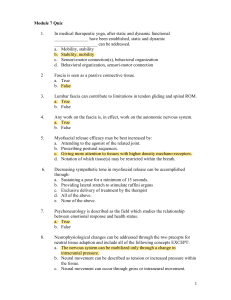
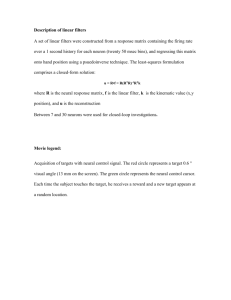
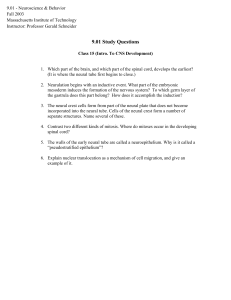
Neural Mobilization MUST READINGS • Shacklock. 2005. Clinical Neurodynamics (229, 98-104, 118-152, 154-158, 160-216) • Butler. 2002. Mobilisation of the Nervous System (55-90, 203-210) Briefly: Neural Testing & Mobilization • Neural testing and mobilization has to be used with care and precision • By using neural testing or mobilization too forceful you may cause more harm than benefit! Houglum 2010, 185, 191-192 Length change in the spinal canal SPINAL CORD MOVEMENT During Flexion Neural Mobilization • Mobilisation of the nervous system is an approach to physical treatment of pain. • The method relies on influencing pain physiology via mechanical treatment of neural tissues (direct method) and the non-neural structures surrounding the nervous system (indirect method). Shackloc 1995 Neural Testing and Mobilization • GOAL: differentiate symptomatic tissue - Testing: Does provocation testing reveal/increase the type of symptoms customer has had, compare to the uneffected side - Treatment: Does treatment decrease symptoms the customer has had • PHYSIOLOGY: Compression or tension or both > effects to nerve’s conduction and metabolism and itraneural blood flow • Refresh your memory: How and which direction nerve move/slide in the joint Shackloc 2005 Physiological effects of Neural Mobilization • Restore the dynamic balance between the relative movement of neural tissues and surrounding mechanical interfaces • Facilitation of nerve gliding • Reduction of nerve adherence (viscoelastic properties), • Dispersion of noxious fluids, • Increased neural vascularity (intraneural bloodflow), and • Improvement of axoplasmic flow Ellis et al. 2008 Indications • Use in non-irritable conditions (neurpathic/neurogenic) • For pathomecanical causes: - Fibrosis - Connective tissue adhesions - Restriction of normal tissue mobility Houglum 2010, 192 CONTRAINDICATIONS • Malignancies of the nervous system or vertebral column (selkäranka) • Acute inflammatory infections • Areas of instability • Spinal Cord Injuries • Suspected disc lesions • Cauda equina lesions • Dizziness related to vertebral artery insufficiencies • Any central nervous system disorders (e.g. spina bifida, MS) • Worsening neurological signs Houglum 2010, 104 Concepts of Nerve Testing and Mobilization • CLOSING: Closing mechanisms are those that produce increased pressure on a neural structure by way of reducing the space around it (Phalen) • OPENING: Opening mechanism are those that procude reduced pressure on a neural structure. The reduced pressure occurs when the space around the neural structure is increased by a particular manouvere (Spinal flexion) • Combining to muscle and tendon testing improves sensitivity. • Validity and reliability in testing is correlated with performance (repeats, repeats, repeats in exercising techniques) Shackloc 2005 OPENING and CLOSING in the SPINE Shackloc 2005 Concepts of Nerve Testing and Mobilization • Slider – goal is to produce gliding movement in relation to surrounding tissues • Tension – goal is to produce tension in the certain part of peripheral nerve. - Activity in ”normal area” - do not exceed the limits of elasticity (no lesions, is not a ”strech”) > may improve viscoelastic properties and physiological function of nerve) • In testing (ant treatment) directly to nerve tissue ➢ 1. SLIDER, 2. TENSIONER (observe symptoms, decreased ROM or change in muscle activity) Shackloc 2005 Testing Neural Tissue • THE IDEA is to determine can we provoce the symptoms of the customer has and compare the uneffected side to the symptomatic side. Tension Test 1. stop – First sensation of resistance Final stop – Symptoms