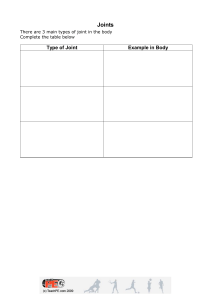
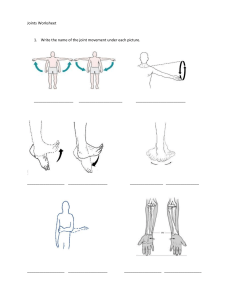
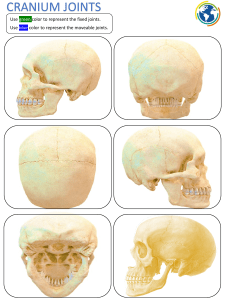
Notes by Morgan Payne Structure and Function Musculoskeletal System consists of bones, joints, and muscles , Needed for support and to stand > Needed for movement > Encases and protects inner vital organs > Produces RBCs in the bone marrow Serves as a reservoir for storage of essential minerals • Musculoskeletal Components Bones and cartilage are specialized forms or connective tissue Fibrous, cartilaginous and synovial joints Bursa: enclosed fluid sac that serves as a cushion in our joints > Ligaments: fibrous bands that connect bone to bone and prevent unwanted movement > Muscle: skeletal, voluntary control connected by tendon to bone > Tendon: connect bone to muscle • } Joints Fibrous Joints > These do not move; sutures in the skull Cartilaginous Joints Separated by fibrous cartilage and slightly moves; vertebrae • Synovial Joints Freely movable joint > Separated and enclosed in a cavity with synovial membrane that secretes fluid > Contains avascular cartilage > Surrounded by ligaments > Bursae located in areas of friction, and help the movement of muscles and tendons • • } Where are synovial joints? Ankle, knee, hip, elbow, shoulder, wrist, sacroiliac, neck, and intervertebral • The key is to remember that the synovial joints produce the greatest range of movements; they allow us to do everyday activities. Skeletal Muscles Skeletal muscles produce these movements: Flexion; extension Abduction; Adduction > Pronation; supination > Circumduction: This is circular motion of the shoulder > Inversion; eversion > Protraction; retraction > Rotation > Elevation; Depression : Temporomandibular Joint • • • Articulation of mandible and temporal bone TMJ allows us to speak and chew This is a synovial joint no Three motions: > Hinge action to open and close action for protrusion and retraction } Gliding Gliding for side to side movement of jaw Notes by Morgan Payne Structure and Function Musculoskeletal System consists of bones, joints, and muscles , Needed for support and to stand > Needed for movement > Encases and protects inner vital organs > Produces RBCs in the bone marrow Serves as a reservoir for storage of essential minerals • Musculoskeletal Components Bones and cartilage are specialized forms or connective tissue Fibrous, cartilaginous and synovial joints Bursa: enclosed fluid sac that serves as a cushion in our joints > Ligaments: fibrous bands that connect bone to bone and prevent unwanted movement > Muscle: skeletal, voluntary control connected by tendon to bone > Tendon: connect bone to muscle • } Joints Fibrous Joints > These do not move; sutures in the skull Cartilaginous Joints Separated by fibrous cartilage and slightly moves; vertebrae • Synovial Joints Freely movable joint > Separated and enclosed in a cavity with synovial membrane that secretes fluid > Contains avascular cartilage > Surrounded by ligaments > Bursae located in areas of friction, and help the movement of muscles and tendons • • } Where are synovial joints? Ankle, knee, hip, elbow, shoulder, wrist, sacroiliac, neck, and intervertebral • The key is to remember that the synovial joints produce the greatest range of movements; they allow us to do everyday activities. Skeletal Muscles Skeletal muscles produce these movements: Flexion; extension Abduction; Adduction > Pronation; supination > Circumduction: This is circular motion of the shoulder > Inversion; eversion > Protraction; retraction > Rotation > Elevation; Depression : Temporomandibular Joint • • • Articulation of mandible and temporal bone TMJ allows us to speak and chew This is a synovial joint no Three motions: > Hinge action to open and close action for protrusion and retraction } Gliding Gliding for side to side movement of jaw • Spine and Vertebrae Notes by Morgan Payne Vertebrae 33 connecting bones stacked in a vertical column 7 Cervical = 12 thoracic 5 lumbar 5 sacral 3 to 4 coccygeal Surface landmarks > Spinous process of C7 and T1 prominent at base of neck > Inferior angle of scapula normally at level of interspace between T7 and T8 > Imaginary