Muscle hypertrophy
From Wikipedia, the free encyclopedia
Jump to navigationJump to search
Athletes use a combination of strength training, diet, and nutritional supplementation to induce muscle
hypertrophy.
Muscle hypertrophy or muscle building involves a hypertrophy or increase in size
of skeletal muscle through a growth in size of its component cells. Two factors
contribute to hypertrophy: sarcoplasmic hypertrophy, which focuses more on increased
muscle glycogen storage; and myofibrillar hypertrophy, which focuses more on
increased myofibril size.[1] It is the most major part of the bodybuilding-related activities.
Contents
•
•
•
•
•
•
•
•
•
1Hypertrophy stimulation
o 1.1Strength training
o 1.2Anaerobic training
2Temporary swelling
3Factors affecting hypertrophy
4Changes in protein synthesis and muscle cell biology associated with
stimuli
o 4.1Protein synthesis
o 4.2Microtrauma
5Myofibrillar vs. sarcoplasmic hypertrophy
6In sports
7See also
8References
9Further reading
Hypertrophy stimulation[edit]
A range of stimuli can increase the volume of muscle cells. These changes occur as an
adaptive response that serves to increase the ability to generate force or resist fatigue
in anaerobic conditions.
Strength training[edit]
Strength training is used to regulate muscle hypertrophy.
Main article: Strength training
Strength training (resistance training) causes neural and muscular adaptations which
increase the capacity of an athlete to exert force through voluntary muscular
contraction: After an initial period of neuro-muscular adaptation, the muscle tissue
expands by creating sarcomeres (contractile elements) and increasing non-contractile
elements like sarcoplasmic fluid.[2]
Muscular hypertrophy can be induced by progressive overload (a strategy of
progressively increasing resistance or repetitions over successive bouts of exercise in
order to maintain a high level of effort).[3] However, the precise mechanisms are not
clearly understood; currently accepted hypotheses involve some combination of
mechanical tension, metabolic fatigue, and muscular damage.
Muscular hypertrophy plays an important role in competitive bodybuilding and strength
sports like powerlifting, football and Olympic weightlifting.
Anaerobic training[edit]
Main article: Anaerobic exercise
The best approach to specifically achieve muscle growth remains controversial (as
opposed to focusing on gaining strength, power, or endurance); it was generally
considered that consistent anaerobic strength training will produce hypertrophy over the
long term, in addition to its effects on muscular strength and endurance. Muscular
hypertrophy can be increased through strength training and other short-duration, highintensity anaerobic exercises. Lower-intensity, longer-duration aerobic
exercise generally does not result in very effective tissue hypertrophy; instead,
endurance athletes enhance storage of fats and carbohydrates within the muscles,[4] as
well as neovascularization.[5][6]
Temporary swelling[edit]
This section needs more medical references for verification or relies too
heavily on primary sources. Please review the contents of the section
and add the appropriate references if you can. Unsourced or poorly sourced
material may be challenged and removed.
Find sources: "Muscle
hypertrophy" – news · newspapers · books · scholar · JSTOR (May 2017)
During a workout, increased blood flow to metabolically active areas causes muscles to
temporarily increase in size, also known as being "pumped up" or getting "a
pump".[7] About two hours after a workout and typically for seven to eleven days,
muscles swell due to an inflammation response as tissue damage is repaired. [8] Longerterm hypertrophy occurs due to more permanent changes in muscle structure.
Factors affecting hypertrophy[edit]
Biological factors (such as DNA and sex), nutrition, and training variables can affect
muscle hypertrophy.[9]
Individual differences in genetics account for a substantial portion of the variance in
existing muscle mass. A classical twin study design (similar to those of behavioral
genetics) estimated that about 53% of the variance in lean body mass is
heritable,[10] along with about 45% of the variance in muscle fiber proportion.[11]
Testosterone helps to increase muscle hypertrophy.
During puberty in males, hypertrophy occurs at an increased rate. Natural hypertrophy
normally stops at full growth in the late teens. As testosterone is one of the body's major
growth hormones, on average, males find hypertrophy much easier (on an absolute
scale) to achieve than females and on average, have about 60% more muscle mass
than women.[12] Taking additional testosterone, as in anabolic steroids, will increase
results. It is also considered a performance-enhancing drug, the use of which can cause
competitors to be suspended or banned from competitions. Testosterone is also a
medically regulated substance in most[13][14] countries, making it illegal to possess without
a medical prescription. Anabolic steroid use can cause testicular atrophy, cardiac
arrest,[15] and gynecomastia.[16]
A positive energy balance, when more calories are consumed rather than burned, is
required for anabolism and therefore muscle hypertrophy. An increased requirement for
protein, especially branched-chain amino acids (BCAAs), is required for elevated
protein synthesis that is seen in athletes training for muscle hypertrophy.[17]
Training variables, in the context of strength training, such as frequency, intensity, and
total volume also directly affect the increase of muscle hypertrophy. A gradual increase
in all of these training variables will yield the muscular hypertrophy. [18]
Changes in protein synthesis and muscle cell biology
associated with stimuli[edit]
Protein synthesis[edit]
Main article: Protein biosynthesis
Protein biosynthesis starting with transcription and post-transcriptional modifications in the nucleus. Then the
mature mRNA is exported to the cytoplasm where it is translated. The polypeptide chain then folds and is posttranslationally modified.
