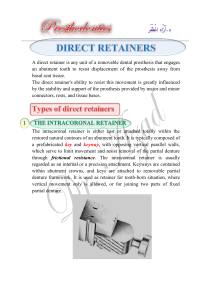
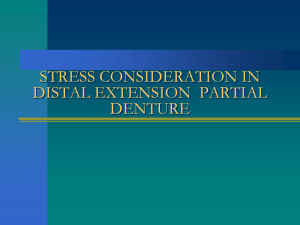
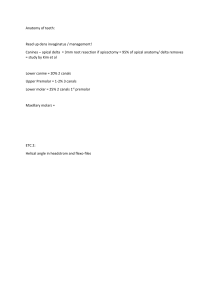
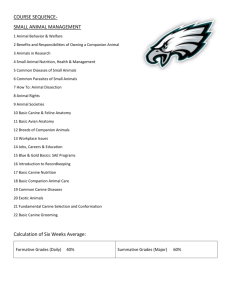
TechniqueTips Supported by Technique Tips – Management of a De-bonded, Fixed- fixed, Resin-bonded Bridge Figure 1. Clinical photograph of the failed 3-unit fixed-fixed RBB replacing a missing maxillary first premolar. Resin-bonded Bridges (RBBs) have been used for the last 40 years with different success rates. The use of RBBs is a conservative approach for replacing missing teeth and gives the patient the advantages of using the fixed prosthesis. Since their introduction, a great deal of effort has been put into their development in order to increase their longevity and clinical use. When a RBB is used, ideally the abutment tooth should be decay- and/or restorationfree. The preparation should be conservative and confined within the enamel.1,2 Maximum surface coverage and wraparound are required to obtain a maximum surface area of the abutment tooth for bonding.3,4 In this clinical tip, a missing maxillary left first premolar was replaced with a fixed-fixed RBB using the canine and the second premolar teeth as abutment (Figures 1 and 2). The bridge failed as the retainer on the maxillary left canine was de-bonded. The patient was made aware of different treatment options and their advantages and disadvantages. The patient chose to have the bridge converted into a cantilever type without removing and re-cementing the bridge. The connecter between the pontic and the canine retainer was cut using a coarse diamond bur and the metal retainer was removed. The remaining resin cement left on the palatal surface of the canine tooth was smoothed down and the palatal surface was coated with fluoride varnish (Duraphat® 22,600 ppm fluoride) (Figure 3). The bridge now works as a cantilever RBB (Figure 4). Figure 2. Occlusal view of the failed RBB. The distal retainer covers the palatal cusp. Note the space between the fitting surface of the retainer and the canine abutment tooth. A cupping defect in the incisal edge of the canine abutment is obvious. This cupping is treated with a composite resin restoration (not seen). TSL can also be seen in the second premolar abutment at the margin of the retainer. Figure 3. Post-operative clinical photograph. The resin cement can be seen covering almost all palatal surface of the abutment. This indicates that the failure is adhesive in nature and occurs between the fitting surface of the retainer and the cement and not between the abutment surface and the cement. Note the gingival inflammation around the abutment canine and the cupped defect on the incisal edge of the abutment canine. References 1. 2. 3. St George G, Hemmings K, Patel K. Resinretained bridges re-visited. Part 1. History and indications. Prim Dent Care (Journal of the Faculty of the General Dental Practitioners (UK)) 2002; 9: 87–91. St George G, Hemmings K, Patel K. Resinretained bridges re-visited Part 2. Clinical considerations. Prim Dent Care (Journal of the Faculty of the General Dental Practitioners (UK)) 2002; 9: 139–144. Saad AA, Claffey N, Byrne D, Hussey D. Effects of groove placement on retention/ resistance of maxillary anterior resinbonded retainers. J Prosthet Dent 1995; Figure 4. The intra-oral clinical photograph taken in the recall visit at three months. The remaining lutting cement can be seen. The cupping is treated with a composite resin restoration. 4. 74: 133–139. Ibrahim AA, Byrne D, Hussey DL, Claffey N. Bond strengths of maxillary anterior base metal resin-bonded retainers with different thicknesses. J Prosthet Dent 1997; 78: 281–285. Aslam Fadel Alkadhimi, Third-year Dental Science Student, Mohammad Ashkanani, Third-year Dental Science Student, Ahmed Sultan, Fourth-year Dental Science Student and Abdulhadi Warreth, BDS, MDentSci, PhD, Clinical Supervisor in Restorative and Periodontology Division, Dublin Dental University Hospital, Dublin, Ireland. 520 DentalUpdate September 2012 © MA Healthcare Ltd. Downloaded from magonlinelibrary.com by 144.082.238.225 on October 24, 2017. Use for licensed purposes only. No other uses without permission. All rights reserved.