Heart Rate-Based Training Intensity and Its Impact on Injury Incidence Among Elite-Level Professional Soccer Players
advertisement

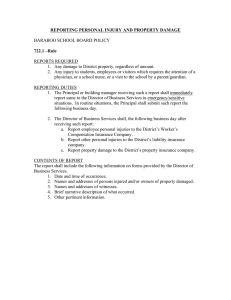
HEART RATE–BASED TRAINING INTENSITY AND ITS IMPACT ON INJURY INCIDENCE AMONG ELITE-LEVEL PROFESSIONAL SOCCER PLAYERS ADAM L. OWEN,1,2 JACKY J. FORSYTH,3 DEL P. WONG,4 ALEXANDRE DELLAL,5 SEAN P. CONNELLY,1 6 AND KARIM CHAMARI 1 Servette Football Club, Center for Football Research, Geneva, Switzerland; 2Center of Sports Research and Innovation, Claude Bernard University Lyon.1, Lyon, France; 3Center for Sport Health and Exercise Research, Staffordshire University, Stafford, United Kingdom; 4Human Performance Laboratory, Technological and Higher Education Institute of Hong Kong, Hong Kong, China; 5Medical Center Excellence FIFA, Santy Orthopedicae Clinical, Lyon, France; and 6Athlete Health and Performance Research Center, ASPETAR, Qatar Orthopaedic and Sports Medicine Hospital, Doha, Qatar ABSTRACT Owen, AL, Forsyth, JJ, Wong, DP, Dellal, A, Connelly, SP, and Chamari, K. Heart rate–based training intensity and its impact on injury incidence among elite-level professional soccer players. J Strength Cond Res 29(6): 1705–1712, 2015—Elite-level professional soccer players are suggested to have increased physical, technical, tactical, and psychological capabilities when compared with their subelite counterparts. Ensuring these players remain at the elite level generally involves training many different bodily systems to a high intensity or level within a short duration. This study aimed to examine whether an increase in training volume at high-intensity levels was related to injury incidence, or increased the odds of sustaining an injury. Training intensity was monitored through time spent in high-intensity (T-HI) and very high-intensity (T-VHI) zones of 85–,90% and $90% of maximal heart rate (HRmax), and all injuries were recorded over 2 consecutive seasons. Twentythree, elite professional male soccer players (mean 6 SD age, 25.6 6 4.6 years; stature, 181.8 6 6.8 cm; and body mass, 79.3 6 8.1 kg) were studied throughout the 2-years span of the investigation. The results showed a mean total injury incidence of 18.8 (95% confidence interval [CI], 14.7– 22.9) injuries per 1,000 hours of exposure. Significant correlations were found between training volume at T-HI and injury incidence (r = 0.57, p = 0.005). Further analysis revealed how players achieving more time in the T-VHI zone during training increased the odds of sustaining a match injury (odds ratio = 1.87; 95% CI, 1.12–3.12, p = 0.02) but did not increase the odds of sustaining a training injury. Reducing the number of Address correspondence to Dr. Adam L. Owen, adamowen@ outlook.com. 29(6)/1705–1712 Journal of Strength and Conditioning Research Ó 2015 National Strength and Conditioning Association competitive match injuries among elite-level professional players may be possible if greater focus is placed on the training intensity and volume over a period of time ensuring the potential reduction of fatigue or overuse injuries. In addition, it is important to understand the optimal training load at which adaptation occurs without raising the risk of injury. KEY WORDS soccer, injury, odds ratio, training, periodisation INTRODUCTION S occer is a high-intensity intermittent contact sport that exposes elite-level players to continual physical, technical, tactical, psychological, and physiological demands (33,36). The stressors encountered during actual match-play have been suggested to show no detrimental effect of consecutive games’ physical performance, but a greater injury risk (8,12). From a training perspective, cardiovascular and neuromuscular adaptations are suggested to be stimulated through a high training load (TL), induced through manipulation of intensity, duration, and frequency of training (10). However, if the intensity or volume is increased by an amount above the level at which various physiological systems can adapt, injury may result (26). Therefore, it is important to understand the optimal TL at which adaptation occurs without raising the risk of injury. The implications of a high number of training days and matches lost because of injury is suggested to be to the detriment of team success (2), especially for soccer teams unable to replace players of similar abilities because of limited resources. Recently, Eirale et al. (16) even showed a clear relationship between teams’ ranking and injury rate. Indeed, in the Qatari Professional league, it resulted that lower injury incidence rate was strongly correlated to team success over an entire season. In soccer, high-intensity training has increasingly been advocated and used to elicit cardiovascular adaptations VOLUME 29 | NUMBER 6 | JUNE 2015 | 1705 Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. Training Load, Intensity, and