The message filters down to alter the pattern of gene expression. The additional
contractile proteins appear to be incorporated into existing myofibrils (the chains
of sarcomeres within a muscle cell). There appears to be some limit to how large a
myofibril can become: at some point, they split. These events appear to occur within
each muscle fiber. That is hypertrophy results primarily from the growth of each muscle
cell rather than an increase in the number of cells. Skeletal muscle cells are however
unique in the body in that they can contain multiple nuclei, and the number of nuclei can
increase.[19]
Cortisol decreases amino acid uptake by muscle tissue, and inhibits protein
synthesis.[20] The short-term increase in protein synthesis that occurs subsequent to
resistance training returns to normal after approximately 28 hours in adequately fed
male youths.[21] Another study determined that muscle protein synthesis was elevated
even 72 hours following training.[22]
A small study performed on young and elderly found that ingestion of 340 grams of
lean beef (90 g protein) did not increase muscle protein synthesis any more than
ingestion of 113 grams of lean beef (30 g protein). In both groups, muscle protein
synthesis increased by 50%. The study concluded that more than 30 g protein in a
single meal did not further enhance the stimulation of muscle protein synthesis in young
and elderly.[23] However, this study didn't check protein synthesis in relation to training;
therefore conclusions from this research are controversial. A 2018 review of the
scientific literature [24] concluded that for the purpose of building lean muscle tissue, a
minimum of 1.6 g protein per kilogram of body weight is required, which can for example
be divided over 4 meals or snacks and spread out over the day.
It is not uncommon for bodybuilders to advise a protein intake as high as 2–4 g per
kilogram of bodyweight per day.[25] However, scientific literature has suggested this is
higher than necessary, as protein intakes greater than 1.8 g per kilogram of body weight
showed to have no greater effect on muscle hypertrophy.[26] A study carried out by
American College of Sports Medicine (2002) put the recommended daily protein intake
for athletes at 1.2–1.8 g per kilogram of body weight.[26][27][28] Conversely, Di
Pasquale (2008), citing recent studies, recommends a minimum protein intake of 2.2
g/kg "for anyone involved in competitive or intense recreational sports who wants to
maximize lean body mass but does not wish to gain weight. However athletes involved
in strength events (..) may need even more to maximize body composition and athletic
performance. In those attempting to minimize body fat and thus maximize body
composition, for example in sports with weight classes and in bodybuilding, it's possible
that protein may well make up over 50% of their daily caloric intake." [29]
Microtrauma[edit]
Main article: Microtrauma
Muscle fibres may be "microtorn" during microtrauma
Microtrauma is tiny damage to the muscle fibers. The precise relation between
microtrauma and muscle growth is not entirely understood yet.
One theory is that microtrauma plays a significant role in muscle growth. [30] When
microtrauma occurs (from weight training or other strenuous activities), the body
responds by overcompensating, replacing the damaged tissue and adding more, so that
the risk of repeat damage is reduced. Damage to these fibers has been theorized as the
possible cause for the symptoms of delayed onset muscle soreness (DOMS), and is
why progressive overload is essential to continued improvement, as the body adapts
and becomes more resistant to stress.
However, other work examining the time course of changes in muscle protein synthesis
and their relationship to hypertrophy showed that damage was unrelated to
hypertrophy.[31] In fact, in one study[31] the authors showed that it was not until the
damage subsided that protein synthesis was directed to muscle growth.
