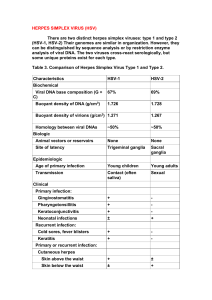
MINISTRY OF HEALTH OF UKRAINE VINNITSA NATIONAL PIROGOV MEMORIAL MEDICAL UNIVERSITY “ Approved ” on methodical meeting of the department of skin and venereal diseases record № 1 Heard of department ________prof. Bondar S.А. «_27_»__August_2021_ GUIDELINES for independent work of students in preparation to a practical lesson Academic discipline Theme of the lesson № 6 Dermatology and venereology Diseases due to virus infection. Etiology. Pathogenesis. Classification. Clinical features. Diagnostics. Treatment. Prevention. Course 4 Faculty Medical faculty Vinnytsia VINNITSA NATIONAL PIROGOV MEMORIAL MEDICAL UNIVERSITY Department of skin and venereal diseases Guideline of the practical lessons on dermatovenerology for self-study students of fourth year of medical faculty MODULE I THEMATIC MODULE 3 LESSON 6 Theme: DISEASES DUE PATHOGENESIS. TO VIRUS INFECTION. CLASSIFICATION. CLINICAL DIAGNOSTICS. TREATMENT. PREVENTION. Amount of hours for lesson: 2 ETIOLOGY. FEATURES. Guideline for self-study of students for practical lesson Module I . Dermatology and Venereology Thematic module 3. Сontagious Dermatoses LESSON 6 Diseases due to virus infection. Etiology, pathogenesis. Classification. Clinical features. Diagnostics. Treatment. Prevention.. 1. Theme urgency Dermatoses of virus etiology form a rather large and frequently encountered group of skin diseases. It includes herpes, warts, molluscum contagiosum, and condyloma acuminatum. These diseases are quite common among children, particularly from the age of 5 years (virus dermatoses are recorded most in 5- to 8-year-old children). Virus diseases of the skin account for 3 to 4 per cent of adult and 9.5 per cent of child cases with dermatoses. Though the virus flora may be transmitted by the intrauterine route, during delivery or in the first days of the infant's life, the disease does not develop then because antivirus antibodies are transferred in the mother's blood, which causes passive immunity in the fetus and the infant. This immunity weakens by the beginning of the second year of life, owing to which virus dermatoses may develop. The virus enters the body by various routes: through the skin, contaminated articles or mucous membranes (during sexual intercourse with a sick person or virus carrier, through kissing) and with droplets. In the absence of or reduced immunity, the incubation period ranges from a few days to two or three weeks. 2. Concrete Objectives: Students must know: 1. The etiology and pathogenesis of viral infection. 2. Clinical forms of viral infection. 3. Treatment and prevention of viral infection. Students should be able to: 1. 2. 3. 4. To collect the medical history of patient with viral infection. To diagnose viral infection in patient in typical case. To prescribe the treatment for patient with viral infection in typical case. To recommend preventive measures for patient with viral infection. 3. Tasks for self-study during preparation for lesson. 3.1. Theoretical questions for the lesson: 1. 2. 3. 4. 5. 6. The etiology and pathogenesis of herpes simplex. Clinical forms of herpes simplex. Treatment and prevention of herpes simplex. The etiology, pathogenesis and clinical picture of herpes zoster. Treatment of herpes zoster. The etiology, pathogenesis and clinical forms of warts (verruca vulgaris, verruca palmaris or plantaris, verruca plana, condyloma acuminatum). 7. Treatment and prophylaxis of warts. 8. The etiology, pathogenesis and clinical picture of molluscum contagiosum. 9. Treatment and prevention of molluscum contagiosum. The subject-matter: HERPES SIMPLEX Herpes simplex virus (HSV) infection is one of the most commonly encountered human viral infections. HSV is a double-stranded DNA virus that is subdivided into two closely related types: HSV-1 and HSV-2. Oral-facial herpes is most commonly caused by HSV-1, while HSV-2 is most frequently implicated in genital lesions. It has been estimated that there are more than 500 000 new cases of genital HSV per year in the United States. Infection most often results from direct mucous membrane or skin contact between an infected individual and an uninfected individual. The risk factors for primary infection therefore include unprotected sexual contact and kissing. Other well described but less commonly encountered modes of transmission include nonsexual rubbing, as occurs with wrestlers and rugby players, and herpetic whitlow, acquired when health or dental workers have contact with an infected patient. Infections with either HSV-1 or HSV-2 occur either at mucosal surfaces or at sites of abraded skin. The virus infects epidermal and dermal cells, causing vesicles as a result of an influx of fluid