The Peripheral Blood Film (Trevor A. Harper (Auth.)) (z-lib.org)
advertisement
) (z-lib.org)")
The
Peripheral
Blood Film
Second Edition
TREVOR A. HARPER
M.B,B.S. (Madras) M.R.C. Path.
Haematologist, Department of Laboratory
Haematology, Sunnybrook Medical Center,
University of Toronto Clinic, Toronto, Canada
Butterworths
ENGLAND:
BUTTERWORTH & CO. (PUBLISHERS) LTD.
LONDON: 88 Kingsway, WC2B 6AB
AUSTRALIA:
BUTTERWORTHS PTY. LTD.
SYDNEY: 586 Pacific Highway, 2067
MELBOURNE: 343 Little Collins Street, 3000
BRISBANE: 240 Queen Street, 4000
CANADA:
BUTTERWORTH & CO. (CANADA) LTD.
ONTARIO: 2265 Midland Avenue,
Scarborough, M1P 4SI
NEW ZEALAND: BUTTERWORTHS OF NEW ZEALAND LTD.
WELLINGTON: 26-28 Waring Taylor Street, 1
SOUTH AFRICA: BUTTERWORTH & CO. (SOUTH AFRICA) (PTY.) LTD.
DURBAN: 152-154 Gale Street
©
Butterworths & Co. (Publishers) Ltd.
1974
Suggested U.D.C. Number: 612:11 - 086: 616-155 - 076
ISBN 0 407 76001 6
Printed in Great Britain by
Lowe & Brydone (Printers) Ltd.,
London · Thetford
To
My Wife
Preface to Second Edition
The present edition has been extensively revised, rewritten and
expanded to incorporate new information. Current concepts of the
origin, development and functions of blood cells are briefly discussed.
The differential diagnosis is classified more thoroughly and additional
tables are included. Laboratory investigations are now tabulated in a
separate chapter with alphabetical listing of diseases, disorders and
abnormal film appearances for easier reference. Cytochemical tests of
value in the diagnosis of disorders such as acute leukaemia, 'hairy' cell
leukaemia, abnormal leucocyte function and abnormal haemoglobins
are described in Appendix A. A bibliography and reference section is
now included at the end of the book. All the monochrome photomicrographs now appear in a separate plate section at the end of the
book and their various magnifications have been standardized. The
'Atlas of Haematology' by George A. McDonald, T. C. Dodds and Bruce
Cruickshank (Livingstone) is still highly recommended.
I wish to thank the staff of the Department of Medical Illustration at
Sunnybrook Medical Center for their professional help. I am grateful to
the publishers for their patience and understanding during the delay in
the preparation of this manuscript.
T.A.H.
IX
Preface to First Edition
Microscopic examination of a stained peripheral blood film is one of
the commonest of laboratory investigations and the most important of
its diagnostic applications is the assessment and interpretation of the
cellular pattern that is observed. The appearances of the blood film in
disease are described and discussed in textbooks of haematology but
only after extensive reading and experience does the laboratory technician and trainee pathologist become familiar with the basic abnormal
patterns of the blood film and fully aware of the significance of any
alterations in their known cellular composition.
The aim of this book is to present a practical guide to the types of
film appearances that may be encountered in the routine examination
of peripheral blood films and to list the diseases and disorders in which
they may be seen. A knowledge of the morphology of cells that are
likely to occur in blood is essential and descriptions of blood cells and
their precursors are included in the early chapters.
This book is not intended to be an atlas and although monochrome
photomicrographs have a limited value in haematology they are used to
illustrate some cells and film appearances; the reader is advised to
consult the excellent colour pictures in t h e ^ t e of Haematology by
George A. McDonald, T.C. Dodds and Bruce Cruickshank (Livingstone).
I am grateful to the staff of the Department of Medical Illustration
at Wythenshawe Hospital for their professional help in the preparation
of the photomicrographs.
T.A.H.
xi
1
Introduction
Blood is a suspension of cells in a pale yellow fluid (plasma); the
cell-to-plasma ratio is approximately 45/55. The cells are heterogenous
and consist of haemoglobin-containing red cells (erythrocytes), platelets
(thrombocytes) and white cells (leucocytes). The red cells and platelets
are disc-shaped, non-nucleated and non-motile cells. The leucocytes are
nucleated, motile and may be further sub-divided into two groups: the
polymorphonuclear cells — the neutrophil, eosinophil and basophil
granulocytes, and the mononuclear cells — the monocytes and
lymphocytes. In addition to these peripheral blood cells, a mononuclear
non-motile cell that is derived from the lymphocyte and termed the
plasma cell (plasmacyte) may be seen in 'normal' blood. Plasma is a
complex fluid. It consists principally of water and many organic and
inorganic compounds such as proteins (albumin, globulin, fibrinogen,
enzymes, etc.) electrolytes (sodium, potassium, chloride, bicarbonate,
etc.), materials absorbed from the gastro-intestinal tract (iron, amino
acids, fats, glucose etc.) and products of tissue activity (bilirubin, urea,
uric acid etc.).
Blood cells have a limited life span which is further shortened in
diseases. They are continuously replaced through a process of
sequential and multiplicative mitotic division, and maturation of
differentiated precursor cells located within the haemopoietic system
which comprises the bone marrow and lymphatic tissues (thymus,
spleen and lymph nodes). The earliest morphologically identifiable
precursor cell of each series of cells is the 'blast' cell: for example,
pro-erythroblast (red cells), megakaryoblast (platelets), myeloblast
(granulocytes), monoblast (monocytes), lymphoblast (lymphocytes)
and plasmablast (plasma cells). The differentiated precursor cells are
not self-sustaining. Blast cells develop from progenitor cells that have
differentiated from ancestral, self-renewable pluripotent cells with
multiple differentiating capacities. These primitive haemopoietic cells
have not as yet been morphologically identified and are termed 'stem'
cells.
1
THE PERIPHERAL BLOOD FILM
Apart from the erythrocytes which give the blood its red colour,
haemopoietic cells are colourless and transparent. They may be studied
by electron or phase contrast microscopy. Their morphology, however,
is commonly ascertained by examination of a stained smear on a glass
slide using conventional light microscopy techniques. Romanovsky dyes
are universally used for staining the cells because they differentially
stain the nucleus, cytoplasm and any inclusions that may be present. In
disease states cytochemical techniques may be necessary to
differentiate some cell classes and to demonstrate the presence, absence
or excess of certain cellular constituents. Cytochemical staining is the
application of specific chemical reactions to 'fixed' smears or to
suspensions of metabolically active cells; the latter is referred to as
'supravital' staining.
In addition to the blood cells previously mentioned, an occasional
precursor cell may be seen in films from normal subjects. However, in
disease not only are the normal parameters altered either absolutely or
relatively, but non-haemopoietic cells and increased numbers of normal
or pathological precursor cells may be observed in the stained blood film.
Many disorders have characteristic cell populations in the blood; the
disappearance of some cell types and the appearance of others may
herald changes in the prognosis of the disease. Thus the microscopic
examination of the stained blood film is an important laboratory
investigation. The blood picture, by corroborating or refuting the
clinical diagnosis, by indicating the presence or development of
complications, by providing a differential diagnosis, is of diagnostic
and/or prognostic value. The peripheral blood film is also used for the
haematological diagnosis of the sex of an individual, the detection of
foetomaternal transplacental haemorrhage and the detection of
infestation by blood parasites such as plasmodia which cause malaria.
2
2
Preparation and Staining of
Blood Films
BLOOD COLLECTION
Peripheral blood films may be made with capillary blood or with
anticoagulated venous blood. To obtain capillary blood pierce the
cleansed skin of the finger, ear lobe, or in the case of infants the plantar
surface of the heel with a disposable sterile lancet. Obtain venous blood
from an accessible vein, such as the antecubital vein of the forearm with
a sterile syringe and needle; remove the needle from the syringe and
transfer the blood to a tube or bottle containing as anticoagulant the
dipotassium salt of ethylenediaminetetra-acetic acid (EDTA, 1 - 2 ng/ml
blood). Venous blood may also be collected directly into a
rubber-stoppered 'Vacutainer' tube containing EDTA.
PREPARATION OF THE THIN BLOOD FILM
Thin blood films may be spread on microscope slides or on square
coverslips; these should be dry, chemically clean, grease-free and
dust-free. The use of microscope slides is preferable. New unused slides
should be polished with a dry dust-free cloth; they may be rinsed in
methanol before polishing. A second slide with cut-out corners may be
used as a spreader; the narrow spreading edge must be ground smooth.
Apply a drop of blood, approximately 3 mm in diameter, to the
midline of the microscope slide, 1 - 2 cm from a narrow edge and place
the slide on a flat horizontal surface. Holding the spreader at an angle
to the horizontal, place the narrow edge on the surface of the slide in
front of the drop of blood and gently draw it backwards until it
touches the drop. Surface attraction will cause the blood to run
between the spreader's edge and the microscope slide. Hold the
spreader slide at an angle of 30-45° to the horizontal and slide it along
the microscope slide with a quick, smooth movement. The spreader
must at all times be in contact with the slide and lifted off only after
the drop of blood has been completely spread. Allow the film to dry in
air and pencil the patient's name and laboratory number on the slide.
3
THE PERIPHERAL BLOOD FILM
The length and thickness of the film depends on the size of the drop
of blood that is spread, the angle of the spreader to the microscope
slide and the speed of movement of the spreader slide. The larger the
drop of blood, the greater the angle at which the spreader is held, and
the faster the sliding movement of the spreader, the thicker the film
formed. However, thick blood films do not stain well and these
variables must be adjusted to produce a good film; this can be achieved
with a little experience. The ideal thin blood film should be about 3 cm
long, appear smooth without wrinkles or serrations and occupy the
middle one-third of the slide. The film should have two long free
margins and not extend to the edges of the microscope slide.
PREPARATION OF THE THICK BLOOD FILM
The thick blood film is only of value for the detection of malarial
infestation of blood, especially when the number of parasites is scanty.
Apply a drop of blood approximately 6 mm in diameter to a
microscope slide. With the corner of another clean slide spread the drop
out rapidly so as to cover an area that would make it possible to read
the hands of a watch or small print through it when dried. Cover the
slide and allow the film to dry in air for at least 30 minutes. Drying
may be hastened by placing the covered slide in an incubator at 37°C.
Do not heat the smear over a naked flame; this will fix the smear and
hinder subsequent haemolysis of the red cells during the special staining
techniques (see Appendix A). The advantage of the thick blood film is
that a larger volume of blood in a smaller area may be examined.
However, identification of the type of malarial parasite may be
difficult.
CELL CONCENTRATION TECHNIQUES
In certain haemopoietic disorders, scanty numbers of bone marrow cells
enter the circulation. The detection of these cells may be of diagnostic
importance but their presence may not be evident in the routinely
prepared blood film; a concentration technique is necessary for easier
detection. Cell concentration is simply and readily carried out by
centrifugation of anticoagulated blood in a long narrow tube, such as
Wintrobe's haematocrit tube. The blood separates into three layers. The
thin white buffy coat layer, separating the lower red cell column from
the clear supernatant plasma, is aspirated together with a small amount
of the plasma and transferred to a separate tube where the cells are
resuspended. Films are then spread and stained on microscope slides in
the usual manner.
4
PREPARATION AND STAINING OF BLOOD FILMS
This centifugation technique is commonly employed for detecting
the L.E. cell phenomenon after incubation of defibrinated whole blood
at 37°C. It is also used for concentrating abnormal erythrocytes and,
when there has been an incompatible blood transfusion, for separating
recipient's red cells from transfused donor red cells. Nucleated red cells,
reticulocytes, stomatocytes, red cells infested with malarial parasites
and the red cells of a blood transfusion recipient are more numerous in
the upper portion of the red cell column. Normal erythrocytes,
macrocytes, spherocytes, older red cells and transfused donor red cells
are concentrated in the lower portion of the column. Red cells
containing haemoglobin F and cells with precipitated haemoglobin H
also settle to the bottom of the centrifuged column.
Concentration techniques are of value in the study of leucocyte
biochemistry and physiology and in the detection of small numbers of
tumour cells that may circulate in the blood of a patient with a
malignancy. The rapid red cell sedimentation method of Skoog and
Beck (1956) may be used. Mix two volumes of 3 per cent dextran (mol.
wt. 228,000) in a long tube with one volume of anticoagulated venous
blood and allow to stand at room temperature for at least 15 minutes.
Approximately 99 per cent of the red cells sediment rapidly because of
marked rouleaux formation; this sedimentation may be hastened by
slight tilting of the tube from the vertical. Transfer the supernatant
dextran-plasma mixture (contains 75 per cent - 100 per cent of the
leucocytes, approximately 1 per cent of the red cells and most of the
tumour cells if present in the blood sample) to a plastic or siliconized
tube and centrifuge at 600 - 1,000 rev/min to sediment the cells. Wash
the cell button after discarding the dextran-plasma and resuspend the
cells in an appropriate quantity of suspending fluid. An advantage of
this method is that it can be carried out at 0 - 4°C. Better separation of
tumour cells may be effected with Seal's (1959) differential density
separation method as modified by Fleming and Stewart (1967). Overlay
silicone fluid (sp. gr. 1.070) in a siliconized tube with a mixture of
polyvinylpyrrolidone (PVP) and blood; centrifuge at 700 g for 15
minutes. The red cells and polymorphs sediment to the bottom of the
tube, while the lymphocytes and tumour cells form a grey layer at the
silicone-supernatant interface. Remove this layer and wash the cells
with PVP. After fixation collect the cells on a Millipore filter and stain.
FIXATION OF BLOOD FILMS
Fixation is the chemical treatment applied to tissues and cellular smears
for the purpose of preserving cell structure with the minimum of
distortion and alteration of composition, and protection of cells from
5
THE PERIPHERAL BLOOD FILM
disruption during subsequent staining with aqueous dye solutions.
Fixation is effected by reagents that interrupt cell metabolism by
precipitating protein and other cellular compounds. Fixative reagents
should effectively inhibit lysosomal enzymes that induce autocatalytic
degeneration of cells separated from the body but they should produce
only minimal or no inhibition of other enzyme systems.
Methanol, ethanol, acetone and 10 per cent alcoholic solution of
formaldehyde are commonly used fixatives for haematological staining.
Better fixation and less inhibition of enzymes is obtained at 0 - 4°C with
these reagents. Fixation prior to carrying out the staining reaction may
not be necessary in all procedures (see Romanovsky staining in
Appendix A). If there is likely to be a delay in staining blood films,
they should be immersed in the fixative recommended for the
technique for up to 15 minutes and then stored in the dark at 0 - 4°C.
Prolonged fixation must be avoided as the reagents affect subsequent
staining and induce some inhibition of intracellular enzymes.
ROUTINE STAINING OF BLOOD FILMS
Romanovsky staining
Romanovsky dyes employed for the routine staining of blood films are
Jenner's stain, May-Griinwald's stain, Giemsa's stain, Irishman's stain
and Wright's stain. They are mixtures of méthylène blue (a basic dye),
which may or may not be polychromed (that is, ripened or oxidized),
and eosin (an acidic dye). Méthylène blue is polychromed by allowing
the dye solution to age by standing for a number of weeks at room
temperature; this process may be hastened by boiling the solution in
the presence of an alkali such as sodium bicarbonate. Poly chroming of
méthylène blue produces coloured compounds known as 'azures'.
During the staining process, the basic dyes in the Romanovsky stain
solution react with acidic structures in the cells, staining them a blue,
purple or violet colour; these structures are said to be basophilic. The
eosin reacts with basic cellular structures; these stain red or orange in
colour and are said to be acidophilic or eosinophilic.
Stock methanolic solutions of powdered Romanovsky dyes are
readily prepared in the laboratory or may be purchased from
commercial sources. This stock solution is added first to the air-dried
film and subsequently diluted with buffered water. Preliminary fixation
is not necessary because during the alcoholic phase of the staining
process, fixation takes place with no significant staining of cells.
Staining occurs during the aqueous phase when dilution of the alcoholic
stock solution with water causes dye precipitation; the greater the
dilution and the longer the staining time, the better the results. Control
6
PREPARATION AND STAINING OF BLOOD FILMS
of the pH of the staining reaction is important for the development of
the full range of colours. Buffered deionized or distilled water at the
appropriate pH level for the Romanovsky stain must be employed as
the diluent and for the final wash of the film. The méthylène blue
component will be accentuated if the pH is too alkaline for the
particular stain(s) and the eosin component if the pH is too acid.
Nuclear chromatin stains various shades of purple; the nucleus of the
malarial parasite, however, is red in colour. Mien present, nucleoli
appear as pale staining or pale blue areas within the nucleus. The
cytoplasm varies from pale blue to deep blue, the degrees of basophilia
depending on the quantity of ribonucleic acid (RNA); plasma cells and
the more immature haemopoietic cells appear deeply basophilic because
of their increased amount of RNA. Cytoplasmic granules may be red
(azurophilic), orange (eosinophilic), pink (neutrophilic) or blue to
purple (basophilic) in colour. Erythrocytes stain reddish-pink to orange
in colour, depending on the pH of the staining reaction. Reticulocytes
and the cytoplasm of some nucleated red cells appear grey-blue to pale
grey, the colour depending on the proportions of eosinophilic-staining
haemoglobin and basophilic-staining RNA.
Stains and staining techniques vary according to the preference of
the haematologist or pathologist. Dilute Giemsa's stain is now
commonly used in conjunction with Jenner's or May-Griinwald's stain
(Pappenheim's panoptic method) because it considerably improves the
poor nuclear detail, a drawback of the latter stains. Leishman's and
Wright's stain are usually employed by themselves; they differentially
stain the nucleus, cytoplasm and granules. The staining qualities of
Wright's stain are enhanced by including Giemsa's dye in the stock
solution. In this author's experience Jenner-Giemsa's staining has
produced the best variation and gradation of colours and differentiation
of cellular constituents. Blood films may be stained on a staining rack
or by an automatic staining machine. Rack techniques are described in
Appendix A; they may be easily modified for staining in jars. Because
of variation in reagents from different commercial sources, it is
important to experiment with immersion times to produce a
well-stained blood film. If it becomes necessary to decolorize a
Romanovsky-stained blood film, immerse the slide in methanol.
CYTOCHEMICAL STAINING OF 'FIXED' BLOOD FILMS
The principle of cytochemical staining of fixed blood films is to
incubate the film, after fixation in the appropriate reagent, in a
chemical solution which reacts with the intracellular constituent to
produce either a coloured precipitate or a reaction product that may be
7
THE PERIPHERAL BLOOD FILM
altered by further treatment to form an insoluble coloured compound.
Techniques of diagnostic and/or prognostic value in haemopoietic and
other disorders are listed in Table 2.1.
TABLE 2.1
Cytochemical Staining of Fixed Films
Deoxyribonucleic acid (DNA)
Glycogen
Ferric iron (water insoluble)
Haemoglobin F-containing red cells
Peroxidase enzyme
Esterase enzymes
Chloroacetate esterase
Naphthyl acetate esterase
Bromoindoxyl acetate esterase
Alkaline phosphatase
Acid phosphatase
— Feulgen reaction
- Periodic acid » Schiff reaction
- Prussian blue reaction
- Acid elution reaction
- Peroxidase reaction
— Azo-dye coupling reactions
Feulgen reaction
Deoxyribonucleic acid (DNA) is present in chromosomes and
nuclear chromatin but not in the nucleolus. This is demonstrated by the
Feulgen reaction. Warm acid hydrolysis exposes aldehyde groups of
deoxyribose by breaking up the purine-deoxyribose bond; the
aldehydes react with colourless Schiffs reagent (leucobasic fuchsin) to
form a magenta-coloured substance at the reaction sites. The Feulgen
reaction is not often carried out in routine clinical laboratories.
However, by sharply defining nucleoli which do not stain, the reaction
is of value in differentiating micromyeloblasts from lymphocytes. The
reaction may be used for the staining of chromosomes in chromosome
preparations, but simpler techniques are available for this purpose.
Periodic acid - Schiff (PAS) reaction
Glycogen that is present in the cytoplasm of cells is demonstrated by
the periodic acid - Schiff (PAS) reaction. Periodic acid does not
hydrolyse nucleic acids but oxidizes 1:2 glycol groups (CHOH-CHOH)
to produce aldehydes and these react with colourless Schiff reagent to
form a magenta-coloured substance which precipitates either diffusely
or in granular form at the reaction sites. A control film previously
exposed to diastase, a glycogen-destroying enzyme, demonstrates that
glycogen is the substance giving the PAS reaction.
PAS reactivity varies in the different normal and abnormal
8
PREPARATION AND STAINING OF BLOOD FILMS
haemopoietic cells. It is stronger in neutrophil polymorphs than in (1)
immature cells of this series, and (2) cells of the lymphocytic and
monocytic series. The degree of PAS reactivity in individual
lymphocytes may be semi-quantitatively rated on a 0 - 3 scale (see
Appendix A); the PAS score is the sum of ratings of 100 consecutive
lymphocytes in the peripheral blood film. This score is higher than
normal in lymphocytic leukaemia, lymphosarcoma and in Hodgkin's
disease. The PAS reaction may be of diagnostic value in 'blast' or acute
leukaemia; the reaction is negative in myeloblasts and monoblasts and is
strongly positive in some lymphoblasts. No PAS-positive material is
normally demonstrable in mature and immature red cells, except in the
erythroblasts of neonatal cord blood. A positive PAS reaction in
erythroblasts may be seen in the disorders listed in Table 2.2.
TABLE 2.2
Disorders with PAS-positive Erythroblasts
Strong reaction
Di Guglielmo's syndrome
Thalassaemia syndrome
Moderate to weak reaction
Sideroblastic anaemia
Iron deficiency anaemia
Haemolytic anaemia
Myelofibrosis
(some
(some
(some
(some
cases)
cases)
cases)
cases)
Prussian blue reaction
Water-insoluble ferric iron may be present as aggregates
(haemosiderin) in histiocytes of the bone marrow, liver and spleen, and
as granules in immature and mature red cells (sideroblasts and
siderocytes respectively). Perls' (1867) Prussian blue reaction will
demonstrate water-insoluble ferric iron but not water-soluble ferric iron
(ferritin). The cellular ferric iron combines with potassium ferrocyanide
in a mixture of this reagent with hydrochloric acid, to form the
insoluble Prussian blue precipitate of ferro-ferricyanide. The reaction
may be carried out at room temperature; Hutchison (1953), however,
has stressed the importance of using warm reagents (56°C) to detect
low concentrations of iron in the cells. The Prussian blue reaction is of
value in the diagnosis of anaemia of chronic disorders, sideroblastic
anaemia, iron deficiency and of haemochromatosis.
9
THE PERIPHERAL BLOOD FILM
Acid elution reaction
Haemoglobin F is the normal haemoglobin of the foetus. Its
synthesis normally commences to decline as that of haemoglobin A
increases; postnatally, synthesis reaches a minimum at the age of 2
years and usually continues at this reduced rate throughout life. After
the age of 2 years less than 2 per cent of blood haemoglobin is foetal
haemoglobin. However, elevated levels of Hb-F are found in some
congenital disorders (Table 2.3) because of arrest of the normal decline
in synthesis. Levels greater than 2 per cent may also occur in certain
conditions (Table 2.3) because of re-appearance of increased Hb-F
synthesis.
TABLE 2.3
Postnatal Elevation of Haemoglobin F
Delayed disappearance of Hb-F (arrest of synthetic decline)
Congenital disorders of haemoglobin synthesis
Hereditary persistence of foetal haemoglobin (HPFH)
Beta-thalassaemia syndrome
Sickle cell anaemia
Chromosomal aberrations
D-Trisomy syndrome
Reappearance of Hb-F (renewed synthesis)
Children
Fanconi syndrome
Myelocytic leukaemia (Ph ' chromosome negative)
Lymphoblastic leukaemia
Adults
Di Guglielmo's syndrome
Paroxysmal nocturnal haemoglobinuria
Molar pregnancy
Acquired aplastic anaemia
(some cases)
Agnogenic myeloid metaplasia (some cases)
The physicochemical properties of Hb-F differ from those of Hb-A.
Foetal haemoglobin is more resistant to alkali denaturation and less
soluble in acidic solution than adult haemoglobin. The former property
is utilized for determining the concentration of Hb-F in the blood and
the latter for the cytochemical detection of red cells containing Hb-F.
The acid (pH 3.3) elution technique of Kleihauer, Braun and Betke
(1957) or the technique (pH 1.1) of Nierhaus and Betke (1968) may be
10
PREPARATION AND STAINING OF BLOOD FILMS
used to diagnose hereditary persistence of foetal haemoglobin (HPFH).
In this disorder all the red cells contain Hb-F and the treated film
reveals only deeply stained red cells. Blood films from subjects with the
other disorders listed in Table 2.3 show a patchy distribution of deeply
stained Hb-F-containing red cells among Hb-A-eluted ghost cells. The
acid elution reaction is also of value for detecting foetal cells in the
maternal circulation and for calculating the volume of foetomaternal
transplacental haemorrhage.
Peroxidase reaction
Peroxidase is an enzyme that catalyses the transfer of oxygen from
hydrogen peroxide to an acceptor substance. The reaction is carried out
in vitro by incubating the blood film in a mixture of hydrogen peroxide
and alcoholic solution of benzidine; intracellular enzyme activity is
detected by the deposition of brown oxidized benzidine granules.
Inclusion of sodium nitroprusside in the reaction mixture (Washburn,
1928) results in the deposition of blue-black granules which are more
clear cut and striking than the brown-coloured granules of the basic
method. The nature of the chemical reaction with nitroprusside is
uncertain; the reagent may stabilize the initial and transient blue
colouration of the deposit formed in the basic method. Kaplow's
(1965) method utilizes benzidine hydrochloride and zinc sulphate.
0-tolidine may be used as a substitute for benzidine (Quaglino and
Flemans, 1958; Jacobs, 1958) but not for benzidine hydrochloride
(Kaplow, 1965).
Peroxidase is important for the bactericidal activity of neutrophils.
The in vitro reaction is strongly positive in the granulocytic series of
cells, except basophils and myeloblasts, is weak or absent in monocytes,
and no activity is demonstrable in cells of the lymphocytic or plasma
cell series. Diminished activity in neutrophil granulocytes may be
observed in infections, in some cases of Hodgkin's disease and in
leukaemic granulocytes.
Esterase enzyme reactions
There are various types of esterase enzymes but cytochemically only
the acetate esterases and the phosphatases appear to have useful
applications. The former enzymes hydrolyse acetate esters and the
latter phosphate esters of naphthol compounds. Simultaneous coupling
of the liberated naphthol with a capture reagent, such as a diazonium
salt of various dyes, results in the formation of a chromogenic product
which, if insoluble in the reaction mixture, is precipitated in
microcrystalline form at the intracellular sites of enzyme activity.
11
THE PERIPHERAL BLOOD FILM
Acetate esterase
Acetate esterases have cell and substrate specificities. Yam, Li and
Crosby (1971) showed that with their techniques acetate esterases are
of value as marker enzymes for distinguishing mono cytes and
neutrophilic granulocytes. According to these investigators the activities
of 'non-specific' esterase (alpha naphthyl acetate as substrate) and
chloroacetate esterase (naphthol AS-D chloroacetate as substrate) at pH
7.4 - 7.6 are respectively very strong in monocytes and the neutrophuic
series of cells (Table 2.4). Thus cytochemical demonstration of these
TABLE 2.4
Acetate Esterase Activity in Haemopoietic Cells *
Neutrophil series of
cells, including
many myeloblasts
Eosinophils
Basophils
Tissue mast cells
Lymphatic cells
Monocytes, macrophages
and histiocytes
Plasma cells
Megakaryocytes
Erythroblasts
A Ipha-naph thy I
acetate
esterase
Naph th ol
A S-D ch loroac eta te
esterase
-
+++
(Absent in agranular
cells)
?
+++
+++
- or +
- to ++
+++
-
- ΟΓ +
+++ in malignant
erythroblasts
No activity, - ; weak activity, + ; moderate activity, ++ ; strong and granular
activity, +++
* After Yam, Li and Crosby, 1971
esterases, either individually or as a combined reaction on the same
smear, is useful in the diagnosis of those leukaemias in which the
neutrophilic leucocytes and monocytes are indistinguishable.
Szmigielski, Litwin and Zupanska (1965) reported on the value of the
acid acetate esterase method (5-bromoindoxyl acetate as substrate) of
Pearson and Defendi (1957) for differentiating normal and reactive
plasma cells from those occurring in myeloma. Enzyme hydrolysis at
pH 5.0 of colourless 5-bromoindoxyl acetate liberates an intermediate
unstable compound, 5-bromoindoxyl which readily oxidizes to 5.5'
bromoindigo; this reaction product precipitates as deep blue (or indigo)
12
PREPARATION AND STAINING OF BLOOD FILMS
fine crystals at the sites of esterase activity in plasma cells. These
investigators found that 45 - 55 per cent of normal and reactive plasma
cells showed slight to moderate activity but 70 - 80 per cent of
neoplastic plasma cells showed a marked increase in acid esterase
activity with the formation of big dye aggregates in some cells.
Phosphatases
Phosphatases are classified as alkaline (pH 9.5 - 10) or acid (pH 5.0)
phosphatases according to the pH optima of their reactivity. Alkaline
phosphatases may be detected with alpha-naphthyl phosphate and
brentamine fast garnet (Hayhoe and Quaglino, 1958) or withnaphthol
AS-BI phosphate and fast red violet salt (Kaplow, 1963). However,
these methods are not without certain disadvantages. Brentamine fast
garnet is unstable in solution and some batches react poorly or not at
all. Kaplow's method cannot be used on films made from blood
anticoagulated with EDTA because of the inhibitory effect of EDTA on
enzyme reactivity with the substrate. Alkaline phosphatase activity can
be demonstrated only in segmented neutrophil polymorphs and in
histiocytes; malignant neutrophils and all other haemopoietic cells give
negative reactions. Intracellular enzyme activity in the segmented
neutrophils is semi-quantitatively rated on a 0 - 4 scale. The leucocyte
alkaline phosphatase (LAP) score is the sum of the ratings of 100
consecutive segmented neutrophils in the peripheral blood film and
normally ranges from 15-100. LAP activity in various diseases and
disorders is listed in Table 2.5. The low levels in myelocytic leukaemia
may be helpful in differentiating this condition from a leukaemoid
reaction. Apart from this, LAP scores appear of limited value.
TABLE 2.5
Leucocyte Alkaline Phosphatase (LAP)
Normal score
Secondary polycythaemia
Leucocytosis of sickle cell anaemia
Myeloblastic leukaemia (some cases)
Lymphocytic leukaemia
Lymphosarcoma
Myeloma
Hodgkin's disease (inactive)
Diminished score
Myeloid leukaemia — acute and chronic
Hereditary hypophosphataemia
Paroxysmal nocturnal haemoglobinuria
Sarcoidosis
cont.
13
THE PERIPHERAL BLOOD FILM
Table 2.5 cont.
Sometimes diminished
Aplastic anaemia
Myelofibrosis (some cases)
Collagen disease
Idiopathic thrombocytopenic purpura
Infectious mononucleosis
Elevated Score
Haemopoietic disorders
Myeloproliferative disorders (excluding myelocytic leukaemia)
Lymphoblastic leukaemia
Hodgkin's disease (active)
Aplastic anaemia
Non-haemopoietic disorders
After surgery
After haemorrhage
Leucocytosis and leukaemoid reactions
During pyogenic infections
Myocardial infarction
Acute gout
Diabetic acidosis
Mongolism
Women on contraceptive pill
During pregnancy
Newborn infants
Steroid and progesterone therapy
Acid phosphatase activity in haemopoietic cells varies according to
the technique employed to demonstrate it. Using naphthol AS-BI
phosphate and fast garnet, Li and his colleagues (Li, Yam and Lam,
1970; Yam, Li and Lam, 1971; Yam, Li and Finkel, 1972) observed
strong activity in plasma cells, monocytes, some atypical mononuclear
cells of infectious mononucleosis and in the malignant 'hairy' cell of
leukaemic reticulo-endotheliosis; moderate to weak activity was seen in
neutrophils, eosinophils, lymphocytes and platelets. These investigators
found that L^ ^ tartaric acid inhibited enzyme activity in all cells except
the 'hairy' cells and suggested that the diagnosis of leukaemic
reticulo-endotheliosis may be made with certainty by the cytochemical
demonstration of tartrate-resistant acid phosphatase in the atypical
mononuclear cells characteristic of this disorder.
SUPRAVITAL STAINING
Supravital staining may be defined as the dye or chemical staining of
'unfixed', metabolically active cells prior to their being spread on a glass
14
PREPARATION AND STAINING OF BLOOD FILMS
slide or coverslip. It is useful for the study of fragile cells that readily
disrupt when being spread on a slide, cellular constituents that may be
altered or inhibited by fixatives, metabolic activity within cells, and of
leucocytes by phase-contrast microscopy. The techniques consist of
preliminary incubation of mixtures of cell suspensions and aqueous
dyes or chemical solutions at room temperature or at 37°C. With the
exception of phase-contrast microscopy techniques, air-dried films are
then prepared in the usual manner. Further treatment may include
fixation and counterstaining for ideal visualization of the end result.
Techniques of diagnostic and/or prognostic value in haemopoietic and
other disorders are listed in Table 2.6.
TABLE 2.6
Supravital Staining
Residual RNA in reticulocytes — Brilliant cresyl blue or new méthylène
blue staining
Heinz bodies
— Methyl violet staining
Brilliant/green/neutral red staining
Precipitated haemoglobin H
— Brilliant cresyl blue staining
Haemoglobin S
— High molarity buffer elution reaction
The sickling reaction
— Nitroblue tetrazolium (NBT)
PMN bactericidal function
reduction reaction
Reticulocyte staining
The reticulocyte or juvenile non-nucleated red cell contains residual
RNA. Whereas this RNA is uniformly precipitated by alcoholic
fixatives, the action of basic dyes on the I*NA of the unfixed cell causes
it to precipitate either as a coloured reticulum of fine filaments or as
granules, depending on the maturity of the cell. Brilliant cresyl blue and
new méthylène blue produce a deep blue precipitate which
differentiates the granular reticulocyte from red cells containing Heinz
bodies and precipitated haemoglobin H (pale blue precipitate) and from
red cells with Pappenheimer bodies (blue-black precipitate). After
splenectomy, particularly in cases of haemolytic anaemia, there may be
difficulty in supravitally distinguishing reticulocytes from siderocytes
(red cells with Pappenheimer bodies). A double staining technique is
useful. The Prussian blue reaction is carried out on the supravitally
stained film and the red cells count er stained with a dilute solution of
safranin or eosin. The precipitate of the reticulocyte is deep blue and
15
THE PERIPHERAL BLOOD FILM
that of the siderocyte is green. Reticulocyte staining and estimation of
their absolute number is of value in the diagnosis of occult haemorrhage
and haemolysis. This reticulocyte count is useful to assess the response
in anaemic subjects treated with specific haematinics and, when
corrected for reticulocyte maturation time, to measure erythropoietic
activity.
Staining for Heinz bodies
Heinz bodies are aggregates of precipitated complexes of denatured
haemoglobin and oxidized glutathione (cf. Chapter 4). Their occurrence
is commonly associated with drug-induced haemolytic anaemia and
with haemoglobinopathies due to 'unstable' haemoglobins. The
structures are not visible in Romanovsky-stained blood films but may
be seen as colourless refractile bodies in unfixed air-dried films when
the microscope condenser is racked down, and as pale blue inclusions in
reticulocyte preparations. They can be demonstrated after supravital
staining with methyl violet, when they appear as one or more coloured
masses up to 2 μπι in diameter. The residual RNA of reticulocytes stainsa
very pale blue colour and Pappenheimer bodies almost black with a
bluish tinge. Schwab and Lewis (1969) recommend supravital staining
with brilliant green because of the greater specificity of the dye for
Heinz bodies and, as the remainder of the cell is only lightly stained,
the inclusions may be better visualized by counterstaining with a
complementary colour. The residual RNA of reticulocytes stains a very
pale green colour (personal observation).
Supravital staining for Heinz bodies is commonly carried out on
fresh blood. However, the detection of in vivo produced inclusions is
difficult in subjects with a normally functioning spleen. The test should
therefore be repeated on an aliquot of blood that has been incubated,
at 37°C for 18 hours under sterile conditions, to allow the development
of methaemoglobin within the red cells. Normally only a little
methaemoglobin (2 - 3 per cent) forms and no Heinz bodies are detectable. In unstable haemoglobinopathy many Heinz bodies are produced
due to excessive methaemoglobin formation revealed macroscopically by
brownish discoloration of the incubated blood sample.
Staining for haemoglobin H inclusions
Haemoglobin H is a beta chain tetramer that results from diminished
synthesis of alpha chains and commonly occurs as an hereditary
abnormality; it has also been reported to occur as an acquired
abnormality in Di Guglielmo's syndrome (Hamilton et al, 1971 ). Because
of the lack of alpha chains the haemoglobin molecule is unstable,
susceptible to precipitation and readily denatured. While Hb-H may be
16
PREPARATION AND STAINING OF BLOOD FILMS
seen as a fine blue stipple in Romanovsky stained blood films, it is
better demonstrated supravitally with brilliant cresyl blue which causes
the abnormal haemoglobin to precipitate as a pale blue granular deposit
within the red cells. The granules are more numerous and less intensely
coloured than those seen in reticulocytes; the appearance of the cell has
been likened to that of a golf-ball.
Tests for haemoglobin S
Haemoglobin S is a genetically determined abnormal haemoglobin.
Its presence in red cells may be detected by the high molarity buffer
elution reaction (Yakulis and Heller, 1964) and by the sickling reaction
(Daland and Castle, 1948; Itano and Pauling, 1949). The former
reaction is based on the lowered solubility of reduced Hb-S, when
compared with Hb-A, in high molarity buffered solutions. The blood
film (unfixed) is immersed in a dithionite-phosphate buffer solution
(2.48M, pH 7.26) and then examined microscopicallly. Hb-A is eluted
from the red cells which become decolorized and appear as ghosts;
because reduced Hb-S is less soluble in the buffer solution, it is not
eluted and the cells containing Hb-S remain pigmented or appear red in
colour if the film has been counterstained with eosin.
The sickling reaction is based on the tendency of Hb-S to form
reversible tactoid crystals in the deoxygenated state; this intracellular
crystallization causes the red cells to become deformed (the sickling
mechanism is discussed in Chapter 4). In vitro deoxygenation is achieved
by incubating a sealed mixture of whole blood and a solution of a
reducing agent, such as sodium metabisulphite (Daland and Castle,
1948) or sodium dithionite (Itano and Pauling, 1949). Erythrocytes of
subjects with sickle cell anaemia (Hb-S/S) transform into thin elongated
cells with pointed ends and assume sickle, V or L forms; the red cells of
those with the sickle cell trait (Hb-A/S) develop a holly-leaf appearance.
The rate of sickling depends on the Hb-S concentration within the red
cells; it is more rapid in sickle cell anaemia than in sickle cell trait. The
reaction is inhibited if the Hb-S is associated with high concentrations
of Hb-F in the same cell; this occurs in subjects heterozygous for the S
gene and the 'high' F gene. Sickled cells revert to the discoid form on
reoxygenation of the blood; consequently a special technique (Stenton,
1959) is necessary for the preparation of permanent smears. These
cytochemical tests are of value only as a rapid screen for Hb-S; a
positive result should be confirmed by an electrophoretic technique.
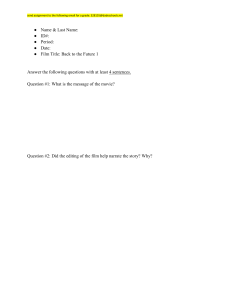
The nitroblue tetrazolium (NBT) reduction test
Polymorphonuclear neutrophil (PMN) leucocytes are phagocytic
cells with potential mechanisms, such as the myeloperoxidase-iodide17
THE PERIPHERAL BLOOD FILM
hydrogen peroxide system described by Klebanoff (1968), for killing
ingested bacteria. Phagocytic activity is associated with degranulation
due to emptying of granular enzymes into the cytoplasmic phagosomes
containing the ingested bacteria, enhanced glucose oxidation, stimulation
of the hexose-monophosphate shunt pathway with the production of
carbon dioxide, higher concentration of nucleotides and increased
production of hydrogen peroxide by nucleotide oxidases {Figure I).
The bactericidal property of PMN can be demonstrated in vitro with
In vivo
Oxygen -
. Reduced nucleotide.
NADH -*-i
In vitro
■ Soluble yellow
tetrazolium
«~ NADPH
O
NAD
Hydrogen peroxide Iodide ■
NADP
-Nucleotide «
► Insoluble blueblack formazan
• Myeloperoxidasc
Bactericidal
action
Figure I. PMN bactericidal activity and NBT reduction test
a standardized culture of Staphylococcm aureus. It can also be assessed
with a tetrazolium-linked system, the dye functioning as an electron
acceptor from the oxidases of the co-enzymes reduced NAD and NADP
{Figure 2). Nitroblue tetrazolium (NBT), a water-soluble pale yellow
dye which on reduction precipitates as blue-black formazan deposits
within the cell cytoplasm, is commonly used in the various tests
(Baehner and Nathan, 1966; Windhorst, Holmes and Good, 1967;
Park, Fikrig and Smithwick, 1968; Bannatyne, Skowron and Weber,
1969; Gifford and Malawista, 1970). The techniques of Park and his
18
PREPARATION AND STAINING OF BLOOD FILMS
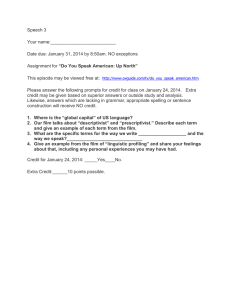
8000,
20
40
60
NBT positive PMN, per cent
Figure 2. Spontaneous reduction by PMN - categorization of patients
(Reproduced from Feiginei al, 1971 by courtesy of the Authors and the Editor
of Journal of Pediatrics.)
colleagues (1968) and of Gifford and Malawista (1970) are described in
Appendix A. Disorders with normal and abnormal numbers of
PMN reducing NBT are listed in Table 2.7.
TABLE 2.7
Nitroblue Tetrazolium (NBT) Reduction Test
Normal NBT score
Normal subjects, 2 - 6 5 years of age
Postpartum women
Effective antibacterial therapy
Viral infections
Neutrophilia of non-bacterial origin
Congenital heart disease
Surgical procedures
Organ transplant
Measles and rubella vaccination
Diminished NBT score
Chronic granulomatous disease of children
Job's syndrome
Myeloperoxidase deficiency
cont.
19
THE PERIPHERAL BLOOD FILM
Table 2.7 cont.
Lipochrome histiocytosis
G6PD deficiency of neutrophils
Agammaglobulinaemia
Mixed cryoglobulinaemia
Pneumococcal meningitis in sickle cell disease
Pulmonary tuberculosis
Drug therapy - chloramphenicol, corticosteroids, phenylbutazone
Elevated NBT score
Active bacterial infections including bacterial meningitis, bacterial
endocarditis, osteomyelitis, septic arthritis, peritonitis, empyema
Miliary tuberculosis and tuberculous meningitis
Pulmonary nocardiosis
Candida albicans septicaemia
Malaria (Andersen, 1971)
2 - 4 hours after Salmonella vaccination (TAB)
Multiple drug therapy
Chediak-Higashi-Steinbrinck syndrome
Newborn infants less than 2 months of age
The NBT reduction test is useful for detecting chronic
granulomatous disease and its variants in children. In these rare
inherited disorders, the subject's PMN exhibit defective bactericidal
activity for micro-organisms that are not effective hydrogen peroxide
producers. Consequently the number of formazan-containing cells are
reduced when compared with the normal. The test is valuable as a
diagnostic aid in differentiating patients with a neutrophilia (Park,
Fikrig andSmithwick, 1968;Park, 1971) and with febrile illnesses (Feigin
et al., 1971). It thus helps to support a diagnosis of bacterial infection,
to distinguish bacterial from non-bacterial diseases and to assess the
adequacy of antibiotic therapy. According to Feigin and his colleagues
(1971) plotting of the percentage and absolute number of NBT-positive
cells on their nomogram (Figure 2) permits categorization of the
patient into one of four groups: (A) normal; (B) viral infection,
partially treated bacterial infection, and non-infectious febrile illness;
(C) untreated bacterial infection; and (D) ineffectively treated bacterial
infection.
20
3
Normal Peripheral Blood
Cells
CELL TYPES
Normal peripheral blood cells are the red cell (erythrocyte),
polymorphonuclear neutrophil (PMN) granulocyte, polymorphonuclear
eosinophil granulocyte, polymorphonuclear basophil granulocyte,
monocyte, lymphocyte and platelet (thrombocyte). Of these cells only
the monocyte and the lymphocyte is not a 'mature' or 'end' cell. The
monocyte is at a transition stage, completing its maturation into a
macrophage in the tissues. An indeterminate number of blood
lymphocytes are in a temporary 'inactive phase' of their life cycle
(Yoffey and Courtice, 1970); on exposure to antigenic stimulation
these cells undergo blastogenic transformation and clonal proliferation
with the production of 'effector' end cells. For convenience plasma
cells, which are not strictly peripheral blood cells, are included in this
chapter. They are the mature end cells of the B-lymphocyte series and
are located in the haemopoietic organs. Occasionally, however, they
may be observed in a 'normal' peripheral blood film.
THE RED CELL OR ERYTHROCYTE
Morphology (see Plate 1)
The normal red blood cell (RBC) is anucleate, reddish-pink to orange in
colour and circular or slightly oval in shape with a smooth outline. A
small central area of pallor is commonly seen because of the cell's
biconcave surfaces. The normal RBC in the blood film is called a
normochromic normocyte; the lack of a nucleus results from its
extrusion at an earlier stage of development of the cell in the bone
marrow. The staining characteristic of the cell is due to its content of
haemoglobin, its size and its shape. The red cell has a mean corpuscular
diameter (MCD) of approximately 7.2 Mm and a mean corpuscular average
thickness (MC AT) of approximately 2.1 μηι. The 'absolute'
values, that is the mean corpuscular volume (MCV), the mean
corpuscular haemoglobin (MCH) and the mean corpuscular haemo21
THE PERIPHERAL BLOOD FILM
globin concentration (MCHC) are listed in Table 10.3; they vary
according to the age and sex of the subject. The size of the RBC
appears to be governed by the rate of haemoglobin synthesis in the early
precursor cells; this rate of synthesis has been proposed to regulate the
number of cellular reduction divisions by cutting off DNA synthesis
when a critical cytoplasmic haemoglobin concentration has been
attained. (Stohlman, 1967; Stohlman et al, 1968). The circulating red
cell has a discoid shape with biconcave surfaces. The shape depends on
the fluidity of cell contents, the adenosine triphosphate (ATP)
concentration within the cell, the actin-like protein ('spectrin') and
lipid content of the cell membrane, and a surface area in excess of the
minimal area required to enclose the volume of the cell contents. The
shape and fluid content render the cell highly deformable thus enabling
it to traverse through the microcirculation.
Haemoglobin
The haemoglobin molecule consists of a colourless tetrameric protein
(90 per cent of the molecule) known as globin and a prosthetic group
termed haem. Globin contains two pairs of dissimilar polypeptide
chains - two identical alpha (a) chains and two identical non-alpha chains
that may be epsilon (e), gamma (7), delta (δ) or beta (β) chains. The
structure and nomenclature of normally occuring haemoglobins are
indicated in Table 3.1; the percentages of these haemoglobins in a
TABLE 3.1
Structure and Nomenclature of Normally Occurring Haemoglobins
Hb-Gower 2
Hb-F
Hb-A 2
Hb-A
a2e2
a2y2
α2δ2
α 2 02
Embryonic haemoglobin
Foetal haemoglobin
Adult haemoglobins
)
TABLE 3.2
Haemoglobins in Neonatal Infants and Subjects over 2 Years
Neonatal infants
Percentage of total haemoglobin
Subjects over 2 years
Percentage of total haemoglobin
Hb-Gower 2
Hb-F
Hb-A 2
Hb-A
Hb-Gower 2
Hb-F
Hb-A 2
Hb-A
22
NÜ
45-90
Trace
10-55
Nu
<2
1-3
95-98
NORMAL PERIPHERAL BLOOD CELLS
neonatal infant and in subjects over the age of 2 years is given in
Table 3.2. High molarity buffer solutions can elute these haemoglobins
from red cells in air-dried films; an acid solution, however, has no effect
on haemoglobin F.
Many 'abnormal' haemoglobins have been detected; they have
physicochemical properties that are different from the normal types.
These variants result from gene mutations producing substitutions,
additions or deletions of peptide residues, particularly in the beta and
alpha chains. The majority of the abnormal haemoglobins produce no
physiological aberrations and are of biochemical interest only. Some,
however, cause certain signs and symptoms and may be classified as
indicated in Table 3.3. Thalassaemia is a special type of
TABLE 3.3
Haemoglobinopathy
A. Haemolytic anaemia
Defect in the rate of chain synthesis
Thalassaemias
Thalassaemic syndromes
Peptide substitutions
Crystallizing haemoglobins - Hb-S and Hb-C
Other haemoglobins — Hb-D and Hb-E
Unstable haemoglobins (Table 4.9)
M haemoglobins
Polycythaemic haemoglobins
B. Cyanosis
M haemoglobins
Unstable haemoglobins (Table 4.9)
Polycythaemic haemoglobins — increased oxygen affinity
C. Abnormal oxygen transport
Increased oxygen affinity
Polycythaemic haemoglobins
Unstable haemoglobins (Table 4.9)
Decreased oxygen transport
Alpha chain variants of M haemoglobins
Beta chain variant of M haemoglobins — Hb-M Milwaukee
Haemoglobins C, D and E
Hb-Kansas and Hb-Seattle
haemoglobinopathy; it is a spectrum of diseases, no abnormal
haemoglobin is present and it is due to diminished synthesis of normal
globin chains.
Haem is iron-pro toporphyrin 9, the pro to porphyrin being a
tetrapyrrolic pigment which gives haemoglobin its red colour. Each
23
THE PERIPHERAL BLOOD FILM
haem molecule contains one atom of hexa-covalent iron in the ferrous
(Fe ++ ) form. Four valencies of the iron are joined to the pyrrolic rings
of protoporphyrin, one to the globin chain and one that combines
reversibly with oxygen. Each of the globin chains in the haemoglobin
molecule carries a haem molecule that lies in a pocket formed by the
folding of the chain. The iron atoms of haem have the property of
reversible oxygénation, that is, they have the ability to take up and give
up oxygen without a change in valency. Since the iron remains in the
ferrous state the reaction is termed oxygénation and not oxidation.
Other constituents
In addition to haemoglobin, red cells contain other organic and
inorganic compounds. The cells are metabolically active and many
enzymes are present in the cell. However, only those concerned with or
linked to glucose metabolism are important for the normal functioning
of the cell. Erythrocytes contain no free water-insoluble iron nor any
residual RNA material; the Prussian blue reaction is negative and no
blue granular deposit is demonstrable with the supravital brilliant cresyl
blue or new méthylène blue reactions. While a little glycogen may be
shown by biochemical means, the PAS reaction is usually negative.
Function
The principal function of red cells is to transport oxygen from the
lungs to the tissues and carbon dioxide from the tissues to the lungs.
Effective tissue oxygénation depends not only on the quantity and
quality of haemoglobin but also on 2,3 diphosphoglycerate (2,3 DPG),
an intermediate product of the Embden-Meyerhoff glycolytic pathway,
and on glutathione stability within the cell. Methaemoglobin (MetHb),
in which the ferrous iron (Fe ++ ) of haemoglobin has been oxidized to
the ferric (Fe + + + ) form, is unable to transport oxygen because it is
incapable of being oxygenated. If the MetHb concentration within the
red cells is greater than 2 per cent of the total haemoglobin, the subject
becomes cyanosed and the blood assumes a brown colour. Normally the
MetHb concentration is less than 2 per cent because the red cells have
an active enzyme system which reduces MetHb back to haemoglobin.
Life-span
Erythrocyte life-span is approximately 120 days; cell function
during this time is carried out entirely within the circulation. Viability
is dependent on carbohydrate metabolism, glutathione stability and
normal electrolyte concentration within the cell. These are crucial to
the integrity of haemoglobin and cell membrane and red cell
defor inability within the circulation.
24
NORMAL PERIPHERAL BLOOD CELLS
THE POLYMORPHONUCLEAR NEUTROPHIL
(PMN) GRANULOCYTE
Morphology (see Plate 1)
The neutrophil polymorph is a round cell, 10-12 Mm in diameter. The
nucleus is deep blue or purple in colour and segmented into 2, 3,4 or 5
lobes joined by 1, 2, 3 or 4 thin filaments of chromatin. The lobar
chromatin is coarse and arranged in clumps. The faintly basophilic
cytoplasm is abundant and packed with numerous fine pink granules
(the neutrophilic granules) which mask the cytoplasmic basophilia. The
number of nuclear lobes is generally accepted as an indicator of the
maturity of the neutrophil polymorph; the greater the number of lobes
the older the cell. However, Fliedner and his colleagues (1964) reported
no distinct difference in the maturation time of the various segmented
forms. Thus it appears that segmentation is determined by the number
of nuclear indentations that occur in the precursor cell and bears no
relationship to ageing of the cell.
Nuclear appendages
Nuclear appendages are seen in some PMN and may be classified as
drumsticks, sessile nodules, racquet forms, small clubs and rod or hook
tags. The drumstick (satellite body or hanging drop) is a pedunculated
mass of dense chromatin, 2 X 1.5 Mm in size, attached to a nuclear lobe by
a fine strand of variable length. The shape and size of this nodule is
constant; only one is seen in any cell. The sessile nodule is similar in
size and appearance to the drumstick but no stalk is evident and the
nodule is directly attached to the nuclear lobe by a broad base. Racquet
forms differ from drumsticks in showing a central pale area. Small clubs
are clumps of chromatin joined by a thin filament to a nuclear lobe, but
they are smaller than drumsticks. Rod or hook tags have no masses at
their free ends.
On rare occasions the drumstick is seen in an occasional PMN in a
blood film of a male patient; the significance of this finding is
uncertain. Drumsticks and sessile nodules are usually seen in blood
films of female subjects. The drumstick count varies from 1 to 16 per
cent of PMN. The appendage is generally accepted to be the female sex
chromatin and equivalent to the Barr body or nuclear sex chromatin
mass visualized, after special staining techniques, on the inner surface of
nuclear membranes of some somatic cells derived from females.
Drumsticks, however, have been shown to be unrelated to the Banbody (Ashley, 1957; Murthy and von Haam, 1958). Nevertheless, the
drumstick count is useful for determining an individual's sex.
25
THE PERIPHERAL BLOOD FILM
Granules
Pleomorphism of the neutrophilic granules has been demonstrated
by electron microscopy. Specific or secondary granules constitute
80 - 90 per cent and 10-20 per cent are primary granules that have lost
their azurophilic staining characteristics (cf. Myelopoiesis in Chapter 8).
A few 'tertiary' granules, similar to the granules found in other
leucocytes, have been described in PMN. The granules (or lysosomes)
are membrane-bound organelles, rich in hydrolytic enzymes. Primary
granules contain peroxidase, acid phosphatase and other enzymes;
secondary granules contain alkaline phosphatase and lysozyme (or
muramidase). Tertiary granules contain acid phosphatase.
Cytochemical reactions
PMN are Feulgen positive. The PAS reaction reveals tightly packed
magenta-coloured granules which do not obscure the nucleus; they are
produced by the glycogen in the cytoplasm. The peroxidase and
chloroacetate esterase reactions are positive (Table 3.4); these two
TABLE 3.4
Cytochemical Enzyme Activity in Leucocytes and Plasma Cells
Peroxidase
Neutrophils
+++
Eosinophils
Basophils
Monocytes
+++
+
Lymphocytes
Plasma Cells
—
-
Esterases
Naphthyl
Acetate
—
+++
Granular
—
- to ++
Phosphatases
Chloroacetate
+++
Granular
—
—
—
-
Alkaline
Acid
- to +++ + to ++
—
+ to ++
+++
—
-
+ to ++
+++
No activity, —; weak activity, +; moderate activity, ++; strong activity, +++
enzymes are used as markers for the neutrophilic series of cells.
Naphthyl acetate esterase activity is not demonstrable. Acid
phosphatase activity is weak to moderate. Alkaline phosphatase is
demonstrable in only some cells and the strength of the reaction is
variable in the different cells. The activity may be semi-quantitatively
rated on a 0 - 4 scale; the sum of the ratings of 100 consecutive PMN in
a peripheral blood film is referred to as the leucocyte alkaline
phosphatase (LAP) score, the normal range being 15 - 100. This LAP
score declines with age in both sexes and is higher in females from the
26
NORMAL PERIPHERAL BLOOD CELLS
second to the fifth decades than in the males (Ray and Pinkerton,
1969).
Neutrophil PMN pools
Neutrophil PMN are found predominantly in three pools in the
body. Of the granulocytes in the bone marrow 36 per cent are
segmented neutrophils. Of the total PMN in the blood 56 per cent
adhere to the walls of small blood vessels (the marginated granulocyte
pool or MGP), particularly in the lungs, and 44 per cent circulate in the
blood stream (the circulating granulocyte pool or CGP). There appears
to be no appreciable pool in extramedullary tissues. Release of PMN
from the bone marrow pool may be regulated by (1) the porosity of the
trilaminar barrier separating the cells from the vascular sinuses; (2) the
deformability of the cells; and (3) humoral factors which may act on
the cell itself, on the barrier, or on the delivery of the cells from the
sinuses to the general circulation (Lichtman, 1970). Release of mature
cells from the bone marrow pool appears to be related to their
utilization rate in the tissues and is possible because of the
deformability of the cells.
The half-life of the PMN in the circulation is 6 -12 hours. The cells
are transported to the site of their activity and those not destroyed
during antibacterial activity are excreted from the body in the
gastro-intestinal, respiratory and urinary tracts etc. Granulocytic
turnover in health is reflected by the serum lysozyme (muramidase)
concentration.
Functions — phagocytosis and bacteriolysis
The PMN is also referred to as a microphage or short-lived
phagocyte. Its function, which is principally carried out extravascularly
in the tissues, is to phagocytose and digest micro-organisms (except
viruses) and tissue debris at sites of inflammation. Activity is dependent
on enzymes concerned with or linked to glucose metabolism within the
cell and on a number of potential bactericidal mechanisms. The latter
include (1) cationic proteins which affect bacterial viability by
attaching themselves to the membranes (Zeya and Spitznagel, 1968);
(2) lysozyme (muramidase, mucopolysaccharidase, mucopeptide
N-acetyl muramyl hydrolase) which digests the cell wall of many
pathogenic bacteria and non-pathogenic organisms such zsMicrococcus
lysodeikticus\ and (3) the myeloperoxidase-halide (particularly
iodide)-hydrogen peroxide system described by Klebanoff (1968).
Generation of hydrogen peroxide within the cell is thus of considerable
importance for the antibacterial function of the PMN, particularly for
those organisms that are themselves not effective hydrogen peroxide
27
THE PERIPHERAL BLOOD FILM
producers. PMN contain oxidases capable of oxidizing the reduced
forms of nicotinamide adenine dinucleotide (NADH) and nicotinamide
adenine dinucleotide phosphate (NADPH) in the presence of oxygen to
form hydrogen peroxide (see Figure 1). The roles of NADH oxidase
and NADPH oxidase in the generation of hydrogen peroxide is
controversial (Holmes, Page and Good, 1967: Karnovsky et al, 1970).
Phagocytic activity is accompanied by increased glycolysis, oxygen
consumption, hydrogen peroxide generation within the cell and
degranulation with release of enzymes into the phagosome (phagocytic
vacuole). As resynthesis of PMN granules does not take place, cell death
eventually follows.
THE POLYMORPHONUCLEAR EOSINOPHIL GRANULOCYTE
Morphology
The cell is commonly called the eosinophil and is 10 - 12 μηι in diameter. The nucleus is a pale purple colour and segmented into 2 or 3 lobes
joined by 1 or 2 thin filaments of chromatin. The faintly basophilic
cytoplasm is abundant and packed with large round orange-red granules
that may be so numerous as to obscure the nucleus. The colour reaction
of the granules is due to their content of strongly basophilic protein
rich in arginine.
Nuclear appendages: granules
Some eosinophils contain drumsticks similar in appearance to those
in PMN; their presence may not be readily noted because of the
eosinophilic granules. Unlike the granules of the PMN, those of the
eosinophil are not polymorphic, and only one type has been
demonstrated in the mature cell by electron microscopy. Peroxidase
and acid phosphatase enzymes are present in the granules.
Cytochemical reactions
Eosinophils are peroxidase positive. They may show weak or no
naphthyl acetate esterase activity and moderate acid phosphatase
activity. Chloroacetate esterase and alkaline phosphatase activities are
not demonstrable (Table 3.4). The specific granules do not contain
PAS-positive material and are unstained, but there is positive staining in
the cytoplasmic background.
Eosinophil pools : functions
Eosinophils are found in the bone marrow, blood (circulating and
marginated pools) and the tissues, particularly in the skin and
sub-epithelial layers of the gastro-intestinal and respiratory tracts. The
28
NORMAL PERIPHERAL BLOOD CELLS
cells present in the tissues have migrated from the blood and the
majority do not re-enter the circulation. The functions of eosinophils
are to phagocytose antigen-antibody complexes, detoxify histamine,
5-hydroxy-tryptamine and bradykinin and to supply plasminogen to
localized deposits of intravascular fibrin.
THE POLYMORPHONUCLEAR BASOPHIL GRANULOCYTE
Morphology: cytochemical reactions : functions
This cell is commonly called the basophil. It may also be termed the
'mast' leucocyte or basophil with soluble granulations. It is
approximately 10 Mm in diameter. The nucleus is pale purple and usually
bi-lobed. The cytoplasm is faintly basophilic and contains relatively large,
coarse, met achromatic, bluish-black granules which may overlie
the nucleus. The staining reaction of the granules is due to their large
content of sulphated acid mucopolysaccharides. Sometimes irregular
staining of the granules may be noted due to the methyl alcohol
content of the staining solutions; only a few granules are seen in the cell
and the cytoplasm appears vacuolated. Like the eosinophil, electron
microscopy has demonstrated only one type of granule in the basophil.
The granules contain histamine and heparin. Cytochemically the cells
show no pèroxidase, esterase nor phosphatase activity (Table 3.4). The
PAS reaction reveals coarse magenta-coloured material in the
cytoplasm. Basophils are found in the blood and bone marrow. They
differ from mast cells (tissue basophils) which are also present in the
bone marrow and elsewhere. Basophils play a role in allergic reactions.
They degranulate and release histamine at sites of inflammation or
when allergens react with immunoglobulin E (IgE). Heparin is probably
not released from the cells.
Tissue mast cell
The tissue mast cell or tissue basophil is a granular connective tissue
cell, 20 - 25 μτη in diameter. It has an irregular outline and a round
nucleus. The granules are similar to those of the blood basophil but are
more numerous, pack the cytoplasm and are insoluble in alcohol.
THE MONOCYTE
Morphology (see Plate 2)
The monocyte is the largest cell usually seen in the blood film. It
measures 1 6 - 2 2 Mm in diameter (approximately three times the size of
normal red cell). The nucleus occupies an eccentric position in the cell
and its snaps is not constant; it may be round, oval, reniform,
29
THE PERIPHERAL BLOOD FILM
horse-shoe shaped or lobulated. It stains a blue or purple colour; the
chromatin is coarse but has a regular pattern. The cytoplasm is
abundant, slate grey to blue in colour and has a ground-glass appearance
because of numerous fine lilac granules. Electron microscopy has shown
that these granules are principally of one type. They contain acid
hydrolases and esterases such as acid phosphatase and lipase. They are
rich in lysozyme (muramidase); normally this enzyme does not make as
significant a contribution as that from degraded PMN to the lysozyme
concentration in serum.
Cytochemical reactions
The PAS reaction reveals fine PAS-positive material scattered
throughout the cytoplasm; it may be negative in some cells. The
peroxidase reaction is usually negative but some cells may show weak
positivity. The a-naphthyl acetate esterase activity is strong in
monocytes and can be used as a marker for these cells. The
cytochemical reaction for acid phosphatase is strong in monocytes;
however, its usefulness as a marker is limited because some activity can
be demonstrated in other leucocytes. The chloroacetate esterase and
alkaline phosphatase reactions are negative (Table 3.4).
Monocytic pools; life-span; macrophages
The pool of monocytes in the bone marrow is small. The half-life of
the cell in the circulation is 1 - 3 days. Monocytes migrate at random to
the tissues where they undergo further maturation into tissue
macrophages and survive for as long as 60 days. The tissue pool is
approximately 400 times greater than that of the circulating pool of
monocytes. Macrophages are morphologically similar to monocytes but
are larger and have more abundant cytoplasm. Metabolically they are
more active and have a greater functional capacity than the monocyte.
The characteristics of the two types of cells are indicated in Table 3.5.
Functions
Monocytes and macrophages belong to what has been termed the
'reticulo-endothelial system' (RES) and the 'mononuclear phagocytic
system' (MPS). They play a role in virus inhibition by producing
interferon, inflammatory reactions and cellular and humoral immunity.
The physiological functions of the cells include erythrophagocytosis,
removal of senescent cells and cellular debris, antigen processing and
reaction with lymphocytes during an immune response. The cells
provide a defence against micro-organisms such as mycobacteria, listeria
and brucella. Although some monocytes may show peroxidase activity,
macrophages lack this enzyme. Some monocytes reduce nitroblue
30
NORMAL PERIPHERAL BLOOD CELLS
TABLE 3.5
Characteristics of Monocytes and Macrophages
Cell diameter
Nucleus
Cytoplasm
Rough endoplasmic reticulum
Mitochondria
Polyribosomes
Golgi apparatus
Lysosomes
Lysosomal enzymes
Peroxidase
Properties
Membrane ruffling
Adherence to surfaces
Phagocytosis
Pinocytosis
Monocyte
Macrophage
16 - 22 Mm
Reniform or
lobulated
>22μπι
Reniform or
lobulated
+
Small
++
Large and
numerous
+
Small
Small and
scanty
++
±
±
Large
Large and
numerous
++++
-
+++
+++
++++
++
++++
++++
++++
+++
tetrazolium in the NBT reduction test; this number of formazanproducing monocytes appears to be of value in detecting bacterial
infection in patients with severe neutropenia (Park et αί, 1972). The
bactericidal activity of the cells is only partly dependent on the
generation of hydrogen peroxide; it is principally due to their lysosomal
enzymes. Unlike the microphages (PMN), monocytes and macrophages
resynthesize their granules and survive in vivo after phagocytosis.
THE LYMPHOCYTE
Morphology (see Plate 3a, b)
Lymphocytes in the peripheral blood are pleomorphic in
appearance. For descriptive purposes they may be divided into small
and large cells. The small lymphocyte (see Plate 3a) measures
approximately 8 Mm in diameter, and has a high nucleocytoplasmic
ratio. The nucleus appears hyperchromatic, is a dark purple-blue colour,
is round or slightly indented in form (Rieder form) and almost fills the
cell; the chromatin is coarse and clumped. A nucleolus or nucleolar
remnant may be evident in some cells; however, all lymphocytes possess
nucleoli (Yoffey and Courtice, 1970), best observed after wet fixation,
31
THE PERIPHERAL BLOOD FILM
or with phase contrast or electron microscopy. The pale blue scant
cytoplasm forms a thin rim around the nucleus and may contain an
occasional azurophilic granule.
The large lymphocyte (see Plate 3b) measures 12 -15jum in diameter.
The nucleus is purple, slightly oval and usually located eccentrically in
the cell; the chromatin has a loose structure and is not as dense or
coarse as that of the small cell. A nucleolus or nucleolar remnant may
be evident. The abundant cytoplasm is pale blue with a clear-glass
appearance. A few medium-sized azurophilic granules may be present.
Cytochemical reactions
The lymphocyte nucleus is Feulgen positive; the nucleolus is not
clearly demonstrable. The PAS reaction of the cytoplasm is variable;
approximately 20 per cent of the cells may show some coarse granules
arranged in concentric rings or forming a crown at the periphery of the
cell. The degree of PAS-positivity may be semi-quantitatively rated on a
0-3 scale; the sum of the ratings of 100 consecutive lymphocytes in a
peripheral blood film is referred to as the PAS score, the normal range
being 0-20. Peroxidase, alkaline phosphatase and chloroacetate esterase
activity is not demonstrable. The α-naphthyl acetate esterase reaction is
weak or absent; the acid phosphatase reaction is usually weak (Table
3.4).
Classes of lymphocytes
Lymphocytes are a heterogenous population of cells with varying
life-spans, metabolic properties and functional capacities; morphologically the various classes are indistinguishable. The cells may be
broadly classified, on the basis of their life-spans, as short-lived (days)
and long-lived (months-years). The pools of lymphocytes in the central
or primary organs (thymus and 'bursa of Fabricius' equivalent organ,?
bone marrow) are predominantly short-lived cells. Long-lived
T-lymphocytes (T-L) or thymus-derived cells and short-lived Blymphocytes (B-L) or bursa (? bone marrow)-derived cells are in the
peripheral or secondary organs (spleen, lymph nodes, subepithelial
follicles) and in the circulatory pool. A third class of lymphocytes, the
'Α' or accessory cells, has been found in the spleen and lymph nodes
(Osoba, 1972). T-L and B-L are considered to comprise 80-90 per cent
and 1 0 - 2 0 per cent respectively of circulating lymphocytes. The
characteristics of T-L and B-L are summarized in Table 3.6.
Functions
Lymphocytes play an important role in the body defence against
foreign antigen (bacterial, fungal, viral and tissue) invasion. The
32
NORMAL PERIPHERAL BLOOD CELLS
TABLE 3.6
Characteristics of T-Lymphocytes and B-Lymphocytes
Life-span
Cell markers
Functions
Cellular immunity
Humoral immunity
Antigen-stimulated
secretions
Stem cell
Origin
Migrates to
Blood lymphocyte
Origin
Blastogenic response
Mitogen
Antigen
Recirculating cells
Diseases with disordered
function
T-Lymphocy tes
B-Lymphocytes
Months-years
Theta antigen in
mouse, perhaps in
man
Days
C receptor site
Weak
Yes
No and yes,
Yes
depends on antigen
Interferon-like
substances
Immunoglobulins
Antibodies
Lymphokines
Immunoglobulins
IgG, IgA, IgM,
IgD, IgE after
transformation
into plasma cells
Bone marrow
Thymus
Bone marrow
Spleen, Lymph nodes
Thymus and
T-dependent areas
of spleen and
lymph nodes
Bone marrow and
B-dependent areas
of spleen and
lymph nodes
Yes
Yes < 3% of cells
Majority
Memory cells
No
Yes < 3% of cells
Minority
Hodgkin's disease
Sarcoidosis
Lymphocytic leukaemia
(CLL)
Auto-immune disease
Organ specific type Non-organ specific type
linkage
Destroyed by
Anti-lymphocyte serum Yes
No
Corticosteroids
Yes
No
development of body immunity relies on an interplay of the different
types of lymphocytes (Daniels, Ritzmann and Levin, 1968; Roitt et al,
1969; Craddock, Longmire and McMillan, 1971; Richter and Algom,
1972), on the monocyte-macrophage system and on the complement
(C') system. Antigen-stimulated T-L secrete a number of soluble
33
THE PERIPHERAL BLOOD FILM
substances, termed 'lymphokine' factors by Dumonde (1970), into the
local milieu. These factors increase vascular permeability, induce
mitotic activity in other lymphocytes, are cytotoxic for a wide variety
of target cells, inhibit the migration of macrophages from
antigen-containing areas and activate macrophages. Antigen-stimulated
B-L, influenced by 'A' lymphocytes and T-L, eventually transform into
plasma cells; the secretions of these cells are termed immunoglobulins
and are described later.
THE PLASMA CELL
Morphology
The plasma cell (plasmacyte) is commonly an elliptical or egg-shaped
cell, 1 2 - 1 6 μιη in diameter. The purple nucleus is located eccentrically
within the cell, is round or oval and has no nucleolus. Nuclear
chromatin is coarse and clumped; in histological sections the chromatin
shows a radial arrangement, giving the nucleus a cart-wheel appearance,
but this is not evident in films. The cytoplasm is abundant and deeply
basophilic; a white or faint pink perinuclear halo or 'flare' is commonly
adjacent to the nucleus and represents the cell's Golgi apparatus. The
normal mature plasma cell shows considerable morphological variation.
The outline of the cell may be irregular, the cytoplasm slate-grey to
grey-blue in colour, and the nucleus located centrally: sometimes the
cell is larger than usual and multinucleated with up to four nuclei.
Different forms of vacuoles or hyaline structures may be seen; these are
termed Russell bodies and represent collections of retained globulin.
They may be eosinophilic or basophilic in colour, depending on the pH
of the staining reaction (Goldberg and Deane, 1960) and arecommonly
PAS positive. Plasma cells with these inclusions have various names. The
cytoplasm of a Mott, mulberry or morula cell is almost filled with many
small or a few large vacuoles. The grape cell has large vacuoles partially
covering the nucleus and extending to the edge of the cytoplasm which
becomes irregular in outline.
Cytochemical reactions
The deep basophilic staining of the plasma cell cytoplasm with
Romanovsky dyes is due to its rich content of ribonucleic acid (RNA);
marked pyroninophilia is seen with the methyl green-pyronin reaction.
