the vasodilation seen in their presence can be opposed by
hyperventilating the patient to hypocapnia. Clinically, the risk of induced cerebral
ischaemia with this practice is high enough to render it an emergency manoeuvre in
the control of a raised ICP.
Cerebral blood vessels are also responsive to the neurotransmitters released during
signalling of the autonomic system. It is controversial as to how much this influences
cerebral blood flow, but theoretically, reduced cardiac output secondary to the
presence of volatile anaesthetics may play a part.
The flow dynamics may also be altered by volatiles. Their incurred vasodilation may
prevent the ordinarily seen vasoconstriction of resistance arterioles. This would
normally occur when they are exposed to the shear stresses of increased flow.
No volatile agent is considered fully beneficial to the management of ICP but
Sevoflurane is accepted as the gold standard in neuroanaesthesia as it is least likely
to cause a detrimental effect if used appropriately.
Dinsmore J. Anaesthesia for elective neurosurgery. Br J Anaesth 2007; 99(1):68–74.
Nathanson M, Moppett I, Wiles M. Neuroanaesthesia. Oxford Specialist Handbooks in Anaesthesia, 1st Ed.
Oxford: Oxford University Press, 2011.
93
94
Chapter 3
2. E Reduced preload, reduced left ventricular wall tension
The aim of Intra-aortic balloon pump (IABP) counterpulsation is to better match
myocardial oxygen demand and supply and thus improve cardiac function. The
physical premise is one of ‘counterpulsation’, which in the context of an IABP
describes balloon inflation in diastole and deflation in early systole.
Once inserted, the inflation cycle of the balloon needs to be set. This can either be
achieved with reference to the ECG or arterial pressure (Table 3.4).
Table 3.4 Intra-aortic balloon pump counterpulsation
Point in the cardiac cycle
ECG
Arterial pressure
waveform
Inflation
After closure of the aortic valve
Mid-point of the T wave
After dicrotic notch
Deflation
Before opening of the aortic
valve
Peak of the R wave
Point just before the
upstroke of the arterial
trace
The inflation of the balloon in diastole causes displacement of blood both proximally
(in the direction of the coronary arteries) and distally. The implication of this is that
both coronary flow and distal systemic flow may increase. By inflating during diastole,
aortic diastolic pressure will increase (therefore excluding option C). Deflation of
the balloon during early systole effectively reduces the volume of blood in the
aorta – leading to lower aortic systolic pressure (thereby excluding option A) and left
ventricular afterload. As aortic systolic pressure is lowered, the left ventricle (LV) will
not have to generate as much pressure to cause opening of the aortic valve. The time
for isovolumetric contraction (IVC) is therefore shorter, and, since IVC accounts for the
majority of myocardial oxygen consumption, oxygen demand is reduced. As the LV
is able to eject blood more effectively, stroke volume increases, end-systolic volume
is reduced (excluding option D) and preload is subsequently reduced (option B). This
leads to lower LV wall tension and option E is therefore correct.
The haemodynamic effects of IABP counterpulsation are summarised in Table 3.5 below:
Table 3.5 Haemodynamic effects of IABP counterpulasation
Aorta
Left ventricle
Heart
Systemic
Systolic pressure ↓
Systolic pressure ↓
Cardiac output ↑
Mean arterial pressure ↑
Diastolic pressure ↑
End-diastolic pressure ↓
Afterload ↓
Renal blood flow ↑
Volume ↓
Preload ↓
Wall tension ↓
Coronary blood flow ↑
The main indications for IABP counterpulsation are:
• Acute myocardial infarction pending re-vascularisation
Answers
• Cardiogenic shock not reversed by pharmacological therapy
• As a bridging therapy in ventricular failure pending definitive treatment
(ventricular assist device or cardiac transplantation)
• Facilitation of weaning from cardiopulmonary bypass
• Refractory ventricular arrhythmias
There are a number of contraindications and cautions. Given the propensity for an
IABP to increase diastolic blood flow, it may worsen aortic regurgitation. It should
also not be used where there is a suspicion of damage to the aortic wall (dissection/
arch aneurysm). The device is inserted via the femoral artery and therefore should be
avoided in patients with severe peripheral vascular disease or bypass grafts.
The balloon is initially programmed to inflate and deflate with each cardiac cycle, i.e.
a ratio of 1:1. As the patient improves, weaning can occur in a stepwise manner; from
1:1, to 1:2 then 1:3–4.
Complications arising from IABP insertion relate to direct trauma to the femoral artery
as well as the aorta, thrombosis, infection and balloon rupture leading to gas embolism.
Krisha M, Zacharowski K. Principles of intra-aortic balloon counterpulsation. Contin Educ Anaesth Crit Care
Pain 2009; 9(1):24–28.
Scheidt S, Wilner G, Mueller H, et al. Intra-aortic balloon counterpulsation in cardiogenic shock. Report of a
co-operative clinical trial. N Engl J Med 1973; 288(19):979.
3. A Deflate the bronchial cuff
Hypoxaemia is an anaesthetic emergency and may occur with the use of double
lumen tubes (DLTs) and subsequent one-lung ventilation (OLV) because of shunt
and failure to ventilate. In this scenario, the most likely reason for sudden and serious
desaturation is misplacement of the DLT following repositioning of the patient.
Proximal migration of the DLT may lead to obstruction of the trachea by the
bronchial cuff, whilst distal migration may lead to obstruction to ventilation of one
or more lobes (Figure 3.3). Other clues to malposition are a decrease in compliance
(which may manifest as high peak inspiratory pressures).
a Optimal position
b Proximal migration
Obstruction
of
LUL flow
c
Distal migration (left + right)
Obstruction
of
RUL flow
Figure 3.3 Schematic diagram of DLT malpositioning. (a) demonstrates optimal positioning; (b)
demonstrates proximal migration therefore both tracheal and bronchial cuffs are inflated above the carina;
(c) demonstrate distal migration of the DLT obstructing right and left upper lobe bronchi and flow.
95
96
Chapter 3
Immediate deflation of the bronchial cuff (option A) may allow two-lung ventilation
(via the tracheal lumen) if the DLT has migrated proximally or restoration of
ventilation to the upper lobes in the case of distal migration. This manoeuver may
restore oxygenation and can then be swiftly followed by definitive repositioning of
the DLT with a fibrescope (option C). Advancement of the DLT blindly and without
deflating the bronchial cuff (option E) is not optimal management due to the risk of
bronchial injury.
Options B and D are accepted methods to improve oxygenation in the event of
hypoxaemia that is not due to tube malposition.
Campos JH, Hallam EA, Van Natta T, Kernstine KH. Devices for lung isolation used by anesthesiologists
with limited thoracic experience: comparison of double-lumen endotracheal tube, Univent torque control
blocker, and Arndt wire-guided endobronchial blocker. Anesthesiology 2006; 104(2):261–66.
Ng A, Swanevelder J. Hypoxaemia during one lung ventilation. Br J Anaesth 2011; 106(6): 761–63.
4.B Stop the flow of all airway gases and remove the
endotracheal tube
Laser technology allows precision microsurgery and improved haemostasis which
makes it an appealing surgical tool for operating in the airway. However, since lasers
generate a considerable amount of thermal energy, they also represent a potential
fire hazard. Fire requires the presence of an oxidiser (oxygen), ignition source (laser)
and fuel (endotracheal tube), all of which are present within the airway in this
scenario.
Although laser-resistant endotracheal tubes offer some protection against airway
fires, they are still flammable under certain conditions. The endotracheal cuff is
particularly susceptible to puncture from misdirected laser energy which will lead
to oxygen enrichment around the surgical site and an increased risk of catastrophic
airway fire. The most important step after stopping lasering and flooding the
site with saline is to stop the flow of all airway gases (oxidisers) and remove the
endotracheal tube (fuel). Wet swabs placed around the surgical site prior to lasering
can minimise the risk but should not be used to treat an airway fire. In the event
of an airway fire, all flammable materials should be removed from the airway. The
patient can subsequently be bag valve mask ventilated with air once the fire is out.
To assess for airway damage, rigid bronchoscopy is recommended afterwards.
Gentle bronchoalveolar lavage and fibreoptic assessment of the more distal airways
is of benefit and if the damage is severe, a tracheostomy may be indicated. Smoke
inhalation and thermal damage to the lungs may necessitate prolonged intubation
and mechanical ventilation.
Kitching A, Edge C. Lasers and surgery. Contin Educ Anaesth Crit Care Pain 2003; 3(5):143–146.
Apfelbaum J, Caplan RA, Barker SJ, et al. Practice advisory for the prevention and management of
operating room fires: an updated report by the American Anesthesiologists Task Force on operating room
fires. Anesthesiology 2013; 118(2):271–90.
Answers
5.B Halve usual morning dose, take usual insulin with
evening meal
Patients with well controlled type 1 diabetes having suitable elective procedures will
benefit from day surgery as it aims to minimise disruption to their usual routine and
allows patients to resume self-management of their diabetes.
Starvation time should be less than 12 hours so that they only miss one meal. They
should be placed first on a list and anaesthetic techniques that promote early return
to normal oral intake should be used. The ideal insulin regimens for diabetics can be
seen in Table 3.6.
Patients that have an HbA1c in the last 12 months > 69 mmol/mol (8.5%) should be
considered for referral to their GP or clinic for stabilisation prior to elective surgery. A
high level of plasma glucose leads to greater amount of glycosylated haemoglobin
molecules where glucose binds to the globin chain. This persists for the duration
of the molecule’s lifespan, and so this HbA1c measurement acts as an indicator of
glucose control over the preceding 8–12 weeks.
Table 3.6 Insulin regimens (on day of surgery)
Injection regimen
Morning surgery
Afternoon surgery
Once daily injection in morning
(Glargine, Levemir, Insulatard,
Humulin I)
Take normal dose
Take normal dose
Once daily injection in evening
(Glargine, Levemir, Insulatard,
Humulin I)
Take normal dose
Take normal dose
Twice daily injections
(Novomix 30, Humulin M3,
Humalog Mix 25/50)
Halve usual morning dose
Take normal evening dose
Halve usual morning dose
Take normal evening dose
3, 4 or 5 daily injections
Omit morning dose (unless
long acting basal insulin) or
Halve morning dose (if premixed insulin)
Take normal morning dose
Omit lunchtime dose
Omit lunchtime dose
Take normal evening dose
Take normal evening dose
Dhatariya K, Flanagan D, Hilton L, et al. Management of adults with diabetes undergoing surgery and
elective procedures; improving standards. London: NHS/Department of Health, 2011.
97
98
Chapter 3
6.D Call for help, ask the surgeon to empty the uterus. Place
the patient head up. Give a fluid challenge and high-flow
oxygen
Gas embolism can occur either into the venous system or the arterial system, and
may involve gases other than air e.g. carbon dioxide in the case of laparoscopic
misadventure. The pathophysiology and principles of management should be clear
in your mind.
Incidence
In the clinical arena, clinically obvious air embolism is thankfully rare; however in
studies looking for the condition, venous air embolism (VAE) was discovered in 100%
of seated craniotomies, 40% of Caesarean sections and 30% of hip replacements.
Dose of air is important, as is the size of the patient and the rate of air ingress. Rapid
air entry is worst with a lethal dose of around 1 mL/kg.
Pathophysiology
Gas entering the venous system returns to the right heart and can cause a right
ventricular outflow obstruction as the air is compressible and causes mechanical
dysfunction. Distal flow of air causes trapping in the pulmonary vessels and a
massive increase in pulmonary vascular resistance (PVR) and fulminant right
heart failure. Some micro-emboli may pass into the distal tree and produce noncardiogenic pulmonary oedema by secondary mechanisms. Air may also pass
through the lungs and on into the systemic circulation or through a patent foramen
ovale. Clinically the patient will exhibit tachypnoea, tachycardia and cardiovascular
collapse if the volume is great enough. Smaller doses may give chest pain, shortness
of breath and mental disturbance.
During anaesthesia the end-tidal CO2 falls as shunt increases, and desaturation will
occur with variable ECG changes and cardiovascular instability. Pulmonary oedema
may develop as a later sign, and central venous pressure can be elevated.
Detection
Clinical suspicion and vigilance are imperative in the detection of VAE. Classically
described tools for detection such as the precordial and oesophageal stethoscope
have poor sensitivity and are not often used. Doppler, in transoesophageal or
transcranial positions are very sensitive detectors of air.
Treatment
Immediate treatment is supportive and resuscitative along the ABC algorithm. It
should then focus on preventing further air entry, reducing the size of the embolus,
and overcoming the mechanical obstruction in the right side.
Preventing further air ingress can be achieved surgically at the site of bleeding,
either by covering or compressing bleeding areas and flooding the area with saline.
Venous pressure can be increased by positioning the site lower than the heart,
administering intravenous fluids, performing a Valsalva manoeuvre or increasing
intrathoracic pressure.
Answers
Reducing the size of an embolus is achieved by immediate discontinuation of
nitrous oxide and giving 100% oxygen that promotes nitrogen diffusion out of the
bubble. Aspiration from the right atrium via a central line may be possible if the
embolus is large and the patient positioned either lateral or head down position
to prevent further forward movement of air out of the right ventricle. This would
depend on the line already having been situated and the tip positioned in the right
atrium. Hyperbaric oxygen therapy will also promote rapid clearance of emboli.
Overcoming mechanical obstruction relies on judicious use of fluid and inotropic
agents to support a right ventricle against the sudden rise in pulmonary vascular
resistance.
One may not classically attribute gynaecological surgery with a high risk of venous
air embolism, but as described hitherto the only requirements are pressurised gas
and an open vascular system.
The key elements here in terms of management are:
• Recognise this as an anaesthetic emergency and summon help
• Preventing further air ingress
The aim therefore is to promote higher venous pressure at the site to reduce air
entrainment. Given the uterine site of bleeding, a head up position will be best.
Bear in mind the need for resuscitation may necessitate laying the patient flat if
cardiac arrest ensues. Other measures include compressing the wound edges by
the surgeon, and flooding with saline. In this case, with a full uterine cavity, external
compression may increase the pressure gradient and promote residual gas inflow.
The safest compromise is likely to be to empty the cavity such that the pressure
driving gas into the venous system is removed.
Supportive measures
Increasing the fraction of inspired oxygen to 100% will increase the partial pressure
of oxygen and favours nitrogen washout from bubbles to the alveoli. This will also
ensure that, if used, nitrous oxide would also be washed out.
A fluid bolus will assist in raising the venous pressure, and also assist the right
ventricle combating elevated pulmonary pressures, as well as support systemic
perfusion pressure.
Aspirating the air lock within the right atrium may be possible if there is a central line
already in situ. However, insertion after diagnosis is likely to distract from immediate
management and is not recommended.
Webber S, Andrzejowski J, Francis G. Gas embolism in anaesthesia. Br J Anaesth CEPD Reviews 2002;
2(2):53–57.
7. A Increasing the driving pressure
High frequency jet ventilation is a specialised ventilation modality designed to
achieve gas exchange by using high frequency, low tidal volume breaths. It differs
from conventional ventilation since gas exchange is not primarily dependent on
bulk flow to the alveoli (as the tidal volumes are often lower than the dead space).
99
100
Chapter 3
Instead, gas exchange is believed to occur due to Pendelluft ventilation, enhanced
molecular diffusion, cardiogenic mixing and co-axial flow.
High frequency jet ventilators work by generating high frequency jet streams which
entrain air at the jet nozzle by the Venturi principle. Adjustable settings include the
driving pressure, inspiratory time, ventilation frequency and Fio2.
Responses to adjustments are different when compared to conventional ventilation
modes and may seem counterintuitive. For example, an increased ventilation
frequency can worsen CO2 retention by impeding passive exhalation. It is therefore
recommended to reduce the ventilation rate when treating hypercapnoea if there
is evidence of air trapping. Increasing the inspiratory time (% ventilator cycle)
improves oxygenation, but at high values may also impair passive exhalation
and cause CO2 retention. The action most likely to improve CO2 clearance is to
increase the driving pressure since this will increase the tidal volumes and alveolar
ventilation. Increasing the expiratory time (by reducing the inspiratory time) will
not improve CO2 clearance in this scenario as the tidal volumes will be reduced and
there is no evidence of air trapping. Increasing the Fio2 will improve oxygenation but
has no effect on CO2 clearance (Figure 3.4).
Figure 3.4 High frequency
jet ventilation gas exchange
theories
1
4
2
3
(1) Co-axial flow: Gas inflow is confined to the centre of the
airway, while gas exits the lung circumferentially along the
periphery
(2) Pendelluft ventilation: Movement of gas between lung unit
with different time constants.
(3) Cardiogenic mixing: Cardiogenic oscillations are transmitted
through the lung parenchyma which augments gas mixing.
(4) Enhanced molecular diffusion: Enhanced kinetic activity of gas
molecules increase their diffusion across the alveolocapillary
membrane.
Answers
Evans E, Biro P, Bedforth N. Jet ventilation. Contin Educ Anaesth Crit Care Pain 2007; 7(1):2–5.
Brice JW, Davis WB. High frequency ventilation in the adult. Clin Pulm Med 2004; 11(2):101–6.
8. D Epicardial pacing wires
Safety considerations when anaesthetising patients for MRI scans include:
•
•
•
•
•
•
•
Remote location
Limited access to the patient
The projectile effect of the magnetic field on ferromagnetic equipment
The heating effect and risk of burns from conductive wires and coils
Risk of equipment malfunction
Noise protection
Risk of contrast reactions
MRI scanners operate with magnetic field strengths of 0.5–3 Tesla (T). The strength
of the field decays exponentially with distance from the magnet, which is always
kept on. Zones around the magnet are described in terms of Gauss (G), where 1T =
10,000G. Within 50G zone a significant attractive force will risk ferromagnetic objects
to act as projectiles potentially causing serious harm or damage, and an area of 5G is
set where no unscreened personnel should enter (see Figure 1.2). Currents may be
generated in cables especially in coils causing a local heating effect that may cause
burns to the patient.
Special MRI safe anaesthetic machines, ventilators and monitors should be available.
MRI compatible ECG electrodes, and fibreoptic pulse oximetry should be used
and all cables should be kept away from the area being imaged, in straight lines
away from the patient to avoid burns. ST-T wave artefacts may occur due to the
heating effect of blood around the aortic arch. Blood pressure cuffs without metal
connectors and invasive pressure transducers may be used. Gas sampling lines
will be longer, increasing the lag time and dead space. Epicardial pacing wires and
pulmonary artery catheters containing conductive wires risk myocardial heating and
burns, and scans cannot be performed in cases where these cannot be removed.
The spring in an endotracheal tube pilot balloon is safe, however it should be taped
away from the area being scanned as it may cause image artefact. Only essential
infusions should be continued and long extensions attached to pass through a wall
port so that the syringe pumps can stay in the control room.
Most orthopaedic prostheses, surgical clips and sternal wires are safe, but may
distort images. Other implanted metallic devices such as pacemakers, cochlear
implants, intraocular metallic objects and aneurysm clips will cause internal heating,
malfunction or risk movement and so would contraindicate a scan.
Reddy U, White MJ, Wilson SR. Anaaesthesia for magnetic resonance imaging. Contin Educ Anaesth Crit
Care Pain 2012; 12(3):140–44.
9. C Constant current generator
The use of a peripheral nerve stimulator to localise nerves is still the commonest
technique employed worldwide in regional anaesthesia. The method is based on the
101
102
Chapter 3
principle that muscle contraction becomes obvious when enough electrical current
is applied to the nerve in order to depolarise the nerve fibres.
The main objective in regional anaesthesia is to stop nerve conduction by infiltrating
enough local anaesthetic close to the nerve fibres and provide motor and sensory
block. This goal is possible due to the capability of nerve stimulators to approximate
the distance between the nerve and the needle tip and hence can localise the
optimal injection site.
Nerve fibres differ anatomically according to their thickness and degree of
myelination. Stimulating motor fibers with nerve stimulator is easier than
stimulating sensory fibres because Aα motor fibers have the maximal velocity of
impulse spreading and a relatively low threshold for extrinsic activation because
of a large diameter and high degree of myelination. In contrast, C-fibres have a
small diameter and very little or no myelin sheath, hence have a high threshold for
external stimulation and relatively slow action potential propagation.
An ideal nerve stimulator should have the following features:
1. Constant current generator: They must be able to supply a constant electrical
current between the negative pole and the positive pole irrespective of the
wide range of impendences encountered by the tissue around the nerve. Nerve
stimulators provide a current range between 0.01–5 mA.
When performing a nerve block, the ideal initial current is 1–2 mA. The needle is then
inserted until the desired muscle contraction is seen. The stimulating current is then
gradually decreased until twitches are still seen at a final range of 0.2–0.5 mA which
is the most acceptable current threshold. A current above 0.5 mA may mean the
needle tip is far from the nerve and the block may not be successful. Twitches should
not be seen below 0.2 mA because motor response below 0.2 mA may mean the
needle is inside the nerve and injecting maybe harmful.
2. Stimulation polarity: In order to get maximum benefit from the delivered current,
the needle should be connected to the negative pole (cathode) to depolarise nerve
fibres. Stimulating nerves with the anode will lead hyperpolarisation of the fibres,
thus a stronger current will be required to depolarise the nerve. Modern nerve
stimulators are designed in order to only allow the needle to be connected to the
cathode electrode.
3. Stimulation frequency: This affects the speed of nerve localisation. The ideal
current frequency is 1–2 Hz, where a higher frequency makes nerve detection faster,
but causes more patient discomfort. Therefore, the most common frequency used is
2 Hz.
4. Pulse duration: This is the time for which the electrical current is applied to the
nerve. A short pulse duration (0.1 ms) ensures motor neurons are stimulated but not
the sensory neurons.
5. Accuracy: The current generated by the nerve stimulator must be similar to the
displaced one on the digital screen. Accurate current generation is mandatory for
correct needle insertion and successful nerve block.
Answers
The above features of nerve stimulators are all essential for successful nerve block.
However, the most important characteristic of peripheral nerve stimulators is the
constant current generation. This allows the current to remain the same regardless
of resistance variation encountered by tissue, thus decreases the chance of nerve
damage or unsuccessful nerve block.
Sardesai AM. Lyer U. Nerve stimulation for peripheral nerve blockade. Anaesthesia Tutorial of the Week no
149. London: World Federation of Societies of Anaesthesiologists, 2009.
Shariat AN, Horan PM, Gratenstein K, McCally C, Frulla AP. Electrical nerve stimulators and localization of
peripheral nerves, New York: The New York School of Regional Anaesthesia, 2013.
10. D Thread the epidural catheter through the punctured
dural hole and use it as intrathecal catheter. Make sure
only an anaesthetist gives every top-up dose
Inadvertent dural puncture can occur following many procedures, for example spinal
surgery. However, in anaesthetic practice it is usually a consequence of epidural
analgesia and anaesthesia.
Every year, approximately 140,000 labouring women receive an epidural in the
UK. 1,400 (1%) will suffer an accidental dural puncture. The commonest reported
complication is post-dural puncture headache (PDPH), with an incidence varying
from 60% to 90%. Headache usually develops 12–24 hours following dural puncture.
PDPH may cause significant morbidity and mothers may be unable to properly care
for their newborn or themselves for some time.
Puncturing the dura with a 16G Touhy needle usually results in an obvious
cerebrospinal fluid (CSF) flow through the epidural needle. The CSF is warm to touch
and tests positive to glucose with urine dipstick.
Each obstetric unit should have a plan of action for accidental dural tap.
At the time of recognised dural puncture, the anaesthetist must decide whether
to use the catheter for a continuous subarachnoid (intrathecal) technique or
re-site the epidural in another interspace. Whichever decision is made, only the
anaesthetist should give every dose of local anaesthetic top-up. Therefore, stem D is
inappropriate here as the midwife gives the top-up.
The patient should be informed about the dural puncture and counseled regarding
potential complications and further management options. A senior anaesthetic
colleague, the obstetric registrar and the midwife should also be informed, and the
operator must ensure everything is documented in the patient’s notes.
If no PDPH is present during labour, pushing at full dilation can be encouraged.
However, if a headache is present, forceps delivery may be advised.
After delivery, remove the catheter as usual. There is little evidence that leaving a
subarachnoid catheter in place for 24 hours can reduce PDPH.
If no headache is present post delivery, do not restrict patient’s mobilisation,
as immobilisation will not prevent the development PDPH. However, if a PDPH
103
104
Chapter 3
develops, encourage bed rest, regular analgesia, oral fluid and oral caffeine intake,
and consider epidural blood patch. Epidural blood patch is the gold standard
therapy for PDPH, however if performed within 24 hours of onset of symptoms there
is a failure rate of 70%, which reduces to 4% if performed after 24 hours. Therefore, it
is preferable to perform blood patch more than 24 hours after the dural tap occured.
Studies investigating the use of epidural saline as a preventative measure against
PDPH failed to reach statistical significance. In addition, pooled results of the
four randomised trials failed to show statistical significance for the use of epidural
blood patch as prophylactic measure to treat PDPH. The use of sumatriptan and
adrenocorticotrophic hormone (ACTH) has also previously been advocated, but
again there is a large disparity in the evidence base for their use.
Royal College of Anaesthetists. Major complications of central neuraxial blocks in the United Kingdom: the
3rd National Audit Project (NAP3). Br J Anaesth 2009; 102(2): 179–90.
Apfel CC, Saxena A, Cakmakkaya OS, et al. Prevention of postdural puncture headache after accidental
dural puncture: A quantitative systematic review. Br J Anaesth 2010; 105(3):255–63.
Sharpe P. Accidental dural puncture in obstetrics. BJA CEPD Reviews 2001; 1(3):81–84.
11. B Attempt to assess his capacity, and discuss with your
consultant. Defer immediate management to the security
staff and police
There are multidisciplinary rapid response teams in some hospitals, for the purpose
of sedating disturbed psychiatric inpatients, which do include anaesthetists. The
Royal College of Anaesthetists has issued position statement guidance in tandem
with the Royal College of Psychiatrists, the noteworthy points include:
• Anaesthetists should only act as part of a multidisciplinary response team
incorporating mental healthcare professionals including a psychiatrist
• Trainee anaesthetists should not routinely be involved in initiating
pharmacological restraint, but if the urgency of the clinical situation dictates they
must only act within their competence and, whenever possible, after consultation
with a consultant anaesthetist
• When rapid tranquillisation is deemed appropriate the minimum intervention
possible should be used as guided by the local protocol
• The full range of ventilatory/resuscitation equipment and trained assistance must
be immediately available when rapid tranquillisation is administered
• The College does not support under any circumstances the use of rapid
tranquillisation to manage violence or aggression in visitors or other individuals
on hospital premises
This question, like some past exam SBAs, reflects some of the more difficult ‘reallife’ clinical situations we can find ourselves in as practising anaesthetists. The
important points to draw from the stem are the lack of any evidence of confusion
or signs of organic mental illness. The man is aggressive and violent, but as a visitor
is not a patient of the hospital. This means that his behaviour should be managed
by security staff, who have been specially trained to do so, and if necessary by the
police. If the police after their initial assessment were to believe him to be mentally
disturbed, they would convey him to the emergency department or other place of
Answers
safety for specialist assessment. This does not remove our responsibility to respond
to treat visitors in an emergency, such as in the case of a collapse or cardiac arrest.
Royal College of Anaesthetists. Position statement on the involvement of anaesthetists in restraint teams.
London: Royal College of Anaesthetists, 2014.
National Institute for Health and Care Excellence (NICE). Violence: The short-term management of
disturbed/violent behaviour in psychiatric in-patient settings and emergency departments. CG No 25.
London: NICE, 2005.
12. E Compound sodium lactate, at 700 mL/hour
Fluid resuscitation after burns injury is widely guided by the Parkland formula:
4 mL/kg/% body surface area burn, where half of this volume is given in the first
8 hours after the burn injury, and the second half over the next 16 hours. Thus for the
above patient:
4 x 60 x 40 = 9600 mL
Therefore this patient requires 4800 mL in the first 8 hours.
Two litres has already been given in the first 4 hours since the burn, and so 2800 mL
should be given over the next 4 hours, which is 700 mL/hour.
Intravenous fluids are given in cases of more than 15% total body surface area
(TBSA) burns or 10% with smoke inhalation. The fluid of choice is a balanced
crystalloid solution, and initially a urine output of greater than 0.5 mL/kg/hour is
used to guide adequate resuscitation.
Criteria for referral to a specialist burns unit include:
•
•
•
•
•
> 2% TBSA in children or > 3% in adults
Full thickness burns
Circumferential burns
Unhealed burn after 2 weeks
Any suspicion of non-accidental injury
Discuss with a burns specialist with an opinion to transfer:
•
•
•
•
•
Burns to hands, feet, face, perineum or genitalia
Chemical, electrical or friction burns
Cold injuries
Febrile child with a burn
Co-morbidities affecting treatment or healing of the burn
Intubation for a burn is indicated in the presence of stridor, oropharyngeal oedema,
deep facial or neck burns, a GCS < 8, hypoxia or hypercapnia, or suspicion of
inhalational injury. Facial oedema can progress rapidly and an early intubation using
a large uncut endotracheal tube should be performed prior to transfer if there are
any concerns. A rapid sequence induction using suxamethonium is acceptable if
within the first 24 hours after the burn.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–22.
National Network for Burn Care. National Burn Care Referral Guidance. London: NHS Specialised Services,
2012.
105
106
Chapter 3
13. E Diabetic ketoacidosis
This patient has presented with a raised anion gap metabolic acidosis.
Causes of raised anion gap metabolic acidosis indicate the presence of an
unmeasured anion; in this case ketones, the anion gap can be calculated as follows:
(Na+ + K+) – (HCO3– + Cl–)
Normal range: 8–16 mmol/L
The causes can be remembered using the acronym ‘MUDPILES’:
• Methanol
• Uraemia
• Diabetic ketoacidosis
• Propylene glycol
• Isoniazid
• Lactic acidosis
• Ethylene glycol
• Salicylates
The abdominal pain and polyuria together with the biochemical profile make
diabetic ketoacidosis (DKA) a likely diagnosis. DKA is commonly precipitated by
infection or non-compliance to insulin therapy in the known type 1 diabetic mellitus
patient. However an increasing proportion occurs in the undiagnosed diabetic
patient and may indeed be the presenting feature as in this case.
Severe sepsis would also cause a raised anion gap but is unlikely given the history
and normal lactate.
Normal anion gap metabolic acidosis may be due to loss of bicarbonate ions which
is replaced by chloride ions, a loss of sodium ions or an excess of chloride ions.
Causes can be classified into:
• Gastointestinal; such as diarrhoea, fistulae (pancreatic, ureters, biliary, small
bowel, ileostomy)
• Renal such as renal tubular acidosis and Addison’s
• Iatrogenic such as administration of normal saline solution
Hence option A, C and D would be differential diagnoses if the anion gap was
normal in this patient.
Badr A, Nightingale P. An alternative approach to acid–base abnormalities in critically ill patients. Contin
Educ Anaesth Crit Care Pain 2007; 7(4):107–11.
14. A Fluid bolus of 500 mL crystalloid and repeat studies
Cardiac output monitoring is increasingly more important in the management of
haemodynamically unstable patients on the intensive care unit. There are many
different options available including the invasive pulmonary artery catheter (PAC),
minimally invasive measurements including pulse contour analysis and oesophageal
doppler techniques and non-invasive methods (such as thoracic bio-impedance).
Answers
The most popular currently is a minimally invasive technique, requiring arterial
access for pulse-contour or pulse-power analysis. Two different types exist:
1. Trans-pulmonary dilution curve for calibration for increased accuracy of analysis
(e.g. PiCCO uses thermodilution to measure pulse-contour and LiDCO uses
lithium dilution to measure pulse-power);
2. No calibration is performed and therefore no central line is required. Analysis
of the arterial waveform is conducted by proprietary formulae, which are more
convenient but less accurate (e.g. FloTrac/Vigileo).
The readings above are from a minimally invasive device using trans-pulmonary
dilution curve analysis, which offer the advantages of accuracy comparable to a PAC
in addition to continuous waveform analysis. Cold or lithium injectate is injected
through the central line and the temperature or lithium concentration is measured
at an arterial line placed in a large artery (femoral or axillary).
The injectate mixes with the following before reaching the arterial line (Figure 3.5).
EVLW
EVLW
Cold injectate
LA
PBV
RA
RV
RA
:
RV
:
LA
:
LV
:
EDV :
GEDV :
ITBV :
RAEDV :
RVEDV :
PBV :
EVLW :
LAEDV :
LVEDV :
EVLW
Right atrium
Right ventricle
RAEDV
RVEDV
Left atrium
Left ventricle
End-diastolic volume
Global end-diastolic volume
GEDV
PBV
Intra-thoracic blood volume
Right atrial end diastolic volume
Right ventricular end diastolic volume
ITBV
Pulmonary blood volume
Extra-vascular lung water
Left atrial end diastolic volume
Left ventricular end-diastolic volume
EVLW
LVEDV
LV
LAEDV
Figure 3.5 Diagram demonstrating the blood volumes involved in calculation of PiCCO values.
From analysis of the dilution curve (Stewart-Hamilton Equation) one can calculate:
• Cardiac output
• Detection of volumes:
–– Global end-diastolic volume (GEDV) is a sum of all of the end-diastolic volumes
–– Intra-thoracic blood volume (ITBV) is the GEDV in addition to the pulmonary
blood volume (PBV)
–– Extra-vascular lung water (EVLW)
Continuous cardiac output monitoring is displayed after calculation of aortic
compliance (derived from blood pressure and blood flow recording simultaneously)
107
108
Chapter 3
and is also dependent on heart rate. Systemic vascular resistance index (SVRI) may
also be calculated using the following equation
SVRI =
80 × (MAP-RAP)
CI
Where:
MAP is mean arterial pressure
RAP is right atrial pressure
CI is cardiac index in dyn·s·cm−5·m−2
80 is a unit-conversion constant
ITBV (GEDV + PBV) may be used as a marker of cardiac pre-load, which may guide
volume therapy. EVLWI reflects the amount of pulmonary interstitial fluid. It does
not correlate well with oxygenation or chest radiograph lung opacification but does
reflect severity of illness and length of ventilation. Reducing the ITBV to normal
levels may reduce the EVLWI.
Most values are best looked at as a function of patient size and a therefore indexed
according to body surface area.
Referring back to our very sick and problematic patient, the decision tree that may
aid management is summarised in Figure 3.6.
The patient described above has a low cardiac output, reduced pre-load (ITBVI) and
is over-vasoconstricted (SVRI). The EVLWI is raised and the ventilation is deteriorating
muddying the management waters.
Efforts to exclude an ischaemic cause for shock is warranted and commencing
haemofiltration is important for modifying fluid balance once the inflammatory
cascade has settled, but both will help little with the haemodynamic compromise in
the immediate term.
The most appropriate intervention given the values above is more intravenous
volume administration, monitoring for an improvement in the cardiovascular status
CI
(c/min/m2)
<3
ITBV
(mL/m2)
>3
< 850
> 850
< 850
> 850
EVLWI
(mL/kg)
< 10
> 10
< 10
> 10
< 10
> 10
< 10
> 10
Treatment
+ Vol
+ Vol/Cat
Cat
Cat/-Vol
+ Vol
+ Vol
Good
– Vol
Figure 3.6 Decision tree using PiCCO monitoring. + Vol = volume loading; - V = volume reduction; Cat =
catecholamines/vasoactive agents.
Answers
including a higher MAP and decreasing noradrenaline requirements. If this fails
or if a further deterioration of the patient's ventilation occurs, an inotrope such as
dobutamine would be the next appropriate intervention.
Drummond K. Minimally invasive cardiac output monitors. Contin Educ Anaesth Crit Care Pain 2012;
12(1):5–10.
15. B Intubation and ventilation
This is a delayed presentation of paracetamol overdose with evidence consistent
with fulminant liver failure requiring urgent management. Paracetamol overdose is
the leading cause of acute fulminant (or hyperacute) liver disease in the UK.
90% of ingested paracetamol (N-acetyl-p-aminophenol) is metabolised by the
liver. In non-toxic doses the predominant metabolic pathway is via glucuronidation
and sulphation, with less than 10% metabolised by an alternative pathway via
cytochrome P450 to the toxic metabolite N-acetyl-p-benzoquinone imine (NAPQI).
In health, NAPQI is inactivated by glutathione.
This patient has taken a toxic dose of paracetamol which probably represents
> 150 mg/kg. The usual pathway of glucuronidation and sulphation are exhausted
and the cytochrome P450 represents an increased proportion of the metabolism.
Once glutathione reserves are depleted, unconjugated NAPQI exerts toxic
effects through hepatocellular damage. In this patient, the delayed presentation
has compounded this damage. A staggered overdose may also have a similar
presentation.
The management principles of a paracetamol overdose, as with other overdoses, is a
systematic ‘ABC’ approach with specific management to reduce absorption, increase
elimination and treat organ failure.
This patient is tachyponeic due to the profound underlying metabolic acidosis. He is
likely to tire from the work of breathing and his underlying problems are difficult to
assess and manage with the agitation, so intubation and ventilation is the next most
appropriate step.
Fulminant liver disease is consistent with a high cardiac output and low systemic
vascular resistance and may require vasopressor support. However, at present he
is not adequately fluid resuscitated and unlikely to tolerate an awake insertion of a
central line. Hence option A may become appropriate in his ongoing management
but not clinically indicated at present.
Unfortunately he has presented beyond the window for gastric decontamination
with activated charcoal; this should be considered within two hours of ingestion or
where a staggered overdose is suspected. He has correctly been started empirically
on N-acetyl cysteine (NAC), indicated by the severity of his overdose.
NAC increases glutathione reserves and hence enhances conjugation with NAPQI.
The dose is 150 mg/kg loading over 15 minutes, followed by 50 mg/kg over the
next 4 hours and 100 mg/kg over the subsequent 16 hours. Where a non-toxic dose
of paracetamol is suspected, waiting for 4 hours post ingestion paracetamol level
is appropriate and comparing with the new single line paracetamol treatment
nomogram.
109
110
Chapter 3
This patient clearly needs to be discussed with the local liver specialist intensive care
unit as an urgent priority. Once resuscitated, a liver transplant may represent his
only hope for survival. The King’s College Hospital Criteria for consideration for liver
transplantation in paracetamol overdose are:
Either:
• pH < 7.3 (or 7.25 if on NAC)
Or all of the following:
• Prothrombin time (PT) > 100 seconds (INR > 6.5)
• Creatinine > 300 μmol/L
• Grade 3 or above encephalopathy
He will require a urinary catheter to measure urine output. The cause for his agitation
is most likely his acidosis and possible encephalopathy. If the circumstances around
his overdose raised suspicion of trauma or collapse a CT head should be considered,
however at present is not an immediate action.
Maclure P, Salman B. Management of acute liver failure in critical care. Anaesthesia Tutorial of the Week
251. London: World Federation of Societies of Anaesthesiologists, 2012.
16. C Information from a bedside transthoracic echo
The incidence of pulmonary embolism (PE) is around 60–70 per 10,000, and more
than half occur in hospital. Prompt recognition and consideration of the diagnosis is
essential to prevent progression of the embolism and death.
Pulmonary embolism may be categorised into small, non-massive (or sub-massive),
and massive, the major difference being the degree of cardiac instability:
• A small PE is an embolism that does not cause hypotension or right ventricular
dysfunction
• A non-massive PE is one in which the patient remains normotensive but right
ventricular dysfunction can be demonstrated
• A massive PE is onme that causes right ventricular dysfunction and hypotension
In the majority of patients CT pulmonary angiography (CTPA) is the investigation
of choice. This is a contrast-enhanced scan, which is conducted rapidly (less than
one second) to avoid movement artifact due to respiration and cardiac pulsation
and reduce the radiation exposure, making it safe in pregnancy. A filling defect that
is seen in the pulmonary vasculature is diagnostic. The problem with this ‘snapshot’ image is that it gives little information over the course of the cardiac cycle. A
bed-side echo is essential for obtaining detailed information regarding pulmonary
artery pressures, right ventricular dysfunction and right atrial enlargement when
considering a potentially life-threatening intervention. In addition if the embolism
is intra-cardiac or within the proximal pulmonary artery it may be directly visualised
using this technique.
Returning to our scenario, the assumption is that this young lady has a massive
PE and that she is hypotensive as a result. There are relative and absolute
contraindications for thrombolysis.
Answers
Absolute contra-indications:
•
•
•
•
•
•
Previous intracranial bleeding at any time
Stroke within the last 6 months
Closed head or facial trauma within 3 months
Suspected aortic dissection
Uncontrolled high blood pressure (> 180 systolic or > 100 diastolic)
Known structural cerebral vascular lesion, arteriovenous malformations,
aneurysm or brain tumors
• Thrombocytopenia or known coagulation disorders
• Pericardial effusion
• Septic emboli
Relative contra-indications:
•
•
•
•
•
•
•
Current anticoagulant use
Invasive or surgical procedure in the last 2 weeks
Prolonged cardiopulmonary resuscitation
Pregnancy
Hemorrhagic or diabetic retinopathies
Active peptic ulcer
Controlled severe hypertension
This patient has several relative contraindications and in this critical situation these
factors will not help you make a final decision regarding the need for thrombolysis
as clearly a young healthy patient has everything to loose from not receiving
treatment. The CTPA may diagnose a PE (which appears clinically obvious) but the
patient must undergo a hazardous transfer and the scan takes valuable time to be
performed and reported. The test that will give most information at this stage is
the bedside echo which will visualise right ventricular dysfunction. This is seen as a
dilated ventricle equal or larger in diameter when compared to the left ventricle with
paradoxical septal movement, which in conjunction with hypotension means the
diagnosis is massive PE. The treatment is therefore thrombolysis and the sooner it is
administered the better.
van Beek EJR. Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism.
Contin Educ Anaesth Crit Care Pain 2009; 9(4):119–24.
17. B Test the patient for HIV
HIV testing remains a contentious topic. Recent guidance recommends that, where
possible, consent from the patient should be sought. However within the intensive
care environment, valid consent in a patient with capacity is challenging. HIV testing
can be performed without antecedent consent, where there is reasonable clinical
suspicion of HIV, and it is in the best interests of the patient. The prognosis following
a diagnosis of HIV is significantly improved with early diagnosis and treatment.
This man has recurrent pneumonia and his current episode is severe requiring
intubation. This should prompt the clinician to consider underlying diagnoses that
lead to immunosuppression including HIV. A HIV test is indicated in the clinical
111
112
Chapter 3
management of this patient. The result of the HIV test will impact on the length
of post exposure prophylaxis for the junior colleague, who sustained a needle
stick injury. However it must be emphasised, this is not the primary indication for
performing a HIV test in this patient.
Consent by the next of kin is not valid unless there is a lasting power of attorney
or advance directive in place. Assent can be gained from the next of kin in certain
situations such as the decision to perform a percutaneous tracheostomy. Due
to confidentiality issues surrounding the result of a HIV test, it is not appropriate
to request assent from the relatives to perform a HIV test. In the sedated patient
with no prior documented advance directive or lasting power of attorney, it is the
clinician’s role to act in the best interests of the patient.
This man has a severe pneumonia and it is currently unclear when he is likely to gain
capacity. It does not seem appropriate to wait for this, especially as this may delay
starting treatment in the presence of HIV.
Taegtmeyer M, Beeching N. Practical approaches to HIV testing in the intensive care unit. J Intens Care Soc
2008; 9(1):37–41.
Jones AB, Hughes A, Barton SE. Guidance on occupational-related HIV post-exposure prophylaxis (PEP) in
the intensive care setting. J Intens Care Soc 2012; 13(4):332–36.
British HIV Association (BHIVA). BHIVA Guidelines for HIV testing. London: BHIVA, 2008.
18. B Delay LSCS until ENT have performed surgical
tracheostomy
In this scenario there is a lot to consider. Your priority as the anaesthetist is the life of
the mother, even if you are under pressure from the obstetricians to save the baby.
Airway always comes first!
Although you have successfully managed to oxygenate the mother, a needle
cricothyroid puncture is not a definitive airway. Allowing the surgeons to proceed
with lower segment Caesarean section (LSCS) places the mother at further risk of
morbidity and mortality, especially if there is excessive bleeding intraoperatively.
Furthermore, there is still a risk of aspiration and you are not ventilating the mother,
as carbon dioxide clearance is not effective. There are the added risks of barotrauma
and surgical emphysema with the high pressures needed to pass gas through the
cannula, and the LSCS may take longer than expected.
The LSCS should be delayed until a definitive airway is placed, in this case a surgical
tracheostomy. As soon as the ENT surgeon has secured the airway, the obstetricians
should proceed with the Caesarean section. Hence, they should already be prepared
with the patient cleaned and draped as far as is feasible in this situation.
Performing a tracheostomy and Caesarean at the same time is not appropriate, as
it would not be possible to adequately deal with any complications occurring from
either surgical site without putting the mother in jeopardy. Again, airway always
comes first!
Completely abandoning the LSCS and waking the patient up would be correct if this
was an elective procedure; however, as this is an emergency it needs to go ahead
Answers
once the airway is secured. If there was a threat to the mother’s life, then it may be
necessary to proceed before ENT arrives.
Performing a spinal anaesthetic at this point would use up even more valuable time,
considering the tension of the situation.
There are many newer devices now available for emergency cricothyroidotomy that
are actually cuffed tubes. Whether it is appropriate to perform emergency surgery
using any of these is debateable and would very much be a case specific decision.
Rucklidge M, Hinton C. Difficult and failed intubation in obstetrics. Contin Educ Anaesth Crit Care Pain
2012; 2(2):86–91.
Morris S. Management of difficult and failed intubation in obstetrics. BJA CEPD Reviews 2001; 1(4):117–21.
19. D Sevoflurane
Anaesthesia for urgent surgery in the pregnant patient can be a challenge and the
maternal physiological changes of pregnancy must be considered in these cases.
Although anaesthetic drugs have not been shown to be teratogenic in clinical
doses, surgery occurring in the first trimester does have a high miscarriage rate.
The ideal time to perform urgent surgery is the second trimester, as the risk of
preterm labour increases as the pregnancy progresses. Elective surgery must be
postponed until at least six weeks after delivery. Obviously, if emergency surgery is
needed, it should not be delayed, and a discussion with obstetricians, surgeons and
paediatricians must take place to decide whether early delivery is necessary before
surgery.
The disease process and the associated pyrexia can cause preterm labour due to
uterine irritability. This risk is very high in both appendicitis and peritonitis. Nonintentional surgical interference with the uterus can also lead to preterm labour and
often laparoscopy may be the preferred technique.
Volatile agents reduce uterine tone and therefore actually help to reduce uterine
contractions. Therefore, sevoflurane is the least likely cause of this patient’s preterm
labour.
Nejdlova M, Johnson T. Anaesthesia for non-obstetric procedures during pregnancy. Contin Educ Anaesth
Crit Care Pain 2012; 12(4):203–6.
Walton NKD, Melachuri VK. Anaesthesia for non-obstetric surgery during pregnancy. Contin Educ Anaesth
Crit Care Pain 2006; 6(2):83–85.
20. E Proceed with surgery under general anaesthesia
supplemented with regional anaesthesia and admit postoperatively for apnoea monitoring
Prematurity, anaemia and gestational age less than 46 weeks are all risk factors for
postoperative apnoea in this patient. He is at significant risk of postoperative apnoea
regardless of anaesthetic technique, and should be admitted for postoperative
apnoea monitoring, making day case surgery inappropriate. The recent history of
obstructed hernia increases the risk of incarceration; therefore postponing surgery is
also not appropriate. The most appropriate anaesthetic management of this patient
113
114
Chapter 3
would be to proceed with surgery under general anaesthesia supplemented with
regional anaesthesia with postoperative apnoea monitoring due to his high risk of
apnoea.
Sale SM. Neonatal Apnoea. Best Prac Res Clin Anaesth 2010; 24:323–36.
Wilkinson KA, Gibson J. Anaesthesia for common conditions in infancy. Contin Educ Anaesth Crit Care Pain
2003; 3:79–82.
21. A Cerebral oedema
Diabetic ketoacidosis (DKA) is the leading cause of morbidity and mortality in
children with diabetes. Unlike in the adult diabetic population, the most common
cause of death in children with DKA is cerebral oedema, and a high index of
suspicion is always required. Risk factors associated with development of cerebral
oedema include:
•
•
•
•
•
•
•
•
•
Younger age
Newly diagnosed diabetes
> 40 mL/kg of fluid given in the first 4 hours
Bolus insulin therapy
Administration of hypotonic fluid
Raised serum urea
Initial pH < 7.1
Hypocapnia
Bicarbonate therapy
Cerebral oedema is a clinical diagnosis with varying signs and symptoms including
deterioration in neurological status, headache, cranial nerve palsies, bradycardia,
and hypertension. The patient was afebrile and did not present with headache or
neck stiffness, making meningitis unlikely. Hypokalaemia does not typically lead to a
reduced level of consciousness. Dehydration and exhaustion are also unlikely since
the patient was awake and alert on presentation, and had been fluid resuscitated
since.
If cerebral oedema is suspected then treatment should begin immediately using
either hypertonic saline (saline 3%, 3–5 mL/kg) or mannitol (0.5 g/kg or 2.5 mL/kg of
20% solution) while arranging for a CT scan. This should be repeated until a clinical
improvement in neurological status has occurred.
Steel S, Tibby SM. Paediatric diabetic ketoacidosis. Contin Educ Anaesth Crit Care Pain 2009; 9:194–99.
Wolfsdorf J, Craig ME, Daneman D, et al. Diabetic ketoacidosis in children and adolescents with diabetes.
Pediatr Diabet 2009; 10(suppl 1):118–33.
22. B Gabapentin 900 mg
There is now increasing evidence that perioperative gabapentinoids such
as pregabalin and gabapentin can reduce the incidence of chronic pain
postoperatively. Moderate evidence exists that shows their effect in acute pain.
Although ketamine has shown effects in reducing perioperative pain, this is not a
first line treatment and its evidence so far is less than that of the gabapentinoids.
Preoperative epidural analgesia was shown in a retrospective study to reduce
Answers
phantom limb pain but this was disproved by prospective trials. Morphine and
amitriptyline should only be used for treating pre-existing pain and gabapentin or
pregabalin are much safer drugs than amitriptyline due to the more tolerable range
of side effects and reduced incidence of adverse events.
Clarke H, Bonin RP, Orser BA, et al.The prevention of chronic postsurgical pain using gabapentin and
pregabalin: a combined systematic review and meta-analysis. Anesth Analg 2012; 115(2):428–42.
23. C Amitriptyline
Fibromyalgia is a chronic pain condition that can be very debilitating. Its key features
are pain of more than 3 months’ duration affecting the trunk and all four limbs (with
tenderness over at least 11 of 18 defined trigger points), sleep disturbance and
marked fatigue.
There is no cure, and treatment is aimed at control of symptoms. Like the
approach to any chronic pain presentation, the management should be holistic
and multidisciplinary. General non-pharmacological measures should include
patient education, support and motivation. They should be encouraged to take a
proactive role in their own management. Psychological therapies such as cognitive
behavioural therapy (CBT) and physiotherapy with regular exercise may contribute
towards overall well-being and hence towards improvement in symptoms.
Pharmacologically, drugs that affect the reuptake of serotonin and/or noradrenaline
in the central nervous system seem to be most useful. Of these, tricyclic
antidepressants (TCAs) such as amitriptyline are first choice. They have been found
to be effective not only in reducing pain, but also improving sleep, mood, muscle
stiffness, and fatigue. A suitable starting dose would be 5–10 mg at night, and this
can be increased over time as required. Duloxetine is a suitable alternative.
Other agents such as gabapentin have been used with mixed success.
Strong opioids are less effective but tramadol may be helpful. It acts at the spinal
level and inhibits the reuptake of serotonin and noradrenaline.
Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) may help and can
be used in addition to the agents discussed above, but are usually inadequate if
used alone.
Trigger point injections with local anaesthetic ± depot steroids may be of benefit in
some patients, but those with widespread pain will get short-term relief only in the
areas injected.
Dedhia JD, Bone ME. Pain and fibromyalgia. Contin Educ Anaesth Crit Care Pain 2009; 9(5):162–66.
Carville SF, Nielsen SA, Bliddal H et al. EULAR evidence-based recommendations for the management of
fibromyalgia syndrome. Ann Rheum Dis 2008; 67: 536–41
24. C 75 mg
Paracetamol is widely used, very effective and safe. The intravenous preparation
provides greater bioavailability than the oral route and is frequently administered
intraoperatively.
115
116
Chapter 3
However, overdose of intravenous paracetamol is being increasingly reported in
small children, infants and neonates. This has resulted in one fatality and significant
morbidity in several children. In most of these cases, there has been a miscalculation,
and up to ten times the recommended dose had been given.
In young children, dose miscalculation is an easy error to make and potentially more
hazardous than in an older child, as drug handling is different with different levels of
organ maturity.
In 2013, the MHRA and Royal College of Anaesthetists released dose
recommendations for paracetamol in children. This is summarised in Table 3.7.
Hence in a 10 kg patient, the correct dose of intravenous paracetamol would be 75 mg.
Table 3.7 Recommended doses of intravenous paracetamol in children
Weight (kg)
Safe administration dose
(mg/kg)
Safe maximum daily dose
≤ 10
7.5
30 mg/kg
10–33
15
60 mg/kg (maximum 2 g)
33–50
15
60 mg/kg (maximum 3 g)
> 50
1g
4g
Sharma CV, Mehta V. Paracetamol: mechanisms and updates. Cont Educ Anaesth Crit Care Pain 2014;
14(4):153–58.
MHRA Drug Safety Advice. Intravenous paracetamol (Perfalgan): risk of accidental overdose, especially in
infants and neonates. Drug Safety Update 2010; 3(12):2–3.
25. A Severe preoperative pain
Chronic post surgical pain (CPSP) is a significant complication of surgery, but
relatively little is known about its precise aetiology, mechanisms, or prevention.
There is no uniformly agreed definition, and this has led to variable reporting, with
unreliable figures of incidence or prevalence. Consequently, evidence regarding its
management and prevention is limited.
One definition of CPSP is pain of at least 2 months’ duration that develops after a
surgical procedure, and that cannot be explained by any other cause or pre-existing
pain problem. Several theories regarding its mechanism have been proposed, one
of which is of intraoperative nerve damage, leading to central sensitisation, but it
is acknowledged that not all patients who develop CPSP have had surgical nerve
damage, and not all those with nerve damage subsequently acquire CPSP.
Some associations have been found, leading to identification of certain factors that
may help to predict risk of developing CPSP (see Table 3.8).
Answers
Table 3.8 Risk factors associated with developing CPSP
Preoperative
Intraoperative (type of surgery)
Postoperative
• Severity and intensity of
preoperative pain
• Younger patients
• Genetic susceptibility
• Psychosocial factors
(such as fear of surgery,
depressive traits)
• Amputation
• Thoracotomy
• Inguinal hernia repair (repeat
surgery more than primary repair)
• Mastectomy
• Sternotomy
• Open rather than laparoscopic
technique
• Severe postoperative pain
• Additional interventions,
e.g. radiotherapy
In this scenario, the nature of the operation, an amputation, and the fact that the
patient had severe pain preoperatively both put him at increased risk of developing
CPSP.
It is unclear what can be done to prevent CPSP. Regional anaesthesia does not
seem to make a difference, but epidural analgesia commenced pre operatively and
continued into the post operative period may be a preventive measure. Adjuvant
agents such as ketamine and clonidine have been investigated, but cannot be
recommended at present for lack of robust studies. There is an increasing evidence
base suggesting that gabapentinoids such as gabapentin and pregabalin may
reduce the progression to postoperative chronic pain states.
Searle RD, Simpson KH. Chronic post surgical pain. Contin Educ Anaesth Crit Care Pain 2010; 10(1):12–14.
26. A Neuropathic pain requires a disease or lesion of the
somatosensory system to be present
The International Association for the Study of Pain (IASP) defines pain as “an
unpleasant sensory and emotional experience associated with actual or potential
tissue damage or described in terms of such damage.” It serves predominantly as a
protective function to body tissue. There are some important definitions used in the
description of pain states.
• Nociception – The sensation of noxious stimuli in the central nervous system. This
is different to pain, but is a component of pain symptoms
• Allodynia – Painful responses to normally painless stimuli
• Hyperpathia – Increased sensation from a sensory stimulus with a raised
sensation threshold
• Hyperalgesia – Exaggerated pain response to normally painful stimuli
• Dysaesthesia – An unpleasant abnormal sensation
• Paraesthesia –An abnormal sensation
• Chronic pain – Pain persisting beyond removal of stimulus and beyond the
period of time expected for healing and recovery
117
118
Chapter 3
• Neuropathic pain – Defined by the IASP as pain caused by a lesion or disease of
the somatosensory nervous system
• Complex regional pain syndrome – A chronic, painful condition that can
be either spontaneously occurring or due to nerve injury characterised by a
collection of sensory, vasomotor, sudomotor and trophic skin changes
Thus it is clear that of the options given, the most correct answer describes neuropathic
pain as requiring a disease or lesion of the somatosensory nervous system.
Merskey H, Bogduk N. Classification of chronic pain. Descriptions of chronic pain syndromes and
definitions of pain terms. Seattle, WA: IASP Press; 1994:209–13.
27. C Fluid requirement should be calculated as per the
Baxter formula: 4 mL/kg/% burn. Half the fluid should be
given in the first 8 hours and the remaining half over the
next 16 hours from the time of burn
Major burns cause a systemic inflammatory response syndrome resulting in
increased capillary permeability and large fluid shifts. It is therefore important to
maintain intravascular volume to ensure end organ perfusion. However, it should
be remembered that hypovolaemic shock in the first few hours following a burn is
never due solely to the burn and an alternative injury/source should be sought.
Two large bore IV cannulae should be inserted ideally through unburned skin.
The groins are often spared making femoral CVC access practical. However fluid
resuscitation should not be delayed if IV access through unburned skin is proving
difficult.
IV fluid resuscitation is required in adults if the burn involves more than 15% BSA or
10% with smoke inhalation.
There are various formulae that attempt to estimate the fluid deficit but these clearly
provide no more than a rough guide. The Parkland formula (also known as the Baxter
formula) is the most widely used. The modified Brooke formula (2 mL/kg/% burn in
the first 24 hours) can also be used but is less well known and was hoping to address
the issues of ‘fluid creep’.
Parkland formula: 4 mL/kg/% burn in the first 24 hours
Half of the fluid is given in the first 8 hours and the remaining half is given over the
next 16 hours.
The calculation should start from the time of the initial burn and not the time
of presentation to hospital. It is generally accepted that the fluid of choice is
Hartmann’s solution. Any pre-hospital fluid administered should be deducted from
the calculated requirement.
Given the volume of fluid often administered and the propensity of burns patients to
hypothermia, the Hartmann’s should be warmed. After the first 24–48 hours capillary
permeability should have returned to normal and fluid balance is much less of an issue.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–22.
Answers
28. A Increased preload, increased afterload
Application of aortic cross-clamp can cause significant rise in systemic blood
pressure. This is caused by an increase in left ventricular afterload, due to the cross
clamp. Reflex venoconstriction below the clamp, particularly in the splanchnic
circulation, causes an increase in the blood volume in the inferior and superior vena
cavae, hence causing increase in preload.
The change in afterload is consistent. The change in preload is variable when aortic
cross clamping is applied infrarenally, but is present in 90% of cases when the clamp
is applied above the coeliac arteries.
Gelman S. The pathophysiology of aortic cross-clamping and unclamping. Anesthesiology 1995; 82:1026–60.
29. A Creatinine kinase
This patient has presented with clinical features suggestive of rhabdomyolysis.
Rhabdomyolysis is a clinical spectrum, which occurs as a result of the breakdown of
striated muscle. The muscle degradation leads to elevated intracytoplasmic calcium,
which causes myocyte constituents to be released into blood, eventually leading to
acute kidney injury and hyperkalaemia.
The aetiology of rhabdomyolysis can be traumatic, including crush injuries,
electrocution or blunt trauma, or non-traumatic such as infection (legionella,
tetanus), drugs (cocaine, alcohol) or immune mediated (polymoyositis,
dermatomyositis).
Alcohol is thought to be involved in up to 20% of cases of rhabdomyolysis in the UK.
Alcohol-induced coma leads to prolonged immobilisation and muscle compression
with ischaemia. It also leads to myopathy and damages cell sarcolemma, increasing
sodium permeability. This influx of sodium activates the sodium-calcium exchange
pump, which increases cytosolic calcium along with direct influx of calcium due to
cellular damage.
It presents with a spectrum, from asymptomatic to hypovolaemic shock
accompanied with life threatening electrolyte imbalance and acute kidney injury.
Clinically, it is syptomised by malaise, muscle pains, fever and tachycardia.
Myocyte injury leads to severe hyperkalaemia, hyperuricaemia and
hyperphosphataemia, while muscle necrosis causes lactic acidosis, further
exacerbating the hyperkalaemia.
The most sensitive test for rhabdomyolysis is serum creatinine kinase (CK), an
enzyme released by striated muscle when damaged. An five-fold increase in serum
CK is expected in rhabdomyolysis. Serum CK concentrations greater than 5000 units/
litre are associated with a >50% incidence of acute renal failure.
High concentrations of myoglobin released can cause myoglobinuria, which is
responsible for the brown discolouration of urine. Routine dipstick test of urine
cannot differentiate between haemoglobinuria (haemoglobin in urine), haematuria
(red blood cells in urine) or myoglobinuria (haem-containing myoglobin in urine)
119
120
Chapter 3
as it detects presence of haem which is positive in all cases. As the liver normally
metabolises myoglobin rapidly, an absence of it in blood or urine does not eliminate
the diagnosis of rhabdomyolysis.
Treatment consists of prompt fluid resuscitation, control of hyperkalaemia and renal
support with filtration if indicated.
Hunter JD, Greeg K, Damani Z. Rhabdomyolysis. Contin Educ Anaesth Crit Care Pain 2006; 6(4):141-143.
30. A Ascorbic acid
This patient has clinical features suggestive of scurvy, caused by vitamin C (ascorbic
acid) deficiency. It is rarely seen in developed countries, except in extremes of age
most commonly due to malnourishment, but can occur due to dietary vitamin
C insufficiency. As vitamin C is an essential component for collagen synthesis it’s
deficiency leads to fragile capillaries, impaired wound healing, poor bone formation
and muscle symptoms. Administering a diet rich in vitamin C including products
such as citrus fruits, tomatoes and bell peppers can prevent it.
Iron deficiency leads to anaemia, which could cause lethargy, breathlessness and
palpitations.
Vitamin B1 or thiamine deficiency leads to beriberi, which is characterised, by heart
failure, oedema (wet) and neuropathies (dry).
Vitamin A deficiency leads to predominant visual symptoms including xeropthalmos
and blindness, while vitamin D deficiency leads to osteogenic defects such as rickets
disease and osteomalacia.
Raynaud-Simon A, Cohen-Bittan J, Guoronnec A, et al. Scurvy in hospitalized elderly patients. J Nutr
Health Aging 2010; 14(6):407-410.
Longmore M, Wilkinson I, Torok E. Oxford Handbook of Clinical Medicine, 8th ed. Oxford: Oxford University
Press, 2010.
Chapter 4
Mock Paper 4
Questions
1. A 32-year-old man is admitted to the intensive care unit. 2 weeks ago he suffered a
bout of gastroenteritis, following which he noticed bilateral leg pain and weakness
which then progressed proximally and he soon had difficulty coughing and
swallowing. Since admission he has been persistently tachycardic and sweaty with
episodes of hypertension and hypotension.
Which of the following clinical features is most likely to confirm his diagnosis?
A
B
C
D
E
Progressive areflexic weakness in more than one limb
Progressive rise in CSF protein levels > 0.4 g/L
Symmetrical weakness
Autonomic dysfunction
Bulbar palsy
2. A 44-year-old woman with a past history of hypothyroidism has suffered a
traumatic brain injury and is on the neurointensive care unit. She had an isolated
seizure following a blunt force to her cranium and remains intubated and
ventilated. She is clinically euvolaemic but her investigations reveal the following:
• Serum sodium 122 mmol/L (normal range 135–145 mmol/L)
• Serum osmolality 270 mOsm/kg (normal range 278–305 mOsm/kg)
• Urine osmolality 300 mOsm/kg (normal range 500–800 mOsm/kg)
Which of the following is the most likely cause of her biochemical derangement?
A
B
C
D
E
Hypotonic fluid administration
Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
Cerebral salt-wasting syndrome (CSWS)
Phenytoin administration
Myxoedema
3. You are asked to see a 60-year-old woman with a suspected myocardial infarction.
She is known to have a permanent pacemaker and implantable cardioverterdefibrillator (ICD). Shortly after arriving she suffers a cardiac arrest. The monitor
shows ventricular fibrillation.
Which of the following best describes the optimum position of the defibrillation
pads?
122
Chapter 4
A
B
C
D
E
Anterior-posterior position
Directly over the pacemaker
At least 8 cm from the generator position
Anterior-lateral position
No defibrillation pads should be applied
4. A 7-year-old child is experiencing breathing difficulties. After suffering from
coryza and a 3-day low-grade fever, his parents noticed a rapid deterioration in his
breathing overnight. He is now stridulous with a high-grade fever and is producing
copious secretions. He is lying flat, moving his neck freely and there is no response
to nebulised adrenaline and steroids.
What is the most likely diagnosis?
A
B
C
D
E
Epiglottitis
Viral croup
Bronchiolitis
Retropharyngeal abscess
Bacterial tracheitis
5. You are involved in a critical incident in the neuroradiology suite. A patient
undergoing an angiogram received a total of 7 mg/kg of plain lignocaine to
anaesthetise the groin for femoral arterial access. The patient then lost cardiac
output which returned following administration of intravenous lipid emulsion,
according to national guidelines. They have since been transferred to the intensive
care unit.
Which of the following describes your most appropriate action immediately after
the event?
A
B
C
D
E
Report the case to the NHS Commissioning Board Special Health Authority
Ensure that you have fully documented the event in the patient records
Contact your medical indemnity provider
Organise an ‘after action review’ with all personnel involved
Instigate the local reporting mechanism for critical incidents
6. An 80-year-old man for an open oesophagectomy has a cardiopulmonary exercise
test (CPET) as follows:
• Anaerobic threshold (AT) 10 mL/kg/min
.
• Peak oxygen consumption (V O2 max) is 75% of that predicted
When describing the results the most correct description includes:
A
B
C
D
E
His AT gives him a higher rate of complications
His AT
. gives him a higher risk of death
His V.O2 max max gives him a low risk of death
His V O2 max max is associated with the highest risk of complications
He should be nursed in intensive care postoperatively
Questions
7. A 76-year-old frail lady is undergoing an awake fibreoptic nasal intubation.
She received intravenous glycopyrrolate as an antisialagogue and midazolam
for anxiolysis. Her nasal mucosa was prepared with co-phenylcaine, and the
anaesthetist is using a “spray as you go” and nebuliser anaesthetic technique
with lignocaine. Remifentanil is used for sedation. She suddenly complains of
lightheadedness, tinnitus, confusion and peri-oral paraesthesia.
Which is the most likely drug responsible for her symptoms?
A
B
C
D
E
Glycopyrrolate
Midazolam
Lignocaine
Phenylephrine
Remifentanil
8. A 45-year-old man is brought to the emergency department following a 30 minute
out-of-hospital cardiac arrest. He has a return of spontaneous circulation, is
intubated, has a blood pressure of 110/60 mmHg, a heart rate of 80 beats per
minute in sinus rhythm, GCS 3/15, blood glucose 5 mmol/L and core temperature
of 34.6°C.
What is the most appropriate step to consider post-cardiac arrest management?
A
B
C
D
E
Transfer the patient to intensive care for further management
Start surface cooling with ice packs
Insert an arterial and central line
Call his family and discuss likelihood of poor prognosis
Start sedation and muscle relaxation
9. A 76-year-old man has undergone an arthroscopic acromioclavicular joint
decompression. He had an interscalene block and a general anaesthetic. His past
medical history includes obesity, moderate chronic obstructive pulmonary disease
(COPD) and obstructive sleep apnoea (not on CPAP). In the recovery room he is
awake, but struggling to breathe. He has four twitches and no fade to peripheral
nerve stimulation, and saturations are 96% on oxygen via facemask. There is
minimal wheeze on auscultation.
The best treatment is likely to involve:
A
B
C
D
E
Another dose of neostigmine reversal
Perform an arterial blood gas analysis
BiPAP until the block wears off
CPAP until opioid free
Nebulisers and steroids
10. A 70-year-old man is to have a number of tendons repaired in his hand. After
discussion with the patient, a regional anaesthetic technique has been agreed;
your preferred approach is an infraclavicular block under ultrasound guidance.
123
124
Chapter 4
Which part of the brachial plexus is most likely to be blocked by this approach?
A
B
C
D
E
Roots
Trunks
Divisions
Cords
Branches
11. A 20 kg 5-year-old is admitted to the emergency department with a fractured femur
following a bicycle fall. His leg was splinted prior to arrival and he received two
crystalloid boluses of 400 mL. His has a respiratory rate of 40 breaths per minute, a
capillary refill time of 4 seconds and heart rate of 160 beats per minute.
What is the next step in the resuscitation phase while waiting for surgery?
A
B
C
A further bolus of 200 mL of colloid
200 mL bolus of O negative blood
Call the transfusion lab and order crossmatched blood, fresh frozen plasma
(FFP) and platelets
D Change the temporary femoral splint to a plaster of paris cast
E Insert an arterial line
12. You are caring for a 35-year-old patient on the neurointensive care unit who has a
serious traumatic brain injury following an assault.
According to the Academy of Medical Royal Colleges 2008 Code of Practice for the
Diagnosis and Confirmation of Death, brainstem death should only be diagnosed
when:
A
B
The blood glucose is 4.0–8.0 mmo/L
Prior to an apnoea test the Paco2 must be 6.0-8.0 kPa and the arterial pH 7.20–
7.40
C Two complete sets of tests have been performed a minimum of 4 hours apart
D The serum sodium is > 124 mmol/L
E After 5 minutes of observed apnoea the Pao2 is < 8 kPa
13. A 47-year-old woman collapsed due to a grade 3 sub-arachnoid haemorrhage. An
extra-ventricular drain was inserted and she is ventilated on the intensive care
unit. On examination the blood pressure is 90/60 mmHg, heart rate is 110 beats
per minute and the peripheral capillary refill time is 6 seconds. She has passed
1000 mL of urine since catheterisation 4 hours ago.
What is the most useful course of action?
A
B
C
D
E
Insert a femoral central line and commence a noradrenaline infusion
Request urinary and plasma osmolarity measurements
Administer 20 mL/kg intravenous crystalloid
Request urinary sodium concentration measurement
Administer intravenous desmopressin (DDAVP) 0.4 mg.
Questions
14. A 67-year-old woman presents with an acute onset illness and progressive
physiological deterioration. She has a pyrexia of 39.7°C, a heart rate of 135 beats
per minute (in atrial fibrillation), a systemic blood pressure of 85/48 mmHg, a
respiratory rate of 28 breaths per minutes, oxygen saturations of 89% on a nonrebreathe reservoir face mask with oxygen at 15 L/min, is drowsy and has a
capillary blood glucose in 12.2 mmol/L.
The best choice of fluid type to bolus as a first step in cardiovascular resuscitation
would be:
A
B
C
D
E
0.9% sodium chloride
A balanced crystalloid
A gelatin solution
4.5% human albumin in 0.9% sodium chloride
A starch solution
15. A 54-year-old man with known alcoholic liver disease presents to the emergency
department with confusion. On examination he has stigmata of decompensated
liver disease and is oedematous with marked ascites. His respiratory rate is 30
breaths per minute, the oxygen saturations are 94% on air, his blood pressure is
90/60 mmHg and his heart rate is 120 beats per minute. After catheterisation he
produces 10 mL of urine in the first hour.
What would be the most useful investigation to establish the cause of his
confusion?
A
B
C
D
E
CT head
Rectal examination
Arterial blood gas
Renal function tests
Amylase
16. The cardiologists have inserted a temporary transvenous pacing wire in an 83-yearold man in the intensive care unit.
In which of the following scenarios is the urgent placement of a temporary cardiac
pacing system the best treatment option?
A
B
Verapamil overdose with shock
Incidental finding of a heart rate of 38 beats per minute, sinus rhythm with
a PR interval of 260 ms and very frequent, multifocal, supraventricular and
ventricular ectopic beats without shock
C Hyperkalaemia with shock
D A patient with a PR interval of 220 ms and left bundle branch block who
requires emergency surgery under general anaesthesia
E Second degree heart block with frequent pauses > 2 seconds associated with
syncope
125
126
Chapter 4
17. A 24-year-old primagravid woman presents in the anaesthetic antenatal clinic for
pre-assessment for a high body mass index (BMI). She is currently 26/40 pregnant
and already has a BMI of 49.
What is the best line of advice to give to her at this stage?
A
B
Lose weight before the due date
Early intravenous access, early epidural for labour and risk of difficult
neuraxial blockade or intubation in an emergency Caesarean section
C Early intravenous access, remifentanil PCA for labour and risk of difficult
intubation in an emergency Caesarean section
D Aim for normal delivery without any anaesthetic intervention
E Aim for normal delivery but be prepared for difficult epidural or spinal
anaesthesia if needed
18. A 5-year-old 20 kg girl is scheduled for an elective adenotonsillectomy for
obstructive sleep apnoea (OSA) as a day case. She has Trisomy 21. Her parents
inform you that she snores when she sleeps. A recent sleep study showed
significant periods of apnoea and desaturation, with an apnoea/hypopnoea index
of 12 (severe OSA). An echocardiogram done in her first year of life showed normal
intra-cardiac anatomy. Her thyroid function is also normal.
The most important preoperative preparation for this case is:
A
Check the full blood count for polycythaemia secondary to recurrent
desaturations
B Request a repeat echocardiogram
C Arrange an inpatient bed so that the patient can be admitted overnight for
respiratory monitoring postoperatively
D Prescribe a sedative premedication
E Apply local anaesthetic cream to potential sites for intravenous access
19. A 38 kg 14-year-old girl is in recovery after scoliosis correction surgery. Apart from
idiopathic scoliosis, there is no other past medical history of note and no known
drug allergies. She was given 7 mg of morphine near the end of surgery, and was
started on a morphine patient controlled analgesia (PCA) with 1 mg bolus doses, 5
minute lock-out time, and 1 mg/hour background infusion.
After 4 hours of observation in recovery, she appears drowsy, but responds to
voice. Her respiratory rate is 10 breaths per minute. On 2 L/min of oxygen via nasal
cannulae her oxygen saturation is 96%. Her pupils measure 2 mm bilaterally, and
are equally reactive to light.
The PCA pump shows a total of 18 mg of morphine had been delivered with the
most recent patient requested bolus an hour ago.
The most appropriate immediate action is:
A
Inform the ward to keep her on oxygen to maintain Spo2 over 94%
Questions
B
Give a 2 µg/kg bolus dose of naloxone and repeat if necessary and reduce PCA
bolus and background doses
C Keep her in recovery for further observation
D Request an arterial blood gas analysis from the arterial line
E Ask the patient not to use the PCA for the next hour
20. A 4-year-old 18 kg boy fractured his left forearm and was put on the emergency
theatre list for a manipulation under anaesthesia (MUA) and K-wire insertion.
After induction of anaesthesia with fentanyl, propofol and atracurium, a
laryngeal mask airway was inserted and the patient ventilated on oxygen, air
and sevoflurane. You gave him 540 mg of co-amoxiclav intravenously. A few
minutes later, his heart rate increased from 100 to 160 beats per minute, his
oxygen saturation drops from 100% to 97% on 50% oxygen, and you cannot get
an automated blood pressure reading. You noticed on auscultation that he has
bilateral wheeze and a rash appears around the patient’s neck, arms and torso.
Your first immediate action is:
A
B
C
D
E
Increase the inspired oxygen concentration to 100%
Give chlorpheniramine 2.5 mg intravenously
Give an intravenous fluid bolus of 20 mL/kg 0.9% saline
Give adrenaline 10 µg/kg intramuscularly
Give epinephrine 1:10 000, 1 µg/kg intravenously
21. An 86-year-old woman is on the trauma list for a hemiarthroplasty following a
mechanical fall. She weighs 45 kg and can manage two flights of stairs. Her ECG
is unremarkable and a recent echocardiogram showed preserved left ventricular
function with no significant valvular defects. Bloods show a haemoglobin of 101
g/L, platelets of 200 ×109/L, normal coagulation studies and her creatinine is 87
μmol/L. She has a past medical history of hypertension, hypercholesterolaemia
and ischaemic heart disease. She takes aspirin, clopidogrel, bisoprolol, ramipril
and atorvastatin.
What would be the most appropriate way to manage her postoperative pain relief?
A
Combined spinal and epidural anaesthesia. Placing 2.5 mL of heavy 0.5%
bupivacaine and 300 µg of diamorphine intrathecally and using standard low
dose mixture as a patient controlled epidural analgesia in the postoperative
phase
B Spinal anaesthesia with 2.8 mL of heavy 0.5% bupivacaine. Regular intravenous
paracetamol 1g 6 hourly and tramadol 50 mg up to 6 hourly as required for
breakthrough pain
C General anaesthesia with a lumbar plexus block. Regular oral paracetamol 1g
6 hourly and ibuprofen 400 mg up to 8 hourly as required for breakthrough pain
D General anaesthesia with a fascia iliaca block. Regular oral paracetamol 1 g
6 hourly and immediate release morphine 5–10 mg up to 4 hourly as required
for breakthrough pain
127
128
Chapter 4
E
General anaesthesia with no regional component. Regular oral paracetamol 1 g
6 hourly and ibuprofen 400 mg 8 hourly with a morphine PCA
22. A 75-year-old man with severe debilitating osteoarthritis in both knees presents
with worsening pain despite treatment with multiple analgesic medication
including paracetamol, ibuprofen, oral morphine sulphate and buprenorphine
patch. He is unfit for surgery, but is keen to try acupuncture for symptomatic relief.
Which of the following would preclude his use of acupuncture?
A
B
C
D
E
Insufficient Qi
Cellulitis over needle insertion site
Local anaesthetic hypersensitivity
Abnormal anatomy
Use of buprenorphine patch
23. A 62-year-old woman presents with severe episodes of pain in the distribution
of the right mandibular branch of the trigeminal nerve. The attacks are usually
precipitated by cold wind and are short lived. She has no relief from paracetamol
or tramadol, and is on no other medication.
What would be the most appropriate first line treatment?
A
B
C
D
E
Carbamazepine
Microvascular decompression
Percutaneous trigeminal continuous radiofrequency neurotomy
Gabapentin
Glycerol gangliolysis of the Gasserian ganglion
24. A 70-year-old patient develops pain after a stroke. He has weakness and sensory
loss of his right arm and leg.
Which feature of his pain is most accurate:
A
B
C
D
E
Morphine is a good choice of analgesia for the acute phase
Pain as a result of the stroke is rare
He is unlikely to develop allodynia
Pain usually occurs in an area of altered sensation
A thalamic lesion has lead to his post-stroke pain
25. A 73-year-old man with advanced pancreatic cancer presents with worsening
upper abdominal pain. Despite treatment with opioids and adjuvant medication,
he has no pain relief and is being considered for a procedural intervention.
Which of the following procedures is the most appropriate option for this patient?
A
B
C
D
E
Thoracic epidural injection
Coeliac plexus block
Lumbar sympathetic plexus block
Superior hypogastric plexus block
Sphenopalatine ganglion block
Questions
26. A 40-year-old man is fast-tracked through the emergency department with a
penetrating eye injury. He is haemodynamically stable, has no other injuries,
no past medical history and has not been fasted. He needs to undergo an urgent
operation and you are due to perform the anaesthetic.
Which of the following drugs should be avoided in this patient?
A
B
C
D
E
Suxamethonium
Thiopentone
Rocuronium
Propofol
Ketamine
27. You are called to review an 82-year-old man with type 2 diabetes in recovery. He
underwent an uneventful right common femoral and popliteal angioplasty and
stenting in the endovascular radiology suite. The procedure took approximately 8
hours. The nurse is concerned because he continues to ooze from the right groin
despite continuous application of pressure on the wound site.
What would be the next step in diagnosing the potential cause of his ongoing
bleeding?
A
B
C
D
E
Check his haemoglobin
Perform an arterial blood gas
Check his blood sugar
Check activated clotting time (ACT)
Check his core temperature
28. A 23-year-old man for elective foot surgery is to have a popliteal nerve block for
postoperative analgesia. You use an ultrasound-guided technique and infiltrate
20 mL of 0.5% bupivacaine.
Which of the following nerve fibre modalities is most likely to be blocked first once
the local anaesthetic has been infiltrated?
A
B
C
D
E
Touch and pressure
Motor
Pain and temperature
Preganglionic autonomic
Proprioception and muscle tone
29. A 78-year-old patient is admitted to the intensive care unit (ITU) following an
exacerbation of chronic obstructive pulmonary disease (COPD). He has known
prolonged QTc syndrome. His list of medications includes salbutamol, nifedipine
for hypertension, glyceryl trinitrate for ischaemic heart disease and digoxin and
warfarin for atrial fibrillation. Whilst on the ITU he requires an amiodarone
infusion for fast atrial fibrillation (AF) and intravenous cefuroxime for a suspected
chest infection. He has now developed ‘torsades de pointes’ syndrome.
129
130
Chapter 4
Which one of his medications would most likely have been responsible for the
dysrhythmia?
A
B
C
D
E
Salbutamol
Nifedipine
Digoxin
Amiodarone
Cefuroxime
30. Two days following a right hemicolectomy for bowel carcinoma, a 64-year-old man
develops breathlessness and pleuritic chest pain. His observations reveal:
•
Pulse rate of 88 beats per minute
•
Blood pressure of 120/74 mmHg
•
Oxygen saturation of 94% on 2 L/minute of oxygen
His heart sounds are normal and chest sounds are clear.
Which one of the following investigations would be the most appropriate to
confirm a diagnosis in this scenario:
A
B
C
D
E
12-lead ECG
CT angiography
Transoesophageal echocardiography
Serum D-dimer
Arterial blood gas
Answers
Answers
1. A Progressive areflexic weakness in more than one limb
The history described is classical of the development of Guillain–Barré syndrome.
Guillain-Barré syndrome is a progressive, infective, demyelinating neuropathy. It has
an incidence of 1–2 per 100,000 and usually has a precursor of gastric or respiratory
viral illness in its history. Diagnostic features are progressive weakness accompanied
by areflexia in more than one limb. Features that support identification of the
syndrome include symmetry of limb signs, cranial nerve involvement, respiratory
muscle weakness, autonomic dysfunction, mild sensory symptoms and the
investigative findings of increasing cerebrospinal fluid (CSF) protein levels (> 4.0 g/L)
over subsequent days or slowed nerve conduction studies. Therefore the most
relevant diagnostic clinical feature in this patient is progressive areflexia in more
than one limb.
Pollard BJ. Handbook of Clinical Anaesthesia, 2nd edn. Philadelphia: Elsevier, 2003.
Singer M, Webb AR. Oxford Handbook of Critical Care, 2nd edn. Oxford: Oxford University Press, 2005.
2.B Syndrome of inappropriate antidiuretic hormone
secretion (SIADH)
Sodium and water go hand in hand to maintain intravascular homeostasis. Serum
osmolality is predominantly dictated by sodium concentration, and the control of
sodium is a powerful determinant of water distribution. If the serum osmolality
increases, hypothalamic osmoreceptors signal the production of antidiuretic
hormone (ADH, vasopressin) to reduce water excretion and thereby rectify the
imbalance. Total body sodium itself, is controlled by the sympathetic nerves and
natriuretic peptides that govern its renal reabsorption once it has been filtered at the
glomerulus.
Hyponatraemia can be classified as a serum concentration < 135 mmol/L and
may be associated with hyper-, hypo- or euvolaemia. The most common causes
of hyponatraemia in a brain injured patient are syndrome of inappropriate ADH
secretion (SIADH) and cerebral salt-wasting syndrome (CSWS).
SIADH leads to unregulated ADH release and lack of feedback response such that
water is indiscriminately reabsorbed. It is characterised by:
1.
2.
3.
4.
5.
Serum sodium < 135 mmol/L
Reduced serum osmolality < 280 mOsm/kg
Urine osmolality greater than serum osmolality
Low urine output
Normovolaemia (occasionally hypervolaemia)
Treatment includes fluid restriction, furosemide (to encourage water excretion) and
demeclocycline (to inhibit renal ADH response, or direct ADH receptor antagonists).
131
132
Chapter 4
CSWS is not fully understood but is associated with increased natriuretic peptides
and ultimately involves increased renal sodium loss and subsequently, water is lost
in tandem. It is characterised by:
1.
2.
3.
4.
5.
Normal or low serum sodium
Normal or low serum osmolality
Normal or high urine osmolality
Normal or high urine output
Hypovolaemia
Treatment involves replacement of sodium and water. This is usually commenced
with 0.9% saline solution but hypertonic 1.8% or 3% solutions may be required if the
loss has been acute and the patient is symptomatic.
The negative fluid balance is usually the distinguishing feature between CSWS and
SIADH, but can be hard to assess clinically. Very infrequently CSWS can biochemically
masquerade as SIADH. In this instance the induced hypovolaemia is such that it
results in a consequential rise in ADH.
Iatrogenic hyponatraemia can be seen after hypotonic fluid infusions or as the side
effect of some medications such as anticonvulsants, especially carbamazepine and
phenytoin.
Systemic disease, such as hypothyroidism, can also be associated with
hyponatraemia. Hypothyroid coma or myxoedema is rare but may be triggered by
trauma, particularly in the absence of replacement medication.
SIADH is therefore the most likely cause from the options given.
Bradshaw K, Smith M. Disorders of sodium balance after brain injury. Contin Educ Anaesth Crit Care Pain
2008; 8(4):129–133.
3. C At least 8 cm from the generator position
The patient has a shockable rhythm and requires defibrillation immediately.
In patients with an implantable cardioverter-defibrillator (ICD) or permanent
pacemaker, it is important not to delay defibrillation; the ICD may not be functional
or failed to have detected the dysrhythmia.
Although the strength of evidence is low, the pad should be placed at least 8 cm
from the generator; it is possible that automated external defibrillator (AED) devices
may sense pacing spikes and so not detect ventricular fibrillation (VF). The other pad
can then be placed in the lateral position or the posterior position. Placement of
defibrillation pads over the pacemaker/ICD may cause subsequent malfunction of
the device and should be avoided.
Resuscitation Council (UK). Adult Resuscitation Guidelines. London: Resuscitation Council (UK), 2010.
4. E Bacterial tracheitis
Certain childhood respiratory tract infections have the potential to progress
to life threatening airway obstruction if they are not diagnosed and managed
correctly. Children with acute severe stridor represent an anaesthetic challenge as
Answers
any agitation from the child might precipitate complete obstruction. Intravenous
cannulation and throat examination in this scenario should therefore not be
attempted. Early, experienced anaesthetic and ENT involvement is recommended
and the priority is to examine and secure the airway under anaesthesia.
Bacterial tracheitis is a rare but life threatening condition commonly caused
by Staphylococcus aureus and characterised by subglottic oedema with thick
mucopurulent secretions compromising the airway. Typically, the child experiences
viral upper respiratory tract prodromal symptoms for 2–3 days which is followed by a
rapid clinical deterioration over 8–10 hours. At this stage the child may appear toxic,
stridulous and have a high fever as described in the above case. A distinguishing
feature from epiglottitis is the usual ability of the child to lie flat and the absence of
drooling and dysphagia.
Croup is the most common cause of acute stridor in children but usually affects
younger age groups (6 months to 3 years). Commonly caused by the parainfluenza
virus family, sufferers classically display a barking cough preceded by a prodrome of
nasal congestion and rhinorrhea. The deterioration is not as marked as in bacterial
tracheitis and copious secretions are not typical features. Furthermore, children
often want to sit upright as opposed to lie flat and may show a marked clinical
improvement following nebulized adrenaline and steroids.
Since the introduction of the Haemophilus influenzae type b vaccine, epiglottitis
has become rare. Epiglottitis normally affects children aged 2–6 years and usually
presents abruptly with a high fever, dysphagia, stridor and drooling. The child may
prefer leaning forwards with their mouth open to keep their airway open. The
presence of antecedent viral symptoms, current secretions as well as the child’s
position in the case above makes epiglottitis not the most likely diagnosis.
A retropharyngeal abscess arises in the space between the posterior pharyngeal
wall and prevertebral fascia and can cause airway obstruction by physical expansion.
The abscess can be formed after a penetrating pharyngeal injury or infected lymph
nodes associated with an upper respiratory tract infection. Crucially these patients
commonly complain of limited neck movement contrary to the above scenario.
Bronchiolitis is a common and usually self-limiting lower respiratory tract infection
caused by the respiratory syncytial virus. Children under 2 years old are most
commonly affected and present acutely with rhinorrhea, cough and a low grade
fever preceded by a prodrome of several days. Since it is a lower respiratory tract
infection, stridor is not usually present. Treatment is supportive and includes oxygen
and intravenous fluid therapy as needed. Conflicting evidence remains as to the
effectiveness of steroids and nebulised adrenaline in treating this condition.
Maloney E, Meakin G. Acute stridor in children. Contin Educ Anaesth Crit Care Pain 2007; 7(6):183–186.
Rafei K, Lichenstein R. Airway infectious disease emergencies. Pediatr Clin North Am 2006; 53(2):215–242.
5.B Ensure that you have fully documented the event in the
patient records
Clinical risk management is at the centre of ensuring patient safety and may be
prospective or retrospective. Prospective management can be at an individual level,
133
134
Chapter 4
e.g. planning a patient-specific anaesthetic, or at a department level to comply with
Clinical Negligence Scheme for Trust (CNST) regulations. In order to manage risk
there are five sequential stages of process to be completed.
1.
2.
3.
4.
5.
Awareness
Identification
Assessment
Management
Re-evaluation
Awareness
A critical incident or Patient Safety Incident (PSI) is that which could or did cause
harm, be it unexpected or unintended. It has been reported in the literature that up
to 50% of PSIs are preventable.
Identification
Risk is identified in several ways. Local incident reporting mechanisms, by clinical
staff or patients, and national data from the NHS Commissioning Board Special
Health Authority, formerly the National Patient Safety Agency (NPSA), serve to
highlight threats. Case note review is fundamental for recognition and education
regarding events. Root cause analysis (RCA) provides a more formal and structured
investigation to identify failings in a system.
RCA is undertaken by a team of risk managers including clinicians and, on occasion,
lay people. RCA aims to analyse each case thoroughly from documented data (from
the whole admission), construction of accurate timelines and personnel contribution
to an event, and subsequent interrogation of all information collected to identify
the cause. It detects barriers to safe practice which are classified as physical, natural
(temporal or distance related), human action and administrative.
Assessment
Identified risk can then be scored according to its potential severity and frequency.
This enables a trust to stratify its resources accordingly for the prevention of risk
recurrence.
Management
This describes the arrangements implemented to reduce the risk to as low a level
as possible. It involves improving those barriers to patient safety identified through
RCA. At a local level it may be prudent to hold an after action review (AAR). This
is an informal discussion between the staff involved in an incident. It is led by an
independent and objective facilitator with the aim of identifying problems and
improvements without the allocation of blame.
Re-evaluation
This is essential in order to confirm the absence of renewed risk in light of any
changes made. Although all of the options are applicable to action following a
Answers
critical incident, full contemporaneous documentation provides the basis of all
further risk analysis.
Bould M, Hunter D, Haxby E. Clinical Risk Management in Anaesthesia. Contin Educ Anaesth Crit Care Pain
2006; 6(6):240–43.
