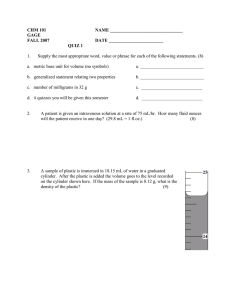
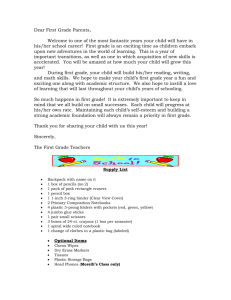
Propionibacterium acnes Suture Contamination in Arthroscopic Rotator Cuff Repair: A Prospective Randomized Study Kotaro Yamakado, M.D., Ph.D. Purpose: To examine the contamination rate of the anchor-suture and to determine the efficacy of 2 different surgical skin preparation solutions with or without a plastic adhesive drape from suture contamination in arthroscopic rotator cuff repair. Methods: A prospective randomized study was undertaken to evaluate 126 consecutive patients undergoing arthroscopic rotator cuff repair. Each shoulder was prepared with one of 2 randomly selected solutions according to an assigned envelope that indicated the procedure to be used: chlorhexidine-alcohol (1% chlorhexidine gluconate and 70% isopropyl alcohol) or povidone-iodine. Then, each group was further divided according to the usage of a plastic drape. The first cut-tails of the anchor-suture after cuff fixation were submitted to aerobic and anaerobic cultures. Results: The overall rate of Propionibacterium acnesepositive cultures was 47% (14 of 31 cases) in the povidone-iodine group, 33% (11 of 33 cases) in the povidone-iodine with a drape group, 33% (10 of 30 cases) in the chlorhexidine-alcohol group, and 9.3% (3 of 32 cases) in the chlorhexidine-alcohol with a drape group. The positive culture rate in the chlorhexidinealcohol with a drape group was lower than that in the povidone-iodine group (relative risk, 0.2; 95% confidence interval: 0.064-0.63; number needed to treat, 2.7; P < .0001). Coagulase-negative staphylococci were isolated in the povidone-iodine with a drape (1 case) and chlorhexidine-alcohol with a drape group (2 cases). No other bacteria were isolated, and no infections occurred in any of the patients treated in this study during the minimum 12-month follow-up period. Conclusions: Chlorhexidine-alcohol solution with an adhesive plastic drape was more effective than chlorhexidine-alcohol without a plastic drape and povidone-iodine with/without a plastic drape in eliminating P acnes suture contamination. However, the usage of a plastic drape slightly increased the risk of coagulase-negative Staphylococcus proliferation. Level of Evidence: Level I, therapeutic, prospective, randomized trial. See commentary on page 1156 D eep infection following shoulder arthroscopy is a rare but severe problem. Several techniques are used to prevent bacteria from entering the surgical site. The use of an effective skin preparation solution could play a significant role in preventing such infections. However, because the main factors affecting bacterial growth are temperature, pH, water, and nutrients, the wet surgical field and body temperature during arthroscopic procedure favor bacterial proliferation. From the Department of Orthopaedics, Fukui General Hospital, Fukui, Japan. The author reports that he has no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material. Received July 27, 2017; accepted October 13, 2017. Address correspondence to Kotaro Yamakado, M.D., Ph.D., 58-16-1 Egami, Fukui, Fukui 9108561, Japan. E-mail: yamakadok@gmail.com Ó 2017 by the Arthroscopy Association of North America 0749-8063/17878/$36.00 https://doi.org/10.1016/j.arthro.2017.10.029 Moreover, skin preparation solutions are washed out with irrigation fluid after surgery begins, and induced hypothermia by fluid extravasation increases the risk of surgical site infections (SSIs).1-6 Propionibacterium acnes, which is part of the normal skin microbiome, has been implicated as one of the most common causal organism associated with shoulder surgeries.6-11 Researchers have warned that standard surgical skin preparation solutions are often inadequate at sterilizing the incision site because propionibacteria typically reside in the pilosebaceous glands.6-11 In particular, during the arthroscopic rotator cuff repair procedure, sutures loaded on the suture anchors can be exposed on the skin until the rotator cuff fixation of knotted or knotless configurations (Fig 1). The commonly used braided sutures have higher water absorbency than monofilament sutures, which pose a risk of contamination and infection. P acnes infections are known as the “stealth” infection, and