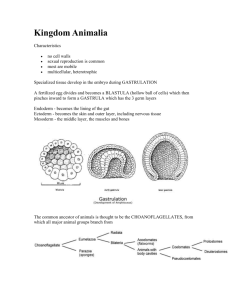
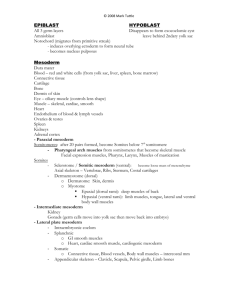
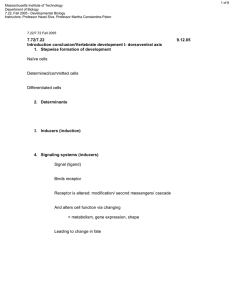
Development of Human Body: 2nd week and Formation of Germ layers: 3rd Week Gametogenesis/Fertilisation/Embryo Development Week 1: days 1-6 • • • • • Fertilization, day 1 Cleavage, day 2-3 Compaction, day 3 Formation of blastocyst, day 4 Ends with implantation, day 6 2. Week (2 layered Embryo disc) • Implantation (Embedding) • Bilaminar (two layered) embryonic disc, • Amniotic cavity, • Umbilical vesicle, • Connecting Stalk, • Chorion sac Week 2: days 714 implantation -Bilaminar Embryonic Disc- • Implantation of the blastocyst is completed by the end of the second week. • Cells of embryoblast organize into two layers: • (1) the hypoblast layer, and • (2) the epiblast layer. Together, the layers form a flat, almost circular embryonic disc. 8th day • The second week of development is known as the week of twos: • The embryoblast forms two layers, the epiblast (5) and hypoblast (7). • The trophoblast differentiates into two layers, the cytotrophoblast and syncytiotrophoblast. • The extraembryonic mesoderm splits into two layers, the somatopleure (10) and splanchnopleure (11). • Two cavities, the amniotic (3) and yolk sac (1) cavities, form. Additionally, during the 2nd week; • Isolated cavities known as lacunae (9) appear in the syncytiotrophoblast. • The communication of the eroded endometrial capillaries with the lacunae establishes the primordial uteroplacental circulation. A large fluid-filled cavity, the extraembryonic coelom or chorionic cavity (4), appears within the extraembryonic mesoderm. The connecting stalk (6) occurs. Primary chrionic vili (8) develop. • The cytotrophoblast cells are mitotically active and migrate into the increasing mass of syncytiotrophoblast, where they fuse and lose their cell membranes. • The syncytiotrophoblast is a rapidly expanding, multinucleated mass in which no cell boundaries are discernible. • The erosive syncytiotrophoblast invades the endometrial connective tissue, and the blastocyst slowly embeds itself in the endometrium. • The endometrial cells undergo apoptosis, which facilitates the invasion. • The syncytiotrophoblast produces human chorionic gonadotropin (hCG) which promotes the maintenance of the corpus luteum, causing it to secrete progesterone. • The molecular mechanisms of implantation involve synchronization between the invading blastocyst and a receptive endometrium. • The microvilli of endometrial cells (pinopodes), cell adhesion molecules, cytokines, prostaglandins, growth factors, and matrix metalloproteins play a role in making the endometrium receptive. • As the conceptus implants, the endometrial connective tissue cells undergo a transformation, the decidual reaction. • The connective tissue cells around the implantation site accumulate glycogen and lipids and assume a polyhedral appearance. Endometrium at the time of implantation • Swollen stromal cells because of the accumulation of glycogen and lipid are known as decidual cells. • The primary function of the decidual reaction is to provide nutrition for the early embryo and an immunologically privileged site for the conceptus. • Levels of hCG may be measured in the blood or urine. Most commonly, this is done as a pregnancy test. • Enough hCG is produced at the second week to give a positive pregnancy test, even though the woman is probably unaware that she is pregnant. • As known, EPF (early pregnancy factor) is present in the maternal serum shortly after fertilization. EPF has been detected as soon as within six hours of conception. EPF is believed to be the earliest possible marker of pregnancy. DAY 8 As the erosive syncytiotrophoblast invades the endometrial connective tissue, the blastocyst is partially embedded in the endometrial stroma. At the meantime, a small cavity or cleft appears within the inner cell mass. This cavity enlarges to become the amniotic cavity. A layer of high columnar cells between the amniotic cavity and the hypoblast, the epiblast layer, occurs. The epiblast forms the floor of the amniotic cavity and is continuous peripherally with the amniotic membrane consisting of