6. B His AT gives him a higher risk of death
Cardiopulmonary exercise testing (CPET) is no longer the reserve of research labs or
specialist centres, and is now widespread. The detailed physiological data produced
gives a wealth of information, the correct use and interpretation of which takes skill
and experience. Whilst not expecting this standard of candidates, the examiners
have recently demonstrated their willingness to scrutinise candidates on the subject.
Risk stratification is an ever-changing topic, and thus there are several factors
one has to consider in terms of any question on the subject. Firstly a thorough
history and patient examination are a sound foundation, and from there one can
incorporate the information into relevant scoring systems such as the ASA, Goldman,
Lee and Detsky. Frequently, these give a figure based on single organ, especially
cardiac, demise. A detailed history to reveal functional ability is an essential tenet
of any pre-assessment and this can be assimilated into a tool such as the Duke
Activity Index. Unfortunately the revealed levels of activity may not truly reflect
ability and history is subject to bias and recall error. So, in search of more objective
data we arrive in the arena of testing. The traditional tests of function, such as
echocardiography and spirometry give limited data as they are non-dynamic tests
performed at rest.
In addressing this need for another functional test, CPET has evolved into the gold
standard for objective functional assessment and measurement.
Performing the test
The test requires two staff and special equipment. One member of staff will attend
to and coach the patient whilst the other attends to the data and testing equipment.
The equipment has two parts; a fixed exercise cycle, the resistance of which can
be adjusted by the control computer to increase or decrease the work done by the
patient. The other element is the metabolic cart, which is formed by a facemask
with a gas analyser to measure oxygen use, carbon dioxide evolution, and a
pneumotachograph to quantify gas flows and volumes. A 12-lead ECG is also
connected to the computer of the cart which assimilates all the gas and ECG data to
produce live displays of results alongside a continuous ECG with ST segment analysis.
Pre-test, the exercise bike seat has to be adjusted for height and the facemask straps
adjusted and tested for a good seal. A Spo2 probe is attached and a non-invasive
blood pressure (NIBP) cuff fitted alongside the 12-lead ECG. The patient then enters
the warm up phase, pedalling unloaded at 60 rpm, while baseline spirometry
is performed. This unloaded phase continues into the first 3 minutes of testing,
followed by sequential increased loading to the pre-calculated ramp protocol. At
the end of the test the patient has a cool down period, and remains monitored for a
further 10 minutes to observe recovery.
135
136
Chapter 4
Safety
The quoted mortality of the test is in the region of three patients per 100,000 tests,
and full resuscitation facilities must be immediately available. Certain conditions
preclude testing, such as severe or unstable cardiac/respiratory conditions,
thrombosis and dissection and those conditions which may preclude cooperation
such as mental disabilities. Whilst wearing the facemask patients cannot talk, so a set
of previously agreed signals are used to indicate fatigue and chest pain.
Measurements and results
.
Gas exchange. measurements include oxygen consumption (Vo2), carbon dioxide
production (Vco2), and the respiratory exchange ratio (RER). Ventilatory measures
of respiratory rate, minute ventilation (VE) and tidal volume (VT) are taken, as are
cardiovascular parameters of NIBP, ECG, heart rate and oxygen pulse (Vo2/hour).
Pulmonary exchange calculations can be taken from the ventilatory equivalents for
O2, CO2 and Spo2.
Cardiac output
.
The oxygen pulse Vo2/hour, is an approximation of stroke volume. Increased work
requires more oxygen to fuel energy usage, and so oxygen consumption
increases.
.
Cardiac output is seen to increase in a linear fashion alongside V
o2, until a peak
.
oxygen extraction ratio of 75% is reached. The gradient of the Vo2 increase is a
measure of the exercise driven increase in cardiac output.
.
Anaerobic threshold/Vo2 max
This oft quoted measure is a marker of the efficiency of the cardiorespiratory system.
It is also largely unchanged with age, and is unaffected by effort or motivation and is
reliable and repeatable for a given patient.
The anaerobic threshold (AT) gives a value for the point at which the oxygen
demand outstrips supply as work increases, and therefore anaerobic respiration is
evoked. The production of lactate generates
an extra acid load to the system and
.
(V
co
).
Thus
the AT is the inflection point of a
thus increases
the
production
of
CO
2
2
.
graph of Vco2against O2. In other terms, the AT is also the point at which the RER rises
above 1, and is the lowest point on the plot of ventilatory equivalents for oxygen.
Patients can exercise. well beyond their. AT, and in most tests this represents roughly
the half way mark. Vo2 max, is the peak Vo2 usually measured at the time the test is
terminated.
It is should be remembered that the variables discussed are part of a whole testing
package and a raft of results which should ideally not be considered in isolation. The
results can be considered to be interlinked in physiological terms and in terms of
complications. For example a complication can give rise to mortality if of sufficient
severity.
The AT is shown to correlate with mortality, and the key ‘cut off’ figure in this
regard is considered to be. 11 mL/kg/min. Thus he has a higher risk of inpatient
postoperative mortality. Vo2 max has more often been shown to correlate with
Answers
complications, but as alluded to the delineation .between morbidity and mortality
is not always established in studies. However, a VO2max of < 60% predicted is known
to be associated with both of these bad outcomes. The AT certainly suggests the
patient would benefit from critical care postoperatively, but in most centres this
would be normal for other oesophagectomy patients as well.
Agnew N. Preoperative cardiopulmonary exercise testing. Contin Educ Anaesth Crit Care Pain 2010; 10
(2):33–37.
7. C Lignocaine
Awake fibre-optic intubation is an invaluable anaesthetic tool to help safely manage
patients with difficult airways. Its successful execution requires not only familiarity
with handling of the scope, but also effective sedation and topical anaesthesia.
Multiple agents are frequently given to optimise the intubating conditions and an
awareness of common or serious side effects of these drugs is important.
When anaesthetising the airway, it is important to keep a close track of the amount
of local anaesthetic administered to prevent inadvertent drug toxicity. Lignocaine is
frequently given in different concentrations via various routes and is also present in
co-phenylcaine which is sometimes not appreciated. In practice, not all patients are
weighed, and caution should be exercised when administering local anaesthetics
in the elderly. Lignocaine is a sodium channel blocker and during systemic toxicity,
firstly inhibits the inhibitory central nervous system neurons which manifests as
confusion, tinnitus and paraesthesia before culminating in convulsions. As further
toxicity ensues, a more global central inhibition occurs which results in the loss of
consciousness and respiratory depression. Negative inotropy and dysrhythmias
which are difficult to treat may also be seen at this stage. The British Thoracic Society
recommends that the total dose of lignocaine applied during bronchoscopy should
be limited to 8.2 mg/kg. Local anaesthetic toxicity is the most likely answer in the
above case in view of the specific excitatory symptoms occurring after multiple
administrations of lignocaine to the elderly patient.
Glycopyrrolate is an anti-cholinergic drug which is frequently used to reduce the
amount of secretions produced in the patient’s upper airway to aid visualisation
during bronchoscopy. Anticholinergics act by competitive antagonism at the
muscarinic acetylcholine receptor and toxic central effects include agitation,
delirium, hallucinations and seizures. Glycopyrrolate however, has a quaternary
ammonium group and therefore does not cross the blood-brain barrier as freely
as other anticholinergics such as atropine or hyoscine. Central effects are therefore
minimal.
Midazolam is a short acting benzodiazepine which produces amnesia, anxiolysis and
sedation. Paradoxical excitement can occur, although this is very rare, and not the
most likely explanation for the above scenario.
Phenylephrine is found in co-phenylcaine and provides vasoconstriction to the
nasal mucous membrane via α1agonism. Absorption across the mucous membrane
can occur which may cause hypertension and reflex bradycardias. Central nervous
system effects are unusual and not the most likely cause for the symptoms in the
above case.
137
138
Chapter 4
Remifentanil is an ultra-short acting synthetic pure μ-receptor opioid agonist
commonly used as a sedative, analgesic and antitussive agent during awake fibreoptic intubations. Central nervous system effects include respiratory depression,
drowsiness and reduced psychomotor functioning. Excitatory symptoms seen in the
case above are rare.
British Thoracic Society. Guidelines on diagnostic flexible bronchoscopy. Thorax 2001;56 (Supp 1):1–22.
Williams K, Barker G, Harwood R, Woodall N. Combined nebulization and spray-as-you-go topical local
anaesthesia of the airway. BJA 2005; 95(4):549–553.
Peck T, Hill S, Williams M. Pharmacology for Anaesthesia and Intensive Care. 3rd ed. Cambridge: Cambridge
University Press, 2008.
8. E Start sedation and muscle relaxation
Therapeutic hypothermia is now recommended by NICE for all patients following
a cardiac arrest that resulted in return of spontaneous circulation. This treatment
has potential to reduce the burden of neurological disability that is associated
with survival post cardiac arrest. However, recent evidence suggests that it is the
targeting of temperature management, rather than the specific temperature chosen
that confers neurological benefit. This may begin a new shift in the understanding
and management of therapeutic hypothermia in post-cardiac arrest patients.
Insertion of invasive monitoring and transferring the patient to intensive care are
important steps in the management of this patient. Early discussion with the family
is appropriate but discussing the prognosis might be premature in light of the
circumstances.
The priority at this point would be to commence sedation to reduce his cerebral
metabolic rate (CMRO2) and administer muscle relaxation to minimise rises in
intracranial pressure secondary to shivering, coughing and gagging.
Peberdy MA, Callaway CW, Neumar RW, et al. Post cardiac arrest care: 2010 AHA guidelines for
cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010;122: s768–S786.
Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after
cardiac arrest. N Engl J Med 2013; 369(23):2197–206.
9. C BiPAP until the block wears off
There are a variety of ways to block the brachial plexus principally to facilitate
surgery to the upper limb. The type of block is named in reference to the anatomical
location where the block is performed. Each approach to block the brachial plexus
has its advantages and disadvantages with an associated clinical relevance:
Interscalene – This is the most proximal block of the plexus as it arises between
the scalene muscles of the neck. This block produces good coverage for distal
clavicle, shoulder and proximal upper arm procedures. Interscalene blocks are often
unpredictable for forearm and hand procedures due to common ulnar (C8 & T1)
sparing at this level.
A reliable complication is unilateral phrenic nerve blockade, unless low volumes or
a low neck insertion site are used. The resultant hemidiaphragmatic paralysis can
produce respiratory difficulties in those with airway or chest disease, the obese,
Answers
or those with contralateral phrenic nerve palsy (which is often asymptomatic).
Other complications include a Horner’s syndrome from sympathetic stellate
ganglion blockade, epidural or spinal spread, laryngeal nerve block, and vertebral
artery injection. The migration of local anaesthetic into cerebrospinal fluid (CSF),
presumably via the dural cuff of a nerve root, can result in a total spinal anaesthetic.
However, at least four cases of direct injection into the cervical spinal cord have also
been documented, associated with devastating permanent neurological damage.
Supraclavicular – This is mainly considered as blockade focussed at the brachial
plexus mid-point, as the plexus passes behind the clavicle and in relation to the
subclavian artery in the supraclavicular fossa.
A supraclavicular block will provide coverage for distal humerus, elbow, forearm and
hand procedures. With this approach one is less likely to encounter ulnar sparing,
but it may still occur. Complications more associated with this approach include
pneumothorax, due to the proximity of the pleura. Phrenic nerve involvement is
much reduced from the interscalene approach to about 30% of all blocks.
Infraclavicular and axillary – The infraclavicular block is performed below the
clavicle, but before the axilla while the axillary brachial plexus block is performed, as
the name suggests, in the axilla in direct relation to the axillary artery. These blocks
give good coverage for elbow, forearm and hand surgery. The axillary block can also
cover the medial upper arm, and is used for AV fistula formation in some patients.
From a complication standpoint, these approaches greatly reduce the incidence
of phrenic nerve palsy, and other severe complications. In addition, the use of
ultrasound reduces the possibility of inadvertent vascular puncture, which is the
particular concern at these sites.
This question relates to a perennial exam favourite – the unwell patient in recovery.
The key here is to work through the differential diagnoses to leave the most plausible.
Here the clue relates to the block. The nerve stimulator result indicates no
significant residual curarisation, and clinically there is little wheeze with acceptable
saturations, hinting at a problem more of ventilation than oxygenation. Performing
an arterial blood gas analysis will not be an appropriate treatment for this patient.
Continuous positive airway pressure (CPAP) may be a sensible idea in a patient
with obstructive sleep apnoea (OSA) to maintain a patent airway, especially if there
is co-administration of opioids. However the combination of obesity, COPD, and
the inevitable unilateral phrenic nerve blockade from the block can give rise to
respiratory embarrassment. This is often most obvious in the supine position, and
should recede as the block resolves. Therefore the most appropriate management
option in this clinical scenario is administration of BiPAP until the block wears off.
Raju PKBC, Coventry DM. Ultrasound guided brachial plexus blocks. Contin Educ Anaesth Crit Care Pain
2010; 10 (2):48–52.
10. D Cords
A brachial plexus block represents the most common use of nerve blocks in current
regional anaesthetic practice. A good anatomical knowledge is essential for
successful brachial plexus block.
139
140
Chapter 4
The plexus is formed by the anterior primary rami of the lower four cervical nerve
roots (C5-C8) and first thoracic nerve root (T1). The brachial plexus supplies sensory
and motor innervation to the entire upper limb with the exception of the trapezius
muscle (innervated by the spinal accessory nerve) and the cutaneous innervation of
the area of the axilla (supplied by intercostobrachial nerve).
The brachial plexus consists of roots, trunks, divisions, cords and terminal and
collateral branches.
Roots: the ventral rami of C5-T1 spinal nerves form the five roots of the plexus.
An interscalene block mainly targets the upper roots (C5-C7) and, because of the
vertical arrangement of the brachial plexus roots in the interscalene groove, C8 and
T1 are often missed hence the ulnar nerve may not be blocked.
Trunks: shortly after leaving the intervertebral foramina, the roots unify to form
three trunks (upper (C5-C6), middle (C7) and lower (C8-T1) trunks).
Supraclavicular blocks are performed at the level of the brachial plexus trunks so the
entire upper limb is blocked more reliably.
Divisions: each trunk then divides into two divisions to form six divisions in total
(three anterior and three posterior). The divisions generally cannot be blocked
reliably because they lie behind the clavicle.
Cords: The six divisions unite again to form the three cords. The posterior divisions
merge to form the posterior cord (C5-T1). The anterior divisions from the upper and
the middle trunks form the lateral cord (C5-C7). And finally, the anterior division of
the lower trunk will continue to become the medial cord (C8-T1). The brachial plexus
cords are described according to their relation to the axillary artery.
Infraclavicular blocks are performed at the level of the cords of the brachial plexus.
At this level each of the three cords of the brachial plexus are and therefore it may
achieve anaesthesia of the entire arm.
Terminal branches: these are mixed nerves that contain sensory and motor nerve
fibres.
• The ulnar nerve (C8, T1) arises from the medial cord. It provides motor innervation
to the intrinsic muscles of the hand and sensation to the medial one and a half
fingers.
• The musculocutaneous nerve (C5, C6, C7) is derived from the lateral cord. It
provides motor innervation to the flexor muscles (the coracobrachialis, biceps
brachii and the brachialis) and sensory innervation to the lateral surface of the
forearm. The musculocutaneous nerve continues as the lateral cutaneous nerve of
the forearm.
• The median nerve (C5-T1) arises form the both the medial (C5, C6, C7) and the
lateral cords (C8, T1). It provides motor innervation to most of flexor muscles in
the forearm and thenar muscles of the thumb. It provides cutaneous innervation
to the thumb, index finger, middle finger, the lateral half the ring finger, along
with the nail bed of these fingers.
• The radial nerve (C5-T1) is the largest branch of the brachial plexus. It is derived
from the posterior cord, providing motor innervation to the extensor muscles of
Answers
the elbow, wrist and fingers. It also supplies sensation to the dorsum of the hand.
The radial nerve continues as the posterior cutaneous nerve of the forearm.
• The axillary nerve (C5-C6) also arises from the posterior cord. It supplies the
deltoid and the teres minor muscles. It also provides sensation at the point just
below the shoulder. The axillary nerve continues as the lateral cutaneous nerve of
the arm.
The axillary blocks are performed at the level of the terminal branches of the brachial
plexus and depend on the relationship of nerves to the axillary vessels.
Supraclavicular branches of the BP (Figure 4.1): These nerves are also derived from
the BP but provide innervation above the clavicle.
• The long thoracic nerve (C5, C6, C7) supplies the serratus anterior muscle.
• The dorsal scapular nerve (C5) supplies the rhomboid muscles and the levator
scapulae muscle.
• The nerve to the subclavius (C5, C6) supplies the subclavius muscle.
• The suprascapular nerve (C4, C5, C6) supplies the supraspinatus and the
infraspinatus muscles.
T
Supraclavicular
DS
D
C
Infraclavicular
B
Axillary
Musculocutaneous
Lateral
pectoral
C5
R
Interscalene
SS
LC
Radial
N2S
C6
L
C8
Median
Thoracodorsal
PC
Lower
subscapular
M
Upper
subscapular
C7
Axillary
MC
Medial cutaneous
forearm
Medial cutaneous
arm
LT
Medial pectoral
T1
Ulnar
Figure 4.1 Schematic representation of the brachial plexus. LT: long thoracic nerve; DS: dorsal scapular
nerve; SS: suprascapular nerve; N2S: nerve to subclavius; U: upper trunk; M: middle trunk; L: lower trunk;
LC: lateral cord; PC: posterior cord; MC: medial cord.
141
142
Chapter 4
Branches of the cords: see Table 4.1
Table 4.1 Branches of the cords of the brachial plexus
Posterior cord branches
ULTRA
Upper subscapular, lower subscapular, thoracodorsal, radial, axillary
Lateral cord branches
LLM
Lateral pectoral, lateral root of the median nerve, musculocutaneous
Medial cord branches
MMMUM
Medial pectoral, medial cutaneous nerve of arm, medial cutaneous nerve
of forearm, ulnar, medial root of the median nerve
Al-Haddad MF, Coventry DM. Brachial plexus blockade. BJA CEPD Reviews 2002; 2(2): 33–36.
Neal JM, Gerancher JC, Hebl JR. Upper extremity regional anesthesia: essentials of our current
understanding. Reg Anesth Pain Med 2009 Mar-Apr;34(2):134–70.
11. B 200 mL bolus of O negative blood
In the management of paediatric trauma, it is crucial to recognise what the normal
physiological parameters are for different aged patients (Table 4.2).
Table 4.2 The normal physiological parameters for different aged children
Age (years)
Respiratory rate (breaths
per minute)
Heart rate (beats per
minute)
Systolic blood pressure
(mmHg)
<1
30–40
110–160
70–90
1–2
25–35
100 –150
80–90
2–5
25– 30
95–140
80– 105
5–2
20–25
80–120
90– 110
> 12
15–20
60–100
100–120
It is thus clear that this patient is expressing deranged parameters and has had
significant haemorrhage from the trauma sustained. Fluid resuscitation in paediatric
trauma is similar to adult trauma but with some key differences. If the patient fails
to respond to repeated boluses of crystalloid or colloid up to a maximum of 40 mL/
kg, the next most appropriate step is to use blood and blood products. The dose
of packed red cells is 10 mL/kg. This patient has already had the allocated 40 mL/kg
and still demonstrates instability therefore should be transfused O negative blood. If
the bleeding continues following this, fresh frozen plasma and platelets need to be
administered to avoid the coagulopathy worsening the bleeding.
Changing the temporary splint may result in the bone fragments being disrupted
causing further bleeding, and will not immediately assist in replenishing the
significant blood loss. Insertion of an arterial line will become necessary to monitor
the patient intra-operatively but in the current clinical scenario is unlikely to add
more to the clinical picture.
Cullen P. Paediatric trauma. Contin Educ Anaesth Crit Care Pain 2012; 12(3):157–161.
Answers
12.B Prior to an apnoea test the Paco2 must be 6.0–8.0 kPa
and the arterial pH 7.20–7.40
The Academy of Medical Royal Colleges 2008 code of practice for the diagnosis and
confirmation of death is the current reference manual for brainstem death (BSD)
testing in the UK.
In order to undertake BSD testing the following preconditions must be fulfilled:
• An unresponsive coma and apnoea with a recognised date and time of onset
• Evidence of irreversible brain damage of known aetiology
You must then exclude potentially reversible causes for the coma and/or apnoea.
These exclusions are:
•
•
•
•
•
•
•
•
•
•
The presence or persistence of depressant drugs (or their active metabolites)
A body temperature ≤ 34°C
The presence of a reversible circulatory, metabolic or endocrine disorder
Respiratory failure due to neuromuscular blocking agents, other drugs
or potentially reversible causes of apnoea (e.g. cervical injury, profound
neuromuscular weakness)
Sodium levels at time of coma onset must be 115–160 mmol/L
Sodium levels at time of first test. must be 115–160 mmol/L and not have
changed by > 0.5 mmol/L per hour between time of coma onset and first test
Potassium levels at time of first test must be > 2 mmol/L
Phosphate levels at time of first test must be 0.5–3.0 mmol/L
Magnesium levels at time of first test must be 0.5–3.0 mmol/L
Glucose levels at time of first test must be 3.0–20.0 mmol/L
To confirm BSD, the following bedside tests must be conducted. (Note, two
complete sets must be performed, however these can be conducted successively
without any fixed interval.):
• Absence of any pupillary reaction to light
• Absence of any eyelid movements when each cornea is touched in turn
• Absence of nystagmus or any eye movement when each ear is instilled with 50 mL
ice cold water
• Absence of a gag reflex
• Absence of a cough reflex when a suction catheter is passed down into the
trachea
• Absence of any motor response when supraorbital pressure is applied
• Absence of any spontaneous breathing efforts for 5 minutes
• Preconditions to apnoea test: Paco2 6.0-8.0 kPa and arterial pH 7.20–7.40
• Apnoea test only valid if, after 5 minutes: Paco2 increases by > 0.5 kPa; and Pao2
is > 5 kPa; and the systemic mean arterial pressure is ≥ 60 mmHg throughout.
If one or more of these preconditions are not met or the bedside tests cannot be
performed then ancillary investigations are required to confirm the diagnosis. The
legal time of death is when the first set of tests indicates death due to the absence of
brain-stem reflexes.
Academy of Medical Royal Colleges. A Code of Practice for the Diagnosis and Confirmation of Death.
London: Academy of Medical Royal Colleges, 2008.
143
144
Chapter 4
13. B Request urinary and plasma osmolarity measurements
This question requests the most useful option, not the first action. The most useful
strategy to aid ongoing management would be to work out why the patient is
hypotensive and polyuric so that treatment can be tailored appropriately. The
hypotension and poor peripheral perfusion will most likely respond to intravenous
crystalloid and a noradrenaline infusion but will not aid identification and correction
of the underlying condition which is most likely to be diabetes insipidus given the
clinical history.
Diabetes inspidus (DI)
The clinical manifestations are due to the failure of release of anti-diuretic hormone
(ADH) or reduced activity of ADH on the renal collecting duct. Without ADH there
is no re-absorption of water at the collecting duct of the nephron, resulting in loss
of plasma as urine which results in hypovolaemia. As a result of renal conservation
of sodium, a high plasma sodium concentration and a normal urinary sodium
concentration is seen.
DI is caused by:
• Central nervous system DI
• Traumatic brain injury (35%)
• Sub-arachnoid haemorrhage
• Intra-cerebral haemorrhage
• Pituitary surgery
• End-stage cerebral oedema
• Nephrogenic DI
• Renal DI may be caused by lithium treatment
The differential diagnosis includes:
• Diabetes mellitus
• Osmotic diuretics (which may have been given in this case)
Diagnosis may be made with the following criteria:
•
•
•
•
Increased urine volume > 3000 mL per day or > 1000 mL in 4 hours
High serum sodium > 145 mmol/L
High serum osmolarity > 305 mmol/kg
Low urine osmolarity < 350 mmol/Kg
A plasma osmolarity measurement would be the most useful intervention out of the
available options to confirm the diagnosis. The diagnosis of DI will enable correction
of her fluid-balance status by administrating exogenous anti-diuretic hormone.
Bradshaw K, Smith M. Disorders of sodium balance after brain injury. Contin Educ Anaesth Crit Care Pain
2008; 8(4):129–33.
14. B A balanced crystalloid
The clinical scenario is suggestive of septic shock. Fluid resuscitation is indicated
and should commence with a 10 mL/kg bolus of crystalloid. Though controversial,
Answers
there is a strong theoretical argument, though an absence of definitive evidence
to suggest that balanced solutions are less harmful than the unphysiological 0.9%
sodium chloride. 0.9% sodium chloride is mildly hyperosmotic and contains 50%
more chloride ions per litre than plasma and hence infusion of any significant
volume may result in a hyperchloraemic acidosis. Although the acidosis is
rapidly buffered, the effects of hyperchloraemia are several and include impaired
mental function, nausea, gastrointestinal dysfunction, renal vasoconstriction,
hyperkalaemia, impaired coagulation and a pro-inflammatory response. What is less
clear is whether these effects are clinically important.
Starch solutions have been withdrawn from the UK market due to concerns over
safety and questionable evidence. Albumin has not been demonstrated to confer
any survival benefit in sepsis but carry a more significant risk of reactions. Finally,
gelatins are unbalanced solutions, and again have not been demonstrated to be
superior to balanced crystalloid solutions in these circumstances.
Therefore the most appropriate choice of fluid would be a balanced crystalloid
solution.
Dellinger RP, Levy MM, Rhodes A. Surviving Sepsis Campaign: International Guidelines for Management of
Severe Sepsis and Septic Shock. Crit Care Med 2013; 41(2):580–637.
Handy JM, Soni N. Physiological effects of hyperchloraemia and acidosis. Br J Anaesth 2008; 101(2):141–50.
15. B Rectal examination
Alcoholic chronic liver disease is a physiological disaster, with some of the clinician’s
concerns being:
• Airway:
• an obtunded patient with a full stomach (possibly blood)
• Breathing:
• Fluid overload results in pulmonary oedema,
• Pleural effusions
• Ascites may splint the diaphragm
• Cardiovascular:
• Myocardial disease (the symptoms of which may be difficult to differentiate
from reflux or pancreatitis) due to:
–– Chronic hypervolaemia
–– Hypertension
–– Alcohol-induced cardiomyopathy
–– Pericardial effusion
–– Ischaemic myopathy
–– Loss of occult blood (chronic or acute) and coagulopathy:
–– Gastritis and ulcer disease
–– Mallory–Weiss tear
–– Varices
• Disability (an acute deterioration in cognition may be multi-factorial):
• Hypoglycaemia
• Intoxication
• Withdrawal
145
146
Chapter 4
• Seizures
• Hyponatraemia
• Delayed presentation of head trauma
• Encephalopathy
• Others:
• Hypothermia
• Infections and sepsis
• Hepatorenal syndrome
• Immuno-suppression
• Pancreatitis
• Diabetes mellitus
• Peripheral neuropathy
• Dementia syndromes
• Malnourishment
• Self-harm and depression
You are presented with such a patient who has an acute change in cognition
associated with hypotension and low urine output. As is often the case you do not
have further detailed information regarding this gentleman’s prior medical history.
Given the complicated picture the appropriate approach is a prioritisation-centred
examination and treatment management pathway (A-B-C-D-E). The most pressing
concern is cardiovascular instability and a rectal examination looking particularly
for occult blood (be it altered or otherwise) is indicated as a matter of urgency.
The finding of rectal blood will focus this scenario from a complicated differential
diagnosis into haemorrhagic shock in a patient with a presumed coagulopathy.
An arterial blood gas does have a haemoglobin measurement, but early on in
haemorrhagic shock the concentration may remain static and chronic anaemia
may complicate the interpretation. The other tests are all important but excluding
immediately life-threatening conditions must be your first priority and a rectal
examination in this group of patients is mandatory.
Lai WK. Management of acute liver failure. Contin Educ Anaesth Crit Care Pain 2004; 4(2):40–43.
16. E Second degree heart block with frequent pauses >2
seconds associated with syncope
Temporary transvenous cardiac pacing is a last resort in the management of bradydysrhythmias due both to the logistical difficulties related to insertion and the high
complication rates of this procedure. In asymptomatic brady-dysrhythmias / cardiac
conduction abnormalities, the indications for, and values of, permanent pacemaker
insertion are reasonably well defined.
In acute brady-dysrhythmias, the indications for treatment include shock, syncope,
malignant escape ventricular tachy-dysrhythmias and asystoles > 2 seconds. Primary
treatment should simultaneously include definitive treatment of any acutely
reversible cause and a trial of positive chronotropes. The later can be considered
in two groups, parasympathetic antagonists (atropine and glycopyrronium) and
sympathetic agonists (isoprenaline adrenaline, dobutamine, dopexamine and
salbutamol). Failure of this simultaneous treatment approach should lead to an
Answers
immediate trial of rescue, transcutaneous cardiac pacing, but only as a bridging
therapy either to definitive treatment of the reversible cause or insertion of a
temporary (or permanent) transvenous system.
In the above question, the specific treatment for calcium channel overdose is
hyperinsulinaemic euglycaemia. Failure to respond to the combination of this and
positive chronotrope therapy may warrant the insertion of a temporary transvenous
pacing system.
Scenario B warrants consideration of a permanent pacemaker but gives no
indication for a temporary system.
Hyperkalaemia causing brady-dysrhythmia should be treated immediately with a
combination of intravenous calcium, continuous insulin and dextrose infusion (safer
than a bolus infusion, which may be followed by a rebound hyperkalaemia) with the
possible additions of salbutamol and/or sodium bicarbonate, followed by definitive
therapy such as haemofiltration or haemodialysis.
The patient in scenario D is at significant risk of brady-dysrhythmias and their
complications. As such, discussion with the cardiology team and formation of a
plan(s), should this occur, would be prudent.
Scenario E represents the clearest indication amongst the given scenarios for
insertion of a temporary pacing system, though, depending upon the setting and
circumstances, a permanent system may be more appropriate.
Brignole M, Auricchio A, Baron-Esquivias G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac
resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the
European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm
Association (EHRA). Eur Heart J 2013; 34(29):2281–2329.
17.B Early intravenous access, early epidural for labour and
risk of difficult neuraxial blockade or intubation in an
emergency Caesarean section
Obesity in pregnancy is becoming more commonplace and is associated with
many complications, such as gestational diabetes, pre-eclampsia, post-partum
haemorrhage, macrosomia, miscarriage and stillbirth. Joint guidelines produced
by the Centre for Maternal and Child Enquiries (CMACE) and the Royal College of
Obstetricians and Gynaecologists (RCOG) in 2010 recommend that pregnant women
with a body mass index (BMI) ≥ 40 should be seen by an obstetric anaesthetist
antenatally. When assessing these patients, the following should be considered:
• Airway – higher incidence of difficult intubation and difficult mask ventilation
• Respiratory – desaturate quicker and higher incidence of obstructive sleep
apnoea
• Cardiovascular – aortocaval compression may be more pronounced in the supine
position. Hypertension, myocardial ischaemia, heart failure and cardiomyopathy
are more common, while venous thromboembolism is also a greater risk
• Gastrointestinal – higher aspiration risk due to higher gastric volumes
• Anaesthesia – difficult venous access, difficult epidural or spinal anaesthesia
• Delivery – increased risk of instrumental delivery and Caesarean section
147
148
Chapter 4
The patient should be advised of the main risks surrounding her delivery
(intravenous access, regional anaesthesia, failed intubation), but also be able to
trust you as her anaesthetist, as she is already likely to be anxious. It may be difficult
for the patient to lose weight during the pregnancy, and this should not be the
mainstay of the advice given. Early intravenous access and an early labour epidural
should be advised, due to the potential for difficulty and the need to accomplish
these outside of an emergency situation. The risks of general anaesthesia should also
be explained. A normal delivery without any anaesthetic intervention is the ideal
situation, but practically, complications must be prepared for.
Gupta A, Faber P. Obesity in pregnancy. Contin Educ Anaesth Crit Care Pain 2011; 11 (4):143–46.
Modder J, Fitzsimons KJ. CMACE/RCOG Joint Guideline: Management of women with obesity in
pregnancy. London: Centre for Maternal and Child Enquiries, and Royal College of Obstetrics and
Gynaecologists, 2010.
18.C Arrange an inpatient bed so that the patient can
be admitted overnight for respiratory monitoring
postoperatively
Obstructive sleep apnoea (OSA) is common in children, and can be associated with
significant morbidity. OSA belongs to a spectrum of diagnoses known as sleep-related
breathing disorders in which the airway is completely (apnoea) or partially (hypopnoea)
occluded during sleep despite continued respiratory efforts. In young children,
adenotonsillar hypertrophy is the most common anatomical abnormality associated
with OSA, and adenotonsillectomy is, therefore, the most common surgical intervention.
Other risk factors for OSA include midface hypoplasia, macroglossia, muscular hypotonia
(all three are features of Down’s syndrome), micrognathia, and obesity.
The apnoea/hypopnoea index (AHI), counts the number of apnoea or
hypoapnoea events secondary to obstructive events during sleep for 60 min. An
AHI > 10 in children is classified as severe OSA. Respiratory complications after
adenotonsillectomy are more common in children with severe OSA. Other risk
factors for postoperative complications include age < 3 years, obesity, Down’s
syndrome, failure to thrive, history of prematurity and neuromuscular diseases.
Optimal perioperative management of OSA includes thorough preoperative
assessment, opioid-sparing anaesthetic and analgesic approaches, and close
respiratory observation and monitoring. Postoperative respiratory monitoring of
children with OSA should include continuous pulse oximetry to assess oxygenation
and clinical observation with measurement of the respiratory rate at frequent
intervals as a secondary assessment of the adequacy of ventilation. Measurement
of a full blood count for polycythaemia is not an effective method of assessing
desaturations. As this patient has had an echocardiograph showing normal intracardiac anatomy, a repeat echocardiograph is unlikely to provide information that
would change management. Sedative premedications increase the risks of airway
complications in OSA patients and are unlikely to benefit this patient. Finally,
application of topical anaesthesia at potential intravenous access sites is valuable,
but not the most important preoperative preparation for this case.
Patino M, Sadhasivam S, Mahmoud M.Obstructive sleep apnoea in children: perioperative considerations.
Br J Anaesth 2013;111(suppl 1): i83–i95.
Answers
19.B Give a 2 µg/kg bolus dose of naloxone and repeat if
necessary and reduce PCA bolus and background doses
Patient controlled analgesia (PCA) using intravenous morphine is an excellent way
to manage postoperative pain in older children. It has better analgesic efficacy and
patient satisfaction compared to other common analgesia modalities. However, it is
not without side effects or complications – itching and respiratory depression being
two of the most common. The risk is higher when a PCA is used with a continuous
background.
The history, symptoms and signs of this patient are all consistent with opioid
induced drowsiness and respiratory depression. A small dose of naloxone, a
µ-receptor antagonist, is appropriate in this case. Naloxone has a shorter half-life
than morphine, so repeated doses may be required. Ideally, the naloxone would be
titrated to reverse the drowsiness and respiratory depression, but not the analgesic
effects. In severe overdoses, airway and ventilator support may be indicated.
Different patients have different sensitivity to opioid. The initial PCA setting was
evidently inappropriate for this patient. The bolus dose should be reduced, and the
background infusion either reduced or removed.
Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI). Good Practice in
Postoperative and Procedural Pain Management, 2nd ed. Paed Anaesth 2012;22 (suppl 1):1–79.
Macintyre PA. Safety and efficacy of patient-controlled analgesia. Br J Anaesth 2001;87:36–46.
20. A Increase the inspired oxygen to 100%
This is a case of suspected anaphylaxis. It is a life-threatening allergic reaction
triggered by a wide range of antigens and involves multiple organ systems. Signs
suggestive of anaphylaxis include hypotension, difficulty in ventilation, cutaneous
flushing, coughing, an urticarial rash, desaturation and wheeze.
The most common causes of anaphylaxis during anaesthesia are neuromuscular
blocking agents (most commonly succinylcholine), latex, colloids and antibiotics.
Every anaesthetist should be familiar with an anaphylaxis drill. The one published by
AAGBI (revised 2009) is widely used in the UK. The immediate management includes:
• Stop the administration of all agents likely to have caused the anaphylaxis
• Call for help
• Maintain the airway, give oxygen 100% and lie the patient flat with the legs
elevated
• Give adrenaline (epinephrine) 1:10 000. Adult dose: 50 µg (0.5 mL); paediatric
dose: 1 µg/kg
• Give intravenous fluid bolus (avoiding colloids that have a higher incidence of
allergy) Adult: 500–1000 mL; paediatric 20 mL/kg
Subsequent management:
• Give antihistamines (chlorpheniramine 2.5 mg intravenously for a child aged 6
months to 6 years)
• Give corticosteroids (hydrocortisone 50 mg IV for a child aged 6 months to 6 years)
149
150
Chapter 4
• Bronchodilators may be required for persistent bronchospasm
• Catecholamine infusion as cardiovascular instability may last several hours
• Take blood samples for mast cell tryptase
Ryder SA. Anaphylaxis. Cont Educ Anaesth Crit Care Pain 2004;4:111–113.
Mills AT, Sice PJ, Ford SM. Anaesthesia-related anaphylaxis: investigation and follow-up. Cont Educ
Anaesth Crit Care Pain 2014; 14 (2): 57-62.
21.D General anaesthesia with a fascia iliaca block.
Regular oral paracetamol 1 g 6 hourly and immediate
release morphine 5–10 mg up to 4-hourly as required for
breakthrough pain
Patients with hip fractures are often frail and elderly with multiple co-morbidities.
As such they have a relatively high incidence of perioperative morbidity and
mortality. High quality care requires a co-ordinated and timely multidisciplinary
approach. Early fixation not only aids analgesia but also reduces morbidity and
mortality. Hip fractures are painful and optimal pain relief will aid rehabilitation
and ultimately improve outcomes. Extracapsular fractures are more painful than
intracapsular fractures. It is important that both static and dynamic pain scores are
considered so that physiotherapy can be as effective as possible. As with all pain,
a multimodal approach should be adopted. Local anaesthetic nerve blocks reduce
the amount of supplemental opioids required. A number of different approaches
such as femoral nerve block, lumbar plexus block or fascia iliaca block could be
used. Central neuraxial blockade is also useful for both intraoperative anaesthesia
and postoperative analgesia. However this would not be the method of choice
in a patient taking both aspirin and clopidogrel. Clearly care must be taken when
performing fascia iliaca blocks and ultrasound may reduce the incidence of
haematoma formation.
Paracetamol should be used as first line therapy as it is not only very effective but
also has a good side-effect profile. The dose of intravenous paracetamol should be
reduced in those weighing less than 50 kg. Non-steroidal anti-inflammatory drugs
(NSAIDs) should largely be avoided as many of this patient population have impaired
renal function. In the example above the creatinine may only be 87 μmol/L but when
weighing 45 kg with reduced muscle mass this will no doubt represent a degree of
renal impairment. Codeine and tramadol should also be avoided. Opioids should
be used with extreme care at reduced doses due to renal impairment and increased
postoperative confusion.
R Griffiths. Anaesthesia for patients undergoing hip fracture surgery. Association of Paediatric
Anaesthetists of Great Britain and Ireland (APAGBI): Core Topics in Anaesthesia, 2012.
22. B Cellulitis over needle insertion site
Acupuncture is a widely practiced complementary therapy, with its origins China
approximately 3000 years ago. It is based on the principle that the flow of vital
energy (Qi) through the body along set pathways (known as meridians) is the
key to good health. An imbalance between two opposing forces, yin (cold, slow,
Answers
passive elements), and yang (hot, excited, active elements) disrupts this flow, and
is the cause of ill-health, including pain.
There are said to be 12 main and 8 secondary meridians. These are connected by
over 2000 specified points on the body, which are used as acupuncture points.
Depending on where the imbalance is thought to lie, fine needles are placed in the
relevant points on the appropriate part of the body, and left in place for seconds to
minutes.
How or why this is meant to work is a matter of hypothesis, and theories include
placebo or psychological effects, intrinsic release of endorphins which then act
on the descending inhibitory pain pathways, or confounding factors such the
spontaneous resolution of the disease process anyway.
Convincing evidence for or against the use of acupuncture is scarce, mainly due to
the lack of well-conducted studies. However, it seems to have found a place in pain
management, mainly as a last resort where all other methods have failed. Pain of
osteoarthritis, chronic neck pain, chronic low back pain, and labour analgesia are
some of its more common uses in clinical practice by those who believe it may help.
Risks of needling are small but are not dissimilar to any other needle-based
procedure to which we may be more accustomed. These potentially include
pneumothorax, infection, bleeding, bruising, and local pain or discomfort.
Contraindications include patient refusal, poor cooperation, systemic sepsis, local
burns or cellulitis and severe coagulopathy or bleeding diatheses.
Wilkinson J, Faleiro R. Acupuncture in pain management. Contin Educ Anaesth Crit Care Pain 2007; 7(4):
135–138.
Surah A, Baranidharan G, Morley S. Chronic pain and depression. Contin Educ Anaesth Crit Care Pain 2014;
14 (2): 85–89.
23. A Carbamazepine
Trigeminal neuralgia is neuropathic pain in the distribution of the trigeminal
nerve, which most commonly presents in middle age. It is often characterised as
lancinating and the worst pain imaginable. It most frequently occurs in the maxillary
or mandibular divisions of the trigeminal nerve and is always unilateral in nature. It is
usual triggered by benign stimuli such as hair brushing or shaving. There is complete
resolution of pain between the episodes, which usually last only seconds, and there
is no associated neurological deficit.
About 70% of patients with trigeminal neuralgia can be managed medically.
Carbamazepine is the most effective agent, probably followed by gabapentin.
Amongst the surgical options microvascular decompression is the most effective but
is invasive. Glycerol gangliolysis has a greater success rate than alcohol injection of
the trigeminal nerve at various points along its course. Radiofrequency ablation is
looking promising but is not yet well validated.
W Rea, S Kapur, H Mutagi. Radiofrequency therapies in chronic pain. Contin Educ Anaesth Crit Care Pain
2011; 11(2): 35–38.
K Farooq, P Williams. Headache and chronic facial pain. Contin Educ Anaesth Crit Care Pain 2008;
8(4):138–142.
151
152
Chapter 4
24. D Pain usually occurs in an area of altered sensation
This clinical scenario provides an example of central post-stroke pain. It is poorly
recognised but common and can occur in up to 8% of all stroke patients at one year.
It was once thought to be only a consequence of thalamic lesions but any lesion in
the spinothalamic tract can cause this pain. Given the motor changes, it is unlikely
that this patient has suffered a thalamic lesion. Post-stroke pain occurs generally in
an area with altered sensation, and 70% of patients also suffer from allodynia (pain in
response to non-painful stimuli). Treatment of these patients is difficult and opioids
have been shown to have poor efficacy. The most appropriate therapy in this patient
is anticonvulsants such as lamotrigine.
Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and
management. Lancet Neurol 2009; 8(9):857–868.
25. B Coeliac plexus block
The pathophysiology of chronic pain is complex and incompletely understood. It is
thought to have a somatic component, but also a contribution from the sympathetic
nervous system (SNS). For this reason, blockade of sympathetic ganglia is widely
used to provide relief to those in whom other forms of analgesia have been
inadequate. Robust evidence for the use of sympathetic blocks is lacking, and often
pain is not completely relieved with these techniques alone, but may be reduced. If
the patient is taking chronic pain medication, this should usually be continued after
the procedure.
The SNS is thought to have a particular role in pain of neuropathic nature, or of
vascular or visceral origin. There may be more than one mechanism. While neurological
sensitisation is suggested in neuropathic pain, sympathetic mediated vasoconstriction
may contribute to chronic vascular pain such as what occurs in Raynaud’s disease.
Indications for a sympathetic block are seen in Table 4.3.
Table 4.3 Indications for sympathetic block
Vascular disease
Visceral pain
Neuropathic pain
Others
Acute vasospastic conditions e.g.
cold injury, traumatic spasm, inadvertent arterial drug injection
Chronic pancreatitis
Complex regional
pain syndrome
(CRPS) types 1 and 2
Hyperhydrosis
Chronic vasospastic conditions
e.g. Raynaud’s disease, chronic
spinal cord injury
Upper abdominal
malignancy
Postherpetic neuralgia
Chronic arterial occlusion syndromes e.g. atherosclerosis
Upper abdominal
surgery
Neuropathy, e.g. diabetic, carcinomatous
Microvascular surgery e.g.
arterio-venous fistula formation
Perineal/pelvic
cancer
Cardiac pain, e.g.
refractory angina
Chronic nonmalignant pelvic pain
Answers
Contraindications include patient refusal, bleeding diathesis or coagulopathy, local
infection, local malignancy and hypersensitivity to the drugs used in the block.
There are several types of sympathetic block. These are summarised in Table 4.4.
Table 4.4 Types of sympathetic block
Diagnostic block
Prognostic block
Therapeutic block
Assesses the sympathetic component of chronic pain, which
can then be used to plan future
treatment
Assesses the effect of the
block, prior to neuro-ablative
techniques
Longer lasting block, mainly for
vascular disease and malignancy
False positive results are
common because of concomitant inadvertent blockade of
somatic nerves
Because false positives may occur, should be performed more
than once to assess results
before decision to proceed
with neuroablation
Not permanent
1% lignocaine commonly drug
of choice
0.25–0.5% bupivacaine commonly used
Commonly used drugs include
0.25–0.5% bupivacaine and
neurolytics such as phenol or
alcohol
Neurolytics cause non-specific
neural tissue destruction, and
can cause neuritis in other
nerves
Blocks are usually performed under sedation or general anaesthesia in a setting that
has facilities and skills for resuscitation. Image intensifier is used for accurate needle
placement.
In this scenario, the patient has a chronic upper gastrointestinal malignancy,
and a coeliac plexus block would be the most suitable choice for him. A lumbar
sympathetic block is better for lower limb pain (e.g. CRPS or vascular) or rectal
pain. A superior hypogastric plexus block is the best choice for pelvic pain.
Sphenopalatine ganglion blocks are used to treat intractable headaches and facial
pain.
Menon R, Swanepoel A. Sympathetic blocks. Contin Educ Crit Care Pain 2010; 10(3):88–92.
26. E Ketamine
Penetrating eye injury is an ophthalmic emergency and patients require urgent
surgical intervention to avoid the loss of sight. The concern in anaesthesia is that a
rise in intraocular pressure (IOP) may lead to expulsion of the contents of the globe
through the injured opening.
The normal IOP is 10–20 mmHg and is influenced by aqueous humour regulation,
choroidal blood flow and extraocular muscle tone. Most anaesthetic induction
agents and volatile agents actually reduce IOP, hence propofol and thiopentone are
safe to use. Ketamine, however, causes an increase in IOP, probably by increasing
arterial pressure, and it should be avoided in this scenario.
153
154
Chapter 4
Non-depolarising neuromuscular blocking drugs do not increase IOP and may
actually cause a slight reduction due to the relaxation of the extraocular muscles.
On the other hand, suxamethonium causes an increase in IOP by up to 10 mmHg for
up to 10 minutes after administration. This can be offset by the concurrent use of an
induction agent, such as propofol or thiopentone, and is often favourable due to the
rapid intubating conditions it creates in a non-fasted patient. It would be reasonable
to use suxamethonium in a rapid sequence induction in this scenario, but benefits
versus risks must be weighed up in each case, especially as rocuronium 1 mg/kg
can be used as an alternative now that sugammadex is available. Laryngoscopy and
intubation can also cause significant increases in the IOP and so agents to obtund
the response, such as high dose opioids and β-blockers, may also be used.
Murgatroyd H, Bembridge J. Intraocular pressure. Contin Educ Anaesth Crit Care Pain 2008; 8 (3):100–103.
Raw D, Mostafa SM. Drugs and the eye. BJA CEPD Reviews 2001; 1(6):161–165.
27. E Check his core temperature
Prolonged endovascular procedures in radiology suite are frequently associated
with hypothermia and significant blood loss. This can be increased further by
the intraoperative use of unfractionated heparin (UFH). At 7–150 units per kg the
effects of UFH become clinically insignificant after 2–4 hours. Whilst checking his
haemoglobin and performing an arterial blood gas would provide the answers
regarding his acid-base status it will not reveal the cause of those changes. The
activated clotting time (ACT) measurement is only valid when large doses of heparin
are used to ensure safety during cardiopulmonary bypass operations. It is not
validated to be used for checking the degree of anticoagulation provided by heparin
at lower doses. A blood sugar analysis will not help establish the cause of his altered
coagulation.
Effects of hypothermia on the coagulation cascade translate into increased risk of
perioperative blood loss. Normothermia is essential for normal enzymatic activity
of serum proteases within the clotting cascade. Prothrombin time is known to
increases gradually with increasing hypothermia: 20% increase at 34°C, 30% at 31°C
and 50% at 28°C. Partial thrombin time also increases according to the temperature
by 5% at 34°C to 30% at 31°C and 60% at 28°C. It is therefore necessary to check the
patient’s core temperature prior to proceeding with further management.
Rohrer MJ, Natale AM. Effect of hypothermia on the coagulation cascade. Crit Care Med 1992
;20(10):1402–1405.
28. D Preganglionic autonomic
A typical nerve cell, also called neuron, has cell body (stoma), dendrites and an axon
(Figure 4.2). Each neuron gives up many dendrites to form a dendritic tree. However,
only one axon is derived from each cell body, which can reach as far as 1 metre in
human beings.
A nerve is cable like structure that contains many axons (nerve fibres). A layer of
connective tissue called the endoneurium wraps each axon within the neuron. The
axons are packed together into bundles called fascicles. A layer of connective tissue
Answers
Spinal nerve
Epineurium
(around the spinal nerve)
Figure 4.2 Schematic
representation of spinal nerves
(top) and a neuron (bottom).
Perineurium
(around the axon)
Endoneurium
(around the fascicle)
Fascicle
Dendrites
Axon.
Nucleus
Myelin
sheath
Cell
body
Axon
Node of
Ranvier
Axon terminals
called the perineurium, that acts as a diffusion layer to local anaesthetics, surrounds
each fascicle. And, finally, a layer of connective tissue called the epineurium covers
the entire nerve.
A layer of a dielectric material called myelin sheath surrounds most axons. Myelin
increases the speed of impulse propagation along the nerve fibres and is essential
for the optimum function of the nervous system. In the peripheral nervous system,
myelin is produced by Schwann cells. However, oligodendrocytes supply myelin in
the central nervous system.
Peripheral nerve fibres are classified into three types according to their physiological
and anatomical characteristics: A, B and C nerve fibres (Table 4.5).
Table 4.5 Characteristics of A, B and C nerve fibres
Type
Diameter
(micrometre)
Conduction
speed (meters/
second)
Myelin
content
Function
A alpha
12–20
70–120
+++
Motor
A beta
5–12
30–70
+++
Touch and pressure
A gamma
1–4
15–30
++
Proprioception and muscle tone
A delta
1–4
12–30
++
Fast pain and temperature
B fibres
1–3
3–15
+
Preganglionic autonomic
C fibres
0.5–1
0.5–2
Unmyelinated
Slow pain and temperature
A fibres
Postganglionic autonomic
155
156
Chapter 4
Several layers of myelin wrap the A and B fibres. However, the myelin sheath is
interrupted by nodes of Ranvier resulting in a fast, non-homogenous saltatory
conduction. The impulse conduction in C fibres, however, is uniform and
homogenous but slow because C fibres are unmyelinated.
Two important factors determine the sensitivity of nerves to local anaesthetics: the
diameter and the myelination of the nerve fibres. Smaller and myelinated fibres are
more sensitive to local anaesthetics than larger and/or unmyelinated fibres. Smaller
nerves require less local anaesthetic to halt action potential transmission down their
axons, while myelinated nerves only require three consecutive nodes of Ranvier to
be blocked to achieve axonal blockade. An exception to this rule is the autonomic
B fibres. Although C fibres are smaller than B fibres, B nerve fibres are blocked first
because C fibres are unmyelinated.
The order of the blocking is therefore B fibres > C fibres > A fibres. This means the
preganglionic sympathetic block happens before the sensory block, which appears
before the motor block.
Hadzic A. Textbook of Regional Anaesthesia and Acute Pain Management. 1st ed. New York: McGraw-Hill,
2006: 159.
29. D Amiodarone
The QT interval is measured from the start of the Q wave till the end of the T wave.
The corrected QT interval is calculated using Bazett’s formula:
QTc = (QT interval )
√(RR Interval)
A QTc of > 440 msec is considered prolonged. The causes of prolonged QTc are
either congenital or acquired, due to sympathetic overactivity, stress, electrolyte
disturbances or drugs. A prolonged QTc increases the risk of rhythmic degeneration
to Torsade de pointes. Polymorphic ventricular tachycardia (VT) is a form of VT
caused by multiple ventricular foci with varying duration, amplitude and axis. When
polymorphic VT occurs with a prolonged QT, this is known as Torsade de pointes.
There are a number of drugs whose administration risks converting a prolonged QTc
to Torsades de pointes, including:
Amiodarone
Fluoconazole
Chlorpromazine
Fluoxetine
Haloperidol
Cisapride
Methadone
Clarithromycin
Procainamide
Disopyramide
Quinidine
Droperidol
Sotalol
Erythromycin
Flecainide
Thioridazide
In the context of this clinical picture, the most likely agent to degenerate a
prolonged QTc into polymorphic VT is amiodarone.
Hunter JD, Sharma P, Rathi S. Long QT syndrome. Contin Educ Anaesthes Crit Care Pain 2008; 8(2):67–70.
Answers
30. B CT angiography
The most likely diagnosis in this clinical scenario is that of a pulmonary embolism
(PE).
The European Society of Cardiology published guidelines in 2014 on the diagnosis
and management of acute PEs. There are a number of prognosticating tests of PE
severity, of which the Pulmonary Embolism Severity Index (PESI) and simplified PESI
(sPESI) are recommended. Due to ease of application and validation, the sPESI is
used most frequently, taking in to account:
• Age > 80–1 point
• Cancer–1 point
• Chronic heart failure or pulmonary disease – 1 point
• Pulse rate > 110 beats per minute –1 point
• Systolic blood pressure < 100 mmHg –1 point
• Arterial oxyhaemoglobin saturations < 90% – 1 point
0 points gives patients a 30-day mortality of 1.0%, while ≥ 1 point gives a 30-day
mortality of 10.9%.
Additional markers are also applied to stratify patients:
Clinical: Shock, hypotension
Right ventricular (RV) dysfunction: RV dilatation, hypokinesia or pressure overload
on echocardiogram, RV dilatation on CT or elevated right heart pressure on cardiac
catheterisation.
Cardiac laboratory biomarkers: Cardiac troponin T or I, brain natriuretic peptide
(BNP) elevation
These can then be put together to quantify the risk severity for patients (Table 4.6)
Table 4.6. Classification of acute PE based on 30-day mortality
30-day mortality risk
Risk scores and parameters
Shock or hypotension
High risk
Intermediate
risk
Low risk
sPESI ≥ 1
RV dysfunction
on imaging
Cardiac lab
biomarkers
+
+
+
Intermediate-high
–
+
Both positive
Intermediate-low
–
+
One or none positive
–
–
Both negative
It can be seen therefore that a hypotensive or shocked patient will immediately be
classified as high risk. In these patients imaging with transthoracic echocardiography
or CT angiography is recommended. Treatment of the PE must not be delayed for
imaging if there is a high clinical suspicion.
157
158
Chapter 4
In patients without clinical evidence of shock, such as the patient described in the
scenario above, investigations could be undertaken prior to initiation of treatment
of anticoagulation or thrombolysis. Chest X ray, arterial blood gas analysis and ECG
do not have a high specificity for detecting pulmonary embolism, even though
they may contribute to some extent in confirming diagnosis. Chest X-ray may
demonstrate hypovascularity or peripherally placed wedge shaped consolidation
suggesting infarction. ECG may show a S1Q3T3 pattern suggestive of right heart
strain and arterial blood gases may show hypoxia. It is suggested that in case of a
high clinical probability it is advisable to use a radiological investigation rather than
a non-radiological modality such as a D-dimer test which would in all probability
be high in the majority of in-patient postoperative patients. Transoesophageal
echocardiography is generally reserved for patients that are too unstable to undergo
diagnostic CT angiography, although bedside transthoracic echocardiography is
recommended.
Using CT angiography is most appropriate in this patient as it not only shows the
severity of the embolus but also depicts right heart dysfunction by demonstrating
enlarged size of the right ventricle and a flattened interventricular septum. In
addition, CT angiography may reveal the chronicity and possible clot location.
van Beek EJR. Diagnosis and initial treatment of patients with suspected pulmonary thromboembolism
Contin Educ Anaesth Crit Care Pain 2009; 9(4): 119-124.
Konstantinides S, Torbicki A, Agnelli G, et al. 2014 ESC Guidelines on the diagnosis and management
of acute pulmonary embolism: The Task Force for the Diagnosis and Management of Acute Pulmonary
Embolism of the European Society of Cardiology (ESC). Endorsed by the European Respiratory Society
(ERS). 2014 Eur Heart J (epub ahead of print). doi:10.1093/eurheartj/ehu283.
Chapter 5
Mock Paper 5
Questions
1. An asthmatic 40-year-old woman with myasthenia gravis (MG) presents for a
multi-level lumbar decompression. She was diagnosed with MG 8 years ago,
has difficulty with swallowing solids, and her current medication includes
pyridostigmine 720 mg/day and her forced vital capacity (FVC) is 2.9 litres.
Which of the following is most likely to predict her requirement for a period of
postoperative ventilation?
A
B
C
D
E
Bulbar symptoms
Pyridostigmine use of 720 mg/day
FVC of 2.9 litres
Duration of disease > 6 years
Concurrent history of asthma
2. You are anaesthetising a 68-year-old patient for bowel resection for sub-acute
obstruction. He had been vomiting intermittently for 3 days. After induction of
anaesthesia he became hypotensive so you commenced a noradrenaline infusion
which is currently running at 0.2 µg/kg/min. A thoracic epidural has been sited but
only a test dose has been given so far. Blood pressure is 110/70 and capillary refill
time is 4 seconds. An oesophageal Doppler is in situ.
Stroke volume (SV) = 30 mL (60–100 mL)
Flow time corrected (FTc) = 250 ms (330–360 ms)
Cardiac output (CO) = 3.3 L/min (4–8 L/min)
Peak velocity (PV) = 22 cm/s (50–80 cm/s)
Heart rate = 115 bpm
Figure 5.1 Oesophageal
Doppler waveform seen.
160
Chapter 5
Based on the waveform and data shown in Figure 5.1, what is the appropriate first
course of action?
A
B
C
D
E
Increase the noradrenaline infusion
Commence a dobutamine infusion
Commence the epidural infusion and leave the noradrenaline
Commence a GTN infusion and leave the noradrenaline
Administer 250 mL of Hartmann’s solution and decrease the noradrenaline
3. A patient in the cardiac intensive care unit suffers a cardiac arrest following three
vessel coronary artery bypass grafting. He has epicardial pacing wires with the box
set to DDD. The monitor shows pulseless electrical activity with pacing spikes.
Cardiopulmonary resuscitation (CPR) is commenced.
What is the most appropriate next step?
A
B
C
D
E
1 mg adrenaline IV
300 mg bolus of amiodarone
Institution of external pacing
Exclusion of a tension pneumothorax
Turn off the pacemaker
4. A 70-year-old smoker with limited mouth opening having previously undergone
a neck dissection with adjuvant radiotherapy is scheduled for surgery to treat his
right middle lobe tumour. A difficult airway is anticipated and it is likely that postoperative ventilatory support will be required.
Which of the following is the most appropriate airway management strategy?
A
Fibreoptic intubation with a single-lumen tube and a right sided bronchial
blocker
B Fibreoptic intubation with a single lumen tube and a left sided bronchial
blocker
C Videolaryngoscopy and insertion of a left sided double-lumen tube
D Fibreoptic left sided endobronchial intubation with a single-lumen tube
E Awake tracheostomy and insertion of right sided double-lumen endobronchial
tracheostomy tube
5. A 75-year-old man is to have a cystoscopy and bladder biopsy as a day surgery
case. He has a 40 pack year history of smoking. Recent spirometry has shown his
FEV1/FVC is 0.6, and echocardiography has shown an ejection fraction of 40%. He
has been consented for a spinal anaesthetic.
What is the most appropriate solution for the spinal injection?
A
B
C
D
E
Hyperbaric bupivacaine 0.5% 2 mL
Hyperbaric bupivacaine 0.5% 2 mL with 300 µg diamorphine
Plain bupivacaine 0.5% 2 mL with 10 µg fentanyl
Hyperbaric prilocaine 2% 2 mL with 10 µg fentanyl
Hyperbaric lignocaine 2% 2 mL with 10 µg fentanyl
Questions
6. You are asked to review a confused 72-year-old man in recovery. He has had a
transurethral resection of his prostate for benign prostatic hyperplasia (BPH). A
brief assessment reveals him to be disorientated in time and place, and restless.
Whilst you review his anaesthetic chart he has a short seizure, which resolves
spontaneously.
After assessing his airway breathing and circulation, which of the following would
be the best immediate management:
A
B
C
Administration 2 mg of intravenous midazolam
Starting an infusion of magnesium sulphate
Sending an urgent U&Es, FBC and osmolality, and prepare intravenous
lorazepam in case of further seizure
D Administering 20–40 mg of intravenous frusemide
E Infusing 1–2 mL/kg 3% NaCl
7. An obese 45-year-old woman with progressive conductive hearing loss secondary
to chronic suppurative otitis media is due to undergo tympanoplasty. During the
preoperative safety check list, the team is informed by the surgeon that intubation
and facial nerve monitoring is required.
Which of the following would be the most appropriate to use as part of your
anaesthetic technique?
A
B
C
D
E
Remifentanil infusion
Ketamine bolus
Nitrous oxide
Clonidine infusion
Magnesium sulphate infusion
8. A 63-year-old man with a confirmed inherited pseudocholinesterase deficiency
(EuEa) is attending for his first course of electroconvulsive therapy.
Which of the following drug combinations is most appropriate for his induction of
anaesthesia?
A
B
C
D
E
Propofol and mivacurium
Propofol and rocuronium
Propofol and alfentanil
Thiopentone and rocuronium
Thiopentone and alfentanil
9. A 70-year old man is scheduled for foot surgery under general anaesthesia and a
sciatic nerve block. There are no ultrasound machines available and you decide on
a landmark technique to perform the block.
Which one of the following described techniques results in the most proximal
approach to performing a sciatic nerve block?
A
B
Mansour’s approach
Raj’s approach
161
162
Chapter 5
C Labat’s approach
D Beck’s approach
E Guardini’s approach
10. A 68-year old man with emphysema is listed for elbow surgery under regional
anaesthesia.
Which of the following would be the most appropriate nerve block for this patient?
A
B
C
D
E
Interscalene brachial plexus block
Supraclavicular brachial plexus block
Medial infraclavicular brachial plexus block
Axillary brachial plexus block
Mid-arm peripheral nerve block
11. You have been called to assist in the care of a 17-year-old girl who has become
increasingly agitated in the emergency department. She has a history of mental
illness and has recently been behaving strangely. Now her actions are violent and
compromising her safety and that of those around her. You are unable to assess her
formally, and she has not had any blood tests, intravenous access or observations.
Security officers are present, and the emergency department registrar tells you
he would like to perform bloods, a CT head and a lumbar puncture. The plan has
been approved by the girl’s mother and the paediatric consultant.
How will you proceed?
A
Use security staff to hold the patient, insert intravenous access, and give 2 mg
midazolam and 2 µg/kg fentanyl in the room
B Use security staff to hold the patient, and give intramuscular 4 mg/kg
ketamine, then transfer to the resuscitation bay
C Do nothing, and refuse to get involved with this case
D Encourage her to take 20 mg oral temazepam and review
E Using security staff to hold the patient, transfer to theatre, and perform an
inhalational induction with sevoflurane
12. A 34-year-old man sustained a traumatic brain injury 3 days ago and is currently
intubated and ventilated on the intensive care unit. The nurse informs you during
your daily review that the plasma sodium concentration is 121 mmol/L.
What other piece information would be most useful in establishing the cause?
A
B
C
D
E
Urine output volume measurement
Central venous pressure measurement
Degree of peripheral oedema
Urinary osmolarity measurement
Plasma osmolarity measurement
13. A 13-year-old boy presented to the emergency department with acute severe asthma
1 hour ago. His usual peak expiratory flow (PEF) is 68%, and takes long acting β 2
agonist and high dose corticosteroid inhalers with montelukast tablets. You are
Questions
called for advice as despite 4 x 2.5 mg nebulised salbutamol, 500 µg nebulised
ipratropium and 40 mg of soluble prednisolone the patient’s PEF remains 35%
predicted, respiratory rate 32 per minute, speaking words, Spo2 93% on 10L/min of
warm humidified supplemental oxygen and transcutaneous carbon dioxide level of
5.1 kPa.
Which of the following should be the next intervention?
A
Rapid sequence induction using thiopentone and suxamethonium following
by positive pressure ventilation on an anaesthetic machine using isoflurane to
maintain anaesthesia and ease bronchoconstriction
B Commence an intravenous salbutamol infusion at 10 µg/minute
C Give 20 mmol of intravenous magnesium sulphate over 10–20 minutes
D Give a further 5 mg nebulised salbutamol
E Give a loading dose of 5 mg/kg aminophylline followed by an infusion at
500 µg/kg/hour
14. During the high dependency unit ward round you are called to the bedside of a
64-year-old gentleman with a background of hypertension who is awaiting primary
angioplasty planned for the following day after being admitted with a non-ST
segment elevation myocardial infarction. He is feeling anxious and has central
chest pain. The heart rate has recently increased to 150 beats per minute and the
blood pressure is 90/60 mmHg. The ECG shows atrial fibrillation and widespread
ST segment depression.
What is your immediate course of action?
A
Ring the anaesthetist on call and arrange for direct current (DC) cardioversion
in theatre
B Ring the anaesthetist on call and arrange for direct current (DC) cardioversion
on the HDU
C Administer amiodarone 300 mg intravenously over 30 minutes
D Administer 2 g intravenous magnesium and optimise the serum potassium
concentration
E Ring the cardiologist on call and organise an urgent angiography
15. A 72-year-old man on the intensive care unit has an APACHE II score of 48.
Which of the following variables is the most heavily weighted in intensive care
severity of illness scoring systems?
A
B
C
D
E
Age
Glasgow coma scale
Systolic blood pressure / dose of vasopressor
Pao2:Fio2 (PF ratio)
Arterial lactate concentration
16. A 34-year-old woman with end-stage liver disease due to auto-immune hepatitis
presents with a 2-day history of productive cough and breathlessness and
has been commenced on antibiotics for a chest infection. She has stigmata
163
164
Chapter 5
of decompensated liver disease with peripheral oedema and ascites. Her
blood pressure is 70/40 mmHg, her heart rate is 130 beats per minute and her
temperature 38.9oC. An arterial blood gas analysis returned a lactate concentration
0f 6.8 mmol/L.
Which of the following treatment options do you administer first?
A
B
C
D
E
20 mL/kg Hartmann’s solution
20 mL/kg 0.9% sodium chloride
10 mL/kg gelofusine
10 mL/kg human albumin solution (HAS) 20%
Commence vasopressor support as soon as possible
17. A 29-year-old woman, with a history of rheumatic fever is undergoing a category 1
Caesarean section under general anaesthesia for cord prolapse. After delivery of the
baby and placenta, the estimated blood loss is 1100 mL. The patient receives a total of
10 IU of syntocinon intravenously plus 10 IU/hour intravenous syntocinon infusion,
intravenous ergometrine 500 µg, 250 µg intramuscular carboprost, misoprostol 1 mg
rectally, four units of packed red blood cells and two units of fresh frozen plasma. As
the obstetricians are closing, the patient begins to produce frothy pink sputum up the
endotracheal tube.
Which of the following is the least likely cause of the pink frothy sputum?
A
B
C
D
E
Syntocinon
Ergometrine
Carboprost
Blood products
Misoprostol
18. You have been fast bleeped to one of the delivery rooms on labour ward where a
38-year-old multiparous woman who is in the first stage of labour has suddenly
become short of breath. Initial observations show oxygen saturations of 87%, a
respiratory rate of 35, heart rate of 110 beats per minute and a blood pressure of
85/40 mmHg.
What is the least likely cause of her presentation?
A
B
C
D
E
Amniotic fluid embolism
Pulmonary embolism
Antepartum haemorrhage
Anaphylaxis
Tension pneumothorax
19. A 6-week-old boy presents with a 3-day history of progressive non-bilious vomiting
and poor feeding. An ultrasound scan confirms the diagnosis of pyloric stenosis.
The capillary blood gas is shown in Table 5.1.
Questions
Table 5.1 Capillary blood gas test results
Parameter
Result
pH
7.46
pCO2
5.1 kPa
pO2
6.8 kPa
–
HCO3
31 mmol/L
Base excess
+6
Cl–
100 mmol/L
+
Na
133 mmol/L
K+
3.1 mmol/L
The paediatric surgical team wants to perform an urgent pyloromyotomy. The
infant last fed 12 hours previously.
The immediate anaesthetic management of this infant should be:
A
B
Perform a rapid sequence induction because of delayed gastric emptying
Insert a nasogastric tube to aspirate any residual gastric content before
induction of anaesthesia
C Postpone anaesthesia and surgery until the infant is adequately fluid
resuscitated and the acid-base balance corrected
D Perform a caudal block after induction of anaesthesia to minimise analgesic
opioid requirement
E Arrange for postoperative intensive care monitoring because of increased risk
of apnoea
20. A healthy 15 kg 3-year-old boy is scheduled for an elective right orchidopexy for
cryptorchidism. Intravenous induction was performed with fentanyl, propofol
and rocuronium, and facemask ventilation was satisfactory. Direct laryngoscopy
showed a grade 3 view. You had two unsuccessful attempts at intubation with
direct laryngoscopy.
The surgeon wants to proceed with surgery because this patient was previously
cancelled for an upper respiratory tract infection.
The best course of action now is:
A
B
Insert a supraglottic airway device to ensure airway patency and adequate
ventilation. Proceed with surgery with positive pressure ventilation through
the supraglottic airway device
Reverse rocuronium with sugammadex, monitor neuromuscular blockade
with a peripheral nerve stimulator. Wake the patient up and postpone surgery
165
166
Chapter 5
C
Insert a supraglottic airway device to ensure airway patency and adequate
ventilation. Perform a fibreoptic intubation through the supraglottic airway
device and proceed with surgery
D Ensure airway patency and adequate ventilation using facemask. Perform a
fibreoptic intubation and proceed with surgery
E Have two further attempts at laryngoscopy. Check head and neck position,
laryngoscopy technique, external laryngeal manipulation and adequate
paralysis. Consider using a different laryngoscope, a smaller tube, a stylet or a
bougie
21. A 30-year-old man with Crohn’s disease has had a right hemicolectomy. You are
asked to see him in recovery for uncontrolled abdominal pain. He declined an
epidural preoperatively. Intraoperatively he had paracetamol and 20 mg morphine.
So far in recovery he has had a total of 25 mg morphine with little effect. He is alert
but very distressed with a normal respiratory rate. He does not normally take any
strong opiates and has no allergies.
What would be the most appropriate next step in the management of his acute
pain?
A
Further titrate morphine up to a maximum of 20 mg provided there are no
overt signs of overdose
B Give 2 mg midazolam
C Give 10 mg ketamine intravenously
D Give 100 mg tramadol intravenously
E Give 50 µg clonidine intravenously
22. A 23-year-old woman had an above knee amputation for a localised osteosarcoma.
She has developed unusual sensations at the amputated limb, pain at the stump,
and a feeling that the limb is still there.
Which of the following features are most likely to suggest true phantom limb pain
in this patient?
A
B
C
D
E
Painful sensations at the stump
Good response to opioid analgesia
Intermittent pain
Inadequately working preoperative epidural analgesia
Sensations that the amputated limb is still present
23. A 62-year-old woman presents for a left lobectomy. She is generally fit and well,
and not on any regular medications.
Which of the following is the best option for analgesic management:
A
B
C
D
E
Lumbar epidural
Intrathecal diamorphine
PCA morphine
Interpleural block
Thoracic epidural
Questions
24. A 48-year-old man is referred to the pain clinic with poorly controlled upper
abdominal pain. He is known to have pancreatic cancer, which is now palliative.
As a result of his medication he is now feeling increasingly tired and is having
difficulty concentrating.
He is on the following medication:
•
•
•
•
Paracetamol 1g four times daily
Gabapentin 900 mg three times daily
Modified release oxycodone 30 mg twice daily
Immediate release oxycodone 10 mg for breakthrough pain
What would be the most appropriate treatment option?
A
Increase modified release oxycodone to 40 mg twice daily and immediate
release oxycodone to 15 mg for breakthrough pain
B Add amitriptyline
C Perform a coeliac plexus block
D Perform a lumbar sympathetic block
E Perform a thoracic paravertebral block T10–T12
25. A 4.2 kg, 26-day-old neonate is admitted for repair of an inguinal hernia. He
was born at term by normal vaginal delivery. There are no other known medical
problems and no allergies.
What would be the most appropriate analgesic plan for post operative pain relief?
A
Single shot caudal combined with 15 mg/kg paracetamol intravenously
6-hourly and codeine phosphate 1 mg/kg orally 6-hourly as required
B Single shot caudal combined with 10 mg/kg paracetamol orally 6-hourly and
ibuprofen 5 mg/kg orally 8-hourly as required
C Single shot caudal combined with 10 mg/kg paracetamol orally 6-hourly and
codeine phosphate 1 mg/kg orally 6-hourly as required
D Local anaesthetic infiltration by surgeon combined with paracetamol 7.5 mg/
kg intravenously 6-hourly and codeine phosphate 1 mg/kg orally 6-hourly as
required
E Local anaesthetic infiltration by surgeon combined with paracetamol 15 mg/kg
orally 6-hourly and morphine sulphate 100 µg/kg orally 4–6-hourly as required
26. A 26-year-old woman was pulled unconscious from a campervan fire and was
intubated at the scene. She has 40% burns with moderate inhalational injury, and
has been fluid resuscitated according to the Parkland formula.
Her heart rate is 96 beats per minute, blood pressure 110/77 mmHg, capillary refill
time <2 seconds, temperature 38°C, and urine output is 70 ml/hour. Arterial blood
gas analysis on a Fio2 of 50% shows: pH 7.12, Pao2 40 kPa, Paco2 3.3 kPa, Hco3– 16
mmol/L, base excess –4.0, lactate 12.3 mmol/L.
167
168
Chapter 5
What is most likely to account for the lactic acidosis:
A
B
C
D
E
Sepsis
Volume depletion
Acute kidney injury from rhabdomyolysis
Cynaide poisoning
Ethanol poisoning
27. You are anaesthetising a 72-year-old man for an elective open abdominal
aneurysm. He is a known hypertensive and type II diabetic and his medication
includes amlodipine 5 mg, ramipril 10 mg and metformin 1 gm b.d.
What is the single most important intervention that would limit potential
postoperative renal impairment?
A
B
C
D
E
Start dopamine at 2.5 µg/kg/min
Administer mannitol 20% 0.5 g/kg
Optimise his circulatory blood volume
Keep his circulating haemoglobin > 90 g/L
Administer furosemide 40 mg
28. A 6-year-old boy is admitted with fulminant hepatic failure, bleeding oesophageal
varices, ascites and marked splenomegaly.
His liver function tests show an elevated bilirubin, alanine transaminases and
aspartate transaminases. He has low albumin, prolonged prothrombin time and
examination of his cornea on slit lamp examination demonstrate a brown, dark
ring encircling his iris.
Which of the following is the most likely diagnosis for this clinical picture?
A
B
C
D
E
Alpha-1 antitrypsin deficiency
Wilson’s disease
Primary biliary cirrhosis
Haemochromatosis
Sclerosing cholangitis
29. A 92-year-old man is brought to emergency department with a fractured neck of
femur following a fall.
To be categorised using the fraility phenotype, which of the following
characteristics would not be assessed?
A
B
C
D
E
Self-reported exhaustion
Mental state
Weight loss
Grip strength
Low activity
Questions
30. A new antiemetic drug is being evaluated. The percentage of patients who suffered
postoperative nausea and vomiting (PONV) after administration of either the drug
or placebo is reported:
• percentage of patients with PONV after drug A = 20%
• percentage of patients with PONV after placebo = 25%
Which of the following is the number needed to treat (NNT)?
A
B
C
D
E
20
25
5
75
1
169
170
Chapter 5
Answers
1. D Duration of disease > 6 years
Myasthenia gravis (MG) is an autoimmune disease with a prevalence between 1
in 10,000–100,000. Women are more likely to be affected with a female:male ratio
of 3:2. The disease is caused by IgG antibodies to the post-synaptic acetylcholine
(ACh) receptors at the neuromuscular junction of skeletal muscle. These receptors
are occupied by the antibodies and ultimately destroyed through complementmediated immune processes. MG is therefore associated with fatiguing muscle
weakness, as only a limited response to ACh released at the neuromuscular junction
is possible and any subsequent stimulation results in fewer and fewer receptors
available for activation.
The extent of muscle involvement and severity of disease was classified by Osserman
as seen in Table 5.2.
Table 5.2 Osserman Classification for the severity of MG
CLASS I
Limited to eye muscle involvement
CLASS IIa
Mild and generalised, responding to treatment
CLASS IIb
Moderate and generalised, response to treatment not satisfactory
CLASS III
Severe and generalised, including respiratory dysfunction
CLASS IV
Requiring ventilation
15% of patients fall into Class I, the remaining 85% suffer from generalised MG.
Cardiac and smooth muscle is entirely unaffected.
An anaesthetic and surgery can impact on a patient with MG in a number of ways.
The physiological stress in itself can exacerbate symptoms and, for a patient who
may be unable to achieve adequate tidal volumes or cough ordinarily, lack of preoperative planning could prove fatal.
There are four recognised risk factors that are associated with an increased likelihood
of requiring a period of postoperative ventilation.
1.
2.
3.
4.
MG duration of > 6 years – this has the greatest predictive value
Concurrent history of chronic respiratory disease
Pyridostigmine requirements of > 750 mg/day in the preceding 48 hours
Forced vital capacity < 2.9 litres
Other considerations for trying to predict the need for respiratory support include
surgery – type, length and need for intubation; anaesthetic – general +/– local, need
for muscle relaxation and perhaps reversal; medication – opiate use in a patient
with affected respiratory reserve, drugs such as aminoglycosides or beta-blockers
that can cause an exacerbation of MG and administration of the patient's normal
Answers
medication immediately post operatively, i.e. conversion of oral pyridostigmine to
intravenous equivalent doses (30 mg orally = 1 mg intravenously).
The factor most likely to predict this patient’s requirement for postoperative
ventilation is her duration of MG of > 6 years.
Thavasothy M, Hirsch N. Myasthenia gravis. Contin Educ Anaesth Crit Care Pain 2002; 2(3):88–90.
Banerjee A, Wilson I. Anaesthesia and myasthenia gravis. Anaesthesia Tutorial of the Week no 122. London:
World Federation of Societies of Anaesthesiologists, 2008.
2.E Administer 250 mL of Hartmann’s solution and decrease
the noradrenaline
The oesophageal Doppler is a minimally invasive cardiac output monitor. The
physical principle underlying the technology is the Doppler Effect, where the
changing frequency of ultrasound waves reflected from red blood cells as they pass
along the descending aorta is used to calculate the blood velocity. The Doppler
equation uses this frequency shift to estimate the velocity of red blood cells as they
pass the probe. By integrating this with time, and taking the area under the curve
(velocity vs time) the velocity time integral can be calculated (VTI). This is a measure
of stroke distance (Figure 5.2, distance=velocity x time). When multiplied by the
aortic cross sectional area the stroke distance gives the volume of blood passing the
probe in a given period of time.
Velocity
Contractility
afterload
Peak velocity
Acceleration
Stroke volume
Stroke distance
Composite of contractility,
afterload and preload
FTc
Figure 5.2 Sample oesophageal
Doppler waveform showing the
variables and cardiac parameters
on which information can be
derived. Data can be used as
a surrogate for contractility/
afterload (peak velocity &
acceleration), stroke volume
(stroke distance), and
contractility/afterload and
preload (FTc). Interpretation of
data must be made in the clinical
context
Time
The aortic cross sectional area is usually estimated from a normogram based on the
patient’s age, weight and height (which are input by the operator at start up) but can
also be measured with transoesophageal echocardiography. It should be apparent
that not all of the blood ejected via the aortic valve travels in the descending aorta
so a correction factor is used to account for coronary, brachiocephalic, carotid
and subclavian flow to give a figure for stroke volume (SV). Cardiac output is then
calculated by multiplying SV by heart rate.
Correct positioning of the probe gives the characteristic waveform seen above.
Elements of the waveform can be used to indicate left ventricular contractility,
171
172
Chapter 5
stroke volume, preload and afterload. When interpreting data from the oesophageal
Doppler it is important to appreciate the interdependency of the variables.
Peak velocity
The speed at which blood is ejected from the left ventricle is proportional to
inotropy. It declines with age, with normal values for a 20-year-old being around
100 cm/s compared with around 30–60 cm/s at the age of 90. The peak velocity
measurement in the patient in question is 22 cm/s; almost certainly lower than
expected. As well as reflecting contractility, peak velocity (PV) is inversely related to
afterload for a given level of inotropy.
Stroke distance/stroke volume
Although stroke volume involves the use of an estimated aortic cross sectional area,
the values are almost certainly more familiar to most than those of stroke distance.
The patient in the question has a low stroke volume which should then prompt the
user to think about the causes of this - low preload, pump failure, dysrhythmia, high
afterload, and then to use the other information (both from the Doppler and clinical
sources) to guide treatment. The stroke volume calculated in this example is lower
than would be expected.
FTc = flow time corrected = systolic ejection time corrected for heart rate
This has been used as a measure of preload because the fuller the left ventricle is, the
longer it will contract. However, this assumes a given level of inotropy and afterload
and therefore is susceptible to changes in these variables, not just preload. Normal
FTc is 330-360 ms (based on the assumption that systole occupies around a third of
the cardiac cycle (corrected for a heart rate of 60, so a total cycle time of 1000 ms = 1
s). In the patient described above, the FTc is 250 ms so is lower than expected.
Afterload
Changes in afterload will alter the width and peak of the waveform according to the
work undertaken by the left ventricle. An increase in afterload will result in shorter
FTc and lower PV whilst lowering afterload with reduce left ventricular work and
result in higher PV and longer FTc.
Any change in left ventricular dynamics will therefore lead to a change in the shape
of the waveform created (assuming other factors including aortic cross section and
regional blood flow are constant).
To summarise the data from the patient above, he has a good chance of
preoperative hypovolaemia, compounded by surgery and general anaesthesia and
has Doppler data suggestive of: low cardiac output, low stroke volume, low peak
velocity and low FTc.
The most likely clinical explanation for this is that the patient is being over-treated
with a vasoconstrictor (in this case noradrenaline) which is in turn masking
significant hypovolaemia; A is therefore not the correct option. The appropriate first
Answers
step is therefore option E; to give a fluid bolus and assess response; an appropriate
Doppler response would be widening of the waveform and an increase in the area
under the curve (and so stroke volume). This may allow a reduction in the dose of
catecholamine which in turn will reduce afterload and improve myocardial oxygen
balance and contractility.
Although commencement of the epidural infusion is part of optimal perioperative
management, doing so before correction of hypovolaemia may lead to hypotension
and escalating noradrenaline requirements (a similar scenario may occur with GTN).
It should be noted that epidurals, and indeed anaesthetic agents, will alter the shape
of the Doppler waveform by lowering systemic vascular resistance and therefore
raising FTc, making the waveform appear wider.
Although cardiac index is low, in primary pump failure left ventricular end-diastolic
volume would be expected to increase leading to normal FTc. In addition, the
patient already has a tachycardia, which dobutamine may well exacerbate, and so
option B is not currently advisable.
Drummond KE, Murphy E. Minimally invasive cardiac output monitors. Contin Educ Anaesth Crit Care Pain
2012; 12 (1): 5-10.
3. E Turn off the pacemaker
Although the incidence of cardiac arrest post cardiac surgery is low (0.7–2.9%),
survival following an arrest is high, primarily due to a reversible cause often being
present. In up to 50% of cases ventricular fibrillation (VF) is the cause. A protocol
has been developed and published by the European Association for Cardiothoracic
Surgery. In the situation described above, the patient is being paced, so underlying
VF would not be immediately obvious.
Accordingly, the appropriate first step would be to cease pacing, check the
underlying rhythm and defibrillate as indicated. If 3 DC shocks are unsuccessful,
300 mg amiodarone can be given whilst preparing for sternotomy.
If no dysrhythmia is present, attention should then turn to other reversible causes
such as tamponade, tension pneumothorax and haemorrhage. Asystole or severe
bradycardia would be treated with pacing (in this instance via the epicardial wires)
or atropine pending immediate sternotomy.
Concurrent management would include verification of endotracheal tube
placement, ventilation with 100% oxygen, CPR and further DC shocks every 2
minutes in the case of an ongoing shockable rhythm.
Immediate use of adrenaline, and especially doses of 1mg, followed by correction
of a reversible cause and restoration of cardiac output may lead to severe rebound
hypertension and consequent bleeding. Answer A would not be an appropriate first
step in this instance.
Dunning J, Fabbri A, Kolh PH, et al. EACTS Clinical Guidelines Committee. Guideline for resuscitation in
cardiac arrest after cardiac surgery. Eur J Cardiothorac Surg 2009; 36(1):3–28.
173
174
Chapter 5
4.A Fibreoptic intubation with a single-lumen tube and a
right sided bronchial blocker
Anaesthetists are often asked to isolate and selectively ventilate a single lung to
improve the surgical field. Lung isolation is achieved by collapsing the lung in the
operative hemithorax and can be achieved by the use of double lumen tubes,
bronchial blockers and endobronchial tubes. Familiarity with the advantages
and disadvantages of these different techniques is important, particularly when
presented with patients who are likely to have a difficult intubation and need postoperative ventilation.
In the case above, the safest way to establish an appropriate airway is by performing
an awake oral or nasal fibreoptic intubation with a single lumen tube followed
by insertion of a right sided bronchial blocker to collapse the operative lung. A
bronchial blocker is a balloon tipped device which can be inserted down a single
lumen endotracheal tube and be placed under fibrescopic guidance into main
bronchi or lobar segments to cause distal lung deflation. Bronchial blockers can
be useful in patients with difficult airways when there is a plan to ventilate postoperatively, since a potentially hazardous tube exchange at the end of the operation
is avoided. Compared to double lumen tubes however, bronchial blockers achieve
less reliable and slower lung deflation with an increased likelihood of intra-operative
dislodgement. The inflated balloon also prevents access to the deflated lung for
suctioning or oxygen delivery.
Double lumen tubes consist of a tracheal and an endobronchial tube attached to
one another in parallel thereby allowing isolation of either lung when correctly sited.
They are divided into right and left-sided tubes according to the orientation of the
endobronchial tube within the tracheobronchial tree. Since the right upper lobe
bronchus arises in closer proximity to the carina when compared to the left, there
is a higher risk of inadvertent upper lobe collapse when right sided tubes are used.
Advantages of double lumen tubes over bronchial blockers include the ability to
deflate and re-expand both lungs easily intra-operatively (Table 5.3). There is also
unimpeded access to either lung for bronchoscopy, suctioning and oxygen delivery.
Since double lumen tubes are large diameter and pre-shaped, they may be difficult
to site in patients with a limited mouth opening (case above) or with distorted lower
airway anatomy.
Table 5.3 Advantages of double lumen tube and bronchial blockers
Double lumen tubes
Bronchial blockers
Rapid lung deflation
Slower lung deflation
Allows rapid isolation of either lung
Time consuming to change isolated lung
Allows suctioning, oxygen delivery to either lung
No access distal to the inflated balloon
Difficult to site in smaller airways
Easier to site in smaller airways
Requires tube exchange in intubated patients
Easy to use in intubated patients
Does not allow lobar blockade
Allows selective lobar blockade
Answers
An uncut single lumen tracheal tube can be advanced into a bronchus to isolate the
lungs in emergency situations such as an acute contralateral tension pneumothorax or
airway haemorrhage. For elective operations however, the use of double lumen tubes
or bronchial blockers are better choices for controlled lung isolation (Figure 5.3).
Lung isolation with a
bronchial blocker
Lung isolation with a
left double lumen tube
Single lumen
eal
endotracheal
tube
Right sided
bronchial
blocker
Tracheal cuff
Bronchial
ronchial cuff
Left main
bronchus
bro chus
Right main bronchus
Left main
bronchus
R
Right
chus
main bro
bronchus
Figure 5.3 Correctly places bronchial blocker and double lumen tube.
Rarely, patients may require lung isolation via a tracheostomy and double lumen
endobronchial tracheostomy tubes are available for this purpose. In the above
scenario where there has been previous surgery and radiotherapy to the neck, the
formation of a tracheostomy may be technically challenging.
Campos J. Lung isolation techniques for patients with difficult airway. Curr Opin Anaesthesiol 2010;
23(1):12–7.
Brodsky J. Lung separation and the difficult airway. Br J Anaesth 2009; 103(suppl 1):66–75.
5. D Hyperbaric prilocaine 2% 2 mL with 10 µg fentanyl
A spinal anaesthetic in this patient with significant respiratory disease avoids the
need for airway manipulation and ventilation, with the risks of increased airway
reactivity, pneumothorax and postoperative respiratory compromise. Selective
spinal anaesthesia is a technique favoured in day surgery that describes a block
concentrated on the operative site and aims for a predominately sensory rather than
complete motor block. In higher risk day surgery patients it allows earlier recovery
and mobilisation and avoids the cardiovascular instability associated with more
extensive spread.
175
176
Chapter 5
The ideal agent for such a block would:
•
•
•
•
have a rapid onset
provide a dense predictable sensory block
have a short duration of action to allow early recovery and ambulation
have a favourable side-effect and safety profile
Hyperbaric prilocaine 2% has been licensed for spinal use in the UK since 2010 and
is now widely accepted as the agent of choice for day surgery. It has both a rapid
onset and resolution of block and confers a higher degree of cardiovascular stability
compared to bupivacaine.
Low doses of hyperbaric bupivacaine can achieve selective blockade but doses
higher than 7 mg are associated with urinary retention especially in those having
urology procedures and those older than 70 years. Plain solutions are slightly
hypobaric at 37oC and less predictable as they produce greater variability in spread,
so are less likely to result in a selective block.
Lignocaine has an early onset time and a short duration of action, but has been
associated with TNS (transient neurological symptoms – self-limiting pain and
dysaesthesia in the buttocks) especially after day surgery in the lithotomy position.
Fentanyl acts synergistically with the local anaesthetic allowing reduced dose and
prolonged analgesia. Using small doses (10–25 µg) avoids respiratory depression and
is less likely to cause pruritus.
Before attempting to mobilise after a spinal anaesthetic, patients should have
return of perianal sensation, plantar flexion of the foot to pre-operative strength
and proprioception of the big toe, and discharged after voiding and other standard
criteria have been met.
British Association of Day Surgery (BADS). Spinal anaesthesia for day surgery patients; a practical guide.
3rd Ed. London: BADS, 2013.
Black AS, Newcombe GN, Plummer JL, McLeod GH, Martin DK. Spinal anaesthesia for ambulatory
arthroscopic surgery of the knee: a comparison of low dose prilocaine and fentanyl with bupivacaine and
fentanyl. Br J Anaesth 2011; 106(2):183–8.