prevalence of these infections after shoulder Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 34, No 4 (April), 2018: pp 1151-1155 1151 1152 K. YAMAKADO Fig 1. Sutures are exposed on the skin during the arthroscopic rotator cuff repair. surgery is likely underreported.6-11 Clinical presentation of P acnes infection is often nonspecific and typically lacks features of fever, erythema, or wound drainage. Most cases only demonstrated impaired range of motion (stiffness) and pain. The surgeon must maintain a high index of suspicion to identify this type of infection, especially in a patient with unexplained pain and stiffness after shoulder arthroscopy. However, correct diagnosis is extremely difficult. In the majority, the erythrocyte sedimentation rate and C reactive protein level are normal or nearly normal.6-11 Because of its slowly growing characteristic, isolating P acnes may require up to 3 weeks when using culture-based methods.6-11 Thus, effective preventive measures are of utmost importance. The objectives of this study were to examine the contamination rate of the anchor sutures and to determine the efficacy of 2 different surgical skin preparation solutions with or without a plastic adhesive drape from suture contamination of P acnes and other bacteria in the arthroscopic rotator cuff repair procedure. Our hypothesis was that the application of chlorhexidine-alcohol solution with a drape was more effective than chlorhexidine-alcohol without a drape and povidone-iodine with/without a drape in eliminating suture contamination. Methods In this study, data were obtained in a prospective randomized fashion between August 2015 and February 2016 (Fig 2). All procedures were performed by the author, and randomization was performed at the end of anesthetic induction: the disinfectant solution used for each patient was chosen by opening a sealed, randomly assigned envelope that indicated the agent to be used; then another sealed, randomized assigned envelope was opened to determine whether to use a plastic drape. This study was approved by the institutional review board, and every patient provided informed consent before the study began. Notably, Fig 2. Flow diagram showing enrolment, allocation, and analysis of patient. PROPIONIBACTERIUM ACNES SUTURE CONTAMINATION chronically immunosuppressed patients and those with an open wound, a current infection, or any prior shoulder surgery were excluded from this study. Preoperative antibiotics (i.e., 1 g of cefazolin, noneweight-adjusted) were administered to all patients enrolled in this study. All patients were positioned in the beach-chair position with the arm held in flexion and with 1 to 3 kg of longitudinal traction, according to their body weight. Each shoulder was prepared with one of 2 randomly selected solutions according to a randomly assigned envelope that indicated the procedure to be used: chlorhexidine-alcohol (1% chlorhexidine gluconate and 70% isopropyl alcohol) or povidone-iodine. Then, each group was further divided according to the usage of a plastic drape. The shoulder was draped. The superficial anatomy was identified: the skin was marked to outline the clavicle, acromion, scapular spine, coracoid process, and lateral border of the scapula. In groups with the plastic adhesive drapes, antibacterial nonimpregnated barriers (Steri-Drape; 3M Healthcare, St. Paul, MN) were applied. The Arthropump (ConMed Linvatec, Largo, FL) was turned on, and the pressure was set at 50 mmHg. The routine arthroscopy portals were used (i.e., posterior, lateral, anterior, and anterolateral), and diagnostic arthroscopy using a 30 arthroscope was initiated using a standard posterior portal. The viewing portal was subsequently changed to a lateral portal (midway between the anterolateral and posterolateral acromial corner). A standard arthroscopic rotator cuff repair was performed using 1 to 5 suture anchors; all rotator cuff tears were repaired using a Healix Ti or a Healix BR (DePuy-Synthes) loaded 3 high-strength sutures, Orthocord (DePuy-Synthes). The number of anchors was decided according to the tear size and repair configuration in terms of the single-row or suture-bridge repair. The anchor was placed through the plastic cannula, and the anchor sutures