Myofibrillar vs. sarcoplasmic hypertrophy[edit]
This article's factual accuracy is disputed. Relevant discussion may be found
on the talk page. Please help to ensure that disputed statements are reliably
sourced. (May 2017) (Learn how and when to remove this template message)
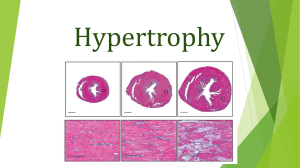
Hypertrophy of cell
In the bodybuilding and fitness community and even in some academic books skeletal
muscle hypertrophy is described as being in one of two types: Sarcoplasmic or
myofibrillar.[qualify evidence] According to this hypothesis, during sarcoplasmic hypertrophy, the
volume of sarcoplasmic fluid in the muscle cell increases with no accompanying
increase in muscular strength, whereas during myofibrillar
hypertrophy, actin and myosin contractile proteins increase in number and add to
muscular strength as well as a small increase in the size of the muscle. Sarcoplasmic
hypertrophy is greater in the muscles of bodybuilders because studies suggest
sarcoplasmic hypertrophy shows a greater increase in muscle size while myofibrillar
hypertrophy proves to increase overall muscular strength making it more dominant
in Olympic weightlifters.[32] These two forms of adaptations rarely occur completely
independently of one another; one can experience a large increase in fluid with a slight
increase in proteins, a large increase in proteins with a small increase in fluid, or a
relatively balanced combination of the two.
In sports[edit]
Examples of increased muscle hypertrophy are seen in various professional sports,
mainly strength related sports such as boxing, olympic weightlifting, mixed martial
arts, rugby, professional wrestling and various forms of gymnastics. Athletes in other
more skill-based sports such as basketball, baseball, ice hockey, and football may also
train for increased muscle hypertrophy to better suit their position of play. For example,
a center (basketball) may want to be bigger and more muscular to better overpower his
or her opponents in the low post.[33] Athletes training for these sports train extensively
not only in strength but also in cardiovascular and muscular endurance training.[citation needed]
See also[edit]
•
•
•
•
•
•
•
•
Anabolism
Colorado Experiment
Davis' law
Lean body mass
Muscle atrophy
Muscle dystrophy
Myostatin
Follistatin
References[edit]
1.
^ Baechle TR, Earle RW, eds. (2008). Essentials of strength training
and conditioning (3rd ed.). Champaign, IL: Human Kinetics. ISBN 9780-7360-5803-2.[page needed]
2. ^ Schoenfeld B (2016). Science and Development of Muscle
Hypertrophy. Human Kinetics. pp. 1–15. ISBN 978-1-4925-1960-7.
3. ^ Seynnes OR, de Boer M, Narici MV (January 2007). "Early skeletal
muscle hypertrophy and architectural changes in response to highintensity resistance training". Journal of Applied Physiology. 102 (1):
368–
73. doi:10.1152/japplphysiol.00789.2006. PMID 17053104. S2CID 289
81041.
4. ^ van Loon LJ, Goodpaster BH (February 2006). "Increased
intramuscular lipid storage in the insulin-resistant and endurancetrained state". Pflügers Archiv. 451 (5): 606–16. doi:10.1007/s00424005-1509-0. PMID 16155759. S2CID 6567497.
5. ^ Soares JM (June 1992). "Effects of training on muscle capillary
pattern: intermittent vs continuous exercise". The Journal of Sports
Medicine and Physical Fitness. 32 (2): 123–7. PMID 1279273.
6. ^ Prior BM, Yang HT, Terjung RL (September 2004). "What makes
vessels grow with exercise training?". Journal of Applied
Physiology. 97 (3): 1119–
28. doi:10.1152/japplphysiol.00035.2004. PMID 15333630. S2CID 366
56568.
7. ^ Joseph Eitel. "What Causes Your Muscles to Expand When You
Work Out?". Retrieved May 5, 2017.
8. ^ Claire Lunardoni (January 22, 2010). "Why Do You Swell After
Workout?".
9. ^ "How do muscles grow?".
10. ^ Arden, N. K. and Spector, T. D. (1997), Genetic Influences on
Muscle Strength, Lean Body Mass, and Bone Mineral Density: A Twin
Study. J Bone Miner Res, 12: 2076-2081.
doi:10.1359/jbmr.1997.12.12.2076
11. ^ Simoneau JA, Bouchard C (August 1995). "Genetic determinism of
fiber type proportion in human skeletal muscle". FASEB
Journal. 9 (11): 1091–
5. doi:10.1096/fasebj.9.11.7649409. PMID 7649409. S2CID 9613549.
12. ^ Miller AE, MacDougall JD, Tarnopolsky MA, Sale DG (1993).
"Gender differences in strength and muscle fiber
characteristics". European Journal of Applied Physiology and
Occupational Physiology. 66 (3): 254–
62. doi:10.1007/BF00235103. hdl:11375/22586. PMID 8477683. S2CI
D 206772211.
13. ^ "Search National Drug Schedule - NAPRA". Archived from the
original on February 1, 2014.
14. ^ "Controlled Substances Act". Food and Drug Administration.