6.C Sending an urgent U&Es, FBC and osmolality, and
prepare intravenous lorazepam in case of further seizure
Transurethral resection of the prostate (TURP) is a common procedure, and the best
available treatment for benign prostatic hyperplasia (BPH) with obstructive lower urinary
tract symptoms. TURP syndrome is caused by the absorption of hypotonic irrigation
fluid. The quantity of absorbed fluid is important and the probability of developing TURP
syndrome increases with the following factors which all increase absorption:
• Length of resection, especially > 1 hour
• Significant bleeding, implying large quantities of open vessels
• Bladder or prostatic capsular perforation, (fluid is rapidly absorbed from the
peritoneum)
• Height of the irrigation fluid bag. This corresponds to the hydrostatic pressure
within the bladder. Heights > 70 cm are unusual
The syndrome is caused by changes in:
Answers
Volume
This is biphasic in nature. Initially, the circulation absorbs large volumes and there
can be hypertension with a reflex bradycardia. This may also cause signs and
symptoms of volume overload with left sided heart failure and pulmonary oedema.
Later as the irrigation fluid shifts to the extracellular space (due to its hypotonic
composition), there may be a relative hypovolaemia and hypotension. It’s worth
bearing in mind that the first stage of hypertension is often masked by the low
systemic vascular resistance (SVR) state of a spinal sympathetic block.
Treatment of hypervolaemia resulting in left ventricular failure (LVF) involves
frusemide, but hypervolaemia without LVF is better treated with mannitol as this
lowers serum sodium less than frusemide. Hypotension and reduced heart rates are
addressed with vasoconstrictors, calcium and atropine.
Plasma sodium and osmolality
The hyponatraemia of TURP syndrome is mainly dilutional, and produces headaches,
nausea and vomiting, seizures and coma. However, of the two values, osmolality
is by far the more important. This is because rapid falls in osmolality cannot be
countered by pumps in neuronal cell walls, and the cells thus get flooded with water
down its osmotic gradient, leading to cerebral oedema and increased intracranial
pressure. If osmolality is relatively normal, low sodium does not need treatment in an
asymptomatic patient. Sodium should only be corrected slowly to prevent pontine
demyelination, and only correct until symptoms resolve, not to normal values.
Treatment of hyponatraemia should be titrated to symptoms, slowly, not > 1 mmol/L/
hour. Remember to measure the osmolality also. If the sodium is < 120 mmol/L, give
3% NaCl (weight in kg x 0.6 x 2 = number of mL 3% NaCl needed to elevate sodium
by 1 mmol/L).
Glycine
Although glycine is an inhibitory neurotransmitter, it does have effects increasing
NMDA receptor activity. This can produce the phenomenon of dis-inhibition,
such that the first neurological symptoms may be of irritability and seizures. As
concentrations increase, coma may follow. Due to its physiological antagonist
action at NMDA receptors magnesium is a useful second line treatment for seizures
associated with TURP syndrome.
Treatment of seizures is supportive and if needed involves benzodiazepines such as
lorazepam and if required magnesium.
The first stems A and B suggest treatments primarily focussed on seizure control.
While the possibility of a further seizure should be at the forefront of one’s mind,
a self-terminating isolated seizure may not require treatment. Instead the focus
should be on identifying the severity of the condition and thus determining whether
specific treatment is required, as in stem C. Empirical treatment without knowing the
sodium or osmolarity first may be dangerous (E), and treatment with frusemide (D) is
reserved for heart failure secondary to fluid overload.
Milligan L J, Bellamy M C. Anaesthesia for transurethral resection of the prostate. Contin Educ Anaesth Crit
Care Pain 2009; 9(3):92–96.
177
178
Chapter 5
7. A Remifentanil infusion
The middle ear is a delicate air filled cavity containing three ossicles which transmit
sound vibrations from the eardrum to the cochlea. Due to its small size, location
and fragile content, the provision of anaesthesia for surgery to this unique site is
especially challenging.
Maintaining the surgical field is difficult since small amounts of bleeding or
movements can significantly degrade the view during microsurgery. Furthermore,
the use of neuromuscular blocking drugs to provide akinesia is frequently restricted
due to the need for intraoperative facial nerve monitoring. A smooth, cough-free
wake up is desirable to avoid compromising the surgical result, and patients are at
an increased risk of developing post-operative nausea and vomiting.
Remifentanil is the most appropriate drug to use in this scenario since it addresses a
number of problems associated with middle ear surgery anaesthesia in addition to
providing adequate intraoperative analgesia. To minimise blood loss, remifentanil
can be used to rapidly control the blood pressure to deliver safe hypotensive
anaesthesia and a stable pulse in suitable patients. Remifentanil also allows
mechanical ventilation without neuromuscular blocking agents which enables
uninterrupted facial nerve monitoring. Remifentanil also attenuates coughing on
emergence, and if used in conjunction with propofol as part of a total intravenous
anaesthetic, reduces the incidence of post-operative nausea and vomiting.
Ketamine produces intense analgesia and dissociative anaesthesia via NMDA
receptor antagonism at both spinal cord and central sites. It can however cause
hypertension due to an increased sympathetic outflow which can result in bleeding
into the surgical field. Another drawback is the risk of emergence delirium and
coughing due to hypersalivation after extubation. For these reasons, it is not the
most appropriate option.
Nitrous oxide produces analgesia by inducing endogenous opioid release centrally.
Unfortunately, since the relative solubility of nitrous oxide in blood is far greater than
that of nitrogen, it will diffuse into the middle ear cavity at a more rapid rate than
nitrogen can leave. Subsequent raised middle ear pressures can cause displacement
of tympanoplasty grafts and promote nausea and vomiting, making this option
inappropriate.
Clonidine is a central acting presynaptic α2 adrenoceptor agonist with numerous
effects which lend themselves favourably to anaesthesia for middle ear surgery.
Not only does clonidine provide intraoperative analgesia, but also a reduction in
sympathetic outflow and therefore hypotension to minimise blood loss. Its sedative
effects may also contribute to a smooth wake up. In contrast to remifentanil
however, clonidine does not obviate the need to administer neuromuscular blocking
drugs which will interfere with facial nerve monitoring.
Magnesium is a versatile drug also with many favourable pharmacodynamic
properties. As a result of its NMDA receptor antagonism, magnesium provides
analgesia. It also inhibits smooth muscle contraction and has a direct vasodilator
effect which causes hypotension. Magnesium does impede neuromuscular
transmission by inhibiting acetylcholine release at the pre-synaptic nerve terminal,
Answers
but this is not enough on its own to cause paralysis and allow safe, controlled
ventilation.
Ravi R, Howell T. Anaesthesia for paediatric ear, nose and throat surgery. Contin Educ Anaesth Crit Care
Pain 2007; 7(2):33–37.
Liang S, Irwin M. Review of anaesthesia for middle ear surgery. Anesthesiol Clin 2010; 28(3):519–28.
Stoelting R, Hillier S. Pharmacology and Physiology in Anesthetic Practice, 4th ed. Philadelphia: Lippincott
Williams & Wilkins, 2005.
8. B Propofol and rocuronium
The choice of anaesthetic agents for ECT depends on the ability to:
• provide rapid onset and recovery from unconsciousness
• provide adequate muscle relaxation to avoid injury from an uncontrolled tonicclonic seizure
• have minimal effect on the seizure duration or quality
The original gold standard was methohexital as it has minimal anticonvulsant
properties, rapid induction and recovery, and a wide therapeutic range. However, it
has now been replaced by newer hypnotic agents, and the widespread availability
of propofol, its good cardiovascular stability profile and quick emergence properties,
mean that it is the most commonly used agent. Low doses such as <1 mg/kg are
used to avoid reducing duration of seizures. Etomidate may reduce seizure threshold
allowing lower currents to be used, but has a pronounced hyperdynamic response
and long emergence times. Thiopentone reduces the duration of seizures and
there is an increased arrhythmia risk. Inhalational induction with sevoflurane has
a reduced seizure duration compared to methohexital and is time consuming for
the anaesthetist. It is important that whichever agent is chosen, the same one is
used throughout the course of treatment to avoid influencing changes in seizure
threshold. Combining with opioids may reduce seizure duration but overall has an
induction agent sparing effect.
Muscle relaxants are essential in preventing uncontrolled convulsions and
musculoskeletal injury. Succinylcholine is still the most commonly used, typically a
dose of 0.5 mg/kg.
Mivacurium is short acting and doses 0.15 mg/kg should be used to control
muscle movements. Individuals with variations in the genes coding for the
pseudocholinesterase enzyme exhibit prolonged neuromuscular blockade. 4
alleles are described depending on the degree of enzyme inhibition; normal (Eu),
atypical or dibucaine resistance (Ea), fluoride resistant (Es) and silent (Es). 96% of
the population is homozygotes for the normal gene. Homozygotes for the atypical
or silent gene exhibit prolonged paralysis for up to 4 hours and homozygotes for
the fluoride resistant up to 2 hours. Heterozygotes exhibit mild prolonged paralysis
up to 10 minutes. Both suxamethonium and mivacurium are contraindicated in
cases of pseudocholinesterase deficiency, even in heterozygotes with intermediate
dibucaine numbers. Rocuronium or vecuronium are the most appropriate
alternatives, in view of the increasing availability of sugammadex.
Uppal V, Dourish J, Macfarlane A. Anaesthesia for electroconvulsive therapy. Contin Educ Anaesth Crit Care
Pain 2010; 10(6):192–97.
179
180
Chapter 5
9. A Mansour’s approach
The merger of the anterior rami of spinal nerves L4, L5, S1, S2, S3 and S4 forms the sacral
plexus. This plexus provides sensory and motor innervation to the posterior thigh, most
of the lower leg and the foot. The two most important branches for the lower limb
surgery are the sciatic nerve and the posterior femoral cutaneous nerve of the thigh.
The sciatic nerve is derived from the ventral rami of L4–S3 and is the longest and
widest nerve in the body. It supplies the posterior thigh and almost the entire lower
limb below the knee. It exits the pelvis through the greater sciatic notch below the
piriformis muscle to enter the lower limb between the ischial tuberosity and the
greater trochanter. The sciatic nerve then descends in the posterior thigh toward the
popliteal fossa where it runs posterolateral to the popliteal vessels in the upper part
of the fossa.
The sciatic nerve is actually a mixture of two nerves from its origin (tibial and
common peroneal nerves). In the pelvis, the two nerves are packed together by
connective tissues to form the sciatic nerve. At the proximal pole of the popliteal
fossa, the sciatic nerve divides into its component nerves. Sometimes, the two
components separate early at the upper thigh or even in the pelvis.
The posterior femoral cutaneous nerve (PFCN) is found in the pelvis from the
anterior rami of S1, S2 and S3. This is purely a sensory nerve and it descends with
the sciatic nerve in the upper part of the thigh. It gives off the inferior cluneal nerve
(sensation to the lower buttock), perineal branches (sensation to the external
genitalia), and femoral and sural branches (sensation to the back of the thigh and
calf ). It ends in the popliteal fossa where it anastomoses with the sural nerve.
The most common indications for sciatic nerve block are anaesthesia and
postoperative analgesia for foot and ankle surgery. It is also useful for operations
above the knee, and for management of chronic pain conditions in the lower limbs
such as sciatic neuropathy.
Various approaches have been described to block the sciatic nerve because of its
deep location and the difficulties associated with positioning.
Mansour’s parasacral block: Mansour describes this block in 1993. It is the most
proximal approach to sciatic nerve and mainly used to provide analgesia following
major ankle and foot surgeries. It is more than an isolated sciatic nerve block
because it may block the entire sacral plexus, and this is advantageous for knee and
above the knee operations when compared with distal sciatic nerve approaches. It
reliably blocks the two components of sciatic nerve and the PFCN.
The patient is positioned in the lateral decubitus position and a line is drawn
connecting the posterior superior iliac spine (PSIS) and the ischial tuberosity. The
point of insertion is 6 cm caudal from PSIS along this line. A 100 mm insulated
block needle is used because the nerve is deep in this area. The motor response is
inversion and planter flexion (tibial) or dorsiflexion and eversion (peroneal) that can
be elicited at a depth of 7–9 cm.
Answers
Labat’s transgluteal approach: This is a posterior approach to the sciatic nerve
(Figure 5.4). The patient is positioned in Sims’ position (lateral decubitus with a slight
forward tilt) with the operative side up and hip flexed. Three lines are drawn. Line 1 is
connecting the PSIS and the greater trochanter (GT), line 2 is extended from the GT
to the sacral hiatus and line 3 is dropped perpendicularly from the midpoint of line 1
to intersect line 2. The needle entry point is where line 3 and line 2 meet. A 100 mm
22G block needle is used and inserted perpendicular to all planes. The sciatic motor
response is usually observed at around 5–8 cm depth.
Figure 5.4 Mansour's and
Labat's approaches.
(Mansour’s approach)
Parasacral (Man
1. Posterior supe
superior iliac spine
2. Isc
Ischia
hi l tuberos
Ischial
tuberosity
Needle
insertion point
6 cm
1
2
approac
pp
Labat’s approach
e
1. Posterior supe
superior
iliac spine
2 Greater trocha
a
2.
trochanter
Sacral
r hiatus
3. Sac
1
1/2
2
1/2 º
90
Needle insertion
ion point
3
Raj approach (lithotomy subgloteal): This has the advantages of supine
approach to the sciatic nerve and easy landmarks. The patient is posited in a
supine position with both hip and knee flexed. A line is drawn extending from
the greater trochanter and the ischial tuberosity. The sciatic nerve twitches are
elicited by inserting a 100 mm 22G block needle perpendicularly at the line
midpoint. (Figure 5.5)
181
182
Chapter 5
Figure 5.5 Raj's and Beck's
approaches.
Raj’s approach
1. Ischial tuberosity
2. Greater trochanter
1
2
Needle insertion point
Beck’s anterior approach
1. Anterior superior iliac spine
2. Public tubercle
3. Greater trochanter
2
1
Needle insertion point
3
Beck’s anterior approach: This approach to a sciatic nerve block has the advantage
of maintaining the patient in the supine position and the lower limb in the neutral
position. A longer needle (150 mm) is needed because the nerve is deep to the
adductors. Three lines are drawn: line 1 connects the anterior superior iliac spine and
the pubic tubercle, line 2 is parallel to line 1 but drawn from the greater trochanter,
and line 3 is dropped perpendicularly from the junction of the medial and the
middle thirds of line 1 to intersect line 2. The needle insertion point is where line 3
intersects line 2. This block is technically challenging and requires a deep insertion of
the needle, hence can be a painful block to perform awake (Figure 5.5).
Guardini’s subtrochanteric approach: This block uses a lateral approach to the
sciatic nerve with a supine position and neutral lower limb. The point of entry is 4 cm
distal and 2 cm inferior to the greater trochanter. A 100 mm 22G needle is used to
perform this block. It is not a common approach because it is technically difficult to
perform and may be painful (Figure 5.6).
Popliteal approach: this is the most common approach to sciatic nerve because the
nerve is superficial and easy to find either by a peripheral nerve stimulator (PNS) or
ultrasound (US) technique (Figure 5.6).
There are two approaches to PNS guided popliteal block: posterior and lateral.
Answers
Figure 5.6 Guardini's and
popliteal approaches.
Guardini’s subtrochanteric approach
Greater trochanter
Needle insertion point
Semimebranous
medial
Popliteal nerve block
L
Popliteal
creases
7 cm
Needle
insertion
point
M
Biceps
femoris
(lateral)
L
M
Sciatic
nerve
Posterior approach: with the patient prone, a triangle is drawn in the popliteal fossa.
The popliteal crease forms the base, the biceps femoris tendon forms the lateral
border and semimembranosus tendon forms the medial border. A line is drawn
connecting the apex to the midpoint of the base. The needle entry point is 1 cm
lateral to this midline and around 7–9 cm above the skin crease (base). A 50 mm 22G
block needle is used for this block and 25–40 mL of local anaesthetic may be used.
In most people, the sciatic nerve divides into tibial and common peroneal nerves
near the apex of the popliteal fossa (8–10 cm above the crease). However, in some
patients, as previously mentioned, the nerve separates more proximally. Therefore,
multi-stimulation or US-guided technique is advocated for a successful block.
Lateral approach: with the patient supine and the hip flexed to 30 degrees and the
groove between the vastus lateralis and biceps femoris is palpated. A 100 mm 22G
block needle is inserted perpendicularly about 7–9 cm above the popliteal fossa
crease. The common peroneal nerve is stimulated in this approach.
Ultrasound guided popliteal nerve block: a linear high frequency US probe is
placed parallel to the popliteal fossa crease. Then the probe is moved proximally
until the popliteal artery pulsation is seen. The sciatic nerve (or its two components)
is generally located lateral and superficial to the popliteal artery. The best place to
inject local anaesthetic is just before the division of the sciatic nerve. This can be
obtained by tracing the two components upwards until a single nerve is seen.
183
184
Chapter 5
Enneking K, Chan V, Greger J. Lower-extremity peripheral nerve blockade: essentials of our current
understanding. Reg Anesth Pain Med 2005; 30(1):4-35.
Al-Haddad MF, Coventry DM. Major nerve blocks of the lower limb. Br J Anaesth CEPD Reviews 2003;
3(4):102–105.
10. D Axillary brachial plexus block
Patients undergoing upper limb surgery have several options of anaesthesia,
including local, regional and general anaesthesia. Brachial plexus block represents
the most common use of nerve blocks in current regional anaesthetic practice.
There are different approaches to block the brachial plexus. According to the site of
the surgery they are divided into two groups: blocks above the clavicle (interscalene
and supraclavicular) and blocks below the clavicle (infraclavicular and axillary).
Interscalene blocks are mainly indicated for shoulder and upper arm surgery. This
approach targets the upper roots (C5-C7) and, because of the vertical arrangement
of the brachial plexus roots in the interscalene groove, C8 and T1 nerve roots are
missed, hence the ulnar nerve may not be blocked. Therefore, this approach is
unreliable for hand and forearm surgery. Because the phrenic nerve runs anterior
to the anterior scalene muscle, local anaesthetic injection at this level will almost
always lead to a phrenic nerve blockade and may present a significant problem in
patients with respiratory compromise, while the rare but important side effect of
pneumothorax is also a possibility. The interscalene approach to a brachial plexus
block is therefore is unsuitable in this clinical scenario.
Supraclavicular blocks are performed at the level where the brachial plexus trunks
are in close proximity to each other so the entire upper limb is blocked reliably.
The usual indications of this block are arm and hand surgery, but it can also be
used for shoulder surgery if a suprascapular block is performed separately. Ulnar
sparing might be a problem with the supraclavicular approach because of the
medial location of the inferior trunk in this area; however the use of ultrasound
might overcome this problem. The incidence of pneumothorax in supraclavicular
blocks is high due to the proximity of the brachial plexus to the dome of the pleura
at this level. However, the risk of pneumothorax can be reduced with a modified
approach and the use of ultrasound. This block may present a danger for patients
with respiratory problems such as emphysema, hence should be avoided unless
performed by anaesthetists with extensive skill in this technique.
Infraclavicular blocks are performed at the level of the cords of the brachial plexus
(See Figure 4.1). It blocks each of the three cords of the brachial plexus and therefore
it anesthetises the entire arm successfully. It is a simple block to perform without
the aid of ultrasound; however, the infraclavicular approach to brachial plexus block
is not popular because of the fairly high failure rate and the risk of pneumothorax.
The use of ultrasound significantly improves the success rate of this block but is
remains a difficult procedure to perform. This block is not suitable for patients with
respiratory compromise, again due to the high pneumothorax risk, particularly with
a medial infraclavicular approach.
The safest and the most commonly used and studied brachial plexus approach is
the axillary block. It has few side-effects and usually covers the entire upper limb
Answers
with the exception of the lateral part of the arm and the forearm, which requires
additional musculocutaneous nerve block. This approach blocks the brachial
plexus terminal branches and depends on the relationship of nerves to the axillary
vessels. It is usually performed for elbow, arm and hand surgery. With no risk of
pneumothorax and phrenic nerve block, the axillary block is the most suitable
brachial plexus approach for patients with respiratory problems and lung diseases,
and is therefore the most appropriate choice of block in this scenario.
Radial, ulnar and median nerves can all be easily blocked in the arm as well.
However, the duration of the regional anaesthesia tends to be shorter than with
brachial plexus blocks. It is also limited by the requirement to block several nerves
and the application tourniquet for most surgery. Therefore, this mid-arm peripheral
nerve block is not the optimal option to consider in this clinical scenario.
Al-Haddad MF. Brachial plexus blockade. Br J Anaesth CEPD Reviews 2002;2;2: 33-36.
Neal JM. Upper extremity regional anesthesia. Essentials of our current understanding. Reg Anaesth Pain
Med 2009; 34(2):134–70.
11. B Use security staff to hold the patient, and give 4 mg/kg
ketamine intramuscularly, then transfer to rhesus
The usual tenets of sedation applicable in the elective situation are not necessarily
appropriate in the emergency setting. The important issues here are consent,
holding/restraint as well as the provision of safe sedation.
Consent
At the age of 17 the patient is legally still a child. If she were able to demonstrate
maturity and understanding and be judged to be Gillick competent, she would be
able to give her consent. When it comes to refusing treatment the child may not do
this in the same way, even if competent. A parent may still be able to consent for the
child in this case. In the case of a parent refusing treatment on behalf of their child,
(which the medical team believe is indicated), an interim care order may be granted
by the Courts allowing treatment.
In this scenario, the child lacks capacity. In England a doctor may act to provide
treatment in the best interests of a child, even without parental consent. In this
case parental assent/consent was available. All clinical information should be
nevertheless clearly documented, alongside the reasons for the treatment plan, and
a consent Form 4 could also be used for procedures, e.g. the CT/lumbar puncture.
Holding and restraint
In general, the principle is to use restraint only as a technique of last resort. Minimal force
required for safety (of staff and patient) should be employed, by appropriate numbers of
experienced and trained staff. The plan should be discussed with the parent beforehand,
and opportunity for a discussion with parent and child should exist afterwards.
Answering notes
In this instance, oral medication is impractical (in option D), and as outlined above
the legal case to intervene is clear, ruling out the attractive option of C. This leaves
185
186
Chapter 5
the use of intramuscular, intravenous or inhalational methods alongside minimal
restraint. Most emergency departments would lack the facility of an anaesthetic
machine, thus the degree and duration of restraint needed to transfer this girl to
theatre and perform an inhalational induction makes option E impractical and
dangerous. Holding to achieve intravenous access may be reasonable, but the
choice of agents is not, as the CT scan and bloods should be relatively painless
therefore the fentanyl in option A may not be required, as such the increased
number of agents only serves to increase risks. In addition, a single dose of
midazolam is unlikely to be successful for the duration of the investigations required.
Thus, the option which minimises holding, involves only one agent, and provides an
appropriate duration would be intramuscular ketamine. Thought does have to be
given to inserting intravenous access and establishing safe monitoring for transfer,
which is probably best achieved in a resuscitation area.
Tan L, Meakin GH. Anaesthesia for the uncooperative child. Contin Educ Anaesth Crit Care Pain 2010;
10(2):48–52.
12. A Urine output volume measurement
This question is testing your knowledge and reasoning in an attempt to differentiate
between two common causes of hyponatraemia in a patient with a head injury. The
differential diagnosis is between syndrome of inappropriate anti-diuretic hormone
(SIADH) and cerebral salt wasting (CSW).
Hyponatraemia is serious: in-hospital mortality is increased by 2–4 times and a
difference in survival outcome is still present at 1-year follow-up. Correcting the serum
sodium concentration is also hazardous and if done too rapidly may precipitate severe
neurologic complications, such as central pontine myelinosis, which can produce
spastic quadriparesis, swallowing dysfunction and pseudobulbar palsy.
The classic way to differentiate between causes of hyponatraemia is to assess fluid
balance (see Table 5.4).
CSW is a condition that is poorly understood. Proposed mechanisms include
increased sympathetic activity causing a higher glomerular filtration rate and excess
atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) release resulting
in reduced renal water re-absorption.
It occurs most commonly in traumatic brain injury and presents in the first week
after injury and is normally self-limiting. The key clinical feature is hypovolaemia
with a high urine output production. The serum osmolarity may be normal or high
and urinary sodium is usually raised. The management involves replacing sodium
and water with 0.9% sodium chloride and if symptoms develop (anorexia, confusion,
unconsciousness and seizures) hypertonic saline may be indicated.
SIADH occurs as a result of traumatic brain injury, sub-arachnoid haemorrhage, brain
tumors and meningitis. Excess ADH results in increased water absorption from the
collecting duct of the nephron. The key clinical feature is hypervolaemia and low
urinary volume. The plasma has a low serum osmolarity due to the dilutional effect
of excess water and the urine osmolarity is usually high. The management involves
restricting water intake.
Answers
Table 5.4 Establishing the cause of hyponatraemia by assessing fluid status
Fluid status
Pathophysiology
Conditions
Hypovolaemic
Sodium and water loss
Cerebral salt wasting
Renal loss:
• Diuretics
• Ketonuria
• Glycosuria
• Addison’s disease
Gastrointestinal loss:
• Diarrhoea and vomiting
Other:
• Sweating
• Bleeding
Normovolaemic
Sodium loss
without water loss
SIADH
Diuretics
Addison’s disease
Hypothyroidism
Iatrogenic
Hypervolaemic
Excess water
SIADH
Cardiac failure
Hepatic failure
Renal failure
Iatrogenic
In the intensive care unit great care is paid to getting the ‘numbers’ right. The fluid
balance is often adjusted according to a planned daily target. Central venous
pressure is of dubious benefit and a discrete value as is offered here is unhelpful.
Peripheral oedema may be multi-factorial and may be apparent even in the presence
of intravascular volume depletion. Osmolarity measurements are important in
making the diagnosis but in both differential diagnoses it may be normal and a
urinary sodium concentration is the more discerning test.
Considering the available options in the question above, urine output is the most
important piece of information: a high urine volume being produced in CSW and a
low urine volume being produced in SIADH.
Bradshaw K, Smith M. Disorders of sodium balance after brain injury. Contin Educ Anaesth Crit Care Pain
2008; 8(4):129–33.
Sushrut P, Waikar S. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J
Med 2009; 122(9):857–65.
13. C Give 20 mmol of intravenous magnesium sulphate over
10–20 minutes
This child has acute severe asthma and has failed to respond adequately despite
optimal first line therapy. Though at risk of further deterioration, the severity of his
current condition does not warrant intubation and positive pressure ventilation
– both of which may be hazardous. There is no evidence to support an additional
dose of nebulised salbutamol, or the use of intravenous bronchodilators.
187
188
Chapter 5
The next intervention likely to reverse his current pathophysiology is intravenous
(as opposed to nebulised) magnesium sulphate although the optimal regime
remains controversial.
Somasundaram K, Ball J. Medical emergencies: pulmonary embolism and acute severe asthma.
Anaesthesia 2013; 68(suppl 1):102–16.
14. D Administer 2 g intravenous magnesium and optimise
the serum potassium concentration
Atrial fibrillation (AF) is a common problem in the critical care environment with up
to 15% of medical critical care patients developing AF at some point during their
stay.
The risk factors for developing AF are:
Patient factors:
•
•
•
•
•
•
•
Age > 65 years old
Disease severity
Hypertension
Previous AF
Congestive heart failure
Chronic obstructive pulmonary disease
Previous use of calcium-channel blockers, beta-blocker or angiotensin-converting
enzyme-inhibitor and withdrawal of catecholamine infusions
Acute illness:
• Hypoxia
• Cardiac ischaemia
Sepsis or systemic inflammatory response syndrome
• Fluid shifts (hypervolaemia and hypovolaemia)
• Low serum magnesium and potassium
Iatrogenic
• Intra-cardiac catheter: central line or pulmonary artery catheter
AF probably occurs as a result of a final atrial insult (the last straw) on the
background of chronic disease most commonly hypertensive or ischaemic
myopathy. A sudden change in atrial dimensions as a result of filling pressures
(either too high with fluid or too low with dehydration and sepsis), a change in
electrochemical gradients across the myocyte (potassium and magnesium flux) or an
ischaemic event are the common precipitating factors.
In health the atria contribute around 10% of cardiac output, increasing to 30%
during exercise. This is well tolerated in patients with normal left ventricular function
but in patients who depend on the higher filling pressures, loss of the ‘atrial kick’
Answers
results in low cardiac output. In addition the tachycardia results in poorer coronary
blood flow and increased myocardial oxygen demand, which can result in even
poorer ventricular performance. Patients in AF stay longer in ICUs and have an
increased mortality in a general population but a causative relationship is hard to
prove in medical or cardiac ICUs.
Management of acute compromised AF (as in this scenario) is not that easy from
an exam point of view: most intensivists practice on their experience and there are
no randomised controlled trials to base your decisions on. Advanced Life Support
guidelines suggest direct current (DC) cardioversion in the peri-arrest scenario and
all critical care recommendations are based on a mixed group of studies, which
compare effective treatments. So what do you do?
In summary, the available evidence suggests:
• Magnesium is more effective than amiodarone in restoring sinus rhythm, equally
effective as amiodarone at achieving rate control and is safe
• Amiodarone infusion converts AF into sinus rhythm in 70% of cases in the first
12 hours in medical critical care patients and 75% within 48 hours in general ICU
population
• In a mixed population with left ventricular impairment amiodarone did not cause
significant haemodynamic compromise but transient hypotension may occur in
systemic illness
• The success rate of DC cardioversion in post-surgical and medical critical care
patients is low and the recurrence rate is high
• Digoxin is not effective in this population
Given the information above, and that the single best answer questions test
judgment and reasoning (not just recall of life-support algorithms) the question can
be re-visited. DC cardioversion requires sedation, which takes time to organise no
matter where you do it. It also has a low chance of success in this patient group and
a high chance of recurrence as the presumed ischaemic focus has not been dealt
with. Expediting the angiography may be prudent but you must stabilise the patient
first. The choice between amiodarone and magnesium is less obvious, but given that
magnesium causes less hypotension and is at least as effective as amiodarone at rate
and rhythm control, this is the most appropriate first step.
M Sleeswijk, TVanNoord, J Zijlstra, Clinical review: treatment of new-onset atrial fibrillation in medical
intensive care patients: a clinical framework. Crit Care 2007; 11(6):233.
15. B Glasgow coma scale
Most scoring systems use the Glasgow coma scale (GCS) or include data from the
GCS to assess the degree of neurological system failure. Furthermore, the GCS
frequently makes up a large component of the acute physiology score or equivalent.
For example, GCS constitutes 25% of the physiological score in Acute Physiology
and Chronic Health Evaluation (APACHE) II, 20% in APACHE III and 22% in Simplified
189
190
Chapter 5
Acute Physiology Score (SAPS) II. The explanation for this is that in multivariant
analysis of admission physiological variables, GCS is often the most highly predictive
of hospital mortality.
Ball JAS, Redman JW, Grounds RM. Severity of illness scoring systems – do they tell us what we want to
know? In: Vincent J-L (ed). Intensive Care Medicine Annual Update 2002. Berlin: Springer-Verlag, 2002:
911–933.
16. B 20 mL/kg 0.9% sodium chloride
Don’t panic – this question isn’t actually testing your knowledge of the big fluid trials
that have been published in the last couple of years (although they are interesting).
This is a question of judgement and emergency management.
Even though the history seems complicated, here is a case of classic sepsis or septic
shock (depending on how much fluid has been given so far). The more complicated
aspects include liver failure which produces a multitude of problems when trying to
assess fluid balance:
• Sodium and water retention due to failure to metabolise steroid hormones
(including aldosterone) result in oedema
• Ascites and peripheral oedema may develop due to portal hypertension
• Cardiac failure may occur secondary to chronic volume overload, due to the
causative disease process itself (e.g. alcoholic cardiomyopathy) or a pericardial
effusion
These patients are often intra vascularly volume depleted associated with total body
water overload, which is harder to recognise and manage.
The lactate in Hartmann’s solution is usually metabolised very quickly in the liver into
bicarbonate which then acts as a buffer within the plasma. In this case administering
lactate-containing solutions to a septic patient who hyperlactaemic and is unable
to metabolise it is counter-intuitive. In some analysis colloid administration is
associated with an increased incidence of renal impairment, length of stay in ICU
and mortality (which extends beyond the use of starch containing solutions). Also
in terms of cardiovascular parameters there is no difference between crystalloid and
colloid administration. See Table 5.5 for a quick summary of the fluid trials.
Considering the options in the question, the choice remains between 0.9% sodium
chloride administration and vasopressor administration. As you have not been told
how much intravenous fluid has been administered (as is often the case), with the
knowledge that resuscitation on medical wards tends to be on the conservative
side and with a patient that needs immediate intervention the choice in this case is
0.9% sodium chloride (although this is contentious in a patient with liver cirrhosis).
A timely and appropriately aggressive intervention is probably the most important
factor in this case.
Bartels K, Thiele R, Gan T. Rational fluid management in today’s ICU practice. Crit Care 2013; 17(suppl 1):S6.
Strunden M, Heckel K, Goetz AE, Reuter D. Perioperative fluid and volume management: physiological
basis, tools and strategies. Ann Intensive Care 2011; 1(1): 2.
Answers
Table 5.5 Recently published fluid trials
Trial
Summary
Interpretation
RaFTinG
Rational fluid treatment in Germany.
Prospective registry analysis of a
database of 4,500 patients receiving
fluid treatment 2010–11. Colloid vs
crystalloid
No difference between HES and
crystalloid (HES was avoided in AKI).
Gelatins increased risk of AKI
CRISTAL (JAMA
2013)
Any colloid vs and crystalloid given
throughout ICU stay. Multi-national
RCT of 2,800 patients
Colloids decreased mortality at 90 days
in septic and septic shock sub groups,
no difference in 28-day mortality
CHEST
(NEJM 2012)
Crystalloid vs HES. 7 mL/kg administered in first 4 days. 7,000 patients RCT
No 90-day mortality difference, but
higher risk of needing renal replacement therapy in the HES group
ALBIOS
(NEJM 2014)
20% albumin + crystalloid vs crystalloid based on patients albumin level.
1,800 patients RCT
No difference in 28-or 90-day mortality
between groups
SAFE (NEJM
2012)
4% albumin vs normal saline, blinded
RCT with 7,000 patients
No difference in 28-day mortality,
ventilator days and length of stay
17. E Misoprostol
This woman has a history of rheumatic fever and may well have valvular heart
disease. Stenotic valvular lesions can lead to fixed cardiac output states, with atrial
contraction being more essential for adequate ventricular filling. Tachycardia or
tachyarrhythmias will compromise this and lead to reductions in cardiac output,
hence the need to maintain sinus rhythm. The systemic vascular resistance must also
be maintained, as well as the preload.
Uterotonics are necessary in this situation to control the ongoing haemorrhage,
however, they can precipitate pulmonary oedema in patients with cardiac disease.
Syntocinon can cause vasodilatation, tachycardia and pulmonary oedema, hence
potentially compromising the cardiac output in fixed output states. It has been
stated that the bolus dose of syntocinon should be avoided in severe cardiac
disease, and an infusion used instead. Ergometrine can cause hypertension and
increase the risk of myocardial infarction and pulmonary oedema. Carboprost also
has the potential to cause pulmonary overload.
Transfusion-related acute lung injury (TRALI) can occur following transfusion of
blood products, and leads to pulmonary oedema, hypotension and hypoxia.
Misoprostol is a prostaglandin E1 analogue and although there are rare reports of
pulmonary oedema in the literature, it is unlikely to have caused this fast an onset of
pulmonary oedema via rectal administration. It is therefore the least likely cause of
this patient's apparent pulmonary oedema.
Burt CC, Durbridge J. Management of cardiac disease in pregnancy. Contin Educ Anaesth Crit Care Pain
2009; 9(2):44–47.
191
192
Chapter 5
18. C Antepartum haemorrhage
The differential diagnosis of this presentation includes all of the above answers.
It is clinically difficult to distinguish between amniotic fluid embolism (AFE) and
pulmonary embolism, as they can both present with cardiovascular and respiratory
compromise. Certain aspects of this case pointing more towards AFE include the
advanced maternal age, multiparity and onset during labour. AFE is one of the six
direct causes of death as identified in the most recent Centre for Maternal and Child
Enquiries (CMACE) report (2006–2008). The other five are:
•
•
•
•
•
Sepsis (commonest cause)
Pre-eclampsia and eclampsia
Thrombosis and thromboembolism
Early pregnancy deaths
Haemorrhage
Management of AFE is supportive, which may include intubation and ventilation
and delivery of the baby.
Anaphylaxis and tension pneumothorax can also cause the above symptoms
and auscultation of the chest would reveal wheezing or absent breath sounds
respectively.
Although haemorrhage causes hypotension, tachycardia and tachypnoea, it does
not usually present with a sudden onset of breathlessness and hypoxia.
Lewis G. Centre for Maternal and Child Enquiries (CMACE) – Saving mother’s lives: reviewing maternal
deaths to make motherhood safer: 2006-2008. The Eighth Report of the Confidential Enquiries into
Maternal Deaths in the United Kingdom. BJOG 2011; 118 (suppl. 1):1–203.
Dedhia JD, Mushambi MC. Amniotic fluid embolism. Contin Educ Anaesth Crit Care Pain 2007; 7(5):152–156.
19. C Postpone anaesthesia and surgery until the infant is
adequately fluid resuscitated and the acid-base balance
corrected
Pyloric stenosis is not a surgical emergency, but is a medical emergency. Gastric
outlet obstruction and vomiting of gastric acid cause dehydration, hypovolaemia
and a hypokalaemic, hyponatraemic, hypochloraemic metabolic alkalosis. Preoperative rehydration and correction of acid-base and electrolyte abnormalities
should be the immediate treatment goal.
There is little or no gastric emptying with pyloric stenosis. Aspirating the gastric
content with a nasogastric tube and performing a rapid sequence induction are
sensible precautions, but are not be the immediate anaesthetic management.
There is increased risk of postoperative apnoea with pyloric stenosis. Using local or
regional anaesthesia to minimise postoperative analgesic opioid requirement and
arranging close post operative monitoring are sensible, but are not the immediate
anaesthetic management.
Fell D, Chelliah S. Infantile pyloric stenosis. BJA CEPD Reviews 2001; 1(3):85-88.
Peutrell JM, Wilkins DG. Pyloric stenosis in full term babies. A postal survey of the management by
paediatric anaesthetists. Pediatr Anesth 1994; 4:93–97.
Answers
20. E Have two further attempts at laryngoscopy. Check
head and neck position, laryngoscopy technique,
external laryngeal manipulation and adequate paralysis.
Consider using a different laryngoscope, a smaller tube, a
stylet or a bougie.
The Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI)
and the Difficult Airway Society (DAS) published several joint guidelines on airway
management in children in 2012 (Figure 5.7). In an unanticipated difficult tracheal
intubation during routine induction of anaesthesia, when mask ventilation is
satisfactory, no more than four attempts should be made at direct laryngoscopy and
intubation. After four attempts, the secondary tracheal intubation plan should be
initiated, which may include proceeding with surgery with a supraglottic airway device
if appropriate, fibreoptic intubation if indicated, or postponing surgery otherwise.
In this clinical scenario, it would therefore be most appropriate to optimise patient
position, laryngoscopic technique and consider the use of alternative equipment.
The Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI) and the Difficult Airway
Society (DAS). Unanticipated Difficult Tracheal Intubation – During Routine Induction of Anaesthesia in a
Child Aged 1 to 8 Years (Guidelines). London: APAGBI-DAS, 2012.
21. C Give 10 mg ketamine intravenously
Poorly controlled pain at the time of surgery is now thought to predispose to chronic
post surgical pain. This patient has already received a large dose of morphine
without much effect so further loading is also likely to be ineffectual. Midazolam
should not be used as a treatment for pain. Tramadol is a general opioid receptor
agonist but has particular affinity for the μ receptor. It also prevents the re-uptake of
noradrenaline and serotonin so may confer some benefit.
Ketamine is an NMDA antagonist that non-competitively blocks the NMDA receptors
resulting in an ‘anti-hyperalgesic’ and ‘anti-tolerance’ effect. Ketamine has been
shown to reduce pain intensity by up to 25% and reduce analgesic requirements by
up to 50% in the first 48-hours postoperatively.
Doses of greater than 30 mg in a 24-hour period do not result in improved pain
scores. In this setting major side-effects are uncommon.
Clonidine is thought to confer some analgesic benefit but is less effective than
ketamine and non-steroidal anti-inflammatory drugs. It also results in unwanted
hypotension and bradycardia.
Ramaswamy S, Wilson J, Colvin L. Non-opioid-based adjuvant analgesia in perioperative care. Contin Educ
Anaesth Crit Care Pain 2013; 13(5):152–157.
22. C Intermittent pain
There are three different sensations patients may experience in amputated limbs:
• Stump pain: This is pain localised at the surgical site
193
No
Yes
SpO2 >80%
SpO2 >80%
Attempt intubation:
• Consider paralysis
Fail
Succeed
Go to scenario cannot intubate
cannot ventilate (CICV)
Proceed
Wake up patient
Continue
Maintain anaesthesia/CPAP
Deepen anaesthesia (Propofol first line):
• If relexant given – intubate
• If intubation not successful, go to unanticipated
difficult tracheal intubation algorithm
Consider:
• SAD (e.g. LMA™) malposition/blockage
• Equipment malfunction
• Bronchospasm
• Pneumothorax
Call for help again if not arrived
Consider deepening anaesthesia
Use CPAP
Depth of anaesthesia
Call for help
Figure 5.7 The Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI) and the Difficult Airway Society (DAS) joint guidelines on airway management
in children in 2012. (Reproduced with permission from the Association of Paediatric Anaesthetists of Great Britain and Ireland.)
Good airway
• Insert SAD (e.g. LMA™) not > 3 attempts
• Consider nasopharyngeal airway
• Release cricoid pressure
Step C second-line: Insert SAD (e.g. LMA™)
Assess for cause difficult mask ventilation:
• Light anaesthesia
• Laryngospasm
• Gastric distension – pass OG/NG tube
Step B Insert oropharyngeal airway
Consider changing:
• Circuit
• Mask
• Connectors
if equipment failure is suspected. change to self-inflating
bag and isolate from anaesthetic machine promptly
Check equipment
Give 100% oxygen
Difficult mask ventilation (MV) – during routine
induction of anaesthesia in a child aged 1–8 years
Consider:
• Adjusting chin lift/jaw thrust
• Inserting shoulder roll if <2 years
• Neutral head position if >2 years
• Adjusting cricoid pressure if used
• Ventilating using two person bag mask technique
Step A optimise head position
Difficult MV
APA
194
Chapter 5
Answers
• Phantom sensations: This occurs when the patient feels that the limb is present
but is not always painful
• Phantom pain: This is pain that arises in the imagined, amputated limb
Phantom pain, occurring in 30–85% of post-amputation patients, is very difficult
to treat and tends to respond poorly to opioids. Various pharmacological therapies
have been trialled, with some success with calcitonin, amitriptyline and gabapentin,
although non-pharmacological therapies have an important role. Pre-emptive
epidural analgesia has not been shown to reduce the incidence of development of
phantom limb pain. The pain is most commonly intermittent and only rarely does
the pain become constant. In this patient therefore, true phantom pain is most
likely suggested by pain that is intermittent in nature.
Nikolajsen L, Jensen TS. Phantom limb pain. Br J Anaesth 2001; 87(1):107–116.
23. E Thoracic epidural
Thoracotomy ranks amongst the most painful of surgical procedures. Apart
from patient discomfort, the consequences of post-thoracotomy pain lead to
several other complications. Reduced tidal volumes from shallow breathing
and the inability to cough may result in hypoxia and hypercarbia, placing the
patient at increased risk of developing respiratory failure and postoperative
pneumonia. This is further complicated by increased myocardial oxygen
demand from the sympathetic response to pain, which may precipitate an
adverse cardiac event.
There are several possible options for achieving analgesia. What method is chosen
depends on patient, anaesthetic and surgical preference (Table 5.6).
In the above clinical scenario therefore, the most appropriate analgesic option
would be a thoracic epidural.
Hughes R, Gao F. Pain control for thoracotomy. Contin Educ Anaesth Crit Care Pain 2005; 5(2):56–60.
24. C Perform a coeliac plexus block
A coeliac plexus block can be used to relieve autonomically mediated pain from
non-pelvic abdominal organs. It is most commonly used in intractable malignant
pain. Firstly it would be performed with local anaesthetic to assess efficacy and then
can be repeated as a neurolytic block with 6% aqueous phenol.
The coeliac plexus consists of coeliac ganglia that lie on either side of the L1
vertebral body. It provides the autonomic supply to the non-pelvic abdominal
organs and the first two-thirds of the large intestine.
It consists of:
• Greater splanchnic nerve: T5–T6 to T9–T10
• Lesser splanchnic nerve: T10–T11
• Least splanchnic nerve: T11–T12
195
196
Chapter 5
Table 5.6 Analgesic options for thoracotomy pain
Method
Description
Epidural analgesia
Thoracic epidural sited at the level of the midpoint of the scar is considered
gold standard
Disadvantages:
failure rate of 15%; bilateral sympathetic block (hypotension)
technical difficulty; intercostals muscle paralysis (hypoventilation)
risk of spinal cord damage; urinary retention
Intrathecal morphine
Morphine is less lipid-soluble than diamorphine or fentanyl. Given intrathecally, this allows a more cranial spread, making it appropriate for thoracic
surgery.
Good analgesia for 12–24 hours postoperatively
Disadvantages:
delayed respiratory depression and sedation if spreads too high
cannot be topped up so additional analgesia eventually required
Paravertebral block
Unilateral block, which reduces the limitations of a bilateral epidural block,
e.g. hypotension, hypoventilation, urinary retention. There is also less risk
of spinal cord damage. Can be placed by surgeon under direct vision, and a
catheter can be left in situ
Disadvantages:
only suitable for unilateral surgery
Intercostal block
Quick and simple to perform
Disadvantages:
short acting,
usually misses the posterior division of the nerve, so posterior pain common
Interpleural block
Injection between visceral and parietal pleura at appropriate level; can be
placed by surgeon
Disadvantages:
May be ineffective due to pooling in dependent lung or loss through chest
drain
The left and right vagal trunks supply the parasympathetic supply to the upper
abdominal organs.
This block is certainly not without its risks and should only be used once other
avenues have been exhausted.
The potential complications include profound hypotension, bleeding from aortic or
inferior vena caval injury and sexual dysfunction. Should the phenol be injected into
the arterial supply of the spinal cord this can even result in paraplegia.
A lumbar sympathetic block would have no benefit in pancreatic pain. Similarly a
paravertebral block from T8–T10 would be necessary to block the innervation to the
pancreas.
Menon R, Swanepoel A. Sympathetic blocks. Contin Educ Anaesth Crit Care Pain 2010; 10(3):88–92.
Answers
25. C Single shot caudal combined with 10 mg/kg
paracetamol orally 6-hourly and codeine phosphate
1 mg/kg orally 6-hourly as required
Despite having immature nociceptive pathways, it is now well accepted that
neonates experience pain and as such, post operative pain needs to be well
managed. As with adults, a multimodal approach should be used to minimise sideeffects.
Paracetamol is the most commonly used analgesic both in the adult and paediatric
populations and should be used as a base in most analgesic regimes.
However as per the British National Formulary (BNF) the paracetamol dose varies:
Orally:
• Preterm neonate 28–32 weeks post-conceptual age 20 mg/kg loading dose
followed by 10–15 mg/kg 8–12-hourly. Maximum dose 30 mg/kg daily
• Neonate over 32 weeks post-conceptual age 20 mg/kg loading dose followed by
10–15 mg 6–8-hourly. Maximum dose 60 mg/kg daily
Intravenously:
• Preterm neonate over 32 weeks post-conceptual age 7.5 mg/kg 8-hourly.
Maximum dose 25 mg/kg daily
• Neonate 10 mg/kg 4–6 hourly. Maximum dose 30 mg/kg daily
Non steroidal anti-inflammatory drugs (NSAIDs) should also be used in children
wherever possible. However, ibuprofen is not recommended for neonates or infants
under 5 kg and diclofenac is not recommended for infants under 6 months.
Opiates should also be used with care in this setting. Codeine is a pro-drug that
is metabolised to morphine via the p450 cytochrome. The particular enzyme
responsible, CYP2D6, has low activity at birth and becomes more effective with
age. In addition to its immaturity, it also exhibits genetic polymorphism leading to
significant differences in efficacy between patients. This explains its good safety
profile in the young but is perhaps not the best analgesic agent. However, the
combination of paracetamol and codeine has been shown to reduce postoperative
pain in infants.
Morphine is also commonly used and can be administered via a number of different
routes. Reduced doses should be used in neonates due to their increased potency.
This is due to a combination of an immature blood-brain barrier and reduced
protein binding. Morphine will also have a longer duration of action due to slower
metabolism (immature enzymes) and reduced excretion (reduced glomerular
filtration rate).
Local anaesthetic, whether in the form of surgical wound infiltration, nerve block
or regional technique, should be used wherever possible. Caudals remain the most
popular central neuroaxial technique used in neonates. Opioids are not commonly
added to the local anaesthetic due to concerns over postoperative respiratory
depression. In the neonates, caudals result in adequate analgesia below T10.
197
198
Chapter 5
Williams G. Analgesic regimens for children. In: AAGBI Core Topics in Anaesthesia. Johnston I, HarropGriffiths W, Gemmell L, eds. London: AAGBI, 2012.
Haidon JL, Cunliffe M. Analgesia for neonates. Contin Educ Anaesth Crit Care Pain 2010; 10(4): 123–27.
Gormley SMC, Crean PM. Basic principles of anaesthesia for neonates and infants. BJA CEPD Reviews 2001;
1(5):130–33.
26. D Cyanide poisoning
In the Western world, the most common cause of cyanide poisoning is house fires
and subsequent smoke inhalation. When exposed to high temperatures, products
containing carbon and nitrogen may liberate cyanide during combustion. These
materials include wool, silk and synthetic polymers.
Cyanide toxicity is dangerous as it prevents aerobic cell metabolism, causing
intracellular hypoxia by reversibly binding to cytochrome oxidase a3 within
the mitochondria, which is essential for oxidative phosphorylation. Oxidative
phosphorylation is crucial to the synthesis of adenosine triphosphate (ATP) and
the continuation of cellular respiration. As supplies of ATP become depleted,
mitochondria cannot extract or use the oxygen they are exposed to. As a result,
metabolism shifts to glycolysis through anaerobic metabolism which produces
lactate. Production of lactate results in a high anion-gap metabolic acidosis. The
cells are no longer able to use oxygen for aerobic metabolism which results in high
venous oxygen saturations.
Signs and symptoms of cyanide poisoning occur soon after exposure. Early
manifestations include anxiety, headache and mydriasis. As hypoxia progresses, GCS
drops and seizures can occur.
Cyanide poisoning should be suspected in burns patients with an unexplained and
persistent lactic acidosis despite adequate fluid resuscitation.
Currently there is no test available for rapid diagnosis of cyanide poisoning, so
treatment should be based on clinical suspicion. The treatment of choice for
cyanide poisoning in burns patients is hydroxocobalamin. Hydroxocobalamin
binds to cyanide to form the non-toxic cyanocobalamin (vitamin B12) which is
then excreted by the kidneys. Cyanide has a greater affinity for hydroxocobalamin
than for cytochrome oxidase a3 within the mitochondria. This then allows the
mitochondria to perform aerobic metabolism. As it binds with cyanide without
forming methaemoglobin, it is particularly helpful in burns patients who may have
part of their haemoglobin in the form of carboxyhaemoglobin thus already reducing
their oxygen carrying capacity.
Cyanide (CN–) is metabolised in any of the three following pathways:
• Converted by rhodanase in liver to thiocyanate (SCN–) which is then excreted in
urine. This is the major pathway, accounting for 80% of CN– metabolism
• Combines with vitamin B12 to form cyanocobalamine (non-toxic) which is also
excreted in the urine
• Combines with methemoglobin to form cyanomethemoglobin (non-toxic)
Sepsis can be a major problem in the burns patient but not at this early stage
and prophylactic antibiotics are not advocated. Volume depletion is also a likely
Answers
contender but not in the context of a good urine output and normal capillary refill
time. Acute kidney injury (AKI) in burns patients can also be problematic but again
too early to show such gross acid base anomalies. AKI may be due to either volume
depletion or rhabdomyolysis, the latter of which is a particular problem in electrical
burns.
Substance abuse must always be considered in this group of patients and alcohol
intoxication also leads to a lactic acidosis but not of this severity.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–22.
Hamel J. A review of acute cyanide poisoning with a treatment update. Crit Care Nurse 2011; 31(1):72–81.
27. C Optimise his circulatory blood volume
Renal impairment is a significant postoperative complication following elective
aortic aneurysm repairs. It is associated with prolonged hospital stay, risk
of progression to renal replacement therapy and increased mortality. The
pathophysiology of renal impairment during an aortic aneurysm repair is
multifactorial. It involves decreased blood flow across the renal arteries during
aortic cross-clamping, cholesterol emboli as a result of clamping a heavily calcified
aorta, the use of nephrotoxic medication in the preoperative phase and ischaemiareperfusion syndrome. Over the last decade several drugs listed as options in
the question have been researched in an attempt to find one to prevent the
development of acute kidney injury. Low dose dopamine and dopexamine were
used in an attempt to stimulate diuresis postoperatively. Free radical scavengers
such as mannitol given before or soon after aortic cross-clamping also failed
to show a decrease in postoperative renal impairment. Except for achieving an
optimum intravascular volume by replacing losses and correcting any coagulation
abnormalities, all the other strategies have failed to produce a positive result.
Frederick JR, Woo YJ. Thoracoabdominal aortic aneurysm. Ann Cardiothorac Surg 2012; 1(3):277–28.
28. B Wilson’s disease
Kayser-Fleischer rings (brown or dark rings encircling the iris) are pathognomonic
of Wilson’s disease which is an autosomal recessive inherited disorder characterised
by toxic accumulation of copper in the liver and brain. The ATP7B enzyme prevents
excessive accumulation of copper by either combining it with caeruloplasmin and
releasing it into the bloodstream, or secreting it in the bile. The functions of this
enzyme are affected in Wilson’s disease, causing the toxic accumulation of copper in
the blood.
Children usually present with hepatic complications such as hepatitis, cirrhosis
or fulminant hepatic failure. Adults tend to present with neurophsychiatric signs
including dysarthria, tremors, seizures, migraine, ataxia, cognitive decline and
behavioral disturbances.
Kayser-Fleischer rings are caused by deposition of copper in the Descemet’s
(basement) membrane and can be visualised by slit lamp examination. Treatment for
199
200
Chapter 5
Wilson’s disease consists of administering chelating agents like penicillamine or in
extreme cases hepatic transplantation.
Alpha-1 antitrypsin is a protease inhibitor and its deficiency leads to cholestasis
and pulmonary symptoms including emphysema. Primary biliary cirrhosis is
caused by damage of interlobular bile ducts, leading to cholestasis coupled with
portal hypertension and cirrhosis. Haemochromatosis is caused by increased
iron absorption and deposition in the liver, heart or pancreas. Primary sclerosing
cholangitis is inflammation of intra- and extra-hepatic ducts, which leads to liver
failure and death.
Longmore M, Wilkinson I, Torok E. Oxford Handbook of Clinical Medicine, 8th ed. Oxford: Oxford University
Press, 2010.
29. B Mental state
The elderly proportion of society is expected to increase significantly over the
coming years, leading to a higher rate of surgery in this age group. The postoperative
morbidity associated with surgery in the geriatric population is high due to multiple
comorbidities and the influence of geriatric syndromes. These syndromes can be
collectively termed as a phenotype as they cannot be termed into a disease process
or an organ specific pathology. Frailty is thus termed as ‘a condition associated
with a decreased physiological reserve across various organ systems that can lead
to an increased vulnerability to physiological stressors'. Having a tool to measure
frailty helps to stratify this population according to their risks. Fried et al. originally
described the frailty phenotype based upon features observed across more than 500
patients over 65 years.
• Weight loss (unintentional): > 10 pounds from baseline in prior year
• Sarcopenia (loss of muscle mass): grip strength - lowest 20th population centile
(by gender and body mass index)
• Weakness: self-reported exhaustion
• Poor endurance: Walking time per 15 feet, slowest 20th population centile (by
gender and height)
• Slowness: kcal per week, lowest 20th population centile
• Low activity: males < 383 kcal/week, females < 270 kcal per week
Mental state is not incorporated in frailty assessment.
Positive frailty phenotype: > 3 criteria present
Intermediate or pre-frail : 1 or 2 criteria present
The frailty phenotype is predictive of progressive decline, repeated falls, hospital
visits and eventually death.
Griffiths R, Mehta M. Frailty and anaesthesia: what we need to know. Contin Educ Anaesth Crit Care Pain
2014; 14(6):273-277.
Answers
30. A 20
The number needed to treat (NNT) is the number of patients to whom a clinician
would need to administer a particular treatment for one patient to receive benefit
from it. The NNT is calculated either as:
• 100/absolute risk reduction (ARR) expressed as a percentage, or
• 1/ARR expressed as a proportion
The absolute risk reduction is defined as:
Control event rate – experimental event rate; which in the example given above
equates to:
25–20% = 5%
The NNT is therefore:
100/5 or 1/0.05 depending on whether the ARR is expressed as a percentage or
number. The NNT is therefore 20.
NNTs have a number of important limitations. The true value of a NNT can be higher
or lower than the value given; It is therefore useful to know the 95% confidence
intervals of the NNT. If there is a large confidence interval there can be less certainty
in the reported NNT and so clinical decisions based on this must be made with
caution.
An additional important point is that the NNT depends on the baseline frequency of
a given event. So, in the case of PONV, advances in perioperative care and surgical
techniques may mean that the baseline frequency of PONV changes over time; A
NNT of 8 observed for agent A based on a study from 1970 may not necessarily be
comparable to a NNT of 10 for agent B based on a similar study conducted in 2010.
McQuay HJ, Moore RA. Using numerical results from systemic reviews in clinical practice. Ann Intern Med
1997; 126:712–720.
Lalkhen AG, McCluskey A. Statistics V: Introduction to clinical trials and systematic reviews. Contin Educ
Anaes Crit Care Pain 2008; 8:143–146.
201
Chapter 6
Mock Paper 6
Questions
1. A 44-year-old woman is on the intensive care unit having had a grade 3
subarachnoid haemorrhage secondary to an anterior communicating artery
aneurysm one day ago. She is currently stable neurologically. Her past medical
history comprises of hypercholesterolaemia, hypertension and smoking. She has a
drug history of simvastatin and lisinopril.
Which of the following would most likely prevent the development of delayed
cerebral ischaemia in this patient?
A
B
C
D
E
‘Triple H therapy’
Magnesium administration
Statin administration
Nimodipine administration
Antiplatelet therapy
2. A 29-year-old woman who suffered a blow to the left side of her skull vault with
a resulting depressed fracture is awaiting transfer to a tertiary centre. She lost
consciousness for approximately 1 minute after the incident. Her GCS is currently
14/15 (E4 V4 M6).
Which of the following, in isolation, indicates that intubation is essential before
transfer?
A
B
C
D
E
Pao₂ of 13 kPa an Fio₂ of 0.6
A discrete and short-lived seizure en route to your hospital
Drop in GCS from E4 V4 M6 to E3 V4 M5 in the emergency department
An increase in respiratory rate leading to a Paco₂ of 4.0kPa
Blood in the oropharynx
3. A 65-year-old man presents to the emergency department with acute central
chest pain radiating to the back. He has a history of hypertension and smoking.
The ECG shows evidence of left ventricular hypertrophy and his blood pressure is
190/100 mmHg, heart rate 105 beats per minute. There is a collapsing pulse and an
early diastolic murmur.
204
Chapter 6
What is the next most appropriate management step?
A
B
C
D
E
Commencement of sodium nitroprusside infusion
Site an arterial line
Arrange urgent aortography
Titrate intravenous morphine
Arrange transfer to a cardiothoracic centre
4. A 65-year-old woman is recovering from an uneventful total thyroidectomy
as treatment for a large substernal goitre. On the third postoperative day, she
becomes progressively more stridulous and wheezy. She is tachypnoeic, confused
and complaining of circumoral paraesthesia. There is no obvious neck swelling or
pain.
What is the most likely cause of her symptoms?
A
B
C
D
E
Bilateral vocal cord paralysis
Tracheomalacia
Haematoma
Tracheal necrosis
Hypocalcaemia
5. A 36-year-old woman with an impacted food bolus needs to go to theatre
imminently. She has been unable to swallow her saliva for 24 hours. On inquiring
about her anaesthetic history she reports collapsing due to a severe allergic
reaction under anaesthesia, but she is unsure which agent was responsible. There
are no notes available, nor relatives to elaborate on the history.
Which of the following should you avoid as the most likely causative agent?
A
B
C
D
E
Rocuronium
Latex
Morphine
Chlorhexidine
Gelofusine
6. A 34-year-old man presents for laparoscopic excision of his left adrenal gland for
phaeochromocytoma. During your preoperative assessment, he tells you that he
has been taking medication for blood pressure for about a month.
Which of the following is most likely to indicate that he is prepared for surgery?
A
B
C
D
E
Good exercise tolerance, but a history of dizziness on standing
Lack of a history of palpitations, and a normal ECG
A normal echocardiogram, and chest X-ray
History of dizziness on standing, a 5-minute ECG with no premature
ventricular complexes, and nasal congestion
Several blood pressure recordings of < 160/90 mmHg
Questions
7. A 45-year-old man is admitted to the surgical ward with a fever, toothache and
neck discomfort. Whilst waiting for surgery you are called to his bedside as he
is more breathless and complaining of substernal pain. On examination he is
hypotensive and there is tender, ’woody‘ induration of his neck. On auscultation
you hear a pericardial rub.
Which investigation is most appropriate to guide management in this scenario?
A
B
C
D
E
Cervical and chest ultrasound
Cervical and chest computed tomography
Cervical and chest magnetic resonance imaging
Cervical and chest radiograph
Echocardiogram
8. A 35-year-old cyclist suffered a severe traumatic brain injury with a large subdural
haematoma and an associated C2–C3 cervical spine fracture. He is comatose and
apnoeic, with neurosurgeons confirming that he is not a candidate for surgery
due to poor prognosis. Confirmation of brainstem death is underway, with
examination of cranial nerves just being completed.
What is the next most appropriate test that will support the neurological diagnosis
of death?
A
B
C
D
E
Apnoea testing
Somatosensory evoked potentials
No further tests necessary
A second neurological examination of the cranial nerves
Electroencephalogram
9. An 84-year-old woman with an extracapsular hip fracture is scheduled for a
dynamic hip screw on your morning trauma list. On examination she has an
ejection systolic murmur in the aortic area and anaemia with a haemoglobin
of of 90 g/L. She has previously had a coronary stent and is on both aspirin and
clopidogrel. Your hospital's echocardiogram technician is unavailable.
How do you proceed?
A
B
Postpone the surgery until an echocardiogram can be performed urgently
Proceed with the case under general anaesthesia and invasive blood pressure
monitoring, with one unit of packed red blood cells
C Perform a spinal anaesthetic after administration of one pool of platelets
D Insert a lumbar epidural and use small volume incremental top-ups to achieve
a surgical block
E Proceed with the case under general anaesthesia and an ultrasound-guided
fascia iliaca block with invasive blood pressure monitoring
10. A 35-year old man for elective ankle surgery is to have an ultrasound guided
popliteal nerve block.
205
206
Chapter 6
What is the most frequently used combination of ultrasound view and needle
visualisation for this nerve block?
A
B
C
D
E
Short-axis view with in-plane needle approach
Long-axis view with out-of-plane needle approach
Short-axis view with out-of-plane needle approach
Long-axis view with in-plane needle approach
Any of the above combinations
11. You are called to the emergency department to assess a young woman that was
rescued from a house fire following a gas leak after being trapped confined in a
room. She is awake, with normal observations but suffered 10% body surface area
(BS) partial thickness burns over her arms and face. You are asked to transfer her
to the nearest burns unit that is 2 hours away. On examination she has singed nasal
hair, a normal airway and no change in voice. Burns resuscitation is underway with
intravenous fluids and analgesia.
What is the next step in ensuring her safe transfer?
A
B
C
D
E
Add the operating department practitioner to your transfer team
Full monitoring including invasive blood pressure measurement
Prepare difficult airway equipment for the transfer
Prepare Intubating equipment and drugs
Elective intubation of the patient
12. A 72-year-old man has been on the intensive care unit after being treated for an
infective exacerbation of his chronic obstructive pulmonary disease. He has been
mechanically ventilated for 5 days and has acceptable gas exchange. He has been
weaned to pressure support ventilation requiring 12 cmH2O inspiratory support
and 5 cmH2O of positive end-expiratory pressure (PEEP) with an inspired oxygen
concentration of 0.35. He is currently obeying commends.
How would you best assess his suitability for extubation?
A
Change the patient to continuous positive airway pressure (CPAP) and assess
ventilation and cardiovascular parameters for 30 minutes
B Reduce the pressure support gradually over the next 48 hours by 2 cmH2O per
12 hours and assess ventilation and cardiovascular parameters
C Reduce the inspired oxygen fraction to 0.25 and repeat an arterial blood gas 30
minutes later
D Repeat a chest radiograph to ensure resolution of his consolidative process
E Assess the patient’s sputum production and send a repeat sample for
microscopy to ensure clearance of the infective process
13. You are asked to review a 72-year-old man who was admitted to your intensive
care unit 6 hours ago following elective coronary artery bypass grafts. He is
haemodynamically stable with no evidence of end organ hypoperfusion. The
concern is that he has been slowly bleeding into his drains (total 570 mL since
theatre) and has slow oozing through his sternotomy wound and around his lines
Questions
and drains. His core temperature is 36.2°C and pH 7.32. An urgent full blood count
and clotting tests were sent 30 minutes ago and the results have just come back
and show: Haemoglobin concentration 78 g/L; platelet count 102 ×109/L; INR
1.4; aPTTr 1.6; fibrinogen 1.8 g/L; and ionised calcium 0.9 mmol/L. The patient is
on long-term aspirin 75 mg daily (not stopped for surgery). He received heparin
in theatre that was reversed with protamine. He also received a single dose of 1 g
tranexamic acid.
Given this information the most appropriate treatment strategy is:
A
1 unit packed red blood cells (pRBC) + 1 pool of platelets + 15 mL/kg fresh
frozen plasma (FFP) + 1 dose of cryoprecipitate
B 20 mmol of calcium chloride + protamine + 1 pool of platelets + tranexamic
acid
C 2 units packed red blood cells (pRBC)
D 20 mmol of calcium chloride + 1 pool of platelets + 15 mL/kg fresh frozen
plasma (FFP)
E Perform a thromboelastogram
14. A 60 kg, 55-year-old woman has been admitted to the intensive care unit with
severe community acquired pneumonia. Two days later she develops worsening
hypoxaemia with new bilateral infiltrates on chest radiography. She is currently
ventilated with the following settings:
• Fio2 1.0
• Inspiratory pressure (Pinsp) 35 cmH2O
• Positive end expiratory pressure (PEEP) 12 cmH2O
• Inspiratory:expiratory (I:E) ratio 1:1
• Tidal volume (Vt) 250 mL
An arterial blood gas reveals results shown in Table 6.1.
Based on current evidence, which of the following would be an appropriate next
step to improve her oxygenation and reduce mortality?
Table 6.1 Arterial blood gas test results
Parameter
Result
pH
7.28
Paco2
8.6 kPa
Pao2
7.1 kPa
Base excess
–3.4 mmol/L
Bicarbonate concentration (HCO3–)
21.4 mmol/L
Lactate
2.3 mmol/L
Haemoglobin concentration (Hb)
96 g/L
Glucose concentration
6.7 mmol/L
207
208
Chapter 6
A
B
C
D
E
Extracorporeal membrane oxygenation
Prone positioning
Inhaled nitric oxide
High frequency oscillation ventilation
Increase Pinsp
15. A 58-year-old man is brought in by ambulance following a house fire in an
enclosed area. He is confused with a GCS 14/15.
On examination he has singed facial hair with voice changes. He is noted to have
partial thickness burns to the front of his torso, bilateral palms and palmar aspect
of upper limbs. His body weight is 70 kg.
According to the Parkland formula his estimated fluid requirement in the first 8
hours following his burn is:
A
B
C
D
E.
7560 mL
4850 mL
4620 mL
3910 mL
780 mL
16. A male motorcyclist of unknown age has been transferred to hospital after having a
high-speed accident. The paramedics report states that the patient is unresponsive,
has chest, abdominal, pelvic injuries and a traumatic right leg amputation
currently secured with a tourniquet. The respiratory rate is 10 breaths per minute,
there is a weak carotid pulse and the Glasgow coma score is 3.
The trauma team members are present and you decide to prepare to intubate the
patient.
What technique is most appropriate?
A
B
Modified rapid sequence with rocuronium 1 mg/kg and midazolam 0.05 mg/kg
Rapid sequence induction with thiopentone 3 mg/kg and suxamethonium
1 mg/kg
C Modified rapid sequence induction with midazolam 0.05 mg/kg, fentanyl
1–3 µg/kg and rocuronium 1 mg/kg
D Modified rapid sequence induction with propofol 1–2 mg/kg, fentanyl 1–3 µg/
kg and rocuronium 1 mg/kg
E Modified rapid sequence with ketamine 2 mg/kg, fentanyl 1–3 µg/kg and
rocuronium 1 mg/kg
17. The obstetric registrar has asked you to review a 22-year-old woman on the postnatal
ward who underwent a Category 2 Caesarean section for chorioamnionitis 2 days
ago. She was otherwise previously fit and well. She has a respiratory rate of 28 breaths
per minute, a heart rate of 100 beats per minute, blood pressure of 92/50 mmHg
and oxygen saturations of 91% on air. She was prescribed intravenous antibiotics
postoperatively, but had only received one dose before being changed to oral
Questions
antibiotics as her cannula had tissued and the team had been unable to re-site
another. Her temperature is 38.7°C and she is complaining of abdominal tenderness.
What is the next most appropriate line of management?
A
High flow oxygen, blood cultures, intravenous fluids and urgent discussion
with microbiology consultant
B High flow oxygen, intravenous fluids and intravenous broad spectrum antibiotics
C High flow oxygen, intravenous fluids and intravenous paracetamol
D High flow oxygen, blood cultures, intravenous fluids and oral antibiotics
E High flow oxygen, blood cultures and intravenous fluids
18. A 4-year-old 18 kg girl is scheduled for elective squint surgery. She was born at 31
week gestation, was ventilated for 1 week, and then was on CPAP for a month. She
now suffers from recurrent episodes of wheeze and hospital admissions requiring
nebuliser therapy.
She takes salbutamol and beclomethasone inhalers regularly. Her mother reported
she had just recovered from another viral respiratory tract infection a week ago, but
no longer had any cough or coryzal symptoms. On examination, she is comfortable
with no respiratory distress. Her respiratory rate is 16 breaths per minute and her
oxygen saturation is 98% on air. On auscultation, there is a soft bilateral expiratory
wheeze.
The most appropriate management plan for this patient is:
A
Ask the mother to give the patient an extra dose of her salbutamol inhaler
before induction of anaesthesia
B Give the patient nebulised salbutamol before induction of anaesthesia
C Reschedule the surgery for when the patient is 6 weeks from the most recent
viral respiratory illness
D Give the patient a dose of intravenous steroid intraoperatively
E Refer the patient to the paediatric respiratory team for further management
19. A 10-year-old 24kg girl is scheduled on your day surgery list for an upper gastrointestinal endoscopy to investigate her unexplained recurrent abdominal pain.
There is no other significant past medical history. On preassessment, the patient was
anxious but both mother and patient agreed to a gaseous induction of anaesthesia.
On arrival in the anaesthetic room, the child is crying, combative and refusing to
cooperate. After 10 minutes in the anaesthetic room, the child only allowed you to
put on a pulse oximeter.
She is the final patient on the morning list, and the endoscopist has a clinic to
attend in the afternoon.
Your best plan of action is:
A
B
Send the child back to the waiting area to have a sedative pre-medication
Ask the mother to help restrain the child for a quick gas induction
209
210
Chapter 6
C
Give the child a dose of sublingual midazolam in the anaesthetic room as
premedication before induction of anaesthesia
D Give the child a dose of intramuscular ketamine in the anaesthetic room as
premedication before induction of anaesthesia
E Reschedule for another day with a plan for midazolam pre-medication on the
ward
20. A 6-year-old 20 kg girl is scheduled to have an emergency laparoscopic
appendicectomy. She is clinically stable and appears comfortable at rest. You
discover in your preoperative assessment that the patient’s maternal uncle has a
possible history of malignant hyperthermia, but the patient and both her parents
have not been investigated for malignant hyperthermia susceptibility (MHS).
The most appropriate anaesthetic management is:
A
Postpone anaesthesia and surgery until the possibility of MHS in the patient
has been investigated
B Postpone anaesthesia and surgery until more information is available about
the uncle’s history of malignant hyperthermia
C Proceed with anaesthesia and surgery, but with modified anaesthesia
technique to avoid known triggers for malignant hyperthermia
D Proceed with anaesthesia and surgery. Malignant hyperthermia is not
maternally inherited, so modification of anaesthetic technique is not required.
E Proceed with anaesthesia and surgery, but with a high vigilance for malignant
hyperthermia.
21. A 73-year-old woman suffering with depression and poorly controlled chronic
back pain who is taking paracetamol, diclofenac and fluoxetine is started on
tramadol. The following day, she presents to the emergency department with
tremor, confusion and restlessness. On examination she is febrile, hyperreflexic
and has mydriasis.
What is the most likely cause of her symptoms?
A
B
C
D
E
Opioid toxicity
Opioid withdrawal
Hyponatraemia
Serotonin syndrome
Anaphylaxis
22. A 41-year-old woman presents for repeated wide local excision for breast cancer,
and is due to have adjuvant radiotherapy. Her past medical history includes
diabetes and depression. She is worried about the operation, especially pain after
her surgery.
Which of the following is not a risk factor for chronic post-surgical pain?
A
B
Diabetes
Fear of surgery
Questions
C Repeated surgery
D Younger age
E Adjuvant radiotherapy
23. A 65-year-old man presents to the pain clinic with long-standing poorly controlled
lower back pain. He is frightened by the painful sensations and admits to feeling
depressed since he is no longer able to walk unaided.
Which of the following is the most appropriate assessment tool to evaluate his
painful experience?
A
B
C
D
E
Numeric rating scale
Visual analog scale
Verbal descriptor scale
McGill pain questionnaire
Wong–Baker FACES scale
24. You are asked to review an 84-year-old woman overnight on the ward with a right
hip fracture. The orthopaedic core trainee is unable to control her pain despite
administering paracetamol and 15 mg Oramorph.
What is the most appropriate next step for managing this patient’s pain?
A
B
C
D
E
Add gabapentin
Give a stat one off dose of ibuprofen
Start a patient controlled analgesia (PCA)
This patient needs emergency surgery
Perform a nerve block
25. A 59-year-old man with a 2 year history of type I complex regional pain syndrome
affecting his left leg presents to the pain clinic after a failed trial of epidural
injections and physiotherapy. He has a fentanyl patch and is taking paracetamol,
ibuprofen, amitriptyline and gabapentin. Despite this, he suffers from severe
debilitating leg pain, allodynia and hyperalgesia.
What intervention is the most appropriate next step in managing his symptoms?
A
B
C
D
E
Spinal cord stimulation
Radiofrequency lumbar sympathectomy
Below knee amputation
Guanethidine-sympathetic blockade
Non-invasive brain stimulation
26. You are pre-assessing a 6-year-old child in the day unit for re-do strabismus
surgery to the right eye. The mother tells you that the child underwent the
procedure six months prior and had to stay overnight due to intractable postoperative nausea and vomiting.
Which of the following is least likely to prevent a repeat of this?
211
212
Chapter 6
A
B
C
D
E
Avoidance of perioperative opioids
Atropine 20 µg/kg at induction
Ondansetron 0.15 mg/kg
Sevoflurane maintenance over desflurane
Ondansetron 0.15 mg/kg plus dexamethasone 0.15 mg/kg
27. You are called to the emergency department to assess a 65-year-old noninsulin dependent diabetic man presenting with an ischaemic foot. He also has
hypertension and exertional angina. He admits to getting progressively short of
breath over the last 6 months but he is able to climb one flight of stairs without
stopping. Physical examination reveals no basal crackles and heart sounds are
normal.
What is the next most appropriate step in the management of his acutely ischaemic
foot?
A
B
C
D
E
Delay surgery until an echocardiogram can be performed
Proceed to surgery without delay
Proceed to surgery after discussing the case with your consultant
Proceed to surgery after booking a bed in HDU/ITU
Delay surgery until an arteriogram to identify the location of the blockage can
be performed
28. An obese 45-year old patient has undergone an inguinal hernia repair under
general anaesthesia and a first generation supraglottic airway device was used. In
recovery, he becomes hypoxic and short of breath. You are suspecting a pulmonary
aspiration of gastric contents.
Which of the following lung segments is most likely to be contaminated following
an episode of aspiration during a general anaesthetic?
A
B
C
D
E
Apical segments of the lower lobes
Posterior basal segments of the lower lobes
Lateral segment of the right middle lobe
Lateral basal segments of the lower lobes
Apical segments of the upper lobes
29. A 17-year-old girl with a body mass index (BMI) of 15 has been brought to the
emergency department with a heart rate of 42 beats per minute and a blood
pressure of 76/34mmHg. Her respiratory rate is 10 breaths per minute and she is
complaining of epigastric discomfort. Her investigations reveal an atrioventricular
block and her blood gases demonstrate a metabolic alkalosis. Her mother states
that she has lost weight and has had amenorrhoea for the past six months.
The most likely diagnosis is:
A
B
C
Ectopic pregnancy
Duodenal perforation
Anorexia nervosa
Questions
D Acute hypothyroidism
E Opioid overdose
30. A 33-year-old man who suffers from chronic alcohol and drug abuse was admitted
to the intensive care unit with a head injury 5 days ago. He has been intubated and
ventilated since admission and has been receiving enteral nutrition. Whilst on the
unit he has developed refeeding syndrome.
Which of the following is the most appropriate management in this patient?
A
B
C
D
E
Omitting fluids containing potassium
Avoiding thiamine in his enteral feed
Infusion of 10% dextrose to correct hypoglycaemia
Infusion of phosphate
Infusion of calcium chloride to counter hyperkalaemia
213
214
Chapter 6
Answers
1. D Nimodipine administration
Delayed cerebral ischaemia describes neurological deterioration that occurs
secondary to ischaemia alone (i.e. not hydrocephalus or seizure activity) and persists
for greater than 1 hour. It develops in more than 60% of subarachnoid haemorrhage
(SAH) patients and confers a less favourable outcome. Patients are at greatest risk
of ischaemia from day 3 to day 10 post-SAH. Their risk is also augmented by a poor
grade of SAH (Table 6.2), a large volume haemorrhage within the subarachnoid
space or extending to the ventricles and a smoking history. Delayed ischaemia is
frequently labelled as intracranial vasospasm, but until confirmed by investigation
the two terms should be separately defined. They are treated in an identical fashion.
Table 6.2 Grade of SAH as classified by the World Federation of Neurosurgical Societies
(WFNS)
Grade
WFNS classification
1
No motor deficit + GCS 15
2
No motor deficit +
GCS 13–14
3
Motor deficit +
GCS 13–14
4
GCS 7–12
(motor testing irrelevant for score)
5
GCS 3–6
(motor testing irrelevant for score)
The use of triple H therapy (hypertension, hypervolaemia and haemodilution) is
now controversial. Those who advocate it do so in order to improve cerebral blood
flow by increasing cerebral perfusion pressure (CPP), volume status and blood
rheology. Targets for each are CPP > 70 mmHg, CVP 12–15 mmHg and haematocrit
0.3 respectively. More recent studies have failed to show conclusive benefits from
any element but it is widely accepted that hypovolaemia and hypotension are
deleterious. The patient’s premorbid blood pressure must also be acknowledged
when calculating a suitable target.
Hypermagnesaemia has been promoted as reducing the risk of cerebral ischaemia
as magnesium is a vasodilator and thought to have a role in neuroprotection. The
2011 IMASH trial (Intravenous Magnesium Sulphate in Aneurysmal Subarachnoid
Haemorrhage) failed to show any benefit but it is felt that further studies are needed
to ascertain the optimum level required to improve outcome. A magnesium level
below the normal range should definitely be corrected.
Answers
In addition to treating hypercholesterolaemia, statins have been found to modulate
the cytokine response. They also reduce the quantity of reactive oxygen molecules
produced in brain injury. Overall, the subsequent inflammatory response is
minimised and they have therefore been suggested as part of the treatment for
SAH to prevent vasospasm and delayed ischaemic injury. However, data from
the international, multicentre, randomised controlled STASH trial (Simvastatin in
Aneurysmal Subarachnoid Haemorrhage) published in 2014 suggests that there is
no short-term or long-term benefit to using statins in these patients, despite earlier
enthusiasm with the idea.
In 2007, a Cochrane review noted that antiplatelet therapy was associated with a
non-significant trend indicating a benefit to outcome in patients at risk of delayed
cerebral ischaemia. Unsurprisingly, this trend was counteracted by a parallel increase
in haemorrhage. Therefore antiplatelet agents, in this setting, are restricted to use
following endovascular stenting for SAH management.
The only proven effective treatment in the prevention of delayed cerebral ischaemia
is nimodipine. As a calcium antagonist it is thought to protect against vasospasm
and there is level 1 evidence that it improves outcome. Every patient with a
diagnosis of SAH should be started on nimodipine (60 mg every 4 hours) for a course
of 21 days. A side-effect can be systemic hypotension which can be avoided by the
more frequent administration of half doses. If this does not remedy the situation, the
blood pressure should take precedence.
All of these treatments have been considered in the prevention of delayed cerebral
ischaemia. Nimodipine is the only one to have withstood repeated testing with
consistent results.
Luoma A, Reddy U. Acute management of aneurysmal subarachnoid haemorrhage. Contin Educ Anaesth
Crit Care Pain 2013; 13(2):52–58.
2.B A discrete and short-lived seizure en-route to your
hospital
This patient has suffered a head injury by a mechanism significant enough to cause
a depressed skull fracture. This will most probably lead to an evolving brain injury
secondary to underlying contusions. It is important that she is managed in an
appropriate environment, to expedite swift treatment of any complications, and is
likely to involve further transfer to a tertiary hospital with on-site neurosurgical care.
Prior to transfer it is imperative to assess her ability to maintain her physiology such
that secondary brain injury is avoided as much as possible. This includes adequate
ventilation via a patent airway, preservation of an appropriate blood pressure
[cerebral perfusion pressure (CPP) = mean arterial pressure (MAP) - intracranal
pressure (ICP)] and optimisation of cerebral metabolism. The aim is to minimise
further rises in ICP and secure brain tissue perfusion following the suspected injury.
The following are suggested targets during transfer:
• Pao₂ > 13 kPa
• Paco₂ 4.5–5.0 kPa
215
216
Chapter 6
•
•
•
•
•
•
•
MAP > 80 mmHg
Adequate analgesia
Sufficient sedation (and therefore intubation) if agitated
Treatment of any seizures
Normothermia
Blood glucose 6–10 mmol
Optimal cerebral venous drainage – head-up, avoidance of neck ties
In the scenario given you are asked to choose an instance that would obligate
you intubate the patient in order to maintain each target en route. The AAGBI has
published guidelines for the safe transfer of head injured patients and they include
indications that should initiate intubation and ventilation before any journey:
•
•
•
•
•
•
•
•
Glasgow coma score < 8/15
Glasgow coma score drop of 2 points in the motor score
Pao₂ < 13kPa with oxygen administration
Paco₂ < 4.0 or > 6.0 kPa
Concern regarding laryngeal reflexes
Seizure(s) since the injury
Bilaterally fractured mandible
Significant bleeding threatening the airway
A Pao₂ of 13kPa whilst receiving an Fio₂ of 0.6 implies a significant alveolar to arterial
gradient. The value for Pao₂, however, is acceptable and there is scope to improve it
with optimal positioning and increased oxygen administration.
A drop in GCS from E4 V4 M6 to E3 V4 M5 is a drop of 2 points and significant
enough to warrant consideration of intubation prior to transfer but guidelines allow
for individual clinical decision making. Intubation is regarded as essential if 2 points
are dropped within the motor score.
An increased respiratory rate leading to hypocapnia in this patient could be as a
result of pain. If, despite treatment, this continues and reduces further to jeopardise
cerebral circulation then control of ventilation may be warranted.
Blood in the oropharynx may be small and resolved or ongoing, potentially
interfering with ventilation. Clinical examination and judgement are required to
assess whether this, in isolation, would necessitate intubation.
Seizures in the period following head trauma imply increased severity of the injury
and may recur to further increase intracranial pressure and cerebral metabolic
requirements. All of the options could trigger a decision to secure the airway before
transfer, but seizure activity makes it essential.
Dinsmore J. Traumatic brain injury: an evidence-based review of management. Contin Educ Anaesth Crit
Care Pain 2013; 13(6):189–195.
The Association of Anaesthetists of Great Britain and Ireland. Recommendations for the Safe Transfer of
Patients with Brain Injury. London: The Association of Anaesthetists of Great Britain and Ireland, 2006.
Answers
3. D Titrate intravenous morphine
The history and clinical signs are suggestive of aortic dissection with aortic
regurgitation. Other clinical signs relate to the area of the aorta involved and are
summarised in Table 6.3.
Table 6.3 Features associated with vascular anatomical areas involved
Anatomical area involved
Clinical feature
Aortic valve
Aortic regurgitation, cardiac failure
Coronary ostia
Coronary ischaemia
Carotid/brachiocephalic artery
Stroke, syncope, seizure
Subclavian artery
Limb ischaemia
Intercostal arteries (spinal arteries)
Lower limb weakness
Coeliac trunk, mesenteric arteries
Abdominal pain, bowel ischaemia
Renal arteries
Flank pain, renal failure
There are a number of risk factors for aortic dissection, including:
•
•
•
•
•
•
Hypertension (72% of patients)
Smoking
Trauma – deceleration and falls from height
Aortic surgery/cannulation
Vasculitis
Collagen disorders
There are two different classification systems of which the Stanford system is most
widely used. It denotes that dissections involving the ascending aorta are Type A
with all others as Type B.
The priorities are to make an accurate diagnosis, limit the stress on the aortic lumen
(by lowering systolic blood pressure and left ventricular contractility) and forming
a definitive treatment plan, which may include urgent transfer to a cardiothoracic
centre.
It is particularly important to diagnose Type A dissections (i.e. those involving
the ascending aorta) as these are considered surgical emergencies. Non-invasive
diagnostic methods have superseded traditional aortography (option C) with CT,
transthoracic and transoesophageal echo being the most common modalities
employed. Transthoracic echocardiography can be performed at the bedside but is
not able visualise the distal ascending and descending aorta reliably.
The management steps outlined by the European Society of Cardiology guidance
are shown below:
217
218
Chapter 6
•
•
•
•
•
Detailed medical history and physical examination
Intravenous line, blood samples, cardiac enzymes
ECG, heart rate and blood pressure monitoring (both sides)
Pain relief
Reduction of systolic blood pressure using beta-blockers/calcium channel
blockers + additional vasodilators if needed
• Diagnostic imaging
• Intensive care level monitoring – right radial arterial line as standard
Although pharmacological control of systolic hypertension may be required, a large
proportion of patients will have pain which may of course exacerbate hypertension.
Titrated morphine is therefore the most appropriate first step in this scenario. If
further blood pressure control is required, beta-blockers are recommended before
pure vasodilators such as sodium nitroprusside. Attainment of clinical stability and
institution of invasive blood pressure monitoring would usually be obtained before
transfer to a surgical centre, however planning for this possible eventuality early will
ensure timely subsequent management.
Survival after surgical repair of Type A dissection is 96% and 91% at 1 and 3 years
respectively. Complicated Type B aortic dissections may be amenable to treatment
with endovascular stents, although some centres are also treating Type A dissections
in this manner as well.
Poor prognostic factors at presentation include:
•
•
•
•
•
•
Age > 70 years
Hypotension, shock or tamponade at presentation
Preoperative renal failure
Preoperative bleeding/massive transfusion
Prior myocardial infarction
Abnormal ECG
Erbel R, Alfonso F, Boileau C, et al. Diagnosis and management of aortic dissection. Eur Heart J 2001;
22(18):1642–1681.
Hebballi R, Swanevelder J. Diagnosis and management of aortic dissection. Contin Educ Anaesth Crit Care
Pain 2009; 9 (1):14-18.
4. E Hypocalcaemia
It is important to remain vigilant for any signs of respiratory distress after head and
neck surgery since progression can be rapid with catastrophic consequences. After
thyroid surgery, there are a number of complications which can cause respiratory
difficulties and an appreciation of the associated signs can help identify them.
Iatrogenic injury to the recurrent laryngeal nerve resulting in vocal cord damage
is a recognised complication following thyroid surgery. Post-operative symptoms
depend on whether both the left and right recurrent laryngeal nerves are involved.
Unilateral injury manifests as a hoarse voice, difficulties phonating and aspiration
on swallowing whereas bilateral injuries present acutely following extubation with
stridor necessitating reintubation and tracheostomy formation. Bilateral vocal
cord paralysis is not the most likely cause in the above scenario, as the stridor only
presents after four days. Furthermore, bilateral vocal cord paralysis does not directly
cause circumoral paraesthesia or confusion.
Answers
Tracheomalacia is believed to occur as a result of longstanding extrinsic tracheal
compression causing a loss of tracheal cartilage rigidity. Removal of this compressive
source (thyroidectomy) may then precipitate life threatening dynamic airway
collapse. It is a very rare complication and does not explain the confusion and
paraesthesia in the above scenario.
Post-operative haemorrhage is a well recognised complication following thyroid
surgery and can result in a rapidly expanding haematoma compromising airway
patency. The haematoma usually presents as a large, tense and immobile swelling
under the wound, which will have to be re-opened at the bedside if there is
impending airway obstruction. The majority of bleeds occur within 24 hours and
presenting symptoms can include stridor, dyspnoea, neck pain, dysphagia and
confusion. Although an important differential to consider, it is not the most likely
diagnosis in the above case due to the normal neck examination and lack of pain.
Symptom occurrence on day four postoperatively and the presence of circumoral
paraesthesia is also not typical.
The blood supply to the upper trachea is primarily from small branches of the
inferior thyroid artery and life threatening tracheal necrosis due to excessive cautery
near the trachea has been described. Tracheal disruption is unlikely to be causing
the symptoms in the case described since there is no subcutaneous emphysema
(formed from the tracheal air leak). Furthermore, stridor, confusion and paraesthesia
are not usually associated with this very rare complication.
Hypocalcaemia is the most common complication following thyroidectomy and
the most likely cause of the clinical picture described. Since the parathyroid glands
are located on the posterior surface of the thyroid gland, these can be damaged
or devascularised following surgery to this area. The fall in calcium levels generally
occurs within 24–48 hours post-operatively and can be sufficient to produce
symptoms. Hypocalcaemia directly increases neuromuscular excitability and
many of the clinical manifestations stem from this underlying problem. The stridor
described in the above case is due to laryngospasm which is an exaggeration of the
normal glottic closure reflex. Circumoral paraesthesia and bronchospasm also arise
as a consequence of neuromuscular irritability.
Malhotra S, Sodhi V. Anaesthesia for thyroid and parathyroid surgery. Contin Educ Anaesth Crit Care Pain
2007; 7(2):55–58.
Findlay J, Sadler G, Bridge H, Mihai R. Post-thyroidectomy tracheomalacia: minimal risk despite significant
tracheal compression. Br J Anaesth 2011; 106(6):903–906.