The cells show strong acid phosphatase activity and moderate
a-naphthyl acetate esterase activity (Table 3.4); the peroxidase, alkaline
phosphatase and chloroacetate esterase reactions are negative. Up to 55
per cent of the cells show slight to moderate acid acetate esterase
activity (Szmigielski, Litwin and Zupanska, 1965).
34
NORMAL PERIPHERAL BLOOD CELLS
Immunoglobulins
Plasma cells are short-lived end cells of the B-L series, essential for
the development of humoral immunity. They secrete the antibodies
that react with the antigens inducing their formation. Antibodies are
complex, structurally related glycoproteins termed immunoglobulins
(Ig). Each Ig molecule is composed of two dissimilar pairs of
polypeptide chains covalently linked by disulphide bonds. One pair of
chains consists of two identical 'heavy' (H) chains and a second pair of
two identical 'light' (L) chains. Six classes of immunoglobulins are
known; IgG, IgA, IgM, IgD, IgE and IgF and each has distincitive H
chains, gamma (7), alpha (a), mu (μ), delta (δ), epsilon (e) and phi (0).
The L chains are of two structural types, kappa (κ) and lambda (λ),
common to all Ig classes. Individual molecules, however, have only
kappa or lambda light chains, never both. IgF occurs transiently in the
foetus and has not been found post-natally (Hobbs, 1971). Thus there are
10 major types of immunoglobulins; approximately 75 per cent of
the light chains are kappa and 25 per cent are lambda. One plasma cell
is considered to secrete only one type of immunoglobulin. IgM is the
major antibody produced after primary exposure of the body to new
antigen and IgG is predominantly synthesized after re-exposure to the
specific antigen. IgA is the principal antibody of external secretions;
IgE is a reaginic antibody. No specific antibody activity has been
demonstrated for IgD.
THE PLATELET OR THROMBOCYTE
Morphology (see Plate 4)
The circulating platelet is a small colourless structure with a thin
disc-like shape. It measures 1.5 - 4.0 Mm in the blood film and appears as a
blue or purple, anucleate structure with centrally located red granules
and a spicular outline. The size, staining characteristics and lack of a
nucleus are due to its derivation from the cytoplasm of mature
megakaryocytes in the bone marrow and lungs. Heterogeneity of the
granules has been demonstrated by electron microscopy. Some contain
hydrolases, phospholipids and nucleotides and others are serotonin storage granules; glycogen is also present in the form of small scattered
granules. Many other organelles such as mitochondria and microtubules
are evident on electron microscopy. Cytochemically the PAS reaction is
positive and no peroxidase is demonstrable.
Contents
The platelet contains proteins (such as thrombosthenin, a contractile
protein with ATPase activity); phospholipids (particularly platelet
35
THE PERIPHERAL BLOOD FILM
factor 3, a clot-promoting substance); carbohydrates (glycogen and
glucose); enzymes of the glycolytic pathway and Krebs' citric acid
cycle; large concentrations of adenosine triphosphate; a pool of
adenosine diphosphate stored in granules; cyclic adenosine monophosphate and its related enzymes (adenyl cyclase and phosphodiesterase); platelet factors that play a role in the haemostatic
mechanism; amines (serotonin absorbed from plasma); and inorganic
substances like calcium, magnesium and potassium.
Functions
Platelets play a role in immunological reactions, in maintaining the
integrity of vascular endothelium and in haemostasis. The cellular
activity is related to their capacity to (1) phagocytose viruses and
immune complexes; (2) to adhere to 'foreign' surfaces which in vivo
may be collagen or vascular basement membrane or in vitro may be
glass or other silica-containing material; (3) aggregate or adhere to one
another when activated by stimuli such as proteolytic enzymes
(thrombin), amines and adenosine diphosphate; and (4) secrete or
release certain constituents, particularly those stored within the
granules.
Life-span : platelet pools
The life-span of the circulating platelets ranges from 8 to 12 days; the size
and functional activity decreases with age. Approximately 80 per cent
and 20 per cent of blood platelets originate from pools respectively in
the bone marrow and lungs, the megakaryocytes in the lungs having
migrated there from the bone marrow. A reserve pool of platelets is
sequestered in the spleen. The site and manner of destruction of the
cells not consumed in maintaining vascular integrity is uncertain.
According to Karpatkin (1969), platelets die by senescence rather than
by random utilization and destruction.
36
4
Abnormal Red Cells
CLASSIFICATION
Morphological abnormalities of red cells may be classified into four
categories; staining, size (small and large), shape (smooth and irregular
margins) and inclusion-containing red cells (Table 4.1). The visual and
physical characteristics of some cells are such that they may be
included in more than one category. An example is the spherocyte
which is abnormal in size and shape and appears densely stained in the
TABLE 4.1
Abnormal Red Cells
Staining abnormalities
Hypochromic red cell
Target cell or leptocyte
Stomatocyte
Spherocyte (dense staining cell)
Red cells with inclusions
Size abnormalities
Small red cells
Microcyte
Spherocyte (visual microcyte)
Schistocyte
Large red cells
Round macrocyte
Oval macrocyte
Stomatocyte
Spherocyte (volume macrocyte)
Target cell (visual and volume macrocyte)
Shape abnormalities or poikilocytes
Cell with smooth margins
Elliptocyte
Oval macrocyte
Spherocyte
37
THE PERIPHERAL BLOOD FILM
Table 4.1 cont.
Cells with irregular margins
Sickle cell
Blister cell
Crenated red cell
Acanthocyte
Burr/spur cell
Pyknocyte
Schistocyte
Tear-drop cell
Cottage-loaf (dumb-bell) cell
Red cells with inclusions
Red cell with Howell-Jolly body
Red cell with Pappenheimer bodies (siderocyte)
Red cell with punctate basophilia
Red cell with Heinz bodies
Red cell with malarial parasite
blood film. The morphology of an abnormal red cell is described in that
category which is important for its recognition in the film.
Normal red cells are flexible and deformable. These properties
depend on cell shape, physical (visco-elastic) and chemical (particularly
lipid) characteristics of the cell membrane, and fluidity of the cell
contents. They are essential for the passage of the cells through the
microvasculature where the diameter of the blood vessels may be
smaller than that of the cells themselves. Abnormal red cells have a
shorter life-span than normal. Intracellular abnormalities and/or
changes in the composition of the cell membrane predispose to cellular
rigidity, fragmentation with or without loss of haemoglobin from the
cell and premature removal of the cell from the circulation by the
macrophages of the reticulo-endothelial system. The 'culling' and
'pitting' functions of the spleen are important for the destruction of
damaged cells and for the removal of rigid inclusions without
immediate cell destruction. This latter function may produce pits in the
red cells' surface ('pocked' erythrocytes) that have been noted by
scanning electron microscopy. Certain types of abnormal red cells may
not be readily observed in the blood film from subjects with a normally
functioning spleen; however, these cells become more numerous and
readily detectable after splenectomy or if asplenia supervenes in the
disease state.
STAINING ABNORMALITIES
Hypochromic red cell
The hypochromic red cell appears as a pale cell with a thin peripheral
pink ring (anulocyte or pessary form) or as a red cell with a central
38
ABNORMAL RED CELLS
pallor greater than normal. The size and shape of the
cell is variable. Hypochromia of a red cell is due to defective
haemoglobinization; the degree of pallor depends on the extent to
which the haemoglobin concentration within the cell is reduced. The
factors responsible for the production of hypochromia are listed in
Table 4.2. Iron deficiency and defective mobilization of iron from the
TABLE 4.2
Hypochromic Red Cells
Abnormalities of iron metabolism
Absent iron stores
Iron deficiency
Nutritional inadequacy
Impaired iron absorption
Increased iron requirements — pregnancy
Inability to transport iron — transferrin deficiency
Chronic iron loss — haemorrhage
Focal sequestration of iron in lungs and kidneys
Normal iron stores
Defective mobilization of iron from body stores — chronic
disorders
Impaired protoporphyrin 9 and haem synthesis
Quantitative and qualitative defects of enzymes
Delta-amino levulinic acid (delta-ALA) synthetase
Haem synthetase
Abnormalglobin chain synthesis
Quantitative - thalassaemias
Qualitative - unstable haemoglobins
Unknown pathogène sis
Sideroblastic anaemia
Pi Guglielmo's syndrome
body stores are common, followed by diminished globin chain synthesis
in certain races and ethnic groups, e.g., Greeks, Italians and Negroes.
The Hb-A2 concentration is decreased in hypochromic cells resulting
from iron deficiency, alpha-thalassaemia, sideroblastic anaemia and Di
Guglielmo's syndrome. The red cells in disorders with impaired
protoporphyrin synthesis in the erythroblasts may show red
fluorescence when exposed to UV light.
Target cell or leptocyte (see Plate 5)
The target cell (Table 4.3) has a central pink nodule separated from
an outer pink ring by a circular area of pallor; in some cells a bridge
may join the two pink zones. This distribution of the red cell's
39
THE PERIPHERAL BLOOD FILM
TABLE 4.3
Target Cells or Leptocytes
Reduced volume of contents
Hypochromic red cells (Table 4.2)
Increased surface area
Defect of lecithin-cholesterol acyl transferase (LCAT) in plasma
Absent LCAT synthesis
Hereditary LCAT deficiency
Inhibited LCAT activity
Obstructive jaundice
Hepatitis with biliary obstruction
haemoglobin is seen only in films; in wet preparations the cells appear
cup-shaped. They may occasionally develop as an artefact in normal
cells due to increasing hypertonicity in the fluid medium surrounding
individual cells as the film dries. Target cells commonly form when thin
flat cells or leptocytes are spread on a glass slide. Characteristic features
of target cells are (1) visual macrocytosis — the cell's MCD as measured
in the film is greater than 7.9 Mm but the MCV is within normal limits; (2)
leptocytosis, that is, a MCAT less than 1.9 Mm; (3) macroplania or a
surface area greater than 140 Mm2; (4) a surface area-to-volume ratio
greater than normal (which is the reverse of that seen with spherocytes)
- this increased ratio may be due to reduction in the volume of cell
contents as in hypochromic red cells or due to increased surface area as
in obstructive jaundice; and (5) increased resistance to osmotic lysis in
hypotonie solutions. The development of target cells in subjects with
abnormal lecithin-cholesterol acyl transferase (LCAT) activity is due to
an increase in the cells' surface area resulting from an accumulation of
cholesterol and lecithin in the cell membrane. Diminished LCAT
activity in plasma is followed by reduced cholesterol esterifîcation and
an increase in free cholesterol and lecithin in the plasma. Because cell
membrane lipids are in equilibrium exchange with plasma lipids
(Cooper, 1970b) cholesterol and lecithin accumulate in the cell
membrane, expanding its surface without any alteration of the cell
contents. In obstructive jaundice, the bile salts (cholic and deoxycholic
acid) in the jaundiced plasma inhibit LCAT activity and influence the
equilibrium partition of free cholesterol between serum lipoproteins
and red cell membranes (Cooper and Jandl, 1968). According to
Kilbridge and Heller (1969) volume macrocytosis appears in liver
disorders when haemorrhage or haemolysis has occurred or when there is
concomitant megaloblastosis due to vitamin B i 2 and/or folate
deficiency.
40
ABNORMAL RED CELLS
Stomatocyte (see Plate 6)
The stomatocyte (Table 4.4) is a large red cell with a linear,
mouth-like, unstained area across the centre of the cell. In wet
preparations the cell's appearance has been described as bowl-shaped,
mushroom-cupped and spherical vwith a deep invagination on one side.
TABLE 4.4
Stomatocytes
Hereditary
Intra-erythrocytic electrolyte reversal
Hereditary stomatocytosis
With blood group abnormalities
Rh n u u disease
Acquired
Acute alcoholism
Liver disorders
The cell may occur as an hereditary or an acquired anomaly. The
hereditary stomatocytes have a slightly shortened survival and are
mechanically and osmotically more fragile then normal cells. The MCV
is greater than 100 Mm3 due to its high water content, and there is a
disturbance of cation regulation by the cell membrane which is
abnormally permeable to sodium and potassium. The major cation of
the cell in hereditary stomatocytosis has been shown to be sodium
rather than potassium; this is a reversal of that seen in normal red cells.
Sodium and potassium concentrations in normal red cells are 10mEq/l
and 95 mEq/1 of red cells respectively; in hereditary stomatocytes the
sodium and potassium concentrations are approximately 100 and 40
mEq/1 of red cells respectively (Zarkowsky et al, 1968; Oski et al,
1969). The phospholipid content of the cell membrane is normal and
stable. The increased osmotic fragility is possibly a reflection of the
increased volume and reduced surface area-to-volume ratio. The
stomatocytes of Rhnuy] disease are characterized by non-agglutinability
with anti-Rh typing sera and by abnormalities in several other blood
group systems (Schmidt and Holland, 1972). The acquired stomatocyte
commonly occurs as a transient phenomenon. Alteration in intracellular
electrolytic concentration may not be demonstrable and the fragility of
the cell is within normal limits.
Spherocyte (see Plate 7)
The spherocyte (Table 4.5) appears as a densely eosinophilic red cell,
smaller (MCD approximately 5 μτή) than a normal red cell and without
any central pallor; the outline of the cell is smooth and regular. The
41
THE PERIPHERAL BLOOD FILM
TABLE 4.5
Spherocytes
Hereditary
Hereditary spherocytosis
Acquired
Decreased surface area
Fragmentation of cell membrane
Haemoglobinopathies - thalassaemias and Hb-S disease
Antibody injury to cell membrane - blood group specific,
drug-induced or auto-antibodies
Loss of lipids from cell membrane
Thermal injury — burns
Stored anticoagulated blood — bank blood
Increased cell volume
Osmotic swelling
Red cells suspended in hypotonie solution
characteristics of the cell are (1) a spherical or globular shape, (2) visual
microcytosis with a normal or raised MCV, (3) a surface area-to-volume
ratio less than normal (which is the reverse of that seen with target
cells), (4) increase in the rigidity of the cell membrane and (5) increase
in the osmotic fragility in hypotonie solutions. The cell may occur as an
hereditary (autosomal dominant) or acquired anomaly. The hereditary
anomaly is not apparent in the precursor cells. The shape of the
hereditary spherocyte (HS) is generally accepted as due to an abnormal
cell membrane (Jacob 1969) which leaks sodium at excessive rates. The
cholesterol and phospholipid content of the HS cell membrane is less
than normal in subjects with spleens but reverts to normal levels after
splenectomy. The spherical shape and increased osmotic fragility of the
HS are unaffected by splenectomy, and factors other than lipid
concentration may be responsible for the anomaly. The underlying
genetic defect appears to be an altered muscle-like protein of the cell
membrane (Weed, 1970, Jacob et al, 1971) which may be the material
termed 'spectrin' by Marchesi and Steers (1968).
The acquired spherocyte (AS) commonly results from a decrease in
the surface area of a normal or abnormal red cell and may be secondary
to successive fragmentation of the cell membrane or to loss of
membrane lipids. The AS of thalassaemia may be produced by splenic
pitting of precipitated globin chains and that of sickle cell disease from
fracture of protruding portions of sickled cells. The AS of antibody
injury may be due to partial phagocytosis by splenic macrophages of
localized areas of membrane rigidity, the unphagocytosed portion of
the cell becoming increasingly spherocytic (Rosse and Lauf, 1970). The
42
ABNORMAL RED CELLS
mechanism for cell rigidity depends on the sensitizing antibody and
varies with ATP instability, decrease in glycolytic activity and the
formation of roughened finger-like processes extruding from the surface
and visible only by the stereoscan electron microscope (Rosse and Lauf,
1970). The red cells in bank blood stored at 4°C become spherocytic
from progressive loss of membrane lipids — a consequence of
esterification of free cholesterol in the plasma by lecithin-cholesterol
acyl transferase (LCAT); after transfusion these cells rapidly revert to
their normal shape. Red cells suspended in vitro in hypotonie solutions
assume a spherical shape; the cell volume increases owing to osmotic
swelling.
SIZE ABNORMALITIES
SMALL RED CELLS
Microcyte
The microcyte is smaller than a normocyte. The MCD is less than 6.7
Mm and the MCV less than 77 Mm3. The cell outline may be round or
slightly irregular. It may appear normochromic or hypochromic. The
former type is distinguished from a spherocyte by the less intense
eosinophilic staining and/or the presence of central pallor. Microcytes
are seen in most anaemias and are particularly evident in anaemias
characterized by defective haemoglobinization. Their formation may
result from an increase in the number of reduction divisions of the
immature cells in the bone marrow. The haemoglobin concentration in
these immature cells may regulate the number of reduction divisions by
inhibiting DNA synthesis when a critical 'cytoplasmic haemoglobin
concentration' (CHC) has been attained (Stohlman, 1967; Stohlman et
al., 1968). In anaemias with defective haemoglobinization there is a
delay in attainment of the critical CHC, with a consequent increase in
the number of reduction divisions and the production of microerythroblasts which mature into microcytes.
LARGE RED CELLS
Round macrocyte (see Plate 8a)
The round macrocyte is larger than a normocyte and appears
normochromic. The MCD is greater than 7.9 μιτι. Characteristics of the
cell are (1) 'volume' macrocytosis, that is, an MCV greater than 100
Mm3 ; (2) a MCAT greater than 2.4 Mm; and (3) derivation from macronormoblastic precursor cells in the bone marrow. Their formation may
result from a decrease in the number of reduction divisions of the
immature cells in the bone marrow. The haemoglobin concentration in
these immature cells may regulate the number of reduction divisions
43
THE PERIPHERAL BLOOD FILM
by inhibiting DNA synthesis when a critical 'cytoplasmic haemoglobin
concentration' (CHC) has been attained (Stohlman, 1967; Stohlman et
0/., 1968). In anaemias due to acute blood loss (haemorrhage or
haemolysis) and in anaemias responding to specific haematinic therapy,
this critical CHC may be attained earlier than normal because of
accelerated haemoglobin synthesis; as a consequence there is a decrease
in the number of reduction divisions and the production of macronormoblasts which mature into round macrocytes.
Oval macrocyte (see Plate 8b)
The oval or pear-shaped macrocyte is larger than a normocyte and
commonly appears normochromic. The MCD is approximately 10 Mm.
Characteristics of the cell are (1) 'volume' macrocytosis, that is, an
MCV of 120 - 130 Mm3; (2) a MCAT greater than 2.4 Mm; and (3)
derivation from megaloblastic precursor cells which are characterized
by early haemoglobinization of their cytoplasm and asynchronic
nucleocytoplasmic maturation. The presence of these cells in the blood
film is suggestive of vitamin B ^ and/or folate deficiency. The large size
of the cell is due to megaloblastosis of erythropoietic tissue. The factors
responsible for the shape of the cell are not known.
SHAPE ABNORMALITIES
CELLS WITH SMOOTH MARGINS
Elliptocyte (see Plate 9)
The elliptocyte is a normochromic oval-shaped red cell, approximately
8.0 Mm long and 5.2 Mm wide; longer and narrower cells with rounded
ends (rod forms) may also be seen and should not be confused with
sickle cells which have pointed ends. The cell may occur as an hereditary
(autosomal dominant) or acquired anomaly. The hereditary anomaly is
not apparent in the normoblastic stages; it is first observed at the
reticulocyte stage. Elliptocytes are not seen in the blood of neonatal
infants; the anomaly becomes evident only in the second week of life
and the number of elliptocytes reaches the maximum percentage after
the age of 3 months when they comprise more than 25 per cent of the
red cells in the blood. According to Rebuck and van Slyck (1968) the
cell is a biconcave dumb-bell shaped structure in one plane, an ellipse in
another plane and shows bipolar massing of haemoglobin. The basic
anatomical defect appears to reside in the cell membrane. Surviving cells
in hypotonie solutions remain elliptical. Further, the cell envelope
retains its shape after evacuation of the cell contents; this may be due
44
ABNORMAL RED CELLS
to the concentration of cholesterol at the two poles of the cell, which
are the sites of greatest convexity. The MCV and the MCH is usually
normal but may be reduced. While no abnormal haemoglobin has been
demonstrated in hereditary elliptocytosis, the rod forms are associated
with disorders of haemoglobin synthesis such as thalassaemia, Hb-S and
Hb-C diseases. The rod forms are also prominent in hereditary
haemorrhagic telangiectasia. The osmotic fragility and glycolytic
enzymes of the cells are usually normal. However, in 12 per cent of
subjects the autohaemolysis and the incubated osmotic fragility are
greater than normal and there may be multiple enzyme defects in the
cells which are predominantly oval shaped. Acquired elliptocytosis is
commonly seen in blood films of anaemic patients. The elliptocytes
represent less than 25 per cent of the red cells in these films.
CELLS WITH IRREGULAR MARGINS
Sickle cell (see Plate 10)
There are two types: the mildly sickled cell which is oat-shaped or like
a holly leaf in appearance and the filamentous type. The latter is a thin
elongated red cell with pointed ends which distinguish it from the rod
form of elliptocyte; the cell may assume a sickle, V or L form. Both
types of cells contain haemoglobin S, a genetically determined
abnormal haemoglobin with molecular formula oc2 Aj32 s . The beta chain
of Hb-S differs from that of Hb-A in that valine replaces the normally
occurring glutamyl residue in the sixth position from the amino
terminus. According to Murayama (1964) the valine in the first position
of the beta chain interlocks by hydrophobic bonding with that present
in the sixth position to form a ring or cyclic structure at the N-terminal
end of the chain.
Haemoglobin S may constitute the predominant haemoglobin in the
red cells (sickle cell disease); it may be associated with Hb-A (sickle cell
trait), Hb-F, other haemoglobins such as Hb-C or with thalassaemia.
The presence of Hb-S may be detected by electrophoresis of red cell
haemolysates, the sideling phenomenon or by cytochemical reactions.
On starch gel electrophoresis at pH 8.6, Hb-S migrates faster than
Hb-A2 and more slowly than Hb-A. Red cells containing oxygenated
Hb-S are morphologically normal. On removal of oxygen the cells sickle
due to molecular aggregation and intracellular tactoid (unidirectionally
formed crystals) formation, but revert to their original form on reexposure to oxygen. Repeated cycles of sickling and unsickling, particularly of red cells in which Hb-S is the predominant haemoglobin,
may result in the formation of sickle cells that have lost their ability to
revert to the discoid form. These irreversibly sickled cells (ISC) are
rigid, incapable of traversing the microcirculation and prone to frag45
THE PERIPHERAL BLOOD FILM
mentation. Electron microscopy has shown these ISC to have irreversibly deformed and inelastic cell membranes (Döbler and Bertles,
1968). The sickle cells seen in blood films of subjects with sickle cell
disease are likely to be ISC unless they are experiencing a sickling crisis.
The number of ISC in the blood is relatively constant in an individual
but varies between patients (Serjeant, Serjeant and Milner, 1969).
A mechanism for the sickling phenomenon, the key and lock
hypothesis, has been proposed by Murayma(1964). On deoxygenation
of haemoglobin, the ß chains of a haemoglobin molecule separate
slightly from one another and the distance between the ß chain of one
molecule and the a chain of an adjacent molecule is shortened.
According to Murayama, the cyclic structure at the N-terminal end of
the 0 s chain, acting as a 'key' now fits into a complementary part
('lock') or receptor site on the a chain of the neighbouring molecule;
rod-like polymers form and these align into fibres which distort the cell.
On reoxygenation of haemoglobin, the movement of the paired 0 s
chains is reversed and they come closer together. The ring structure of
the j3s chain is removed from the complementary site on the a chain;
the 'key' is now pulled out of the 'lock', the deformed cell unsickles
and reverts to its original discoid form.
Blister cell
The blister cell is a red cell with a bleb or bubble on its surface. The
haemoglobin in the opposite pole appears condensed and sharply
separated from the colourless area. The shape of the cell varies but
commonly resembles a round or conical basket with a handle or a
bonnet. Blister red cells are seen in sickle cell anaemia patients with
pulmonary emboli (Barreras, Diggs and Bell, 1968).
Crenated red cell or echinocyte (see Plate 11)
The crenated red cell has a uniformly serrated edge. The cell may be
normocytic or elliptocytic and the serrations are commonly formed by
short, blunt, evenly spaced protuberances, giving the effect of a wavy
edge; the polar ends of an elliptocytic cell are usually free of serrations.
The 'sea-urchin' type of cell appears as a dark-staining spheroidal cell
with a surface covered by numerous small needle-Hke projections.
Crenation is an artefact produced when the film dries slowly and is due
to the development of increasing fluid hypertonicity immediately
surrounding individual red cells. 'Sea-urchin' crenation is striking in
films prepared from old anticoagulated blood. Crenated red cells are of
no significance but must be differentiated from other spinous
erythrocytes.
46
ABNORMAL RED CELLS
Acanthocyte: burr/spur cell: pyknocyte (Table 4.6)
Acanthocyte (from the Greek word, acanthos - spine or thorn),
burr and spur cell and pyknocyte are terms that have been applied to
irregularly contracted poikilocytes with bizarre shapes and thorny
excrescences. They are disinguished from crenated red cells by the
irregular spacing and unequal lengths of their spines. Acanthocytes (see
Plate 12) are star-shaped, deeply eosinophilic, spheroidal cells with long
sharp-pointed spines. They are seen particularly in the rare hereditary
disorder of beta lipoprotein deficiency. The shape of the cell is
irreversible and although it appears spheroidal, the osmotic fragility is
normal. According to Cooper (1970b) the cell membrane cholesterol of
TABLE 4.6
Spinous Erythrocytes
Crenated red cells
Artefact
Sickle and holly leaf cells (Table 12.27)
Haemoblogin S-containing red cells
Acanthocytes
Hereditary abetalipoproteinaemia
Burr/'spur cells (Table 12.28)
Intra-erythrocytic factors — fragmentation of abnormal red cells
Hypochromic red cells
Macro-ovalocytes
Cell membrane lipid abnormalities
Haemoglobinopathies
ATP instability
Glutathione instability (Table 4.8)
Antibody-injured red cell
Iso-immune antibodies
Auto-immune antibodies
Drug-induced antibodies
Plasmatic and/or vascular factors — fragmentation of normal red cells
Physical
Mechanical
Toxic
Pyknocytes
Immaturity of red cell enzymes in premature infants
Schistocytes
Fragmentation of abnormal red cells
Fragmentation of normal red cells
Disseminated intravascular coagulation (Table 12.7)
Tissue thromboplastin in circulation
Partial thromboplastin in circulation
Factor XII and/or or platelet activation
47
THE PERIPHERAL BLOOD FILM
the acanthocyte is normal or slightly increased, the phospholipid
content is normal, but the lecithin content is markedly decreased.
Burr cells (Schwartz and Motto, 1949) are irregularly contracted
discoidal or ellipsoidal cells with spines that may terminate in a sharp
point, a blunt knob or bud-like swelling. Their appearances have been
likened to small beetles, crabs and turtles (see Plate 13). Dense staining
burr cells that may be seen in premature infants have been called
'pyknocytes'. Triangular or crescent-shaped red cells with two long
spines are sometimes referred to as 'horned' cells or keratocytes. Burr
cells are also called spur cells. They are stiff and poorly deformable cells
with shortened life-spans and increased osmotic fragility. Fragmentation of abnormal red cells due to intra-erythrocytic factors and of
normal red cells due to plasmatic and/or vascular factors appears to be
the fundamental mechanism for the development of burr/spur cells.
Bell (1963) postulated that the horned cell and possibly other types of
burr cells arise from rupture of a peripheral intra-erythrocytic vacuole,
formed as a result of mechnical or toxic injury or senescence at the
periphery of the cell. The nature of the vacuoles has not been
established and some investigators consider them to be artefacts.
According to Cooper (1970a), the burr cell occurring in uraemia has a
normal membrane lipid composition and results from the presence of a
heat-labile, non-dialysable 'burr cell factor' in the uraemic plasma.
Mechanical fragmentation of red cells occurs when blood is pumped
against prosthetic or calcified and stenosed heart valves or when red
cells impinge on the fibrin mesh of intravascular thrombi resulting from
disseminated intravascular coagulation. In micro-angiopathic disorders
burr cells also form by cell fragmentation when portions of the red cell
stick to epithelial cells of tumour emboli or to rough vascular surfaces
(Brain, 1970). Fragmentation of abnormal red cells may take place
spontaneously as the rigid, poorly deformable cells traverse minute
orifices in the microvasculature (Cooper, 1969). Fragmentation of the
terminal spherules on sickled cells may also occur during reoxygenation
and reconversion of the cell to the disc form. The burr cells in liver
disorders are unusual in that, like target cells, they have an increased
cholesterol-to-lecithin ratio (Cooper, 1969). This author considered
that accumulation of chenodeoxycholic acid and its toxic degradation
product, lithocholic acid, in the plasma may be of importance in the
genesis of burr cells in liver disorders. McBride and Jacob (1970),
however, suggested that stagnation of cell membrane cholesterol due to
sluggish flux to and from cell membranes and, less importantly,
cholesterol accumulation may produce conformational changes in the
structural lipoproteins of the membranes and the morphological
abnormality.
48
ABNORMAL RED CELLS
Schistocyte (Table 4.6)
The schistocyte is a small (3 Mm or less) haemoglobinized fragment
of a red cell. The shape varies but triangular and helmet forms are
common. They are produced by cell fragmentation and associated with
burr cells. Large numbers of schistocytes are particularly seen in
patients with a bleeding diathesis due to acute (or decompensated)
disseminated intravascular coagulation (DIC). The pathogenesis of DIC
varies. It results from the entry of tissue or partial thromboplastic
substances into the circulation; it also follows factor XII and/or platelet
activation.
Tear-drop cell (see Plate 14)
The tear-drop poikilocyte is an oval-shaped cell with one polar end
drawn out in the form of a tongue, 2 - 3 μπ\ in length. It is usually
normochromic and may be normocytic or macrocytic. A variant is the
hand-mirror or raquet form which has a long tongue and appears
normocytic. The normocytic forms are prominent in agnogenic myeloid
metaplasia (myelofibrosis of the bone marrow) and aplastic anaemia.
The macrocytic forms are observed in megaloblastic anaemia.
Cottage-loaf (dumb-bell) cell
The cottage-loaf or dumb-bell type of poikilocyte is a red cell with
an equatorial constriction. It may be seen in haemolytic anaemias.
RED CELLS WITH INCLUSIONS
Red cell with Howell-Jolly body (see Plate 15)
The Howell-Jolly body is a non-refractile purple or dark violet mass,
approximately 1 μπι in diameter, situated in an eccentric position in the
red cell; one or more bodies may be present in a single cell. The
inclusion is a Feulgen-positive, DNA-containing nuclear remnant,
formed by karyorrhexis of the late erythroblast nucleus; the detached
body is not extruded with the pyknotic nucleus and persists through
the reticulocyte stage to the mature cell. Red cells containing
Howell-Jolly bodies occur in various haemolytic anaemias; cells with
two or more bodies are suggestive of megaloblastosis.
Red cell with Pappenheimer bodies (siderocyte) (see Plate 16)
Pappenheimer bodies are coarse, pale blue granules which may be
seen in red cells of varying size, shape and colour. Cells with numerous
fine granules may appear stippled. The inclusions represent aggregates
of ferric iron that have not been utilized for haem synthesis in the
precursor cells. They give a positive Prussian blue reaction, and their
blue coloration in the Romanovsky-stained film may be due to their
association with basophilic staining material. Red cells with Pappen49
THE PERIPHERAL BLOOD FILM
heimer bodies are termed siderocytes. They are rarely, if ever, seen in
normal blood films and do not occur in iron deficiency anaemias or in
anaemias of inflammatory disorders. Their presence in the blood film is
suggestive of sideroblastic anaemia, disordered haemoglobin synthesis
(hereditary — haemoglobinopathy; acquired — lead poisoning) and
sometimes of haemolytic anaemia. If splenic function is intact the
number of siderocytes is usually small and difficult to detect in the film
but this number increases considerably after splenectomy.
Red cell with punctate basophilia (Table 4.7)
The red cell with punctate basophilia may be a polychromatic,
normochromic or hypochromic cell with many fine dark blue granules.
The principal constituent of the granules may be ribonucleoprotein,
free globin chains or iron not utilized for haemoglobin synthesis. Their
nature is distinguished by supravital dye staining and the Prussian blue
reaction. The stippled red cell may thus represent a 'reticulocyte', a
'thalassaemic' cell or a 'siderocyte'. The pathogenesis of the stippled
cell varies with the disorder in which it occurs. The stippled form of
reticulocyte is commonly associated with polychromasia of the red cell,
and electron microscopy shows the granules to be composed of
clumped ribosomes that do not pre-exist in the cell but develop during
staining of the blood film. By varying their Romanovsky staining
technique, Jensen, Moreno and Bessis (1965) demonstrated the
interchangeability of the punctate and diffuse basophilic appearance of
reticulocytes. In beta-thalassaemia stippling appears in young erythrocytes, while in haemoglobin H disease (alpha-thalassaemia intermedia) it
appears in older cells. In the former condition the excess alpha chains
precipitate in the cytoplasm of the nucleated precursor cells, and in the
TABLE 4.7
Red Cells with Punctate Basophilia
Reticulocyte type
Premature release of erythrocyte antecedent cell
Haemorrhage
Haemolysis
Lead poisoning
Thalassaemic type
Diminished globin chain synthesis
Thalassaemias
Siderocytic type
Defect in haem synthesis
Heavy metal poisoning (lead, silver, mercury, bismuth)
Sideroblastic anaemia (some cases)
50
ABNORMAL RED CELLS
latter disorder the beta chain tetramers slowly precipitate during the
life of the mature cell in the circulation.
The siderocytic type of stippled cell is commonly hypochromic
because of a defect in haem synthesis (not due to iron deficiency). In
lead poisoning there is inhibition of several enzymic steps including that
required for the incorporation of iron into protophorphyrin 9.
Basophilic stippling in lead workers is more numerous in capillary blood
films than in films prepared with anticoagulated (EDTA) venous blood
(Clark, Jones and Jones, 1967). However, the count is no longer
recognized as a reliable screening test for lead poisoning; stippled cells
may not be seen in tetraethyl lead poisoning or in acute poisoning in
children (Flink, 1971). Basophilic stippling in some cases of sideroblastic anaemia is due to impairment of mitochondrial enzyme
(delta-ALA and haem synthetases) activity; in other cases the pathogenesis is not certain.
Red cell with Heinz bodies (Tables 4.8 and 4.9)
Heinz bodies are not seen in Romanovsky stained blood films, but
are routinely detected by supravital staining with methyl violet or
brilliant green; they can also be demonstrated by phase contrast and
electron microscopy. Heinz bodies appear as round or irregularly
TABLE 4.8
Glutathione Instability
Physiological immaturity of enzymes in neonates
Normal enzyme activity
Regular occurrence with drugs such as dapsone, phenacetin
Deficient enzyme activity
Hereditary G6PD deficiency
Hereditary 6PGD deficiency
Hereditary glutathione reductase deficiency
Glutathione deficiency
TABLE 4.9
Unstable Haemoglobins
Abnormalities in haem pocket
Deletions
- Hb-Gun Hill
Beta chain substitutions
— Hb-Zurich, Hb-Köln, etc.
— Hb-Norfolk
Alpha chain substitutions
Proline substitution in helical regions
Hb-Bibba, Hb-Sabine
Substitution in alpha-beta contact area
Hb-Philly, Hb-Bronx-Riverdale
51
THE PERIPHERAL BLOOD FILM
shaped coccoid structures, 1-2 μιη in diameter, situated at or close to
the periphery of the red cell. The inclusions are composed of
precipitated globin-glutathione complexes, formed in the interior of the
cell by the binding of denaturing haemoglobin thiols with cytoplasmic
glutathione (Jacob, 1970). Electron microscopy studies have shown
these precipitated complexes to coalesce and migrate to the cell
periphery where they attach themselves to the red cell membrane
through mixed disulphide linkages.
The mechanistic pathways for Heinz body formation are shown
in Figure 3; exposure to oxidant drugs and chemicals is not the only
initiating factor (see Table 12.32). Glutathione instability (Table 4'8),
Oxidant stress
GSH instability
Hb-A
MetHb -*-
Unstable Hb
/3-chain haem
pocket
abnormality
Haem
a/3 contact area
abnormality
/3-haem
Haem
Precipitated
o
OL , β
Precipitated
Precipitated
οΛ
Haem
chains
chains
<*2
Haem
.
02
chains
+ Glutathione
+ Glutathione
White
Red
Heinz bodies
Heinz bodies
I
Figure 3. Mechanism of Heinz body formation
52
chains
I
ABNORMAL RED CELLS
deficiency of triosephosphate isomerase of the Embden-Meyerhoff
glycolytic pathway or the presence of an 'unstable' haemoglobin (Table
4.9) is fundamental to the genesis of the inclusions. Unstable
haemoglobins are inherited mutant haemoglobin molecules characterized by decreased affinity of globin for haem. Loss of haem from the
haemoglobin molecule, either spontaneously or after methaemoglobin
formation as a result of oxidant stress, is followed by precipitation of
the globin chains as the presence of the haem molecule is essential for
globin stability. The Heinz bodies that eventually appear are white.
Haemoglobin Philly and haemoglobin Bronx-Riverdale are unstable
because of peptide mutations in the alpha-beta chains contact area.
However, their precipitated globin chains are haem-replete and the
Heinz bodies are red in colour.
Heinz bodies are rigid structures and their production is associated
with haemolytic anaemia. Heinz body anaemia due to an unstable
haemoglobin has been shown to be a variety of the congenital
non-spherocytic haemolytic anaemias that may occur in premature
infants.
Red cell with malarial parasite (Table 4.10)
There are four principal species of malarial parasite that infect man.
They are Plasmodium vivax, Plasmodium falciparum, Plasmodium ovale
and Plasmodium malariae. They respectively cause benign tertian,
malignant tertian, benign tertian and quartan malaria. Plasmodium
ovale specifically occurs in tropical Africa and Plasmodium malaria in
the Far East. The plasmodia are obligate intracellular parasites. Their
life cycle can be divided into two stages: a sexual stage (sporogony) in
the female Anopheles mosquito and an asexual stage (schizogony) in
vertebrates. Human malaria commonly results from the bite of an
infected female Anopheles mosquito. It may also be caused by transfusion of malaria-infected blood and by use of contaminated needles by
drug addicts. There are two phases to the asexual cycle, the exoerythrocytic phase in liver cells and the erythrocytic phase. Sporozoites
(fine filamentous forms of the parasite produced at the end of the
sexual cycle) in the mosquito's salivary fluid enters the blood stream
through the puncture wound. Within one hour they migrate to and
invade liver parenchymal cells, initiating the exo-erythrocytic phase.
Here the sporozoites undergo further development and multiplication
(schizogony) into small round merozoites. After approximately 8 days,
the infected liver cells (each filled with many merozoites) rupture,
freeing their merozoites. Some of the merozoites re-enter other liver
cells (except P. falciparum which has no secondary exo-erythrocytic
phase); some are phagocytosed by histiocytes. Other merozoites enter
53
Like P. vivax
Bizarre forms. Band
form stretching
across red cell
Like P. vivax
Like P. vivax
Multiple invasion is
common. Small blue
rings with single or
double red chromatin
dots. Some rings may lie
along edge of cell
(applique' form).
Rings are smaller
than those in P. vivax
Not seen
Deep blue signet
ring with redchromatin
dot. Size= 1/3 of red
cell
Blue, oval or
round body occupying more than Vi
red cell. Irregular outline.
Scattered red dots
Trophozoite,
early
Trophozoite,
late
No increase in cell
size. Ziemann's
dots (pink granules)
Large oval cell
with fimbriation
of ends
No increase in cell
size. Maurer's dots
(blue granules)
Large and pale.
Schüffner's dots
(red granules)
Morphology of
infected cell
Mature red cells
Reticulocytes
Reticulocytes and
mature red cells
Plasmodium malariae
Piasmodium ovale
Reticulocytes
Plasmodium falciparum
Affinity for
Plasmodium vivax
Morphological Appearances of Plasm odia in Red Cells
TABLE 4.10
Like P. vivax
Like P. vivax
Like P. vivax
Not seen
Elongated, kidneyshaped, reddish-blue
cytoplasm with scattered
red chromât in.
Red cell remnant
in concave area
Deep blue crescentshaped (10 X 3 Mm)
cytoplasm. Compact
red nucleus near
centre
Irregular, cluster
of approximately 16
small (1.5-2.0 Mm)
blue bodies each
with a bright red
dot
Oval nearly fills
the red cell. Pale
blue cytoplasm.
Diffuse pale pink
nucleus
Oval nearly fills
the red cell. Dark
blue cytoplasm.
Compact deep red
nucleus at periphery
Schizont
Microgametocyte
(male)
Macrogametocyte
(Female)
Table 4.10 cont.
Like P. vivax with
abundant brown
pigment
Like P. vivax but
smaller
Daisy-head. Central
green pigment surrounded by 8 small
blue bodies each
with a bright red dot
THE PERIPHERAL BLOOD FILM
red blood cells and initiate the erythrocytic phase of the life cycle. P.
vivax and P. ovale have an affinity for reticulocytes and young erythrocytes and P. malariae for aged red cells. P. falciparum is indifferent to
the red cell it invades; it enters reticulocytes and young or aged red
cells. G6PD deficiency and Hb-S partially protect the heat against P.
falciparum Hb-E against P. vivax and Hb-F against all plasmodia
(Allison, 1963).
The developmental stages of the malarial parasite within the red cell
(erythrocytic schizogony) are termed trophozoite and schizont. In the
early trophozoite stage the parasite is ring shaped (see Plate 17a). It
feeds on the haemoglobin and derives its energy by glucose phosphorylation; the haemoglobin is incompletely metabolized and residues of
glob in and haematin remain. In the late trophozoite stage the parasite
has grown, occupies more than half of the red cell and has an irregular
shape due to amoeboidal movement (see Plate 17b). The schizont
(multiplication) stage begins with radial segmentation of the parasite
which almost fills the red cell. Division into a number of small round or
oval cells (1.5-2 μηι in diameter) termed merozoites is usually
completed within 48 hours (72 hours for P. malariae) from the initial
invasion of the red cells. Rupture of the merozoite-filled red cells is
followed by a new erythrocytic cycle due to invasion of further red
cells by liberated merozoites that have not succumbed to immunological processes of the host. After two to three erythrocytic cycles,
gametocytogenesis occurs. Gametocytes are the sexual cells which
remain inactive in human blood. They are incapable of reproduction
until they are ingested by the female Anopheles mosquito. Fertilization
takes place in the insect's intestines; the oöcyst ruptures into the body
cavity and the released sporozoites migrate to the salivary glands.
The Romanovsky-stained malarial parasite has a blue cytoplasm and
a red nucleus. The morphology of the four parasites in the different
erythrocytic stages is summarized in Table 4.10. Because of insignificant cross-immunity double infection may occur and a blood sample
may show P. vivax and P. falciparum. Only the early trophozoite (ring
forms) and crescent-shaped gametocytes of P. falciparum are seen in the
peripheral blood because falciparum-infected red cells tend to sojourn
in capillaries and blood sinuses of internal organs.
56
5
Abnormal Leucocytes,
Plasma Cells and Platelets
CLASSIFICATION
Morphological abnormalities of leucocytes and plasma cells may be
classified into three categories: nuclear, cytoplasmic and nucleocytoplasmic abnormalities (Table 5.1). The group of atypical cells
characteristically seen in infectious mononucleosis, the Sézary cell of
mycosis fungoides and the neoplastic cell of leukaemic reticuloendotheliosis are classified in this book as 'atypical monocuclear' cells.
Abnormal platelets may be classified in a similar manner to abnormal
red cells. However, anticoagulants, temperature, surface contact and
other factors influence their morphology in the stained film and
TABLE 5.1
Abnormal Leucocytes, Plasma Cells and Platelets
A bnormal granulocytes
Nuclear abnormalities
Pelger-Huët anomaly
Hypersegmented neutrophil and macropolycyte
Twinning deformity
Cytoplasmic abnormalities
Vacuolation of cytoplasm
Hypogranular polymorphs
Agranular neutrophil polymorphs
Toxic granules
Alder-Reilly granules
Chediak-Higashi-Steinbrinck anomaly
Dohle or Amato bodies
May-Hegglin anomaly
Erythrophagocytosis
L.E. cell
Nucleocytoplasmic abnormalities
Malignant neutrophil polymorphs
Necrobiotic neutrophil polymorphs
Disrupted granulocyte
57
THE PERIPHERAL BLOOD FILM
Table 5.1 cont.
Abnormal
monocytes
Nuclear abnormalities
Pelger-Huët anomaly
Segmented nucleus
Cytoplasmic abnormalities
Vacuolation of cytoplasm
Alder-Reilly granules
Chediak-Higashi-Steinbrinck anomaly
Erythrophagocytosis
'Tart* cell or nucleophagocytosis
Nucleocytoplasmic abnormalities
Malignant monocyte
Necrobiotic monocyte
Disrupted monocyte
Abnormal
lymphocytes
Nuclear abnormalities
Pelger-Huët anomaly
Notch nucleus
Radial segmentation
Twinning deformity
Cytoplasmic abnormalities
Vacuolation of cytoplasm
Alder-Reilly granules
Chediak-Higashi-Steinbrinck anomaly
Nucleocytoplasmic abnormalities
Malignant lymphocytes
Disrupted lymphocyte
Atypical mononuclear cells
Mononucleosis cells
Sézary cell
Leukaemic reticulo-endotheliosis (LRE) cell
Abnormal plasma cells
Nuclear abnormalities
Turk irritation cell
Intranuclear inclusions
Cytoplasmic abnormalities
'Buhot' cell
Saurocyte or flaming plasma cell
Thesaurocyte
Phagocytic plasma cells
Nucleocytoplasmic abnormalities
Malignant plasma cells
A bnormal Platelets
Macroplatelet or megathrombocyte
Microplatelet or microthrombocyte
Agranular or blue platelet
58
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
meaningful classification is difficult. Only abnormal platelet size and
agranular platelets are distinguishable.
ABNORMAL GRANULOCYTES
Nuclear abnormalities
Pelger-HiïètAnomaly (see Table 12.52)
The nucleus of the polymorphonuclear neutrophil (PMN) is shaped like
a peanut, a dumb-bell or a pair of spectacles (pince-nez type); the
chromatin is coarse and clumped. The cytoplasm shows the usual
granular appearance of the mature cell. This retarded segmentation of
the nucleus may be an inherited or an acquired anomaly. When
inherited (autosomal dominant), it is usually in the heterozygous form
and nuclear abnormalities may be recognized in monocytes and
lymphocytes; the funtional capacity of the cells is unaltered. The
'Stodtmeister' variant is a granulocyte with a round pomegranateshaped nucleus containing large fragments of chromatin. It has been
described in a family with the homozygote form of the anomaly and is
not seen in the hétérozygote. The acquired or 'pelgeroid' anomaly (see
Plate 18) is seen in various disorders (see Table 12.52); the functional
and cytochemical characteristics of these cells may be abnormal.
Hypersegmented neutrophil and macropolycyte(see Table 12.53)
The nucleus of the hypersegmented PMN consists of six or more
lobes which may be twisted, lie without an obvious pattern or may
radiate from a common point of convergence. Norberg (1969) reported
that the latter appearance may be an in vitro artefact and a
manifestation of radial segmentation of leucocyte nuclei, a
phenomenon occurring when anticoagulated blood has stood for some
time before the film is prepared. The 'macropolycyte' is a large
hypersegmented PMN with a diameter greater than 14 Mm(see Plate 19).
As discussed earlier, the number of lobes in a PMN is not a reflection of
cell age. Hypersegmentation may result from abnormal development of
precursor cells in the bone marrow; it may be due to tetraploidy of the
nucleus and not to maturation from the 'giant' metamyelocyte which
may not be capable of further maturation (Chanarin, 1969).
Twinning deformity
The PMN contains two segmented nuclei which are not connected
by chromatin filament; the cell may be larger than normal. The
abnormality may be associated with hypersegmentation and occurs
with other bizarre types of segmentation in paramyeloblastic
leukaemia.
59
THE PERIPHERAL BLOOD FILM
Cytoplasmic abnormalities
Vacuolation öf cytoplasm
Various sized, non-specific vacuoles are present in the neutrophilic
PMN cytoplasm. They occur in severe infections and in anticoagulated
blood that has stood for some time before the film is prepared.
Iipid-containing vacuoles occur in Jordans' anomaly (Jordans, 1953)
and Niemann-Pick's disease (sphingomyelin lipidosis). Vacuolated
eosinophils may be seen in myeloid and myelomonocytic leukaemia.
Hypogranular polymorph
The hypogranular PMN has a segmented nucleus and a cytoplasm
with pale azurophilic stippling. The number of specific neutrophilic
granules is reduced and may not be readily observed between the larger
than normal azurophilic granules. The peroxidase and chloroacetate
esterase reactions are positive; alkaline phosphatase activity is reduced
or absent. The PAS reaction is positive but weaker than normal.
Hypogranular PMN are characteristically seen in myeloid and
myelomonocytic leukaemia. Reduction of the specific granule content
appears to represent a failure in their development during otherwise
normal maturation of the cytoplasm (Hayhoe and Cawley, 1972).
Hypogranular eosinophils may also be noticed in these leukaemias;
vacuolation is present and the pale blue cytoplasm may be observed
between the granules and vacuoles.
Agranular neutrophil polymorph
The agranular PMN has a segmented nucleus and a pale blue
cytoplasm devoid of any granules. Cytochemically, the peroxidase
reaction may be weak or absent and no acetate esterase or phosphatase
activity is demonstable. The PAS reaction may be weaker than normal.
The agranular polymorph is characteristically seen in acute myeloid and
myelomonocytic leukaemia. It probably develops from malignant
precursor cells by asynchronic maturation of the nucleus and
cytoplasm. The Romanovsky-stained cell may be mistaken for a monocyte. However, the agranular PMN is smaller than a monocyte; cytochemically the naphthyl acetate esterase is negative in the PMN and
positive in the monocyte.
Toxic granules (see Table 12.54)
Toxic granules appear as coarse blue-black or dark purple stipples in
the PMN cytoplasm. When small in size the granules are distributed
among the fine pink specific granules; when large in size only a few
specific granules may be evident. Toxic granulation of PMN is
associated with increased cytoplasmic basophilia and irregular nuclear
staining. The peroxidase reaction of the cell may be weaker than
normal.
60
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
Alder-Reilly granules (see Table 12.54)
Alder-Reilly granules are prominent lilac-coloured or azurophilic
granules which are seen in the PMN of subjects with certain types of
genetic disorders. The granules are larger than the specific granules, are
distributed throughout the cytoplasm and may be so numerous as to
partly obscure the nucleus. The granules are peroxidase negative and
PAS positive; metachromatic staining has been reported as positive and
negative (Brunning, 1970).
The Alder-Reilly granules in eosinophils are violet coloured and
similar in appearance to the specific granules of basophils;
distinguishing between eosinophils and basophils may be difficult in
these genetic disorders (Brunning, 1970). The colour of the anomalous
granules in basophils is the same as the basophilic granules but the
anomalous granules are larger and more numerous.
Chediak-Higashi-Steinbrinck anomaly
The cytoplasm of the granulocytes contains giant anomalous
granules; they are grey, blue, green or orange in PMN, polymorphic in
eosinophils and basophils. Similar inclusions may be seen in monocytes
and lymphocytes. The anomalous granules in the PMN are peroxidase
and PAS positive; they may contain acid phosphatase. The
Chediak-Higashi-Steinbrinck syndrome is an hereditary disorder
(autosomal recessive) associated with albinism.
Dohle orAmato bodies (see Table 12.55)
A Dohle body is a blue-staining pyroninophilic structure,
approximately 2 μπι in diameter, with an irregular poorly defined
margin. It appears only in PMN and one or two bodies may be observed
near the periphery of the cytoplasm; toxic granulation may also be
evident in the same cell. Pathogenesis of the Dohle body is speculative.
It contains RNA and electron microscopy shows that the inclusion is
composed of rough endoplasmic reticulum concentrated together as
strands in ill-defined areas of the cytoplasm (Cawley and Hayhoe,
1972). According to these authors the Dohle body may represent a
focal failure of cytoplasmic maturation, as precursor cells (myelocytes)
contain appreciable amounts of rough endoplasmic reticulum often
arranged in a similar fashion.
May-Hegglin anomaly
The May-Hegglin anomaly is a blue-staining, pyroninophilic, spindle
or crescent-shaped structure measuring 2-5 μιη. It has a well-defined
margin and is located near the periphery of the cell cytoplasm. More
than one inclusion may be observed; the remaining cytoplasm appears
normal. The anomaly may be found in granulocytes and monocytes but
not in lymphocytes. The structure is peroxidase negative. It is also PAS
61
THE PERIPHERAL BLOOD FILM
negative and appears as a clear area against the strong positive
cytoplasmic background (Cawley and Hayhoe, 1972). Electron
microscopy shows that the inclusion may be incompletely surrounded
by a strand of rough endoplasmic reticulum and is composed of RNA
fibrils and small spherical particles which may be ribosomes (Cawley
and Hayhoe, 1972). The May-Hegglin anomaly is inherited as an
autosomal dominant trait and is associated with the presence of giant
platelets and varying degrees of thrombocytopenia.
Erythrophagocytosis
PMN with an ingested red cell may be seen in buffy coat films of
anticoagulated venous blood from patients with auto-immune
haemolytic anaemia, paroxysmal nocturnal haemoglobinuria and
haemolytic anaemias associated with septicaemia. Erythrophagocytosis
may also be observed in films prepared for detecting the L.E cell
phenomenon; in this case it is of no significance.
LE. cells (see Plate 20)
The L.E. cell is a PMN distended by a large round homogenous
reddish-purple mass (the L.E. body); the darker segments of the PMN
nucleus are displaced to the periphery of the cell and may partly
encircle the inclusion. The L.E. body is composed of phagocytosed
nuclear material derived from dead or traumatized PMN; it shows no
nuclear detail but is Feulgen positive, in the film the L.E. cell may be
associated with purplish irregularly shaped 'extracellular material'
(ECM), similar in composition to the L.E. body and with PMN clusters
forming rosettes around this ECM.
The L.E. cell is not present in circulating blood. It is an in vitro
phenomenon; the L.E. factor, serum complement and denuded nuclei
of dead or traumatized PMN are essential for its development in
defibrinated blood incubated at 37°C. The L.E. factor releases the
enzyme deoxyribonuclease from a complex with its inhibitor. The
enzyme destroys the chromatin structure of the denuded nuclei,
depolymerizing the nucleoprotein; the nuclear membrane ruptures and
the liberated nuclear material assumes an irregularly shaped
homogenous and swollen mass. The L.E. factor also stimulates the
metabolically active PMN to phagocytose this transformed nuclear
material which after ingestion by the PMN becomes the L.E. body.
The L.E. cell phenomenon may be demonstrated by a variety of
techniques in 80 per cent of patients with systemic lupus
erythematosus (SLE), occasionally in other connective tissue disorders,
in patients with penicillin reactions and in women taking oral
contraceptives; the phenomenon does not occur in discoid lupus
erythematosus. Nearly all patients with SLE and some patients with
62
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
other connective tissue disorders (Schur, 1970) possess antinuclear
factor (ANF) in high titre. The term antinuclear factor refers to a group
of auto-antibodies, predominantly of IgG type but occasionally of IgA
or IgM type, that may react with whole nuclei, DNA, soluble and
particulate deoxyribonucleoprotein or DNA-histone. The antibodies
may have been produced against DNA liberated into the circulation
(Tan, Schur and Carr, 1966); they may be detected by an
immunofluorescent technique using bare granulocytic or lymphocytic
nuclei but preferably rat-liver nuclei. Presence of an auto-antibody,
however, is not synonymous with a disease process; up to 40 per cent
of healthy subjects over the age of 60 years may have weak ANF in
their serum (Whittinghameiu?/., 1969).
Nucleocytoplasmic abnormalities
Malignant neutrophil polymorphe
The appearance of malignant PMN ranges from cells with normal
morphology to cells with abnormal nuclei (pelgeroid cells) and/or
granular composition (hypogranular and agranular cells). All malignant
PMN show metabolic features of abnormal development (Stuart, 1972;
Hayhoe and Cawley, 1972; Pedersen and Hayhoe, 1971) and relative
cytoplasmic immaturity. Alkaline phosphatase activity is diminished or
absent, glycogen content is reduced and phagocytic capacity is poor.
The cells seen in Philadelphia chromosome-negative myelocytic
leukaemia and in myelomonocytic leukaemia are commonly associated
with high serum levels of lysozyme (muramidase).
Necrobiotic neutrophil polymorphs
Necrobiotic PMN may be smaller than normal cells. Due to
chromatin liquefaction, the lobes appear as dense dark violet globules,
the number corresponding with the number of lobes in the
disintegrating cell. At a more advanced stage of necrobiosis, the
globules may break up into several small drops or coalesce to form a
single large mass located eccentrically in the cytoplasm which may be
vacuolated. Necrobiotic PMN are commonly seen in films prepared
from anticoagulated blood which has stood for some time. They may
be observed in fresh blood films from subjects with myeloid or
myelomonocytic leukaemia.
Disrupted granulocytes
The disrupted granulocyte is larger than normal because of
cytoplasmic spreading. The nuclear segments are crushed and appear as
irregular, blue-violet smudges or 'shadows'. The specific granules are
usually undamaged and those of the eosinophil are dispersed in the
vicinity of the crushed nucleus. Disruption of granulocytes occurs
during film preparation and may be seen in the leukaemias.
63
THE PERIPHERAL BLOOD FILM
ABNORMAL MONOCYTES
Nuclear abnormalities
Pelger-Hu'êt anomaly
The monocytic nucleus is less indented and irregular in shape; the
chromatin is denser than normal. The anomaly is associated with the
more readily recognizable anomaly affecting the PMN nucleus and
never occurs by itself.
Segmented nucleus
The monocytic nucleus is segmented by a number of deep
indentations; radial segmentation is present if the segments appear to
radiate from a point of convergence. Segmented nuclei commonly
occur as an in vitro artefact in anticoagulated blood that has stood for
some time before film preparation. Pathological segmentation is seen
when there is an increased number of monocytes in the blood, in
Hodgkin's disease and in myelomonocytic leukaemia. Polymorphoid
monocytes may be mistaken for PMN and difficult to distinguish from
agranular PMN. The combined esterase technique (cf. Appendix A) is
the most useful cytochemical means of differentiation.
Cytoplasmic abnormalities
Vacuolation of cytoplasm
One or more vacuoles are commonly seen in the cytoplasm of
monocytes. They are colourless with sharp outlines and are usually in
vitro artefacts, forming when anticoagulated blood has stood for some
time before film preparation.
Alder-Reilly granules (see Table 12.54)
Lilac-coloured Alder-Reilly granules similar to those seen in PMN
may be observed in monocytes of subjects with the genetic
mucopolysaccharidoses.
Chediak-Higashi-Steinbrinck anomaly
In the Chediak-Higashi-Steinbrinck syndrome the cytoplasm of some
monocytes may contain yellow to yellow-orange granules, measuring up
to 3 μιη in diameter, and resembling ingested red cell fragments
(Brunning 1970). This granular anomaly is associated with giant
granules in PMN.
May-Hegglin anomaly
Basophilic inclusions similar to those in PMN may be observed in
monocytes (Cawley and Hayhoe, 1972). However, they may not be
readily recognized against the basophilic background of the monocyte's
cytoplasm.
64
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
Erythrophagocytosis
Monocytes with engulfed erythrocytes may be seen in buffy coat
smears from patients with auto-immune haemolytic anaemia,
paroxysmal nocturnal haemoglobinuria and haemolytic anaemias
associated with septicaemia. Erythrophagocytosis may also be observed
in films prepared for L.E. cell detection.
'Tart' cell or nucleophagocytosis
The 'Tart' cell, named after the patient in whom it was first
observed, is commonly a monocyte with an engulfed lymphocyte
nucleus; the inclusion still retains its chromatin pattern and shows no
nuclear digestion. At times the ingested nucleus may appear
homogenous and resemble an L.E. body; however, the surface is rarely
smooth and there may be a denser staining rim. Nucleophagocytosis is
an in vitro phenomenon which may be seen in buffy coat films from
subjects with drug allergy. It is commonly observed in films prepared
for L.E. cell detection; the significance of the 'tart' cell in this
preparation is unknown.
Nucleo-cytoplasmic abnormalities
Malignant monocyte (see Plate 5.4a, b)
The malignant monocyte is larger than the normal cell. Its outline is
often irregular due to ruffling of the surface membrane or to the
presence of short pseudopodal projections. In some cells the cytoplasm
may appear divided into two zones; an outer transparent area free of
granules, and an inner ground-glass or frosted area filled with granules.
An occaional vacuole may be present in the cytoplasm. The nucleus is
large and may have a bizarre shape; it may be polymorphoid or show
radial segmentation. Nucleoli are inconspicuous and the chromatin is
fine and reticulated. Cytochemically the peroxidase, alkaline
phosphatase and chloroacetate esterase reactions are negative while the
naphthyl acetate esterase and the acid phosphatase are positive. The
PAS reaction is variable; it may be negative in some cells or a few
magenta granules may be seen in other cells. The cell is distinguished
from the leukaemic reticulo-endotheliosis (LRE) cell by ascertaining
the effect of L^+^ tartaric acid on the acid phosphatase reaction in the
cell; the reagent inhibits the enzyme reaction in the monocyte but not
in the LRE cell (Yam, Li and Lam, 1971).
Malignant monocytes occur in myelomonocytic leukaemia and are
associated with high serum levels of lysozyme (muramidase), the
concentration depending on the number of circulating monocytes.
Lysozyme is an aminopolysaccharidase which hydrolyses mucopolysaccharides in cell walls of a variety of micro-organisms, resulting in cell
lysis. It is present in many biological fluids, in the monocytic series of
65
THE PERIPHERAL BLOOD FILM
cells and in neutrophil granulocytes except the myeloblast. The serum
concentration may be measured by turbidimetric or agar plate diffusion
techniques using the killed cells of Micrococcus lysodeikticus. The
enzyme may also be demonstrated cy to chemically by histobacterial,
immunocytochemical or immunofluorescent procedures. Determination
of serum lysozyme concentration is of value in the diagnosis of
myelomonocytic leukaemia. However, the prognostic value of serial
determinations during chemotherapy is controversial.
Necrobiotic monocyte
A necrobiotic monocyte may show a nucleus perforated with holes
or one in which the chromatin has disintegrated into various sized
fragments. At a later stage of liquefaction the nucleus may be replaced
by a large dark violet globular mass located eccentrically in the
cytoplasm which is vacuolated.
Disrupted monocyte
The disrupted monocyte may consist of a denuded boomerangshaped nucleus with compacted chromatin or a 'basket' cell composed
of a fibrillary network of pale purple material with or without an
attached nucleus. Disruption occurs when the film is prepared from
anticoagulated blood that has stood for some time.
ABNORMAL LYMPHOCYTES
Nuclear abnormalities
Pelger-Hu'èt anomaly
The chromatin of the lymphocyte nucleus appears more clumped than
usual. The anomaly is associated with the more readily recognizable
anomaly affecting the PMN nucleus and never occurs by itself.
Notch nucleus (see Table 12.56)
This is an exaggeration of the Rieder form of nucleus. The nuclear
indentation may be so great that it appears as a large V-shaped cleft
almost dividing the nucleus. It is commonly seen in the large
lymphocytes and immature cells in lymphatic leukaemia. It may
develop in normal lymphocytes after exposure of lymphatic tissue to
irradiation.
Radial segmentation
The lymphocyte nucleus is segmented, the segments appearing to
radiate from a point of convergence like the leaflets of a clover-leaf
(Norberg and Söderström, 1967). The anomaly may be seen in
lymphatic leukaemia. However, it is commonly observed as an artefact
66
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
of normal lymphocytes when the film is prepared with anticoagulated
blood that has stood for some time.
Twinning deformity
Two nuclei, one often smaller than the other, may be seen in
lymphocytes of patients with viral infections and lymphatic leukaemia.
The deformity may develop after exposure of lymphatic tissue to
irradiation. It is rarely seen in normal blood.
Cytoplasmic abnormalities
Vacuolation of cytoplasm (see Table 12.57)
The cytoplasm of the lymphocytes may contain small vacuoles with
sharp, clear-cut edges or large vacuoles with indistinct outlines; the
latter type of vacuolation gives the cytoplasm a foamy appearance. In
Niemann-Pick disease, the vacuolated lymphocytes are more prominent
in younger patients and this is associated with the presence of a
characteristic foamy histiocyte (the Niemann-Pick cell) in haemopoietic
and lymphoid tissue. In Tay-Sachs and Batten-Spielmeyer-Vogt
diseases the number and size of the vacuoles increase with prolongation
of the diseases (Brunning, 1970). The PAS staining of the vacuoles in
the lipidoses is variable; it is positive in the acquired atypical
lymphocyte and is most intense in the lymphocytes of Pompe's disease.
Alder-Reilly granules (see Table 12.54)
Prominent lilac-coloured or azurophilic granules are present in the
cytoplasm of lymphocytes. The granules are similar to those seen in the
PMN of subjects with certain types of genetic disorders.
Chediak-Higashi-Steinbrinck anomaly
The cytoplasm of the lymphocytes may contain single or multiple
red inclusion bodies measuring up to 4 Mm in diameter. The anomaly
together with those observed in the neutrophils and monocytes is
associated with albinism.
Nucleocytoplasmic abnormalities
Malignant lymphocytes
Malignant 'small' and 'large' lymphocytes have slightly larger and
more dense nuclei than their normal counterparts. Their cytoplasm may
be decreased and appear more basophilic. No esterases or alkaline
phosphatase activity are demonstrable. The acid phosphatase reaction is
weaker than normal and iso-enzyme 3 is prominent (Yam, l i and
Crosby, 1971). The PAS reaction in individual cells is variable. The PAS
score in lymphocytic leukaemia is higher than normal while in
lymphoblastic leukaemia it is within or less than the normal limit
probably because many of the blood lymphocytes are derived from
67
THE PERIPHERAL BLOOD FILM
PAS-negative malignant lymphoblasts (Hayhoe and Cawley, 1972).
Malignant lymphocytes may be associated with the 'lymphosarcoma'
cell. The leukaemic reticulo-endothelial (LRE) or 'hairy' cell may be
misdiagnosed as a lymphocyte.
Disrupted lymphocyte
A disrupted lymphocyte is commonly referred to as a 'smudge' cell.
The lymphocyte has lost its cytoplasm and the denuded nucleus
assumes an irregular shape with blurred edges, the so-called 'Gumprecht
shadow'. This artefact is commonly observed in blood films of subjects
with high lymphocyte counts and particularly in lymphatic leukaemia.
It is suggestive of increased cellular fragility and occurs when the blood
film is being prepared.
ATYPICAL MONONUCLEAR CELLS
Mononucleosis cells
Mononucleosis cells are pleomorphic non-malignant mononuclear
leucocytes commonly seen in infectious mononucleosis (glandular
fever). Morphologically three types of cells may be recognized: the
'lymphocytoid', the 'plasmacytoid' and the 'monoblastoid'. The
lymphocytoid cell (see Plate 22a) is larger than a normal 'large'
lymphocyte. The cytoplasm is abundant and light blue and has a foamy
(vacuolated) appearance with an irregular basophilic outline. The
eccentrically located nucleus may be oval or reniform with coarse
clumped chromatin. Some cells may have a fenestrated (Osgood, 1935)
or 'Swiss cheese' (Ghaemi and Seaman, 1963) nucleus. The latter
authors considered this morphological anomaly to be due to the
development of intersecting intranuclear tunnels as an anticoagulant
artefact. Ultrastructurally the lymphocytoid cells resemble lymphocytes. However, their cytochemical reactions are not wholly
characteristic of this class of cells. The alpha naphthyl acetate esterase
and acid phosphatase reactions are strongly positive (similar to those
observed in monocytes — see Table 3.4) and in some cases the activity
of the latter enzyme is resistant to L^+^ tartaric acid (Yam, Li and Lam,
1971 ; Yam, l i and Finkel, 1972).
The plasmacytoid cell is larger than the previous type. The
cytoplasm is deeply basophilic and there may be a pale perinuclear
zone; the nucleus is round or coved and has a fine chromatin network.
The monoblastoid cell (see Plate 22b) is as large or larger than a normal
monocyte. The eccentric nucleus may be round, oval, reniform or may
have a scalloped border; the chromatin has a diffuse sieve-like pattern in
which small clumps may be seen. One, sometimes two nucleoli rimmed
with dense chromatin are commonly present. The cytoplasm is
68
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
abundant, basophilic and not usually vacuolated.
Mononucleosis cells are associated with the presence in serum of a
variety of antibodies: the heterophile Paul-Bunnell antibody which is
resistant to adsorption by guinea-pig cells, the Epstein-Barr (E-B) virus
antibody and 'cold' antibodies such as iso-immune anti-i and
'spontaneous' lymphocytotoxins which are distinct from the other
antibodies. The cells are not specific for infectious mononucleosis.
They may be seen in infections with various viruses and
micro-organisms (see Table 12.59); in these cases the serum test for
Paul-Bunnell antibody is negative. A positive serological test without
the accompanying haematological picture has also been reported (Table
5.2) in other disorders. The evidence linking the E-B virus as the
causative factor in infectious mononucleosis is not conclusive
(Bannatvala, 1970); the virus appears to be a common infectious agent
and high titre E-B virus antibody has been detected in other disorders
(Table 5.2).
TABLE 5.2
Positive Serological Tests in Disorders
other than Infectious Mononucleosis
Positive Paul-Bunnell heterophile antibody test
Hodgkin's disease
Lymphocytic leukaemia
Acute leukaemia
Tularaemia
Positive E-B virus antibody test (high titre)
Some healthy subjects
Burkitt's lymphoma
Hodgkin's disease
Lymphocytic leukaemia
Sarcoidosis
Sezary cell
The Sézary cell is double the size of a neutrophil polymorph. It has a
large reniform, convoluted or bi-lobed nucleus with a condensed
chromatin pattern. The pale blue cytoplasm is abundant and clear but
may be sparse with a ground-glass appearance from the presence of fine
granules. Vacuoles that react positively with the PAS reaction may be
seen in the perinuclear zone. The outline of the cell may be irregular
because of the pseudopodal projections of the cytoplasm.
Leukaemic reticulo-endotheliosis (LRE) cell
Synonyms for the leukaemic reticulo-endotheliosis (LRE) cell are
malignant reticulum cell or histiocyte, neoplastic lymphoid reticulum
69
THE PERIPHERAL BLOOD FILM
cell, 'hairy' cell and 'flagellated' cell. Morphologically the LRE cell
superficially resembles a lymphocyte but is approximately twice as
large. It is a round or slightly oval cell with a nucleocytoplasmic ratio of
1:1; occasionally elongated forms with tapering ends are seen. The
nucleus which may be centrally or eccentrically located, is round, oval
or slightly indented. The chromatin appears spongy with a lacy pattern;
the strands are coarser than those in 'blast' cells, more granular than
those of monocytes and less clumped than those of lymphocytes.
Nucleoli are infrequent and indistinct; however, one may be seen. The
cytoplasm is sky-blue and may contain azurophilic granules. The cell
margin is irregular with a serrated or wind-blown appearance; this
feature is better appreciated when the blood film is stained at pH 7.2 7.4 (Yam, Li and Finkel, 1972). The 'hairy' appearance of the LRE cell
is particularly noted in wet preparations examined by phase contrast
microscopy; the cell margin appears irregular with many villous or
pseudopodal cytoplasmic projections up to 1 Mm in length.
Cytochemically the peroxidase, alkaline phosphatase and chloroacetate esterase reactions are negative. Various investigators have
reported naphthyl acetate esterase activity as being present or absent.
The PAS staining varies from weak to moderate in the different cells.
Weak pyroninophilia may be demonstrable with the methyl green pyronin reaction. The acid phosphatase reaction, however, is strongly
positive but varies in intensity from cell to cell and from patient to
patient (Yam, Li and Lam, 1971; Yam, l i and Finkel, 1972).
According to these researchers the quantity and quality of this enzyme
allow the cell to be characterized and differentiated from other
leucocytes including monocytes. They showed by cytochemical and
disc acrylamide gel electrophoresis that the acid phosphatase in the
LRE cell was uniquely composed of L^+^ tartrate-resistant iso-enzyme 5.
The nature and origin of the LRE cell is not definitely established.
The cell lacks phagocytic activity. Transmission and scanning electron
microscopy has shown the LRE cell to be distinctly different from
normal and leukaemic lymphocytes (Trubowitz, Masek and Frasca,
1971). Further, the cytochemical reactions are not wholly typical of
either lymphocytes or monocytes. According to Yam, Li and Finkel
(1972) the LRE cell may be derived from sinusoidal endotheHal cells of
the reticulo-endothelial system.
ABNORMAL PLASMA CELLS
Nuclear abnormalities
Turk irritation cell
The Turk irritation cell is an atypical plasma cell which has also been
called a plasmacytoid lymphocyte and a virocyte. It measures 12-35 μτα
70
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
in diameter and may be round or oval in shape. The nucleus is usually
located eccentrically within the cell; it is round or oval with a
chromatin that is less coarse and clumped than normal. The cytoplasm
is deeply basophilic; a perinuclear halo or a few vacuoles may be
present. The Turk irritation cell is commonly seen in the peripheral
blood in viral infections and may appear in drug-induced allergic
reactions.
Intranuclear inclusions
Solitary or multiple bluish-grey round bodies, which may be rimmed
by dark material, may be present in the atypical plasma cell nucleus.