15. ^ Fineschi V, Riezzo I, Centini F, Silingardi E, Licata M, Beduschi G,
Karch SB (January 2007). "Sudden cardiac death during anabolic
steroid abuse: morphologic and toxicologic findings in two fatal cases
of bodybuilders". International Journal of Legal Medicine. 121 (1): 48–
53. doi:10.1007/s00414-005-00559. PMID 16292586. S2CID 20004739.
16. ^ Basaria S (April 2010). "Androgen abuse in athletes: detection and
consequences". The Journal of Clinical Endocrinology and
Metabolism. 95 (4): 1533–43. doi:10.1210/jc.20091579. PMID 20139230.
17. ^ Phillips SM (July 2004). "Protein requirements and supplementation
in strength sports". Nutrition. 20 (7–8): 689–
95. doi:10.1016/j.nut.2004.04.009. PMID 15212752. Retrieved May
15, 2017.
18. ^ Wernbom M, Augustsson J, Thomeé R (March 1, 2007). "The
influence of frequency, intensity, volume and mode of strength training
on whole muscle cross-sectional area in humans". Sports
Medicine. 37 (3): 225–64. doi:10.2165/00007256-20073703000004. PMID 17326698. S2CID 31127952.
19. ^ Bruusgaard JC, Johansen IB, Egner IM, Rana ZA, Gundersen K
(August 2010). "Myonuclei acquired by overload exercise precede
hypertrophy and are not lost on detraining". Proceedings of the
National Academy of Sciences of the United States of
America. 107 (34): 15111–
6. Bibcode:2010PNAS..10715111B. doi:10.1073/pnas.0913935107. P
MC 2930527. PMID 20713720.
20. ^ Manchester KL (1970). "33 – Sites of Hormonal Regulation of
Protein Metabolism". Mammalian Protein Metabolism. Academic
Press, New York. p. 229. doi:10.1016/B978-0-12-510604-7.500116. ISBN 978-0-12-510604-7.
21. ^ Tang JE, Perco JG, Moore DR, Wilkinson SB, Phillips SM (January
2008). "Resistance training alters the response of fed state mixed
muscle protein synthesis in young men". American Journal of
Physiology. Regulatory, Integrative and Comparative
Physiology. 294 (1): R1728. doi:10.1152/ajpregu.00636.2007. PMID 18032468. S2CID 9743221.
22. ^ Miller BF, Olesen JL, Hansen M, Døssing S, Crameri RM, Welling
RJ, et al. (September 2005). "Coordinated collagen and muscle
protein synthesis in human patella tendon and quadriceps muscle after
exercise". The Journal of Physiology. 567 (Pt 3): 1021–
33. doi:10.1113/jphysiol.2005.093690. PMC 1474228. PMID 1600243
7.
23. ^ Symons TB, Sheffield-Moore M, Wolfe RR, Paddon-Jones D
(September 2009). "A moderate serving of high-quality protein
maximally stimulates skeletal muscle protein synthesis in young and
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
elderly subjects". Journal of the American Dietetic
Association. 109 (9): 1582–
6. doi:10.1016/j.jada.2009.06.369. PMC 3197704. PMID 19699838.
^ Schoenfeld BJ, Aragon AA (February 27, 2018). "How much protein
can the body use in a single meal for muscle-building? Implications for
daily protein distribution". Journal of the International Society of Sports
Nutrition. 15 (1): 10. doi:10.1186/s12970-018-02151. PMC 5828430. PMID 29497353.
^ "Bodybuilders and Protein – Part 2". Leehayward.com.
Retrieved June 19, 2011.
^ Jump up to:a b Tarnopolsky MA, Atkinson SA, MacDougall JD,
Chesley A, Phillips S, Schwarcz HP (November 1992). "Evaluation of
protein requirements for trained strength athletes". Journal of Applied
Physiology. 73 (5): 1986–
95. doi:10.1152/jappl.1992.73.5.1986. PMID 1474076.
^ Rankin JW (August 2002). "Weight loss and gain in
athletes". Current Sports Medicine Reports. 1 (4): 208–
13. doi:10.1249/00149619-200208000-00004. PMID 12831697.
^ Lemon PW (1991). "Effect of exercise on protein
requirements". Journal of Sports Sciences. 9 Spec No: 53–
70. doi:10.1080/02640419108729866. PMID 1895363.
^ Di Pasquale MG (2008). "Utilization of Proteins in Energy
Metabolism". In Ira Wolinsky, Judy A. Driskell (ed.). Sports Nutrition:
Energy metabolism and exercise. CRC Press. p. 79. ISBN 978-08493-7950-5.