Injury (11,30,36). Often, this type of training is reported to require players working at high to very high intensities, indicated through high heart rate responses (.85% maximal heart rate [HRmax]) (36). Within the literature, mean match HRs of ;85% HRmax have been reported; however, these are averaged values that include numerous, recovering low-intensity bursts that follow extremely high-intensity efforts. At the elite level, the accumulative high intensity nature of soccer match-play combined with multiple high-intensity sessions may cause excessive bodily strain (3,34). The continual strain over a prolonged period of time may lead to performance decrements and increase the risk of injury (5,35). Injury incidence in soccer is high with approximately 20–35 injuries occurring per 1,000 hours of match exposure (14,17) and injuries during training sessions ranging between 5.8 and 7.6 per 1,000 hours (2,38). Some authors report that a greater number of overuse injuries occur in the preseason training period (28,29), because of a greater intensity and volume of training causing a residual fatigue that may be attributed with an increased injury risk. It may be important to consider whether training intensity relates to injury incidence, to educate coaches or other sport professionals involved within the physical development of players. Program or session design must ensure that TLs = volume 3 intensity are not significantly exceeded, eliciting accumulative fatigue responses and predisposing players to overuse injuries. Gabbett and Dumrow (25) found that TL increased the odds of sustaining an injury; however, this particular study involved rugby players, and injury exposure was estimated based on average training duration rather than calculated per player. Furthermore, ratings of perceived exertion (RPE) scores were used as a measure of intensity (TL = RPE 3 training duration). Although popular owing to its ease of use (1,6), this method depends on the personal perception of physical effort a period after (6,26). Therefore, although it does provide a valid estimate of total session mean intensity, it does not provide data about the periods spent at various training intensities (31). Heart rate training zones have been used as an alternative and objective measure of estimating training intensity (6,15,23,36), with HR being reported as a valid and reliable indicator of exercise intensity within soccer training (30,36). Currently, there are no studies investigating the relationship between injury incidence and high intensity quantified through HR within elite-level professional soccer. Because of the limited amount of research within this area, the purpose of the investigation was to examine whether a relationship exists between training volume and intensity on injury incidence and also the odds of sustaining an injury in both training sessions, and competitive matches. Many publications have highlighted specific audits of injury types at many levels of the game; however, no literature exists regarding the potential effect of TL on injury rates. It was hypothesized that a greater time spent in the very highintensity HR zones would increase the odds of injury, and therefore be associated with a higher injury incidence. 1706 the METHODS Experimental Approach to the Problem This prospective, cohort surveillance study was carried out over 2 competitive soccer seasons. To examine if a greater time spent at 85–,90% (time spent in high-intensity zone [T-HI]) and $90% (time spent in high-intensity zone [T-VHI]) of HRmax is associated with a higher injury incidence, the relationship between training intensity and injury incidence was determined. Secondary outcome measures of the study included injury severity, type, and frequency. Furthermore, odds ratios (ORs) were determined to examine if a higher individual TL would increase the odds of injury. Injury incidence was presented as the number of injuries per 1,000 hours of exposure, with exposure recorded for each player rather than being estimated for the group (27). Because relationships have been previously reported between injury incidence and players’ age, body composition, maximal oxygen consumption (V_ O2max), and vertical jump height (4,17,18) these variables were measured in this study to examine their impact on injury. Subjects Twenty-three elite, male professional soccer players participated in this investigation. At the initiation of the study, players involved had a mean 6 SD age of 26.8 6 4.6 (range: 18–38) years, stature of 181.8 6 6.8 (1.70–1.92) cm, and body mass of 79.3 6 8.1 (62.5–93.6) kg. Percentage body fat for the 23 players was 10.1 6 2.7 (5.1–16.3) %, and mean V_ O2max was 53.7 6 4.3 (52.1–68.6) ml$kg21$min21. All participants had been playing soccer for 8 years or more, and all but 3 of them were competing at the international level. Participants were