containing free virus and degenerated epithelial cells. Sensory and autonomic nerve endings also are infected, with the virus traveling to the nucleus through retrograde axonal flow. In the sensory ganglia, the virus establishes latent infection for the lifetime of the host. During reactivation, the virus actively replicates, leading to lesions in the distribution of the affected nerve. Once a patient has undergone primary infection, he or she may experience intermittent recurrences. Although they are not necessary for a recurrence to occur, certain factors put a patient at risk of a recurrence, including ultraviolet (UV) radiation, tissue injury, stress, and menstruation. In recent years, it has been determined that asymptomatic virus shedding occurs with greater frequency than was previously recognized. Indeed, asymptomatic viral expression is much more common that are symptomatic episodes. Patients infected with HSV who have no sings or symptoms of active infection have cultures positive for virus between 1 and 7 percent of the days when they are tested. This asymptomatic shedding may result in infection of the sexual partners of an affected individual. The disease is characterized by eruption, on a hyperemic area, of grouped vesicles filled with a clear and then cloudy content. The favoured sites are the lips (herpes labialis), cheeks (herpes facialis), the wings of the nose (herpes nasalis), oral mucosa (herpes buccalis), cornea (herpes cornealis), and genitals (herpes genitalis). The vesicles dry into crusts which leave no scars when they drop off. Ruptured vesicles on the oral mucosa leave painful erosions with hyperemic swollen edges (aphthous stomatitis). The eruption tends to recur, which is facilitated by stress reactions to cooling, infectious diseases, overstrain, neuro-psychic and physical traumas, and insolation. Herpes simplex occurs after disorders of gastro-intestinal activity, pneumonia, toxicosis, insolation, febrile diseases (herpes febrilis), and in dysmenorrhea (herpes menstrualis). The eruption is often preceded by indisposition, a chill, restlessness, a sensation of burning, poor appetite, and insomnia. The regional lymph nodes are enlarged. The following clinical forms are distinguished: (1) mild (abortive) variety with rapid resolution of the few lesions that had erupted; (2) edematous form accompanied with bright hyperemia and marked swelling (e.g. on the cheeks); (3) severe form (herpes simplex ulcerosa); (4) zosteriform (herpes simplex zosteriformis); (5) frequently recurring form localized on the lips (vermilion border), buttocks, and external genitals. Histopathology. The characteristic findings are ballooning and, to a lesser extent, reticular degeneration of the epidermal cells and acantholysis. Intranuclear eosinophilic inclusions are found in the ballooning cells and dilated blood vessels, oedema, and mild perivascular infiltration in the dermal papillary layer. Diagnosis. In a typical clinical picture the diagnosis is easily made. Herpes simplex zosteriformis is distinguished from herpes zoster by the absence of pain irradiating along the distribution of the peripheral nerves. In aphthae the edges are not polycyclic. Polycyclic edges of the erosive surfaces, absence of sclerosis in the base, negative results of laboratory tests, and the medical history allow differential diagnosis with erosive hard chancre when herpes simplex is found on the genitals. The history of an acute onset of new or recurrent vesiculobullous lesions on an erythematous base is often highly suggestive of the diagnosis of HSV infection. However, adjunctive tests often are needed to confirm or establish the diagnosis. With any of the following techniques, the sensitivity of the test is highly dependent on the type of lesion sampled, with new vesicles giving the highest yield. Tzanck smear may be performed rapidly in the office and should demonstrate vitropathic multinucleated giant cells. This technique requires a great deal of training. In brief, a sharp sterile blade is used to gently scrape cells from the bottom of an erosion or from the lower portion of a vesicle roof, and this material is smeared onto a microscope slide. A Giemsa, or similar staining technique allows one to see the viropathic cells. This technique does not differentiate HSV from varicella zoster virus. Viral culture should grow HSV within 48 h. It is capable of differentiating HSV-1, HSV-2, and varicella zostervirus (VZV). As in the Tzanck procedure, a sharp sterile blade is used to gently scrape cells from the bottom of an erosion or from the lower portion of a vesicle roof, and this material is placed into a viral transport medium. Immediate transportation to a viral laboratory