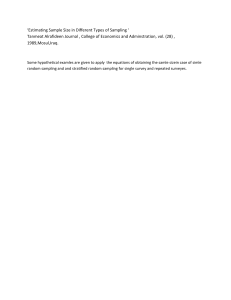
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/7033302 Application of an acceptance sampling plan for post-production quality control of chemotherapeutic batches in an hospital pharmacy Article in European journal of pharmaceutics and biopharmaceutics: official journal of Arbeitsgemeinschaft fur Pharmazeutische Verfahrenstechnik e.V · September 2006 DOI: 10.1016/j.ejpb.2006.04.002 · Source: PubMed CITATIONS READS 22 2,915 7 authors, including: Isabelle Borget Angelo Paci Institut de Cancérologie Gustave Roussy Institut de Cancérologie Gustave Roussy 323 PUBLICATIONS 4,914 CITATIONS 241 PUBLICATIONS 3,906 CITATIONS SEE PROFILE SEE PROFILE Stefan Michiels Lionel Mercier Institut de Cancérologie Gustave Roussy Institut de Cancérologie Gustave Roussy 562 PUBLICATIONS 20,374 CITATIONS 26 PUBLICATIONS 344 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: 2-HydroxyGlutarate as surrogate IDH mutations biomarker View project LACE-Bio2 View project All content following this page was uploaded by Angelo Paci on 04 December 2017. The user has requested enhancement of the downloaded file. SEE PROFILE Journal of Oncology Pharmacy Practice http://opp.sagepub.com/ Safety and quality assurance of chemotherapeutic preparations in a hospital production unit: Acceptance sampling plan and economic impact A Paci, I Borget, L Mercier, Y Azar, R.P Desmaris and P Bourget J Oncol Pharm Pract published online 10 May 2011 DOI: 10.1177/1078155211402865 The online version of this article can be found at: http://opp.sagepub.com/content/early/2011/05/06/1078155211402865 Published by: http://www.sagepublications.com Additional services and information for Journal of Oncology Pharmacy Practice can be found at: Email Alerts: http://opp.sagepub.com/cgi/alerts Subscriptions: http://opp.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 Journal of Oncology Pharmacy Practice Article Safety and quality assurance of chemotherapeutic preparations in a hospital production unit: Acceptance sampling plan and economic impact J Oncol Pharm Practice 0(0) 1–8 ! The Author(s) 2011 Reprints and permissions: sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/1078155211402865 opp.sagepub.com A Paci Pharmacology and Drug Analysis Department and Department of Clinical Pharmacy, Institute Gustave Roussy, Villejuif, France I Borget Service of Health Economy, Biostatistic and Epidemiology Department, Institute Gustave Roussy, Villejuif, France L Mercier Pharmacology and Drug Analysis Department and Department of Clinical Pharmacy, Institute Gustave Roussy, Villejuif, France Y Azar Pharmacology and Drug Analysis Department, Institute Gustave Roussy, Villejuif, France R.P Desmaris Department of Clinical Pharmacy, Institute Gustave Roussy, Villejuif, France P Bourget Department of Clinical Pharmacy, Institute Gustave Roussy, Villejuif, France Abstract Objective.The opportunity to apply a sampling plan was evaluated. Costs were computed by a microcosting study. Setting. In 2003, a sampling plan was defined to reduce the number of chemotherapy quality controls while preserving the same level of quality. Recent qualitative and quantitative changes led us to define a second sampling plan supplemented by an economic evaluation to determine the cost and cost-savings of quality control. Methods. The study considers preparation produced during four semesters classified into three groups. The first one includes drugs produced below 200 batches a semester. Group 2, those for which the lot of preparation lots would have been rejected twice among these four semesters. Group 3, those would have been accepted (3 ‘acceptable lot’). A single sampling plan by attributes was applied to this group with an acceptance quality level of 1.65% and a lot tolerance percent defective below 5%. A micro-costing study was conducted on quality control, from the sampling to the validation of the results. Results. Among 39 cytotoxic drugs, 11 were sampled which enabled to avoid a mean of 17,512 control assays per year. Each batch of the 28 non-sampled drugs was however analyzed. Costs were estimated at 2.98E and 5.25E for control assays depending of the analytical method. The savings from the application of the sampling plans was 153,207E in 6 years. Conclusion. The sampling plan allowed maintaining constancy in number of controls and the level of quality with significant costsavings, despite a substantial increase in drugs to assay and in the number of preparations produced. Corresponding author: Angelo Paci, Pharmacology and Drug Analysis Department, Institute Gustave Roussy, Villejuif, France Email: angelo.paci@igr.fr Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 2 J Oncol Pharm Practice 0(0) Keywords Quality assurance, sampling plan, cost, chemotherapy, oncology practice Introduction The drug supply chain in health establishments is composed of series of successive stages: drug prescription is a medical task, preparation and dispensation are pharmaceutical