amnioblasts. • Meanwhile, flattened cells probably originating from the hypoblast form a thin membrane, the exocoelomic (Heuser's) membrane that lines the inner surface of the cytotrophoblast. • So, the blastocyst cavity becomes the exocoelomic cavity or primitive yolk sac. The hypoblast forms the roof of the exocoelomic cavity. The embryonic disc now lies between the amniotic cavity and the primitive yolk sac. At the time of implantation, the mucosa of the uterus is in the secretory phase, during which time uterine glands and arteries become coiled and the tissue becomes succulent. Normally, the human blastocyst implants in the endometrium along the anterior or posterior wall of the body of the uterus, where it becomes embedded between the openings of the glands. myometrium endometrium DAYS 9-10 The blastocyst is more deeply embedded in the endometrium, and the penetration defect in the surface epithelium is closed by a fibrin coagulum. Particularly at the embryonic pole, vacuoles appear in the syncytiotrophoblast. When these vacuoles fuse, they form large lacunae, and this phase of trophoblast development is known as the lacunar stage. 8th day 9th day • During the 9th to 10th days, a new population of cells appears between the inner surface of the cytotrophoblast and the outer surface of the exocoelomic cavity. • These cells, derived from yolk sac cells, form a fine, loose connective tissue, the extraembryonic mesoderm, which eventually fills all of the space between the trophoblast externally and the amnion and exocoelomic membrane internally. At 10th day, lacunar network is particularly evident at the embryonic pole; at the abembryonic pole, the trophoblast still consists mainly of cytotrophoblastic cells. Maternal blood and gland secretion flows into the lacunae. The fluid in the lacunae passes to the embryonic disc by diffusion. 10th day DAYS 11-12 The trophoblastic lacunae at the embryonic pole are in open connection with maternal sinusoids (congested and dilated capillaries) in the 12th day endometrial stroma. So, primitive uteroplacental circulation starts . By day 12, an almost completely regenerated uterine epithelium covers the closing plug. As the syncytiotrophoblast layer grows and expands toward the abembryonic pole, new lacunae appear also in this pole. Soon, large cavities develop within the extraembryonic mesoderm. • In the meantime, the hypoblast produces additional endodermal cells that migrate along the inside of the exocoelomic membrane. • These cells proliferate and gradually form a new cavity within the exocoelomic cavity. This new cavity is known as the secondary yolk sac or definitive yolk sac. DAYS 13-14 • Secondary yolk sac is much smaller than the primitive yolk sac. • During its formation, large portions of the exocoelomic cavity are pinched off. • These portions are represented by exocoelomic cysts. • When the large cavities in the extraembryonic mesoderm become confluent, they form a new space known as the extraembryonic coelom, or chorionic cavity. 13th day 14th day • The chorionic cavity surrounds the primitive yolk sac and amniotic cavity, except where the embryonic disc is connected to the trophoblast by the connecting stalk. • With development of blood vessels, the stalk becomes the umbilical cord. • The extraembryonic mesoderm lining the cytotrophoblast and amnion is called the extraembryonic somatopleuric mesoderm; the lining covering the yolk sac is known as the extraembryonic splanchnopleuric mesoderm. • The extraembryonic mesoderm lining the inside of the cytotrophoblast is known as the chorionic plate. Thus, the extraembryonic coelom splits the extraembryonic mesoderm into two layers: • Extraembryonic somatic mesoderm, lining the trophoblast and covering the amnion • Extraembryonic splanchnic mesoderm, surrounding the umbilical vesicle (yolk sac) • The prechordal plate develops as a localized thickening of the hypoblast, which indicates the future cranial region of the embryo and the future site of the mouth; • The prechordal plate is also an important organizer of the head region. . • By the 13th day of development, the surface defect in the endometrium has usually healed. • Occasionally, however, bleeding