were retrieved from the anterior or posterior working portals and exposed on the skin. The sutures were passed using a retrograde suture passer (Spectrum II; ConMed Linvatec). The first cut tail of the anchor suture after tying the knot was submitted for aerobic and anaerobic culturing. The sutures exposed on the skin for more than 30 minutes were excluded. The culture specimens were retrieved, sealed, and delivered to a microbiology laboratory within 30 minutes. Patients were clinically evaluated for infection (e.g., erythema, warmth, and excessive pain with passive range of motion) at 10 days, 28 days, 3 months, 6 months, and 12 months postoperatively. Each sample was plated on a blood agar plate and a bromothymol blue lactose agar plate for 2 days and plated on Brucella blood agar plate for 21 days. Positive P acnes cultures were identified as anaerobic, gram-positive rods with confirmation by BD BBL Crystal ID system (Becton, Dickinson, Franklin Lakes, NJ). 1153 Postoperative Care The patients were immobilized with an abduction pillow for 4 to 6 weeks. Passive range-of-motion exercises were initiated postoperatively from the first postoperative day. Strengthening exercises commenced at 12 weeks postoperatively. Sample Size and Statistical Analysis Sample size calculation was based on a pilot nonrandomized, prospective cohort study performed with povidone-iodine solution without a drape, which included various arthroscopic shoulder procedures using multiple sutures and demonstrated a 50% (21 of 42 patients) contamination rate of P acnes, indicating a baseline failure rate of 0.5. If the true relative risk of failure for experimental subjects relative to controls is 0.3, we will need to study 27 experimental subjects and 27 control subjects to be able to reject the null hypothesis that this relative risk equals 1 with a probability (power) of 0.8. Given the anticipated dropout of 10%, it was concluded that a minimum of 30 patients should be enrolled into each group to detect a large (30% to 50%) difference in contamination rates between groups. The type I error probability associated with this null hypothesis testing is 0.05. Demographic and clinical characteristics of groups were examined by comparative multivariate analysis. Categorical variables were evaluated using frequencies and proportions, associations were tested with c-square tests, and continuous variables were assessed using analysis of variance. Results This prospective randomized study enrolled 126 consecutive patients who underwent arthroscopic rotator cuff repair (Fig 2). Table 1 shows the demographic characteristics of the patients. No significant differences were observed among the 4 groups for any assessed variables (i.e., age, gender, tear size, body mass index, and presence of diabetes mellitus). The overall rate of P acnesepositive cultures was 47% (14 of 31 cases) in the povidone-iodine group, 33% (11 of 33 cases) in the povidone-iodine with a drape group, 33% (10 of 30 cases) in the chlorhexidine-alcohol group, and 9.3% (3 of 32 cases) in the chlorhexidinealcohol with a drape group (Table 2). The positive culture rate in the chlorhexidine-alcohol with a drape group was lower than that in the povidone-iodine group (relative risk, 0.2; 95% confidence interval: 0.064-0.63; number needed to treat, 2.7; P < .0001). Coagulase-negative Staphylococcus were isolated in the povidone-iodine with a drape group (1 of 31 cases, 3%) and in the chlorhexidine-alcohol with a drape group (2 of 32 cases, 6%). No other bacteria were isolated, and no infections occurred in any of the patients treated in this study during the minimum 12-month follow-up period. 