informed that they were free to withdraw from the study at any time. Procedures followed were in accordance with the Helsinki Declaration of 1975, approved by the Ethical Committee of the collaborating University and followed the standards of the Sport Science and Medical Department of the researching soccer club. Measure of Injury The injury definitions and method used for analysis of each injury followed the guidelines recommended by the International Soccer Injury Consensus Group (22,27). In this regard, an injury was defined as any physical complaint sustained by the soccer player either in training or in competition, which prevented the injured player from participating in competition or normal training for at least 1 day, but not including the day of the injury (22). This type of injury has been referred to as a timeloss injury (22). Injury incidence was categorized according to incidence per match (i.e., the number of match injuries in relation to the time spent in matches), and incidence per training (the number of injuries during time spent in training), and total injury incidence (sum of training and match injuries in relation to overall training and match exposure) (22,27). The severity of each injury was defined by the time lost from usual training or competition and was categorized TM Journal of Strength and Conditioning Research Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. the TM Journal of Strength and Conditioning Research | www.nsca.com uptake (V_ O2max) and HRmax to determine individual HR TABLE 1. Site of injury. training zones. Players followed the V_ O2 max running Match injuries Training injuries Site of injury N (%) N (%) protocol of Hoff et al. (30), and a precalibrated breath-byCalf/lower leg 18 (20.7) 4 (12.5) breath metabolic system was Ankle and foot 18 (20.7) 9 (28.1) used (Medical Graphics CarKnee 15 (17.2) 4 (12.5) diopulmonary Exercise System, Hamstring 14 (16.1) 4 (12.5) Thigh 12 (13.8) 5 (15.6) CPX/D; Medgraphics Corp., Groin 4 (4.6) 1 (3.1) St. Paul, MN, USA). Individual Head 3 (3.4) 0 (0.0) HRmax and V_ O2max were Chest and abdomen 2 (2.3) 1 (3.1) derived by using the mean of Spine 1 (1.1) 26.3 the 2 highest 15-second averShoulder 0 (0.0) 2 (6.3) Total 87 32 ages achieved during the final stage of the V_ O2max test. A true HRmax and V_ O2max were considered to have been achieved, if both variables in the following way: slight as 1–3 days, minor as 4–7 days, failed to increase despite an increase in exercise intensity moderate as 8–21 days, and major as .21 days (28). Injuries (37). The protocol is commonly used for testing endurance were classified according to whether they were overuse or performance in professional football players (26) and traumatic (22). Other information recorded about the injury involved participants running on a treadmill at a 38 incline included the nature of the injury (sprain, fracture, etc.), the with speed increases of 1 km$h21 every minute until exhauslocation (body part), the date, and whether or not the injury tion. Before the protocol test, players performed a 3-minute was a preceded by a previous one (recurrent), the latter warm-up eliciting an intensity of around 70% HRmax in being defined as an injury that had occurred previously at addition to self-selected stretching exercises. the same location and of the same nature (22). All injuries Heart rate was recorded and assessed at 5-second intervals were diagnosed and recorded by the club’s medical staff. by portable HR monitors (Polar Team System 2; Polar Electro Injuries were recorded throughout both seasons. Illness OY, Kempele, Finland) throughout the training sessions for was not taken into account within this study. the duration of the investigation (36). Goalkeepers were not included within the data group. After each testing session, HR data was downloaded to a computer using dedicated software Training Load (Polar Precision S-Series Software SW 3.0; Polar Electro OY) A laboratory-based, maximal incremental running treadmill and stored for analysis. The mean and %HRmax achieved test (Run 500 model; Technogym, Cesena, Italy) was during each game was calculated for each player, with each conducted once during preseason before the commenceplayer’s total time spent in specific HR zones following ment of the training period to determine maximal oxygen methods used in previous studies (25,36): #50%; 50–,60%; 60–,70%; 70–,85%; 85– ,90% HRmax (T-HI) and TABLE 2. Type of injury. $90%HRmax (T-VHI). However, for the purpose of this parMatch Training ticular study, the time spent injuries injuries Type of injury N (%) N (%) within the higher intensity zones, T-HI and T-VHI, has Muscle and tendon (muscle rupture/tear/strain; 42 (48.3) 13 (40.6) been assessed and reported to tendinopathy) differentiate between “training Contusions (hematoma, contusion, effusion, bruise) 28 (32.2) 9 (28.1) Sprain/ligament