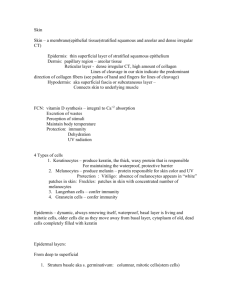
Hypopigmentation disorders Localized or generalized Congenital/hereditary or acquired Circumscribed, diffuse, linear or reticulated Hypopigmented skin: The only feature, the main feature, or part of a syndrome with other clinical manifestations Pigment cell biology Melanocytes: Pigment-producing dendritic cells of the skin, originated from the neural crest from where they migrate during embryogenesis; located mainly in the basal layer of the epidermis and the matrix of the hair follicle Melanosomes: Specific organelles in the cytoplasm of the melanocytes, where melanin is deposited As the melanosomes mature and acquire melanin, they move to a perinuclear position into the dendrites. Each melanocyte interconnects with 36 keratinocytes. These surronding keratinocytes phagocytize the tips of the melanosome-containing dendrites and transfer the pigment!!→→ normal skin pigmentation Leukoderma and Hypopigmentation Defects in the number or function of melanocytes Decrease melanization of melanosomes Decrease of the transfer process from melanocytes to keratinocytes VİTİLİGO Vitiligo is characterized clinically by development of totally white macules, microscopically by complete absence of melanocytes. Epidemiology Sex: Equal in both sexes. Age of onset: At any age, but in 50% between the ages of 10 and 30 yeras. A few cases at birth. Race:All races. Inheritance: Polygenic. > 30% have reported vitiligo in a parent, sibling or a child. Pathogenesis The autoimmune theory The neurogenic hypothesis The self-destruct hypotesis History After a -physical trauma ( Koebner), illness or emotional stress. After the death of a relative or after severe physical injury After a sunburn reaction Physical examination “Chalk” or pale white, sharply marginated macules, 5 mm to 5 cm or more in diameter Focal type, segmental type, generalized Around the eyes, mouth, digits, elbows, knees, low back, genital areas Associated cutaneous findings: White hair (poliosis), prematurely gray hair, alopecia areata, halo nevi. General examination: Up to 30% of cases associated with thyroid disease (Hashimoto thyroiditis, Graves’ disease); diabeytes mellitus (< 5%); pernicious anemia; Addison’disease( uncommon), MEN (rare). Differential diagnosis (1) Oculocutaneous albinism Fenilketonüri, homosistinüri, histidinemi (AR) Selenium and copper deficiency Pityriasis alba Pityriasis versicolor Chemical leukoderma (phenolic germicides) Leprosy Nevus depigmentosus (congenital, nonprogressif, stable in size, normal or decreased number of melanocytesdecrease in the synthesis and transfer of melanosomes, trunk, proximal extremities, isolated, segmental or systematized ( unilateral whorls and streaks) Nevus anemicus Secondary syphilis Differential diagnosis (2) Waardenburg’s syndrome (commonest cause of congenital sensorineural deafness, poliosis, white macules and white forlock, iris heterochromia, dystopia canthorum, broad nasal root, limb defects, Hirschprung disease) Tuberous sclerosis (multiple hypomelanotic macules, “ash leaf”, decreased number of melanosomes…. Decreased epidermal melanin, facial angiofibromas, periungual fibromas, CNS, retinal astrocytomas, cardiac rabdomyomas, dental enamel pits, hepatic, renal hamartoma, lung involvement) Piebaldism: congenital, complete absence of melanin and melanocytes or a reduced density, remain stable throughout life, white forelock, poliosis of the eyebrows and eyelashes, premature graying of the scalp hair, hyperpigmented macules in normal skin and within the areas of leukoderma, anterior trunk, mid extremities, mid forehead, frontal scalp, do auditory testing! (Woolf sndrome, WS), no treatment, sunscreens, minigrafts transplantation of uninvolved skin Differential diagnosis (3) Post-inflammatory leukoderma Menkes syndrome (X-linked recessif, inappropriate intracellular copper storage, pili torti,CNS involvement) Hypopigmented Mycosis Fungoides Vogt-Koyanagi-Harada Syndrome ( uveitis, vision problems, photophobia, bilateral dysacusia, CNS involvement, sensorineural hearing loss) Hypomelanosis of ITO: normal or decreased number of melanocytes and melanosomes, decreased melanin , neurocutaneous syndrome, whorled and streaked, linear lesions following the lines of Blaschko, trunk and extremities, at birth, during infancy or childhood, alopecia, teeth alterations, neurologic, musculuskletal, cardiac and ocular abnormalities Course and prognosis Chronic disease The course is highly variable. Up to 30%, spontaneous repigmentation in a few areas. Therapy Sunscreens Cosmetic coverup Repigmentation: Topical glucocorticoids, topical photochemotherapy, systemic photochemotherapy, narrow-band UVB, tacrolimus, pimecrolimus Minigrafting Depigmentation