occurs at the implantation site as a result of increased blood flow into the lacunar spaces. • Because this bleeding occurs near the 28th day of the menstrual cycle, it may be confused with normal menstrual bleeding and, therefore, may cause inaccuracy in determining the expected delivery date. • The trophoblast is characterized by villous structures. • Cells of the cytotrophoblast proliferate locally and penetrate into the syncytiotrophoblast, forming cellular columns surrounded by syncytium. • Cellular columns with the syncytial covering are known as primary villi. Primary chorionic villus Abnormal implantation • Abnormal implantation sites sometimes occur even within the uterus. • Normally, the human blastocyst implants along the anterior or posterior wall of the body of the uterus. • Occasionally, the blastocyst implants close to the internal os (opening) of the cervix, so that later in development, the placenta bridges the opening (placenta previa) and causes severe, even life-threatening bleeding in the second part of pregnancy and during delivery. • Occasionally, implantation takes place outside the uterus, resulting in extrauterine pregnancy, or ectopic pregnancy. • Ectopic pregnancies may occur at any place in the abdominal cavity, ovary, or uterine tube. 95% of ectopic pregnancies occur in the uterine tube, however, and most of these are in the ampulla. • In the abdominal cavity, the blastocyst most frequently attaches itself to the peritoneal lining of the rectouterine cavity, or pouch of Douglas. • Sometimes, the blastocyst develops in the ovary proper, causing a primary ovarian pregnancy. In most ectopic pregnancies, the embryo dies about the second month of gestation, causing severe hemorrhaging and abdominal pain in the mother. 4.5-week human embryo ECTOPIC TUBAL PREGNANCY • Abnormal blastocysts are common. • It is likely that most abnormal blastocysts would not have produced any sign of pregnancy because their trophoblast was so inferior that the corpus luteum could not have persisted. • These embryos probably would have been aborted with the next menstrual flow and, therefore, pregnancy would not have been detected. • In some cases, however, the trophoblast develops and forms placental membranes, although little or no embryonic tissue is present. Such a condition is known as a hydatidiform mole. Moles secrete high levels of hCG and may produce benign or malignant tumors. Although cells of complete moles are diploid, their entire genome is paternal. Thus, most moles arise from fertilization of an oocyte lacking a nucleus followed by duplication of the male chromosomes. The exact number of abnormal zygotes formed is unknown because they are usually lost within 2 to 3 weeks of fertilization, before the woman realizes she is pregnant, and therefore are not detected. Estimates are that as many as 50% of pregnancies end in spontaneous abortion and that half of these losses are a result of chromosomal abnormalities. These abortions are a natural means of screening embryos for defects, reducing the incidence of congenital malformations. Without this phenomenon, approximately 12% instead of 2% to 3% of infants would have birth defects. Week 3: Days 14-21 • • • • • • Two layer germ disc Primitive streak forms Gastrulation forms tri-laminar embryo Neural induction Left-right asymmetry 0.4mm - 2.0mm On this stage (3rd week) • Early development of cardiovascular system • Further diffentiation of chorionic villi • Neurolation: Development of the neural tube Gastrulation At gastrulation the two layered epiblast is converted into the three primary embryonic germ layers: – Ectoderm: outside, surrounds other layers later in development, generates skin and nervous tissue – Mesoderm: middle layer, generates most of the muscle, blood and connective tissues of the body and placenta – Endoderm: eventually most interior of embryo, generates the epithelial lining and associated glands of the gut, lung, and urogenital tracts Formation of trilaminar germ Trilaminar germ disc primitive streak, primitive groove primitive node, primitive pit 3rd week 3rd week 1. Endoderm: primitive groove →hypoblast → endoderm 2. Mesoderm: primitive