injury 15 (17.2) 9 (28.1) intensity” (11). These 2 HR Dislocation 0 (0.0) 1 (3.1) zones were chosen because preLaceration 1 (1.1) 0 (0.0) vious and current research Concussion 1 (1.1) 0 (0.0) investigating elite-level soccer Total 87 32 has reported how HR .85% is key when discussing training adaptations (36). VOLUME 29 | NUMBER 6 | JUNE 2015 | 1707 Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. Training Load, Intensity, and Injury Odds ratios were used to examine whether the TL increased or decreased the odds of injury. Odds ratios were derived by tallying the frequency of injury on a monthly basis, because training was organized into mesocycles (4 weeks). Training load per mesocyle was categorized according to whether it was considered to be a “high TL” or a “low TL,” by using a median split of the data. Odds of TL increasing the frequency of match injuries, training injuries, traumatic and Figure 1. Individual training intensity (time spent in HR zone) and frequency of training injuries on a monthly basis. overuse injuries, and total injuT-HI = mean time spent in the 85–89% heart rate training zone; T-VHI = mean time spent at or above 90% maximum heart rate. ries, and of increasing the frequencies of injury severity, were examined. Statistical Analyses A x2 test was used to determine whether the observed Before analysis, injury incidence and HR data were explored injury frequency differed from the expected injury frequency. (and confirmed) for normality and for equality of variances. Expected injuries were calculated as the same proportion of Data are expressed as mean 6 SD, percentages, and 95% the total injuries as the mesocycle TL score was of the total confidence intervals (CIs), where relevant. Statistical signifiTL score, following the method of Gabbett (23). cance was set at p # 0.05. The TL within the previous mesocycle before the injury Pearson’s correlations were used to examine the relationbeing sustained was determined and assessed to provide an ships between TL and injury (incidence, severity, type, and accurate picture of the relationship between TL and injury. frequency), as well as between injury incidence and physioThis was due to anticipation that TLs would be lower in the logical/anthropometrical data. The magnitude of the corremonth when an injury was sustained because of reduced lations was determined using the modified scale by Hopkins training availability. An independent samples t-test was then (2000): trivial: r , 0.1; low: 0.1–,0.3; moderate: 0.3–,0.5; used to examine whether TL, training exposure, and match high: 0.5–,0.7; very high: 0.7–,0.9; nearly perfect $0.9; exposure differed significantly in the mesocycle before injury, and perfect: 1. compared with the mesocycles when injury did not occur. A stepwise, multiple linear regression analysis was used to RESULTS predict injury incidence; variables having a higher correlation coefficient than r = 0.50 (and a significant relationship) Over the 2 seasons, the players were exposed to a total of were included in the analysis. The adjusted R2 was used to 1,704.4 hours of match-play, and 5350.0 hours of training, assess the proportion of the variance explained by the indewhich equated to an average of 4.8 6 3.8 hours of training pendent variables. time per match hour. The team played 116 matches, 54 in TABLE 3. Odds ratios (95% CI) of sustaining a match or training injury because of training load.*† Training injury T-HI T-VHI Match injury Odds ratios p Odds ratios p 0.60 (0.28–1.28) 0.52 (0.24–1.12) 0.20 0.10 1.87 (1.12–3.12) 1.28 (0.78–2.10) 0.02 0.38 *CI = confidence interval; T-HI = mean time spent in the 85–89% maximum heart rate training zone; T-VHI = mean time spent at or above 90% maximum heart rate training zone. †p denotes significance using Fisher’s exact probability test using a 2-tailed analysis. 1708 the TM Journal of Strength and Conditioning Research Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. the TM Journal of Strength and Conditioning Research | www.nsca.com and 48 (55.2%) were traumatic. Seventeen of the 32 training injuries (53.1%) were overuse, and 15 (46.8%) were traumatic. Total injury incidence was 18.8 (95% CI, 14.7–22.9) injuries per 1,000 hours of exposure. Training injury incidence was 6.7 injuries per 1,000 hours of training exposure (95% CI, 3.7–9.6), and match injury incidence was of 54.1 (95% CI, 39.7–68.6). Of the match injuries, 9.2% (n = 8) were slight, 35.6% (n = 31) were minor, 33.3% (n = 29) were moderate, and 21.8% (n = 19) were major. Of the training injuries, 28.1% (n = 9) were slight, 21.9% Figure 2. Mean differences (including SD represented by error bars) in time spent in each heart rate zone (T-HI and T-VHI) in the month preceding an injury, and in the month when an injury did not occur. T-HI = mean time spent (n = 7) were minor, 28.1% (n = in the 85–89% heart rate