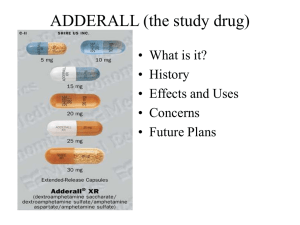
Amphetamines (Adderall, Adderall XR) General Prescribing Tip: Amphetamine (AMP) vs methylphenidate (MPH). New data recently suggested that, based on safety and efficacy, methylphenidate is a better choice in kids and adolescents whereas amphetamine-class agents are better in adults. Generally, this is a Coke vs Pepsi decision—some people like one better than the other, and you can’t predict their preference ahead of time. We recommend a methylphenidate over an amphetamine in most cases, because amphetamines may tend to have MORE side effects and are MORE likely to be abused or diverted. Dose Equivalents and Switching Strategies: From amphetamine to another amphetamine. With the exception of Vyvanse, all amphetamines, including both Adderall IR and XR, are roughly equivalent in potency. For example, if a patient is taking Dexedrine 10 mg TID, you can switch this to Adderall 15 mg BID or Adderall XR 30 mg QD. There is a belief that Dexedrine may be more potent than Adderall, but the effect is most likely negligible in most people. Vyvanse is composed of both lysine and amphetamine, with amphetamine making up only about 30% of Vyvanse. This means that it’s much less potent than straight Dexedrine. So, when switching from another amphetamine to Vyvanse, you have to at least DOUBLE the dose. Cross-tapering is not necessary when switching from an amphetamine to another amphetamine once dose equivalence is determined. Take stimulant A on day 1 and stimulant B (new) on day 2. The new stimulant may need to be started at a somewhat lower dose. Key Cardiovascular and Safety Concerns: Amphetamines should be avoided in patients with known or suspected cardiovascular disease. Asking about cardiac problems and consulting the child’s pediatrician or cardiologist must be done to explore if an issue exists. Amphetamines may cause hypertension and tachycardia. Adult vs Pediatric Prescription: Adults maximum Adderall ER dosage is 60mg/day, whereas the max dose is 30 mg/day for children, and adolescents max dose at 40 mg/day. Point of Interest from TCRP about Adult-onset ADHD: Adult-onset ADHD is a complex diagnosis which requires an extensive “rule out” criteria. ADHD and bipolar disorder can have over lapping symptoms. For example, about 1 in 5 patients with bipolar disorder do have genuine ADHD. The alternative causes of “ADHD” symptoms that need to be further assessed are medical disorders such as thyroid disorder, inflammatory illnesses, and sleep apnea. Traumatic brain injuries, age related cognitive decline (typically begins after 45), medication effects (benzodiazepines, substance abuse, anticholinergics), sleep deprivation, depression and bipolar disorder, personality disorders, and learning disorders. Common co-morbidities associated w/ ADHD: Major Depressive Disorder (MDD), Bipolar Disorder, Anxiety disorders, Oppositional Defiant Disorder, Substance Abuse Disorders, Tic Disorder, and Learning Disorders. References: Feder, J., Tien, E., Puzantian, T.(2018). Child Medication Fact Book for Psychiatric Practice.Newburyport, MA: Carlat Publishing, LLC. ISBN # 978-0-9975106-8-3 Carlat Publishing (2019, November/December). Adult Onset ADHD. The Carlat Report Psychiatry, Vol. 17, issue 11-12. Johnson, K.,Vanderhoef, D.(2016) Psychiatric-Mental Health Nurse Practitioner: Review and Resource Manual (4th ed.) Silver Spring MD: American Nursing Association (Optional: Strongly Recommended). Puzanian, T.(2018.) Medication Fact Book for Psychiatric Practice (4th ed.) Newburyport, MA: Carlat Publishing, LLC. ISBN-# 978-0-9975106-6-9