1154 K. YAMAKADO Table 1. Demographic Data Age, y, M SD Sex, male-female Cuff tear size, n Partial Small to medium Large to massive BMI, M SD DM, n (%) Povidone-Iodine (n ¼ 31) 67.4 6.4 24:7 Povidone-Iodine With Plastic Drape (n ¼ 33) 67.7 7.7 25:8 Chlorhexidine-Alcohol (n ¼ 30) 64.8 7.9 19:11 Chlorhexidine-Alcohol With Plastic Drape (n ¼ 32) 66.0 7.2 20:12 P Value .35 .42 23 7 30 24.8 3.4 4 (12.9) 25 8 33 23.9 2.9 7 (21.2) 19 11 30 23.3 3.2 5 (16.7) 20 12 32 24.1 2.6 6 (18.8) .26 .88 BMI, bone mass index; DM, diabetes mellitus; M, mean; SD, standard deviation. Discussion Although the purpose of this study was to assess the suture contamination that does not necessarily imply infection, contaminated suture could be the potential source of SSI. This study demonstrated that the overall rate of P acnesepositive cultures was 30.4%, and about half of the patients (47%) in the povidone-iodine group were contaminated. Conversely, the contamination rate decreased with using the chlorhexidine-alcohol solution and applying a plastic adhesive drape; however, the possibility of contamination could not be eliminated in this group. Anchor sutures exposed on the wet surgical field were considered to be the potential source of contamination/infection; therefore, the use of cannula during insertion of the anchor or passing sutures may minimize the contamination risk. The number of suture-passing attempts should be minimized so as not to introduce the contaminated part of the suture. Furthermore, we recommend not using the remaining part of the cut suture tail if it was considerably longer for the side-to-side fixation. In this study, the application of an adhesive plastic drape demonstrated a reduction in P acnes contamination; however, positive cultures of coagulase-negative Staphylococcus were observed in only plastic drape groups. Whether using the plastic drape decreases SSIs is a matter of debate,12-15 because no Level I or II study has demonstrated the reduction of SSI with the plastic drape application. The 2017 CDC guidelines15 described that the use of plastic adhesive drapes with or without antimicrobial properties is not necessary for the prevention of SSI (Category IIdweak recommendation; high- to moderate-quality evidence suggesting a tradeoff between clinical benefits and harms). In fact, several studies have suggested that a plastic drape may increase the risk of infection.12-14 For example, FalkBrynhildsen et al. performed a randomized controlled study in cardiac surgery patients to compare the bacterial growth in a wound with a plastic adhesive drape and the recolonization time of the adjacent skin intraoperatively13; their study found that the adhesive drape did not reduce bacterial recolonization. Another study reported that recolonization of the skin was faster in the plastic drape group than in the group without a plastic drape, and significantly more positive cultures were identified in the plastic drape group than in the group without a drape.14 Other technical concerns in using a plastic drape were ripping and involving a part of the removed drape during anchor or cannula insertion. Hence, the application of a plastic drape would be determined on a case-by-case basis such as male gender, anticipated operative time, and comorbidity conditions. This study established better results with chlorhexidine-alcohol solution than povidone-iodine. Several researchers reported that a chlorhexidinealcohol solution showed better results in disinfection.8-18 The 2017 CDC Guidelines15 suggest performing Table 2. Positive Culture Rate With Respect to Skin Preparation Positive culture of Propionibacterium acnes Relative risk 95% confidence interval P value NNT NNT, number needed to treat. *Statistically significant (c2 test). Povidone-Iodine (n ¼ 31) 47% (14/31 cases) 1 Povidone-Iodine With Plastic Drape (n ¼ 33) 33% (11/33 cases) Chlorhexidine-Alcohol (n ¼ 30) 33% (10/30 cases) Chlorhexidine-Alcohol With Plastic Drape (n ¼ 32) 9.3% (3/32 cases) 0.71 0.39, 1.32 .28 7.5 0.71 0.38, 1.35 .29 7.5 0.2* 0.064, 0.63 .001 2.7 PROPIONIBACTERIUM ACNES SUTURE CONTAMINATION intraoperative skin preparations with an alcohol-based antiseptic agent unless contraindicated (Category IAdstrong recommendation; high-quality evidence). Hence, we considered chlorhexidine-alcohol solution as a better option for arthroscopic shoulder surgery. Limitations There were several limitations in this study. First, the exposure time of the suture was not standardized (although less than 30 minutes in all samples) and no control suture was placed (a suture that was placed but immediately removed to determine the “baseline” contamination rate). Second, the surgical time and the length of time from the scrub to the time when the suture specimen was obtained were not measured in this prospective protocol. Third, the suture was standardized