They are similar to the Russell bodies of the cytoplasm but can appear
independently of the latter. Plasma cells with intranuclear inclusions
may be seen in the bone marrow in myelomatosis, particularly IgA
myelomatosis. However, they are not diagnostic of this type of neoplasia (Drivishalm and Clausen, 1944) and may also be seen in nonmalignant plasmacytosis of the bone marrow.
Cytoplasmic abnormalities
'Buhot' cell
The 'Buhot' cell is a plasma cell containing numerous purple
inclusions of varying size and shape. Some of the inclusions may be
large, irregular and surrounded by clear vacuoles; they may stain
metachromatically. This atypical plasma cell is seen in the bone marrow
in the genetic mucopolysaccharidoses and is associated with the
Alder-Reilly granulation anomaly of leucocytes.
Saurocyte or flaming plasma cell
The saurocyte or flaming plasma cell has abundant cytoplasm which
may be pink or slate-grey with pink staining material at its periphery.
The intensity of the cell eosinophilia is influenced by the pH of the
staining reaction; a pH of 6.5 gives better results than a pH of 7.0
(Drivisholm and Clausen, 1964). The saurocyte is frequently seen in the
bone marrow in IgA myelomatosis but is not a specific or a diagnostic
feature of this disorder (Drivisholm and Clausen, 1964). It may also be
observed in other types of myelomatosis in non-malignant plasmacytosis and occasionally in normal bone marrow smears.
Thesaurocyte (see Hate 23)
The thesaurocyte is a large plasma cell with a small pyknotic nucleus
and abundant grey or pink cytoplasm compartmentalized by basophilic
trabeculae. The cytoplasm is PAS positive (diastase resistant) and the
trabeculae PAS negative. The thesaurocyte contains a large amount of
stored globulin with high carbohydrate content. This cell may be
71
THE PERIPHERAL BLOOD FILM
observed in the bone marrow in the same disorders in which saurocytes
occur.
Phagocytic plasma cells
Plasma cells are specialized protein-secreting cells. They are not
normally phagocytic but may develop this property under abnormal
conditions. Salmonella typhosum and Histoplasma capsulatum have
been seen within plasma cells respectively in the regional lymph nodes
(Goodpasture, 1937) and in bone marrow (Rohr and Bond, 1953).
Platelet phagocytosis by plasma cells has been reported in mumps
(Fames and Barker, 1968) and in children systemically exposed to
pokeweed (Barker, Fames and La Marche, 1967). Red cells
(Butterworth, Frommeyer and Riser, 1953), mature haemopoietic cells
and normoblasts (Abramson, von Kapff and Ginsburg, 1970), mature
haemopoietic cells, normoblasts and plasma cells (see Plate 24a, b, c)
have been seen within neoplastic plasma cells in bone marrow smears.
Morphological alteration and/or lysis of the phagocytosed cell is not
evident. The pathogenesis of plasma cell phagocytosis is not known.
Nucleocytoplasmic abnormalities
Malignant plasma cells
Morphologically, malignant plasma cells may appear similar to
normal cells. However, the nuclear chromatin is more dense and the
nucleus of some cells may have a bizarre appearance. Cytochemically
the ATPase activity in the cytoplasm may be decreased and 70-80 per
cent of the cells show a marked increase in acid acetate esterase activity
(Szmigielski, Litwin and Zupanska, 1965). Malignancy may be
suspected if the majority of the plasma cells have a uniform appearance
and/or are clumped together in the bone marrow smears.
ABNORMAL PLATELETS
Macroplatelet or megathrombocyte
A macroplatelet or megathrombocyte appears normal but has a
diameter greater than 4 μη\ . In some very large cells the centrally
packed granules may simulate a nucleus. Large platelets, sometimes
referred to as 'shift' platelets, are young platelets and functionally are
more active than normal size cells. Up to 5 per cent of the platelets in
the normal peripheral blood film are large Their number in the film can
be used as an index of active thrombopoiesis in the bone marrow
(Karpatkin, 1969, 1972) and as a prediction of the megakaryocyte
number (Garg, Amorosi and Karpatkin, 1971). Macroplatelets may occur
as an hereditary or an acquired anomaly. In myeloproliferative disorders,
particularly in essential thrombocythaemia, they may assume bizarre
72
ABNORMAL LEUCOCYTES, PLASMA CELLS AND PLATELETS
forms such as dumb-bell, Indian club or banana shapes.
Microplatelet or microthrombocy te
A microplatelet or microthrombocyte appears normal but has a
diameter less than 1.5 μηι. Up to 10 per cent of the platelets in the
normal peripheral blood film are small cells. Functionally microplatelets are old cells with reduced adhesive properties. They may occur as a
hereditary or an acquired anomaly.
Agranular or blue platelet
An agranular or blue platelet is commonly a cytoplasmic fragment of
an immature or atypical megakaryocyte. It is seen in films of subjects
with the hereditary May-Hegglin anomaly. Agranularity may also result
from cytopathic changes associated with platelet clumping due to
antibodies. Basophilic hyaline structures resembling agranular platelets
are seen in films showing many crushed mononuclear cells, especially
lymphocytes. These are pseudo-platelets and are cytoplasmic fragments
which have been dispersed in the vicinity of the disrupted cell.
73
6
Haemopoiesis
HAEMOPOIETIC COMPARTMENTS
The haemopoietic system consists of the red bone marrow and the
lymphatic organs. In the neonatal infant, red marrow occupies all
marrow cavities; in the adult it is found only in the sternum, ribs,
vertebrae, pelvic bones, flat bones of the skull and proximal portions
of the long bones of the upper and lower extremities. The lymphatic
organs are the thymus, spleen and lymph nodes; lymphatic tissue is
present in the walls of the gastro-intestinal and respiratory tracts, and
also occurs in the bone marrow. Haemopoiesis is an orderly progression
of cellular proliferation and differentiation from a primitive pluripotent
stem cell to the functional cells. A model of the origin and genesis of
haemopoietic cells is illustrated in Figure 4. Activity may be broadly
divided into three compartments: (1) the stem cell compartment
consisting of morphologically unrecognizable but funtionally identifiable cells which are the ancestral cells; (2) the 'poietic' or
differentiated cell compartment containing the morphologically
identifiable cells which by a process of reduction divisions finally
mature into the cells of (3) the functional cell compartment — red cells,
granulocytes, monocytes, lymphocytes and platelets.
STEM CELL COMPARTMENT
Stem cells have the capacity for self-renewal and for differentiation into
the various cell lines. They are a heterogenous group of cells and three
classes may be functionally recognized: (1) the pluripotent stem cell,
the most primitive ancestor of the haemopoietic cells; (2) the
multipotent stem cells of the 'myeloid' and 'lymphoid' group of cells;
and (3) the progenitor stem cells which are committed to a specific
developmental pathway and are antecedent to the 'blast' cells of the
differentiated cell compartment. Transition from the pluripotent to the
progenitor stem cells is normally associated with a diminishing capacity
for self-renewal and acquisition of differentiated cell characteristics.
74
B-lymphocyte
progenitor cell
T-lymphocyte
progenitor cell
Lymphoid stem
cell in thymus
Thrombopoietin
sensitive cell
Colony-forming
unit-culture
(CFU-C)
Lymphoid stem
cell in bone
marrow
Myeloid stem
cell in bone
marrow
Erythropoietin
sensitive cell
Pre-T-lymphocyte
in the thymus
Effector T-lymphocytes
in blood and tissues
Memory cells
Lymphoblast in
lymphatic tissue
T-lymphocytc in —
blood and tissues
Antigen-sensitive
1
Plasma cell in
lymphatic tissue
1
blood and tissues
/\iiiigeii-seiiMiivc
Platelets
Plasmablast in
lymphatic tissue
Pre-B-lymphocyte
in bone marrow
Megakaryoblast
Monocytes
Monoblast
Figure 4. Haemopoiesis
HZ
Granulocytes
Red cells
Myeloblast
Pro-erythroblast
*J
<
c
THE PERIPHERAL BLOOD FILM
Pluripotent stem cell
The pluripotent stem cell is of mesenchymal origin. Antenatally it
originates extra-embryonically in the blood islands of the yolk-sac; it
soon migrates and establishes itself in the liver, then in the spleen, bone
marrow and thymus. Postnatally it is located principally in the bone
marrow. While the cell has not been morphologically recognized in
sections, smears or imprints of red marrow tissue, modern techniques
have clearly shown that the pluripotent stem cell is not identical with
the 'reticulum' cell in haemopoietic tissue. Existence of the pluripotent
stem cell in the bone marrow of mice has been functionally
demonstrated by the spleen colony assay (Till and McCulloch, 1961).
In this assay, mouse bone marrow is injected intravenously into a
second lethally irradiated mouse; after 9 days, colonies of haemopoietic
cells are found in the spleen. The pluripotent stem cell is also referred
to as a 'colony-forming unit-spleen' (CFU-S). In the bone marrow it
may be in a quiescent and/or actively proliferating state. It
differentiates into the multipotent 'myeloid' and 'lymphoid' stem cells;
it also migrates via the blood stream to the thymus where it becomes
the T-lymphocyte ancestral cell. The inductive stimulus for
differentiation of the pluripotent stem cell into the multipotent stem
cells is not known. Intracellular and short range environmental factors
may play a role in this process.
Multipotent 'myeloid' and 'lymphoid' stem cells
Experiments have shown the existence of 'myeloid' (red cells,
granulocytes, monocytes, platelets) and 'lymphoid' (T-,Blymphocytes) stem cells. The myeloid and B-lymphocyte stem
cells are located in the bone marrow; the T—lymphocyte stem cell is in
the thymus. These cells appear to be induced by a 'determination step'
to further differentiate into the progenitor or committed stem cells
which proliferate along specific and restrictive pathways (Metcalf and
Moore, 1971). Micro-environmental factors such as the microcirculation
and non-haemopoietic cells in specialized regions of the haemopoietic
system appear to play an important role in this differentiation.
Progenitor or committed stem cells
There is experimental evidence that the progenitor or committed
stem cells derived from the 'myeloid' multipotent stem cell are sensitive
to humoral regulators which influence their rate of proliferation and
development into 'blast' cells. The red cell progenitor is activated by
erythropoietin, the granulocytic-monocytic progenitor cell or 'colonyforming unit-culture' (CFU-C) by colony-stimulating factor and
platelet progenitor by thrombopoietin. Humoral regulation of the
76
HAEMOPOIESIS
T—lymphocyte progenitor cell by thymosin is controversial. Regulation
of the B—lymphocyte progenitor cell is not known.
Erythropoietin
Erythropoietin appears to be generated principally by the enzymic
action of renal erythropoietic factor (REF) on an inactive protein
factor (erythropoietin precursor) present in the plasma. Erythropoietin
concentration in the plasma depends on (1) the oxygen tension in the
tissues, particularly in the kidneys, which in turn is governed by the
quantity, quality and oxygen affinity of haemoglobin; and (2) other
endocrine hormones. It is decreased in polycythaemia and increased in
anaemia. Erythropoietin may be demonstrated by injecting the test
material, e.g., serum or urine, into mice whose endogenous
erythropoietin production and erythropoietic activity have been
suppressed by anoxia or by hypertransfusion of red cells. Renewed
erythropoietic activity is usually detected by measuring the
incorporation of radio-iron into red cells.
Colony-stimulating factor
Colony-stimulating factor may be demonstrated by carrying out in
vitro colony-forming assay techniques (Bradley and Metcalf, 1966;
Pluznick and Sachs, 1965). Haemopoietic cell suspensions, e.g., bone
marrow aspirate, are cultured under suitable conditions in semi-solid
agar. Colonies of granulocytes and macrophages appear within 7-10
days if the colony-stimulating factor is present in a 'feeder' layer below
that of the culture layer. The number of colonies depends on the
concentration of the colony-stimulating factor in this feeder layer. This
factor is present in serum, urine, embryonic tissue cells and in
myelo-monocytic leukaemic cells. According to Metcalf and Moore
(1971), the urinary factor tends to produce macrophagic colonies and
the factor from myelomonocytic leukaemic cells, granulocytic colonies.
Thrombopoietin
Thrombopoietin has been found in the plasma of recently bled or
splenectomized animals. It may be demonstrated by measuring the rise
of platelet count after injection of the test material, e.g., plasma, into
an animal. Instead of the platelet count, the uptake of 7 *Se labelled
methionine may be used, as this amino acid is incorporated into the
cytoplasm of immature megakaryocytes.
THE 'POIETIC OR DIFFERENTIATED CELL COMPARTMENT
Types and sites of 'poietic' activity
The poietic or differentiated cell compartment contains morphologically identifiable cells exhibiting mitotic activity and maturation
77
THE PERIPHERAL BLOOD FILM
processes. The poietic cells originate with the progenitor-derived 'blast'
cell and, after a series of amplification steps, terminate with the
precursors of blood cells. The production pathways for red cells,
granulocytes, monocytes, platelets, lymphocytes and plasma cells are
respectively termed erythropoieses, myelopoiesis (granulocytopoiesis),
monopoiesis, thrombopoiesis, lymphopoiesis and plasmapoiesis. The
first four cell series are normally located in the bone marrow, the
B-lymphocyte and plasma cell series in the bone marrow and lymphatic
organs, and the T-lymphocyte series in the thymus and lymphatic
organs. Lymphopoiesis takes place in two phases, a primary and a
secondary. Primary lymphopoiesis in the bone marrow and thymus is
concerned with the production of antigen-sensitive B-lymphocytes and
T-lymphocytes respectively. Secondary lymphopoiesis and plasmapoiesis occur in the lymphatic organs. Plasma cell production also takes
place to a small degree in the bone marrow.
General characteristics of 'blast' cells
The blast cells which initiate the production pathways of the various
cell lines are called pro-erythroblast, myeloblast, monoblast,
megakaryoblast, lymphoblast and plasmablast. Except for the
megakaryoblast, which is a large cell, the blasts measure 15-20 Mm in
diameter. Because of the rich content of ribonucleic acid (RNA), the
cytoplasm is deeply basophilic. The degree of basophilia varies in the
different cells and is proportional to the RNA content; the greater the
amount of cytoplasmic RNA the deeper is the basophilia. Granules are
not usually present in the cytoplasm. The nucleus is large, has a spongy
appearance and is composed of fine chromatin threads forming a
lace-like network; one or more nucleoli are usually evident.
Morphological changes in cells
Sequential mitotic divisions of the blast cells and their derivatives,
and maturation of the non-dividing pool of cells are associated with
changes in the cytochemistry and morphological appearance of the cells.
The changes common to all series are (1) reduction of the
nucleocytoplasmic ratio, (2) disappearance of nucleoli, (3) clumping of
nuclear chromatin, (4) increase in the strength of the Feulgen reaction
of the nucleus, (5) decrease in cytoplasmic basophilia, and (6) gradual
appearance of, and increase in morphological markers characteristic of
the functional cells, for example, haemoglobin in the red cells and
specific granules in the granulocytes. For convenience of description
the pathway of each cell series is divided into stages according to morphological criteria. However, transition between the stages is gradual and
cells intermediate between two consecutive stages may be observed.
78
HAEMOPOIESIS
FUNCTIONAL CELL COMPARTMENT
Red cells, granulocytes (neutrophil polymorphs, eosinophfls, basophils),
monocyte-macrophages, lymphocytes, plasma cells and platelets belong
to this compartment. They are discussed in Chapter 3.
79
7
Erythropoiesis
NORMAL ERYTHROPOIETIC CELLS
Normoblastic erythropoiesis: stages and cell changes
In the post-natal period, erythropoiesis takes place extravascularly and
normally only within the bone marrow. It is stimulated by
erythropoietin and hormones such as androgens, thyroxine and growth
hormone; it is inhibited by oestrogens and progesterone. Apart from
the reticulocyte which is anucleate, immature red cells are nucleated
and are generally referred to as erythroblasts. Normal erythropoietic
cells are termed normoblasts and comprise approximately 25 per cent
of the nucleated cells in the bone marrow. Hie developmental stages
are: pronormoblast, early (basophilic) normoblast, intermediate
(polychromatophilic) normoblast, late (orthochromatic) normoblast
and reticulocyte. The sequential morphological changes observed are
(1) reduction in the cell diameter and nucleocytoplasmic ratio, (2)
reduction in nuclear size until it becomes pyknotic and eventually
extruded from the cell, (3) alteration in the nuclear chromatin which
becomes coarse and clumped, and (4) alteration of the cytoplasmic
basophilia from a deep-blue to a greyish-pink or polychromatic colour
which becomes more eôsinophilic as the cell matures. This colour
change is due to a decrease in the RNA content and an increase in
haemoglobin concentration.
Haemoglobin synthesis is initiated, stimulated and regulated by
erythropoietin. It commences with progenitor cell differentiation into
the pronormoblast and the greatest synthetic activity takes place in the
intermediate and late stages of development. The haemoglobin
concentration within the cell cytoplasm has been proposed as the
regulator of the number of reduction divisions occurring during
erythropoiesis (Stohlman, 1967; Stohlman, et al 1968). According to
these authors DNA synthesis within the cells ceases when a critical
'cytoplasmic haemoglobin concentration' (CHC) is attained. Normally
this CHC is reached at the intermediate stage and mitotic activity is not
80
ERYTHROPOIESIS
observed in the late normoblasts. Erythropoiesis may thus be broadly
separated into a dividing or 'multiplicative' phase and a 'maturation'
phase {Figure 5). The reticulocyte of the latter phase is released from
the bone marrow into the circulation and completes its maturation to
the red cell in the spleen. The rate of reticulocyte release from the bone
marrow is regulated by erythropoietin.
Multiplicative phase
Pronormoblast
Early
^"normoblast
Intermediate
normoblast
Maturation phase
normoblast -Reticulocyte
-
Figure 5. Erythropoiesis
Morphology of normoblasts and reticulocyte
Pronormoblast (15-20 μιη)
The pronormoblast is a round cell with a large nucleus, a high
nucleocytoplasmic ratio and deeply basophilic cytoplasm in which no
granules or vacuoles are present. The nucleus is round and contains
nucleoli; the chromatin shows a fine reticular pattern. Cy to chemically
the Feulgen reaction is not intense. The peroxidase and PAS reactions
are negative. No free iron is demonstrable within the cytoplasm.
Early (basophilic) normoblast (10-15 μηι)
The cytoplasm of the early normoblast is deeply basophilic and
appears abundant. The nucleus is centrally located and nucleoli may
not be present; the chromatin is coarse and early clumping may be seen.
The Feulgen reaction of the nucleus is moderately intense. The other
cytochemical reactions including that for iron are negative.
Intermediate (pofychromatophilic) normoblast (8 -12 Mm) (see Plate 25)
The cytoplasm of the intermediate normoblast is greyish-pink due to
the presence of haemoglobin. The nucleus is round, usually centrally
located but may be in a slightly eccentric position; the chromatin is
coarse and condensed into nodular masses. The Feulgen reaction of the
nucleus is more intense than in the earlier cells. The other cytochemical
reactions are usually negative. A few siderotic granules may be seen in
the cytoplasm of an occasional cell; these represent iron that has not
as yet been utilized for haemoglobin synthesis.
Late (orthochromatic) normoblast (7-12 μπι) (see Plate 26)
The cytoplasm is more eosinophilic than its precursor cell because of
the greater haemoglobin concentration; however, it is not fully pink in
colour and exhibits a lesser shade of grey than the intermediate
normoblast. The nucleus has shrunk and is pyknotic with condensed
81
THE PERIPHERAL BLOOD FILM
chromatin and of homogenous appearance. The cytoplasm of an
occasional cell may contain a purple round Howell-Jolly body or may
show basophilic stippling. The nucleus and Ho well-Jolly body give an
intense Feulgen reaction. The basophilic stippling is commonly due to
the precipitation of RNA but may represent siderotic granules which
can be detected by the Prussian blue reaction. The other cytochemical
reactions, including the PAS, are usually negative. At this stage no
mitotic activity is seen and the late normoblast matures into the
reticulocyte by expulsion of the condensed pyknotic nucleus; a little
haemoglobinized cytoplasm is also lost during this process. The
extruded nucleus and cytoplasm are phagocytosed by local histiocytes.
Reticulocyte (10 μπι)
The reticulocyte is an anucleate bluish-grey or polychromatic cell.
The staining characteristics of the cell are due to the uniform
precipitation of the residual basophilic ribonucleoprotein throughout
the cytoplasm by the methanol of the Romanovsky stain. Some cells
may also contain fine dark blue granules if there is uneven precipitation
of the ribonucleoprotein (cf. Red cell with punctate basophilia in
Chapter 4). The residual RNA in a reticulocyte decreases as the cell
matures and is best detected by supravital staining techniques using
brilliant cresyl blue or new méthylène blue. In the younger cell it
appears as blue reticular filaments or numerous granules; in the older
cells only a few granules or scattered filaments are seen. The reticular
material cannot be seen by dark-ground illumination or by phase
contrast microscopy. The Prussian blue reaction is usually negative.
The specific gravity of the reticulocyte is lower than that of the red
cell; consequently it is found in the upper portion of the red cell
column when anticoagulated venous blood has been centrifuged. The
cell is more active metabolically than the red cell. Enzyme activity is
greater in reticulocytes and they can synthesize lipids, nucleic acids,
purine nucleotides, haem and globin chains. The concentration of
adenosine tripohosphate (ATP) and other organic phosphates is higher
in the reticulocyte than in the mature red cell.
Reticuolcyte count of blood
After 1 - 2 days in the bone marrow maturation pool, the
reticulocyte, under the influence of erythropoietin, is released into the
circulation. It migrates to the spleen where its maturation into the red
cell is completed. Bone marrow reticulocytes are younger, larger and
more basophilic than those seen in the blood. If, however, as a result of
erythropoietin, they are prematurely released into the blood, the
extramedullary maturation time is longer than normal; these
prematurely released cells are called 'shift' reticulocytes. The
82
ERYTHROPOIESIS
reticulocyte count of the peripheral blood is commonly expressed as a
percentage, the normal value being 1 t 0.6 per cent. It represents a
balance of the rate of reticulocyte release from the bone marrow
maturation pool, the degree of immaturity of these newly released cells,
and the disappearance rate of mature red cells from the blood. The
count is of diagnostic and prognostic value in anaemia. It may be used
as an index of the effectiveness of erythropoietic activity when adjusted
for variation in haematocrit (absolute count) and maturation time of
'shift' reticulocytes in the blood (Hillman and Finch, 1967, 1969).
Absolute reticulocyte
count(%)
Corrected reticulocyte
count (%)
_ ~u
,
. tnt. w Observed haematocrit
- Observed count (%)X
^
_
Absolute count (%)
Maturation time (days)
The reticulocyte maturation time in the blood is proportional to the
degree of anaemia, e.g., 1.5 days, 2 days, and 2.5 days for haematocrits
of 35 per cent, 25 per cent and 15 per cent respectively. If the normal
reticulocyte count is taken as 1 per cent the corrected count represents
the 'production index'; an index greater than 2 is suggestive of
increased erythropoietic activity.
Haemoglobin synthesis
Globin chain production
The haemoglobin molecule (mol. wt. = 65,000) consists of four
polypeptide chains of globin, each with an attached molecule of haem
(iron-protoporphyrin 9). The nomenclature of the chains and the
structure of the normal haemoglobins has been mentioned in Chapter 3.
The globin chains are synthesized in the cytoplasm by polysomes
located near the mitochondria. These polysomes build up the chains by
sequentially adding transfer-RNA-bound amino acids (a total of 141 for
alpha chains and 146 for beta chains) according to the instructions
coded from DNA, the carrier of genetic information. The amino acid
composition and sequences in the different chains are not identical. All
chains form an alpha-helix (a right-handed coil, shaped like a spring or a
spiral staircase), interrupted by non-helical segments. There are eight
helical regions, labelled A to H. Globin synthesis is controlled by a set
of genes, a separate gene for each chain type. In the adult the rates of
alpha and beta chain formation are synchronous (imbalance is seen in
the thalassaemic syndromes).
Haem synthesis {Figure 6)
Haem is a red iron-containing tetrapyrrolic pigment. The molecule
measures 14X 1 7 Â ( 1 Â= 10"7mm). The biochemical pathway for
its synthesis from glycine and succinylCoA is shown in Figure 6. Of the
83
THE PERIPHERAL BLOOD FILM
Mitochondrion
r
Glycine ♦ Succinyl
i
CoA
Haem
Iron (Fe**)
£ - A l A synthetase
t
Haem synthetase
Vitamin Bg
J-ALA
PBG
'
I
I
Protoporphyrin-9
>■ UPG
*~ CPG
► PPG
Figure 6. Haem synthesis (b-ALA, delta-amino levulinic acid; PBG, porphobilinogen; UPG; uroporphyrinogen; CPG, coproporphyrinogen; PPG; protoporphyrinogenj
enzymes catalysing the reactions, only delta-ALA synthetase and haem
synthetase are found in the mitochondrion and both require
pyridoxal-5-phosphate (vitamin B 6 ) as a co-enzyme. The final step in
the formation of haem, the incorporation of ferrous iron into the
porphyrin ring, takes place in the mitochondria. Haem synthesis
depends on the quantity and quality of the various enzymes which are
governed by gene action and on iron availability within the
erythroblasts. Erythropoietin and the final concentration of haem
appear to control the rate of synthesis. The former, whose action may
be mediated through cyclic adenosine 3', 5'-monophosphate (Bottomley
et αί, 1971), stimulates the production of delta-ALA synthetase. The
latter, acting through a feedback mechanism, influences the activity of
this enzyme, depressing or stimulating it when the haem concentration
is high or low.
Iron incorporation
Immature red cells obtain their iron for haem synthesis from the
plasma where iron is bound to its transport protein - transferrin synthesized by the parenchymal cells of the liver. This plasma iron
(Figure 7) represents a balance between iron absorbed in the
duodenum, iron derived from the storage sites (liver parenchymal cells
and reticulo-endothelial system), iron being transported to the liver
parenchymal cells and to erythroid tissue and iron lost in desquamating
epithelial cells and in menstrual blood in women of child-bearing age.
Extravascular transferrin, which is in equilibrium with plasma
transferrin, coats the surface of the erythroblasts. The iron-saturated
molecules attach themselves to specific receptor sites in the cell
membranes. The ferric iron is reduced to the ferrous state, possibly
with the aid of ascorbic acid, and becomes firmly bound to the
membrane and detached from the transferrin molecule which is
84
ERYTHROPOIESIS
Iron absorbed
from G-I tract
R-E cells containing
■ catabolized haemoglobin
of phagocytosed red cells
Plasma Iron
bound to
transferrin
Iron in liver
parenchymal cells -
Iron loss in desquamating
-*» epithelial cells and in
menstrual blood
Erythroblasts
in bone marrow
Figure 7. Plasma iron
displaced and returned to the extravascular pool. The membrane-bound
ferrous iron is actively transferred to the cell interior; the mechanism
requires adenosine triphosphate as the source of energy and
pyridoxal-5-phosphate (viatamin B 6 ) as a co-enzyme. Within the cell,
the iron is complexed by a cytoplasmic carrier substance which
transports it to the mitochondria for haem synthesis. Any iron not
immediately utilized is stored as ferritin in the cytoplasm where it may
be visualized by electron microscopy and occasionally detected
cytochemically. This stored iron may be (1) lost from the late
erythroblast in the little cytoplasmic material that escapes with
extrusion of the pyknotic nucleus; (2) later used for haem synthesis,
which is normally completed during maturation of the reticulocyte; or
(3) pitted out of the reticulocyte in the spleen. The amount of iron
delivered to and incorporated into immature red cells varies with the
degree of erythropoietic activity, the functional state of the cells and
the percentage saturation of transferrin, which normally is approximately 30 per cent.
Formation of haemoglobin molecule
The final stages in the formation of the complete haemoglobin
molecule is not known. The size of the molecule is approximately 65 x
55 X 50 Â (1 Â = 10~7mm), and this is only possible by the folding
of the globin chains in the non-helical segments. Haem is located in a
pocket on the surface of each chain, attachment being effected through
the iron atom. Four of the six iron valencies are joined to the four
85
THE PERIPHERAL BLOOD FILM
pyrroles of the porphyrin ring; the fifth valency is joined to a histidine
residue on one side of the globin chain pocket, and the sixth is
indirectly linked by an oxygen molecule to another histidyl residue
further along the chain and on the other side of the pocket. The
stability of the haemoglobin molecule depends on the attachment of
haem to each chain. The synthesis of globin and of haem appear to be
interrelated and co-ordinated as little excess of either material is found
in the normal red cell.
ABNORMAL ERYTHROPOIETIC CELLS
Abnormal erythropoiesis
Erythropoietic activity may be normal, increased (Table 7.1) or
decreased (Table 7.2) and is indicated microscopically by the cellularity
of the erythroid series of cells. Morphologically the cells may be
normoblastic in type and/or abnormal erythroblasts. Erythroid
hyperplasia (the erythroblastic cellularity must be at least 5 X normaV to
affect the overall cellularity of haemopoietic tissue as seen in
histological sections of the bone marrow) is commonly reflected by a
proportional reticulocytosis in the peripheral blood. This hyperactivity
may be termed 'effective' erythropoiesis. However, if there is a
peripheral blood reticulocytopenia or a 'production index' (cf.
Reticulocyte count of blood) not proportionate to the erythroid
hyperplasia, the hyperactivity is termed 'ineffective' erythropoiesis.
This type of erythropoiesis is usually associated with the presence of an
excessive number of abnormal erythroblasts (more than 15 per cent of
TABLE 7.1
Hypercellularity of Erythropoietic Tissue
A. Increased stem cell availability
Increased input of stem cells into 'poietic' compartment
Disturbance of stem cell regulatory mechanism
Polycythaemia rubra vera
Di Guglielmo's syndrome (erythraemic myelosis)
B. Humoral stimulation
Increased erythropoietin production
Inappropriate and compensatory secondary polycythaemia
Anaemia
Endocrinopathies
C. Ineffective erythropoiesis
Abnormal erythroblastosis
D. Hypo cellularity of myelopoietic tissue (Table 8.3)
Relative hypercellularity of erythropoietic tissue
86
ERYTHROPOIESIS
TABLE 7.2
Hypocellularity of Erythropoietic Tissue
A. Failure of cell renewal system
Diminished input of stem cells into 'poietic' compartment
Defect of stem cells
Defect of micro-environment
B. Failure of humoral regulation
Impaired production of erythropoietin
Endocrinopathies
C. Hyperplasia of other cell lines
Myelopoietic (granulocytic) tissue
Monopoietic tissue
Lymphoid tissue including plasma cells
Fibrous tissue
D. Infiltration of bone marrow by foreign tissue
Metastatic carcinoma
erythroblasts). There is increased intramedullary haemolysis of these
abnormal cells by local histiocytes and reduction in the number of
viable cells being released into the blood. In addition, many of the red
cells in the blood, particularly those derived from the abnormal
erythroblasts, have a shortened life-span, the extramedullary haemolysis
being extravascular and/or intravascular in type. Ferrokinetically the
plasma iron turnover (PIT) rate (calculated from the plasma iron
concentration and rate of clearance of injected radio-iron from the
plasma — Tl/2), is markedly elevated when erythropoietic tissue is
hyperactive. However, the erythrocyte iron turnover (EIT) rate (derived
from the PIT and RBCU - the percentage of injected radio-iron utilized
for haemoglobin synthesis and determined from the radioactivity
present in the circulating red cells 14 days after the injection) which is
a measure of the effectiveness of erythropoietic activity, may be normal
or only slightly increased in ineffective erythropoiesis because of the
reduced RBCU percentage and intramedullary haemolysis. Erythroid
hypoplasia may be due to a variety of causes, including abnormal
erythroblastosis. Ferrokinetically the Tl/2 is prolonged and the PIT is
decreased; in addition, EIT and RBCU are depressed.
Classification of anbormal erythroblasts
Abnormal erythroblasts may arise from unknown causes, malignancy
and from defects in the synthesis of DNA and of haemoglobin. Some
cells may be morphologically normal, that is, appear normoblastic, but
may have intrinsic defects. Morphological abnormalities of erythroblasts may be classified into three categories: nuclear, cytoplasmic and
nucleocytoplasmic abnormalities (Table 7.3).
87
THE PERIPHERAL BLOOD FILM
TABLE 7.3
Abnormal Erythroblasts
Nuclear abnormalities
Binucleate and multinucleate erythroblasts
Trefoil or clover leaf nucleus
Cytoplasmic abnormalities
Vacuolated erythroblasts
Erythroblasts with inclusions
Sideroblasts
Fluorescent erythroblasts
Nucleocytoplasmic
abnormalities
Megaloblasts and megaloblastic erythropoiesis
Malignant erythroblasts
Nuclear abnormalities
Binucleate and multinucleate erythroblasts (Table 7.4)
Erythroblasts with two or more nuclei are larger than normal; very
large cells are referred to as 'gigantoblasts'. Intranuclear chromatin
bridges may be seen and the cytoplasm of some cells may show
punctate basophilia or contain vacuoles. Up to 1 per cent of the
normoblasts in a normal bone marrow are binucleate. In irradiated
subjects the binucleation may result from increased cell fusion rather
TABLE 7.4
Binucleate and Multinucleate Erythroblasts
Hereditary erythroblastic multinuclearity (Heimpel and Wendt, 1968)
Type I: megaloblastoid erythroblasts with intranuclear chromatin
bridges
Type II: normoblastoid erythroblasts with nuclear karyorrhixis and
positive acid serum haemolysis (Ham's) test
Type II: normoblastoid erythroblasts with nuclear karyorrhexis and
Aplastic anaemia
Megaloblastosis
Haemolytic anaemia
Sideroblastic anaemia
Di Guglielmo's syndrome (malignant erythroblastosis)
Radiation therapy
May be observed in:
Sarcoidosis
Collagen disorders
Active liver disease
Hypersplenism
88
ERYTHROPOIESIS
than abnormal cell division. The PAS reaction is positive in the cells
observed in Di Guglielmo's syndrome. The anomalies occur at any
developmental stage and the atypical cells may otherwise show
normoblastic or megaloblastic features.
Trefoil or clover leaf nucleus (see Plate 27)
The trefoil or clover-leaf nucleus, in which the chromatin appears
homogenous, may occur in the late erythroblast stage. Its formation
represents accelerated nuclear karyorrhexis and may be associated with
other anomalies, such as Howell-Jolly bodies and stippled cytoplasm. It
is frequently seen in ineffective erythropoiesis.
Cytoplasmic abnormalities
Vacuolated erythroblasts (Table 7.5) (see Plate 28)
Vacuoles may be seen in early and/or late erythroblasts. The
vacuoles in early erythroblasts are small, clear and have sharp outlines.
Those in late erythroblasts are larger and have indistinct outlines.
Vacuolated late erythroblasts are usually smaller and have more
basophilic cytoplasm than their normal counterparts. They may show
weak PAS-positive staining in their cytoplasm.
TABLE 7.5
Vacuolated Erythroblasts
Vacuolated early erythroblasts
Chronic alcoholism
Drugs: chloramphenicol, aminopyrine
Malignancy: Di Guglielmo's syndrome
Riboflavine deficiency
Vacuolated late erythroblasts
Defective haemoglobin synthesis (Table 12.16)
Sideroblastic anaemia (Table 7.6)
Malignancy: Di Guglielmo's syndrome
Phenylalanine deficiency
Erythroblasts with inclusions
Inclusions that may be seen in the cytoplasm of erythroblasts are
Howell-Jolly bodies, Pappenheimer bodies and punctate basophilic
granules. Late normoblasts may contain one Howell-Jolly body and late
megaloblasts two or more; they result from karyorrhexis or the nucleus.
Erythroblasts with Pappenheimer bodies are termed sideroblasts.
Punctate basophilic granules may represent ribonucleoprotein, free
globin chains or non-haem iron. Their nature is distinguished by
supravital dye staining and the Prussian blue reaction.
89
THE PERIPHERAL BLOOD FILM
Sideroblast (Table 7.6)
A sideroblast is an erythroblast with cytochemically detectable
non-haem iron within the cytoplasm; the iron is in the form of
aggregates and appears as blue granules in the Prussian blue reaction.
Siderotic granules are not readily demonstrable in normoblasts. Their
presence is commonly suggestive of pathological sideroblastosis and is
observed in disorders associated with plasma transferrin levels that are
greater than 35 per cent. In some disorders (Table 7.6 A) the
erythroblasts are considered to undergo a sideroblastic change because
the size and number of the siderotic granules are proportional to
transferrin saturation and the granules are randomly distributed within
the cells. (Mollin and Hoffbrand, 1968). In other disorders (Table 7.6
B) the morphological characteristics of the granules are not
proportional to transferrin saturation. Their number, size and
coarseness increase as the cells multiply and mature. These
TABLE 7.6
Pathological Sideroblasts
A. Erythroblasts with diffusely distributed siderotic granules
Haemochromatosis and haemosiderosis
Secondary sideroblastic anaemia (Table 12.24)
B. Erythroblasts with siderotic granular ring around nucleus
Hereditary sideroblastic anaemia (Table 12.24)
Acquired sideroblastic anaemia (Table 12.24)
Primary
Secondary
erythroblasts are the hallmark of sideroblastic anaemia (see Table 12.24)
and are designated 'ring' sideroblasts because the siderotic granules,
which are located in the mitochondria, form a ring or collar around the
nucleus. Except in acquired primary sideroblastic anaemia, the ring
form is not seen in early erythroblasts but only in intermediate and late
erythroblasts. In a Romanovsky-stained film the sideroblasts may
appear vacuolated because of defective haemoglobinization due to
abnormal iron metabolism, reduced protoporphyrin and haem synthesis
and to deranged gjobin production with decreased alpha chain
synthesis. The aetiology and pathogenesis of ring sideroblasts is
unknown. Abnormal metabolism of pyridoxal-5-phosphate (vitamin
B 6 ) may play a role. This vitamin acts as a co-enzyme for mitochondrial
enzymes (delta-ALA and haem synthetases) concerned with haem
synthesis, assists in the uptake of iron by erythroblasts, and mobilizes
iron from the mitochondria. There may also be a somatic mutational
90
ERYTHROPOIESIS
defect as sideroblastic anaemias show some similarity to Di Guglielmo's
syndrome and may terminate as a myeloid or myelomonocytic
leukaemia.
Fluorescent erythroblasts
A variable number of erythroblasts in congenital erythropoietic
porphyria, congenital erythropoietic protoporphyria and lead poisoning
may show red fluorescence of their cytoplasm when exposed to
ultraviolet light. In the first disorder, the fluorescence is particularly
noted in the nucleus. In the Romanovsky-stained film the nucleus of
this fluorescent late erythroblast may show incompletely stained areas.
The phenomenon of erythroblastic fluorescence is due to the marked
increase in free protoporphyrin concentration in the cells.
Nucleocy toplasmic abnormalities
Megaloblasts and megaloblastic erythropoiesis (see Tables 12.10-12.14)
Vitamin Β± 2 and folate are essential requirements for DNA synthesis
and normoblastic erythropoiesis. The co-enzyme forms of these
vitamins play a role in purine and pyrimidine synthesis, activation of
formate and amino acid interconversion by oxidation-reduction, and
transfer of single carbon units (Figure 8). Vitamin B 6 , in addition to its
role in haem synthesis, is also involved as a co-enzyme in folate
metabolism. Diminished availability of vitamin B i 2 (Table 12.11) and
Homocysteine
Methyl trqnsferase
Methyl
Formate
Bi:
_J_
Formyl
THF
Histidine
Urocanic
acid—^FIGLU
Formimino
transferase
Glutamic acid M
Cyclodeaminase
Cyclohydrolase
Methenyl
THF
Dehydrogenase
figure 8. Vitamin B12 and folate in DNA synthesis
91
THE PERIPHERAL BLOOD FILM
folate (Table 12.13) and deficiency or inactivation of enzymes
concerned with folate matabolism and DNA synthesis (Table 12.14)
result in cellular and nuclear enlargment of erythropoietic and other
rapidly dividing series of cells (myelopoietic or granulocytic,
thrombopoietic, epithelial cells of tongue, gastro-intestinal tract, cervix
uteri, spermatozoa). The atypical erythroblasts are termed megaloblasts. They have finer strands of nuclear chromatin arranged in an open
reticular pattern and have more abundant cytoplasm than their normal
counterparts. The microscopic appearance of the cells may be related to
(1) the presence of larger, slender and less tightly coiled chromosomes;
(2) a defect in the biosynthesis of purines and thymidylate, a
pyrimidine precursor of DNA; (3) a delay in the synthesis of DNA; and
(4) an increase in RNA and protein synthesis. Megaloblastic
erythropoiesis is usually characterized by ineffective erythroid
hyperplasia, asynchronic maturation of the nucleus and cytoplasm,
early haemoglobinization, a late megaloblast with a pink (fully
haemoglobinized) cytoplasm, and by absence of a reticulocyte stage.
The intermediate megaloblast may be considered to be the only cell of
this series with morphological features that are diagnostic of
megaloblastic erythropoiesis.
Promegaloblast (20 - 30 Mm). - The cytoplasm is deeply basophilic
and there may be a pale perinuclear zone. The nucleus contains
nucleoli. The chromatin is fine and delicate with an open reticulated
pattern.
Early megaloblast (18-25 μτή). - The cytoplasm is deeply basophilic
and abundant. The nucleus may contain a nucleolus, and the chromatin
may show the clock-face sign described below. Binucleate cells may be
seen.
intermediate megaloblast (12-15 μπι). - The cytoplasm is abundant
and greyish-pink. The nucleus is usually round and single (see Plate 29).
The chromatin is composed of fine widely separated strands which
form an open reticular pattern. In 30-50 per cent of these cells
chromatin particles, appearing like round 'hillocks' with convex
surfaces towards the centre of the nucleus, may adhere to the interior
of the nuclear membrane and arranged circumferentially like the
minute markings on the face of the clock (Kass, 1968). Cells with
bizarrely - shaped nuclei may be seen.
Late megaloblast ( 1 0 - 1 5 μπι). — The cytoplasm is pink and in an
occasional cell two or more Howell-Jolly bodies may be noted. The
nucleus is small and situated eccentrically in the cell. It may be round,
indented, trefoil or bizarre in shape. The nuclear chromatin retains an
open reticular arrangement. The late megaloblast matures directly into
the macro-ovalocyte by extrusion of the nucleus.
92
ERYTHROPOIESIS
Malignant erythroblasts
Malignant erythroblasts, also called para-erythroblasts, are seen in Di
Guglielmo's syndrome (erythraemic myelosis and erythroleukaemia).
The erythroblasts are pleomorphic in appearance. They may be of the
following types.
(1) Cells with atypical nuclei: (a) multinucleated gigantoblasts; (b)
basophilic erythroblasts with multilobulated nuclei; (c) erythroblasts
with homogenized, vacuolated or fragmented nuclei.
(2) Cells with atypical cytoplasm: (a) basophilic erythroblasts with
granular and/or vacuolated cytoplasm, (b) polychromatic or orthochromatic erythroblasts with vacuolated cytoplasm.
(3) Cells showing asynchronic maturation of the nucleus and
cytoplasm: (a) normoblastoid erythroblasts with a dense mature
nucleus and basophilic cytoplasm; (b) megaloblastoid erythroblasts
with an immature nucleus and polychromatic or orthochromatic
cytoplasm. These cells are unaffected by vitamin B 1 2 and/or folate
therapy.
In contrast with normal erythroblasts, the alpha-naphthyl acetate
esterase activity of malignant erythroblasts is strongly positive and
Perls' Prussian blue reaction may show the presence of ring sideroblasts.
In addition, a variable number of the erythroblasts give a strongly
positive PAS reaction; the magenta staining appears granular in the
early malignant erythroblasts and diffuse in the later stages.
93
8
Myelopoiesis (Granulopoiesis);
Monopoiesis; Thrombopoiesis
MYELOPOIESIS - GRANULOPOIESIS
NORMAL MYELOPOIETIC CELLS
Normal myelopoiesis: stages and cell changes
As with erythropoiesis, myelopoiesis normally takes place
extravascularly within the bone marrow and consists of two phases, a
dividing or 'multiplicative' phase and a 'maturation' phase. The
development stages are myeloblast, promyelocyte, myelocyte, metamyelocyte and stab cell {Figure 9); mitotic activity last occurs at the
myelocyte stage. According to Cartwright, Athens and Wintrobe
(1964), one of the daughter cells of a myelocyte division remains as a
myelocyte to divide again; that is, the myelocyte functions as a
'semi-stem' cell, the other daughter cell becoming a metamyelocyte.
The neutrophilic, eosinophilic and basophilic series of granulocytic cells
are all derived from the myeloblast Neutrophilic cells are predominant in the bone marrow (approximately 75 per cent of the
nucleated cells); the basophilic series of cells are few in number.
Multiplicative phase
Myeloblast
».Promyelocyte
Maturation phase
► Myelocyte —»►Metamyelocyte
► Stab cell — J
Figure 9. Myelopoiesis (granulopoiesis)
Sequential morphological changes observed are (1) reduction of the
nucleocytoplasmic ratio; (2) disappearance of the nucleoli; (3)
coarsening and clumping of nuclear chromatin; (4) decrease in
cytoplasmic basophilia; (5) the initial appearance of azurophilic or
'primary' granules in the promyelocyte; (6) the appearance of'specific'
(neutrophil, eosinophil or basophil) or 'secondary' granules, the
morphological markers of the granulocytic cells, at the myelocyte stage
and their numerical increase with cell maturity; and (7) indentation of
the nucleus at the metamyelocyte stage followed by its elongation to
94
v©
—
—
—
-
—
—
—
+
+
+
-
++
+++
-
+++
—
+++
Alpha-naphthyl
acetate esterase
Peroxidase
No activity, —; weak activity, +; moderate activity, ++; strong activity, +++.
Myeloblast
Promyelocyte
Myelocyte
Neutrophil
Eosinophil
Basophil
Metamyelocyte
Neutrophil
Eosinophil
Basophil
Stab cell
Neutrophil
Eosinophil
Basophil
Myelopoietic
cells
—
—
+++ Granular
—
—
+++ Granular
—
—
+++ Granular
+++ Granular
+++ Granular
Naphthol AS-D Chloroacetate esterase
Cytochemical Reactions of Mylelopoietic Cells
TABLE 8.1
+++
+++
+ Coarse granules
++
++
+ Coarse granules
++
+
+ Coarse granules
_
+
PAS
THE PERIPHERAL BLOOD FILM
the 'stab' or band form. The cytochemical characteristics of
myelopoietic cells are indicated in Table 8.1.
Morphology of normal myelopoietic cells
Myeloblast (14-18μ)
The myeloblast is a round or slightly oval cell with a nucleus that
occupies the greater part of the cell. One to five nucleoli are seen and
may be better demonstrated with the Feulgen reaction. The nuclear
chromatin is loosely arranged and has a fine reticular structure. The
cytoplasm is intensely basophilic but to a lesser degree than that seen in
normoblasts and plasma cells. No granules or other inclusions are
present.
Promyelocyte (16-25 μηι)
The promyelocyte is larger than its precursor. The nucleus occupies
an eccentric position within the cell and its chromatin is coarser than
that seen in the myeloblast. The nucleolus is large and prominent. The
cytoplasm is abundant, basophilic and contains a variable number of
azurophilic or 'primary' granules. Peroxidase and acid phosphatase
enzymes are constituents of these granules.
Myelocyte (12-18 μπι)
The myelocyte is a round or slightly oval cell with an eccentrically
located nucleus occupying approximately 50 per cent of the cell (see
Plate 30). There is no nucleolus and the chromatin is condensed but
still has a reticular pattern. The cytoplasm is slightly basophilic and
contains many specific (neutrophil, eosinophil or basophil) or
'secondary' granules. These have been discussed in Chapter 3. Primary
granules are also present in the cytoplasm but their intensity of staining
is decreased and they are masked by the specific granules. There is no
alkaline phosphatase activity demonstrable in the cytoplasm.
Metamyelocyte (10-15μ)
The metamyelocyte is a non-dividing cell. The granular content of
the cytoplasm is similar to that of its precursor but more numerous.
The cell is characterized by an indented nucleus; the indentation
becomes deeper as the cell matures into the stab cell.
Stab cell (see Plate 31)
The stab cell is smaller than the metamyelocyte and slightly larger
than the segmented cell into which it matures. The granular content of
the cytoplasm is similar to that of the precursor. The nucleus is
sausage-shaped and may be bent on itself or have a horse-shoe
appearance. An occasional stab cell is released into the blood. The
majority normally mature in the bone marrow into the corresponding
segmented cells which form a reserve storage pool in this site.
96
MYELOPOIESIS (GRANULOPOIESIS); MONOPOIESIS; THROMBOPOIESIS
ABNORMAL MYELOPOIETIC CELLS
Abnormal myelopoiesis: cellurarity and maturation arrest
Neutrophil myelopoiesis may be normal, increased (Table 8.2)
or decreased (Table 8.3) and is indicated microscopically by
the cellularity of the myeloid series of cells. Hyperplasia is
commonly reflected by a neutrophilia (an increased number of
neutrophil polymorphs in the peripheral blood). At times
there may be a neutropenia (decreased number of neutrophil
polymorphs in the peripheral blood) due to 'ineffective myelopoiesis'
and a 'maturation arrest' at one of the stages of the multiplicative
phase. Maturation arrest may occur at any developmental stage. In the
multiplicative phases there is an amplification block which is indicated
by hypercellularity of the immature cells, up to and including the
arrested stage, associated with hypocellularity of the more mature cells.
Impaired maturation may be apparent or real. The apparent form is
seen in some neutropenias and is due to premature release of
non-dividing cells from the bone marrow. Real maturation arrest occurs
in 'ineffective myelopoiesis' and is due to the production and
intramedullary destruction of abnormal cells showing asynchronic
nucleocytoplasmic maturation. Ineffective myelopoiesis due to vitamin
Bj2 and/or folate deficiency is suggested by the occurrence of giant
TABLE 8.2
Hypercellularity of Myelopoietic Tissue
A. Increased stem cell availability
Increased input of stem cells into 'poietic' compartment
Neutrophilia in peripheral blood
Disturbance of stem cell regulatory mechanism
Polycythaemia rubra vera
Myelocytic (granulocytic) leukaemia
Neutropenia in peripheral blood
Premature release of mature cells
B. Stimulation by various agents
Increased level of regulator?: neutropenia
Infectious agents
En docrinopa thies
C. Ineffective myelopoiesis
Diminished availability of essential substances
Vitamin Bï2 and folate deficiency
Malignant change
Myeloblastic leukaemia
D. Hypocellularity of erythropoietic tissue (Table 7.2)
Relative hypercellularity of myelopoietic tissue
97
THE PERIPHERAL BLOOD FILM
TABLE 8.3
Hypocellularity of Myelopoietic Tissue
A. Failure of cell renewal system
Diminished input of stem cells into 'poietic' compartment
Defect of stem cells
Defect of micro-environment
B. Failure of humoral regulation
Reduced level of regulator?
Endocrinopathies
C. Hyperplasia of other cell lines
Erythropoietic tissue
Monopoietic tissue
Lymphoid tissue including plasma cells
Fibrous tissue
D. Infiltration of bone marrow by foreign tissue
Metastatic carcinoma
metamyelocytes and/or stab cells. Malignant myelopoiesis is characterized by maturation arrest at one of the stages of the multiplicative
phase and morphological abnormalities at all developmental stages.
Hypercellularity in myeloblastic leukaemia is due to accumulation of
non-dividing malignant myeloblasts which are unable to proliferate
along the usual pathway for elimination from the bone marrow (Stuart,
1972). The hypercellularity in myelocytic leukaemia is considered to be
due to a disturbance of stem cell regulatory mechanisms which results
in stem cell proliferation and an expanded myelopoietic compartment
(Stuart, 1972; Galbraith and Abu-Zahra, 1972); in addition, however, a
degree of maturation arrest at the myelocyte stage is observed.
Hyperplasia of the eosinophilic and basophilic series of cells may
accompany some neutrophilic hyperplasias; eosinophilic leukaemia may
be a variant of myeloid leukaemia. Eosinophilic myelopoiesis is
prominent in subjects with an eosinophilia (increased number of
eosinophils in the peripheral blood). Basophilic myelopoiesis per se is
rarely prominent. Myeloid hypoplasia may be due to a variety of causes
and its pathogenesis is often complex.
Morphology of abnormal myelopoietic cells
Giant metamyelocyte and stab cell
The giant metamyelocyte and stab cell are almost twice the size of
their normal counterparts. Apart from size, the morphology of these
cells is similar to the normal cells.
98
MYELOPOIESIS (GRANULOPOIESIS); MONOPOIESIS; THROMBOPOIESIS
Malignant myelopoietic cells
Malignant myeloblast (see Plate 32). - The leukaemic myeloblast
varies in size and shape. The cell seen in the peripheral blood in
myeloblastic leukaemia may be smaller than that in the bone marrow
and may be mistaken for a lymphocyte. Occasionally those seen in
the bone marrow may also be small (micromyeloblast); the Feulgen
reaction is valuable for distinguishing them from lymphocytes. The
leukaemic cell nucleus is similar in appearance to that of a normal
myeloblast but shows marked pleomorphism. The basophilic cytoplasm
is usually agranular but may show a pale (peroxidase positive)
polychromatic area near the nucleus and/or contain a few small clear
vacuoles with sharp outlines; an Auer rod may be observed. The Auer
rod is an azurophilic structure measuring up to 6 μηι in length and up
to 1.5 Mm in width; it may appear rectangular and rarely spherical. It
contains RNA, peroxidase and acid phosphatase; it is PAS positive but
the reaction is not abolished by pretreatment with diastase. The Auer
rod is probably formed by fusion of 'primary' granules. The peroxidase
reaction in the leukaemic myeloblast varies; it is negative except in cells
with an Auer rod or with the polychromatic flare near the nucleus. The
PAS and alpha-naphthyl acetate esterase reactions are negative; there is
moderate acid phosphatase activity and strong naphthol AS-D
chloroacetate esterase activity. The cytochemical reactions of
leukaemic myeloblasts, monoblasts and lymphoblasts are indicated in
Table 8.4
Paramyeloblast - The paramyeloblast is a leukaemic blast cell with
an indented nucleus. The cells which subsequently develop show
marked asynchronic maturation of the nucleus and cytoplasm. Cell
staging is difficult in this type of leukaemia.
Leukaemic promyelocyte. - The leukaemic promyelocyte is
pleomorphic in size, shape and morphology. The eccentric nucleus has
one or more nucleoli. The cytoplasm contains many azurophilic
granules. The peroxidase reaction is positive and the PAS staining may
be more intense than that usually seen in a normal promyelocyte. An
occasional cell may contain an Auer rod.
Leukaemic myelocyte. - The leukaemic myelocyte may appear
normal. The cytoplasm of some cells may be agranular or contain a few
coarse, pale azurophilic granules. Nuclei with a small central 'hole' have
been reported in a patient with Di Guglielmo's syndrome (Stavem et al,
1969).
99
-
Myeloblast
-
Lymphoblast
+
-
Alpha-naphthyl
acetate esterase
-
+++
Naphthol AS-D
chloroacetate esterase
No activity, —; weak activity, +; moderate activity, ++; strong activity, +++
-
Monoblast
Some cells
are positive
Peroxidase
Leukaemic blast
cells
Cytochemical Reactions of Leukaemic Blast Cells
TABLE 8.4
+
+++
++
Acid
phosphatase
80-90%
positive
Some cells
are positive
-
-
PAS
MYELOPOIESIS (GRANULOPOIESIS); MONOPOIESIS; THROMBOPOIESIS
MONOPOIESIS
NORMAL MONOPOIETIC CELLS
Normal monopoiesis: stages
Monopoiesis normally takes place extravascularly within the bone
marrow and consists of a dividing or 'multiplicative' phase and a
'maturation' phase {Figure 10). The developmental stages are
monoblast and promonocyte; mitotic activity last occurs at the
promonocyte stage. The progenitor cell of the series is identical with
that of the myelopoietic (granulocytic) series. The factors that cause
the progenitor cell to differentiate into a monoblast rather than into a
myeloblast are not known. According to Metcalf and Moore (1971), the
Multiplicative phase
Stem cd Is
► Promonocyte
Figure 10. Monopoiesis
in vitro colony-stimulating factor present in urine tends to stimulate
monoblastic differentiation in agar cultures of bone marrow aspirates.
Sequential morphological changes observed are (1) reduction of the
nucleocytoplasmic ratio, (2) disappearance of the nucleoli, (3) increase
in the size of the cell and (4) appearance of fine granules which give the
cytoplasm a ground-glass appearance.
Morphology of normal monopoietic cells
Monoblast (12-20 Mm)
The monoblast has a large round or indented nucleus. The chromatin
has a well-defined network pattern with a skein-like appearance.
Nucleoli are small and up to five may be seen. The basophilic cytoplasm
is abundant, forming a moderately wide border round the nucleus, and
agranular. Cytochemically the chloroacetate esterase and PAS reactions
are negative; the alpha-naphthyl acetate esterase and acid phosphatase
reactions are positive. The acid phosphatase reaction is inhibited by
L(+) tartaric acid.
Promonocyte
The promonocyte is usually larger than the precursor cell. The
nucleus is round or there may be partial lobulation. Nucleoli are not
evident. The cytoplasm is pale blue. Fine granules giving the cytoplasm
a ground-glass appearance, are present. The alpha-naphthyl acetate
esterase reaction is positive but there is no chloroacetate esterase
activity. The peroxidase activity is variable and the PAS reaction may
show a few fine magenta-coloured granules in the cytoplasm.
101
THE PERIPHERAL BLOOD FILM
ABNORMAL MONOPOIETIC CELLS
Abnormal monopoiesis: leukaemia
Leukaemia involving monopoietic cells may be divided into two types:
the Schilling type (monocytic leukaemia) composed predominantly of
monocytic cells, and the Naegeli type (myelomonocytic leukaemia) in
which a mixture of leukaemic myelopoietic and monopoietic cells are
present. The two types are classified by Hayhoe and his colleagues
(Hayhoe and Cawley, 1972; Hayhoe, Quaglino and Doll, 1964) as
variants of a single category designated myelomonocytic leukaemia.
Morphology of abnormal monopoietic cells
Leukaemic monoblast (see Plate 33)
The leukaemic monoblast is pleomorphic in size and shape; it usually
has an irregular outline. The nucleus may be oval, reniform, horse-shoe
shaped or convoluted with up to five nucleoli. The basophilic
cytoplasm is more abundant than that of a normal monoblast or
myeloblast, and there may be some pseudopodal projections. Vacuoles
and fine azure granules may be present. An occasional cell may contain
an Auer rod. The peroxidase and chloroacetate esterase reactions are
negative. Alpha-naphthyl acetate esterase and acid phosphatase
activities are demonstrable; the latter is inhibited by L^+^ tartaric acid.
The PAS reaction is variable; some cells are negative and others show
weak diffuse magenta staining with a few fine granules. The
cytochemical reactions of leukaemic monoblasts, myeloblasts and
lymphoblasts are indicated in Table 8.4.
THROMBOPOIESIS
NORMAL THROMBOPOIETIC CELLS
Normal thrombopoiesis: stages and cell changes
Thrombopoiesis principally takes place extravascularly in the bone
marrow; some may occur within the blood vessels of the lungs
(Kaufman et al., 1965). The developmental stages are megakaryoblast,
promegakaryocyte and megakaryocyte {Figure 11); the latter cell may
Nuclear
Cytoplasmic
mulliplicalive phase
maturation phase
Megakaryblast
_ +. Promegakaryocyte
». Megakaryocyte J
Figure 11. Thrombopoiesis
be sub-classified into the reserve megakaryocyte and the plateletforming megakaryocyte. Reduction division does not take place in
102
MYELOPOIESIS (GRANULOPOIESIS); MONOPOIESIS; THROMBOPOIESIS
these cells, and their cellularity in the bone marrow depends on the
availabiltiy and entry of the thrombopoietin-sensitive stem cell into the
'poietic' compartment. The megakaryoblast undergoes nuclear division
within the cytoplasm; the number of nuclear units doubles with each
mitosis. The daughter nuclei usually unite to form a large nucleus which
may appear lobulated or segmented. The amount of cytoplasm
increases with each division and is proportionate to the number of
nuclear units. Cytoplasmic maturation commences only after cessation
of nuclear replication and is indicated by the appearance of azurophilic
granules. The signal for switching off DNA synthesis and controlling
the number of nuclear divisions is not known; it may be the synthesis
of thrombosthenin, an actomyosin-like protein, within the cytoplasm.
Megakaryocytes may have four (10 per cent of cells), eight (65 per cent
of cells) or 16 (25 per cent of cells) nuclear units. Approximately 25
per cent of cells in the poietic compartment have no apparent granules,
25 per cent are partially granulated and 50 per cent are fully
granulated.
Platelet formation
Platelet formation commences when the cytoplasm is filled with
azurophilic granules and may occur with four, eight or 16 nuclear units.
Microvescicles appear and coalesce, and the cytoplasm is demarcated
into platelet sub-units by a membrane network. The number of
platelets formed by each megakaryocyte is proportionate to its
cytoplasmic mass; estimates of the number of platelets produced by a
single megakaryocyte range from 2,000 to 11,000. After cytoplasmic
maturation is complete, the platelets are apparently discharged through
an opening in the cell's outer membrane. This release may take place
intravascularly with protrusion of the megakaryocyte's cytoplasm
through the pores of the marrow sinusoids. Platelet delivery may also
take place from circulating megakaryocytes and from megakaryocytes
that have migrated to the pulmonary blood vessels (Kaufman et al.,
1965). After discharge of its platelets, the bare megakaryocyte nucleus
is phagocytosed by macrophages.
Thrombopoiesis control
The mechanism for controlling thrombopoiesis is not known.
Feedback regulation by the blood platelet concentration appears to
exist because megakaryocyte size (and number of nuclear units) is
inversely related to the platelet count. A humoral regulator,
thrombopoietin, has been detected in the plasma of patients with
thrombocytopenia (decreased number of platelets in the peripheral
blood). Thrombopoietin is considered to increase (1) the proliferation
and differentiation of progenitor cells, (2) the number of mitotic
103
THE PERIPHERAL BLOOD FILM
divisions and thus the cytoplasmic mass and (3) the rate of cytoplasmic
maturation. The source of thrombopoietin is not known.
Morphology of normal thrombopoietic cells
Megakaryoblast (15-30 Mm) (see Plate 34)
The megakaryoblast may have two myeloblast-like nuclei or a single
large bi-lobed nucleus. The chromatin is reddish-blue and has a
sieve-like pattern. Many nucleoli are present. The cytoplasm is intensely
basophilic, non-granular and may have small pseudopodal projections.
Promegakaryocyte (30 - 50 μηι)
The size of the promegakaryocyte depends on the number of nuclear
units it contains. The cell has an irregular outline with pseudopodal
projections. The nucleus appears multilobulated. The chromatin is
coarse and no nucleoli can be identified. The cytoplasm is less
basophilic than that of the blast cell. A cluster of fine pink or
reddish-purple granules is located near the nucleus. The PAS reaction
shows the presence of coarse masses of magenta-staining material.
Megakaryocyte (40 - 80 Mm) (see Plate 35)
The megakaryocyte usually has a multilobulated nucleus; polynuclear cells with varying size nuclei may be seen if the post-mitotic
nuclei have not united to form a single large nucleus. The cell outline is
irregular and the cytoplasmic mass is proportionate to the number of
nuclear units. Two types of cells may be recognized: the 'reserve' or
non-platelet-forming megakaryocyte and the platelet-forming
megaryocyte. The cytoplasm of the reserve cells has two zones, an inner
granular zone and an outer narrow rim which is pale blue and agranular.
In the platelet-forming cell the granules extend to the periphery of the
cytoplasm. The density and staining characteristics of the granules
increase with cytoplasmic maturation. When the platelet stage is reached
the granules appear coarse and dark in colour.
ABNORMAL THROMBOPOIETIC CELLS
Abnormal thrombopoiesis: cellularity
Thrombopoiesis may be normal, increased (Table 8.5) or decreased
(Table 8.6), and is indicated microscopically by the cellularity of the
megakaryocyte series of cells and the degree of cytoplasmic maturation.
As reduction division of the cells does not take place, megakaryocytic
hyperplasia in the bone marrow is due to an increased input of stem
cells into the 'poietic' compartment, and is commonly reflected by a
thrombocytosis (an increased number of platelets in the peripheral
104
MYELOPOIESIS (GRANULOPOIESIS); MONOPOIESIS; THROMBOPOIESIS
TABLE 8.5
Hypercellularity of Thrombopoietic Tissue
A. Increased stem cell availability
Increased input of stem cells into 'poietic' compartment
Disturbance of stem cell regulatory mechanism
Polycythaemia rubra vera
Essential thrombocythaemia
Other myeloproliferative disorders
B. Stimulation by various agents
Increased level of regulator?: thrombocytopenia
Drugs such as steroids
C. Ineffective
thrombopoiesis
Diminished availability of essential substances
Vitamin B i 2 and folate deficiency
Impaired cytoplasmic maturation
Drugs and antiplatelet antibodies
D. Hypocellularity of myelopoietic tissue (Table 8.3)
Relative hypercellularity of thrombopoietic tissue
TABLE 8.6
Hypocellularity of Thrombopoietic Tissue
A. Failure of cell renewal system
Diminished input of stem cells into 'poietic' compartment
Defect of stem cells
Defect of micro-environment
B. Failure of humoral regulation
Reduced level of regulator?
C. Hyperplasia of other cell lines
Erythropoietic tissue
Myelopoietic tissue
Monopoietic tissue
Lymphoid tissue including plasma cells
D. Infiltration of bone marrow by foreign tissue
Metastatic carcinoma
blood). However, hyperplasia may be associated with thrombocytopenia (decreased number of platelets in the peripheral blood) and
results from 'ineffective' thrombopoiesis. There is accumulation of
non-maturing megakaryocytes which are unable to complete their usual
pathway for elimination from the bone marrow. While megakaryocytic
hypoplasia is commonly due to hypercellularity of other cell lines, it
may be due to failure of the cell renewal system which occurs in certain
hereditary disorders.
105
THE PERIPHERAL BLOOD FILM
Abnormal megakaryocytes
Ineffective thrombopoiesis is characterized by nuclear hypersegmentation and delay in cytoplasmic maturation. When caused by
toxic agents, particularly drugs and antiplatelet antibodies, other
morphological abnormalities are seen. There may be nuclear pyknosis
or vacuolation and multinuclearity in some cells; agranularity,
hyalinization and aggregation of granules into a spherical mass, and
peripheral vacuolation of the cytoplasm may be observed.
The phenomena of 'peripolesis' and 'emperipolesis' of lymphocytes
may occur in lymphoma. Peripolesis is lymphocyte satellitism of
megakaryocytes. In emperipolesis, intact lymphocytes are within the
cytoplasm of megakaryocytes and appear to be wandering in and about
the cell. These phenomena are not considered to be fortuitous
occurrences, but their pathogenesis and significance is not known.
106
9
Lymphopoiesis, Plasmapoiesis,
Non-haemopoietic Cells
LYMPHOPOIESIS: PLASMAPOIESIS
NORMAL LYMPHOPOIETIC CELLS
Normal lymphopoiesis: types, stages and cell changes
Lymphopoiesis may be broadly classified into two types, primary and
secondary. Primary lymphopoiesis takes place extravascularly in the
primary or central lymphoid organs - the bone marrow and the thymus
— and is principally concerned with the initial production of
immunocompetent B - and T - lymphocytes. Secondary lymphopoiesis
takes place extravascularly in the secondary or peripheral lymphoid
organs — spleen, lymph nodes, lymphoid aggregates in the walls of the
gastro-intestinal and respiratory tracts. It is concerned with maintaining
the blood levels of lymphocytes and the immunological integrity of the
individual. Plasmapoiesis may be considered to be a variety of
secondary lymphopoiesis because the plasmablast is derived from
antigen-sensitized B—lymphocytes. It is concerned with the production
of the various immunoglobulin classes necessary for humoral immunity.
Primary lymphopoiesis
The lymphatic cells in the bone marrow are usually dispersed among
the haemopoietic cells of the red marrow tissue. An occasional small
lymphoid aggregate may be seen in histological sections of aspirated
bone marrow from approximately 10 per cent of normal subjects.
These focal collections of lymphocytes usually do not display a pale
central area and have irregular and indistinct margins which merge into
adjacent haemopoietic tissue. Lymphopoiesis in the bone marrow is
under genetic control (Yoffey and Courtice, 1970) and starts with the
'transitional' cell composed of a spectrum of cells intermediate between
lymphocytes and blast cells, and ends with the production and release
of B-lymphocytes into the blood. This pre-B-lymphopoiesis is
ineffective because the majority of the cells are short-lived and undergo
intramedullary lysis.
107
THE PERIPHERAL BLOOD FILM
Thymic lymphopoiesis depends on the availability and migration of
stem cells from the bone marrow. Pre—T—lymphopoiesis may be
regulated by gene control, contact with the thymic epithelial cells or by
short-range humoral factors acting only within the thymus. As with the
bone marrow there is marked ineffective lymphopoiesis; the majority of
the cells in the thymus are short-lived and undergo intrathymic lysis.
Secondary lymphopoiesis {Figure 12)
Lymphocytes released into the blood from the primary lymphopoietic organs migrate to the peripheral lymphoid organs where they
populate specific areas; the T-lymphocyte sites are different from
those of the B—lymphocyte. Secondary lymphopoiesis is antigen
dependent. The proliferative response is influenced by the type and
dose of antigen, its handling by the macrophages of the
reticulo-endothelial system, the level of steroid hormones and the
nutritional state of the individual (the lymphoid tissue of the body is
reduced in malnutritional disorders). Antigen-stimulated T - and
T-lymphocyte | -+»
Multiplicative phase
|
Lymphoblast -*. Prolymphocyte
-J
Plasmablast —>-Proplasmacyte
-\
t
Antigen
1
B- Lymphocyte
—
Figure 12. Secondary
lymphopoiesis
B—lymphocytes undergo blastogenic transformation in the lymphoid
organs; lymphoblasts and plasmablasts are produced. The developmental stages of lymphopoiesis are lymphoblast and prolymphocyte;
additional lymphocytes (the effector cells) are formed by reduction
division of these cells. The morphological changes observed during
lymphopoiesis are nuclear chromatin condensation and decreased
cytoplasmic basophilia. The developmental stages of plasmapoiesis are
plasmablast and proplasmacyte; plasma cells are formed by reduction
division of these cells. The morphological changes observed during
plasmapoiesis are increase in the size and cytoplasmic content of the
cells, and nuclear chromatin condensation.
Morphology of normal lymphopoietic cells
Lymphoblast (14-18 μιή)
The lymphoblast is the same size as the myeloblast. It is a round cell
with a round nucleus which occupies the greater part of the cell. The
chromatin has a coarse reticular structure. Nucleoli are clear cut and
108
LYMPHOPOIESIS, PLASMAPOIESIS, NON-HAEMOPOIETIC CELLS
prominent because of chromatin condensation around them; one to
two may be seen. The cytoplasm is basophilic and contains no
inclusions. The peroxidase, acetate esterases and alkaline phosphatase
reactions are negative. Acid phosphatase activity is weak and is sensitive
to l/ + ) tartaric acid. The PAS reaction may show a few
magenta-coloured granules.
Prolymphocytes (12 -15 μτη)
The prolymphocyte has denser chromatin and more abundant
cytoplasm than the lymphoblast. The nucleus is usually in an eccentric
position and indistinct nucleoli may be evident. The basophilic
cytoplasm has a hyaline or transparent appearance; there may be a few
azurophilic granules. The cell is peroxidase, alkaline phosphatase and
acetate esterases negative. Acid phosphatase activity is weak.
Morphology of abnormal lymphopoietic cells
Leukaemic lymphoblast (see Plate 36)
The leukaemic lymphoblast varies in size and shape. The nucleus may
be indented, notched or have a bizarre shape due to several deep clefts
(these may suggest lobulation of the nucleus). The chromatin is denser
than normal but retains the reticular pattern; one to two nucleoli are
seen. The basophilic cytoplasm may contain large azurophilic granules
or vacuoles. Auer rods« are never seen. Cytochemically the peroxidase
and acetate esterases reactions are negative. Acid phosphatase activity is
demonstrable; it is weaker than that present in myeloblasts and
monoblasts. The PAS reaction is variable. Of the cells 80-90 per cent
contain coarse magenta-coloured granules or dense blocks against a
negative cytoplasmic background. The pattern of reactivity rather than
the percentage of positive blast cells is of diagnostic importance
(Hayhoe and Cawley, 1972). The cytochemical reactions of leukaemic
lymphoblasts, myeloblasts and monoblasts are indicated in Table 8.4.
Lymphosarcoma cell
The lymphosarcoma cell in the blood resembles cells seen in
Romanovsky-stained imprints of lymph nodes with 'lymphosarcoma'.
The cell is the same size as a large lymphocyte. The pleomorphic
nucleus has a reticulated chromatin pattern and a nucleolus whose edge
is rimmed with dense chromatin. The nucleolus may be located near the
centre of the nucleus; it becomes more prominent if the
Romanovsky-stained film is prepared on a slide previously smeared with
brilliant cresyl blue. The slate-grey cytoplasm may be scanty or
abundant and may contain azurophilic granules.
109
THE PERIPHERAL BLOOD FILM
MORPHOLOGY OF NORMAL PLASMAPOIETIC CELLS
Plasmablast (15-20 Mm)
The plasmablast has a large centrally located nucleus with a single small
nucleolus and fine dark-staining chromatin. The cytoplasm is deeply
basophilic except for a narrow pale area immediately adjacent to the
nucleus. The acid phosphatase reaction is strong but is inhibited by
L(+) tartaric acid.