ones, whereas drug administration belongs to nurses. Potential errors such as wrong dosage, solvent’s errors, wrong labeling or, in some exceptional cases, chemotherapeutic active substances’ errors can occur, leading to potential risks of morbidity and mortality for patients. Recommendations and quality assurance processes have since been applied to ensure safety at each stage of the drug supply chain. Concerning pharmaceutical tasks, the pharmacist is responsible for procurement, distribution, surveillance, and control of all drugs used in the hospital. Drug preparation and quality control are also mandatory activities for a hospital pharmacy.1 The drug preparation activity must be performed in conformity with good practices,2 according to article L. 5121-5 of the Public Health Code.3 Moreover, drug preparation and quality control activities performed in a hospital pharmacy must also adhere to the principles defined in Hospital Pharmacy Good Practices (HPGP).4 According to HPGP principles, the final product of drug preparation must be inspected to verify that it has been accurately compounded using the correct ingredients and the specific amounts of each ingredient in an appropriate reservoir.5,6 Even if these rules concern all drugs, particular attention must be paid to fragile or potentially toxic preparations, like sterile compounds, cytotoxic drugs, or preparations for parenteral nutrition. By allowing the identification of qualitative and quantitative preparation non-conformity, verification of the finished product contributes to ensuring drug supply chain safety. However, these quality controls were rare in the hospital pharmacy setting. In 2002, a study showed that only 4.7% of American pharmacies compounding cytotoxic preparations performed these controls and were thus compliant with 2000 ASHP guidelines on quality assurance for pharmacy-prepared sterile products.7,8 Since 1998, our clinical pharmacy department has been equipped with an analytical platform using both high performance thin-layer chromatography (HPTLC) and high performance liquid chromatography (HPLC) to ensure post-production quality control of chemotherapeutic preparations, both qualitatively (identification) and quantitatively (concentration).9,10 These analyzes allow post-production quality control assays of most of the cytotoxic drug solutions commonly used, as given in Table 1. For 5 years, more than 75% of the entire production was analyzed which led to a decline in the non-conformity (NC) rate from 8.9% to 2.2%. In 2003, faced with the growing number of chemotherapy preparations to control, the need for systematic quality control versus sampling of manufactured preparations arose. The opportunity to reduce the number of control assays while preserving the same level of quality was seized by implementing a sampling plan. It used a statistical approach between no control and 100% of controls: the size of the sample to be controlled was determined for each chemotherapy drug in order to obtain the same level of quality (expressed as a percent of NC) in the sample as in all preparations.11,12 The Table 1. Classification of drugs into three groups Category of drugs Drugs concerned Group 1: drugs produced less than 200 preparations per semester 20 drugs: actinomycin D, asparaginase, carmustine, daunorubincin, dacarbazine, liposomal doxorubicin, fludarabine, idarubicin, melphalan, thioguanine, novantrone, pemetrexed, streptozotocin, thiothepa, paclitaxel, vindesine, cetuximab, toptecan, mitoxantrone, busulphan 8 drugs: bleomycin, irinotecan, methotrexate, rituximab, docetaxel, vinblastine, vinorelbine, etoposide 11 drugs: epirubicin, 5-fluorouracil, cytarabine, carboplatin, cisplatin, cyclophosphamide, gemcitabine, doxorubicin, ifosfamide, oxaliplatin, vincristine Group 2: drugs outside the specification limits for sampling Group 3: drugs for which the acceptance sampling plan was applied Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 Paci et al. 3 possibility of applying the plan was evaluated for nine drugs whose production exceeded 400 per year. The size of the sample of the others was too small to obtain correct estimations of the NC rate. Six chemotherapy drugs (fluorouracil, cisplatin, cyclophosphamide, ifosfamide, doxorubicin, and epirubicin) were then sampled, allowing a reduction of 50–83% in the sample size to be controlled. From 2003 to 2007, the sampling plan enabled us to avoid about 8000 control assays out of 21,000 per annum, representing 38% of the overall number of analyzes. Among the nine drugs whose production exceeded 400 per year, three (methotrexate, cytarabin, and etoposide) were not included in the sampling plan, as they represented a higher risk of NC than the others: it was decided that all preparations of those drugs would be controlled.13 However, some major elements in the production and/or in the control process have changed since 2003. First, the number of preparations produced annually has increased from 30,000 to 52,000. Second, 39 