^ Chargé SB, Rudnicki MA (January 2004). "Cellular and molecular
regulation of muscle regeneration". Physiological Reviews. 84 (1):
209–
38. doi:10.1152/physrev.00019.2003. PMID 14715915. S2CID 955638
6. Lay summary – Len Kravitz. {{cite journal}}: Cite uses
deprecated parameter |lay-url= (help)
^ Jump up to:a b Damas F, Phillips SM, Libardi CA, Vechin FC,
Lixandrão ME, Jannig PR, et al. (September 2016). "Resistance
training-induced changes in integrated myofibrillar protein synthesis
are related to hypertrophy only after attenuation of muscle
damage". The Journal of Physiology. 594 (18): 5209–
22. doi:10.1113/JP272472. PMC 5023708. PMID 27219125.
^ Kraemer WJ, Zatsiorsky VM (2006). Science and practice of strength
training. Champaign, IL: Human Kinetics. p. 50. ISBN 978-0-73605628-1.
^ Khorshidi E (September 10, 2012). "Chris Bosh Gaining Weight to
Play Center". SLAM. Retrieved April 7, 2017.
Further reading[edit]
•
•
•
Bodine SC, Stitt TN, Gonzalez M, Kline WO, Stover GL, Bauerlein R, et al.
(November 2001). "Akt/mTOR pathway is a crucial regulator of skeletal
muscle hypertrophy and can prevent muscle atrophy in vivo". Nature Cell
Biology. 3 (11): 1014–9. doi:10.1038/ncb11011014. PMID 11715023. S2CID 16284975.
Frontera WR, Meredith CN, O'Reilly KP, Knuttgen HG, Evans WJ (March
1988). "Strength conditioning in older men: skeletal muscle hypertrophy
and improved function". Journal of Applied Physiology. 64 (3): 1038–
44. doi:10.1152/jappl.1988.64.3.1038. PMID 3366726.
Glass DJ (October 2005). "Skeletal muscle hypertrophy and atrophy
signaling pathways". The International Journal of Biochemistry & Cell
•
•
•
•
Biology. 37 (10): 1974–
84. doi:10.1016/j.biocel.2005.04.018. PMID 16087388.
Schuelke M, Wagner KR, Stolz LE, Hübner C, Riebel T, Kömen W, et al.
(June 2004). "Myostatin mutation associated with gross muscle
hypertrophy in a child". The New England Journal of Medicine. 350 (26):
2682–8. doi:10.1056/NEJMoa040933. PMID 15215484. S2CID 6010232.
Charette SL, McEvoy L, Pyka G, Snow-Harter C, Guido D, Wiswell RA,
Marcus R (May 1991). "Muscle hypertrophy response to resistance training
in older women". Journal of Applied Physiology. 70 (5): 1912–
6. doi:10.1152/jappl.1991.70.5.1912. PMID 1864770.
Cureton KJ, Collins MA, Hill DW, McElhannon FM (August 1988). "Muscle
hypertrophy in men and women". Medicine and Science in Sports and
Exercise. 20 (4): 338–44. doi:10.1249/00005768-19880800000003. PMID 3173042.
Glass DJ (February 2003). "Signalling pathways that mediate skeletal
muscle hypertrophy and atrophy". Nature Cell Biology. 5 (2): 87–
90. doi:10.1038/ncb0203-87. PMID 12563267. S2CID 8938588.
show
Exercise
show
Strength-training exercises
Categories:
•
•
•
•
•
Muscular system
Tissues (biology)
Physiology
Exercise physiology
Bodybuilding
Navigation menu
•
•
•
•
•
Not logged in
Talk
Contributions
Create account
Log in
•
•
•
Read
Article
Talk
•
•
Edit
View history
Search
•
•
•
•
•
•
•
Main page
•
•
•
•
•
Help
•
•
•
•
•
•
•
What links here
Related changes
•
•
Download as PDF
Printable version
Contents
Current events
Random article
About Wikipedia
Contact us
Donate
Contribute
Learn to edit
Community portal
Recent changes
Upload file
Tools
Special pages
Permanent link
Page information
Cite this page
Wikidata item
Print/export
Languages
•
•
•
•
•
العربية
বাাংলা
•
•
•
•
Bahasa Indonesia
Deutsch
Español
한국어
Italiano
Português
Русский
5 more
•
•
Edit links
This page was last edited on 17 February 2022, at 15:45 (UTC).
Text is available under the Creative Commons Attribution-ShareAlike License 3.0; additional terms may apply. By using this
site, you agree to the Terms of Use and Privacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc.,
a non-profit organization.