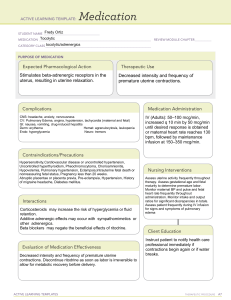
LIPPINCOTT ADVISOR FOR EDUCATION PROBLEM‐BASED CARE PLANS FOR STUDENTS Problem-Based Care Plan Worksheet WHAT ASSESSMENT DATA DOES THE NURSE FIND AS PERTINENT (RECOGNIZE CUES)? Short stature Prolonged stage of labor Gestational diabetes Turtle head Fetal heart rate within 120-130 Fatigue Anxiety Fast respirations Diaphoresis Advanced maternal age WHAT IS THE DISEASE PROCESS CAUSING THESE ASSESSMENT FINDINGS (ANALYZE CUES)? The problem occurs at the second stage of labor, when the fetal head is born but the shoulders are too broad to ender and be born through the pelvic outlet. This is hazardous to the woman because it can result in vaginal or cervical tears. It is hazardous to the fetus if the cord is compressed between the fetal body and the bony pelvis/ The force of birth can result in a fractured clavicle or a brachial plexus injury. WHAT IS THE MAIN PROBLEM WITH THE PATIENT THE NURSE CAN TREAT (PRIORITIZE HYPOTHESES)? Risk for injury (maternal) related to gestational diabetes secondary to short stature, advanced maternal age WHAT (GENERATE SOLUTIONS & TAKE ACTION)? CREATE ACHIEVABLE, REALISTIC, AND TIMETABLE (SMART) OUTCOMES. IS THE GOAL FOR THE PATIENT SPECIFIC, MEASURABLE, Patient will remain free from injury during delivery and birth a healthy baby with no post-partum complications. WHAT INTERVENTIONS WILL THE NURSE IMPLEMENT WHEN CARING FOR THIS PATIENT (GENERATE SOLUTIONS & TAKE ACTION)? INCLUDE THE EVIDENCE. LIST INTERVENTIONS IN ORDER OF PRIORITY. INCLUDE COLLABORATIVE AND NURSE‐INITIATED INTERVENTIONS. -Review the history of labor, onset, and duration: Helpful in identifying possible causes, needed diagnostic studies, and appropriate interventions. Uterine dysfunction may be caused by an atonic or a hypertonic state. Uterine atony is classified as primary when it occurs before the onset of labor (latent phase) or secondary when it occurs after well-established labor (active phase). -Note timing/type of medication(s). Avoid administration of narcotics or of epidural block anesthetics until the cervix is 4 cm dilated: A hypertonic contractile pattern may occur in response to oxytocin stimulation; sedation/analgesia given too early (or in excess of needs) can inhibit or arrest labor. -Note the condition of cervix. Monitor for signs of amnionitis. Note elevated temperature or WBC; odor and color of vaginal discharge: A rigid or unripe cervix will not dilate, impending fetal descent/labor progress. Development of amnionitis is directly related to length of labor, so that delivery should occur within 24 hr after rupture of membranes. -Assess uterine contractile pattern manually (palpation) or electronically via external, or internal monitor with internal uterine pressure catheter (IUPC): Dysfunctional contractions lengthen labor increasing the risk of maternal/fetal complications. -Evaluate the current level of fatigue, as well as activity and rest prior to onset of labor: Excess maternal exhaustion contributes to secondary dysfunction or may be the result of prolonged labor/false labor. Note effacement, fetal station, and fetal presentation: These indicators of labor progress may identify a contributing cause of prolonged labor. For example, breech presentation is not as effective a wedge for cervical dilation as is vertex presentation. -Evaluate degree of hydration. Note amount and type of intake: Prolonged labor can result in a fluid-electrolyte imbalance as well as depletion of glucose reserves, resulting in exhaustion and prolonged labor with increased risk of uterine infection, postpartal hemorrhage, or precipitous delivery in the presence of hypertonic labor. -Graph cervical dilation and fetal descent against time (i.e., Friedman curve): May be used on occasion to record progress/ prolongation of labor. -Review bowel habits and regularity of evacuation: Bowel fullness may hinder uterine activity and interfere with the fetal descent. -Encourage client to void every 1–2 hr. Assess for bladder fullness over symphysis pubis: A full bladder may inhibit uterine activity and interfere with the fetal descent. Place client in lateral recumbent position and encourage bed rest or sitting position/ambulation, as tolerated: Relaxation and increased uterine perfusion may correct a hypertonic pattern. Ambulation may assist gravitational forces in stimulating normal labor pattern and cervical dilation. -Have emergency delivery kit available: May be needed in the event of a precipitous labor and delivery, which are associated with uterine hypertonicity. -Remain with the client if possible, arrange for the presence of doula as appropriate; provide a quiet environment as indicated: Decrease external stimuli may be important to allow sleep after administration of medication to a client in the hypertonic state -Palpate the abdomen of thin client for the presence of pathological retraction ring between uterine segments: In obstructed labor, a depressed pathological ring (Bandl’s ring) may develop at the juncture of lower and upper uterine segments, indicating an impending uterine rupture. HOW WILL THE NURSE EVALUATE THE PATIENT'S RESPONSE (EVALUATE OUTCOMES)? AND WHAT WAS THE PATIENT’S RESPONSE TO THE INTERVENTIONS? WHAT OTHER PROBLEMS COULD THE NURSE LINK TO THIS PATIENT PROBLEM? Acute Pain related to prolonged stage of labor. Last Updated 1/12/2021 3|P a g e