line connecting highest point on each iliac crest at L4 >Imaginary line joining two symmetric dimples that overlie posterior superior iliac spines crosses sacrum - - • Spine Has four curves; a double s shape : Cervical and lumbar curves are concave; inward Thoracic and sacro > Intervertebral disks are elastic fibrocartilaginous >Motions of vertebral column Flexion, extension, abduction, rotation - - > Abnormal Curves of spine Lordosis: inward; think of pregnancy, lumbar area Kyphosis: outward curve, thoracic curvature increases > Scoliosis: lateral curve, sideways > > • • • • • Shoulder Shoulder girdle: humerus, scapula, clavicle, joints, and muscle Glenohumeral Joint: articulation of humerus with glenoid fossa of scapula > Ball and socket joint allows mobility of arm in many ways Rotator Cuff: , Group of four muscles and tendons support and stabilize shoulder Subacromial bursa: > Assists with abduction of the arm Palpable landmarks to help guide your examination: Scapula and clavicle form shoulder girdle Should feel the bump of the scapula's acromion process at very top of shoulder > > Elbow; wrist; carpals • Elbow ,Joint contains three bony articulations: humerus, radius, and ulna or forearm > Palpable landmarks: medial and lateral epicondyles of humerus and large olecranon process; the bony parts of the sides of your elbows > Radius and ulna articulate with each other at two radioulnar joints, one at elbow and one at wrist aaa Wrist, or radiocarpal, joint > Articulation of radius on thumb side and row of carpal bones >Condyloid action permits movement in two planes at right angles; flexion and extension, and side to side deviation >Midcarpal joint: articulation allows flexion, extension, and some rotation Bones in the hand, palm area, are condoyles; they are rounded :Hip Articulation between acetabulum and head of the femur > Ball and socket action permits wide range of motion More stability for weight bearing Muscles enhance stability and bursae facilitate movements Palatable landmarks: Iliac creat; anterior superior spine to posterior Ischial tuberosity Greater trochanter of the femur • The "sitting bone" is the Ischial Tuberosity • MM • Notes by Morgan Payne Ankle and Foot Ankle or tibiotalar joint: articulation of tibia, fibula, and talus > Hinge joint: limited to flexion and extension Landmarks are two bony prominences on either side • Joints distal to ankle give additional mobility to foot Subtalar joint permits inversion and eversion of foot; this does not come from ankle > Foot has an arch, to distribute the weight of the body evenly • ? Knee Knee Joint: articulation of three bones: femur, tibia, and patella; in common articular cavity , Largest joint in the body; hinge joint, permitting flexion and extension of lower leg in single plane me Synovial Membrane is largest in body • Two wedged shaped cartilages, called medial and lateral menisci, cushion the tibia and femur Knee stabilized by two sets of ligaments: % Cruciate give anterior and posterior stability and help control rotation > Collateral ligaments give medial and lateral stability and prevent dislocation • Landmarks of the knee: > Quadriceps muscle, felt on anterior and lateral thigh > Tibial tuberosity, felt as bony prominence in the midline > Note lateral and medial condyles of tibia > Medial and lateral epicondyles of femur are on either side of patella • Developmental Competence: Infants and Children By 3 months, the fetus has a "scale model" of the Skelton of cartilage Ossification of true bone continues in utero • Bone growth continues rapidly during infancy and childhood Until adolescence growth spurt Bone growth occurs in two dimensions Epiphyses: specialized growth plates at end of long bones Longitudinal growth continues until closure of epiphyses, last closure occurs at about age 20 Although Skelton contributes to linear growth, muscles and fat are significant for weight increase , muscles vary in size and strength in different people due to genetics, nutrition, and exercise may } • } • • • Notes by Morgan Payne Developmental Competence: Pregnant Women Increased levels of circulating hormones causes increased mobility in joints