Chauhan A, Ganguly M, Saidha N, Gulia P. Tracheal necrosis with surgical emphysema following
thyroidectomy. J Postgrad Med 2009; 55(3):193–195.
5. A Rocuronium
This patient’s limited anaesthetic history raises the suspicion of a previous episode of
anaphylaxis. Without prior records available it is prudent to avoid agents most likely
to cause such a reaction.
Anaphylaxis is an immune reaction that is triggered by hypersensitivity to an
antigen, e.g. the β lactam ring found in some antibiotics. It results in IgE antibody
production and a subsequent IgE-antigen mediated cascade of events. This leads to
the widespread release of inflammatory mediators such as histamine, leukotrienes
219
220
Chapter 6
and prostaglandins. The reaction results in an increase in vascular permeability,
bronchial hyper-reactivity and subsequent circulatory compromise that can be fatal
(10% of those reported to the UK Medicines Control Agency).
Similar, and often indistinguishable, reactions may occur that do not involve IgE
release in response to an antigen. They manifest secondary to direct histamine
release or activation of the complement pathway by other means. They are known as
anaphylactoid reactions. An example of which could be initiated by morphine which
acts directly on mast cells to cause histamine release.
The culture of reporting anaphylactic reactions is variable between countries
and thus the frequency of its occurrence (based on information from Australia
and France) ranges from 1 in 10 000 to 1 in 20 000. The 6th National Audit Project
(Perioperative Anaphylaxis) may help determine the incidence of anaphylaxis in the
UK, which is currently unknown.
The following table (Table 6.4) lists the most commonly known triggers for
anaphylaxis and their proposed incidence when associated with anaesthesia.
Table 6.4 Incidence of anaphylaxis with common triggers used in anaesthetic practice
Agent
Incidence
Muscle relaxants
60–70%
Latex
12–20%
Antibiotics
2–15%
Colloids
4%
Induction agents
rare
Opioids
1.7%
Local anaesthetics
rare
Disinfectant and antiseptic agents
Unknown but increasing
As muscle relaxants are reported to be the agents with the highest risk of triggering
anaphylaxis, rocuronium should be avoided in this scenario if at all possible. If the
use of a muscle relaxant is necessary, using a benzyl-isoquinolinium instead of an
aminosteroid may reduce the risk as they are less associated with such a reaction.
To further avoid histamine release, and therefore the possibility of an anaphylactoid
reaction, cisatracurium may be the best option.
The remaining agents can also be associated with anaphylaxis. Further modifications to
the anaesthetic, such as fentanyl instead of histamine-producing morphine or iodine in
place of chlorhexidine and avoidance of all colloids, can be simple enough to make. The
majority of theatres are now run as ‘latex-free’ or can easily be made so these days.
The Association of Anaesthetists of Great Britain and Ireland. Suspected anaphylactic reactions associated
with anaesthesia. Anaesthesia 2009;64:199–211.
Ryder SA, Waldmann C. Anaphylaxis. Contin Educ Anaesth Crit Care Pain 2004; 4(4):111–113.
Answers
6.D History of dizziness on standing, a 5-minute ECG with
no premature ventricular complexes (PVCs), and nasal
congestion
Phaechromocytomas, although rare in clinical practice are more common in
exams. This secreting tumour is named a chromaffinoma, because of its derivation
from chromaffin cells which evolve from the neural crest to make up the normal
sympathetic system. The classical clinical syndrome of severe hypertensive crises
accompanied by headache, sweating, palpitations and anxiety, with resolution
afterwards, is variable and depends mainly on the secretory properties of the
tumour. Most secrete noradrenaline; with some producing both noradrenaline and
adrenaline and a few may also secrete active peptides such as adrenocorticotrophic
hormone (ACTH), calcitonin, vasoactive intestinal peptide (VIP) and somatostatin
also. Tumours are 90% adrenal and 10% extra-adrenal, known as paragangliomas.
The full range of imaging techniques is used for their identification, with functional
PET scanning in some centres. M-iodobenzylguanidine (MIBG) isotope uptake scans
are useful to identify tumour foci and locate extra-adrenal or secondary deposits.
Preoperative assessment and preparation is of paramount importance, and
focuses on assessment for pathology associated with the tumour, namely endorgan damage caused by hypertension, and pharmacological suppression. With
pharmacological suppression the classic target criteria are:
•
•
•
•
•
Blood pressure < 160/90 mmHg
Postural hypotension, but not severe (< 80/45 mmHg)
ECG free from ST/T wave changes for 7 days
No greater than one premature ventricular contraction on ECG every 5 minutes
Nasal congestion
Agents used include the non-specific α-blocker phenoxybenzamine (which due to
α2 blockade also causes tachycardia, and therefore must be given with a β-blocker).
Selective α1 blockers, such as doxazosin can now be used alone. If β-blockade
is required, a stable a block has to be established first to prevent the loss of β2
vasodilatation, and therefore increased hypertension.
Some of the stems in this question look for signs of α blockade. These may include
postural hypotension, and nasal congestion. Lack of cardiac irritability feature in
B and D, and are also reassuring, but the normal ECG reading in B cannot exclude
ectopic beats. The normal chest X-ray and echocardiogram in C are reassuring, but
cannot exclude acute physiological changes seen with this condition. Repeated
blood pressure readings <160/90 mmHg (E) are also reassuring about good blood
pressure control, but the stem with both reassuring symptoms and physiological
investigations is option D.
Pace N, Buttigieg M. Phaeochromocytoma. BJA CEPD Reviews 2003; 3(1):20–23.
7. B Cervical and chest computed tomography
The above case describes Ludwig’s angina which is an aggressive, rapidly spreading
“woody” cellulitis of the submandibular space, commonly arising from an infected
221
222
Chapter 6
molar tooth. There is a lack of lymphadenopathy since the typically polymicrobial
infection spreads along fascial planes as opposed to the lymphatic system. Two
life-threatening complications of Ludwig’s angina are upper airway obstruction and
descending necrotising mediastinitis. Sufferers are at risk of airway obstruction due
to posterior infective extension and tongue distension with posterior displacement.
Descending necrotising mediastinitis describes the spread of infection from neck
to mediastinum via contiguous fascial planes which is promoted by gravity and the
negative intrathoracic pressure. Since the disease is rare and early symptoms often
nebulous, diagnosis and treatment can be delayed with fatal consequences.
Computed tomography is the imaging modality of choice for acute deep-seated
neck infections and the correct answer to the above scenario. Imaging the neck
allows a rapid assessment of the depth of involvement as well as the presence of
abscesses which may be amenable to surgical drainage. Chest imaging provides
confirmation and allows an assessment of the extent of mediastinal involvement
which is important for surgical planning. Since a pericardial rub was heard in the
above scenario, computed tomography will also be useful in assessing for secondary
pericardial involvement and the presence of an effusion.
Magnetic resonance imaging does provide excellent soft tissue resolution and
diffusion weighted imaging can help delineate complex fluid collections. This
imaging modality is particularly useful for infections involving the retropharyngeal
space where extension into the spinal column is suspected. However, it is more
time consuming than computed tomography and patients may feel claustrophobic
during scanning. Patient compatibility also needs to be assessed. In the above
scenario where the airway patency can deteriorate rapidly and an early diagnosis
and treatment plan is needed, computed tomography is more appropriate.
Cervical ultrasound can be useful in characterising soft tissue masses and collections
but is unable to penetrate bone or air filled structures. It is also operator dependent
and not as accurate as computed tomography in assessing the extent of mediastinal
involvement.
Plain radiography is easily accessible but is of little value in planning the
management of descending necrotising fasciitis complicating Ludwig’s angina. A
lateral cervical radiograph can highlight pretracheal gas bubbles and a loss of the
normal lordosis, whereas a chest radiograph may show a widened mediastinum
and an enlarged cardiac silhouette if there is mediastinitis or a pericardial effusion
respectively. Computed tomography however provides a much more accurate
picture of the severity of the infection.
An echocardiogram can provide information regarding the extent of the pericardial
effusion and whether it is affecting cardiac function. Echocardiography is not
the most appropriate investigation to plan management since it provides no
information on the degree of cervical involvement or whether there are any
collections amenable to drainage.
Hurley M, Heran M. Imaging studies for head and neck infections. Infect Dis Clin N Am 2007; 21(2):305–
353.
Wippold F. Head and neck imaging: the role of CT and MRI. J Magn Reson Imaging 2007; 25(3):453–465.
Boscollo-Rizzo P, Da Mosto MC. Submandibular space infection: a potentially lethal infection. Int J Infect
Dis 2009; 13(3):327–333.
Answers
8. E Electroencephalogram
The patient fulfils the prerequisites for brainstem testing because he has suffered
irreversible brain injury and he is in an apnoeic coma. The neurological confirmation
of death consists of cranial nerve II – XI examination and apnoea testing performed
by two doctors at two different times. At the end of each set of cranial nerves
examinations an apnoea test occurs. In a patient with a high cervical spine injury,
apnoea might not be due to a central cause but due to spinal cord injury, therefore
ancillary tests are employed to confirm de the diagnosis. Electroencephalogram
(EEG) is the most widely used and validated assessment in this circumstance.
The second battery of brainstem tests cannot be performed in isolation without the
apnoea testing; therefore an EEG is the next most appropriate step to support the
diagnosis of death by neurological criteria. Somatosensory evoked potentials are
used for monitoring of depth of anaesthesia and play no part in the diagnosis of
death.
Oram J, Murphy P. Diagnosis of death. Contin Educ Anaesth Crit Care Pain 2011; 11(3):77–81.
9.E Proceed with the case under general anaesthesia and a
ultrasound-guided fascia iliaca block with invasive blood
pressure monitoring
The management of patients presenting for operative fixation of proximal femoral
fractures is clinically and politically of huge importance, the examiners recognise
this. Therefore it is essential to be familiar with at least one of the national or
international consensus guidelines on the issue. The key elements of these
guidelines are as follows:
Timing of surgery and delays
The Department of Health (UK) guidance recommends surgery within 36 hours
of admission, and evidence clearly shows adverse outcomes in terms of mortality,
complications and stay length if fixation is delayed past 48 hours. Nevertheless,
this cannot override the obvious sensibility of stabilisation and resuscitation of
an unstable patient. The AAGBI lists several situations in which an operative delay
may be acceptable to allow for interim treatment. This list includes reversible
coagulopathic states, severe glucose or electrolyte disorders, uncontrolled
arrhythmias with heart rates above 120 beats per minute, overt heart failure, and
chest sepsis.
Echocardiography
The presence of a murmur may indicate serious valvular heart disease, and indeed
aortic stenosis (AS) is more common in hip fracture patients occurring in 20-40%, ten
times the rate of the general elderly population. That said, some studies demonstrate
similar early postoperative mortality in patients with AS and those without. One
could argue also that an echo demonstrating AS will not change management, in
that surgery is still required and that therefore the best way to proceed in these
223
224
Chapter 6
patients is to treat as if moderate AS were present. Guidelines do support a request
for an echo if no recent study is available, but not at the cost of timely surgery.
Anaemia and transfusion
Anaemia is common in this group, affecting about 40% of patients, and a fall
in haemoglobin around the time of surgery is inevitable. As with many other
patient groups the trigger for transfusion should be tailored to the individual
patient taking account of specific cardiorespiratory and neurological risk factors.
The large hip fracture transfusion (FOCUS) study seems to show little difference
in mortality of a trigger of 80 vs 100 g/L. However, given that the haemoglobin
concentration is likely to fall, the AAGBI recommend the routine point-of-care
testing in recovery as a means to avoid missing dangerously anaemic patients
postoperatively.
This is a perennial clinical conundrum facing any anaesthetist covering the
trauma list. The first issue relates to lack of echo, which is listed by the AAGBI
as an ‘unacceptable reason to delay hip fracture surgery’. One has to assume a
moderate degree of AS, and proceed accordingly with invasive blood pressure
monitoring and adequate provision to treat sudden changes promptly. The next
problem relates to the dual antiplatelet therapy, of which details are sparse. Here
the assumption has to be that the patient has a drug-eluting stent and as such
the main risk is of antiplatelet reversal or cessation is in-stent thrombosis leading
to major cardiac adversity, as opposed to bleeding. Thus central neuraxial blocks
are contraindicated, whereas the use of peripheral nerve blocks is more judged
on risk versus benefit for every case. In this case, the proposed fascia iliaca block is
one with a relatively low risk of bleeding, as with ultrasound it can be reliably sited
without immediate needle proximity to the femoral artery. Therefore, the most
appropriate course of action in this patient would be to proceed with the operation
under general anaesthesia and a ultrasound-guided fascia iliaca block with invasive
blood pressure monitoring.
Maxwell L, White S. Anaesthetic management of patients with hip fractures: an update. Contin Educ
Anaesth Crit Care Pain 2013; 13(5):179–83.
Association of Anaesthetists of Great Britain and Ireland. Management of proximal femoral fractures.
Anaesthesia 2012;67:85–98.
Scottish Intercollegiate Guidelines Network. Management of Hip Fracture in Older People. CG 111.
Edinburgh: Scottish Intercollegiate Guidelines Network, 2009.
10. A Short-axis view with in-plane needle approach
The use of ultrasound (US) in regional anaesthesia has significantly increased in the
recent years. Choosing the correct US view and needle orientation is essential for
successful and safe nerve block. When scanning nerves the structures viewed by US
beam will either be in a short-axis view or long-axis view.
In the short-axis view, the nerves and the blood vessels are visualised in section
(sliced across their diameter), nerves are easier to find, and the US image is relatively
stable making this view ideal for introducing a needle.
Answers
In the long-axis view, however, the nerves and blood vessels are visualised
longitudinally along their length (demonstrating a tube like structure) making the
US image produced unstable and not ideal for needle insertion.
When introducing the needle, it can be passed either along the long-axis of the US
beam (in-plane) or across the short-axis of the beam (out-of-plane). With an in-plane
approach, the needle is visualised entirely throughout the block and produces good
views of needle-nerve proximity. Therefore this is the safest approach.
With an out-of-plane technique, the needle crosses the US beam as a bright dot
and the accurate location of the needle tip is uncertain and it could be advanced
in unwanted tissue, making this approach less safe for needle insertion. However,
anaesthetists the out-of-plane approach is ideal when inserting catheters as it allows
parallel advancement of the catheter along the long-axis of the nerve as it exits the
tip of the needle (Figure 6.1).
Figure 6.1 Orientations for
ultrasound-guided nerve block.
A. Long-axis out-of-plane. B.
Long-axis in-plane C. Shortaxis out-of-plane. D. Short-axis
in-plane.
a
c
b
d
In this example, the combination of short-axis view and in-plane needle visualisation
is the safest approach for the above reasons.
Carty S, Nicholls B. Ultrasound-guided regional anaesthesia. Contin Educ Anaesth Crit Care Pain 2007;
7(1):20-24.
Snaith R, Dolan J. Ultrasound-guided peripheral upper limb nerve blocks for day-case surgery. Contin
Educ Anaesth Crit Care Pain 2011; 11(5):172-176.
11. E Elective intubation of the patient
Inhalational injury is the aspiration of heated gases, hot liquids, steam, or noxious
substances of incomplete combustion. It can be categorised as:
• Upper airway thermal injury – supraglottic burns causing stridor, a change in
voice quality or uvular oedema
• Lower airway thermal injury – infraglottic burns most commonly by noxious byproducts of incomplete combustion leading to dyspnoea, wheeze and secretions
• Noxious gases injury – including inhalation of carbon monoxide and cyanide
225
226
Chapter 6
This patient has a high risk of inhalation injury due to an enclosed space fire with
significant burns to the face. The onset of airway oedema is often unpredictable, but
fluid resuscitation is likely to worsen any impending oedema, while the relatively
long duration of transfer indicates the need to have a secure airway during transfer.
Therefore it is appropriate to plan elective intubation of the patient in controlled
circumstances with senior support, a difficult airway trolley and skilled assistance.
Adding a competent team member to the transfer is reassuring and can help
should complications arise during transfer, but it is often impractical. All transfers
should have full monitoring, including ECG, pulse oximetry and non-invasive blood
pressures, but invasive blood pressure monitoring is only indicated if you anticipate
cardiovascular instability or it is required to guide ongoing therapy. Availability of
difficult airway equipment is necessary once elective intubation has been decided,
and devices such as video laryngoscopes are useful to have when a patient is being
transferred. However, the most appropriate approach would be to ensure a secure
airway prior to transfer.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12 (3):118–122.
12. A Change the patient to continuous positive airway
pressure (CPAP) and assess ventilation and cardiovascular
parameters for 30 minutes
The majority of patients who receive mechanical ventilation have acute respiratory
failure in the postoperative period, pneumonia, congestive heart failure, sepsis,
trauma or acute respiratory distress syndrome (ARDS). Respiratory muscle
weakness may not be a contributing factor to their respiratory failure and once
the acute pathophysiological problem is resolved, invasive ventilation may be
downgraded and patients extubated. The duration of mechanical ventilation is
often unnecessarily prolonged in the setting of a short period of ventilator support
(less than 7 days) with the weaning process accounting for up to 50% of the total
ventilation time. A delay of 48 hours in extubation results in an increased risk of
extubation failure, ventilator acquired pneumonia, thromboembolic disease, longer
intensive care and hospital stay and increased mortality.
Weaning involves progression from a controlled mode of ventilation to a support
mode and then reduction of support delivered until a trial of readiness for
extubation. This trial is termed a spontaneous breathing trial (SBT).
Typical readiness criteria for attempted weaning include:
• Improvement in the underlying condition that caused the respiratory failure
• Pulmonary: fractional inspired oxygen Ratio (PFR) of more than 200 with a
positive end-expiratory pressure (PEEP) of 5 cmH2O
• Haemodynamic stability
• No electrolyte, metabolic, haematological or nutritional deficits
• Neurologically appropriate with cough and gag reflexes present
Once deemed suitable, a SBT may be initiated with minimal pressure support such
as 5 cmH2O, CPAP or a T-piece or tracheostomy mask (no PEEP). A SBT should be
Answers
attempted for a minimum of 30 minutes but should be terminated and deemed
unsuccessful if:
•
•
•
•
•
The respiratory rate remains above 35 breathes per minute for 5 minutes
Oxygen saturations of less than 90%
Heart rate increases to over 140 beats per minute
Systolic blood pressure > 180 mmHg or < 90 mmHg
Panic or diaphoresis
The following classification of the results of the spontaneous breathing trial may be
applied:
• Simple: successful first trial followed by extubation
• Difficult: up to three spontaneous trials but discontinuation of ventilation within
7 days
• Prolonged: more than three unsuccessful trials or more than 7 days of mechanical
ventilation
10–20% of ventilated patients may have prolonged weaning and in-hospital
mortality is increased in this group. In patients who fail a SBT, the strategy is to
reduce the support the patient is receiving and try again. A period of rest between
SBTs is advocated of 24–48 hours. Gradual reductions in the pressure support
by 2–4 cmH2O per 24 hours or a short SBT period every hour with increasing the
duration are both advocated.
Even assessing in a careful manner such as described above, 10–15% of extubations
fail, necessitating re-intubation. If this occurs the mortality rate in this group is
increased.
In the patient above, the criteria for initiating a SBT is met and if successful, a trial of
extubation is warranted. In this patient with COPD, a greater-than-average sputum
production and poorer gas-exchange may have been present prior to the acute
infection and must be accepted in order to avoid the complications of on-going
mechanical ventilation.
McConville JF, Kress JP. Weaning patients from the ventilator. N Engl J Med 2012;367:2233–2239.
13. D 20 mmol of calcium chloride + 1 pool of platelets +
15 mL/kg fresh frozen plasma (FFP)
In order to form effective blood clots a patient needs an adequate number of
functioning platelets, adequate levels of all the clotting factors, an adequate
haematocrit, an adequate level of ionised calcium, a relatively normal pH and an
absence of significant hypothermia. The critical levels of these variables cannot be
defined and are mutually dependent. The clinical scenario described suggests that
there is ongoing bleeding due to a coagulopathy rather than a failure of surgical
haemostasis. The temperature, pH, haematocrit and platelet count are acceptable.
However, the patient has been receiving long term antiplatelet therapy and has
been on cardiopulmonary bypass, thus, in the absence of a platelet function test
it is reasonable to deduce that platelet transfusion is warranted to correct the
coagulopathy. The clotting tests suggest there is a consumptive and /or dilutional
227
228
Chapter 6
component to this coagulopathy. Given the degree of abnormality, a dose of FFP
should elevate the levels of all factors, including fibrinogen, without the need to give
additional cryoprecipitate. Administration of FFP and platelets is likely to result in
a further drop in ionised calcium, it would be prudent to administer a replacement
dose. Given the scenario and timings, a further dose of protamine is likely to result
in an anti-coagulant effect. In the absence of evidence for hyperfibrinolysis, a
second dose of tranexamic acid is not indicated at this stage. The threshold for
pRBC transfusion in this context is <70g/L. A thromboelastogram would refine the
diagnosis further and repetition after intervention guide further therapy. This is a
common practice in many centres but not universal.
Dyke C, Aronson S, Dietrich W, et al. Universal definition of perioperative bleeding in adult cardiac surgery.
J Thorac Cardiovasc Surg 2014; 147(5):1458–63.
Gorlinger K, Shore-Lesserson L, Dirkmann D, Hanke AA, Rahe-Meyer N, Tanaka KA. Management of
hemorrhage in cardiothoracic surgery. J Cardiothorac Vasc Anesth 2013; 27(Suppl 4):S20–34.
Davidson S. State of the art - How I manage coagulopathy in cardiac surgery patients. Br J Haematol 2014;
146(6):779–89.
14. B Prone positioning
The worsening hypoxaemia, new bilateral radiology infiltrates and low Pao2:Fio2 (P:F
ratio) within one week of the onset of severe pneumonia suggests acute respiratory
distress syndrome (ARDS).
ARDS is an acute, diffuse inflammatory lung syndrome that results in respiratory
failure. The 1994 American-European Consensus Conference definition of ARDS has
now been superseded by the 2012 Berlin Definition (Table 6.5).
Table 6.5 The 2012 Berlin Definition of ARDS
Severe ARDS
Moderate ARDS
Mild ARDS
Timing
Within one week of known clinical insult or new or worsening respiratory symptoms
Chest Imaging
Bilateral opacities not explained by effusions, lobar/lung collapse or nodules
Paco2 (kPa):Fio2
Paco2 (mmHg):Fio2
< 13.3
< 100
13.3-26.7
100-200
26.7-40
200-300
PEEP (cmH2O)
≥5
≥5
≥5
Mortality (%)
45
32
27
The cause of ARDS in this patient is severe pneumonia, which is a direct (or
pulmonary) cause. Other direct causes of ARDS include aspiration, lung contusions
and inhalational injury. Indirect (non-pulmonary) causes include sepsis, trauma,
pancreatitis and burns.
The pathophysiology of ARDS is complex and involves the interplay of various body
systems. A simplified view of this pathogenesis is presented here but this is an area
of ongoing exploration.
Answers
1. Exudative phase: Alveolar capillary membrane disruption resulting in leakage
of protein rich fluid. Inflammatory cells (e.g. neutrophils) infiltration forming
exudate.
2. Proliferative phase: Proliferation of abnormal type II alveolar cells and
inflammatory cells. There is a resultant dysfunction in surfactant with decreased
pulmonary compliance.
3. Fibrotic phase: Infiltration with fibroblasts replacing alveolar cells and ducts
resulting in marked reduction in pulmonary compliance.
4. Restorative phase: Slow and incomplete repair of pulmonary architecture.
The management of ARDS can be subdivided as below:
General (‘FLATHUGS’)
•
•
•
•
•
Feeding – early nutrition
Lines – as per catheter-related blood stream infection bundle
Analagesia – adequate to maintain patient comfort, avoid under or oversedation
Thromboprophylaxis – consider non-pharmacological and pharmacological
Hydration – FACCT trial (2006) did not show a difference in fluid therapy guided
by pulmonary artery flotation catheter versus central venous catheter
• Ulcer prophylaxis – according to local protocol and review daily
• Glycaemic control – no definitive evidence for tight glycemic control, aim for
glucose < 10 mmol/L
• Sedation/Spontaneous breathing trial – consider daily sedation holds and
breathing trials
Mechanical ventilation (based on ARDSnet mechanical ventilation protocol
summary)
• Tidal volume 6 mL/kg : ARMA study (2000) investigated 12 mL/kg versus 6 mL/kg
in acute lung injury, lower tidal volumes resulted in improved outcomes
• Plateau pressures (Pplateau)< 30 cmH20
• Permissive hypercapnia, aim for pH > 7.3
• PEEP; ALVEOLI trial (2004) demonstrated an absence of data proving superiority of
lower or higher PEEP for survival
‘Rescue’ therapies for refractory hypoxaemia
Prone positioning
Prone positioning is based on the theory of recruiting areas of lung that are
non-dependent in the supine position, leading to reduced ventilation-perfusion
mismatching. There are additional benefits of improved secretion clearance
and increased homogeneity of ventilation due to decreased lung deformation
by mediastinal structures. There are potential adverse effects such as line or
endotracheal tube displacement, reduced preload and functional restriction in
cardiac contraction, pancreatitis, raised intracranial pressure and pressure related
nerve damage. The process itself needs to be meticulously performed with adequate
numbers of staff.
PROSEVA (2013) was a landmark prospective, multicenter randomised control
trial investigating early prone positioning in moderate to severe ARDS. It suggests
229
230
Chapter 6
benefit in terms of oxygenation and mortality. Previous studies appeared to show
improved oxygenation, but no clear mortality benefit.
Inhaled nitric oxide
Nitric oxide (NO) is known to cause pulmonary vasodilatation and hence improve
pulmonary blood flow. The inhaled route delivers NO selectively to ventilated lung
units and hence improves oxygenation. Although inhaled nitric oxide improves
oxygenation, there does not appear to be a mortality benefit.
Extracoporeal membrane oxygenation (ECMO)
ECMO involves insertion of large cannulae into central vessels. It is similar to a simple
cardiopulmonary bypass circuit. Blood leaves a central vessel and is pumped around
a circuit through a membrane oxygenator to allow gas exchange, then returned
to the patient via a central vessel. As oxygenation is predominantly achieved
through the extracorporeal circuit, ultra low tidal volumes can be used to ventilate
the patient minimising ventilator associated lung injury. ECMO requires systemic
anticoagulation, carrying a risk of bleeding.
The CESAR trial (2009) was a multicentre randomised control trial investigating
conventional management or referral to consideration for treatment by ECMO
in severe potentially reversible respiratory failure. It concluded that referral to a
tertiary respiratory centre for consideration of ECMO resulted in improved survival.
It is unclear what proportion of this benefit is attributed to optimum conventional
ventilation in a tertiary referral centre.
High frequency oscillation ventilation (HFOV)
HFOV works on the principle of high frequency (120–600 breaths/min) oscillation
around a continuous high distending airway pressure. This results in lower tidal
volumes, approximating at 3 mL/kg. The OSCAR (2013) and OSCILLATE (2013) trials
were two multicentre randomised control trials investigating the role of HFOV in
ARDS. The failed to show a benefit and possibly showed harm with HFOV compared
to conventional ventilation. At present, HFOV cannot be recommended in refractory
hypoxemia secondary to ARDS in adults.
Of the options given in this question, based on current evidence the options for
refractory hypoxaemia in ARDS appear to be prone positioning and ECMO. Given
that ECMO remains controversial and requires a specialist centre, prone positioning
would be the most appropriate option in this patient. If an option was given for
‘referral to a tertiary respiratory centre’, that would also be appropriate.
Pharmacological
No proven mortality benefit but many have been trialed including surfactant
replacement therapy, glucocorticoids, and β-adrenoceptor agonists.
Ranieri VM, Rubenfeld GD, Thompson BT, et al. ARDS Definition Task Force: Acute respiratory distress
syndrome: the Berlin Definition. JAMA. 2012 ;307(23):2526–2533.
National Heart, Lung and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials
Network. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006;
354:2564–2575.
Answers
The Acute Respiratory Distress Syndrome Network. Ventilation with low volumes as compared with
traditional tidal volumes for acute lung injury and acute respiratory distress syndrome. N Engl J Med
2000;342:1301–1308.
Brower RG, Lanken PN, MacIntyre N, et al. National Heart, Lung, and Blood Institute ARDS Clinical Trials
Network. Higher versus lower positive end-expiration pressures in patients with the acute respiratory
distress syndrome. N Engl J Med 2004;351(4):327–336.
Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N
Engl J Med 2013;368(23):2159–2168.
Taylor RW, Zimmerman JL, Dellinger RP, et al. Low-dose inhaled nitric oxide in patients with acute lung
injury: a randomized controlled trial. JAMA 2004; 291(13):1603–1609.
Peek J, Mugford M, Tiruvoipati R, et al. The CESAR trial collaboration: Efficacy and economic assessment
of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult
respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 2009; 374:1351–1363.
Young D, Lamb SE, Shah S, et al. The OSCAR Study Group. High-frequency oscillation for acute respiratory
distress syndrome. N Engl J Med 2013; 368(9):806–813.
Ferguson ND, Cook DJ, Guyatt GH, et al. The OSCILLATE Trial Investigators; Canadian Critical Care
Trials Group. High-frequency oscillation in early acute respiratory distress syndrome. N Engl J Med
2013;368(9):795–805.
15. E 3780 mL
This patient has sustained a significant thermal injury with evidence of inhalational
injury. Significant burns cause a profound systemic inflammatory response
syndrome and early aggressive management is paramount. Mortality from major
burns is in the order of 10–20% with multiorgan failure and sepsis being leading
causes.
Management should follow ALTS guidelines, especially where the mechanism is
unknown. During the primary survey, early intubation is advised where airway
compromise or significant inhalational injury is suspected. A rapid sequence
induction is advised and intubation performed with an uncut cuffed endotracheal
tube; ideally size 8 or larger to aid assessment of the airway via bronchoscopy.
Suxamethonium is considered safe in the first 24 hours following injury, an
exaggerated hyperkalaemic response may occur after this time frame.
As part of the ‘Breathing’ assessment, carbon monoxide poisoning should be
excluded. In this case the confusion at presentation may be an early sign and an
arterial blood gas should be done urgently. Normal carbon monoxide levels can be
up to 10% in smokers and a level greater than 20% raises the suspicion of significant
inhalation injury and carbon monoxide poisoning. It is important to note that pulse
oximetry overestimates Spo2 in the presence of carbon monoxide. Therefore the
saturations of 100% in this case should be corroborated with arterial gas analysis via
co-oximetry. High-flow oxygen decreases the half-life of carbon monoxide from 4 to
1 hours, and should be administered empirically until carboxyhaemoglobin (HbCO)
levels are attained.
Another point of concern in this patient as part of the ‘Breathing’ assessment
is the anterior torso burn. The chest wall should be examined for evidence of
circumferential burn which may require early escharotomies. There is evidence to
support that, where possible, these should be done in specialist burns centres.
231
232
Chapter 6
The focus of this question is on the assessment of circulation. As the burns surface
area affects the management of fluid resuscitation, this must be calculated at this
stage. The body surface area (BSA) takes into account partial and full thickness burns
and can be calculated using the ‘rule of 9s’. In this patient the burn to the anterior
torso represents 18% BSA and bilateral palmar surfaces of upper limbs represent a
further 9% (i.e. 2 x 4.5%); the total BSA is 27% (Figure 6.2).
Figure 6.2 Estimating the total
BSA affected by burns using the
'rule of 9s.'
9%
Front 18%
Back 18%
18%
9%
9%
Front 18%
Back 18%
1%
9%
9%
18%
18%
1%
13.5% 13.5%
Adult
Child
The Parkland formula is widely used in the UK for calculation of fluid resuscitation
with warmed crystalloid. It calculates the fluid requirement for the first 24 hours,
from the time of injury, not the time of first presentation.
Parkland formula for fluid requirement = 4 mL/kg/% BSA
Fluid requirement in this patient = 4 mL x 70 kg x 27% = 7560 mL
According to the Parkland formula, half of this volume should be given in the
first 8 hours making 3780 mL correct. The Parkland formula is an estimation and
fluid therapy should be guided by clinical and physiological parameters; there are
detrimental consequences of both under and over resuscitation with fluids.
Management of the burn itself with early decontamination and ensuring
normothermia are important early considerations. Antibiotic use should be reserved
Answers
to where there is a strong clinical suspicion of active infection, there appears to
be little evidence for prophylactic antibiotics. There are burns specific criteria for
diagnosing sepsis which can guide clinical decision making.
This patient represents a BSA greater than 10%, with burns to hands and a possible
inhalational injury mandating discussion and transfer to a regional burns centre. The
British Burns Association criteria for referral to a burns centre are shown in Table 6.6
below.
Table 6.6 British Burns Association ciritera for referral to a regional burns centre
Criteria
Age (years)
≤ 5 or ≥ 60
Site
Face, hands, feet, perineum, circumferential
BSA (%)
≥ 10% in adults, ≥ 5% in children
Injury
Inhalational, chemical, electrical or complex trauma
Comorbidities
Significant cardiorespiratory disease, diabetes mellitus,
immunocompromised, liver disease
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–122.
16. E Modified rapid sequence with ketamine 2 mg/kg,
fentanyl 1–3 µg/kg and rocuronum 1 mg/kg
Anaesthesia service representation in the trauma team may come from the
anaesthetic department or intensive care unit (ICU). The answer to this question is
often the technique in which the clinician has the most experience with because
a stressful situation is not the ideal time to be trying out novel methods; however,
consideration of the different options is still important.
Your responsibility is to secure the airway while your colleagues simultaneously
manage some of the other issues. Your choice of induction technique is vital with
some of the popular options listed above. The considerations include:
• Speed of induction:
–– The patient has been obtunded for some time and therefore performing
an induction designed to progress from unconsciousness to endotracheal
intubation in as rapid a time as possible is less vital. The classic rapid sequence
induction of thiopentone and suxamethonium causes vasodilation, reflex
tachycardia, decreased myocardial contractility and suxamethonium causes a
transient rise in intracranial pressure.
• Cardiovascular stability is the most important aspect of this situation. Therefore the
use of anaesthetic agents known to cause vasodilatation and decreased myocardial
contractility should be avoided, at least in standard doses. The options include:
233
234
Chapter 6
–– Propofol and thiopentone may cause cardiovascular instability due to
vasodilation and decreased contractility. The use of vasoconstrictor medication
may be required, which may result in rebound hypertension and could worsen
active bleeding.
–– Midazolam may also cause hypotension, but less marked than propofol and
thiopentone and may therefore be an appropriate choice.
–– Fentanyl is a potent analgesic, which does not release histamine and therefore
maintains cardiac stability. It is hypnotic-sparing and may reduce the
cardiovascular side-effect profile of induction agents. In addition it obtunds the
cardiovascular reflex to laryngoscopy, which is beneficial to prevent an increase
in blood pressure and intracranial pressure.
–– Rocuronium is a steroid non-depolarising paralytic agent. Administration does
not cause the release of histamine and therefore maintains cardiovascular
stability. In addition when used in larger doses of 0.9–1.2 mg/kg, the onset of
intubating conditions is rapid, occurring between 60 and 90 seconds.
–– Ketamine is a non-competitive N-methyl-D-aspartate (NMDA) receptor
antagonist at the glutamate pre-synaptic calcium channel and is used to
provide ‘dissociative anaesthesia’. It has become the drug of choice in the prehospital setting in combination with fentanyl due to its cardiovascular effect
profile. It causes an increase in systemic vascular resistance and maintains
blood pressure via this mechanism. It should be noted that as a calcium
antagonist it decreases myocardial contractility and therefore may result in a
drop in blood pressure in extreme hypovolaemia. Ketamine has a prolonged
length of action of 30–40 minutes negating the need for an infusion. When
used in conjunction with controlled mechanical ventilation it does not increase
intracranial pressure as described in the 1970s, and may in-fact offer neuroprotection preventing cellular apoptosis.
Pre-hospital care consensus has advocated the use of fentanyl 3 µg/kg, ketamine
2 mg/kg and rocuronium 1 mg/kg (remembered as 3/2/1). This is considered the
safest induction technique at the scene of the accident for the reasons described
above. Whether or not we can translate this technique directly to hospital care is not
certain, but securing the airway in a poly-trauma patient in hospital has the same
priorities as at the scene of the accident. Therefore the most appropriate anaesthesia
induction technique is one that has been tried and tested on this group of patients.
Sengupta S. Trauma anaesthesia and critical care: the post trauma network era. Contin Educ Anaesth Crit
Care Pain 2014;14 (1): 32–37.
17. A High flow oxygen, blood cultures, intravenous fluids
and urgent discussion with microbiology consultant
With a temperature > 38.3°C, a heart rate > 90 beats per minute and tachypnoea,
this lady meets the diagnostic criteria for sepsis based on the general variables as
outlined by the Surviving Sepsis Campaign. She is also at risk of developing severe
sepsis, as her blood pressure and oxygen saturations are low. The site of infection
must be investigated, as she may have developed intra-abdominal sepsis post
surgery, amongst other possibilities.
Answers
Genital tract sepsis was the commonest direct cause of maternal death in the last
triennium, as outlined by the most recent Centre for Maternal and Child Enquiries
(CMACE) report (2006–2008), with Group A streptococcal disease being the
responsible pathogen in many cases. Recommendations were made that high dose
intravenous broad spectrum antibiotics should be administered within 1 hour of
recognition of sepsis as mortality increases with each hour of delay.
In this case, the patient has been on antibiotics via an inadequate route. She has
become more unwell, and blood cultures should be taken and an urgent discussion
with the consultant microbiologist made to determine the most appropriate
antibiotics given her recent antibiotic therapy. This treatment should ideally be
commenced within 1 hour. She is likely to need an escalation in treatment and
admission to a critical care area may be warranted. Fluid challenges should be given
and there should be a low threshold for bladder catheterisation to ensure a urine
output of at least 0.5 mL/kg/hour. Oral antibiotic treatment is not appropriate and IV
paracetamol will not treat the sepsis. Option B is incorrect, as her management must
include the taking of blood cultures.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: International Guidelines for
Management of Severe Sepsis and Septic Shock: 2012. Crit Care Med 2013; 41(2):580–637.
Lewis G. Centre for Maternal and Child Enquiries (CMACE): Saving mother’s lives: reviewing maternal
deaths to make motherhood safer: 2006-2008. BJOG 2011; 118(suppl 1):1–203.
18. C Reschedule the surgery for when the patient is 6 weeks
from the most recent viral respiratory illness
Asthma is one of the most common pulmonary disorders encountered by
paediatric anaesthetists. Asthma patients carry a small but significantly increased
risk for perioperative complications. Paediatric asthmatic patients require careful
preoperative evaluation and preparation.
Essential points to review in the preoperative evaluation are the level of asthma
control and the current medication regimen. In addition, review of the level of
activity, use of rescue medications, hospital visits (tracheal intubation or intravenous
infusions required), allergies, and previous anaesthetic history are important. A Also
an inquiry regarding cough and sputum production should also occur. Although
otherwise healthy children can often be anaesthetised safely during an acute
upper respiratory infection, the risk of bronchospasm in asthmatics is very high.
They should ideally be postponed 4–6 weeks after such an event, particularly if the
surgery is non-urgent, as is the case with the patient in this question.
Preoperative preparation for a controlled asthmatic can include administration of
inhaled β2 adrenergic agonist 1–2 hours before surgery. For moderately controlled
asthma, additional optimisation with an inhaled corticosteroid and regular use
of inhaled β2 agonists 1 week before surgery can be instituted. Poorly controlled
asthmatics might need addition of systemic corticosteroid 3–5 days before surgery.
Lauer R, Vadi M, Mason L. Anaesthetic management of the child with co-existing pulmonary disease. Br J
Anaesth 2012; 109(suppl 1):i47–i59.
Bhatia N, Barber N. Dilemmas in the preoperative assessment of children. Contin Educ Anaesth Crit Care
Pain 2011; 11:214–218.
235
236
Chapter 6
19. E Reschedule for another day with a plan for midazolam
pre-medication on the ward
Anaesthetists frequently have to cope with a child who is uncooperative at induction
of anaesthesia and must be familiar with strategies for preventing and dealing with
this problem.
Psychological and pharmacological interventions aimed at reducing preoperative
anxiety can improve compliance at induction and reduce postoperative behavioural
changes. Psychological interventions include preoperative ward visit, play therapy,
parental presence at induction, music, lighting and distraction. Various drugs can
be used as premedication for the uncooperative child, midazolam being the most
common. The preferred route of administration is oral, followed by nasal. The rectal
and intramuscular route should be avoided if possible.
Uncooperative children are often preschool or young children with an anxious
temperament, anxious parents, or both. These patients may appear cooperative
when interviewed in the surgical ward, but then become uncooperative in the
anaesthetic room or at induction of anaesthesia. Fortunately, they are usually
amenable to reasoning and encouragement possibly backed up by sedative
premedication. The use of physical restraint (overpowering), holding still
(immobilising), and containing (preventing escape or self-harm) in children raises
ethical, legal, and practical problems, and should only be used as a last resort.
If the surgery is elective, as in the case above, then the option of postponing the
procedure should be considered. Postponing the procedure gives more time for
planning, but may not be convenient for the parents. Giving premedication in a day
surgery environment may not be appropriate, so rescheduling the operation for
another day, as inpatient, is the best plan of action in this case.
Tan L, Meakin GH. Anaesthesia for the uncooperative child. Contin Educ Anaesth Crit Care Pain 2010;
10:48–52.
20. C Proceed with anaesthesia and surgery, but with
modified anaesthesia technique to avoid known triggers
for malignant hyperthermia
Malignant hyperthermia (MH) is an inherited disorder of skeletal muscle that can
be pharmacologically triggered to produce a potentially fatal combination of
hypermetabolism, muscle rigidity and muscle breakdown. Malignant hyperthermia
susceptibility (MHS) is inherited in an autosomal dominant fashion. However, a
parent with MHS may not necessarily have a positive history of MH. Anaesthetic
technique must be modified to avoid known triggers for MH (halothane, enflurane,
isoflurane, sevoflurane, desflurane, and succinylcholine) in any cases of suspected
or confirmed MHS. The anaesthetic machine should be prepared by removal of
vapourisers and flushing through the machine and ventilator with 100% oxygen at
maximal flows for 20–30 minutes, and a new breathing circuit should be used.
The key to successful management of MH is its early diagnosis and the rapid
instigation of several modes of treatment simultaneously. Administration of volatile
anaesthetics should be discontinued and the patient’s lungs hyperventilated
Answers
using 100% oxygen with fresh gas flows and type of breathing circuit optimised to
eliminate the anaesthetic from the body. Anaesthesia should be maintained with
intravenous drugs while surgery is concluded as rapidly as possible. Active cooling
measures should be commenced. At the onset of treatment, one member of staff
must be assigned to the preparation of dantrolene sodium for infusion. Repeated
doses of dantrolene (1 mg/kg up to maximum of 20 mg) should be administered
intravenously as soon as possible until the tachycardia, rise in CO2 production and
pyrexia start to subside. Up to 10 mg/kg may be required.
Postponing surgery for further information and investigation is not an option in this
case due to the urgency of the surgery. Proceeding with an 'MH-safe' anaesthetic is
the most appropriate approach in this clinical scenario.
Halsall PJ, Hopkins PM. Malignant hyperthermia. Contin Educ Anaesth Crit Care Pain 2003;3:5–9.
21. D Serotonin syndrome
Serotonin syndrome is a potentially lethal condition resulting from excess agonist
activity at central and peripheral serotonergic receptors. It can result from therapeutic
drug use, intentional self-poisoning or interactions between drugs, many of which
anaesthetists are involved with. The syndrome is characterised by neuromuscular
excitability, autonomic hyperactivity, and altered mental status. It is a clinical
diagnosis and the presence of tremor, clonus, or akathisia without extrapyramidal
signs should lead clinicians to consider the syndrome, particularly if the patient is
taking drugs known to elevate serotonin levels. Tramadol is a commonly prescribed
analgesic and works by activation of central μ-opioid receptors. In addition to its
opioid receptor effects, tramadol also inhibits neuronal reuptake of serotonin and
noradrenaline. This property of tramadol can lead to elevated plasma serotonin
levels which increases the risk of developing the serotonin syndrome. When
tramadol is taken in conjunction with serotonergic agents like SSRIs (such as in
the case above), this risk increases. Treatment is generally supportive and involves
removing the offending agent(s) and controlling the agitation, autonomic instability
and hyperthermia. The antihistamine cyproheptadine, which is also a serotonin
antagonist, is reserved for severe cases. Serotonin syndrome is the most likely
diagnosis in the case above since there are clinical signs of neuromuscular excitability,
autonomic hyperactivity and altered mental status in a patient known to be taking
two agents which can increase serotonin levels.
Opioid toxicity can occur with tramadol administration, although symptoms such
as drowsiness and lethargy would be more likely than the restlessness described.
Furthermore, miosis as opposed to mydriasis would be expected on examination
of the pupils. Hyperreflexia, tremor and pyrexia are also not typical presentations of
opioid toxicity.
Opioid withdrawal shares many of the symptoms and signs seen in the serotonin
syndrome such as restlessness, tremor, mydriasis and tachycardia. The temporal
relationship between tramadol use and the symptoms in the above scenario
however makes opioid withdrawal unlikely. Withdrawal symptoms usually occur
following cessation of opioids after several weeks of steady use in which physical
dependence is attained. In the above scenario tramadol was only taken for 1 day,
and there was no history of its cessation.
237
238
Chapter 6
The symptoms associated with hyponatraemia are predominantly neurological
due to cerebral oedema associated with a reduced serum osmolality. The muscle
hyperactivity and confusion as seen in the above case are typical symptoms of
hyponatraemia which can progress to seizures, coma and respiratory arrest if
the hyponatraemia is not corrected. Tramadol can cause hyponatraemia on rare
occasions, thought to be due to opioid and serotonin receptor induced ADH release.
The fever described in the above case however is not typical of hyponatraemia, but
is frequently seen in the serotonin syndrome due to autonomic hyperactivity.
Anaphylaxis should always be in the differential diagnosis for any patient who
becomes unwell after starting a new medication. In the above case however, the
tremor and hyperreflexia suggest an alternative diagnosis.
Boyer E, Shannon M. The serotonin syndrome. NEJM 2005; 352(11):1112–20.
Frank C. Recognition and treatment of serotonin syndrome. Can Fam Physician. 2008; 54(7):988–92.
Lota A, Dubrey S, Wills P. Profound hyponatremia following a tramadol overdose. QJM 2012; 105(4): 397–8.
22. A Diabetes
Chronic post-surgical pain (CPSP) is recognised as:
•
•
•
•
Pain developing after a surgical procedure
Pain of at least 2 months duration
Other causes of pain excluded (such as infection)
Pain continuing from a pre-existing pain problem excluded
Risk factors for development of CPSP can be patient factors or surgical factors.
Surgical factors include type of procedure (breast surgery, amputation,
thoracotomy), length of surgery and repeat surgery for the same pathology. Surgical
approach is also important, as the use of a laparoscopic technique results in less
CPSP for cholecystectomy and hernia repairs. The use of adjuvant radiotherapy is
also associated with a significantly increased risk of CPSP.
Patient factors include age (CPSP after breast cancer surgery decreases by 5% for
each yearly increase in the patient’s age ), genetic susceptibility and psychosocial
risk factors. For example, fear of surgery after breast surgery is associated with
worse pain and a higher risk of progression to CPSP. Additionally, the severity of
postoperative pain positively correlates with the incidence of development of CPSP.
Diabetes is not a recognised risk factor for the development of CPSP.
Searle RD, Simpson KH. Chronic post-surgical pain. Contin Educ Anaesth Crit Care Pain 2010; 10(1):12–14.
23. D McGill pain questionnaire
Pain is a complex, subjective experience which often requires specialised assessment
tools to fully evaluate and quantify. Numerous pain rating scales have been developed
over the years and it is important as anaesthetists to appreciate the context in which
they should be used. Unidimensional pain scales are useful for evaluating acute pain
of clear aetiology (e.g. postoperative pain) since they allow quick assessment of pain
intensity and response to treatment. However, they are less effective in evaluating
chronic pain, since they often fail to measure the associated affective and disabling
Answers
components. Multidimensional pain scales are more appropriate in these cases since
they allow measurement of these other facets of the pain experience.
The McGill pain questionnaire is one of the most extensively tested
multidimensional scales, and is the most appropriate tool to use in the above clinical
scenario. The three-part questionnaire assesses not only the sensory aspects but
also the affective component of pain which the above patient is suffering from.
This assessment tool may also help identify whether there are any specific pain
syndromes (such as neuropathic pain) present.
The numeric rating scale is a commonly used unidimensional pain scale where
patients rate their pain intensity on a ten point scale with a score of ten representing
'the worst imaginable pain'. It is easy to use and has been validated in numerous
settings and pain types. However, it only measures one dimension of pain which
limits its usefulness in the chronic pain setting. It is also less reliable in patients with
cognitive impairment.
The visual analog scale is an assessment tool composed of a ten centimetre line
representing the spectrum of pain intensity from ‘no pain’ to the ‘worst pain
imaginable’. Patients are instructed to mark a point on the line which corresponds
to their level of pain, and the distance between this mark and zero is measured. This
tool is sensitive for variations in pain intensity with treatment and is reproducible.
However, like the numeric rating scale, it only measures one component of the
complex multidimensional nature of chronic pain.
The verbal descriptor scale is a six point categorical scale of descriptive words from
‘no pain’ to ‘worst possible pain’ which the patient can use to express their pain
experience. It allows for a rapid assessment of pain intensity and is easy to use at the
bedside. However, it forces the patient to use someone else’s words to describe their
pain and does not measure the multidimensional components of chronic pain.
The Wong–Baker FACES scale is another categorical scale with faces conveying
expressions of pain with increasing severity. Patients are instructed to select the face
which best matches how they are feeling to provide a crude measure of their pain
experience. It is a useful assessment tool for children and patients with cognitive
impairment who may otherwise have difficulties in quantifying their pain but it is
not the most appropriate scale to use in patients with chronic pain.
Breivik H, Borchgrevink P, Allen S, et al. Assessment of pain. Br J Anaesth 2008; 101(1);17–24.
Garra G, Singer A, Taira B, et al. Validation of the Wong-Baker FACES Pain Rating Scale in pediatric
emergency department patients. Acad Emerg Med 2010; 17(1):50–54.
24. Perform a nerve block
Preoperative pain management for fractured neck of femur patients is a significant
problem. As such, the National Institute for Health and Care Excellence (NICE) have
issued guidelines (CG124) aiming to optimise analgesic management for these
patients whilst awaiting definitive surgery. This guideline states:
• Offer immediate analgesia to all patients presenting to hospital with a suspected
hip fracture, including people with cognitive impairment
• Ensure analgesia is sufficient to allow movements necessary for investigations
and nursing care
239
240
Chapter 6
• Offer paracetamol 6 hourly unless contraindicated
• Offer additional opiates if paracetamol alone does not provide sufficient
preoperative pain relief
• Considering adding a nerve block if paracetamol and opioids do not provide
sufficient preoperative pain relief, or to limit opioid dosage
• Non-steroidal anti-inflammatory drugs (NSAIDs) are not recommended
This patient would therefore most likely benefit from an ultrasound-guided femoral
nerve block or a fascia iliaca block. This is relatively simple to perform and has been
demonstrated to have a significant impact on preoperative analgesia.
National Institute for Health and Care Excellence (NICE) guidelines: Hip fracture: The management of hip
fracture in adults. CG no 124. London: NICE, 2011.
25. A Spinal cord stimulation
Complex regional pain syndrome (CRPS) is a debilitating, painful condition which
is classified into type I and II subtypes, depending on the absence or presence of
an antecedent peripheral nerve injury respectively. The lead symptom of CRPS is
limb-confined pain, but the syndrome also encompasses autonomic, motor, skin
and bone changes. If the pain is unrelenting and the physical impairment persists for
more than 2 years, the condition is considered long-term.
The aim of medication is to minimise pain and support physical rehabilitation.
Although no drugs are licensed to treat CRPS in the UK, national guidelines
encourage the use of drugs targeting neuropathic pain if simple medication is
unsuccessful after 4 weeks.
In the UK, the only National Institute for Health and Care Excellence (NICE) approved
method to treat CRPS is spinal cord stimulation, and should be considered in patients
who have not responded to appropriate integrated management. Stimulation of the
spinal cord is achieved by application of an electrical current to the dorsal columns
of the spinal cord through a catheter inserted into the epidural space. The exact
mechanism of action is unclear but some investigators suggest that spinal cord
stimulation may activate Aβ afferents which modulate the transmission of pain based
on the gate control theory. Others suggest that spinal cord stimulation may block
spinothalamic tract transmission or enhance descending inhibitory mechanisms. In
the above case where simple analgesia and medication targeting neuropathic pain
have failed, spinal cord stimulation is an appropriate next management step. In order
to assess the potential benefit of spinal cord stimulation, the electrodes are initially
stimulated by an external stimulating device prior to permanent pulse generator
insertion. Patient satisfaction is generally high, although there is some evidence that
the efficacy of this treatment generally declines over time.
The autonomic vasomotor changes seen in CRPS have led observers to previously
view the associated pain as sympathetically mediated, and although common in
early CRPS, it is actually rare in long-term cases. The use of guanethidine (which
depletes the limb autonomic nerve endings of noradrenaline) to achieve chemical
sympathectomy in the affected limb has been shown to be ineffective in randomised
controlled trials, and is not recommended.
Answers
Lower limb sympathectomy can also be achieved by creating a thermal lesion from
the application of a high frequency current to lumbar sympathetic ganglia via
percutaneous electrodes. Proponents of this intervention (termed radiofrequency
ablation), suggest that it is less invasive than surgical resection and can help break
the cycle of pain. The most recent Cochrane review however, judged that there was
no evidence from controlled trials that sympathectomy (including radiofrequency)
was no more effective than placebo or no treatment.
Amputation should not be used to provide pain relief in CRPS, and should only be
considered in rare cases of intractable infection of the affected limb. Amputation
may worsen CRPS, with symptoms recurring in the stump.
An interesting approach to tackle the symptoms of CRPS is through the use of
non-invasive brain stimulation. The treatment is based on the hypothesis that
CRPS is primarily a disease of cortical organisation which results in changes in the
way somatosensory systems process tactile, noxious and thermal information. The
aim of non-invasive brain stimulation is to induce cortical modulation through
the application of a repetitive current to improve symptoms. This treatment is an
interesting concept, however further research is needed to evaluate its efficacy.
O’Connell N, Wand B, McAuley J, et al. Interventions for treating pain and disability in adults with complex
regional pain syndrome. Cochrane Database Syst Rev 2013 Apr 30;4:CD009416.
Goebel A. Complex regional pain syndrome in adults. Rheumatology 2011; 50:1739–50.
Goebel A, Barker CH, Turner-Stokes L, et al. Complex regional pain syndrome in adults: UK guidelines for
diagnosis, referral and management in primary and secondary care. London: Royal College of Physicians, 2012.
National Institute for Health and Clinical Excellence (NICE). Spinal cord stimulation for chronic pain of
neuropathic or ischaemic origin. TA guidance 159. London: NICE, 2008.
26. D Sevoflurane maintenance over desflurane
Strabismus surgery is one of the most common paediatric ophthalmic operations.
The oculocardiac reflex and postoperative nausea and vomiting (PONV) are major
anaesthetic concerns in this procedure.
The oculocardiac reflex occurs due to traction on the extraocular muscles, which
causes bradycardia. This can be attenuated by release of surgical traction or the
administration of anticholinergic medication such as atropine. Hypercarbia can also
increase the incidence of bradycardia, therefore ventilating the patient to maintain a
normal CO2 is a technique often used.
PONV is more likely to occur in children who demonstrate the oculocardiac
reflex, therefore preventing this reflex should prevent PONV. Atropine 20 µg/kg
is advocated as a result, and so option B is not the correct answer. Intraoperative
intravenous fluids, avoiding opioid analgesia and using antiemetic prophylaxis helps
to reduce PONV incidence. Evidence suggests that ondansetron in combination with
dexamethasone is more effective than ondansetron alone.
All the volatile agents increase the risk of PONV and there is currently no evidence to
show that any one is less emetogenic than the other, hence D is the correct answer.
Carr AS, Courtman S, Holtby H, et al. Guidelines on the prevention of post-operative vomiting in children.
London: The Association of Paediatric Anaesthetists of Great Britain and Ireland, Spring 2009.
James I. Anaesthesia for paediatric eye surgery. Contin Educ Anaesth Crit Care Pain 2008; 8(1): 5–10
241
242
Chapter 6
27. C Proceed to surgery after discussing the case with your
consultant
The patient has two risk factors for moderate postoperative cardiac risk: stable
congestive heart failure and stable angina. According to the ACC/AHA 2007
guidelines for managing cardiac risk of patients for non-cardiac surgery, surgical
risk and urgency are used in conjunction with clinical risk and clinical assessment of
exercise tolerance to outline the best approach of managing complex situations such
as this. The patients with the highest risk of major adverse cardiac events (MACE), i.e.
death or myocardial infarction, are those that possess several clinical diagnoses:
•
•
•
•
•
Unstable angina
Overt congestive cardiac failure
Uncontrolled arrhythmias
Severe stenotic valvular disease
Recent myocardial infarction (within 4 weeks).
This only applies to non-emergent situations. An emergency would override those
considerations in view of the risk of MACE being higher if the operation would be
delayed.
Stable heart failure, stable angina, rate controlled atrial fibrillation, chronic renal
impairment or history of cerebrovascular event are risk factors for MACE and
increase the burden of post-operative morbidity, however delaying life or limb
saving operations to further investigate them would expose the patient to a higher
than necessary risk of MACE. The evidence presented in the guidelines suggests
that an initial assessment and improvement of the above conditions may result in a
decrease of MACE.
In this case it is a potential life or limb saving procedure has a lower risk than waiting
for a cardiology opinion to optimise his heart failure and angina. Conditioning life
or limb saving surgery to availability of a high care bed is not advisable. Early senior
involvement is the most likely step towards a safe and effective intra-operative
management for this patient.
Fleisher L, Beckman JA, Brown KA, et al. ACC/AHA 2007 Guidelines on perioperative cardiovascular
evaluation and care for noncardiac surgery. Circulation 2007; 116:e418–e450.
28. A Apical segments of the lower lobes
Pulmonary aspiration of gastric contents is one of the most serious complications
after general anaesthesia. Acid aspiration may cause immediate lung tissue injury
and subsequent severe inflammatory response.
The anatomy of the lung lobes and bronchopulmonary tree affects zonal
contamination if aspiration of gastric contents happens.
The trachea is a 10–12 cm long tube that connects the larynx to the lungs. In the first year
of life, the tracheal diameter is 3 mm or less. The diameter then increases by about 1 mm
per year until it reaches the adult size (around 20–25 mm). The trachea comprises fifteen
to twenty C-shaped cartilaginous rings. These rings are incomplete posteriorly allowing
the trachea to collapse slightly during the passage of the food in the esophagus.
Answers
It commences at the cricoid cartilage, level with the 6th cervical vertebra (C6), and
divides into right and left main bronchi at the level of the 5th thoracic vertebra (T5).
The right main bronchus (RMB) is about 3 cm long. It is shorter, wider and aligned
more vertically than the left main bronchus. Therefore, tracheal intubation and
foreign body inhalation are more likely to happen in the right main bronchus instead
of the left. The RMB gives off to 10 bronchopulmonary segments (3 in the upper lobe,
2 in the middle lobe and 5 in the lower lobe). After around 2.5–3 cm, the RMB gives off
the right upper lobe bronchus (RULB). The RULB is further divided into apical, anterior
and posterior segments after. Because the RULB arises early from the right main
bronchus, it is most at risk from occlusion by a right-sided double lumen tube.
The RMB then gives off the right middle lobe bronchus (RMLB). The RMLB is oriented
forwards and downwards and further divides into medial and lateral segments. The
RMB then continues on it’s downwards course as the right lower lobe bronchus
which gives off five segments (apical, medial basal, anterior basal, lateral basal and
posterior basal).
The left main bronchus (LMB) is around 5 cm in length, and the anatomy is slightly
different from the right lung. After 5 cm, the LMB gives off the left upper lobe
bronchus, which bifurcates into a superior division and a lingular division. The
superior division gives off the apical, posterior and anterior segments of the upper
lobe, while the lingular division gives off the superior and the inferior segments. The
left lower lobe bronchus (LLLB) differs from the right lower lobe bronchus in that it
gives four segments instead of five (apical, anterior basal, lateral basal and posterior
basal). The medial basal segment is usually small and arises with the anterior
segments. Technically, this means there are four rather than five bronchopulmonary
segments on the left (see Figure 6.3).
Figure 6.3 The bronchopul­
monary segments.
Right upper lobe
• Apical
• Posterior
• Anterior
Right middle lobe
• Lateral
• Medial
Right lower lobe
• Apical
• Medial basal
• Anterior basal
• Lateral basal
• Posterior basal
Left upper lobe
• Apical
• Posterior
• Anterior
Lingula
• Superior
• Inferior
Left lower lobe
• Apical
• Medial basal
• Anterior basal
• Lateral basal
• Posterior basal
243
244
Chapter 6
Zonal contamination of the lung lobes and the bronchopulmonary segments after
aspirating is dependent on the patient’s position during the aspiration.
In a supine patient the apical segment of the lower lobe is more likely to be
contaminated because of the direct posterior orientation of the segment. If the
patient is prone, then aspiration is more likely to affect the right middle lobe or the
lingula because of their forward and downward projection. If in the upright sitting
position, the lateral or posterior basal segments of the lower lobes will be the site of
the problem, and in the lateral position, the upper lobes would be contaminated.
Engelhardt T, Webster NR. Pulmonary aspiration of gastric contents in anaesthesia. Br J Anaesth 1999;
83(3):453–460.
Bricker S. The Anaesthesia Science Viva Book, 2nd ed. Cambridge: Cambridge University Press, 2008 pp
39–41.
29. C Anorexia nervosa
Anorexia nervosa is a psychiatric disorder which affects numerous systems in the
body and involves the following diagnostic criteria:
• Body weight is less than 15% of expected or body mass index (BMI) less than or
equal to 17.5
• Self-induced weight loss involving food avoidance, purging, self-induced
vomiting or using diuretics
• Distorted body image
• Multiple endocrine dysfunctions involving hypothalamic-pituitary-gonadal axis
• Delayed pubertal events if it manifests prior to puberty
The condition affects numerous physiological systems in the body including:
• Cardiovascular – hypotension, bradycardia, myocardial dysfunction, mitral valve
prolapse, cardiomyopathy and arrhythmias
• Respiratory – metabolic alkalosis, decreased lung compliance, aspiration
pneumonia
• Gastrointestinal – enlarged salivary glands, dental caries, Mallory–Weiss tears,
oesophagitis, gastric dilatation/perforation, increased amylase, abnormal liver
function tests
• Renal – proteinuria, reduced serum Na+, K+, Cl-, H+, Mg2+, Ca2+ and renal calculi
• Endocrine – reduced FSH, LH, GnRH, T3, T4 and glucose, increased serum cortisol
• Haematological – anaemia, leucopenia, thrombocytopenia
• Neurological – reduced cognitive function, seizures, coma, neuropathy
• Musculoskeletal – osteopenia, pathological fractures, myalgia
An ectopic pregnancy, duodenal perforation or peritonitis would lead to tachycardia
along with hypotension. Hypothyroidism would lead to a reduced basal metabolism,
which would prevent weight loss. An opioid overdose would cause respiratory
acidosis as the major component in an arterial blood gas.
Denner AM. Anorexia nervosa: perioperative complications. Contin Educ Anaesth Crit Care Pain 2009;
9(2):61–64.
Answers
30. D Infusion of phosphate
Refeeding syndrome is defined as the shift of electrolytes and fluids that can occur in
patients who are malnourished and have been started on artificial feeding (enteral
or parenteral) and could have potentially fatal consequences. The hallmark feature is
hypophosphatemia but may also include hypokalaemia, hypomagnesaemia along
with abnormal sodium and fluid balance. Patients with long-standing nutritional
deficiencies like anorexia, chronic alcoholics, oncological disorders and chronic
malnutrition are at high risk. Malnourishment increases ketone bodies as fatty acids
are used as the primary source of energy. Intracellular minerals such as phosphate
are depleted, although the serum levels may be normal due to contraction of the
intracellular compartment and reduced excretion. On refeeding, glycaemia causes
insulin secretion which stimulates glycogen, fat and protein synthesis. This leads to
consumption of minerals like phosphate and magnesium, as well as co-factors such
as thiamine. Insulin secretion causes intracellular migration of glucose and water
along with a phosphate and magnesium shift thereby causing acute depletion.
Management of refeeding syndrome consists of sequential screening of serum
levels of potassium, magnesium, calcium and potassium. The levels of phosphate,
potassium, magnesium and calcium need to be replenished along with
administration of thiamine.
Excessive administration of glucose in a patient suffering from refeeding syndrome
could lead to hyperglycaemia induced diuresis, dehydration, metabolic acidosis and
ketoacidosis.
In this patient, it is therefore most appropriate to supplement the probable
hypophosphatemia with a phosphate infusion.
Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ
2008; 336:1495–1498.
245
Chapter 7
Mock Paper 7
Question
1. You are anaesthetising a previously well 43-year-old woman for a craniotomy to
remove a frontoparietal meningioma. The patient is supine, with a 30° head-up tilt.
1 hour into the operation her oxygen saturations suddenly drop from 98% to 65%,
her end-tidal CO₂ from 4.5 kPa to 2 kPa and her blood pressure, which initially
rises, begins to fall rapidly.
Which of the following best describes your initial step in the management of the
situation?
A
B
Administer 100% oxygen
Insert a right internal jugular central venous pressure catheter and aspirate any
air
C Raise the patient’s venous pressure at the operative site by levelling the table
+/– inotropic agent +/– performing a Valsalva manoeuvre
D Alert the surgeons and ask them to flood the operative site
E Turn the patient into the left lateral, head down position
2. You are caring for a 70 kg man undergoing coronary artery bypass grafting. Long
term 75 mg aspirin (once daily) was discontinued 5 days preoperatively. His
separation from cardiopulmonary bypass (CPB) was uneventful but during sternal
wiring the surgeon states that the patient is ‘oozy’ and you note there is already
500 mL in the mediastinal drain. The activated clotting time (ACT) is 115 seconds.
You send a sample for thromboelastography (TEG).
Based on the results shown below in Table 7.1, what is the most appropriate treatment?
Table 7.1
Parameter
Value
Reference range
r time
32 mm
15–30 mm
k time
12 mm
6–12 mm
α°
40°
40–50°
Maximum amplitude (MA)
40 mm
50–60 mm
Ly30
5.0%
< 7.5%
ACT
115 seconds
90–130 seconds
248
Chapter 7
A
B
C
D
E
Further 50 mg protamine and 2 units of fresh frozen plasma
2 g tranexamic acid
10 units cryoprecipitate and 50 mg protamine
2 units of fresh frozen plasma and 2 pools of platelets
Re-open the patient and explore for bleeding immediately
3. You are asked to assess a 78-year-old man scheduled for a tansurethral resection of
his prostate (TURP) for prostate cancer. He appears fit and well but complains of
being intermittently ‘light headed’. A portion of his ECG is shown in Figure 7.1.
I
aVR
V1
V4
II
aVL
V2
V5
III
aVF
V3
V6
II
Figure 7.1
What is the most appropriate course of action to take?
A
B
C
D
E
Refer for DDD pacemaker preoperatively
Schedule for surgery after reviewing a transthoracic echocardiograph
Refer for an AAI pacemaker preoperatively
Refer for a VVIR pacemaker postoperatively
Check electrolytes and if normal schedule for surgery
4. A 65-year-old man with severe obstructive sleep apnoea/hypopnoea syndrome has
recently started using an auto-titrating nasal continuous positive airway pressure
(CPAP) device to treat his day time somnolence after lifestyle modifications
failed to help. In clinic, he feels no better and admits to not fully complying with
the treatment because of nasal stuffiness and irritation at night with occasional
epistaxis.
What is the most appropriate next step in managing his sleep apnoea?
A
B
C
D
E
Change to fixed level CPAP
Change to bilevel positive airway pressure
Apply humidification
Introduce a mandibular repositioning device
Offer uvulopalatopharyngoplasty
Questions
5. A 39-year-old woman with a body mass index of 46 kg/m2 for umbilical hernia
repair is seen in day surgery pre-assessment clinic. She has well controlled
hypertension. She has been told she snores loudly but sleeps well with no daytime
somnolence. Her neck circumference is 35 cm, and her oxygen saturation on air is
96%. Her ECG is normal.
Which of the following options is the most appropriate next action?
A
B
C
D
E
She can proceed for day case surgery
She should be listed for inpatient surgery
She should be referred for sleep studies
She should have a glucose tolerance test
She should be advised to lose weight prior to surgery
6. A 73-year-old man in the recovery room is extremely confused, combative and is
tachypnoeic. The recovery staff are struggling to perform any other observations.
He has had a radical robotic prostatectomy for locally confined prostatic
carcinoma. The surgery was technically complex and the procedure duration was
nearly 7 hours. On examination the only obvious signs are his severe delirium and
agitation, and you also notice significant periorbital swelling.
The immediate treatment for the likely condition includes:
A
B
C
D
E
Non-invasive humidified CPAP by mask
Non-invasive BiPAP by mask
Heliox with added entrained oxygen and urgent ENT referral
Ophthalmology opinion
Reintubation and head-up positioning
7. A 50-year-old man awaiting surgery for a mediastinal tumour becomes
progressively more tachypnoeic and stridulous on room air. Heliox is administered
as a holding measure until more definitive treatment is instituted and his
symptoms slowly improve.
Which physical property of helium is most important in improving his respiratory
distress?
A
B
C
D
E
A reduced density compared to air
A higher viscosity compared to air
A higher thermal conductivity compared to air
A lower blood: gas solubility coefficient compared to air
Its non-reactivity within the airway
8. A 55-year-old man is undergoing emergency coronary angioplasty for myocardial
infarction in the cardiac catheterisation suite after return of spontaneous
circulation from a ventricular fibrillation (VF) cardiac arrest. You have been
urgently called to provide a general anaesthetic as he is becoming increasingly
drowsy and confused with a Glasgow coma score of 10/15. There is an anaesthetic
machine present in the room.
249
250
Chapter 7
What should you prioritise as your first action?
A
B
C
D
E
Check the anaesthetic machine
Ensure suction and a tipping trolley is present
Take a history and perform a brief neurological examination
Draw up the emergency drugs
Call for anaesthetic assistance
9. A 75-year old woman with chronic anaemia and angina is to have a Colles' fracture
reduction under Bier’s block.
Which local anaesthetic agent would be the most appropriate to use for this block?
A
B
C
D
E
Levobupivacaine
Lignocaine
Ropivacaine
Prilocaine
Chloroprocaine
10. A 65-year-old woman is to have a palmar fasciectomy of the middle finger under
axillary nerve block. 30 minutes after performing the block, it is apparent that the
median nerve is spared. You decide to perform a supplementary median nerve
block.
Which of the following approaches to the median nerve would be the most
appropriate for this case?
A
B
C
D
E
Wrist
Mid-forearm
Axillary
Antecubital fossa
Supraclavicular
11. A 6-year-old boy with global developmental delay is first on your surgical list for an
orchidopexy procedure. At your pre-assessment visit his mother tells you he can
be a “nightmare” and is not up to date with vaccinations after a bad experience at
their local health centre. She doesn’t think he will cooperate with induction, and
is clearly anxious herself. The child will not interact with you and runs off to the
play area as you approach. In the anaesthetic room, you make a single attempt
for intravenous access, which is unsuccessful. The child is inconsolable and the
mother is visibly distressed.
The best way to proceed would be:
A
B
Cancel this elective case and explain to the mother counselling/play therapy
will be required before rebooking
Overpower the child and proceed with an inhalational induction with
sevoflurane at 8% in oxygen
Questions
C
Overpower the child and proceed with an inhalational induction with
sevoflurane at 8% in oxygen and nitrous oxide
D Send the child back to the ward and prescribe an oral midazolam premedication
at a dose of 0.5 mg/kg, resending for the child at 15 minutes post dose
E Send the child back to the ward and prescribe an oral ketamine premedication
at a dose of 5 mg/kg, resending for the child at 15 minutes post dose
12. A 35-year-old man has presented with a syncopal episode the day after a fall
during a rugby match, and CT scan has confirmed an extra-dural haematoma.
What features would indicate that intubation should be performed before transfer
to a neurosurgical centre?
A
B
C
D
E
Glasgow coma score (GCS) 11/15
An episode of vomiting
A seizure
Suspected skull fracture
A drop in GCS by 1 point on the verbal scale
13. A 45-year-old man has suffered an isolated, catastrophic, irrecoverable traumatic
brain injury. In the last few minutes he has become progressively tachycardic,
hypotensive and polyuric despite aggressive filling with intravenous crystalloid.
His observations include: heart rate 100 beats per minute sinus rhythm, blood
pressure 75/45 mmHg, stroke volume 82 mL.
The first vasoactive drug of choice in this scenario is:
A
B
C
D
E
Adrenaline
Dopamine
Labetalol
Vasopressin
Metaraminol
14. A 76-year-old man has undergone an uneventful 3-vessel on-pump coronary
artery bypass grafting (CABG) 4 hours ago and is currently sedated and ventilated
on the intensive care unit. He has normal ventricular function demonstrated
on a pre-operative transthoracic echo (TTE). On review the noradrenaline dose
has increased from 0.08 µg/kg/min to 0.2 µg/kg/min to maintain a target blood
pressure while the central venous pressure is static at 12 mmHg. There is a total
of 300 mL of blood in the chest drains. An arterial blood gas demonstrates a
worsening metabolic acidosis.
What is the next appropriate intervention?
A
B
C
D
E
Organise an urgent TTE
Request the cardiothoracic surgeon to attend immediately
Give sequential intravenous crystalloid boluses of 100 mL
Commence dobutamine at 2.5 µg/kg/min
Insert a pulmonary artery catheter to guide fluid therapy
251
252
Chapter 7
15. A 65-year-old man with an established history of moderate COPD was admitted
with an acute, infective exacerbation 5 days ago. He has never required invasive
ventilation and has a good exercise tolerance.
Following a sedation hold, the patient is awake and co-operative. He appears
comfortable on CPAP 5 cmH2O with 18 cmH2O of inspiratory pressure support
(iPS). His Pao2 is 8.5 kPa on a Fio2 of 0.28. He coughs spontaneously with moderate
strength but has a significant secretion load. He is cardiovascularly stable. A
spontaneous breathing trial is performed, but within 5 minutes he has rapid
shallow breaths and looks to be struggling, while a repeat blood gas shows a
significant increase in his Paco2, recurrence of a mild acute respiratory acidosis
and a modest fall in his Pao2.
On the basis of this spontaneous breathing trial the best strategy is:
A
B
C
D
E
Extubate onto mask ventilation
Perform a percutaneous tracheotomy later today and wean the iPS as tolerated
Institute protocolised gradual reduction in pressure support
Initiate titrated interval sprint weaning (work and rest cycles)
Re-sedate and recommence synchronised intermittent mandatory ventilation
(SIMV)
16. A 74-year-old man has been ventilated on the intensive care unit for 3 days after
having an emergency laparotomy for bowel obstruction, which was complicated
by acute kidney injury requiring filtration. Overnight he spiked a temperature and
required an increase in his noradrenaline infusion and inspired oxygen delivery.
Which investigation is going to be most useful in determining the most appropriate
choice of immediate empirical antibiotic treatment?
A
B
C
D
E
Blood cultures from a peripheral site and from the central line
CT abdomen
Sputum and urine cultures
Stool sample
Chest radiograph
Questions
17. A 69-year-old woman with an established history of essential hypertension, type
2 diabetes mellitus and chronic renal impairment (baseline urea 9.8 mmol/l and
creatinine 142 μmol/l), underwent elective, on-pump, coronary artery bypass
grafts yesterday. She successfully met all of her enhanced recovery cardiovascular
and respiratory parameters and has consequently been extubated and not on any
continuous infusions of vasoactive drugs. Her fluid balance is positive 2,430 mL
and her urine output has been averaging 18 mL/hour (actual body weight 92 kg,
ideal body weight 62.5 kg) (see Table 7.2).
Table 7.2 Blood results
ICU admission (16 hours ago)
Now
Bicarbonate (HCO3
20 mmol/l
14 mmol/l
Sodium
140 mmol/l
130 mmol/l
Potassium
5.6 mmol/l
6.4 mmol/l
Urea
7.6 mmol/l
17.6 mmol/l
Creatinine
110 µmol/l
182 µmol/l
–)
On the basis of this information the best renal treatment strategy is:
A
B
C
D
E
Commence dopamine infusion at 2.5 mg/kg/hour
Give 15 units of short acting insulin in 50 mL of 50% dextrose in 15 minutes
Give 500 mL of 1.23% sodium bicarbonate over 1 hour
Give 20 mg of furosemide intravenously followed immediately by an infusion
at 5 mg/hour
Commence renal replacement therapy
18. A late booking 37-year-old Bangladeshi woman presents to the labour ward
stating she has been having painless vaginal bleeding intermittently for most of
the pregnancy. She is 37/40 pregnant, haemodynamically stable and not in active
labour. After review by the obstetric team, a Grade III placenta praevia is diagnosed
and she is to have a category III Caesarean section.
Which of the following should form part of your anaesthetic plan?
A
B
C
D
E
Large bore intravenous access, group and save
Large bore intravenous access, cross-matched blood, general anaesthesia
Cross-matched blood, intraoperative cell salvage, regional anaesthesia
Group and save, intraoperative cell salvage, general anaesthesia
Large bore intravenous access, cross-matched blood, intraoperative cell
salvage
253
254
Chapter 7
19. A 27-year-old woman is rushed into theatre from the midwifery-led birthing
centre with a post-partum haemorrhage (PPH) of 800 mL. The obstetric registrar
has diagnosed uterine inversion and has tried manual reduction without success.
The patient has a blood pressure of 100/60 mmHg and a heart rate of 95 beats
per minute. She has adequate intravenous access, is receiving a second litre of
crystalloid and is comfortable on Entonox.
What is the best line of management to undertake next?
A
B
C
D
E
General anaesthesia and immediate laparotomy
Administration of a tocolytic agent
Immediate infusion of 2 units of O– blood
Regional anaesthesia to relax the uterus
Rapid infusion of 500 mL of crystalloid, then regional anaesthesia
20. A 3-year-old, 16 kg child is scheduled for adenotonsillectomy for recurrent
tonsillitis and mild obstructive sleep apnoea. He is the second case on the
afternoon ENT list. His mother gave him a light breakfast at 7 am, and he has had
nothing to eat or drink since. The morning list is overrunning, it is now 1 pm, and
the child is unlikely to be anaesthetised until 4 pm. The nurse on the ward informs
you that the child is getting upset because he is hungry and thirsty.
The best course of action is:
A
B
Postpone the case for another day, and let the child eat and drink
Let the child drink clear water until 2 pm, with plan to anaesthetise the child at
4 pm
C Start an intravenous infusion of 0.9% saline
D Start an intravenous infusion of 0.9% saline with 5% dextrose
E Continue to fast the child, and aim to do the child as soon as possible
21. A 2-month-old, 6 kg boy is having an emergency laparotomy for bowel obstruction.
The temperature from a nasopharyngeal thermistor reads 35.8 °C.
The best way to reduce heat loss through radiation is:
A
B
C
D
E
Turn the theatre temperature up
Use a warm air blanket
Use an overhead radiant heater
Cover the patient’s head with a hat
Use warm irrigation fluid
22. A 46-year-old man developed back pain after heavy lifting 6 months ago, and still
has pain in his lower back radiating to his buttocks. He finds that he has to limit his
gardening and play golf due to the pain.
Questions
Which of the following is the most likely cause of his pain?
A
B
C
D
E
Epidural adhesions
Facet joint
Disc prolapse
Discogenic
Sacroiliac pain
23. A 36-year-old primigravida who is 38/40 pregnant presents to the labour ward.
She has a body mass index (BMI) of 40 and is known to have pre-eclampsia
for which she takes labetalol. Currently her blood pressure is 158/96 mmHg. A
vaginal examination reveals she is 6cm dilated and she is coping well with her
contractions. Bloods show platelets of 98 x 109/L with normal clotting.
What would be the most appropriate way to manage her labour analgesia?
A
B
C
D
E
Remifentanil patient-controlled analgesia
Intramuscular pethidine
Entonox
Epidural with patient controlled epidural analgesia
She does not require any analgesia at present
24. A 69-year-old man is undergoing elective hip replacement surgery. He has a
history of significant chronic obstructive pulmonary disease (COPD) which is
controlled with regular inhalers. You offer him a spinal anaesthetic for his surgery.
Which of the following would be the most appropriate post operative analgesia
option?
A
B
C
D
E
Patient controlled analgesia with morphine
Patient controlled analgesia with fentanyl
Oral opioids on a regular basis
Intrathecal diamorphine
Femoral nerve catheter and infusion of bupivacaine
25. A 38-year-old woman who is well known to the pain clinic presents with acuteon-chronic lower back pain. There is no radiation of pain and there are no red flag
symptoms. Previous MRI was unremarkable. She has had facet joint injections
in the past which have been effective for up to 2 weeks. She is currently taking
paracetamol 1 g four times daily and Oxycontin 20 mg twice daily.
What would be the most appropriate next step in the management of this patient’s
ongoing pain?
A
Increase Oxynorm to 30 mg twice daily with Oxynorm 5 mg for breakthrough
pain
B Book for further facet joint injections
C Book for lumbar epidural
D Add amitriptyline
E Referral to a pain management program
255
256
Chapter 7
26. A 30-year-old man with ulcerative colitis is undergoing a total colectomy. He has
been on long term opioids via a fentanyl patch at 50 µg per hour for the past year.
He has refused an epidural for post operative analgesia.
What would be the most appropriate option for pain relief?
A
Patient controlled analgesia (PCA) with morphine 1 mg bolus and keeping his
fentanyl patch on
B Doubling the dose of the fentanyl patch
C Bilateral transverse abdominis plane (TAP) blocks
D Increasing the fentanyl patch to 75 µg per hour and using a PCA using fentanyl
bolus of 20 µg only
E PCA with fentanyl bolus 10 μg and a background infusion of 10 µg per hour
27. You review a 7-year-old boy in the emergency department of a district general
hospital. He has an 11% total body surface area (TBSA) burn involving his chest
from hot cooking oil. It looks mostly partial thickness in nature. His vital signs
including GCS are stable.
Which of the information provided above meets referral criteria to a specialised
burns centre?
A
B
C
D
E
Being 7 years old
Having an 11% TBSA scald
A likely significant inhalational injury
Any burn involving hot oil
He does not meet any of the criteria required for referral to a specialised burns
centre
28. A 72-year-old man had an elective above-knee amputation under a combined
spinal-epidural. The operation was uneventful and finished at 2 pm. The surgeon is
keen to start the thromboprophylaxis with dalteparin 2,500 units subcutaneously
at 10 pm.
What specific instructions do you need to convey to the ward nurses concerning
removal of the epidural catheter and administration of further doses of
thromboprophylaxis?
A
Remove the catheter after checking the prothrombin time and activated
prothrombin time
B Remove the catheter after 10 am the following day and then administer the
dalteparin immediately afterwards
C Remove the catheter at 10 pm the following evening and then administer the
dalteparin immediately afterwards
D Remove the epidural catheter at 11 am the following day and administer the
dalteparin after 4 hours
E Keep the epidural catheter in situ and wait for anaesthetic advice
Questions
29. A 42-year-old female being pre-assessed for gastric banding surgery is known to
snore at night and has a body mass index (BMI) of 48 kg/m2.
As per the STOP-BANG questionnaire, which of the following assessment criteria
would she need to fulfill in order to be termed high risk for obstructive sleep
apnoea (OSA)?
A
B
C
D
E
Collar size of 38 cm
High blood pressure
Diabetes
Pulmonary hypertension
Collar size of 33 cm
30. A 64-year-old man is brought to the emergency department with dizziness and
difficulty in breathing. He has a heart rate of 68 beats per minute and a blood
pressure of 76/40 mmHg. On auscultation he has generalised rhonchi and is
wheezy. There is no rash on examination. He states that he suffers from chronic
glaucoma and his ophthalmologist has recently changed his eye drops.
Which of the following eye drops is the most likely cause for this clinical picture?
A
B
C
D
E
Phenylephrine
Adrenaline
Brimonidine
Levobunolol
Apraclonidine
257
258
Chapter 7
Answers
1.D Alert the surgeons and ask them to flood the operative
site
Venous air embolism is a potentially fatal clinical situation. Aspiration of
approximately 1mL/kg can generate an ‘air locked’ pulmonary circulation. It can
occur in any surgical position providing the operative site is above the level of the
heart. If the hydrostatic gradient between the site and the right atrium is negative,
air can potentially move into the venous circulation and directly into the right
atrium. From here it passes into the right ventricle and on to the pulmonary artery. If
large enough it will entirely obstruct flow of blood through the ventricular outflow
tract. Subsequently, an air embolism initially increases right heart pressures and
critically impairs gas exchange. Cardiac output, end-tidal CO₂ and O₂ saturations
decrease. Ultimately, such deterioration can lead to cardiac arrest. Neurosurgical
procedures are especially high risk as veins may be held open by boney structures.
Management priorities are to stop further air inflow, reduce the volume or remove
any air that has accumulated and to treat any development of cardiovascular (CVS)
collapse. The initial action should therefore be to immediately alert the surgeons
who should obstruct any further air entry by flooding or applying a wet swab to the
site. 100% oxygen should then be administered, followed by methods to increase
venous pressure at the site. This can be achieved by levelling the table, applying
pressure to the neck, administering a fluid challenge +/- an inotrope or conducting
a Valsalva manoeuvre. If a central venous line is in situ, it should be aspirated. If CVS
collapse occurs the patient should then be turned into the left lateral, head down
position if possible, and cardiopulmonary resuscitation initiated.
Webber S, Andrzejowski J, Francis G. Gas embolism in anaesthesia. Contin Educ Anaesth Crit Care Pain
2002; 2(2):53–57.
Pollard BJ (ed). Handbook of Clinical Anaesthesia, 2nd edn. London: Elsevier Science, 2003.
2. D 2 units of fresh frozen plasma and 2 pools of platelets
It has been reported that up to 20% of cardiac surgery patients bleed significantly
postoperatively. The need for resternotomy increases the chance of further
complications including prolonged mechanical ventilation, adult respiratory distress
syndrome (ARDS) and wound infection. In addition to obvious surgical causes of
bleeding, dysfunction of the coagulation cascade can occur for a variety of reasons.
Causes of perioperative coagulopathy can have the mnemonic ‘ACHE’:
•
•
•
•
•
•
Antiplatelet agents
Contact with cardiopulmonary bypass circuit
Haemodilution
Heparin
Hypothermia
Excessive fibrinolysis
Answers
Coagulation defects may not be fully appreciated with more simple tests such
as the activated clotting time (ACT), prothrombin time (PT) or activated partial
thromboplastin time (APTT). The thromboelastograph (TEG) tests the entire
process of coagulation and gives five parameters which may be used to identify a
coagulation defect (Table 7.3).
Table 7.3 Key parameters of a thromboelastograph test
Parameter
Definition
Function of
Reference
range*
Derangements
r time
Time from test
initiation to fibrin
formation
Clotting factor
activity
15–30 mm
7.5–15 minutes
Prolonged by:
Clotting factor deficiencies
Anticoagulants
Severe hypofibrinogenaemia
k time
Time taken to
achieve a certain
level of clot
strength, usually
20 mm amplitude
Clotting factors, fibrin and
platelets
6–12 mm
3–6 minutes
Prolonged by:
Clotting factor deficiencies
Anticoagulants
Hypofibrinogenaemia
α°
Speed at which
clot forms
Fibrin polymerisation
40–50°
Decreased by:
Clotting factor deficiencies
Anticoagulants
Hypofibrinogenaemia
Maximum
amplitude
(MA)
Maximum
strength (amplitude) of clot
Platelet
function
Fibrin bonding
50–60 mm
Decreased by:
Thrombocytopenia
Platelet dysfunction
Hypofibrinogenaemia
Ly30
The percentage
decrease in
amplitude 30
minutes after MA
Fibrinolysis
< 7.5%
Increased by:
Excessive fibrinolysis
*Reference ranges for each parameter differ depending on whether or not the sample has been
activated with celite or kaolin (both of which hasten the formation of clot). The values given here refer
to unactivated whole blood. The X axis of the TEG (time) is given in mm, where 2 mm is usually equal to
1 minute.
The TEG from this patient shows a prolonged r time and low maximum amplitude,
implying a delay in the initiation of fibrin formation and formation of a low strength
clot (Figure 7.2). This suggests a problem with the quantity and/or function of
clotting factors, fibrinogen and platelets; a situation best addressed with option D.
There is no suggestion of excessive fibrinolysis from the TEG so further tranexamic
acid would not be optimal management at this stage (option B). Although the other
options may improve the situation by providing clotting factors (A) and fibrinogen
(C) only option D provides platelets too. Resternotomy may be required if bleeding
increases or continues after normalisation of the coagulation profile.
As MA is a composite of the dynamic relationship between platelet function and
fibrin formation, standard TEG may not be sensitive to residual effects of antiplatelet
259
260
Chapter 7
α
r
20 mm
Ly30
k
MA
Delayed clot initiation
= prolonged r time
Figure 7.2 Sample TEG tracings
from a patient with normal
coagulation (top) and one with
signs suggestive of clotting
factor deficiency and low platelet
function (either quantitative or
qualitative).
Low clot strength
= Low MA
r
drugs. A modification of the technique, the platelet mapping assay, utilises the
addition of activators (arachidonic acid and ADP) to quantify the degree of platelet
aggregation and inhibition due to aspirin and clopidogrel respectively.
Paparella D, Brister SJ, Buchanan MR. Coagulation disorders of cardiopulmonary bypass: a review.
Intensive Care Med 2004; 30(10):1873–81.
Thakur M, Ahmed AB. A review of thromboelastography. Int J Periop Ultrasound Appl Technol 2012;
1(1):25–29.
Curry ANG, Pierce JMT. Conventional and near-patient tests of coagulation. Contin Educ Anaesth Crit Care
Pain 2007; 7(2):45–50.
Weitzel NS , Weitzel LB, Epperson LE, et al. Platelet mapping as part of modified thromboelastography
(TEG) in patients undergoing cardiac surgery and cardiopulmonary bypass. Anaesthesia 2012;
67(10):1158–65.
3. A Refer for DDD pacemaker preoperatively
The ECG shows Mobitz II atrioventricular (AV) block that is symptomatic based on
the history given. This is a class I indication for pacemaker insertion which should be
performed preoperatively, thereby excluding options B and E. The other indications
for permanent pacemaker insertion in the context of acquired AV block are outlined
in Table 7.4.
As the problem is with AV conduction at a level defined during electrophysiology
(EP) studies, atrial pacing alone (option C) will not prevent ventricular
bradyarrhythmias. Ventricular pacing (option D) alone cannot maintain AV
synchrony and may lead to pacemaker syndrome, where loss of synchrony leads
to symptoms of fatigue and functional limitation. A dual chamber mode with
adaptive rate control (option A) preserves AV synchrony, protects against ventricular
bradycardia and enables a normal chronotropic response to activity. Therefore
the most appropriate management step for this patient is to refer for preoperative
pacemaker on DDD mode.
For full understanding of the pacemaker codes, it is useful to refer to the NAPSE/
BPEG coding system (Table 7.5).
A summary of the various pacing modes is given in Table 7.6.