Proplasmacyte
The proplasmacyte may be larger than the blast cell. The nucleus is
usually located in an eccentric position, the chromatin is coarse and a
small blue nucleolus may be seen. The cytoplasm is deeply basophilic
with an area of pallor adjacent to the nucleus. Vacuoles may be present.
Morphology of abnormal plasmapoietic cells
Malignant plasma cells - 'myeloma' cells (see Plate 37)
Malignant cells of the plasma cell series are seen in myelomatosis, a
malignant disease that principally involves the bone marrow and is
characterized by a monoclonal gammopathy in the serum. As with
leukaemia of other cell lines, myelomatosis may show a preponderance
of plasmacytic or plasmablastic cells. In the plasmacytic type, the cells
may be morphologically indistinguishable from normal cells, thus
making haematological diagnosis difficult. A moderate increase in
binucleate and multinucleate cells may be seen; this feature is not
diagnostic because it also occurs in reactive plasmacytosis of the bone
marrow. Malignancy, however, may be suspected if the cells show a
monotonous morphology and focal aggregation in the bone marrow
smears.
The malignant plasmablast may be oval in shape and 1 5 - 2 5 μπι in
diameter. The eccentric nucleus has dense clumped chromatin. A single
large prominent nucleolus is present. Multinucleolation and intranuclear
Russell body-like inclusions may be seen but are not diagnostic of a
malignant change in plasmoblasts. The cytoplasm is deeply basophilic
or grey-blue in colour. Inclusions similar to those seen in mature cells
may be present. On rare occasions an Auer rod-like structure, which is
peroxidase negative, may be seen. Giant multinuclearity of plasmablasts
(megakaryocytoid plasmablasts) (see Plate 38) may be observed in some
patients with myelomatosis (Di Guglielmo, 1966; Herbut and Erf, 1946,
Gunn and Mahle, 1938; personal observation). The cellular diameter is
greater than 35 μηι; up to 20 nucleolated nuclei with coarse clumped
chromatin may be piled up in the cell. The slate grey or blue cytoplasm
is abundant, has an irregular edge and may contain vacuoles. The cell
110
LYMPHOPOIESIS, PLASMAPOIESIS, NON-HAEMOPOIETIC CELLS
resembles a megakaryocyte but lacks the nuclear lobulation, chromatin
pattern and cytoplasmic granulation of the latter cell. Cytochemically
the acid phosphatase reaction is strong. ATPase activity is less than
normal. The majority of malignant plasma cells show a marked increase
in acid acetate esterase activity and big dye aggregates may be seen in
some cells (Szmigielski, litwin and Zupanska, 1965). The PAS reaction
is variable; when it is positive the magenta staining may be diffuse or
localized in the form of irregular granules. Intranuclear inclusions and
Russell bodies also give a positive PAS reaction.
NON-HAEMOPOIETIC CELLS
Normal non-haemopoietic cells present in the bone marrow cavity are
stromal cells, vascular cells and bone cells (Table 9.1). The fibroblasts
and their fibres provide the supporting framework for the haemopoietic
cells. The endothelial cells line the capillaries and sinusoids while the
bone cells occur at the junction of marrow and bony tissue. In certain
pathological states, abnormal cells appear. They must be indigenous to
the marrow or are foreign tissue cells.
TABLE 9.1
Non-haemopoietic Cells
Normal cells
Stromal cells
Fibroblasts
Fat cells
Mast cells
'Fixed' macrophages or histiocytes
Vascular cells
Endothelial cells
Bone cells
Osteoblasts
Osteoclasts
Abnormal cells
Histiocytes
Sea-blue histiocyte
Gaucher cell
Niemann-Pick cell
Reed-Sternberg cell
Vascular cell
Leukaemic reticulo-endotheliosis (LRE) cell
Foreign tissue cell
Metastatic carcinoma cells
111
THE PERIPHERAL BLOOD FILM
NORMAL NON-HAEMOPOIETIC CELLS
Stromal cells
Fibroblast
The fibroblast is a flattened stellate cell with abundant basophilic
cytoplasm and a round or ovoid nucleus containing one or more
prominent nucleoli. The fibrocyte is a quiescent fibroblast and is
spindle-shaped with a pale ovoid nucleus and scanty cytoplasm. The
fibrous meshwork supporting haemopoietic tissue is derived from the
fibroblast and is composed of reticulin and/or collagen fibres. Although
these fibres are essentially similar when examined by electron
microscopy, they appear different by light microscopy and are
distinguished by cytochemical methods. Reticulin is composed of fine
branching fibres that are argyrophilic and do not stain with van
Gieson's stain. Collagen fibres on the other hand are straight or wavy
non-branching fibres that lie singly or in coarse bundles. They stain red
with van Gieson's stain and green or blue with Masson's trichrome stain;
they are biréfringent with polarized light and are not argyrophilic.
Fat cell
The fat cell is a large round or oval cell with a single large vacuole, an
inconspicuous nucleus displaced to one side and a thin rim of
cytoplasm surrounding the vacuole. The vacuole contained neutral fat
which was dissolved out during the staining of the film.
Mast cell
The tissue mast cell must not be confused with the basophil
leucocyte. The morphology is described in Chapter 3.
'Fixed' macrophage or histiocyte (20 - 30 Mm)
The 'fixed' macrophage or histiocyte has an irregular outline and a
round or oval nucleus located in an eccentric position in the cell. The
nucleus stains a pale violet colour and has a fine reticular chromatin
pattern. A nucleolus is usually present. The abundant cytoplasm is pale
blue, contains a few azurophilic granules and may be vacuolated. The
cell is readily distorted and disrupted when preparing smears of
aspirated bone marrow material. The cell belongs to the reticuloendothelial system (RES) or mononuclear phagocytic system (MPS). It
is better recognized when it contains phagocytosed material such as cell
nuclei, nuclear fragments, other cell debris and haemosiderin. These
materials are derived from abnormal erythroblasts, extruded nuclei of
late erythroblasts, haemoglobinized erythroblastic cytoplasm that has
escaped with the extruded nucleus, senescent and abnormal
erythrocytes and leucocytes. The haemosiderin appears as blue-black
granules or masses; they give a positive Prussian blue reaction.
112
LYMPHOPOIESIS, PLASMAPOIESIS, NON-HAEMOPOIETIC CELLS
Cytochemically the acid phosphatase reaction is strong in the cells but
activity is inhibited by l/ + ) tartaric acid; they also give a positive
alkaline phosphatase reaction.
Vascular cells
Endothelial cell ( 1 5 X 9 μιη)
The endothelial cell is a long spindle-shaped or round cell with an
oval nucleus; the chromatin is dense and a nucleolus may be visible.
Sometimes the nucleus appears pyknotic. The cytoplasm is profuse and
pale blue with a cloudy texture. Bare nuclei are commonly seen because
of cytoplasmic rupture and dispersion during preparation of the film.
Bone cells
Osteoblast (35 X 20 μχή)
Osteoblasts may be confused with plasma cells. However, they are
larger, have two to three nucleoli and contain a circular polychromatic
flair at some distance from the nucleus and never adjacent to it. The
cytoplasm is intensely basophilic and contains no vacuoles.
Osteoclast (100 μνα or more)
The osteoclast is a giant multinucleated bone cell. Usually only a
fragment of the cell may be observed in smears of aspirated bone
marrow. The number of nuclei depends on the size of the fragment
which may measure 100 μηι (or more) in diameter. The nuclei have a
sponge-like structure and a small blue nucleolus is visible in each
nucleus. The cytoplasm is pale blue and may be finely granular.
Sometimes azurophilic bodies which may represent degradation
products of bone substance may be observed.
ABNORMAL NON-HAEMOPOIETIC CELLS
Abnormal histiocytes
Sea-blue histiocyte (20 - 60 μτη) (Table 9.2)
The sea-blue histiocyte has a single eccentric nucleus with a medium
size nucleolus. The cytoplasm is foamy and contains few to many
sea-blue or blue-green granules of varying size (up to 4 μπι), shape and
staining intensity; the number of granules in some cells may be so
numerous as to obscure the nucleus. Cytochemically these granules give
positive Sudan black B, Nile blue sulphate, acid phosphatase and PAS
(diastase resistant) reactions. The negative toluidine blue reaction helps
to distinguish this cell from the tissue mast cell.
The sea-blue histiocyte can occur as a hereditary or an acquired
anomaly. Many sea-blue histiocytes packed with granules are seen in the
bone marrow and other organs (liver, lungs, gastro-intestinal tract,
113
THE PERIPHERAL BLOOD FILM
TABLE 9.2
Sea-blue Histiocyte
Hereditary abnormality
Sea-blue histiocyte syndrome
Acquired abnormality
Hereditary disorders
Hurler's syndrome
Niemann-Pick disease
Tay-Sachs disease
Wolman's disease
Sickle cell disease
Acquired disorders
Chronic granulomatous disease of childhood
Hyperlipoproteinaemia
Vitamin E deficiency
Diets containing excessive amounts of polyunsaturated fats
Hodgkin's disease
Myelocytic leukaemia
Di Guglielmo's syndrome
Polycythaemia rubra vera
Rheumatoid arthritis
central nervous system) in an hereditary (autosomal recessive)
syndrome occurring predominantly in subjects from the Carribean area
(Sawitsky, Rosner and Chodsky, 1972). The syndrome is characterized
by hepatosplenomegaly, mild thrombocytopenia, streaky pulmonary
infiltrates, skin pigmentation, optic atrophy and a white foveal ring.
The acquired anomaly is seen in miscellaneous conditions; its
pathogenesis is not known. The cells are frequently observed in
disorders with excessive production of lipid-rich cells or with marked
intramedullary lysis of cells (Silverstein and Ellefson, 1972: Dosik,
Rosner and Sawitsky, 1972).
Gaucher cell (20 - 80 Mm)
The Gaucher cell is a large round, oval or spindle-shaped cell with
abundant pale blue-grey cytoplasm showing a striated, fibrillary or
wrinkled appearance due to the presence of fine fibrils arranged parallel
to the long axis of the cell. One or more pyknotic nuclei may be
located eccentrically or centrally in the cell. The PAS reaction gives
variable degrees of positivity and fat stains are negative. The Prussian
blue reaction may indicate the presence of haemosiderin which may
have originated from catabolized haemoglobin of phagocytosed red
cells. The morphology of the cell, which at times may appear foamy, is
due to lipid accumulation within the cytoplasm. The cell occurs in
Gaucher's disease, a hereditary disorder which is characterized by gluco114
LYMPHOPOIESIS, PLASMAPOIESIS, NON-HAEMOPOIETIC CELLS
cerebrosidase deficiency. Similar cells have also been observed as an
acquired anomaly in congenital dyserythropoietic disorders, myelocytic
leukaemia and beta-thalassaemia major; in these conditions only a few
cells occur.
Niemann-Pick cell (20 - 50 μιη)
The Niemann-Pick cell is a large round, oval or polyhedral cell with a
centrally or eccentrically located nucleus. The pale blue cytoplasm may
have a honey-comb or foamy appearance. The vacuolation is due to the
accumulation of cholesterol and sphingomyelin in the cytoplasm.
Rarely, phagocytosed red cells may also be present within the
cytoplasm. The cell occurs in Niemann-Pick disease, a hereditary disorder which is characterized by a deficiency of a sphingomyelincleaving enzyme in histiocytic cells of the reticulo-endothelial system.
Similar cells have also been observed as an acquired anomaly in
hyperchylomicronaemia, hypercholesterolaemia and in Tangier disease
(familial high density lipoprotein disease).
Reed-Sternberg cell (25 - 80 μτή)
The size and shape of the Reed-Sternberg (R-S) cells is variable. Up
to 10 round, ovoid or indented nuclei may be present. A giant cell with
a bizarre polymorphoid nucleus may be seen. Nuclear chromatin is
coarse and aggregated into clumps. A characteristic feature of the cell is
the large nucleolus which is usually clearly visible; this feature is
important for distinguishing the giant R-S cell from other large cells
such as osteoclasts, erythroid gigantoblasts, megakarocytic cells and
megakaryocytoid plasma cells which may occur in the bone marrow.
The cytoplasm of the R-S cell is homogenous and pale blue; it may
appear granular or show vacuolation. The R-S cell may be observed in
the bone marrow of patients with Hodgkin's disease. Rarely the cell has
also been seen in the peripheral blood in this disease
Abnormal vascular cells
Leukaemic reticulo-endotheliosis (LRE) cell
The leukaemic reticulo-endotheliosis (LRE) cell has been described
and discussed in the atypical mononuclear section of Chapter 5.
According to Yam, l i and Finkel (1972) the LRE cell may be derived
from sinusoidal endothelial cells of the reticulo-endothelial system.
Foreign tissue cells
Metastatic carcinoma cells
The metastatic carcinoma cell is larger than all haemopoietic cells
except megakaryocytes and abnormal giant cells. The nucleus may
occupy the greater part of the cell and is usually eccentric in location.
115
THE PERIPHERAL BLOOD FILM
The chromatin is dense and the nucleoli are large. Occasionally mitotic
activity may be observed. The cytoplasm varies from a scanty to an
abundant amount; it is basophilic and has an irregular margin and may
contain vacuoles or granules. Mucus-secreting carcinoma cells give a
strongly positive PAS reaction.
The morphology of metastatic carcinoma cells varies according to the
type and site of origin of the cells which may be the lung, liver, breast,
thyroid or prostate. Common features are the pleomorphism of the
cells and the nucleoli. The cells are often clumped together but isolated
cells may be seen. Tumour cells are rarely detectable in direct
peripheral blood films but may be demonstrable in leucocyte
concentrates. When tumour cells are seen either in buffy coat smears or
in bone marrow smears and sections, it may not be possible to establish
with certainty their primary site of origin.
116
10
The Peripheral Blood Film
THE BLOOD FILM
Definition: distribution of cells
The peripheral blood film is a sheet of red cells with diffusely scattered
leucocytes and platelets. For descriptive purposes it may be divided
into a head, body and tail (Figure 13). The thickness of the film
decreases from the head to the tail. There is marked overlapping and
piling up of the red cells in the head of the film and this decreases
towards the tail where the red cells are widely separated and show
morphological distortion. The majority of the lymphocytes are present
AB
C
}
Figure 13. The peripheral blood film (A, head of blood film; B, body of blood
film; C, area of ideal film thickness; D, tail of blood film)
in the body, while neutrophils and monocytes are unevenly distributed
throughout the film and in a badly spread film many are found at the
long free margins and in the trails of the tail. Leucocytes in the head
and greater part of the body of the film may show crush anomalies. The
ideal film thickness for microscopic examination is that area where the
red cells are one layer deep with their edges almost touching and where
distortion of leucocyte morphology is minimal. Physically the area is
situated between the body and the tail of the film. The pattern of
platelet distribution is dependent on whether the film was made with
capillary blood or with anticoagulated venous blood. In a capillary
blood film the platelets are unevenly dispersed among the red cells.
Varying size masses composed of adherent platelets may be seen,
particularly at the free margins and at the end of the trails in the tail.
117
THE PERIPHERAL BLOOD FILM
The platelets in anticoagulated venous blood rarely adhere to one
another. In a film made with this blood the platelets are relatively
evenly spread among the red cells; this distribution facilitates a
semi-quantitative determination of their number.
Appearance of a well-spread and well-stained blood film
A blood film must be well spread and well stained for accurate
assessment and interpretation of the microscopic picture. The
macroscopic appearance of a well-spread and unstained blood film has
been described in Chapter 2. After Romano vsky staining the film
should be bluish-pink in colour and microscopically the cells in the area
of ideal film thickness should appear as described in Chapters 3,4 and 5
and in Chapters 7, 8 and 9. The spaces between the cells (the dried
plasma areas) should be clear; there should be no stain precipitate in
any part of the film. Factors which may be responsible for a poorly
stained blood film are: a high plasma protein content, numerous
leucocytes, anaemic blood, a film that is too thick or too thin, poor
stain reagents, understaining, overstaining or the use of buffered water
at the wrong pH value. An unsatisfactory blood film is best discarded
except when it is not possible to prepare another film.
EXAMINATION OF THE BLOOD FILM
Technique and check list
A systematic technique is essential for the microscopical examination
of the stained blood film. The inexperienced will find a check list
(Table 10.1) of value for a thorough inspection. If mounting with a
coverslip is not desired, smear a little immersion oil over the film. Then
scan at low magnification (X 100) to assess the quality of the film and
to locate the area of ideal film thickness. The free margins and the tail
of the film must be included in the scan, as the larger nucleated cells
tend to accumulate in these areas. This preliminary inspection may
provide pertinent clues to the type of abnormality present. Rouleaux
formation of red cells, cell agglutination and the staining characteristics
of the cells are best observed at this low magnification. Leucocytosis
and leucopenia (that is, total white cell counts above and below the
limits of normality) may be readily confirmed, the predominant
leucocyte ascertained and the prominence of eosinophils, basophils,
monocytes and plasma cells determined. Features useful for leucocyte
type identification are summarized in Table 10.2. Cells not readily
recognizable as normal peripheral blood cells should be immediately
inspected at a higher magnification and categorized as to type; they
may be immature and/or atypical cells. After the scan use a high dry or
oil-immersion objective lens to examine critically the area of ideal
118
THE PERIPHERAL BLOOD FILM
TABLE 10.1
Check List
Rouleaux
Auto-agglutination
Polycythaemia (crowding
of red cells)
Degree of haemoglobinization
Red cells
absent, present
absent, present
absent, present
normochromia, hypochromia
or anisochromia
predominant abnormality
absent, present, type
absent, present, type
absent, present, type
Size and shape
Inclusions
Parasites
Precursor cells
Leucocytes
absent, present
absent, present
neutrophil, lymphocyte,
monocyte
Abnormal mature leucocytes
absent, present, type
Eosinophils, basophils
any increase
Plasma cells
absent, present
Precursor cells
absent, present, type
Leucocytosis
Leucopenia
Predominant leucocyte
Platelets
Present in normal amounts, absent, diminished, increased
Other nucleated cells
absent, present, type
TABLE 10.2
Identification of Leucocytes
Size of cell
Small (iy 2 X RBC)
Medium (2J/2 X RBC)
Large
lymphocyte
neutrophil polymorph
monocyte
Cytoplasm
Many small pink granules
Few small pink granules
Large orange-red granules
Large purple to blue granules
Transparent and light blue
Ground-glass and grey to blue
Opaque and deep blue
neutrophil
lymphocyte
eosinophil
basophil
lymphocyte
monocyte
plasma cell
cont
119
THE PERIPHERAL BLOOD FILM
Table 10.2 cont.
Nucleus
Segmented
Non-segmented
neutrophil polymorph
eosinophil polymorph
basophil polymorph
monocyte (some cells)
lymphocyte (rare, atypical)
stab granulocyte
monocyte (spongy)
lymphocyte (dense)
plasma cell (dense, eccentric)
thickness. Assess the cell morphology, carry out a differential leucocyte
count and estimate whether the platelets are within normal limits,
increased or decreased in numbers. While examination with dry
objective lenses is usually adequate, anomalies such as punctate
basophilia of red cells and toxic granulation of neutrophil polymorphs
may be detectable only with the oil-immersion lens. Blood films from
subjects who have been living in or who have recently visited areas
where diseases like malaria and filariasis are endemic should be
routinely scrutinized for the appropriate parasites.
Differential leucocyte count
The relative and absolute numbers of the different leucocytes can be
rapidly enumerated with automated equipment (the Hemalog D*) in
which the cytochemically stained cells are identified in fluid suspension
or more slowly by the microscopic examination of a Romanovskystained blood film. The Hemalog D employs continuous automation,
cytochemical staining techniques (except for lymphocytes) that are
specific for the cell, photometric counting and an electronic logic
system. The instrument contains four channels, each with its own
manifold, flow-cell and counting system for the analysis of a particular
cell type. The specifically stained cells, in fluid suspension, are
identified by their absorption and light-scattering characteristics, and
not by the pattern of their contents or shape. Lymphocytes are
counted by a sizing technique. The electronic logic system integrates
the information from each channel and prints out the percentages of
the various cells based on a count of 10,000 leucocytes per cell type.
Microscopical examination of a Romanovsky-stained blood film is
commonly used for the differential count. Because of the leucocyte
distribution in the film, accurate counts are not possible. To reduce this
inaccuracy, various techniques {Figure 14) the longitudinal system (Dacie
♦Manufactured by Technicon Instruments Corporation, Tarrytown, New York, U.S.A.
120
THE PERIPHERAL BLOOD FILM
Ξ)
(a)
W)
(b)
7UU
(c)
Figure 14. Leucocyte differential count systems (A, longitudinal system; B,
cross-sectional system; C, battlement system)
and Lewis, 1968), the cross-sectional system (Miller, 1966) and the
battlement system (MacGregor et al., 1940) are advocated and the
counting of 200, 300 and even 500 - 1,000 cells has been proposed.
For routine differential counts at least 100 leucocytes should be
analysed and the cells counted on a multiple manual or electronic
register. Although the differential count is commonly reported in
percentages, it is more meaningful and of greater clinical value when
expressed in absolute terms; to obtain the absolute counts multiply the
total leucocyte count (in mm 3 ) by the various percentages.
Indirect platelet count
The platelet count may be indirectly determined from the blood
film if the total red cell count is known. Ascertain the platelet to red
cell ratio in the area of ideal film thickness with the aid of an adjustable
diaphragm or a cardboard screen containing a central square window (see
Reticulocyte staining in Appendix A) inserted in an eyepiece of the
microscope; then multiply the total red cell count by this ratio
expressed as a percentage. For example, if the red cell count is 5 X 10^
per mm 3 and the ratio of platelets to red cells in the film is 1:20 (5 per
cent), then the indirect platelet count is 5 X 10^ X 5/100 = 250,000 per
121
THE PERIPHERAL BLOOD FILM
mm 3 . A rough assessment of the platelet to red cell ratio may be
rapidly made, if the approximate number of red cells per oil-immersion
lens (OIL) field in the area of ideal film thickness is known, by
counting the average number of platelets per OIL field. After some
experience this average of number of platelets per OIL field may be
used per se as a semi-quantitative guide to the platelet concentration of
the blood sample. That is, it may indicate whether the platelet count is
above, below or within normal limits. The indirect platelet count is
useful if the original blood sample is no longer available for carrying out
a direct count. It is also of value for checking the relative accuracy of a
direct count if the blood film suggests that there may be a gross error.
The indirect platelet count method, however, is inapplicable if platelet
clumping is present in the film.
Measurement of cell diameters
Cell diameters in the blood film may be measured with a disc
micrometer placed on a shelf in one eyepiece of the microscope. The
disc micrometer is a flat circular piece of clear glass with an etched scale
at its centre. Before use, however, the etched scale requires calibration
for the particular microscope; a 2 mm micrometer slide, that is, a
microscope slide with a 2 mm scale divided at 0.01 mm (10 μτή)
intervals, or a blood cell counting chamber may be used for this
purpose. The eyepiece micrometer may be employed for the determination of the mean corpuscular diameter (MCD) of the red cells in
the blood film and for the construction of a Price-Jones curve (graphic
illustration of the numbers of various sized red cells. In practice the
method is tedious. The MCD is more readily estimated by employing
the principles of light diffraction through a grating such as that formed
by the red cells in the thin part of the blood film (Pijper, 1919,1929,
1935; Emmons, 1927; Eve, 1929; Pryce, 1929; Haden, 1940). Instruments for measuring the MCD are called eriometers (Emmons, 1927)
and halometers (Eve, 1929) and are available commercially. The construction of simple laboratory halometers using one and two light
sources has been described by Pryce (1929). Today the measurement of
red cell MCD is hardly ever carried out. The mean corpuscular volume
(MCV) of red cells, which is accurately determined by electronic blood
cell counting machines such as the Coulter S, has now replaced the
MCD as the parameter of red cell size.
THE NORMAL BLOOD FILM
Familiarity with the appearance of the 'normal' blood film and
knowledge of the 'normal ranges' of the haematological parameters for
a particular population are prerequisites for the recognition of blood
122
Up to 2
Reticulocytes (%)
Up to 2
150-450
150-450
150-450
Up to 2
5-16
3-8
40-70
2-6
30-40
200-800
2-5
40-600
1-3
0-200
0-1
4-12
2-7
40-70
1-4
20-45
200-800
2-5
40-400
1-4
0-200
0-1
4-12
2-7
40-70
1-4
20-45
200-800
2-8
40-400
1-4
0-200
0-1
12-16
35-45
3.5-5.5
75-99
24-30
30-35
Leucocytes ( 1 0 3 m m 3 )
Neutrophils ( 1 0 3 / m m 3 )
(%)
Lymphocytes ( 10 3 /mm 3 )
(%)
Monocytes (mm 3 )
(%)
Eosinophils (mm 3 )
(%)
Basophils (mm 3 )
(%)
Platelets ( 1 0 3 / m m 3 )
12-18
35-55
3.5-6.0
77-99
27-32
30-35
Child
over 4 years
13-20
40-60
4-7
77-99
27-32
30-35
Adult
female
Haemoglobin (g/100 ml)
Haematocrit (%)
RBC(106/mm3)
MCV(Mm 3 )
MCH (pg)
MCHC (%)
Adult
male
Peripheral Blood Cells - Normal Ranges
TABLE 10.3
100-350
4H6
Up to 2
18-25
8-20
40-80
2-4
30
200-800
2-5
200-800
1-3
0-200
0-1
14-21
45-62
6.5-7.5
85-120
24-34
27-34
Neonatal
infant
150-450
6-18
2-8
30-40
2-8
50-60
200-800
2-5
40-600
1-3
0-200
0-1
13-16
36-44
4-5
75-99
24-30
28-33
Child
under 4 years
THE PERIPHERAL BLOOD FILM
abnormality. The haematology profile (or blood formula) of a healthy
child changes from the neonatal period to the pubertal stage of life.
After puberty some red cell parameters depend on the sex of the
individual (Table 10.3); this difference is less marked in the elderly. The
profile of any subject may be further modified by geographic location
(for example, high altitude affects the red cell count), their ethnic
group (which may influence the differential leucocyte count) and the
laboratory technique used in determining the quantitative data. Care
must also be exercised in interpreting the data, particularly the values
near the upper and lower limits of the normal ranges. Each individual
has his own normal profile, and values which are normal for one person
may be abnormal for another.
Blood film of an adult
The red cells are normochromic normocytes; an occasional
polychromatic cell (less than 2 per cent of red cells) may be noticed.
The leucocytes are distributed as previously described. The neutrophil
polymorphs (PMN) are usually predominant. The percentages of PMN
with 2, 3, 4 and 5 lobes are given in Table 10.4; the average number of
lobes ranges from 2.3 to 3.0 per PMN. Drumstick appendages are seen
in up to 16 per cent of the PMN in the blood film of a female subject ;this
appendage is not usually seen in the blood film of a male subject. An
TABLE 10.4
Segmented Neutrophil Lobe Count
2 lobes
26-36%
3 lobes
42^8%
4 lobes
17-19%
5 lobes
0-3%
Lobe average
2.3-3.0
occasional stab cell (less than 1 per cent of leucocytes) may be observed.
The lymphocyte is the next most prominent leucocyte; the larger type
is more noticeable in the thinner parts of the film. A few monocytes
and an occasional to a few eosinophils are present. Platelets are
distributed as previously described.
Cells that may occasionally be observed in small numbers are
spherocytes, stomatocytes, oval-shaped red cells, target cells,
myelocytes, atypical lymphocytes and megathrombocytes. A rare
hypersegmented neutrophil may be noticed. In African subjects due to
genetic (Shaper and Lewis, 1971) and/or dietary (Ezeilo, 1972) factors,
the lymphocyte rather than the neutrophil is the predominant
leucocyte in the blood film.
124
THE PERIPHERAL BLOOD FILM
Blood film of a child
The red cells are normocytic and may appear hypochromic; an
occasional polychromatic cell (less than 2 per cent of red cells) may be
noticed. Under the age of 4 years lymphocytes are predominant and
over that age the neutrophil polymorph becomes the predominant
leucocyte. At the age of 4 years the percentage of lymphocytes and
neutrophil polymorphs are equal. A few monocytes and an occasional
to a few eosinophils are present. Platelets are distributed as previously
described.
Blood film of a neonatal infant
Good films may be difficult to prepare because of the high
haematocrit. The red cells are normochromic macrocytes and are
crowded together, even in the area of ideal film thickness. Late
normoblasts, 3 - 10 per 100 leucocytes, are seen and an occasional
intermediate normoblast may be present. In comparison with an adult
blood film there is a leucocytosis with the neutrophil polymorph as
predominant cell (after 2 weeks, the lymphocyte becomes the
predominant leucocyte). Morphological distortion of the cells may be
seen. Up to 10 per cent of the leucocytes may be immature cells
(myelocytes, metamyelocytes and stab cells). There are a moderate
number of large lymphocytes, a few monocytes and an occasional
eosinophil. Platelets are distributed as previously described; because of
the red cell crowding they may appear to be reduced in number.
125
11
Abnormal Blood Films
CLASSIFICATION
An abnormal blood film is one in which quantitative and/or qualitative
abnormalities are observed in one or more of the classes of
haemopoietic cells. The terminology used to indicate that specific
cellular concentrations lie above or below the accepted limits of
normality are listed in Table 11.1. For descriptive purposes the film
TABLE 11.1
Terminology of Cell Counts Outside Normal Ranges
Limits of normality
Below lower
Above upper
red cells
Hbg%
PCV%
X 10 6 /mm 3
leucocytes
X 10 3 /mm 3
neutrophils
X 10 3 /mm 3
eosinophils
X - /mm 3
basophils
X - /mm 3
monocytes
X - /mm 3
lymphocytes
X 10 3 /mm 3
plasma cells
X - /mm 3
platelets
X 10 3 /mm 3
126
anaemia
erythraemia / polycythaemia vera
erythrocytosis
leucopenia
leucocytosis
neutropenia
neutrophilia
eosinopenia
eosinophilia
—
basophilia
—
monocytosis
lymphocytopenia
lymphocytosis
—
plasmacytosis
thrombocytopenia
thrombocytosis
thrombocythaemia
ABNORMAL BLOOD FILM
appearances of the red cells, leucocytes and platelets may be classified
as shown in Tables 11.2, 11.4 and 11.7.
TABLE 11.2
Abnormal Film Appearances of Red Cells
A. Normochromic red cells
B. Hypochromic red cells
Normocytic type
Normocytic type
Microcytic type
Microcytic type
Round macrocytic type
Micro-macro-ovalocytic type
Oval macrocytic type
Leptocytic (target cell) type
Stomatocytic type
C. Anisochromic red cells
Dimorphic type
D. Abnormally shaped red cells
E. Inclusion-containing red cells
Elliptocytic type
Howell-Jolly body type
Spherocytic type
Siderocytic type
Sickle cell type
Stippled cell type
Irregular poikilocytic type
F. Immature red cells
G. Aggregated red cells
Polychromatic cell type
Rouleaux type
Erythroblastic type
Auto-agglutination type
The abnormal film appearances of the red cells (Table 11.2) can be
divided into seven categories: films with normochromic red cells,
hypochromic red cells, anisochromic red cells, abnormally shaped red
cells, inclusion-containing red cells, immature red cells and aggregated
red cells. Normochromic normocytic, normochromic macrocytic,
hypochromic normocytic, hypochromic microcytic, leptocytic (target
cell type), poikilocytic and polychromatic cell types are the most
frequently seen abnormal films of red cells. Of the two quantitative
abnormalities, anaemia and polycythaemia, the former is the more
common. Clinically, absolute anaemia is a symptom complex and not a
disease. It may occur as a congenital or an acquired abnormality and
results from diminished production of red cells in the bone marrow or
loss of mature red cells (Table 11.3). Good films may be difficult to
TABLE 11.3
Pathogenesis of Anaemia
Diminished production of red cells
Hypoplasia of erythropoietic tissue (Table 7.2)
Ineffective erythropoiesis (Table 7.1 C)
Loss of mature red cells
Haemorrhage (Table 12.6)
Haemolysis (Table 12.8)
127
THE PERIPHERAL BLOOD FILM
prepare from markedly anaemic blood, it may be necessary to
centrifuge an aliquot of blood, remove some of the supernatant plasma
and then spread the film after thorough resuspension of the cells. The
blood film appearance of the majority of the anaemias is generally
characterized by an exaggeration of the normal variation in red cell size,
the degree of anisocytosis being proportionate to the severity of the
anaemia. Elliptocytosis (oval-shaped red cells) and poikilocytosis are
commonly present. Other abnormal red cells and in some anaemias
immature erythropoietic cells may be seen. If the fall in blood
haemoglobin concentration occurs pan passu with the decrease in the
red cell count or haematocrit, the red cells appear normochromic, but if
it is greater, the red cells are hypochromic; the degree of hypochromia
depends on the extent of the dissociation. Anaemias due to loss of red
cells by haemorrhage or haemolysis are usually characterized by
polychromatophilia and/or macrocytosis due to erythropoietic
stimulation and early release of reticulocytes from the bone marrow.
Polycythaemia (see Table 12.2) is also a symptom complex.
Absolute polycythaemia may be congenital or acquired, primary or
secondary, and results from the production of an excessive number of
red cells by hyperplastic tissue in the bone marrow (see Table 7.1 A, B).
Primary polycythaemia may be considered to be a mild form of
neoplasia and is one of the myeloproliferative disorders. The
morphology of the erythroblasts, however, appears normal. Neoplasia
of erythropoietic tissue is characterized by the presence of malignant
erythroblasts and is termed erythraemic myelosis or erythroleukaemia,
depending on whether the myelopoietic (granulocytic) cells are also
involved in the malignant process. These two types form part of a
spectrum of neoplastic change generally referred to as Di Guglielmo's
syndrome.
The abnormal film appearance of leucocytes (Table 11.4) can be
broadly divided into two categories: the predominant leucocyte and the
prominent leucocyte. Leucocytosis occurs more frequently than
leucopenia and is commonly due to an elevation of the absolute
neutrophil or lymphocyte counts which result from neoplasia
(leukaemia) or from some stimulus (neutrophilia and lymphocytosis
respectively). Neutrophilia may be due to migration of polymorphs
TABLE 11.4
Abnormal Film Appearances of Leucocytes
Predominant leucocytes
A. Films with predominant neutrophils
Relative neutrophilia, absolute lymphocytopenia type
128
cont.
ABNORMAL BLOOD FILM
Table 11.4 cont.
Absolute neutrophilia type
Neutrophilic leukaemoid type
Leuco-erythroblastic type
Myelocytic (granulocytic or chronic myeloid) leukaemia
Promyelocytic (progranulocytic) leukaemia
Myeloblastic (acute myeloid or granulocytic) leukaemia
Paramyeloblastic leukaemia
Di Guglielmo's syndrome - erythraemic myelosis: erythroleukaemia
Myelomonocytic leukaemia
B. Films with predominant lymphocytes
Relative lymphocytosis, absolute neutropenia type
Pancytopenia type
Absolute lymphocytosis type
Lymphatic leukaemoid type
Lymphocytic (chronic lymphocytic) / lymphosarcoma cell
(chronic lymphosarcoma cell) leukaemia
Lymphoblastic (acute lymphatic) leukaemia
Myeloblastic leukaemia
Erythroleukaemia (Di Gugleilmo's syndrome)
Prominent leucocytes
A. Films with prominent atypical neutrophils
Pelger-Huèt / pelgeroid type
Hypersegmented neutrophil type
Neutrophil polymorphs with basophilic granules
Neutrophil polymorphs with basophilic inclusions
B. Films with prominent atypical lymphocytes
Lymphocytes with notched nuclei
Lymphocytes with vacuolated cytoplasm
C. Films with prominent monocytes
Absolute monocytosis type
Monocytic leukaemoid type
Myelomonocytic leukaemia
D. Films with atypical mononuclear cells
Mononucleosis type
Leukaemic reticulo-endotheliosis or 'hairy' cell leukaemia
E. Films with prominent eosinophils
Absolute eosinophilia type
Hypereosinophilia type
'Eosinophilic' leukaemia
F. Films with prominent basophils
Absolute basophilia type
G. Films with prominent plasma cells
Plasmacytosis type
Myeloma type
Plasma cell leukaemia
129
THE PERIPHERAL BLOOD FILM
from the extramedullary marginated pool of cells into the circulating
pool. However, it is commonly associated with hypercellularity of the
myelopoietic (granulocytic) tissue in the bone marrow (see Table 8.2 A,
B). Lymphocytosis results from antigenic stimulation of the
lymphocyte which undergoes blastogenic transformation and proliferation in the peripheral (secondary) lymphoid organs. Leucopenia in
adults and older children is due to absolute neutropenia (Table 11.5)and
in children below the age of 4 years to absolute lymphocytopenia
(Table 11.6).
TABLE 11.5
Pathogenesis of Neutropenia
Diminished production of neutrophils
Hypoplasia of myelopoietic (granulocytic) tissue (Table 8.3)
Ineffective myelopoiesis (granulopoiesis). (Table 8.2 C)
Loss of mature neutrophils
Sequestration in spleen, inflammatory sites, etc.
Destruction or lysis (Table 12.47)
TABLE 11.6
Pathogenesis of Lymphocytopenia
Failure of primary lymphoid organs particularly thymus
Defect of stem cells
Defect of thymic environment
Failure of secondary lymphoid organs
Nutritional deficiency
Endocrinopathies
Neoplasias
Immunosuppressive therapy
Loss of lymphocytes
Immunosuppressive therapy
Autocytotoxins and autocytolysins
The second category — prominent leucocyte — contains film
abnormalities of leucocytes normally not present in great numbers in
the blood, of certain atypical leucocytes and of plasma cells. Relative or
absolute increase in their numbers make these cells appear prominent in
the film which may be predominantly neutrophilic or lymphocytic.
Occasionally the cell concentrations may be sufficiently elevated not
only to affect the total white cell count but also to make them the
predominant cell in the film.
130
ABNORMAL BLOOD FILM
The abnormal film appearance of platelets (Table 11.7) can be
divided into four categories: films with increased number of platelets,
decreased number of platelets, atypical platelets and aggregated
platelets. Thrombocytosis and thrombocytopenia are the principal
abnormalities seen. Thrombocytosis results from overproduction of
TABLE 11.7
Abnormal Film Appearances of Platelets
A. Films with increased number of platelets
Thrombocytosis type
Thrombocythaemic type
B. Films with decreased number of platelets
Thrombocytopenic type
C. Films with atypical platelets
Megathrombocytosis
Microthrombocytosis
D. Films with aggregated platelets
Auto-agglutination type
Platelet satellitism
platelets by megakaryocytes (which have increased in numbers) and
represents a temporary and reversible increase in the platelet count. The
term thrombocythaemia is used to indicate an irreversible elevation of
the platelet count; the cells may be morphologically and/or qualitatively
abnormal. Thrombocytopena may be a congenital or an acquired
abnormality which results from diminished production in the bone
marrow and/or loss of platelets from the circulation (Table 11.8).
TABLE 11.8
Pathogenesis of Thrombocytopenia
Diminished production of platelets
Hypoplasia of megakaryocytes (Table 8.5)
Ineffective thrombopoiesis (Table 8.4)
Megakaryocytolysis
Loss of platelets
Sequestration in spleen, etc.
Excessive consumption
Thrombocytolysis
ABNORMAL FILM APPEARANCES OF RED CELLS
A. Films with normochromic red cells
Normocytic type (see Tables 12.1 -12.3)
The red cells are normochromic and essentially normocytic in size. In
131
THE PERIPHERAL BLOOD FILM
addition to being seen in normal blood, this type of film may be
observed in polycythaemia as well as in anaemia (see Table 12.1). In
uncomplicated cases of polycythaemia the blood film is usually thick
and microscopically the red cells are crowded together even in the area
of ideal film thickness (see Plate 39). Polycythaemia (see Table 12.2)
may be of the relative or spurious type due to an acute reduction of
plasma volume; the red cell mass is usually normal and may be
decreased. Absolute polycythaemia (venous haematocrit greater than
53 per cent in females and greater than 60 per cent in males), in which
the red cell mass is increased, may be erythraemic or erythrocytic in
type. The former is a true polycythaemia and one of the
myelproliferative disorders. It is distinguished from the erythrocytic
type by the presence of a panmyelosis in the blood and bone marrow.
Immature red cells and neutrophils are seen in the film and there may
be an eosinophilia and/or basophilia. In addition the serum vitamin B 1 2
level may be elevated and the leucocyte alkaline phosphatase (LAP)
score is increased. The erythrocytic type or secondary polycythaemia is
seen more frequently. While normoblasts may be observed in the film,
neutrophilia and thrombocytosis are not usually present unless there
are complications in the disorders in which erythrocytosis occurs.
Films of anaemic blood do not show red cell crowding in the area of
ideal film thickness. Anisocytosis, some poikilocytosis and elliptocytosis are usually present unless the anaemia is mild. The anaemia may
be relative (pseudo-anaemia) or absolute and pathogenically divided into
six types (see Table 12.1). Anaemia due to failure of erythropoietic
tissue is often associated with neutropenia and thrombocytopenia
(pancytopenia) and is then termed aplastic anaemia. Replacement/
infiltration of haemopoietic tissue may also produce a leucoerythroblastic type of blood film. Haemorrhage, and erythropoietic
depression that occurs in chronic disorders are the commonest causes of
normochromic normocytic anaemia. Assessment of red cell chromicity
in anaemias of chronic disorders is often subjective and some observers
may describe the red cells as hypochromic normocytes. Macrocytosis
and polychromatophilia usually accompany haemolytic anaemia.
Microcytic type (see Table 12.4)
The red cells are normochromic and there are a moderate to an
abundant number of microcytes in the film. An anaemia is commonly
present and this picture is often a prelude to the development of
hypochromic red cells.
Round macrocytic type (see Tables 12.5-12.9)
The red cells are normochromic and round macrocytes are
prominent. In polycythaemia the cells are crowded together and
132
ABNORMAL BLOOD FILM
variation in cell size is not particularly evident. In anaemia there is
marked anisocytosis and other abnormal red cells are seen; an increase
in the number of polychromatic cells is common. This picture is
suggestive of blood loss from haemorrhage (see Tables 12.6 and 12.7)
or haemolysis (see Table 12.8). The latter type of anaemia produces
unconjugated hyperbilirubinaemia which, however, may also be caused
by a number of other disorders (see Table 12.9). The association of
normochromic round macrocytes and hypochromic microcytes in the
same blood film is discussed later (see under dimorphic type).
Macro-ovalocytic type (see Tables 12.10-12.14)
The red cells are normochromic and few to many macro-ovalocy tes
are seen in the film. Anaemia is usually present, and depending on its
severity, other red cell anomalies such as anisocytosis, microcytosis and
poikilocytosis may be associated with the macro-ovalocytosis (see Plate
40). In addition, hypersegmented neutrophils and/or macropolycytes
and an increase in the lobe average of the neutrophil polymorphs may
be observed. The number of platelets in the film may be reduced. This
film appearance is characteristic of megaloblastic anaemia and is due to
vitamin B 1 2 deficiency (see Table 12.11), folate deficiency (see Table
12.13) or enzyme abnormalities that interfere with DNA synthesis (see
Table 12.14) in rapidly dividing cells. In severe anaemias a late
megaloblast may be observed in the thin film or in stained buffy coat
films. Detection of this type of blood picture in a subject with a normal
haematology profile is suggestive of megaloblastosis complicating
polycythaemia. On rare occasions patients with subacute combined
degeneration of the cord may have a normal profile and show
megaloblastosis in the bone marrow. The normochromia of the red cells
in megaloblastic anaemia may change to hypochromia soon after the
commencement of specific haematinic therapy. This is due to the
effective use and subsequent exhaustion of body iron stores. It is
particularly evident if the iron stores at the time of diagnosis are at the
lower limit of normality or already absent. Certain diseases are
associated with pernicious anaemia (see Table 12.12). The blood films
of patients with these diseases should be carefully scrutinized for
evidence of megaloblastosis.
Stomatocytic type (see Table 12.15)
A moderate number to many stomatocytes are seen in the film (see
Plate 41). Commonly target cells are also present and the patient has
alcoholic cirrhosis of the liver. This type of blood film may also appear
as a transient phenomenon in acute alcoholism. Stomatocytosis
associated with evidence of haemolysis is suggestive of a hereditary
disorder. The red cells in Rh n u n disease are characterized by
133
THE PERIPHERAL BLOOD FILM
non-agglutinability with anti-Rh typing sera and by abnormalities in
several other blood group systems (Schmidt and Holland, 1972).
B. Films with hypochromic red cells
Normocytic type (see Tables 12.16 and 12.17)
The degree of hypochromia varies from mild to moderate and the
red cells are essentially normocytic in size. Artefactual hypochromia is
often seen. Commonly this is due to the poor staining quality of the
eosin component in a particular batch of stain solution. Occasionally it
results from a bad film preparation and all the red cells appear to have a
punched-out central area of pallor surrounded by an eosinophilic
peripheral ring. The hypochromic normocytic type of blood film occurs
in polycythaemic subjects who have developed iron deficiency from
chronic haemorrhage and/or repeated phlebotomies. The blood
haemoglobin concentration, red cell haematocrit and total red cell
count may be within normal limits. In anaemic patients other red cell
anomalies may be noticed in the film; the type of abnormal red cells
depends on the clinical picture, which is commonly that of a chronic
disorder. The anaemia of chronic disorders is characterized by a low
serum iron concentration, a normal or low total iron-binding capacity
of serum, reduced percentage saturation of transferrin and
demonstrable haemosiderin in the bone marrow. The degree of
hypochromia is rarely marked except in patients who develop iron
deficiency as a complication of their chronic disorder. Assessment of
red cell chromicity is often subjective and the film appearance of the
red cells may be described as normochromic normocytic by some
examiners. The pathogenesis of the anaemia is usually complex and
varies with the disorder. There may be reduced iron absorption, toxic
depression of the bone marrow and excessive destruction of red cells;
some may be complicated by a haemorrhagic anaemia. However, lack of
iron availability, due to a block in the mobilization of iron from the
iron storage sites in the reticulo-endothelial cells, is common to all
disorders.
Microcytic type (see Tables 12.18 and 12.19)
The red cell hypochromia is moderate to marked. There are many
microcytes and a variable number of target cells and irregular
poikilocytes in the film. This type of blood picture is commonly seen in
iron deficiency anaemia (see Table 12.19) and the thalassaemias. Red
cells with basophilic stippling may be recognized in the thalassaemic
blood film. They are, however, not diagnostic of thalassaemia, and if
present to any great degree are suggestive of heavy metal poisoning,
particularly lead intoxication. Apart from the serum iron concentration, which is low in iron deficiency anaemia and normal or elevated in
134
ABNORMAL BLOOD FILM
the thalassaemias, the two conditions may be distinguished by analysis
of the quantitative parameters of the red cells. In iron deficiency
anaemia the red cell count, MCV, MCH and the MCHC are reduced.
Thalassaemia is suggested if there is a relative erythrocytosis for the
blood haemoglobin concentration, a marked microcytosis (MCV
approximately 65 Mm3), marked hypochromia (MCH approximately 20
pg) and an MCHC that is within normal limits (greater than 31 per
cent). In haemoglobin H disease (alpha thalassaemia intermedia) the
MCHC may be less than 31 per cent; it is readily differentiated from iron
deficiency anaemia by detecting Hb-H inclusions in a supravitally
stained film and by a positive heat precipitation test for unstable
haemoglobin. There may be difficulty in detecting thalassaemia if there
is co-existent iron deficiency. In these cases examination of the blood
film and the tests for thalassaemia should be repeated after an adequate
course of iron therapy. It must be remembered that chronic paroxysmal
nocturnal haemoglobinuria and persistent anaemia of chronic disorders
may present with a hypochromic microcytic type of blood picture. If
there is an associated polychromatophilia, chronic haemoglobinuria and
Di Guglielmo's syndrome must be considered unless there is a history of
acute haemorrhage. The presence of normochromic round macrocytes
is discussed later (see Dimorphic type of blood film).
Microcytic - macro-ovalocytic type (see Tables 12.20 and 12.21)
The film appears predominantly hypochromic microcytic with a few
to a moderate number of macro-ovalocytes which may be hypochromic
(see Plate 42). The picture is usually seen in nutritional anaemias and
sometimes in malabsorption syndrome (Table 12.21). The macroovalocytes may not be obvious if few in number; the overt
megaloblastosis may become evident only after iron therapy. The
presence of hypersegmented neutrophil polymorphs is not particularly
helpful in the diagnosis of megaloblastosis; these cells also occur in
blood films in iron deficiency and other disorders (Table 12.53).
Target cell or leptocytic type (see Table 12.22)
A moderate number to many target cells are present. The film
appears hypochromic because of the morphological (ring of pallor) and
physical characteristics (thinness) of the cells. The target cell type of
blood film may be an artefact of normal red cells and results from the
increasing hypertonicity that develops in the fluid surrounding
individual cells when the film dries. The true leptocytic film is
characterized by a visual macrocytosis and an MCV within normal
limits. The occurrence of volume macrocytosis (MCV greater than 100
Mm3) in leptocytosis of liver disorders is suggestive of gastro-intestinal
haemorrhage or megaloblastosis (Kilbridge and Heller, 1969). A haemo135
THE PERIPHERAL BLOOD FILM
globinopathy may be present if spherocytes and stippled cells are
observed in the film or if target cells are seen in blood films of infants,
children and young adults. Sickle cells may be found in haemoglobin S
disease; intra-erythrocytic crystals may form in haemoglobin C disease
and in haemoglobin S/C disease. Leptocytosis in the post-splenectomy
syndrome may be associated with red cells containing Howell-Jolly
bodies. Target cells are commonly present in the hypochromic
microcytic type of blood film; this film appearance has been discussed
earlier in this section.
C. Films with anisochromic red cells
Dimorphic type (see Tables 12.23 and 12.24)
The dimorphic blood film contains a mixed population of red cells.
There are hypochromic microcytes and normochromic macrocytes.
This picture may be seen in polycythaemic subjects who are becoming
iron deficient. In dimorphic anaemias, target cells, poikilocytes and
elliptocytes are present. Anisochromia without obvious polychromatophilia is commonly seen in the blood film of an iron deficient patient
who is continuing to respond to specific therapy. Here the
normochromic macrocytes are prominent, appear flat without any
central pallor and are deeply stained. Dimorphic anaemia with an
absolute reticulocytopenia is suggestive of sideroblastic anaemia. This is
characterized by a raised serum iron concentration, a normal or raised
total iron-binding capacity, an increased percentage saturation of
transferrin, ineffective erythropoietic hyperplasia, ringed sideroblasts in
the bone marrow and a considerable increase in haemosiderin in the
reticulo-endothelial cells. If folate deficiency co-exists with the
sideroblastic anaemia, macro-ovalocytes appear in the film. The above
features of sideroblastic anaemia can also be present in Di Guglielmo's
syndrome; the myelopoietic (granulocytic) tissue in this syndrome is
often leukaemic in type.
D. Films with abnormally shaped red cells
Elliptocytic type (see Table 12.25)
The red cells are normochromic and more than 25 per cent are oval
shaped; many rod forms are also present (see Plate 43). In the majority
of cases this appearance is characteristic of hereditary elliptocytosis,
and the haematology profile is within normal limits. Subjects with this
hereditary anomaly may develop anaemia in the same manner as any
other individual. However, if rod forms are not prominent and there is
morphological evidence of extramedullary haemolysis, the anaemia may
be hereditary elliptocytic anaemia and not an acquired disorder. Rod
forms are prominent in hereditary haemorrhagic telangiectasia; they are
associated with target cells in the haemoglobinopathies. As mentioned
136
ABNORMAL BLOOD FILM
previously, mild elliptocytosis (oval shaped cells prominent) occurs in
all anaemias.
Spherocytic type (see Table 12.26)
Few to many spherocytes are present in the blood film and, in
addition, there is morphological evidence of extramedullary haemolysis
such as macrocytosis and poly chromât ophilia. Hereditary spherocytosis
is characterized by spherocytes that are uniform in size and appearance
(see Plate 44). In acquired spherocytosis the spherocytes are of varying
size and commonly associated with irregular poikilocytosis and in some
cases with schistocytosis (see Plate 45). Except in hereditary
spherocytosis and acquired haemolytic anaemias, the number of
spherocytes are few and not readily evident in the film. The spherocytic
type of film is still seen after splenectomy in subjects with hereditary
spherocytosis; it is, however, modified and the blood picture may not
show the striking macrocytosis and polychromatophilia commonly seen
pre-splenectomy.
Sickle cell type (see Table 12.27)
A few to a moderate number of sickle cells are present in a film
which contains target cells, polychromatic cells, macrocytes and an
occasional spherocyte (see Plate 46). If the blood film is prepared
during an in vivo sickling crisis the number of sickled cells is increased
and the morphological evidence of haemolysis is marked. Blister red
cells may be noticed in patients with pulmonary embolism (Barreras,
Diggs and Bell, 1968). Sickle cells are not usually observed in the blood
film of subjects with the sickle cell trait (Hb-A/S) but they may become
evident if the patient undergoes general anaesthesia. Target cells are
more prominent in Hb-S/C disease; in addition, bizarrely-shaped cells
containing masses of crystallized haemoglobin may be found. In
Hb-S/thalassaemia disease, the red cells show the quantitative and
qualitative features of thalassaemia.
Irregular poikilocytic type (see Table 12.28)
The blood film, which may be normochromic, hypochromic or
dimorphic in appearance, contains a varying number of irregular
poikilocytes. Except for acanthocytosis and tear-drop poikilocytosis,
the film appearance is suggestive of a fragmentation haemolytic
anaemia. The degree of polychromatophilia is variable. Marked
schistocytosis with thrombocytopenia and evidence of haemolysis in a
patient with a 'spontaneous' bleeding diathesis indicates an acute or
decompensated disseminated intravascular coagulation (see Table 12.7).
Tear-drop poikilocytes are particularly associated with megaloblastic
anaemia and agnogenic myeloid metaplasia (myelofibrosis of the bone
marrow).
137
THE PERIPHERAL BLOOD FILM
E. Films with inclusion-containing red cells
Howell-Jolly body type (see Table 12.29)
Normochromic red cells with Howell-Jolly bodies may be observed
in small numbers in films showing evidence of haemolysis. They may
also be seen in the target cell and macro-ovalocytic types of blood
films.
Siderocytic type (see Table 12.30)
Normochromic, hypochromic or leptocytic cells with Pappenheimer
bodies are seen in this type of blood film. The cells may appear as
stippled cells and their numbers are usually small but increase after
splenectomy. They may be associated with red cells containing
Howell-Jolly bodies (haemolytic anaemias, post-splenectomy
syndrome), polychromatic cells (haemolytic anaemias), non-siderocytic
stippled cells (haemoglobinopathy, lead poisoning) or with dimorphic
cells and a reticulocytopenia (sideroblastic anaemia).
Stippled cell type (see Table 12.31)
Polychromatic, normochromic or hypochromic red cells with
punctate basophilia may be seen in small numbers in blood films, and
more readily observed in the thicker part of the film and if the film is
dried slowly (Jensen et al, 1965). The nature of the cells — whether they
are reticulocytes, thalassaemic cells or siderocytes—may be distinguished
by supravital dye staining and the Prussian blue reaction. The presence
of stippled cells in a hypochromic microcytic blood film helps to
differentiate thalassaemia from iron deficiency. Basophilic stippling is
particularly striking in lead poisoning, except in poisoning with
tetraethyl lead and in acute poisoning in children (Flink, 1971).
Heinz body type (see Tables 12.32 and 12.33)
Heinz bodies are not visible in the Romanovsky-stained blood film.
The blood picture shows an acute or compensated haemolytic anaemia
with some fragmented red cells; pyknocytes are observed in films from
premature infants. The inclusions may be noticed in the supravitally
stained reticulocyte preparation; their presence, however, is best
detected with the supravital methyl violet staining reaction. The
number of red cells with Heinz bodies depends on splenic function and
on the degree of haemolytic activity at the time of examination.
Drug-induced Heinz body anaemia is clinically characterized by
cyanosis due to excessive production of methaemoglobin within the red
cells. Other causes of methaemoglobinaemia are listed in Table 12.33.
138
ABNORMAL BLOOD FILM
F. Films with immature red cells
Polychromatic cell type (see Table 12.34)
A variable number (more than 2 per cent of the red cells) of
polychromatic cells are seen in the film which may be normochromic or
hypochromic. Macrocytosis usually accompanies the polychromatophilia; stippled cells, erythroblasts or immature neutrophils may also be
observed. This type of film commonly results from blood loss,
haemorrhage or haemolysis, and is indicative of erythropoietic
hyperactivity in the bone marrow. The presence or absence of large
polychromatic cells that are more basophilic than those commonly seen
in a blood film, should be noted. The significance of these 'shift'
reticulocytes has already been discussed in Chapter 7 (see Reticulocyte
count of blood).
Erythroblastic type (see Table 12.35)
A few to a moderate number of erythroblasts may be seen in
different types of blood films. An increase in the number of
polychromatic cells usually accompanies but does not necessarily
correlate with the erythroblastaemia. The presence or absence of
immature neutrophils is valuable in differentiating the disorders with
this blood picture. Normoblasts are seen in haemorrhagic and
haemolytic anaemias, vacuolated normoblasts in severe iron deficiency
anaemia and Di Guglielmo's syndrome, and megaloblasts in severe
megaloblastic anaemia. The blood picture of Di Guglielmo's syndrome
is described later (see Films with predominant neutrophils).
G. Films with aggregated red cells
Rouleaux type (see Tables 12.36 -12.40)
Rouleaux is a face-to-face aggregation of red cells resembling
columns of stacked coins (see Plate 47). The phenomenon probably
results from an alteration of the negative electrical charge on the
surface of the red cells and depends on the protein composition of the
plasma, particularly with respect to the fibrinogen and globulin
concentrations. Rouleaux formation of red cells occurs in subjects with
hyperfibrinogenaemia (see Table 12.37) and hyperglobulinaemia (see
Tables 12.38 and 12.39). The erythrocyte sedimentation rate (ESR) in
these patients is markedly elevated. In the blood film the columns of
aggregated red cells intertwine with one another and appear to form a
meshwork best visualized in the area of ideal film thickness. The open
spaces between the columns of cells may be clear or tinged blue
according to the pathogenesis of the rouleaux. The blue tinge is usually
seen in hyperglobulinaemia and is due to the basophilic staining of the
excess globulin that has dried in these areas. Care must be taken not to
confuse rouleaux with auto-agglutination and vice versa. The red cells
139
THE PERIPHERAL BLOOD FILM
may be normochromic or hypochromic. It may be difficult to assess
accurately the chromicity of the red cells, particularly when there is
massive rouleaux, because free red cells may be seen only in the tail of
the film where morphological distortion is marked. The shape of
spherocytes and sickle cells is not conducive to rouleaux formation and
the phenomenon is not seen in polycythaemic blood. Hyperglobulinaemia may result from exessive production of (1) a single class of
immunoglobulin by a clone of plasma cells derived from one precursor
cell (monoclonal gammopathy), or (2) a number of different classes of
immunoglobulins by more than one clone of cells derived from
different precursor cells (polyclonal gammopathy). Some disorders with
hyperglobulinaemia, particularly those due to IgM overproduction, may
exhibit cryoglobulinaemia (see Table 12.40). These cyroglobulins are
considered to be IgM auto-antibodies which form a complex with IgG
in the cold and precipitate out.
Auto-agglutination type (see Table 12.41)
Masses of irregularly aggregated red cells are scattered throughout
the blood film (see Plate 48). Free red cells are normochromic. An
occasional spherocyte, fragmented red cell and other evidence of
extramedullary haemolysis may be seen. Leucocyte agglutination,
particularly affecting neutrophils, may be evident in some films. The
auto-agglutination type of blood film is caused by warm, cold or
bithermic auto-antibodies in the plasma. The agglutinates caused by
warm antibodies may be irreversible, while those formed by the action
of cold antibodies may be dispersed or reduced in numbers by warming
the blood sample prior to spreading the film. Red cell autoagglutination may supervene on rouleaux formation as auto-antibodies
and dysproteinaemia may occur in the same disorders. Autoagglutination due to cold antibodies affects the red cell count and the
MCV obtained by automated electronic equipment such as the Coulter
S. Accurate values are obtained only after prior incubation of the blood
sample at 37°C; Erythrophagocytosis by neutrophil polymorphs and/or
monocytes may be noticed in the routine thin film but is usually more
evident in buffy coat films.
ABNORMAL FILM APPEARANCES OF LEUCOCYTES
THE PREDOMINANT LEUCOCYTE
A. Films with predominant neutrophils
Relative neutrophilia, absolute lymphocytopenia type (see Tables 12.42
and 12.43).
The neutrophil polymorph is the predominant leucocyte in the film
because of a reduction in the percentage and/or absolute number of
140
ABNORMAL BLOOD FILM
lymphocytes. In infants with hereditary cellular immunodeficiency
diseases, no lymphocytes may be seen. The absolute neutrophil
polymorph count is within normal limits or increased. Polymorphs may
be absent in infants with reticular dysgenesis and markedly depressed in
patients being treated with cytotoxic drugs. Infants with hereditary
lymphocytopenia (except that due to ataxia telangiectasia) have a brief
survival and suffer from viral, fungal and other opportunistic infections.
Lymphocytopenia in adults is usually not significant clinically except in
those with endocrinopathies or lymphoma, or in those on
immunosuppressive therapy with cytotoxic drugs. Immunoglobulin
deficiency is often associated with many of the lymphocytopenias.
Cellular immunodeficiency states will thus have to be differentiated
from the humoral deficiency syndromes (see Table 12.43) characterized
by a diminished number or complete absence of plasma cells in the
bone marrow and peripheral (secondary) lymphoid organs.
Absolute neutrophilia type (see Table 12.44)
The neutrophil polymorph is the predominant leucocyte in the film
and the absolute cell count is elevated. The percentage of lymphocytes
is reduced but the absolute count of these cells is commonly within
normal limits. A leucocytosis is usually present; sometimes the total
white cell count is within normal limits. The polymorph lobe average is
decreased and many stab cells are seen; occasionally a few
metamyelocytes are present. In some films the lobe average may be
increased and some hypersegmented neutrophils are observed. Toxic
granulation and/or Dohle bodies frequently appear in some disorders
(see Table 12.54). The red cells' parameters may be normal,
polycythaemic or anaemic; their chromicity is variable. The number of
platelets in the films is not constant.
Neutrophilic leukaemoid type (see Table 12.45)
There is a marked leucocytosis (total white cell count is greater than
50,000 per microlitre) and the majority of the leucocytes are neutrophil
polymorphs. Immature neutrophils, including a few promyelocytes and
at times an occasional myelobast, are present. Morphologically the cells
appear normal. The pelgeroid anomaly is not obvious and there is no
concomitant eosinophilia or basophilia. The morphology of the red
cells is variable and an occasional normoblast may be present. Toxic
granulation and/or Dohle bodies may be seen. The leucocyte alkaline
phosphatase (LAP) score, which is normal or increased, distinguishes
this type of film from that of a myelocytic (granulocytic) leukaemia. A
low score in a blood sample containing no malignant neutrophils should
be rechecked at weekly intervals; a fluctuating score may suggest a
pre-leukaemic state.
141
THE PERIPHERAL BLOOD FILM
Leuco-erythroblastic type (see Table 12.46)
Neutrophil polymorphs are predominant and a variable number of
immature neutrophils and erythroblasts (commonly normoblasts) are
present. The immature cells may not be noticed during the routine
leucocyte differential count and their presence may be detectable only
while the film is being scanned. The total white cell count is variable;
morphologically the neutrophils, mature and immature, appear normal.
Except for the leuco-erythroblastic type of picture that is seen in
neonatal infants and in polycythaemia rubra vera, there is usually an
anaemia; the red cells appear normochromic or slightly hypochromic.
Polychromatic cells are seen in the film but the number of these cells
and erythroblasts do not show any correlation. The peripheral blood of
some severe megaloblastic anaemias may contain immature neutrophils
in addition to the megaloblastaemia. Occasionally a leukaemia may
present as a leuco-erythroblastic anaemia; in the case of a myeloid or
myelomonocytic leukaemia the immature neutrophils may show
neoplastic characteristics such as hypogranularity and/or agranularity of
the cytoplasm.
Myelocytic (chronic myeloid or granulocytic) leukaemia
The total leucocyte count is unusually high. The blood film is
packed with cells of the neutrophilic series and all developmental stages
including myeloblasts (2-5 per cent) are seen (see Plate 49). The
pelgeroid anomaly may be noticed. Myelocytes comprise more than 15
per cent of the leucocytes and the differential count may suggest an
amplification block at this stage. An eosinophilia and/or basophilia is
often present. Thrombocytosis with marked platelet anisocytosis may
accompany this blood picture. There is usually an anaemia, the red cells
appearing normochromic normocytic and rarely macro-ovalocytic
because of an associated diminished availability of vitamin B 1 2 . An
occasional erythroblast may be present. The leucocyte alkaline
phosphatase (LAP) score is diminished or nil. Adult myelocytic
leukaemia is characterized by the presence of the Philadelphia (Ph1)
chromosome (90 per cent of cases). The juvenile type is Ph1 negative
and is associated with thrombocytopenia and increased level of Hb-F
due to renewed synthesis. Serum and urinary lysozyme (muramidase)
concentrations may be elevated in Ph1 negative myelocytic leukaemias.
Promyelocytic (progranulocytic) leukaemia
The total leucocyte count is elevated. The blood film shows all the
developmental stages of the neutrophilic series of cells. Many
leukaemic promyelocytes are present. The pelgeroid anomaly and
hypogranular cells which may be mistaken for monocytes may be
observed. An Auer rod may be observed in an occasional promyelocyte
142
ABNORMAL BLOOD FILM
and/or myeloblast. The leucocyte alkaline phosphatase (LAP) score is
diminished or nil.
Myeloblastic (acute myeloid or granulocytic) leukaemia
The leucocyte count is variable; the neutrophil polymorph or the
lymphocyte is the predominant cell in the film. The pelgeroid anomaly,
hypogranular and/or agranular neutrophils (these may be mistaken for
monocytes) are often present. A variable number of myeloblasts are
scattered in the film. They are often smaller than the myeloblasts seen
in the bone marrow and may be missed by the casual observer or
considered to be lymphocytes by the inexperienced. An Auer rod may
be observed in an occasional myeloblast. Monocytes are not particularly
prominent and the lymphocytes show no significant abnormality.
Platelet numbers are usually reduced. The patient is anaemic and the
appearance of the red cells is variable; macro-ovalocytes may be
present. Tear-drop poikilocytes and late normoblasts may be seen. The
leucocyte alkaline phosphatase (LAP) score is diminished or nil.
The leukaemia may arise de novo or may be the termination of a
miscellany of disorders such as paroxysmal nocturnal haemoglobinuria,
polycythaemia rubra vera and myelomatosis; it may result from
ionizing irradiation and therapy with phenylbutazone and
chloramphenicol. Myeloblastic leukaemia is one variety of acute
leukaemia that may occur in adults. Erythroleukaemia (Di Guglielmo's
syndrome) can be excluded by the absence of malignant erythroblasts
in the blood film and bone marrow. The acetate esterase enzyme
reactions are valuable for differentiating myeloblastic from myelomonocytic leukaemia.
Paramyeloblastic leukaemia
There are many atypical neutrophils at all stages of development and
because of marked nucleocytoplasmic asynchronic maturation, staging
of the cells is difficult. Agranular polymorphs, cells with twinning
deformity of the nucleus, myeloblasts with indented nuceli and an
occasional Auer rod are present. The patient is anaemic and platelet
numbers are reduced. Alkaline phosphatase is not demonstrable in any
cell.
Di Guglielmo 's syndrome
Erythraemic myelosis type. — Neutrophil polymorphs are
predominant in the blood film. The total white cell count may be
within normal limits. Platelets are scanty and the red cells are
normochromic normocytic or macrocytic. There is moderate
polychromatophilia. A variable number of vacuolated normoblasts
and/or malignant erythroblasts are seen.
143
THE PERIPHERAL BLOOD FILM
Erythroleukaemia. — The picture is similar to that of myeloblastic
leukaemia. However, vacuolated and malignant erythroblasts are
observed in the blood film and the bone marrow.
Myelomonocytic leukaemia
The total white cell count may be reduced. Neutrophils are
predominant and there is a variable number of monocytic cells.
Malignant monocytes and neutrophils at all stages of development
(including 'blast' cells) are present. Eosinophilia may be prominent. An
anaemia is usually present and platelets may be within normal limits.
This leukaemia is characterized by high levels of serum and urinary
lysozyme (muramidase).
B. Films with predominant lymphocytes
Relative lymphocytosis, absolute neutropenia type (see Table 12.47)
Lymphocytes, which may be normal or atypical in appearance, are
predominant in the film because of a reduction in the percentage
and/or number of neutrophil polymorphs. There may or may not be a
leucopenia; monocytes and eosinophils may be prominent. The
morphology of the polymorphs is usually normal and immature
neutrophils are rarely seen. However, all absolute neutropenia blood
films should be carefully scrutinized for immature and/or malignant
neutrophils as this type of blood picture may result from myeloblastic
leukaemia. Neutropenias in subjects of African origin may not be
pathological (Ezeilo, 1972; Shaper and Lewis, 1971; Rippey, 1967;
Broun, Herbig and Hamilton, 1966). Absence of neutrophils and
lymphocytes in an infant is suggestive of reticular dysgenesis. An
associated neutropenia and a lymphocytopenia may also be seen in
patients on cytotoxic therapy. Careful inspection of the lymphocytes
and any 'lymphocytoid' cells that may be present in the film, will
exclude leukaemic reticulo-endotheliosis ('hairy' cell leukaemia).
Pancytopenia type (see Tables 12.48 -12.50)
Lymphocytes are predominant in the film and there is neutropenia,
anaemia and thrombocytopenia. Immature neutrophils and erythroblasts may be seen. Erythrocyte morphology is variable and depends on
the type and severity of the anaemia. Lymphocytopenia is rarely
associated with pancytopenia; this is seen in reticular dysgenesis and in
patients on cytotoxic therapy. Clinically the patient may have a
splenomegaly (see Table 12.49) and the pancytopenia may be due to
hypersplenism (see Table 12.50) which is characterized by hyperplasia
of the precursor tissues in the bone marrow. Hypersplenism can be
established by cure of the pancytopenia and improvement of the
life-span of the blood cells after splenectomy (Crosby, 1972).
144
ABNORMAL BLOOD FILM
Absolute lymphocytosis type (see Table 12.51)
Lymphocytes are predominant in the film and the absolute
lymphocyte count is elevated above the upper limit of normality for
the particular subject. The neutrophil percentage is reduced but the
absolute count is usually within normal limits. A viral infection is the
commonest cause of this type of blood picture and many of the
lymphocytes contain atypical nuclei and/or vacuolated cytoplasm. Cells
with severely deformed nuclei are seen in whooping cough. The atypical
'lymphocyte' of infectious mononucleosis is associated with other
forms of atypical mononuclear cells. Turk irritation cells are often
present in viral lymphocytosis and during hyper sensitivity reactions.
The blood picture of infectious lymphocytosis is characterized by the
presence of normal small lymphocytes (Riley, 1953). Careful inspection
of the lymphocytes and any 'lymphocytoid' cells that may be present
in the film will exclude lymphocytic/lymphosarcoma cell leukaemia,
mycosis fungoides (Sézary variant) and leukaemic reticulo-endotheliosis
('hairy' cell leukaemia).
Lymphatic leukaemoid type (see Table 12.51)
Lymphocytes are predominant in the film and the absolute
lymphocyte count is markedly elevated. The lymphocytes may be
normal or atypical in appearance. Many smudge cells are present and
prolymphocytes may be prominent. The leukaemoid type of film may
be distinguished from that of lymphocytic/lymphosarcoma leukaemia
by the PAS reaction; the PAS score of the lymphocytes is usually
normal in the former and high in the latter. The lymphatic leukaemoid
film may be seen in the same disorders in which lymphocytosis can
occur.
Lymphocytic (chronic lymphocytic) j lymphosarcoma cell (chronic
lymphosarcoma cell) leukaemia
The total white cell count is markedly elevated; 90-99 per cent of
the leucocytes in the film are malignant lymphocytes consisting of
small and large lymphocytes and cells resembling 'lymphosarcoma' cells
(see Plate 50). The proportions of the different malignant cells vary
during the course of the disease; the percentages of the small and large
lymphocytes also depend on the area of the film in which the
differential count is carried out. There are many smudge cells;
malignant lymphoblasts are rarely observed. The patient is usually
anaemic. The red cells are normochromic normocytic; there may be
morphological evidence of a haemolytic process, and rouleaux
formation due to a monoclonal gammopathy may be seen. Platelets
appear normal but may be reduced in number if there is hypersplenism
or crowding out of megakaryocytes in the bone marrow by
145
THE PERIPHERAL BLOOD FILM
lymphocytic leukaemic infiltrates. The high PAS score of the
lymphocytes may help to distinguish lymphocytic leukaemia from a
lymphatic leukaemoid reaction where the score is normal.
Many laboratories label the disorder with this blood picture as
chronic lymphocytic leukaemia (CLL) and do not differentiate
according to cell types; the morphological features are considered as
different expressions of the same disorder (Scott, 1957; Heller, 1970).