Increased mobility in sacroiliac, sacrococcygeal, and symphysis pubis joints in pelvis Contributes to noticeable changed in maternal posture > Lordosis > Compensatory postural change anterior flexion of neck and slumping of shoulder girdle > Pressure on ulnar and median nerves seen in last trimester > Developmental Competence: Aging Adult Bone remodeling is cyclic process or resorption and deposition > After age 40, resorption occurs more than deposition > Risk for osteoporosis Postural changes and decreased height > Kyphosis with slight flexion of hips and knees to compensate Distribution of subcutaneous fat changes > Leaves bony prominences more marked > subcutaneous fat typically moves to trunk • Significant loss in muscle > Decrease in size and atrophy producing weakness • • D8 • • • Culture and Genetics Earlier peak and rapid decline of BMD with increased fracture risk seen in Caucasian women Use BMD to educate patient about preventing injury from falls DEXA screening recommended for females aged 65 and up: measures bone density • Bone Mineral Density: BMD Higher BMD: denser bone > Low BMD: predictor of fractures > Subjective Data Notes by Morgan Payne Ask About: > Joints: pain, stiffness, swelling, heat, redness, limitation of movement > Knee joint if injured > Muscles: pain, cramps, or weakness Bones: pain, deformity, trauma > Functional Assessment of ADLS > Patient centered care: prevention, exercise • > What is the difference between a functional assessment and a physical assessment? • • • Functional: , You are trying to figure out how the person is living their daily life > Are they able to get around and do all the things they are suppose to? Physical: > You are just documenting your objective findings Order of Examination Inspection, Palpation, then range of motion ROM > Active ROM is patient voluntary moving themselves If we see a limitation we gently use passive ROM and move the patient ourselves :Test Muscle Testing and ROM Strength of prime mover muscle groups for each joint; repeat motions for active ROM Ask person to flex and hold as you apply opposing force Muscle strength should be equal bilaterally and fully resist opposing force • Use standardized grading scale to report results: 0 to 5 range , 0: no muscle contraction > 1: slight contraction > 2: Poor, full contraction with gravity eliminated: passive motion > 3: fair, full ROM with gravity > 4: good, full ROM against gravity and some resistance 5: NORMAL full ROM against gravity and full resistance • • :Temporomandibular Joint: TMJ Inspect and Palpate Audible and palpable snap or click occurs in many healthy people as mouth opens Palpate contracted temporalis and masseter muscles as person clenches teeth > Bilateral comparison Ask person to move jaw forward and laterally against your resistance, and to open mouth against your resistance This joint is testing Cranial Nerve v motor function of Trigeminal nerve > > : Cervical Spine Inspect alignment and head of neck: spine should be straight and head erect Tested with cranial nerve XI: spinal accessory nerve > Have patient shrug shoulders and turn head side to side, first without resistance then with • ROM: you can have the patient move chin to chest, lift chin to ceiling, turn chin towards shoulders, or touch ear to shoulder • • Shoulder • Inspect and compare both shoulders posteriorly and anteriorly , Do NOT attempt if you suspect neck trauma • Ask about pain: it can be from local causes or may be referred pain which could be serious , Pain from local cause is reproducible by palpation or motion aaaaa ROM: flexion, abduction, adduction, internal rotation, external rotation • Tests cranial nerve XI: Spinal accessory Notes by Morgan Payne Elbow Check that olecranon bursa and the normally present hollows on each side olecranon process for abnormal swelling Palpate elbow flexed at 70 degrees and relaxed ROM: bend and straighten elbow, then with resistance Allt Mr Wrist and Hand Mao NB PHALEN Test was 2m Inspect Palpate ma Perform ROM; assess grip strength PHALEN TEST: wrist produces numbness and burning if positive for Carpal Tunnel > Place back of hands together at a 90 degree angle and