Answers
Table 7.4 Indicators for permanent pacemaker insertion
Class I indications – general consensus of benefit
Third-degree and advanced second-degree AV block associated with:
– Symptomatic bradycardia
– Arrhythmias requiring drug therapy
– Documented periods of asystole
– Neuromuscular disease
– Cardiomegaly or LV dysfunction
– Exercise
Class II indications – evidence/opinion generally in favour
Asymptomatic second degree block at intra/infra His levels on electrophysiological studies
Third-degree block with rate > 40, no symptoms and structurally normal heart
Table 7.5 The NAPSE/BPEG coding system
I
II
III
IV
V
Chamber(s)
paced
Chamber(s)
sensed
Mode(s) of
response
Programmable functions
Anti-tachycardia
function
V = ventricle
V = ventricle
T = triggered
R = rate modulated
O = none
A = atrium
A = atrium
I = inhibited
C = communicating
P = paced
D = dual
D = dual
D = dual
M = multiprogrammable
S = shocked
O = none
O = none
O = none
P = simple programmable
D = dual
O = none
Table 7.6 Summary of pacemaker modes
Pacemaker mode
Description
AOO, VOO, DOO
Asynchronous modes which pace atria (A), ventricles (V) or both chambers (D)
irrespective of the patient’s own heart rate
May compete with the patient’s own cardiac rhythm and lead to tachyarrhythmia and decreased battery life
VVI, VVT
Ventricular pacing modes where the intrinsic R wave is sensed
Indicated in atrial flutter, atrial fibrillation and instances of ventricular pauses
Not used for AV nodal disease (see above)
DDD, DVI, DDI
and VDD
Dual chamber modes so there are atrial and ventricular electrodes
AV sequential pacing modes which preserve normal AV contraction sequence
Indicated in AV block and sinus node disease
Epstein AE, Ellenbogen KA, Freedman RA, et al. Guidelines for Device-Based Therapy of Cardiac Rhythm
Abnormalities: A Report of the American College of Cardiology/American Heart Association Task Force on
Practice Guidelines. J Am Coll Cardiol 2008; 51(21):e1–e62.
Salukhe TV, Dob D, et al. Pacemakers and defibrillators, anaesthetic implications. Br J Anaesth 2004;
93(1):95–104.
261
262
Chapter 7
4. C Apply humidification
Obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is a common disorder
characterised by intermittent upper airway collapse during sleep. An apnoea is
defined as a ten second breathing pause due to complete airway closure, whereas
a hypopnoea describes an episode where ventilation is reduced by at least 50% for
10 seconds due to partial collapse. OSAHS is graded into mild, moderate and severe
categories by the apnoea-hypopnoea index (number of events per hour of sleep)
and the severity of symptoms.
In order to improve daytime somnolence, the treatment aim is to reduce the
frequency of nocturnal apnoeas/hypopnoeas with options including lifestyle
modification, dental devices, surgery and the application of continuous positive
airway pressure (CPAP). The National Institute for Health and Care Excellence (NICE)
have recently recommended that all moderate to severe symptomatic cases of
OSAHS should be offered CPAP therapy. There is also a role for CPAP therapy in
symptomatic mild cases of OSAHS, but only if lifestyle modification has failed to
make a difference.
CPAP devices work by producing a continuous positive pressure (set between 5
and 20 cmH2O) which prevents upper airway collapse and subsequent apnoeas
or hypopnoeas during sleep. Problems with compliance to therapy are common
since upper airway symptoms such as nasal dryness, bleeding and throat irritation
can occur as a result of high flows of dry, cool air through the nose. Humidification
devices are now frequently used in conjunction with CPAP devices to prevent these
symptoms. In the above case, application of a humidifier is the most appropriate
next management step since this may improve CPAP compliance in order to
accurately assess treatment effect before exploring other options.
Fixed CPAP devices as the name suggests, deliver air at a set pressure throughout
the night which can lead to non-adherence due to pressure intolerance. To
minimise these side effects and reduce mean airway pressures, auto-titrating
CPAP devices have been developed. These devices vary the treatment pressure
applied automatically based on feedback from changes in airflow resistance. In the
above scenario, the patient is already using an auto-titrating CPAP device and is
not complaining of pressure intolerance so changing to a fixed device is therefore
unlikely to improve adherence.
Bilevel positive airway pressure (BiPAP) delivers positive airway pressure at different
levels during inspiration and expiration. BiPAP not only prevents upper airway
collapse but also augments tidal volume and can achieve lower mean airway
pressures when compared to CPAP. In relation to the above case, it is unlikely to
improve the upper airway symptoms affecting compliance however.
Mandibular repositioning devices are designed to improve upper airway patency by
protruding the mandible to expand the posterior airspace. However, the maximum
attainable airspace expansion is perceived to be modest, and currently these
devices are only considered appropriate for mild to moderate OSAHS. Mandibular
repositioning devices can be used in patients who refuse to use or fail to respond
to CPAP. It is not the most appropriate next management step in the featured case
Answers
since the OSAHS is severe and the treatment benefit of CPAP has not yet fully been
established.
In the absence of a resectable obstructing lesion such as tonsillar hypertrophy, the
role of surgery in treating OSAHS remains contentious.
Uvulopalatopharyngoplasty (UPPP) is a common surgical approach which involves
resection of the uvula, retrolingual soft tissue and palatine tonsillar tissue in an
attempt to improve airway patency in this context. However, surgery does not
guarantee symptom improvement and may compromise future CPAP therapy by
promoting mouth leakage and limiting the maximum pressure level tolerated. In
the above case, surgery is not the most appropriate management step as there is no
obvious obstructing lesion, and symptoms may improve by increasing adherence to
the CPAP machine alone.
Appraisal Committee and National Institute for Health and Care Excellence (NICE) project team.
Continuous positive airway pressure for the treatment of obstructive sleep apnoea/hypopnoea syndrome.
Technology appraisal guidance 139. London: NICE, 2008.
McDaid C, Griffin S, Weatherley H, et al. Continuous positive airway pressure devices for the treatment
of obstructive sleep apnoea-hypopnoea syndrome: a systematic review and economic analysis. Health
Technol Assess 2009; 13(4):1–119,143–274.
Scottish Intercollegiate Guidelines Network (SIGN).Guideline development group. Management of
obstructive sleep apnoea/hypopnoea syndrome in adults. A national clinical guideline. Edinburgh: SIGN,
2003.
Weaver T, Grunstein R. Adherence to continuous positive airway pressure therapy. The challenge of
effective treatment. Proc Am Thorac Soc 2008; 5:173–178.
5. A She can proceed for day case surgery
AAGBI guidelines for perioperative management of obese patients recommend that
patients should not be excluded from day surgery on the basis of their BMI alone.
Units with appropriate resources and experienced staff can safely manage these cases
where their management would not be changed by overnight admission and in fact
benefit from early mobilisation. Patients with morbid obesity should be carefully preassessed for symptoms of cardiac, respiratory and metabolic disease. Stable OSA with
established CPAP also does not preclude day surgery, but measures such as avoiding
long acting opioids and careful postoperative monitoring are required.
A validated questionnaire STOP-BANG has been developed to identify and riskstratify patients:
•
•
•
•
•
•
•
•
Snoring – do you snore loudly? (loud enough to be heard through a closed door)
Tired – do you often feel tired or sleepy during the daytime?
Observed – has anyone observed you stop breathing in your sleep?
Blood pressure – do you have or are you treated for high blood pressure?
Body mass Index > 35 kg/m2
Age > 50 years
Neck circumference > 40 cm
Gender – male
A score of greater than 5 requires further investigation and careful perioperative
management as does the presence of any other features such as poor functional
263
264
Chapter 7
capacity, abnormal ECG, uncontrolled hypertension or ischaemic heart disease,
saturations less than 94% on air, concurrent airways disease and previous venous
thromboembolism.
In this case, the STOP-BANG score is 3 and further cardio-respiratory investigation is
not required. Sleep studies are not indicated unless symptoms of excessive daytime
sleepiness or witnessed apnoeas in the presence of other risk factors are reported.
In-patient surgery or overnight admission is not required if her postoperative Spo2
is maintained at baseline levels on air without stimulation, and routine discharge
criteria can be met. Although diabetes should be screened for with a random blood
glucose check a formal glucose tolerance test is not indicated. Pre-assessment clinics
are an ideal place for advice regarding lifestyle modification, however weight loss
must be carefully controlled and monitored and is unlikely to alter management in
this case if surgery is postponed.
Association of Anaesthetists of Great Britain and Ireland (AAGBI). Peri-operative Management of the
Morbidly Obese Patient. London: AAGBI, 2007.
Chung F, Subramanyam R, Liao P, et al. High STOP-Bang score indicates a high probability of obstructive
sleep apnoea. Br J Anaesth 2012; 108(5):768–775.
Society for Obesity and Bariatric Anaesthesia. Anaesthesia for the Obese Patient: BMI> 35 kg/m2. London:
Society for Obesity and Bariatric Anaesthesia, 2014.
6. E Reintubation and head-up positioning
Robotic surgery is becoming increasingly widespread, and may now be found in
many centres and specialties including general surgery and gynaecology. In the
UK by far the largest body of established work involves urology, and specifically
prostatectomy. The perceived benefits include increased nerve preservation within
the pelvic field and thus higher chances of retaining urinary continence and erectile
function. There may also be some advantages in terms of comfort/analgesia and
reduced blood loss. Indeed, it is now not uncommon for patients to be discharged in
the first 24 hours following surgery.
The robot
The da Vinci system is the most common system in use in the UK at the current time.
This system is made up of a surgical control console with an immersive high-definition
visual display, a computer tower, and the robotic surgical manipulator. The manipulator
is a large, heavy trolley comprising the surgical arms which is then ‘docked’ to the
patients table. One arm supports the camera, and others are then inserted into the
ports. A scrubbed assistant is still required, while the unscrubbed surgeon sits at the
console, which may be distant from the patient. The robot has no autonomy in function;
it merely acts as a ‘telemanipulator’ transmitting the surgeon’s movements from the
console. There are case reports of surgery having been performed with the surgical
console being situated in a different country from the patient.
The advantage over standard laparoscopic surgery comes from several sources.
First, fewer assistants are required, with one scrubbed surgeon and a scrub nurse.
The camera contains dual optical apparatus meaning that a stereoscopic picture is
possible in the display console, allowing for depth perception. The robot arms have
extra jointed articulations allowing advanced movements and greater degrees of
Answers
freedom compared to normal laparoscopic instruments. The apparatus filters tremor
and automatically scales movements, all greatly facilitating microsurgery.
Specific physiological considerations
For the most part the considerations are those of laparoscopic surgery, however
access to the patient is severely limited, and the position is very extreme. This
exaggerates all the physiological changes such that complications may ensue if
precautions are not taken. Due to the time taken to uncouple the robot from the
patient, (may be several minutes) a plan for emergency access to the patient must
be rehearsed.
The surgery requires steep head-down in the Trendelenburg position which may
be as steep as 45°. For this reason, the attention to detail during positioning is vital.
Strapping of the shoulders to prevent patient slipping can produce traction on the
brachial plexus, and the lower limbs must be carefully positioned to reduce the
risk of well leg syndrome and thromboembolism. The transition to this position
can cause movement of the tracheal tube, due to migration of the tube in either
direction, but also movement of the trachea and the diaphragm upward. Once
in this position the added cardiovascular insult of pneumoperitoneum can cause
major haemodynamic instability which if not resolved by countermeasures, may
necessitate conversion to an open procedure.
The degree and duration of Trendelenburg present a series of problems less
common in other types of surgery, but still thankfully rare. Reflux of gastric
secretions can cause chemical damage to the mucosa of the mouth and also
unprotected eyes. Antacid premedication can be helpful. The increase in systemic
vascular resistance, mean arterial pressures and intracranial pressures accompanied
by decreased venous return can cause oedema of the dependent head and
neck tissues, and patients are often warned to expect facial and eye swelling
postoperatively. This has been associated with laryngeal oedema and stridor, and
cerebral oedema with marked confusion, requiring reintubation and head up
positioning for some hours before successful extubation. For this reason, and to
reduce ureteric flow a conservative fluid strategy is often adopted once the head
down position is achieved.
Confusion in recovery is a popular exam topic with a vast array of differentials. The
clue here is the type and duration of surgery, and knowing something about the
position involved during the robotic technique obviously helps. The patient could be
hypoxic, but in this condition is unlikely to tolerate non-invasive ventilation anyway.
Airway oedema can occur in these patients, but no mention is made of stridor in the
stem. Facial swelling and cerebral oedema should subside in hours with supportive
measures and head up position. CT scanning should also be considered.
Irvine M, Patil V. Anaesthesia for robot-assisted laparoscopic surgery. Contin Educ Anaesth Crit Care Pain
2009; 9(4):125–129.
7. A A reduced density compared to air
Helium is an odourless, colourless and biologically inert noble gas whose unique
physical properties can be exploited when managing an upper airway obstruction.
265
266
Chapter 7
It is presented as Heliox 21, which is the generic name for the mixture of 21% oxygen
and 79% helium. In order to appreciate its role in the management of an upper
airway obstruction, the types of flow within the airway needs to be revisited.
Gas flow within the respiratory tract can be either laminar or turbulent. Laminar flow
is unidirectional and smooth with molecules moving in parallel creating a parabolic
flow profile. This is an efficient type of flow. Turbulent flow on the other hand has an
essentially flat flow profile with molecules swirling in eddies and vortices rather than
an orderly way. This is an inefficient form of flow and conversion from laminar to
turbulent flow approximately halves the flow rate for a given pressure drop.
Whether or not flow is turbulent or laminar depends on a dimensionless number
called the Reynolds number (Re) (turbulent flow being more likely if Re > 2000):
Re = ρvd/μg
ρ = density, v = linear velocity, d = diameter of the tube, μ = viscosity, g =
gravitational factor.
In constricted upper airways, the airflow is turbulent and inefficient. Since heliox
is approximately three times less dense than air, its administration will cause a
reduction in the Reynolds number thus increasing the likelihood of more efficient
laminar flow. Even in situations where turbulent flow persists, heliox still flows much
easier when compared to air since the flow rate is inversely related to the density of
the carrying gas.
The viscosity of helium is in fact very similar to air, and does not explain why heliox
is beneficial in upper airway obstruction scenarios. Flow rate is inversely related to
the gas viscosity in established laminar flow, which is different to the turbulent flows
seen in the above case.
Helium does have a high thermal conductivity and prolonged administration may be
associated with a lowering of body temperature. This however does not significantly
affect the airflow patterns within the respiratory tree.
Another useful physical property of helium is its very low blood: gas solubility. The
helium dilution technique works on the principle that helium remains within the
lung due to its low solubility in blood allowing the functional residual capacity to be
estimated.
Helium is chemically inert because its filled valence orbitals are less able to interact
with other compounds. Helium has no direct pharmacological effects and is not a
treatment in its own right. It should be viewed as a bridging therapy whilst waiting
for the effects of other treatments to have effect (Table 7.7).
Table 7.7 Physical properties of helium, oxygen and nitrogen at 20°C and 1 atmosphere
Helium
Oxygen
Nitrogen
Density (ρ; g/L)
0.1785
1.251
1.429
Viscosity (μ; micropoises)
188.7
167.4
192.6
Thermal conductivity (K; μcal/s/°K)
352
58
58.5
Answers
Mitchell V. Gas, tubes and flow. Anaesthesia and intensive care medicine. 2010; 11(1):32–35.
Harris P, Barnes R. The uses of helium and xenon in current clinical practice. Anaesthesia 2008; 63:284–293.
Gainnier M, Forel J. Clinical review: use of helium-oxygen in critically ill patients. Crit Care 2006; 10(6):241.
8. E Call for anaesthetic assistance
Anaesthesia in remote locations is associated with risk. It represents an unfamiliar
environment, using anaesthetic equipment and monitoring, which may be only used
on occasion, and personnel that do not routinely work together and are unfamiliar
with anaesthetic practices. In the cardiac catheter lab the radiology equipment
often makes it difficult to access and visualise the patient and the table may be fixed
and unable to tilt head down. The focus of the staff is often on the revascularisation
and in these challenging situations especially when dealing with patients that are
critically unstable, communication and effective team working are paramount.
The 2013 Royal College of Anaesthetists (RCoA) guidelines on anaesthesia in nontheatre settings outline the staffing, drug, equipment and safety requirements that
should be met when anaesthesia is provided in these remote locations. Equipment for
induction, maintenance and emergence from anaesthesia should be available as is in
theatre, and monitoring should be ideally separate from that used by the cardiologist.
Space and equipment should be set up to deal with the possibility of cardiac arrest.
In this scenario, there are many essential checks and tasks that need to be swiftly
performed before anaesthesia can be administered. The RCoA guidelines state
that anaesthesia in remote locations cannot be performed by a single individual,
and that a dedicated, qualified and skilled anaesthetic assistant should always be
available, and provide exclusive help to anaesthetist. Clearly the machine, drug and
equipment checks are all important, however, calling early for anaesthetic assistance
is essential and the other tasks can be conducted once this has been requested.
Peden C. Guidelines for provision of services for anaesthetic care in the non theatre environment 2013.
Guidelines on the provision of anaesthetic services. London: Royal College of Anaesthetists, 2013.
9. B Lignocaine
Bier’s block anaesthesia is a form of intravenous regional anaesthesia (IVRA) that
was first introduced by the German surgeon August Bier in 1908. It involves the
administration of local anaesthetic (LA) intravenously into a tourniquet-blocked
limb thus localising the anaesthetic in that limb. The technique is based on the
principle that local anaesthetic diffuses from the vascular bed to the capillary plexus
surrounding the nerve, causing conduction block in the nerve involved.
IVRA is primarily indicated for surgical procedures on the elbow, forearm or hand
requiring anaesthesia for up to one 1 hour, such as fracture manipulation. It can also
be successfully performed on quick lower limb procedures of the foot, ankle and
lower leg. However, the block is difficult to perform in the lower limb and requires
larger amount of local anaesthetic.
The steps to perform a Bier’s block involve:
1. Before commencing the Bier’s block, patient should be informed and consented
adequately and fully starved. IVRA should be performed in a safe environment
267
268
Chapter 7
2.
3.
4.
5.
6.
7.
8.
9.
10.
where the patient is fully monitored with resuscitation equipment and
emergency drugs available.
Two intravenous cannulae are established, one in the operated arm (as distal as
possible) and another in the contralateral limb to administer sedation or other
drugs if required.
A double cuff tourniquet is applied on the arm involved. The arm is then
exsanguinated either by applying Esmarch bandage or raising it for two minutes
while compressing the axillary artery.
The distal cuff is inflated to at least 100 mmHg above the patient’s systolic blood
pressure followed by inflating the proximal cuff to the same pressure.
Once the tourniquet is secure, the distal cuff can be deflated.
The LA solution is injected in the operated arm after confirming the absence of a
radial pulse. It is very important to inject the local anaesthetic slowly to prevent
the peak venous pressure from exceeding the tourniquet occlusion pressure and
hence leakage of LA to the systemic circulation.
Once the injection is completed, remove the cannula and apply pressure on the
puncture site.
After 10–15 minutes, when the anaesthesia is established, the distal cuff is
inflated followed by the deflation of the proximal cuff to relieve the tourniquet
pain below the proximal cuff. The tourniquet must not be deflated before 20
minutes because releasing the tourniquet early may result in a large amount
of LA being released immediately into the systemic circulation, increasing the
danger of LA toxicity.
Once the surgical operation has been completed, the tourniquet should
be deflated in two stages. By deflating the tourniquet for 10 seconds then
reinflating it for 1 minute before the final release, the chance of systemic toxicity
is reduced by gradually washing out the LA from the operated limb.
It is mandatory to continue monitoring the patient for at least 10 minutes after
the procedure.
Although IVRA is a simple and safe technique, specific knowledge in local
anaesthetic pharmacology is required in order to avoid rare but serious
complications.
A variety of local anaesthetic agents have been used to perform a Bier’s block,
however prilocaine and lignocaine are currently the most commonly used drugs.
In the UK, 0.5% prilocaine is the drug of choice for IVRA. It is the least toxic LA as
it is the most rapidly metabolised of the amides. Prilocaine is an amide LA, the
recommended dose is 3 mg/kg (maximum dose is 6 mg/kg), and usually 40 mL of a
0.5% solution is injected in the operated arm.
Prilocaine is associated with methaemoglobinaemia, especially when the dose
exceeds 600 mg. Although this is clinically insignificant in most patients, small
amounts of methaemoglobin can cause a significant decrease in oxygen-carrying
capacity in patients with anaemia and heart disease, hence it should be avoided.
Therefore prilocaine is not appropriate for the patient in this clinical scenario.
In North America, lignocaine remains the most frequent used amide LA in a dose of
not more than 3 mg/kg. Many emergency doctors and anaesthetists in the UK are
Answers
still using lignocaine as their first choice due to its availability and reliability in IVRA.
The New York School of Regional Anesthesia (NYSORA) has recommended 12–15 mL
of 2% lignocaine for upper limb procedures or 30–40 mL of 2% for lower extremities.
It would be the most suitable agent for this clinical scenario.
Bupivacaine is another amide LA. In addition to blocking neurotransmission, it also
affects the myocardium and is avoided in IVRA because of its cardiotoxicity. Death has
also been reported in some studies; therefore its use is contraindicated in many centres.
Although levobupivacaine and ropivacaine are safer and less cardiotoxic than
bupivacaine, the use of these local anaesthetics does not provide rapid onset of
anaesthesia or superior analgesia, and they are not recommended for IVRA.
Chloroprocaine is an ester local anaesthetic. It is a vasoconstrictor and has a rapid
onset time of 3–5 minutes. It is less toxic than lignocaine and has a shorter duration
of action. However, it is not used in IVRA in the UK due urticarial rash and venous
irritation following cuff release in some patients.
Although many drugs have been used as additives to local anaesthetics in IVRA
such as neostigmine, ketamine, clonidine, muscle relaxants and dexamethasone,
ketorolac 20 mg is the primary drug that has demonstrated some evidence in
relieving tourniquet pain and prolonging postoperative analgesia.
The New York School of Regional Anesthesia (NYSORA). Bier’s block. www.nysora.com/techniques/3071–
bier-block.html
Rivera JJ, Villecco DJ, Dehner BK, et al. The efficacy of ketorolac as an adjunct to the Bier block for controlling
postoperative pain following nontraumatic hand and wrist surgery. AANA J 2008; 76(5):341–345.
10. D Antecubital fossa
Upper limb peripheral nerve blocks are used to provide analgesia and anaesthesia
for elbow, forearm, wrist and hand surgery. They may also be used to augment a
brachial plexus block or provide perioperative analgesia after a general anaesthesia.
The median nerve (C5-T1) arises from both the medial (C5, C6, C7) and the lateral
cords (C8, T1) of the brachial plexus. In the arm, the nerve passes lateral to the
brachial artery, which it then crosses, and descends on its medial side to the
antecubital fossa. In the forearm, the median nerve lies between the bellies of flexor
digitorum profundus and flexor digitorum superficialis. And at the wrist, it lies
medial to flexor carpi radials and lateral to the tendon of palmaris longus.
It supplies sensory innervation to the radial side of the palm, and the palmar surface
of the lateral 3 and half fingers, including their dorsal tip to the first interphalangeal
joint. It provides motor innervation to most of flexor muscles in the forearm and
thenar muscles of the thumb.
One of the most important branches of median nerve is the anterior interosseous
nerve. This nerve arises from the median nerve just distal to the antecubital fossa. It
descends between the ulna and the radius along the interosseous membrane. The
anterior interosseous nerve supplies the flexor pollicis longus, the flexor digitorum
profundus (lateral half ) and the pronator quadratus. It is essential to block the
anterior interosseous nerve for successful median nerve block.
269
270
Chapter 7
The median nerve can be blocked at various places and can be performed using
peripheral nerve stimulator, landmark technique and/or ultrasound (US) guided with
a high frequency probe.
At the brachial plexus: the median nerve lies in close relation to the axillary artery and
vein in the axilla and can be blocked independently or in conjunction with the ulnar,
radial and musculocutaneous nerves here. See question 4.10 for further details.
At the mid-arm level: the nerve lies above the brachial artery. Using a high frequency
US probe or nerve stimulator, a single injection of 5–7 mL of local anaesthetic is
enough to block the nerve.
At the antecubital fossa: using a high frequency US probe, the median nerve is seen
as a single hyperechoic elliptical structure immediately medial to the brachial artery.
5–7 mL of local anaesthetic is injected after visualising the nerve. With a peripheral
nerve stimulator technique, the needle is directed perpendicularly and the nerve
should be found within 1–2 cm depth, medial to the brachial artery pulsation. After
stimulating the median nerve (pronation, finger flexion and thumb opposition),
5–7 mL of local anaesthetic is injected.
This approach successfully blocks the anterior interosseous nerve, and for this
clinical scenario it is the correct answer.
At the mid-forearm: a high frequency US probe is moved laterally to visualise the
median nerve in axial section as a hyperechoic structure. Again, 5–7 mL of local
anaesthetic is injected around the nerve.
At the wrist: the nerve lies between the tendons of flexor carpi radialis and palmaris
longus. It can easily be blocked by ultrasound or nerve stimulator techniques, 2 cm
proximal to the wrist crease.
In this scenario, the best place to block the median nerve is in the antecubital fossa
because it is essential to block the anterior interosseous nerve for successful median
nerve block. The anterior interosseous nerve is usually missed in the mid-forearm
and the wrist approach. The axillary approach is not an option in this scenario
because it has already been attempted and was unsuccessful. Spared nerves should
be augmented with local anaesthetic injections distally and not proximally, so a
supraclavicular approach is not the best option.
The radial and ulnar nerves can also be blocked throughout their course. The radial
nerve (C5-T1) is the largest branch of the brachial plexus. It is derived from the
posterior cord. During its course, it gives branches to the triceps muscle and then
enters the spiral groove where it lies behind the humerus. In the spiral groove,
the median nerve gives off the posterior cutaneous nerve of the forearm. It then
descends in the elbow between the brachioradialis and the brachialis muscles. At
the lateral epicondyle of the humerus, it divides into superficial and deep terminal
branches. The superficial branch supplies sensation to the dorsum of the hand, while
the deep branch becomes the posterior interosseous nerve, which provides motor
innervation to the extensor muscles of the elbow, wrist and fingers.
The radial nerve block is not usually performed below the elbow because it of its
division into superficial and deep branches just proximal to the elbow.
Answers
With a peripheral nerve stimulator technique, the nerve is usually found 1-2 cm
above the brachial crease between the biceps tendon and the brachioradialis
muscle. Around 5–7 mL of local anaesthetic is injected after stimulating the nerve
(fingers and wrist extension). Using a high frequency US probe, the radial nerve can
be blocked at the spiral groove below the triceps and above the humerus. It can also
been blocked at the antecubital fossa. The probe is placed in the antecubital crease
and then moved lateral and proximal. At this area, the radial nerve is visualised
as an elliptical structure that divides into superficial and deep branches between
the brachioradialis and the brachialis muscle. Again, 5–7 mL of local anaesthetic is
injected around the two branches.
The ulnar nerve (C8, T1) arises from the medial cord of the brachial plexus. During
its course, it passes behind the medial epicondyle to enter the forearm between the
heads of flexor carpi ulnaris. It supplies the flexor carpi ulnaris and half of the flexor
digitorum profundus. It provides motor innervation to the intrinsic muscles of the
hand and sensation to the medial one and a half fingers.
The ulnar nerve can be blocked below or above the elbow. At the elbow level, the
ulnar nerve lies between the medial epicondyle and the olecranon process. Blocking
the nerve at this level could cause ischaemia due to high compartment pressures
and should be avoided.
The safest approach is distal to the elbow. Placing a high frequency US probe on the
flexor surface of the forearm, the nerve is seen on the medial side of the forearm,
lying medial to the ulnar artery. Follow the nerve with the probe until the ulnar
nerve separates from the artery.
With a peripheral nerve stimulator, the nerve is usually found 3–4 cm proximal to the
ulnar groove. Around 5–7 mL of local anaesthetic is injected after stimulating the
nerve (ulnar deviation of the wrist and medial finger flexion).
Brennan A, Jones M, Gordon J. Ultrasound-guided local anaesthetic blocks of the forearm. Anaesthesia
Tutorial of the Week 208. London: World Federation of Societies of Anaesthesiologists, 2011.
McCahon RA, Bedforth NM. Peripheral nerve block at the elbow and wrist. Contin Educ in Anaesth Crit
Care Pain 2007; 7(2):42–44.
11. Send the child back to the ward and prescribe an
oral midazolam premedication at a dose of 0.5 mg/kg,
resending for the child at 15 minutes post-dose
Having an uncooperative child at induction is not uncommon, in studies distress
at induction occurs in a third of children, with a quarter requiring some form
of physical restraint. There are several factors which predict problems during
anaesthetic induction, and eliciting these can help in making an induction strategy
and preparing the parents beforehand.
Risk factors for induction distress
• Withdrawn, shy, introverted demeanour
• Anxious children
• Ages 1–3 (increased separation anxiety)
271
272
Chapter 7
• Previous negative hospital experiences
• Previous turbulent reaction at vaccination
Drug treatments
Midazolam is the most widespread sedative premedicant in the UK. The oral dose is
0.5 mg/kg, giving an onset at 5-10 minutes peaking at 20–30 minutes. It may also be
given intranasally or sublingually at a dose of 0.2 mg/kg. The intranasal route may be
possible if oral medication is rejected, but it can give a burning sensation.
Fentanyl can be given transmucosally in a lollipop, with a bioavailability of 33%
via this route. A dose of 15–20 µg/kg will produce sedation at 20 minutes with a
peak at 30–40 minutes. The whole host of opioid side-effects including respiratory
depression are a drawback.
Vallergan (trimeprazine) is a sedating antihistamine from the phenothiazine class.
Like other phenothiazines, it is also beneficial in being antiemetic and antimuscarinic.
Since midazolam has been shown to be superior, Vallergan is now used less often.
Ketamine can be given orally at a dose of 5–8 mg/kg, with an onset at 10 minutes
and peak at 25 minutes. Intramuscular ketamine at a dose of 4–5 mg/kg works in 5
minutes and is reserved for those patients in whom all other strategies have failed
and who may be displaying aggressive /combative behaviour. Ketamine side effects
include tachypnoea, hypersalivation, ballistic limb movements and the classical
emergence hallucinations. Where ketamine has been used patients should be
nursed in a calm, quiet area with standby provision of resuscitation equipment.
Holding and restraint
In general, the principle is to use restraint only as a technique of last resort. Minimal
force required for safety (of staff and patient) should be employed, by appropriate
numbers of experienced/trained staff. The plan should be discussed with the
parent(s) beforehand, and opportunity for debrief discussions with parent and child
should exist afterwards.
In this case the induction process has clearly broken down, and the risk of
proceeding with a distressed child and mother has to be balanced against the
urgency of the procedure. In an emergency if the child had already failed with
premedication and the mother had been warned and was happy to proceed/
participate with an inhalational induction, this might be the next step. However the
risk of laryngospasm in a crying, anxious and distressed child is unacceptable here.
Cancellation is an option, but even with further preparation and psychological input
the risk of induction distress still persists, thus sending the child back to the ward
and trying a premed is valid. Midazolam is the first line in this situation.
Tan L , Meakin GH. Anaesthesia for the uncooperative child. Contin Educ Anaesth Crit Care Pain 2010;
10(2):48–52.
12. C A seizure
Intubation for transfer is indicated in patients who have:
• GCS 8 or less
Answers
•
•
•
•
•
•
•
•
Drop in GCS of 2 points or 1 point in the motor scale
Loss of protective laryngeal reflexes
Ventilatory insufficiency: Pao2 < 13 kPa on oxygen, Paco2 > 6 kPa
Spontaneous hyperventilation with Paco2< 4 kPa
Irregular respiratory pattern
Seizures
Unstable facial fractures
Bleeding into the airway
Principles during transfer should be to reduce and avoid surges in intracranial
pressure, maintain cerebral perfusion pressure and prevent secondary brain injury.
• The patient should receive sedation and analgesia via a syringe driver and
adequate muscle relaxation. Aims should be for a Pao2 > 13 kPa, Paco2 4.5–5 kPa
unless there is clinical or radiological evidence of raised intracranial pressure
where hyperventilation to a Paco2> 4 kPa with a higher Fio2 is justified
• Endotracheal tubes should be secured but tight tube ties avoided. The patient
should be placed in a 15–30 degree head up position
• Avoid hypotension. Hypovolaemia is poorly tolerated during transfer due to the
effects of motion, and circulating volume should be normalised before departure.
Inotropes may be indicated to achieve an adequate mean arterial pressure
(> 80 mmHg) after volume expansion if hypotension persists
• Consider loading with an anticonvulsant, e.g. phenytoin prior to transfer
• Avoid hypoglycaemia
National Institute for Health and Care Excellence (NICE). Triage, assessment, investigation and early
management of head injury in children, young people and adults. CG No 176. London: NICE, 2014.
Association of Anaesthetists of Great Britain and Ireland. Recommendations for the safe transfer of
patients with brain injury. London: AAGBI, 2006.
13. D Vasopressin
As catastrophic brain injury progresses into brainstem death, dramatic changes in
cardiovascular physiology often occur due to one or more of the following:
• hypovolaemia secondary to diabetes insipidus caused by acute posterior pituitary
failure
• myocardial depression due to catecholamine and cytokine toxicity
• the transition from hypertensive catecholamine excess into vasoplegic
hypotension
In managing this clinical situation, a rapid, systematic approach to the cardiovascular
system is essential and must encompass cardiac rate and rhythm, preload,
contractility and afterload. The cardiovascular observations given suggest the
patient has diabetes insipidus, has received adequate volume resuscitation but is
vasoplegic. Current expert recommendations and limited trial evidence supports the
use of vasopressin as the optimal first line agent in this scenario.
Bugge JF. Brain death and its implications for management of the potential organ donor. Acta
Anaesthesiologica Scandinavica 2009; 53(10):1239–1250.
Ball J. Optimal management of the potential organ donor following catastrophic brain injury. ICU
Management 2013; 13(2):10–13.
Callahan DS, Neville A, Bricker S, et al. The effect of arginine vasopressin on organ donor procurement and
lung function. J Surg Res 2014; 186(1):452–457.
273
274
Chapter 7
14. C Give sequential intravenous crystalloid boluses of
100 mL
The priorities after coronary artery bypass grafting are as follows: warm, wean, and
wake. This simple list (which has obviously been designed by a surgeon) allows the
consideration of problems at each stage:
Warming
• As warming occurs vasodilation may occur which may result in relative
hypovolaemia
• Reperfusion may result in transient metabolic disturbances
Weaning
• Refers to reducing vasoconstrictor, inotrope and ventilator requirements, which
should be routine if there are no complications as a result of surgery or anaesthesia
Waking
There are several causes of prolonged waking which may be respiratory function
related, metabolic, temperature-related, or anaesthetic and analgesic related, but
most concerning are:
• ‘Pump-head’ a multi-factorial syndrome causing global cerebral dysfunction
due to micro-emboli (particulate and gas) and hypo-perfusion
• Embolic stroke (regional deficit)
• Haemorrhagic stroke (regional deficit)
The complications that may occur which disrupt weaning include:
Cardiac pump-failure
• Global myocardial dysfunction due to pre-existing disease, myocardial
stunning, metabolic and electrolyte disturbances or inappropriate
vasoconstrictor and inotrope usage
• Regional myocardial dysfunction due to a thrombosed graft, embolic
obstruction, a kinked graft or poor cardioplegia delivery
• Arrhythmias:
–– Tachycardia (atrial fibrillation is the most common) treated with
pharmacological measures or rarely electrical cardioversion
–– Bradycardia treated with either atrial pacing (if no atrioventricular
conduction delay is present), ventricular pacing (if an atrioventricular block
is present), or with atrioventricular sequential pacing
Mechanical obstruction
• Tension pneumothorax (pleura surgically opened if internal mammary arteries
used for grafting)
• Cardiac tamponade
• Haemothorax if drains are obstructed with blood clot formation
Bleeding which may be assessed by monitoring the chest drain output
• Surgical
–– Graft anastomotic site
–– Venous graft tributary
–– Site of cannulation (aortic or atrial), suture lines, sternal wire holes
• ‘Anaesthetic’
–– Dilutional coagulopathy
–– Inadequately reversed unfractionated heparin
Answers
In the case above there is evidence of worsening haemodynamic performance (an
increased vasoconstrictor requirement) and end-organ perfusion (a worsening
metabolic acidosis) without an obvious bleeding source and without an increased
central venous pressure. An ABC approach is needed to identify which of the
differential diagnosis are most likely. The immediate intervention, if no obvious
cause is found, is a trial of intravenous fluid therapy (100 – 250 mL boluses) and
assessment of fluid-responsiveness. As mentioned before, the combination of
warming, reperfusion, fluid re-distribution and a small amount of blood loss may be
all that is wrong.
A transthoracic or oesophageal echo is an extremely useful investigation. A visualised
tamponade or regional wall abnormality that may indicate a graft-malfunction
indicates the need to return to theatre however a collection of blood posterior to
the heart causing tamponade may not be visualised. Global dysfunction seen on the
echo due to myocardial stunning may be treated with correction of metabolic and
electrolyte abnormalities or an inotrope such as dobutamine or milrinone.
A repeat full blood count and clotting analysis including a thrombelastogram (TEG)
is helpful to guide blood product administration if bleeding is suspected.
The surgical team should be informed of the developments early. Cardiothoracic
surgeons are experienced in weaning patients after bypass grafting and often have
useful insights regarding the particulars of the surgery. If the patient continues to
deteriorate, a repeat thoracotomy in theatre (or on the intensive care unit in extreme
situations) may be required.
Walcot N, Marchbank A. Postoperative care of adult cardiac surgery patients. Surgery 2012; 30(1):13–16.
15. D Initiate titrated interval sprint weaning (work and rest
cycles)
The scenario suggests a mixed picture of good and bad prognostic factors. In
particular, declining exercise tolerance, low body mass index and/or significant
recent weight loss and more than two hospital admissions per year are poor
prognostic markers in patients with chronic obstructive pulmonary disease (COPD).
This patient fulfils all the criteria for a spontaneous breathing trial, the purpose of
which is to assess the likelihood of successful extubation. He resoundingly fails the
trial by all criteria.
Ventilatory management in this population is challenging and arguably more of an
art than a science. The best answer suggested here is controversial.
Though there is increasing enthusiasm for extubation and immediate application
of mask ventilation in scenarios such as that outlined, the risks and benefits are
complex and the relative merits of this approach are currently the subject of a
number of large, randomised control trials. This patient has a relative contraindication in having a heavy secretion load with only a moderate strength cough.
Non-invasive ventilation (NIV) will increase his difficulty in secretion clearance and
therefore places him at significant risk of ventilator failure despite NIV and requiring
re-intubation. Should this occur, this sequence of events is associated with a higher
morbidity and mortality that continuing invasive support.
275
276
Chapter 7
Performing a tracheostomy at day 5, would be considered too early by most
practitioners, unless, the educated guess was that a patient would clearly need
> 10–14 days of invasive support. There is no clear evidence to support either an
‘always early’ or ‘always late’ strategy.
Protocolised weaning is advocated by many practitioners. Its success is probably
more attributable to the organisational and logistic benefits rather than any
physiological rationale. However, given that respiratory muscle fatigue is the
principal cause of weaning failure in COPD patients, there is a growing body of
evidence ranging from exercise physiology to cardiac rehabilitation to support
a titrated work rest cycle approach utilising short bursts of high activity with
prolonged periods of effective rest. Hence D is considered the best answer.
In the scenario given there is no rationale to re-sedate and SIMV is proven to be
detrimental to weaning as opposed to CPAP with iPS, which promotes it.
Burns KE, Meade MO, Premji A, Adhikari NK. Noninvasive positive-pressure ventilation as a weaning
strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev 2013;12:CD004127.
Gomes Silva BN, Andriolo RB, Saconato H, Atallah AN, Valente O. Early versus late tracheostomy for
critically ill patients. Cochrane Database Syst Rev 2012;3:CD007271.
Blackwood B, Alderdice F, Burns K, et al. Use of weaning protocols for reducing duration of mechanical
ventilation in critically ill adult patients: Cochrane systematic review and meta-analysis. Br Med J
2011;342:c7237.
Gist NH, Fedewa MV, Dishman RK, Cureton KJ. Sprint interval training effects on aerobic capacity: a
systematic review and meta-analysis. Sports Med 2014; 44(2):269–79.
16. E Chest radiograph
This is a very common scenario on the intensive care unit. Patients are predisposed
to getting infections due to immobility, sedation, invasive tubes, relative
immunosuppression and being handled by staff continually.
The differential diagnosis as to the source of infection in this gentleman is broad
and therefore it is worth narrowing it down to the most likely culprit in order to
choose an appropriate antibiotic. In general the first organ systems to consider are
those that have contact with the external environment (skin including invasive lines,
urinary tract, gastrointestinal tract and respiratory tract). These are also the easiest
to investigate, as samples from these organs are relatively easy. If these are negative
then consideration of more anatomically-isolated systems are needed (hepatobiliary,
intra-abdominal, endocardial, central nervous system and bone). Finally if these are
negative, rarer causes such as non-bacterial infections, malignancy, inflammatory,
antibiotic related and neurologically-mediated should be investigated.
The term ventilator-associated pneumonia (VAP) refers to pneumonia occurring
in patients more than 48 hours after endotracheal intubation and mechanical
ventilation. The risk factors include:
• Patient
• Extremes of age
• Immunosuppression
• Respiratory co-morbidities
Answers
• Airway
• Emergency intubation
• Presence of endotracheal tube
–– No coughing
–– Decreased mucociliary clearance
–– Micro-aspiration of sub-glottic
–– Intra-luminal formation of biofilm
• Increased duration of intubation
–– Early onset < 96 hours
–– Late onset > 96 hours
• Late tracheostomy (contentious)
• Head injury or altered consciousness (including sedation)
• Poor mouth care and tracheobronchial toileting
• Gastrointestinal
• Nasogastric feeding
• Prolonged use of proton-pump inhibitors
• Prolonged supine position
Early onset VAP commonly results from community-acquired pathogens such as
Staphylococcus aureus, Streptococcus pneumoniae and Haemophilus influenzae.
Late onset VAP is often a result of infection with drug resistant organisms such as
Pseudomonas sp. and methicillin resistant Staphylococcus aureus (MRSA).
There are several scoring criteria published, which have been suggested in which to
aid the early diagnosis. These include:
• Clinical signs
• Temperature above 38°C or below 36°C
• Leukocytosis or leucopenia
• New purulent secretion production
• Worsening gas exchange or increased oxygen requirement
• Imaging
• Radiographic signs of new consolidation (generalised or focal)
• Microbiology
• Sputum or bronchial lavage samples
In this scenario you are not given specific clinical details so diagnosis is more
difficult. However, infections being common at this early stage of the patient’s
clinical course, a chest infection would be high on the differential diagnosis. In
addition a chest radiograph will give an immediate answer allowing prompt
empirical treatment whereas all other investigations listed will take more time to
return with useful information.
Rea-Neto A, Youssef NCM, Tuche F, et al. Diagnosis of ventilator-associated pneumonia: a systematic
review of the literature. Crit Care 2008; 12:R56.
Sundaram R. Nosocomial pneumonia. Anaesthesia UK, 2006.
277
278
Chapter 7
17. E Commence renal replacement therapy
In patients with normal renal function, on-pump cardiac surgery is associated with a
10–30% risk of acute kidney injury and < 5% risk of needing acute renal replacement
therapy. These risks are significantly increased in patients with pre-existing renal
impairment. Other peri-procedural risk factors include on versus off-pump, longer
bypass times, haemodynamic instability/need for high-dose or protracted inotropes
and/or vasopressors.
In the scenario described, the patient has clearly developed acute kidney injury
(AKI), with oliguria, a metabolic acidosis, hyperkalaemia and uraemia. There is no
place for low dose dopamine or diuretics in either the prevention or management
of AKI. Given the rate of evolution of this patient’s metabolic derangement and
apparently normal renal perfusion, temporising therapy to improve the acidosis and
reduce the serum potassium are unlikely to prevent the need for renal replacement
therapy, hence this is the best answer.
Of note:
• Most centres use bicarbonate based fluids for renal replacement therapy
• Although there is no universally agreed thresholds for commencing renal
replacement therapy in AKI a reasonable suggestion would include:
• Hyperkalaemia (K+ > 6.5 mmol/l or K+ > 5.5 mmol/l and rapidly rising at
> 0.25 mmol/hour for 2 or more hours)
• Correction of severe/unresolving acidosis (pH < 7.1) in particular, acidosis
associated with cardiovascular compromise (shock i.e. end-organ
hypoperfusion) / high vasoactive drug requirements (noradrenaline > 0.5 µg/
kg/min/dobutamine > 10 µg/kg/min)
• Uraemia (urea > 40 mmol/L or rising by > 12 mmol/24 hours)
• Fluid overload causing severe hypertension and/or problematic oedema (e.g.
abdominal compartment syndrome) and/or contributing to hypoxaemia/poor
lung compliance
• There is no evidence to support any specific modality over another in this setting
The use of bolus insulin and dextrose mixtures is a poor practice as it is associated
with a very high incidence of acute, severe dysglycaemia and rapid rebound
hyperkalaemia. If temporisation of hyperkalaemia is required, continuous infusions
of insulin and dextrose are safer and more effective. Adjunctive use of nebulised
salbutamol and intravenous bicarbonate can also be very helpful. If cardiac toxicity is
evident, acute protection is afforded by a slow bolus of intravenous calcium either as
gluconate or chloride.
Bellomo R, Chapman M. Low-dose dopamine in patients with early renal dysfunction: a placebocontrolled randomised trial. Australian and New Zealand Intensive Care Society (ANZICS) Clinical Trials
Group. Lancet 2000; 356(9248):2139–43.
Karajala V, Mansour W, Kellum JA, et al. Diuretics in acute kidney injury. Minerva Anestesiol 2009;
75(5):251–7.
Palevsky PM. Renal replacement therapy in acute kidney injury. Adv Chronic Kidney Dis 2013; 20(1):76–84.
Answers
18. E Large bore intravenous access, cross-matched blood,
intraoperative cell salvage
Placenta praevia occurs when the placenta is implanted in the lower uterine
segment close to the internal cervical os. Painless vaginal bleeding in mid to late
pregnancy is a classical presentation. It is divided into four grades:
•
•
•
•
Grade I – Placenta in the lower segment but not reaching the internal os
Grade II – Placenta reaches internal os but does not cover it
Grade III – Placenta partially covers internal os
Grade IV – Placenta completely covers internal os
Risk factors include advanced maternal age, previous Caesarean section and
multiparity. The obvious concern is the propensity to bleed during labour and often
a Caesarean section is indicated. Uterine contraction may be impaired in the lower
segment, the placenta may be abnormally adherent to the uterine wall and the
placental position may make surgical access difficult. Hence, the risk of blood loss is
significant and the anaesthetic plan should account for this.
The woman must be advised regarding the high risk of blood loss and large bore
intravenous access must be secured, hence C and D are incorrect. At least 4 units of
cross-matched blood should be ready and available for immediate use, i.e. in the
labour ward fridge, if this facility exists. There must be a multidisciplinary approach to
management, with involvement of the obstetric and anaesthetic teams, haematologists
and paediatricians. Intraoperative cell salvage should be used and a rapid infusion
device available and ready. Invasive monitoring should be established if needed.
Cases like this were often performed under general anaesthesia, but there has
been a massive shift to regional techniques, such as spinal or combined spinal
epidural. Ultimately, the decision lies with the anaesthetist and patient and if
regional anaesthesia is chosen, the patient should be advised about the possibility
of conversion to general anesthesia intraoperatively. Option B is incorrect, as
intraoperative cell salvage should be part of the anaesthetic plan.
Banks A, Norris A. Massive haemorrhage in pregnancy. Contin Educ Anaesth Crit Care Pain 2005;
5(6):195–8.
Walfish M, Neuman A, Wlody D. Maternal haemorrhage. Br J Anaes 2009; 103(suppl. 1):i47–i56.
19. B Administration of a tocolytic agent
Uterine inversion is an obstetric emergency, although relatively uncommon. The
uterine fundus becomes displaced above or through the cervix, during the third
stage of labour. The placenta remains attached in many instances, which can lead
to massive haemorrhage. The accompanying haemodynamic instability is classically
stated to be out of proportion to the blood loss, due to traction of uterine ligaments
causing parasympathetic effects. This, however, may not be accurate, as blood loss
may simply be underestimated in many cases.
279
280
Chapter 7
Management focuses on uterine relaxation and reduction, and the management of
haemorrhage. In this case, the patient has lost 800 mL of blood and may lose more.
Basic resuscitation should be applied, namely, intravenous access, fluids and crossmatch. As attempts at manual reduction have failed, tocolytic therapy should be
the next line of management, such as terbutaline, magnesium sulphate or glyceryl
trinitrate. Intravenous terbutaline at a dose of 0.25 mg has been recommended
in relatively stable patients, otherwise 4 g of magnesium sulphate intravenously
is an alternative. 100 µg of glyceryl trinitrate intravenously is relatively familiar to
anaesthetists and has a quick onset of action.
If tocolytic therapy fails, then general anaesthesia to relax the uterus is indicated
and a laparotomy may be required if the uterus still cannot be reduced vaginally.
Regional anaesthesia does not cause uterine relaxation, so D and E are incorrect.
Answer C is incorrect, as the patient has stabilised with intravenous fluids and
does not need immediate O negative blood; hence it is not the best next line of
management.
Abouleish E, Ali V, Joumaa B, Lopez M, Gupta D. Anaesthetic management of acute puerperal uterine
inversion. Br J Anaesth 1995; 75(4):486–7.
Beringer RM, Patteril M. Puerperal uterine inversion and shock. Br J Anaesth 2004; 92(3):439–41.
20. B Let the child drink clear water until 2 pm, with plan to
anaesthetise the child at 4 pm
The reason for preoperative fasting is to reduce the risk of aspiration pneumonitis
at induction of anaesthesia. However, prolonged fasting does not further reduce
the risk of a harmful event for the patient, but adversely affects patient comfort and
hydration. Therefore, the period of preoperative fasting should be minimised as
close as possible to 6 hours for food and formula milk, 4 hours for breast milk and
2 hours for clear fluid, as per published consensus guidelines. If prolonged fasting is
unavoidable, such as in patients with bowel obstruction, then intravenous hydration
should be instituted.
In the case described above, there is no contra-indication to oral hydration up to 2
hours preoperatively, therefore intravenous hydration is not warranted. Postponing
the case is disruptive, unnecessary and would not be the preferred option in the first
instance.
The Association of Anaesthetists of Great Britain and Ireland (AAGBI). Safety Guideline: Pre-Operative
Assessment and Patient Preparation: the Role of the Anaesthetist. London: AAGBI, 2010.
Royal College of Nursing (RCN). Perioperative Fasting in Adults and Children: An RCN Guideline for the
Multidisciplinary Team. London: RCN, 2005.
21. A Turn the theatre temperature up
Perioperative hypothermia is associated with increased energy expenditure,
deranged coagulation, increased risk of postoperative infection, and decreased
patient satisfaction. Heat loss can be from evaporation, conduction, convection
and radiation. The increased body surface area to weight ratio of infants and small
children, combined with their deranged thermoregulation under anaesthesia, make
Answers
them particularly susceptible to inadvertent perioperative hypothermia and the
associated perioperative morbidity.
Ways to reduce heat loss from a patient include using a warm air blanket and an
overhead heater, covering the patient’s heat with an insulating hat, using low
fresh gas flow and a heat moisture exchanger, warming any intravenous fluid and
irrigation fluid, and increasing the theatre temperature and humidity. The most
effective way of reducing heat loss from radiation is to warm the theatre to minimise
the temperature difference between the patient and the surroundings.
Sessler DI. Temperature monitoring and perioperative thermoregulation. Anesthesiology 2008; 109:318–38.
Pearce B, Christensen R, Voepel-Lewis T. Perioperative hypothermia in the pediatric population:
prevalence, risk factors and outcomes. J Anesthes Clin Res 2010, doi:10.4172/2155-6148.1000102.
22. D Discogenic
Back pain is very common and usually settles within 3 months; if it persists then it
is considered chronic back pain. Chronic back pain may be simple musculoskeletal
pain (95%), spinal nerve root pain (4–5%) or serious spinal pathology (1%).
Simple musculoskeletal pain is mechanical in nature and occurs in a younger
population (20–55 years). It is usually described as a dull aching pain over the
lumbrosacral and gluteal area, and can be associated with referred leg pain which is
limited to the thighs. The pain usually varies with physical activity.
Pain from the intervertebral discs (discogenic) accounts for 40% of mechanical back
pain. Sacroiliac joint pain accounts for 20%, lower lumber facet joint pain is the cause
in 10–15% of young patients and 40% of elderly patients with mechanical back pain.
Jackson A, Simpson K. Chronic back pain. Contin Educ Anaesth Crit Care Pain 2006; 6(4):152–155.
23. D Epidural with patient controlled epidural analgesia
This woman should be advised to have an epidural early in labour not only for
pre-eclampsia but also for a raised body mass index (BMI). A working epidural
will attenuate the hypertensive response to pain during labour and also improve
placental blood flow. A low dose local anaesthetic mixture should be used to reduce
the risk of profound hypotension. A working epidural can also be extended should
a Caesarean section be required. This would avoid the risks of a potentially difficult
airway associated with pregnancy, obesity and pre-eclampsia.
It is sensible to perform the epidural with up-to-date bloods as the platelet count
can drop with increasing severity of pre-eclampsia. If there are any concerns it
should also be checked prior to removing the epidural catheter. There is no absolute
cut off for platelet number and local guidelines should be adhered to. It is however
generally accepted that an epidural can be inserted with platelets of 98 x 109 /L
provided clotting is normal. Informed consent is a must.
E Hart, S Coley. The diagnosis and management of pre-eclampsia. Br J Anaesth CEPD reviews 2003;
3(2):38–42.
281
282
Chapter 7
24. C Oral opioids on a regular basis
The risk of opioid induced respiratory depression is greater with patient-controlled
analgesia (PCA) than intrathecal opioids, therefore option D is inappropriate when
considering this patient has underlying severe COPD. In this scenario, fentanyl offers
no advantages compared with morphine and has a shorter duration of action. A
femoral catheter is good for knee surgery but it will not cover the hip well, unless it
is in the fascia iliaca. The motor block from peripheral nerve catheters is undesirable
and will inhibit early rehabilitation. Oral opioids can be continued for a number of
days and will allow mobilisation without motor block so will be the most appropriate
choice out of the available options.
Barrington JW, Halaszynski TM, Sinatra RS, Expert Working Group On Anesthesia And Orthopaedics Critical
Issues. Perioperative pain management in hip and knee replacement surgery.
In: Hip And Knee Replacement Arthroplasty FT. Am J Orthop 2014;43(4 Suppl):S1-S16.
Grant CKR, Checketts MR. Analgesia for primary hip and knee arthroplasty: the role of regional
anaesthesia. Contin Educ Anaesth Crit Care Pain 2008; 8(2):56-61.
25. E Referral to a pain management program
Chronic lower back pain is back pain that persists for greater than 3 months.
Simple musculoskeletal back pain accounts for the vast majority. Troublesome
simple back pain should be managed within a pain management setting using a
multidisciplinary approach.
There is evidence supporting the use of non-steroidal anti-inflammatory drugs
(NSAIDs) and opioids in the management of chronic back pain. Care should however
be taken in prescribing long-term NSAIDs due to their adverse effects. Strong
opioids should also be used with caution and immediate release opioids should
usually be avoided. Opioid usage should follow the principles of good opioid
prescribing set out by the British Pain Society.
There is strong evidence to support psychological approaches such as cognitive
behavior therapy (CBT) and exercise therapy. This would therefore be the most
appropriate next step in this patient’s management.
There is no data to support the use of caudal or lumbar epidural injections in the
treatment of simple back pain.
Transcutaneous electrical nerve stimulation (TENS) may be helpful short term but
there is no evidence of any longer term benefits.
Jackson MA, Simpson KH. Chronic back pain. Contin Educ Anaesth Crit Care Pain 2006; 6(4):152–155.
The British Pain Society. Opioids for persistent pain: good practice. London: The British Pain Society, 2010.
26. E Patient-controlled analgesia with fentanyl bolus 10 µg
and a background infusion of 10 µg per hour
This man is opioid tolerant and takes a background fentanyl patch 50 µg per hour.
Its conversion to morphine is variable but equates to approximately 135–224 µg
oral morphine daily. Although continuing the fentanyl patch may seem sensible
Answers
to keep the background doses, the absorption will be varied due to fluid shifts
and skin circulatory changes as a result of the surgery. It is more reliable to start a
background infusion to add to the PCA background infusion has been shown to
increase the incidence of respiratory depression in patients and there is also an
increase in the incidence of programming errors when this additional feature is
used. Therefore care must be taken when using a background infusion. Although
background infusions should not be used routinely, they can certainly be useful
in patients like in this example who are already on high doses of opioids. The
background dose is primarily included to prevent withdrawal. Increases in opioid
requirements perioperatively is roughly 20% but this also depends on the type of
surgery being performed.
Stone M, Wheatley R. Patient‐controlled analgesia. BJA CEPD Reviews 2002; 2(3):79-82.
Tordoff SG, Ganty P. Chronic pain and prescription opioid misuse. Contin Educ Anaesth Crit Care Pain
2010;10(5):158-161.
Mercadante S, Caraceni A. Conversion ratios for opioid switching in the treatment of cancer pain: a
systematic review. Palliat Med 2011; 25(5):504-15.
27. B Having an 11% TBSA scald
The British Burns Association has devised referral criteria for patients with burn
injuries. They can be viewed in full online, but include the following.
• Patients at extremes of age < 5 or > 60
• < 16 with greater than 5% TBSA burn (dermal or full thickness) or > 16 with greater
than 10% TBSA burn (dermal or full thickness)
• Dermal or full-thickness loss to face, perineum, hands, feet and flexures
• Any significant inhalational injury excluding pure carbon monoxide poisoning
• Significant co-morbidities
• Associated injuries, e.g. fractures and head injuries
• Any suspicion of non-accidental injury
Option C is incorrect in this context as you would not get an associated inhalational
injury with this mechanism.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–122.
28. D Remove the epidural catheter at 11 am the following
day and administer the dalteparin after 4 hours
APTT and PT are not influenced by the administration of low molecular weight
heparin (LMWH) therapy and cannot provide reassurance that the effects of LMWH
are no longer active. Waiting for anaesthetic advice is potentially beneficial but
could cause unnecessary delay in the patient’s mobilisation, therefore option E
is undesirable. Essentially it is recommended that a minimum of 12 hours should
elapse from the last subcutaneous dose and a 4 hour gap should exist until the next
LMWH dose is administered following the catheter removal. The American Society
of Regional Anaesthesia (ASRA) and the European Society of Regional Anaesthesia
(ESRA) guidelines of managing neuroaxial blocks in anticoagulated patients states
283
284
Chapter 7
that single dose LMWH has to be administered at least 2 hours after insertion of
spinal/epidural. Removal of the epidural catheter is only allowed after 10–12 hours
following a prophylactic dose of LMWH, therefore option D is the most appropriate
choice of instructions. Coagulation parameters are unaffected by the either low or
high dose of LMWH and therefore cannot be used to monitor its effect.
Association of Anaesthetists of Great Britain & Ireland (AAGBI), Obstetric Anaesthetists’ Association (OAA),
Regional Anaesthesia UK (RA-UK). A guidance document produced by a Joint Working Party. Regional
Anaesthesia in Patients with Abnormalities in Coagulation. London: AAGBI/RA-UK, 2011.
29. B High blood pressure
Obstructive sleep apnoea (OSA) affects 5-10% of the population, with the highest
incidence occurring in the obese, middle-aged population. Recognising this
risk group is necessary in order to take relevant preventive measures for the
postoperative period. Patients suffering from OSA can be diagnosed from clinical
history, questionnaires and tests such us sleep studies (polysomnography).
The STOP-BANG questionnaire is one such measure. Of the various parameters,
fulfilling 3 or more would place the patient in the high-risk category for suffering
from OSA:
S: Snore - loud snoring
T: Tired - daytime tiredness
O: Observed apnoeas
P: Pressure – Have or being treated for high blood pressure
B: Body mass index (BMI) – BMI >35 kg/m2
A: Age >50 years
N: Neck circumference >40 cm
G: Gender – male
Using polysomnography, OSA can be classified based upon the incidence of
Apnoea/ Hypopnea Index (AHI), which is the number of apnoea or hypopnea
episodes lasting more than 10 secs per hour of sleep:
• Mild OSA – AHI ≥5
• Moderate OSA – AHI ≥15
• Severe OSA – AHI ≥30
Of the options listed, only high blood pressure is a risk factor counted towards the
STOP-BANG questionnaire.
Martinez G, Faber P. Obstructive sleep apnoea. Contin Educ Anaesth Crit Care Pain 2011; 11(1):5-8.
Answers
30. D Levobunolol
Normal intraocular pressure (IOP) is 15-20 mmHg. Glaucoma is considered if the
IOP is greater than 20 mmHg. It contributes towards optic disc cupping and nerve
damage, which eventually leads to visual field defects and blindness if untreated.
Medical management includes topical eye drops. Circulatory absorption of drugs is
rapid through the nasolacrimal duct and the conjunctival capillaries.
Sympathomimetic agents such as 1% adrenaline, 0.1% dipivefrine (an adrenergic
prodrug), 0.2% brimonidine (α2-agonist) and 0.5% apraclonidine (α2-agonist) can be
used. They act by reducing rate of aqueous humor production and increased outflow
via the trabecular meshwork. Side effects include hypertension, arrhythmias and
myocardial ischaemia due to coronary vasospasm.
Adrenoceptor blocking agents including timolol, betaxolol and levobunolol act by
β-adrenoceptor blockage and reducing rate of aqueous humor production. Systemic
absorption of these can cause bradycardia, hypotension, bronchospasm and heart
failure.
This patient has presented with clinical features suggestive of bronchospasm
secondary to β-blocker, the most likely drug of which is levobunolol.
Raw D, Mostafa SM. Drugs and the eye. Contin Educ Anaesth Critical Care Pain 2001; 1(6):161-165.
285
Chapter 8
Mock Paper 8
Questions
1. A 26-year-old man who suffered an isolated blunt force head injury a week ago, is
showing no clinical signs of improvement. He is ventilator dependent and his family
are aware of the situation. You are called to the neurointensive care unit to aid in the
performance of brainstem death testing as there are no consultants available.
Which factor is most likely to make testing inappropriate within the next hour?
A
B
C
D
E
Recent cessation of an infusion of midazolam
Hyperglycaemia
Temperature of 34°C
Administration of atracurium 25 mg 40 minutes ago
Availability of two physicians to perform testing on this shift – an ST7
anaesthetist (yourself ) and an ST7 respiratory physician
2. A 70-year-old man with a history of well-controlled hypertension and smoking, has
a large meningioma resected. It is a 6-hour procedure during which the blood loss
is 600 mL. He coughs briefly on extubation and is transferred to the recovery room
obeying commands. Half an hour later he rapidly drops his GCS to 3/15, becomes
bradycardic and hypoxic. His blood pressure is maintained.
Which of the following is the most likely cause for his deterioration?
A
B
C
D
E
Myocardial infarction
Air embolism
Morphine analgesia
Intracranial haematoma
Hypovolaemia
3. You are anaesthetising a 70 kg patient for coronary artery bypass grafting (CABG).
He suffered a non-ST elevation myocardial infarction (NSTEMI) 10 days ago
but has been becoming increasingly breathless on minimal exertion. Recent
angiography shows an 80% stenosis of the left main coronary artery. Baseline
blood pressure is 130/80 mmHg. Following induction with fentanyl, midazolam
and propofol, the systolic blood pressure drops to 65 mmHg and there is anterior
ST elevation on the ECG. The blood pressure rises to 120/78 after 1.0 mg of
metaraminol. The transoesophageal echo shows worsening anterior hypokinesis.
288
Chapter 8
What is the next most appropriate step?
A
B
C
D
E
Give 500 mL of colloid stat
Give 30,000 units of heparin
Give 1 mg of metaraminol and wait for 2 minutes
Ask the surgeon to insert an intra-aortic balloon pump
Commence milrinone
4. A 45-year-old woman presents for urgent repair of a LeFort III fracture with
involvement of the small bones of the nasal complex following a motor vehicle
accident. Her mandibular molar teeth are loose and she has poor mouth opening
and a clear cervical spine. It is anticipated she will be a difficult intubation and will
require postoperative ventilation.
Which route for airway control is the most appropriate to use in this scenario?
A
B
C
D
E
Nasal intubation
Retromolar intubation
Surgical tracheostomy
Oral intubation via direct laryngoscopy
Submental intubation
5. You are called to assist a junior colleague who has just topped-up an epidural to
enable an emergency Caesarean section for prolonged labour. The block level
was confirmed to be satisfactory. Upon securing the surgical drapes the patient
complained of a strange sensation around her mouth and double vision before
becoming unconscious followed by loss of cardiac output.
What is the most likely diagnosis?
A
B
C
D
E
Concealed haemorrhage
Local anaesthetic (LA) toxicity
Amniotic fluid embolus
Pulmonary embolus
Total spinal block
6. A 54-year-old woman is to undergo an abdominal hysterectomy with lymph node
resection for endometrial adenocarcinoma. She has mild asthma, managed on
inhalers, recently diagnosed diet controlled type II diabetes, and a body mass
index (BMI) of 38. She admits to snoring and daytime sleepiness. Her exercise
tolerance is reasonable.
The most appropriate analgesic plan would include:
A
B
Gabapentin premedication. Simple analgesia and intravenous morphine
intraoperatively with transversus abdominis plane (TAP) blocks at the end of
the procedure. Postoperative PCA fentanyl in the high dependancy unit (HDU)
Lumbar epidural with plain levobupivacaine and simple analgesia. Oral
morphine postoperatively
Questions
C
Simple analgesia and intravenous morphine intraoperatively with TAP blocks
at the end of the procedure. Postoperative PCA morphine in HDU
D Simple analgesia, lumbar epidural PCEA with levobupivacaine/fentanyl
mixture
E Intraoperative Remifentanil target-controlled infusion, asleep spinal at the end
of the procedure, PCA morphine
7. A 27-year-old man is scheduled for surgical exploration and repair of his fractured
mandible after being assaulted the previous night with injuries to the side of
his face. After administration of 100 μg fentanyl, 200 mg propofol and 50 mg
rocuronium, his mouth will not open despite adequate force. He is afebrile with
normal end tidal carbon dioxide levels.
What is the most likely cause of his persistent mouth closure?
A
B
C
D
E
Pain
Masseter spasm
Sub-masseteric abscess
Depressed zygomatic fracture
Anterior dislocation of the mandible
8. 48 hours following a severe traumatic brain injury, a 25-year-old man remains
intubated and ventilated and haemodynamically stable. Sedation was
discontinued 36 hours earlier but his GCS remains 3/15 and he continues to
make no respiratory effort. The critical care team believes the patient has suffered
irreversible traumatic brain injury.
What would be the next step in assessing the suitability of the patient to be an
organ donor?
A
B
C
D
E
Apnoea testing
CT scan of brain to confirm brainstem herniation
Brainstem testing
Cerebral circulation angiogram
Sensory and motor evoked potentials measurement
9. A 66-year-old man with a history of stable angina on exertion presents for revision
of a left total hip replacement, his medications include a statin and low-dose
aspirin. The primary joint has been cemented, and the surgeon is concerned that
the procedure may be ’difficult‘. The patient had haemoglobin of 110 g/L at his preassessment visit. You find a note from the pre-assessment nurse telling you that the
patient is also a Jehovah’s Witness.
The best blood conservation strategy, which is also likely to be acceptable to the
patient would involve:
A
Autologous pre-donation for one month with oral iron supplementation and
recombinant erythropoeitin (EPO). Rescue therapy for severe bleeding with
recombinant factor VII
289
290
Chapter 8
B
Autologous pre-donation for one month with intravenous iron
supplementation. Rescue therapy for bleeding with recombinant factor VII
C Preoperative iron supplementation and EPO. Acute hypervolaemic
haemodilution during the procedure. Rescue therapy for bleeding with
recombinant factor VII
D Preoperative iron supplementation and erythropoietin (EPO). Acute
hypervolaemic haemodilution during the procedure. Rescue therapy for
bleeding with fresh frozen plasma and fibrinogen concentrate
E Preoperative iron supplementation and EPO. Acute normovolaemic
haemodilution, during the procedure. Rescue therapy for bleeding with
recombinant factor VII and platelets
10. A 45-year-old patient requires abdominal surgery to be supplemented by a
regional anaesthetic block.
In which one of the following operations is a unilateral transversus abdominis
plane (TAP) block most reliably able to provide perioperative analgesia?
A
B
C
D
E
Laparoscopic inguinal hernia repair
Open appendicectomy
Paraumbilical hernia repair
Open cholecystectomy
Laparoscopic appendicectomy
11. A 70-year-old man was admitted to your neurosurgical unit following a fall down
flights of stairs. He sustained bilateral subdural haematomas and a C7 fracture. You
are called to secure his airway as his GCS is 9 and he is agitated and confused.
What is the most appropriate method of applying cricoid pressure for the rapid
sequence intubation?
A
B
C
D
E
Remove the collar completely and apply single handed cricoid pressure
Double handed cricoid pressure application without the collar
Keep the collar on and apply single handed cricoid pressure
Do not use cricoid pressure as it worsens laryngoscopy
Awake fiberoptic intubation without cricoid pressure
12. A 55-year-old man is admitted to your intensive care unit following an emergency
laparotomy for faecal peritonitis secondary to a perforated sigmoid diverticulum. He
is paralysed and sedated, intubated and ventilated. His haemodynamic observations
are as follows: heart rate 90 beats per minute sinus rhythm; mean arterial pressure
(MAP) 62 mmHg on 0.36 µg/kg/min of noradrenaline; stroke volume index (SVI)
is 19 mL/m2/beat before, and 20 mL/m2/beat after a 250 mL bolus of Hartmann’s
solution given over 150 seconds; haemoglobin concentration is 84 g/L; arterial blood
lactate is 4.8 mmol/L; central venous oxygen saturation (Scvo2 is 56%; central venous
to arterial carbon dioxide difference is 1.4 kPa; highly sensitive cardiac troponin T
(hs-cTropT) levels are 150 times the upper reference limit.
Given this information the best treatment strategy is:
Questions
A
Increase the rate of the noradrenaline infusion to achieve a MAP of 75–
85 mmHg
B Give a 50 mg bolus of hydrocortisone and repeat 6-hourly
C Give two units of packed red blood cells (pRBC)
D Request an urgent cardiology review as the patient needs an emergency
coronary angiogram and the insertion of an intra-aortic balloon pump
E Commence a titrated dobutamine infusion starting at 5 µg/kg/min
13. A 69-year-old woman with an established history of essential hypertension, type
2 diabetes mellitus and chronic renal impairment (baseline urea 9.8 mmol/L and
creatinine 142 µmol/L), underwent elective, on-pump coronary artery bypass
grafts yesterday. She successfully met all of her enhanced recovery cardiovascular
and respiratory parameters and has consequently been extubated and not on any
vasoactive drugs. Her fluid balance is + 2430 mL since arrival in the intensive care
unit. Her urine output has been averaging 18 mL/hour (actual body weight 92 kg,
ideal body weight 62.5 kg). See Table 8.1 below for this patient’s blood results.
Table 8.1 Blood test results
Parameter
ICU admission (16 hours ago)
Now
Bicarbonate concentration
20 mmol/L
14 mmol/L
Sodium concentration
140 mmol/L
130 mmol/L
Potassium
5.6 mmol/L
6.4 mmol/L
Urea
7.6 mmol/L
17.6 mmol/L
Creatinine
110 µmol/L
182 µmol/L
On the basis of this information, the best renal treatment strategy is:
A
B
C
D
E
Commence a dopamine infusion at 2.5 mg/kg/hour
Give 15 units of short acting insulin in 50 mL of 50% dextrose in 15 minutes
Give 500 mL of 1.23% sodium bicarbonate over 1 hour
Give 20 mg of furosemide intravenously followed immediately by an infusion
at 5 mg/hour
Commence renal replacement therapy
14. A 44-year-old woman presented with a grade 5 subarachnoid hemorrhage 7 days
ago. Brainstem death testing conducted in the appropriate manner has revealed
intact gag and deep tracheal stimulation reflexes. The multi-disciplinary team
agrees that this patient has suffered a non-survivable brain injury.
What is the next most appropriate course of action?
A
B
Monitor for deterioration and conduct brain stem testing at a later date
Inform the family the results of the testing and approach the subject of heartbeating organ donation
291
292
Chapter 8
C
Escalate life support therapy to ensure end-organ perfusion is maintained in
case organ donation is accepted
D Contact the transplant coordinator
E Discuss the case with the coroner
15. A 42-year-old morbidly obese woman is admitted to the high dependency unit
(HDU) after an elective laparoscopic sleeve gastrectomy. Her background includes
type 2 diabetes, a previous deep vein thrombosis and obstructive sleep apnoea.
The patient had a grade 3 laryngoscopy view at intubation and had an internal
jugular central line and right radial arterial line inserted. Surgery was uneventful
but 2 hours after admission the patient becomes agitated and breathless and
an arterial blood gas demonstrates hypercapnic respiratory failure. A trial of
non-invasive ventilation (NIV) was not tolerated and made her more agitated,
tachycardic and hypoxic.
What is the next immediate step?
A
B
C
D
E
Intubate and ventilate
Examine the respiratory system
Request an urgent chest radiograph
Request an urgent CT pulmonary angiogram
Organise an urgent transthoracic echo
16. A 56-year-old woman with a background of chronic kidney disease presents
with a pulmonary embolism. She was admitted to the high dependency unit and
commenced on an unfractionated heparin infusion for anticoagulation. Five
days later she developed hypoxic respiratory failure and became cardiovascularly
unstable. A repeat CT pulmonary angiogram demonstrated an extension of her
pulmonary embolism.
What is the most useful investigation?
A
B
C
D
E
Thrombophilia screen
Full blood count
Transthoracic echocardiogram
Lower limb vein ultrasound
Serotonin release assay
17. A 20-year-old woman who is 37/40 pregnant with twins presents for an elective
Caesarean section. She is normally fit and well and a spinal anaesthetic is
performed. Immediately after performing the spinal she is placed in the supine
position with a left lateral tilt and begins to complain of weak arms and difficulty
in breathing. Her blood pressure drops to 80/50 mmHg, heart rate 43 beats per min
and she loses consciousness. Her pupils are dilated and she has become apnoeic.
Which of the following is the most likely diagnosis?
A
B
Anxiety
Hypoglycaemia
Questions
C Total spinal
D High spinal-induced cardiovascular collapse
E Aortocaval compression
18. The obstetric team wants to deliver a term baby by emergency Caesarean section
for foetal distress. A spinal anaesthetic was quickly established, and the baby was
delivered within minutes. However, the newborn appears floppy and pale. The
midwife asked for help with resuscitation the newborn. A neonatal crash call has
been put out, but the neonatal team has not yet attended. The mother is stable, and
you leave her under the care of a second anaesthetist to assist the midwife.
The first step in the resuscitation of a newborn is:
A
B
Open the airway by maintaining the head in a neutral position
Establish the Apgar score by assessing the newborn’s appearance, pulse,
grimace, activity and respiration
C Deliver five inflation breaths at 30 cmH2O airway pressure for a term baby
D Dry and stimulate the newborn with a towel, replace the wet towel and cover
the baby
E Assess the heart rate by auscultating over the precordium
19. A 3-year-old 16 kg child with sickle cell disease is scheduled for adenotonsillectomy. He is the second case on the ENT list, but the first case is taking
much longer than anticipated. He had dinner at 7 pm the previous night, and a
drink at 9 pm before going to bed. He has had nothing to eat or drink since. It is now
10 am, and the child is unlikely to be anaesthetised until 1 pm. The nurse on the
ward informs you that the child is getting upset because he is hungry and thirsty.
The best course of action is:
A
B
Postpone the case for another day, and let the child eat and drink
Let the child eat and drink until 10 am, with a plan to anaesthetise the child at
4 pm
C Cancel the case, and re-consider the indication for adenotonsillectomy given
the increased risk of anaesthesia and surgery in sickle cell disease
D Start an intravenous infusion of warmed isotonic crystalloid
E Continue to fast the child, and aim to do the child as soon as possible
20. An 11-year-old boy was involved in a road traffic accident. He was brought
in to the emergency department of a local district general hospital, where he
was tachypnoeic, tachycardic, and responsive only to painful stimuli. He was
intubated and ventilated and given 40 mL/kg of crystalloid intravenously. A CT
head was performed after the child was stabilised, and showed an acute subdural
haematoma and signs of raised intracranial pressure. After discussion with
the nearest neurosurgical unit, the decision was made to transfer the child for
urgent haematoma evacuation. The nearest neurosurgical unit is 1 hour away by
ambulance, but the regional paediatric transport team will not be available for at
least another 3 hours.
293
294
Chapter 8
The best option for the transfer of this patient is:
A
Keep the child in the emergency department until the regional paediatric
transport team is available to transfer the child
B Move the child to theatre while waiting for the regional paediatric transport
team to be available to transfer the child
C Move the child to the intensive care unit while waiting for the regional
paediatric transport team to transfer the child
D Use a local non-specialist team to transfer the child immediately to the nearest
neurosurgical unit
E Find an alternative specialist paediatric transport team to transfer the child to
the nearest neurosurgical unit
21. A 39/40 week primiparous patient presents in labour. She is unable to have an
epidural sited due to florid eczema over her back. Other analgesic options have failed,
you have discussed and agreed on a remifentanil patient controlled analgesia (PCA).
With regards to starting the PCA which of the following options is least correct?
A
B
C
D
E
Patients require 1:1 midwife care
They require routine oxygen delivery
It is safe to use within 4 hours of other parenteral opiates
Requires a dedicated cannula
Patients require CTG monitoring
22. A 70-year-old woman presents to the pain clinic with a 4-month history of
neuropathic pain in the distribution of the left T10 dermatome. This was preceded
by skin lesions in the same distribution. She is taking regular paracetamol and has
been taking moclobemide for many years for depression. She also has a pacemaker
for sick sinus syndrome.
What is the most appropriate first line treatment for her pain?
A
B
C
D
E
Transcutaneous electrical nerve stimulation (TENS)
Ten days of acyclovir and steroids
Amitriptyline
Pregabalin
Thoracic sympathetic block
23. A 40-year-old woman with chronic pain from degenerative lumbar spine disease
develops increasing pain in her left leg with weakness and altered sensation.
Which of these statements is the most appropriate course of action?
A
B
C
D
E
An urgent MRI is indicated to assess for nerve dysfunction
Initial treatment is conservative with simple analgesics
Early surgery should be considered to prevent further disease progression
Urgent surgical referral is needed if pain spreads to both legs
Lumbar spine radiography is useful if MRI not available
Questions
24. A 48-year-old man presents for an elective open rotator cuff repair. He is fit and
well and has no known allergies.
What would be the most appropriate perioperative analgesic plan?
A
Interscalene block with 20 mL 0.5% levobupivacaine and regular paracetamol
and ibuprofen
B Suprascapular block with 20 mL 0.5% levobupivacaine and regular
paracetamol and ibuprofen
C Axillary brachial plexus block with 20 mL 0.5% levobupivacaine and regular
paracetamol and ibuprofen
D Regular paracetamol, ibuprofen and morphine patient controlled analgesia
(PCA)
E Intra-articular injection with 10 mg morphine and 20 mL 0.5% levobupivacaine by
surgeons at the end of surgery combined with regular paracetamol and ibuprofen
25. A 26-year-old woman developed a headache 36 hours following a suspected dural
puncture with a 16G Tuohy needle whilst having an epidural for labour analgesia.
She had an epidural blood patch that was effective for 24 hours, but the headache
has now returned. Neurological examination is normal and she is afebrile.
What step would most likely be beneficial in the management of this ongoing
headache?
A
B
C
D
E
Sumatriptan
400 mg caffeine intravenously twice daily
Bed rest
Intravenous fluids
Second blood patch
26. A 73-year-old man is attending the day surgery unit for a cataract operation. He
has a past medical history of atrial fibrillation, well-controlled chronic obstructive
pulmonary disease (COPD) and type II diabetes mellitus. He has had retinal
detachment surgery on the same eye previously and would prefer to have the
procedure performed under regional anaesthesia.
Which of the following is the most significant risk factor for this patient having a
sub-Tenon’s block?
A
B
C
D
E
INR of 2.0
COPD
Previous retinal detachment surgery
Age > 70
Blood glucose of 8 mmol/L
27. The recovery nurses are concerned about a 74-year-old woman following a right
carotid endarterectomy under superficial cervical plexus block. They noticed
the right pupil is smaller than the left. The patient is asymptomatic but you also
observe ptosis of the right eye. The anaesthetic chart shows that the anaesthetist
used 20 mL of 0.25% levobupivacaine for the block.
295
296
Chapter 8
What is the explanation you provide to the concerned patient and nurses?
A
B
This is a surgical complication; need to contact the surgical team
This is a regional anaesthetic related complication, reassure and continue to
observe the patient in recovery for resolution
C The patient had a stroke, alert the surgical team please
D Administer intralipid 20%, to the patient
E This is a congenital abnormality
28. A 65-year-old man is listed for an elective total knee replacement.
What would be the most appropriate nerve block to manage his perioperative
analgesia?
A
B
C
D
E
Femoral nerve block
3-in-1 block
Fascia iliaca block
Adductor canal block
Sciatic and femoral nerve block
29. A 68-year-old lady has been admitted to hospital with suspected infective
endocarditis and has positive blood cultures for Staphylococcus aureus.
Which of the following criterion needs to be met in order to reach a conclusive
diagnosis of infective endocarditis as per the modified Duke's criteria?
A
B
C
D
E
Temperature >38°C
A dilated right ventricle on echocardiogram
Jayneway lesions
Intracardiac mass on echocardiogram
Pericardial effusion on echocardiogram
30. A 73-year-old man is undergoing a laparotomy for perforative peritonitis. He has
a history of ischaemic heart disease and asthma. Intraoperative cardiac output
monitoring is performed using an oesophageal Doppler probe. The readings of the
Doppler are as follows:
• Stroke volume index (SVI) - 110 mL/m2 (35-65 normal range)
• Flow time corrected (FTc) - 490 ms (330-360 normal range)
• Heart rate – 106 beats per minute
• Non-invasive blood pressure - 80/56 mmHg
Following fluid bolus of 200 mL of colloid his SVI changes to 115mL/m2 and FTc
remains 490 ms with minimal change in vital parameters.
Using the current data, which of the following options is the next most appropriate
step in the management of this patient:
A
B
C
D
E
Further 200 mL colloid bolus
Dobutamine infusion to titrate blood pressure
Noradrenaline infusion to titrate blood pressure
Observe for another twenty minutes and repeat measurements
500 mL crystalloid bolus
Answers
Answers
1.E Availability of two physicians to perform testing on
this shift – an ST7 anaesthetist (yourself) and an ST7
respiratory physician
Brainstem death is confirmed when testing demonstrates irreversible loss of
brainstem function in the event of brain damage with known, untreatable aetiology.
To ascertain the irreversibility of the patient’s state, certain criteria must be met as a
pre-condition to testing.
Pre-testing criteria
• Confirmation of the absence of medications at a plasma level significant enough
to cause central nervous system depression. Plasma levels may therefore be
requested in anticipation – those of midazolam should be < 1.0 µg/L
• Resolution of all primary circulatory, metabolic and endocrine disturbances. Blood
glucose is accepted between 3–20 mmol/L
• Temperature > 34.0 °C. The patient may require active warming
• Ventilator dependence without residual muscle relaxation. Effects of recent
administration can be assessed with a nerve stimulator +/- reversed
Providing the above conditions have been met, brainstem testing may be carried
out. For this, 2 physicians are required. They should both have at least 5 years
registration with the General Medical Council and one must be a consultant. Neither
physician should be a member of an organ donation/transplant team.
There is no consultant available to assist with brainstem testing during this shift.
Even if all the other factors where managed to meet pre-testing criteria within
the next hour, including bringing the temperature to above 34°C, reversal of
neuromuscular blockade, corrrection of hyperglycaemia and a reduction in the
plasma concentrations of midazolam, the tests would remain invalid.
Allman K, Wilson I. Oxford Handbook of Anaesthesia, 2nd edn. Oxford: Oxford University Press, 2006.
Academy of Medical Royal Colleges. A Code of Practice for the Diagnosis and Confirmation of Death.
London: Academy of Medical Royal Colleges, 2010.
The NHS Institute for Innovation and Improvement. Neurological Determination of Death. London: The
NHS Institute for Innovation and Improvement, 2010.
2. D Intracranial haematoma
Meningiomas are more commonly seen in women than men and account for 15% of
central nervous system (CNS) tumours. They arise from cells in the arachnoid mater
and often grow very slowly to a great size before symptomatic presentation. 90% are
benign, although even benign meningiomas can invade locally into the dura and
neighbouring bone. Fewer than 10% are multiple but they may be seen in patients
with neurofibromatosis and other genetic syndromes. Meningiomas can be highly
vascular and therefore confer an elevated risk of significant intraoperative bleeding.
Postoperative bleeding usually occurs within hours of surgery and subsequently,
297
298
Chapter 8
often reveals itself in recovery. Factors that may contribute to this event include size
and location of the tumour, coughing on extubation, postoperative vomiting and
inadequate pain relief leading to surges in hypertension and therefore intracranial
pressure.
Although postoperative myocardial infarction is possible with the co-morbidities,
acute onset bradycardia and reduced Glasgow coma score (GCS) makes this
diagnosis less likely. Venous air embolism in intracranial surgery is a recognised
complication due to the positioning of patients in the head up position. The most
common presentation is a reduction in end-tidal CO2 followed by cardiovascular
embarrassment. The timing of a postoperative course of deterioration following
a stable intraoperative course makes venous air embolism less likely as it often
presents acutely intraoperatively. A morphine overdosing may also present similarly
but the rapidity of the deterioration as well as the timing of it makes this less
likely. Hypovolaemia would be expected to present with the telltale signs of high
intraoperative blood loos, hypotension and tachycardia, which is not apparent in
this case. The rapidity of his neurological demise following this particular procedure
makes an intracranial haematoma therefore the most likely cause.
Nathanson M, Moppett I, Wiles M. Neuroanaesthesia. Oxford Specialist Handbooks in Anaesthesia. 1st Ed.
Oxford: Oxford University Press, 2011.
3. B Give 30,000 units of heparin
This is a high-risk cardiac patient given his symptoms, recent non-ST elevation
myocardial infarction (NSTEMI) and the extent of left main coronary disease. Based
on the information given, it appears he is suffering from acute myocardial ischaemia,
which is persisting (as evidenced by worsening wall motion abnormalities on
transoesophageal echo (TOE)) despite restoration of perfusion pressures. Although
the dysfunction may be due to the negative inotropic action of the induction agents,
emergency institution of cardiopulmonary bypass may be indicated, therefore early
administration of heparin with the aim of fully anticoagulating the patient prior to
exposure to the bypass circuit is the best option here. The usual dose given is 300–
400 IU/kg aiming for an activated clotting time (ACT) of over 480 seconds.
Further metaraminol may increase myocardial oxygen consumption by increasing
afterload. An inotrope such as milrinone would most likely be used following
revascularisation rather than before. Fluid administration may be warranted when
guided by real time TOE, but is not the best initial option here. Although insertion
of an intra-aortic balloon pump (IABP) may be beneficial, especially when weaning
from cardiopulmonary bypass (CPB) in this patient, it is unlikely that one can be
placed without slowing institution of CPB (unless there are a plethora of surgeons or
cardiologists available).
Machin D, Allsager C. Principles of cardiopulmonary bypass. Contin Educ Anaesth Crit Care Pain 2006;
5;176–181.
Wasnick J. Cardiac Anesthesia and Transesophageal Echocardiography. New York: McGraw-Hill, 2011.
Answers
4. C Surgical tracheostomy
Maxillofacial trauma presents numerous airway challenges to the anaesthetist and
a clear anatomical understanding of the types of fracture and corrective surgical
approaches is needed to select the most appropriate airway.
The Le Fort classification is used to describe different patterns of mid-facial injury
based on common fracture planes along lines of weakness (Figure 8.1). A Le Fort
I fracture traverses the maxilla horizontally above the apices of the maxillary teeth
and allows the upper jaw to move in relation to the nose. If the fracture line diverges
superiorly, to create a pyramidal segment involving of the medial orbit as well as the
nose, this becomes a Le Fort II fracture. This pyramidal segment can move as a block
in relation to the frontal bone and zygoma. A Le Fort III fracture denotes a complete
separation of the mid-face from the skull base and involves fractures through the
zygomatico frontal suture, floor of the orbit and the nasofrontal suture.
Figure 8.1 Diagramatic
representation of Le Fort
fractures I, II and III.
Le Fort I
Le Fort II
Le Fort III
In an acute emergency, oral intubation is the route of choice whilst keeping cervical
movements to a minimum (if this is yet to be cleared). However, it is not the most
appropriate option in this scenario since temporary intraoperative dental occlusion
will be required to aid surgical correction. An oral endotracheal tube will prevent
this. This is also a predicted difficult intubation, so performing an oral intubation
using direct laryngoscopy would not be appropriate.
In the above case, there is damage to the nasal complex of bones which increases
the complexity since a nasotracheal tube will also interfere with their surgical
correction. In scenarios where surgical access to the nose as well as intraoperative
dental occlusion tests are needed, anaesthetists have historically switched from
nasal to oral intubation intraoperatively. However, this is not ideal since there is a risk
of losing a previously secure airway.
To accommodate nasal surgical access and temporary intraoperative dental
occlusion, the airway can be secured by retromolar and submental intubation or
tracheostomy. The retromolar space is the gap between the last mandibular molar
tooth and the anterior edge of the ascending ramus of the mandible. This space
can accommodate an orotracheal tube and also allow dental occlusion tests to
be performed without interference. The orotracheal tube can be guided into the
299
300
Chapter 8
space following conventional oral intubation or pass through the space en route
to the trachea with the aid of a Bonfils or flexible fibre-optic scope in difficult
airways. The tube is usually held in place by ties to the adjacent tooth which in the
above scenario is loose. It is also not ideal for patients expected to need prolonged
postoperative ventilation.
Submental intubation involves performing conventional oral intubation then
passing the endotracheal tube through a surgical incision in the floor of the mouth.
This keeps the mouth and nose free for the surgical access and avoids the need
to perform a tracheostomy. Compared to a tracheostomy, it also leaves a more
aesthetic scar and carries less serious complications. It is not the ideal airway for
prolonged postoperative ventilation however.
An awake, formal tracheostomy prior to surgery is the most appropriate airway for
the above scenario since surgical field interfere is avoided and a safe, stable airway
for postoperative ventilation is provided.
Curran J. Anaesthesia for facial trauma. Anaesth Intensive Care Med 2011; 12(8):354–359.
Kellman R, Losquadro W. Comprehensive airway management of patients with maxillofacial trauma.
Craniomaxillofac Trauma Reconstr 2008; 1(1):39–47.
Jain G, Dhama S, Singh D. Role of retromolar intubation for airway management in trauma. Adv Trop Med
Pub Health Int 2011; 1(1):21–32.
5. B Local anaesthetic (LA) toxicity
The rapid topping up of an epidural, following its prolonged use, is encumbered
with the significant risk of reaching the threshold of local anaesthetic (LA) toxicity.