improves diagnostic sensitivity. In certain institutions, polymerase chain reaction (PCR) may also be used to detect HSV DNA. This is the fastest, most reliable, and most sensitive technique. In contrast to viral culture, PCR is less subject to specimen degredation, which quickly occurs if specimens are not immediately inocculated into culture media. Accordingly, the PCR technique is rapidly becoming the criterion standard for diagnosis and may replace all other techniques except Tzanck examination. ECZEMA HERPETICATUM KAPOSI Eczema herpeticum is also called Kaposi's varicelliform eruption or pustulosis vacciniformis. It develops in an eczematous child three to seven days after contact with a person who has herpes simplex. The clinical manifestations of the dermatosis are similar to those of disseminated herpes simplex. Disseminated grouped small uniloculated vesicles with an umbilicate depression in the centre and papulovesicular and pustular lesions form here and there on an erythematous and edematous area of the skin. Superficial scars remain after resolution of the vesicles. The mucous membranes of the genitals and oral cavity are often involved. The eruptions occur suddenly with severe toxicosis, sharp elevation of body temperature (up to 39-40° C), confused consciousness, and enlargement of the liver and lymph nodes. Pneumonia, meningeal phenomena and encephalitis, otitis, keratoconjunctivitis sometimes with corneal ulceration, and gastro-intestinal disorders may develop. In some cases the prognosis is unfavourable. The outcome may be fatal if the child is weak and asthenic and the viscera and nervous system are involved in the process. Prevention. Individuals with herpes simplex are not allowed to take care of children. Treatment. Patient education is an important first step in the management of patients with HSV infection. Particularly for genital HSV infection, counseling should be given regarding the natural history of herpes sexual and perinatal transmission, and methods to reduce such transmission. Patients should be informed that the lesions may recur, usually in the same location. They should be instructed that lesional contact should be avoided from prodrome until complete reepithelialization Since asymptomatic shedding of intact viral particles commonly occurs, this topic should be addressed clearly with patients. Additionally, condom use to prevent the transmission of genital HSV infection is prudent even between clinical recurrences, because of the possibility of asymptomatic shedding of the virus. Orolabial HSV frequently is triggered by intense sun exposure, and patients should use sunscreen on the face and lip balm containing a sunscreen. Treatment of herpetic infections is suppressive, not curative. Systemic treatment is clearly much more effective than is topical treatment. However, if systemic treatment is contraindicated or refused, topical treatment may play a minor role in viral suppression. Systemic Therapy Treatment of acute infection For patients with primary HSV infection, whether orofacial or genital, the best studied treatment is acyclovir 200 mg five times daily for 7 to 10 days. This treatment has been shown to decrease pain, new lesion formation, the duration of viral shedding, and the time to crusting and resolution. Since acyclovir is poorly absorbed and requires administration five times per day, it is no longer a treatment of choice. Treatment option that is superior to acyclovir include valacyclovir 500 mg orally twice a day for 7 to 10 days. Valacyclovir is better absorbed than is acyclovir and probably is more effective because of the need for less frequent dosing. The only patient groups for which acyclovir remains appropriate are children. Valacyclovir should be used with extreme caution in immunocompromised patients because of occurrences of thrombotic thrombocytopenic purpura in some patients during clinical trials. None of these treatments has been found to decrease the chance of future recurrences. Treatment of recurrent disease In treating recurrences of HSV infection, acyclovir and valacyclovir have all been found to be effective. Regardless of which one is used, these medications are more effective the earlier they are started. We recommend having patients get the prescription filled for the medication and keep it at home. They are instructed to begin taking the medication at the first tingling or other prodromal symptom they notice. Treatment regimens for recurrent HSV episodes for the various antiviral agents include the following: Acyclovir 200 mg five times a day for 5 days Acyclovir 400 mg three times a day for 5 days Valacyclovir 500 mg twice daily for 5 days In certain situations, one may wish to treat