groove →between epiblast and hypoblat →mesoderm 3. Ectoderm:epiblast →ectoderm The human embryo at gastrulation At gastrulation, primitive endoderm is replaced by definitive or embryonic endoderm then mesoderm is formed Cell movements during gastrulation Mesoderm is patterned in a cranial to caudal gradient Axial mesoderm: passes through the node and migrates along the midline –forms the notochord Paraxial mesoderm: passes just caudal to the node and migrates slightly laterally –forms cartilage, skeletal muscle, and dermis Lateral plate mesoderm: passes more caudal and migrates more laterally –forms circulatory system and body cavity linings. Extraembryonic mesoderm: passes most caudal and migrates most laterally –forms extraembryonic membranes and associated connective tissue & blood vessels. Fate of the “axial” mesoderm The notochord and pre-chordal plate develops from mesoderm arising from cells that passed directly through the node and migrated cranially along the midline The notochord and pre-chordal plate are important signaling centers that pattern the overlying ectoderm and underlying endoderm. Major signaling centers at gastrulation: the node and the anterior visceral endoderm (AVE) • Primitive node positions primitive streak for gastrulation, induces neural differentiation • AVE from primitive endoderm secretes factors that position primitive streak in posterior, induce head formation The node also sets up the neural plate THE EMBRYONIC PERIOD The period in which each of the three germ layers will give rise to a number of specific tissues and organs Ectodermal germ layers Initially the ectodermal germ layer has shape of a disc, not equal at caudal and cranial points Notocord and precordal mesoderm induces overlying ectoderm to thicken and form the neuro plate Induction of neuroectoderm is the initiation of neurulation Neurulation Process by which neuro tube is formed from neuro plate Lateral edges of neuro plates are elevated are elevated to form the neuro fold while the depression makes the neuro groove Neuro folding results in formation of a neural tube Communication with amniotic cavity through neuropores Closure of neuropores marks end of neurulation Neural crest cells These are cells at the lateral border of the neuroectoderm During fusing of the neuro folds the cells will undergo the epithelial to mesenchymal transition Migrates from neuroectoderm to underlying mesoderm Neuro crest cells of the trunk region start migrating in 2 directions following closure of the neuro tube • Dorsal and ventral • Ectoderm germ layer gives raise to organs and structures that maintain contact with the outside world Mesodermal germ layer Mesodermal germ layer tissue under goes proliferation Midline form a thickened tissue known as paraxial mesoderm Laterally remain thin and called lateral plate Lateral plate divides into somatic or parietal mesoderm layer continuous with amnion The layer continuous with the yolk sac is the splanchnic or visceral mesoderm layer • Paraxial mesoderm • Segmental organization known as somitomeres and form in a cephalocaudal manner • Somitomeres further organise into somites • First pair arise from the occipital region at approximately 20th day of development then they appear at the rate of 3 pairs per day until week 5 • 42 to 44 pairs are present, • Age determination Development of Somites There are; • 4 occipital, • 8 cervical, • 12 thoracic, • 5 lumbar, • 5 sacral, • and 8 to 10 coccygeal pairs. The first occipital and the last five to seven coccygeal somites later disappear, while the remaining somites form the axial skeleton. Development of Somites Sclerotome Myotome Dermatome Development of Somites • Cells in the dorsolateral of somites form the muscles of the limb and body wall. • Cells in the dorsomedial of somites migrate under the dorsal epithelial cells to form myotomes. Development of Somites • Myoblasts of the myotome migrate to emerging extremity buds to form limb muscles. • Lateral plaque mesoderm forms the connective tissues of the extremities. Development of Somites • The cells that make up the myotome progress under the dorsal epithelium. • Dermatome cells lose their epithelial properties