training zone; T-VHI = mean time spent at or above 90% maximum heart rate. 9) were moderate, and 21.9% (n = 7) were major. Data for injury frequency season 1 and 62 in season 2, with the higher number in and training intensity are given in Figure 1. There was a sigseason 2 because of UEFA Champions League fixtures. nificant correlation between total injury incidence and trainThere were a total of 130 injuries recorded over the 2 seaing intensity (T-HI: r = 0.57, p = 0.005; T-VHI: r = 0.568, p = sons. Type and site of injuries (for both match-play and 0.005). There was also a significant correlation between training) are given in Tables 1 and 2, respectively. training injury incidence and training intensity, but only for Injuries and illnesses sustained outside of soccer hours T-HI (r = 0.48, p = 0.02). Correlations were low between were excluded from further analysis regarding injury incimatch injury incidence and training intensity (T-HI: r = 0.09, dence, injury type, cause, site, and severity, leaving a total of p = 0.69; T-VHI: r = 0.19, p = 0.38). Correlations were 119 soccer-related injuries. Recurrent injuries were also significant for number of days off because of injury (an indiexcluded when describing injury type, cause, and severity, cation of injury severity) and training intensity (r = 0.51, p = so as not to falsely elevate these values. Of the remaining 119 0.01 for T-HI, and r = 0.47, p = 0.02 for T-VHI). There was injuries, 87 were match injuries and 32 were training injuries. a significant correlation between training intensity and total Thirty-nine of the 87 match injuries (44.8%) were overuse, number of traumatic injuries (r = 0.42, p = 0.04 for T-HI, and r = 0.44, p = 0.03 for T-VHI). A significant negative correlation was observed between injury incidence and percentage body fat (r = 20.43, p = 0.04), but correlations between injury incidence and all other anthropometrical/physiological variables were low and nonsignificant. A forward, stepwise linear regression, with T-HI and T-VHI in the model, gave an adjusted R2 of 0.28, p = 0.014 for injury incidence; hence, training intensity explained 28% of the variance in injury incidence. The ORs of sustaining an injury because of training Figure 3. Number of training injuries and monthly hours of training over the 2 seasons. intensity are given in Table 3. VOLUME 29 | NUMBER 6 | JUNE 2015 | 1709 Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. Training Load, Intensity, and Injury Only one of these values was significant, with a greater time spent in T-HI resulting in a greater odds of sustaining a match injury (x2 = 7.22, p = 0.059). There was a significant difference between the observed total injury frequency and the expected injury, as determined as a proportion of training intensity (mean T-HI, x2 = 33.2, p = 0.04; mean T-VHI, x2 = 33.5, p = 0.04). Differences were also significant when separately analyzing training injuries (for T-HI, x2 = 38.0, p = 0.01; and T-VHI, x2 = 36.7, p = 0.02) and match injuries (for T85, x2 = 48.4, p , 0.001; and T90, x2 = 48.3, p = 0.001). Mean differences (including significance) in time spent in each intensity zone in the month preceding an injury and in the mesocycle when an injury did not occur are given in Figure 2. DISCUSSION The main purpose of this study was to examine whether training intensity, as assessed using T-HI and T-VHI, increased the odds of sustaining an injury. Findings from this study have revealed that individual training intensity and load were highly related to total injury incidence (r = 0.57, p = 0.005). Training intensity (T-HI and T-VHI) explained 28% of the variance in injury incidence. Odds ratios for training intensity and injury incidence were negligible with no discernible pattern apparent. For instance, an increased proportion of time spent at 85–,90% HRmax significantly increased the odds of sustaining a match injury but did not increase the odds of sustaining a training injury (Table 2). Accumulative fatigue derived from high intensity training and competitive match-play may have played a fundamental role because of its residual effect in explaining the higher ORs for match injury incidence. In addition, the significant increase in match contusion injuries (n = 28) vs. training contusion injuries (n = 9) as a result of contact with competitors during match-play should be highlighted as a key factor of increased odds. Using x2 analysis, the observed total injury frequency and the observed training injury frequency were significantly different (p # 0.05) from the number of injuries that were expected to occur based on training intensity, which suggests that training intensity and injury frequency were not associated. It seems, therefore, that TL approach, assessed using specific HR zones, has only a moderate effect on injury incidence and does not increase the odds of injury. This