the patient prophylactically with antiviral therapy to prevent recurrences. Patients who are scheduled to undergo major cosmetic surgery on the face or extensive dental work should receive antiviral therapy in the doses used for recurrent HSV infections. Treatment should begin 2 days before the surgical procedure and continue for 5 days afterward. Suppressive therapy should be considered in patients who develop frequent recurrences and patients who develop erythema multiforme after HSV recurrences. Patients may be started on chronic therapy with either acyclovir 400 mg twice daily or valacyclovir 1 g once daily. Once adequate suppression has been established, patients should be tapered to the minimal effective dose. Topical Therapy Topical antiviral agents such as Zovirax have been found to decrease the duration of outbreaks slightly. In patients who refuse more effective systemic therapy and patients who believe that topical therapy is effective, these agents may be prescribed safely. Zovirax is a cream that should be applied every six waking hours for 4 days. Drying and disinfectant agents are used externally: 1-4 per cent silver nitrate solution, application of 1-2 per cent pyoktanin (gentian violet) solution, 30-50 per cent interferon ointment, Bonaphton, gossypol, tebrophenum, 1-3 per cent Florenal ointment. Mouth gargle with astringent disinfectant solutions containing calendula, potassium permanganate, ethoxydiaminoacridine lactate or hydrogen peroxide is prescribed in herpes simplex of the mouth. A disseminated and frequently recurring process is treated by intramuscular injections of 2-3 ml of interferonogen given every six hours for three days. Favourable results are produced by intradermal injections of polyvalent antiherpes vaccine (0.10.2 ml is injected at intervals of two or three days; treatment consists of two courses of five injections made with an interval of 10 days). Gamma globulin injections, autohemotherapy, and pyrogenal are prescribed to prevent recurrences. Broad spectrum antibiotics are given when concomitant pyococcal infection develops. HERPES ZOSTER Herpes zoster (HZ), also called shingles or zona, is caused by a neurotropic filterable varicella zoster virus (VZV). which resembles or is identical with the chickenpox virus in antigenic structure and the ability to grow in human embryonal tissues. The development of chickenpox in children who had been in contact with a patient suffering from herpes zoster confirms that these strains are related. Cases are known of adults who develop herpes zoster after contact with a child suffering from chickenpox. Lastly, there are cases in which the disease begins as typical herpes zoster and then transforms into chickenpox with the eruption spreading to the trunk and limbs. Latent infection in nerve root ganglions follows an attack of chicken pox; reactivation of latent VZV infection leads to a blistering disease limited to a single or adjacent dermatomes. This self-limited disease often leads to severe pain in the affected region long after the lesions are healed. During an attack of chicken pox, the varicella-zoster virus travels along the sensory nerve fiber centripetally to the spinal and cranial sensory ganglia where the virus establishes a life-long latent infection. On a later date, reactivation of the virus occurs in the ganglia where the virus is most numerous and is triggered by diminished immunity associated with advancing age, immunosuppression due to drugs or diseases like HIV infection or lymphoma, radiation or trauma. Clinical picture. Herpes zoster affects both sexes equally. Occurrence is sporadic, without any seasonal variation. About 10-20% of people are expected to develop HZ in their lifetime. People of all ages may be affected. Frequency increases with advancing age. Two-thirds of patients are over forty years of age. Prodromal phase: is dominated by constitutional symptoms like headache, photophobia, fever, and pain. The pre-eruptive pain may be of varying severity and may be deep aching, sharp neuralgic or there may be allodynia (pain produced by minor stimuli like touching). The pain may mimic acute abdomen, migraine, or myocardial ischemia. The pain is soon followed by a rash limited to one side of the body in the distribution of a single or 2-3 adjacent dermatomes. Redness, papules and plaques appear, may be associated with itching or burning sensation. After an incubation period (seven or eight days), the dermatosis is manifested by eruption of grouped vesicles on a hyperemic skin area corresponding to the segmental distribution of one or more nerves. The eruption is preceded by a prodromal period of attacks of pain along the distribution of the nerves, burning, hyperemia