when myotome comes to the ventral and settles under the ectoderm to form the dermis. Development of Somites • Paraxial mesoderm forms segmented regions on both sides of the neural tube. • Somitomers in the head region • Occipital to caudal somites • Somites • Sclerotome (Ventromedial) Vertebra, costa • Dermatomyotome (Dorsolateral) Myoblast, Dermis (E) Transverse section of an embryo of approximately 26 days showing the dermatome, myotome, and sclerotome regions of a somite Intermediate mesoderm • Forms segmental cell clusters, future nephrotome • More caudally it forms an unsegmented mass of tissue, the nephrogenic cord • Excretory units of the urinary system and gonads form Lateral plate mesoderm • Differentiate into visceral and parietal mesoderm Differentiation of Lateral Plate Mesoderm (Formation of Intraembryonic Coelom) • Small gaps are formed in the lateral and cardiogenic mesoderm. These combine to form intraembryonic coelom. • Intraembryonic coelom continues with extraembryonic coelom. Lateral Plate Mesoderm Intraembryonic coelom separates lateral mesoderm into two leaves: Visceral (splanchnic, splanchnopleuric) mesoderm; is continuous with the extraembryonic splanchnic mesoderm on the vitellus sac. Parietal (somatic, somatopleuric) mesoderm; is continuous with extraembryonic somatic mesoderm covering the amniotic sac. Lateral Plate Mesoderm • Forms lateral and ventral body wall (somatopleura) with ectoderm on somatic mesoderm • Splanchnic mesoderm forms the splanchnopleura (primitive intestinal wall) with embryonic ectoderm. Lateral Plate Mesoderm Mesoderm cells facing the coelom cavity form mesothelial serous membranes. In the 4th week, folding of the embryo longitudinally and laterally intraembryonic coelom divides into pericardial, pleural and peritoneal cavity. Serous membranes cover these cavities. Differentiation of Mesoderm Differentiation of Mesoderm • Cartilage, bone and connective tissues • Smooth and striated muscles • Blood and lymph cells, • Heart, blood and lymphatic vessels • Kidneys, gonads (ovaries and testicles) and their discharge ways • Serous membranes covering body cavities • Spleen • Adrenal gland cortex Endodermal germ layer The gastrointestinal tract is the main organ system derived from the endodermal germ layer the epithelial lining of the respiratory tract the Parenchyma of the thyroid, parathyroids, liver, and pancreas the reticular stroma of the tonsils and thymus the epithelial lining of the urinary bladder and urethra the epithelial lining of the tympanic cavity and auditory tube Development of Primitive Cardiovascular System Vasculogenesis; development of vessels • In 3rd week; • Development of vessels in; • Umbilical vesicle (yolk sac) • Connecting Stalk starts at the extraembryonic mesodem of the chorion. Development of Primitive Cardiovascular System • Development of intraembryonic blood vessels starts two days later. Vasculogenesis • Mesenchyme cells gather and differntiate into angioblasts. These form blood islands. Vasculogenesis • Gaps (lumes) are formed in the middle of blood islands. Angioblasts surrounding the cavity differentiate to primitive endothelial cells. Vasculogenesis • The cells inside differentiate to hematopoietic (blood) cells. • Vessels having lümen and endothel connect with each other to form vessel networks. Angiogenesis • Is the differentiation of new blood vessels and spreding to neighbouring sites with the budding of existing endothel layer. Development Of Primitive Blood Cells And Plasma • In 3rd week • Vessels of the umbilical and allantois vesicle develope from endothelial cells. • After 5th week • Intraembryolal blood production starts. Liver, observed. spleen and bone marrow is Development Of Primitive Heart • Mesenchyme cells at the cardiogenic region form a pair of long endocardial heart tube in the 3rd week. Development Of Primitive Heart • At the end of 3rd week, intraembryonal, connecting stalk, chorionic and umbilical sac vessels and primitive heart tube unite to form primitive cardiovascular system. • At the end of 3rd week (day 21-22) heart starts to beet and blood circulates. • Cardiovascular system is the first functional system of the embryo.