Because clinical and laboratory differences have been demonstrated,
some investigators (Isaacs, 1937; Schwartz et al, 1965; Schrek and
Donnelly, 1971; Schrek, Knopse and Trobaugh, 1971) have suggested that
CLL should be sub-classified into CLL and chronic lymphosarcoma cell
leukaemia (CLSL), the sine qua non for the diagnosis of the latter being
the demonstration of the 'lymphosarcoma' cell in the peripheral blood
and bone marrow (Schwartz et al, 1965). According to Butler (1970)
and Lukes (1970), the histological pictures in the lymph nodes of
patients with CLL and CLSL are respectively well differentiated and
poorly differentiated lymphocytic lymphoma. Zacharski and Linman
(1969) reviewed nearly 500 cases and reported that the clinical and
laboratory differences, between CLL and CLSL were statistically
insignificant. They observed, however, that survivorship was less in
CLSL than in CLL and, on this basis, were of the opinion that CLL
should be sub-classified as CLL and CLSL according to the morphology
of the malignant cells.
CLL usually occurs after the age of 45 years and more commonly in
males; a benign form may occur in elderly subjects. Mu chain (IgM
monomer) disease may present as a CLL. Mycosis fungoides (Sézary
variant), leukaemic reticulo-endotheliosis ('hairy' cell laukaemia) and
Waldenström's macroglobulinaemia may be misdiagnosed as a CLL.
Lymphoblastic (acute lymphatic) laukaemia
This blood picture occurs principally in young children and infants.
The total white cell count is usually elevated but in some cases may be
within normal limits or low. Lymphocytic cells are predominant and a
variable number of malignant lymphoblasts are present. There is also a
pancytopenia. The PAS reaction may show blocks of magenta-coloured
material in some blasts. The PAS score of the mature lymphocytes is
within normal limits. Occasionally the blood picture of a patient with
lymphoblastic leukaemia is that of a leuco-erythroblastic anaemia and
malignant lymphoblasts are not detected in the blood film but crowd
out the haemopoietic tissue in the bone marrow.
Myeloblastic leukaemia
The film appearance is that of myeloblastic leukaemia with
pancytopenia and predominant lymphocytes.
146
ABNORMAL BLOOD FILM
Erythroleukaemia (Di Guglielmo's syndrome)
The blood picture is similar to that of myeloblastic leukaemia with
pancytopenia, predominant lymphocytes and malignant erythroblasts.
THE PROMINENT LEUCOCYTE
A. Films with prominent atypical neutrophil polymorphs
Pelger-HuëtIPelgeroid type (see Table 12.52)
A variable number of the neutrophils show the Pelger-Huët anomaly of
the nucleus. The morphology of the cell is described in Chapter 5. In
the hereditary variety anomalous lymphocytes and monocytes may be
observed. The blood picture of films with the acquired or 'pelgeroid'
variety depends on the disorder in which it occurs. Brunning (1970)
observed the anomaly as a transient phenomenon in a renal transplant
patient with a dermatological reaction to a sulphonamide.
Hypersegmented neutrophil type (see Table 12.53)
A variable number of neutrophils show hypersegmentation of the
nucleus. The total white cell count is variable. The morphology of the
cell is described in Chapter 5. The presence of hypersegmented
neutrophils in a film showing no evidence of neutrophilia (see Table
12.44) is suggestive of but not diagnostic of megaloblastosis (see Table
12.10); they are also seen in other disorders (see Table 12.53).
Hypersegmented eosinophils may be associated with hypersegmented
neutrophils in these disorders. Hypersegmented eosinophils may also be
seen in Hodgkin's disease, tropical eosinophilia and in the rare familial
disorder of eosinophils described by Presentey (1968, 1969 a, b).
Neutrophil polymorphs with basophilic granules (see Table 12.54)
Basophilic granules that may be seen in neutrophil polymorphs are
toxic granules, Alder-Reilly granules or the Chediak-HigashiSteinbrinck anomaly. Toxic granulation is a transient phenomenon and
must not be mistaken for Alder-Reilly granules. The morphology of the
cells with these anomalous granulations is described in Chapter 5.
Because of the staining characteristics of the Alder-Reilly granules in
eosinophils, it may be difficult to distinguish between eosinophils and
basophils in the genetic mucopolysaccharidoses (Brunning, 1970). The
granules in the rare Chediak-Higashi-Steinbrinck syndrome are large and
not readily confused with the other basophilic granules.
Neutrophil polymorphs with basophilic inclusions (see Table 12.55)
A variable number of neutrophil polymorphs contain one or more
blue-staining structures approximately 2 Mm in diameter. The
inclusions may represent the hereditary May-Hegglin anomaly or the
147
THE PERIPHERAL BLOOD FILM
acquired Dohle body. The morphology of the cells with these inclusions
is described in Chapter 5. The May-Hegglin anomaly has a well-defined
margin, may be observed in other leucocytes and is associated with
thrombocytopenia and mega thrombocy tes. The Dohle body has a
poorly defined margin, not seen in other leucocytes, is a transient
phenomenon and may be associated with toxic granules in the same and
other neutrophils; thrombocytopenia and abnormal platelet
morphology is not usually seen in the film. When Dohle bodies are
observed in films from patients with Hodgkin's disease and chronic
lymphocytic leukaemia, they may be due to opportunistic infection.
B. Films with prominent atypical lymphocytes
Lymphocytes with notched nuclei (see Table 12.56)
A variable number of lymphocytes show one (notch) or more (radial
segmentation) indentations or a twinning deformity of the nucleus. The
morphology of the cells is described in Chapter 5. The blood picture is
variable. Notching and radial segmentation of lymphocytic nuclei may
arise as an artefact. The anomalies are commonly seen in viral
infections. Bizarre nuclei may be observed in whooping cough.
Lymphocytes with vacuolated cytoplasm (see Table 12.57)
A variable number of lymphocytes with vacuolated cytoplasm are
present in the film The morphology of the cells is described in Chapter
5. The hereditary disorders are rare but have to be considered in the
differential diagnosis, particularly in infants and young children; the
blood picture may be otherwise normal or may show a leucoerythroblastaemia. In the acquired disorders there is commonly a
lymphocytosis and lymphocytes with abnormal nuclei may also be
seen.
C. Films with prominent monocytes
Absolute monocytosis type (see Table 12.58)
The percentage and absolute number of monocytes is increased.
There may be a leucocytosis. The morphology of the cells is normal
unless there is artefactual distortion such as radial segmentation of the
nucleus and/or extensive vacuolation of the cytoplasm. The neutrophil
percentage may be reduced but the absolute numbers of these cells and
of the lymphocytes are commonly within normal limits. There may be
an anaemia but platelets are normal. Polymorphoid monocytes and cells
with radial segmentation may be seen in Hodgkin's disease and in
myelomonocytic leukaemia. In the latter disease the cells may be
indistinguishable from agranular neutrophils: the combined acetate
esterase reaction is useful for differentiating the cells.
148
ABNORMAL BLOOD FILM
Monocytic leukaemoid type (see Table 12.58)
The total white cell count is markedly elevated owing to an increase
in the absolute number of morphologically normal monocytes.
Promonocytes may be observed in the film. There may be an aenaemia
and/or a thrombocytopenia. This blood picture may occur in the
disorders that cause absolute monocytosis.
Myelomonocytic leukaemia
The total white cell count is variable. Approximately 75 per cent of
the leucocytes are malignant cells of the monocytic series; an occasional
monoblast may contain an Auer rod. The patient is anaemic and a
thrombocytopenia is present.
D. Films with atypical mononuclear cells
Mononucleosis type (see Table 12.59)
The total white cell count may be normal but usually there is a
leucocytosis due to an atypical lymphocytosis and mononucleosis (see
Plate 51). Neutropenia often occurs; the number of neutrophil stab
cells in the film is increased and the pelgeroid anomaly may be noticed.
The three varieties of mononucleosis cells — lymphocytoid,
plasmacytoid and monoblastoid — may be recognized in the film. The
morphology of the cells is described in Chapter 5. The lymphocytoid
type is commonly predominant and the plasmacytoid cell is usually
present. Sometimes, however, many monoblastoid cells are seen and the
picture may be misdiagnosed as a leukaemia by the inexperienced. Up
to 23 per cent of the atypical cells may show a Swiss-cheese nucleus.
These cells may be noticed 2-3 weeks after the commencement of the
illness and only if the films are prepared from anticoagulated blood that
has stood for a while at room temperature. The platelet count is normal
but may be reduced. Commonly, there is no anaemia; if the patient is
anaemic there may be evidence of a haemolytic process. The
Paul-Bunnell heterophile antibody test is usually positive but may be
negative.
The clinical conditions in which the mononucleosis type of blood
film may occur with and without a positive Paul-Bunnell heterophile
antibody test are listed in Table 12.59. A positive serological test
without the accompanying haematological picture has been reported in
Hodgkin's disease, lymphocytic leukaemia, acute leukaemia and in
tularaemia. Other antibodies - the Epstein-Barr (E-B) virus antibody,
auto-antibodies and cold haemagglutinins (anti-i) — may be detected in
infectious mononucleosis. The evidence linking the E-B virus as the
causative factor in infectious mononucleosis is not conclusive
(Banatvala, 1970), as the virus appears to be a common infectious agent
and high-titre E-B virus antibody has been detected in some healthy
149
THE PERIPHERAL BLOOD FILM
subjects, in Burkitt's lymphoma, Hodgkin's disease, lymphocytic
leukaemia and in sarcoidosis.
Leukaemic reticulo-endotheliosis or 'hairy ' cell leukaemia
Pancytopenia is commonly present and a variable number of
leukaemic reticulo-endothelial cells (LRE) are seen in the film. The
morphology of the cell is described in Chapter 5. The anaemia is
normochromic normocytic in type and an occasional normoblast may
be observed. Sometimes the total white cell count is markedly elevated
and because of the resemblance of LRE cells to lymphatic cells in a
Romanovsky-stained film the blood picture may be misdiagnosed as
lymphocytic or lymphosarcoma cell leukaemia. Plenderleith (1970)
found no relationship with other leukaemias or lymphoma and no
transition between leukaemic reticulo-endotheliosis and 'reticulum cell'
sarcoma.
E. Films with prominent eosinophils
Absolute eosinophilia type (see Tables 12.60 and 12.61)
The eosinophils are prominent in the film and there is an absolute
increase in their numbers. This increase should be confirmed by
carrying out direct eosinophil counts in a counting chamber. The total
white cell count may be within normal limits or elevated due to a
neutrophilia. The red cells and platelets are normal.
Hypereosinophilia type (see Table 12.61)
The blood picture is similar to the absolute eosinophilia type except
that the absolute eosinophil count is markedly elevated and produces a
leucocytosis. Morphologically abnormal mature eosinophils with
vacuolated cytoplasm and containing a reduced number of granules
may be observed. Neutrophil polymorphs may show a slight increase.
This film appearance may be seen in the disorders causing eosinophilia;
it occurs particularly in the hypereosinophilic syndrome (Hardy and
Anderson, 1968) and in 'eosinophilic' leukaemia. The hypereosinophilic
syndrome is considered to be a continuum of diseases ranging from the
benign Loeftier's syndrome to the disseminated eosinophilic collagen
disease.
'Eosinophilic' leukaemia
There is a persistent marked leucocytosis; the total white cell count
is greater than 50,000 per microlitre. Mature and immature eosinophilic
granulocytes and a variable number of myeloblasts are present in the
film. Immature neutrophilic granulocytes and an occasional normoblast
may be observed. The patient is usually anaemic and thrombocytopenic. It is not certain whether 'eosinophilic' leukaemia, which at
times is difficult to distinguish from other hypereosinophilic
150
ABNORMAL BLOOD FILM
syndromes, represents a distinct entity (Benvenisti and Ultman, 1969)
or a variant of myelocytic leukaemia.
F. Films with prominent basophils
Absolute basophilia (see Table 12.62)
The total white cell count is variable. There is an absolute increase in
the basophil count. In some disorders there may be an associated
eosinophilia. The film appearances of the red cells and platelets are
variable.
G. Films with prominent plasma cells
Plasmacytosis type (see Table 12.63)
A few to a moderate number of plasma cells and/or Turk irritation
cells are seen and atypical lymphocytes are also present. The total white
cell count and the platelet count is variable. There may be no anaemia
and the red cells may show rouleaux formation. Plasmacytosis is most
frequently seen in virus infections. If there is marked rouleaux of red
cells, the plasmacytosis may be due to hyperimmunoglobulinaemia.
Myeloma type (see Table 12.38)
The blood film shows marked rouleaux of the red cells and an
occasional to a few plasma cells are detected. Morphologically the cells
may appear normal or may be malignant cells of the plasma cell series
('myeloma' cells) (see Plate 47). There is a normochromic normocytic
anaemia and the erythrocyte sedimentation rate (ESR) is markedly
elevated. The number of neutrophils and platelets may be reduced.
Occasionally the 'myeloma' cells are observed in a film showing
leuco-erythroblastaemia. The myeloma type of film is usually
associated with an anomalous monoclonal gammopathy (see Table
12.38) and Bence-Jones proteinuria.
Plasma cell leukaemia
The film appearance is similar to the myeloma type but many
plasma cells or 'myeloma' cells are evident. This leukaemia is a variant
of myelomatosis. It results from an outpouring of tumour cells from
the bone marrow where megakaryocytoid plasmablasts were previously
prominent.
ABNORMAL FILM APPEARANCES OF PLATELETS
A. Films with increased number of platelets
Thrombocytosis type (see Tables 12.64 and 12.65)
The platelet count is above the upper limit of normality and in the
blood film the spaces between the red cells contain many platelets. If the
platelet count is not known, it may be semi-quantitatively assessed by
151
THE PERIPHERAL BLOOD FILM
the indirect method described in Chapter 10. The film appearances of
the red cells and leucocytes depend on the disorder in which the
thrombocytosis occurs. Occasionally platelet clumping is seen in films
prepared with anticoagulated blood. The platelet masses vary in size
and may be observed only at the film edges. This phenomenon may be
due to increased platelet adhesiveness (see Table 12.65). Megathrombocytes are present in the post-splenectomy blood film.
Microthrombocytes are prominent after acute haemorrhage, in iron
deficiency states and in inflammatory disorders.
Thrombocythaemia type (see Table 12.64)
The platelet count is extremely elevated and may be greater than
one million per microlitre. The spaces between the red cells are packed
with platelets; giant and bizarre forms are seen. Masses of clumped
platelets may be observed at the film edges; some of these masses may
represent cytoplasmic fragments of megakaryocytes rather than clumped
platelets. The red cells are normochromic normocytic but may be
hypochromic microcytic. Eosinophils and/or basophils may be
prominent and immature neutrophils are present in the film. This blood
picture is seen only after late middle age. Clinically the patient suffers
from thrombotic episodes and because the platelets are functionally
abnormal they develop iron deficiency from repeated haemorrhages.
B. Films with reduced number of platelets
Thrombocytopenia type (see Tables 12.66 -12.69)
The platelet count is below the lower limit of normality and a scanty
number of platelets are seen in the film. The presence of a few platelets
only in the film suggests a count of less than 10,000 per microlitre. The
appearances of the red cells and leucocytes depend on the disorder
causing the thrombocytopenia. Artefactual decrease of the platelet
count may be due to in vitro platelet clumping. This is readily detected
by careful scrutiny of the film edges. Neonatal thrombocytopenia is
commonly due to maternal factors. The Wiskott-Aldrich syndrome in a
child is characterized by eczema, agammaglobulinaemia, a reduced
platelet count and the presence of microthrombocytes in the blood film
(see Table 12.70). Viral infections, chronic alcoholism, drugs,
megaloblastosis micro-angiopathy, disseminated intravascular coagulation, hypersplenism and acute leukaemia are the most frequent causes of
thrombocytopenia. Clinically they may present with purpura, extensive
bruising, epistaxis, haematuria or occasionally with gastro-intestinal
haemorrhage. Purpura can also occur in subjects without thrombocytopenia (see Tables 12.67 - 12.69).
152
ABNORMAL BLOOD FILM
C. Films with atypical platelets
Megathrombocytosis (see Table 12.70)
More than 5 per cent of the platelets in the blood film are
macroplatelets or megathrombocytes. The platelet count is variable.
Bizarre forms may be observed in the thrombocy tosis and
thrombocythaemic types of films. The appearances of the red cells and
leucocytes depend on the disorder in which megathrombocytosis occurs.
Microthrombocytosis (see Table 12.71)
More than 10 per cent of the platelets in the blood film are
microplat elet s or micro thrombocytes. The platelet count is variable.
The appearances of the red cells and leucocytes depend on the disorder
in which microthrombocytosis occurs.
D. Films with aggregated platelets
Auto-agglutination type
Clumps of platelets are scattered throughout the film prepared with
anticoagulated (EDTA) blood. The platelet masses vary in size and in
some films may be observed only at the film edges. This
auto-agglutination may be responsible for artefactual thrombocytopenia, particularly if the direct platelet count is determined with
automated electronic equipment. It may not occur if the blood is
anticoagulated with citrate or oxalate. Platelet clumping may be seen in
the thombocytosis and thrombocytopenia types of blood film. It may
be due in some cases to specific auto-antibodies (Gowlandei aL, 1969)
or associated with auto-agglutinated red cells (Table 12.41).
Platelet satellitism
Few to many platelets encircle the neutrophil polymorphs in the
film prepared with EDTA-anticoagulated blood. Cytopathic changes of
the involved cells are not commonly seen. However, some platelets may
be adherent to the PMN cell membrane and an occasional PMN with an
intact platelet in its cytoplasm may be found. The number of affected
PMN varies from patient-to-patient and from day-to-day in the same
patient. Platelet satellitism of other leucocytes, including eosinophils
and basophils, is not usually evident (Field and MacLeod, 1963; Crome
and Barkhan, 1963); rarely a few lymphocytes may be affected
(personal observation). The remaining platelets are scattered
throughout the blood film. Marked platelet satellitism, where numerous
platelets surround each PMN, may be associated with the presence of
megathrombocytes, degranulated platelets, agglutinations of platelets
elsewhere in the film and with the formation of PMN pseudo-rosettes.
Masses composed of aggregated platelets with entrapped PMN are
striking in the tail of the film. The direct platelet count may be
153
THE PERIPHERAL BLOOD FILM
artefactually reduced if it is determined from the EDTA blood and it is
advisable for the count to be carried out on capillary or 'native' venous
blood.
Platelet satellitism is of uncertain pathogenesis and unknown
significance. In some patients it may be due to platelet auto-antibodies.
It is not seen in films prepared with capillary or 'native' venous blood.
Investigation has shown that it is caused by a serum factor which is
reactive only in the presence of EDTA. Sera from patients whose
EDTA-anticoagulated blood film exhibited platelet satellitism of PMN
were capable of inducing the phenomenon when added to normal ABO
group-compatible blood anticoagulated with EDTA; the sera had no
effect on normal blood collected in citrate, oxalate or heparin.
154
12
Differential Diagnosis
FILMS WITH NORMOCHROMIC RED CELLS
TABLE 12.1
Normochromic Normocytic Type
Polycythaemia (Table 12.2)
Relative
Absolute
Primary or erythraemic type
Secondary or erythrocytic type
Anaemia
Relative or pseudo-anaemia (increased plasma volume)
Pregnancy
Massive splenomegaly
Hypopituitarism
Oestrogen therapy
Absolute
Diminished production of red cells
Failure of erythropoietic tissue (Table 12.3)
Replacement/infiltration of haemopoietic tissue (Table 12.3)
Depression of erythropoiesis (Table 12.17)
Loss of mature cells
Haemorrhage (Tables 12.6 and 12.7)
Sequestration in spleen
Haemolysis (Table 12.8)
TABLE 12.2
Polycythaemia
Relative, stress or spurious polycythaemia
Acute depletion of plasma volume — dehydration
Diminished fluid intake
Excessive fluid loss from copious sweating, vomiting and
diarrhoea
cont.
155
THE PERIPHERAL BLOOD FILM
Table 12.2 cont.
Absolute
polycythaemia
Primary or erythraemic type (autonomous erythropoiesis with
panmyelosis). Erythropoietin concentration in plasma and urine is
normal or decreased.
Polycythaemia rubra vera (PRV)
Gaisböck's syndrome (PRV with hypertension, without
splenomegaly)
Secondary or erythrocytic type (compensatory and inappropriate
erythropoiesis without panmyelosis)
Compensatory erythropoietin production due to tissue hypoxia
A. Physiological
Erythrocytosis at high altitudes
B. Arterial blood oxygen saturation — normal
(1) Familial
erythrocytosis
due
to
'polycythaemic
haemoglobins', that is, abnormal haemoglobins with
increased oxygen affinity. Haemoglobin Chesapeake,
haemoglobin Rainier.
(2) Acquired heart disease — low output cardiac failure
(3) Increased metabolic demands — thyrotoxicosis,
Cushing's syndrome
C. Arterial blood oxygen saturation - reduced
(1) Arterio-venous blood admixture due to anatomic shunts
Congenital intracardiac, intrapulmonary and great vessel
defects
Acquired — cirrhosis of the liver
(2) Alveolar hypo ventilât ion
Central: impairment of respiratory centre
Cerebral thrombosis
Parkinsonism
Encephalitis
Barbiturate intoxication
Peripheral: mechanical impairment of chest
Pulmonary — obstructive airway disease such as
emphysema and asthma
Chest bellows — kyphoscoliosis
Neuro muscular diseases — poliomyelitis, myasthenia
gravis
Combined central and peripheral
Severe obesity (Pickwickian syndrome)
(3) Diffusion impairment due to restriction of pulmonary
vasculature
Tuberculosis
Silicosis
Pneumoconiosis
Granulomatosis
156
DIFFERENTIAL DIAGNOSIS
Table 12.2 cont.
Sarcoidosis
Pulmonary fibrosis
Hamman-Rich disease
Lymphangitis carcinomatosa
Primary pulmonary hypertension
(4) Methaemoglobinaemia
Inappropriate erythropoietin production
Renal cysts, hydronephrosis, transplants
Tumours
—
hypernephroma,
phaeochromocytoma,
aldosterone-producing
adenoma,
hepatoma,
leiomyoma
(fibroid) of uterus
Cerebellar haemangioblastoma
Hormone therapy — hydrocortisone, androgens (testosterone)
TABLE 12.3
Hypoplasia of Erythropoiecic Tissue
A. Failure of erythropoietic tissue
Hereditary
Fanconi syndrome
Aplasia of Blackfan-Diamond type
Good's syndrome (agammaglobulinaemia with thymoma)
Acquired
Paroxysmal nocturnal haemoglobinuria
Starvation states (Kwashiorkor)
Acute arrest in haemolytic anaemia
Graft-versus-host (GVH) rejection
Viral infections and viral hepatitis
Ionizing irradiation — x-rays, radioactive phosphorus, benzene
Cytotoxic drugs (see Appendix B)
B. Replacement/infiltration of haemopoietic tissue
Myeloproliferative disorders
Lymphoproliferative disorders
Pre-leukaemia
Acute leukaemia
Di Guglielmo's syndrome
Leukaemic reticulo-endotheliosis
Myelomatosis
Lipidoses — Gaucher's disease, Niemann-Pick disease
Metastatic carcinoma from lung, thyroid, breast and prostate
Granulomata — tuberculosis, sarcoidosis, histoplasmosis
Marble bone disease
C. Depression of erythropoiesis (see under Anaemia of chronic
disorders, Table 12.17)
157
THE PERIPHERAL BLOOD FILM
TABLE 12.4
Normochromic Microcytic Type
Pregnancy
Infections
Inflammations
Diarrhoea
Renal diseases
Ionizing irradiation
Drugs and chemical poisons
Haemorrhage — subacute and chronic
Haematological disorders
Hypoplastic anaemia (Table 12.3)
Some haemolytic anaemias
Leukaemia
Di Guglielmo's syndrome
TABLE 12.5
Normochromic Round Macrocytic Type
Polycythaemia (Table 12.2)
Anaemia
Blood loss
Haemorrhage (Tables 12.6 and 12.7)
Haemolysis (Table 12.8)
Chronic liver disease
Hypothyroidism
Primary acquired sideroblastic anaemia
TABLE 12.6
Haemorrhagic Anaemia
Vascular defects
Trauma
Pathological erosions
Purpuric disorders (Table 12.67)
Platelet dysfunction
Thrombocytopenia (Table 12.66)
Decreased platelet adhesiveness (Table 12.68)
Decreased platelet aggregation (Table 12.69)
Hypocoagulable Blood
Procoagulant deficiency
Hereditary
Haemophilia A and variants
Haemophilia B and variants
Hypofibrinogenaemia and other factor deficiencies
158
DIFFERENTIAL DIAGNOSIS
Table 12.6 cont.
Acquired
Liver disorders
Disseminated intra vascular coagulation (Table 12.7)
Oral anticoagulant therapy with Coumadin-Indanedione drugs
Circulating anticoagulants
Increased antithrombin activity
Heparin-like activity
Parent eral heparin therapy
Factor VIII inhibitors/inactivators
Increased fibrinolytic activity
Disseminated intra vascular coagulation (Table 12.7)
Pancreatic surgery
Carcinoma prostate with métastases
Cirrhosis of the liver
Leukaemia
Thrombolytic therapy
TABLE 12.7
Disseminated Intravascular Coagulation (DIC)
Tissue thromboplastin in circulation
Burns
Open heart surgery
Obstetric accidents
Neoplasia and leukaemia
Pulmonary surgery
Shock lung syndrome
Arterial aneurysms (large)
Trauma
Trypsin enzyme
Heat stroke
Partial thromboplastin in circulation
Burns
Open heart surgery
Neoplasia and leukaemia
Drowning
Angiopathic haemolytic anaemia
Incompatible transfusions
Intravascular haemolytic anaemia
Heat stroke
Infections with haemolytic bacteria, e.g., Clostridia and Streptococci
Factor XII and/or platelet activation
Bacteraemia and viraemia
Endotoxin shock
cont
Endothelial damage
159
THE PERIPHERAL BLOOD FILM
Table 12.7 cont.
Antigen/antibody complexes
Idiopathic thrombocytopenic purpura
Primary amyloidosis
Allergic vasculitis
Periarteritis nodosa
TABLE 12.8
Haemolytic Anaemia
Hereditary haemolytic anaemia
A. Intramedullary haemolysis
Hereditary erythroblastic multinuclearity types I, II, and III
(Heimpel and Wendt, 1968)
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Thalassaemia and thalassaemic syndromes
B. Extramedullary haemolysis
Cell membrane defects
Hereditary spherocytosis
Hereditary elliptocytosis (some cases)
Hereditary stomatocytosis
R h n u u disease
Hereditary acanthocytosis
Haemoglobinopathies
Thalassaemia and thalassaemic syndromes
Crystallizing haemoglobins, e.g., Hb-S and Hb-C
Unstable haemoglobins, e.g., Hb-Zurich
Disorder of haem synthesis
Erythropoietic porphyria
Metabolic abnormalities
Deficiency of Glucose-6-phosphate dehydrogenase, glutathione,
hexokinase, phosphohexose isomerase, triosephosphate isomerase,
phosphoglycerate kinase, pyruvate kinase.
Red cell electrolyte imbalance
Hereditary stomatocytosis
R h n u n disease
Acquired haemolytic disease
A. Intramedullary haemolysis
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Di Guglielmo's syndrome
B. Extramedullary haemolysis
(1) Infections
Bacteria
Infection with Clostridium welchii
Streptococcal bacteraemia
160
DIFFERENTIAL DIAGNOSIS
Table 12.8 cont.
Viruses
Measles
Mumps
Infectious mononucleosis
Mycoplasma
Primary atypical pneumonia
Protozoa
Malaria
Blackwater fever
(2) Immunological
Iso-antibodies
Haemolytic disease of newborn
Incompatible transfusions
Auto-immune antibodies
Primary or idiopathic
Secondary
Cold antibodies
Infectious hepatitis
Influenza
Infectious mononucleosis (anti-i)
Primary atypical pneumonia (anti-I)
Cold agglutinin disease
Warm antibodies
Drug-induced haemolytic anaemia (see below)
Collagen diseases
Cirrhosis of the liver
Ulcerative colitis
Metastatic carcinoma
Myeloproliferative disorders
Lymphoma
Amyloidosis
Bi-thermic antibodies
Syphilis
(3) Paroxysmal nocturnal haemoglobinuria
(4) Drug-induced
Intra-erythrocytic factors — idiosyncracy
Heinz body anaemia (Table 12.32)
Extra-erythrocytic factors — immune hypersensitivity
Direct Coombs' test positive
Hapten type (anti-IgG) e.g., penicillin
Innocent bystander type (anti-C'), e.g., quinidine
Auto-immune type (anti-IgG) e.g., methyl dopa
Micro-angiopathy
Angiitis type — haemolytic uraemic syndrome, polyarteritis
Thrombotic thrombocytopenic purpura type
cont.
161
THE PERIPHERAL BLOOD FILM
Table 12.8 cont.
Sequel to drug-induced aplastic anaemia
Paroxysmal nocturnal haemoglobinuria
(5) Mechanical or fragmentation type (Table 12.28)
(6) Hypersplenism (Table 12.50)
(7) Miscellaneous
Heat stroke
Burns
Snake bite
Lead poisoning
TABLE 12.9
Unconjugated Hyperbilirubinaemia
A. Increased formation of bilirubin
Shunt or dyserythropoietic hyperbilirubinaemia
Hereditary erythroblastic multinuclearity types I, II and III
(Heimpel and Wendt, 1968)
Ineffective erythropoiesis
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Di Guglielmo's syndrome
Thalassaemia and thalassaemic syndromes
Haemolysis of red cells
Haemolytic anaemias (Table 12.8)
B. Mixed pathogenesis
Neonates
Physiological jaundice
Immaturity of metabolic processes
Prematurity
Respiratory distress syndrome
Metabolic abnormalities
Babies born to diabetic mothers
Congenital hypothyroidism
Galactosaemia
Carbohydrate deprivation
Dehydration
Infections
Bacterial sepsis
Cytomegalic virus disease
Leptospirosis
Genetic liver disorders
Defective uptake of bilirubin due to Y-protein deficiency
Defective conjugation of bilirubin due to complete and partial
deficiency of glucuronyl transferase
Drugs
Causing haemolysis
162
DIFFERENTIAL DIAGNOSIS
Table 12.9 cont.
Causing liver damage
Competing for bilirubin-binding proteins in liver cells, e.g.,
cholecystographic agents
Inhibiting glucuronyl transferase, e.g., steroids, novobiocin
and Synkavit (vitamin K)
C. Unknown pathogenesis
Gilbert's syndrome (intermittent)
Viral hepatitis
Post portacaval shunt surgery
High altitudes
TABLE 12.10
Normochromic Macro-ovalocytic Type
Haemoglobin within normal limits
Polycythaemia (Table 12.2), complicated by megaloblastosis
Subacute combined degeneration of the cord (some cases)
Anaemia
Megaloblastosis
A. Vitamin B12 deficiency (Table 12.11)
B. Folate deficiency (Table 12.13)
C. Enzyme abnormalities interfering with DNA synthesis (Table
12.14)
TABLE12.il
Vitamin B 1 2 Deficiency
Children
Congenital deficiency of intrinsic factor
Pathological deficiency of intrinsic factor
Imerslund's syndrome or selective malabsorption of vitamin B12
due to lack of ileal receptors for intrinsic factor-vitamin B i 2
complex
Congenital deficiency of transcobalamin II
Young adults
Associated with agammaglobulinaemia (late onset)
Adults and children
Nutritional deficiency
Elderly
Vegans
Starvation states
Gastric disorders
Pernicious anaemia
Subacute combined degeneration of the cord
Gastrectomy - partial or complete
cont.
163
THE PERIPHERAL BLOOD FILM
Table 12.11 cont.
Atrophie gastritis
Hiatus hernia
Chronic alcoholism
Intestinal disorders
Regional ileitis
Heal resection
Zollinger-Ellison syndrome
Severe pancreatic deficiency
Cirrhosis of the liver
Crohn's disease
Coeliac disease
Fish tapeworm {Diphyllobothrium
Bacterial overgrowth
Intestinal stricture
Intestinal fistula
Anatomical blind loop
Scleroderma
Drugs
Colchicine
Para-aminosalicylic acid
Neomycin
Miscellaneous
Endocrine disorders
Hypothyroidism
Hypopituitarism
Sideroblastic anaemia
Aplastic anaemia
cephalum latum) infestation
TABLE 12.12
Diseases Associated with Pernicious Anaemia
Stomach
Carcinoma
Polypi
Small bowel
Steatorrhoea
Intestinal malabsorption
Large bowel
Ulcerative colitis
Endocrines
Diabetes mellitus
Thyroid diseases
Myxoedema
Hashimoto's disease
164
DIFFERENTIAL DIAGNOSIS
Table 12.12 cont.
Miscellaneous
Rheumatoid arthritis
Vitiligo
Plummer-Vinson syndrome
TABLE 12.13
Folate Deficiency
Children
Selective malabsorption of folate
Protein malnutrition — kwashiorkor
Infants fed on goat's milk
Scurvy
Adults (and children)
Nutritional deficiency
Elderly, chronic invalids, poverty
Gastrectomy — partial or complete
Carcinoma of the stomach
Chronic alcoholism
Scurvy
Malabsorption
Jejunal resection
Idiopathic steatorrhoea
Tropical sprue
Coeliac disease
Ulcerative colitis
Intestinal strictures and blind loops
Drugs, e.g., ant icon vulsants and contraceptive pills
Increased requirements
Physiological
Pregnancy and puerperium
Infants
Pathological
Blood diseases
Haemolytic anaemias
Leukaemias
Di Guglielmo's syndrome
Malignant diseases
Inflammatory diseases
Rheumatoid arthritis
Tuberculosis
Crohn's disease
Psoriasis
Metabolic disorders
Hyperthyroidism (thyrotoxicosis)
cont.
165
THE PERIPHERAL BLOOD FILM
Table 12.13 cont.
Diminished availability
Cirrhosis of the liver
Myeloproliferative disorders
Excessive loss
Congestive heart failure
Haemodialysis
TABLE 12.14
Enzyme Abnormalities Interfering with DNA Synthesis
Hereditary
Enzyme for uridine synthesis
Hereditary orotic aciduria
Enzyme for purine synthesis
X-linked Lesch-Nyhan syndrome (van der Zee, Schnetlem and
Monnens, 1968)
Thiamine-dependent megaloblastic anaemia (Rogers, Porter and
Sidbury, 1969)
Folate enzyme abnormalities
Formimino transferase deficiency
Cyclohydrolase deficiency
Methyl transferase deficiency
Methyl cobalamin co-enzyme deficiency
Acquired
Drug therapy
Methotrexate (chemotherapy)
Pyrimethamine (malaria and toxoplasma)
Trimethoprim (antibacterial)
Diamidine compounds (pneumocystis, protozoacidal)
Pyridoxine (vitamin B 6 ) antagonists
Cycloserine, isoniazid (tuberculosis)
Anti-purine and anti-pyrimidine (chemotherapy)
6-Mercaptopurine
6-Thioguanine
Cytosine arabinoside
Pyridoxine deficiency
Chronic alcoholism
Anti-tuberculous drug therapy
Malnutrition
Malabsorption
Lead poisoning
Sideroblastic anaemia (pyridoxine deficiency)
166
DIFFERENTIAL DIAGNOSIS
TABLE 12.15
Stomatocytic Type
Hereditary
Herditary haemolytic anaemia
Hereditary stomatocytosis
R h n u n disease
Glucose-6-phosphate dehydrogenase deficiency (some cases)
Acquired
Acute alcoholism
Liver disorders
FILMS WITH HYPOCHROMIC RED CELLS
TABLE 12.16
Hypochromic Normocytic Type
Polycythaemia (Table 12.2)
With associated iron deficiency (Table 12.19)
Anaemia
Depression of erythropoiesis (Table 12.17)
TABLE 12.17
Anaemia of Chronic Disorders
Protein malnutrition (kwashiorkor)
Vitamin deficiency
Pellagra
Scurvy
Alcoholism
Infections
Miliary tuberculosis
Viral hepatitis
Inflammations
Collagen diseases
Rheumatoid arthritis
Systemic lupus erythematosus
Polyarteritis
Pancreatitis
Liver damage
Renal failure
Endocrinopathies
Hypothyroidism
Hypo-adrenalism
Malignant tumours with necrosis and sepsis
cont.
167
THE PERIPHERAL BLOOD FILM
Table 12.17 cont.
Drugs and ironizing irradition
Replacement/infiltration of haemopoietic tissue (Table 12.3)
TABLE 12.18
Hypochromic Microcytic Anaemia
Abnormal iron metabolism
Absent iron stores (Serum Fe d e c , TIBC inc., % sat. dec.)
Iron deficiency anaemia (Table 12.19)
Normal iron stores (Serum Fe d e c , TIBC N, % sat. dec.)
Defective iron mobilization
Anaemia of chronic disorders (Table 12.17)
Impaired haem synthesis
Normal iron stores (Serum Fe inc., TIBC N, % sat. inc.)
Congenital erythropoietic porphyria
Thalassaemia and thalassaemic syndromes
Lead poisoning
Abnormal globin chain synthesis
Normal iron stores (Serum Fe inc., TIBC N, % sat. inc.)
Thalassaemia and thalassaemic syndromes
Unstable haemoglobinopathy
Unknown pathogenesis
Normal or increased iron stores (Serum Fe inc., TIBC N, % sat. inc.)
Sideroblastic anaemia
Di Guglielmo's syndrome
Chronic haemoglobinuria
Normal iron stores (Serum Fe inc., TIBC N, % sat. inc.)
Acquired haemolytic anaemia with intravascular haemolysis
Chronic infections
Immunological
Infectious hepatitis
Cold agglutinin disease
Paroxysmal cold haemoglobinuria — syphilis
Drug-induced
Mechanical or fragmentation type (Table 12.28)
Paroxysmal nocturnal haemoglobinuria
TABLE 12.19
Iron Deficiency Anaemia
Nutritional inadequacy
Elderly
Infants and children
Pregnancy
Malabsorption
Stomach disorders
168
DIFFERENTIAL DIAGNOSIS
Table 12.19 cont.
Peptic ulcer
Hiatus hernia
Post-gastrectomy syndrome
Mucosal atrophy
Carcinoma
Intestinal disorders
Coeliac disease
Sprue
Steatorrhoea
Regional ileitis
Ulcerative colitis
Ankylostomiasis (hookworm disease)
Transferrin abnormality
Congenital atransferrinaemia
Increased iron requirement
Pregnancy and lactation
Infancy
Adolescence in females
Chronic iron loss
Menstruation in women during child-bearing age
Recurrent epistaxis
Recurrent gastro-intestinal haemorrhage
Recurrent haematuria
Haemoglobinuria/haemosiderinuria
Focal sequestration of iron
In kidney — paroxysmal nocturnal haemoglobinuria and chronic
acquired haemolytic anaemias with intravascular haemolysis
In lungs - idiopathic pulmonary haemosiderosis
In iron stores — severe anaemia of chronic disorders (Table 12.17)
TABLE 12.20
Hypochromic Microcytic Macro-ovalocytic Type
Malnutrition
Elderly
Infants
Poor
Pregnancy
Malabsorption
Post-gastrectomy syndrome
Malabsorption syndrome (Table 12.21)
Hypochromic microcytic type (Table 12.18)
Complicated by megaloblastosis (Table 12.10)
Normochromic macro-ovalocytic type (Table 12.10)
Complicated by iron deficiency (Table 12.19)
169
THE PERIPHERAL BLOOD FILM
TABLE 12.21
Malabsorption Syndrome
A. Intraluminal disorders
Inadequate mixing of food with bile salts and lipase
Post-gastrectomy syndrome
Gastro-jejunostomy
Pyloroplasty
Gastric atrophy
Inadequate lipolysis
Severe protein deficiency
Cystic fibrosis of pancreas
Chronic pancreatitis
Carcinoma of head of pancreas
Pancreatic fistula
Vagus nerve section
Inadequate emulsification of fat - bile salt deficiency
Severe liver disease
Biliary tract disease
Obstructive jaundice
Altered bacterial flora - stagnant loop syndrome
Blind loops of small intestine
Strictures
Fistula
Diverticula
Scleroderma
Intestinal hurry
Post-gastrectomy syndrome
Enteritis
B. Defective mucosal transport (general malabsorption)
Loss of surface
Surgical resection or bypass of bowel
Intestinal fistula
Partial or sub-total atrophy of villi
Steatorrhoea
Coeliac disease
Sprue — tropical and non-tropical
Crohn's disease
Amyloid disease
Scleroderma
Dermatitis herpetiformis
Immunoglobulin alpha chain disease
Pernicious anaemia
Post-gastrectomy syndrome
Vitamin B 1 2 deficiency (reversible atrophy)
Folate deficiency (reversible atrophy)
170
DIFFERENTIAL DIAGNOSIS
Table 12.21 cont.
Alcoholism (reversible atrophy)
Sideroblastic anaemia
Drugs — neomycin, phenindione, para-aminosalicylic acid
Radiation injury
Infections
Enteritis
Hepatitis
Tuberculosis
Whipple's disease
Infestations
Hookwork (ankylostomiasis)
Giardia lamb lia
Mesenteric lymphatic obstruction
Lymphoma
Immunoglobulin alpha chain disease
Whipple's disease
Intestinal tuberculosis
Pneumatosis cystoides intestinalis
Carcinoma
Vascular defects
Mesenteric insufficiency
Constrictive pericarditis
Congestive heart failure
Endocrinopathies
Hypoparathyroidism
Hyperthyroidism
Diabetes mellitus
Zollinger-Ellison syndrome
Addison's disease
Carcinoid syndrome
Miscellaneous
Allergic gastro-enteropathy
Agammaglobulinaemia
Primary (late onset)
Sex-linked (Bruton's syndrome)
Selective inability to produce immunoglobulin A
C. Isolated biochemical abnormality (selective malabsorption)
Abetalipoproteinaemia
Cystinuria
Hartnup disease
Disaccharide insufficiency
Monosaccharide transport defect
Iron deficiency anaemia (Table 12.19)
Vitamin B 1 2 deficiency (Table 12.11)
Folate deficiency (Table 12.13)
THE PERIPHERAL BLOOD FILM
TABLE 12.22
Target Cell Type
Artefact
Normal blood
Hypochromic microcytosis
Iron deficiency anaemia (Table 12.19)
Thalassaemia and thalassaemic syndromes
Sideroblastic anaemia (Table 12.24)
Visual macrocytosis
Hereditary lecithin-cholesterol acyl transferase deficiency
Liver disorders
Obstructive jaundice
Hepatitis with biliary obstruction
Cirrhosis of the liver
Carcinoma of the liver
Haemoglobinopathies
Beta thalassaemia major
Haemoglobin C disease and trait
Haemoglobin S disease
Post-splenectomy syndrome
Lead poisoning
FILMS WITH ANISOCHROMIC RED CELLS
TABLE 12.23
Dimorphic Type
Polycythaemia (Table 12.2)
With developing iron deficiency (Table 12.19)
Anaemia
No polychromatophilia
Sideroblastic anaemia (Table 12.24)
Di Guglielmo's syndrome
Late stages of iron deficiency anaemia (Table 12.19) responding to
Iron Therapy
Development of iron deficiency (Table 12.19) in megaloblastic
anaemia (Table 12.10) responding to specific therapy
Polychromatophilia present
Acute or chronic haemorrhage
Early stages of iron deficiency anaemia (Table 12.19) responding to
Iron Therapy
172
DIFFERENTIAL DIAGNOSIS
TABLE 12.24
Sideroblastic Anaemia
Hereditary
Sex-linked hypochromic anaemia
Acquired
Primary or idiopathic
Secondary
Haematological disorders
Thalassaemia and thalassaemic syndromes
Haemolytic anaemias
Aplastic anaemia
Pernicious anaemia
Myeloproliferative disorders
Di Gugliemlo's syndrome
Leukaemia
Lymphoma
Myelomatosis
Collagen disorders
Rheumatoid arthritis
Polyarteritis nodosa
Drug therapy
Anti-tuberculous
Cycloserine
Isoniazid
Pyrazinamide
Para-aminosalicylic acid
Antibacterial
Chloramphenicol
Anti-inflammatory
Phenacetin
Paracetamol
Cytotoxic drugs
Azathioprine
Toxic
Chronic alcoholism
Lead poisoning
Chronic uraemia
Nutritional
Malnutrition
Malabsorption syndrome (Table 12.21)
Megaloblastic anaemia (Table 12.10)
Chronic alcoholism
Vitamin B 6 (pyridoxine) deficiency
Miscellaneous
Metastatic carcinoma
Myxoedema
Porphyria cutanea tarda
173
THE PERIPHERAL BLOOD FILM
FILMS WITH ABNORMALLY SHAPED RED CELLS
TABLE 12.25
Elliptocytic Type
Elliptocytes more than 25 per cent of red cells
No anaemia
Hereditary elliptocytosis
Anaemia
Hereditary elliptocytic haemolytic anaemia
Hereditary elliptocytosis with acquired anaemia
Elliptocytes less than 25 per cent of red cells
Anaemias
Haemoglobinopathies
Thalassaemia and thalassaemic syndromes
Haemoglobin S disease
Haemoglobin C disease and trait
Hereditary haemorrhagic telangiectasia
Agnogenic myeloid metaplasia (myelofibrosis)
TABLE 12.26
Spherocytic Type
Hereditary spherocytes
Hereditary spherocytosis
Acquired spherocytes
Haemoglobinopathies
Thalassaemia and thalassaemic syndromes
Haemoglobin S disease
Extramedullary acquired haemolytic anaemia (Table 12.8)
Splenomegaly (Table 12.49)
Myeloproliferative disorders
TABLE 12.27
Sickle Cell Type
Sickle
Sickle
Sickle
Sickle
174
cell
cell
cell
cell
disease
trait (occasionally)
— haemoglobin C disease
— thalassaemia disease
DIFFERENTIAL DIAGNOSIS
TABLE 12.28
Irregular Poikilocytic Type
Acanthocytes
Hereditary beta lipoprotein deficiency
Pyknocytes
Premature infants due to immaturity of red cell enzymes
Burr/spur cells
Fragmentation of normal red cells (extrinsic factors)
Physical
Burns
March haemoglobinuria
Mechanical
Prosthetic heart valves
Calcified and stenosed heart valves
Micro-angiopathy
Uraemic-haemolytic syndrome in infancy
Bleeding peptic ulcer
Malignant hypertension
Metastatic carcinoma
Mucin-producing adenocarcinoma
Thrombotic thrombocytopenic purpura
Polyarteritis
Acute hepatic necrosis
Disseminated intravascular coagulation (Table 12.7)
Toxic causes
Acute alcoholism
Uraemia in adults
Drugs regularly producing Heinz bodies, e.g., dapsone
Fragmentation of abnormal red cells (intrinsic factors)
Iron deficiency anaemia (Table 12.19)
Megaloblastic anaemia (Table 12.10)
Cell membrane lipid abnormalities
Liver disorders
Hypothyroidism
Haemoglobinopathies
Thalassaemia and thalassaemic syndromes
Sickle cell anaemia
Unstable haemoglobinopathy
ATP instability
Hexokinase deficiency
Pyruvate kinase deficiency
Heinz body anaemia (Table 12.32)
Antibody-injured red cells
Immunological haemolytic anaemia (Table 12.8)
cont.
175
THE PERIPHERAL BLOOD FILM
Table 12.28 cont.
Schist ocy tes
Disorders listed above
Disseminated intravascular coagulation (Table 12.7)
Tear-drop poikilocytes
Megaloblastic anaemia (Table 12.10)
Failure, replacement or infiltration of erythropoietic tissue (Table
12.3)
FILMS WITH INCLUSION - CONTAINING RED CELLS
TABLE 12.29
Ho well-Jolly Body Type
Haemolytic anaemia (Table 12.8)
Post-splenectomy syndrome
Splenic atrophy
Congenital atrophy of the spleen
Megaloblastic anaemia (Table 12.10)
Malabsorption syndrome (Table 12.21)
TABLE 12.30
Siderocytic Type
Haemolytic anaemia (Table 12.8)
Sideroblastic anaemia (Table 12.24)
Lead poisoning
TABLE 12.31
Stippled Cell Type
Reticulocytic cells
Polychromatic cell type (Table 12.34)
Lead poisoning
Thalassaemic cells
Thalassaemia and thalassaemic syndromes
Siderocytic cells
Heavy metal poisoning
Lead poisoning
Sideroblastic anaemia (Table 12.30)
Haemolytic anaemia (Table 12.8)
176
DIFFERENTIAL DIAGNOSIS
TABLE 12.32
Heinz Body Type
Haemoglobinopathy
Unstable haemoglobins
Congenital Heinz body anaemia in infants
Drug-induced
Bacterial and viral infections
Haemoglobin H disease
Metabolic
HMP-shunt pathway (glutathione instability)
Physiological immaturity of enzymes in neonatal infants
Prophylactic Vitamin K therapy
Normal enzyme activity
Drugs in high doses, e.g., dapsone, phenacetin
Chemicals, e.g., aniline, nitrates/nitrites
Hereditary diminution of enzyme activity and glutathione
deficiency
Bacterial and viral infections
Diabetic acidosis
Environmental factors
Drug-induced
E-M pathway
Hereditary diminution of triose phosphate isomerase activity
Drug-induced
TABLE 12.33
Methaemoglobinaemia
Hereditary
Haemoglobin M variants
Enzymopathies
Methaemoglobin reductase deficiency
Methaemoglobin diaphorase deficiency
Glutathione deficiency
Acquired
Heinz body anaemia (Table 12.32)
Ionizing irradiation
Intestinal obstruction
Clostridium welchii sepsis
177
THE PERIPHERAL BLOOD FILM
FILMS WITH IMMATURE RED CELLS
TABLE 12.34
Polychromatic Cell Type
Polycythaemia (Table 12.2)
Anaemia
Response to blood loss
Haemorrhagic anaemia (Table 12.6)
Haemolytic anaemia (Table 12.8)
Response to specific haematinic therapy
Iron deficiency anaemia (Table 12.19) on iron
Megaloblastic anaemia (Table 12.10) on specific therapy
Pyridoxine-responsive sideroblastic anaemia on pharmacological
doses of pyridoxine
Splenic disorders
Post-splenectomy
Splenic atrophy
Congenital absence of spleen
Malignancy
Metastatic carcinoma in bone marrow
Pre-leukaemia
Leukaemia
Myelomatosis (5 per cent of cases)
Di Guglielmo's syndrome
TABLE 12.35
Erythroblastic Type
With immature neutrophils
Leuco-erythroblastic reaction (Table 12.46)
Without immature neutrophils
Polycythaemia
Secondary polycythaemia (Table 12.2)
Anaemia
Haemorrhagic anaemia (Table 12.6)
Severe iron deficiency anaemia (Table 12.19)
Haemolytic anaemia (Table 12.8)
Severe megaloblastic anaemia (Table 12.10)
Di Guglielmo's syndrome
Miscellaneous
Congenital syphilis
Obliteration of bile ducts in infants
178
DIFFERENTIAL DIAGNOSIS
FILMS WITH AGGREGATED RED CELLS
TABLE 12.36
Rouleaux Type
Hyperfibrinogenaemia (Table 12.37)
Physiological
Acquired
Hyperglobulinaemia
Monoclonal gammopathy (Table 12.38)
Essential or benign type
Malignant type
Primary
Secondary
Polyclonal gammopathy (Table 12.39)
TABLE 12.37
Hyperfibrinogenaemia
Physiological
During menstruation
During pregnancy
Acquired
Acute infections, e.g., pneumonia
Collagen disorders, e.g., rheumatoid arthritis
Liver disorders, e.g., hepatitis
Renal disorders, e.g., nephrosis, renal failure
TABLE 12.38
Monoclonal Gammopathy
Essential or benign type (IgG 65%, IgA 25%, IgM 10%)
May occur in
Gastro-intestinal diseases
Ulcerative colitis
Steatorrhoea
Liver disorders
Cirrhosis
Infective hepatitis
Haemopoietic disorders
Aplastic anaemia
Myeloproliferative disorders
3% of subjects over 70 years of age
Miscellaneous
Heart disease
Sarcoidosis
Collagen diseases
cont.
179
THE PERIPHERAL BLOOD FILM
Table 12.38 cont.
Malignant' type
Primary
With Bence-Jones proteinuria
Myelomatosis (IgG 53%; IgA 22%; Bence-Jones 20%; Biclonal
2%; IgD 1.5%; IgM 0.5%)
Without Bence-Jones Proteinuria
Waldenströms macroglobulinaemia (IgM)
Heavy chain disease
Gamma chain (Fc Fragment) disease
Alpha chain disease
Mu chain or IgM monomer disease
Secondary
Epithelial neoplasms in bowel
Lymphoproliferative diseases
Gaucher's disease (IgG)
Lichen myxoedematosus (IgG lambda)
Pyoderma gangrenosum (IgA)
Cold agglutinin disease (IgM kappa)
TABLE 12.39
Polyclonal Gammopathy
Infections
Viral diseases
Infectious hepatitis
Infectious mononucleosis
Lymphogranuloma
Pneumonia
Bacterial diseases
Chronic severe staphylococcal infection
Subacute bacterial endocarditis
Tuberculosis
Leprosy
Protozoal diseases
Malaria
Leishmaniasis
Trypanosomiasis
Schistosomiasis
Liver diseases
Hepatitis
Cirrhosis of the liver
Sarcoidosis
Auto-immune disorders
Hashimoto's thyroiditis
Haemolytic anaemia
180
DIFFERENTIAL DIAGNOSIS
Table 12.39 cont.
Collagen diseases
Systemic lupus erythematosus
Rheumatoid arthritis
TABLE 12.40
Cryoglobulinaemia
Dysproteinaemias
Waldenstrom's macroglobulinaemia
Myelomatosis (some cases)
Essential benign hyperglobulinaemia
Lymphoproliferative disorders
Collagen disorders
Rheumatoid arthritis
Systemic lupus erythematosus
Polyarteritis
Sjogren's syndrome
Miscellaneous
Chronic hepatitis
Thrombotic thrombocytopenic purpura
TABLE 12.41
Auto-agglutination Type
Acquired haemolytic anaemia
Immunological
Auto-immune antibodies (Table 12.8)
FILMS WITH PREDOMINANT NEUTROPHILS
TABLE 12.42
Absolute Lymphocytopenia
Hereditary cellular immunodeficiency diseases
Environment defect
Thymus
Thymic aplasia (third and fourth pharyngeal pouch defect or
Di George syndrome)
Ataxia telangiectasia
Stem cell defect
Myeloid and lymphoid deficiency
cont.
181
THE PERIPHERAL BLOOD FILM
Table 12.42 cont.
Reticular dysgenesis (De Vaal - Seynhaeve syndrome)
Lymphoid deficiency (with associated Ig deficiency)
Thymic alymphoplasia (Nezelof s syndrome)
Swiss-type agammaglobulinaemia
Sex-linked
lymphopenic agammaglobulinaemia
(Gitlin's
syndrome)
Red cell aplasia with thymoma and agammaglobulinaemia
(Good's syndrome)
Secondary lymphocytopenia
Lymphocyte destruction
Increased plasma corticoid levels
Steroid therapy
Cushing's syndrome
Stress reactions
Immuno-suppressive therapy
Irradiation
Lymphoma
Hodgkin's disease
Gamma chain (Fc fragment) disease
Autocytotoxins
Systemic lupus erythematosus
Miscellaneous
Nutritional deficiencies, e.g., starvation
Uraemia
Miliary tuberculosis
Lymphocyte loss
Thoracic duct drainage
Impaired intestinal drainage
Mesenteric lymphatic obstruction (Table 12.21)
Severe right heart failure
TABLE 12.43
Hypo-immunoglobulinaemia
Hereditary
With lymphocytopenia (Table 12.42)
Without lymphocytopenia
Sex-linked agammaglobulinaemia (Bruton's syndrome)
Selective inability to produce IgA
Agammaglobulinaemia with thrombocytopenia and eczema
(Wiskott-Aldrich syndrome
Secondary
Physiological in neonatal infants
Premature infants
Placental abnormalities
182
DIFFERENTIAL DIAGNOSIS
Table 12.43 cont.
Low Ig in mother
Maternal allo-antibodies to infant's IgG molecule
Excessive chronic plasma protein loss
Kidney — some nephrotic states
Small intestine — protein-losing enteropathy
Skin — extensive burns
Increased Ig catabolism
Thyrotoxicosis
Diabetes mellitus
Toxic factors
Renal failure with uraemia
Cytotoxic drugs
Coeliac disease
Bone marrow disorders
Hypoplasia
Myelofibrosis
Metastatic carcinoma
Lymphatic tissue neoplasia
Lymphoma
Leukaemia
Myelomatosis
Macroglobulinaemia
TABLE 12.44
Absolute Neutrophilia
Polycythaemia
Polycythaemia rubra vera
Gaisbock's syndrome
Erythrocytosis with complications (Table 12.2)
Physiological
Neonatal infants
During pregnancy, labour and puerperium
After strenuous exercise
Infections
Bacteraemia
Septicaemia
Diphtheria
Tonsillitis
Pneumonia
Miliary tuberculosis
Scarlet fever
Acute rheumatic fever
Meningitis
Abscesses — pelvic and subphrenic
cont.
183
THE PERIPHERAL BLOOD FILM
Table 12.44 cont.
Cholera
Typhus
Early stages of viral infections
Acute blood loss
Haemorrhage (Table 12.6)
Haemolysis (Table 12.8)
Trauma and burns
Coronary thrombosis
Intestinal obstruction and volvulus
Post-splenectomy syndrome
During convulsions
Drug reactions and chemical poisoning
Metabolic disorders
Diabetic acidosis
Renal failure and uraemia
Acute gout
Eclampsia of pregnancy
Metabolic disorders in neutrophil polymorphs
Sex-Hnked chronic granulomatous disease in children
Autosomal chronic granulamatous disease in children
Job's syndrome
Lipochrome histiocytosis
Myeloperoxidase deficiency
Malignancies
Necrotic malignant tumours
Hodgkin's disease
Pre-leukaemia
TABLE 12.45
Neutrophil Leukaemoid Reaction
Absolute neutrophilia (Table 12.44)
Pre-leukaemia
Leuco-erythroblastaemia (Table 12.46)
TABLE 12.46
Leuco-erythroblastic Type
Polycythaemia
Primary or erythraemic type (Table 12.2)
Anaemia
Myeloid metaplasia
Primary
Agnogenic myeloid metaplasia — myelofibrosis of bone marrow
184
DIFFERENTIAL DIAGNOSIS
Table 12.46 cont.
Secondary
Replacement/infiltration of haemopoietic tissue (Table 12.3B)
Toxic
Ionizing irradiation
Poisoning by phosphorous, carbon tetrachloride, benzene
Acute blood loss
Severe haemorrhage (Table 12.6)
Haemolytic anaemia (Table 12.8)
Megaloblastic anaemia (some cases) (Table 12.10)
Splenic disorders
Banti's disease
FILMS WITH PREDOMINANT LYMPHOCYTES
TABLE 12.47
Absolute Neutropenia
Diminished production of neutrophils
A. Failure of myelopoietic (granulocytic) tissue
Hereditary
Fanconi syndrome
Aplasia of Blackfan-Diamond type (occasionally)
Reticular dysgenesis (De Vaal - Seynhaeve syndrome)
Acquired
Ineffective haemopoiesis
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Hypersplenism (Table 12.50)
Viral infections and viral hepatitis
Paroxysmal nocturnal haemoglobinuria
Drugs and chemicals and alcohol
Ionizing irradiation — x-rays, radioactive phosphorus
Renal failure
B. Replacement/infiltration of haemopoietic tissue
Excluding myeloproliferative disorders (Table 12.3)
Loss of neutrophil polymorphs
A. Sequestration
In spleen (Table 12.49)
At inflammatory sites, e.g., pneumonia
In extracorporeal shunts, e.g., during open-heart surgery and renal
dialysis
B. Destruction or lysis
Infections
Whooping cough
Undulant fever
cont.
185
THE PERIPHERAL BLOOD FILM
Table 12.47 cont.
Typhoid and paratyphoid
Miliary tuberculosis
Syphilis
Infectious hepatitis
Infectious mononucleosis
Influenza
Measles
Mumps
Chicken pox
Herpes zoster
Infestations
Leishmaniasis (kala-azar)
Immunological
Iso-antibodies
Foetomaternal ABO incompatibility
Immune antibodies
Foetomaternal transplantation antigen incompatibility
Auto-antibodies
Cold, warm, bi-thermic and drug-induced (Table 12.8)
Paroxysmal nocturnal haemoglobinuria
Drug-induced
Direct toxic effects
Immune reaction
Hypersplenism (Table 12.50)
Pathogenesis unknown
Congenital disorders
Familial cyclical neutropenia
Chronic granulocytopenia in children
Chediak-Higashi-Steinbrinck syndrome
Lazy leucocyte syndrome
In infants
In adults without associated disease
In adults with infections, myeloma, agammaglobulinaemia and
bone malignancy
Neutropenia in Africans
Genetic (Shaper and Lewis, 1971)
Dietary (Ezeilo, 1972)
Neutropenia with dysglobulinaemia
Chronic alcoholism
TABLE 12.48
Pancytopenia
Diminished production of cells
A. Failure of haemopoietic tissue
Fanconi syndrome
186
DIFFERENTIAL DIAGNOSIS
Table 12.48 cont.
Paroxysmal nocturnal haemoglobinuria
Viral infections and viral hepatitis
Renal failure
Graft-versus-host (GVH) rejection
Drugs, chemicals and alcohol
Ionizing irradiation
B. Ineffective haemopoiesis
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Hypersplenism (Table 12.50)
C. Replacement/infiltration of haemopoietic tissue (Table 12.3B)
D. Depression of haemopoiesis (Table 12.17)
Loss of cells
A. Sequestration
In spleen
In extracorporeal shunts, e.g., during open-heart surgery and renal
dialysis
B. Destruction or lysis
Severe bacterial and viral infections
Immunological — auto-antibodies
Paroxysmal nocturnal haemoglobinuria
Drugs, chemicals and alcohol
Ionizing irradiation
Hypersplenism (Table 12.50)
TABLE 12.49
Splenomegaly
Infections
Septicaemia
Subacute bacterial endocarditis
Typhoid and paratyphoid
Brucellosis
Tuberculosis
Syphilis
Infectious mononucleosis
Infective hepatitis
Toxoplasmosis
Histoplasmosis
Parasites (tropical diseases)
Malaria
Leishmaniasis
Schistosomiasis
Trypanosomiasis
cont.
187
THE PERIPHERAL BLOOD FILM
Table 12.49 cont.
Anaemias
Thalassaemia in children
Fanconi's syndrome
Megaloblastic anaemia
Chronic iron deficiency
Chronic haemolytic anaemias
Severe pyruvate kinase deficiency
Myeloproliferative disorders
Lymphoproliferative disorders
Leukaemias
Lipid storage diseases
Banti's syndrome
Portal vein hypertension
Cirrhosis of the liver
Congenital stenosis and atresia of portal vein
Thrombosis of portal vein
Pressure of tumours
Splenic vein obstruction
Congenital stenosis and atresia
Thrombosis of splenic vein
Pressure of tumours
Miscellaneous
Sarcoidosis
Amyloidosis
Idiopathic thrombocytopenic purpura
Felty's syndrome
Systemic lupus erythematosus
TABLE 12.50
Hypersplenism
Infections
Miliary tuberculosis
Brucellosis
Syphilis
Infestations
Malaria
Leishmaniasis
Collagen disorders
Rheumatoid arthritis
Felty's syndrome
Systemic lupus erythematosus
Periarteritis no dosa
Banti's syndrome (Table 12.50)
188
DIFFERENTIAL DIAGNOSIS
Table 12.50 cont.
Miscellaneous
Sarcoidosis
Amyloidosis
TABLE 12.51
Absolute Lymphocytosis
Bacterial infections
Tuberculosis
Brucellosis
Whooping cough
Syphilis
Viral infections
Infectious hepatitis
Mumps
Measles
Rubella
Chickenpox
Influenza
Viral pneumonia
Infectious lymphocytosis
Infectious mononucleosis
Post-transfusion syndrome after open-heart surgery
Endocrinopathies
Hyperthyroidism
Adrenal insufficiency
Drug hypersensitivity
Lymphoproliferative disorders
Lymphoma
Macroglobulinaemia (primary)
Leukaemia
Mu chain (IgM monomer) disease
FILMS WITH PROMINENT ATYPICAL NEUTROPHILS
TABLE 12.52
Pelger-Huét / Pelgeroid Type
Hereditary Pelger-Huët anomaly
Acquired Pelgeroid anomaly
Myeloid leukaemia
Agnogenic myeloid metaplasia
Fanconi's syndrome
cont.
189
THE PERIPHERAL BLOOD FILM
Table 12.52 cont.
Prolonged exposure to myelotoxic drugs
Infections
Infectious mononucleosis
Metastatic carcinoma in bone marrow
Severe myxoedema
TABLE 12.53
Hypersegmented Neutrophil Type
Hereditary
Hereditary constitutional hypersegmentation
Chediak-Higashi-Steinbrinck syndrome
Acquired
Artefact due to radial segmentation
Neutrophilia Of pyogenic infections
Megaloblastic anaemia (Table 12.10)
Therapy with folate antagonists
Iron deficiency anaemia
Myeloproliferative disorders
Renal failure (not related to folate deficiency)
TABLE 12.54
Neutrophil Polymorphs with Basophilic Granules
Hereditary
Alder-Reilly granules
Genetic mucopolysaccharidoses (Mckusick, etal., 1965;
Brunning, 1970)
Type I
— Hurler's syndrome
Type II
— Hunter's syndrome
Type III
- Sanfilippo syndrome
Type IV
- Morquio's syndrome
Type V
- Scheie's syndrome
Type VI
— Maroteaux-Lamy syndrome
A form of ganglioside lipidosis (Zeman and Strouth, 1965;
Strouth, Zeman and Merrit, 1966)
Batten-Spielmeyer-Vogt disease
Chediak-Higashi-Steinbrinck Syndrome
Acquired
Toxic granules
Burns
Infections
Toxaemia
Rejection of renal transplant
190
DIFFERENTIAL DIAGNOSIS
TABLE 12.55
Neutrophil Polymorphs with Basophilic Inclusions
Hereditary
May-Hegglin anomaly
Acquired
Dohle or Amato bodies
Infections
Septicaemia
Toxaemia
Burns
Uncomplicated pregnancy (some cases)
FILMS WITH PROMINENT ATYPICAL LYMPHOCYTES
TABLE 12.56
Lymphocytes with Notched Nuclei
Notch nucleus
Viral infections
Ionizing irradiation
Leukaemia
Radial segmentation
Anticoagulant artefact
Whooping cough
Viral infections
Leukaemia
Twinning deformity
Viral infections
Ionizing irradiation
Leukaemia
TABLE 12.57
Lymphocytes with Vacuolated Cytoplasm
Hereditary
Hereditary lipidoses
Niemann-Pick disease (sphingomyelin lipidosis)
Tay-Sachs' disease (amaurotic familial idiocy or ganglioside
lipidosis)
Batten-Spielmeyer-Vogt disease (? ganglioside lipidosis)
Glycogen storage disease
Pompe's disease (type II glycogen storage disease of heart or
idiopathic generalized glycogenosis)
cont.
191
THE PERIPHERAL BLOOD FILM
Table 12.57 cont.
Genetic mucopolysaccharidoses
Hurler-Hunter syndrome
Acquired
Viral infections
Mononucleosis
Lymphatic leukaemia
FILMS WITH PROMINENT MONOCYTES
TABLE 12.58
Absolute Monocytosis
Infections
Bacterial
Tuberculosis
Brucellosis
Subacute bacterial endocarditis
Typhoid (rare)
Rickettsial
Typhus
Rocky Mountain spotted fever
Protozoal
Malaria
Leishmaniasis (kala-azar)
Trypanosomiasis
Recovery from acute infections
Recovery from severe neutropenia
Gastro-intestinal disorders
Sprue
Ulcerative colitis
Regional ileitis
Haematological disorders
Pre-leukaemia
Myelomonocytic leukaemia
Lymphoma
Leukaemic reticulo-endotheliosis
Miscellaneous
Drug poisoning
Systemic lupus erythematosus
Post-splenectomy syndrome
Lipidoses
Gaucher's disease
Niemann-Pick's disease
192
DIFFERENTIAL DIAGNOSIS
Table 12.58 cont.
Histiocytosis X
Hand-Schüller-Christian disease
Eosinophilic granuloma
Letterer-Siwe disease
FILMS WITH ATYPICAL MONONUCLEAR CELLS
TABLE 12.59
Mononucleosis Type
Positive serum test for Paul-Bunnell heterophile antibody
Infectious mononucleosis
Post open-heart surgery (some cases)
Negative serum test for Paul-Bunnell heterophile antibody
Infection with
Cytomegalic virus
Adenovirus
Herpes virus
Mumps virus
Infective hepatitis virus
Toxoplasma gondii
Salmonella typhosa
Brucella
FILMS WITH PROMINENT EOSINOPHILS
TABLE 12.60
Absolute Eosinophilia
Familial or hereditary
Acquired
Hypersensitivity disorders
Infections
Rheumatic fever
Erythema multiforme
Scarlet fever
Mycotic infections
Infestations
Protozoa
Malaria
cont.
193
THE PERIPHERAL BLOOD FILM
Table 12.60 cont.
Amoebiasis
Pneumocystis
Toxoplasma
Metazoa
Nematodes
Toxocariasis
Filariasis
Ankylostomiasis
Trematodes
Schistosomiasis
Cestodes
Taeniasis
Arthropods
Scabies
Allergic disorders
Hay feVer
Asthma
Urticaria
Angioneurotic oedema
Serum sickness
Allergic vasculitis
Stevens-Johnson syndrome
Drugs
Skin disorders
Eczema
Pemphigus
Psoriasis
Ichthyosis
Dermatitis herpetiformis
Gastro-intestinal disorders
Milk precipitin diseases
Protein-losing enteropathy
Ulcerative colitis
Hypereosinophilic syndrome (Table 12.61)
Malignant disorders
Lymphoma e.g., Hodgkin's disease
Myeloproliferative disorders
'Eosinophilic' leukaemia
Miscellaneous
Radiotherapy
Hypo-adrenalism
Splenectomy
Sarcoidosis
Goodpasture's syndrome
194
DIFFERENTIAL DIAGNOSIS
TABLE 12.61
Hypereosinophilia
Disorders causing eosinophilia (Table 12.60)
Loeffler's syndrome
Loeffler's endocarditis
Disseminated eosinophilic collagen disease
Polyarteritis nodosa
Tropical eosinophilia
'Eosinophilic' leukaemia
FILMS WITH PROMINENT BASOPHILS
TABLE 12.62
Absolute Basophilia
Virus infections
Chickenpox
Smallpox
Influenza
Hypersensitivity reactions
To food
To drugs
To inhalants
Endocrinopathies
Myxoedema
Diabetes mellitus
Malignancies
Carcinoma
Hodgkin's disease
Myeloproliferative disorders
Acute myeloblastic leukaemia
Miscellaneous
Tuberculosis
Ulcerative colitis
Ankylostomiasis
Post-splenectomy syndrome
FILMS WITH PROMINENT PLASMA CELLS
TABLE 12.63
Plasmacytosis
Infections
Bacterial
Scarlet fever
cont.
195
THE PERIPHERAL BLOOD FILM
Table 12.63 cont.
Whooping cough
Viral
Measles
Rubella
Mumps
Chickenpox
Drug hypersensitivity
Following irradiation
Malignancy of alimentary tract
Mononucleosis (Table 12.59)
Hyperimmunoglobulinaemia
Monoclonal gammopathy (Table 12.38)
Polyclonal Gammopathy (Table 12.39)
Cryoglobulinaemia (Table 12.40)
FILMS WITH INCREASED NUMBER OF PLATELETS
TABLE 12.64
Thrombocytosis
Thrombocythaemia
Essential or haemorrhagic thrombocythaemia
Other myeloproliferative disorders
Thrombocytosis
Transient
Acute haemorrhage
Post-partum period
Post-operative period
Post-splenectomy syndrome
Infections, e.g., pneumonia
Chronic
Iron deficiency anaemia (Table 12.19)
Haemolytic anaemia (Table 12.8)
Chronic blood loss (Table 12.6)
Acute rheumatic fever
Tuberculosis
Rheumatoid arthritis
Ulcerative colitis
Regional ileitis
Sarcoidosis
Hodgkin's disease
Malignancy
196
DIFFERENTIAL DIAGNOSIS
TABLE 12.65
Increased Platelet Adhesiveness
Physiological
During pregnancy
After a fatty meal
Acquired
Polycythaemia
Generalized arteriosclerosis
Ischaemic heart disease
Multiple sclerosis
Diabetes mellitus
After surgical operations
Oral contraceptive therapy
FILMS WITH REDUCED NUMBER OF PLATELETS
TABLE 12.66
Thrombocytopenia
Diminished production of platelets
A. Failure of thrombopoiesis
Hereditary
Fanconi syndrome
Congenital deficiency of megakaryocytes (thrombocytopenia
with absent radius - TAR syndrome. Hall et al., 1969)
Sex-linked Wiskott-Aldrich syndrome (thrombocytopenia with
agammaglobulinaemia and eczema)
May-Hegglin anomaly
Bernard-Soulier syndrome (some cases)
Acquired
Ineffective haemopoiesis
Megaloblastic anaemia (Table 12.10)
Sideroblastic anaemia (Table 12.24)
Hypersplenism (Table 12.50)
Viral infections
Paroxysmal nocturnal haemoglobinuria
Drugs and chemicals and alcohol
Ionizing irradiation
Renal failure
Graft-versus-host (GVH) refection
B. Replacement/infiltration of haemopoietic tissue
Excluding myeloproliferative disorders (Table 12.3)
Loss of platelets
A. Sequestration
In spleen (Table 12.49)
cont.