of the involved areas, general weakness, chill, and headache. The erupted vesicles are tense, the size of a pea, and are filled with a clear serous content. They coalesce and form foci of affection with finely scalloped edges. The eruptions are characteristically asymmetric and unilateral. The following clinical varieties are distinguished: (1) generalized herpes zoster (herpes zoster generalisatus, disseminatus) marked by bilateral and disseminated lesions; (2) herpes zoster haemorrhagicus, in which the clear contents of the vesicles turn purulent and then, when the process penetrates deeper into the dermis, becomes hemorrhagic; (3) herpes zoster gangraenosus, a severe form, in which the floor of the vesicles undergoes necrosis and scars form in their place; (4) mild (abortive) form; (5) bullous form characterized by the appearance of both vesicles and bullae. The lesions gets crusted and gradually heal over 2-4 weeks. Thoracic segments are most commonly involved (>50%) followed by cervical, trigeminal, lumbosacral dermatomes. Mucosa in the affected dermatome are also involved. Viraemia occur during the course of the illness and a few outlying vesicles may be found elsewhere on the body away from the involved dermatome. Tender, regional lymph node enlargement is common. Stable neuralgia and muscular pareses may remain at the site of the affection after the acute skin manifestations disappear. Localization of the process in the eyes (herpes zoster ophthalmicus) is a very dangerous condition, which sometimes terminates in ulceration of the cornea and panophthalmia. A severe form with involvement of the eyes is usually not encountered in children. Paresis of the trigeminal or facial nerve and loss of hearing are other grave complications. The disease may also be complicated by meningitis (herpes zoster meningitidem) and encephalitis. Infectious diseases, toxicosis, metabolic disorders, diseases of the blood, neuro-psychic overstress, cooling, and physical trauma promote the manifestation of the virus infection. The process usually occurs and exacerbates in the cold season (spring and autumn). Herpes zoster is encountered at any age, with the exception of very young children, among whom it is rare occurrence. Elderly and old patients with herpes zoster following an atypical recurrent course must be examined so as to rule out a malignant new growth and a disease of the blood. Herpes zoster may sometimes precede some forms of hemoderma. Complications: Post-herpetic neuralgia (PHN) is the dominant cause of morbidity in HZ. This is defined as pain persisting after 30 days of onset of rash. The incidence of PHN increases with advancing age. About 75% of patients above 70 years of age may develop this. PHN is limited to the site of the rash and can be extremely disabling, persisting for months to years. The degree of pain is not related to the extent or severity of vesicles or inflammation. Histopathology. Ballooning and reticular degeneration of the epidermal cells, intranuclear viral inclusions, and degenerative changes in the nerve fibres are demonstrated. Acute inflammatory polymorphonuclear infiltration predominantly of a lymphocyto-histiocytic character, oedema, and dilated blood and lymph vessels are found. Diagnosis. Prodromal pain. The irradiating pain preceding and often accompanying the eruption and the linear arrangement of grouped vesicles over the segmental distribution of the involved nerves distinguish herpes zoster from herpes simplex and erysipelas. Typical clinical features of grouped vesicles on an erythematous base in a dermatomal distribution is highly diagnostic. Tzank smear (smear from base of ruptured vesicle stained with Giemsa) reveals multinucleated giant cells. Direct immunofluorescence of cellular material to detect viral antigen. Culture or PCR for viral DNA Herpes zoster is a self-limiting disease. Complete, spontaneous recovery within 2 to 4 weeks is the rule. Some residual sensory change and post-inflammatory dyspigmentation, however, may remain in some. In immunocompromized individuals, severe affection with prolonged disease course and scarring may occur. Second attack of herpes is rare, but in HIV-infected individuals, frequent recurrences may occur. Treatment: Acute attack: salicylates and analgesics, sedatives, vitamins B1, B12, and C, gamma globulin injections, and interferonogens are prescribed. Antiviral therapy: acts best if initiated within 48 hours of onset. Acyclovir (800mg 5 times a day x 7-10 days) or valacyclovir (100mg twice daily x 7 days)). Antiviral therapy reduces acute pain and inflammation, reduce duration of disease and viral shedding and may reduce frequency of PHN. Physiotherapy is advisable, namely