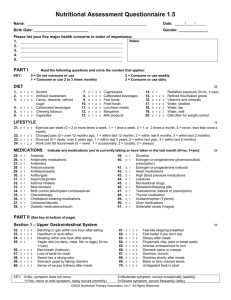
Nutritional Assessment Questionnaire Name: Date: Birth Date: Gender: / / Please list your five major health concerns in order of importance: 1. 2. 3. 4. 5. Notes: PART I KEY: Read the following questions and add the number that applies, after the item(s): 0 = Do not consume or use 1 = Consume or use 2 to 3 times monthly 2 = Consume or use weekly 3 = Consume or use daily DIET (add the key number next to the item. Eg. Fried Foods - 2 1. 2. 3. 4. 5. 6. Alcohol Artificial sweeteners Confectionary or other sweets Fizzy drinks Chewing tobacco Cigarettes 7. 8. 9. 10. 11. 12. 13. Cigars/pipes Caffeinated beverages Fast foods Fried foods Tinned meats/hot dogs Margarine Milk products 14. 15. 16. 17. 18. 19. 20. Radiation exposure (0=no, 1=yes) Refined flour/baked goods Vitamins and minerals Water, distilled Water, tap Water, bottled mineral water Diet often for weight control LIFESTYLE – add the key number next to the description. Eg. Changed jobs - 3 21. 22. 23. 24. Exercise per week (0 = 2 or more times a week, 1 = 1 time a week, 2 = 1 or 2 times a month, 3 = never, less than once a month) Changed jobs (0 = over 12 months ago, 1 = within last 12 months, 2 = within last 6 months, 3 = within last 2 months) Divorced (0 = never, over 2 years ago, 1 = within last 2 years, 2 = within last year, 3 = within last 6 months) Work over 60 hours/week (0 = never, 1 = occasionally, 2 = usually, 3 = always) MEDICATIONS 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. Indicate any medications you’re cu rrently taking or have taken in the last month (0=no, 1=yes): Antacids Antianxiety medications Antibiotics Anticonvulsants Antidepressants Antifungals Aspirin/Ibuprofen/Paracetamol Asthma inhalers Beta blockers Birth control pills/implant contraceptives Chemotherapy Cholesterol lowering medications Cortisone/steroids Diabetic medications/insulin 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. Diuretics Oestrogen or progesterone (pharmaceutical,prescription) Oestrogen or progesterone (natural) Heart medications High blood pressure medications Laxatives Recreational drugs Relaxants/Sleeping pills Testosterone (natural or prescription) Thyroid medication Acetaminophen (Tylenol) Ulcer medications Sildenafal citrate (Viagra) PART II (See key at bottom of page) Section 1 52. 53. 54. 55. 56. 57. 58. 59. 60. Belching or gas within one hour after eating Heartburn or acid reflux Bloating within one hour after eating Vegan diet (no dairy, meat, fish or eggs) (0=no, 1=yes) Bad breath (halitosis) Loss of taste for meat Sweat has a strong odor Stomach upset by taking vitamins Sense of excess fullness after meals KEY: 0=No, symptom does not occur 1=Yes, minor or mild symptom, rarely occurs (monthly) 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. Feel like skipping breakfast Feel better if you don’t eat Sleepy after meals Fingernails chip, peel or break easily Anemia unresponsive to iron Stomach pains or cramps Diarrhoea, chronic Diarrhoea shortly after meals Black or tarry colored stools Undigested food in stool 2=Moderate symptom, occurs occasionally (weekly) 3=Severe symptom, occurs frequently (daily) Nutritional Assessment Questionnaire Page 2 of 4 Section 2 (See key at bottom of page) 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. Pain between shoulder blades Stomach upset by greasy foods Greasy or shiny stools Nausea Sea, car, airplane or motion sickness History of morning sickness (0 = no, 1 = yes) Light or clay colored stools Dry skin, itchy feet or skin peels on feet Headache over eyes Gallbladder attacks (0=never, 1=years ago, 2=within last year, 3=within past 3 months) Gallbladder removed (0=no, 1=yes) Bitter taste in mouth, especially after meals Become sick if you were to drink wine (0=no, 1=yes) Easily intoxicated if you were to drink wine (0=no, 1=yes) 85. 86. 87. 88. 89. 90. 91. 92. 93. 94. 95. 96. 97. 98. Easily hung over if you were to drink wine (0=no, 1=yes) Alcohol per week (0=<3, 1=<7, 2 =<14, 3=>14) Recovering alcoholic (0=no, 1=yes) History of drug or alcohol abuse (0=no, 1=yes) History of hepatitis (0=no, 1=yes) Long term use of prescription/recreational drugs (0=no, 1=yes) Sensitive to chemicals (perfume, cleaning agents, etc.) Sensitive to tobacco smoke Exposure to diesel fumes Pain under right side of rib cage Haemorrhoids or varicose veins Nutrasweet (aspartame) consumption Sensitive to Nutrasweet (aspartame) Chronic fatigue or Fibromyalgia Section 3 (See key at bottom of page) 99. 