finding is contrary to what was reported by Gabbett and Dumrow (25), who found that high TL increased the odds of injury in rugby players. The discrepancy in relation to this study may be explained by how Gabbett and Dumrow (25) estimated training intensity through RPE as opposed to HR zones used in this study. It should also be noted that the previous study (25) defined exposure as the number of players multiplied by session duration to give an average exposure, as opposed to individual exposure data used in this study. Similar to this study, Killen et al. (32) found no relationship between TL (as assessed using RPE) and training injury incidence in rugby 1710 the players. Their suggestion was that the high-caliber nature of the athletes was protective against injury, which may also account for the current findings. However, significant relationships have been found between individual session–RPE and HR-based TL, therefore strengthening the use of HR as a valid method of assessing TL in sports. It may be suggested that injury results from an accumulation of TL. For these reasons, an attempt was made to analyze whether differences in TL occurred before the injury being sustained, through consideration of the TL in the preceding period. On the occurrence of injuries, duration sustained within T-VHI was significantly greater in the preceding mesocycle when compared with the duration accumulated in T-VHI if an injury had not occurred (Figure 2). Although training intensity was related to injury incidence but not increased odds of training injuries, the accumulation of training at high intensity combined with match-play may affect injury incidence; however, further research is needed to confirm this. When analyzing injuries, both training intensity and volume over time should be considered, and coaches should try to ensure that excessive durations’ training at these high levels are avoided through appropriate periodization. On a month-by-month basis, using x2-analysis, the frequency of training injuries reflected training exposure (Figure 3); to note, months when training duration was greater, such as in the preseason period, injury frequency was high. The frequency of training injuries did not, however, reflect the training intensity. Therefore, it could be suggested that when training intensity is $85% HRmax, injury does not necessarily result, but when exposure to training is prolonged, more injuries maybe more prevalent. In agreement with the present findings, other researchers have found a similar relationship between exposure and injury frequency (14,17,18). In this study, the players did not train for long periods of time in comparison to that reported by others (13). Indeed, training was often of a high intensity but short duration, using a predominance of soccer-specific intermittent training. This approach to training might explain the high relationship found between injury incidence and training intensity but further specific investigations are warranted. The low injury incidence for training (6.7 injuries per 1,000 hours of training exposure) was comparable with that previously reported (13), although match injury incidence (54.1 injuries per 1,000 hours of match exposure) was higher (13), although this could be a direct link to the increased number of games played. Match injury incidence has been found to be higher in certain circumstances. For instance, Dupont et al. (12) reported a match injury incidence of 97.7 per 1,000 hours of match exposure when players played 2 matches a week. Dvorak et al. (14) reported a match injury incidence of 81 per 1,000 hours of match exposure in the 2002 FIFA World Cup. The site, type, and severity of injuries reported within this investigation were within the ranges reported previously TM Journal of Strength and Conditioning Research Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. the TM Journal of Strength and Conditioning Research among other professional soccer players. Previous literature purports how a greater proportion of injuries occurred to the lower extremities (Table 1) (20,27–29,36). Results from this study concur with previous findings as a greater number of injuries, both during training and match-play, consisted of muscle strains, contusions, and ligament sprains (Table 2) (17,36). Therefore, the present sample of injuries in the studied team is representative of usual soccer injuries, and the conclusions of the study are more likely to be interpreted as providing knowledge on actual soccer. Relationships between injury incidence and anthropometrical and physiological variables were weak in this study, as also reported by others (18,24,35), possibly explained by the homogenous nature of the players. Considering that training intensity did seem to affect injury incidence, interestingly anthropometrical and physiological variables did not relate to