irradiation with ultraviolet rays, ultrasonics, indirect diathermy of the cervical sympathetic ganglia, diadynamic currents, procaine hydrochloride electrophoresis, circular procaine blockade, a 50 per cent interferon ointment phonophoresis. Topical antiviral therapy: Irritating treatment with ointments and baths is contraindicated in acute eruptions. External application of antivirus ointments (Bonaphton, Gossypol, Tebrophenum, Zovirax, Acyclovir) together with aniline dyes has a beneficial curative effect. A patient with an eruption is not allowed to take a bath or a shower. Prevention. Overcooling and toxicosis should be avoided. WARTS (VERRUCAE) Etiology and pathogenesis. Warts are caused by human papillomavirus (HPV). HPV is a circular, double-standed DNA virus. HPV infection is higly specific for epidermis, especially extremities. Certain types of HPV infection have been associated with the development of malignancy. A subclass of HPV has a malignant potential and may be found in certain cervical carcinomas. Classification of verrucae: 1. Verruca vulgaris or common wart is caused by various strains of human papilloma virus (HPV-2, HPV-4, HPV-29); 2. Verruca palmaris or plantaris (myrmecia or palmoplantar wart) is caused by various strains of human papilloma virus (HPV-1, HPV-2, HPV-4); 3. Verruca plana (HPV-3) 4. Condyloma acuminatum (HPV 6, HPV-11). The disease is contagious. The infection is transmitted either during direct contact from a sick individual to a healthy person or through infected objects. Traumas of the skin and its dryness, reduced pH of the skin water-lipid mantle, vegetoneurosis with acrocyanosis or hyperhidrosis facilitate the development of the disease. Common warts (verruca vulgaris). They are mostly encountered in children and youths and grow on the hands and feet and less frequently on the face. Clearly circumscribed, hard, painless, semispherical lesions appear, which are elevated above the skin surface. They have the colour of normal skin or are greyish or brownish and there is no inflammation. Their surface is granular and rough, sometimes with nodular structures. Their size varies from that of a pin-head to that of a lentil; large conglomerates may form when the warts coalesce. Warts on the planter surface of the foot and the palm are hardly elevated above the skin surface and are characterized by marked keratosis. The number of warts ranges from solitary lesions to several dozens. Histopathology. The histological picture is characterized by hyperkeratosis and papillomatosis. Treatment. Electrocoagulation or diathermocoagulation, curettage, freezing with trichloroacetic acid, solid carbon dioxide or liquid nitrogen (cryotherapy or cryodestruction) are conducted. Carbon dioxide Laser (1-3 séances). Colchicines, 2 per cent Oxolinum, 1-3 per cent Florenal, and gossypol ointments are applied and the lesions are treated with Fowler's solution, solcoderm, or pheresol composed of 40 per cent phenol and 60 per cent tricresol. Plane juvenile warts (verrucae planae juveniles) prevail among children and adolescents. These are slightly elevated, polygonal or rounded, flat hard lesions. They have a smooth surface and vary in size from the size of a millet to that of a lentil. In some cases they have the colour of normal skin, in others they are yellowish-pink or yellowish-brown. Multiple plane warts are usually scattered on the back of the hands, on the face (forehead), neck and forearms; less frequently they form in a line. Histopathology. Hyperkeratosis and acanthosis are characteristic findings. The diagnosis is made easily. The condition sometimes has to be differentiated from lichen planus in which the papules are characterized by a wax-like lustre, an 'umbilicate' depression in the centre, a violet-red colour, and itching. Treatment. External treatment is accomplished with keratolytic ointments containing salicylic, benzoic, and lactic acids and resorcinol. Exposure to erythema doses of ultraviolet rays or Bucky's rays, and interferon, gossypol, propolis, colanchoe, oxolinum, and bonaphton are prescribed. Plantar warts (verrucae plantares) are a variety of the common wart. Compression of the feet by footwear, traumas of the soles, and hyperhidrosis of the feet facilitate their formation. These warts occur sometimes on the nail bed on which they form hard and very painful excrescences. Plantar warts are round or oval and yellowish-brown. Because of the sharp tenderness, they make walking difficult; they resemble corns. They are usually few in number. Just as in the above-described forms of warts, the histological picture is marked by acanthosis, papillomatosis, and hyperkeratosis. Treatment. Liquid nitrogen (cryotherapy), colchamine