197
THE PERIPHERAL BLOOD FILM
Table 12.66 cont.
In extracorporeal shunts, e.g., during open-heart surgery and renal
dialysis
B. Excessive consumption
Disseminated intravascular coagulation (Table 12.7)
Micro-angiopathy (Table 12.28)
C. Destruction or lysis
Mechanical destruction
Prosthetic heart valves
Calcified and stenosed heart valves
Micro-angiopathy (Table 12.28)
In extracorporeal shunts, e.g., during open-heart surgery and
renal dialysis
Viral infections
Toxic
Uraemia
Alcoholism
Immunological
Iso-antibodies
Maternal idiopathic thrombocytopenia
Neonatal thrombocytopenia
Late transfusion reaction
Auto-immune antibodies
Idiopathic thrombocytopenic purpura (ITP)
Viruses
Drugs
Systemic lupus erythematosus
Lymphoproliferative disorders
Drug-induced
Paroxysmal nocturnal haemoglobinuria
Drug-induced
Direct toxic effect
Immunological (a) hapten type, (b) innocent bystander
type, (c) auto-immune type
Micro-angiopathy (Table 12.28)
Drug-induced aplastic anaemia
Hypersplenism (Table 12.50)
TABLE 12.67
Purpura
Thrombocytopenia (Table 12.66)
Thrombocythaemia (Table 12.64)
Platelet function defects
Decreased platelet adhesiveness (Table 12.68)
Decreased platelet aggregation (Table 12.69)
198
DIFFERENTIAL DIAGNOSIS
Table 12.67 cont.
Vascular and perivascular defects
Hereditary familial purpura simplex
Marfan's syndrome
Cushing's syndrome
Ehlers-Danlos syndrome
von Willebrand's disease
Acquired von Willebrand's disease!
Purpura senilis
Purpura cachectic
Orthostatic purpura
Infections
Subacute bacterial endocarditis
Meningococcaemia
Rheumatic fever
Scarlet fever
Measles
Diphtheria
Typhus
Rocky Mountain spotted fever
Allergic disorders
Henoch-Schönlein's syndrome
Associated with erythema
Drugs and chemicals
Iodides
Quinine
Phenacetin
Salicylic acid
Gold salts
Organic arsenicals
Sulpha drugs
TABLE 12.68
Decreased Platelet Adhesiveness
Intrinsic abnormalities
Glanzmann's thrombasthenia
Storage pool disease
Portsmouth syndrome
Glycogen storage disorders
Scurvy
Myeloproliferative disorders
Leukaemia
Extrinsic abnormalities
von Willebrand's disease
Acquired von Willebrand's disease
cont.
199
THE PERIPHERAL BLOOD FILM
Table 12.68 cont.
Hypofibrinogenaemia (Table 12.69)
Factor XII deficiency (Hageman trait)
Factor VIII inhibitors/inactivators
Treated haemophilia A (some cases)
Spontaneous may occur in
Pregnancy
Collagen disorders
Asthma
Ulcerative colitis
Pemphigus
Chronic glomerulonephritis
Uraemia
Dysproteinaemia (Tables 12.37, 12.38, 12.39, 12.40)
Dextran therapy
TABLE 12.69
Decreased Platelet Aggregation
Intrinsic abnormalities
Glanzmann's thrombasthenia
Storage pool disease
Portsmouth syndrome
Scurvy
Myeloproliferative disorders
Leukaemia
Drugs, e.g., aspirin
Extrinsic abnormalities
Factor XII deficiency (Hageman trait)
Factor VIII inhibitors/inactivators (Table 12.68)
Hypofibrinogenaemia
Congenital
Acquired
Diminished synthesis
Avitaminosis
Cachexia
Liver disorders
Amyloidosis
Increased utilization
Secondary fibrinolysis
Pancreatic surgery
Cirrhosis of liver
Carcinoma of prostate with métastases
DIC (Table 12.7)
Carcinomatosis
Leukaemia
Drug reactions
200
DIFFERENTIAL DIAGNOSIS
Table 12.69 cont.
Increased level of fibrinogen degradation products
Cirrhosis of liver
Dysproteinaemia (Tables 12.37, 12.38, 12.39, 12.40)
Uraemia
FILMS WITH ATYPICAL PLATELETS
TABLE 12.70
Megathrombocytosis
Thrombocytosis
Post-splenectomy syndrome
Thrombocythaemia
Essential or haemorrhagic thrombocythaemia
Other myeloproliferative disorders
Thrombocytopenia
Inherited disorders
May-Hegglin anomaly
Bernard-Soulier syndrome
Defective thrombopoiesis
Aplastic anaemia
Megaloblastic anaemia
Enhanced platelet destruction
Mechanical
Prosthetic heart valves
Calcified and stenosed heart valves
Immunological
Systemic lupus erythematosus
Chronic idiopathic thrombocytopenic purpura (Table 12.66)
TABLE 12.71
Microthrombocytosis
Inherited disorders
Storage pool disease (some cases)
Sex-linked Wiskott-Aldrich syndrome (thrombocytopenia with
agammaglobulinaemia and eczema)
Acquired disorders
Acute haemorrhage (Table 12.6)
Iron deficiency (Table 12.19)
Inflammation
201
13
Guide to Laboratory
Diagnosis
ANAEMIA
Chronic disorders
Basic tests (Tables 13.1 and 13.2)
Serum iron concentration: total iron-binding capacity
Ferrokinetic studies
Liver function tests
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Test for hepatitis-associated antigen
Blood urea nitrogen
Serum creatinine
Malabsorption tests
Lead poisoning tests
Thyroid function tests: thyroid antibody tests
Erythropoietic hypoplasia
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Serum iron concentration: total iron-binding capacity
Ferrokinetic studies
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Paroxysmal nocturnal haemoglobinuria
Serum acid phosphatase
Alkali denaturation test for foetal haemoglobin
Acid elution test for Hb-F
Anti-nuclear factor test: L.E. cell test
Haemolytic
A. Diagnosis of haemolysis
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Serum bilirubin — total, direct and indirect
Urine urobilinogen
Red cell survival studies
202
GUIDE TO LABORATORY DIAGNOSIS
TABLE 13.1
Haematology Profile - Peripheral Blood
Red cells
Total RBC count — millions per microlitre
Packed cell volume (PCV) or haematocrit (Hct) - per cent
Blood haemoglobin concentration (Hb) — g per cent
Mean corpuscular volume (MCV) — Mm3
Mean corpuscular haemoglobin (MCH) — pg
Mean corpuscular haemoglobin concentration (MCHC) — per cent
Reticulocyte count
Absolute (corrected for anaemia and reticulocyte maturation time)
count - per cent.
Leucocytes
Total WBC count — thousands per microlitre
Differential count - PMN, Ly, Mo, Eo, Ba, per cent
— PMN, Ly, Mo, Eo, Ba, per microlitre
Platelets
Platelet count — thousands per microlitre
Blood film report
Quantitative estimation of other nucleated cells
Semi-quantitative estimation of abnormal red cells
Diagnosis of type of film
TABLE 13.2
Bone Marrow Aspirate
Tissue smears
Routine
Romanovsky stain
Prussian blue reaction for sideroblasts
Cytochemistry
Periodic acid-Schiff reaction
Peroxidase reaction
Acetate esterases reactions
Acid phosphatase (with L(+) tartrate) reaction for LRE
Feulgen reaction for micromyeloblasts
Tissue histological sections
Routine
Haematoxylin-eosin stain
Prussian blue reaction for assessment of body iron store (Table 13.3)
Cytochemistry
Periodic acid-Schiff reaction
Connective tissue stains for quantitation of reticulin (Table 13.4)
203
THE PERIPHERAL BLOOD FILM
TABLE 13.3
Quantitation of Bone Marrow Haemosiderin
Grade
0
1
2
3
4
5
6
Normal
No demonstrable iron
An occasional iron-containing histiocyte*
4-6 iron-containing histiocytes per high-power field
7-10 iron-containing histiocytes per high-power field
Many histocytes distended with haemosiderint
Histiocytes aggregating into iron containing patches
Large patches dominating each high-power field
Grade 2
* An occasional iron-containing histiocyte may be seen in iron deficiency
anaemia, particularly if the patient had received iron-dextran at some time
previously; this iron cannot be mobilized for erythropoiesis (Henderson and
Hillman, 1969).
f Small haemosiderin particles indicate rapid iron turnover, large particles
decreased iron utilization and retarded iron turnover (Nixon and Olson, 1968)
Data reproduced from Davidson and Jennison (1952), by courtesy of the
Editor, Journal of Clinical Pathology.
TABLE 13.4
Quantitation of Bone Marrow Reticulin
Grade
0
1+
No reticulin fibres demonstrable
Occasional fine individual fibres with foci of fine
fibre network near blood vessels
2+
Fine fibre network throughout most of the section.
No coarse fibres demonstrated
3+
Diffuse fine network with scattered thick coarse
fibres but no true collagen
4+
Diffuse often coarse fibre network with areas of
collagenization
Normal Grade 0 to 1+; occasionally 2+
After Bauermeister (1971)
B. Nature of haemolysis
Intramedullary
Serum iron concentration: total iron-binding capacity
Ferrokinetic studies
Extramedullary — intravascular
Urine for haemoglobin and haemosiderin
Plasma haemoglobin, haptoglobin and haemopexin
Spectroscopic analysis for plasma methaemalbumin (Schumm's
test)
204
GUIDE TO LABORATORY DIAGNOSIS
Extramedullary — extravascular
Serum iron concentration: total iron-binding capacity
Isotope scanning for site of haemolysis
C. Cause of haemolysis
Routine Tests
Direct anti-human globulin (Coombs') test
Osmotic fragility — fresh and 24-hour incubated blood
Autohaemolysis test
Ascorbate/cyanide peroxidative denaturation of haemoglobin
Supravital staining: Heinz bodies, Hb-H inclusions
Haemoglobin electrophoresis
Intrinsic red cell defects
Heinz body anaemia tests
According to red cell morphology
Extrinsic red cell defects
Antibody tests — viral, drug-induced, auto-immune
Anti-nuclear factor: L.E. cell test
Blood culture
Test for specific infections
Micro-angiopathy tests
Blood urea nitrogen
Serum creatinine
Haemorrhagic
Basic tests (Table 13.1)
Faeces for occult blood, ova, cysts and parasites
Urine for red cells and parasitic ova
Blood culture
Serum acid phosphatase
Haemostatic mechanism tests
Disseminated intravascular coagulation tests
Platelet count
Prothrombin time test
Partial thromboplastin time test
Thrombin time: reptilase time
Paracoagulation test with protamine sulphate
Fibrinogen estimation — clottable and antigenic
Serum fibrinogen degradation products assay
Radiology of gastro-intestinal tract
Heinz body
Haemolytic anaemia tests
Drug and chemical history
Basic tests (Table 13.1)
205
THE PERIPHERAL BLOOD FILM
Diagnosis of haemolysis
Nature of haemolysis
Osmotic fragility — fresh and 24-hour incubated blood
Autohaemolysis test
Supravital stain for Heinz bodies — fresh blood sample and after
18-hour incubation for methaemoglobin formation
Metabolic abnormality tests
Brilliant cresyl-blue decoloration test for G6PD deficiency
Glutathione stability test
Gluthathione assay
Screening test for other enzymopathies
Specific enzyme assays
Unstable haemoglobin tests
Supravital stain for Hb-H inclusions
Heat stability test at 50°C
Urine dipyrroles (bilifuscin-mesobilifuscin type)
Haemoglobin electrophoresis
On fresh and stored haemolysate
On methaemoglobin forms
In starch gel with buffer systems of different pH values (Huehns,
1968)
In agar gel with citrate buffer at pH 6.2
Iron deficiency
See Hypochromic microcytosis
Megaloblastic
A. Diagnosis of megaloblastosis
Drug and chemical history
Dietary history
Basic tests (Tables 13.1 and 13.2). The hallmark for the diagnosis
of megaloblastosis is the detection of the characteristic intermediate megaloblasts, particulary those with the 'clock face'
pattern.
B. Nature of deficiency
Direct tests
Serum vitamin Βχ 2 assay
Serum and red cell folate assays
Indirect tests
Valine loading test for vitamin B i 2 deficiency
Histidine loading test for folate deficiency
Folate clearance test for folate deficiency
Therapeutic tests
206
GUIDE TO LABORATORY DIAGNOSIS
C. Cause of deficiency
Vitamin Bi 2
Schilling's urinary excretion test using tracer doses of oral
radioactive vitamin B i 2 with and without intrinsic factor
Augmented histamine test for gastric achylia
Parietal cell antibody test
Intrinsic factor antibody tests
Intrinsic factor assay
Transcobalamin assay and binding capacity
Folate
Folate absorption test
D. Additional tests
Faecal fat analysis
Xylose absorption test
Jejunal mucosa biopsy
Thyroid antibody tests
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Faeces for occult blood, ova cysts and parasites
Other malabsorption tests
Radiological survey of gastro-intestinal tract
Sideroblastic
Drug and chemical history
Basic tests (Tables 13.1 and 13.2) The ring sideroblast is the hallmark
for the diagnosis.
Serum iron concentration: total iron-binding capacity
Tryptophan loading test
Serum vitamin B6 assay
Serum vitamin B1 2 assay
Serum and red cell folate assays
Jejunal mucosa biopsy
Malabsorption tests
Haemoglobin electrophoresis
AUTO-AGGLUTINATED RED CELLS
Basic tests (Table 13.1)
Urine for haemoglobin, haemosiderin and urobilinogen
Serum bilirubin — total, direct and indirect
Direct anti-human globulin (Coombs') test
Osmotic fragility — fresh and 24-hour incubated blood
Autohaemolysis test
Antibody tests — viral, drug-induced, auto-immune, cold
207
THE PERIPHERAL BLOOD FILM
BASOPHILIA
Basic tests (Tables 13.1 and 13.2)
Leucocyte alkaline phosphate test
Faeces for occult blood
Direct anti-human globulin (Coombs') test
Antibody tests - drug-induced, auto-immune
BASOPHILIC STIPPLING OF RED CELLS
Lead and heavy metal history
Basic tests (Tables 13.1 and 13.2)
Cytochemical reactions
Reticulocyte stain
Prussian blue reaction
Haemoglobin H inclusionns
Diagnosis of haemolytic anaemia
Lead poisoning tests
Haemoglobin electrophoresis
Alkali denaturation test for foetal haemoglobin
DIMORPHIC RED CELLS
Sideroblastic anaemia tests
Hypochromic microcytosis tests
Megaloblastic anaemia tests
ELLIPTOCYTOSIS
Basic tests (Table 13.1)
Haemolytic anaemia tests
EOSINOPHILIA
History of residence in tropical climate
Basic tests (Tables 13.1 and 13.2)
Blood parasites
Urine and faeces for ova, cysts and parasites
X-ray of soft tissues for parasites
Intradermal (Casoni) test for hydatid
Serum protein electrophoresis: immuno-electrophoresis
Rat mast cell degranulation test
Immunoglobulin assay: reaginic antibody test
Erythrocyte sedimentation rate (ESR)
Anti-nuclear factor: L.E. cell test
Malabsorption tests
ERYTHROBLASTAEMIA
No immature neutrophils in blood film
Basic tests (Tables 13.1 and 13.2)
Polycythaemia tests
Haemolytic anaemic tests
Haemorrhagic anaemic tests
208
GUIDE TO LABORATORY DIAGNOSIS
Hypochromic microcytosis tests
Megaloblastic anaemic tests
Immature neutrophils in blood film
Leuco-erythroblastaemia tests
HAEMOGLOBINOPATHY
Basic tests (Table 13.1)
Osmotic fragility — fresh and 24-hour incubated blood
Serum iron concentration: total iron binding capacity
Haemoglobin electrophoresis in tris-EDTA-b orate buffer at pH 8.6
Haemoglobin A2 estimation
Alkali denaturation test for foetal haemoglobin
Acid elution test for Hb-F
Specific tests
Sicklemia tests
Unstable haemoglobin tests (cf. Heinz body anaemia)
Acid elution test for Hb-F distribution in red cells
Supravital stain for Hb-H inclusions
Methaemoglobinaemia tests
Polycythaemic haemoglobin tests
HOWELLJOLLY BODY INCLUSIONS IN RED CELLS
Basic tests (Tables 13.1 and 13.2)
Malabsorption tests
Megaloblastic anaemia tests
HYPOCHROMIC MICROCYTOSIS
Preliminary tests
Drug and chemical history
Dietary history
Basic tests (Tables 13.1 and 13.2)
Serum iron concentration: total iron-binding capacity
Faeces and urine for occult blood, ova, cysts and parasites
Gastric analysis
Specific tests
Haemorrhagic anaemia
Malabsorption tests
Thalassaemia tests
Haemoglobin electrophoresis
Haemoglobin A2 estimation
Alkali denaturation test for foetal haemoglobin
Acid elution test for Hb-F
Supra vital stain for Hb-H inclusions
Unstable haemoglobin tests (cf. Heinz body anaemia)
Paraoxysmal nocturnal haemoglobinuria
Iron absorption studies
209
THE PERIPHERAL BLOOD FILM
HYPOCHROMICMICROCYTE-MACRO-OVALOCYTOSIS
Dietary history
Basic tests (Tables 13.1 and 13.2)
Megaloblastic anaemia tests
Hypochromic microcytosis tests
HYPOCHROMIC NORMOCYTOSIS
Anaemia of chronic disorders tests
LEAD POISONING
History of lead ingestion or inhalation of fumes
Basic tests (Table 13.1)
Detection of increased punctate basophilia in red cells
Fluorescence of red cells
Urinary level of delta-amino levulinic acid
Blood and urine lead levels
LEUCO-ERYTHROBLASTAEMIA
Basic tests (tables 13.1 and 13.2)
Agar culture of aspirated bone marrow for CFU-C
Leucocyte alkaline phosphatase score
Liver function tests
Serum protein electro phoresis: immuno-electrophoresis
Alkali denaturation test for foetal haemoglobin
Haemorrhagic anaemia tests
Haemolytic anaemia tests
Polycythaemia tests
LEUKAEMIA
Acute
Basic tests (Tables 13.1 and 13.2)
Cytochemical reactions of blast cells
Agar culture of aspirated bone marrow for CFU-C
Leucocyte alkaline phosphatase score
Serum lysozyme estimation
Serum uric acid
Blood culture for micro-organisms
Neutrophil function tests in non-lymphatic leukaemia
(cf. Neutropenia)
Lymphocyte function tests in lymphatic leukaemia
(cf. Lymphocytopenia)
Disseminated intravascular coagulation tests
(cf. Haemorrhagic anaemia)
Haemostatic mechanism tests
210
GUIDE TO LABORATORY DIAGNOSIS
Di Gugliemlo's syndrome
Basic tests (Tables 13.1 and 13.2)
Serum iron concentration: total iron-binding capacity
Serum bilirubin: total, direct and indirect
Serum vitamin B 12 assay
Serum and red cell folate assays
Serum uric acid
Blood culture for micro-organisms
Agar culture of aspirated bone marrow for colony-forming unit-culture
(CFU-C)
Lymphocytic/lymphosarcoma
Basic tests (Tables 13.1 and 13.2)
PAS score of lymphocytes
Phase contrast microscopy of lymphocytes
Lymphocyte function tests (cf. Lymphocytopenia)
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Haemolytic anaemia tests
Blood culture for micro-organisms
Haemostatic mechanism tests
Disseminated intravascular coagulation tests (cf. Haemorrhagic anaemia)
Myelocytic (granulocytic)
Basic tests (Tables 13.1 and 13.2)
Leucocyte alkaline phosphatase score
Chromosome analysis — Philadelphia chromosome
Serum lysozyme estimation
Serum vitamin B i 2 assay
Serum and red cell folate assays
Blood culture for micro-organisms
Neutrophil function tests (cf. Neutropenia)
Haemostatic mechanism tests
Agar culture of aspirated bone marrow for CFU-C
Myelomonocytic
Basic tests (Tables 13.1 and 13.2)
Cytochemical reactions — acetate esterases
Serum lysozyme estimation
Myelocytic leukaemia tests
Myeloblastic leukaemia tests (cf. Acute leukaemia)
Plasma cell
Basic tests (Tables 13.1 and 13.2)
Bromoindoxyl acetate esterase reaction
Hyperglobulinaemia tests
211
THE PERIPHERAL BLOOD FILM
Promyelocytic
Basic tests (Tables 13.1 and 13.2)
Myelocytic leukaemia tests
Myeloblastic leukaemia tests (cf. Acute leukaemia)
Haemostatic mechanism tests
Leukaemic reticulo-endotheliosis
Basic tests (Tables 13.1 and 13.2)
Phase contrast microscopy of 'lymphocytes'
Acid phosphatase reaction with L(+) tartrate
LEUKAEMOID REACTIONS
Myeloid
Basic tests (Tables 13.1 and 13.2)
Leucocyte alkaline phosphatase score
Neutrophil function tests (cf. Neutropenia)
Blood culture
Blood urea nitrogen
Serum creatinine
Blood sugar estimation
Sputum for Mycobacterium tuberculosis
Lymphocytoid
Basic tests (Tables 13.1 and 13.2)
PAS score of lymphocytes
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Lymph node biopsy
Lymphocyte function tests (cf. Lymphocytopenia)
Monocytoid
Basic tests (Tables 13.1 and 13.2)
Blood and urine culture for micro-organisms
Serological tests
Monocytosis tests
LYMPHOCYTOPENIA
Cellular immunity
Basic tests (Tables 13.1 and 13.2)
Lymphocyte function tests
Blastogenesis test with phytohaemagglutinin
Tuberculin test
Oidomycin (Candida) test
212
GUIDE TO LABORATORY DIAGNOSIS
Histoplasmin test
Contact tests with artificial immunogens
Haemolytic anaemia tests
Biopsy of lymph node or tonsils
Biopsy of jejunum for villus atrophy
X-ray of
Thymus region
Skeleton
Gastro-intestinal tract for nodular lymphoid hyperplasia
Humoral immunity
Basic tests (Tables 13.1 and 13.2)
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Complement assay
Measurement of levels of normally occurring antibodies
Test for antibody formation using vaccines
LYMPHOCYTOSIS
Basic tests (Tables 13.1 and 13.2)
Viral studies
Cough plate for pertussis
Direct anti-human globulin (Coombs') test
Serological tests for viral, heterophile and luetic antibodies
Lymphocytoid leukaemoid reaction tests
MALABSORPTION
A. Diagnosis of malabsorption
Drug and chemical history
Dietary history
Basic tests (Tables 13.1 and 13.2)
Serum and/or body store deficiency of essential substance
B. Nature of malabsorption
Serum iron concentration: total iron-binding capacity
Serum vitamin Bi 2 assay
Serum and red cell folate assays
Serum albumin
Serum calcium and phosphorus
Serum alkaline phosphatase
C. Demonstration of malabsorption
Faecal fat analysis
Faecal pH in children
25 g xylose absorption test
50 g disaccharide (lactose or sucrose) absorption test
100 g glucose tolerance test
213
THE PERIPHERAL BLOOD FILM
Iron aborption test
Folate absorption test
Schilling's urinary excretion test using tracer dose of oral radioactive
vitamin B i 2 with and without intrinsic factor
D. Cause of malabsorption
Gastric analysis
Jejunal biopsy
Radiological survey of gastro-intestinal tract
METHAEMOGLOBINAEMIA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Methaemoglobin level in blood
Detection of haemoglobin M
Spectral analysis of acid and cyan-methaemoglobin forms
Starch gel electrophoresis of methaemoglobin forms at pH 7.1
Heinz body anaemia tests
MICRO-ANGIOPATHY
See Disseminated intravascular coagulation (Haemorrhagic anaemia)
MONOCYTOSIS
Basic tests (Tables 13.1 and 13.2)
Blood parasites
Bone marrow parasites
Blood, urine and faeces culture for micro-organisms
Widal test for Salmonella antibodies
Test for Bruceila antibodies
Weil-Felix reaction
Anti-nuclear factor: L.E. cell test
Malabsorption tests
MONONUCLEOSIS
Basic tests (Table 13.1)
Differential Paul-Bunnell test for heterophile antibody
Liver function tests
Diagnosis of haemolytic anaemia
Serological tests for E-B virus, toxoplasmosis and cytomegalovirus
Urine for cytomegalovirus inclusion body
MYELQMATOSIS
Basic tests (Tables 13.1 and 13.2)
Serum protein electrophoresis: immuno-electrophoresis
214
GUIDE TO LABORATORY DIAGNOSIS
Immunoglobulin assay
Bence-Jones proteinuria
Cryoglobulins
Blood urea nitrogen
Serum creatinine
Serum calcium
Serum viscosity
Platelet functional studies (cf. Thrombocytosis/Thrombocythaemia)
Biopsy of gingiva and rectal musoca for amyloid
Skeletal radiology
NEUTROPENIA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Serial neutrophil counts
Viral studies
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Leuco-agglutinin tests
Direct anti-human globulin (Coombs') test on red cells
Anti-nuclear factor: L.E. cell test
Leucocyte alkaline phosphatase score
Neutrophil function tests
Nitroblue tetrazolium reduction tests
Latex particles or Candida phagocytosis test
Bactericidal test using Staphylococci
Chemotaxis test using Boyden chamber
Random mobility test
In vivo tests
Skin window test for response to inflammation (Rebuck and
Crowley, 1955; Ghosh, Hudson and Blackburn, 1973)
Adrenaline stimulation of marginated pool
Steroid stimulation test
'Piromen' (Pseudomonas polysaccharide) stimulation of bone
marrow storage pool and release reaction
Nitroblue tetrazolium reduction by monocytes
Paroxysmal nocturnal haemoglobinuria tests
Serum lysozyme estimation
Chromosome analysis - Philadelphia chromosome
Agar culture of bone marrow aspirate for CFU-C
215
THE PERIPHERAL BLOOD FILM
NEUTROPHILIA
Basic tests (Tables 13.1 and 13.2)
Blood culture for micro-organisms
Neutrophil function tests (cf. Neutropenia)
Leucocyte alkaline phosphatase score
Philadelphia chromosome
Serum lysozyme estimation
Serum complement assays
Agar culture of bone marrow aspirate for CFU-C
NORMOCHROMIC MACROCYTOSIS
Basic tests (Tables 13.1 and 13.2)
Haemorrhagic anaemia tests
Haemolytic anaemic tests
Liver function tests
NORMOCHROMIC MACRO-OVALOCYTOSIS
See Megaloblastic anaemia
NORMOCHROMIC NORMOCYTOSIS
Anaemia of chronic disorders tests
Erythropoietic hypoplasia tests
Haemorrhagic anaemia tests
Haemolytic anaemia tests
PANCYTOPENIA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Neutropenia tests
Erythropoietic hypoplasia tests
Anaemia of chronic disorders test
Paroxysmal nôctural haemoglobinuria tests
Leukaemia tests
Myelomatosis tests
PAROXYSMAL NOCTURNAL HAEMOGLOBINURIA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Haemolytic anaemia tests
Urine for haemoglobin and haemosiderin
Direct anti-human globulin (Coombs') test
Sucrose haemolysis test
Ham's acid serum haemolysis test
Plasma methaemalbumin test (Schumm's test)
Chromosome analysis
Agar culture of bone marrow aspirate for CFU-C
216
GUIDE TO LABORATORY DIAGNOSIS
PLASMACYTOSIS
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Viral studies
Hyperglobulinaemia tests (cf. Rouleaux of red cells)
POLYCHROMATOPHILIA
Basic tests (Tables 13.1 and 13.2)
History of haematinic therapy
Haemolytic anaemia tests
Haemorrhagic anaemia tests
Polycythaemia tests
POLYCYTHAEMIA
A. Diagnosis of polycythaemia
Basic tests (Tables 13.1 and 13.2)
Red cell and plasma volume determination
Serum uric acid
Leucocyte alkaline phosphatase score
Serum vitamin B 1 2 assay
B. Nature of polycythaemia
Erythropoietin assay
Arterial blood oxygen saturation
C. Cause of polycythaemia
Tests depending on other diagnostic findings
Haemoglobinopafhy
Haemoglobin electrophoresis
Alkali denaturation test for foetal haemoglobin
Blood oxygen dissociation curve
PURPURA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Blood culture
Platelet antibody tests
Haemostatic mechanism tests
Platelet function tests (cf. Thrombocytosis/Thrombocythaemia)
Fibrinogen degradation products assay in serum and urine
Blood urea nitrogen
Serum protein electrophoresis: immuno-electrophoresis
ROULEAUX OF RED CELLS
Hyper fîbrinogenaemia
Basic tests (Tables 13.1 and 13.2)
Fibrinogen estimation
217
THE PERIPHERAL BLOOD FILM
liver function tests
Blood urea nitrogen and other renal function tests
Latex fixation test for rheumatoid arthritis
Anti-nuclear factor: L.E. cell test
Tests for cryoglobulin and cryofibrinogen
Hyperglobulinaemia
Basic tests (Tables 13.1 and 13.2)
Myelomatosis tests
Tests depending on the type of infection
Liver function tests
Anti-nuclear factor: L.E. cell test
Blood culture
Tests for cryoglobulin and cryofibrinogen
SICKLAEMIA
Basic tests (Tables 13.1 and 13.2)
Haemoglobinopathy tests
Sickling reaction
Hb-S insolubility tests on microscope slide or in tube
Blood culture
Disseminated intravascular coagulation tests (cf.
anaemia)
Test for G6PD deficiency (cf. Heinz body anaemia)
Haemorrhagic
SPHEROCYTOSIS
Basic tests (Tables 13.1 and 13.2)
Direct anti-human globulin (Coombs') test
Haemolytic anaemia tests
SPINOUS ERYTHROCYTES
A. Fragmentation type
Normal red cells
Basic tests (Tables 13.1 and 13.2)
Haemostatic mechanism tests
Disseminated intravascular coagulation tests (cf. Haemorrhagic
anaemia)
Blood culture
Liver function tests
Blood urea nitrogen: urine for casts
Abnormal red cells
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Liver function tests
Routine tests for cause of haemolytic anaemia
218
GUIDE TO LABORATORY DIAGNOSIS
Heinz body anaemia tests
Red cell pyruvate kinase assay
Sicklaemia tests
Hypochromic microcytosis tests
Normochromic macro-ovalocytosis type (megaloblastic anaemia)
B. Tear-drop type
Megaloblastic anaemia tests
Erythropoietic hypoplasia tests
Pancytopenia tests
C. Acanthocytes
Basic tests (Tables 13.1 and 13.2)
Serum Lipoproteins
STOMATOCYTIC ERYTHROCYTES
Haemolytic anaemic tests
Red cell electrolyte estimation
Serological tests with blood group antibodies
Screening tests and specific assay for G6PD deficiency
liver function tests
Faeces for occult blood
Megaloblastic anaemia tests
TARGET CELLS
Basic tests (Table 13.1)
Liver function tests
Hypochromic microcytosis tests
Haemoglobinopathy tests
Sicklaemia tests
Megaloblastic anaemia tests
Malabsorption tests
THAL ASSAEMIA
See Haemoglobinopathy tests
Hypochromic microcytosis tests
THROMBOCYTOPENIA
Drug and chemical history
Basic tests (Tables 13.1 and 13.2)
Viral studies
Platelet antibody tests
Disseminated intravascular coagulation tests (cf.
anaemia)
Paroxysmal nocturnal haemoglobinuria tests
Serum protein electrophoresis: immuno-electrophoresis
Immunoglobulin assay
Anti-nuclear factor: L.E. cell test
Haemorrhagic
219
THE PERIPHERAL BLOOD FILM
Blood urea nitrogen
Direct anti-human globulin (Coombs') test on red cells
THROMBOCYTOSIS/THROMBOCYTHAEMIA
Basic tests (Tables 13.1 and 13.2)
History — ?Splenectomy
Hypochromic microcytosis tests
Haemolytic anaemia tests
Platelet function tests (cf. Myelomatosis)
Platelet aggregation with adenosine diphosphate, collagen, thrombin,
epinephrine
Platelet adhesiveness test with a glass bead column
Platelet factor 3 release
Serum uric acid
Serum Lysozyme
Leucocyte alkaline phosphatase score
Red cell and plasma volume determination
UNSTABLE HAEMOGLOBINOPATHY
See Heinz body anaemia
220
14
The Blood Film in Disease
ADRENAL DISORDERS
Hyperadrenalism — Cushing's disease
There may be an erythrocytic type of secondary polycythaemia, a
neutrophiha and a thrombocytopenia. However, no eosinophils are
seen in the film and there may be an absolute lymphocytopenia.
Hypo-adrenalism — Addison's disease
There may be a normochromic normocytic anaemia. However,
because of a concomitant reduction of the plasma volume during a
crisis, the haematology profile may not indicate the decrease in the red
cell mass. The leucocytes may show a neutropenia and a lymphocytosis.
AGAMMAGLOBULINAEMIA PRIMARY ACQUIRED (LATE ONSET)
The patient has a splenomegaly, suffers from chronic infections and a
sprue-like syndrome. Non-caseating granulomata are present in the skin,
lungs, spleen and elsewhere. The blood picture is variable. It may show
features of an auto-immune haemolytic anaemia or a malabsorption
syndrome. The leucocyte count may be low or elevated. No plasma
cells are found in the bone marrow or in the peripheral lymphoid
organs.
AGNOGENIC MYELOID METAPLASIA MYELOFIBROSIS OF THE BONE MARROW
Agnogenic myeloid metaplasia is a myeloproliferative disorder. The
blood picture varies with the stage of the disease. Initially the majority
of patients have a moderate degree of normochromic anaemia which
may become severe as a result of haemolysis and splenic sequestration.
221
THE PERIPHERAL BLOOD FILM
There is marked anisocytosis with microcytes, macrocytes and
sometimes an occasional spherocyte. Significant ovalocytosis and
moderate poikilocytosis with prominent pear-shaped and tear-drop red
cells is often seen. Mild polychromatophilia and an occasional nucleated
red cell may be evident. The degree of polychromasia does not correlate
with the erythroblastaemia. The leucocytes may be normal in number
or show a neutrophilia. Eosinophilia and/or basophilia and a few
myelocytes may be present. The leucocyte alkaline phosphatase (LAP)
score is normal or high. The platelet count is strikingly elevated but
thrombocytopenia gradually develops as the disease progresses. Platelet
morphology may be abnormal and associated with megathrombocytosis; fragments of megakaryocyte cytoplasm may be seen.
Terminally there is an anemia and a thrombocytopenia associated with
leucocytosis and a leuco-erythroblastaemia.
ALCOHOLISM - CHRONIC
The haematology profile of an alcoholic usually shows an anaemia.
Reversible neutropenia and/or thrombocytopenia may occur; occasionally there is a persistent pancytopenia. The type of anaemia is not
constant and may vary at different times in the same individual. The
blood picture may be due to the direct toxic effect of alcohol on the
haemopoietic tissue, to liver damage, to the effects of alcohol on folate
and vitamin B6 matabolism or to hypersplemism, particulary if the
subject has cirrhosis of the liver. Alcohol inhibits (1) tetrahydrofolate
formylase, necessary for purine synthesis and hence for DNA synthesis;
and (2) pyridoxal phosphokinase, required for the conversion of
pyridoxine to pyridoxal phosphate, which in turn has co-enzyme
functions in folate metabolism, haem synthesis and the transfer of iron
from the mitochrondrion to the cytoplasm. Thus the blood film in
alcoholism may show features of an anaemia of chronic disorders,
target cell anaemia, stomatocytic anaemia, haemolytic anaemia,
haemorrhagic anaemia, nutritional anaemia, megaloblastic anaemia or
sideroblastic anaemia. With the exception of the anaemia of chronic
disorders and target cell anaemia, the other types may be reversible
without specific therapy when the intake of alcohol has discontinued.
APLASTIC ANAEMIA
There is a pancytopenia of varying severity and
reticulocytopenia. The red cells are normo chromic
normocytic but they may be macrocytic. Anisocytosis,
and ovalocytosis are minimal and normoblasts are
222
an absolute
and usually
poikilocytosis
not evident.
THE BLOOD FILM IN DISEASE
Lymphocytes and monocytes appear normal. Diagnosis of aplastic
anaemia can be definitely established only by examination of a bone
marrow biopsy sample which should show aplasia of haemopoietic
tissue and its replacement by normal fatty tissue.
AUTO-IMMUNE HAEMOLYTIC ANAEMIA
Warm antibody type
The anaemia is moderate to severe. Auto-agglutinated masses of red
cells may be seen in the film. The free red cells are essentially
normochromic normocytic; macrocytes and polychromatic cells are
present. Spherocytes and fragmented red cells are seen if there is severe
haemolysis. Erythrophagocytosis of red cells by monocytes may be
noticed. The leucocyte and platelet picture varies, depending on the
disorder in which the warm auto-immune antibody developed.
Agglutination of these cells may also accompany that of the red cells.
Cold antibody type
The anaemia is mildly to moderately severe. Large masses of
auto-agglutinated red cells are present in the film. Free red cells are
commonly normochromic normocytic. A few polychromatic cells and
spherocytes are seen. The total leucocyte count may be elevated and
there may be a lymphocytosis.
Bithermic antibody type
During a paroxysm of intravascular haemolysis, pancytopenia may
develop and erythrophagocytosis be observed. The platelet count may
be further reduced by a concomitant disseminated intravascular
coagulation. After a paroxysm there is a leucocytosis, with reversion of
red cell and platelçt counts to their normal ranges. The blood picture
during a remission is usually non-specific.
BANTI'S DISEASE
The film appearance depends on the severity of the associated
hypersplenism. The cytopenia may involve two or more cell lines.
Anaemia may be normochromic or hypochromic in type.
BURNS
The red cells are normochromic and there is evidence of fragmentation
haemolytic anaemia; spherocytes of varying size, burr cells and
schistocytes are present. Neutrophilia with Dohle body inclusions
accompanies the anaemia. The platelets are normal but their numbers
decrease if disseminated intravascular coagulation supervenes.
223
THE PERIPHERAL BLOOD FILM
CARCINOMA OF THE STOMACH
The film appearance is commonly that of a hypochromic microcytic
anaemia due to the iron deficiency that results from chronic
haemorrhage and/or diminished iron absorption. Lack of gastric intrinsic
factor secretion causes vitamin B 1 2 malabsorption and latent or overt
megaloblastosis.
CHEDIAK-HIGASHI-STEINBRINCK SYNDROME
The Chediak-Higashi-Steinbrinck syndrome is a rare autosomal recessive
disorder characterized by partial albinism, photophobia, susceptibility
to infections and a striking giant granular anomaly of the leucocytes.
The peripheral blood is pancytopenic. The neutropenia and the
thrombocytopenia may be due to hypersplenism. The former, however,
commonly results from intramedullary destruction of the abnormal
cells. The morphology of the abnormal leucocytes has been described in
Chapter 5.
CIRRHOSIS OF THE LIVER
The film appearance varies. It may be that of an anaemia of chronic
disorders modified by the irregular poikilocytic type. The anaemia may
be leptocytic or on rare occasions the blood film may show a mixture
of stomatocytes and target cells, particularly if the cirrhosis is a sequel
to chronic alcoholism. Volume macrocytosis of the red cells occurs if
there is associated megaloblastosis or recurrent blood loss (occult or
frank) either from rupture of oesophageal varices or from
decompensated disseminated intravascular coagulation. Thrombocytopenia is commonly seen in alcoholics and may be due to
hypersplenism. Leucocytes in cirrhosis of the liver often do not show
any significant abnormality.
COLLAGEN DISORDERS
Polyarteritis nodosa
In polyarteritis nodosa there is a moderate anaemia of chronic disorders
which may be modified and increased in severity by the development of
renal failure, auto-immune haemolytic anaemia, haemorrhage or
disseminated intravascular coagulation (DIC). The white cell count may
be elevated and in some cases an eosinophilia may be seen. The platelet
count is usually normal unless DIC supervenes, when there is a
thrombocytopenia.
224
THE BLOOD FILM IN DISEASE
Rheumatoid arthritis
The characteristic blood picture of rheumatoid arthritis is that of
an anaemia of chronic disorders. The severity of the anaemia parallels
that of the disease. The film appearances are often modified by the
development of iron deficiency from chronic haemorrhage due to
therapy, megaloblastosis from folate deficiency and haemolytic anaemia
from the production of auto-immune antibodies. Leucocytes and
platelets show no significant abnormality. In the acute phase of the
disease there may be a neutrophilia. A terminal picture of myeloblastic
leukaemia or aplastic anaemia occasionally results from therapy for this
type of arthritis.
Felty 's syndrome (rheumatoid arthritis with splenomegaly)
The anaemia is of moderate severity and cyclic heutropenia occurs.
The red cells are normochromic, sometimes hypochromic. Eosinophilia
may be observed and the platelet count is reduced.
Systemic lupus erythematosus
This disorder may present with a thrombocytopenia or an acquired
haemolytic anaemia. The blood film shows an anaemia of chronic
disorders which may become severe if renal failure supervenes.
Leucocytes vary in appearance. There may be a lymphocytopenia;
eosinophils may be normal or appear prominent. Thrombocytopenia is
commonly present.
DI GUGLIELMO'S SYNDROME
Acute erythraemic myelosis
There is a pancytopenia of variable severity. The red cells are
essentially normochromic normocytic; round and oval macrocytes and
a moderate number of polychromatic cells may be seen. Malignant
erythroblasts with predominantly basophilic cytoplasm are commonly
present; these cells may be missed when the film is examined and a
diagnosis of megaloblastic or haemolytic anaemia may be made.
Erythroblast atypicality may be established by carrying out the
Prussian blue reaction and the PAS reaction. The former may reveal the
presence of ring sideroblasts. With the latter reaction the mature red
cells may assume a deep diffuse magenta colouration while the
erythroblasts may show a granular positivity which is marked in the
more bizarre-looking cells. The neutrophils usually appear morphologically normal and the leucocyte alkaline phophatase (LAP) score
may be increased.
225
THE PERIPHERAL BLOOD FILM
Chronic erythraemic myelosis
The patient has a refractory anaemia in which the red cells are
normochromic or dimorphic in appearance. Mild erythroblastaemia and
polychromatophilia are seen; the late erythroblasts may have
vacuolated cytoplasms.
Erythro-leukaemia
The neoplasia involves the red cell and granulocytic cell series.
There is a pancytopenia. The anaemia is normochromic or dimorphic
and associated with a variable number of polychromatic cells, malignant
erythroblasts and myeloblasts. Auer rods may be found in an occasional
myeloblast. Hypogranular and agranular cells of the neutrophilic series
may be present. The film may be diagnosed as a myeloblastic leukaemia
if the erythroblasts are few in number and not noticed or their
atypicality nor recognized. The true diagnosis becomes apparent on
inspection of bone marrow aspirate smears.
DRUG-INDUCED HAEMOLYTIC ANAEMIA
Prior to exposure to offending drugs, susceptible subjects may not be
anaemic and their red cells appear normal. During drug-induced
haemolysis, the blood film contains spherocytes of varying size,
macrocytes, polychromatic cells and fragmented cells. If the haemolytic
anaemia is immunological and due to hypersensitivity, the direct
Coombs' test may be positive or there may be schistocytosis and
thrombocytopenia resulting from a micro-angiopathy. Heinz body
anaemia develops regularly with drugs such as dapsone even in subjects
with normal red cell glycolytic enzymes. It may also appear after
exposure to other drugs in individuals with enzymopathies affecting the
red cell glycolytic pathway (G6PD deficiency) or with unstable
haemoglobins. The blood film reverts to normal on discontinuance of
the drug. The anaemia may be intramedullary in type and due to
ineffective erythropoiesis; the blood picture is that of a megaloblastic
or a sideroblastic anaemia.
EVAN'S SYNDROME
The blood picture is that of an acute haemolytic anaemia associated
with thrombocytopenia.
GLUCOSE-6-PHOSPHATE DEHYDROGENASE
(G6PD) DEFICIENCY HAEMOLYTIC ANAEMIA
Subjects with G6PD deficiency are rarely anaemic; their red cells appear
normal in the film. Haemolysis is induced by infections such as
226
THE BLOOD FILM IN DISEASE
hepatitis and pneumonia, diabetic acidosis and more commonly by
exposure to certain oxidative drugs. During the haemolytic process
spherocytes, macrocytes and fragmented red cells appear in the film
and Heinz bodies may be demonstrated by supravital staining
techniques. In Negroes the anaemia progressively worsens and after
approximately 5 days begins to improve, even with continued exposure
to the offending agent. This improvement is heralded by a peak in the
number of polychromatic cells in the film. In subjects with the
Mediterranean variant of the enzyme, haemolysis and the consequent
fall in haemoglobin may be arrested only after removal of the offending
agent. In both varieties, the leucocytes and platelets are normal unless
there is an infection or some other factor affecting their number or
their appearance in the film.
HAEMOGLOBINOPATHIES
Crystallizing haemoglobins
Haemoglobin C disease (Hb-C/CJ
There is a mild anaemia with normochromic normocytes and numerous
target cells in the film. An occasional red cell may show crystal
formation especially if the blood film has been allowed to dry slowly.
Haemoglobin C trait (Hb-A/C)
There is no anaemia and the haematology profile is normal. The
blood film will sometimes contain target cells and there may be a mild
increase in the number of irregular poikilocytes.
Haemoglobin S or sickle cell disease (Hb-S/S)
The subject is anaemic. The blood film shows normochromic
normocytes, morphological evidence of haemolysis, target cells and a
variable number of holly-leaf and/or sickle cells. Basophilic stippling
and Howell-Jolly bodies may be noticed. Normoblasts are invariably
present. The total leucocyte count is usually elevated, even in the
absence of any infection; there is a neutrophilia and monocytes may be
prominent. The platelet count is normal unless there is a sickling crisis
when it may be reduced as a result of disseminated intravascular
coagulation. The erythrocyte sedimentation rate (ESR) is low because
of poor rouleaux formation by sickled cells.
In patients with pneumococcal meningitis the number of
neutrophil polymorphs reducing nitroblue tetrazolium in the NBT
reduction test is decreased. 'Blister' red cells are seen in the blood film
of subjects with pulmonary emboli. Patients with haemoglobin S
disease exhibit haemolytic and aplastic crises. The former may be
associated with G6PD deficiency and the crises occur during infections
227
THE PERIPHERAL BLOOD FILM
and after exposure to oxidizing drugs. Both crises result in a further
lowering of the haemoglobin level.
Haemoglobin S or sickle cell trait (Hb-A/S)
There may be no anaemia and the blood film appears normal
except for the presence of a few target cells. Rarely a few holly-leaf
cells may be recognized. The sickling test is positive.
Sickle cell - haemoglobin C disease (Hb-S/C)
The patient has a compensated haemolytic state and there may be
no anaemia. The blood film, however, contains many target cells and
occasional 'fat' sickle cells. In addition, red cells with bizarrely shaped
haemoglobin masses, resulting from a combination of sickling
and haemoglobin C crystallization in the same cells may be observed,
especially if the film has been allowed to dry slowly.
Sickle cell - thalassaemia disease (Hb-S/thal)1
The blood film shows the characteristics of thalassaemia and,
depending on the type of thalassaemia, sickle cells and morphological
evidence of haemolysis may be seen. The haematology profile and the
blood picture are important for differentiating sickle cell disease and
sickle cell trait respectively from sickle cell - beta thalassaemia disease
and sickle cell - alpha thalassaemia disease.
Cyanotic haemoglobins
Haemoglobin M disease (Hb M/M)
Incompatible with foetal survival.
Haemoglobin M trait (Hb A/M)
Subjects with alpha chain variants of haemoglobin M are cyanotic
from birth while those with beta chain variants become cyanotic after 3
months of age when sufficient haemoglobin F has been replaced by the
adult haemoglobin with the abnormal beta chains. Clubbing of the
fingers is not evident in these patients and the cyanosis is not reduced
by méthylène blue or ascorbate therapy. Usually there is no anaemia or
erythrocytosis. Rarely a slight haemolytic anaemia with mild
reticulocytosis may occur.
Polycythaemic haemoglobins
The blood picture is essentially similar to that described for
secondary polycythaemia (erythrocytosis) and is due to increased
oxygen affinity, impaired haem-haem interactions and increased
erythropoietin production. Haemoglobin Rainier shows increased
resistance to alkali denaturation.
228
THE BLOOD FILM IN DISEASE
Thalassaemic syndromes
Beta thalassaemia major
There is usually a severe anaemia. Hypochromia of the red cells is
striking. The blood film contains many target cells, hypochromic
microcytes, irregular poikilocytes, macrocytes and polychromatic cells.
Punctate basophilia is prominent and cells with Howell-Jolly bodies
may be noticed. Nucleated red cells are commonly present and some
may contain basophilic inclusion bodies (precipitated alpha chains) in
their cytoplasm. There may be a neutrophilia. Platelets are within
normal limits. Beta thalassaemia major appears during infancy;
clinically the infant fails to thrive, becomes icteric and has a
splenomegaly.
Beta thalassaemia minor
There may be no anaemia or it may be mild with blood
haemoglobin concentrations above 10g per cent. The blood film,
however, shows moderate to marked hypochromia of the red cell with
microcytosis and leptocytosis. A variable number of irregular
poikilocytes are present and punctate basophilia is observed in an
occasional red cell. Polychromasia is not marked and nucleated red cells
are not found. The MCHC is within normal limits, the MCH
(approximately 20 pg) and MCV (approximately 65 Mm3) levels are
lower than those seen in iron deficiency anaemia and there is a relative
erythrocytosis for the blood haemoglobin concentration. The
thalassaemic blood picture may be masked if there is an associated iron
deficiency anaemia which will lower the haemoglobin A 2 level to
within normal limits. The haematology profile, blood film and
haemoglobin A 2 level should be re-evaluated after adequate iron
therapy.
Alpha thalassaemia major
This type of thalassaemia is incompatible with foetal survival. The
infant is usually stillborn, death being due to hydrops unassociated with
foetomaternal blood group incompatibility.
Alpha thalassaemia minor
Anaemia may be absent or mild in degree. The haematology profile
and the appearance of the red cells in the blood film are essentially
similar to those described for beta thalassaemia minor. An occasional
red cell with haemoglobin H inclusion bodies may be demonstrable with
supravital staining techniques.
Haemoglobin H disease (alpha thalassaemia intermedia)
The subject is usually anaemic due to ineffective erythropoiesis and
blood destruction. The haematology profile and the film appearances of
229
THE PERIPHERAL BLOOD FILM
the red cells are similar to the thalassaemia minors; the MCHC level,
however, may be less than 31 per cent and there is a reticulocytosis.
The characteristic inclusions, composed of precipitated beta chain
tetramers, are demonstrable only with supravital staining. Acquired
haemoglobin H disease has been reported in association with Di
Guglielmo's syndrome (Hamilton et al, 1971); the pathogenesis is
unknown.
Unstable haemoglobins
The blood picture may appear normal or may be that of a
haemolytic anaemia varying in degree from mild to severe.
Haemoglobin Köln may be associated with a thrombocytopenia. There
are no distinctive features in the red cell morphology or in the blood film
appearance to suggest the existence of an unstable haemoglobin. On
exposure to oxidizing drugs and infections, subjects with unstable
haemoglobins develop a Heinz body anaemia.
HAEMOLYTIC (ISO-IMMUNE) DISEASE OF THE NEWBORN
Rh incompatability
The neonate is anaemic and the blood film shows anisopoikilocytosis
with macrocytosis and polychromatophilia. Intermediate and late
normoblasts are present; their numbers depend on the severity of the
disorder. The leucocyte count is variable and there may be an
eosinophilia. Erythrophagocytosis by monocytes may be seen. The
direct Coombs' test is positive.
ABO incompatibility
Mild anaemia may be present. Many spherocytes are seen in the
film. Haemolysis may not be evident and the direct Coombs' test, as
normally carried out, may be negative.
HAEMORRHAGE
The blood film appearance is variable, depending on the type of
haemorrhage — acute or chronic — and on the aetiology. During acute
haemorrhage the red cells are normochromic normocytic and the
absolute reticulocyte count is initially within normal limits. After 24
hours, macrocytes appear and the number of polychromatic cells
increases. An occasional normoblast may be seen. Neutrophilia and
thrombocytosis usually accompany this type of bleeding. The film
appearance may be confused with that of a haemolytic anaemia.
Chronic haemorrhage results in a hypo chromic microcytic anaemia due
to iron loss; a few polychromatic cells are seen but the absolute
230
THE BLOOD FILM IN DISEASE
reticulocyte count is within normal limits. Massive blood transfusion
for severe and prolonged haemorrhage may produce a thrombocytopenia which in turn aggravates the bleeding. Thrombocytopenia
associated with the presence of fragmented red cells, particularly
schistocytes, is suggestive of an acute episode of disseminated
intravascular coagulation.
HEREDITARY ELLIPTOCYTOSIS/HAEMOLYTIC ANAEMIA
The film appearances of hereditary elliptocytosis with and without
haemolytic anaemia have been described in Chapter 11.
HEREDITARY SPHEROCYTOSIS
There is a moderate to a severe haemolytic anaemia. The red cells are
normochromic and show marked anisocytosis. Many spherocytes of
uniform size, round macrocytes and polychromatic cells are present.
Irregular poikilocytes are not prominent but cells with Howell-Jolly
bodies and normoblasts may be seen. In some subjects the anaemia is
mild and only a few spherocytes are observed in the film. In these cases
the diagnosis of hereditary spherocytosis may only be possible by
carrying out the red cell osmotic fragility on a heparinized blood
sample that has been incubated at 37°C for 24 hours.
HIATUS HERNIA
The film appearance is usually that of a hypochromic microcytic
anaemia due to inadequate nutrition and/or gastro-intestinal blood loss.
Megaloblastosis may develop in some patients.
HODGKIN'S DISEASE
The appearance of the blood film is not constant. It varies from patient
to patient and may alter in the same individual as a result of disease
progression or cytotoxic therapy. An anaemia is usually present. The
red cells may be normochromic normocytic, hypochromic microcytic
from iron deficiency or may show the morphological characteristics of
haemolysis. The presence of a neutrophilia is suggestive of active disease
and there may be an associated lymphocytopenia; monocytosis and
eosinophilia may be prominent. Reed-Sternberg cells are rarely found in
the direct blood film and/or films prepared from the buffy coat.
Neutropenia and/or thrombocytopenia may develop as a consequence
of hypersplenism, bone marrow infiltration by lymphomatous tissue,
231
THE PERIPHERAL BLOOD FILM
irradiation or cytotoxic therapy. The leucocyte alkaline phosphatase
(LAP) score is usually elevated during the active phase of the disease
and may be normal during a remission. The PAS score of the
lymphocytes is also elevated. The overall blood picture is modified after
splenectomy that has been carried out for staging of the disease.
IMMUNOGLOBIN HEAVY CHAIN DISEASE
Gamma chain (Fc fragment of IgG) or Franklin's disease
This disease presents as a lymphoma associated with an anomalous
monoclonal gammopathy. The patient is anaemic, lymphocytopenic and
thrombocytopenic. Eosinophilia may be prominent.
Alpha chain disease
This disease is seen principally in Arabs as an abdominal lymphoma
associated with an anomalous monoclonal gammopathy. The blood
picture is predominantly that of a malabsorption syndrome.
Mu chain or IgM monomer disease
Subjects with this disease present as a lymphocytic leukaemia
associated with an anomalous monoclonal gammopathy.
INFECTIONS AND RECOVERY FROM INFECTIONS
Acute bacterial infections
There is usually a neutrophilia with prominent stab cells. Toxic granules
often appear and in some disorders, such as pneumonia, septicaemia
and burns, Dohle bodies may be noticed. At times there may be no
absolute neutrophilia but the toxic changes may still be evident in the
neutrophils. Occasionally there may be a leukaemoid reaction. A mild
anaemia may be associated with the neutrophilic changes, the red cells
in the film being normochromic normocytic or appear hypochromic.
The platelet count varies and may be increased in number. The
leucocyte alkaline phosphatase (LAP) score is usually elevated and the
peroxidase reaction weaker than normal. In chronic granulomatous
disease and its variants, the nitroblue tetrazolium reduction tests reveal
functional abnormalities in the neutrophils.
Recovery from bacterial infection is characterized by disappearance
of the toxic granules, less prominence of the stab cells and a reversion of
the absolute neutrophil count to within normal limits. A monocytosis
and an eosinophilia may become apparent. Persistence of neutrophilia
and/or the leukaemoid picture is suggestive of a continuance of the
infection or may herald the development of pre-leukaemia. Anaemia
either supervenes or becomes more severe in degree due to toxic
232
THE BLOOD FILM IN DISEASE
depression of haemopoietic activity, interference with iron mobilization
from the storage sites and reduced iron absorption in the
gastro-intestinal tract. Factors contributing to this anaemia are loss of
red cells from haemorrhage and/or haemolysis.
Viral infections
In the early stages of some viral infections there may be a
neutrophilia. However, at the time of examination there is usually a
lymphocytotis associated with a mild to moderate neutropenia. The
lymphocytes are commonly of the large variety and show atypical
features in the nuclei and/or cytoplasm. Eosinophils are prominent and
a variable number of plasma cells and/or Turk irritation cells are
present. There may be no anaemia but some virus infections are
complicated by a haemolytic anaemia. Platelets are usually within
normal limits; however, acute thrombocytopenia may supervene and is
clinically suggested by the appearance of petechial haemorrhages and/or
ecchymoses in the patient.
Recovery from virus infection is characterized by an eosinophilia, a
return of the absolute neutrophil and lymphocyte counts to within
normal limits for the subject and a decrease in the number of atypical
lymphocytes in the blood film. Some atypical lymphocytes may persist
and up to 5 per cent may still be observed for some time later.
INFECTIOUS LYMPHOCYTOSIS
There is an absolute lymphocytosis and at times a leukaemoid picture.
Small lymphocytes are prominent and no immature or atypical cells are
seen. There may be an eosinophilia. The red cells and platelets show no
significant abnormality.
INFECTIOUS MONONUCLEOSIS (GLANDULAR FEVER)
The total white cell count is commonly elevated due to an atypical
lymphocytosis and mononucleosis. There is an associated neutropenia;
neutrophil stab cells are increased in number and the pelgeroid anomaly
may be noticed. Eosinophils are not usually obvious. Commonly there
is no anaemia; however, a haemolytic type can occur and is suggested
by polychromatophilia and the presence of a few spherocytes in the
blood film. Platelets are normal in number; occasionally there may be a
thrombocytopenia.
INFECTIVE HEPATITIS
The patient with infective hepatitis often develops a neutropenia. A few
atypical mononuclear cells and atypical lymphocytes are noticed. The
233
THE PERIPHERAL BLOOD FILM
accompanying anaemia is normo chromic normocytic; target cells may
be seen. Occasionally there is morphological evidence of a haemolytic
process. Platelets are normal; there may be a thrombocytopenia.
IONIZING RADIATION
The subject develops a neutropenia with prominence of stab and giant
cells. The absolute lymphocyte count may be reduced. The
lymphocytes in the film may show one or more of the following
cytological abnormalities: (1) lobulation of the nucleus, (2) twinning
deformity of the nucleus, (3) clumping of the nuclear chromatin or
pyknotic degeneration with disintegration of the cytoplasm. Eosinophilia, monocytosis or plasmacytosis may be seen. There may be a
thrombocytopenia and a mild anaemia. If the exposure to the ionizing
radiation has been persistent, the blood picture may become that of a
leukaemia or an aplastic anaemia.
IRON DEFICIENCY
Iron deficiency in adults may result from increased requirements and/or
inadequate iron intake or from chronic haemorrhage. In infants, it may
be due to maternal iron deficiency during pregnancy, premature birth,
an inadequate or unbalanced diet or repeated intercurrent infections.
Three phases — the pre-latent, latent and manifest — may be recognized
in the development of iron deficiency. In the first two phases there is
commonly no anaemia although the iron stores are depleted. The serum
iron concentration is normal in the pre-latent phase and reduced in the
latent phase. The red cells are normochromic normocytic in both
phases. Manifest iron deficiency is associated with a low serum iron
concentration, an elevated total iron-binding capacity, absent iron
stores and a hypochromic microcytic anaemia. Some stainable iron,
however, may still be evident in an occasional reticulo-endothelial cell of
the bone marrow, especially if the patient had, at some previous time,
received iron dextran therapy. This iron is not mobilizable for
haemoglobin synthesis (Henderson and Hillman, 1969). Target cells and
irregular poikilocytes are found in the blood film and occasionally a
late normoblast may be found, particularly in the severe anaemias. The
number of polychromatic cells is within normal limits. The leucocytes
appear normal; in idiopathic pulmonary haemosiderosis an eosinophilia
is present. Platelets are normal and are at the upper limit of normality
or slightly increased in number if the anaemia is the result of chronic
haemorrhage.
Initiation of adequate therapy causes a polychromatophilia
followed by the appearance of normochromic macrocytes. The latter
234
THE BLOOD FILM IN DISEASE
cells gradually increase in number as the polychromasia decreases. The
blood film begins to show anisochromia and dimorphism of the red
cells. With continued effective therapy the hypochromia eventually
disappears and the film reverts to normal.
LEAD POISONING
The red cells are hypochromic and may be normocytic or microcytic.
Irregular poikilocytes and polychromatic cells are present. A variable
number of red cells with punctate basophiliai is usually seen. The
leucocytes and platelets are normal.
LEUKAEMIA
The blood picture of the various types of leukaemia has been described
in Chapter 11. Di Guglielmo's syndrome has also been discussed earlier
in this chapter.
LIPIDOSES (GENETIC)
Batten-Spielmeyer-Vogt disease
This is an autosomal recessive disorder. The blood film shows
vacuolated lymphocytes similar to those seen in Tay-Sachs disease and
abnormal neutrophils with coarse azurophilic granulations similar to
those seen in Morquio's disease (type IV mucopolysaccharidosis).
Gaucher's disease
Gaucher's disease is characterized by the accumulation of ceramide
glucoside, caused by glucocerebrosidase deficiency, in histiocytic cells
of the reticulo-endothelial system. These Gaucher's cells have a foamy
appearance; their morphology has been described in Chapter 9. The
disease may be seen in infants and adults. The peripheral blood shows
an anaemia which may be leuco-erythroblastic. Vacuolation of
lymphocytic cytoplasm is not seen.
Niemann-Pick disease
Niemann-Pick disease is characterized by the accumulation of
sphingomyelin and cholesterol, due to deficiency of a sphingomyelin
cleaving enzyme, in histiocytic cells of the reticulo-endothelial system.
These Niemann-Pick's cells have a foamy appearance; their morphology
has been described in Chapter 9. The disease appears in infants. The
peripheral blood shows an anaemia which may be leuco-erythroblastic.
Vacuolation of lymphocytic cytoplasm is an important diagnostic
feature. In contrast with Tay-Sachs disease, lymphocytic vacuolation is
more prominent in younger infants.
235
THE PERIPHERAL BLOOD FILM
Sea-blue histiocyte syndrome (Primary)
Primary sea-blue histiocyte syndrome is a genetic disorder
characterized by hepatosplenomegaly, frequent lung and eye disorders
and skin pigmentation. Sea-blue histiocytes are found in the bone
marrow, liver, spleen and other organs. The morphology of these cells
has been described in Chapter 9. The peripheral blood shows a
thrombocytopenia and other cytopenias may be seen as a result of
hypersplenism.
Tay-Sachs disease — amaurotit familial idiocy
Infants with Tay-Sachs disease show progressive mental retardation,
blindness, conculsions and a cherry-red spot on the macula of the eyes.
It is an autosomal recessive disorder and is characterized by the
accumulation of gangliosides, due to a deficiency of hexosaminidase A, in
neuronal cells. Vacuolated lymphocytes are present in the peripheral
blood film. However, the number and size of the vacuoles vary with the
duration of the disease; they are larger and more numerous in the older
child.
MALARIA
A varying number of red cells contain malarial parasites; one of the
erythrocytic phases is predominant. Commonly only one species of
parasite is seen; sometimes two species may be recognized in the blood
film. In malignant tertian malaria female (crescent-shaped) gametocytes
of P. falciparum, free of red cells, may be noticed. The morphological
characteristics of the four species of parasites that cause human malaria
have been described in Chapter 4 and summarized in Table 4.10. Parasites may be difficult to detect soon after commencement of antimalarial therapy. The red cells in the blood film are essentially normochromic normocytic. A few polychromatic cells, irregular poikilocyUs
and an occasional spherocyte may be seen. Many fragmented red cells
and a sparse number of platelets are observed in patients exhibiting
signs and symptoms of disseminated intravascular coagulation. The
patient with malaria is often anaemic and this may be more severe than
can be attributed to lysis of parasitized red cells; the mechanisms considered to be responsible for this disproportionate anaemia are controversial (Conrad, 1971). Severe intravascular haemolysis with
haemoglobinuria ('blackwater fever') may occur in malignant tertian (P.
falciparum) malaria.
A monocytosis is usually present and there may be a slight neutrophilia during the paroxysmal stage of the infection. Malarial pigment
236
THE BLOOD FILM IN DISEASE
may be noticed in the PMN and monocytes. The NBT score of the PMN
in the nitroblue tetrazolium reduction test has been shown to be
elevated (Andersen, 1971). Pancytopenia may develop in some patients
with malaria.
MAY-HEGGLIN ANOMALY
The May-Hegglin anomaly is an autosomal dominant disorder
characterized by large basophilic inclusions, resembling (but not
identical with) Dohle bodies in leucocytes (except lymphocytes) and by
platelet abnormalities. The morphology of the affected leucocytes has
been described in Chapter 5. Many platelets in the film are large and
may have abnormal shapes. Ultrastructurally they show no significant
abnormality. Functionally, they have a platelet thromboplastic defect.
In addition, the platelet count is reduced owing to increased peripheral
destruction.
MEGALOBLASTIC ANAEMIA
At the time of diagnosis the severity of the anaemia is variable. The red
cells are normochromic and macro-ovalocytes are obvious in the film.
Severe megaloblastosis may present as a pancytopenia and rarely as a
leuco-erythroblastaemia. In addition to the normochromic macroovalocytes there are marked anisocytosis, microcytosis and irregular
poikilocytosis. Polychromatic cells are not prominent but an occasional
megaloblast may be found in the routine film or in buffy coat films.
Apart from a neutropenia the only other significant abnormality that
may be seen in the neutrophils is nuclear hypersegmentation and/or an
increase in the lobe average. Occasionally the thrombocytopenia in
severe megaloblastosis may cause purpura and a bleeding diathesis. In
subjects with moderate anaemia the anisopoikilocytosis and microcytosis are less striking; hyper segmented neutrophils may not be
observed and the platelets are within normal limits. Megaloblastosis
occasionally develops in patients with polycythaemia; in these cases the
blood haemoglobin concentration lies within normal limits and the
diagnosis may the missed if the blood film is not examined.
MICRO-ANGIOPATHY
The film appearance will range from a mild and chronic to a severe and
acute fragmentation haemolytic anaemia which may be modified by the
occurrence of a haemorrhagic diathesis. The number of schistocytes,
237
THE PERIPHERAL BLOOD FILM
irregular poikilocytes and small spherocytes depends on the severity of
the disorder. The leucocyte picture varies. The platelet count may be
normal or reduced.
MUCOPOLYSACCHARIDOSES (GENETIC)
Hurler-Hunter syndrome (gargoylism)
The Hurler-Hunter syndrome is characterized by disturbances in the
metobolism of chondroitin sulphate B and heparitin sulphate. Physical
development of the child is retarded. Vacuolated lymphocytes and
Alder-Reilly granulation in leucocytic cytoplasm are seen. These
abnormal leucocytes have been described in Chapter 5.
Morquio's syndrome (type IV mucopolysaccharidosis)
Morquio's syndrome is characterized by a disturbance in
keratosulphate metabolism. A large number of neutrophil polymorphs
contain a single or a few small clusters of coarse azurophilic granules
which may be surrounded by a clear halo (Brunning, 1970). No
abnormal granules are observed in eosinophils, basophils, monocytes or
lymphocytes.
MYCOSIS FUNGOIDES
Mycosis fungoides is a lymphomatous disorder that originates in the
skin. In the late stages of the disease and in its erythrodermic form
(Sézary variant) abnormal monocytoid cells (Sézary cells) appear in the
blood in varying numbers. The total white cell count is usually elevated
and there may be an eosinophilia. There may be a mild anaemia with
normochromic normocytic red cells. Platelets are within normal limits.
MYELOMATOSIS
The film appearance varies and is diagnostic only when malignant
plasma cells are found. In many subjects there is striking rouleaux of
red cells and marked elevation of the erythrocyte sedimentation rate
(ESR). The anaemia in myelomatosis varies in type and severity. It may
be due to a multiplicity of factors such as bone marrow replacement by
myelomatous tissue, blood loss from haemorrhage and/or haemolysis,
renal failure, infections and inadequate nutrition. The red cells are
commonly normochromic normocytic. Leucocytes and platelets are
normal or reduced in numbers. The blood picture is occasionally that of
a leuco-erythroblastic anaemia. On occasions it may appear megaloblastic. A few plasma cells, which may not appear atypical, are
238
THE BLOOD FILM IN DISEASE
commonly seen if the film is carefully scrutinized. Plasma cell
leukaemia, which represents a displacement phenomenon is present if
the number of plasma cells in the film is elevated; approximately 20 per
cent of the leucocytes may belong to the plasma cell series.
NUTRITIONAL ANAEMIA
The film appearance is commonly that of an iron deficiency anaemia.
The picture may be modified because of associated protein deficiency
or avitaminosis.
PAROXYSMAL NOCTURNAL HAEMOGLOBINURIA
This acquired haemolytic anaemia is found in adults. The blood picture
may be that of an acute haemolytic anaemia with macrocytosis and
increased polychromasia, iron deficiency due to iron sequestration in
the kidneys or a pancytopenia. Spherocytes are not usually observed in
the blood film. A positive direct Coombs' test may be obtained during a
paroxysm of haemolysis. Thrombocytopenia commonly occurs in the
disorder and may be due to disseminated intravascular coagulation. The
leucocyte alkaline phosphatase (LAP) score is reduced.
PELGER-HUËT ANOMALY
The Pelger-Huët anomaly is an autosomal dominant abnormality of
leucocytes characterized by incomplete segmentation of granulocytic
nuclei. The affected number of cells varies from case to case. Nuclear
abnormalities may be noted in monocytes and lymphocytes. The
morphology of affected cells has been described in Chapter 5. This
hereditary disorder should not be confused with the acquired pelgeroid
anomaly seen in certain diseases and disorders (see Table 5.2).
POLYCYTHAEMIA
Polycythaemia rubra vera (PRV)
The red cells are normochromic normocytic and may appear
macrocytic. They are crowded together even in the area of ideal film
thickness and the spaces between the cells are reduced. A moderate
number of polychromatic cells are present: an occasional normoblast
may be found. The leucocytes show a neutrophilia; metamyelocytes
and band forms are evident. Eosinophils and basophils may be
prominent. Distortion of leucocyte morphology is often seen because
of red cell crowding. There is a thrombocytosis and bizarrely shaped
239
THE PERIPHERAL BLOOD FILM
platelets may be noticed. The peroxidase reaction in the neutrophils
may be reduced while the leucocyte alkaline phosphatase (LAP) score is
elevated. The blood picture is modified by repeated phlebotomies and
therapy. The haemoglobin concentration falls to within normal limits and
the red cells become hypochromic. If megaloblastosis supervenes
macro-ovalocytes appear in the blood film.
Secondary polycythaemia or erythrocytosis
The film appearance of the red cells is similar to that described
above. However, there is no neutrophilia, eosinophilia, basophilia or
thrombocytosis unless there are complications of the primary disorder
causing the erythrocytosis.
POST-GASTRECTOMY SYNDROME
The film appearance is commonly that of an iron deficiency anaemia
due to loss of acid-secreting musoca, villous atrophy of the small
intestine mucosa and intestinal hurry (dumping syndrome). This picture
may be modified in some patients by the presence of an overt or
manifest vitamin B 1 2 and/or folate deficiency. Leucocytes show no
abnormality except a possible hypersegmented neutrophil. Platelets are
normal.
PREGNANCY
The red cells are normochromic normcytic and there may be no
anaemia. Often, however, a physiological anaemia develops when the
increase in plasma volume is greater than the increase in the red cell
mass which normally occurs in pregnancy. Iron deficiency anaemia
commonly occurs and is caused by one or more of the following
factors: depletion or exhaustion of iron stored in the body prior to the
onset of the pregnancy, inadequate iron intake, malabsorption or
increased iron requirements. Folate deficiency sometimes arises and
macro-ovalocytes appear in the film. The erythrocyte sedimentation
rate (ESR) increases as pregnancy advances. The total white cell count
is normally elevated because of a neutrophilia; metamyelocytes and
stab cells become prominent and a few myelocytes are also seen.
Platelets are usually within normal limits but may be moderately
increased in numbers.
PRE-LEUKAEMIA
Pre-laeukaemia is a term applied to haematological abnormalities that
may be interpreted as a prelude to the development of frank myeloid
240
THE BLOOD FILM IN DISEASE
leukaemia. The patient may have a moderate to a severe refractory
anaemia associated with either a reticulocytopenia or haemolysis. Red
cell anisopoikilocytosis becomes prominent as the disorder progresses and
abnormal cells become apparent. There may be a neutropenia or a
neutrophilia which at times is leukaemoid. The pelgeroid anomaly or
hyper segmented neutrophils may be found in the film. Often there is a
monocytosis. Thrombocytopenia associated with the presence of
bizarrely shaped platelets is seen. The patients may exhibit an unusual
bleeding diathesis. In the bone marrow, the haemopoietic tissue is
hypercellular and there is an increase in the number of myeloblasts
and/or promyelocytes.