or pain (scale 1-10) • Useful tool is a mental movement diagram > is the condition - Pain Dominant (pathofhysiologic) - Limitation Dominant (Pathomechanical) Shackloc 2005 Testing Neural Tissue • Start from the uneffected side > effects to the symptomatic side (e.g. SLUMP and SLR) • Upper extrimities: Tension increases when ➢ Lateral flexion of cervical spine (plexus prachialis, > n.med. ja n.rad.) ➢ Depression of Shoulder girdle/scapula (all the nerves of upper extremity) ➢ Shoulder abduction (90-100°) > plexus prachialis and pheripheral parts, LR especially n. medianus, MR n. radialis ➢ Elbow extension > n. medialis, Flexion > n. ulnaris, Supination > n. medianus, Pronation > n. radialis, n. interosseus ➢ Wrist extension > n. medianus ➢ Finger extension > n. medianus Medianus – ULTT1 Medianus – ULTT 1 Testing N. medianus (ULTT 1) 1. 2. 3. 4. 5. 6. 7. 8. Shoulder depression GH 110 abduction (support with thigh) Elbow in flexion Wrist dorsiflexion, Finger extension Arm supination GH Lateral rotation Elbow extension Cervical lateral flexion Medianus - ULTT 2a Testing N. medianus (ULTT 2a) • • • • • • 1. Shoulder depression 2. Elbow extension 3. GH lateral rotation + supination 4. Wrist extension abduction of the thumb 5. Shoulder abduction 6. If distal symptoms > release scapula, If proximal symptoms > release fingers/wrist Radial – ULTT 2b Ulnar – ULTT3 Lumbar area - Ichias SLUMP SLR = Straght Leg Raise Shacklock 2005, 138 Tibial Neurodynamic Test Shacklock 2005, 138 Peroneal Neurodynamic Test PKB = Prone Knee Bent – Mid lumbar & Femoralis Neural Mobilization • Tell the customer what you are doing • Test or mobilize uneffected side first (compare sides in testing) • Use sliders, spine slider (neck) may be beneficial to use before peripheral slider • Stop in the first sign • Be gentle – with inappropriate testing and mobilization may cause more harm than benefit • Throughout the treatment, the customer’s symptoms havs to be monitored > treatment should NOT cause pain • A sequence of of slow oscillations can last 20-30 sec > reassess customer’s condition • Don’t give nerve mobilization home exercises at the first meeting (because you don’t know the response, may occur after several hours) Houglum 2010, 191-193 Neural Mobilization • Start locally • Analyze provocing position or movement accurately and then choose test movement • Refresh your memory: Spine movement in flexion extension increase the length of spine approximately 9cm ➢ the status of tissues and tension ➢ Spinal cord and membranes and nerve roots glide cranially/caudally ➢ Flexion: opener, flexion closer, notice ”tension points” (picture) how spinal cord and membranes glide References • • • • • • • • Butler. 2002. Mobilisation of the Nervous System (55-90, 203-210) Ellis et al. 2008. Neural Mobilization: A Systematic Review of Randomized Controlled Trials with an Analysis of Therapeutic Efficacy. J Man Manip Ther. 2008; 16(1): 8–22. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2565076/?_escaped_fragment_=p o=25.0000 Houglum 2010. Therapeutic Exercise for Musculoskeletal Injuries: Chapter 6: Manual Therapy Techniques (p. 153-198) Huijbregts. 2010. Orthopaedic Manual Physical Therapy- History, Development and Future Opportunities. Journal of Physical Therapy 1, 11-24. Kaltenborn. 2012. 6th Edition. Manual Mobilization of the Joints. Joint Examination and Basic Treatment. Volume II. The Spine. Pickar. 2002. Neurophysiological effects of spinal manipulation. The Spine Journal 2, 357–371. http://www.wellwave.net/resources/Grundlagen/Pickar_02_review_SpinalMan.pdf Shacklock. 2005. Clinical Neurodynamics (2-29, 98-104, 118-152, 154-158, 160216) Shackloc. 1995. Neurodynamics. Pysiotherapy. 81(1), 9-15. http://www.hzf.hr/text/Physio%20Shacklock%2095.pdf