ointment, and painting the lesion with a 10-20 per cent podophyllin solution are prescribed. The following astringent is recommended: Rp: Ac. salicylici 1.0 Ac. acetici 9.0 Collodii elastici 10.0 MDS. For external application The skin around the wart is smeared with zinc paste (to protect the surrounding tissues) and a collodion preparation containing 50 per cent potent substances is applied to the wart. This is repeated once a day for three or four days. A hot foot bath with sodium hydrocarbonate is then taken after which the collodion film and the softened horny masses are removed with scissor blades. The procedure is repeated until the 'root' of the wart is removed. Curettage is an effective method for the removal of plantar warts. CONDYLOMA ACUMINATUM Condyloma acuminatum (syn. moist warts, pointed warts) occur in individuals with poor hygienic habits. The virus may be transmitted during sexual intercourse. Gonorrheal, trichomonad, and discharges of other origin are important in the pathogenesis of the disease. Pointed warts are usually localized on the genitals and in the perianal region and in rare cases in the axillae and under the breasts in women. Small, soft, filiform pink warts form. When they coalesce, papillomatous growths resembling cauliflower or raspberries form. These growths may macerate and ulcerate. Some lesions have a pedicle (a narrow base). Secretion with an offending odour often accumulates between the condylomata. Diagnosis. It is important to differentiate moist condylomata from flat (syphilitic) condylomata. The latter have a wide base, a hard-elastic consistency, and no lobate structure, and very many Treponema pallidum organisms are found in their secretions. Other symptoms of the secondary syphilitic period and positive results of serologic blood tests help in making the diagnosis. Both pointed and flat condylomata may be found in a patient with syphilis at the same time. Treatment. Diathermocoagulation, electro-incision, cryotherapy, and curettage with Volkmann's sharp spoon are carried out. Condyloma acuminatum may be cauterized with a strong solution of potassium permanganate, trichloro-acetic acid, and a 20 per cent podophyllin solution or painted with a mixture of four parts of phenol and six parts of tricresol (pheresol). Cauterizing powder (resorcinol and talc in equal amounts) and colchamine ointment are prescribed. Factors favoring the development of condylomata acuminata are removed. MOLLUSCUM CONTAGIOSUM Molluscum contagiosum (MC) is a common, self-limited, benign viral infection of the skin caused by a member of the pox-virus group. MC is transmitted by close personal contact including sexual contact. The condition typically involves young children. In adults, the infection occurs with increased frequency in presence of HIV infection. The lesions of MC have a distinct appearance of firm papules and nodules with central depressions. MC is caused by molluscum contagiosum virus (MCV), which belongs to the pox-virus group of DNA viruses. It is one the largest known pathogenic viruses. There are more than one types of MCV , MCV1 being the most common type of virus causing MC worldwide, particularly among the children, while MCV2 is the common type found in HIV infected individuals. Transmission occurs by close personal contact and often through fomites – towels, bath, and swimming pools. The virus replicates within the cytoplasm of infected epidermal cells, pathologic changes induced by the virus leads to formations of large hyaline acidophilic masses inside the cytoplasm (known as molluscum bodies of Henderson-Paterson bodies). Localized hypertrophy of epidermis extends into the dermis without disrupting the basement membrane and also projects above the skin as a visible lesion. Secondary infection may lead to an inflammatory reaction. The incubation period is two to eight weeks. A nodule the size of a pea and the colour of normal skin or pearly-grey (mother-of-pearl) in appearance forms. It is semispherical with a crateriform depression in the centre and a caseous-like content. There are no subjective sensations. The nodules may be solitary or may occur in dozens (disseminated lesions). The favoured localization in children is on the face (around the eyes), neck, chest, and the back of the hands. In adults the lesions occur mostly on the external genitals, the pubis and abdomen which testifies to the possibility of the sexual route of infection. The following clinical variants are distinguished: Molluscum contagiosum miliare with multiple tiny lesions; Molluscum contagiosum pediculatum marked by pedunculated lesions; Molluscum giganteum with giant lesions formed after coalescence of smaller ones. Diagnosis. The