chemotherapy drugs can now be controlled, resulting both from the availability of new drugs in the cancer field (trastuzumab, bevacizumab, etc.) and from analytical procedure development. The number of preparations of some drugs produced annually has been significantly modified due to treatment protocol changes. Some of them are now produced fewer than 400 times per year or conversely. Finally, the overall NC rate has decreased from 2.2% to 1.65%. The hypothesis and the estimations that were used for the application of the first sampling plan were also partially obsolete. A new sampling plan was necessary, in order to maintain constancy in the number of control assays and the level of quality, despite a substantial increase in the number of therapeutic preparations produced and cytotoxic drugs to control. Moreover, the unit cost of post-production quality control has never been precisely estimated. Thus, the objective of this study was to evaluate the application of a second sampling plan taking into account the qualitative and the quantitative changes in production, as well as the decrease in the rate of NC. This evaluation was supplemented by an economic evaluation aimed at determining the unit cost of post-production quality control assessment of chemotherapy preparations in the hospital and at evaluating the economic impact of the application of the sampling plans. Methods Quality control methods Our laboratory is equipped since 1998 with an analytical platform composed of HPTLC and HPLC designed to work in tandem with the production unit. Chromatographic methods coupled to spectrometric detection allow undoubtedly the identification of the drug used in the preparation and concomitantly, its amount or concentration determination. As previously published, our chromatographic methods allow the separation of each compound and their identification through the retention time or retention factor combined to their spectra.9 Each method was validated according ICH guidelines. For HPLC, repeatability and intermediate precision were all below 5% while those for HPTLC were evaluated between 3% and 6%. Whatever the drug, a preparation was considered as non-conform (NC) if it contains the wrong drug (qualitative error), or when its measured concentration was outside the specification limits defined as the target concentration 10% for two consecutive assays (quantitative error). If it was not technically possible to perform a second assay after an initial non-conform assay and as the real status of unchecked samples was not known, the preparations corresponding to these samples were considered as non-conform. Application of the second sampling plan The possibility to apply the new version of the acceptance sampling plan was evaluated for the 39 chemotherapy drugs whose analytical assay was available, based on data accumulated over four semesters (years 2005 and 2006). The statistical analysis took into account ‘preparation lots’ composed by all the preparations (n) produced for each drug during one semester. Cytotoxic drugs were then classified into three groups. The first group was composed of drugs whose production was below 200 preparations per semester. The size of the ‘preparation lot’ of these drugs (group composed of drugs produced 17–188 times per semester) was too small to obtain correct estimations of the NC rate. No sampling plan was applied to this group, meaning that each preparation was controlled. The possibility of applying the sampling plan was then evaluated for drug preparations exceeding 200 preparations per semester, by applying acceptance sampling by attributes. It consisted of counting the total number of NC preparations (d) in the ‘preparation lot’ of size (n). If (d) was not greater than the acceptable number of NC defined by the plan (c), the ‘preparation lot’ was evaluated as an ‘acceptable lot’; otherwise it was marked as an ‘unacceptable lot’. Thus, the number of acceptable lots for each drug ranged from 0 (all the lots corresponding to the four semesters were unacceptable) to 4 (all the lots Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 4 J Oncol Pharm Practice 0(0) corresponding to the four semesters were acceptable). Group 2 was composed of drugs for which the ‘preparation lot’ would have been rejected (NC rate higher than 1.65%) at least over two semesters. It was decided that all preparations of this group of drugs would be controlled instead of applying a sampling plan, in order to obtain a correct estimate of the NC rate. Group 3 was composed of drugs whose ‘preparation lot’ would have been accepted at least three out of four semesters (3 ‘acceptable lot’). The sampling plan was only applied to this group. The methodology which allowed us to determine the optimal sample size to control was similar to that used to apply the first sampling plan.13 The AQL, represented the maximum percentage of NC that the pharmacist could tolerate to consider the process as satisfactory. It was fixed at 1.65%, as it represented