100. 101. 102. 103. 104. 105. 106. 107. Food allergies Abdominal bloating 1 to 2 hours after eating Specific foods make you tired or bloated (0=no, 1=yes) Pulse speeds after eating Airborne allergies Experience hives Sinus congestion, "stuffy head" Crave bread or noodles Alternating constipation and diarrhoea 108. 109. 110. 111. 112. 113. 114. 115. Crohn's disease (0 =no, 1=yes in the past, 2=currently mild condition, 3=severe) Wheat or grain sensitivity Dairy sensitivity Are there foods you could not give up (0=no, 1=yes) Asthma, sinus infections, stuffy nose Bizarre vivid dreams, nightmares Use over-the-counter pain medications Feel spacey or unreal Section 4 (See key at bottom of page) 116. 117. 118. 119. 120. 121. 122. 123. 124. 125. Anus itches Coated tongue Feel worse in mouldy or musty place Taken antibiotic for a total accumulated time of (0=never, 1= <1 month, 2= <3 months, 3= >3 months) Fungus or yeast infections Ring worm, "jock itch", "athletes foot", nail fungus Yeast symptoms increase with sugar, starch or alcohol Stools hard or difficult to pass History of parasites (0=no, 1=yes) Less than one bowel movement per day 126. 127. 128. 129. 130. 131. 132. 133. 134. 135. Stools have corners or edges, are flat or ribbon shaped Stools are not well formed (loose) Irritable bowel or mucus colitis Blood in stool Mucus in stool Excessive foul smelling lower bowel gas Bad breath or strong body odours Painful to press along outer sides of thighs (Iliotibial Band) Cramping in lower abdominal region Dark circles under eyes 150. 151. 152. 153. 154. 155. 156. 157. 158. 159. 160. 161. 162. 163. 164. History of bone spurs (0=no, 1=yes) Morning stiffness Nausea with vomiting Crave chocolate Feet have a strong odour History of anaemia Whites of eyes (sclera) blue tinted Hoarseness Difficulty swallowing Lump in throat Dry mouth, eyes and/or nose Gag easily White spots on fingernails Cuts heal slowly and/or scar easily Decreased sense of taste or smell Section 5 (See key at bottom of page) 136. 137. 138. 139. 140. 141. 142. 143. 144. 145. 146. 147. 148. 149. History of carpal tunnel syndrome (0=no, 1=yes) History of lower right abdominal pains or ileocecal valve problems (0=no, 1=yes) History of stress fracture (0=no, 1=yes) Bone loss (reduced density on bone scan) Are you shorter than you used to be? (0=no, 1=yes) Calf, foot or toe cramps at rest Cold sores, fever blisters or herpes lesions Frequent fevers Frequent skin rashes and/or hives Herniated disc (0=no, 1=yes) Excessively flexible joints, "double jointed" Joints pop or click Pain or swelling in joints Bursitis or tendonitis KEY: 0=No, symptom does not occur 1=Yes, minor or mild symptom, rarely occurs (monthly) 2=Moderate symptom, occurs occasionally (weekly) 3=Severe symptom, occurs frequently (daily) Nutritional Assessment Questionnaire Page 3 of 4 Section 6 (See key at bottom of page) 165. 166. 167. 168. Experience pain relief with aspirin (0=no, 1=yes) Crave fatty or greasy foods Low- or reduced-fat diet (0=never, 1=years ago, 2=within Last year, 3=currently) Tension headaches at base of skull 169. 170. 171. 172. Headaches when out in the hot sun Sunburn easily or suffer sun poisoning Muscles easily fatigued Dry flaky skin or dandruff 180. 181. 182. 183. 184. 185. Headache if meals are skipped or delayed Irritable before meals Shaky if meals delayed Family members with diabetes (0=none, 1=1 or 2, 2=3 or 4, 3=more than 4) Frequent thirst Frequent urination 200. 201. 202. 203. 204. 205. 206. 207. 208. 209. 210. 211. 212. Can hear heart beat on pillow at night Whole body or limb jerk as falling asleep Night sweats Restless leg syndrome Cracks at corner of mouth (Cheilosis) Fragile skin, easily chaffed, as in shaving Polyps or warts MSG sensitivity Wake up without remembering dreams Small bumps on back of arms Strong light at night irritates eyes Nose bleeds and/or tend to bruise easily Bleeding gums especially when brushing teeth 226. 227. 228. 229. 230. 231. 232. 233. 234. 235. 236. 237. 238. Arthritic tendencies Crave salty foods Salt foods before tasting Perspire easily Chronic fatigue, or get drowsy often Afternoon yawning Afternoon headache Asthma, wheezing or difficulty breathing Pain on the medial or inner side of the knee Tendency to sprain ankles or "shin splints" Tendency to need sunglasses Allergies and/or hives Weakness, dizziness 245. 246. 247. 248. 249. 