following characteristic sign helps in making the diagnosis: a white gruellike caseous mass of keratotic cells and moluscous (ovoid) bodies is expressed from the central part of the nodule when it is compressed from the sides with forceps. Warts have neither a central depression nor a mother-of-pearl surface. Treatment. The nodules are expressed with forceps or removed by curettage with a sharp spoon after which the area of the affection is painted with a 5-10 per cent iodine tincture and a 3 per cent Oxolinum or interferon ointment is applied. Diathermocoagulation and cryotherapy are also conducted. Prevention: Avoidance of skin-to-skin contact with infected persons. Treatment of lesions prevents further spread and autoinoculation. Chlorination of swimming pools. Materials for self-checking: А. Tasks for self-checking: Tests for verification of initial level of knowledges 1. What lesions are characteristic for herpes simplex? 1) 2) 3) 4) 5) Tubercles; Vesicles; Erosions; Ulcers; Scars. 2. What are the favoured sites of herpes simplex? 1) 2) 3) 4) 5) Lips; Genitals; Mucous membranes of oral cavity; Skin of soles; Scalp. 3. Choose from following signs that correspond to the herpes zoster? 1) Bullae; 2) Ulcers; 3) Pain along the distribution of the nerves; 4) Vesicles; 5) Intense itch along the distribution of the nerves. 4. What forms of warts do you know? 1) 2) 3) 4) 5) Verruca vulgaris; Verruca plana; Pointed warts; Plantar warts; Plane juvenile warts. 5. What medicines are used for treatment of herpes simplex? 1) 2) 3) 4) 5) Prednisolon ointment; Nystatin ointment; Synthomycin emulsion; Tebrophenum; Salicylic ointment. 6. From what lesions the course of herpes simplex begin? 1) 2) 3) 4) 5) Tubercle; Nodule; Papula; Vesicle; Bulla. Literature. The basic: 1. Lecture on the theme. 2. Guideline for self-study of students by preparation for practical lesson 6. 3. Dermatology, Venereology. Textbook / [Stepanenko V.I, Shupenko M.M., Mikheiev O.G. et al.];under edit. of V.I.Stepаnenko. – Kyiv: KIM, 2013.–p. 226-241. 4. V.H. Koliadenko, T.P. Vysochanska, O.I. Denysenko. Dermatovenereology Modules, Kyiv AUS Medicine Publishing, 2010, p.45-52. 5. Yu. K.Skripkin and M.V. Milich. Skin and Venereal Diseases, English translation, Mir Publishers, 1981, p.270-280. The additional: 1. Family Medicine: textbook: in 3 books. – Book 3: . Multidisciplinary General Medical Practice Special part / L.S. Babinets, P.A. Bezditko, S.A. Bondar and et al. – Кyiv: AUS Medicine Publishing, 2020. – 616 p. (in English) 2. Fitzpatrick et al. Dermatology in General Medicine, 4th ed. New York, McGraw-Hill, 1993. 3. Fitzpatrick. Color Atlas and Synopsis of Clinical Dermatology, 3rd Edition, 1997. 4. J.A.A. Hunter, J.A. Savin and M.V. Dahl. Clinical Dermatology, 3rd Edition, 2002, p. 201210. 5. P.N Behl, A. Aggarwal, Govind Srivastava. Practice of Dermatology, 9th Edition, 2002, p.190-200. Tests from Krok – II LESSON 6 Diseases due to virus infection. Etiology. Pathogenesis. Classification. Clinical features. Diagnostics. Treatment. Prevention. 1. A patient complained about general weakness, fever, painful rash on his trunk skin . He has been suffering from this for 3 days. Objectively: lateral surface of trunk on the left is hyperemic and edematic, there are some groups of vesicles with serous and haemorrhagic contents. What is the most probable diagnosis? 1) Herpes zoster;* 2) Herpetiform Duhring's dermatosis; 3) Contact allergic dermatitis; 4) Microbial eczema; 5) Contact dermatitis simplex . 2. 2 days ago a patient presented with acute pain in the left half of chest, general weakness, fever and headache. Objectively: between the 4 and 5 rib on the left the skin is erythematous, there are multiple groups of vesicles 2-4 mm in diameter filled with transparent liquid.What diease are these symptoms typical for? 1) Herpes zoster* 2) Pemphigus 3) Herpes simplex 4) Streptococcal impetigo 5) Herpetiform Duhring’s dermatosis 3. A 27-year-old sexually active female complains of numerous vesicles on the right sex lip, itch and burning. Eruptions regularly turn up beforemenstruation and disappear 8-10 days later.What is themost likely diagnosis? 1) Herpes simplex virus* 2) Bartholinitis 3) Primary syphilis 4) Cytomegalovirus infection 5) Genital condylomata 4. A 67-year-old male patient complains of rash, severe pain in the subscapular region on the right. Objectively: skin in the right subscapular region is covered with linearly arranged pinkred edematous lesions that are somewhat infiltrated, and have clearboundaries. On the lesion surface there are vesicles with transparent exudate. What is the most likely diagnosis? 1) Herpes zoster* 2) Duhring dermatitis 3) Erysipelas 4) Atopic dermatitis 5) Impetigo