hold for 20 seconds > Normal is no pain rang Tinel sign Test: percussion of median nerve produces burning and tingling if positive Mau Hip Inspect hip Joint together with spine later in examination as person stands up Note symmetric levels of iliac crest, gluteal folds, and equally sized buttocks Smooth, even gait reflects leg lengths and functional hip motion ROM: limitation of abduction of hip while in supine position is most common motion dysfunction found in hip disease • i Knee Person should remain supine with legs extended ROM: bend and extend knee, and walk • Swelling: test for bulge sign > Stroke up the knee 2 or 3 times and watch for any fluid displacement • Swelling: test for ballottement of patella This will distinguish between soft tissue swelling or increased fluid in joint • MCMURRAY'S TEST: if meniscal tear is suspected pt supine, flex affected knee and hip while holding heel, other hand on inner side of knee, rotate leg in and out, then straighten leg > If there is a 'click' and pain when straightening leg, they are positive for a meniscal tear • Do ? Ankle and Foot Inspect while person is sitting, standing, and walking % Foot should align with long axis of lower leg Weight bearing should fall on middle of foot Examining well worn shoes helps assess areas of wear and accommodation m Palpate > Metatarsophalangeal joints • Perform ROM: dorsiflexion, plantar flexion, inversion, eversion Assess muscle strength; have pt maintain dorsiflexion and plantar flexion against you resistance > • Spine -4 Inspect , From side, note normal convex thoracic curve and concave lumbar curve • Palpate > Spinous processes; normally straight and not tender Check ROM of spine by stabilizing pelvis with your hands • Spinal ROM: ask person to touch toes, look for flexion 75 to 90 degrees Pelvis ROM: , lateral bending of 35 degrees > Bend backwards, hyperextension of 30 degrees Twist shoulders to one side then the other; rotation of 30 degrees > Ask person to walk on their toes and then heels; strength of spine ⑧ Lordosis: exaggerated lumbar curve seen in obese and pregnant people Kyphosis: Enhanced thoracic curve typically seen in aging people • • • > • Notes by Morgan Payne Straight Leg Raise or Lasegue's Test Raise affected leg and then dorsiflex the foot Test positive if it reproduced sciatic pain • Confirms presence of herniated nucleus pulposus; herniated disc • • Measure Leg Length Discrepancy • • • • Perform this measurement if you need to determine whether one leg is shorter than other For true length measure between fixed points > From anterior iliac spine to medial malleolus, crossing medial side of knee Normally these measurements are equal or within 1 cm, indicating no discrepancy Developmental competence Infants Examine infant fully undressed and lying on back; maintain temperature Feet and Legs , Look for any deformities > Note relationship of forefoot to hind foot Check for tibial torsion; twisting of tibia • Hips Hip dislocation is common, check until the age of 1 year > Ortolani's Maneuver and The Barlow Maneuver Check for hip dysplasia Hands and % InspectArms hands: noting shape, number, position, and palmar creases > Palpate along clavicles The bone most frequently fractured during birth oooo Back > Lift infant and examine back: note normal single C curve of newborns spine Inspect length of spine and any tuft of hair, dimple in midline, cyst, or mass • Observe ROM through spontaneous movements: Test muscle strength by picking up infant with hands under axillae • • } - - ? • • • • Developmental Competence: Preschool and school aged children Lordosis is common throughout childhood Observe legs and feet for various deformities: > Bowleg, knock knees, flatfoot, pigeon toes Particularly check arm for full ROM and presence of pain > Look for subluxation of elbow; partial dislocation Palpate bones, joints, and muscles of extremities as in adult examination Developmental Competence: Adolescents Proceed with same examination as for adults; pay special attention to spinal posture > Kyphosis is common during adolescence because of chronic poor posture > Screen for scoliosis with forward bend test • • • Developmental