Presentation can occur almost immediately up to an hour after LA administration.
It classically begins with signs and symptoms of central nervous system (CNS)
excitability followed by CNS depression and ultimately, cardiovascular instability.
A wide range of arrhythmias may ensue, resulting in cardiac arrest. The other
diagnoses should all be considered but, in light of her anaesthetic history during
labour and systematic progression of signs and symptoms, LA toxicity is most likely
and it should therefore be treated as such.
The Association of Anaesthetists of Great Britain & Ireland (AAGBI). Management of severe local
anaesthetic toxicity. London: AAFGI, 2010.
6.D Simple analgesia, lumbar epidural PCEA with
levobupivacaine/fentanyl mixture
Gynaecological surgery presents a number of challenges, and the added aspects
of gynaecological oncology may provide further problems to the anaesthetist,
especially in the era of more radical surgery for pelvic disease.
Good quality analgesia tailored to the patient is of paramount importance. Chronic
pain after abdominal hysterectomy may occur in up to 30% of patients, and poor
perioperative pain control represents a modifiable risk factor. Interestingly, much of
the pain seems to relate to the visceral trauma of surgery, as there is no difference
in rates of chronic pain when comparing open and laparoscopic approaches to
hysterectomy surgery.
Answers
Most recommendations for analgesia in hysterectomy involve categorising a
patient’s risk of postoperative pain as high or low and then treating accordingly. Risk
factors for postoperative pain are:
•
•
•
•
Chronic pain conditions and ambulatory opioid use
Illicit intravenous drug abuse
Previous chemo/radiotherapy
Surgery with extensive tissue trauma
In a web review of procedure specific pain guidance (PROSPECT), recommendations
in abdominal hysterectomy are for epidural analgesia for high risk patients, whereas in
low risk, patients wound infiltration and opioids are deemed sufficient. Oral gabapentin
is used by some for high risk patients, but side effects include sedation and dizziness,
and thus this should not be given with other sedating agents. It is often started preemptively as a premedicant before induction. Ketamine infusions, usually in combination
with PCA opioids have also been used with success in high risk chronic pain patients.
In ovarian adenocarcinoma, patients with epidural anaesthesia have been shown
to have improved rates of survival at 3 and 5 years. This is postulated to relate to
preservation of immune function by avoidance of anaesthetic and analgesic drugs
allowing for greater immunosurveillance and tumour cell clearance at the time of
surgery.
The key points with this patient are that she is obese, and suffers with respiratory
disease. Of significance, there is some evidence that she may suffer with
obstructive sleep apnoea (OSA). Given the presence of OSA, the ideal postoperative
environment is the high dependency unit (HDU) especially if patient controlled
opiates are to be used. Gabapentin should be avoided. Given the respiratory picture,
removing or minimising the need for systemic opioids would be beneficial, therefore
an epidural is the best choice, in the first instance a low dose mixture should be
tried, and other opiates avoided. A multimodal approach to managing this patient's
postoperative analgesia is required, therefore simple analgesia in combination
with patient controlled epidural analgesia (PCEA) with a levobupivacaine/fentanyl
mixture is the ideal choice of analgesia for this patient.
Morosan M, Popham P. Anaesthesia for gynaecological oncological surgery. Contin Educ Anaesth Crit Care
Pain 2014; 14(2):63–68.
7. D Depressed zygomatic fracture
Airway management decisions for mandibular fractures are difficult due to the
numerous and often co-existing causes of the associated trismus. Trismus describes
the inability to open the mouth and can occur as a result of pain, muscle spasm,
swelling or any mechanical obstruction. During the preoperative assessment, pain
associated with mouth opening may mask other underlying contributors to trismus
and also limit the airway examination. It is therefore important to communicate with
the surgeons if they have any concerns regarding the mechanics of mouth opening
before induction.
With adequate depth of anaesthesia and neuromuscular blockade (as in the case
above), it is expected that trismus secondary to purely pain will be reversed. In cases
301
302
Chapter 8
where it is anticipated that mouth opening will be difficult despite anaesthesia, an
awake fibre-optic intubation is warranted.
The masseter muscle is a powerful muscle of mastication which arises from the
zygomatic arch and inserts on the ramus of the mandible. Masseter spasm will result
in a clenched jaw, and can be an early presentation of malignant hyperpyrexia.
The normal carbon dioxide levels and temperature in the above case makes this
diagnosis unlikely. Furthermore, although rocuronium has on very rare occasions
been associated with malignant hyperpyrexia, the symptoms tend to be delayed.
Increased muscle rigidity affecting mouth opening can also be seen with propofol
and fentanyl, although this would be expected to resolve following paralysis.
Failure of the mouth to open following anaesthesia and paralysis can be caused by
a mechanical obstruction restricting the normal movement of the mandible across
the temporomandibular joint. This can occur as a complication of a submasseteric
abscess where pus accumulates between the ramus of the mandible and the
masseter muscle. These normally arise from molar infections, and when seen in
the context of trauma, usually occur as late presentations of infected fractures. The
absence of fever and the early presentation of the mandibular fracture in the above
scenario make this diagnosis unlikely.
Dislocation of the temporomandibular joint (Figure 8.2) will also affect opening
and closing of the mouth. The joint is formed by the articulation of the mandibular
condyle with the mandibular fossa and the articular eminence of the temporal
bone. An anterior dislocation occurs when the condyle travels along the articular
eminence and becomes lodged anterior to it. This is the most common type of
mandibular dislocation and can occur as a result of trauma, extreme mouth opening
or dystonic reactions. Due to the associated locked position of the mandible, this
type of dislocation results in a fixed open mouth with an inability to close. This does
not fit with the clinical picture.
The most likely cause of the fixed mouth closure in the above case is a co-existing
depressed zygomatic fracture which impinges on the coronoid process of the
Figure 8.2 The temperomandibular joint.
Temporomandibular joint
Anterior
Zygomatic arch
Mandibular fossa
External acoustic
meatus
Mastoid process
Mandibular condyle
Articular eminence
Coronoid process
Masseter muscle
Answers
mandible. This causes a mechanical obstruction preventing mandibular movement
and therefore mouth opening which will not resolve after anaesthesia or paralysis.
Zygomatic arch fractures usually occur after blunt trauma to the side of the face and
can be clinically difficult to diagnose. Signs include a dimple palpable on the arch
which can be subtle and masked by swelling, and a limited mouth opening.
Wetsch W, Böttiger B, Padosch S. Masseter spasm after induction of general anaesthesia using propofol
and remifentanil. Eur J Anaesthesiol 2010; 27(12):1069–70.
Ceallaigh P, Ekanaykee K, Beirne C. Diagnosis and management of common maxillofacial injuries in the
emergency department. Part 3: orbitozygomatic complex and zygomatic arch fractures. Emerg Med J
2007; 24: 120–22.
Shaw I, Kumar C, Dodds C. Oxford Textbook of Anaesthesia for Oral and Maxillofacial Surgery. Oxford:
Oxford University Press, 2010.
8. C Brainstem testing
Death is defined as an irreversible loss of consciousness and an irreversible loss of
capacity to breath; severe traumatic brain injury is the commonest cause of death
in young adults. In order to satisfy the criteria for organ donation it is essential to
demonstrate death by neurological criteria:
• The patient must be deeply unconscious, apnoeic and mechanically ventilated
• There is no doubt that the patient has suffered irreversible brain damage of a
known aetiology
There must be confidence that the effect of depressant drugs such as sedatives has
been excluded and there are no reversible causes of apnoea.
This patient fulfils the criteria for death by neurological criteria, and thus the next
step is a formal assessment to confirm brainstem death by examining cranial nerves
II – XI, followed by apnoea testing. Once brainstem death has been confirmed by
performing the examination twice by separate clinicians, the patient’s suitability for
consideration of organ donation is confirmed.
As mentioned, apnoea testing is performed after brainstem testing. Brain imaging
and cerebral angiograms are occasionally employed where there is doubt about the
aetiology of brain damage, but are not essential tests. Sensory evoked potentials
(SEPs) or motor evoked potentials (MEPs) are used to monitor cerebral pathway
integrity during spinal and neurosurgery and are not used in confirmation of
brainstem death.
John Oram, Paul Murphy. Diagnosis of death. Contin Educ Anaesth Crit Care Pain 2011; 11(3): 77–81.
9.C Preoperative iron supplementation and EPO. Acute
hypervolaemic haemodilution during the procedure.
Rescue therapy for bleeding with recombinant factor VII
The Jehovah’s Witnesses (JW) have around 150,000 members of their movement
in the UK, and are of particular interest due to their stance on transfusion of blood
and its products. Their doctrine states that consumption of blood is forbidden, and
also that any blood removed from the body is unclean. This essentially means that
303
304
Chapter 8
the transfusion of blood or of major blood products is not accepted, and any forms
of blood removal and storage are generally not permitted. Therefore a number of
perioperative management plans must be instituted in this group of patients to
reduce the risks of anaemic morbidity and mortality.
Preoperative
The aim should be to assess and optimise the haemoglobin concentration (Hb).
Thus, anaemia should be investigated and treated vigorously, and any medications
which interfere with clotting, such as antiplatelets and non-steroidal antiinflammatory drugs (NSAIDs), should be discontinued if possible. Recombinant
erythropoietin (EPO) is useful in Jehovah’s witnesses and patients with anaemia who
are also unable to accept transfusion. EPO should be given with iron, and if deficient
or malnourished, B12 and folic acid, to prevent iron deficiency. Some regard
intravenous iron as superior when used with EPO. If time allows, allogenic donation
of blood could be considered, here a patient donates their own red cells for several
weeks prior to surgery. This reduces the risks of infection and blood incompatibility,
but will often be undertaken with EPO/ iron to stimulate regeneration and avoid
anaemia. Unfortunately, as this involves storage of blood this is not often acceptable
to Jehovah’s Witness patients.
Perioperative
It is important to remember that there are various techniques available other than
just drug treatments and cell salvage. Surgically, large procedures can be staged
and use of laser diathermy and haemostatic gels and glues may reduce blood
loss. From an anaesthetic technique viewpoint, a good principle to follow is to
avoid anything which increases venous pressure and thus blood loss, such as high
PEEP/intrathoracic pressures or hypercapnia. Lowering systemic pressures, using
deliberate hypotension can reduce blood loss, but this is offset by the risk to the
patient’s physiological status. Similarly, regional techniques have been shown to
reduce operative losses, but with neuraxial techniques, the risk of massive blood
loss and subsequent coagulopathy and propensity to form an epidural haematoma
has to be considered. General measures such as warming are mandatory to avoid
coagulopathy.
Haemodilution
Acute normovolaemic haemodilution is the perioperative removal of whole
blood, prior to the stage of surgery involving haemorrhage. This is replaced with
crystalloid or colloid, to maintain normovolaemic status, and thus when bleeding
does occur, the actual number of red cells lost per unit volume is lower. There is
also the attractive option of returning whole blood with a normal composition of
clotting factors and platelets at the end of the procedure to assist with haemostasis.
Again, due to the removal and storage considerations, this is often unacceptable
to Jehovah’s Witness patients. Acute hypervolaemic haemodilution is the
dilution of the circulating blood as above, but without removal and storage This
Answers
technique is acceptable, clearly a balance has to be achieved between dilution for
haemodynamics and reducing red cell loss, and avoiding coagulopathy. A reduction
target in packed cell volume (PCV) of 30% was well tolerated in a study of Jehovah’s
Witness patients.
Cell salvage
Widely accepted by Jehovah’s Witness patients, this involves the centrifugal
separation, washing and re-suspension of red cells for transfusion. Importantly, the
circuit should remain in continuity with the patient to avoid the objections over
removal and storage. The washing stage produces red cells and is not designed
to recover platelets or clotting factors. There are several cautions to the use of
the cell saver, and these usually relate to the re-transfusion of undesirable agents
e.g. bacteria or tumour cells. Thus, use in sepsis, tumour beds or direct suction of
amniotic fluid is avoided.
Drugs/blood fractions/recombinant factors
Antifibrinolytics such as tranexamic acid are useful and acceptable to Jehovah’s
Witness patients. Fractionated components of blood such as fresh frozen plasma
(FFP), are usually not acceptable, although this is not universally the case. However,
the acceptance of recombinant factors is widespread such as with the established
use of recombinant Factor VII (NovoSeven). This is likely also the case with other
recombinant protein factors, but not certain with all newer compounds such
as fibrinogen concentrate. Indeed, the only way to be sure, is to ask the patient
explicitly about all eventualities, including their views on transfusion if all else fails
and they are close to death. This should be witnessed independently, and not by
family or Jehovah’s Witness advocates. Some Trusts now have useful and extensive
tick-box consent forms listing all agents especially for those with objections to
conventional allogenic transfusion.
The most important principle in clinical practice, also relevant in the examination
situation, is the individual nature of the patient’s decision. The patient has the choice
over what they are willing to accept, and this can vary in many cases, especially in
the grey area of fractionated products/recombinant agents. The discussion must
obviously take place in advance, and should be open and frank about the risks
involved including death or prolonged intensive care admission. Ideally, discussions
should take place in private, as patients may express different views in front of
relatives/other community members.
The first answer stems, A and B feature pre-donation, which is not an acceptable
practice for Jehovah’s Witness patients. D and E list rescue strategies involving blood
fractions not normally acceptable, but as aforementioned this does vary. Stem E also
features intraoperative normovolaemic dilution, which may also not be acceptable
as it involves blood storage. C remains as the combination of therapies most likely to
be found acceptable by Jehovah’s Witness patients.
Milligan L J, Bellamy M C. Anaesthesia and Critical Care of Jehovah’s Witnesses. Contin Educ Anaesth Crit
Care Pain 2004;4(2): 35–39.
305
306
Chapter 8
10. B Open appendicectomy
The transversus abdominis plane (TAP) block can provide good perioperative
analgesia when used for the appropriate operation. Its use can decrease opioid
consumption allowing patients to breath comfortably and speed mobilisation and
early discharge.
Innervation of the abdominal wall derives from the anterior rami of the lower six
thoracic nerves and the first lumbar nerve (T7-L1).
These nerves enter the transversus abdominis facial plane between the internal
oblique and transversus abdominis muscles.
The TAP block is essentially injecting a large volume of local anaesthetic (LA) in the
transversus abdominis plane targeting the T7 to L1 nerves. This block will provides
adequate analgesia for the abdominal wall but not for the abdominal viscera.
Although the early studies were able show blocks extending from T7 to L1, other
and more recent studies have unable to demonstrate a spread higher than T10.
Therefore, TAP blocks are currently recommended for infraumbilical surgery.
The injection can be done unilaterally or bilaterally depending on the type of the
surgery.
Unilateral block: Open appendicectomy and hernia repair below the umbilicus.
Bilateral block: abdominal hysterectomy, radical prostatectomy, Caesarean section,
midline incision and laparoscopic operations.
The addition of subcostal TAP block can achieve a higher block up to T7 and can
successfully be used with posterior TAP block for supraumbilical procedures such as
cholecystectomies.
In the above question, a right-sided TAP block can provide adequate analgesia for
open appendicectomy procedures. The other options require either bilateral TAP
block or an additional sub-costal block to achieve reliable analgesia.
The TAP block can be performed either by using ultrasound or a landmark technique.
The landmark technique, which was originally described by McDonnell et al, access
to the transversus abdominis plane is achieved through the triangle of Petit. The iliac
crest bound this triangular area inferiorly, anteriorly by the external oblique muscle
and posteriorly by the latissimus dorsi muscle (see Figure 8.3). After passing through
the skin, the needle should be advanced until two pops are felt, at which point
the needle lies in the transversus abdominis plane, immediately superficial to the
transversus abdominis muscle (see figure 8.3). A minimum of 20 mL LA is injected in
each side after aspiration.
In the ultrasound (US) technique, a linear high frequency probe is placed
transversely in the mid-axillary line between the iliac crest and the 12th rib.
The muscle layers and the transversus abdominis plane can easily be identified in this
area. A short bevel 100 mm needle is advanced with an in-plane approach until reaches
this plane, when 20 mL of LA is injected once again superficial to the transversus
Answers
Figure 8.3 Location of the Triangle of Petit for a TAP
block.
External
oblique
Latissimus
dorsi
Iliac crest
Triangle of
Petit
abdominis muscle. The LA spread in the plane will form an elliptical hypoechoic shape
between the transversus abdominis and the internal oblique muscles.
McDonnell JG, O’Donnell B, Curley G, et al. The analgesic effect of transversus abdominis plane block after
abdominal surgery. Anaesth Analg 2007; 104(1):193–197.
Tran TMN, Ivanusic JJ, Hebbard P, Barrington MJ. Determination of spread of injectate after ultrasound
guided transversus abdominis plane block: A cadaveric study. Br J Anaesth 2009; 102(1):123–127.
11. B Double handed cricoid pressure application without
the collar
The use of cricoid pressure for rapid sequence induction (RSI) aims to prevent
regurgitation of gastric content, although the true aims of an RSI are to rapidly and
safely secure a definitive airway. The utility and necessity of cricoid pressure has a
very questionable evidence base currently, with many practitioners doing away with
cricoid pressure completely as it is known to distort the view at direct laryngoscopy.
The pragmatic approach would be to utilise cricoid pressure carefully and advocate
early release if laryngoscopic views are worsened by it.
Although the debate rages on, and is likely to do so for some time, the question
asked here is how to apply cricoid pressure assuming it will be used as part of your
standard RSI technique for a patient with an unstable cervical spine, therefore not
applying cricoid pressure at all is an incorrect answer. An awake fibreoptic intubation
is inappropriate in a patient with a reduced GCS and agitation, thus is best avoided.
The aims here should be to ensure cervical spine stability and control without
sacrificing a safe RSI technique. Therefore removing the collar and having an
assistant provide manual in-line stabilisation (MILS) whilst another providing cricoid
pressure is important. Single-handed cricoid pressure is suitable should the posterior
component of a cervical collar be left in situ as this has been demonstrated to
produce minimal vertebral movement. If the collar is removed completely, singlehanded cricoid pressure leaves the patient at risk of vertebral instability. However, the
safest way to apply cricoid pressure would be with a bimanual approach with collar
removed completely and MILS. This is thought to provide better laryngoscopic views,
maintain the integrity of cervical flexion, and avoid excessive pressure being applied.
Cranshaw J. Airway management after major trauma. Contin Educ Anaesth Crit Care Pain 2006; 6(3):124–127.
Lockey D.J, Crewdson K, HM Lossiusm HM. Pre-hospital anaesthesia: the same but different. Br J Anaesth
2014; 113(2):211–219.
307
308
Chapter 8
12. E Commence a titrated dobutamine infusion starting at
5 µg/kg/min
The patient described is in septic shock despite fluid resuscitation and high dose
vasopressors. The profound degree of shock is evidenced by the lactate, Scvo2 levels
and carbon dioxide gap, all of which are useful measures of global oxygen supply
demand imbalance.
The adequacy of fluid resuscitation is evidenced by the ~5% increase in stroke
volume index (SVI) following the rapid fluid bolus. As a general guide, a ≤ 10%
increase in SVI is considered to be fluid unresponsive. A ≥ 15% increase in SVI is
considered fluid responsive and should prompt the consideration of a further
fluid bolus until the response is ≤ 10% (SVI maximisation). Changes in the 10–15%
range are equivocal and further fluid boluses should balance the risks and benefits.
However, the stroke volume index and hence cardiac index (HR x SVI) is low, despite
optimal heart rate and rhythm, which is consistent with significant myocardial
contractility impairment. This may be due to septic cardiomyopathy and/or ischaemic
heart disease. The highly sensitive cardiac troponin T (hs-cTropT) elevation does
not differentiate between these two diagnoses. A 12-lead ECG with acute/dynamic
changes consistent with ischaemia/infarction in a specific coronary territory, and
echocardiogram showing new regional wall motion abnormalities would be highly
suggestive of a type 1 myocardial infarction, and should be performed. However,
even if the clinical evidence points towards this diagnosis, the role and optimal timing
of acute percutaneous coronary intervention and the use of mechanical support are
highly controversial. The best immediate management therefore is to commence a
positive inotrope, such as dobutamine. There is no definitive trial evidence to support
the choice of one positive inotrope over any other.
In this scenario, the threshold for considering packed red blood cell transfusion
should be < 70 g/L and, as the patient is euvolaemic, the risk of fluid overload is
very high hence pRBC transfusion is not indicated. There is no value in increasing
the mean arterial pressures further as this is likely to have a negative impact on
myocardial function and worsen rather than improve both coronary and global
perfusion. The role of ‘stress dose’ glucocorticoid therapy in this scenario as a
treatment for functional hypoadrenalism remains controversial. It may be worth
considering a therapeutic trial depending upon the patient’s response to the
positive inotrope.
Somasundaram K, Ball J. Medical emergencies: atrial fibrillation and myocardial infarction. Anaesthesia
2013; 68(S1):84–101.
13. E Commence renal replacement therapy
In patients with normal renal function, on-pump cardiac surgery is associated with a
10-30% risk of acute renal injury and a < 5% risk of needing acute renal replacement
therapy. These risks are significantly increased in patients with pre-existing renal
impairment. Other peri-procedural risk factors include on versus off-pump, longer
bypass times, haemodynamic instability, need for high dose or protracted inotropes
and/or vasopressors.
Answers
In the scenario described, the patient has clearly developed acute kidney injury
(AKI), with oliguria, a metabolic acidosis, hyperkalaemia and uraemia. There is no
place for low dose dopamine or diuretics in either the prevention or management
of AKI. Given the rate of evolution of this patient’s metabolic derangement and
apparently normal renal perfusion, temporising therapy to improve the acidosis and
reduce the serum potassium are unlikely to prevent the need for renal replacement
therapy, hence this is the best answer.
There are a number of considerations to take in to account when considering renal
replacement therapy in the acute setting:
• Most centres use bicarbonate based fluids for renal replacement therapy
• Although there is no universally agreed thresholds for commencing renal
replacement therapy in ARF a reasonable suggestion would be:
• Hyperkalaemia (K+ > 6.5 mmol/L or o K+ > 5.5 mmol/L and rapidly rising at
> 0.25 mmol/hr for 2 or more hours).
• Correction of severe/unresolving acidosis (pH < 7.1); acidosis associated with
cardiovascular compromise (end organ hypoperfusion)/high vasoactive drug
requirements (noradrenaline > 0.5 µg/kg/min / dobutamine > 10 µg/kg/min).
• Uraemia (urea > 40 mmol/L or rising by > 12 mmol/24 hrs)
• Fluid overload causing severe hypertension and/or problematic oedema (e.g.
abdominal compartment syndrome) and/or contributing to hypoxaemia / poor
lung compliance.
• There is no evidence to support any specific modality over another in this setting
• The use of bolus insulin and dextrose mixtures is a poor practice as it is associated
with a very high incidence of acute, severe dysglycaemia and rapid rebound
hyperkalaemia. If temporisation of hyperkalaemia is required, continuous
infusions of insulin and dextrose are safer and more effective. Adjunctive use
of nebulised salbutamol and intravenous bicarbonate can also be very helpful.
If cardiac toxicity is evident, acute protection is afforded by a slow bolus of
intravenous calcium either as gluconate or chloride.
Bellomo R, ChapmanM, et al. Low-dose dopamine in patients with early renal dysfunction: a placebocontrolled randomised trial. Australian and New Zealand Intensive Care Society (ANZICS) Clinical Trials
Group. Lancet 2000; 356(9248):2139–2143.
Karajala V, Mansour W, et al. Diuretics in acute kidney injury. Minerva Anestesiol 2009; 75(5): 251–257.
Palevsky P M. Renal replacement therapy in acute kidney injury. Adv Chron Kidney Dis 2013; 20(1):76–84.
14. D Contact the transplant coordinator
When organ transplantation began all organs were retrieved from patients
immediately after cardiorespiratory arrest. In 1976 brainstem testing allowed retrieval
of heart-beating donor organs which has become the principal source of organs for
transplantation for the last 25–30 years. Non heart-beating organ donation (NHBOD)
however is re-gaining popularity. This is partly because the demand for organs is
increasing. In addition, the number of heart-beating donors is declining for two
reasons: fewer younger people are dying as a result of severe injury or catastrophic
cerebrovascular events, and improvements in diagnosis and management of severe
brain injuries mean that fewer fulfill the brainstem testing criteria.
309
310
Chapter 8
Suitability criteria for consideration for NHBOD include:
• A decision has been made to withdraw treatment
• They are expected to die within 2 hours
• They have organs suitable for transplantation
The only absolute contra-indications are human immunodeficiency virus (unless
the recipient is also HIV positive) or Creutzfeldt–Jakob disease. The final decision
regarding suitability is made by the retrieval and transplant surgeons.
Comprehensive guidance from the Intensive Care Society and General Medical
Council exist. The decision to withdraw treatment must be separate from the one to
donate organs. A protocol may be useful to dictate a withdrawal of care approach,
which ensures the interests of the dying patient remain the primary focus. The family
should first be made aware that further treatment is not in the patient’s best interests.
They can then be approached about donation after the transplant coordinator has
been contacted, the organ donor register checked and consent obtained from the
coroner. The coordinator and senior clinician will ideally approach the family together.
The key consideration here is what is deemed to be in the patient’s best interests and
does not cause harm or distress to them or their family. If they have expressed a wish
to donate organs then blood testing and maintenance of life-sustaining treatment
is acceptable (including escalation of treatment). Similarly delaying withdrawal or
moving the patient to facilitate transplantation is considered to be in the patient's
best interests if their wish to donate is known. Systemic heparinisation, femoral
cannulation and CPR are not acceptable as they have a significant risk of harm.
Withdrawal of active treatment should not vary from local practice because organ
donation is being considered and should proceed in accordance with the usual practice
of the critical care unit. Commencing treatment to ensure lack of distress prior to
extubation, termination of ventilation or cardiovascular support is the usual practice.
After withdrawal of care the patient may continue to have a cardiac output for some
time. If the patient is hypoxic or hypotensive for this period of time then the same
physiological conditions that occur in warm ischaemic time are present. Therefore if the
process of dying lasts more than 2–3 hours the retrieval may be abandoned.
The ethical issues are numerous and include: the withdrawal of treatment,
appropriateness of ongoing treatment to facilitate donation, the method of
diagnosis of death and the time left between cessation of cardiorespiratory function
and confirmation of death.
Returning to the scenario above, the next step (which is what the question is asking
for) is to contact the transplant coordinator. They will analyse the case and decide
whether or not it is suitable to continue before putting the family in a position to
make a decision. Breaking the news to the family that their relative will not survive
and approaching the topic of organ donation should be separate conversations
if possible. In addition the transplant coordinator should be present to answer
logistical questions you may not be aware of.
Intensive Care Society Working Group on Organ and Tissue Donation. Guidelines for adult organ and
tissue donation. London: Intensive Care Society, 2005.
Ridley S. UK guidance for non-heart-beating donation, Br J Anaesth 2005; 95(5):592–595.
Answers
15. B Examine the respiratory system
Obesity is a health epidemic facing Western countries. Obesity is defined as a body
mass index (BMI) > 30 kg/m2, ‘morbidly’ obese a BMI > 35 and ‘super morbidly’
obese> 55 kg/m2.. Recent figures suggest that up to 23% of men and 25% of women
in the UK are obese.
Bariatric surgery presents many challenges intra-and postoperatively. Management
of the patient’s co-morbidities is often a reason for high-dependency care
postoperatively as in this case. Complications are increased in this group and this
case explores the differential diagnosis of an immediate postoperative complication.
The list of differential diagnoses (which may not be exhaustive) include:
• Airway obstruction due to obstructive sleep apnoea (OSA), sedation, carbon
dioxide narcosis, anaphylaxis
• Breathing
• Hypoventilation resulting in hypercapnic respiratory failure
–– OSA
–– Residual anaesthesia or long-acting analgesia
–– Abdominal splinting with residual pneumoperitoneum or sub-optimal
position in bed
• Aspiration of gastric contents at induction or extubation
• Pneumothorax as a result of the central venous cannulation or laparoscopic
surgery
• Pulmonary embolism
• Negative pressure pulmonary oedema
• Gas embolism
• Circulation
• Perioperative myocardial ischemic event
• Postoperative bleeding (may be seen in drain output)
• Disability
• Residual sedative drugs
• Focal deficit due to stroke
• Global deficit due to hypoperfusion (e.g. relative hypotension or prolonged
reverse-Trendelenburg position)
• Exposure
• Hypoglycemia
• Hypothermia
• Pain (not only operative, e.g. long standing back pain)
• Urinary retention
The best way to approach a complex patient is perform a rapid examination looking
to exclude some of the dangerous causes above. ‘Agitated’ implies that the airway
is patent for now and with a grade three laryngoscopy (in the optimum conditions
present in theatre) caution and planning is required in order to re-intubate.
Hypercapnic respiratory failure is her main complaint and the focus of management
should be to find a reversible cause of this deterioration in order to prevent
re-intubation. This could potentially avoid significant morbidity and mortality
associated with a prolonged ventilatory period postoperatively.
311
312
Chapter 8
The question requests the next immediate step and therefore a careful examination
of the respiratory system would be of great use. Non-invasive ventilation (NIV)
could convert an undiagnosed simple pneumothorax (caused by a difficult central
line insertion as in this case) to a tension pneumothorax and examination findings
suggestive of this diagnosis would enable rapid decompression and resolution of
the acute deterioration. Aspiration of gastric contents or pulmonary oedema may
also be appreciated on clinical examination. As with all sick patients checking the
electrocardiogram, the surgical drain output, the blood glucose level, the degree
of residual neuromuscular blockade and the temperature are all part of the initial
survey.
Clinical examination should not be forgotten in the intensive care unit as it guides
further investigation and management in a more focused and efficient manner.
Sabharwal A. Anaesthesia for bariatric surgery, Contin Educ Anaesth Crit Care Pain 2010; 10(4):99–103.
16. B Full blood count
This scenario describes a case of Heparin Induced Thrombocytopenia (HIT), which is
seen in 2.5% of patients treated with unfractionated heparin and 0.1% of those on
low molecular weight heparin. It presents with reduced platelets, arterial and venous
thrombosis (30%), a systemic reaction consisting of anaphylactoid symptoms (25%)
and a skin rash, which represents dermal ischemia and necrosis as a result of emboli
(4%).The syndrome is further classified into two types.
Type 1 HIT is a benign decrease in platelet numbers, which appears to be a physical
interaction causing platelet aggregation. It results in a mild drop in the platelet
count and may occur hours after treatment is commenced and usually recovers once
heparin is stopped without any intervention. It is not associated with an increased
risk of thrombosis.
Type 2 HIT is an immune-modulated process caused by formation of
Immunoglobulin G (IgG) or rarely IgM antibodies, against heparin bound to a protein
called Platelet Factor 4 (PF4). The onset is often delayed (day 5–10 after commencing
treatment) but may present within hours if the patient has had previous exposure to
heparin. The tail of the antibody binds to the Fcylla receptor on the platelet surface
resulting in activation, aggregation, clot formation and a consumptive decrease in
numbers. The platelet count usually drops below 50% of baseline values and a prothrombotic state occurs and results in arterial and venous thrombi. The antibodies
persist in the plasma for 2–3 months.
The diagnosis of HIT is a 3-stage process. A scoring system is used to identify
patients requiring further testing. This is called the 4T score and has been validated
by Wakentin and Heddle in 2003. A low score (0–3 out of 8) has a negative predictive
value of 0.998 whereas an intermediate (4–5) or high (5–8) score has a positive
predictive value of 0.14 and 0.68 respectively, thus warranting further investigation
(see Table 8.2).
Answers
Table 8.2 The 4T score for diagnosis of HIT.
Element
Scoring
Thrombocytopenia
2: platelet count fall > 50% or less than 20–100 x 109/L
1: drop of 30–50% or less than 10–19 x 109/L
0: less than 30% drop or lowest count < 10 x 109/L
Timing
2: day 5–10 after starting treatment or day 1 if re-exposure within 30 days
1: after day 10 after starting treatment or day 1 if previous exposure within
30-100 days
0: Early fall with no previous exposure
Thrombosis
2: new proven thrombosis, skin necrosis or systemic reaction
1: progressive or recurrent thrombosis
0: nil
Alternative causes
2: no other possibilities
1: possible other cause
0: probable other cause
A score greater than 4 necessitates an enzyme-linked immune-sorbent assay (ELISA)
test for the IgG against heparin-PF4 complex (termed the ‘HIT screen’). The falsepositive rate is high due to the detection of other antibodies against this complex
that do not cause HIT and therefore if positive, a second test is performed to confirm
the diagnosis. Serotonin release is measured in platelets mixed with patient’s own
plasma and heparin as a marker of platelet activation. This is called the Serotonin
Release Assay (SRA).
In this scenario a full blood count would have revealed thrombocytopenia and
prompted the diagnosis of HIT. This mandates immediate termination of heparincontaining products (including heparin in a renal replacement circuit) and
confirmation of the diagnosis.
This patient obviously requires ongoing anticoagulation, and there are a number of
options which are not heparin-based: Lepirudin is a highly specific and irreversible
inhibitor of thrombin principally metabolised by the renal system and danaparoid is
a glycosaminoglycuronan Factor Xa antagonist principally metabolised by the liver.
Shaikh N. Heparin-induced thrombocytopenia. Journal of Emergencies, Trauma and Shock 2011;4(1):97-102.
17. C Total spinal
The clinical features are suggestive of an ascending block above the level required
for surgery. Interestingly, there is evidence in the literature to suggest that more
cephalad spread of spinal anaesthesia occurs in twin pregnancies compared with
singletons. In this case, the block would need to have ascended above T1 to cause
weakness of the arms and the bradycardia is likely the result of inhibition of cardioaccelerator fibres, which occurs when the block ascends above the level of T1-T4.
313
314
Chapter 8
The onset of apnoea suggests that cervical nerves 3, 4 and 5 supplying the
diaphragm have been affected. Total spinal block involves the brain stem and cranial
nerves, and in this case, the dilated pupils suggest oculomotor nerve palsy, hence a
total spinal is the most likely diagnosis.
Although this lady is likely to be anxious, anxiety alone would not account for the
obvious cardiovascular changes. Incidentally, there has been a suggestion that
preoperative anxiety may cause hypotension after spinal blockade. However, a
tachycardia would fit in more with a diagnosis of anxiety; meaning A is not the most
likely cause.
There have been a few case reports in the literature of hypoglycaemia following
neuraxial blockade in diabetic patients and in a healthy parturient, but given the
clinical features in this scenario, it is not the most likely cause. Hence B is incorrect.
Aortocaval compression in this lady is likely to cause significant hypotension due
to the twin pregnancy, although she has been placed in the left lateral position.
However, again, it would not explain her other symptoms, thus option E is not the
most likely diagnosis. A high spinal-induced cardiovascular collapse would not
explain the pupillary dilatation or the loss of consciousness with a blood pressure of
80/50 mmHg; therefore option D is incorrect.
Jawan B, Lee JH, Chong ZK, Chang CS. Spread of spinal anaesthesia for caesarean section in singleton and
twin pregnancies. Br J Anaesth 1993; 70(6):639–641.
Kuczkowski KM. Acute hypoglycaemia in a healthy parturient following induction of a combined spinalepidural analgesia for labour. Anaesthesia 2003; 58(5):488–489.
Orbach-Zinger S, Ginosar Y, Elliston J et al. Influence of preoperative anxiety on hypotension after spinal
anaesthesia in women undergoing Caesarean delivery. Br J Anaesth 2012; 109(6):943–949.
Palkar NV, Boudreaux RC, Mankad AV. Accidental total spinal block: a complication of an epidural test
dose. Can J Anaesth 1992; 39(10):1058–1060.
Thomas C, Madej T. Obstetric emergencies and the anaesthetist. Br J Anaesth CEPD Reviews 2002;
2(6):174–177.
18. D Dry and stimulate the newborn with a towel, replace
the wet towel and cover the baby
Anaesthetists in the delivery suite are not infrequently asked to assist with the
resuscitation of newborns. It is important to be clear that the primary duty of
care of the obstetric anaesthetist is to the mother. However, if the mother is in a
stable condition, and her care can be delegated to another qualified person, the
anaesthetist should assist with the resuscitation of the newborn.
The Resuscitation Council UK has a consensus and evidence based newborn
resuscitation algorithm (Figure 8.4), which starts with drying and stimulating the
baby, removing any wet towels and covering the newborn. This is followed by
assessing the newborn for tone, colour, breathing and heart rate, and if necessary,
delivering five inflation breaths with sustained positive airway pressure of 30 cmH2O
for 2–3 seconds (20–25 cm H2O in preterm babies). Assessing the Apgar score is not
part of the newborn resuscitation algorithm.
Answers
Dry the baby
Remove any wet towels and cover
Start the clock or note the time
Assess tone, breathing and heart rate
If gasping or not breathing:
Open the airway
Give 5 inflation breathes
Consider monitoring SpO2 monitoring
Birth
Figure 8.4 The newborn
resuscitation algorithm. Modified
from Resuscitation Council
UK, Newborn Life Support
Guidelines.
30 s
60 s
Re-assess
If no increase in heart rate
Look for chest movement
If chest not moving:
Recheck head position
Consider 2-person airway
Manoeuvres repeat inflation
Breaths consider SpO2 monitoring
Look for a response
Acceptable
pre-ductal SpO2
2 min
60%
3 min
70%
4 min
80%
5 min
85%
10 min
90%
If no increase in heart rate
Look for chest movement
When the chest is moving:
If slow (<60 min–1) or undetectable
heart rate start chest compressions
3 compressions to each breath
Reasess heart rate every 30 s
if slow (<60 min–1) or
undetectable heart rate
consider venous access and drugs
Clifford M, Hunt RW. Neonatal resuscitation. Best Pract Res Clin Anaesthesiol 2010; 24:461–74.
Resuscitation Council UK. Newborn Life Support. London: Resuscitation Council UK, 2010.
19. D Start an intravenous infusion of warmed isotonic
crystalloid
The reason for preoperative fasting is to reduce the risk of aspiration pneumonitis
at induction of anaesthesia. However, prolonged fasting does not further reduce
the risk of a harmful event for the patient, but adversely affects patient comfort
315
316
Chapter 8
and hydration, particularly in sickle cell disease, where dehydration can precipitate
an acute sickle crisis. Other potential factors precipitating sickle crisis include
hypothermia, venous stasis, hypoxia and acidosis.
In children with sickle cell disease, it is imperative that the period of preoperative
fasting be minimised. There should be a low threshold to instituting intravenous
fluid preoperatively to avoid dehydration. In the situation described above, the
patient is already dehydrated (thirst, prolonged fasting). Intravenous fluid therapy
should be started without further delay.
O’Meara M, Allford M. Anaesthesia for patients with sickle cell and other haemoglobinopathies. Anaesth
Inten Care Med 2010; 11(6):242–243.
Wilson M, Forsyth P, Whiteside J. Haemoglobinopathy and sickle cell disease. Contin Educ Anaesth Crit
Care Pain 2009; 10:24–28.
20. D Use a local non-specialist team to transfer the child
immediately to the nearest neurosurgical unit
In the UK, acute services for children with head injuries are organised such that
urgent supportive care is initiated locally and subsequent emergency care of
intracranial complications is undertaken centrally. Therefore after an accident, in the
stabilised, resuscitated, severely injured child, the initial priority is to identify those
needing surgical evacuation of haematoma, and to transfer them safely to centres
that provide such a service. For best outcomes, such transfer should be undertaken
within four hours, using the most appropriate resource that is available. As the
regional paediatric transport team will not be available for more than 3 hours, with
a further one hour for transport, it would not be suitable to await them either in the
emergency department, theatre or the local intensive care unit where paediatric
facilities are unlikely to be available. The process of localising and organising an
alternative paediatric transport team is likely to delay meaningful management of
this patient further. The most appropriate resource available is therefore the local
non-specialist transport team.
R C Tasker, Morris KP, Forsyth RJ, et al. Severe head injury in children: emergency access to neurosurgery in
the United Kingdom. Emerg Med J 2006; 23: 519–22.
National Institute for Health and Care Excellence (NICE). Head Injury: Triage, Assessment, Investigation and
Early Management of Head Injury in Children, Young People and Adults. CG No 176. London: NICE, 2014.
Royal College of Surgeons of England (RCSE) and British Orthopaedic Association (BOA). Better Care for
the Severely Injured. London: RCSE/BOA, 2003.
21. C It is safe to use within 4 hours of other parenteral
opiates
Remifentanil patient-controlled analgesia (PCA) is a novel alternative labour
analgesic option for patients that are unable to have an epidural.
Labour wards that offer the service have individual guidelines for the dosing
regimes, patient selection and the required monitoring. Most institutions agree that
a remifentanil PCA should not be started in a patient that has had another form of
opiate within 4 hours.
Answers
In general, guidelines state that mothers should be carefully counselled about the
PCA, explained the risks including respiratory depression, sedation, nausea, vomiting
and the potential for fetal bradycardia. They should also be made aware that the
drug is not licensed for use in pregnant women. Mothers should be taught how to
effectively use the PCA, this involves triggering the dose prior to the start of the
contraction, and this may get easier as the contractions become more regular.
Minimal monitoring requires the constant presence of a midwife with continuous
monitoring of oxygen saturations. Blood pressure, respiratory rate, sedation score
and foetal heart rate via a cardiotocograph (CTG) should also be monitored. Most
guidelines also state the need for oxygen delivery to prevent hypoxia due to
hypoventilation. A dedicated cannula for remifentanil delivery is generally necessary.
Schnabel A, Hahn N, Broscheit J, et al. Remifentanil for labour analgesia: a meta-analysis of randomised
controlled trials. Eur J Anaesthesiol 2012; 29(4):177–85.
22. D Pregabalin
Post-herpetic neuralgia (PHN) is neuropathic pain following herpes zoster infection
lasting longer than 3 months. It most commonly affects the thoracic dermatomes
but can also present in the ophthalmic division of the trigeminal nerve. About
10–20% of patients with shingles develop PHN. Risk factors include increasing age,
female sex and severe pain associated with the initial infection.
Antivirals and steroids during the initial infection stage have been shown to
reduce the incidence of PHN. Once the acute infection has resolved the window of
opportunity is missed.
PHN should be treated as per the National Institute for Health and Care Excellence
(NICE) guidelines for neuropathic pain. First line treatment involves either
amitriptyline or pregabalin. If satisfactory symptom control is not achieved
at the maximum tolerated dose either add in or switch to the other. Tricyclic
antidepressants should not be used in conjunction with a monoamine oxidase
inhibitor (MAOI) as this could lead to a fatal reaction similar to serotonin syndrome.
Opioids have been shown to be good at symptom control but side effects usually
limit their use.
5% lidocaine patches are licensed for the treatment of PHN but the evidence is not
conclusive. Transcutaneous electrical nerve stimulation (TENS) may also be effective
in some cases but would be contraindicated in a patient with a pacemaker.
Sympathetic nerve blocks, including both stellate ganglion blocks for trigeminal
nerve involvement and thoracolumbar sympathetic blocks for truncal involvement,
have limited long term success.
Gupta R, Smith PF. Post-herpetic neuralgia. Contin Educ Anaesth Crit Care Pain 2012; 12(4): 181–85.
National Institute for Health and Care Excellence (NICE). The pharmacological management of
neuropathic pain in adults in non-specialist settings. CG no 96. London: NICE, 2010.
317
318
Chapter 8
23. B Initial treatment is conservative with simple analgesics
Although this is an acute exacerbation of pain there are no red flags that may suggest
spinal cord compression. These red flags include:
•
•
•
•
•
•
•
•
•
•
Unexplained weight loss
Fever
Thoracic pain
History of carcinoma
Bladder or bowel dysfuntion
Presence of other medical illneses
Progressive neurological deficit
Saddle anaesthesia
Gait disturbance
< 20 or > 50 years
Neurological dysfunction in a single limb without progressive neurological
compromise or gait disturbance suggests unilateral spinal nerve root compression.
Most of these will resolve spontaneously and initial conservative therapy is indicated.
Although an MRI is indicated it is not urgent and plain radiography will not show any
nerve compression.
Yellow flags are features that suggest an increased likelihood of long term chronicity
and disability. These include:
•
•
•
•
•
•
Social difficulties
Financial problems
Depression and negative thinking
Passive treatment expectations
Fear avoidance behaviour
Belief that back pain is harmful or potentially disabling
These must be explored and assessed in conjunction with the interventional
treatment for this patient.
Samanta J, Kendall J, Samanta A. Chronic low back pain. BMJ 2003;326:535
24. A Interscalene block with 20 mL 0.5% levobupivacaine
and regular paracetamol and ibuprofen
Shoulder surgery is potentially very painful in the postoperative period. Early
mobilisation and physiotherapy is important to ensure good return of function.
Effective perioperative pain management is therefore required to facilitate
this. As with all pain management a multimodal approach should be adopted.
Regular paracetamol and ibuprofen should be prescribed provided there are no
known contraindications. Some surgeons may wish to avoid non-steroidal antiinflammatory drugs (NSAIDs) in the first 24 hours due to the increased risk of
bleeding.
Interscalene blocks provide good analgesia for up to 15 hours with minimal systemic
effects. Should the expertise be available a catheter technique could be employed. A
strong opioid should be prescribed for when the block wears off.
Answers
Intra-articular analgesia (local anaesthetic + morphine) reduces postoperative
morphine requirements but is less effective than an interscalene block.
Suprascapular nerve blocks can be useful when an interscalene block is not
possible but only blocks a proportion of the pain afferents from the shoulder. It will
provide no cutaneous coverage so will need to be combined with local anaesthetic
infiltration to the skin. An axillary block is not appropriate for shoulder surgery as
blocking the brachial plexus at the level of the terminal branches will only provide
good analgesia for surgery below the elbow.
Table 8.3 summarises the various sensory effects of blocking the brachial plexus at
different points along its course.
Table 8.3 Effects of blocking the brachial plexus at its different locations.
Block
Part of brachial
plexus blocked
Sensory effect
Interscalene
Roots
Shoulder down to elbow. C8 and T1 often missed so ulnar
sparing is common
Supraclavicular
Trunks
Most of the upper limb. The 3 trunks are close together at
this point
Infraclavicular
Cords
Below the elbow
Axillary
Terminal branches
Below the elbow. Musculocutaneous nerve will need to be
blocked
Beecroft C, Coventry D. Anaesthesia for shoulder surgery. Contin Educ Anaesth Crit Care Pain 2008; 8(6):
193–198.
25. E Second blood patch
The risk of post-dural puncture headaches (PDPHs) following a labour epidural is
quoted up to about 10%. The occipital/frontal headache usually develops in the first
72 hours and has a clear postural element. It is commonly associated with nausea,
vomiting, neck stiffness and photophobia. It can also result in tinnitus and hearing
loss. Rarely abducens nerve palsies develop due to diminished cerebral spinal fluid
(CSF) volumes.
Headaches are common in the postpartum period and it is important to get a
thorough history and examination to exclude more serious pathology.
Table 8.4 shows a list of potential differential diagnosis.
Once a diagnosis of PDPH has been made, treatment can be either conservative,
pharmacological or with an epidural blood patch. Conservative treatment comprises
bed rest, good hydration, caffeinated drinks and simple analgesia.
Pharmacological management includes caffeine or 5HT-agonists. These have both
been tried for their cerebral vasoconstrictor properties but with limited success and
in reality are seldom used.
319
320
Chapter 8
Table 8.4 Differential diagnosis for post-partum headache
Tension headache
Migraine
PDPH
Pre-eclampsia
Meningitis
Cortical vein thrombosis
Space occupying lesion
Subarachnoid haemorrhage
An epidural blood patch remains the gold standard and is thought to be most
effective if performed greater than 24 hours after the dural puncture. Historically the
efficacy of this treatment was exaggerated. It is thought 50% of woman will recover
completely after a single blood patch. However, 40% will go on to need a second.
It is postulated to work by blocking the hole in the dura thereby preventing further
CSF leak.
Sabharwal A, Stocks GM. Postpartum headache: diagnosis and management. Contin Educ Anaesth Crit
Care Pain 2011; 11(5):181–85.
Turnbull DK, Shepherd DB. Post-dural puncture headache: pathogenesis, prevention and treatment. Br J
Anaesth 2003; 91(5):718–29.
26. C Previous retinal detachment surgery
Cataract surgery is very common day case procedure often done under regional
anaesthesia. Patients tend to be elderly with numerous co-morbidities so a thorough
preoperative assessment is essential.
The patient in this scenario is a typical cataract patient and care should be taken to
explain the regional technique, its advantages and complications, and rule out any
possible contraindications. Absolute contraindications to regional blocks include
patient refusal, allergy to local anaesthetics and local infection. None of these apply
in this scenario.
Previous retinal detachment surgery is a strong relative contraindication due to the
scleral buckle that is applied during these procedures. This can lead to unreliable
spread of the local anaesthetic and an increased risk of globe perforation due to
scleral scarring. In such scenarios, unless the anaesthetist has extensive experience,
ophthalmologists themselves may choose to perform the block or use topical
anaesthesia instead.
Option A is not the correct answer. An international normalised ratio (INR)
within therapeutic range is not a contraindication, as there is no evidence that
appropriate anticoagulation leads to major haemorrhages. Avoiding retrobulbar
and peribulbar blocks would be wise in anticoagulated patients due to the need to
Answers
use a sharp needle. Sub-Tenon’s blocks, however, are generally safe if the INR is not
inappropriately high (as long as the surgeon is happy to operate).
Age over 70 and blood glucose level of 8 mmol/L are not contraindications. Blood
glucose is likely to be high in many cataract patients, due to the association with
diabetes. Patients with poorly controlled diabetes may need medical review before
surgery anyway. Chronic obstructive pulmonary disease (COPD) alone is not a
contraindication as long as lying flat is not an issue. Patients can have supplementary
oxygen during the procedure if needed and as long as he is cooperative, he can let the
surgeon know if he needs to cough at any point.
Canavan KS, Dark A, Garrioch MA. Sub-Tenon’s administration of local anaesthetic: a review of the
technique. Br J Anaesth 2003; 90(6):787–793.
Gordon HL. Preoperative assessment in ophthalmic regional anaesthesia. Contin Educ Anaesth Crit Care
Pain 2006; 6(5):203–206.
Guise P. Sub-Tenon’s anesthesia: an update. Local Reg Anesth 2012; 5:35–46.
27. B This is a regional anaesthetic related complication,
reassure and continue to observe the patient in recovery
for resolution
Carotid surgery can be performed under either a regional anaesthetic block or
general anaesthesia. In order to be performed awake, the second, third and fourth
cervical dermatomes need to be blocked (C2–4). Many suggest combining this
with blockade of submandibular branches of the trigeminal nerve and infiltration
of the carotid sheath by the surgeons. Superficial cervical plexus blockade is often
sufficient for this purpose, although some advocate combining a superficial with a
deep cervical plexus block.
The superficial cervical plexus is blocked by infiltrating local anaesthetic in the
subcutaneous plane along the posterior border of the sternocleidomastoid muscle.
It is a relatively safe procedure, although a rare complication includes a Horner’s
syndrome, comprising unilateral ptosis, miosis and anhydrosis due to sympathetic
blockade. The patient exhibits the signs of Horner’s syndrome, and this is the most
likely cause of the presentation. The signs presented are unlikely to be due to a postoperative stroke. Intralipid is administered in the management of local anaesthetic
toxicity, which is unlikely with 20 mL of 0.25% levobupivacaine (50 mg in total).
Congenital anisocoria is not associated with ptosis.
Spargo JR, Thomas D. Local anaesthesia for carotid endarterectomy. Contin Educ Anaesth Crit Care Pain
2004; 4(2):62–65.
28. D Adductor canal nerve block
The femoral nerve (FN) arises from the posterior divisions of the ventral rami of the
L2-L4 lumbar spinal nerves. It first descends within the bulk of psoas major muscle
then emerges from its lower part, running downward in the fascial compartment
plane between the psoas and the iliacus muscles. The femoral nerve then passes
under the inguinal ligament into the thigh, where it lies lateral and slightly deeper to
the femoral artery. The femoral artery and vein are contained in the femoral sheath,
321
322
Chapter 8
which lies above the fascia iliaca and underneath the fascia lata. Here the femoral
nerve lies above the iliacus muscle and is sandwiched by the two layers of fascia
iliaca to separate the nerve from the femoral sheath medially (Figure 8.5).
Femoral Femoral Femoral
nerve
artery
vein
Skin
Fascia
lata
Sartorius
muscle
Figure 8.5 Anatomical location
of the femoral nerve beneath the
inguinal ligament.
Femoral
sheath
Pectineous
muscle
Fascia
iliaca
Lateral
Medial
Iliacus muscle Psoas muscle
In the thigh, the femoral nerve gives off anterior and posterior divisions. The anterior
division supplies the sartorius and pectineus muscles. It also gives off articular
branches to the hip joint and cutaneous branches to the anterior and the medial
surface of the thigh.
The posterior division of the femoral nerve provides articular innervation to the
knee joint and muscular branches to the quadriceps muscles (rectus femoris, vastus
lateralis, vastus medialis and vastus intermedius). The posterior division continues
downward to become the saphenous nerve, which is the largest sensory branch of
the femoral nerve.
A femoral nerve block is indicated for operations on the anterior thigh (i.e. skin
graft, muscle biopsy and lacerations) and knee, and postoperative pain relief after
femur and knee surgery. Additionally, femoral nerve blocks can be used to provide
analgesia for hip dislocation and femoral neck fracture. When used in combination
with a sciatic nerve block, femoral nerve blocks can be used for any procedures
below the knee.
There are several approaches to block the femoral nerve, including a nerve
stimulator guided nerve block, 3-in-1 block, fascia iliaca block and ultrasound
guided femoral nerve block.
Nerve stimulator guided femoral nerve block: this block is performed at the
inguinal crease, where the femoral nerve is located below the inguinal ligament and
lateral to the femoral artery. Femoral arterial pulsation is identified first in the middle
of the line joining anterior superior iliac spine and pubic tubercle. The needle (50 mm
22G block needle) is inserted at 60° cephalad, approximately 1–2 cm lateral to the
pulsation. The first twitch observed is the sartorius twitch, followed by the patellar
twitch (quadriceps contraction) caused by stimulation of the posterior division of the
femoral nerve. 15–20 mL of local anaesthetic (LA) is injected at this point.
3-in-1 nerve block: this block uses the same technique as nerve stimulator guided
nerve block. However, in a 3-in-1, a larger volume of LA (25–30 ml) is injected and
Answers
distal pressure is applied during injection to help the LA spread to the lateral femoral
cutaneous nerve and obturator nerve, in addition to the femoral nerve. The reliability
of this block, and the capacity to anaesthetise the obturator nerve, however, has
come in to significant question and it is not a recommended approach.
Fascia iliaca block: to perform this block, one must draw a line connection the
anterior superior iliac spine and the pubic tubercle. Next, this line is then divided
into thirds. The needle (50 mm 22G block needle) is inserted 1–2 cm below the
junction of the middle and lateral thirds. As the needle is advanced, two pops are felt
as the needle pierces the fascia lata and the fascia iliaca. The femoral nerve located in
this fascial plane, where 20-30 of LA is injected at this point. Fascia iliaca block is the
easiest way to block the femoral nerve. Ultrasound guided fascia iliaca block is also
described and is seen as a safer approach to performing this block.
Ultrasound guided femoral nerve block: a high frequency linear probe is used for
this block. This block is performed just below the inguinal crease where the nerve is
fairly superficial (< 3 cm from the skin) and usually has a triangular or flattened oval
shape just lateral to the femoral artery. A 50 mm 22G needle is inserted in-plane
in a lateral to medial orientation to avoid puncture of femoral vessels. The needle
is advanced toward the femoral nerve and 10–20 mL of LA is injected around the
nerve. Ultrasound guidance may reduce the onset time for the block and the volume
of the LA.
Adductor canal (sub-sartorial) block: Recently, the adductor canal block has been
used for perioperative analgesia for knee surgery. With the use of ultrasound, this
block becomes technically straightforward and a reliable approach to block the
saphenous nerve, which is a pure sensory nerve. The adductor canal block requires
injecting LA deep to the sartorius muscle in the adductor canal.
Anatomical examination of the adductor canal shows that, in addition to the
saphenous nerve, this canal also contains medial femoral cutaneous nerve, medial
retinacular nerve and articular branches from the obturator nerve. Thus injecting LA
in the adductor canal might produce sensory block of the whole of the anterior and
medial aspects of the knee without motor blockade. This is helpful in major knee
operations, such as total knee replacement (TKR).
Using a small volume of LA (5–10 mL) will result in adequate analgesia for knee
arthroscopy, anterior cruciate ligament reconstruction and lower leg, foot and ankle
operations involving area covered by the saphenous nerve. Using a large volume of
LA (20–30 mL), results in a proximal spread of the LA in the adductor canal leading to
reliable analgesia for major knee surgery, like TKR.
A high frequency linear ultrasound probe is used in this block. With the patient in
the supine position, the knee is slightly flexed and the leg is externally rotated. The
ultrasound probe is placed on the anterior aspect of the thigh, midway between
the medial epicondyle and the inguinal crease. Once the femur is identified, the
ultrasound probe is moved medially until the boat shape sartorius muscle is seen. At
this point, the femoral artery lies just underneath the sartorius in the adductor canal.
The saphenous nerve is usually too small to be visualised and the objective is to inject
LA around the femoral artery under the sartorius muscle. A 22G 100 mm, short beveled
block needle is inserted ensuring that 20–30 mL of LA spreads in the adductor canal.
323
324
Chapter 8
With enhanced recovery pathways gaining popularity, the addition of nerve blocks
to multimodal analgesic regimen provides optimum pain control in orthopaedic
surgery to improve patient outcomes and speed up a patient’s recovery.
Although many studies have shown that femoral nerve block provides superior
analgesia and causes fewer side effects when compared with intravenous
opioid, they also shown that femoral nerve block prolongs the motor blockade
and increases the risk of patient fall. This might delay the patient’s recovery and
discharge from hospital.
Adequate pain control and preservation of motor activity has become the optimal goal
in TKR surgery to enhance patient recovery. Therefore, in the above clinical scenario, the
most appropriate option is to perform an adductor canal block as it results in a motor
sparing sensory blockade (no quadriceps weakness) with effective pain control.
Kim DH, Lin Y, Goytizolo EA,et al. Adductor canal block versus femoral nerve block for total knee
arthroplasty: a prospective, randomized, controlled trial. Anesthesiology 2014; 120:540–50.
Quemby D, McEwen A. Ultrasound guided adductor canal block (saphenous nerve block). Anaesthesia
(Tutorial Of The Week 301). 13 Jan 2014.
Jaeger P, Nielsen ZJ, Henningsen MH, et al. Adductor canal block versus femoral nerve block and
quadriceps strength: a randomized, double-blind, placebo-controlled, crossover study in healthy
volunteers. Anesthesiology 2013; 118:409–15.
29. D Intracardiac mass on echocardiogram
Infective endocarditis is caused by a microbial infection of a heart valve (either
native or prosthetic) or the endocardium with subsequent tissue destruction and
vegetation formation. The average age at diagnosis of endocarditis in the UK has
increased to 69 years of age, up from 30-40 years of age as rheumatic heart disease is
no longer the primary risk factor. Age-related valvular damage and iatrogenic factors
such as prosthetic valves, pacemakers and indwelling defibrillators form the main
risk group.
Infective endocarditis is a sequelae to an area of the endothelium exposed to high
velocity blood flow or following mechanical damage or post-introduction of foreign
bodies. A sterile thrombotic vegetation acts as a focus for bacterial infestation
which leads to bacterial vegetations. Eventually these lead to the sequelae of sepsis,
abscess formation and emboli.
Clinical investigation and treatment requires a multidisciplinary approach involving
cardiologists, intensivists, anaesthetists, microbiologists, neurologists and surgeons.
The Modified Duke’s criteria offer high specificity and sensitivity when applied to
patients with native valve infective endocarditis and positive blood cultures.
A confirmed diagnosis requires two major, one major and two minor or five minor
criteria. A possible diagnosis is the presence of one major and one minor or three
minor criteria. However, the Duke criteria cannot reasonably be applied when the
blood cultures are not positive or an iatrogenic factor such as a prosthetic valve or
pacemaker is involved, or when infective endocarditis affects the right side of the
heart.
The modified Duke’s criteria includes:
Answers
Major criteria
1. Positive blood culture
2. Echocardiogram positive for:
• Oscillating intracardiac mass
• Intracardiac abscess
• New partial dehiscence of prosthetic valve
Minor criteria
• Fever
• Predisposed heart condition or intravenous drug use
• Vascular or immunological phenomena like major arterial emboli, septic
pulmonary infarcts, mycotic aneurysm, intracranial or conjunctival haemorrhagic
lesions, Janeway lesions
• Microbiological evidence such as polymerase chain reaction (PCR), serological
tests, or positive blood cultures not meeting a major criterion
Of the options given in this clinical scenario, only the presence of an intracardiac
mass or abscess is classified as a major criterion of the Modified Duke’s criteria,
although all the other options are possible occurrences in a patient with infective
endocarditis. Jayneway lesions are haemorrhagic nodules found on the palms
and feet in infective endocarditis patients due to microabscesses caused by septic
emboli. Although a temperature of > 38°C is a minor criterion, it is not required for
the diagnosis of infective endocarditis.
Martinez G, Valchanov K. Infective endocarditis. Contin Educ Anaesth Crit Care Pain 2012; 12(3):134-139.
30. C Noradrenaline infusion titrated to blood pressure
The oesophageal Doppler monitor is a cardiac output monitoring device that
can be utilised for intraoperative fluid optimisation. Once correctly placed in the
oesophagus, it provides a velocity-time waveform by measuring the velocity of
blood flow in the descending aorta. This helps guide intraoperative fluid therapy
based upon derived parameters.
Parameters calculated are:
• Stroke distance (SD) - the distance that a column of blood moves down the aorta
with each contraction. Values are age and size dependent
• Stroke volume (SV) - the volume of blood ejected from the left ventricle during
each contraction. Normal range of 60-100 mL
• Stroke volume index (SVI) - the stroke volume divided by the body surface
area (BSA). Normal range of 35-65 mL/m2. A low SVI could be either due to
hypovolaemia or a high after load. A high SVI may be caused by decreased
afterload
• Flow time corrected (FTc) - the duration of systolic aortic blood flow corrected for
heart rate. Normal range is 330-360 ms. A low FTc may be due to hypovolaemia or
an increased afterload. A high FTc may be seen by a low afterload.
The original oesophageal Doppler reading in this patient suggests a peripherally
vasodilated circulation which could be attributed to a septic response to peritonitis.
325
326
Chapter 8
As per the fluid management protocol suggested for oesophageal Doppler
monitoring, following a bolus of 200 mL of colloid if the SV were to increase by
greater than 10% another bolus could be considered. Under the given circumstances
it would be most appropriate to initiate vasopressor therapy with noradrenaline.
Dobutamine would not be appropriate as its chief action would be to increase
cardiac output rather than cause peripheral vasoconstriction, and may in fact worsen
the vasodilation and hypotension.
Drummond KE, Murphy E. Minimally invasive cardiac output monitors. Contin Educ Anaesth Crit Care Pain
(2012) 12 (1): 5-10.
Chapter 9
Mock Paper 9
Questions
1. A 61-year-old man has been brought to the emergency department intubated and
ventilated. Examination reveals a large frontal haematoma and a single dilated, but
reactive, pupil. His abnormal observations are a blood pressure of 180/100 mmHg,
heart rate of 45 bpm and temperature of 35.5°C. An arterial blood gas shows Pao₂
13 kPa, Paco₂ of 6.9 kPa and blood glucose 8 mmol/L.
Which of the following parameters should be your priority when attempting to
acutely improve this patient's cerebral perfusion?
A
B
C
D
E
Temperature
Paco₂
Blood pressure
Pao₂
Blood glucose
2. You are anaesthetising a 78-year-old man for a right upper lobectomy and
lymphadenectomy for adenocarcinoma via video assisted thoracoscopic surgical
approach (VATS). He is a long-term smoker, has chronic obstructive pulmonary
disease (COPD) and takes aspirin 75 mg o.d. His FEV1 is 1.5 L. Despite your best
efforts, you fail to site a thoracic epidural.
Which of the following would be the most appropriate technique to optimise this
gentleman's perioperative analgesia?
A
B
C
Single shot paravertebral injection at T6
Ask the surgeon to site a paravertebral catheter
Run a remifentanil infusion perioperatively and leave the patient intubated
overnight
D Ask the surgeon to site an intrapleural catheter
E Perform intercostal blocks at T5–8
3. You are asked to urgently review a 57-year-old man 7 days post left
pneumonectomy. He remained intubated and ventilated for 24 hours post
operatively due to intraoperative bleeding and hypothermia. A left sided intercostal
drain was removed 24 hours ago. He is now complaining of cough, shortness of
breath and chest pain. His oxygen saturations are 89% on 15 L/min oxygen.
328
Chapter 9
On examination there is new subcutaneous emphysema of the chest wall. Heart
rate is 60 beats per minute and blood pressure is 80/50 mmHg.
What is the most appropriate next step?
A
B
C
D
E
Urgent chest radiograph (CXR)
Needle thoracocentesis followed by insertion of 22F intercostal drain
Immediate insertion of a 12F intercostal drain by the Seldinger technique
Urgent bronchoscopy
Urgent CT scan and thoracic surgical opinion
4. A 3-year-old boy is under general anaesthesia for the removal of a foreign
body partially obstructing his right main bronchus via rigid bronchoscopy.
He is breathing spontaneously and receiving sevoflurane in air. Foreign body
instrumentation is difficult and after prolonged grasping attempts and suctioning,
he becomes bradycardic with a heart rate of 25 beats per minute.
What is the most likely cause of his clinical deterioration?
A
B
C
D
E
Hypoxia
Depth of anaesthesia
Hypothermia
Hypercarbia
Vasovagal reflex
5. A 48-year-old woman has had an arthroscopic rotator cuff repair. She has received
a general anaesthetic, a supraglottic airway was inserted and had an interscalene
block. Her surgery finished at midday.
Which of the following is most likely to prevent her from being discharged on the
day of surgery?
A
B
C
D
E
Lives in a rural location 30 minutes by car to the nearest hospital
Has an adult relative to act as carer at home only until 20.00
Hasn’t yet passed urine
Is taking a public taxi home with an adult relative
Has residual upper arm weakness
6. A 78-year-old man is listed for a transurethral resection of his prostate (TURP)
under spinal anaesthesia. He has moderate to severe chronic obstructive
pulmonary disease (COPD) with ongoing steroid use, ischaemic heart disease,
and had a coronary stent inserted 15 months ago. He normally takes aspirin
and clopidogrel, but has not been taking the latter for “a few weeks”. He has also
recently started taking rivaroxaban 10 mg at night for an irregular heart rate.
What is the safest way to proceed?
A
B
Ensuring 18 hours after the last dose of rivaroxaban, give a spinal, and then
start a heparin infusion postoperatively
Give a spinal now and use treatment dose low molecular weight heparin
(LMWH) from 2 hours postoperatively
Questions
C
Wait until 24 hours after the last dose of rivaroxaban, then proceed with a
spinal, and give the next dose immediately postoperatively
D Ensure 12 hours after the last dose of rivaroxaban, and give prophylactic
LMWH 6 hours postoperatively
E Discuss with the patient the increased risks of central neuraxial blockade and
proceed under general anaesthesia
7. A 64-year-old man undergoes hip surgery under general anaesthesia. He is positive
pressure ventilated through a size 5 laryngeal mask airway and anaesthesia is
maintained with nitrous oxide and sevoflurane. In recovery, he complains of
paraesthesia over the right anterior aspect of his tongue. There is no dysphagia or
dysarthria and tongue appearance and movements are normal.
What is the most likely cause of his neurological signs in recovery?
A
B
C
D
E
Hypoglossal nerve injury
Lingual nerve injury
Recurrent laryngeal nerve injury
Inferior alveolar nerve injury
Venous drainage obstruction
8. A patient with an acute subarachnoid haemorrhage is undergoing coil
embolisation of the aneurysm in the interventional neuroradiology suite.
Anaesthesia is induced with alfentanil, propofol and rocuronium. Maintenance of
anaesthesia is with sevoflurane and remifentanil infusion. Shortly after intubation
the observations are as follows:
• Blood pressure: 220/110 mmHg
• Heart rate: 90 beats per minute
• Spo2 98%
• ETCO2 4.9 kPa
• End-tidal sevoflurane 1.9%
What is the most appropriate initial management?
A
B
C
D
E
Alert radiologist
Increase depth of anaesthesia
Increase minute ventilation
Give mannitol 1 g/kg
Start intravenous esmolol infusion
9. A 10 kg child with no comorbidities is scheduled for an elective umbilical hernia
repair as a day case.
Which of the following would be the best regime of injectate for caudal epidural
analgesia?
A
B
C
D
E
10 mL of 0.25% levobupivacaine with 10 μg fentanyl
10 mL of 0.25% levobupivacaine
10 mL of 0.25% plain bupivacaine with 300 μg diamorphine
10 mL of 0.25% levobupivacaine with 25 μg clonidine
10 mL of 0.25% bupivacaine
329
330
Chapter 9
10. A 65-year-old man for elective thoracotomy and pulmonary lobectomy is to have a
thoracic epidural for perioperative analgesia.
Which of the following is the best approach for epidural insertion?
A
B
C
D
E
A midline mid-thoracic epidural under general anaesthesia
A paramedian mid-thoracic epidural under light sedation or awake
A paramedian lower-thoracic epidural under general anaesthesia
A midline upper lumbar epidural under light sedation or awake
A midline mid-thoracic epidural under light sedation or awake
11. An 84-year-old ASA 3 woman is listed for multilevel facet joint injections and a
caudal epidural by the orthopaedic surgeons. The patient will need to lie in the
prone position. Comorbidities include moderate chronic obstructive pulmonary
disease (COPD), angina, hypertension and chronic lower back pain. Alongside all
her cardiovascular medications she takes regular co-dydramol and amitriptyline
for her pain.
The safest anaesthetic technique for this procedure is:
A
B
C
D
E
0.25–0.5 mg/kg intravenous ketamine
Local anaesthesia only with no sedation
Infusion of remifentanil at 0.25 mg/kg/min
Target controlled infusion of propofol at a 1 mg/mL
0.5 μg/kg fentanyl followed after several minutes by small doses of intravenous
midazolam titrated to effect
12. A 62-year-old non-diabetic woman presents to the intensive care unit with severe
urosepsis.
Which of the following glucose levels would be the most appropriate to target?
A
B
C
D
E
> 4 mmol/L
4–6 mmol/L
6–8 mmol/L
< 10 mmol/L
< 15 mmol/L
13. A 19-year-old male motorcyclist is admitted following a high speed road traffic
accident. The retrieval team report he has clinical evidence of bilateral flail
segments and a significant neurological injury. He is intubated and sedated by the
retrieval service with intermittent doses of ketamine, propofol and rocuronium
and arrives to the intensive care unit. He has been haemodynamically stable with
moderate and escalating ventilator requirements.
The most appropriate sedation regime for this patient on the intensive care unit
would be:
A
B
Propofol and fentanyl
Clonidine and fentanyl
Questions
C Midazolam and fentanyl
D Ketamine and fentanyl
E Fentanyl alone
14. A 26-year-old woman who is 32/40 pregnant had a witnessed collapse whilst
shopping. She received bystander cardiopulmonary resuscitation (CPR) and
advanced life support (ALS) by the paramedics for one hour prior to transfer to a
teaching hospital. In hospital, a Caesarean section was performed immediately.
ALS continued for a further 45 minutes without return of spontaneous circulation
and a profound metabolic acidosis developed.
What now is the most appropriate management option?
A
B
C
D
E
Terminate life support and organise a team debrief
Administer thrombolysis and continue ALS
Continue ALS until the intensive care consultant arrives
Commence extra-corporeal membrane oxygenation (ECMO)
Administer 10–20 mL of 8.4% sodium bicarbonate
15. A 76-year-old woman has had an upper gastrointestinal bleed and presented with
an acute kidney injury. After resuscitation and an oesophago-duedenoscopy she
is admitted to the intensive care unit for renal replacement therapy. The nurse
requests that you prescribe the particulars of renal haemofiltration including the
anticoagulation.
The most appropriate choice is:
A
B
C
D
E
Unfractionated heparin loading dose followed by a pre-filter infusion
No anti-coagulation
Prostacyclin infusion
Sodium citrate pre-filter infusion
Increasing the fraction of replacement fluid added before the filter
16. A 65-year-old man is recovering on the high dependency unit after an
emergency laparotomy for small bowel perforation for which he received an
effective epidural. His background includes treated hypertension, a smoker of
20 cigarettes per day and mild depression. Overnight he becomes very agitated
and confused and attempts to remove his invasive lines and monitoring.
Examination, review of his blood science investigations and blood gas results are
all unremarkable.
What is the most appropriate course of treatment?
A
B
C
D
E
Reassure the patient regarding his situation
Call his wife to hospital to help calm him down
Prescribe vitamin replacement therapy and benzodiazepine sedation
Prescribe haloperidol
Commence sedation with clonidine
331
332
Chapter 9
17. A 26-year-old woman who is 3 days post-partum has returned to the labour ward
complaining of an ongoing headache. She delivered vaginally after having a
lumbar epidural for labour. On the first day postpartum she had complained of
a frontal headache that worsened with coughing and had been diagnosed with
a post-dural puncture headache (PDPH). At home, she has been taking simple
analgesia and drinking plenty of water for the past 2 days but the headache is
persisting.
What is the next best line of management in this situation?
A
B
C
Encourage her to drink coffee and 3 L of water per day
Encourage her to drink coffee and prescribe sumatriptan
Admit her overnight for intravenous fluid therapy, regular analgesia and
further assessment
D Offer her an epidural blood patch
E Offer her an epidural blood patch and perform routine blood cultures at the
same time
18. A 21-year-old woman in antenatal clinic is due to have an elective Caesarean
section for breech presentation within the next two weeks. She is concerned
about having a spinal anaesthetic as she has been diagnosed with gestational
thrombocytopenia. You review her blood results and her platelet count has been
low but steady.
Which of the following blood results would prevent this lady from having a spinal?
A
B
C
D
E
Platelet count < 50 × 109/L
Activated partial thromboplastin (APTT) time of 30 seconds
Platelet count < 100 × 109/L
Platelet count < 70 × 109/L
Prothrombin time (PT) of 12 seconds
19. A 15 kg, 3-year-old girl was brought to the emergency department with a history of
choking on a piece of apple 6 hours previously. She appears comfortable and not in
respiratory distress. Her chest sounds clear on auscultation but a chest X-ray shows
a right lung that is more inflated and radiolucent compared to the left, particularly
on the expiration film.
Suspecting the child has inhaled the piece of apple, the ENT team want to perform
an urgent examination under anaesthesia (EUA) with a rigid bronchoscopy and
removal of foreign body.
The most appropriate anaesthetic plan for this case is:
A
B
Perform a rapid sequence induction and intubate to secure the airway
Routine intravenous induction with muscle relaxant. Intubate and ventilate
until rigid bronchoscopy
C Routine intravenous induction with muscle relaxant. Insert a supraglottic
airway device for ventilation until rigid bronchoscopy
D Routine intravenous induction without muscle relaxant. Facemask ventilation
until rigid bronchoscopy
Questions
E
Inhalational anaesthetic induction and maintenance with sevoflurane, without
muscle relaxant. Maintain spontaneous respiration throughout the case
20. An 18-month old boy is scheduled for an inguinal hernia repair as a day case. His
mother reports that he developed an anxiety to needles since a hospital admission
for pneumonia 5 months previously, and has not had his MMR vaccination. His
mother requests a gas induction and asks if he could receive his MMR vaccination
while under general anaesthesia.
The best course of action is:
A
B
Administer the MMR vaccination after induction of anaesthesia
Ask the surgical team to administer the MMR vaccination whilst under general
anaesthesia
C Ask the paediatric team to administer the MMR vaccination postoperatively
prior to discharge
D Arrange for the GP to administer the MMR vaccination 4 weeks postoperatively
E Cancel the surgery until the child has had his MMR vaccination
21. A 58-year-old woman is listed for an elective hysterectomy. She states that she has
a morphine allergy which made her eyes and lip swell in the past.
Which of the following analgesics would be unsafe in this patient?
A
B
C
D
E
Pethidine
Tramadol
Buprenorphine
Methadone
Fentanyl
22. A 64-year-old woman with a history of chronic pain is listed for a shoulder
replacement. She normally takes gabapentin 300 mg three times a day,
paracetamol 1 g as needed and a buprenorphine patch at 20 μg/hour.
What is the most appropriate postoperative analgesic regimen for this patient?
A. Paracetamol, ibuprofen, gabapentin, MST 25 mg twice daily, Oramorph 10–
20 mg 4-hourly
B. Paracetamol, diclofenac, a morphine PCA 2 mg bolus with 5 minute lockout
C. Paracetamol, ibuprofen, gabapentin, fentanyl PCA with 25 μg bolus with 5
minute lockout
D. Paracetamol, codeine, tramadol and Oramorph 10–20 mg 4-hourly
E. Paracetamol, ibuprofen, gabapentin, Oxynorm 15 mg twice daily
23. A 35-year-old man with a chronic history of intravenous heroin use and
schizophrenia presents to the emergency department with a perforated duodenal
ulcer. He is septic, coagulopathic and haemodynamically unstable, so is rushed to
theatre for resuscitation and an emergency laparotomy.
What is the most appropriate analgesic regimen to manage his postoperative pain?
333
334
Chapter 9
A
B
C
D
E
Thoracic epidural with plain bupivacaine
Intravenous methadone and ketamine infusion
Oral methadone and intravenous morphine as required
Intravenous methadone and intravenous morphine as required
Morphine patient controlled analgesia (PCA) with a background infusion
24. A 68-year-old woman with advanced breast cancer and poor intravenous access
is suffering from intractable bone pain in her distal right femur. A recent MRI scan
has confirmed a solitary metastases in her right femur and ruled out a fracture.
Management is at a palliative stage and she is currently taking paracetamol,
ibuprofen and morphine sulphate.
What is the most appropriate next step in controlling her pain?
A
B
C
D
E
Internal fixation of femur
Bisphosphonates
Localised external beam radiotherapy
Radioisotope treatment
Gabapentin
25. A 75-year-old woman with metastatic breast cancer is currently on 70 mg MST
twice a day and 20 mg of Oramorph 4-hourly for breakthrough pain. She continues
to suffer from back pain. An MRI excludes any cord compression but confirms the
presence of vertebral bone deposits.
What is next best step in treating her pain?
A
B
C
D
E
Converting the patient to oxycodone
Start calcitonin
Increase the dose of MST
Radiotherapy
Start bisphosphonates
26. A 22-year-old man is brought into a district general emergency department after
being pulled from a burning house with 35% body surface area burns. They include
partial thickness facial and anterior chest wall burns. He has a hoarse voice with
carbonaceous sputum. His Glasgow coma score is 15 and other observations are as
follows:
• Heart rate 98 beats per minute
• Blood pressure 169/82 mmHg
• Respiratory rate 25 breaths per minute
• Saturations 100% on high flow oxygen
• Temperature 38.0°C
There are no other injuries.
What is the most appropriate immediate course of action?
Questions
A
Perform a modified rapid sequence induction with alfentanil, propofol and
rocuronium and intubate with a size 8.0 cuffed oral tracheal tube cut to 24 cm
to reduce dead space
B Perform a rapid sequence induction with thiopentone and suxamethonium
using an uncut size 8.0 cuffed oral tracheal tube
C Refer and transfer to regional burns centre without delay for definitive
treatment
D Give 200 mg hydrocortisone intravenously
E Give 1.5 g ceftriaxone intravenously
27. One of the high dependency unit nurses calls you to review a 73-year-old woman
72 hours post-carotid endarterectomy. The patient appears confused, agitated
and her blood pressure is 210/100 mmHg. The nurse administered 1 g of oral
paracetamol for a persistent headache 1 hour ago after which the patient vomited.
What is the next most appropriate step in the management of her condition?
A
B
C
D
E
Administer a broad spectrum intravenous antibiotic
Administer 50 mL of 20% mannitol
Catheterise the patient
Administer a stat dose of oral amlodipine 10 mg
Administer a bolus dose of intravenous labetalol 10 mg
28. A 38-year-old man scheduled to have a revision of his arteriovenous fistula in the
next 8 weeks is being assessed in the anaesthetic pre-assessment clinic. He suffers
from chronic kidney disease and is on dialysis. His recent blood count shows a
haemoglobin of 68 g/L with a low reticulocyte but a normocytic mean corpuscular
volume.
The most appropriate preoperative strategy for treating this patient's anaemia is:
A
B
C
D
E
Blood transfusion
Human erythropoietin
Perioperative blood transfusion
Folic acid injections
Vitamin B12 injections
29. A 34-year-old parturient had epidural analgesia for a full-term normal delivery. 4
days later, she complains of constant severe back pain along with paraesthesia in
her left leg. On examination she is febrile and has a motor power of 4/5 in both of
her legs and normal power in her upper limbs.
The immediate investigation of choice would be:
A
B
C
D
E
Lumbar puncture
MRI lumbar spine
MRI whole spine
C-reactive protein (CRP)
Erythrocyte sedimentation rate (ESR)
335
336
Chapter 9
30. You are reviewing a study that randomised two groups of patients to receive
sedation either at the discretion of the caregivers or by following a strict protocol.
The study hypothesis is that protocolisation reduces the total cumulative dose of
sedative medications.
Which of the following statistical tests would be most appropriate to analyse the
results of this pilot study?
A
B
C
D
E
Unpaired Student's t-test
Paired Student's t-test
Chi Squared test
Mann-Whitney U test
Paired ANOVA
Answers
Answers
1. B Paco₂
This patient is showing signs of raised intracranial pressure (ICP) from an, as yet,
undiagnosed cause. The dilated pupil infers imminent risk of coning. The priority is
to reduce ICP and optimise cerebral perfusion to prevent secondary ischaemia.
Ordinarily, cerebral blood flow (CBF) is autoregulated across a range of cerebral
perfusion pressure (CPP) (Figure 9.1). This mechanism is uncoupled in the event of
traumatic brain injury (TBI).
Figure 9.1 Graph illustrating
how cerebral blood flow varies
with cerebral perfusion pressure.
Autoregulation prevents
variations in blood flow across a
range of perfusion pressures.
Cerebral blood flow
(mL/100g/min)
100
50
0
50
100
150
Cerebral perfusion pressures (mmHg)
The CBF, therefore, becomes directly proportional to the CPP. As the intracranial
contents are held within a rigid skull, any increase in volume of those contents (e.g.
with haemorrhage) opposes CBF to the brain. ICP must now be considered when
calculating CPP. This relationship is described by the following equation:
CPP= MAP–ICP
In the event of TBI, factors that affect MAP and ICP are evaluated when optimising CPP.
Ventilation (Figure 9.2): The current aim for Pao₂ is > 13 kPa to provide adequate
substrate for cerebral metabolism as hypoxia is known to be associated with a worse
outcome. The reactivity of CBF to Paco₂ remains relatively robust in the event of TBI
and subsequently hyperventilation, leading to reduced CBF, may rapidly reduce ICP.
However, if subnormal levels (< 4.0 kPa) are achieved it is at the expense of perfusion
leading to further cerebral ischaemia. It is therefore advisable to aim for Paco₂ 4.5–
5.0 kPa.
Blood pressure: Increasing MAP may further increase ICP but, in an injured brain,
this may be required to perfuse in the presence of a space occupying lesion.
It is therefore suggested that a target MAP of 80–90 mmHg is maintained. This
can be achieved using intravenous fluid +/– vasopressors. Analgesia should be
administered to obtund any sympathetic response to pain.
337
Chapter 9
Cerebral blood
flow (mL/100g/min)
338
100
Pa CO2
50
Pa O2
0
5
10
15
Partial pressure (kPa)
Figure 9.2 Graph demonstrating
the effect of different partial
pressures on CBF. Between 5-10
kPa Paco2, cerebral blood flow
increases linearly with Paco2,
above and below which there is
no further impact on CBF. Above
a Pao2 of 8 kPa CBF is constant,
but below 8 kPa there is a rapid
rise in CBF.
20
Cerebral metabolism: Reducing cerebral metabolism with sedation and induction
agents results in a reduction in cerebral requirements. There is nothing conclusive,
as yet, regarding induced hypothermia, and normothermia remains the aim.
Actively warming someone is deleterious. Hyper- and hypoglycaemia confer a worse
outcome. A blood glucose < 10 mmol/L is therefore the aim.
Fluid management: A normal circulating blood volume is required to maintain MAP.
Fluid shifts may occur due to an ineffective blood brain barrier and are governed
by plasma osmolality, not oncotic pressure. Coupled with this knowledge is the use
of hypertonic saline and mannitol to manipulate the volume of oedematous brain
tissue and thereby the ICP.
Mechanical increases in ICP via increased venous pressure: Neck ties should be
avoided. Mechanical ventilation should be facilitated by the use of muscle relaxant
to avoid coughing. The patient should be nursed with a head -up tilt.
The priority in this man is to correct the abnormal Paco₂ to 4.5–5.0 kPa before
attending to the stabilisation of the other values. As can be seen from Figure 9.1,
this will have the most significant impact on this patient's CBF.
Pollard BJ (ed). Handbook of Clinical Anaesthesia, 2nd edn. London: Elsevier Science, 2003.
Allman K, Wilson I (eds). Oxford Handbook of Anaesthesia, 2nd ed. Oxford: Oxford University Press, 2006.
Rangel-Castillo L, Gopinath S, Robertson C. Management of Intracranial Hypertension. Neurol Clin
2008;26(2):521–541.
2. B Ask the surgeon to site a paravertebral catheter
The aims of analgesia in this scenario are:
• To use a technique that covers the wide surgical field: The camera is inserted at
approximately T8 in the mid clavicular line, with ports between T9 +/– T5. Further
pain may be felt from any trauma to the parietal pleura adjacent to the right
upper lobe
• To allow thoracotomy and rib resection if required: The rate of conversion to
open thoracotomy is around 10%, and the need for a lymphadenectomy, which
may be technically difficult, may increase this conversion rate further
• To provide effective intra- and postoperative analgesia: The patient has
significant respiratory disease and effective analgesia will allow extubation,
Answers
spontaneous ventilation and coughing. Prompt extubation reduces the risk of
ventilator associated complications in the critical care unit, therefore option C is
not the best choice here
Although thoracic epidural analgesia is seen as the gold standard for this scenario,
injection of local anaesthetic into the paravertebral space aims to block spinal
nerves as they leave the intervertebral foramina; providing unilateral analgesia with
a degree of sympathetic blockade. A single shot injection may give analgesia for
over 20 hours but use of a catheter allows infusion of local anaesthetic in the post
operative period and is the best option of those listed here (option B).
In light of failed attempts to site a thoracic epidural, it may be kinder to perform
further procedures when the patient is asleep; surgically placed catheters during
VATS have been described and it would be worth asking the surgeon whether they
can perform this procedure in the first instance.
Intrapleural local anaesthetic, that is administration of local anaesthetic into the
space between the parietal and visceral pleura, would diffuse around the intercostal
nerves as they travel between the inner and innermost intercostal muscles.
However, disruption of the pleura leads to erratic absorption, potential leakage
into any intercostal drains sited and so less effective analgesia. Systemic absorption
via this route is high so option D is neither the safest nor the most effective of
those given. Intercostal blocks (option E) in general do not have adequate duration
for this scenario and offer inadequate analgesia compared with paravertebral
techniques.
Tighe, SQM, Greene MD, Rajadurai N. Paravertebral block. Contin Educ Anaesth Crit Care Pain 2010;
10(5):133–137.
3.B Needle thoracocentesis followed by insertion of 22F
intercostal drain
The clinical signs are suggestive of a massive air leak, possibly from breakdown
of the bronchial stump. There are signs of cardiovascular impairment (including
paradoxical bradycardia) suggesting impending cardiovascular collapse. The most
likely diagnosis is a bronchopleural fistula leading to tension pneumothorax that
should be decompressed immediately by needle thoracocentesis. Other diagnoses
could include delayed infection and bleeding so it would be prudent to follow
needle decompression with a larger bore (22F) intercostal drain. A smaller 12F
drain inserted via the Seldinger technique may not drain blood/purulent matter
adequately and takes more time to site. Obtaining a chest radiograph often takes
time that may be detrimental in this scenario.
Risk factors for bronchopleural fistulae include increased age, poor wound healing,
pneumonectomy, previous chemo/radiotherapy and prolonged mechanical
ventilation postoperatively.
Although bronchoscopy +/– CT thorax may be needed to make the diagnosis and
assess for any other complications (e.g. empyema) when the patient stabilises, the
priority is restoration of oxygenation and adequate cardiovascular parameters.
339
340
Chapter 9
Early bronchial stump breakdown often requires surgical treatment with direct
closure or coverage with an intercostal flap.
Darling GE, Abdurahman A, Yi QL, et al. Risk of a right pneumonectomy: role of bronchopleural fistula.
Ann Thorac Surg 2005; 79(2):433.
4. A Hypoxia
Foreign body aspiration is a dangerous condition most frequently seen in infants
where inadvertent aspiration of objects disrupts the normal airway structure and
function. The classic triad of symptoms consists of paroxysmal coughing, wheezing
and reduced breath sounds on the affected side occurring after a witnessed choking
episode. It is a leading cause of death in 1–3 year olds and its safe management is
challenging to both surgeon and anaesthetist.
The gold standard for managing foreign body aspiration in children is removal via
rigid bronchoscopy under general anaesthesia. The instrument most commonly
used in children is the Storz ventilating bronchoscope which consists of a metal
tube and a removable optical scope (Hopkins rod). During instrumentation, the
optical scope is within the lumen of the bronchoscope and provides excellent
visualisation of the airway. The scope however significantly reduces the lumen
of the bronchoscope available for ventilation and should only be used for short
periods. Hypoventilation is a real possibility especially if the patient is spontaneously
ventilating.
Bradycardias during bronchoscopy are uncommon and should be assumed to be
secondary to hypoxia until proven otherwise. Hypoxia can occur if the scope is
placed in a bronchus or if instrumentation triggers bronchospasm. Furthermore,
when excessive suctioning is performed, there may be atelectasis and a reduction
in the inspired oxygen concentration. Also, a feared complication which can cause
hypoxia acutely is dislodgement of the foreign body into the trachea creating
complete obstruction of the airway.
In order to reduce the risk of foreign body dislodgement whilst allowing
spontaneous ventilation, anaesthesia needs to be deep enough to minimise
coughing and moving without paralysis. Excessive anaesthesia to achieve this can
trigger bradycardias, but it is not the most likely cause in the above scenario. The
arrhythmia occurred after prolonged instrumentation which would have restricted
the spontaneous ventilation and elevated the boy to a lighter plane of anaesthesia.
Children are commonly affected by inhaled foreign bodies and it is important for the
anaesthetist to also be aware of the challenges of paediatric anaesthesia. Children
are at more risk of becoming hypothermic during anaesthesia which if severe, can
cause arrhythmias. The patient's core temperature in the above case however is
highly unlikely to be sufficiently low to produce this response.
There are vagal sensory nerves within the conducting airways and stimulation
by bronchoscopy can cause reflex spasm and bradycardia. Coughing during
bronchoscopy may also illicit a vagal response. The fact that the bradycardia
occurred after prolonged instrumentation (as opposed to during), and no coughing
occurred makes this diagnosis less likely.
Answers
Hypercarbia occurs frequently during rigid bronchoscopy, particularly in spontaneously
ventilating patients and where there is frequent use of the optical scope or forceps
restricting ventilation. Hypercarbia however is more likely to cause an initial tachycardia
as opposed to a bradycardia due to an increased sympathoadrenal tone.