the maximum percentage of non-conform preparations observed over the period 2005–2006. The pharmacist would like to design a sampling plan such that there is a high probability of accepting a preparation lot that has a NC rate less than or equal to the AQL.13 The lot tolerance percent defective (LTPD), i.e. the risk of accepting a ‘preparation lot’ of unacceptable quality was fixed at 5%. The acceptance sampling plan was then applied as follows: based on the number of preparations (ni) prepared during the last semester (second semester 2006), (ni) was decreased by increments of 500 or less in order to calculate the number of preparations requiring a control assay, while maintaining the AQL at the targeted value (1.65%) and an LTPD of less than 5%. Cost determination Costs were computed from the hospital viewpoint (Gustave Roussy Institute) and were expressed in Euros in 2007. A micro-costing study, restricted to the resources consumed, was conducted to perform a control, from the sampling when the chemotherapeutic preparation was manufactured until the validation of the results by the pharmacist and the transmission of the results. Costs attributed to the production of the preparation (cytotoxic drugs, personnel costs for the production etc.) were not included. The total cost of post-production control assays at IGR corresponded to the sum of direct and indirect medical costs. Direct medical costs corresponded to materials, person costs, and the analytical equipment, whereas indirect costs included overheads and logistics costs. The type and the number of medical devices, consumables, material, and reagents consumed annually were collected retrospectively over three consecutive years (2005, 2006, and 2007) and were expressed per control assay. The unit prices of devices according to the 2007 price list at IGR were used for their valuation. Personnel costs were calculated using the mean lengths of time spent performing the different stages of a series of quality control assays, which were estimated prospectively for 83 series of control assays performed over 14 days in March 2008. For each stage, two measurements of the length of time were estimated: the first one estimated the total length of time spent performing the given stage (including the time spent by the technician and the automatic processing time). The valuation of personnel costs was based on the second estimation, which only considered the length of time needed for the technician to perform the given stage (the automatic processing time spent at the given stage was not valorized, that is, a value was not assigned to it). The valuation of personnel costs used the hourly employee wage by professional category. The laboratory technician was involved in each stage of the post-production control process, except for the validation of the results which was done by the pharmacist. The analytical platform consisted of the CAMAGÕ station and the HPTLC platform, both purchased in 1998. The cost of the analytical equipment per control assay and per method was calculated by taking into account their respective acquisition cost, their depreciation charges (amortization period of 10 years), and an estimated number of control assays performed until the end of that period. Indirect costs included overheads and logistics costs. According to the IGR cost accounting system, indirect costs represented 33% of the amount of direct costs. The number of control assays avoided, since the application of the first sampling plan in 2003 was determined. For each year, it corresponded to the difference between the number of preparations produced and the number of control assays performed annually. The economy generated was then estimated by multiplying the total number of control checks avoided, since 2003 by the unit cost per control assay. Results Application of the second sampling plan In 2006, the analytical platform was able to assess qualitative and quantitative analyzes for 39 cytotoxic drugs (30 by HPTLC and 9 by HPLC). Fewer than 200 preparations of 20 of these 39 cytotoxic drugs were produced per semester (representing 3093 out of 31,890 (9.7%) preparations produced in 2006); hence, they were classified in the first group based on the small Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 Paci et al. 5 Table 2. Determination of the optimal sample size by applying the acceptance sampling plan to the 11 drugs in the third group Epirubicin 5-Fluorouracil Cytarabine Carboplatin Cisplatin Cyclophosphamide Gemcitabine Doxorubicin Ifosfamide Oxaliplatin Vincristine Total Preparations produced per year (n) Preparations analyzed per year (n) Rate of reduction of preparation analysis (%) Controls avoided by the plan per year (n) 832 4813 1658 1260 3367 1512 614 2098 3315 527 1347 21,343 200 630 355 217 414 253 244 382 367 259 510 3831 75 85 67 75 88 83 50 80 88 50 50 632 4183 1303 1043 2953 1259 370 1716 2948 268 837 17,512 ‘preparation lot’. No sampling was performed on this group (Table 1). Eight