Competence: Pregnant Women Notes by Morgan Payne Proceed through same examination as for adult Expected postural changes in pregnancy > Progressive lordosis > Toward third trimester, anterior cervical flexion > Kyphosis and slumped shoulders > When full term; relaxed mobility in joints create "waddling" gait Developmental Competence: Aging Adult Postural changes include decrease in height and more apparent in eight and ninth decades Kyphosis is common with backward head tilt to compensate • Decrease of fat in periphery; fat deposition over abdomen and hips Bony prominences become more marked; less subcutaneous fat for protection ROM testing Get up and Go test to see how they are moving Perform functional assessment for ADLs • • • • • • Health Promotion and Patient Teaching Diet to protect and maintain healthy bones Smoking cessation Alcohol intake pattern Exercise promotion Osteoporosis Screening ,Diet is essential for bone health Fall prevention risk • Vitamin D and calcium need to be taken together to prevent osteoarthritis • • • • • • Joint Abnormalities Inflammatory conditions ,Rheumatoid Arthritis: autoimmune > Ankylosing Spondylitis: Inflamed Vertebrae;begins in adolescence Degenerative conditions > Osteoarthritis: degenerative joint disease > Osteoporosis: decrease in bone density, postmenopausal women and short skin people at risk • • Rheumatoid Arthritis Inflammatory condition of joint Autoimmune disease: affects symmetrical Joints • More likely in women ages 30 to 60 • This causes joint destruction, bone destruction, and visible deformities •Joints will be: > Red, swollen, painful • Early Manifestations: fatigue and fever • Later in disease: visibly malformed joints RA increase cardiovascular risk of heart attack and stroke • • • Osteoarthritis Degenerative joint disease Progressive deterioration of articular cartilage • Stiffness, swelling, pain, and limited ROM are all signs: not symmetrically • Crepitus and pain with ROM: feels like gravel under skin • • Notes by Morgan Payne Abnormalities: shoulder, elbow, and spine • Shoulder: Glenohumeral dislocation is most common joint dislocation, Joint effusion is excess fluid in joint capsule, tear of rotator cuff, frozen shoulder is when fibrous tissue form in joint capsule and limit motion • Elbow: olecranon bursitis is large soft knob with swelling and redness to elbow, epicondylitis or tennis elbow is inflammation of flexor and extensor tendons of elbow joint • Spine: scoliosis, herniated intervertebral disc Wrist and Hand Abnormalities Ganglion Cyst • Carpal Tunnel syndrome with atrophy of thenar eminence , Pain along thumb and index finger from receptive motions > common in 40 to 60 year old women > Ankylosis: rupture of the extensors caused by severe RA > Dupuytren's Contracture: causes progressive flexion of 4th, 5th, and 3rd finger > Ulnar deviation or drift: fingers go to ulnar side > Polydactyl: extra digits > Syndactyl: Webbed digits v08 • • Knee Ankle Foot Abnormalities Knee , Osgood Schlatter disease: commonly in adolescence, swelling of the tibial tubercle; from overuse > Muscle Atrophy > Mild Synovitis > Prepatellar Bursitis Ankle and Foot > Achille's Tenosynovitis > Gout: inflammatory arthritis caused by excessive Uric acid Red, swollen, hot extreme pain Caused by surgery, trauma, alcohol, diuretics, obese pt, HTN, metabolic syndrome, hyperlipidemia Hallux Valgus with bunion and hammer toes Plantar Fasciitis inflamed fascia from receptive trauma and injury; common problem in nurses from standing ÷ Congenital Or Pediatric Abnormalities Developmental dysplasia of the hip , What tests? Ortolani's and Barlow's maneuver • Talipes Equinovarus; clubfoot; inverted, adducted, and pointing downward Spina Bifida > Incomplete closure of the posterior vertebrae > caused by neural tube defect > Seriousness depends by the amount of sac protrusion on Notes by Morgan Payne • Summary Checklist: Musculoskeletal Examination • Inspection Size and contour of joint Skin color and characteristics Do Palpation of joint area Skin, muscles, bony articulations, and joint capsules • ROM Active Passive; if limitation notes in active ROM is present H Muscle Testing