Roberts S, Thornington R. Paediatric bronchoscopy. Contin Educ Anaesth Crit Care Pain 2005; 5(2):41–44.
Farrell P.Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation. Paediatr Anaesth
2004; 14(1):84–89.
5.B Has an adult relative to act as carer at home only until
20.00
In the ‘ten high impact changes’ document published by the NHS Modernisation
Agency it is outlined that day surgery, rather than inpatient surgery, should be
treated as the norm for all elective surgery. Locally agreed protocols exist in most
day case units for selection and exclusion criteria. These fall broadly into medical,
surgical and social considerations (Table 9.1).
Table 9.1 Selection criteria that should be met for appropriateness for day case surgery.
Medical
Surgical
Social
Preoperative assessment of a
patient’s health status should
be made to determine eligibility
rather than use of arbitrary limits,
e.g. BMI, ASA, age
Procedure should not pose any
serious complications, e.g. risk of
haemorrhage and cardiovascular
instability
Patients must understand
procedure, postoperative
care and be able to consent
to day surgery
Chronic stable disease may be
better treated as day case
Oral medications and local
anaesthetic techniques should
be sufficient to manage post
operative symptoms
A responsible adult should
escort the patient home and
be present for the first 24
hours postoperatively
Procedure should not prevent
resumption of oral intake within
a few hours
Domestic circumstances
should be appropriate for
postoperative care
Patients should be able to
mobilise but full mobilisation is
not always required
It is important to note that patients can be discharged with residual effects after
nerve blockade so long as the duration of effects are explained and the patient has
received written and verbal instructions of what to expect. Mandatory oral intake
and ability to void are no longer considered essential discharge criteria unless
manipulation of the bladder has occurred. Distance from the hospital should be
individually assessed, but some units set 60 minutes as a practical limit. An escort
home and for the first 24 hours are still necessary although this may be relaxed in
the future for minor procedures with very short anaesthetics where patient is not
compromised by the time of discharge.
Verma R, Alladi R, Jackson I, et al. Day case and short stay surgery: 2. Anaesthesia 2011: 66;417–434.
341
342
Chapter 9
6.A Ensuring 18 hours after the last dose of rivaroxaban, give a
spinal, and then start a heparin infusion postoperatively
Vast numbers of patients present for surgery on antiplatelet drugs. The perioperative
management of these medications commonly falls to anaesthetists to coordinate,
and there is a significant overlap also in the assessment of cardiac risk for noncardiac surgery. A solid understanding of these issues will help in preparation for
both the written and viva elements of the Final FRCA.
Aspirin and clopidogrel
Aspirin is an irreversible inhibitor of platelet cyclooxygenase (COX), and thus normal
platelet function relies on new platelet manufacture, which takes approximately 7
days. Aspirin is not contraindicated in central neuraxial blockade (CNB), as the risk of
haematoma is not elevated.
Conversely, clopidogrel is associated with haematoma formation in case reports. It
is a thienopyridine adenosine diphosphate (ADP) blocker, and published advice is to
avoid for at least 7 days prior to CNB. Prasugrel, a more potent thienopyridine, should
be avoided for 7–10 days and not restarted until 6 hours after block or catheter
removal, where clopidogrel can be given just afterwards.
Tirofiban/abciximab
These two are glycoprotein IIb/IIIa blockers, in the case of abciximab this is via
binding of a monoclonal antibody. Tirofiban is the shorter acting of the two, and
CNB can be attempted after 8 hours, whereas antibody persistence means a duration
of 24–48 hours is needed for abciximab.
Warfarin
An international normalised ratio (INR) of ≤ 1.5 is known to be associated with
clotting factor levels of > 40% and is regarded as safe for CNB.
Dabigatran/rivaroxaban
Dabigatran is an oral thrombin inhibitor only licensed for venous thromboembolism
(VTE) prophylaxis after surgery. CNB should not be established in patients already
on this drug, as it is contraindicated by the manufacturer. It can be started 6 hours
after the risk period. Rivaroxaban is a direct oral inhibitor of factor Xa. It is becoming
more common as the list of approved indications increases. Previously only for
postoperative VTE prophylaxis, it is now being used in AF and in Europe as an
adjunct to aspirin and clopidogrel in acute coronary syndromes. CNB should be
12–18 hours post-dose, and the drug should only be given 6 hours after a block or
catheter removal.
Heparins
With the low molecular weight heparins (LMWH), the duration between
administration and safe block depends on dosage. Therapeutic dose requires a 24hour delay, whereas prophylactic dose, a gap of 12 hours. In both cases 2–4 hours is
the duration until restarting following block or catheter removal.
Answers
Fondaparinux
Fondaparinux is another factor Xa inhibiting drug, although with a long half-life
of 21 hours. It has little effect on thrombin and no antiplatelet effect. At treatment
doses no CNB is permitted, but in prophylactic doses, CNB can be performed after
36 hours, with 6 hours to elapse before the next dose, but 12 hours after epidural
catheter removal.
Use of dual antiplatelet therapy (DAPT) is essential for the prevention of stent
thrombosis following coronary stenting, particularly after a drug eluting stent.
Here the minimum recommended time for DAPT is normally 12 months, and for
stopping or withholding DAPT, the cardiac risk of stent thrombosis often exceeds the
operative risks of bleeding. This gentleman has been off clopidogrel greater than the
minimum of 7 days, such that his clopidogrel is no longer an issue.
However, the confounding issue is now the rivaroxaban, which is appearing in the
drug history of more and more patients. Mainly used for postoperative venous
thromboprophylaxis there are now indications for atrial fibrillation and in the
treatment of acute coronary syndrome patients. The recommended omission
time here is 12–18 hours, and restarting should be 6 hours after block or catheter
removal. The other important safety issue with rivaroxaban is the lack of any
mechanism of reversal, which probably makes its use here in the immediate
postoperative phase unwise. Therefore the safest approach for this patient is to have
the required 18 hours off rivaroxaban before preforming a spinal anaesthetic with a
heparin infusion postoperatively.
Davies G, Checketts MR. Regional anaesthesia and antithrombotic drugs. Contin Educ Anaesth Crit Care
Pain 2013; 12(1):11–16.
7. B Lingual nerve injury
The laryngeal mask airway (LMA) is a versatile supraglottic airway device which
consists of a tube connected to an inflatable cuff which surrounds a mask designed
to seal off the laryngeal inlet from the gastrointestinal tract. However, it is not a
definitive airway and vigilance against aspiration is advised particularly when used
in conjunction with positive pressure ventilation. Another recognised complication
associated with laryngeal mask airway ventilation is pressure neurapraxia to
anatomically vulnerable nerves within the pharynx or oral cavity.
A neurapraxia refers to a localised and transient conduction block along a nerve
without any anatomical interruption, which in the above case is likely to be caused
by pressure from the cuff. Predisposing factors include the use of nitrous oxide, cuff
over-inflation, using an undersized laryngeal mask airway, the lateral position and a
difficult insertion.
The lingual nerve is a branch from the mandibular division of the trigeminal
nerve and supplies sensory innervation to the anterior 2/3 of the tongue. It also
carries sensory taste fibres from the anterior tongue to the facial nerve via the
chorda tympani. Damage to the lingual nerve characteristically produces a loss of
sensation and taste confined to one side of the anterior tongue without any motor
dysfunction. Although rare, lingual nerve neurapraxia is a recognised complication
343
344
Chapter 9
of laryngeal mask use and is the most likely pathology in the above scenario. The
lingual nerve is vulnerable to compression as it enters the mouth below the superior
constrictor and continues against the medial aspect of the mandible.
The hypoglossal nerve carries purely motor fibres and supplies all the intrinsic
muscles of the tongue. Like its name suggests, it can be found below the tongue
and is vulnerable to compression as it travels above the hyoid bone. Case reports
of damage to this nerve following LMA usage have been documented, although
the symptoms and signs are different from the case above. Sufferers may complain
of difficulties in swallowing, articulating speech and the tongue feeling ‘heavy’.
The protruded tongue will also deviate towards the side of the lesion due to the
unopposed action of the contralateral genioglossus muscle.
The recurrent laryngeal nerve is a branch of the vagus nerve which conveys sensory
and motor innervation to the larynx. This nerve can also be damaged following LMA
siting and symptoms include dysphonia, stridor, dysphagia and postoperative lung
aspiration, but not tongue paraesthesia as in the case above. The recurrent laryngeal
nerve is at risk of being compressed against the cricoid cartilage as it enters the
larynx at the apex of the piriform fossa.
The inferior alveolar nerve is the largest branch of the mandibular division of
the trigeminal nerve, and supplies motor fibres to the floor of the mouth and
sensory innervation to the lower teeth and chin via the mental nerve. Commonly
anaesthetised for dental procedures, blockage of this nerve can also occur following
LMA use. The nerve runs a superficial course between the last molar and the ramus
of the mandible, making it vulnerable to compression there. The featured case
lacked dental or facial symptoms, making this answer incorrect.
The LMA can also impede the venous drainage of the tongue and there have been
case reports of postoperative oedema and cyanosis with or without associated
tongue paraesthesia. The venous drainage of the tongue occurs via the dorsal and
deep lingual veins which can potentially be occluded by the LMA. In the case above,
the normal appearance of the tongue counts against this diagnosis.
Twigg S, Brown JM, Williams R. Swelling and cyanosis of the tongue associated with the use of a laryngeal
mask airway. Anaesth Intensive Care 2000; 28:449–450.
Hanumanthaiah D, Masud S, Ranganath A. Inferior alveolar nerve injury with laryngeal mask airway: a case
report. J Med Case Rep 2011; 5:122.
Brimacombe J, Clarke G, Keller C. Lingual nerve injury associated with the ProSeal laryngeal mask airway:
a case report and review of the literature. Br J Anaesth 2005; 95(3):420–423.
Lowinger D, Benjamin B, Gadd L. Recurrent laryngeal nerve injury caused by a laryngeal mask airway.
Anaesth Intensive Care 1999; 27:202–205.
8. A Alert radiologist
General anaesthesia is often used for aneurysm coiling as it allows control over
parameters to provide optimal cerebral perfusion pressure (CPP), and provides an
immobile patient. These procedures are carried out often in a site remote from the
theatre complex and can be long.
A sudden rise in blood pressure should alert the anaesthetist to the possibility of
aneurysm rupture, which has an intraoperative incidence of 2–19%. Rupture can
Answers
occur spontaneously, during induction, or as a result of guidewire, microcatheter
or coil placement. The priority during induction of anaesthesia is to avoid a
hyperdynamic response to laryngoscopy, whilst maintaining adequate cerebral
perfusion pressure. The pressor response can be attenuated using co-induction with
short acting opiates and beta-blockers and confirming adequacy of muscle paralysis
prior to intubation.
Signs of rupture and bleeding under anaesthesia may be subtle and the
radiologist should be immediately alerted of any sudden haemodynamic
changes. Depending on the stage of procedure and degree of bleeding, coiling
may continue, but transfer to theatre may be required for ventriculostomy
or rescue craniotomy and clipping, so assistance should be sought early. The
other options in this question are appropriate actions but should follow after
communication of the changes to the radiologist in case of rupture. Interventions
can then be made to control arterial pressure by deepening anaesthesia or using
beta-blockers and if necessary to control intracranial pressure by head elevation,
maintaining Paco₂ to 4.5–5.0 kPa, administering mannitol or reversing any heparin
administered with protamine.
Other complications that can occur during these procedures are thromboembolic or
iatrogenic occlusion of a vessel, vasospasm, contrast reactions, and displacement of
lines and tubes by movement of the image intensifier.
Dorairaj IL, Hancock SM. Anaesthesia for interventional neuroradiology. Contin Educ Anaesth Crit Care
Pain 2008: 8(3); 86–89.
Varma MK, Price K, Jayakrishnan V, Manickam B, Kessell G. Anaesthetic considerations for interventional
neuroradiology. Br J Anaesth 2007: 99(1);75–85.
9. B 10 mL of 0.25% levobupivacaine
Caudal epidural analgesia is the commonest regional technique used in children. It
is suitable for all infraumbilical surgery, including hypospadias repair, circumcision
and inguinal or umbilical hernia repair. It provides a reliable block between T10 and
S5 in children less than 20 kg. The combination of minimal side effects and excellent
analgesia make it suitable for day case surgery.
Since motor block is poorly tolerated in awake children, local anaesthetic choice
prioritises weakest motor block and the long lasting analgesic effects possible.
Although bupivacaine meets these criteria, levobupivacaine and ropivacaine are the
drug of choice in paediatric practice. They produce a differential block by preserving
the motor function with the same analgesic effect. They also have less cardiac and
central nervous system toxicity.
The volume of caudally injected local anaesthetic determines the spread of the block
and must be adapted to the procedure. Doses described by Armitage are the most
frequently used regimen in current paediatric practice:
Sacro-lumbar block: 0.5 mL/kg, 0.25% bupivacaine or levobupivacaine
Upper abdominal block: 1 mL/kg, 0.25% bupivacaine or levobupivacaine
Mid-thoracic block: 1.25 mL/kg, 0.25% bupivacaine or levobupivacaine
345
346
Chapter 9
The addition of clonidine (1–2 μg/kg) and preservative-free ketamine (0.5 mg/kg)
increases the duration of analgesia by 5–10 hours. Both drugs at higher dose are
associated with a greater risk of sedation, apnoea or nausea, and therefore should
be avoided in day case surgery. In option D, the dose of clonidine is higher than the
recommended dose.
Morphine 50 μg/kg or diamorphine 30 μg/kg may increase the duration of analgesia
by 24 hours. However, they commonly cause unpleasant side effects such as nausea
and pruritus, and have a risk of delayed respiratory depression. Opioid additive to
the local anaesthetic agents should be avoided in day case surgery settings because
of the side effects, and is therefore inappropriate in this scenario.
Fentanyl, however, does not prolong the duration of analgesia and significantly
increases the incidence of nausea and vomiting thus would be unsuitable in this
scenario.
Lönnqvistand PA, Morton NS. Postoperative analgesia in infants and children. Br J Anaesth 2005;
95(1):59–68.
Patel D. Epidural analgesia for children. Contin Educ Anaesth Crit Care Pain 2006; 6(2):63–66.
Armitage EN. Regional anaesthesia. In: Sumner E, Hatch DJ (eds). Textbook of Paediatric Anaesthetic
Practice. London: Balliere Tindall, 1989: 213–33.
10. B A paramedian mid-thoracic epidural under light
sedation or awake
Thoracic epidural analgesia is commonly used in cardiothoracic surgery for
providing sympatholysis and pain relief during and after operations. The main
objective is to allow cardiothoracic pain-free patients to breath adequately, cough
and cooperate with chest physiotherapy.
A good anatomical knowledge is essential for successful epidural block. The spinous
processes of cervical, thoracic and lumbar vertebrae have different alignment. They
are posteriorly directed and relatively straight at the cervical, lower thoracic and
lumbar levels. However, they are caudally inclined in the high- and mid-thoracic
regions. The highest degree of angulation is at T3–T7, making the paramedian
approach easier at this level.
A thoracic epidural catheter for thoracic surgery is usually sited at a level
corresponding to the upper dermatomal level of the incision, most commonly in
the mid-thoracic level (T6–T7). In this example, an upper lumbar approach will not
provide adequate analgesia.
Always examine patient’s back and identify the bony landmarks before inserting
thoracic epidural needle. Classical landmarks are spine of scapula at T3 and the
inferior angle of scapula at T7. You can confirm the correct interspace by counting up
from L3/4.
Thoracic epidural anaesthesia is better performed in a lightly sedated or awake
patient. Insertion of an epidural needle in the lightly sedated/awake patient has two
advantages: pain and/or paraesthesia warn of any potential neurological damage;
and the sensory block extension can be examined before commencing general
Answers
anaesthesia. Thus in the above clinical scenario, a paramedian mid-thoracic epidural
in a lightly sedated or awake patient would be most appropriate.
McLeod GA, Cumming C. Thoracic epidural anaesthesia and analgesia. Contin Educ Anaesth Crit Care Pain
2004; 4(1):16-19.
McLeod G, Davies H, Munnoch N, Bannister J, MacRae W. Postoperative pain relief using thoracic epidural
analgesia: outstanding success and disappointing failures. Anaesthesia 2001; 56:75–81.
Hughes R, Gao F. Pain control for thoracotomy. Contin Educ Anaesth Crit Care Pain 2005; 5(2):56–60.
11. E 0.5 μg/kg fentanyl followed after several minutes by
small doses of intravenous midazolam titrated to effect
Sedation is required in a myriad of clinical settings and across many specialties.
Complications arise not uncommonly and not just from the inappropriate use
of agents, but from the inadequate skills and training of operators, poor patient
assessment, and lack of or failure to use appropriate levels of monitoring. Despite
the fact that anaesthetists have the detailed knowledge and skills required to give
sedation safely, few had received any formal training in sedation per se. Thus, since
August 2010, the curriculum for anaesthetic training now includes sections on
sedation.
Pre-assessment
Poor or absent pre-assessment is a theme common to many adverse events in
sedation practice. Thus, the pre-assessment must be thorough, and to the same
standard as that required for formal general anaesthesia. This must include all
relevant drugs, allergies, comorbidities and an airway assessment to predict features
associated with difficult intubation and/or mask ventilation.
Monitoring
Guidance recommends the use of non-invasive blood pressure, pulse oximetry
and ECG which may be modified to suit the needs of the patient, or the degree of
sedation being provided. Verbal communication is essential as a monitor of depth of
sedation, and if verbal communication is lost the patient requires the same standard
of care as for general anaesthesia. Capnography is very useful, and may be essential
where clinical assessment during the case is limited by access to the patient, e.g.
MRI. Some would recommend capnography for all patients.
Levels of sedation
• Minimal: Normal verbal response, airway normal and responds to pain
• Moderate: Responds purposefully to voice or pain, no airway intervention
required
• Deep: Only responds after repeated pain, may need airway and ventilator support
Principles and drugs
• Single agents are easier to titrate and tend to be safer
• Synergistic effects (e.g. benzodiazepines following an opioid), may increase risks
by reducing safety margins
347
348
Chapter 9
• Anaesthetic agents such as propofol and remifentanil have narrow therapeutic
windows and thus reduced safety margins
• Painful procedures need to include an analgesic agent
• In an opioid/benzodiazepine combination technique, the opioid should be given
and allowed to have a full effect. Then small amounts of benzodiazepine may be
titrated to effect
• Loss of verbal contact requires the same standard of care as for a general
anaesthetic
The key here is that the procedure (and also the positioning) itself is uncomfortable,
even with local anaesthesia infiltration. The patient also takes an opioid in the
community, and has established chronic back pain. Thus analgesia is essential.
Ketamine would provide sedation and analgesia, but the sympathomimetic effects
may be best avoided in the setting of her angina, the severity of which is not stated.
Remifentanil, despite being a nearly ideal short-acting opioid, carries the significant
risk of respiratory suppression. Thus the best combination is fentanyl, followed later
by small aliquots of midazolam.
Blayney MR. Procedural sedation for adult patients: an overview. Contin Educ Anaesth Crit Care Pain 2012;
12 (4):176–180.
12. D < 10 mmol/L
Whilst poor glycaemic control is associated with worse morbidity and mortality, the
optimal glucose level remains controversial. Early trials suggested benefit from tight
glycaemic control (4–6 mmol/L), however recent evidence suggest that there is no
additional benefit and in fact, may cause possible harm.
Leuven I was a single centre trial of surgical intensive care unit patients comparing
intensive (tight) to conventional glucose control. The results suggested a 34%
decrease in mortality with tight glucose control, with additional reductions in the
occurrence of sepsis, acute renal failure and critical illness polyneuropathy. However
these results were not concurred in a subsequent trial (Leuven II) by the same
author in medical intensive care patients. The uncertainty lead to a large multicentre
randomised control trial (Normoglycemia in Intensive Care Evaluation-Survival
Using Glucose Algorithm Regulation; NICE SUGAR) in 2009. 6,000 patients were
randomised to tight (4.5–6 mmol/L) or conventional glucose control (< 10 mmol/L).
The results of NICE SUGAR suggested an increase in mortality (27.5% vs 24.9%) and
a significant increase in hypoglycemic events (6.8% vs 0.5%) in the tight versus the
conventional glucose control groups. The trial evidence was incorporated into the
‘2010 International recommendations for glucose control in the adult non-diabetic
critically ill’:
• < 10 mmol/L strongly suggested
• severe hypoglycemia is defined as < 2.2 mmol/L
• glucose levels should be sampled from arterial rather than capillary or venous
blood, using laboratory or blood gas analysers rather than point of care anaylsers
This is reiterated in the 2012 Surviving Sepsis guidelines:
Answers
1. A protocolised approach to blood glucose management in ICU patients with
severe sepsis commencing insulin dosing when two consecutive blood glucose
levels are > 180 mg/dL (> 10 mmol/L). This protocolised approach should target
an upper blood glucose ≤ 180 mg/dL rather than an upper target blood glucose
≤ 110 mg/dL (< 6.1 mmol/L)
2. Blood glucose values be monitored every 1–2 hours until glucose values and
insulin infusion rates are stable and then every 4 hours thereafter
3. Glucose levels obtained with point-of-care testing of capillary blood be
interpreted with caution, as such measurements may not accurately estimate
arterial blood or plasma glucose values
Based on these recent guidelines, option D is most appropriate. However this
remains a subject for debate and questions remain whether an interim between
current practice and the intensive glucose targets may be optimal or whether tight
glucose control are in fact beneficial in subgroups of patients.
Egi M, Finfer S, Bellomo R. Glycemic control in the ICU. Chest 2011; 140(1):212–220.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: International guidelines for
management of severe sepsis and septic shock. Crit Care Med 2013; 41:580–637.
13. A Propofol and fentanyl
Sedation protocols are diverse and consideration of the purpose of sedation, patient
characteristics and the pharmacology of the sedative agents should guide the
decision. The purpose of sedation is to allow a reduction in patients’ awareness and
their response to external stimuli. Under-sedation results in hypercatabolism and
increased sympathetic activity, which can have detrimental effects, for example
myocardial ischaemia. However, oversedation is problematic resulting in increased
mechanical ventilation days, respiratory and cardiovascular depression, delayed
neurological recovery and impairs muscular rehabilitation. It is important that
sedation is titrated to the individual patient’s requirement; scoring systems such as
the Richmond Agitation Sedation Scale (RASS) aid this.
In this example, the patient has been involved in a high speed injury and sustained
a neurological injury and a severe thoracic injury. While the extent of his injuries
are ascertained it is sensible to keep him sedated. Clearly in this patient, who has
escalating ventilator requirements, potentially life threatening injuries such as a
pneumothorax need to be excluded. However, the extent of his neurological injury
will need to be assessed at the earliest opportunity, necessitating an early sedation
hold.
Sedation techniques comprise of non-pharmacological and pharmacological.
Non-pharmacological techniques can be used to reduce anxiety and improve
sleep such as frequent communication, day/night orientation and music therapy.
Pharmacological agents can augment this approach, providing analgesia, anxiolysis,
hypnosis and amnesia. The can be classified as inhalational or intravenous
anaesthetic agents (such as propofol), benzodiazepines (e.g. midazolam, diazepam
and lorazepam), opioids (e.g. fentanyl, alfentanil, remifentanil), α2 agonists (such
as clonidine and the newer dexmedetomidine) and neuroleptic agents (such as
haloperidol and chlorpromazine).
349
350
Chapter 9
In the example of a patient who has sustained extensive chest wall injuries, an
opioid to provide analgesia would seem sensible. Whilst clonidine would also
provide an analgesic component, it can result in haemodynamic compromise and is
unadvisable until visceral or vascular injury has been excluded.
While a pure opioid regime can in theory provide an element of hypnosis, in practice
this is difficult to achieve. The ideal characteristic of the choice of hypnotic agent
should include ease of titration, short half-life, minimal pharmacodynamics adverse
effect, cheap and familiar to both nursing and medical teams.
Of the agents listed, propofol is closest to these ideal characteristics. Midazolam
has active metabolites and there are concerns regarding dependence. Ketamine
provides dissociative anaesthesia with associated neuropsychiatric sequelae.
Ketamine is also a sympathomimetic which may be detrimental especially in the
presence of a severe head injury.
Recent trials show promise with dexmedetomidine, when compared to propofol and
midazolam. However it remains expensive and is still associated with significant side
effects, so its role in the intensive care needs to be further investigated.
Rowe K, Fletcher S. Sedation in the intensive care unit. Contin Educ Anaesth Crit Care Pain 2008; 8(2):50–55.
Jakob SM, Ruokonen E, Grounds RM et al. Dexmedetomidine vs midazolam or propofol for sedation during
prolonged mechanical ventilation: two randomized controlled trials. JAMA 2012; 307(11):1151–1160.
14. D Commence extra-corporeal membrane oxygenation
(ECMO)
This scenario is based on a real case and this patient and her child both survived to
discharge neurologically intact.
ECMO uses technology refined from cardiopulmonary bypass circuits used for cardiac
surgery. As the technology advances and with the opportunity to gain experience in
its use (the H1N1 swine-flu epidemic of 2009) the complication rates have decreased.
The CESAR trial evaluated the benefits of ECMO in adult respiratory distress syndrome
(ARDS) and demonstrated that patients transferred to a centre offering ECMO had a
better outcome (less death or severe disability at 6 months) than those treated at the
original hospital with conventional therapy. However, treatment at the ECMO centre
did not always involve ECMO and the improvement in outcome was not shown when
comparing ECMO verses conventional ventilation at the ECMO centre.
An ECMO circuit can be set up in three ways:
• Venoarterial ECMO: blood is pumped from the venous to the arterial side
allowing gas exchange and haemodynamic support
• Venovenous: blood is removed from the venous side and then pumped back into
it facilitating gas exchange only
• Arteriovenous: arterial pressure moves the blood from the arterial side to the
venous side and facilitates gas exchange. No mechanical pump is required.
The large-bore cannulae are placed surgically or with a percutaneous approach
under ultrasound or X-ray guidance. The circuit is more effective at carbon dioxide
removal than oxygenation due to differences in solubility between the two gases.
Anticoagulation is required as the circuit activates the coagulation cascade.
Answers
Complications include:
• Haemorrhagic complications (50% of patients):
–– 50% of these due to the cannulation, especially at the arterial site
–– Intracranial bleeding (5%)
–– Bleeding may occur in any organ
• Thrombosis in the circuit can:
–– Affect the function of the pump or the oxygenator
–– Cause stroke
–– Result in leg ischaemia
• Infective complications can be related to the invasive lines or primary pathology
• Technical complications include:
–– ECMO circuit failure or breakage
–– Cannula displacement
–– Mechanical pump failure
A meta-analysis of studies using ECMO as rescue therapy during cardiopulmonary
resuscitation (CPR) demonstrated an increased survival in younger patients after
instigating ECMO during or immediately after manual CPR. There is an increasing
drive to consider early initiation of ECMO, and the emergency department ECMO
project strives to initiate pre-hospital and emergency department ECMO CPR.
Returning to the scenario, this young woman who has had continuous CPR and has
not responded to support measures should be considered for ECMO if it is available.
To ensure the best outcome, oxygenated blood flow to the brain should be restored
as early as possible. Pregnancy is an absolute contra indication to thrombolysis as
is having a major operation within 14 days. After a rushed emergency department
cesarean section with a low cardiac output state (and therefore difficulty identifying
bleeding points) thrombolysis would have a high complication rate may only be
considered if no alternative was available.
Martinez G. Extracorporeal membrane oxygenation in adults. Contin Educ Anaesth Crit Care Pain 2012;
12(2):57–61.
Cardarelli MG. Use of extracorporeal membrane oxygenation for adults in cardiac arrest (E-CPR): a metaanalysis of observational studies. ASAIO J 2009; 55(6):581–586.
15. C Prostacyclin infusion
One third of critically ill adults develop an acute kidney injury and 5% of these will
require renal replacement therapy. This question highlights some of the complexities
of managing a patient on renal replacement therapy.
The indications for renal replacement therapy include:
•
•
•
•
•
•
Fluid balance management
Hyperkalaemia (potassium over 6.5 mmol/L)
Metabolic acidosis (pH < 7.1)
Raised urea (> 30 mmol/L) or symptomatic ureamia
Severe sepsis to remove inflammatory mediators
Removal of water-soluble, low protein-bound drugs, e.g. some antibiotics to
increase dose administered.
351
352
Chapter 9
The different types of renal replacement therapy are:
• Haemo-(ultra)filtration: venous blood is pumped into an extra-corporeal
circuit which creates a hydrostatic pressure gradient across a semi-permeable
membrane. Plasma (ultrafiltrate) and molecules of less than 50,000 Daltons are
forced across by convection. The plasma is replaced by fluid either before or after
the filter to maintain volume and haematocrit
• Haemodialysis: venous blood is pumped into a dialyser in which blood is
separated by a semi-permeable membrane from a countercurrent flow of dialysis
solution. Solute moves along its concentration gradient from blood to dialysis
solution (e.g. urea) or from solution to blood (e.g. bicarbonate) by diffusion
• Haemodiafiltration: this is a combination of the two.
The methods can be applied intermittently or continuously, with continuous
methods (filtration or dialysis) being preferred on the intensive care unit due to
cardiovascular stability.
Anticoagulation is required as all extra-corporeal circuits activate the clotting cascade.
Clot that forms within the catheter causes an access pressure alarm, whereas clot
that forms in the filter will cause a trans-membrane alarm. The latter will reduce the
efficiency of the filter and if it clots of completely then blood within the circuit is lost.
Non-pharmacological methods to prevent clot formation include:
• Ensure adequate driving pressure (venous pressure)
• Ensure adequate flow rates through the vascular-catheter (vascath):
–– Correct site choice (femoral preferred over right internal jugular which is in turn
preferred over left internal jugular veins)
–– Good insertion technique
–– Catheter position and care
• Adding replacement fluid before the filter (pre-dilution) lowers the haematocrit and
reduces the chance of filter clot but reduces the efficacy of the filtration process
If the patient has a coagulopathy (INR > 2, APTT > 60 seconds) no anti-coagulation is
required, however most patients require pharmacological treatment to prolong the
life of the filter.
Pharmacological methods include:
• Unfractionated heparin: increases anti-thrombin III formation. It is the most
commonly used, fully reversible by protamine and the anticoagulation effect can be
easily titrated by measuring the activated partial thromboplastin ratio (APTR). Given
into the circuit before the filter results in less systemic anticoagulation then when
given systemically, but monitoring is required and the APTR should be less than 2.
There is an increased risk of bleeding and heparin-induced thrombocytopenia
• Prostacyclin or prostaglandin E2 inhibit platelet function and has a short half-life
resulting in rapid reversal of the anti-coagulation effect on termination. It causes
vasodilatation and therefore can worsen cardiovascular instability, hypoxia in
patients dependent on hypoxic pulmonary vasoconstriction, and intracranial
hypertension
Answers
• Regional citrate: infused pre-filter chelates calcium and prevents clot-formation.
Calcium is added post-filter. It is effective and reduces bleeding rates, but may
cause metabolic abnormalities and is rarely used in the UK
• Danaparoid and lepirudin may be used instead of heparin if heparin-induced
thrombocytopenia develops but is no more effective, bleeding rates are equivocal
and they are not easily reversed.
Therefore, in this patient who has been resuscitated (which in the context of a
gastrointestinal bleed means the coagulation has been normalised), the safest
option in this case would be prostacyclin infused into the filter, which will result in
minimal systemic anti-coagulation and may be reversed by terminating the infusion.
Heparin given into the circuit still causes systemic anticoagulation and increases the
bleeding risk.
Baker A, Green R. Renal replacement therapy in critical care. Anaesthesia Tutorial of the Week No 194.
London: World Federation of Societies of Anaesthesiologists, 2010.
16. D Prescribe haloperidol
Delirium in critically ill patients is common, with 60–80% of patients being affected.
It is characterised by an acute change in cognition and disturbance of consciousness
and may follow a fluctuating course. There is an increased length of ventilation,
intensive care stay, hospital stay, risk of infection, risk of long-term cognitive
impairment and mortality. There is a much higher rate of adverse incidents such as
self-extubation and removal of catheters and lines.
The different types of delirium are:
• Hyperactive delirium (5–22%), which is the case described above, and includes
agitation, hallucinations and aggression
Table 9.2 Risk factors associated with developing delirium in critically ill patients
Patient
Age
Substance abuse (alcohol, smoking, illicit drugs)
Hypertension
Depression
Existing cognitive deficiency
Sensory loss (deafness or blindness)
Clinical conditions
Metabolic and electrolyte disturbances (particularly hyponatraemia)
Sepsis
Hypoxia or hypercapnia
Hypotension
Ischaemic myocardial event
Disturbances in blood glucose control
Postoperative pain, urinary retention, constipation
Iatrogenic
Sedation or analgesic medication
Day-night cycle disruption
Immobilization
353
354
Chapter 9
• Hypoactive delirium is more common, presenting with inattention and decreased
situational awareness, but may be peaceful and compliant so is often not diagnosed
• Mixed delirium is a fluctuation between the two extremes above
The risk factors for developing delirium are show in Table 9.2.
There are two different delirium assessment methods in the intensive care unit to be
aware of for the exam, both of which are described in detail in the references below:
• Intensive Care Delirium Screening Checklist (ICDSC): Patients are scored for
alertness from waking, and then their attention, orientation, agitation or
retardation, hallucinations, speech and mood and sleep cycle is scored daily. A
score of 4 or more has a sensitivity of 99% but a low specificity of 64%
• Confusion Assessment Method in the intensive care unit (CAM-ICU): This is
designed for ventilated patients and has a high sensitivity and specificity.
Following a level of consciousness assessment (Richmond agitation sedation scale
is commonly used), attention, organised thinking and ability to follow instructions
is assessed
Preventative management includes ensuring a correct and adequate sleep pattern,
constant information and reassurance regarding their situation and as consistent
as possible attendants (family members are the best). The management of delirium
is multi-factorial, and includes exclusion of reversible organic causes as described
above, which requires an examination and review of relevant investigations.
Pharmacological management can be considered in an escalating fashion:
• Haloperidol 2.5 mg intravenously, doubling the dose every 30 minutes until
settled followed by a regular regime. Side-effects include prolongation of the QT
interval and an extra-pyramidal movement disorders
• Olanzapine 5 mg orally or intramuscularly may be considered as an alternative
• Quetiapine, an atypical antipsychotic is being used increasingly as an alternative
to haloperidol, has equal efficacy and safety, without extra-pyramidal side effects
• Dexmedetomidine, an α2 adrenoceptor agonist, similar to clonidine, has also been
used in ventilated patients with delirium and is as effective as haloperidol. A bolus
of 0.1 mg/kg followed by 0.2-0.7 mg/kg/hour may be used.
It is worth noting that other sedation methods including opioids and
benzodiazepines may contribute to delirium, although benzodiazepines do have a
role in alcohol withdrawal.
The question describes a patient in danger of harming himself in the immediateterm, and therefore the preventative measures are likely to be unhelpful. There is
no firm evidence of alcohol consumption excess and it is too early in the patients
clinical course to blame this on alcohol withdrawal, therefore benzodiazepine
treatment may exacerbate his condition. The first line treatment is haloperidol,
followed by other measures if unsuccessful.
Cavallazzi R. Delirium in the ICU: an overview. Ann Intensive Care 2012; 2:49.
King K, Gratrix A. Delirium in intensive care. Contin Educ Anaesth Crit Care Pain 2009; 9(5):144–147.
Answers
17. D Offer her an epidural blood patch
Post dural puncture headache (PDPH) is a well-known complication of central
neuraxial blockade. In epidural anaesthesia, dural puncture is not always obvious at
the time of the procedure, as the Tuohy needle may nick the dura, but not enough
to cause a frank CSF spill. Patients with PDPH usually present within 72 hours of the
incident with the typical low-pressure headache – worse on standing, coughing,
straining and better on lying supine. The headache is usually frontal or occipital and
may be associated with symptoms such as neck stiffness, photophobia, nausea or
tinnitus. Gutsche’s test may be positive – pressing over the liver with the patient at
45o relieves the headache.
When assessing a patient with suspected PDPH it is important to take a full history
and complete a full neurological examination in order to try to rule out more sinister
differential diagnosis such as meningitis, cortical vein thrombosis, cerebral infarction
and subarachnoid haemorrhage. Other causes such as tension headache, migraine
and sinusitis should also be considered, which a thorough history will help with.
Management can be conservative with hydration, paracetamol and non-steroidal
anti-inflammatory drugs. Bed rest is also encouraged, but this can be impractical
for a nursing mother. Caffeine causes cerebral vasoconstriction and so may provide
some relief of the headache, although concrete evidence of benefit is lacking.
Sumatriptan is a serotonin receptor agonist used for the treatment of migraine,
which again lacks evidence of benefit in PDPH.
This patient has already tried conservative therapies for the past 2 days and the fact
that she has returned to the labour ward suggests that she is not coping. Although
intravenous fluids may help, it is not the best line of management to take next, as an
epidural blood patch (EBP) has the best chance of curing her symptoms. The patient
should be offered an EBP with all the risks and benefits explained. Blood cultures
were at one point taken routinely at the time of an EBP, but this has fallen out of
favour in many units since patients are usually apyrexial and cultures come back
negative. In fact, if a patient was pyrexial, this should deter the performance of an
EBP and prompt further investigation of another cause for the headache.
Sabharwal A, Stocks GM. Postpartum headache: diagnosis and management. Contin Educ Anaesth Crit
Care Pain 2011; 11(5):181–185.
18. A Platelet count <50 x 109/L
The risk of developing a spinal or epidural haematoma as a result of central neuraxial
blockade increases in the presence of abnormal coagulation. In the obstetric
population, there may be a number of reasons for abnormal coagulation, including
pre-eclampsia, disseminated intravascular coagulation (DIC) and gestational
thrombocytopenia. If there is any reason to suspect a clotting problem in a patient
who may need central neuraxial blockade, a full blood count and clotting screen
should be checked.
355
356
Chapter 9
Gestational thrombocytopenia occurs due to a combination of haemodilution and
increased platelet turnover, particularly in the third trimester. The platelet count is
usually > 70 x 109/L. The increased risks of regional anaesthesia and haemorrhage
during delivery should be explained to the mother so she can make an informed
decision on choice of anaesthetic.
The lowest acceptable platelet count for performing neuraxial blockade has
gradually reduced over the past few years. Current expert opinion is that neuraxial
blockade can be performed in parturients with platelet counts > 50 x 109/L, as long
as the count is stable and all other clotting indices are normal. Hence, option A is the
only scenario in this case that would prevent this lady having a spinal.
Different hospitals have different protocols for regional analgesia, and in general,
advocate that a discussion with the consultant anaesthetist take place if the platelet
count is less than 70 or 80 x 109/L. In this case, the lady is coming for an elective
Caesarean and hence, a consultant anaesthetist should be on the labour ward on the
day and often may choose to perform the block themselves instead of the trainee.
An APTT of 30 seconds and a PT of 12 seconds are both within normal limits, hence
would not prevent this lady from having a spinal.
Bedson R, Riccoboni A. Physiology of pregnancy: clinical anaesthetic implications. Contin Educ Anaesth
Crit Care 2014; 14(2):69-72.
Kam PCA, Thompson SA, Liew ACS. Thrombocytopenia in the parturient. Anaesthesia 2004; 59(3):255–264.
Lyons G, Hunt BJ. Platelet counts and obstetric analgesia and anaesthesia. Clinical Guidelines: Regional
anaesthesia and coagulation. London: Obstetric Anaesthetists’ Association, www.oaa-anaes.ac.uk
19. E Inhalational anaesthetic induction and maintenance
with sevoflurane, without muscle relaxant. Maintain
spontaneous respiration throughout the case
Presentation of inhaled foreign body can vary from asymptomatic, to partial
obstruction with coughing, wheezing, stridor and dyspnoea, to complete
obstruction of the upper airway with hypoxia and cardiac arrest. Most foreign bodies
are radiolucent and the chest X-ray will often be normal. Therefore, a positive history
and clinical signs of aspiration alone may be enough evidence for endoscopy. A
chest X-ray in inspiration and expiration may aid location of the foreign body and
show any atelectasis, pneumonia, or air trapping.
Whatever anaesthetic technique is used, spontaneous respiration is best preserved,
although inhalation induction may be prolonged in the presence of hypoventilation.
Sevoflurane in 100% oxygen and topical anaesthesia to the airway is the technique
of choice. Care must be taken to maintain spontaneous breathing or gentle assisted
ventilation as positive pressure may drive the foreign body distally.
Roberts S. Paediatric bronchoscopy. Contin Educ Anaesth Crit Care Pain 2005; 5:41–44.
Fidkowski CW, Zheng H, Firth PG. The anesthetic considerations of tracheobronchial foreign bodies in
children: a literature review of 12,979 cases. Anesth Analg 2010; 111:1016–1025.
Answers
20. D Arrange for the GP to administer the MMR vaccination
4 weeks postoperatively
The Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI)
published a guideline on the subject of vaccination around the time of anaesthesia
and surgery. One of the questions addressed was: should vaccines be given
opportunistically during anaesthetic procedures? The APAGBI concluded that
in general, vaccination should not be administered during anaesthesia, in order
that paracetamol or other anti-inflammatory agents can be used freely as part
of the anaesthetic technique and post-surgical care. This is due to concerns that
paracetamol and non-steroidal anti-inflammatory drugs reduce the efficacy and
antibody responses to vaccines.
If indicated, vaccination may be given when the child has recovered, but before
discharge. However, in the case of this infant with an inguinal hernia repair,
paracetamol and other anti-inflammatory drugs are useful for post operative
analgesia, so vaccination is best delayed for at least 72 hours. As this clinical scenario
refers to a day-case operation, the most appropriate course of action is to arrange for
the GP to administer the vaccination after a suitable interval postoperatively.
The Association of Paediatric Anaesthetists of Great Britain and Ireland (APAGBI). Immunisation Guideline:
The Timing of Vaccination with Respect to Anaesthesia and Surgery. London: APAGBI, 2013.
Prymula R, Siegrist CA, Chlibek R, et al. Effect of prophylactic paracetamol administration at time of
vaccination on febrile reactions and antibody responses in children: two open-label, randomised
controlled trials. Lancet 2009; 374:1339–1350.
21. C Buprenorphine
True morphine allergy is rare, but when it does occur patients can safely be
prescribed alternate opioids as long as they are structurally different.
Structural classes:
• Diphenylheptanes: methadone
• Phenanthrenes: morphine, codeine, buprenorphine, oxycodone
• Phenylpiperidines: fentanyl, remifentanil, pethidine
Tramadol is a cyclohexanol derivative and is structurally different to morphine.
Methadone shows no cross-tolerance with other opioids and can be used safely in a
true morphine allergy.
Fentanyl and pethidine are synthetic opioids of the phenylpiperidine class. This
class of opioid has structures different enough that they can be given to a patient
intolerant to the natural or semi-synthetics without fear of cross reactivity. They are
also very different from others in this same class.
Buprenorphine is a semi-synthetic opioid and therefore has some structural
similarities to morphine, suggesting that there maybe some cross reactivity.
357
358
Chapter 9
Barnett M. Alternative opioids to morphine in palliative care: a review of current practice and evidence.
Postgrad Med J 2001; 77:371–378.
DeDea L. Prescribing opioids safely in patients with an opiate allergy. JAPA 2012; 25(1):17.
22. A Paracetamol, ibuprofen, gabapentin, MST 25 mg twice
daily, Oramorph 10–20 mg 4-hourly
The conversion of transdermal buprenorphine to oral morphine is 1:100.
20 μg/hour = 20 x 24 = 480 μg/day
480 μg x 100 = 48,000 μg = 48 mg per day
Therefore option A gives a background dose to cover the patch and then an as
required (PRN) dose which is one-sixth of the daily usage. This is a safe starting point.
B is unsafe with a 2 mg bolus with a short lockout time of 5 minutes as longer
lockout times are advocated with larger bolus doses.
C gives a standard fentanyl bolus protocol and there is no cover for background
requirement of opiate this patient clearly will need.
D is a standard protocol and does not consider the patient's normal opiate
requirement
E Oxycodone is twice as potent as oral morphine therefore a 15 mg b.d. of a modified
release oxycodone (Oxycontin) would give a sufficient background. However, the
immediate release Oxynorm is not suitable for this purpose.
British National Formulary (BNF). Section 4.7. Pain management with opioids. Analgesics. London: BNF,
2014 www.bnf.org
23. E Morphine patient controlled analgesia (PCA) with a
background infusion
Anaesthetists have a fundamental role in providing safe and adequate analgesia
for surgical patients, which sometimes includes individuals who are already
taking recreational opioids or have preceding chronic pain issues. The salient
features in the above case include the history of intravenous heroin use (and likely
physiological dependence), the type of surgery (affecting the postoperative route of
administration and absorption), as well as the diagnosis of schizophrenia (affecting
suitable analgesic choices).
The term ‘opioid’ describes all substances active at the opioid receptor, which
includes heroin (diamorphine) and morphine. Chronic opioid use leads to
suppression of the noradrenergic system and a compensatory up-regulation of the
cyclic adenosine monophosphate signalling pathways in the neurons involved in
noradrenaline release. If opioid intake then ceases abruptly, patients will experience
a ‘noradrenergic storm’ of withdrawal, which includes shivering, goose bumps,
anxiety, and lacrimation. Patients presenting for surgery with a chronic history of
heroin use need to be protected against withdrawal, by maintaining adequate
opioid receptor agonist, which is commonly achieved by administering methadone
Answers
or morphine. There are means of estimating oral methadone equivalence with street
heroin, but these are not always reliable.
The problem with oral methadone in this clinical scenario is the anticipated postoperative nil by mouth status and the unpredictable absorption following major
abdominal surgery. It is not appropriate to use intravenous methadone as dose
equivalence with street heroin can be difficult to determine.
Neuraxial blockade can provide excellent postoperative analgesia following major
abdominal surgery, but should not be the sole form of analgesia in the above
scenario since the plain bupivacaine epidural solution will not address the opioid
dependency. Siting an epidural in the presence of sepsis and coagulopathy will also
increase the risk of developing an epidural abscess or haematoma.
Care needs to be taken when providing complex pain management to patients with
schizophrenia since certain medications can exacerbate a psychosis. Ketamine and
cannabinoid receptor agonists are both associated with this side-effect and should
not be used.
The most appropriate way to manage the above patient is to address both his opioid
dependency and analgesic requirements by commencing a morphine patient
controlled analgesia regime on top of a continuous morphine infusion. These
patients need to be monitored closely to assess adequacy of pain relief and for any
signs of respiratory depression. Early involvement of the pain team is also advised.
The British Pain Society. Pain and substance misuse: improving the patient experience. London: The British
Pain Society, 2007:1–60.
Maldonado R. Participation of noradrenergic pathways in the expression of opiate withdrawal:
biochemical and pharmacological evidence. Neurosci Biobehav Rev 1997; 21(1):91–104.
24. C Localised external beam radiotherapy
The neurophysiology of cancer pain is complex and can encompass inflammatory,
neuropathic, ischaemic as well as compressive processes from multiple sites. It is
therefore important when assessing cancer pain to not only identify the location and
severity but also recognise the underlying aetiology to help guide management.
Skeletal pain in cancer patients is most commonly associated with bony metastases
and management can be tailored to a solitary site or multi-focal areas depending on
symptoms. In the above scenario, where the pain is localised to a single metastasis
which is refractory to opioids, the most appropriate next step is to apply targeted
radiotherapy. The efficacy of this treatment modality in managing metastatic
bone pain has been confirmed in a Cochrane review and it can be applied in the
palliative setting. The exact mechanism by which radiotherapy provides analgesia
is not known, although a reduction in tumour load and local osteoclast activity is
believed to play a role. The pain relief evolves consistently over 4–6 weeks from the
start of treatment and approximately 80% of patients will have a recorded response.
Symptoms such as nausea and increased stool frequency are recognised side-effects
of treatment, but are more likely to occur when radiotherapy is applied to bony areas
with a significant amount of surrounding bowel (such as the pelvis or lumbar spine).
359
360
Chapter 9
Stabilising surgery is a recognised treatment option for metastatic bony pain
in cancer patients, but only in the presence of a pathological fracture. If this is
inoperable, patients can still achieve pain relief through application of localised
radiotherapy to the fracture site. Since there is no femoral fracture in the above
scenario, surgery is not appropriate.
Bisphosphonates are a group of drugs which inhibit osteoclastic bone resorption
and can be used in the management of cancer induced bone pain and to prevent
skeletal events. However, they do not specifically target solitary metastases, and are
more appropriate for when the pain is scattered. Bisphosphonates also have a very
poor oral bioavailability and are usually given as intravenous infusions, which may
be difficult in patients with poor intravenous access such as the case above.
Radioisotope treatment involves the delivery of radiotherapy to multiple bony
metastases via the intravenous administration of a bone seeking radio isotope
(usually Strontium 89). It has a similar efficacy to wide field radiotherapy but with a
better side effect profile. However, it is more appropriate for patients with pain from
multiple bony metastases as opposed to a single site.
Neuropathic pain is a feature which can occur in conjunction with bony metastases
(particularly vertebral) to heighten the nociceptive experience. In such cases, drugs
such as gabapentin which specifically target the neuropathic component may be
applicable. However, it is not the most appropriate next management step in the
above scenario since there is no evidence of neuropathic pain.
McQuay H, Collins S, Carroll D. Radiotherapy for the palliation of painful bone metastases. Cochrane
Database Syst Rev 2000; 2:CD001793.
The British Pain Society. Cancer Pain Management. London: The British Pain Society, 2010: 1–116.
25. D Radiotherapy
Metastatic bone pain is a common problem in patients with disseminated
malignancy and can be difficult to control with opioid analgesia alone.
In this case increasing her MST is unlikely to help as despite large dose of
intermittent Oramorph, pain remains an issue. Opioid rotation can be effective in
patients that are developing tolerance to morphine; however this is not the best
option here.
Radiotherapy is a very effective treatment for localised bone pain, as shown by two
Cochrane reviews. Relief was achieved in 60% of patients with a number needed to
treat (NNT) of 3.6 (95% CI 3.2–3.9).
There is evidence to suggest that the use of adjuvant bisphosphonates reduces
morbidity from bone metastasis. Results from a Cochrane review suggested that
there is only a modest reduction in pain when used in addition to analgesics.
Finally, there is no evidence for the use calcitonin to control pain from bone
metastases currently.
The British Pain Society. Cancer Pain Management. London: The British Pain Society, 2010: 1–116.
McQuay H, Carroll D, Moore RA. Radiotherapy for painful bone metastases: a systematic review. Clin Oncol
1997; 9:150–154.
Answers
Ross JR, Saunders Y, Edmonds PM, et al. Systematic review of role of bisphosphonates on skeletal
morbidity in metastatic cancer. Br Med J 2003; 327:469–472.
Wong R, Wiffen PJ. Bisphosphonates for the relief of pain secondary to bone metastases. Cochrane
Database of Systematic Reviews 2002; 2:CD002068.
Martinez MJ, Roqué M. Calcitonin for metastatic bone pain. Cochrane Database of Systematic Reviews
2006; 3:CD003223.
26. B Perform a rapid sequence induction with thiopentone
and suxamethonium using an uncut size 8 cuffed oral
tracheal tube
As with all emergency situations an ABC approach should be used. While assessing
the airway high flow oxygen should be administered via a non-rebreathing mask.
The following features are suggestive of an airway which is at risk:
• Burns sustained in an enclosed space. Flash burns rarely cause an inhalational
injury
• Singed eyebrows and nasal hair
• Carbonaceous sputum
• Erythematous and swollen oral mucosa and uvula
• Difficulty swallowing
• Hoarse voice
• Stridor
• Deep facial and neck burns
If there is any concern over the airway it is safer to intubate early. Early intubation
is technically easier as the oropharyngeal swelling is not yet established. An uncut
large oral tracheal tube should be used. This will allow for any subsequent facial
swelling. The large calibre tube will facilitate later bronchoscopy to assess inhalation
injury.
Suxamethonium is safe to use in the 24 hours following a burn injury but should
be avoided thereafter for up to a year. This is thought to be due to extra-junctional
acetylcholine receptors that are expressed following burns which, when activated,
leads to a massive efflux of potassium resulting in possible cardiac arrest.
Following a burn injury, the thermostatic centre in the hypothalamus is reset,
resulting in a core temperature 1–2 degrees higher than normal.
There is no evidence for the use of prophylactic antibiotics or steroids in burns
patients.
Bishop S, Maguire S. Anaesthesia and intensive care for major burns. Contin Educ Anaesth Crit Care Pain
2012; 12(3):118–122.
27. E Administer a bolus of intravenous labetalol 10 mg
Confusion in the high dependency unit following carotid endarterectomy (CEA)
has a number differential diagnoses but in the context of the above presentation
points towards a rare but potentially fatal complication called cerebral reperfusion
361
362
Chapter 9
syndrome. It complicates 1% of carotid endarterectomies. Its presentation ranges
from 2 to 7 days, and occurs due to a combination of sustained hypertension
associated with various neurological signs and symptoms of cerebral oedema.
It is associated with 60% mortality and the mainstay of its treatment is accurate
and rapid control of raised blood pressure. The pathophysiology involves lack of
auto-regulation of surges in blood pressure due to operation around the carotid
bifurcation. This will result in carotid baroreceptor being injured by the surgery and
as a result the exposure of intracranial circulation to a rapidly elevated perfusion
pressure, resulting in cerebral oedema.
The first option is true if the patient had meningitis, but a normal temperature and
no signs of meningism makes it unlikely. Urinary retention is a common cause of
confusion in the immediate postoperative phase but is unlikely 3 days later. Mannitol
administration is a temporising measure to control intracranial pressure in a patient
at risk of cerebral or cerebellar herniation, which is unlikely in a conscious patient.
The definitive treatment of this rare syndrome is rapid control of hypertension which
means intravenous hypotensive agent such as labetalol.
Ladak N. General or local anaesthesia for carotid endarterectomy? Contin Educ Anaesth Crit Care Pain
2012; 12(2):92–96.
28. B Human erythropoietin
Preoperative anaemia is associated with increased perioperative morbidity and
should be diagnosed and optimised prior to surgery. In order to differentiate the
causes of anaemia, a reticulocyte count can be performed to gauge bone marrow
response. A high reticulocyte count suggests regenerative anaemia, which is
associated with blood loss or haemolysis. A low reticulocyte count can be further
differentiated based on mean corpuscular volume (MCV) into microcytic, normocytic
or macrocytic anaemia.
• Microcytic anaemia is associated with iron deficiency or β-thalassaemia
• Macrocytic anaemia can be associated with folate and B12 deficiency if
megaloblasts are visualised in a peripheral blood smear. Chronic alcoholism, liver
disorders and thyroid disease can cause non-megaloblastic macrocytic anaemia
• Normocytic anaemia with low reticulocytes is associated with renal and hepatic
dysfunction, chronic anaemia and myelodysplasia
Erythropoiesis is controlled by erythropoietin, which is a glycoprotein hormone
released by the renal cortices. Recombinant human erythropoietin is recommended
for anaemia caused by chronic kidney disease and is administered as subcutaneous
injections three times a week.
Hans GA, Jones N. Preoperative anaemia. Contin Educ Anaesth Crit Care Pain 2013; 13(3):103-105.
Answers
29. C MRI whole spine
The classical triad of fever, backache and neurological symptoms can be seen in
patients with suspected epidural abscess. Back pain is the commonest symptom
followed by fever and neurological symptoms. Neurological manifestations are
noticed late and the diagnosis should be suspected prior to the onset of these signs.
The neurological features occur due to pressure symptoms coupled with vascular
effects including ischaemia or thrombosis. Leucocytosis occurs in two thirds of
patients and an elevated erythrocyte sedimentation rate (ESR) is much more
commonly associated. Normal C-reactive protein (CRP) values cannot exclude
epidural abscess.
Magnetic resonance imaging (MRI) with gadolinium is the investigation of choice
and should include the whole spine as the catheter tip may lie proximal as compared
to the lumbar entry site.
Lumbar punctures may not be positive and more importantly could potentially
spread the infection or cause coning in case of elevated intracranial pressures.
Management must be expeditious and use a multidisciplinary approach including
radiology, neurosurgeons, intensive care and anaesthesia.
Simpson KH, Al-Makadma YH. Epidural drug delivery and spinal infection. Contin Educ Anaesth Crit Care
Pain 2007; 7(4):112-115.
30. D Mann-Whitney U test
Statistics is an essential part of critical appraisal. To ascertain the most appropriate
statistical test to be applied, a flow chart may help (see Figure 9.3). First the
data needs to be ascertained as either qualitative (categorical) or quantitative
(continuous).
Qualitative data is descriptive data such as gender, eye colour or ethnicity. The Chi
squared test is a good example of a statistical test used for analysis of qualitative
data. For smaller samples where the results can be collated by a ‘2 by 2’ table, the
Fisher’s exact test may be more appropriate.
Quantitative data can be classified as either parametric (normal) or non-parametric.
Further decisions can be guided by whether there are two groups or more than
two groups in the study. Within the groups the data can be paired, that is the
data was collected from the same sample group. An example would be a study
investigating blood pressure measurements in a group of patients before and after
a trial antihypertensive is given. Unpaired data suggests two different groups were
studied. For example, this study, which compares two groups of patients; those who
received discretionary sedation versus those who received protocolised sedation.
From the statistical test employed, a p-value is derived. The p-value reflects the
probability the result happened by chance. A commonly applied threshold p-value
in clinical trials is < 0.05. This means there is a less than 5% (or 1 in 20) chance
of the result occurring by chance. As clinicians, the fundamental outcome has
to be considered on the basis of clinical significance, rather than pure statistical
significance.
363
364
Chapter 9
Figure 9.3 Flow chart to guide
choice of statistical test for
different forms of data.
Which statistical test?
Key:
P = paired
UP = unpaired
Qualitative
Chi Squared test
Fisher’s Exact test
Quantitative
Parametric
Non-parametric
2 groups
>2 groups
2 groups
>2 groups
P
UP
P
UP
P
UP
P
UP
Paired Student's t-test
Unpaired Student's t-test
Paired analysis of
variance (ANOVA)
Unpaired ANOVA
Wilcoxon Signed
Rank test
Mann-Whitney U test
Friedman test
Kruskal-Wallis test
As can be seen from Figure 9.3, the data presented in the study in question is
qualitative and non-parametric, as a normal distribution cannot be assumed. There
are two independant groups of patients, therefore the data is unpaired. In this
instance, a Mann-Whitney U test is best applied.
McCluskey A, Lankhen AG. Statistics III; probability and statistical tests. Contin Educ Anaesth Crit Care Pain
2007; 7(5):167–170.
Chapter 10
Mock Paper 10
Questions
1. A 36-year-old man requires trans-sphenoidal surgery for a large anterior pituitary
tumour with suprasellar extension.
Prior to induction, which of the following are you most likely to need to prepare?
A
B
C
D
E
Fibreoptic scope
Lumbar drain
Invasive arterial blood pressure monitoring
Intravenous insulin administration
Postoperative ventilation
2. A 20-year-old male trauma patient has arrived in the emergency department
was had flaccid paralysis of both lower limbs before being intubated at scene for
transfer. A full body CT scan revealed a complex vertebral fracture of T5 with a
retropulsed fragment and an undisplaced sacral fracture. Despite 2 litres of fluid
resuscitation his blood pressure remains 80/40 mmHg with a heart rate of 69 beats
per minute.
Which of the following is the most likely reason for his fluid resistant hypotension?
A
B
C
D
E
Spinal shock
Tension pneumothorax
Haemorrhage
Pulmonary embolus
Neurogenic shock
3. You are asked to anaesthetise a 68-year-old man for rigid bronchoscopy for biopsy
of a posterior tracheal mass. He has normal mouth opening and neck extension.
Which of the following is the most appropriate anaesthetic technique?
A
B
C
Spontaneous ventilation with lidocaine topicalisation of the airway and
sedation with intravenous midazolam
Inhalational induction and maintenance of deep anaesthesia with sevoflurane
and oxygen via a facemask removed when the bronchoscope is inserted
Intravenous induction with propofol and atracurium. Oxygen and sevoflurane
maintenance with intermittent positive pressure ventilation (IPPV) via a
microlaryngeal tube
366
Chapter 10
D Intravenous induction with propofol and atracurium followed by low
frequency jet ventilation via the bronchoscope. Maintenance of anaesthesia
with propofol and remifentanil target controlled infusion (TCI)
E Placement of cricothyroid cannula followed by anaesthesia with propofol and
remifentanil TCI. Jet ventilation via the cricothyroid cannula
4. A 33-year-old man is extracted from a house fire and admitted to the emergency
department. He cannot remember being rescued and on examination has
singed nasal hair, burns across his neck and productive carbonaceous sputum.
He is receiving high flow oxygen through a non-rebreathing mask and is not in
respiratory distress.
Which investigation will be most useful in assessing and managing his upper airway?
A
B
C
D
E
Pulse oximetry
Chest X-ray
Computed tomography
Arterial blood gas
Flexible bronchoscopy
5. A previously well 9-year-old boy is having a laparoscopic appendicectomy.
Anaesthesia was induced uneventfully with thiopentone and suxamethonium,
followed by a sevoflurane/oxygen mix. 10 minutes after port insertion his airway
pressures increase and his oxygen saturations begin to fall. Despite adjusted
mechanical ventilation, his end-tidal CO₂ reaches 9.0 kPa. His heart rate rises to
180 beats per minute and his temperature to 40°C.
Which of the following actions will ameliorate the situation most definitively?
A
B
C
D
E
Hyperventilation with 100% oxygen
Cooling the patient
Switching maintenance of anaesthesia to propofol
Treating any hyperkalaemia
Dantrolene 1–10 mg/kg
6. A 53-year-old man presents for a laparoscopic gastric bypass procedure. He has
a BMI of 46 kg/m2 and is an ex-smoker. He has a diagnosis of obstructive sleep
apnoea, but doesn’t really use his CPAP machine. He has severe reflux and a neck
circumference of 46 cm, his Mallampati score is 1 and he has good mouth opening.
The most appropriate anaesthetic plan includes:
A
Ramped head-up position, preoxygenation, and a rapid sequence induction
(RSI) with suxamethonium and cricoid pressure. ITU postoperatively
B Ramped head-up position, preoxygenation, and a RSI with rocuronium and
cricoid pressure. HDU postoperatively
C Ramped head-up position, preoxygenation, and a RSI with suxamethonium
and cricoid pressure. HDU postoperatively
D An awake fibreoptic intubation. Ward level postoperative care.
E Ramped head-up position, preoxygenation, standard induction.
Questions
7. A 62-year-old woman who presented for a laparoscopic cholecystectomy
experienced an unanticipated difficult intubation. An endotracheal tube was
eventually correctly sited following multiple attempts and the use of an intubating
stylet. The following day she is febrile with cervical surgical emphysema and
complains of neck stiffness and dysphagia.
What is the most likely cause of her symptoms?
A
B
C
D
E
Oesophageal perforation
Uvular necrosis
Tracheal rupture
Arytenoid dislocation
Aspiration pneumonia
8. A cardiac arrest call brings you to a 78-year-old man admitted to coronary care
following urgent percutaneous coronary intervention for inferior myocardial
infarction. The coronary care nurses administered a total of 3 mg of atropine 5
minutes ago for bradycardia. He is now has a blood pressure of 80/40 mmHg, a
heart rate of 35 beats per minute (regular), but is alert.
What is the next appropriate step in the management of his condition?
A
B
C
D
E
Administer 500 μg atropine
Start a dopamine infusion
Urgent transvenous electrical pacing
Start an adrenaline infusion
Give a fluid bolus of 250 mL of colloid
9. A 17-year-old girl presents for surgical correction of a spinal scoliosis. She has
dysmenorrhoea and menorrhagia for which she takes oral iron supplementation,
and is otherwise fit and well. Her haemoglobin concentration is 101 g/L. The
surgeon reminds you that his current practice involves spinal cord monitoring in
these cases.
Along with two large-bore peripheral cannulae, which of the following would be
the most appropriate anaesthetic technique for this case:
A
Volatile with target controlled infusion (TCI) remifentanil maintenance. An
internal jugular central line and a radial arterial line. Tranexamic acid.
B A radial arterial line. Propofol and remifentanil TCI. Cell salvage and
tranexamic acid.
C Volatile with nitrous oxide maintenance. A radial arterial line. Cell salvage and
tranexamic acid.
D Propofol and remifentanil TCI. A radial arterial line. A femoral central line and
cell salvage.
E TCI propofol with boluses of fentanyl. A radial arterial line with an internal
jugular central line. Tranexamic acid.
367
368
Chapter 10
10. A 75-year-old man with significant co-morbidities is admitted for elective foot
surgery under an ultrasound-guided ankle block.
In order to minimise the amount of time required to wait for the block to be
adequate for surgery, which one of the following nerves needs to be blocked first?
A
B
C
D
E
Superficial peroneal nerve
Deep peroneal nerve
Sural nerve
Saphenous nerve
Tibial nerve
11. You are asked to transfer a 27-year-old man to the local neurosurgical centre who
was admitted two hours ago with an acute traumatic subdural haematoma. On
admission he was alert but unable to recall the event, and he vomited twice. On
your assessment, he is asleep but rousable to voice, has slurred speech and is
obeying commands. His observations include a blood pressure of 180/90 mmHg,
heart rate of 90 beats per minute sinus rhythm and pupils of equal size and
reacting to light. He continues to vomit in spite of antiemetics.
What the most appropriate next step before the transfer?
A
B
C
D
E
Perform an arterial blood gas
Repeat the CT scan
Rapid sequence induction
Administer mannitol 20 % 0.5 g/kg
Cool the patient
12. A 42-year-old man presents to the emergency department after an out-of-hospital
cardiac arrest. He was successfully defibrillated out of ventricular fibrillation after
20 minutes of cardiopulmonary resuscitation (CPR). The airway was secured and
the patient was transferred to hospital. The blood pressure is 120/76 mmHg without
the need for inotropes or vasopressors and he is coughing on the endotracheal tube.
There is no ischaemia demonstrated on his electrocardiogram (ECG).
What is the clinical action that is likely to be most beneficial?
A
B
C
D
E
Administrating anti-platelet therapy via a nasogastric tube
An urgent coronary angiogram
An urgent transthoracic echocardiogram
A CT pulmonary angiogram
Targeted temperature management for 24 hours
13 A 59-year-old woman is on the high dependency unit following a bowel resection
for adenocarcinoma which finished 8 hours ago. She weighs 60 kg, has a past
medical history of type 2 diabetes and has a baseline creatinine of 120 μmol/L.
Postoperatively she has been passing 40 mL/hour of urine, which has decreased to
10 mL/hour for the past 2 hours despite her maintaining a normal blood pressure.
A repeat blood sample demonstrates a creatinine of 180 μmol/L.
Questions
Which of this patient's risk factors is most significant?
A
B
C
D
E
Chronic renal impairment preoperatively
Major intra-abdominal surgery
Oliguria
Serum creatinine rise
Diabetes
14. A 72-year-old man with hypertension has been referred to you 2 days after having
an emergency laparotomy for an incarcerated hernia. His oxygen saturations are
94% on an inspired oxygen concentration of 60%, his respiratory rate is 28 breaths
per minute and on auscultation there is bi-basal crepitus. On examination the
blood pressure is 100/60 mmHg, the pulse is regular, the heart rate is 110 beats
per minute and the jugular venous pressure (JVP) is visible at 6 cm. He has passed
10 mL of urine per hour for the last 6 hours and is agitated.
What is the next appropriate course of action?
A
B
Urgent blood tests to assess renal function
Continuous positive airway pressure (CPAP) support in the high dependency
unit
C Urgent fluid administration of 5–10 mL/kg of fluid and assess response
D Admit to the intensive care unit for haemofiltration
E Intravenous administration of 40 mg of furosemide and 2.5 mg of diamorphine
15. The intensive care unit dietician suggests commencement of enteral nutrition on a
67-year-old patient.
Which of the follow represents an absolute contraindication to starting enteral
nutrition?
A
B
C
D
E
Ischaemic bowel
Small bowel anastomosis
Short gut syndrome
Paralytic ileus
Pancreatitis
16. A 52-year-old hypertenisve woman presents to the emergency department
with a history of a sudden onset, severe headache, photophobia and confusion.
Her Glasgow coma score (GCS) suddenly declines to 7/15 (E2, V2, M3) with no
focal neurology elicited. She is intubated for a CT head, which shows extensive
subarachnoid blood. Her current location does not have neurosurgical facilities.
According to the World Federation of Neurological Surgeons Scale (WFNSS), her
clinical grade is:
A
B
C
D
E
I
II
III
IV
V
369
370
Chapter 10
17. A 38-year-old woman presents for a category 2 lower segment Caesarean section
(LSCS) for breech presentation. She has recently arrived in the UK from Burma,
is 37/40 pregnant and contracting. On examination of her back you notice skin
dimpling and a patch of hair at the base of her spine. She tells you that her mother
said she was born with an ‘abnormal spinal cord’ but she does not have any further
details. She is otherwise fit and well and functions normally.
What is the best line of management for her delivery?
A
Urgent MRI before the LSCS, then spinal anaesthesia if an acceptable lumbar
level is unaffected
B Perform the LSCS under spinal anaesthesia without prior MRI
C Perform the LSCS under epidural anaesthesia without prior MRI
D Perform the LSCS under general anaesthesia
E Request that the obstetricians deliver her vaginally
18. An 11-year-old boy has been hit by a car travelling at 20 mph.
On arrival to the emergency department. His head and neck are immobilised in
a cervical collar, and his respiratory rate is 24 breaths per minute, with oxygen
saturations of 94% on 15 litres per minute of oxygen. There is reduced air-entry on
the left. His heart rate is 158 beats per minute and blood pressure is 88/32 mmHg,
with a peripheral capillary refill time of 4 seconds. He has noticeable bruising
to the left side of his chest and abdomen. He does not open his eyes, makes no
sounds, and does not respond to commands, but tries to withdraw his arm when
an intravenous cannula is sited.
A chest X-ray shows consolidation of the left lung, but no obvious pneumothorax
or haemothorax. Bloods have been sent for full blood count and cross match.
A 500 mL bag of 0.9% saline is running through his intravenous cannula, and a
second intravenous cannula is being inserted.
The next immediate step in his management should be:
A
Perform a rapid sequence induction and secure his airway with an
endotracheal tube
B Arrange for an urgent CT head, chest and abdomen
C Perform a peritoneal lavage
D Rapid transfusion of 20 mL/kg of O-negative packed red cells
E Perform a Focused Assessment with Sonography for Trauma (FAST) scan
19. A fit and well 7-month-old 6 kg boy is scheduled for an elective inguinal hernia
repair as a day case. As you were inserting an intravenous cannula, you noticed
bruises of different ages on both arms and legs. When the infant was positioned
for a caudal block, you again noticed bruises of different ages on his back and
buttocks. The patient had an eventful surgery and is now in recovery.
What is the most appropriate action regarding the bruises?
Questions
A
B
C
D
E
Send a blood sample for an urgent coagulation screen
Speak to the parents and ask them to explain the bruises
Discuss the case with the hospital’s child protection team
Advise the surgical team to follow-up the bruises
Document the bruises in the patient’s medical notes
20. A 19 kg 3-year-old boy is scheduled for an elective dental procedure under general
anaesthesia. After an inhalational induction, you have four unsuccessful attempts
at placing an intravenous cannula. The patient is maintained under general
anaesthesia with oxygen and sevoflurane, breathing spontaneously via a face mask.
The most appropriate next step is:
A
B
Have further attempts at intravenous access until successful
Increase the inhalational anaesthesia and secure the airway before further
attempts at intravenous access
C Ask another colleague to attempt intravenous access
D Wake the patient up and postpone the procedure
E Insert an intra-osseous needle
21. A 61-year-old man has been suffering from long-term low back pain. His MRI one
year ago shows multiple degenerative changes and there is no evidence of nerve
root compression. He has tried simple analgesics, non-steroidal anti-inflammatory
drugs (NSAIDs) and weak opioids without success. Injection therapy has also been
unsuccessful.
What would be the most appropriate next step in this patient’s management?
A
B
C
D
E
Add gabapentin 300 mg three times a day
Repeat the MRI
Referral to surgery
Referral to a pain management programme
Offer transcutaneous electrical nerve stimulation (TENS)
22. A 26-year-old woman presents with a 5-year history of generalised pain, stiffness
and poor sleep. Extensive investigations have ruled out serious causes and she has
been given a diagnosis of fibromyalgia.
Which of the following would apply to this patient?
A
B
C
D
E
Rheumatoid arthritis co-exists in 10%
The incidence decreases with age
Complete resolution of symptoms is expected
Pharmacological therapy should be avoided
Serotonin is increased in most patients
23. A 64-year-old asthmatic man presents with severe burns to his upper left arm and
abdomen. The wounds on his left arm extend as far as his shoulder, and now have
a foul smelling purulent discharge. He complains of a constant aching pain, which
371
372
Chapter 10
can become very severe at times, both in his arm and his abdomen. The surgeons
want to take him to theatre for debridement of his arm wounds.
The most appropriate option for his postoperative analgesia is:
A
B
C
D
E
Left interscalene block
Paracetamol and ibuprofen
Left axillary block
Intraoperative opioids and postoperative patient-controlled analgesia (PCA)
Left supraclavicular block
24. A 3-week-old neonate is to have a hernia repair under general anaesthesia with
caudal analgesia. His parents ask about alternative methods of pain relief, rather
than a caudal block.
Which of the following would be an appropriate alternative?
A
B
C
D
E
Intravenous paracetamol and codeine phosphate
Intravenous morphine intraoperatively
Paracetamol, ibuprofen, codeine phosphate
Ibuprofen, morphine, and local anaesthetic infiltration to the wound by
surgeons
Paracetamol, local anaesthetic infiltration to the wound, titrated morphine
25. A 42-year-old man with obstructive sleep apnoea and known sickle cell disease
presents with an acutely painful crisis. He suffers from recurrent crises, and on
previous hospital admissions he has required significant amounts of opioids
administered frequently to control his pain. He regularly takes paracetamol and
ibuprofen.
Which of the following is the most appropriate option for his analgesia?
A
B
C
D
E
Morphine PCA
Pethidine
Codeine
Fentanyl PCA
Tramadol
26. A 78-year-old woman is admitted with a type 4 (Crawford classification) aortic
aneurysm. She is haemodynamically stable but the surgical team is asking for
your help in siting an arterial line in preparation for an endovascular repair of her
aneurysm using a fenestrated aortic graft.
Which of the following sites would be most appropriate for inserting an arterial
line?
A
B
C
D
E
Right radial artery
Left radial artery
Right dorsalis pedis artery
Left dorsalis pedis artery
Right femoral artery
Questions
27. A 72-year-old man requires a unilateral intercostal nerve block for severe pain
caused by a fractured rib.
When performing the intercostal nerve block, where would be the most
appropriate place to infiltrate the local anaesthetic to achieve the highest success
rate for the block?
A
B
C
D
E
At the angle of the rib
Any point proximal to the mid-axillary line
Medial to the angle of the rib
At the mid-axillary line
Lateral to the angle of the rib
28. A 60-year-old patient with a 5-year history of myasthenia gravis is scheduled for a
transcervical thymectomy. He has generalised moderate muscle weakness and has
recently been requiring higher doses of pyridostigmine to control his symptoms.
His preoperative investigations show forced vital capacity (FVC) of 3.5 litres.
Which of the following would be the most appropriate postoperative management
for this patient:
A
B
C
D
E
Reversal and extubation followed by same day discharge
Transfer to the intensive care unit for overnight ventilation
Reversal and extubation followed by monitoring in the high dependency unit
Reversal and use of airway exchange catheter in case re-intubation required
Use of elective plasma exchange to assist chances of successful extubation
29. An 83-year-old man is admitted intubated to the intensive care unit following
a laparotomy for perforative peritonitis. On the fourth day of his admission his
oxygen requirements increase and he begins to desaturate. His oxygen saturation
on 75% Fio2 is 86%. His findings are as follows:
• Pulse 96 beats per minute
• Blood pressure 104/74 mmHg without inotropic support
• Arterial blood gas on 75% Pio2 is pH 7.31, Pao2 7.11 kPa, Paco2, 6.14 kPa
• Chest X-ray shows a positive ‘Luftsichel sign’.
The most likely lung finding is:
A
B
C
D
E
Left upper lobe collapse
Right upper lobe collapse
Right lower lobe collapse
Right middle lobe collapse
Left lower lobe collapse
30. You have been asked to re-write the departmental guidelines for the treatment of
postoperative nausea and vomiting. As part of the research you are reviewing a
recent meta-analysis of pharmacological therapy.
With regards to the forest plot in Figure 10.1 which of the following answers is
most appropriate?
A
All studies would be expected to be weighted equally
373
374
Chapter 10
Figure 10.1 Forest plot of studies comparing
Gipasone and Hurlatron.
Butler et al., 2001
Dexx et al., 2007
Shorey et al., 2010
Ream et al., 2012
Total
Gipasone better
B
Hurlatron better
Gipasone should be part of the treatment algorithm for postoperative nausea
and vomiting
C We can have the most confidence that the results of Butler et al., are
representative of the observed effect
D We would expect that all studies comparing Gipasone with Hurlatron would be
included in the meta-analysis
E Sample size determines the size of the box assigned to each study
Answers
Answers
1. C Invasive arterial blood pressure monitoring
The majority of pituitary tumours are approached surgically by the trans-sphenoidal
route. This involves passage through the sphenoid sinus and removal of the floor
of the pituitary fossa (sella turcica). The fossa is defined laterally by the cavernous
sinus and superiorly by the sella diaphragma. It is important to remain aware that
the cavernous sinus contains portions of the carotid arteries – a cause of significant
and rapid blood loss in the event of surgical trauma. For this reason, in addition to
the potential requirement of careful blood pressure manipulation, invasive arterial
pressure monitoring is essential for all trans-sphenoidal pituitary surgery.
The most common pituitary tumours arise from the anterior lobe and are usually
adenomas, 75% of which are hormone secreting. Hyper-or hyposecretion of growth
hormone (GH), adrenocorticotrophic hormone (ACTH), prolactin (PRL) and thyroidstimulating hormone (TSH) can occur depending on the cell-origin or mass effect of
the tumour. If an adenoma is present that leads to GH or ACTH secretion, the patient
may develop acromegaly or Cushing’s disease respectively. In either case, this may
lead to glucose intolerance or frank diabetes requiring insulin.
Acromegalic patients often present with soft tissue changes particularly of the
larynx and oropharynx. This leads to thickened mucosa, affecting visualisation of
the airway, and glottic stenosis. They may also have an enlarged mandible and
maxilla resulting in poor occlusion of the dental aperture. This renders them at
risk of a difficult airway which can be graded from 1–4. Grade 1 is classified as
minimal mucosal involvement, grade 2 as mucosal hypertrophy in the region of
the naso pharynx and oropharynx, grade 3 as isolated glottic changes and grade 4
as comprising of elements from both 2 and 3. It is recommended that a fibreoptic
intubation is considered for grades 1–2 and a surgical tracheostomy for grades 3–4.
Many patients who suffer Cushingoid or acromegalic effects from their tumour
acquire obstructive sleep apnoea. This obligates consideration of safe postoperative
airway management and possible ventilation strategies as any positive pressure
ventilation applied nasally is prohibited in the immediate period following transsphenoidal surgery.
Large pituitary tumours may still be resected trans-sphenoidally, provided they
remain midline. If suprasellar extension has occurred a lumbar drain may be
required preoperatively. This enables aliquots of normal saline to be introduced
during surgery thereby causing increased intracranial pressure and subsequent
protrusion of the tumour for improved surgical access. It is also used for drainage
postoperatively in the event of cerebrospinal fluid leak from the surgical site.
Trans-sphenoidal surgery may require preparation for all of the options but invasive
arterial pressure monitoring is always indicated.
Pollard BJ. Handbook of Clinical Anaesthesia. 2nd ed. London: Elsevier Science, 2003.
Smith M, Hirsch NP. Pituitary disease and anaesthesia. Br J Anaesth 2000; 85:3–14.
375
376
Chapter 10
2. E Neurogenic shock
A tension pneumothorax should always be considered in a patient who is
undergoing positive pressure ventilation after intubation. As a result of increasing
pressure within the pleural cavity, the lung collapses and ultimately the
mediastinum shifts. This leads to obstructed venous return and therefore persistent
hypotension until the pressure is released by needle decompression or chest drain
insertion. Hypotension is therefore a relatively late sign and considering the recent
CT scan did not show an existing pneumothorax this is not the most likely reason.
All trauma patients with hypotension should be treated with ongoing suspicion
of haemorrhage. Most sources of significant blood loss, without obvious external
injury, should be identified by a CT scan using contrast media. Even though this
patient has had negative imaging, a sacral fracture can lead to the development of a
retroperitoneal haematoma. The fracture is, however, undisplaced and although this
is not currently the most likely reason it is still one to bear in mind.
Pulmonary embolism is defined as the obstruction of a pulmonary artery or arteriole
by intravascular matter such as air, thrombus or fat. If large, it may lead to prevention
of flow to the left heart, failure of the right heart and subsequent circulatory
collapse. Pulmonary emboli in trauma patients mainly occur as fat (classically
secondary to long bone fractures) or thrombus (more often after significant periods
of lower limb immobilisation). Although this should be considered it is less likely
within the time frame, or associated with the injuries described.
Neurogenic shock occurs when the autonomic pathways are interrupted as in a
spinal cord injury. It leads to hypotension and bradycardia. High thoracic injuries are
particularly associated with these signs as the cardiac sympathetic fibres originate
from T2-T5 thereby resulting in reduced inotropy, unchallenged vagal tone and
decreased systemic vascular resistance. This is the most likely reason in this example.
Spinal shock is described as the absence of reflexes below the level of injury. This
would produce the flaccid areflexia noted in this case and although normally seen
with hypotension from neurogenic shock, does not best define the reason for the
patients fluid resistant hypotension.
Bonner S, Smith C. Initial management of acute spinal cord injury. Contin Educ Anaesth Crit Care Pain
2013; 13(6):224–31.
3D Intravenous induction with propofol and atracurium
followed by low frequency jet ventilation via the
bronchoscope. Maintenance of anaesthesia with propofol
and remifentanil TCI
Anaesthesia for airway surgery raises a number of issues including:
• Shared airway with conflicting needs of the surgeon (clear, unobstructed views
of the operative field) and anaesthetist (airway protection and maintenance of
oxygenation, ventilation and anaesthesia)
• Co-morbidities of the patient group who may have malignant, respiratory and
cardiovascular disease
Answers
Procedures such as the one outlined above are often relatively short (30 minutes)
but intensely stimulating; smooth balanced anaesthesia is essential to reduce the
risk of perioperative myocardial ischaemia.
The rigid bronchoscope is a large instrument and it is highly unlikely that a patient
would be able to tolerate the procedure without general anaesthesia. Although
inhalational induction may be a valid technique, deep anaesthesia alone may
not be sufficient (without paralysis) and the use of intermittently removing the
facemask will increase the risk of awareness as well as hypoxaemia. Use of a
microlaryngeal tube may be acceptable for certain procedures (e.g. supraglottic)
but a microlaryngeal tube may occlude the posterior trachea and when inflated the
cuff will mean any lesions in all but the most proximal part of the trachea would be
inaccessible. These are therefore unfeasible options in this case.
Low frequency jet ventilation is delivered via a handheld trigger device (e.g.
Manujet) attached via a Luer lock connector to the rigid bronchoscope. The operator
can manually deliver oxygen under pressure at a rate of 10–20 breaths per minute.
Volatile anaesthetic agents cannot be delivered via the rigid bronchoscope so total
intravenous anaesthesia (TIVA) is required. Intravenous induction with propofol
and atracurium with low frequency bronchoscopic jet ventilation and TIVA provides
good surgical conditions as well as anaesthesia and is best response given here. It
should be noted that there is a risk of barotrauma and gas trapping when using jet
ventilation and it is not possible to accurately monitor end tidal carbon dioxide or
airway pressures.
High frequency jet ventilation can be delivered via a cricothyroid cannula which may
be left in place for emergency perioperative oxygenation in patients felt to be ‘at
risk’; for example those will difficult laryngoscopy. This would therefore not be the
first choice technique in this case based on the information given.
As these patients are at risk of complete airway obstruction or complications
including bleeding, airway oedema, laryngospasm and barotrauma/
pneumothoraces it is prudent to be familiar with the difficult airway trolley and have
equipment and personnel available to deal with any complications.
English J, Norris A, Bedforth N. Anaesthesia for airway surgery. Contin Educ Anaesth Crit Care Pain 2006;
6(1):28–31.
4. E Flexible bronchoscopy
Smoke inhalation injury is a serious complication of burns and significantly increases
patient morbidity and mortality. Airway injuries in this context can be difficult to
safely manage and requires an appreciation of the risk factors, natural progression
and appropriate investigations available.
During a fire, the upper airway may be injured from chemical irritation and direct
thermal insult resulting in oedema, erythema and ulceration, which can threaten
airway patency. Other factors detrimental to the airway include the systemic
inflammatory response, aggressive fluid administration and accompanying neck
burns causing external compression. The airway oedema is variable but generally
peaks at 24 hours and clinical symptoms such as stridor or dyspnoea may not be
377
378
Chapter 10
obvious until this is substantial. A timely and controlled intubation to protect the
airway is preferable to an emergency procedure so determining which patients are
at risk of upper airway injury or obstruction is important.
Patients who have lost consciousness and been exposed to heat or flames in an
enclosed space for a prolonged time are at higher risk of airway injury. Physical signs
suggestive of airway injury include facial burns, singed nasal hairs, carbonaceous
sputum, stridor, hoarseness and drooling. Certain investigations can also guide
assessment and management of inhalational airway injuries
Flexible bronchoscopy is considered the gold standard for early evaluation of
the upper airway in patients with smoke inhalational injuries and it is the correct
answer for the above scenario. Bronchoscopy allows direct visualisation of the
laryngeal structures and an appreciation of any oedema, ulceration, necrosis or
soot contaminating and threatening the airway. Furthermore, bronchoscopy
allows removal of any airway debris, and the placement of an endotracheal tube if
indicated. Repeat examinations can also be performed to assess the progression of
airway injury.
Pulse oximetry provides continuous non-invasive monitoring of the haemoglobin
oxygen saturation in the arterial blood. It is an important monitor for patients
with suspected smoke inhalation injury as desaturations may indicate worsening
associated upper or lower airway damage. However, in the presence of carbon
monoxide, the monitor will provide an inaccurately high saturation reading since
it cannot distinguish between carboxyhaemoglobin and oxyhaemoglobin. Unlike
bronchoscopy, it cannot diagnose nor grade the severity of the upper airway injury.
Admission chest X-rays are frequently performed in patients admitted with burns
but are insensitive for an inhalational injury diagnosis. Since burns patients are at
risk of developing chest infections and acute lung injury during their illness, the
admission chest radiograph is however still important for establishing a baseline.
Computed tomography has a role in selected burns patients where inhalation injury
is suspected. For example the bronchial wall thickness measured by this imaging
modality can be useful as a predictor for the number of ventilator days and the
development of pneumonia. Unlike bronchoscopy however, direct visualisation and
interventions to treat upper airway pathology is not possible.
Arterial blood gas analysis provides important information concerning the adequacy
of ventilation and acid base status of burns patients. If there is co-existing carbon
monoxide poisoning, this can also be assessed by carboxyhaemoglobin levels.
However, a normal blood gas result does not rule out an inhalation injury, and
the investigation provides no direct information on whether the upper airway is
threatened.
Micak R, Suman O, Herndon D. Respiratory management of inhalation injury. Burns 2007; 33:2–13.
Palmieri T, Gamelli R. Diagnosis and management of inhalation injury. In: Handbook of Burns. Kamolz LP,
Jeschke MG, Brychta P et al, eds. New York: Springer, 2012, pp163–72.
Yamamura H, Kaga S, Kanada K, Mizobata Y. Chest computed tomography performed on admission helps
predict the severity of smoke inhalation injury. Crit Care 2013; 17(3):R95.
Answers
5. E Dantrolene 1–10 mg/kg
In the event of an unexplained significant rise in end-tidal CO₂ and heart rate
with simultaneous increased oxygen requirements, the possibility of malignant
hyperthermia must not be overlooked.
Malignant hyperthermia is a genetically determined error of skeletal muscle
metabolism that is triggered by suxamethonium and volatile anaesthetic agents.
It is thought to arise from a defective gene for the ryanodine/dihydropyridine
receptor on chromosome 19. This leads to an uncontrolled inward flux of calcium
ions and subsequent rapid development of skeletal muscle rigidity. This generates
a hypermetabolic state producing dramatic rises in CO₂, O₂ consumption and
temperature. As the condition persists, haemodynamic instability, rhabdomyolysis,
hyperkalaemia, metabolic acidosis and disseminated intravascular coagulation develop.
The mainstays of initial treatment are to rapidly acquire dantrolene at the earliest
point of suspicion, whilst simultaneously minimising the deleterious effects of
the process. These include informing the team of your diagnosis, calling for help,
hyperventilating the patient on 100% oxygen, removing volatile anaesthesia from
the circuit, maintaining anaesthesia via intravenous agents, cooling the patient and
treating any biochemical abnormalities.
Dantrolene is the only known antidote to malignant hyperthermia and is therefore
the most definitive treatment. The Association of Anaesthetists of Great Britain
and Ireland (AAGBI) guidelines on the recommended stages of management are
available on the AABGI website
Halsall PJ, Hopkins PM. Malignant hyperthermia. Contin Educ Anaesth Crit Care Pain 2003; 3(1):5–9.
Yentis SM, Hirsch NP, Smith GB. Anaesthesia and Intensive Care A-Z. An Encyclopaedia of Principles and
Practice. 3rd ed. London: Elsevier Science, 2003.
6.C Ramped head-up position, preoxygenation, and a
RSI with suxamethonium and cricoid pressure. HDU
postoperatively
Obesity is on the rise in the UK. Weight loss surgery is also a growing field. The
procedures fall into two categories:
Restrictive
The commonest example of this type is the adjustable gastric band (AGB). Here a
fluid-filled band is placed around the proximal stomach creating a small pouch that
fills quickly with food creating the sensation of fullness. The band can be adjusted
by saline insufflation via a subcutaneous port. The AGB is now more popular
than the other types of restrictive treatment, such as the sleeve gastrectomy, and
luminal gastric balloon. The laparoscopic AGB is minimally invasive, reversible and
technically easier and safer than malabsorptive surgery. Complications often relate
to relative obstruction or reflux of food or gastric contents, such as oesophagitis.
379
380
Chapter 10
Malabsorptive
The most common procedure of this type is the Roux-en-Y gastric bypass. This
surgically creates a small pouch of proximal stomach which is then plumbed
directly to the jejunum, ‘bypassing’ the duodenum altogether. Thus the stomach
firstly has an element of volume restriction, with the added benefit of a degree of
malabsorption. This makes the gastric bypass the gold standard weight loss surgery,
with body mass index (BMI) reductions of 10 kg/m2 possible in the first year alone.
It is irreversible, more complex, and has added complications including nutritional
deficiency and dumping syndrome.
Preoperative assessment
Airway assessment should include neck measurement. Studies have shown that
obesity alone doesn’t predict difficult laryngoscopy, but alongside a Mallampati
grade III/IV or a high neck circumference, it does. Difficulty rates were 5% with
a 40 cm neck, rising to 35% with a 60 cm neck. Medical co-morbidities should
be assessed in the usual manner, but particular attention paid to screening for
obstructive sleep apnoea, pulmonary hypertension, right heart dysfunction and
heart failure. Functional testing in the form of cardiopulmonary exercise testing or
stress echocardiography may be indicated. Bariatric patients are regarded as high
risk of aspiration regardless of reflux symptoms and prokinetics, and antacids are the
norm.
