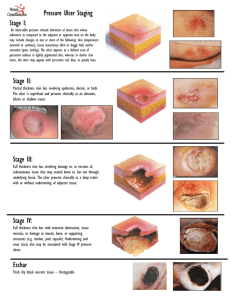
ULCERS Abdallah General Surgery ttcih-Ifakara Outline Definition Aetiology Classification Pathophysiology Clinical presentation Workup Treatment Definition A break in the continuity of the covering epithelium of the skin or mucous membrane It may either follow molecular death of the surface epithelium or its traumatic removal Aetiology Trauma Vascular insufficiency Neoplastic conditions Metabolic diseases e.g. diabetis mellitus, Infective processes eg TB, syphilis Neurogenic Classifications Clinical classification Pathological classification Clinical classification Spreading ulcer Healing ulcer Callous ulcer Spreading ulcer Surrounding skin is inflammed Floor is covered by slough No evidence of granulation tissue Purulent discharge Healing ulcer Surrounding skin not inflamed Floor covered with granulation tissue Edges show bluish outline of the growing epithelium Slight serous discharge Callous ulcer Pale granulation tissue in the floor Considerable induration at the base, edge and surrounding skin Show no tendency towards healing Pathological classification Non specific ulcers Specific ulcers Non specific ulcers Traumatic ulcers Arterial ulcers Mechanical Physical – electrical, radiation etc Chemical Due to ischaemia eg following atherosclerosis, Buergers disease Venous ulcers Varicose ulcer Neurogenic ulcers (trophic ulcer) Ulcers associated with malnutrition eg tropical ulcer Ulcers associated with other diseases eg bed sores, perforating ulcers eg anemia, avitaminosis, gout, rheumatoid arthritis Miscellaneous ulcer eg Bazin ulcer, martorell’s (hypertensive ulcer) Specific ulcers Infective ulcers eg syphilitic ulcers, tuberculous ulcer Malignant ulcers eg Squamous cell carcinoma Basal cell carcinoma ( rodent ulcer) Malignant melanoma Ulcerating adenocarcinoma Pathophysiology The natural history of an ulcer consists of three phases: Extension phase Transition phase Repair phase Extension phase The floor is covered with exudate and sloughs The base is indurated The discharge is purulent or even blood stained Transition phase Prepares for healing The floor becomes cleaner and the slough separates The induration of the base diminishes The discharge become more serous Small reddish area of granulation tissue appear on the floor Repair phase Transformation of granulation to fibrous tissue, which gradually contracts to form scar The epithelium gradually extends from the new shelving edge to cover the floor (at a rate of 1mm/day) The healing edge consists of three zones: Outer zone: this is white in color Middle zone: bluish in color, granulation tissue covered by few layers of epithelium Inner zone: reddish in color, a zone of granulation tissue covered by a single layer of epithelial cells. The red granulation tissue is due to density of new capillaries (neo-angiogenesis) Clinical presentation I History; note the following: Duration i.e. how long is the ulcer present? Mode of onset i.e. how has the ulcer developed? Acute: present for short time Chronic: present for long time Following trauma Spontaneously eg following- swelling eg ulcerating LN in TB or a scar of burn Marjolin ulcer Pain i.e. is the ulcer painful? Painful: ulcers associated with inflammation Slight painful: tuberculous Painless eg syphilitic, neurogenic, malignnt ulcer Clinical presentation II History (cont’d) Discharge: i.e does the ulcer discharge or not? Associated diseases which may lead to ulcer formation If YES: note the nature of discharge- pus, bloody, serous E.g. TB, Syphilis, DM, nervous diseases Physical examination General examination Local examination Systemic examination Clinical presentation III PE (cont) General examination may be normal Local examination Inspection Site: gives clue to the diagnosis Varicose ulcer- lower limb on the medial malleolus Rodent ulcer-face Tuberculus ulcer-cervical Trophic ulcer – heal Malignant ulcer- anywhere Clinical presentation III Shape: Tuberculus ulcer- oval in shape Syphilitic ulcer– circular in shape Varicose ulcer – vertically oval in shape Malignant – irregular in shape Size: May determine the time of healing E.g. the smaller the ulcer the shorter the time it will take to heal Clinical presentation IV Surrounding skin Floor/surface i.e. exposed part of the ulcer may give clue to the diagnosis E.g. red and edematous- acute inflammation Eg red granulation – healing ulcer Black floor- malignant melanoma Number Tuberculous ulcer Gummatous ulcer Varicose ulcer may be more than one Clinical presentation V Edge: five types: Undermined edge Punched out edge Eg healing ulcer Raised edge Eg. Gummatous ulcer, deep trophic ulcer Sloping edge Eg; tuberculous ulcer-destroy subcutanous faster the skin Rodent ulcer Rolled out (everted)- eg SCC, Clinical presentation V Discharge: the character of the discharge should be noted e.g. Healing ulcer- scant serous discharge Spreading ulcer- purulent discharge Tuberculus ulcer- serosanguinous Malignant ulcer- bloody discharge Whole limb: should be examined e.g. varicose veins Clinical presentation VI Palpation: note: Tenderness: Edge and surrounding skin Tender- acutely inflamed ulcer Slightly tender- tuberculous ulcer, syphilitic ulcer Non-tender- malignant ulcer, chronic ulcer, neurogenic ulcer Hard induration- malignant ulcer Firm induration- chronic ulcer, syphilitic ulcer Base (i.e. on which the ulcer rest) Slightly induration- syphilitic ulcer Marked induration- malignant ulcer Clinical presentation VII Depth: Bleeding; easy bleed on touch is a feature of malignant Fixity to the deep structures eg trophic ulcer may be deep to reach the bones Eg malignant ulcers are usually fixed to deep structures Examination of lymph nodes Examination of vascular insufficiency eg pulses Examination of nervous system eg sensation workup Lab studies Imaging studies Pus swab for- c/s FBP +ESR CXR : to detect primary focus in the lungs in case of tuberculus ulcer X-ray of the bone or joint if the ulcer is situated near a bone or joint Biopsy- to conform the diagnosis Treatment Depends on the underlying cause Generally: Dressing Skin grafting flaps