cytotoxic drugs were classified in the second group, as the ‘preparation lot’ would have been rejected over at least two semesters. The sampling plan was not applied to this group of drugs. This means that each of the 7454 preparations produced had to be controlled (23.3% of overall production). The sampling plan was applied to 11 cytotoxic drugs which constituted the third group whose production attained 21,343 preparations (66.9% of overall production) in 2006. The application of the sampling plan showed that it was possible to reduce preparation analysis by 50–88% for these 11 drugs (Table 2). In 2006, as the estimated number of quality control assays was 3831, the application of the sampling plan to these drugs made it possible to avoid 17,512 control assays (55% of overall production). Unit cost of quality control checks From 2004 to 2006, the mean annual expenditures for material, consumables, and reagents was estimated at 22,794 3301E, for a mean number of 24,929 2507E quality control assays performed annually. The mean cost of the resources consumed for performing a control assay was then estimated at 0.91 0.08E. The mean lengths of time spent performing a control assay by stage and analytical methods are presented in Table 3. The total lengths of time (including both the technician and automatic processing times) were estimated at 3.6 1.2 and 16.0 5.4 min for assays performed by HTPLC and by HPLC, respectively. During this time, the technician was occupied, respectively, for 2.1 0.7 and 2.9 2.2 min performing an HPTLC and an HPLC control assay. The personnel costs for performing a post-production assay were 1.00 0.19E and 1.35 0.92E for HPTLC and HPLC control assays, respectively. Concerning the cost of equipment, the acquisition cost of the CAMAGÕ station amounted to 63,093E. Based on a mean annual number of 18,332 HPTLC control assays per year and a damping period of 10 years, the cost attributed to the acquisition and the damping of the analytical equipment for performing an HPTLC control assay was then estimated at 0.33E per control assay. The acquisition cost of the HPLC platform was 20,747E. With an average of 1228 control assays performed annually and a damping period of 10 years, the mean cost of acquisition and damping of the HPLC platform was calculated at 1.69E per control assay. The mean direct costs of control assays were, respectively, 2.24 0.19E and 3.95 0.92E for HTPLC and HPLC. By including the indirect costs, the total cost for performing a post-production control assay amounted to, respectively, 2.98 0.25E and 5.25 1.22E (Table 4). Economic impact of applying the sampling plans Since 2003, 201,787 preparations have been produced. As the analytical process was not yet available, 5692 of these preparations were not controlled. During this period, the total number of preparations produced and for which a control was available was then equal to 196,095. Among this, 146,927 quality control assays were performed from 2003 to 2008, resulting in a total cost for the hospital estimated at 457,824E. The application of the sampling plan then enabled the avoidance of 49,168 control assays (representing 25.1% of the Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 6 J Oncol Pharm Practice 0(0) Table 3. Mean lengths of time spent performing an assay by stage and by method (minutes) HPLC Separation of dosage and storage (if necessary) Preparation of the analysis plan Dilution Deposit Chromatography Revelation Analysis Interpretation Printing Transmission of results Preparation of laboratory (preparation of reagents, maintenance, waste, control tube) Total Total time (technician + automatic process) Technician’s time alone Total time (technician + automatic process) Technician’s time alone 0.18 0.30 0.34 0.19 1.06 0.96 – 13.38 3.38 – – 0.51 0.13 0.41 0.24 0.06 0.05 0.05 0.11 0.18 0.30 0.34 0.20 1.06 0.96 – 0.25 0.25 – – 0.51 0.13 0.41 0.24 0.06 0.05 0.05 0.11 0.12 0.06 0.37 0.07 0.70 0.12 0.91 0.21 0.34 0.17 0.18 0.15 0.26 0.07 0.31 0.08 0.34 0.16 0.04 0.04 0.06 0.09 0.12 0.06 0.37 0.07 0.70 0.12 0.05 0.01 0.05 0.01 0.05 0.01 0.05 0.01 0.31 0.08 0.34 0.16 0.04 0.04 0.06 0.09 15.99 5.36 2.86 2.24 3.62 1.22 2.12 0.68 Table 4. Cost for performing an HPLTC and an HPLC control assay (euros) Direct medical cost (E) Consumables, reagents, and material cost Personnel cost Equipment cost Total direct cost (E) Indirect costs (E) Total cost (E) HPTLC HPTLC HPLC 0.91 1.00 0.33 2.24 0.74 2.98 0.91 1.35 1.69 3.95 1.30 5.25 HPTLC, high performance thin-layer chromatography; HPLC, high performance liquid chromatography. production that can be assayed). About 24,841 control assays were avoided from 2003 to 2006 (first plan), whereas the application of the second plan in 2006 allowed the hospital to avoid 24,327 control assays in 2 years (Figure 1). The savings generated by the application of the sampling plans were estimated at 153,207E in 6 years. Discussion Post-production quality control of chemotherapy is not a common practice in hospital