Operative factors
Induction often occurs in theatre on table to avoid moving and handling concerns,
but if required a hover mattress may be used for moving patients. The ideal position
is with the patient ‘ramped’ or ‘stacked’, this uses pillows and blankets to raise the
upper torso, shoulders and head to align the tragus of the ear with the angle of
Louis. This has been shown to improve direct laryngoscopy and should facilitate
preoxygenation by increasing functional residual capacity. A proprietary pillow, the
Oxford HELP pillow, is marketed in the UK for this purpose. The surgical position is
usually a modification of the Lloyd–Davis with steep head-up. A shelf is put at the
foot of the table to avoid slippage, and the arms are often out on arm boards. The
physiological strain of pneumoperitoneum is often well-tolerated, and ventilation is
sometimes better than expected due to the degree of positioning the chest above
the abdomen. Pressure point protection must be fastidious, as obese patients are
at high risk. Greatest risks are from venous thromboembolism, with an incidence of
about 5%, and low molecular weight heparin doses must be adjusted to weight as
per local protocol.
The crucial elements of the stem here are the presence of untreated obstructive
sleep apnoea (OSA), in determining postoperative care, and the airway assessment
influencing induction planning. From the outset this gentleman requires higher than
ward level care for his OSA and the gastric bypass procedure. HDU should suffice
unless he encounters any intraoperative obstacles. In terms of the induction, as
discussed the presence of obesity alone doesn’t equal a difficult laryngoscopy, but
increasing neck circumference is shown to correlate. His neck circumference does
Answers
not put him into the highest risks group. In any event, ramped positioning is crucial
to facilitate preoxygenation, laryngoscopy and mask ventilation (if required).
Sabharwal A, Cristelis N. Anaesthesia for Bariatric Surgery. Contin Educ Anaesth Crit Care Pain 2010;
10(4):99–103.
7. A Oesophageal perforation
Repeated instrumentation during a difficult intubation can lead to significant
damage to the airway and surrounding structures resulting in potentially
fatal complications. An unrecognised oesophageal perforation can lead to
retropharyngeal abscess formation, acute mediastinitis, pneumonia and eventually
multi-organ failure and death. Early symptoms and signs can be non-specific;
therefore a high index of suspicion is crucial to avoid delays in management. The
case above contains strong risk factors for an oesophageal perforation which
includes female gender, age older than sixty years and a difficult intubation. Early
symptoms of perforation include sore throat, cervical pain, and cough, whilst fever
and dysphagia may indicate secondary bacterial invasion and abscess formation. Air
may also dissect along cervical fascial planes resulting in subcutaneous emphysema,
pneumomediastinum and pneumothorax. Management depends on lesion severity
and includes cessation of oral intake, intravenous antibiotics, parenteral nutrition
and if indicated surgical repair.
Tracheal rupture can also occur following a forceful difficult intubation and repeated
trauma from airway adjuncts. Following atraumatic intubations, tracheal injury
can still occur if the endotracheal tube is incorrectly sized or the tube cuff overinflated. The most common clinical signs are subcutaneous emphysema, mediastinal
emphysema and pneumothorax, which often develop soon after extubation. Other
signs include dyspnoea, dysphonia, cough, haemoptysis and pneumoperitoneum.
The history of fever and dysphagia in the case above make oesophageal perforation
more likely. The management of a tracheal rupture can be conservative (intubation
with the cuff distal to the rupture, tracheal aspiration, pleural drain if required and
empirical antibiotics) or involve surgical correction.
Uvular necrosis is a rare occurrence and can result from mechanical trauma during
intubation or suctioning. Intraoperative impingement from the endotracheal tube
compromising uvular blood flow has also been described. Symptoms include a
foreign body sensation, sore throat, pain on swallowing, coughing and in severe
cases airway obstruction. Subcutaneous cervical emphysema as described in the
above case is not a usual presentation of uvular necrosis. Treatment is conservative
and management options reported in the literature includes steroids, antibiotics,
topical adrenaline administration and antihistamines.
Arytenoid dislocation can occur as a consequence of direct trauma to the
cricoarytenoid joint during endotracheal intubation. Symptoms include persistent
hoarseness, sore throat dysphagia and stridor. Prompt diagnosis and early operative
correction is important to prevent articular adhesions and ankylosis. A primary
arytenoid dislocation does not cause surgical emphysema as described in the case
above.
381
382
Chapter 10
Aspiration of gastric contents into the lung can occur following repeated intubation
attempts to a difficult airway. The clinical manifestations are wide ranging and
depend partly on the type and amount of aspirate. Solid matter aspiration can lead
to an acute airway obstruction resulting in rapidly progressive hypoxia, whereas
gastric acid contamination can result in an aspiration pneumonitis and the acute
respiratory distress syndrome. Infection from bacteria that normally reside in the
stomach or upper airway can give rise to pyrexia, wheezes and crackles. Treatment is
mainly supportive and sometimes prolonged mechanical ventilation is necessary.
Antibiotics should only be administered to patients who develop pneumonia.
Surgical emphysema, dysphagia and neck stiffness are not common presentations of
aspiration pneumonia.
Domino K, Posner K, Caplan R, Cheney F. Airway Injury during Anaesthesia: a closed claims analysis.
Anesthesiology 1999; 91(6):1703–11.
Miñambres E, Burón J, Ballesteros M, et al. Tracheal rupture after endotracheal intubation: a literature
systematic review. Eur J Cardiothorac Surg 2009; 35(6):1056–62.
Hagberg C, Georgi R, Krier C. Complications of managing the airway. Best Pract Res Clin Anaesthesiol
2005; 19(4):641–59.
8. D Start an adrenaline infusion
The patient most likely has a symptomatic complete heart block that is usually
associated with an inferior myocardial infarction (MI). He demonstrates adverse
features in the form of hypotension; others to be concerned about include syncope,
heart failure or myocardial ischaemia.
The initial management would be administration of 500 μg of atropine intravenously
and assess the patient’s response. If the patient fails to respond to 3 mg of Atropine
in total, the next step is to start a second line agent such as an isoprenaline infusion
at 5 μg/minute or an adrenaline infusion at 2–10 μg/minute. Alternative drugs can be
considered such as aminophylline, dopamine, glucagon or glycopyrronium bromide,
however in a hypotensive patient, adrenaline is a more appropriate option.
Fluids are an appropriate option to treat hypotension without bradyarrhythmia
following an inferior MI but will not correct the cause of hypotension.
Transcutaneous and transvenous cardiac pacing are suitable alternatives to the
pharmacological treatment, the latter requiring significant expertise that might not
be immediately available, but is ultimately the aim.
Resuscitation Council (UK). ALS guidelines for bradyarrhythmias (2010 Resuscitation Guidelines). London:
Resuscitation Council (UK), 2010.
9.B A radial arterial line. Propofol and remifentanil TCI. Cell
salvage and tranexamic acid
Operations on the spine are liable to cause serious complications, and the
understanding of the type of surgery and the general principles is essential to
prevent attendant morbidity. Massive haemorrhage requiring transfusion is one of
the most common, but respiratory or airway compromise, eye injuries (including
blindness), and spinal cord damage may also occur.
Answers
Spinal cord monitoring
Monitoring is used to try to reduce the risk of cord damage during surgery, and
uses electrophysiology to monitor two types of evoked potentials. Somatosensory
evoked potentials (SSEPs), are measured from the brain and receive small signals
from stimuli applied peripherally, usually to the posterior tibial nerves. These are
not affected by volatile anaesthetics, and signals may even be improved by muscle
relaxation as muscle tremor noise goes down. Motor evoked potentials (MEPs), are
larger signals applied to the motor cortex and measured by electrodes in the target
muscles. This type of monitoring allows for interrogation of the integrity of specific
tracts of interest and is increasingly used both in spinal and neurosurgery. Deep
neuromuscular blockade will abolish these measurements and volatile anaesthetic
concentrations above 0.5 MAC make the readings invalid, therefore if MEPs are to be
used total intravenous anaesthesia (TIVA) is the maintenance of choice.
Prone position
Essential for most surgery with a posterior approach, this is best accomplished with
diligence and an experienced team. The tracheal tube must be well fixed, and a ‘bail
out’ emergency plan for airway loss whilst prone must have been considered and
discussed amongst the team. The patient’s body must be supported at the level of
the mid chest (lower pectoral) and waist levels, leaving the abdomen relatively free
and uncompressed. There are ready made padding systems to deliver this position,
such as the Montreal mattress. If well positioned, there is less compression of the
inferior vena cava and less impairment of venous return. This avoids reduced cardiac
output and increased transmitted pressure into the epidural venous plexus (which is
vulnerable to pressure effects due to an absence of valves), and also reduces the risk
of lower limb thrombosis.
Once this position is safely achieved, meticulous detail must be paid to ensuring
pressure areas are well padded. Particular problems can be encountered with the
ulnar nerve at the elbow, as well as the brachial plexus. Avoiding traction on the
brachial plexus is achieved by ensuring the arms, if by the head, have the humeri
abducted to < 90° and the forearms lying slightly below the level of the chest. If the
arms are to be by the side, then the hands should be slightly supinated with the
thumbs pointing downward.
Eyes
Spinal surgery has the highest rate of eye and visual complications. Postoperative
visual loss may result from two types of damage: ischaemic optic neuropathy
(ION) and central retinal artery occlusion (CRAO). Of the two, ION is by far the most
common. ION is thought to be caused by optic nerve hypoperfusion, and is linked
to intraoperative anaemia/massive blood loss, long surgery (especially > 6 hours),
obesity, and male sex. Interestingly diabetes and vascular disease are not clear risks
for ION. CRAO is caused by direct extrinsic pressure, and is mostly unilateral, and
seen with other sequelae of damage to the local area such as ptosis.
As described above in this case where cord monitoring is to be used, volatile
anaesthesia will detract from the readings ruling out stems A and C. Given the preexisting history of anaemia and the type of surgery, most would regard the use
383
384
Chapter 10
of cell salvage as mandatory, removing stem E. The final discriminator between
the two remaining options, B and D relates to the use of supplementary central
venous access. Whilst many would choose to place a central venous catheter, in this
relatively well patient with good peripheral access it is not essential. If used, femoral
is not the ideal site for a patient in the prone position.
Nowicki RWA. Anaesthesia for major spinal surgery. Contin Educ Anaesth Crit Care Pain 2013 14(4):147–52.
10. E Tibial nerve
Ankle blocks are indicated for foot and toe surgery. They are easy to perform and
provide adequate analgesia for a variety of procedures on the foot. Five nerves
innervate the ankle; four are branches of the sciatic nerve (tibial, superficial and
deep peroneal, and sural) and one is a branch of the femoral nerve (saphenous
nerve).
Good anatomical knowledge is essential for a successful ankle block. Two of the five
nerves are deep (tibial and deep peroneal) and three are superficial (sural, superficial
peroneal and saphenous nerves) (Figure 10.2).
Figure 10.2 Sensory distribution
of nerves of the foot.
1. Superficial peroneal nerve
2. Saphenous nerve
3. Sural nerve
4. Deep peroneal nerve
5. Calcaneal nerve
6. Lateral plantar nerve
3
7. Medial plantar nerve
4
2
7
6
1
2
3
4
5
Tibial nerve: This is one of the deep terminal branches of the sciatic nerve. The
nerve is divided into medial plantar and lateral plantar nerves, and also gives off
the calcaneal nerve. It innervates the plantar surface of the foot and heel. The tibial
nerve is blocked by injecting local anaesthetic (LA) behind the medial malleolus. The
injecting needle is advanced posterior to the pulsation of the posterior tibial artery.
Once contact with the bone is felt, the needle is withdrawn 2 mm, and 2–5 mL of LA
is injected at this point. The tibial nerve is the largest terminal branch of the sciatic
nerve and takes up to 20 minutes for the nerve block to be established. Therefore,
you should always start an ankle block with the tibial nerve. It is also the only nerve
in the ankle that can be identified by a nerve stimulator (plantar flexion of the toes).
Answers
Deep peroneal nerve: this nerve innervates the webbed space between the 1st
and 2nd toes. This nerve can be blocked just lateral to the tendon of extensor
hallucis longus (EHL). The tendon can be made more obvious by asking the patient
to dorsiflex the big toe. After palpating the dorsalis pedis artery lateral to the EHL,
the needle is introduced until a contact is made with the bone. The needle is then
withdrawn slightly and 2–3 mL of LA is injected after aspiration.
Saphenous nerve: This is a terminal cutaneous branch of the femoral nerve. It
descends on the medial side of the calf. It supplies the medial aspect of the leg
and the medial malleolus, and may also supply the medial margin of the foot. The
saphenous nerve is blocked with a subcutaneous injection of 5 mL of LA above the
medial malleolus.
Superficial peroneal nerve: This is a branch of the common peroneal nerve. It
travels down the leg between peroneus longus and peroneus brevis muscles. It
then runs under the deep facia in a groove between the peroneus brevis and the
extensor digitorum longus. After piercing the deep fascia, it becomes superficial in
the anterolateral compartment of the leg and then divides into superficial branches
that innervate the dorsum of the foot. Injecting 5 mL of LA subcutaneously along the
inter-malleolar line can block the nerve successfully.
Sural nerve: The sural nerve is derived from the tibial nerve in the popliteal fossa. It
is a superficial nerve and it travels down the posterior aspect of the leg and behind
the lateral malleolus. It supplies the lateral malleolus and the lateral margin of the
foot. Injecting 5 mL of LA in the midpoint between the Achilles tendon and the
lateral malleolus can block this nerve.
Allan A, Scarfe M. Ankle block: landmark and ultrasound technique. Anaesthesia Tutorial of the Week 178.
10th May 2010.
11. C Rapid sequence induction
This patient needs urgent neurosurgical intervention to evacuate his haematoma.
His clinical picture suggests rapid progress of the haematoma. A new CT scan
would not add more the clinical picture and it may delay the transfer. Although an
isolated arterial blood gas sample is a useful result to have, it is unlikely to change
the outcome, speed or safety of transfer. A rise in intracranial pressure (ICP) may be
the cause of his deterioration but mannitol is only used as an acutely temporising
measure in a patient who is coning whilst waiting for surgery. Hypothermia for
management of acute brain injury is suggested to be beneficial for reducing the
cerebral metabolic rate of oxygen (CMRO2), but its acute use has not yet been
proven and, again, is unlikely to change the outcome of this patient.
However, the rapid neurological progress and ongoing vomiting renders a transfer
without a secure airway unsafe. Therefore rapid sequence induction and securing the
patients airway is the appropriate next step. This would also enable the anaesthetist
to optimise ventilation to control the intracranial pressure by targeting a Paco2 of
4.0–5.0 kPa.
National Institute for Health and Care Excellence (NICE). Head injury: triage, assessment, investigation and
early management of head injury in infants, children and adults. CG No 65. London: NICE, 2007.
Mishra LD, Rajkumar N, Hancock SM. Current controversies in neuroanaesthesia, head injury management
and neuro critical care. Contin Educ Anaesth Crit Care Pain 2006; 6(2):79–82.
385
386
Chapter 10
12. E Targeted temperature management for 24 hours
This is a difficult question. All are appropriate actions to ensure complete
management of your patient. The differential diagnosis of a sudden collapse is
broad, but most significantly could be:
• Arrhythmogenic (sudden acute arrhythmia such as ventricular fibrillation or
complete heart block);
• Cardiogenic (such as an acute myocardial infarction causing myocardial failure);
• Vascular (aortic aneurysm rupture);
• Obstructive (such as a pulmonary embolism);
• Intracranial event (such as a subarachnoid hemorrhage).
Making efforts to diagnose the cause of arrest will no doubt help in management.
For the options above:
1. There is no evidence of ischaemia on the ECG, suggesting no sudden occlusion of a
coronary vessel. Therefore anti-platelets may not be the key intervention. Similarly a
coronary angiogram may demonstrate unobstructed coronary arteries.
2. An urgent echocardiogram is vital to look at cardiac function. It is particularly
helpful at diagnosing a sudden ischaemic event (with regional wall abnormality)
or suggesting a pulmonary embolism (with a dilated right ventricle and high
pulmonary pressures). However since blood pressure is maintained without
augmentation it is questionable whether the echocardiogram will provide you
with information that will alter the management in the immediate-term.
3. A CT pulmonary angiogram is an important test and may provide a diagnosis.
With a normal blood pressure thrombolysis is not indicated. Treatment with
anticoagulation may be presumptively commenced (also indicated for coronary
vessel disease).
4. There is no option for an urgent CT head but this would also be a vital investigation
as an intra-cranial event may require emergency surgical management.
The question is asking for the most beneficial intervention, not the first. Therapeutic
hypothermia after out-of-hospital cardiac arrest has got a good body of evidence
that suggests improved neurological outcome and mortality outcomes at 6 months.
A recent study has demonstrated that a targeted temperature management
approach of 36°C is non-inferior to targeting a temperature of 33°C, the suggestion
is that a targeted approach and avoidance of pyrexia are more important than
the specific temperature chosen. Many departments would still opt to target a
temperature of 33°, but this practice appears to be decreasing.
Should a temperature of 32–34°C be chosen, cooling should be commenced in the
emergency department with infusion of cool crystalloids and application of cooling
blankets if possible. In the intensive care unit this is continued until a temperature
of 32–34°C is achieved within 4 hours of return of spontaneous circulation. This
may be done with cooling blankets or intravascular extra-corporeal devices,
controlled electronically and titrated to maintain desired temperature. Hypothermia
is maintained for 12–24 hours before re-warming commences at 0.25–0.5°C/
hour and neurological function can then be assessed. Complications should be
managed in a supportive manner including shivering, which should be treated with
Answers
pharmaceutical paralysis as it is metabolically demanding and increases myocardial
oxygen demand. It remains to be seen if this therapeutic method will remain
accepted practice in the future, but what is accepted is that targeted temperature
management is perhaps more important than the specific temperature chosen.
Luscombe M. Clinical applications of induced hypothermia. Contin Educ Anaesth Crit Care Pain 2006; 6
(1):23–27.
Deakin CD, Nolan JP, Soar J, et al. European Resuscitation Council guidelines for resuscitation 2010,
Section 4: adult advanced life support. Resuscitation 2010;81:1305–52.
Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after
cardiac arrest. N Engl J Med 2013; 369(23):2197–206.
13. D Serum creatinine rise
Acute kidney injury (AKI), is defined as an abrupt deterioration in renal function
occurring over 48 hours. The prevalence in hospitals is 1–7% and even a small rise in
creatinine is associated with an increased mortality, ranging from 10% to 80%.
In 2009 the National Confidential Enquiry into Patient Outcome and Death (NCEPOD)
published ‘Adding Insult to Injury’ which found that we were deficient in identifying
patients at risk of AKI and in 50% of cases our management could have been more
timely to prevent renal deterioration. This prompted the National Institute for Health
and Care Excellence (NICE) to publish recommendations highlighting the importance
of identification of risk factors and of prompt treatment.
Risk factors include:
•
•
•
•
Age over 65 years old
Male gender
Pre-existing renal disease
Co-morbidities:
–– Congestive cardiac disease
–– Hypertension
–– Diabetes
–– Ascites
• Surgery:
–– Emergency
–– Prolonged, major surgery
–– Intra-peritoneal
• Anaesthesia:
–– Hypotension
–– Hypovolaemia
–– Blood transfusion
–– Nephrotoxic drug administration
The diagnosis may be made with either the RIFLE, AKIN or KDIGO classifications (the
latter two being very similar). They are based on RIFLE (Risk, Injury, Failure, Loss,
End-stage), which is a useful way to remember the steps to disaster, but the recent
modification is more sensitive and reflects recent evidence that even a small increase
in the serum creatinine concentration results in significantly increased morbidity and
mortality (see Tables 10.1 and 10.2).
387
388
Chapter 10
Table 10.1 AKIN diagnostic criteria for AKI
Timing
Abrupt loss of kidney function (within 48 hours)
Diagnosis (any of
the following)
An absolute increase in serum creatinine of 26.4 μgmol/l
A 1.5 times increase in serum creatinine compared to baseline
A decrease in urine production of less than 0.5 mL/kg for 6 hours or more
Table 10.2 AKIN Classification of AKI
Stage
Serum creatinine criteria
Urine output criteria
1
Increase in serum creatinine ≥ 26.4 μmol/L
or
Increase > 1.5–2 times from baseline
< 0.5 mL/kg/hour for > 6 hours
2
Increase in serum creatinine 2–3 times from
baseline
< 0.5 mL/kg/hour for > 12 hours
3
Increase in serum creatinine > 3 times from
baseline
or
Serum creatinine ≥ 354 μmol/l with an acute
increase ≥ 44 μmol/L
or
Receiving renal replacement therapy (RRT)
< 0.3 mL/kg/hour for > 24 hours
or anuria for 12 hours
To qualify for a particular stage the patient must meet either urine output or serum
creatinine criteria.
The patient described above has many risk factors that may pre-dispose her to
developing AKI. In addition to her co-morbidities, she has had intra-peritoneal
surgery in which crystalloid administration is often rationalised to prevent
anastomotic oedema and dehiscence.
Having six of the above risk factors infers a greater than 10% risk of AKI. The oliguria
described in the question does not meet AKI criteria by itself. The most evidencebased concerning element in her story is her creatinine rise of 1.5 times her baseline
which indicates AKI stage 1 and is associated with a 10% mortality or greater
depending on how this situation progresses. Early intervention is indicated to
prevent further deterioration in the renal function.
C Battle, A Hellewell. Peri-operative renal dysfunction. Anaesthesia Tutorial of the Week 227. London:
World Federation of Societies of Anaesthesiologists, 13 June 2011.
National Institute for Health and Care Excellence (NICE). Acute kidney injury: prevention, detection and
management of acute kidney injury up to the point of renal replacement therapy. CG No 169. London:
NICE, 2013.
Answers
14. E Intravenous administration of 40mg of furosemide and
2.5 mg of diamorphine
This man has the following clinical issues:
1. Clinical evidence of pulmonary oedema with a raised jugular venous pressure
(JVP)
2. Hypotension with evidence of end-organ dysfunction (agitation)
3. Acute kidney injury (AKI) Stage 1 on the basis of his urine output being less than
0.5 mL/kg/hour for 6 hours, according to the AKIN classification (see Table 10.2,
Question 13).
The pulmonary oedema may be due to different etiologies, either due to
excess intravascular fluid or ineffective cardiac activity. Excess intravenous fluid
administration for the treatment of oliguria post-operatively may be implicated.
Alternative possibilities include acute cardiac decompensation due to an ischaemic
cardiac event, electrolyte disturbance or a cardiac arrhythmia.
Acute heart failure should be managed with an ABC approach. Sitting the patient
upright reduces the central venous pressure and therefore the preload, which
can result in improved cardiac output. Oxygen therapy, intravenous access,
electrocardiogram, a chest radiograph, an arterial blood gas and repeat blood
science analysis including serum troponin concentration are all immediately
indicated. Treatment options include:
• Treat reversible causes:
–– Coronary reperfusion therapies
–– Anti-arrhythmic agents
–– Electrolyte correction
• To reduce the preload via venodilation:
–– Loop diuretic administration results in immediate venodilation
–– Diamorphine or morphine administration reduces central sympathetic activity
resulting in venodilation
–– Glyceryl trinitrate (GTN) infusion
• To reduce the preload by reducing circulating volume:
–– Loop diuretic administration results in delayed diuresis
–– Haemofiltration for accurate control of fluid balance
• To augment cardiac output:
–– Continuous positive airway pressure or non-invasive ventilation reduces
ventricular distention and improves cardiac contractility
–– Inotrope administration
–– Mechanical augmentation such as a intra-aortic balloon pump
• To provide cardiac or respiratory replacement:
–– Extra-corporeal membrane oxygenation
Regarding the options in the question, all interventions may be needed at some
stage. Investigations are important but take time to yield results and more urgent
action is required in this situation. Fluid administration may be used to treat
hypotension and oliguria but in the presence of pulmonary oedema (the more
pressing clinical priority) may be detrimental. That leaves us with management of
389
390
Chapter 10
his heart failure with the most appropriate therapy at this stage being the easiest to
administer, the least invasive and the most rapid to instigate.
Valchanov K. Inpatient management of advanced heart failure. Contin Educ Anaesth Crit Care Pain 2008;
8(5):167–71.
15. A Ischaemic bowel
During critical illness or the perioperative period, it is important to consider every
patient’s nutritional status and requirements. Nutritional requirements should aim
to address any pre-existing malnutrition, support the catabolic response to surgery
or critical illness and aid rehabilitation. Malnutrition is associated with impaired
immunological function and increased morbidity and mortality.
The detection of acute malnutrition can be challenging and at present no
specific markers exist. Surrogate markers for chronic nutritional status include
anthropometric measures and biomarkers such as albumin, pre-albumin,
transferring and haemoglobin.
Following the advent of acute critical illness, the early (within 24–48 hours)
instigation of nutritional support has been demonstrated to improve patient
outcomes, however conflicting evidence exists concerning the merits of hypocaloric
verses normocaloric targets. Furthermore, the optimal method (continuous verses
bolus) and composition remains undefined.
The National Institute for Health and Care Excellence (NICE) recommendations for
assessing a patient’s nutritional requirements are summarised below:
1. Screening on admission to include:
• assessment of body mass index (BMI)
• percentage unintentional weight loss and time over which nutrient intake has
been unintentionally reduced
• likelihood of future impaired nutrient intake
2. Recognise
• Malnutrition
–– BMI < 18.5 kg/m2
–– unintentional weight loss > 10% in past 3–6 months
–– BMI <20 kg/m2 or > 5% unintentional weight loss
–– over 3–6 months
• At risk of malnutrition
–– eaten little or nothing for more than 5 days and/or likely to eat little or
nothing for the next 5 days or longer
–– poor absorptive capacity, and/or high nutrient losses and/or increased
nutritional needs from causes such as catabolism
3. Treat
• Oral if safe swallow
• Enteral if unsafe swallow or inadequate oral intake and gastrointestinal tract
accessible
• Parenteral if unsafe swallow or inadequate enteral intake and gastrointestinal
tract inaccessible
• Correct prescribing
Answers
4. Monitor indications, route, risks, benefits and goals of nutrition support at regular
intervals
There are published guidelines by NICE and The American Society for Parenteral and
Enteral Nutrition (ASPEN) in partnership with the Society of Critical Care Medicine
(SCCM), covering all aspects of nutritional support in the acute patient and critical
care settings. Though much debate continues with regard to the appropriate
indications for parenteral nutrition, most agree that it should not be commenced
unless the enteral route is inaccessible and likely to remain so for > 7days. The UK
CALORIES Trial published in October 2014 found no mortality difference between
enteral and parenteral routes of feeding critically ill patients. The current balance
of evidence suggests significant advantages of the enteral route that include less
infectious complications, thought to be secondary to reduced villous atrophy and
bacterial translocation within the gastrointestinal tract.
Previous theories mandating ‘resting of the gut’ have been disproven. Traditionally
enteral nutrition was avoided in pancreatitis, however the British Society of
Gastroenterology now recommend enteral feed; there appears to be little difference
in outcomes between nasogastric or nasojejunal routes. Similarly paralytic ileus does
not preclude enteral nutrition and starting a low rate with vigilance for intolerance is
advised. Intolerance should be monitored through 4-hourly feeding tube aspirates
and prokinetics such as metoclopramide and erythromycin can be added pending
no contraindications. Bowel anastomosis should not prevent enteral nutrition
unless a concern regarding anastomotic leak exists. Short bowel syndrome results
in problems with malabsorption and high output stoma / fistulae. Enteral nutrition
can be trialed with the use of thickening agents; however it is likely that a combined
enteral and parenteral approach may need to be adopted. Enteral nutrition may
induce or worsen bowel ischaemia especially in the presence of hypotension and is
therefore not recommended in suspected or proven bowel ischaemia.
National Institute for Health and Care Excellence (NICE). Nutritional support in adults. CG No 32. London:
NICE, 2006.
Edmondson WC. Nutritional support in critically ill patients. Contin Educ Anaesth Crit Care Pain 2007;
7(6):199–202.
Fremont RD, Rice TW. How soon should we start interventional feeding in the ICU? Curr Opin
Gastroenterol 2014; 30(2):178–81.
McClave SA, Martindale RG, Vanek VW et al. The ASPEN Board of Directors, and the American College of
Critical Care Medicine. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the
Adult Critically Ill Patient. J Parenter Enteral Nutr 2009; 33:277–316.
Working Party of the British Society of Gastroenterology, Association of Surgeons of Great Britain and
Ireland, Pancreatic Society of Great Britain and Ireland, Association of Upper GI Surgeons of Great Britain
and Ireland. UK Guidelines for the Management of Acute Pancreatitis. Gut 2005; 54(3):1–9.
Harvey SE, Parrott F, Harrison DA, et al. CALORIES Trial Investigators. Trial of the route of early nutritional
support in critically ill adults. N Engl J Med 2014;371(18):1673-84.
16. D IV
Subarachnoid haemorrhage (SAH) is a neurological emergency. Anaesthetists may
be involved at presentation, intraoperatively during neurosurgical procedures or to
manage the patient in a critical care environment.
391
392
Chapter 10
Subarachnoid haemorrhage is bleeding into the subarachnoid space; it is important
to differentiate it from intracerebral haemorrhage (ICH), which is bleeding within the
brain parenchyma.
SAH has female preponderance, usually presenting between 40 and 60 years of
age, as in this case. SAH represents approximately 5% of all cause cerebrovascular
accidents, which is equivalent to 6–12/100,000 of the UK population. Though rare,
it has potentially devastating and rapidly irreversible sequela, with an estimated
mortality of 50%.
Spontaneous (as opposed to traumatic) SAH is invariably caused the rupture of a
saccular aneurysm, at bifurcations within the circle of Willis. Associations include
acquired conditions such as hypertension, atherosclerosis, sympathomimetic use
such as cocaine and alcohol, alongside congenital causes such as polycystic kidney
disease and Ehlers-Danlos syndrome.
The presentation of subarachnoid haemorrhage is classically with a ‘thunderclap’
headache, decreased GCS and signs of meningism as in this case. Focal neurology
may also be present. A careful history is required, where possible, to exclude
differential diagnosis such as cluster migraines, meningitis and other causes of
cerebrovascular accidents.
Urgent imaging is required for diagnosis, and excludes serious complications such
as hydrocephalus and cerebral oedema. Although a non-contrast head CT should
suffice, MRI can also be performed to diagnose SAH; however the logistics involved
are usually not merited in the emergency situation. Where available, CT angiography
should be performed to identify the source of the SAH; this investigation has both
high sensitivity and specificity. Due to the sensitivity of neurological imaging, a
lumbar puncture is reserved where clinical uncertainty persists in the face of nonconclusive imaging.
Grading the SAH can be clinical or radiological. The World Federation of Neurological
Surgeons Scale (WFNSS) provides a clinical grading system (Table 10.4).
Table 10.4 The World Federation of Neurological Surgeons Scale (WFNSS)
Grade
GCS
Motor deficit
I
15
Absent
II
13–14
Absent
III
13–14
Present
IV
7–12
Absent or present
V
3–6
Absent or present
Mortality increases from 30% with grade 1 to 90% with a grade V SAH. This patient
had a GCS 7/15 prior to intubation and no focal neurology, thus representing a grade
IV haemorrhage on the WFNSS scale. An alternative grading system is the Fischer
scale which is a radiological grading system.
Answers
This patient did not present to a neurosurgical centre and timely management
will affect prognosis. The decrease in GCS mandated intubation and ventilation in
view of the diagnosis. As with other neurological emergencies, neuroprotection to
prevent secondary injury is vital.
Specific to the management of a subarachnoid haemorrhage are supportive and
surgical strategies. Supportive strategies include:
• Adequate sedation and analgesia
• Blood pressure < 200/100 mmHg in unsecured aneurysms, balancing the risks of
further bleeding against those of hypoperfusion
• Avoid hypomagnesaemia, however hypermagnesaemia does not provide
additional benefit (IMASH Trial 2010)
• Nimodipine – to reduce the incidence and severity of cerebral arterial vasospasm
(calcium channel antagonist)
• Non-pharmacological venous thromboprophylaxis and stress ulcer prophylaxis
Fundamentally, urgent neurosurgical advice and intervention should be sought.
Interventional options are:
• neuroradiological: coiling of intracranial aneurysm
• neurosurgical: clipping intracranial aneurysm
The ISAT trial (2005) was a multicenter, randomised controlled trial comparing
coiling to clipping. The trial suggested more independent survivors with coiling
at one year; however the coiling group also had a higher risk of re-bleeding.
Neurosurgical centres now follow local protocols, but increasingly clipping is
reserved for aneurysms not amenable to coiling. Coiling is less expensive and avoids
the patient undergoing a craniotomy.
Securing the aneurysm in a timely fashion is core to the management of SAH.
However a number of complications affect the course of the patient with SAH, which
need to be sought on presentation and during the critical care management.
• Re-bleeding: particularly within first 2 weeks
• Vasospasm: challenging to definitely diagnose, transcranial Doppler maybe
useful. Mainstay of management is currently supportive, intra-arterial vasodilators
are controversial
• Hydrocephalus: relatively common (20–30%), diagnosed on CT and requires
urgent external ventricular drainage
• Seizures: no evidence for prophylactic anti-seizure medications, but aggressive
management of seizures is paramount
• Endogenous catecholamine induced severe myocardial depression: diagnosed
clinically using biomarkers such as troponin and brain natriuretic peptide (BNP)
and echocardiography. Management is supportive
• Endocrine abnormalities including cerebral salt wasting syndrome (SWS) and
syndrome of inappropriate antidiuretic hormone (SIADH, see paper 4, question 2)
Wong GK, Poon WS, Chan MT, et al. Intravenous magnesium sulphate for aneurysmal subarachnoid
hemorrhage (IMASH): a randomized, double-blinded, placebo-controlled, multicenter phase III trial.
Stroke 2010; 41(5):921–26.
Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical
393
394
Chapter 10
clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised
trial. Lancet 2002; 360:1267–74.
Luoma A, Reddy U. Acute management of aneurysmal subarachnoid haemorrhage. Contin Educ Anaesth
Crit Care Pain 2013;13(2):52–58.
Dorhout Mees SM, Rinkel GJ, Feigin VL, et al. Calcium antagonists for aneurysmal subarachnoid
haemorrhage. Cochrane Database Syst Rev 2007;(3):CD000277.
17. D Perform the LSCS under general anaesthesia
This patient is suspected of having spina bifida and, unfortunately, there is no
information about her condition. Immigrants often present late antenatally and
organising their care can be a challenge for the obstetricians and anaesthetists.
An urgent MRI may be possible prior to delivery in certain hospital settings, but
in this case it is impractical since the patient is already contracting. It will be
uncomfortable for her to undergo an MRI in her present state. Although there is
no evidence that MRI is unsafe in pregnancy, it is best performed when there is an
urgent clinical need, such as neurological compromise, which does not exist in this
case.
Performing the LSCS under central neuraxial blockade is an option, but without a
prior scan, there is no way of knowing at what level the abnormality lies. Even if this
level were to be known, both epidural and spinal local anaesthetic spread can be
wildly unpredictable, with a high block or even an inadequate block being possible.
For these reasons amongst others, many anaesthetists would steer well clear of any
central neuraxial blockade in such patients.
Performing the LSCS under general anaesthetic is the best option in this case. This
should obviously be explained to the mother, with the risks and benefits being made
clear. There is always a difficult airway risk in the obstetric population, but patients
with spina bifida may also have a difficult airway. Full airway assessment must be
undertaken and difficult airway equipment checked and ready.
Vaginal delivery of the breech baby, although possible, is not without risks, and if
undertaken, there is still the risk that an even more urgent Caesarean section may
become necessary. Obviously, a Caesarean section would be best undertaken with
as much planning as possible. This is not the kind of case you want to be doing in a
rush.
Griffiths S, Durbridge JA. Anaesthetic implications of neurological disease in pregnancy. Contin Educ
Anaesth Crit Care Pain 2011; 11(5):157–61.
18. A Perform a rapid sequence induction and secure his
airway with an endotracheal tube
The first priority in managing a child with trauma is to ensure a patent and protected
airway. Indications for intubation are similar to adults: respiratory inadequacy,
reduced Glasgow coma scale (<8), suspected raised intracranial pressure, need
for prolonged ventilation, and need for transport to tertiary centre. This child has
a Glasgow coma scale of 6 (eyes 1, motor 4, verbal 1), and had a high probability
of head injury with raised intracranial pressure. His airway should first be secured
Answers
with an endotracheal tube, before proceeding to other treatment (further fluid
resuscitation, blood transfusion, chest drain) and investigations (FAST scan, X-rays
and CT scan).
Advanced Life Support Group. Advanced Paediatric Life Support: The Practical Approach, 5th ed. London:
BMJ Publishing Group, 2011).
Cullen PM. Paediatric trauma. Contin Educ Anaesth Crit Care Pain 2012; 12:157–61.
Kochanek PM, Carney N, Adelson PD, et al. Guidelines for the Acute Medical Management of Severe
Traumatic Brain Injury in Infants, Children, and Adolescents, 2nd Ed. Pediatr Crit Care Med 2012; 13 (suppl
1): S1–82.
19. C Discuss the case with the hospital’s child protection
team
Child abuse is not uncommon. Evidence from a national UK survey suggests that
the prevalence of serious physical abuse in childhood is around 7%, while sexual,
emotional abuse and neglect each have a prevalence of around 6%. Increased
awareness and familiarity with reporting procedures forms part of an effective
preventive strategy for all healthcare professionals. Anaesthetists may encounter
abused children during resuscitation in the emergency department, in the paediatric
intensive care unit, during routine preoperative assessment, or intraoperatively
during the course of a surgical procedure.
Clinical features that should raise concern or suspicion of non-accidental injury
include:
•
•
•
•
•
•
•
Unusual or excessive bruising, particularly in the non ambulant baby/child
Cigarette burns
Bite marks
Unusual injuries in inaccessible areas e.g. neck, ear, hands, feet & buttocks
Intra-oral trauma
Damage to intra-oral frena, or unexplained frenum injury in a non-ambulant child
Genital/anal trauma where no clear history of direct trauma is offered or part of
the clinical presentation
• Trauma without adequate history eg. intra-abdominal injury
The Royal College of Anaesthetists in association with a number of stakeholders
have developed a flow-chart to guide anaesthetists in the operating theatre who
have child protection concerns. Hospitals generally have designated child protection
doctors, nurses, and midwives to whom more serious concerns can be raised and
cases discussed both formally and informally. There should also be an on call rota
for emergency referrals, and it is important that anaesthetists are familiar with their
local procedures and policies. This often involves the on call consultant paediatrician
who also has a clear safeguarding role, and may be the first person to consult.
Royal College of Anaesthetists, Association of Anaesthetists of Great Britain and Ireland, Royal College of
Paediatrics and Child Health, The Association of Paediatric Anaesthetists of Great Britain and Ireland. Child
Protection and the Anaesthetist : Safeguarding Children in the Operating Theatre. 2014
Melarkode K, Wilkinson K. Child protection issues and the anaesthetist. Contin Educ Anaesth Crit Care Pain
2012;12:123–27.
395
396
Chapter 10
20. C Ask another colleague to attempt intravenous access
Intravenous access in children can be difficult, time-consuming and frustrating,
particularly in the small premature infant, the chubby child, and in children
who have undergone multiple previous cannulations. Unhurried preoperative
examination for possible cannulation sites, avoidance of long starvation times and
the use of adjuncts including topical local anaesthetic creams and oral sedatives
improve success rates. Despite these measures, failure of intravenous cannulation
will still occur. A range of alternative methods to access the circulation include
ultrasound guided peripheral intravenous cannulation and central venous
cannulation. Occasionally, drug administration via other routes can be considered,
for example intramuscular or intra-osseous.
Instrumenting the airway without intravenous access is a subject of debate both
in the literature and among practicing anaesthetists. In paediatric anaesthesia,
this practice generally considered unsafe because of the risk of precipitating
laryngospasm without an established route for its management.
In most situations, including the one described above, asking a colleague with a
fresh pair of eyes and hands is the most appropriate next step before the other
options are considered.
Tremlett M, Bajwa S. Failed intravenous access in children. Anaesth Intens Care Med 2009; 10:87–92.
Martin R. Instrumentation of the airway in the absence of intravenous access. Paediatr Anaesth 2003;
13:366.
Mohiuddin S, Mayhew JF. Tracheal Intubation without intravenous access. Paediatr Anaesth 2004; 14:621.
21. D Referral to a pain management programme
Patients with long-term back pain often do not recover and the risk of their
symptoms persisting is high. He is not a likely candidate for surgery because
there is no evidence of nerve root compression, and the MRI is unlikely to change
unless he develops new symptoms or signs. There is no evidence that gabapentin
is effective in chronic nociceptive pain and its use in chronic low back pain is not
based on any good randomised trials. Transcutaneous electrical nerve stimulation
(TENS) is a common treatment that uses electrical stimulation over the back to mask
the patient’s pain. TENS delivers high-frequency pulses at sub-motor intensities
to modulate the pain pathways by ‘closing the gate’ to pain fibres. However, all
the evidence thus far points out its lack of effect. This leaves a pain management
programme that aims to improve patient’s ability to cope and manage their
symptoms rather than a reduction in their pain. It has good evidence on improving
functional outcomes and is the most appropriate step in this clinical scenario.
National Institute for Health and Care Excellence (NICE). Low back pain: Early management of persistent
non-specific low back pain. CG 88. London: NICE, 2009
22. D Pharmacological therapy should be avoided
Fibromyalgia is a common cause of widespread pain and is diagnosed clinically
as more than 3 months of widespread pain with 11 out of 18 tender points on
clinical examination. It occurs mostly in the 20–50 year age group but the incidence
Answers
increases with age. Other medical conditions such as rheumatoid arthritis can coexist in approximately 25%. Most patients do not get resolution of their condition
and the aim of therapy is to teach patients to manage their symptoms with a
multidisciplinary strategy. Pharmacotherapy can be useful in the short term but
strong opioids are not recommended. Serum biological amines such as serotonin
and noradrenaline are often decreased.
Dedhia JA, Bone M. Pain and fibromyalgia. BJA: Contin Educ Anaesth Crit Care Pain. 2009. 9(5):162–166.
23. D Intraoperative opioids and postoperative patient
controlled analgesia (PCA)
Burns are extremely painful, not only at initial presentation, but also throughout
their hospital stay pain is a significant cause of distress, and may potentially evolve
into a chronic problem. Effective provision of good analgesia at an early stage is vital.
Typically, patients may experience a constant dull background discomfort, with
sporadic episodes of breakthrough pain. This can be unpredictable and regular
assessment and re-assessment of analgesic requirement and provision is essential.
Furthermore, a burns patient may undergo several painful procedures such as skin
grafting, wound debridement, dressing changes and physiotherapy. Occasionally,
burns patients may have other causes of pain such as fractures associated with the
initial injury or compartment syndrome. These should be sought and addressed
appropriately.
Patients should be assessed and analgesia prescribed on an individual basis. Options
include simple analgesics (paracetamol, non-steroid anti-inflammatory drugs (NSAIDs)
if not contraindicated), opioids, and regional anaesthetic techniques. Analgesia should
ideally be administered in anticipation as a preventive measure, for example, 1 hour
prior to a dressing change. For prolonged procedures, general anaesthesia may be
the best option. Multimodal analgesia is frequently required, and the significant
psychological burden of substantial burns injuries should not be ignored.
Table 10.5 suggests some analgesic options for some of the problems that may be
encountered with burns patients.
Table 10.5 Analgesic options for burns patients.
Type of pain
Burns-related procedures:
Wound debridement, dressing changes, skin
graft
Dressing change
Physiotherapy
Analgesic options
NSAIDs, regional block, LA* patches, Entonox,
LA, regional block, ketamine, opioids
Background pain
Regular NSAIDs, oral opioids
Breakthrough pain
Opioids
Chronic pain
Conventional analgesics, TCAs+, anti-epileptic
medications, CBT++
*Local anaesthetic + Tricyclic antidepressants ++ Cognitive behavioural therapy
397
398
Chapter 10
In this scenario, the patient has an infected wound that would make a suitable
regional block inappropriate. A history of asthma and the fact that significant burns
may be associated with a coagulopathy would make NSAIDs less preferable. His
abdominal pain, together with his postoperative arm pain would best be managed
with a suitable opioid regime.
Norman AT, Judkins KC. Pain in the patient with burns. Contin Educ Anaesth Crit Care Pain 2004; 4(2):57–61.
European Burns Association. European Best Practice Guidelines for Burn Care. Vienna: European Burns
Association, 2013.
24. E Paracetamol, local anaesthetic infiltration to the
wound, titrated morphine
Neonatal pain is often unrecognised and inadequately addressed. Apart from
discomfort to the patient, mismanagement of pain at this stage may have a
significant influence on the way pain is processed in later life. There is some evidence
to suggest that insufficiently treated pain in the first few weeks of life may lead to
hyperalgesia when painful experiences are encountered later.
As with any other age group, pain management should follow a structured
approach. Non-pharmacological techniques which may help include skin-to-skin
contact 10-15 minutes before a painful procedure, oral sucrose administration, or
sucking on a soother. The latter seems to produce a calming effect in the newborn.
Paracetamol is used commonly, and is safe when given in the correct dose. The oral
route is preferred. Rectal absorption is unpredictable, and bioavailability is higher.
Non-steroidal anti-inflammatory drugs (NSAIDs) are generally avoided, unless they
are used to close a patent ductus arteriosus. Use of NSAIDs non-specifically inhibits
prostaglandins that are essential in the development of many organ systems. They
may also cause additional unwanted effects such as impaired thermoregulation,
alterations in renal and cerebral blood flow and disrupted sleep.
Codeine phosphate is often used to good effect in neonates via the oral, rectal, or
intramuscular routes. It should never be administered intravenously as it may cause
severe hypotension.
Morphine is used widely, both intra- and postoperatively. It is often given as a nurse
controlled analgesia (NCA) arrangement. Reduced protein binding and immature
renal and hepatic function mean that the free fraction of morphine in the plasma is
higher, and the plasma half-life is longer. Hence, the dose requirement is less than
one may expect. The unwanted effects are the same in neonates as in any other age
group, but may be more difficult to detect. Respiratory rate can be monitored, but
pruritus and sedation for example, often go unnoticed. After receiving morphine,
neonates should be nursed in an observed area where they can be monitored with
apnoea alarms, oxygen saturation, and electrocardiogram.
Regional anaesthesia remains an excellent choice of analgesia and can often avoid
many of the unwanted effects of systemic analgesia.
In this scenario the most appropriate option is to administer paracetamol, local
anaesthetic infiltration to the wound and titrated morphine.
Haidon JL, Cunliffe L. Analgesia for neonates. Contin Educ Anaesth Crit Care Pain 2010; 10(4):123–127.
Answers
25. D Fentanyl PCA
Sickle cell crises are a frequent reason for referral to pain teams and can be
challenging to treat. Pain itself can precipitate a crisis in those with sickle cell disease.
The National Institute for Health and Care Excellence (NICE) recommend that
patients should be offered analgesia within 30 minutes of hospital presentation.
Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) should be given
regularly if there are no contraindications, in conjunction with an opioid. If no
analgesia has been taken before, a weak opioid, such as codeine, can be used
initially.
Pethidine should be avoided altogether in sickle cell crises, as there is increasing
evidence that it is detrimental to outcome, namely due to the accumulation of
its metabolite, norpethidine. Norpethidine is an irritant to the central nervous
system and can cause dysphoria and convulsions. It is renally excreted, and patients
with sickle cell crises may have a degree of renal impairment, possibly due to
dehydration, NSAID use, or a vaso-occlusive event. Furthermore, a single dose is
unlikely to be effective, necessitating repeated administration.
Judging by previous opioid requirements, a weak opioid such as codeine or
tramadol is unlikely to provide this patient relief, and a PCA seems the most sensible
option.
In view of his obstructive sleep apnoea, morphine is best avoided if possible, and
a fentanyl PCA would be the most appropriate option in this patient although he
should continue to take his paracetamol and NSAID throughout.
National Institute for Health and Care Excellence. Sickle cell acute painful episode: management of an
acute painful sickle cell episode in hospital. CG 143. London: NICE, 2012.
Stone M, Wheatley B. Patient-controlled analgesia. Cont Educ Anaesth Crit Care Pain 2002; 2(3):79–82.
26. B Left radial artery
Crawford classification of the aortic thoracoabdominal aneurysms (TAAA) consists of
five types:
• Type I involves most of the descending thoracic aorta from the origin of the left
subclavian to the suprarenal abdominal aorta
• Type II is the most extensive, extending from the subclavian to the aortoiliac
bifurcation
• Type III involves the distal thoracic aorta to the aortoiliac bifurcation
• Type IV TAAAs are limited to the abdominal aorta below the diaphragm
• Safi’s group have modified this scheme by adding Type V, which extends from the
distal thoracic aorta including the celiac and superior mesenteric origins but not
the renal arteries
Deploying a fenestrated aortic graft requires multiple guide wires to correctly align
the fenestrations with the renal arteries and the mesenteric arteries. Right axillary/
subclavian access is usually required for deploying the superior mesenteric artery
guide wire due to the angle of take off of the artery from the aorta which makes it
impossible to wire from the common femoral or external iliac arteries. The aortic
stent is inserted via the common femoral artery which makes this site and pedal
399
400
Chapter 10
arteries site impractical for insertion of arterial lines. This means the left upper limb
arteries are the only possible arterial monitoring access points that are possible and
practical.
Frederick JR, Woo YJ et al. Thoraco-abdominal aortic aneurysm. Ann Cardiothorac Surg 2012; 1(3):277–85.
27. A At the angle of the rib
The intercostal nerve (ICN) block is used to provide effective analgesia for breast
surgery, thoracic and upper abdominal surgery (thoracotomy, cholecystectomy and
gastrectomy) and fracture ribs. It also used for acute and chronic pain conditions
like herpes zoster, post-thoracotomy pain and cancer related pain. The analgesia
provided by the block is usually lasts for up to 12 hours.
The thoracic nerve roots exit from their respective intervertebral foramina,
then divide into ventral and dorsal primary rami. The dorsal ramus supplies the
paravertebral skin and muscles. The ventral ramus continues as the intercostal nerve,
which enters the subcostal groove of the corresponded rib to lie initially between
the pleura and the posterior intercostal membrane (medial to the rib angle). At the
angle of the rib, the ICN passes between the internal intercostal and the innermost
muscles. At the mid-axillary line, it gives off the lateral cutaneous branch that
supplies the skin and the muscles of the lateral chest and abdominal walls. The final
branch arises as the anterior cutaneous branch which is the continuation of the ICN,
and innervates the skin and the muscles of the anterior thoracic and abdominal
walls.
During its course in the subcostal groove of the rib, the ICN runs in a neurovascular
bundle containing the intercostal vein superiorly, the intercostal artery in the middle
and the intercostal nerve inferiorly.
There are some specific differences at certain levels. T1 intercostal nerve lacks
the lateral and the anterior cutaneous branches. T2 and T3 contribute to the
intercostobrachial nerve. T12 is really a subcostal nerve and some its fibres join with
fibres from the lumbar plexus to form ilioinguinal, iliohypogastric and genitofemoral
nerves.
An ICN block can be performed in different positions, including the prone position,,
lateral decubitus, supine or sitting position. However, it is best performed in prone
position with a pillow under the abdomen and the arms hangings from the sides of
the bed. This accentuates the intercostal spaces and rotates the scapula laterally
The injection point for an ICN block must be proximal to the mid-axillary line before
the the nerve divides. Performing the block at or lateral to the mid-axillary line might
fail to anaesthetise the lateral cutaneous branch. The optimal place to perform the
ICN block is at the angle of the rib where the rib is thicker and the intercostal space
is wider, decreasing the chance to contact the pleura (Figure 10.3). The chance of
pneumothorax increases if the block performed lateral to the angle of the rib.
If the injection site is medial to the angle of the rib, there is a possibility of
subarachnoid spread because the dural sack can extend up to 8 cm from the
midline.
Answers
Figure 10.3 Distribution and
location of the intercostal nerves.
Vein
Artery Intercostal
Nerve
Innermost intercostal muscle
Internal intercostal muscle
External intercostal muscle
Dorsal branch
Intercostal muscle:
External
Internal
Innermost
Intercostal nerve
Lateral cutaneous
branch
Anterior
cutaneous branch
Pleura
Sternum
After cleaning the area with antiseptic solution, the skin over the blocked area is
tensed gently up before a 23–25 G needle is advanced to come in contact with
the lower surface of the rib. The tension is then released, allowing the needle to
move to its correct position and angulation (about 20° cephalad). Maintaining the
20° cephalad angulation increases the chances that the block needle is in close
proximity to the nerve.
The needle is carefully walked off the inferior edge of the rib. and is then advanced
a further 2-3 mm in the intercostal groove to pierce the posterior intercostal
membrane and enter the neurovascular bundle. About 3–5 mL of long acting local
anaesthetic is injected after a negative aspiration. The block then can be repeated in
the remaining spaces.
Complications of the ICN block include pneumothorax (incidence < 1%), local
anaesthetic toxicity due to rich vascular supply and rapid vascular absorption,
visceral and peritoneal injury and spinal anaesthesia.
Kopacz DJ, Thompson GE. Intercostal nerve block. In: Waldman SD (ed), Interventional Pain Management,
2nd Ed. Philadelphia: WB Saunders, 2001:401–408.
28. C Reversal and extubation followed by monitoring in
high dependency unit
Myasthenia gravis is an autoimmune disease caused by the production of IgG
antibodies against the post-synaptic acetylcholine (ACh) receptors located within
the neuromuscular junction. Patients suffering from myasthenia gravis have a
401
402
Chapter 10
reduction in the number of ACh receptors to just 30% of normal. It is clinically
represented by weakness, which is exacerbated by exercise and relieved by rest. It
can be classified by the clinical symptoms into four grades:
Grade I: Ocular signs and symptoms
Grade IIA: Generalised mild muscle weakness responding well to therapy
Grade IIB: Generalised moderate muscle weakness responding poorly to therapy
Grade III: Acute fulminant condition and/or respiratory symptoms
Grade IV: Myasthenic crisis requiring artificial ventilation
The factors which determine elective ventilation post-thymectomy include:
•
•
•
•
Long standing disease (> 6 years)
Forced vital capacity (FVC) < 2.9 litres
History of chronic respiratory disease
Type III or Type IV myasthenia gravis
There is a greater chance of requiring postoperative ventilation for a trans-sternal
thymectomy. Preoperatively well controlled patients can be extubated following
surgery but should be monitored in a high dependency unit postoperatively due
to the high risk of respiratory weakness and decompensation. As this patient has
a vital capacity which is well above the threshold and is not having a trans-sternal
procedure it would be judicious to extubate him and then monitor him overnight for
any respiratory complications if they were to develop.
Thavasothy M, Hirsch N. Myasthenia gravis. Contin Educ Anaesth Crit Care Pain 2002; 2(3):88–90.
29. A Left upper lobe collapse
Atelectasis is the loss of lung volume due to collapse of either whole or part of the
lung. It can be broadly classified into obstructive or non-obstructive.
Obstructive atelectasis is commoner and caused by:
•
•
•
•
•
Tumour
Mucus plugs
Inflammation and infections
Foreign bodies
Blood clots
Non-obstructive atelectasis is less common and is caused by:
•
•
•
•
•
•
•
Interstitial disease
Collapse under anaesthesia
Thoraco-abdominal surgery
Chest trauma
Pleural effusion
Pneumothorax
Pneumonia
The loss of lung volume affects the ventilation/perfusion ratio, impairing compliance
and oxygenation and also can cause increased pulmonary vascular resistance.
Questions
A chest X-ray can be diagnostic in assessment of lung collapse. There can either be
a direct radiographic signs, such as loss of lung volume, or indirect signs including
mediastinal shift A unilateral complete ‘white-out’ suggests involvement of an entire
lung. More often, atelectasis involves a particular lobe with characteristic findings for
each involved lobe.
• Right upper lobe: elevation of the right hilum and oblique fissure on an anteroposterior view. The oblique fissure on the lateral view appears convex superiorly,
unless there is a mass lesion inferiorly which may cause it to appear concave
superiorly. This is called the ‘Golden S’ sign
• Right middle lobe: This is most often overlooked in lobar collapse. There is
radiographic loss of the right heart border silhouette. On a lateral view the right
horizontal and oblique fissures move towards each other leading to a wedge
shaped opacity
• Right lower lobe: There is a triangular opacity along the right heart border along
with obliteration of the right hemidiaphragm
• Left upper lobe: Due to lack of a left horizontal fissure, a left sided upper lobe
collapse leads to a veil-like opacity extending from the hilum and fading as it
progresses inferiorly. On lateral view the oblique (major) fissure is displaced
anteriorly and a hyperexpanded superior segment of the left lower lobe is
apparent. In half the cases this hyperexpanded lobe is positioned between a
collapsed upper lobe and the aortic arch below which gives the appearance of a
crescent of aerated lung called the ‘Luftsichel sign’.
• Left lower lobe: This leads to a retrocardiac opacity, which silhouettes the left
hemidiaphragm.
There are various therapeutic measures which can be utilised to deal with lung
collapse including continuous positive airway pressure, positive end-expiratory
pressure, bronchoscopy and washout, prone position ventilation and high frequency
oscillatory ventilation. The method selected depends on the condition of the
patient, etiology and co-morbidities.
Ray K, Bodenmham A, Paramasivam E. Pulmonary atelectasis in anaesthesia and critical care. Contin Educ
Anaesth Crit Care Pain 2014; 14(5):237-245.
30. C We can have the most confidence that the results of
Butler et al., are representative of the observed effect
A meta-analysis is a means to combine the results of a number of studies statistically,
thus aiming to increase the power of any subsequent analysis and the accuracy and
precision of any conclusion drawn from the data.
The process begins with a systematic review of the relevant literature. Prior to
starting the review the reviewers must draw up criteria that each study must fulfill
in order to be included. Studies which do not fulfill these criteria are rejected as
significant methodological flaws may distort the results and lead to incorrect
conclusions. Such methodological considerations include the randomisation
process, blinding, placebo-control and number of participants. Answer D is therefore
not the best one given here.
403
404
Chapter 10
Once the appropriate studies have been identified and appraised, data can be
extracted and the studies can then be weighted. There are a number of ways in
which this is done but the principle is to assign more weight to those studies that
provide more information about the treatment in question, in this case the ability
of a drug to treat postoperative nausea and vomiting. It is expected that larger
studies exhibit less variance than smaller ones, and therefore large studies are often
weighted more; making answer A incorrect. The effect of the weighting process
could be that smaller, valid studies have less impact on the final position of the
‘diamond’.
Methods of weighting used, for example, by the Cochrane Collaboration take into
account the sample size and the event rate. The statistical concept encompassing
these is the variance. The degree of weighting is shown by the size of the box.
Answer E is therefore only partially correct, in addition to sample size; the event rate
is needed to calculate variance.
Although the results of this fictitious meta-analysis suggest that Gipatron is a
superior treatment for post operative nausea and vomiting, integration into clinical
practice requires further considerations pertaining to side effect profile, cost,
availability, routes of administration etc. More information is therefore needed
before choosing option B.
The horizontal line is the confidence interval and a measure of how uncertain we
are about the described effect. A longer line therefore implies less confidence in
the effect and therefore the true value described in the study. It can be seen that
the study by Butler et al. appears to have the narrowest confidence intervals and so
statistically speaking we can be more confident in those results not being due to
chance.
Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions 4.2.6. The Cochrane
Library 2006; 4, 8a.4.
Egger M, Smith GD, Phillips AN. Meta-analysis: principles and procedures. Br Med J 1997; 315;1533–37.
Index
Note: Page numbers in bold or italic refer to tables or figures respectively.
A
Abciximab 342
Abdominal compartment syndrome 56–57, 66–67
management 67
risk factors 67
Abdominal perfusion pressure (APP) 56
Abdominal trauma, fluid resuscitation in 62
Absolute risk reduction (ARR) 201
Accidental dural puncture (ADP) 30
Activated clotting time (ACT) 76, 154
Activated partial thromboplastin time (aPTT) 17
Acupuncture, in pain management 150–151
Acute kidney injury (AKI) 28, 387
diagnosis 387, 388
principles of management of 29
RIFLE criteria 28, 28
risk factors 387
stage 1 388
Acute renal failure (ARF) 278
Acute respiratory distress syndrome (ARDS) 25, 228
Berlin definition 228
causes of 228
classification of severity 25
extracoporeal membrane oxygenation in 230
general management 229
high frequency oscillation ventilation in 230
inhaled nitric oxide in 230
mechanical ventilation in 229
pathophysiology of 228–229
pharmacological management 230
prone positioning in 229–230
severe, management of 25–26
Adductor canal block 321–324
Adjustable gastric band (AGB) 379
Adrenaline
in anaphylaxis management 79
in hypotension with bradyarrhythmia 382
Adrenoceptor blocking agents 285
Aerobic gram negative bacilli (AGNB) 29
After action review (AAR) 134
Airway management, in children 193, 194
Airway surgery, anaesthesia for 376–377
Alcoholic chronic liver disease 145–146
Alcohol use, and rhabdomyolysis 119
Allodynia 117
Alpha-1 antitrypsin 200
Amiodarone 156
in atrial flutter 14
Amitriptyline
in fibromyalgia 115
in neuropathic pain 36
overdose, management of 26–27
Amniotic fluid embolism (AFE) 192
Anaemia, preoperative 362
Anaesthesia
for airway surgery 376–377
anaphylaxis during 149–150
in remote locations 267
for urgent surgery in pregnant patient 113
Anaphylactoid reactions 220
Anaphylaxis 149–150, 219–220
triggers for 220
Aneurysm coiling, general anaesthesia for 344–345
Anion gap metabolic acidosis 106
Ankle blocks 384–385
Anorexia nervosa 244
Anterior interosseous nerve 269, 270
Anticonvulsants, in post surgical pain 34
Anticubital fossa 269, 270
Anti-diuretic hormone (ADH) 131, 144
Anti-embolism stockings 17
Antimicrobial prophylaxis, in surgery 14
Aortic aneurysm repair, and renal impairment 199
Aortic cross-clamping 39, 118–119
Aortic dissection
with aortic regurgitation 217, 217–218
classification systems 217
management of 217–218
risk factors for 217
Apnoea/hypopnea index (AHI) 148, 284
Apnoea testing 303
ARDSNet ventilator strategy 26
Arrhythmias 39
direct current cardioversion in 39–40
Arterial blood gas (ABG) analysis
burns patients 378
fat embolism syndrome 60–61
Arytenoid dislocation 381
Ascorbic acid deficiency 120
Aspiration pneumonia 382
Aspirin 342
Asthma 67, 187–188
in children 235
management of 68–69
preoperative evaluation and preparation 235
severity of 68
Index
406
Atelectasis 402–403
characteristic of lobe involved 403
chest X-ray in 403
non-obstructive 402
obstructive 402
Atosiban 69
Atrial fibrillation (AF) 188
risk factors 188
treatment 189
Atrial flutter 13
DC cardioversion in 13–14
management 13–14
risk factors 13
Atrial pacing 14
Automated external defibrillator (AED) 132
Awake fibre-optic intubation 137
Axillary block 139
B
Back pain 281, 318, 363
lower 282, 396
Bacterial tracheitis 132–133
Bariatric surgery 311–312
Bazett’s formula, for corrected QT interval 156
Bier’s block anaesthesia 267–269
Bilateral vocal cord paralysis 218
Bilevel positive airway pressure (BPAP) 262
Bisphosphonates, in cancer induced bone pain
359–360
Bleeding, maxillary down-fracture and 18
Brachial plexopathy, and chest wall pain 34
Brachial plexus 140, 141 see also Brachial plexus
blocks
branches of cords 142
cords 140
divisions 140
roots 140
supraclavicular branches 141
terminal branches 140–141
trunks 140
Brachial plexus blocks 138–142, 184
axillary 139, 184–185
infraclavicular 139, 184
interscalene 138–139, 184
supraclavicular 139, 184
Brain injury see also Traumatic brain injury (TBI)
safe transfer of patients with 272–273
severe, and brainstem death 273
Brain natriuretic peptide (BNP) 54
Brainstem death (BSD) testing 143, 223, 297, 303
Brainstem herniation 59
Bronchial blockers 174, 174, 175
Bronchiolitis 133
Bronchopleural fistula 339–340
Bupivacaine 269
Buprenorphine 357
Burns
‘Breathing’ assessment in 231
in children 32–33
cyanide poisoning in 198–199
enteral nutrition in 38
fluid resuscitation after 105, 118, 232
intubation for 105, 225–226, 361
management in 38–39, 118, 231–233, 361
pain in 397–398
referral criteria in 105, 233, 233, 283
rule of 9s, for body surface area (BSA) estimation
232, 232
C
Campylobacter jejuni 27
Cancer pain 36–38, 37, 359–360
Carbamazepine, in trigeminal neuralgia 33–34, 151
Carboprost 69
Cardiac arrest
after cardiac surgery 173
management after 138
targeted temperature management after 386–387
Cardiac disease, in pregnancy 191
Cardiac output monitoring 106–109
Cardiac patients, and non-cardiac surgery 53–54
Cardiac risk index (Lee Index) 53
Cardiac surgery, and coagulation defects 258–260,
259, 260
Cardiopulmonary exercise testing (CPET) 135
anaerobic threshold 136–137
cardiac output 136
measurements and results 136
performing test 135
safety 136
Carotid endarterectomy (CEA) 361–362
Carotid surgery, anaesthesia for 321
Caudal epidural analgesia 345–346
Cell salvage 76
Central neuraxial block (CNB), and epidural abscess
20–21
Central post-stroke pain 152
Central retinal artery occlusion (CRAO) 383
Central venous catheters 24
Centre for Maternal and Child Enquiries (CMACE)
report, on maternal deaths 192
Cerebral blood flow (CBF) autoregulation 337, 337
volatile anaesthetics and 92, 92–93, 93
Cerebral oedema 114
Cerebral perfusion pressure (CPP) 337
Cerebral reperfusion syndrome 361–362
Cerebral salt-wasting syndrome (CSWS) 131–132,
186, 187
Cervical ultrasound 222
Child abuse 395
Child, uncooperative 185–186, 236, 271–272
Chi squared test 363
Chloroprocaine 269
Chronic lower back pain (LBP) 282
Index
Chronic obstructive pulmonary disease (COPD)
protocolised weaning in 276
ventilatory management in 275–276
weaning failure in 276
Chronic post surgical pain (CPSP) 116–117, 117, 238
Clinical Negligence Scheme for Trust (CNST)
regulations 134
Clinical Pulmonary Infection Score (CPIS) 29
Clinical risk management 133–134
assessment 134
awareness 134
identification 134
management 134
re-evaluation 134–135
Clonidine, as anaesthesia for middle ear surgery 178
Clopidogrel 342
Coagulopathy in cardiac surgery patients,
management of 227–228
Coarctation of the aorta 31–32
Codeine, in neonates 197
Codeine phosphate 398
Coeliac plexus block 195–196
in chronic upper gastrointestinal malignancy
152–153
Cognitive behavior therapy (CBT) 282
Complex regional pain syndrome (CRPS) 34, 117,
240–241
Budapest criteria 34, 35
diagnosis 34–35
treatment 35, 35–36
Computed tomography (CT)
burns patients 378
neck infections 222
Confusion Assessment Method in the intensive care
unit (CAM-ICU) 354
Continuous positive airway pressure (CPAP) 139, 262
Coronary artery bypass grafting (CABG) 13
care after 274–275
Coronary artery dominance 77
Crawford classification, of aortic thoracoabdominal
aneurysms (TAAA) 399
Creatinine kinase (CK) 119
Cricoid pressure, use of, for rapid sequence induction
307
Croup 133
CT pulmonary angiography (CTPA) 110–111
Cyanide poisoning 198–199
Cyproheptadine 237
D
Dabigatran 18, 342
Danaparoid 17
Dantrolene, in malignant hyperthermia 379
Da Vinci system 264–265
Day case surgery, selection criteria for 341, 341
Death, criteria 303
Delayed cerebral ischaemia 214–215
Delirium, in critically ill patients 353, 353–354
assessment methods 354
management of 354
risk factors associated with 353
types of 353–354
Dexametomidate, in delirium 354
Diabetes inspidus (DI) 144
Diabetic ketoacidosis (DKA) 65, 106
in children with diabetes 114
management of 65–66
Diabetic patient, and surgery 96
insulin regimens 96
Dobutamine, in septic shock 308
Double lumen tubes 174, 175
and bronchial blockers 174, 174
malpositioning 95, 95–96
Dual antiplatelet therapy (DAPT) 343
Duke Activity Index 135
Duke’s criteria, for infective endocarditis 324–325
Dural puncture, and post-dural puncture headache
103–104
Dysaesthesia 117
E
Echocardiography 222
Electroconvulsive therapy (ECT) 19
anaesthesia for 19–20, 179
and biphasic physiological response 19
Electroencephalogram (EEG), for diagnosis of death
223
Emergence delirium (ED) 70
Endobronchial intubation 55–56
Endotracheal tube (ETT) 55
Epidural abscess, diagnosis and management of
20–21, 363
Epidural analgesia 281
Epidural blood patch (EBP) 355
Epiglottitis 133
Ergometrine 69
Erythropoiesis 362
European Society of Cardiology (ESC) guidelines,
for assessment of cardiac patients for non-cardiac
surgery 53–54
Exercise therapy 282
Extracorporeal membrane oxygenation (ECMO) 26,
230, 350–351
Extra-vascular lung water (EVLW) 107, 108
Extra-ventricular drain (EVD) 63–64
Eye injury, penetrating 153–154
F
Fascia liaca block, in hip fractures 72–73
Fat embolism syndrome 60–61
Femoral catheter 282
Femoral nerve (FN) 321–322, 322
fascia iliaca block 323
3-in-1 nerve block 322–323
407
Index
408
nerve stimulator guided nerve block 322
ultrasound guided block 323
Fentanyl 176, 272, 357
in poly-trauma patient 234
Fentanyl PCA, in sickle cell crises 399
Fibromyalgia 115, 396–397
Filtration gradient (FG) 57
FLACC (Face, Legs, Arms, Cry, Consolability) scale 71,
71
Flexible bronchoscopy, in smoke inhalational injuries
377–378
Flow-volume loops 58, 59
Fluid resuscitation
burns injury 32, 39, 105
paediatric trauma 142
septic shock 144–145
Fluid trials 190, 191
Fondaparinux 17, 18, 343
Foot, nerves of 384, 384
deep peroneal nerve 385
saphenous nerve 385
superficial peroneal nerve 385
sural nerve 385
tibial nerve 384
Foreign body aspiration 340–341, 356
Frailty phenotype 200
Fulminant liver disease, paracetamol overdose and
109–110
G
Gabapentin
post-herpetic neuralgia 73–74
post surgical pain 34, 114–115
Gas embolism 98
detection 98
incidence 98
pathophysiology 98
treatment 98–99
Gas flow within respiratory tract 266
Gastric volume, in injured patient 70
Gate theory of pain 36, 36
Genital tract sepsis 234–235
Gentamicin 14
Gestational thrombocytopenia 356
Glasgow coma scale (GCS) 189
paediatric 78–79
Glaucoma 285
Global end-diastolic volume (GEDV) 107, 108
Glucose control, in non-diabetic patient 348–349
Glycerol gangliolysis 151
Glycopyrrolate 137
Guanethidine 240
Guillain–Barré syndrome 27–28, 131
H
Haematoma, after thyroid surgery 219
Haemochromatosis 200
Haemorrhage 376
Haemorrhagic shock, classes of 62, 62
Haloperidol, in delirium 354
Head and neck infections, imaging studies for
221–222
Head injuries
in children 316
patient transfer in 215–216
Heart failure, management of 389–390
Helium 265–266, 266
Heparin-induced thrombocytopenia (HIT) 17, 18,
312–313
diagnosis of 312–313, 313
4T score for 313, 313
type 1 312
type 2 312
Heparins 298, 342
High frequency jet ventilation 99–100, 100, 377
High frequency oscillation ventilation (HFOV), in
ARDS 230
High impact intervention care bundle, for ventilationassociated pneumonia prevention 29–30
Hip fractures 72–73, 223
anaemia and transfusion 224
echocardiography 223–224
postoperative pain relief 150
preoperative pain management 239–240
timing of surgery and delays 223
Hip replacement surgery, pain management in 282
HIV testing 111–112
Horner’s syndrome 139, 321
Hydroxocobalamin, for cyanide poisoning in burns
patients 198
Hyperalgesia 117
Hyperbaric bupivacaine 176
Hyperbaric prilocaine 2% 176
Hypercarbia, during rigid bronchoscopy 341
Hyperpathia 117
Hypocalcaemia, after thyroid surgery 218–219
Hypoglossal nerve 344
Hyponatraemia 131–132
in brain injury 186–187, 187
Hypotension following aortic cross-clamping 39
Hypothermia
effects of, on coagulation cascade 154
perioperative 280–281
Hypoxaemia 95
Hypoxia, during rigid bronchoscopy 340–341
Hysterectomy surgery, analgesia in 300–301
I
Implantable cardioverter-defibrillator (ICD) 132
Infant, anaesthesia for surgery in 113–114
Infantile pyloric stenosis 192
Infective endocarditis 324–325
Inferior alveolar nerve 344
Infraclavicular block 139
Index
Inhalational injury 225–226
Intensive Care Delirium Screening Checklist (ICDSC)
354
Intercostal nerve (ICN) block 400–401, 401
International Association for the Study of Pain (IASP),
definition of pain 117
International normalised ratio (INR) 17
Interscalene blocks 138–139
Intra-abdominal hypertension 56
Intra-abdominal pressure (IAP) 56, 67
elevated 56–57
and intra-abdominal hypertension 67
measurement of 66–67
normal 56, 67
Intra-aortic balloon pump (IABP) counterpulsation
94, 94
aim of 94
contraindications and cautions 95
haemodynamic effects of 94
indications for 94–95
Intracranial haematoma 297–298
Intracranial pressure (ICP) 337–338
Intracranial pressure (ICP) bolt 51, 52
Intracranial pressure (ICP) waveform 51, 51, 62–63, 63
Lundberg A waves 51, 52
Lundberg B waves 51–52
Lundberg C waves 52
in non-compliant brain 51, 52
peaks 51
Intralipid 71
Intraocular pressure (IOP) 75, 153–154, 285
Intra-thoracic blood volume (ITBV) 107, 108
Intravenous access, in children 396
Intravenous regional anaesthesia (IVRA) 267 see also
Bier’s block anaesthesia
Intubation for transfer, indications for 272–273
Invasive arterial pressure monitoring, in transsphenoidal surgery 375
Iron deficiency 120
Ischaemic optic neuropathy (ION) 383
Isovolumetric contraction (IVC) 94
J
Jayneway lesions 325
Jehovah’s Witnesses (JW), strategies for 303–304
cell salvage 305
drugs/blood fractions/recombinant factors 305
haemodilution 304–305
perioperative 304
preoperative 304
K
Kayser-Fleischer rings 199–200
Ketamine 272
middle ear surgery 178
perioperative pain management 193
poly-trauma patient 234
L
Lamotrigine, in post-stroke pain 152
Landmark technique, for TAP block 306, 307
Laryngeal mask airway (LMA) 55, 343–344
Laser-resistant endotracheal tubes 96
Laser technology, and airway fire 96
Le Fort classification, of mid-facial injury 299, 299
Le Fort I osteotomy, and complications 18–19
Left anterior descending artery (LAD) 77, 77
Left circumflex artery (LCX) 77, 77
Left coronary artery (LCA) 77, 77
Lepirudin 17, 313
Levobunolol 285
Levobupivacaine 269
Lignocaine 137, 176
in Bier’s block 267–269
Linear array probes 61–62
Lingual nerve 343–344
Liver failure, fluid management in 190, 191
Liver transplantation, in paracetamol overdose 110
Local anaesthetic (LA) toxicity 70–71, 300
Lower limb surgery 180 see also Sciatic nerve block
Lower segment Caesarean section (LSCS)
airway management and 112–113
under general anaesthesia 394
Low frequency jet ventilation 377
Low-molecular-weight heparin (LMWH) 17, 283–284,
342
Ludwig’s angina 221–222
Lumbar sympathetic plexus block 153
Lung isolation, difficult airway and 174, 174–175, 175
M
Macrocytic anaemia 362
Magnesium, as anaesthesia for middle ear surgery
178–179
Magnesium sulphate, in pre-eclampsia 31
Magnetic resonance imaging (MRI) 12, 12, 222
anaesthesia for, safety considerations in 101
contraindications to 13
for epidural abscess diagnosis 20–21
equipment safety in MR settings 12–13
whole spine 363
MAGPIE Trial 31
Major adverse cardiac events (MACE), risk factors for
241
Malignant hyperthermia (MH) 236–237, 379
Malignant hyperthermia susceptibility (MHS) 236
Mandibular repositioning devices 262
Masseter spasm 302
Maxillofacial trauma, airway management in 299–300
McGill pain questionnaire 238–239
Mean arterial pressure (MAP) 56
Mechanical ventilation 226
weaning from 226–227
Median nerve block 269–270
Meningiomas 297–298
409
Index
410
Meta-analysis 403–404
Metaraminol 298
Methadone 357, 358–359
Methicillin-resistant Staphylococcus aureus (MRSA) 29
and antibiotic regimens in surgery 14
Methicillin sensitive Staphylococcus aureus (MSSA),
and ventilator associated pneumonia 29–30
Microcytic anaemia 362
Microlaryngeal tube 377
Midazolam 137, 272
in poly-trauma patient 234
Middle ear surgery, anaesthesia for 178–179
Minimally invasive cardiac output monitors 106–109,
107, 108
Misoprostol 69, 191
Mivacurium 179
Mobitz II atrioventricular (AV) block 260
Morphine
for pain in neonate 197, 398
in porphyria 75
for postoperative pain 70
Morphine allergy 357
Morphine patient controlled analgesia (PCA) 358–359
Motor evoked potentials (MEPs) 303, 383
Muscle relaxants 179
Myasthenia gravis (MG) 170, 401–402
Osserman classification 170
requirement for post op ventilation 170–171
Myocardial infarction (MI) 76
coronary circulation and 76–77, 77
ECG changes 77–78, 78
Myoglobinuria 119
N
N-acetyl cysteine (NAC) 109
N-acetyl-p-benzoquinone imine (NAPQI) 109
Naloxone 149
Nasal endotracheal tube 19
Neonatal apnoea, postoperative 113–114
Neonatal pain, analgesia for 398
Neonatal resuscitation 314–315, 315
Neonates, analgesia for 197
local anaesthetics 197
non steroidal anti-inflammatory drugs 197
opiates 197
paracetamol 197
Neonates, critically ill, evaluation and management
of 31–32
Nerve block needles 21–22, 22
cutting tip needle 21, 22
pencil point needles 22, 22
Nerve fibres 154–156, 155, 155
Nerve stimulators 101–103
Neurapraxia 343
Neurogenic shock 376
Neuron 154, 155
Neuropathic pain 117
Nimodipine, in delayed cerebral ischaemia
prevention 215
Nitrous oxide, as anaesthesia for middle ear surgery
178
Nociception 117
Non heart-beating organ donation (NHBOD) 309–310
Non-invasive ventilation (NIV) 275
Normocytic anaemia 362
Number needed to treat (NNT) 201
Numeric rating scale 239
Nutritional support, in critically ill patients 390–391
O
Obese patients, perioperative management of
263–264
Obesity 311
in pregnancy 147–148
and weight loss surgery 379–381
Obstetrics, management of difficult and failed
intubation in 112–113
Obstructive hydrocephalus 63–64
Obstructive sleep apnoea (OSA) 284
in children 148
Obstructive sleep apnoea/hypopnoea syndrome
(OSAHS) 262–263
Oculocardiac reflex 241
Oculomotor nerve palsy 314
Oesophageal Doppler 171, 171–173, 325–326
afterload and 172
peak velocity and 172
stroke distance/stroke volume and 172
Oesophageal perforation 381
Olanzapine, in delirium 354
Opioid-induced hyperalgesia 38, 74
Opioid rotation 38
Opioids
after hip replacement surgery 282
in cancer-related pain 37–38
for pain management 358
Opioid toxicity 237
Opioid withdrawal 237, 358
Oral intubation 299
Organ donation 309–310
Oxcarbazepine, in trigeminal neuralgia 33–34
P
Pacemakers
indications for insertion of 260, 261
NAPSE/BPEG coding system 261
summary of pacing modes 261
Paediatric trauma 142
Pain
assessment of, in children 71, 71–72, 72
in cancer 36–38, 37
control of, strategies for 37
definition of 117
gate theory of 36, 36
Index
Pain scales 238–239
Paracetamol
intravenous, in children 115–116, 116
in neonates 197
overdose, and fulminant liver failure 109–110
Paraesthesia 117
Paravertebral block 338–339
Parkland formula, for resuscitation fluid volumes 32,
39, 105, 118, 232
Patent ductus arteriosus (PDA) 32
Patient-controlled analgesia (PCA) 149, 282–283
Patient Safety Incident (PSI) 134
Peripheral nerve blocks, needles for 21–22, 22
Peripheral nerve fibres 155, 155
Peripheral nerve stimulator 101–103
Pethidine 357, 399
Phaechromocytomas 221
Phantom limb pain 193, 195
Phenylephrine 137
PiCCO monitoring 106–109, 107, 108
Pituitary tumours 375
Placenta praevia 279
Polymorphic ventricular tachycardia (VT) 156
Porphyria 74–75, 75
Post-dural puncture headache (PDPH) 103–104,
319–320, 320, 355
Posterior femoral cutaneous nerve (PFCN) 180
Post-herpetic neuralgia (PHN) 73–74, 317
Post-mastectomy pain 34
Postoperative nausea and vomiting (PONV),
strabismus surgery and 241
Post partum haemorrhage (PPH) 69
Pre-eclampsia 31, 281
Pregnancy
anaesthesia for non-obstetric surgery during 113
anaesthesia for parturients 355–356
cardiac disease in 191
obesity in 147–148
painless vaginal bleeding in 279
pre-eclampsia in 31
Preoperative fasting, in patients 280, 315–316
Prilocaine 268
Primary biliary cirrhosis 200
Primary sclerosing cholangitis 200
Prolonged QT 156
Propofol 179
in poly-trauma patient 234
Prostin intravenous infusion, in critically ill neonate
31–32
Pulmonary artery catheter (PAC) 106
Pulmonary aspiration of gastric contents 242
bronchopulmonary segments and 242–244, 243
Pulmonary embolism (PE) 110–111, 376
CT angiography in 157–158
diagnosis and management of 157–158
Pulmonary Embolism Severity Index (PESI) 157
simplified PESI (sPESI) 157
Pulmonary oedema 389
Pulseless ventricular tachycardia (VT) cardiac arrest
70–71
Pulse oximetry 378
Pyloric stenosis 192
Q
QT interval 156
Qualitative data 363
Quantitative data 363
Quetiapine, in delirium 354
R
Radial nerve block 270–271
Radiography 222
Radiotherapy, for bone pain 360
Rapid response teams, anaesthetists in 104–105
Rapid sequence induction (RSI)
cricoid pressure for 307
in head injury 385
unanticipated difficult intubation during 54–55, 55
Recombinant erythropoietin (EPO) 304, 362
Rectal examination, in liver disease 145–146
Recurrent laryngeal nerve 344
Refeeding syndrome 245
Regional anaesthesia
peripheral nerve stimulator use in 101–103
use of ultrasound in 224–225, 225
Remifentanil 138
in maxillofacial surgery 19
in middle ear surgery 178
Remifentanil patient-controlled analgesia (PCA)
316–317
Renal impairment, aortic aneurysm repair and 199
Renal replacement therapy, in acute kidney injury
278, 308–309, 351
clot formation, prevention of 352–353
indications for 351–352
types of 352
Resuscitation and maintenance fluid, in burns 32
Retromolar space 299
Retropharyngeal abscess 133
Reynolds number (Re) 266
Rhabdomyolysis 119
Right coronary artery (RCA) 76–77, 77
Rigid bronchoscope 377
Rigid bronchoscopy, for foreign body removal
340–341
Rivaroxaban 18, 342–343
Robotic surgery 264–265
Rocuronium 219–220
in poly-trauma patient 234
Root cause analysis (RCA) 134
Ropivacaine 269
Roux-en-Y gastric bypass 380
Royal College of Anaesthetists (RCoA) guidelines, on
anaesthesia in non theatre settings 267
411
Index
412
S
Sacral plexus 180
Sciatic nerve 180
Sciatic nerve block 180
Beck’s anterior approach 182, 182
Guardini’s subtrochanteric approach 182, 183
Labat’s transgluteal approach 181, 181
Mansour’s parasacral block 180, 181
popliteal approach 182–183, 183
Raj approach 181, 182
Sedation 347
in intensive care 349–350
levels of 347
monitoring 347
pre-assessment 347
principles and drugs 347–348
Sensory evoked potentials (SEPs) 303
Sepsis 64–65
intra-abdominal 234–235
Septic shock, fluid resuscitation in 144–145
Serotonin Release Assay (SRA) 312
Serotonin syndrome 237–238
Serum osmolality 131
Sevoflurane 92–93, 356
Shingles 73
Shoulder surgery, anaesthesia for 318–319, 319
Sickle cell crises 399
Sickle cell disease 316
Smoke inhalation injury 377–378
Sodium chloride 145
Somatosensory evoked potentials (SSEPs) 383
Sphenopalatine ganglion block 153
Spinal anaesthesia, in day surgery 175–176
Spinal catheter 30
Spinal cord compression, and pain 318
Spinal cord stimulation, in complex regional pain
syndrome 240–241
Spinal infection, epidural drug delivery and 20–21
Spinal shock 376
Spinal surgery 382–384
eye and visual complication 383
prone position 383
spinal cord monitoring 383
Spontaneous breathing trial (SBT) 226–227, 275
Staphylococcus aureus 14, 133
Staphylococcus epidermidis 14
Starch solutions 145
Statistical tests 363–364, 364
Status epilepticus 53
STOP-BANG questionnaire 263–264, 284
Storz ventilating bronchoscope 340
Strabismus surgery 241
Stroke volume index (SVI) 308
Subarachnoid haemorrhage (SAH) 214, 214, 391–393
delayed cerebral ischaemia in 214–215
imaging for diagnosis of 392
management of 393
presentation of 392
spontaneous 392
World Federation of Neurological Surgeons Scale
(WFNSS) 392
Subdural haematoma 385
Submasseteric abscess 302
Submental intubation 300
Sub-Tenon’s blocks 320–321
Superior hypogastric plexus block 153
Supraclavicular block 139
Surgical tracheostomy 299–300
Surviving Sepsis Guidelines 64–65
Sympathetic block 152
contraindications to 153
indications for 152
types of 153
Sympathomimetic agents 285
Syndrome of inappropriate antidiuretic hormone
secretion (SIADH) 131–132, 186, 187
Syntocinon 69, 191
Systemic vascular resistance index (SVRI) 108
T
Temporary transvenous cardiac pacing, insertion of
146–147
Temporomandibular joint 302, 302
Tension pneumothorax 376
Therapeutic hypothermia, in post-cardiac arrest
patients 138
Thiopentone, in poly-trauma patient 234
Thoracic epidural anaesthesia 346–347
Thoraco-abdominal aortic aneurysm 399–400
Thoracotomy pain, analgesic options for 195, 196
Thromboelastograph (TEG) tests 259, 259–260, 260
Thromboembolic deterrent stockings (TEDS) 17
Thyroidectomy, and hypocalcaemia 218–219
Tic douloureux see Trigeminal neuralgia (TN)
Tirofiban 342
Tocolytic therapy, in uterine inversion 279–280
Torsade de pointes 156
Total intravenous anaesthesia (TIVA) 377
Total knee replacement (TKR), adductor canal block
in 323–324
Total spinal block 313–314
Tracheal necrosis 219
Tracheal rupture 381
Tracheomalacia 219
Tracheostomy airway emergencies, management of
15, 15–16
Tramadol 237, 357
Tranexamic acid 76, 305
Transcutaneous electrical nerve stimulation (TENS)
36, 36, 282, 317, 396
Transfusion-related acute lung injury (TRALI) 191
Transport of critically ill adult, planning before 24–25
Trans-sphenoidal pituitary surgery 375
Index
Transurethral resection of the prostate (TURP) 176
Transversus abdominis plane (TAP) block 306–307
Trauma anaesthesia 233–234
Trauma, paediatric 142, 394
Traumatic brain injury (TBI) 22
airway/ventilation 23
drugs, use of 24
haemodynamics 23
hyponatraemia in 186–187, 187
initial assessment and resuscitation 22
intracranial pressure (ICP), management of 23–24
intubation prior to transfer in 215–216
Tricyclic antidepressants (TCA) 26
overdose, management of 26–27
Trigeminal neuralgia (TN) 33–34, 151
Trigeminocardiac reflex 19
Trismus 301
TURP syndrome 176
glycine in 177
plasma sodium and osmolality in, changes in 177
volume in, changes in 177
U
Ulnar nerve block 271
Ultrasound-guided nerve block 224–225, 225
in-plane approach 225
long-axis view 225
out-of-plane technique 225
short-axis view 224
Ultrasound probe 61–62
curved array probes 61
hockey stick footprint probes 61
linear array probes 61, 62
phased array probes 61
Unanticipated difficult intubation, management of
54–55, 55
Uncooperative child patient, anaesthesia for 185,
236, 271–272
consent 185
drug treatments 272
holding/restraint 185, 272
provision of safe sedation 185–186
risk factors for induction distress 271
Unfractionated heparin 17
Upper airway obstructions 58
extrathoracic 58
flow-volume loops 58, 59
intrathoracic 58
Upper limb peripheral nerve blocks 269
median nerve block 269–270
radial nerve block 270–271
ulnar nerve block 271
Upper limb surgery, anaesthesia for 184
Uterine inversion 279–280
Uterotonics 191
Uvular necrosis 381
Uvulopalatopharyngoplasty (UPPP) 263
V
Vaccination at time of anaesthesia 357
Vallergan (trimeprazine) 272
Vancomycin 14
Vancomycin resistant enterococci (VRE) 29
Varicella zoster virus (VZV) 73
Vasopressin 59, 273
Venous air embolism (VAE) 98–99, 258 see also Gas
embolism
during head and neck surgery 19
Venous thromboembolism (VTE)
prevention of 17–18
risk of, after day surgery 16
Ventilator associated infection (VAI)
causative organisms 29
definition 29
diagnosis 29
prevention and management 29–30
Ventilator-associated pneumonia (VAP) 276
diagnosis 277
risk factors 276–277
Ventricular fibrillation (VF) 132
Verbal descriptor scale 239
Violence/aggression in visitors, management of
104–105
Visual analogue scale (VAS) 71, 239
Vitamin A deficiency 40, 120
Vitamin B1/thiamine deficiency 120
Vitamin C deficiency 120
Vocal cord damage, after thyroid surgery 218
Volatile anaesthetics, and cerebral blood flow
autoregulation 92, 92–93, 93
W
Warfarin 17, 342
Weaning from ventilator 226–227
Weight loss surgery 379
malabsorptive 380
operative factors 380
preoperative assessment 380
restrictive 379
Wilcoxon signed rank test 363–364, 364
Wilson’s disease 199–200
Wong–Baker FACES scale 72, 239
Z
Zygomatic arch fractures 302–303
413