injury incidence, other intrinsic risk factors, such as joint instability, functional skill, psychology (34) and other extrinsic factors such as playing surface and foul play (34,35) may have contributed to injury. Based on this information, it can be confirmed that the cause of injury is multifactorial, with this study highlighting training intensity being a significant factor. Participants within the study were elite-level footballers, and unique with respect to comparisons of previous research in the area of injury incidence and training intensity (19,25). Killen et al. (32) described that it is difficult to compare results obtained from semiprofessional/amateur players with those from professional players, therefore suggested research on professional players was required. Amateur players generally have lower cardiovascular endurance capability, strength, and skill base, which may predispose them to a greater injury risk (25). To date, this study is the only one having investigated the relationship between HR intensity and injury incidence in professional soccer players. As a result, the practical implication that injury incidence is highly related to high-intensity training is important considering the professional nature of the players, and the individual auditing. Continual bodily strain eliciting greater training durations at T-VHI levels during training may increase the odds of sustaining a match injury, but not the odds of sustaining a training injury. PRACTICAL APPLICATIONS In professional soccer, training is generally comprised of a variation of small-, medium-, and large-sided games alongside high-intensity intermittent bouts used as a time efficient and effective means of enhancing cardiovascular fitness (9,30,36). Such training methods may impose more stress on the body than more traditional training methods, with heart rates of .85% often being elicited (9,36). This is the first study to have examined the relationship between HR-based assessment of training intensity and injury incidence in soccer. Based on the data collected in this study, it is recommended that training intensity be considered as one of the many factors in injury prevention. Reducing the | www.nsca.com number of competitive match injuries among elite-level professional players may be possible if greater focus is placed on the training intensity and volume over a period of time, ensuring the potential reduction of fatigue or overuse injuries. In addition, it is important to understand the optimal TL at which adaptation occurs without raising the risk of injury. Therefore, monitoring training to ensure that optimal loading is not significantly exceeded, should be considered as vitally important at the elite level of professional soccer with respect to injury incidence. ACKNOWLEDGMENTS The authors thank Prof. Anthony Stewart, who advised on statistical approaches, and critically reviewed the article for statistical accuracy; Mr. Jordan White, who assisted with initial data compilation; the soccer players for their participation in the study; and the sport science and medical staff. REFERENCES 1. Alexiou, H and Coutts, AJ. A comparison of methods used for quantifying internal training load in women soccer players. Int J Sports Physiol Perform 3: 320–330, 2008. 2. Arnason, A, Andersen, TE, Holme, I, Engebretsen, L, and Bahr, R. Prevention of hamstring strains in elite soccer: An intervention study. Scand J Med Sci Sports 18: 40–48, 2008. 3. Arnason, A, Sigurdsson, SB, Gudmundsson, A, Holme, I, Engebretsen, L, and Bahr, R. Physical fitness, injuries, and team performance in soccer. Med Sci Sports Exerc 36: 278–285, 2004. 4. Bahr, R and Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br J Sports Med 39: 324– 329, 2005. 5. Banister, EW. Modelling elite athletic performance. In: Physiological Testing of the High-performance Athlete. J.D. MacDougall, H.A. Wenger, and H.J. Green, eds. Champaign, IL: Human Kinetics, 1991. pp. 403–424. 6. Borresen, J and Lambert, MI. Quantifying training load: A comparison of subjective and objective methods. Int J Sports Physiol Perform 3: 16–30, 2008. 7. Carling, C, Le Gall, F, and Dupont, G. Are physical performance and injury risk in a professional soccer team in match play affected over a prolonged period of fixture congestion. Int J Sports Med 33: 36–42, 2012. 8. Chamari, K, Haddad, M, Wong del, P, Dellal, A, and Chaouachi, A. Injury rates in professional soccer players during Ramadan. J Sports Sci 30(Suppl 1): S93–S102, 2012. 9. Coutts, AJ, Rampinini, E, Marcora, SM, Castagna, C, and Impellizzeri, FM. Heart rate and blood lactate correlates of perceived exertion during small-sided soccer games. J Sci Med Sport 12: 79–84, 2009. 10. Coyle, EF. Physical activity as a metabolic stressor. Am J Clin Nutr 72: 512S–520S, 2000. 