pharmacy units. In our institution, it has been developed since 1998, to contribute to an overall quality assurance program started in 2000 at the IGR and is designed to ensure the safety of the preparation of anti-neoplastic agents and of their administration conditions. During the first 4 years, routine assays of manufactured preparations reached considerable maturity with 28 cytotoxic drugs controlled and 23,000 assays performed per year. In 2003, faced with an increase in the number of preparations produced, the acceptance sampling plan was decided as an analytical strategy to maintain constancy in the number of control assays and the level of quality. It was applied to six cytotoxic drugs, and resulted in the avoidance of about 8000 control assays of the 26,000 preparations produced annually. First, the decrease in the number of control assays allowed us to save time, which was used to develop analytical control assays of drugs recently introduced in cancer treatment and/or which had not yet been assayed. From 2003 to 2006, the number of drugs available for assay thus increased from 23 to 39. The analytical platform had therefore reached a high level of exhaustivity, as 98% of overall production could be qualitatively and quantitatively assayed. Second, it allowed us to focus our attention on the other drugs that were systematically controlled. Corrective measures were implemented, resulting in an improvement of overall quality (a decrease in the rate of NC from 2.2% to 1.65%) despite a continuous increase in the number of preparations produced (+1400 preparations produced annually). The corrective actions that have been introduced were a review of the fabrication processes’ and a vocational training of the personnel. The results of the dosage were used as indicators of quality that involve salaries in an approach of continuous improvement. However, the increase in the number of drugs controlled also led to Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 Paci et al. 7 50000 Controls not yet available Controls avoided by the sampling plan Controls performed 40000 30000 20000 2nd SP 10000 0 2000 1st SP 2001 2002 2003 2004 2005 2006 2007 2008 Years Figure 1. Evolution of the number of preparations produced and controlled from 2000 to 2008. an increase in the number of control assays (a series of 23 control assays per quality control check). At the same time, HPGP recommended that the production of cytotoxic preparation henceforth be totally centralized in the Pharmacy Department of the hospital, this organization being mandatory for the reimbursement of expensive cytotoxic drugs. This centralization at the IGR translated into a considerable increase in the number of preparations produced (from 31,910 to 51,643 from 2006 to 2008). By responding to both qualitative and quantitative changes in production, the second sampling plan allowed us to maintain constancy in the number of control assays performed, since the application of the first plan, by taking into account the new rate of NC. As the number of drugs produced more than 200 times per semester had increased, 11 cytotoxic drugs were now concerned by the sampling plan and the number of control assays avoided was 17,000 per year. Without implementing the second sampling plan, the Centralized Pharmacy Department would have had to have set up alternative solutions to deal with the increase in the number of control assays. The recruitment of a second technician and/or the acquisition of a second analytical platform could have been considered but those are expensive alternatives. Some hospital pharmacies have chosen to control only some cytotoxic drugs, while other drugs are not controlled. This provides only a partial estimation of the rate of NC and criteria used to determine the selection of drugs to control are unclear (based on the number of preparations produced or analytical method development). In our institute, preference was given to the efficiency of the analytical platform in terms of a constant level of human and material resources. Based on our estimation, the sampling plan will allow us to avoid between 30,000 and 50,000 control assays among the 80 to 90,000 chemotherapy preparations that will be produced annually in the very near future. The sampling plan has also made it possible to continue the routine inspection of every preparation of drugs that is not included in the sampling plan, and thus to continue to improve their quality and reduce the total rate of NC. This systematic inspection of drugs which are not included in the plan (groups 1 and 2) is also possible as they represented only 33% of the total preparations produced. The quality assurance process engaged by the Department also includes estimating quality indicators, providing results in bi-annual meetings and reflecting upon the manufacturing process with the pharmaceutical and analytical teams. This article also aimed at estimating the unit cost of post-production quality control for the hospital. It showed