PYRUVATE KINASE DEFICIENCY
A haemolytic anaemia is usually present. The blood film contains
normochromic red cells, macrocytes, fragmented cells and a variable
number of polychromatic cells. Spherocytes are rarely seen. Leucocytes
and platelets show no significant abnormality.
RENAL FAILURE
The patient is anaemic; the blood haemoglobin concentration is lower
in those with blood urea nitrogen levels higher than 100 mg per cent.
The pathogenesis of the anaemia is complex. There may be
erythropoietic depression because of reduced erythropoietin levels,
infection and increase in circulating toxic products. The anaemia may
be aggravated by haemorrhage resulting from thrombocytopenia and/or
platelet dysfunction. Blood loss may occur from micro-angiopathic
haemolysis. In the film there is rouleaux of red cells which are
essentially normochromic normocytic but show moderate anisocytosis.
There may be no polychromatophilia but burr cells and schistocytes are
prominent, particularly in the later stages of renal failure. The
appearances of the leucocytes vary. There may be a neutrophilia as a
result of infection. Hypersegmentation of neutrophil polymorphs, not
related to vitamin B 1 2 ° r folate deficiency, may be seen. Platelets are
usually normal. However, thrombocytopenia may develop as a result of
hypersplenism, disseminated intravascular coagulation or dialysis
procedures.
RUBELLA
The blood picture is that of a neutropenia with prominent monocytes,
some of which may be bi-lobed, and a plasmacytosis. In the later stages
of the infection, the plasma cells are replaced by large mononuclear
241
THE PERIPHERAL BLOOD FILM
cells that have an eccentric oval-shaped nucleus with a nucleolus and a
pale light blue cytoplasm containing vacuoles and azurophilic granules.
Platelets may be reduced in numbers.
SCARLET FEVER
There is a neutrophilia with prominent band forms and a few
myelocytes. An eosinophilia occurs during the first week of the illness
and the neutrophils revert to normal limits by the end of the second
week. Platelets are within normal limits. There is no anaemia unless
nephritis develops as a complication of the infection.
SIDEROBLASTIC ANAEMIA
Sideroblastic anaemia is characterized by the dimorphic appearance of
the red cells in the film. Normochromic mildly macrocytic cells may be
prominent in the acquired primary disease and hypochromic microcytes
in the hereditary disease. The MCHC is normal or slightly reduced. A
few target cells are present and poikilocytosis may be marked.
Siderocytes are not prominent because of intramedullary haemolysis
and/or splenic destruction. There is a reticulocytopenia but an
occasional nucleated red cell may be found. Detection of pathological
sideroblasts, particularly the ring sideroblast, is a sine qua non for the
diagnosis of sideroblastic anaemia. The total white cell count is normal;
any reduction is due to a neutropenia. Lymphocytes, monocytes and
platelets show no significant abnormality. The leucocyte alkaline
phosphatase (LAP) score is reduced in many cases. Sideroblastic
anaemia may be complicated by megaloblastosis or a pancytopenia. The
disease may terminate as a myeloblastic leukaemia.
SPLENIC DISORDERS
Splenomegaly
The film appearance is that of the disorder (see Table 12.49) causing
the splenomegaly. It may be modified by hypersplenism.
Hypersplenism
One or more cytopenias, not due to the primary disorder, are seen
in the blood film. The corresponding immature cells in the bone
marrow are hyperplastic.
Post-splenectomy syndrome
Target cells and irregular poikilocytes are numerous and cells with
Howell-Jolly bodies and Pappenheimer bodies are present. There is
242
THE BLOOD FILM IN DISEASE
some polychromasia and an occasional nucleated red cell may be found.
The number of platelets and leucocytes is increased. Eosinophils and
basophils may be prominent. The blood picture of the primary disorder
may still be evident in the post-splenectomy blood film.
THROMBOCYTHAEMIA (ESSENTIAL OR HAEMORRHAGIC)
Essential (or haemorrhagic) thrombocythaemia is a myeloproliferative
disorder with platelet counts that are persistently greater than 750,000
per microlitre and may be greater than one million per microlitre. Giant
and bizarre forms of platelets are seen in the film and large masses of
clumped platelets are a striking feature. Neutrophilia and an associated
eosinophilia are usually present; immature granulocytes may be
identified but they are not prominent. The leucocyte alkaline
phosphatase (LAP) score is higher than normal. The red cell picture is
variable. There may be an erythrocytosis with some normoblastaemia
or the film may show a chronic haemorrhagic anaemia with
hypochromic red cells, poikilocytes and polychromatophilia.
THYROID DISORDERS
Hyperthyroidism or Grave's disease
The red cells show mild hypochromia. A macro-ovalocytic anaemia may
develop. Neutropenia and thrombocytopenia may result from
therapeutic measures.
Hypothyroidism or myxoedema
There is a mild to moderate anaemia that is usually normochromic
normocytic. Nutritional deficiencies often complicate the picture;
gastric achylia is frequently associated with myxoedema. Hypochromic
microcytic anaemia due to iron deficiency or macro-ovalocytic anaemia
due to vitamin B 1 2 deficiency may appear. According to Wardrop and
Hutchison (1969), irregular poikilocytes similar to burr cells are
present in small numbers in the films of about two-thirds of patients
with untreated hypothyroidism and are of diagnostic value. These cells
slowly disappear with therapy. Leucocytes and platelets are normal in
the film.
TUBERCULOSIS
There is no specific blood picture. The red cells may be normochromic
normocytic or hypochromic microcytic. In miliary tuberculosis there
may be a leukaemoid reaction or leuco-erythroblastaemia. Pulmonary
fibrosis resulting from the tuberculosis may cause a secondary
polycythaemia. Treatment with drugs such as cycloserine and isoniazid
243
THE PERIPHERAL BLOOD FILM
may be responsible for the development of a sideroblastic anaemia. The
red cells will then appear dimorphic and ring sideroblasts are recognized
in films of the bone marrow.
UNDULANT FEVER
There is a moderate hypochromic microcytic anaemia and a variable
white cell count. Often there is a neutropenia associated with a
moderate lymphocytosis and sometimes a monocytosis. Platelets are
normal.
VITAMIN DEFICIENCIES
Vitamin Bx (thiamine,aneurine) deficiency
Thiamine deficiency does not normally produce any direct
haematological defect. However, a case of thiamine-responsive
megaloblastic anaemia was reported by Rogers, Porter and Sidbury
(1969). The patient was a diabetic child aged 3 years who developed a
severe macrocytic anaemia with megaloblastosis in the bone marrow.
The anaemia was refractory to vitamin B 1 2 , folate and pyridoxine
therapy but was corrected by pharmacological doses of thiamine. The
child exhibited no clinical signs or symptoms of beriberi. Further, the
blood thiamine levels, the thiamine-dependent enzymes and the
erythrocyte transketolase activity were normal.
Vitamin B2 (Riboflavin) deficiency
Pure red cell aplasia with a reticulocytopenia appeared in humans
given riboflavin antagonists and fed on a riboflavin- deficient diet. The
leucocytes and platelets were unaffected (Lane and Alfrey, 1965).
Vitamin B6 (Pyridoxine) deficiency
Pyridoxine deficiency may occur as part of a generalized
malnutrition and avitaminosis in alcoholics, in the malabsorption
syndrome, in pregnancy and in infants and it may result from
anti-tuberculous therapy with cycloserine, pyrazinamide and isoniazid,
which are pyridoxine antagonists. In infants the anaemia may be
hypochromic microcytic, while in adults it is usually dimorphic in type.
Some macro-ovalocytes due to megaloblastosis may occur. The
leucocytes vary in number. Although some sideroblastic anaemias
respond to pharmacological doses of the vitamin, a deficiency state has
not been established.
Nicotinic (niacin) deficiency
The anaemia of pellagra is commonly due to iron, vitamin B 1 2 or
folate deficiency.
244
THE BLOOD FILM IN DISEASE
Vitamin B 1 2 (cobalamins) deficiency
The blood picture is that of a megaloblastic anaemia.
Folate deficiency
The blood picture is that of a megaloblastic anaemia.
Vitamin C (ascorbic acid) deficiency
In adults there is a moderate anaemia which is essentially
normochromic normocytic and results from erythropoietic depression.
A haemolytic process may occur and polychromasia is seen in the blood
film. In infants the anaemia may be hypochromic microcytic because of
iron defiency and/or haemorrhage resulting from increased vascular
permeability and thrombopathy. Vitamin C deficiency may play a role in
the development of megaloblastosis, particularly in children. Leucocytes and platelets are morphologically normal.
WHOOPING COUGH
During the paroxysmal stage of whooping cough there is a
lymphocytosis which may at times be leukaemoid. Many atypical
lymphocytes with bizarrely shaped nuclei are present in the film. The
red cells and platelets usually show no significant abnormality.
245
Appendix A
ROMANOVSKY, CYTOCHEMICAL AND SUPRA-VITAL STAINING
TECHNIQUES
JENNER-GIEMSA STAINING
(PAPPENHEIM'S PANOPTIC METHOD)
Reagents
Jenner's stain
Add 0.5 g of powdered dye to 100 ml of acetone-free methanol in a
conical flask and reflux the mixture for at least one hour. Store the
solution in glass-stoppered bottles. Filter before use.
Giemsa's stain
Add 1 g of powdered dye to 66 ml of glycerol and heat to 50°C for
2 hours; add 66 ml of methanol and after thorough mixing store at
room temperature for at least 7 days before use.
Working Giemsa solution: Prepare a 20% solution by diluting the
stock dye solution with buffered water (pH 6.4). This must be freshly
prepared.
Buffered water (pH 6.4)
Stock solution A: Dissolve 9.1 g of potassium dihydrogen phosphate
in 1 litre of deionized water.
Stock solution B: Dissolve 9.5 g of anhydrous disodium hydrogen
phosphate in 1 litre of deionized water.
Working buffered waters: Mix solutions A and B in the amounts
indicated to obtain the required pH.
pH
5.4
5.6
5.8
6.0
246
Soin. A, ml
97.0
95.0
92.2
88.0
Soin. B, ml
3.0
5.0
7.8
12.0
APPENDIX A
Soin. A, ml
pH
Soin. B, ml
6.2
81.0
6.4
73.0
6.6
63.0
6.8
50.8
7.0
38.9
7.2
28.0
7.4
19.2
7.6
13.0
7.8
8.5
8.0
5.5
Commercial buffer tablets may be used. They are
recommended volume of deionized water.
Method
Place slide, film uppermost, on staining rack
Pour 2.5 - 3 ml Jenner's stain
Add 2.5 - 3 ml buffered water, pH 6.4, mix
Pour off diluted Jenner's stain
Flood slide with 20% Giemsa's stain
Rinse in tap water
Flood slide with buffered water, pH 6.4
Pour off buffered water, dry in air or blot dry
19.0
27.0
37.0
49.2
61.1
72.0
80.8
87.0
91.5
94.5
dissolved in the
2 min
4 min
9 min
Vi min
MAY-GRÜNWALD-GIEMSA STAINING
Reagents
May-Grunwald's stain
Prepare in a similar manner to Jenner's stain, but use 0.3 g of the
powdered May-Grünwald dye.
Giemsa's stain and working Giemsa solution
See Jenner-Giemsa staining.
Buffered water (pH 6.8)
See Jenner-Giemsa staining.
Method
As for Jenner-Giemsa staining.
LEISHMAN STAINING
Reagents
Leishman 's stain
Add 0.2 g of powdered Irishman's stain to a conical flask containing
100 ml of methanol and warm to 50°C for 15 minutes with occasional
247
THE PERIPHERAL BLOOD FILM
shaking or grind the powdered stain in a mortar with successive
amounts of methanol until it is dissolved in the appropriate quantity of
alcohol. The stain solution improves with standing and must be filtered
before use.
Buffered water (pH 6.8)
See Jenner-Giemsa staining.
Method
Place slide, film uppermost, on the staining rack
Pour 2.5 - 3 ml Irishman's stain
Add 2.5 - 3 ml buffered water, pH 6.8, mix . . . .
Pour off diluted Irishman's stain
Rinse in tap water
Flood slide with buffered water, pH 6.8
Pour off buffered water, dry in air or blot dry
1 min
10-15 min
. . . . Vi min
WRIGHT STAINING
Reagents
Wright's stain
Add 3 g of dry powdered stain and 30 ml of glycerine to a mortar. Mix
by grinding. Incubate at 37°C for a few days, stirring a few times each
day. Then add 1 litre of acetone-free methanol with constant stirring.
Store at room temperature for 2 4 weeks. Filter before use.
Buffered water (pH 6.6)
See Jenner-Giemsa staining.
Method
Place slide, film uppermost, on the staining rack
Pour 2.5 - 3 ml of Wright's stain
Add 2.5 - 3 ml of buffered water, pH 6.6, mix
Pour off diluted Wright's stain
Rinse in tap water
Flood slide with buffered water, pH 6.6
Pour off buffered water, dry in air or blot dry
STAINING FOR MALARIAL PARASITES
THIN BLOOD FILMS
DILUTE GIEMSA TECHNIQUE
Reagents
Fixative
Methanol.
248
1 min
2 - 4 min
Vi min
APPENDIX A
Giemsa 's stain
Stock solution: See Jenner-Giemsa staining.
Working Giemsa solution: Prepare a fresh 10% solution by diluting
the stock dye solution with buffered water (pH 7.2).
Buffered water (pH 7.2)
See Jenner-Giemsa staining.
Sodium chloride solution 0.9%
Method
Place slide, film uppermost, on the staining rack
Flood the slide with methanol
Pour off methanol and allow the film to air dry
Pour on working Giemsa solution
Pour off stain and rinse in buffered water, pH 7.2
Rinse in sodium chloride solution
Place slide upright to dry
%min
30 min
ACRIDINE ORANGE FLUORESCENT TECHNIQUE
(Richards, Hunter and Janis, 1969)
Reagents
Fixative
Mix equal volumes of ether and methanol.
Acridine orange solution
Stock solution: Dissolve 100 mg of powdered dye in 100 ml of
deionized water.
Working solution: Prepare a fresh 1 in 100,000 dilution by adding 1
volume of the stock solution to 99 volumes of buffered water (pH 6.4).
Buffered water (pH 6.4)
See Jenner-Giemsa staining.
Gearing solution
M/15 calcium chloride solution: Dissolve 16.5 g of calcium chloride
in 1 litre of deionized water.
Alcohols
80%, 70%, 50%.
Method
Place slide, film uppermost, on the staining rack
Flood the slide with the fixative solution
Pour off the fixative; add 80% alcohol
Pour off 80% alcohol; add 70% alcohol
15 min
&min
VA min
249
THE PERIPHERAL BLOOD FILM
Pour off 70% alcohol; add 50% alcohol
Pour off 50% alcohol; add buffered water, pH 6.4
Rinse the slide in fresh buffered water, pH 6.4
Flood the film with working stain solution
Pour off stain solution; add buffered water, pH 6.4
Pour off buffered water; add clearing solution
Pour off clearing solution
Place the slide upright and allow to dry. DO NOT BLOT
VA min
Vi min
Vi min
% min
3 min
3 min
Reaction
Examine microscopically with ultraviolet light. Malarial parasites
fluoresce a vivid red colour. Mature red cells show no fluorescence.
Leucocytes fluoresce green.
THICK BLOOD FILMS
DILUTE GIEMSA TECHNIQUE
Reagents
Giemsa 's stain
Stock solution: See Jenner-Giemsa staining.
Working Giemsa solution: Prepare a fresh 5% solution by diluting
the filtered stock solution with buffered water (pH 7.2).
Buffered water (pH 7.2)
See Jenner-Giemsa staining
Sodium chloride solution 0.9%
Method
Pour working Giemsa solution into Coplin jar
Immerse the slide containing the unfixed thick blood
film into the solution
Remove the slide
Rinse in buffered water, pH 7.2
Rinse in the sodium chloride solution
Place the slide upright and allow to dry. DO NOT BLOT
30 min
FIELD'S TECHNIQUE (1940, 1941)
Reagents
Stain A - poly chromed méthylène blue solution
Method 1: Dissolve 5.0 g of anhydrous disodium hydrogen
phosphate and 6.25 g of anhydrous potassium dihydrogen phosphate in
500 ml deionized water. Place 0.8 g of méthylène blue and 0.5 g of
250
APPENDIX A
Azur I in a mortar and grind with successive small quantities of the
buffered water until the dyes are completely dissolved in the total
volume of 500 ml. Allow the stain to stand at room temperature for 24
hours, filter and store.
Method 2: Dissolve 1.3 g of méthylène blue and 12.6 g of hydrated
disodium hydrogen phosphate in 50 ml of deionized water. Evaporate
almost to dryness in a boiling water bath. Add 500 ml of freshly boiled
deionized water containing 6.25 g of anhydrous potassium dihydrogen
phosphate. Stir until solution is complete. Allow the stain to stand at
room temperature for 24 hours. Filter and store.
Stain B - eosin solution
Dissolve 5 g of anhydrous or 12.6 g of hydrated disodium hydrogen
phosphate and 6.25 g of anhydrous potassium dihydrogen phosphate in
boiling deionized water and then 1.3 g of water-soluble eosin. When
solution is complete, allow the stain to stand at room temperature for
24 hours. Filter and store.
Buffered water (pH 6.8)
See Jenner-Giemsa staining.
Method
Filter each stain into separate Coplin jars
Immerse the slide containing the unfixed thick
blood film into Stain A
(up to 10 sec if patient is severely anaemic)
Rinse in buffered water, pH 6.8
Immerse the slide into Stain B
Rinse in buffered water, pH 6.8
Shake off excess water
Place slide upright and allow to dry. DO NOT BLOT
1 - 3 sec
. 10 sec
I - 3 sec
. 10 sec
FEULGEN REACTION
Reagents
Fixative
Methanol, 15 parts; 5% acetic acid, 5 parts; 40% solution of
formaldehyde, 1 part; and water, 5 parts.
N hydrochloric acid
Schiffs reagent or leucobasic fuchsin
Method 1: Decolorize 0.5% solution of basic fuchsin by bubbling
sulphur dioxide through it for one hour; if not completely decolorized,
add activated charcoal (1 g per 100 ml), shake and then filter.
251
THE PERIPHERAL BLOOD FILM
Method 2: Add 1 g of basic fuchsin to 400 ml of boiling deionized
water; cool the solution to 50°C and filter. Add 1 ml of thionyl
chloride to the filtrate and store in the dark for 12 hours. Add 2 g of
activated charcoal to the solution, shake and filter. Store the final
solution in the dark at 0-4°C in an amber bottle.
Sulphite solution
Method 1: Bubble sulphur dioxide through water until it is
saturated.
Method 2: Mix N/l hydrochloric acid, 1 part; 10% sodium
metabisulphite, 1 part; and distilled water, 9 parts.
Jenner's stain solution
See Jenner-Giemsa staining.
Method
Fix the air-dried blood film in the fixative solution
Wash in tap water
Wash in deionized water
Immerse in N/1 HC1 at room temperature
Immerse in N/1 HC1 at 60°C
Rinse in N/1 HC1 at room temperature
Immerse in Schiffs reagent
Rinse in 3 changes of sulphite solution
Wash in tap water
Counterstain with Jenner's stain or dehydrate
Clear and mount
. . . 10 min
10-20 min
. . . . 2 min
. . . . 2 min
8-10 min
1-2 hours
, 2 min each
10-15 min
Reaction
Nuclear chromatin is magenta coloured. Nucleoli do not stain and
appear as holes surrounded by a ring of stained chromatin. The
intensity of the reaction increases with cell maturity. Howell-Jolly
bodies stain a magenta colour.
GREIG'S SUBSTITUTE FEULGEN REACTION (1959)
Reagents
Fixative solution
Formaldehyde solution (40%), 10 parts; methanol, 90 parts.
N/l hydrochloric acid
Romanovsky stain
Dilute a Romanovsky stain 1 in 10 with buffered water, pH 6.8.
Buffered water (pH 6.8)
See Jenner-Giemsa staining.
252
APPENDIX A
Method
Fix the air-dried blood film in the fixative solution
3 min
Rinse in deionized water
Immerse in N/1 HC1 at 56° C
15 min
Rinse in deionized water
Immerse in dilute Romanovsky stain solution
1 min
Rinse in deionized water, dry in air and mount
Reaction
Chromatin and chromosomes stain shades of deep blue-black.
Nucleoli do not stain and appear as holes surrounded by a ring of
stained chromatin. The cytoplasm of cells does not usually stain but
eosinophil and azurophil granules stain.
PERIODIC ACID-SCHIFF (PAS) REACTION
Reagents
Fixative
Methanol
Periodic acid
Dissolve 1 g of periodic acid in 100 ml deionized water.
Schiffs reagent or leucobasic fuchsin
See Feulgen reaction.
Sulphite solution
See Feulgen reaction.
Haematoxylin solution
Dissolve 2 g of haematoxylin in 100 ml deionized water.
Scott's tap water substitute
Dissolve 3.5 g of sodium bicarbonate and 20 g of magnesium
sulphate in 1 litre tap water.
Method
Fix the air-dried blood film in methanol
Dry in air
Flood slide with periodic acid solution
Wash in running tap water
Flood slide with Schiffs reagent
Rinse in 3 changes of sulphite solution
Wash in running tap water
Flood slide with haematoxylin solution
Pour off haematoxylin
Blue in Scott's tap water substitute
Wash in tap water and dry in air
10 min
10 min
30 min
2 min each
4 min
253
THE PERIPHERAL BLOOD FILM
Reaction (cf. Tables 2.2 and 8.1)
A positive reaction is indicated by the presence of diffuse magenta
coloration of the cytoplasm or the presence of magenta-coloured
granules or blocks in the cytoplasm.
Semi-quantitative rating of PAS activity in cells
The PAS activity in each cell may be semi-quantitatively rated as
indicated below. The sum of the ratings of 100 consecutive cells of a
series is the 'score'. This technique of assessing the PAS activity is
particularly applied to the lymphocytes and lymphoblasts.
0 — Cells without PAS-positive granules
1 — Cells with scattered PAS-positive granules or with one annular
ring of granules
2 — Cell with two concentric annular rings of PAS-positive granules
3 — Cell with three or more concentric annular rings of PAS-positive
granules and cells with blocks of PAS-positive material
PRUSSIAN BLUE REACTION
Reagents
Potassium ferrocyanide solution
Dissolve 2 g of potassium ferrocyanide in 100 ml of de ionized water.
Hydrochloric acid 2% (by volume)
Working solution
Mix equal volumes of potassium ferrocyanide and hydrochloric acid
solutions immediately before use and filter into a Coplin jar.
Eosin solution
Dissolve 0.1 g of eosin in 100 ml deionized water.
Method
Fix the air-dried blood film in methanol .
Dry in air
Immerse slide in working solution at 56°C
Wash in running tap water
Rinse in hydrochloric acid solution
Wash in running tap water
Counterstain with eosin solution
Wash in deionized water and dry in air
10 min
10 min
%min
Reaction
Free iron granules stain a Prussian blue colour.
Note
Prussian blue staining can be carried out on Romanovsky-stained
254
APPENDIX A
blood films. However, to demonstrate the presence of sideroblasts in
the blood film, it is advisable to decolorize the film first by immersing
the slide in a Coplin jar containing methanol.
PEROXIDASE REACTION
GRAHAM-KNOLL TECHNIQUE
Reagents
Fixative solution
Ethanol.
Benzidine or o-tolidine
Hydrogen peroxide (20 volumes)
Reaction mixture
Prepare a fresh saturated solution of benzidine or o-tolidine by
adding a knife-point of the chemical to 6 ml of ethanol. Make up the
solution to 10 ml with deionized water and add 0.02 ml of the
hydrogen peroxide.
Giemsa's stain
Stock solution: See Jenner-Giemsa staining.
Working solution: Prepare a 20% solution by diluting the stock
solution.
Method
Fix the air-dried blood film in ethanol
Rinse in tap water
Flood the slide with the reaction mixture
Rinse in tap water
Flood the slide with working Giemsa solution
Wash in tap water and dry in air
1 min
5 min
5 min
Reaction (cf. Tables 3.4, 8.1 and 8.4)
Peroxidase activity is indicated by the presence of brownish-green
granules in the cytoplasm of the cells.
MODIFIED WASHBURN'S (1928) TECHNIQUE
Reagents
Fixative
Ethanol.
Benzidine or o-tolidine
Sodium nitroprusside solution
Prepare a saturated (36%) solution in deionized water.
255
THE PERIPHERAL BLOOD FILM
Hydrogen peroxide (20 volumes)
Solution A
Dissolve 0.3 g of benzidine or o-tolidine in 99 ml of ethanol and to it
add 1 ml of saturated sodium nitroprusside solution.
Solution B
Add 6 drops of hydrogen peroxide to 25 ml deionized water.
Romanovsky stain(s)
Method
Place slide, film uppermost, on staining rack
Add 10 drops of solution A to the film
Add 2 drops of solution B to solution A and mix
Wash thoroughly in tap water and air dry
Carry out Romanovsky staining of the film
l^min
4% min
Reaction (cf. Tables 3.4, 8.1 and 8.4)
Peroxidase activity is indicated by the presence of blue-black
granules in the cytoplasm of the cells. In some cells the intensity of the
reaction may be so great that the nucleus is obscured by the granules.
NAPHTHOL AS-D CHLOROACETATE ESTERASE REACTION
(Yam, Li and Crosby, 1971)
Reagents
Fixative solution
Dissolve 20 mg of disodium hydrogen phosphate and 100 mg of
potassium dihydrogen phosphate in 30 ml of deionized water. Add
acetone, 45 ml and formalin, 25 ml. Mix and store at 4-10°C.
Buffered water (pH 7.6)
See Jenner-Giemsa staining.
Sodium citrate solution
Dissolve 4 g of sodium citrate in 100 ml deionized water. Prepare
fresh every week and store at 0-4° C.
Hexazotized new fuchsin solution
Dissolve 1 g of new fuchsin in 25 ml of 2N hydrochloric acid. Mix an
equal volume of this solution and fresh 4% sodium citrate solution just
before use.
Naphthol AS-D chloroacetate solution
Prepare a 2 mg/ml solution of naphthol AS-D chloroacetate in N-N
dimethyl formamide.
256
APPENDIX A
Working reaction mixture
Mix hexazotized new fuchsin solution, 0.05 ml; naphthol AS-D
chloroacetate solution 0.5 ml; and buffered water (pH 7.6), 9.5 ml.
Incubate at room temperature for 10 minutes before use. Do not filter.
Buffered methyl green solution
Prepare a 1% methyl green solution and buffer it to pH 4.2 with
N/10 sodium acetate.
Method
Place slide, film uppermost, on staining rack
Pour on cold fixative solution
Wash thoroughly in deionized water
Air dry
Pour on working reaction mixture
Wash with tap water
Counterstain with methyl green solution ..
Wash with tap water
Air dry and mount
...
VL
min
10 - 30 min
. . . 10 min
. . 1 - 2 min
Reaction (cf. Tables 2.4,3.4,8.1 and 8.4)
Naphthol AS-D chloroacetate esterase activity is indicated by the
presence of bright red granules in the cytoplasm of the cells.
ALPHA-NAPHTHYL ACETATE ESTERASE REACTION
(Yam, Li and Crosby, 1971)
Reagents
Fixative solution
See Naphthol AS-D chloroacetate esterase reaction.
Buffered water (pH 7.6)
See Jenner-Giesma staining.
Sodium citrate solution
See Naphthol AS-D chloroacetate esterase reaction.
Hexazotized pararosanilin solution (Barka and Anderson, 1962)
With gentle warming dissolve 1 g of pararosanilin hydrochloride in
20 ml deionized water and 5 ml concentrated hydrochloric acid. Filter
after cooling and store at room temperature. Mix an equal volume of
this solution and fresh 4% sodium citrate solution just before use.
Alpha-naphthyl acetate solution
Prepare a 20 mg/ml solution of alpha-naphthyl acetate in ethylene
glycol monoethyl ether.
257
THE PERIPHERAL BLOOD FILM
Working reaction mixture
Mix hexazotized pararosanilin solution, 0.6 ml; alphanaphthyl
acetate solution, 0.5 ml; and buffered water (pH 7.6), 8.9 ml. Adjust
pH to 6.1 with N/l NaOH. Filter before use.
Buffered methyl green solution
See Naphthol AS-D chloroacetate esterase reaction.
Method
Place slide, film uppermost, on staining rack
Pour on cold fixative solution
Wash thoroughly in deionized water
Air dry
Pour on working reaction mixture
Wash with tap water
Counterstain with methyl green solution
Wash with tap water
Air dry and mount
l
A min
10-30 min
45 min
1-2 min
Reaction (cf. Tables 2.4, 3.4,8.1 and 8.4)
Alpha-naphthyl acetate esterase activity is indicated by the presence
of dark red granules in the cytoplasm of the cells.
COMBINED ESTERASE REACTION
(Yam, Li and Crosby, 1971)
Reagents
Fixative solution
See Naphthol AS-D chloroacetate esterase reaction.
Buffered water (pH 7.4)
See Jenner-Giemsa staining.
Naphthol AS-D chloroacetate solution
See Naphthol AS-D chloroacetate esterase reaction.
Working fast blue-chloroacetate reaction mixture
Add 0.5 ml of naphthol AS-D chloroacetate solution to 9.5 ml of
buffered water (pH 7.4) and dissolve 5 mg of fast blue BBN in the
mixture. Filter before use.
Workingpararosanilin-alpha-naphthyl acetate reaction mixture
See Alpha-naphthyl acetate reaction mixture.
Buffered methyl green solution
See Naphthol AS-D chloroacetate esterase reaction.
258
APPENDIX A
Method
Place slide, film uppermost, on staining rack
Pour on cold fixative solution
Wash thoroughly in deionized water
Air dry
Pour on pararosanilin-acetate reaction mixture .
Wash thoroughly with tap water
Pour on fast blue-chloroacetate reaction mixture
Wash with tap water
Counterstain with methyl green solution
Wash with tap water
Air dry and mount
. . . . lA min
10 - 30 min
. . . . 45 min
. . . . 10 min
. 1 - 2 min
Reaction
Blue granules are present in granulocytes. Dark red granules are seen
in monocytes.
BROMOINDOXYL ACETATE ESTERASE REACTION
(Pearson and Defendi, 1957)
Reagents
Fixative solution
Cold (4°C) formaldehyde solution.
Potassium ferricyanide solution (0.05M)
Dissolve 1.6 g of potassium ferricyanide in 100 ml of deionized
water.
Potassium ferricyanide solution (0.05M)
Dissolve 2.1 g of potassium ferrocyanide in 100 ml of deionized
water.
Acetate buffer (0. IM, pH 4.8)
Acetic acid solution: Add 1.13 ml of glacial acetic acid to 50 ml
deionized water and make up to 100 ml with water.
Sodium acetate solution: Dissolve 1.64 g of anhydrous sodium
acetate in 100 ml deionized water.
Working buffer solution (pH 4.8): Mix 20 ml of diluted acetic acid
solution and 30 ml of sodium acetate solution. Adjust the pH to 4.8
and make up to 200 ml with deionized water.
5-Bromoindoxyl acetate solution
Dissolve 0.5 g of 5-bromoindoxyl acetate in 100 ml ethanol.
Working reaction mixture
Mix potassium ferricyanide solution, 5 ml; potassium ferrocyanide
259
THE PERIPHERAL BLOOD FILM
solution, 5 ml; 5-bromoindoxyl acetate solution, 2 ml; and working
acetate buffer solution, 15 ml.
Method
Fix the film in cold formalin vapour . ,
Wash thoroughly in deionized water
Incubate the smear at 25°C in working
reaction mixture
Wash thoroughly, air dry and mount
.4 min
20 min
Reaction
Slight to moderate number of deep blue-coloured granules in normal
plasma cells. Numerous deep blue-coloured granules in malignant
plasma cells. Large aggregates may be seen in some cells.
ALKALINE PHOSPHATASE REACTION
ALPHA-NAPHTHYL PHOSPHATE TECHNIQUE
(Hayhoe and Quaglino, 1958)
Reagents
Fixative solution
Methanol, 9 parts; formaldehyde (40%) solution, 1 part. Store in ice
compartment of refrigerator.
Propanediol buffer solution (0.2M)
Dissolve 10.5 g of 2-amino-2-methyl propane (l:3)-diol in 500 ml of
deionized water. Store at 04°C.
Dye-substrate mixture (dry)
Prepare mixtures of 20 mg of sodium alpha-naphthyl phosphate and
20 mg of brentamine fast garnet (GBC salt) in dry test tubes. Some
batches of the dye react poorly and a new batch should always be first
tested.
Working reaction mixture
This is prepared immediately before use. Add 10 ml of the buffer
solution to a test tube containing the dry dye-substrate mixture and
shake thoroughly. Filtering is not essential.
Methyl green solution
Prepare a 2% aqueous solution of methyl green. Methyl violet
contamination is removed by extraction with half its volume of
chloroform for 48 hours.
260
APPENDIX A
Method
Place the slide, film uppermost, on the staining rack
Pour on the cold fixative
1 min
Wash in deionized water, drain and dry
Pour on cold working reaction mixture
10 min
Rinse in tap water
Counterstain with methyl green solution
15 min
Rinse in tap water and blot dry
Reaction
Alkaline phosphatase activity is indicated by the presence of a
reddish-brown granular precipitate in the cytoplasm.
Semi-quantitative rating of activity in PMN
See Naphthol AS-BI phosphate technique.
NAPHTHOL AS-BI PHOSPHATE TECHNIQUE
(Kaplow,J963)
Reagents
Fixative solution
Add 10 ml of formaldehyde (40%) solution to 90 ml of methanol.
Store in freezing compartment of refrigerator.
Propanediol buffer solution
Stock solution: See Alpha-naphthyl phosphate reaction.
Working solution (0.05M, pH 9.7): Add 5 ml of 0.1N hydrochloric
acid to 25 ml of stock buffer solutions. Adjust the pH to 9.7 and make
up volume to 100 ml with deionized water.
Naphthol AS-BI phosphate solution
Dissolve 20 mg of naphthol AS-BI phosphate (naphthol AS-CI,
AS-TR, AS-AN and AS-E phosphates may be used) in 1 ml of dimethyl
formamide and add it to 250 ml of working buffer solution. Aliquot
into stoppered containers and store at -20°C. Will keep stable for at
least 8 months.
Working reaction mixture
Thaw stock phosphate solution at room temperature. Add 4 mg of
red violet LB salt to each 10 ml of solution, agitate vigorously for 30
seconds and filter directly on to slides.
Haematoxylin solution
Add 1 g of haematoxylin to 500 ml of deionized water. Heat to
boiling and add a further 500 ml of water. Add 0.2 g of sodium iodate
and 50 g of aluminium potassium sulphate. Shake well. Filter and store
in a brown bottle at room temperature.
261
THE PERIPHERAL BLOOD FILM
Method
Place slide, film uppermost, on staining rack
(Do not use film of EDTA anticoagulated blood)
x
Pour on cold fixative solution
h min
Wash in tap water
1 min
Air dry
10-30 min
Pour on filtered working reaction mixture
10 min
Wash in tap water
1 min
Pour on haematoxylin solution
10 min
Wash in tap water
Vi min
Dry and mount
Reaction
Alkaline phosphatase activity is indicated by the presence of
pale-pink to brilliant ruby red granules in the cytoplasm.
Semi-quantitatiye rating of activity in PMN
Alkaline phosphatase activity is found only in neutrophil
polymorphs and may be semi-quantitatively rated in each cell as
indicated below. The sum of the ratings of 100 consecutive polymorphs
is the leucocyte alkaline phosphatase (LAP) score. The normal range is
15 -100.
0 — No staining or granular precipitate
1 —Very weak cytoplasmic staining with an occasional small
moderately stained granule
2 — Weak cytoplasmic staining with a few to moderate number of
medium sized granules
3 — Strong cytoplasmic staining with a moderate number to many
granules
4 — Numerous coarse, medium to large, deeply stained granules
filling the cytoplasm. Background staining of the cytoplasm is not
visible.
ACID PHOSPHATASE REACTION
(Li, Yam and Lam, 1970)
Reagents
Fixative solution
Mix ethanol, 10 ml; acetone, 60 ml; and citrate buffer, 40 ml.
Citrate buffer (0.03M, pH 5.4)
Dissolve 21 g of citric acid in 200 ml of N/l sodium hydroxide
solution and make up to 1 litre. Mix 76.5 ml of this solution with 23.5
ml of 0.1N sodium hydroxide solution and make up to 300 ml with
deionized water.
262
APPENDIX A
Acetate buffer solution (0. IM, pH 5.0)
Stock acetic acid and sodium acetate solutions: See Bromoindoxyl
acetate esterase reaction.
Working acetate buffer solution: Mix 14.8 ml of the acetic acid
solution and 35.2 ml of the sodium acetate solution. Make up to 200
ml with deionized water.
Naphthol AS-BI phosphate solution
Dissolve 10 mg of naphthol AS-BI phosphate in 0.5 ml of dimethyl
formamide and add it to 100 ml of working acetate buffer solution. It
is stable at 0 - 4° C for 2 months.
Working reaction mixture
Dissolve 5 mg of Fast Garnet (GBC salt) in 10 ml of naphthol AS-BI
phosphate solution. Filter before use.
Working reaction mixture with tartaric acidÇYam, l i and Lam, 1971)
Dissolve 75 mg of (L + ) tartaric acid in 10 ml of naphthol AS-BI
phosphate solution. Shake well and adjust the pH to 5.0 with
concentrated sodium hydroxide. Dissolve 5 mg of fast garnet in 10 ml
of this solution. Filter before use.
Haematoxylin solution
See Naphthol AS-BI phosphate technique for alkaline phosphatase
reaction.
Method
Place slide, film uppermost, on staining rack
Pour on cold fixative solution
. . . VL min
Wash thoroughly in deionized water
Air dry
10 - 30 min
Transfer slide to Coplin jar containing
working reaction mixture at 37°C
. . . 45 min
Wash in tap water
Pour on haematoxylin solution
. 1 - 3 min
Wash in tap water
. . . xâ min
Dry and mount
Reaction
Acid phosphatase activity is indicated by the presence of a
reddish-brown granular deposit in the cytoplasm of the cells.
Note
The acid phosphatase reaction is of value only in the diagnosis of
leukaemic reticulo-endotheliosis ('hairy' cell leukaemia) and the above
technique is best carried out with the working reaction mixture
containing tartaric acid instead of the usual working reaction mixture.
263
THE PERIPHERAL BLOOD FILM
NITROBLUE TETRAZOLIUM REDUCTION TEST
HEPARINIZED BLOOD TECHNIQUE
(Park, Fikrig and Smithwick, 1968)
Reagents
Nitroblue tetrazolium (NBT) stock solution
Dissolve 20 mg of powdered nitroblue tetrazolium in 10 ml of 0.9%
sodium chloride solution. Store in small aliquots at -20° C. Thaw at
room temperature just before use.
Sodium chloride solution (0.9%)
Dry the sodium chloride to constant weight. Dissolve 9 g in 1 litre of
deionized water.
Phosphate buffer, iso-osmotic (0.15M)
Stock solution A: Dissolve 2.34 g of hydrated sodium dihydrogen
phosphate in 100 ml of deionized water.
Stock solution B: Dissolve 2.13 g of anhydrous disodium hydrogen
phosphate in 100 ml of deionized water.
Buffered saline (pH 7.2)
Mix buffer solution A, 2.4 ml; buffer solution B, 7.6 ml; and sodium
chloride solution, 10 ml.
Reaction mixture
Mix equal volumes of NBT stock solution and buffered saline just
before use.
Romanovsky stain(s)
Method
Mix 0.1 ml volumes of heparinized blood and reaction mixture in a
siliconized concave microslide. Place the slide in a moist Petri dish.
Incubate at 37°C for 15 minutes and then leave at room temperature
for a further 15 minutes. Resuspend the cells with a small capillary
pipette. Make coverslip smears and air dry. Romanovsky stain the
smears.
Reaction
Neutrophils and monocytes with large blue-black deposits in their
cytoplasm are NBT-positive or formazan-containing cells. 'Equivocal
cells' are those that are not clearly identifiable as to type.
NBT Score
Using the oil-immersion objective lens of the microscope, count at
least 100 neutrophils and record the percentage of NBT-positive cells.
The normal range is 3 - 10%. If the number of equivocal cells added to
264
APPENDIX A
the number of NBT-positive neutrophils raises the final count into the
normal range, an additional 100 or more neutrophils should be counted
(Matula and Paterson, 1971) to establish the NBT response. Calculate
the absolute number of NBT-positive neutrophils from the absolute
neutrophil count. The normal range is 145 - 720 NBT-positive
neutrophils per mm 3 . With the use of the nomogram (see Figure 2)
devised by Feigin and his colleagues (1971), the patient may be
categorized into one of four groups: group A, normal; group B, viral
infection, partially treated bacterial infection, and non-infectious
febrile illness; group C, untreated bacterial infection; and group D,
ineffectively treated bacterial infection.
Note
(l)Low NBT scores should be checked by carrying out the
'stimulated' NBT test (Park and Good, 1970). Prepare a 200 mg/ml
solution of endotoxin (Difco) in buffered saline (pH 7.2). Mix 0.05 ml
of this solution and 0.5 ml of heparinized blood; incubate at room
temperature for 10 minutes. Carry out the NBT reduction test
described above. In normal controls more than 50% of the neutrophils
are NBT-positive.
(2) In neutropenic states, count the number of NBT-positive
monocytes (Park et ai, 1972). An NBT score that is greater than 15%
or 500 NBT-positive monocytes per mm3 or a rising daily score is
strong evidence of bacterial infection.
CAPILLARY BLOOD TECHNIQUE
(Gifford and Malawista, 1970)
Reagents
Pooled human serum
Mix equal volumes of serum from five healthy subjects. Store in small
aliquots at -20° C. Thaw at room temperature just before use.
Nitroblue tetrazolium (NBT) stock solution
Dissolve 28 mg of powdered nitroblue tetrazolium in 10 ml of 0.9%
sodium chloride solution. Sterilize by ultra-fine sintered glass filtration.
Store in small aliquots at -20°C.Thaw at room temperature just before
use.
Sodium chloride solution (0.9%)
See Heparinized blood technique.
Phosphate buffer, iso-osmotic (0.15M)
See Heparinized blood technique.
265
THE PERIPHERAL BLOOD FILM
Buffered saline (pH 7.2)
See Heparinized blood technique.
Reaction mixture
Mix pooled human serum, 0.5 ml; buffered saline, 0.3 ml; and NBT
stock solution, 0.6 ml.
Safranin solution
Dissolve 1 g of safranin 0 in 100 ml of deionized water and add 40
ml of glycerine.
Method
Isolation of granulocytes: Prick the fingertip with a sterile disposable
lancet. Place a large drop of the capillary blood in the centre of a clean
coverslip. Transfer the coverslip to a moist Petri dish and incubate at
37°C for 25 minutes. Using a Pasteur pipette wash away the clot with
sterile saline. Many neutrophils, occasional eosinophils and monocytes
remain adherent to the coverslip.
Exposure of granulocytes to NBT: Remove excess saline by gently
tapping the edge of the coverslip against filter paper. (Do not allow the
film to dry.) Immediately invert the coverslip on a drop of reaction
mixture on a clean glass slide. Remove excess solution by gently
blotting the coverslip with filter paper. Place the slide in a moist Petri
dish. Incubate at 37°C for 20 minutes. Remove the coverslip and
quickly air dry (5 sec) the film. Fix in absolute methanol (60 sec), wash
in running tap water (15 sec), immerse in safranin solution (5 min),
wash in running tap water (10 sec), blot dry. Fix the coverslip to a
microscope slide with clear permanent mounting.
Reaction
Normal and degenerate (necrobiotic) neutrophils are seen. The latter
cells may be mistaken for monocytes; their morphology is described in
Chapter 5. Only the degenerate neutrophils contain blue-black
formazan deposits.
NBT score
In normal subjects more than 30% of the neutrophils are
formazan-containing cells.
Note
(1) A normal control blood should be treated simultaneously with
the patient's blood.
(2) The addition of latex particles to the reaction mixture does not
increase the percentage of formazan-containing cells.
266
APPENDIX A
RETICULOCYTE STAINING
Reagent
Supravital staining solution
Dissolve 1 g of water-soluble brilliant cresyl blue or new méthylène blue
in 100 ml of citrate-saline solution (3% sodium citrate solution, 1 part;
0.9% sodium chloride solution, 4 parts). Filter before use.
Method
Mix equal volumes of blood and filtered staining solution in a glass
tube and incubate at 37°C for 15 minutes. Resuspend the red cells and
prepare films in the usual manner. After air drying, the films may be
examined microscopically with the oil-immersion objective lens.
Reaction
The residual RNA material of the reticulocyte stains a deep blue
colour and is seen against the pale green-blue background of the red
cell. The RNA material may appear granular or as a reticulum of fine
filaments depending on the maturity of the cell. When present other red
cell inclusions are also stained. Heinz bodies and haemoglobin H
inclusions are pale blue in colour while Howell-Jolly and Pappenheimer
bodies appear almost black in colour.
Reticulocyte count
Reticulocyte counting is best carried out in the area of ideal film
thickness. To narrow the microscope field and to make it easier for
counting, use either an eyepiece with an adjustable diaphragm or
construct a diaphragm with a window as follows. Remove the top lens
of an eyepiece. Cut out a circular piece of thin cardboard the same
diameter as the internal diameter of the eyepiece. Then cut out a 4 mm
square window in the centre of the cardboard which is next placed on a
shelf inside the eyepiece. Replace the top lens and return the eyepiece.
Count a minimum of 100 red cells and note the number of
reticulocytes present. Normally not more than 2% are seen, except in
the newborn when the upper limit is 6%. The 'Absolute' reticulocyte
count (%) is the observed count (%) multiplied by PCV/45. If 'shift'
reticulocytes, that is, large blue polychromatic cells, are seen in the
Romanovsky-stained blood film, divide the absolute count by the
reticulocyte maturation time which is 1 day for a PCV of 45%, 1.5 days
for a PCV of 35%, 2 days for a PCV of 25% and 2.5 days for a PCV of
15%. The corrected count represents the 'production index' (Hillman and
Finch, 1967,1969).
267
THE PERIPHERAL BLOOD FILM
STAINING FOR HEINZ BODIES
METHYL VIOLET TECHNIQUE
Reagents
Methyl violet solution
Dissolve 50 mg of powdered methyl violet in 10 ml of 0.9% sodium
chloride solution.
Eosin solution
Dissolve 10 mg of powdered eosin in 10 ml of deionized water.
Method
Add 1 volume of blood to 4 volumes of methyl violet solution in a
glass tube. Mix and leave at room temperature for 10 minutes.
Resuspend the red cells and prepare films in the usual manner. After air
drying, the films may be examined microscopically with the
oil-immersion objective lens. For permanent preparations, fix the film
in formaldehyde vapour for 10 minutes and then wash it thoroughly in
deionized water. Counterstain with eosin solution, wash and air dry.
Reaction
Heinz bodies stain an intense purple colour. When present, other red
cell inclusions are also stained. The RNA material of reticulocytes
appears pale blue in colour, while HowellJolly and Pappenheimer
bodies appear dark, almost black with a bluish tinge.
BRILLIANT GREEN/NEUTRAL RED TECHNIQUE
(Schwab and Lewis, 1969)
Reagents
Brilliant green solution (0.5%)
Dissolve 50 mg of powdered brilliant green in 10 ml of 1% sodium
chloride solution. Prepare fresh and filter before use.
Neutral red solution (0.5%)
Dissolve 50 mg of powdered neutral red in 10 ml of 1% sodium
chloride solution. Prepare fresh and filter before use.
Sodium chloride solution
Dissolve 1 g of dry sodium chloride in 100 ml of deionized water.
Method
Mix 1 volume of heparinized blood and 1 volume of neutral red
solution in a glass tube; after 1 minute add 2 volumes of brilliant green
solution and mix. After 2 minutes resuspend the red cells and make
films in the usual manner. Examine microscopically with the
oil-immersion objective lens.
268
APPENDIX A
Reaction
Heinz bodies appear bright green in colour against an7 eosinophilic
background. Residual RNA of reticulocytes stains very pale green.
DETECTION OF UNSTABLE HAEMOGLOBINS
(Hutchison, 1967)
Reagents
Buffered water (pH 6.5)
Stock solutions A and B: See Jenner-Giemsa staining.
Working solution: Mix solution A, 7 parts and solution B, 3 parts.
Dispense in 1 ml amounts in bijou bottles and sterilize.
Antibiotic solutions
Streptomycin solution: Dissolve 1 g of powdered streptomycin in 2
ml of sterile deionized water.
Penicillin solution: Dissolve 1 mega unit of powdered penicillin in 2
ml of sterile deionized water.
Reagents for Heinz body staining
Method
Add 1 ml of citrated or heparinized blood to a bijou bottle
containing 1 ml of sterile working buffer solution and mix. With a
sterile Pasteur pipette add 1 drop of streptomycin solution and 1 drop
of penicillin solution to the diluted blood. Incubate at 37°C for 18
hours. Resuspend the red cells and supravitally stain for Heinz bodies.
Reaction
Normal blood shows no brown discolouration and Heinz bodies are
not detectable. In unstable haemoglobinopathy, the blood has a brown
discolouration and many Heinz bodies are seen in the red cells.
STAINING FOR HAEMOGLOBIN H INCLUSIONS
Reagents
Supravital staining solutions
See Reticulocyte staining.
Method
As for reticulocyte staining but incubate the mixture of blood and
staining solution for 30-60 minutes at 37°C.
Reaction
Haemoglobin H inclusions are of varying size and appear as pale blue
spherical bodies against a pale blue-green background. The staining
269
THE PERIPHERAL BLOOD FILM
reaction of other inclusions is described in reticulocyte staining.
ACID ELUTION TEST FOR HAEMOGLOBIN F
HAEMATOXYLIN-FERRIC CHLORIDE (pH 1.1) TECHNIQUE
(Nierhaus and Betke, 1968)
Reagents
Fixative solution
80% ethanol.
Haematoxylin solution
Dissolve 750 mg of haematoxylin in 100 ml of 96% ethanol. No
ripening of the dye is necessary.
Feme chloride solution
Dissolve 2.4 g of ferric chloride in 100 ml of 0.5% hydrochloric acid
solution.
Reaction mixture (pH 1.1)
Mix 2 volumes of haematoxylin solution, 1 volume of ferric chloride
solution and 1 volume of 80% ethanol. The pH is not critical. Filter
before use.
Scott's tap water substitute
See Periodic acid-Schiff reaction.
Eosin solution
Dissolve 2.5 g of powdered eosin in 100 ml of deionized water.
Method
Place slide, film uppermost, on the staining rack
Pour on fixative solution
Wash in tap water and air dry
Pour on reaction mixture
Wash in deionized water
Pour on Scott's tap water substitute
Air dry
Pour on eosin solution
Wash briefly in deionized water
Air dry and mount
5 min
3 min
1 min
2 min
Reaction
Red cells containing haemoglobin F and the rare polycythaemic
haemoglobin Rainier are bright red in colour. Cells with other
haemoglobins (normal and variants) appear as pale pink ghosts.
Lymphocytes stain a grey colour.
270
APPENDIX A
An occasional foetal cell may be detected in normal blood. When
present in greater numbers the stained cells are usually patchily
distributed in the film except in subjects with hereditary persistence of
foetal haemoglobin (HPFH), when all the red cells are stained.
Volume of foetomaternal transplacental haemorrhage (FMTPH)
(1) Count the number of foetal cells in 50 low power objective fields
of maternal blood. Foetal scores greater than 3 indicate FMTPH. Scores
of 5 and 60 respectively represent 0.25 ml and 3.0 ml of foetal blood
(Woodrowétfa/., 1965).
(2) Count the foetal cells in 50 mm2 of the area of ideal film
thickness of maternal blood. Divide the foetal score by 100 to
determine the volume of FMTPH (Grobbelaar, 1968; Grobbelaar and
Dunning, 1969).
(3) Determine the percentage of foetal cells in the maternal blood
film and multiply the foetal score by 50 (Kleihauer, 1966).
PHOSPHATE-CITRATE BUFFER (pH 3.3) TECHNIQUE
(Kleihauer, Braun and Betke, 1957)
Reagents
Fixative solution
80% ethanol.
Phosphate solution (0.2M)
Dissolve 2.84 g of anhydrous disodium hydrogen phosphate (or 3.56
g of Na 2 HP0 4 .2H 2 0 or 5.36 g of Na 2 HP0 4 .7H 2 O) in 100 ml of
deionized water.
Citric acid solution (0.1M)
Dissolve 2.1 g of citric acid in 100 ml of deionized water.
Reaction mixture (pH 3.3)
Mix 26.6 ml of phosphate solution and 73.4 ml of the citric acid
solution. Check that the pH is 3.3.
Eosin solution
Dissolve 1 g of powdered eosin in 100 ml of deionized water.
Method
Place slide, blood film uppermost, on staining rack
Pour on fixative solution
Wash in tap water and air dry
Transfer the slide to a Coplin jar containing
the reaction mixture incubated at 37°C
Wash in tap water and air dry
. 5 min
15 min
271
THE PERIPHERAL BLOOD FILM
Counterstain with eosin solution
1 min
Wash in tap water and air dry
Reaction
See Haematoxylin-ferric chloride (pH 1.1) technique. The lymphocytes, however, do not stain a grey colour.
Volume of foetomaternal transplacental haemorrhage (FMTPH)
See Haematoxylin-ferric chloride (pH 1.1) technique.
ELUTION TEST FOR HAEMOGLOBIN S
(Yakulis and Heller, 1964)
Reagents
Phosphate buffer (2A8My pH 7.26)
Dissolve 29.9 g of dipotassium hydrogen phosphate and 16.3 g of
potassium dihydrogen phosphate in 100 ml of deionized water. Store at
room temperature. The buffer is stable for 3 months.
Buffered sodium dithionite solution
Dissolve 100 mg of sodium dithionite in 50 ml of the phosphate
buffer.
Eosin solution
Dissolve 200 mg of powdered eosin in 100 ml of deionized water.
Method
Immerse the blood film in the buffered dithionite
solution at 37°C
10 min
Air dry
Fix the film in ethanol
5 min
Rinse in tap water
Counterstain with eosin solution
Reaction
Residually pigmented red cells indicate the presence of haemoglobin
S or precipitated haemoglobin H. Vacuoles may be seen and red cell
distortion is more marked in blood films from patients with sickle cell
disease, sickle cell-thalassaemia disease and sickle cell-haemoglobin C
disease. Red cells containing other haemoglobins (normal or variants)
are decolorized and appear as ghosts.
SICKLING REACTION
Reagents
Sodium metabisulphite solution (2%)
Dispense 200 mg amounts of sodium metabisulphite into a number of
272
APPENDIX A
test tubes. Seal and store. Dissolve the contents of a tube in 10 ml of
buffered water (pH 6.8) immediately before use.
Buffered water (pH 6.8)
See Jenner-Giemsa staining.
Method
Place a drop of freshly collected anticoagulated blood in the centre
of a microscope slide. Add 3 drops of fresh sodium metabisulphite
solution and mix. Place a coverslip over the mixture and remove excess
fluid by gently blotting the coverslip with filter paper. Seal the edges of
the coverslip with petroleum jelly, molten paraffin wax or nail varnish,
applied with an orange stick. Allow the slide to stand at room
temperature or at 37°C. Examine microsopically every half-hour.
Reaction
Red cells containing haemoglobin S assume sickle or holly-leaf forms
within 18 hours. Haemoglobins Bart, I and C Georgetown may give a
positive sickling reaction. Haemoglobin C crystallization may be
misinterpreted as sickling.
False negative results may be due to (1) old blood, (2) deterioration
of reducing agent, (3) trapped air under the coverslip, (4) blood
haemoglobin concentration less than 7 g per 100 ml, (5) haemoglobin S
associated with hereditary persistence of foetal haemoglobin which is
detected by the acid elution test for haemoglobin F.
PERMANENT SICKLE CELL PREPARATION
(Stenton, 1959)
Reagents
Sodium metabisulphite solution (2%)
See Sickling reaction.
Buffered water (pH 6.8)
See Sickling reaction.
Liquid paraffin
Fixative solution
Mix 10 ml of formaldehyde (40%) solution and 90 ml of 0.9%
sodium chloride solution.
Eosin solution
Dissolve 50 mg of powdered eosin in methanol.
273
THE PERIPHERAL BLOOD FILM
Method
Set up the sideling reaction previously described. In addition mix 0.2
ml of freshly collected anticoagulated blood and 0.4 ml of freshly
prepared sodium metabisulphite solution in a test tube. Layer liquid
paraffin on the surface of the mixture to a depth of 0.5 cm. Mien
sickling has occurred in the slide test, introduce 2 ml of the fixative
solution through the liquid paraffin by means of a Pasteur pipette.
After 30 minutes of fixation, remove the liquid paraffin and portion of
the reaction mixture by suction. Check that sickling has occurred in the
tube. Prepare films in the usual manner. Allow to air dry. Stain with the
alcoholic eosin solution for 2 minutes. Wash in tap water and dehydrate
the film through graded alcohols. Clear in xylol and mount.
274
Appendix B
HAEMOTOXIC EFFECTS OF DRUGS AND CHEMICALS
Drugs and chemicals which have been reported in the medical literature
to have caused: (1) megaloblastic anaemia, (2) haemolyic anaemia, (3)
methaemoglobinaemia, (4) sideroblastic anaemia, (5) aplastic anaemia,
(6) neutropenia or agranulocytosis, (7) leukaemia, (8) thrombocytopenia, and (9) thrombopathy are listed alphabetically by their
'approved' names. The asterisk signifies an antimitotic and cytotoxic
drug; HB, Heinz body type haemolytic anaemia; IM, immunological
type haemolytic anaemia or thrombocytopenia; and M, microangiopathic type haemolytic anaemia.
MEGALOBLASTIC ANAEMIA
Isoniazid
Alcohol
6-Mercaptopurine *
Aminopterin*
Methotrexate*
Barbiturates
Para-aminosalicylic acid
Colchicine
Phenylbutazone
Contraceptives (oral)
Phenytoin
Cycloserine
Pyrazinamide
Cytosine arabinoside*
Pyrimidone
Diamidine compounds
Pyrimethamine
Diopterin*
Teropterin*
Diphenylhydantoin
6-Thioguanine*
Epanutin
Ethotoin
HAEMOLYTIC ANAEMIA
Acetanilide (HB)
Acetylsalicylic acid (HB, Im)
Acetazolamide
Aminopyrine (Im)
Amphetamine
Acetomenaphthonum
Aniline (HB)
Acetophenetidine (HB)
Antazoline
Acetylphenylhydrazine (HB)
275
THE PERIPHERAL BLOOD FILM
Haemolytic anaemia (cont.)
Antimony compounds
Antistine (Im)
Arsenic and compounds
Benzene
Bromates
Carbon disulphide
Chloramphenicol
Chlorates
Chlorobenzene
Chloroquine (HB, Im)
Chlorpromazine (Im)
Chlorpropamide (M)
Dapsone (HB)
Dexamphetamine
Dichlorobenzene
Dichlorohydrine
Dimercaprol
Dinitrobenzene
Diphenylsemicarbazide
Diphenylsulphone (HB)
Dipyrone
Ethopropazine
Fava beans (HB)
Fuadin (Im)
Furaltadone
Furazolidine (HB)
Gold salts (M)
Insecticides (Im)
Isoniazid (Im)
Mepacrine (HB)
Mephenesin
Methoin
Methylamphetamine
Methyldopa (Im)
Naphthalene and derivatives (HB)
Neoarsphenamine (HB, Im)
Nitrobenzene
Nitrofurantoin (HB)
Nitrofurazone (HB)
Pamaquin (HB)
Para-aminosalicylic acid (Im)
Paramethadone
Paraphenylenediamine
Penicillin (Im, M)
Pentaquin (HB)
Phenacetin (Im)
Phenazone
Phenylbutazone (M)
Phenylhydrazine (HB)
Phenylsemicarbazones
Phosphorus
Plasmaquin (HB)
Primaquin (HB)
Primizole
Probenecid
Promin
Pyramidon (Im)
Pyrimethamine
Quinidine (Im, M)
Quinine (HB, Im)
Solapsone
Stibophen (Im)
Sulphonamides (HB, Im)
Thiacetazone
Thiouracil
Thiourea
Trinitrotoluene
Tripelennamine
Vitamin K (HB)
Vaccines
METHAEMOG
METHAEMOGLOBINAEMIA
Acetanilide
Acetophenetidine
Aminobenzene
Aniline and derivatives
In marking ink
In shoe dyes
In blanket dyes
In wax crayons and chalk
276
Benzocaine
Bismuth subnitrate
Chlorates
Nitrates
I« meat
In well water
Nitrites
Nitrobenzenes
APPENDIX B
Methaemoglobinaemia (cont.)
Nitroglycerine
Nitrotoluenes
Nitrous gases
Arc welders
Phenacetin
Phenylhydrazine
Plasmoquin
Pyrogallol
Quinones
Resorcinol
Sulfonal
Sulphonamides
Trional
SIDEROBLASTIC ANAEMIA
Alcohol
Azathioprine*
Chloramphenicol
Cycloserine
Isoniazid
Lead
Para-aminosalicylic acid
Paracetamol
Phenacetin
Pyrazinamide
APLASTIC ANAEMIA - PANCYTOPENIA
Acetarsol
Acetazolamide
Acetophenetidine
Acetylsalicylic acid
Actinomycin D and C*
Aloxidone
Aminopterin*
Aminopyrine
Aminouracil*
Amphotericin B
Apronal
Arsenic compounds
Asparaginase*
Azaserine*
6-Azauracil
Benzene
Bismuth and compounds
Busulphan (Myleran)*
Carbimazole
Carbon tetrachloride
Carbutamide
Chlorambucil*
Chloramphenicol
Chlorates
Chlordane
6-Chloro purine
Chlorothiazide
Chlorpheniramine
Chlorpromazine
Chlorpropamide
Chlort et r a cy cline
Cy clophosphamide *
Cytosine arabinoside*
Demecolcin
Dinitrophenol
Diopterin*
Diphenylhydantoin
Ethosuximide
5-Fluorouracil
Gamma benzene hexachloride
Gold salts
Hydrallazine
Isoniazid
Mepacrine
Mephalan*
Meprobamate
6-Mercaptopurine *
Mercurial salts
Methimazole
Methoin
Methotrexate*
Methsuximide
Methyldopa
Methylthiouracil
Methylphenylhydantoin
Naphthyl chlorethylamine
277
THE PERIPHERAL BLOOD FILM
Aplastic anaemia-pancytopenia (cont.)
Quinidine
Neomycin
Salicylamide
Nitrogen mustard*
Streptomycin
Paramethadione
Paraphenylenediamine
Sulphonamides
Pecazine
Teropterin*
Phenacemide
Thioridazine
Phenothiazines
Thiosemicarbazones
Phensuximide
Thio-tepa
Phenylacetylurea
Tolbutamide
Phenylbutazone
Triethylenemelamine
Phosphor amides *
Trimethadione
Phosphorus
Trinitrotoluene
Primidone
Tripelennamine
Prochlorperazine
Troxidone
Propylthiouracil
Urethane*
Pyrimethamine
Vinca alkaloids*
Quinacrine
NEUTROPENIA - AGRANULOCYTOSIS
Acetanilide
Cyclophosphamide*
Acetarsol
Dapsone
Acetazolamide
Demecolcine*
Amidopyrine
Desipramine
Aminopterin*
Dicoumarol
Aminouracil*
Diethazine
Amodiquine
Dihydrallazine
Antazoline
Dihyprylone
Antimony and compounds
Dinitrophenol
Arsenic and compounds
Ethotoin
Gold salts
Barbiturates
Hydrallazine
Benzene
Hydroxyphenylbutazone
Biallylamicol
Imipramine
Bismuth and compounds
Isoniazid
Busulphan (Myleran)*
Mephenesin
Carbimazole
Mepyramine
Carbutamide
Mercaptomerin
Chlorambucil*
6-Mercap t opurine *
Cinchophen
Mercurial salts
Chlorophenothane
Chloroquin
Mersalyl
Chlorothiazide
Metapheniline
Chlorpheniramine
Methicillin
Chlorpromazine
Methimazole
Chlorpropamide
Methoin
Colchicine
Methylthiouracil
278
APPENDIX B
Neutropenia-agranulocytosis (cont.)
Naphthylchlorethylamine *
Nitrogen mustards*
Novobiocin
Paracetamol
Para-aminosalicylic acid
Paramethadione
Pecazine
Perphenazine
Phenacetin
Phenazone
Phenindione
Phenothiazine
Phensuximide
Phenylbutazone
Phenytoin
Phosphorus
Plasmaquin
Primaquin
Procaineamide
Prochlorperazine
Promazine
Promethazine
Propylthiouracil
Pyrimethamine
Pyrithyldione
Quinine
Ristocetin
Streptomycin
Sulphasalazine
Sulphonamides
Tetracyclines
Thiacetazone
Thiantoin
Thiocyanates
Thioglycollate
Thioridazine
Thiosemicarbazones
Thiourea
Thiouracils
Tolbutamide
Triethylenemelamine *
Trifluoperazine
Urethane*
LEUKAEMIA
Phenylbutazone
Sulphonamides
Aminopyrine
Chloramphenicol
Ionizing radiation
THROMBOCYTOPENIA
Acetarsol
Acetazolamide (Im)
Acetylcarbromal
Acetylsalicylic acid (Im)
Amidopyrine
Aminouracil*
Antazoline (Im)
Antipyrine (Im)
Apronal
Arsenicals, organic (Im)
Barbiturates (Im)
Benzene
Bismuth and compounds (Im)
Bromvaletone
Busulphan (Myleran)*
Carbimazole
Carbromal
Carbutamide
Cephalothin (Im)
Chlorambucil*
Chloramphenicol
Chlorophenothane
Chloroquine (Im)
Chlorothiazide (Im)
Chlorpromazine
Chlorpropamide (Im)
Colchicine
Demecolcin*
Desipramine (Im)
Digitoxin (Im)
279
THE PERIPHERAL BLOOD FILM
Thrombocytopenia (cont.)
Dihydrallazine
Dilantin (Im)
Dinitrophenol
Ergot and preparations
Glyceryl trinitrate
Gold salts (Im)
Insulin (Im)
Iodides
Isoniazid
Mephenesin
Meprobamate (Im)
6-Mercaptopurine *
Mercurial salts
Mersalyl (Im)
Methoin
Methyldopa (Im)
Naphthylchlorethyiamine *
Nitrogen mustards*
Novobiocin (Im)
Oestrogens
Para-aminosalicylic acid (Im)
Paracetamol (Im)
Penicillin (Im)
Phenindione
Phenylbutazone
Phenytoin
Piperazine
Prochlorperazine (Im)
Propylthiouracil
Quinidine (Im)
Quinine (Im)
Reserpine
Ristocetin
Salicylates
Sedormid (Im)
Stibophen (Im)
Streptomycin (Im)
Sulphonamides (Im)
Tetanus Toxoid (Im)
Tetracyclines
Thallium
Thiocyanates
Thiouracils (Im)
Thiourea
Tolbutamide (Im)
Triethylenemelamine *
Triflupromazine
Trimeprazine
Trimethadione
Tripelennamine
Troxidone
Vaccines
THROMBOPATHY
Acetylsalicylic acid
Amitryptyline
Chloroquin
Citrate
Cocaine
Colchicine
Dextran
Dihydroergotamine
Dipyridamole
Furosemide
Heparin
Imipramine
Indomethacin
280
Isoprenaline
Methylxanthines
Nitrofurantoin
Papaverine
Penicillin (high doses)
Phentolamine
Phenylbutazone
Procaine
Sequestrene
Sulfinpyrazone
Theophylline
Vinca alkaloids*
Plate 1. Red cells and polymorphonuclear neutrophil (PMN) leucocyte ( x 1,200)
Plate 2. Monocyte ( x 1,200)
(a)
Plate 3 (a). Small lymphocyte
(x 1,200)
(h)
(b) Large lymphocyte ( x 1,200)
Plate 4. Platelets ( x 1,200)
Plate 5. Target cells ( x 1,200)
Plate 6. Stomatocytes ( x 1,200)
Plate 7. Spherocytes (x 1,200)
(a)
Plate 8 (a). Round macrocyte
(x 1,200)
(b)
(b) Oval macrocyte ( x 1,200)
Plate 9. EUiptocytes ( x 1,200)
Plate 11. Crenated cells ( x 1,200)
(a)
Plate 10. Sickle cells ( x 1,200)
Plate 12. Acanthocytes ( x 1,200)
(b)
Plate 13 (a), (b) and (c). Burr cells ( x 1,200)
(c)
Plate 14. Tear drop cells ( x 1,200)
Plate 15. Howell - Jolly bodies
( x 1,200)
Plate 16. Pappenheimer bodies
( x 1,200)
(a)
Plate 17 (a). Malarial parasite —
ring trophozoite ( x 1,200)
(b)
(b) Malarial parasite — amoebo
idal trophozoite ( x 1,200)
Plate 18. Pelgeroid
anomaly ( x 1,200)
Plate 19. Hypersegmented PMN — macropolycyte (x 1,200)
Plate 20. L.E. cell
( x 1,200)
(a)
(b)
Plate 21 (a) and (b). Malignant monocytes ( x 1,200)
(a)
Plate 22 (a). Lymphocytoid mononucleosis cell.
(b)
(b). Monoblastoid mononucleosis
cell ( x 1,200)
Plate 23. Thesaurocyte (x 1,200)
(a)
Plate 24 (a).
(b)
(c)
Plate 24 (a), (b) and (c). Phagocytîc plasma cells ( x 1,200)
Plate 25. Intermediate
normoblast (x 1,200)
Plate 26. Late normoblast (x 1,200)
Plate 27. Trefoil
nucleus ery thro blast
(x 1,200)
Plate 28. Vacuolated
late erythroblast
(x 1,200)
Plate 30. Myelocyte
( x 1,200)
Plate 33. Malignant
monoblast ( x 1,200)
Plate 29. Intermediate
megaloblast ( x 1,200)
Plate 31. Stab cell
( x 1,200)
Plate 32. Malignant
myeloblast ( x 1,200)
Plate 34. Megakaryoblast ( x 1,200)
Plate 35. Megakaryocyte ( x 1,200)
Plate 36. Malignant lymphoblasts ( x 1,200)
Plate 37. Malignant plasma blasts ( x 1,200)
Plate 38. Megakaryocytoid plasmablast ( x 1,200)
Plate 39. Polycythaemîa ( x 700)
Plate 40. Megaloblastic anaemia ( x 700)
Plate 41. Acquired stomatocytosis ( x 700)
Plate 42. Nutritional anaemia ( x 700)
Plate 43. Hereditary elliptocytosis ( x 700)
Plate 44. Hereditary spherocytosis ( x 700)
Plate 45.
Acquired
Plate 46.
spherocytosis
Sicklaemia
( x 700)
( x 700)
Plate 47. Rouleaux of red cells ( x 700)
Plate 48. Agglutination of red cells ( x 700)
Plate 49.
Plate 50.
Myelocytic
Lymphocytic
leukaemia
leukaemia
( x 700)
( x 700)
Plate 51. Infectious mononucleosis ( x 700)
Bibliography and References
Abramson, N., von Kapff, C. and Ginsburg, A.D. (1970): 'The phagocytic plasma cell'. New Engl. J. Med.} 283, 248
Allison, A.C. (1963). 'Inherited factors in blood conferring resistance to
protozoa'. In Immunity to Protozoa. A Symposium, p. 109. Eds
P.C.C. Garnham, A.E. Pierce and I.M. Roitt. Oxford; Blackwell
Scientific Publications
Andersen, B.R. (1971). 'N.B.T. test in malaria'. Lancet 2, 317
Ashley, D.J.B. (1957). 'Occurrence of sex chromatin in the cells of the
blood and bone marrow in man'. Nature, Lond. 179, 969
Baehner, R.L. and Nathan, D.G. (1966). 'Deficient glucose oxidation in
the intact leucocytes of chronic granulomatous disease'. Blood 28,
1010
Bannatvala, J.E.
(1970).
'Infectious
mononucleosis.
Recent
developments'.^. / . Haemat. 19, 129
Bannatyne, R.M., Skowron, P.N. and Weber, J.L. (1969). 'Job's
syndrome — a variant of chronic granulomatous disease'. / . Pediat.
75,236
Barka, T. and Anderson, P.J. (1962). 'Histochemical methods for acid
phosphatase using hexazonium pararosanilin as coupler'. J.
Histochem. Cytochem.,
10,741
Barker, B.E., Fames, P. and La Marche, P.H. (1967). 'Haematologic
effects of pokeweed'. Lancet 1, 437
Barreras, L., Diggs, L.W, and Bell, R. (1968). 'Erythrocyte morphology
in patients with sickle cell anaemia and pulmonary emboli'. /. Am.
med. Ass. 203, 569
Bauermeister, D.E. (1971). 'Quantitation of bone marrow reticulin — A
normal range'. Am. J. clin. Path. 56, 24
Bell, R.E. (1963). 'The origin of "burr" erythrocytes'. Br. J. Haemat. 9,
552
Benvenisti, D.S. and Ultmann, J.E. (1969). 'Eosinophilic leukaemia'.
Ann. intern. Med. 71, 731
Bottomley, S.S., Whitcomb, W.H., Smithee, G.A. and Moore, M.J.