11. Dellal, A, Chamari, K, Pintus, A, Girard, O, Cotte, T, and Keller, D. Heart rate responses during small-sided games and short intermittent running training in elite soccer players: A comparative study. J Strength Cond Res 22: 1449–1457, 2008. 12. Dupont, G, Nedelec, M, McCall, A, McCormack, D, Berthoin, S, and Wisløff, U. Effect of 2 soccer matches in a week on physical performance and injury rate. Am J Sports Med 38: 1752–1758, 2010. 13. Dvorak, J and Junge, A. Football injuries and physical symptoms. A review of the literature. Am J Sports Med 28: S3–S9, 2000. VOLUME 29 | NUMBER 6 | JUNE 2015 | 1711 Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited. Training Load, Intensity, and Injury 14. Dvorak, J, Junge, A, Grimm, K, and Kirkendall, D. Medical report from the 2006 FIFA world cup Germany. Br J Sports Med 41: 578– 581, 2007. 15. Edwards, S. The Heart Rate Monitor Book. Sacramento, CA: Fleet Feet Press, 1993. 16. Eirale, C, Tol, JL, Farooq, A, Smiley, F, and Chalabi, H. Low injury rate strongly correlates with team success in Qatari professional football. Br J Sports Med 47: 807–808, 2013. 27. Hägglund, M, Waldén, M, Barhr, R, and Ekstrand, J. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br J Sports Med 39: 340–346, 2005. 28. Hägglund, M, Waldén, M, and Ekstrand, J. UEFA injury study-an injury audit of European Championships 2006 to 2008. Br J Sports Med 43: 483–489, 2009. 17. Ekstrand, J, Hägglund, M, and Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br J Sports Med 45: 553–558, 2011. 29. Hawkins, RD, Hulse, MA, Wilkinson, C, Hodson, A, and Gibson, M. The association football medical research programme: An audit of injuries in professional football. Br J Sports Med 35: 43– 47, 2001. 18. Ekstrand, J, Waldén, M, and Hägglund, M. Risk for injury when playing in a national football team. Scand J Med Sci Sports 14: 34–38, 2004. 30. Hoff, J, Wisløff, U, Engen, LC, Kemi, OJ, and Helgerud, J. Soccer specific aerobic endurance training. Br J Sports Med 36: 218–221, 2002. 19. Eriksson, LI, Jorfeldt, L, and Ekstrand, J. Overuse and distortion soccer injuries related to player’s estimated maximal aerobic work capacity. Int J Sports Med 7: 214–216, 1986. 31. Impellizzeri, FM, Rampinini, E, Coutts, AJ, Sassi, A, and Marcora, SM. Use of RPE-based training load in soccer. Med Sci Sports Exerc 36: 1042–1047, 2004. 20. Faude, O, Jung, A, Kindermann, W, and Dvorak, J. Risk factors for injuries in elite female soccer players. Br J Sports Med 40: 785–790, 2006. 32. Killen, NM, Gabbett, TJ, and Jenkins, DG. Training loads and incidence of injury during the preseason in professional rugby league players. J Strength Cond Res 24: 2079–2084, 2010. 21. Foster, C, Florhaug, JA, Franklin, J, Gottschall, L, Hrovatin, LA, Parker, S, Doleshal, P, and Dodge, C. A new approach to monitoring exercise training. J Strength Cond Res 15: 109–115, 2001. 33. Little, T and Williams, AG. Suitability of soccer training drills for endurance training. J Strength Cond Res 20: 316–319, 2006. 22. Fuller, CW, Ekstrand, J, Junge, A, Andersen, TE, Bahr, R, Dvorak, J, Hägglund, M, McCrory, P, and Meeuwisse, WH. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med 40: 193–201, 2006. 23. Gabbett, TJ. Influence of training and match intensity on injuries in rugby league. J Sports Sci 22: 409–417, 2004. 34. Mallo, J, González, P, Veiga, S, and Navarro, E. Injury incidence in a Spanish sub-elite professional football team: A prospective study during four consecutive seasons. J Sports Sci Med 10: 731–736, 2011. 35. Östenberg, A and Roos, H. Injury risk factors in female European football. A prospective study of 123 players during one season. Scand J Med Sci Sports 10: 279–285, 2000. 24. Gabbett, TJ. Changes in physiological and anthropometric characteristics of rugby league players during a competitive season. J Strength Cond Res 19: 400–408, 2005. 36. Owen, A, Wong del, P, McKenna, M, and Dellal, A. Heart rate responses and technical comparison between small-vs. large-sided games in elite professional soccer. J Strength Cond Res 25: 2104– 2110, 2011. 25. Gabbett, TJ and Dumrow, N. Relationships between training load, injury, and fitness in sub-elite collision sport athletes. J Sports Sci 25: 1507–1519, 2007. 37. Rhea, MR, Lavinge, DM, Robbins, P, Esteve-Lanao, J, and Hultgren, TL. Metabolic conditioning among soccer players. J Strength Cond Res 23: 800–806, 2009. 26. Haddad, M, Chauochi, A, Castagna, C, Wong, DP, Behm, DG, and Chamari, K. The construct validity of session RPE during an intensive camp in young male taekwondo athletes. Int J Sports Phys Perform 6: 252–263, 2011. 38. Schmikli, SL, de Vries, WR, Inklaar, H, and Backx, FJG. Injury prevention target groups in soccer: Injury characterstics and incidence rates in male junior and senior players. J Sci Med Sport 14: 199–203, 2011. 1712 the TM Journal of Strength and Conditioning Research Copyright © National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.