that the costs of quality control by HPTLC and HPLC were, respectively, estimated at 2.98E and 5.25E and appeared to be similar to that of other Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 8 J Oncol Pharm Practice 0(0) biological determinations performed in the hospital. Cost drivers were the use of personnel and consumables. Depreciation charges were low in our case because the number of control assays was substantial. HPLC determinations were more expensive than those performed by HPTLC but they only slightly affected the total cost of post-production quality control, as HPLC determinations represented only 6% of the assays performed. Some authors described recently the use of rapid HPLC method which could reduce the cost.14 However, the identification was based only on the UV spectrum of the drug as the time of analysis was to short for a real separation. As UV detection is not considered as an efficient analytical method alone for identification of an active substance, we preferred the use of a less rapid HPLC method to separate analytes. To circumvent the lack of selectivity of single UV-detection, we are currently using a more rapid and accurate analytical method, which uses infra-red detection combined to a UV one (IRTF–UV). This new technology reduces considerably the time of analysis without any doubt of identification for most of the drugs used in onco-hematology. We plan to investigate its economic impact on our quality assurance program in the next future. Excepted the indirect costs, which were specific to our institution, the unit costs used for the valuation corresponded to those of the market. Our results are therefore generalizable to other hospitals and allowed us to inform pharmacists and hospital managers about the economic impact of post-production quality control. However, even if these are mandatory activities, the pharmaceutical activities of drug preparation or quality control are not coded like other medical activities (e.g., radiology or biology). Thus, the hospital does not receive any financial compensation when it conducts these control checks: control check costs represent exclusively an item of expenditure for a hospital. The sampling plan contributed to hospital efficiency, as it both allowed us to maintain the same level of quality and to reduce the overall cost of quality control. Based on our estimation, the application of the sampling plan enabled savings of about 150,000E over the past 6 years, representing 25% of the overall budget of this activity. Finally, control check costs appeared to be very low as compared to potential litigation costs, which can occur in case of errors during the production of chemotherapy preparations. References 1. Decree n 2000–1316, 2000. 2. Projet de Guide de Bonnes Pratiques de Préparations. Agence Française de Sécurité Sanitaire des Produits de Santé (A.F.S.S.A.P.S.), Bonnes Pratiques de Préparation, Paris, 21st November, 2007. 3. Article L. 5121–5 of the Public Health Code. 4. Arrêté du 22 juin 2001 et B.O. MES n 2001-BOS 2 bis, 2001. 5. Boylan JC. Essential elements of quality control. Am J Health-Sys Pharm 1983; 23: 1936–1939. 6. American Society of Health System Pharmacists. ASHP guidelines on preventing medication errors with antineoplastic agents. Am J Health-Syst Pharm 2002; 29: 1648–1668. 7. American Society of Health System Pharmacists. ASHP guidelines on quality assurance for pharmacy-prepared sterile products. Am J Health-Syst Pharm 2000; 57: 1150–1169. 8. Morris AM, Schneider PJ, Pedersen CA and Mirtallo JM. National survey of quality assurance activities for pharmacy-compounded sterile preparations. Am J Health-Syst Pharm 2003; 60: 2567–2576. 9. Bourget P, Paci A, Rey JB, Mercier L and Dermidjian S. Contribution of high-performance thin-layer chromatography to a pharmaceutical quality assurance program in a hospital chemotherapy manufacturing unit. Eur J Pharm Biopharm 2003; 56: 445–451. 10. Gravel E, Bourget P, Mercier L and Paci A. Fluorescence detection combined with either HPLC or HPTLC for pharmaceutical quality control in a hospital chemotherapy production unit: application to camptothecin derivatives. J Pharm Biomed Anal 2005; 39: 581–586. 11. Weber RT. An easy approach to acceptance sampling: how to use MIL-STD-105E, 1st ed. Madison, WI: American Society for Quality Press, 1991. 12. Montgomery DC. Introduction to statistical quality control, 4th ed. New York: Wiley, 2000. 13. Borget I, Laville I, Paci A, Michiels S, Mercier L, Desmaris RP, et al. Application of an acceptance sampling plan for post-production quality control of chemotherapeutic batches in a hospital pharmacy. Eur J Pharm Biopharm 2006; 64: 92–98. 14. Delmas A, Gordien JB, Bernadou JM, Roudaut M, Gresser A, Malki L, et al. Quantitative and qualitative control of cytotoxic preparations by HPLC-UV in a centralized parenteral preparations unit. J Pharm Biomed Anal 2009; 09: 1213–1220. Downloaded from opp.sagepub.com at Institut Gustave Roussy on May 12, 2011 View publication stats