(1971). 'Effect of cyclic adenosine — 3', 5'-monophosphate in bone
marrow delta-amino-levulinic acid synthetase and erythrocyte iron
uptake'./. Lab. clin. Med. 77, 793
281
THE PERIPHERAL BLOOD FILM
Bradley, T.R. and Metcalf, D. (1966). 'The growth of mouse bone
marrow cells in vitro'. Aust. J. exp. Biol. med. Sei. 44, 287
Brain, M.C. (1970). 'Microangiopathic haemolytic anaemia'. A. Rev.
Med. 21, 137
Broun, O.G., Herbig, F.K. and Hamilton, J.R. (1966). 'Leucopenia in
Negroes'. New Engl. J. Med. 275, 1410
Brunning, M.D. (1970). 'Morphologic alterations in nucleated blood
and marrow cells in genetic disorders'. Human Pathol. 1, 99
Bunn, H.F. and Jandl, J.H. (1970). 'Control of haemoglobin function
within the red cell'. New Engl. J. Med. 282, 1414
Butler, J J . (1970). 'Histology of malignant lymphomas and Hodgkin's
disease'. In Leukaemia-Lymphoma. Proceedings of the Fourteenth
Annual Clinical Conference on Cancer, p. 123. Ed. C.J. Zarafonitis.
Chicago; Year Book Medical Publishers Inc.
Butterworth, C E . , Frommeyer, W.B. and Riser W.H. (1953).
'Erythrophagocytosis in a case of plasma cell leukaemia'. Blood 8,
519
Cartwright, G.E., Athens, J.W. and Wintrobe, M.M. (1964). 'The
kinetics of granulopoiesis in normal man'. Blood 24, 780
Cawley, J.C. and Hayhoe, F.G.J. (1972). 'The inclusions of the
May-Hegglin anomaly and Dohle bodies of infection: an
ultrastructural comparison'. Br. J. Haemat. 22, 491
Chanarin, I. (1969). 'The Megaloblastic Anaemias'. Oxford; Blackwell
Scientific Publications.
Clark, R.L., Jones, J.H. and Jones, J.F. (1967). 'Screening lead workers
for the presence of stippled erythrocytes'. / . clin. Path. 20, 166
Conrad, M.E. (1971). 'Haematologic manifestations of parasitic infections'. Semin. Haemat. 8, 267
Cooper, R.A. (1969). 'Anaemia with spur cells. A red cell defect
acquired in serum and modified in the circulation'. /. clin. Invest.
48, 1820
- (1970a) 'The pathogenesis of burr cells in uraemia'. / . clin. Invest.
49, 22a
- (1970b) 'Lipids of human red cell membrane. Normal composition
and variability in disease'. Semin. Haemat. 7, 296
- and Jandl, J.H. (1968). 'Bile salts and cholesterol in the pathogenesis
of target cells in obstructive jaundice'./, clin. Invest. 47, 809
Craddock, CG., Longmire, R. and
McMillan, R. (1971).
'Lymphocytes and the immune response'. New Engl. J. Med. 285,
324, 378
Crome, P.E. and Barkhan, P. (1963). 'Platelet adherence to
polymorphs'. Br. med. J. 2, 871
Crosby, W.H. (1972). 'Splenectomy in haematologic disorders'. New
Engl. J. Med. 286, 1252
Dacie, J.V. and Lewis, S.M. (1968). Practical Haematology. Fourth
Edition. London; J. and A. Churchill
Daland, G.A. and Castle, W.B. (1948). Ά simple and rapid method for
282
BIBLIOGRAPHY AND REFERENCES
demonstrating sickling of the red cells; the use of reducing agents'. / .
Lab. din. Med. 33, 1082
Daniels, J.C., Ritzmann, S.E. and Levin, W.C. (1968). 'Lymphocytes.
Morphological, developmental and functional characteristics in
health, disease and experimental study — An analytical review'. Tex.
Rep. Biol. Med. 26, 5
Davidson, W.M. and Jennison, R.F. (1952). 'The relationship between
iron storage and anaemia'. /. clin. Path. 5, 281
Di Guglielmo, R. (1966). Unusual morphologic and humoral conditions
in the field of plasmocytoms and M-proteinaemia'. A eta med. Scand.
Suppl. 445, 206
Döbler, J. and Bertles, J.F. (1968). 'The physical state of haemoglobin
in sickle cell anaemia erythrocytes in vivo*. J. exp. Med. 127, 711
Dosik, H., Rosner, F. and Sawitsky, A. (1972). 'Acquired lipidosis.
Gaucher-like cells and "blue cells" in chronic granulocytic
leukaemia'. Semin. Haemat. 9, 309
Drivisholm, A. and Clausen, J. (1964). 'The relationship between the
cytology and the immunoelectrophoretic pattern in 105 cases of
myelomatosis'.ylcte med. Scand. 175, 609
Dumonde, D.C. (1970). ' "Lymphokines": Molecular mediators of
cellular immune responses in animals and man'. Proc. R. Soc. Med.
63,899
Emmons, W.F. (1927). 'Clinical eriometer'. Q. Jl Med. 21, 83
Eve, F.C. (1929). 'Early diagnosis of pernicious anaemia by halometer'.
Br. med. J. 1,48
Ezeilo, J.C. (1972). 'Non-genetic neutropenias in Africans'. Lancet 2,
1003
Fairbanks, V.F. and Lampe, L.T. (1968). Ά tetrazolium linked
cytochemical method for estimation of glucose-6-phosphate
dehydrogenase activity in individual erythrocytes. Applications in
the study of hétérozygotes for glucose-6-phosphate dehydrogenase
deficiency'. Blood 3 1 , 1589
Farnes, P. and Barker, B.E. (1968). 'Blood mononuclear cell
abnormalities in m u m p s ' . ^ w . / . clin. Path. 49, 398
Feigin, R.D., Shackelford, P.G., Choi, S.C., Flake, K.K., Franklin, F.A.
and Eisenberg, C.S. (1971). 'Nitroblue tetrazolium dye test as an aid
in the differential diagnosis of febrile disorders'. /. Pediat. 78, 230
Field, E.J. and MacLeod, I. (1963). 'Platelet adherence to polymorphs'.
Br. med. J. 2, 388
Field, J.W. (1940). 'The morphology of malarial parasites in thick
blood films. Part IV. The identification of species and phase'. Trans.
R. Soc. trop. Med. Hyg. 34, 405
- ( 1941 ) 'Further note on a method of staining malarial parasites in
thick blood films'. Trans. R. Soc. trop. Med. Hyg. 35, 35
Finch, CA., Deubelbeiss, K., Cook, J.D., Esbach, J.W., Harker, L.A.,
Funk, D.D., Marsaglia, G., Human, R.S., Slichter, S., Adamson, J.W.,
Ganzoni, A. and Giblett, E.R. (1970). 'Ferrokinetics in man'.
283
THE PERIPHERAL BLOOD FILM
Medicine, Baltimore 49. 17
Fleming, J.A. and Stewart, J.W. (1967). Ά critical and comparative
study of methods of isolating tumour cells from the blood'. J.clin.
Path. 20, 145
Fliedner, T.M., Cronkite, E.P., Killmann, S.A. and Bond, V.P. (1964).
'Granulocytopoiesis II. Emergence and pattern of labelling of
neutrophil granulocytes in humans'. Blood 24, 683
Flink, E.B. (1971). 'Heavy metal poisoning'. In Textbook of Medicine.
Eds. R.L. Cecil and R.F. Loeb. Thirteenth revised edition, p. 65. Eds
P.B. Beeson and W. McDermott. Philadelphia, Pa. and London; W.B.
Saunders
Galbraith, P.R. and Abu-Zahra, H.T. (1972). 'Granulopoiesis in chronic
granulocytic leukaemia*. Br. J.Haemat. 22, 135
Gall, J.C., Brewer, G.J. and Dem, R.J. (1965). 'Studies in
glucose-6-phosphate
dehydrogenase
activity
of
individual
erythrocytes. The methaemoglobin-elution test for identification of
female heterozygous for G-6PD deficiency'. Am. J. Hum. Genet. 17,
359
Garg, S.K., Amorosi, E.L. and Karpatkin, S. (1971). 'Use of the
megathrombocyte as an index of megakaryocyte number'. New
Engl. J. Med. 284, 11
Ghaemi, A. and Seaman, A J . (1963). '"Swiss Cheese" nuclei - An
incubation induced form of infectious mononucleosis lymphocytes'.
Am. J. din. Path. 39,492
Ghosh, M.L., Hudson, G. and Blackburn, E.K. (1973). 'Skin window
macrophages in malignant lymphoma.' Br. J. Haemat. 25, 293
Gifford, R.H. and Malawista, S.E. (1970). Ά simple rapid micromethod
for detecting chronic granulomatous disease of childhood'. /. Lab.
din. Med. 75,511
Goldberg, A.F. and Deane, H.W. (1960). Ά comparative study of some
staining properties of crystals in a lympho-plasmacytoid cell, of
Russell bodies in plasmacytes and of amyloids — with special
emphasis on their iso-electric points'. Blood 16, 1708
Goodpasture, E.W. (1937). 'Concerning the pathogenesis of typhoid
fever'. Am. J. din. Path. 13, 175
Gowland, E., Kay, H.E.M., Spillman, J.C. and Williamson, J.R. (1969).
'Agglutination of platelets by a serum factor in the presence of
EDTA'./. din. Path. 22, 460
Greig, H.B.W. (1959). Ά substitute for the Feulgen staining technique'.
/. din. Path. 12, 93
Grobbelaar,
B.G.
(1968).
'Transplacental
haemorrhage
in
Rh-haemolytic disease'. Br. Med. J. 2, 300
- and Dunning, E.K. (1969). Ά method for calculating the volume of
transplacental foeto-maternal haemorrhage'. Br. J. Haemat. 17,231
Gunn, F.D. and Mahle, A.E. (1938). 'Megakaryoblastic myeloma with
crystalline protein in the renal tubules — report of a case'. Archs.
Path. 26, 377
284
BIBLIOGRAPHY AND REFERENCES
Haden, R.L. (1940). Ά new instrument for the diffraction
measurement of the diameter of red blood cells'. / . Lab. clin. Med.
25, 399
Hall, J.G., Levin, J., Kuhn, J.P., Ottenheimer, E.J., van Berkum, K.A.P.
and McKusick, V.A. (1969). Thrombocytopenia with absent radius
(TAK)\ Medicine 4S, 411
Hall, R. and Losowsky, M.S. (1966). 'Distribution of erythroblast iron
in sideroblastic anaemia'. Br. J. Haemat. 12, 334
Hamilton, R.W., Schwartz, E., Atwater, J., and Erslev, A.J. (1971).
'Acquired haemoglobin H disease'. New Engl. J. Med. 285, 1217
Hardy, W.R. and Anderson, R.E. (1968). T h e hypereosinophilic
syndrome'. Ann. intern. Med. 68, 1220
Hayhoe, F.G.J. and Cawley, J.C. (1972). 'Acute leukaemia cellular morphology, cytochemistry and fine structure'. In Clinics
in Haematology. Acute Leukaemia. Volume I, No.l, p.49. Ed. S.
Roath. London; W.B. Saunders
- a n d Quaglino, D. (1958). 'Cytochemical demonstration and
measurement of leucocyte alkaline phosphatase activity in normal
and pathological states by a modified azo-dye coupling technique'.
Br. J. Haemat. 4, 375
and Doll, R. (1964). The Cytology and Cytochemistry of Acute
Leukaemia.: M.R.C. Special Report Series No. 304 H.M.S.O.
Heimpel, H. and Wendt, F. (1968). 'Congenital dyserythropoietic
anaemia with karyorrhexis and multinuclearity of erythroblasts'.
Helv. med. A eta 34, 103
Heller, P. (1970). T h e blood and blood forming organs'. Year Book of
Medicine, p.312. Chicago; Year Book Medical Publishers Inc.
Henderson, P.A. and Hillman, R.S. (1969). 'Characteristics of iron
utilisation in man'. Blood 34, 357
Herbut, P.A. and Erf, L.A. (1946). 'Lipoblastic and megakaryocytoid
multiple myeloma'. Am. J. clin. Path. 16, 13
Hillman, R.S. and Finch, C.A. (1967). 'Erythropoiesis. Normal and
abnormal'. Semin. Haemat. 4, 327
(1969) T h e misused reticulocyte'. Br. J. Haemat. 17, 313
Hobbs, J.R. (1971). 'Immunocytoma o' mice an' men'. Br. med. J. 2,
67
Holmes, B., Page, A.R. and Good, R.A. (1967). 'Studies of the
metabolic activity of leucocytes from patients with a genetic
abnormality of phagocytic function'. / . clin. Invest. 46, 1422
Huehns, E.R. (1968). 'Haemoglobins'. In Chromatographie
and
Electrophoretic Techniques. Second edition. Volume 2, p. 291. Ed. I.
Smith. London; Heinemann.
Hutchison, H.E. (1953). T h e significance of stainable iron in sternal
marrow sections - its applications in the control of iron therapy'.
Blood 8, 236
- ( 1 9 6 7 ) . An Introduction to the Haemoglobinopathies
and the
Methods Used for their Recognition, p.70. London; Edward Arnold.
285
THE PERIPHERAL BLOOD FILM
Isaacs, R. (1937). 'Lymphosarcoma cell leukaemia'. Ann. intern. Med.
11,657
Itano, H.A. and Pauling, L. (1949). Ά rapid diagnostic test of sickle cell
anaemia'. Blood 4, 66
Jacob, H.S. (1969). T h e defective red blood cell in hereditary
spherocytosis'. A. Rev. Med. 20, 41
— (1970). 'Mechanisms of Heinz body formation and attachment to
red cell membrane'. Semin. Haemat. 7, 341
— Ruby, A., Overland, E.S. and Mazia, D. (1971). 'Abnormal
membrane protein of red blood cells in hereditary spherocytosis'. /.
clin. Invest. 50, 1800
Jacobs, A. (1958). 'Staining for leucocyte peroxidase'. Lancet 1, 697
Jensen, W.N., Moreno, G.D. and Bessis, M.C. (1965). 'Electron
microscopic description of basophilic stippling iixred cells'. Blood 25,
933
Jordans, G.H.W. (1947). 'Hereditary granulation anomaly of the
leucocytes (Alder).' Acta med. Scand. 129, 348
— (1953). 'The familial occurrence of fat containing vacuoles in the
leucocytes diagnosed in two brothers suffering from dystrophia
musculorum progressera.' Acta med. Scand. 145, 419
Kaplow, L.S. (1963). 'Cytochemistry of leucocyte alkaline
phosphatase. Use of complex naphthol AS phosphate in azo-dye
coupling techniques.'Λm. J. clin. Haemat. 39, 439
- ( 1 9 6 5 ) . 'Simplified peroxidase stain using benzidine dihydrochloride'.
Blood 26, 215
Karnovsky, M.L., Simmons, S., Noseworthy, J. and Glass, E.A. (1970).
'Metabolic patterns that control the functions of leucocytes'. In
Formation and Destruction of Blood Cells, p. 215. Eds. T.J.
Greenwalt and G.A. Jamieson. Philadelphia, Pa.; J.B. Lippincott.
Karpatkin, S. (1969). 'Heterogeneity of human platelets'./, clin. Invest.
48, 1073
— (1972). 'Biochemical and clinical aspects of megathrombocytes.' In
Platelets and Their Role in Haemostasis. Ed. H.J. Weiss. Ann. N.Y.
Acad. Sei. 201, 262
Kass, L., (1968). A clockface chromatin pattern in the intermediate
megaloblast of vitamin B 1 2 or folate deficiency.' Blood 32, 711
Kaufman, R.M., Airo, R., Pollack, S. and Crosby, W.H. (1965).
'Circulating megakaryocytes and platelet release in the lung.' Blood
26, 720
Kay, H.E.M. (1971). 'Lymphocyte function.' Br. J. Haemat. 20, 139
Kilbridge, T.M. and Heller, P. (1969). 'Determinants of erythrocyte size
in chronic liver disease.' Blood 34, 739
Klebanoff, S.J. (1968). 'Myeloperoxidase-halide-hydrogen peroxide
antibacterial system.'/. Bact. 95, 2131
Kleihauer, E. (1966). Fetales Hämoglobin und Fetale Erythrozyten, p.
76. Stuttgart; Enke
- Braun, H. and Betke, K. (1957) 'Demonstration von fetalem
286
BIBLIOGRAPHY AND REFERENCES
Hämaglobin in den Erythrozyten eines Blutausstrichs.' : Klin. Wschr.
35,637
Lane, M. and Alfrey, C.P. (1965). 'The anaemia of riboflavin
deficiency.' Blood 25, 432
Li, C.Y., Yam, L.T. and Lam, K.W. (1970). 'Acid phosphatase
isoenzyme in human leucocytes in normal and pathological
conditions.'/. Histochem. Cytochem. 18,473
lichtman, M.A. (1970). 'Cellular deformability during maturation of
the myeloblast - Possible role in marrow egress.' New Engl. J. Med.
283,943
Lukes, R.J. 'The pathologic picture of the malignant lymphomas.' In
Leukaemic-Lymphoma.
Proceedings of the Fourteenth Annual
Clinical Conference on Cancer, p. 333. Ed. C J . Zarafonitis. Chicago;
Year Book Medical Publishers Inc.
McBride, J.A. and Jacob, H.S. (1970). 'Abnormal kinetics of red cell
membrane cholesterol in acanthocytes. Studies in genetic and
experimental abetalipoproteinaemia and in spur cell anaemia.' Br. J.
Haemat. 18,383
MacGregor, R., Scott G., Richards, W. and Loh, G.L. (1940). 'The
differential leucocyte count.' / . Path. Bact. 5 1 , 337
McKusick, V.A., Kaplan, D., Wise, D., Hanley, W.B., Suddarth, S.B.,
Sevick, M.E. and Maumanee, A.E. (1965). 'The genetic
mucopolysaccharidoses.' Medicine 44, 445
Marchesi, V.T. and Steers E. (Jnr.) (1968). 'Selective solubilization of a
protein component of the red cell membrane.' Science, Washington.
159,203
Matula, G. and Paterson, P.Y. (1971). 'Spontaneous in vitro reduction
of nitroblue tetrazolium by neutrophils of adult patients with
bacterial infection.' New. Engl. J. Med. 285, 311
Metcalf, D. and Moore, M.A.S. (1971). 'Haemopoietic cells'. In
Frontiers of Biology. Volume 24. Eds A. Neuberger and E.L. Tatum.
Amsterdam; North Holland Publishing Co.
Miller, S.E. (1966). Textbook of Clinical Pathology. Seventh Edition,
Baltimore; Williams and Wilkins
Mollin, D.L. and Hoffbrand, A.V. (1968). 'Sideroblastic anaemia.' In
Recent Advances in Clinical Pathology. Series V. p. 273. Ed. S.C.
Dyke. London; J. and A. Churchill
Murayama, M. (1964). Ά molecular mechanism of sickled erythrocyte
formation.' Nature, Lond. 202, 258
Murthy, M.S.N. and von Haam, E. (1958). 'The occurrence of the sex
chromatin in white blood cells of young adults.' Am. J. clin. Path.
30,216
Nierhaus, K. and Betke, K. (1968).'Eine vereinfachte Modifikation der
sauren Elution für die cytologische Darstellung von fetalem
Hämoglobin. ' Klin. Wschr. 46, 47
Nixon, K. and Olson, J.P. (1968). 'Diagnostic value of marrow
haemosiderin pattern.' Ann. intern. Med. 69, 1249
287
THE PERIPHERAL BLOOD FILM
Norberg, R. (1969) 'Neutrophil segmentation and radial segmentation.'
Scand. J. Haemat. 6, 274
- and Söderström, N. (1967). 'Radial segmentation' of the nuclei in
lymphocytes and other blood cells induced by some anticoagulants.'
Scand. J. Haemat. 4, 68
Osgood, E.E. (1935). 'Fenestration of nuclei of lymphocytes. A new
diagnostic sign in infectious mononucleosis.' Proc. Soc. exp. Biol.
Med. 33,218
Oski, F.A., Naiman, J.L., Blum, S.F., Zarkowsky, H.S., Whaun, J.,
Shohet, S.B., Green, A. and Nathan, D.G. (1969). 'Congenital
haemolytic anaemia with high-sodium and low-potassium red cells.'
New Engl. J. Med. 280, 909
Osoba, D. (1972). Thymic function, immunologie deficiency and
auto-immunity'. In Clinical Immunology, p. 319. Ed. J. Harris Med.
ClinsN. Am. 56, No. 2.
Park, B.H. (1971). 'The use and limitations of the nitroblue tetrazolium
test as a diagnostic aid.' /. Pediat. 78, 370
- and Good, R.A. (1970). 'NBT test stimulated'. Lancet 2, 616
- Fikrig, S.M. and Smithwick, E.M. (1968). 'Infection and nitrobluetetrazolium reduction by neutrophils. A diagnostic aid.' Lancet 2,
532
- Biggar, W.D., L'Espérance, P. and Good, R.A. (1972). 'NBT test on
moncytes of neutropenic patients'. Lancet 1, 1064'
Pearson, B. and Defendi, V. (1957). Ά comparison between the
histochemical demonstration of non-specific esterase activity by
5-bromoindoxyl acetate, a-naphthyl acetate and naphthol-AS
acetate'./. Histochem. Cytochem. 5, 72
Pedersen, B. and Hayhoe, F.G.J. (1971). 'Cellular changes in chronic
myeloid leukaemia'. Br. J. Haemat. 2 1 , 251
Perkins, R.P. (1971). 'Inherited disorders of haemoglobin synthesis and
pregnancy'. Am. J. Obstet. Gynec. I l l , 120
Perls, M. (1867). 'Nachweiss von Eisenoxyd in gewissen Pigmenten.
Vir chow s Arch. path. Anat. Physiol. 39, 42
Pijper, A. (1919). 'Diffraction phenomenon in films of blood cells'.
Med.JIS.Afr.
14,472
- (1929). 'Improved diffraction method for diagnosing and following
the course of pernicious and other anaemias'. Br. med. J. 1,635
- (1935). 'On measuring red blood cells; with special reference to new
diffraction apparatus'. Lancet 1, 1152
Plenderleith, I.HL (1970). 'Hairy cell leukaemia'. Can. med. assoc. J.
102, 1056
Pluznik, D.H. and Sachs, L. (1965). 'The cloning of normal "mast" cells
in tissue cultures'. / . cell. comp. Physiol 66, 319
Presentey, B. (1968). Ά new anomaly of eosinophil granulocytes'.^lm.
/ . din. Path. 49, 887
- (1969a). 'Cytochemical characterisation of eosinophils with respect
to a newly discovered anomaly'. A m. J. clin. Path. 51, 451
288
BIBLIOGRAPHY AND REFERENCES
-
(1969b). 'Morphologic observations and genetic follow-up of a
familial anomaly of eosinophils'. Am. J. clin. Path. 5 1 , 458
Pryce, D.M. (1929). Ά simplification of the "halo" method of measuring the diameter of red blood corpuscles'. Lancet 2, 275
Quaglino, D. and Flemans, R. (1958). Teroxidase staining in leucocytes'.
Lancet!, 1020
Ray, P.K. and Pinkerton, P.H. (1969). 'Leucocyte alkaline phosphatase.
The effect of age and sex'. Ada haemat. 42, 18
Rebuck, J.W. and Crowley, J.H. (1955). Ά method of studying leucocyte functions in vivo'. Ann. N. Y. A cad. Sei. 59, 757
- and van Slyck, E.J. (1968). 'An unsuspected ultrastructural fault in
human elliptocytes'. Am. J. clin. Path. 49, 19
Richards, D.F., Hunter, D.T. and Janis, B. (1969). 'Detection of
plasmodia by acridine orange stain'. Am. J. clin. Path. 51, 280
Richter, M. and Algom, D. (1972). 'The heterogeneity of lymphocytes'.
In Clinical Immunology, Ed. J. Harris. Med. Clins. N. Am. 56, No. 2
Riley, H.D. (1953). 'Acute infectious lymphocytosis'. New Engl. J.
Med. 248, 9?
Rippey, J.J. (1967). 'Leucopenia in West Indians and Africans'. Lancet
2,44
Rogers, L.E., Porter, F.S. and Sidbury, J.B. (1969). 'Thiamine
responsive mégaloblastic anaemia'. / . Pediat. 74, 496
Rohr, R.J. and Bond, W.H. (1953). 'The value of routine bone marrow
culture for Histoplasma capsulatum in paediatric haematology'.
Blood 8, 329
Roitt, I.M., Greaves, M.F., Torrigiani, G., Brostoff, J. and Playfair,
J.H.L. (1969). 'The cellular basis of immunological responses'.
Lancet 2, 367
Rosse, W.F. and Lauf, P.K. (1970). 'Effects of immune reactions on the
red cell membrane'. Semin. Haemat. 7, 323
Sawitsky, A., Rosner, F. and Chodsky, S. (1972). 'The sea blue
histiocyte syndrome. A review. Genetic and biochemical studies'.
Semin. Haemat. 9, 285
Schmidt, P.J. and Holland, P.V. (1972). 'Rhnull disease'. In Proceedings
of the Twelfth Congress of the International Society of Blood
Transfusion, Moscow, 1969, p.230. Ed. K. Stampfli. Bibl. Haemat.
38, Part 1
Schrek, R. and Donnelly, W. (1971). 'Cytology in lymphosarcoma cell
leukaemia'. Am. J. clin. Path. 55, 646
- Knopse, W.H. and Trobaugh, F.E. (1970). 'Chromatin and other
cytologie indices in chronic lymphocytic leukaemia'. / . Lab. clin.
Med. 75, 217
- Mayron, L.W. and Knopse, W.H. (1971). 'Quantitative electron
microscopy of normal and leukaemic lymphocytes'. Lancet 1, 348
Schur, P.H. (1970). Ά.Ν.Α.' New Engl. J. Med 282, 1205
Schubert,
J.C. and Schubert, H. (1969). 'Cytodiagnosis of
myelomatosis by the determination of adenosinetriphosphatase in
289
THE PERIPHERAL BLOOD FILM
the myeloma cells of the bone marrow'. (In German.) Blut 19, 78
Schwab, M.L.L. and Lewis, A.E. (1969). 'An improved stain for Heinz
'bodies'. Am. J. clin. Path. 5 1 , 673
Schwartz, D.L., Pierre, R.V., Scheerer, P.P., Reed, E.C. and Linman,
J.W. (1965). 'Lymphosarcoma cell leukaemia'. Am. J. Med. 38, 778
Schwartz, S.O. and Motto, S.A., (1949). 'The diagnostic significance of
"burr" red blood cells'. Am. J. med. Sei. 218, 563
Scott, R.B. (1957). 'Chronic lymphatic leukaemia'. Lancet 1, 1162
Seal, S.H. (1959). 'Silicone flotation: a simple quantitative method for
the isolation of free floating cancer cells from the blood'. Cancer,
Philad. 12,590
Serjeant, G.R., Serjeant, B.E. and Milner, P.F. (1969). 'The irreversibly
sickled cells; a determinant of haemolysis in sickle cell anaemia'. Br.
J. Haemat. 17, 527
Shaper, A.G. and Lewis, P. (1971). 'Genetic neutropenia in people of
African origin'. Lancet 2, 1021
Silverstein, M.N. and Ellefson, R.D. (1972). 'The syndrome of the
sea-blue histiocyte'. Semin. Haemat. 9, 299
Skoog, W.A. and Beck, W.S. (1956). 'Studies on the fibrinogen, dextran
and phytohaemagglutinin methods of isolating leucocytes'. Blood
11,435
Stavem, P., Hjort, P.F., Vogt, E. and van der Hagen, C.B. (1969).
'Ring-shaped nuclei of granulocytes in a patient with acute
erythroleukaemia'. Scand. J. Haemat. 6, 31
Stenton, P. (1959). 'Permanent sickle cell preparations'./, clin. Path.
12,484
Stohlman, F. (1967). 'Some aspects of erythrokinetics'. Semin.
Haemat. 4, 304
- Ebbe, S., Morse, B., Howard, D. and Donovan, J. (1968). 'Regulation
of erythropoiesis XX. Kinetics of red cell production'. Ann. N.Y.
A cad. Sei. 149, 156
Strouth, J.C., Zeman, W. and Merrit, A.D. (1966). 'Leucocyte
abnormalities in familial amaurotic idiocy'. New Engl. J. Med. 274,
36
Stuart, J. (1972). 'Disordered leucocyte proliferation in leukaemia'. Br.
med.J. 2, 152
— Bitensky, L. and Chayen, J. (1969). 'Quantitative enzyme chemistry
of leukaemic cells'./, clin. Path. 22, 563
Szmigielski, S., Litwin, J. and Zupanska, B. (1965). 'Cytochemical
differentiation of normal and neoplastic plasma cells'. /. clin. Path.
18,345
Tan, E.M., Schur, P.H. and Carr, R.I. (1966). 'Deoxyribonucleic acid
(DNA) and antibodies to DNA in the serum of patients with
systemic lupus erythematosus'./. clin. Invest. 45, 1732
Till, J.E. and McCulloch, E.A. (1961). Ά direct measurement of the
radiation sensitivity of normal mouse bone marrow cells'. Radiât.
Res. 14,213
290
BIBLIOGRAPHY AND REFERENCES
Trubowitz, S., Masek, B. and Frasca, J.M. (1971). 'Leukaemic
reticuloendotheliosis'. Blood 38, 288
Waldenström, J. (1970). Diagnosis and Treatment of Multiple Myeloma.
New York; Grune and Stratton
Wardrop, C. and Hutchison, H.E. (1969). 'Red cell shape in hypothyroidism'. Lancet 1, 1243
Washburn, A.H. (1928). Ά combined peroxidase and Wright's stain for
routine blood smears'./. Lab. clin. Med. 14, 246
Weed, R.I. (1970).'New thoughts on hereditary spherocytosis'. Med.
Coll. Virginia Q. 6, 50
Whittingham, S., Irwin, J., Mackay, I.R., Marsh, S. and Cowling, D.C.
(1969). 'Autoantibodies in healthy subjects'. Australas. Ann. Med.
18, 130
Windhorst, D.B., Holmes, B. and Good, R.A. (1967). Ά newly defined
X-linked trait in man with demonstration of the Lyon defect in
carrier females'. Lancet 1, 737
Wood, T.A. and Frenkel, E.P. (1967). 'The atypical lymphocyte'. Am.
J. Med. 42, 923
Woodrow, J.C., Clarke, C A . , Donohoe, W.T.A., Finn, R., McConnell,
R.B., Sheppard, P.M., Lehane, D., Russell, S.H., Kulke, W. and
Durkin, CM. (1965). 'Prevention of Rh-haemolytic disease. A third
report'. Br. Med. J. 1, 279
Yakulis, V.J. and Heller, P. (1964). 'An elution test for the visualisation
of haemoglobin-S in blood smears'. Blood 24, 198
Yam, L.T., Li, C.Y. and Crosby, W.H. (1971). 'Cytochemical
identification of monocytes and granulocytes'. Am. J. clin. Path. 55,
283
- - and Lam, K.W. (1971). 'Tartrate resistant acid phosphatase
isoenzyme in the reticulum cells of leukaemic reticulo-endotheliosis'.
New Engl. J. Med. 284, 357
— - and Fink el, H.E. (1972). 'Leukaemic reticuloendotheliosis. The
role of tartrate resistant acid phosphatase in diagnosis and
splenectomy in treatment. Archs intern, Med. 130, 248
Yoffey, J.M. and Courtice, F.C. (1970). Lymphatics, Lymph and the
Lymphomyeloid Complex. London; Academic Press
Zacharski, L.R. and Linman, J.W. (1969). 'Chronic lymphocytic
leukemia versus chronic lymphosarcoma cell leukemia. Analysis of
496 cases.' Am. J. Med. 47, 75
Zarkowsky, H.S., Oski, F.A., Sja'afi, R., Shohet, S.B. and Nathan, D.G.
(1968). 'Congenital
haemolytic anaemia with high-sodium,
low-potassium red cells'. New Engl. J. Med. 278, 573
van der Zee, S.P.M., Schnetlem, E.D.A.M. and Monnens, L.A.H. (1968).
'Megaloblastic anaemia in the Lesch-Nyhan syndrome'. Lancet 1,
1427
Zeman, W. and Strouth, J . C (1965). 'Leucocytic hypergranulation
versus lymphocytic vacuolisation as markers for hétérozygotes and
homozygotes with Batten-Spielmeyer-Vogt disease'. In Inborn Errors
291
THE PERIPHERAL BLOOD FILM
of Sphingolipid Metabolism, p. 475. Eds S.M. Aronson and B.M.
Volk. New York; Pergamon Press
Zeya, H.I. and Spitznagel, H.K. (1968). 'Arginine-rich proteins of
polymorphonuclear leucocyte lysosomes. Antimicrobial specificity
and biochemical heterogeneity'. /. exp. Med. 127, 927
292
Index
Acanthocytes, 3 8 , 4 7
laboratory guide, 219
Acanthocytosis, 137
Acetate buffer, 259, 263
Acetate esterases, 12
Acid elution reaction, 10, 270
Acid phosphatase reaction, 262
Acridine orange fluorescent technique, 249
Acridine orange solution, 249
Addison's disease, 221
Adrenal disorders, blood film in,
221
Agammaglobulinaemia, 20
blood film in, 221
Agnogenic myeloid metaplasia,
10,49, 137,221
Agranular platelets, 58
Agranulocytosis, substances causing, 278
Alcoholism, 89, 133,222
stomatocytes in, 41
Alder-Reilly granules, 57, 58
leucocytes, in, 71
lymphocytes, in, 67
monocytes, in, 64
neutrophils, in, 61
differential diagnosis, 147,
190
Alkaline phosphatase reaction,
260
Allergy, 194
basophil function in, 29
eosinophilia, 194
Alpha-naphthyl acetate esterase
reaction, 257
Alpha-naphthyl phosphate technique, 260
Amaurotic familial idiocy (see
Tay-Sachs disease)
Anaemia, 9
aplastic, 14, 222
acquired, 10
erythroblasts in, 88
substances causing, 277
tear-drop cells in, 49
chronic disorders, in, 132, 134,
167
differential diagnosis, 155, 158,
163, 172, 176, 178, 184,
190
film appearance, 132
haemolytic, 9, 88, 231
acquired, 181
auto-immune, 62, 65, 223
G6PD deficiency, 226
differential diagnosis, 160,
162
erythrophagocytosis in, 62
haemoglobinopathy in, 23
Heinz bodies in, 16, 53
laboratory diagnosis, 205
substances causing, 226, 275
haemorrhagic, 134
differential diagnosis, 158
laboratory diagnosis, 205
Heinz body, 175,226
iron deficiency, 9, 134, 234
differential diagnosis, 168
pregnancy, in, 240
293
THE PERIPHERAL BLOOD FILM
Blast cells - cont.
morphological changes in, 78
Blister cells, 3 8 , 4 6
Blood, description of, 1
Blood cells, 1, {see also specific
types)
colour of, 2
concentration techniques, 4
distribution in films, 117
life span, 1
normal, 21
precursors of, 1
types of, 21 {see also specific
types)
Blood films, 117
abnormal, 126
appearance of, 118
cell counts outside normal ranges,
126
definition, 117
examination of, 118
checklist, 119
normal, 122, 123
adult, 124
child, 124
Bacteriolysis by neutrophils, 27
neonatal infant, 125
Band's disease, 223
Blue platelets, 58, 73
Barr bodies, 25
Basophilia, laboratory diagnosis, Bone cells, 111, 113
Bone marrow
208
eosinophil pools, 28
Basophilic granules, leucocytes
erythropoiesis in, 80
abnormal, 147
haemosiderin in, 203
normal {see Basophils)
lymphatic cells in, 107
red cells {see Erythrocyte, puncmyelofibrosis of {see Agnogenic
tate basophilia in)
myeloid metaplasia)
Basophilic normoblasts, 80, 81
neutrophil PMN pools in, 27
Basophils, 29, 95
plasmacytosis of, 71
cytochemical enzyme activity
pluripotent stem cells in, 76
in, 26
reticulin in, 204
cytochemical reactions, 29
thrombopoiesis in, 102
differential diagnosis, 151, 195
Bone marrow aspirate, 203
functions, 29
Brilliant green/neutral red techmorphology, 29
nique, 268
Batten-Spielmeyer-Vogt
disease,
Brilliant green solution, 268
67,235
Bromoindoxyl acetate esterase reBence-Jones protein, 151
action, 259
Blast cells, 1
'Buhot'cell, 58,71
general characteristics, 78
Anaemia - cont.
megaloblastic, 133, 137, 139,
160,237
substances causing, 275
nutritional, 239
pathogenesis of, 127
pernicious, 133
diseases associated with, 164
reticulocyte count in, 16, 82
sickle cell, 13 {see also Sickle cell)
blister cells in, 46
sideroblastic, 9, 50, 88, 89, 9 1 ,
136, 160, 172,242
differential diagnosis, 173
red cells in, 39
secondary, 90
substances causing, 277
Anisocytosis, 132
Antinuclear factor, 63
Ascorbic acid deficiency, 245
Auerrod, 99, 102, 143
294
INDEX
Burkitt's lymphoma, 69
Burns, 159
blood film in, 223
stomatocytes in, 42
Burr cell, 3 8 , 4 7 , 4 8
differential diagnosis, 175
Carcinoma, metastatic, 87, 98,
105
Cell diameters, measurement of,
122
Cellular immunity, laboratory
tests, 212
Chediak-Higashi-Steinbrinck anomaly, 57, 5 8 , 6 1 , 6 4 , 1 4 7 , 1 9 0
lymphocytes, in, 67
neutrophils, in differential diagnosis, 147, 190
Chediak-Higashi-Steinbrinck syndrome, 2 0 , 2 2 4
Chemicals, haemotoxic effects of,
275
Chromosomal aberrations, haemoglobin levels in, 10
Citrate buffer, 262
Collagen disease, 14, 88, 181,
188,224
Collagen fibres, 112
Colony-forming unit-culture, 76
Colony-forming unit-spleen, 76
Colony-stimulating factor, 77
Combined esterase reaction, 258
Cottage-loaf (dumb-bell) cells, 38,
49
Cryoglobulinaemia, 20
differential diagnosis, 181
Cushing's disease, 221
Cytochemical staining, 2, 7
Cytoplasmic granules, staining, 6
Cytoplasmic haemoglobin concentration, 44, 80
Deoxyribonucleic acid (DNA)
Deoxyribonucleic acid (DNA) - cont.
demonstration by Feulgen reaction, 8
synthesis
enzyme abnormalities interfering with, 166
inhibition, 44
normoblasts, in, 80
vitamin Bi 2 and folate in, 91
Di Guglielmo's syndrome, 9, 10,
86,88,89,91,114,128,129,
136, 143, 144, 1 4 7 , 2 2 5 - 2 2 6
haemoglobin in, 16
laboratory diagnosis, 211
malignant erythroblasts in, 93
myelocytes in, 99
red cells in, 39
Disseminated intravascular coagulation
differential diagnosis, 159
schistocytes in, 47, 49
tests, 205
Dohle (Amato) bodies, 57
diagnosis, in, 141
neutrophils, in, 61
differential diagnosis, 148,
191
Drugs, haemotoxic effects of, 275
Drug therapy, nitroblue tetrazolium reduction test in, 20
Dumping syndrome, 240
Dye substrate mixture, 260
Dysproteinaemias,
differential
diagnosis, 181
Echinocytes {see Erythrocytes,
crenated)
Elliptocytosis, 44, 128
differential diagnosis, 174
laboratory tests, 208
Emperipolesis, 106
Endothelial cells, 111, 113
Enzymes in red cells, 24
Eosinophilia
absolute, differential diagnosis,
150, 193-195
295
ΓΗΕ PERIPHERAL BLOOD FILM
Eosinophilia - cont.
Erythrocyte(s) - cont.
diseases causing, 195
diagnosis, 208
laboratory tests, 208
concentrating, 5
Eosinophils, 2 8 - 2 9 , 95
crenated, 3 8 , 4 6 , 4 7
dimorphic, laboratory diagAlder-Reilly granules in, 61
nosis, 208
cytochemical enzyme activity,
electrolyte imbalance, 160
26
elliptocytic, 127
cytochemical reactions, 28
diagnosis, in, 136, 174
granules in, 28
erythroblastic, 127
hypogranular, 60
differential diagnosis, 139,
morphology, 28
178
nuclear appendages, 28
fragmentation of, 47, 48
pools, 28
differential diagnosis, 175
Eosin solution, 251, 254, 272
function, 24
Epstein-Barr virus antibody, 69,
Heinz bodies in, 38, 51
149
differential diagnosis, 138,
Erythroblastaemia laboratory tests,
177
208
formation of, 52
Erythroblastosis abnormal, 86
Howell-Jolly bodies in, 38, 49,
Erythroblasts
127,136,138
abnormal, classification, 87
laboratory tests, 209
binucleate and multinucleate, 88
hypochromic, 38
fluorescent, 91
hypochromic microcytic, diagHowell-Jolly bodies in, 89
nosis, in, 134, 168-169
inclusions in, 89
malignant, 93
laboratory tests, 209
Pappenheimer bodies in, 89
hypochromic
microcyticP.A.S. reaction in, 9
macro-ovalocytic,
vacuolated, 89
diagnosis, in, 135, 169—171
Erythrocyte(s), 2 1 - 2 4 , 124
laboratory tests, 210
abnormal, 3 7 - 5 6
hypochromic normocytic, diagnosis, in, 134, 167
classification, 37
immature, 139,
film appearances, 127, 131
differential diagnosis, 178
fragmentation of, 47
inclusions in, diagnosis, in, 138,
inclusions in, 49
176
shape, 44
iron incorporation in, 84
size, 3 7 , 4 3
iron turnover, 87
staining, 37, 38
irregular margins, with, 45
aggregated, differential diagirregular poikilocytic, diagnosis,
nosis, 1 3 9 , 1 7 9 - 1 8 1
in, 137, 175
anisochromic-dimorphic, diaglarge, 43
nosis, in, 1 3 6 , 1 7 2 - 1 7 3
leptocytic, 127
auto-agglutination, 127
life-span, 24
differential diagnosis, 140,
malaria parasites in, 38, 53
181
microcytic, 127
laboratory diagnosis, 207
micro-macro-ovalocytic, 127
basophilic stippling, laboratory
296
INDEX
Erythrocyte(s) - cont.
morphology, 21
normochromic
macrocytic,
laboratory diagnosis, 216
normochromic macro-ovalocytic,
diagnosis, in, 133, 1 6 3 - 1 6 6
laboratory diagnosis, 216
normochromic
microcytic,
diagnosis, in, 132, 158
normochromic
normocytic,
diagnosis, in, 131, 155, 216
normochromic round macrocytic, diagnosis, in, 132,
158-163
normochromic
stomatocytic,
diagnosis, in, 133, 167
normocytic, 127
outside normal range, 126
oval shaped, 124
Pappenheimer bodies in, 38,
49,138
poikilocytic, 127
polychromatic, 127
production pathways, 78
punctate basophilia in, 38, 50
rouleaux, 127
differential diagnosis, 139,
179-181
laboratory diagnosis, 217
round and oval macrocytic, 127
'sea-urchin' type, 46
sickle cell type, 17, 127
diagnosis, in, 137, 174
siderocytic, 127
diagnosis, in, 138, 176
Skoog and Beck's sedimentation method, 5
small, 43
smooth margins, with, 44
spherocytic, 127
diagnosis, in, 137, 174
spinous
classification, 47
laboratory diagnosis, 218
stippled cell type, 127
differential diagnosis, 138,176
stomatocytic, 127
Erythrocyte(s) - cont.
stomatocytic - cont.
laboratory diagnosis, 219
Erythrocyte sedimentation rate,
139
Erythrocytosis, 240
Erythroid hypoplasia, 87
Erythrophagocytosis, 57, 58, 62
monocytes, in, 65
Erythropoiesis, 80—93
abnormal cells, 86
depression of, differential diagnosis, 157
ineffective, 86, 127
megaloblastic, 91
normal cells, 80
normoblastic, 80
stem cell abnormalities, 8 6 - 8 8
Erythropoietic hypoplasia
differential diagnosis, 157
laboratory diagnosis, 204
Erythropoietin, 7 7 , 8 0
controlling haem synthesis, 84
impaired production of, 87
increased production^ 86
Esterase enzymes reactions, 11
Evans' syndrome, 226
Examination of blood films, 118
checklist, 119
Fanconi syndrome, 10
Fat cells, 111, 112
Felty's syndrome, 225
Female sex chromatin, 25
Feulgen reaction, 8, 251
Greig's substitute, 252
Fibroblasts, 111, 112
Field's technique, 250
Filariasis, 120
Fixation of blood films, 5
Flagellated cells, 70
Foetomaternal transplacental haemorrhage, volume of, calculation of, 271
Folate
DNA synthesis, in, 91
297
THE PERIPHERAL BLOOD FILM
Folate - cont.
Haem - cont.
deficiency, 44, 97, 105, 136,
synthesis, 83
163,240,245
impaired, 39, 50, 160, 168
differential diagnosis, 165
Haematology profile, 202
laboratory diagnosis, 207
Haematoxylin
solution,
253,
Folate enzyme abnormalities, 166
261
Haemochromatosis, 9, 90
Haemoglobin
abnormal, 23
Gammopathy, 140
concentration in red cell, 22,
differential diagnosis, 179
43
monoclonal, 179
crystallizing, 227
polyclonal, 180
cyanotic, 228
Gaucher cells, 111, 114
cytoplasmic concentration, 80
Gaucher's disease, 235
formation of molecule, 85
Giemsa's stain, 6, 7, 246
globin chain production, 83
dilute, 248, 250
abnormal, 39, 168
Gigantoblasts, 88
nomenclature, 22
Glandular fever (see Infectious
polycythaemic, 228
structure, 22
mononucleosis)
synthesis, 80, 83
Glanzmann's thrombasthenia, 199,
disorders of, 1 0 , 5 0 , 8 9
200
unstable, 51, 230
Globin chain synthesis, 83
detection of, 206, 269
abnormal, 39, 168
Glucose 6-phosphate dehydro- Haemoglobin Bibba, 51
Haemoglobin Bronx-Riverdale, 51,
genase deficiency, 20, 51, 226
53
Glutathione instability, 47, 51
Haemoglobin C disease, 136, 227
Glycogen storage diseases, 191
elliptocytes in, 45
Gout, 14
Haemoglobin C trait, 227
Graham-Knoll technique, 255
Haemoglobin F (foetal), 10, 22
Granulocytes
acid elution test for, 270
abnormalities, 5 9 - 6 3
postnatal elevation of, 10
cytoplasmic, 57, 60
reappearance of, 10
nuclear, 57
nucleocytoplasmic, 57
Haemoglobin Gower 2, 22
Haemoglobin Gun Hill, 51
disrupted, 57, 63
Haemoglobin H, 16
May-Hegglin anomaly in, 61
staining for, 269
Pelger-Huët anomaly, 59
Granulomatous disease of child- Haemoglobin H disease, 50
hood, 114
film appearance, 135
Granulopoiesis (see Myelopoiesis) Haemoglobin Köln, 51
Grave's disease, 243
Haemoglobin M, 23, 177
Gumprecht shadow, 68
Haemoglobin M disease, 228
Haemoglobin M trait, 228
Haemoglobin Norfolk, 51
Haemoglobin Philly, 5 1 , 5 3
Haem, 23.
Haemoglobin Rainier, 228
298
INDEX
Haemoglobin S, cells containing,
45,47
tests for, 17, 272,273
Haemoglobin S disease, 136, 137,
227 {see also Sickle cell disease)
Haemoglobin Sabine, 51
Haemoglobin Zurich, 51
Haemoglobinopathies, 23
blood film in, 2 2 7 - 2 3 0
burr cells in, 47
differential diagnosis, 160, 172,
174,177
laboratory diagnosis, 209
spherocytes in, 42
target cells in, 135
Haemoglobinuria, chronic, 168
Haemolysis, 127
laboratory diagnosis, 204
Haemolytic anaemia hereditary,
differential diagnosis, 160
Haemolytic disease,
acquired, differential diagnosis,
160
of newborn, 230
Haemopoiesis, 7 4 - 7 9
compartments, 74
functional cell, 79
poietic (differentiated), 77
stem cell, 74
ineffective, 187
Haemopoietic cells, acetate esterase activity in, 12
Haemorrhage
blood film in, 230
iron deficiency in, 134
Haemorrhagic anaemia
differential diagnosis, 158
laboratory diagnosis, 205
Haemosiderin in bone marrow,
quantitation of, 203
Haemosiderosis, 90
Hairy cells, 68, 70, 129, 145, 150,
263
Ham's test, 88
Heart disease, congenital, 19
Heinz bodies
erythrocytes, in, 38, 51
Heinz Bodies - cont.
erythrocytes, in - cont.
differential diagnosis, 138,
177
formation of, 52
staining, 15, 1 6 , 2 6 8 , 2 6 9
HemalogD, 120
Hepatitis, infective, 233
Hereditary abetaliproteinaemia, 47
Hereditary elliptocytosis, 45, 231
Hereditary haemorrhagic telangiectasia, 136
Hereditary lipidoses, 191
Hereditary spherocytosis, 42, 137,
231
Hexazotized new fuchsin solution,
256
Hexazotized pararosanilin solution, 257
Hiatus hernia, 231
Histiocytes, 111, 112, 113
foamy, 67
phosphatase activity in, 13
sea-blue, 111, 113
Histiocytosis X, 193
Hodgkin's disease, 8, 114, 231
LAP in, 13, 14
monocytes in, 64
Paul-Bunnell test in, 69
Reed-Sternberg cells in, 115
Howell-Jolly bodies
erythroblasts, in, 89
erythrocytes, in, 38, 49, 127,
136,138
laboratory tests, 209
megaloblasts, in, 92
normoblasts, in, 82
Hurler-Hunter syndrome, 238
Hurler's syndrome, 114
Hyperadrenalism, 221
Hyperbilirubinaemia, 133
differential diagnosis, 162
Hypercholesterolaemia, 115
Hyperchylomicronaemia, 115
Hypereosinophilia, differential diagnosis, 150,195
Hyperfibrinogenaemia, 179
299
THE PERIPHERAL BLOOD FILM
Hyperglobulinaemia
Iron - cont.
differential diagnosis, 179
deficiency - cont.
laboratory diagnosis, 218
pregnancy, in, 240
Hyperimmunoglobinaemia, 151,
incorporation in erythrocytes,
196
84
Hyperlipoproteinaemia, 114
metabolism, abnormalities of,
Hypersensitivity disorders, 193
39
Hypersplenism, 88, 162, 242
plasma, in, 85, 87
differential diagnosis, 188
Irradiation, 67, 234
Hyperthyroidism, 243
Hypo-adrenalism, 221
Hypo-immunoglobulinaemia, 18 2
Hypophosphataemia, hereditary, Jaundice
obstructive, target cells in, 40
13
unconjugated hyperbilirubinaeHypothyroidism, 243
mia, 162
Jenner's stain, 6, 7, 246
Job's syndrome, 19
Immunity, lymphocyte, role of, Jordans' anomaly, 60
32
Immunodeficiency diseases, 141
181,182
Immunoglobulins,
classes of, 35
plasma cells, in, 35
Immunoglobin heavy chain disease, 232
Immunological reactions, platelets
in, 36
Infections
basophilia in, 195
blood films in, 232
lymphocytosis in, 189
monocytosis in, 192
neutrophilia in, 183
plasmacytosis in, 195
splenomegaly in, 187
Infectious lymphocytosis, 233
Infectious mononucleosis, 14, 68,
149, 193,233
laboratory diagnosis, 214
Iron
cytochemical staining, 9, 254
deficiency, 134,135
blood film in, 234
differential diagnosis, 168
haemorrhage causing, 134
300
L.E. cells, 62
Lead poisoning, 138, 235
laboratory tests, 210
red cells in, 50
Lecithin-cholesterol acyl transferase (LCAT), 40, 43
Leishman staining, 6, 7, 247
Leptocytes (see Target cells)
Leptocytosis, 135, 172
Leucocytes
abnormalities, SI—12
classification, 57
cytoplasmic, 57
differential diagnosis, 140
nuclear, 57
nucleocytoplasmic, 57
agglutination, 140
Alder-Reilly granules in, 57
alkaline phosphatase in, 13
Chediak-Higashi-Steinbrinck
anomaly, 57
concentration techniques, 5
differential count, 120
Dohle (Amato) bodies, 57
identification of, 119
May-Hegglin anomaly, 57
INDEX
Leucocytes - cont.
Pelger-Huët anomaly, 57, 129
twinning deformity, 57
Leucocytosis, 14, 118, 129
differential diagnosis, 147-151
Leuco-erythroblastaemia, laboratory tests, 210
Leucopenia, 118
Leukaemia, 128,235
acute, laboratory diagnosis, 210
acute myeloid, agranular neutrophils in, 60
chronic lymphocytic, 146
chronic lymphosarcoma cell,
diagnosis, 145
disrupted granulocytes in, 63
eosinophilic, 129
differential diagnosis, 150
hairy cell, 129, 145, 150, 212,
263
hypogranular polymorphs in,
60
laboratory diagnosis, 210
lymphatic, 66
lymphoblastic, 10, 14, 109,
129
lymphocytic, 8, 13
laboratory diagnosis, 211
lymphocytes in, 67
Paul-Bunnell test in, 69
lymphosarcoma cell, laboratory
diagnosis, 211
monoblasts in, 102
monocytic, 99, 102
myeloblastic, 97, 129, 143, 146
myelocytic (granulocytic), 10,
14,97, 114, 115
differential diagnosis, 142
laboratory diagnosis, 211
myeloid, 13
neutrophils in, 60, 63
myelomonocytic, 13, 63, 77,
102, 129
agranular neutrophils in, 60
differential diagnosis, 149
laboratory diagnosis, 211
monocytes in, 64, 65
Leukaemia - cont.
myelomonocytic - cont.
neutrophils in, 60
paramyeloblastic, 59,129, 143
Philadelphia chromosome-negative myelocytic, 63
plasma cell, 129, 151
laboratory diagnosis, 211
promyelocytic, 99, 142
laboratory diagnosis, 212
substances causing, 279
Leukaemic reticulo-endotheliosis,
129, 145, 150,263
cell, 5 8 , 6 5 , 6 9 , 111, 115
laboratory diagnosis, 212
Leukaemoid reactions, laboratory
diagnosis, 212
Lipidoses, 191, 2 3 5 - 2 3 6
Lipochrome histiocytosis, 20
Liver
cirrhosis, 224
disease
erythroblasts in, 88
stomatocytes in, 41
target cells in, 135
Lupus erythematosus
discoid, 62
systemic, 62, 225
Lymphoblasts, 1, 78
cytochemical reactions, 100
leukaemic, 109
morphology, 108
Lymphocytes, 3 1 - 3 4 , 197
abnormal, 58, 66
film appearance, 128
Alder-Reilly granules, 58, 67
atypical, 124
differential diagnosis, 148,191
B , 3 2 , 78
in bone marrow, 76
characteristics, 33
formation, 107
Chediak-Higashi-Steinbrinck
anomaly, 58, 67
classes of, 32
cytochemical enzyme activity
in, 26
301
THE PERIPHERAL BLOOD FILM
Lymphocytes - cont.
cytochemical reactions, 32
disrupted, 68
flagellated, 70
functions, 32
large, 32
malignant, 67
loss of, 130
malignant, 67
morphology, 31
notched nucleus, 58, 66, 129
differential diagnosis, 148,191
outside normal range, 126
Pelger-Huet anomaly, 58, 66
peripolesis and emperipolesis,
106
radial segmentation in, 66, 191
small, 31
malignant, 67
T,32,76
characteristics, 33
origin of, 76
pre-, 108
production, 107
twinning deformity, 58, 67,
191
vacuolation of cytoplasm, 67
differential diagnosis, 148,
191
Lymphocytoid, mononucleosis
cell, 68
Lymphocytopenia
laboratory diagnosis, 212
pathogenesis, 130
secondary, 182
Lymphocytosis, 128
absolute, differential diagnosis,
145,189
infectious, 145
laboratory tests, 213
relative, differential diagnosis,
144,185
Lymphokine factors, 33
Lymphoma, 106, 141
Lymphopoiesis, 107—109
abnormal, 108
normal, 108
302
Lymphopoiesis - cont.
primary, 107
secondary, 108
thymic, 107, 108
types of, 107
Lymphosarcoma, 8, 13
Lymphosarcoma cells, 109, 145
Lysosomes in neutrophils, 26
Lysozyme, 30, 63, 65
Macrocytes
oval, 44
round, 43
Macrocytosis, differential diagnosis, 172
Macrophages, 30
characteristics, 31
'fixed', 111,112
functions, 30
Macroplatelets, 58, 72
Macropolycyte, 59
Malabsorption syndrome, 165
differential diagnosis, 170
laboratory diagnosis, 213
Malaria, 4, 5, 120,236
erythrocytes in, 53
staining for parasites, 248
Malnutrition, 168, 169
Mast cells, 29, 111, 112
May-Grünwald-Giemsa staining, 6,
7,247
May-Hegglin anomaly, 57, 73
granulocytes, in, 61
monocytes, in, 64
neutrophils, in,
differential
diagnosis, 147, 191
Mean corpuscular average thickness of red cell, 21
Mean corpuscular diameter of red
cell, 21, 122
Mean corpuscular haemoglobin
concentration, 21, 123
Mean corpuscular volume, 122, 123
Measles, 19
Megakaryoblasts, 1, 78, 102
INDEX
Megakaryoblasts, - cont.
morphology, 104
Megakaryocytes, 102, 131
abnormal, 106
hypoplasia of, 131
morphology, 104
Megaloblastosis, 40, 44, 88, 135
laboratory diagnosis, 206
Megaloblasts, 91, 92
Megathrombocytes, 72, 124
Megathrombocytosis, differential
diagnosis, 153, 201
Metamyelocytes, 94, 96, 98
Metastatic carcinoma cells, 111,115
Methaemoglobin, 24
Methaemoglobinaemia
differential diagnosis, 138, 157,
177
laboratory diagnosis, 214
substances causing, 276
Méthylène blue solution, polychromed, 250
Methyl green solution, 260
buffered, 257
Methyl violet technique for Heirtz
bodies, 268
Micro-angiopathy, 237 (see also
Disseminated intravascular coagulation)
burr cells in, 48
laboratory diagnosis, 214
Microplatelets, 58, 73
Microthrombocytes, 73, 152
Microthrombocytosis, differential
diagnosis, 153, 201
Monoblastoid, 68
Monoblasts, 1,78
cytochemical reactions, 100
leukaemic, 102
morphology of, 101
Monocytes, 29—31
abnormalities, 58
Alder-Reilly granules, 58, 64
characteristics, 31
Chediak-Higashi-Steinbrinck
anomaly, 58, 64
cytochemical enzyme activity
Monocytes — cont.
in, 26
cytochemical reactions, 30
disrupted, 58, 66
erythrophagocytosisby, 65
functions, 30
identification, 12
life-span, 30
malignant, 65, 144
May-Hegglin anomaly in, 61, 64
morphology, 29
necrobiotic, 66
Pelger-Huèt anomaly, 58, 64
pools of, 30
prominent in films, 129
segmented nucleus, 64
vacuolation of cytoplasm, 64
Monocytosis
differential diagnosis, 148, 192
laboratory diagnosis, 214
Mononuclear cells, atypical, 68
Mononucleosis, differential diagnosis, 149,193
Mononucleosis cells, 68
Monopoiesis, 1 0 1 - 1 0 2
abnormal, 102
normal, 101
Morquio's syndrome, 238
Mucopolysaccharidoses
genetic, 238
differential diagnosis, 190
Mumps, 72
Muramidase (see Lysozyme)
Mycosis fungoides, 238
Myeloblasts, 1 , 7 8 , 9 4 , 9 5 , 9 6
cytochemical reaction, 100
malignant, 99
Myelocyte, 94, 96, 124
leukaemic, 99
Myelofibrosis, 9, 14
Myeloma cells, 110
Myelomatosis, 71, 110, 151,238
laboratory diagnosis, 214
Myeloperoxidase deficiency, 19
Myelopoiesis
(granulopoiesis),
94-100
abnormal cells, 97
303
THE PERIPHERAL BLOOD FILM
Myelopoiesis - cont.
ineffective, 97
malignant, 98, 99
morphology of cells, 96, 98
normal cells, 94
Myocardial infarction, 14
Myxoedema, 243
Naegeli type cell, 102
Naphthol AS-BI phosphate solut i o n n a i , 263
Naphthol AS-BI phosphate technique, 261
Naphthol
AS-D
chloroacetate
esterase reaction, 256
Neutral red solution, 268
Neutropenias
differential diagnosis, 144
laboratory diagnosis, 215
pathogenesis, 130
substances causing, 278
Neutrophil(s), 2 5 - 2 8 , 95, 97, 124
agranular, 60
Alder-Reilly granules in, 61
basophilic granules in, differential diagnosis, 147,190
Chediak-Higashi-Steinbrinck
anomaly in, 61
cytochemical reactions, 26
diminished production of, 130
differential diagnosis, 185
Dohle (Amato) bodies in, 61
differential
diagnosis, in,
148,191
function, 27
granules in, 26
half-life, 27
hypersegmented, 59
differential diagnosis, 147,
190
hypogranular, 60
identification, 12
ingested red cells in, 62
leuco-erythroblastic type, differential diagnosis, 142, 184
304
Neutrophil(s) - cont.
leukaemoid type, differential
diagnosis, 141, 184
malignant, 63
phosphatase activity in, 13
May-Hegglin anomaly in, differential diagnosis, 147, 191
morphology, 25
necrobiotic, 63
nitroblue tetrazolium reduction test, 17
nuclear appendages, 25
Pelger-Huët anomaly, 59
differential diagnosis, 147,189
pelgeroid, 59
differential diagnosis, 147,189
phagocytosis and bacteriolysis
by, 27
phosphatase activity in, 13
pools of, 27
Stodtmeister, 59
toxic granules in, 60
twinning deformity, 59
vacuolation of cytoplasm, 60
Neutrophilia, 128
laboratory diagnosis, 216
absolute, 141, 183
relative, 140, 181-183
Nicotinic acid deficiency, 244
Niemann-Pick cell, 67, 111, 115
Niemann-Pick's disease, 60, 114,
115,235
Nitroblue tetrazolium reduction
test, 17,264
Nitroblue tetrazolium stock solution, 264, 265
Normoblasts, 80
developmental stages, 80
Howell-Jolly bodies in, 82
morphology of, 81
Nuclear chromatin, staining of, 6
Orthochromatic normoblasts, 80,
81
Osteoblasts, 111, 113
INDEX
Osteoclasts, 111, 113
Oxygen transport, abnormal, 23
Pancytopenia
differential diagnosis, 186
laboratory diagnosis, 216
substances causing, 277
Pappenheimer bodies
erythroblasts, in, 89
erythrocytes, in, 38, 49, 138
Pappenheimer's panoptic method,
7
Par a-ery thro blasts, 93
Paramyeloblast, 99
Paramyeloblastic leukaemia, 143
Parasites
malarial, 53, 236
splenomegaly caused by, 187
Paroxysmal nocturnal
haemoglobinuria, 10, 13, 62, 65, 161,
239
laboratory diagnosis, 216
Paul-Bunnell antibody, 69, 193
Pelger-Huèt anomaly, 57, 58, 239
leucocytes, in, 129
lymphocytes, in, 66
monocytes, in, 64
Pelgeroid anomaly, 63, 141
Periodic acid-Schiff (PAS) reaction, 8, 253
Peripolesis, 106
Peroxidase reaction, 11, 255
Phagocytosis, 27
Philadelphia chromosome-negative
myelocytic leukaemia, 63, 142
Phosphatases, 13
reactions, 2 6 0 - 2 6 3
Phosphate buffer, 264, 271, 272
Phosphate-citrate
buffer
technique, 271
Phospholipids, platelets, in, 35
Plasma, 1
Plasmablasts, 1,78, 110
malignant, 110
Plasma cells, 3 4 - 3 5 , 110
Plasma cells - cont.
abnormality, 5 7 - 7 2
classification, 57
cytoplasmic, 57
nuclear, 57
nucleocytoplasmic, 57
'Buhot', 58
cytochemical enzyme activity
in, 26
cytochemical reactions, 34
flaming, 58, 71
immunoglobulins in, 35
malignant, 5 8 , 7 2 , 110
morphology, 34
outside normal ranges, 126
phagocytic, 58, 72
Russell bodies, 71
Turk irritation cell, 70
Plasma cell leukaemia, 129, 151
laboratory diagnosis, 211
Plasmacyte {see Plasma cells)
Plasmacytoid lymphocyte, 68, 70
Plasmacytosis
differential diagnosis, 151, 195
laboratory diagnosis, 217
non-malignant, 71
Plasmapoiesis, 110—111
Plasmodium falciparum, 53, 236
Plasmodium malariae, 53
Plasmodium ovale, 53
Plasmodium vivax, 53
Platelets, 3 5 - 3 6
abnormal, 58, 72, 131, 151
agranular (blue), 58, 73
atypical, differential diagnosis,
153,201
auto-agglutination type, differential diagnosis, 153
contents, 35
decreased adhesiveness, 199
decreased aggregation, 200
diminished production of, 131,
197
differential diagnosis, 152,
197
formation of, 103
functions, 36
305
ΓΗΕ PERIPHERAL BLOOD FILM
Platelets - cont.
immunological reactions, in, 36
increased adhesiveness, 197
indirect count, 121
life-span, 36
morphology of, 35
pools, 36
satellitisni, 153
Polychromatophilia, laboratory
diagnosis, 217
Poly chromât ophilic normoblasts,
80,81
Polychromed
méthylène
blue
solution, 250
Polycythaemia, 128, 132, 136,
155,239
absolute, 132, 155
laboratory diagnosis, 217
secondary, 13, 132, 155, 240
Polycythaemia rubra vera, 86, 97,
105, 114,239
Polymorphonuclear
basophil
granulocyte {see Basophil)
Polymorphonuclear
eosinophil
granulocyte {see Eosinophils)
Polymorphonuclear
neutrophil
granulocyte {see Neutrophil)
Post-gastrectomy syndrome, 240
Post-splenectomy syndrome, 242
Potassium ferricyanide solution,
259
Potassium ferrocyanide solution,
254,259
Pregnancy, 14, 240
Pre-leukaemia, 240
Preparation of blood films, 3 - 6
concentration techniques, 4
fixation, 5
thick, 4
thin, 3
Price-Jones curve, 122
Pro-erythroblasts, 1, 78
Prolymphocytes,
morphology,
109
Promegakaryocytes, 102, 104
Promegaloblasts, 92
Promonocyte, morphology, 101
306
Promyelocyte, 94, 96
leukaemic, 99, 142
Pronormoblasts, 80, 81
Propanediol buffer solution, 260,
261
Proplasmacyte, 110
Protoporphyrin, impaired synthesis, 39
Prussian blue reaction, 9, 254
Purpura, differential diagnosis,
152,198
laboratory diagnosis, 217
Pyknocytes, 3 8 , 4 7 , 4 9
Pyridoxal-5-phosphate
(vitamin
B ), 90
Pyridoxine, 90
deficiency, 166, 244
Pyruvate kinase deficiency, 241
Red cell {see Erythrocyte)
Reed-Sternberg cells, 111, 115,
231
Renal erythropoietic factor, 77
Renal failure, 241
Reticulin, 112
bone marrow, in, 204
Reticulocytes, 82
count, 82, 267
morphology, 81
RNAin, 15
'shift', 82, 139
staining, 7, 15, 267
Rheumatoid arthritis, 114, 225
R h n u l l disease 4 1 , 133, 230
Riboflavine deficiency, 89, 244
Ribonucleic acid (RNA)
plasma cells, in, 34
reticulocytes, in, 82
supravital staining, 15
Romanovsky staining, 2 , 6 , 246
Rubella, 241
Russell bodies, 71
INDEX
Safranin solution, 266
Saurocyte, 58, 71
Scarlet fever, 242
Schiffs reagent, 251
Schilling type cell, 102
Schistocytes, 3 7 , 4 7 , 4 9
Schistocytosis, 137
Scott's tap water substitute, 253
Sea-blue histiocyte, 113
Seal's differential density separation method, 5
Sex chromatin, 25
Sezary cells, 5 8 , 6 9 , 2 3 8
Sickle cells, 3 8 , 4 5 , 137, 174
Sickle cell disease, 13, 45, 114,
227
blister cells in, 46
differential diagnosis, 174
elliptocytes in, 45
laboratory diagnosis, 218
spherocytes in, 42
Sickle cell preparation, permanent,
273
Sickle cell trait, 45, 137, 228
Sickling reaction, 17
mechanism, 46
staining for, 272
Sideroblasts, 90
'ring', 90
Siderocytes, 15, 16, 49
Skin disorders, 194
Skoog and Beck's red cell sedimentation method, 5
Sodium citrate solution, 256
Sodium metabisulphite solution,
272
Spectrin, 42
Spherocytes, 3 7 , 4 1 , 124, 136
acquired, 42
Spherocytosis,
differential diagnosis, 174
laboratory diagnosis, 218
Splenic disorders, 242
Splenomegaly, 242
differential diagnosis, 187
Spur cells, 3 8 , 4 7 , 48
differential diagnosis, 175
Stab cells, 94, 95, 96
dignosis, 141
giant, 98
Stains and staining techniques,
6-20, 246-274
acid elution reaction, 10, 270
acid phosphatase reaction, 262
acridine orange
fluorescent,
249
alkaline phosphatase reaction,
260
alpha-naphthyl acetate esterase
reaction, 257
brilliant green/neutral red technique, 268
bromoindoxyl acetate esterase
reaction, 259
combined esterase reaction,
258
cytochemical, 2, 7
diluted Giemsa technique 248,
250
elution test for haemoglobins,
272
esterase enzyme reactions, 11
Feulgen reaction, 8,251
Greig's substitute, 252
Field's technique, 250
Giema's, 6, 7
Graham-Knoll technique, 255
haemoglobin H inclusions, for,
269
Heinz bodies, for, 268, 269
Jenner-Giemsa, 6, 7, 246
Leishman's, 6, 7, 247
May-Grünwald-Giemsa, 6, 7,
247
methyl violet technique, 268
naphthol
AS-D
chloroacetate
esterase reaction, 256
nitroblue tetrazolium reduction
test, 264
periodic acid-Schiff (PAS) reaction, 8, 253
peroxidase reaction, 11, 255
phosphate-citrate buffer technique, 271
307
PERIPHERAL BLOOD FILM
Stains and staining techniques - cont.
Prussian blue reaction, 9, 254
reticulocytes, 267
Romanovsky, 6, 260
sickling reaction, 272
supravital, 14
Washburn's modified technique,
255
Wright's, 6, 7, 248
Stem cells, 74, 75, 76
defect of, 87
increased availability, 86
multipotent myeloid and lymphoid, 76
pluripotent, 76
progenitor or committed, 76
Stem
cell compartments
in
haemopoiesis, 74
Stomach, carcinoma of, 224
Stomatocytes, 3 7 , 4 1 , 124
Stomatocytosis, 133, 167
Stromal cells, 111, 112
Supravital staining, 14
Swiss cheese nucleus, 68, 149
Target cells, 37, 39, 124, 127,
133,135, 172
characteristics, 40
diagnosis, in, 135, 172
haemoglobinopathies, in, 137
laboratory diagnosis, 219
Tart cells, 58, 65
Tay-Sachs disease, 67, 114, 235,
236
Tear-drop cells, 38, 49, 137, 143
differential diagnosis, 176
laboratory diagnosis, 219
Thalassaemia, 9, 23, 115, 137,
228,229
differential diagnosis, 160
elliptocytes in, 45
film appearances, 134
globin chain formation in, 83
red cells in, 39, 50
spherocytes in, 42
308
Thesaurocyte, 58, 71
Thiamine deficiency, 244
Thrombocytes {see Platelets)
Thrombocythaemia, 72, 201, 243
differential diagnosis, 152, 196
essential, 105
laboratory diagnosis, 220
Thrombocytopenia,
103, 131,
152,201
laboratory diagnosis, 219
May-Hegglin anomaly in, 62
pathogenesis of, 131
substances causing, 279
Thrombocytosis, 131, 201
differential
diagnosis,
151,
196-197
laboratory diagnosis, 220
Thrombopathy, substances causing, 280
Thrombopoiesis, 102—106
abnormal, 104
control of, 103
ineffective, 105, 106
normal, 102
Thrombopoietin, 77, 103
Thrombosthenin, platelets, in, 35
Thymic lymphopoiesis, 108
Thymosin, 77
Thymus
failure of, 130
T lymphocytes in, 76
Thyroid disorders, 243
Tuberculosis, 20, 243
Tularaemia, 69
Tumours, 88, 98, 105
cells, 111, 115, 116
Turk irritation cell, 70
Undulant fever, 244
Uraemia, burr cells in, 48
Vascular cells, 111, 113
Virocyte, 70
INDEX
Vitamin deficiencies, 244
Vitamin Bi deficiency, 244
Vitamin B 2 deficiency, 244
Vitamin B 6 , 90
deficiency, 166, 244
Vitamin B 1 2
DNA synthesis, in, 91
deficiency, 44, 97, 163, 240,
245
differential diagnosis, 163
laboratory diagnosis, 207
Vitamin C deficiency, 245
Vitamin E deficiency, 114
Washburn's technique, modified,
255
Whooping cough, 245
Wiskott-Aldrich syndrome, 152
Wright staining, 6, 7, 248
309