in Orthocord. Masini et al.19 suggested that the bacterial adherence to high-strength sutures varies according to the product, and Orthocord has significantly less bacterial adherence than MaxBraid (Zimmer-Biomet) and FiberWire (Arthrex). Fourth, although several different subtypes of P acnes have been identified that may explain the diversity in clinical manifestation of P acnes infection; these variations were not considered in this study. Finally, chlorhexidine gluconate is available in a variety of concentrations (0.5%-4%). Further studies are required to determine the efficacy of lower or higher concentrations. Conclusions Chlorhexidine-alcohol solution with an adhesive plastic drape was more effective than chlorhexidinealcohol without a plastic drape and povidone-iodine with/without a plastic drape in eliminating P acnes suture contamination. However, the usage of a plastic drape slightly increased the risk of coagulase-negative Staphylococcus proliferation. References 1. Insler SR, Sessler DI. Perioperative thermoregulation and temperature monitoring. Anesthesiol Clin 2006;24: 823-837. 2. Kurz A. Thermal care in the perioperative period. Best Pract Res Clin Anaesthesiol 2008;22:39-62. 3. Putzu M, Casati A, Berti M, Pagliarini G, Fanelli G. Clinical complications, monitoring and management of perioperative mild hypothermia: Anesthesiological features. Acta Biomed 2007;78:163-169. 4. Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N Engl J Med 1996;334: 1209-1215. 1155 5. Portillo ME, Corvec S, Borens O, Trampuz A. Propionibacterium acnes: An underestimated pathogen in implantassociated infections. Biomed Res Int 2013;2013:804391. 6. Achermann Y, Goldstein EJ, Coenye T, Shirtliff ME. Propionibacterium acnes: From commensal to opportunistic biofilm-associated implant pathogen. Clin Microbiol Rev 2014;27:419-440. 7. Horneff JG, Hsu JE, Voleti PB, O’Donnell J, Huffman GR. Propionibacterium acnes infection in shoulder arthroscopy patients with postoperative pain. J Shoulder Elbow Surg 2015;24:838-843. 8. Hsu JE, Bumgarner RE, Matsen FA 3rd. Propionibacterium in shoulder arthroplasty: What we think we know today. J Bone Joint Surg Am 2016;98:597-606. 9. Pinder EM, Ong JC, Bale RS, Trail IA. Ten questions on prosthetic shoulder infection. Shoulder Elbow 2016;8: 151-157. 10. Leheste JR, Ruvolo KE, Chrostowski JE, et al. P. acnesdriven disease pathology: Current knowledge and future directions. Front Cell Infect Microbiol 2017;7:81. 11. Atesok K, MacDonald P, Leiter J, McRae S, Stranges G, Old J. Postoperative deep shoulder infections following rotator cuff repair. World J Orthop 2017;8:612-618. 12. Webster J, Alghamdi AA. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev 2007;4:CD006353. 13. Falk-Brynhildsen K, Söderquist B, Friberg O, Nilsson UG. Bacterial recolonization of the skin and wound contamination during cardiac surgery: A randomized controlled trial of the use of plastic adhesive drape compared with bare skin. J Hosp Infect 2013;84:151-158. 14. Falk-Brynhildsen K, Friberg O, Söderquist B, Nilsson UG. Bacterial colonization of the skin following aseptic preoperative preparation and impact of the use of plastic adhesive drapes. Biol Res Nurs 2013;15:242-248. 15. Berríos-Torres SI, Umscheid CA, Bratzler DW, et al. Healthcare Infection Control Practices Advisory Committee. Centers for Disease Control and Prevention Guideline for the prevention of surgical site infection. JAMA Surg 2017;152:784-791. 16. Uppal S, Bazzi A, Reynolds RK, et al. Chlorhexidinealcohol compared with povidone-iodine for preoperative topical antisepsis for abdominal hysterectomy. Obstet Gynecol 2017;130:319-327. 17. Darouiche RO, Wall MJ, Itani KM, et al. Chlorhexidinealcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med 2010;362:18-26. 18. Mimoz O, Lucet JC, Kerforne T, et al., CLEAN trial investigators. Skin antisepsis with chlorhexidine-alcohol versus povidone iodine-alcohol, with and without skin scrubbing, for prevention of intravascular-catheterrelated infection (CLEAN): An open-label, multicentre, randomised, controlled, two-by-two factorial trial. Lancet 2015;386:2069-2077. 19. Masini BD, Stinner DJ, Waterman SM, Wenke JC. Bacterial adherence to high-tensile strength sutures. Arthroscopy 2011;27:834-838.