250. Height under 4' 10" (0=no, 1=yes) Decreased libido Excessive thirst Weight gain around hips or waist Menstrual disorders Delayed sexual development (after age 13) (0=no, 1=yes) Tendency to ulcers or colitis Section 7 (See key at bottom of page) 173. 174. 175. 176. 177. 178. 179. Awaken a few hours after falling asleep, hard to get back to sleep Crave sweets Binge or uncontrolled eating Excessive appetite Crave coffee or sugar in the afternoon Sleepy in afternoon Fatigue that is relieved by eating Section 8 (See key at bottom of page) 186. 187. 188. 189. 190. 191. 192. 193. 194. 195. 196. 197. 198. 199. Muscles become easily fatigued Feel exhausted or sore after moderate exercise Vulnerable to insect bites Loss of muscle tone, heaviness in arms/legs Enlarged heart or congestive heart failure Pulse below 65 per minute (0=no, 1=yes) Ringing in the ears (Tinnitus) Numbness, tingling or itching in hands and feet Depressed Fear of impending doom Worrier, apprehensive, anxious Nervous or agitated Feelings of insecurity Heart races Section 9 (See key at bottom of page) 213. 214. 215. 216. 217. 218. 219. 220. 221. 222. 223. 224. 225. Tend to be a "night person" Difficulty falling asleep Slow starter in the morning Tend to be keyed up, trouble calming down Blood pressure above 120/80 Headache after exercising Feeling wired or jittery after drinking coffee Clench or grind teeth Calm on the outside, troubled on the inside Chronic low back pain, worse with fatigue Become dizzy when standing up suddenly Difficulty maintaining manipulative correction Pain after manipulative correction (eg osteopathy) Section 10 (See key at bottom of page) 239. 240. 241. 242. 243. 244. Height over 6' 6" (0=no, 1=yes) Early sexual development (before age 10) (0=no, 1=yes) Increased libido Splitting type headache Memory failing Tolerate sugar, feel fine when eating sugar (0=no, 1=yes) 251. KEY: 0=No, symptom does not occur 1=Yes, minor or mild symptom, rarely occurs (monthly) 2=Moderate symptom, occurs occasionally (weekly) 3=Severe symptom, occurs frequently (daily) Nutritional Assessment Questionnaire Page 4 of 4 Section 11 (See key at bottom of page) 252. 253. 254. 255. 256. 257. 258. 259. Sensitive/allergic to iodine Difficulty gaining weight, even with large appetite Nervous, emotional, can't work under pressure Inward trembling Flush easily Fast pulse at rest Intolerance to high temperatures Difficulty losing weight 260. 261. 262. 263. 264. 265. 266. 267. Mentally sluggish, reduced initiative Easily fatigued, sleepy during the day Sensitive to cold, poor circulation (cold hands and feet) Constipation, chronic Excessive hair loss and/or coarse hair Morning headaches, wear off during the day Loss of lateral 1/3 of eyebrow Seasonal sadness 272. 273. 274. 275. 276. Waking to urinate at night Interruption of stream during urination Pain on inside of legs or heels Feeling of incomplete bowel evacuation Decreased sexual function 287. 288. 289. 290. 291. 292. 293. 294. 295. 296. Breast fibroids, benign masses Painful intercourse (dysparenia) Vaginal discharge Vaginal dryness Vaginal itchiness Gain weight around hips, thighs and buttocks Excess facial or body hair Hot flashes Night sweats (in menopausal females) Thinning skin 302. 303. 304. 305. 306. Ankles swell, especially at end of day Cough at night Blush or face turns red for no reason Dull pain or tightness in chest and/or radiate into right arm, worse with exertion Muscle cramps with exertion 310. 311. Cloudy, bloody or darkened urine Urine has a strong odor 317. Never get sick (0 = sick only 1 or 2 times in last 2 years, 1 = not sick in last 2 years, 2 = not sick in last 4 years, 3 = not sick in last 7 years) Acne (adult) Itchy skin (Dermatitis) Cysts, boils, rashes History of Epstein Bar, Mono, Herpes, Shingles, Chronic Fatigue Syndrome, Hepatitis or other chronic viral condition (0 = no, 1 = yes in the past, 2 = currently mild condition, 3 = severe) Section 12 – Men Only (See key at bottom of page) 268. 269. 270. 271. Prostate problems Difficulty with urination, dribbling Difficult to start and stop urine stream Pain or burning with urination Section 13 – Women Only (See key at bottom of page) 277. 278. 279. 280. 281. 282. 283. 284. 285. 286. Depression during periods Mood swings associated with periods (PMS) Crave chocolate around periods Breast tenderness associated with cycle Excessive menstrual flow Scanty blood flow during periods Occasional skipped periods Variations in menstrual cycles Endometriosis Uterine fibroids Section 14 (See key at bottom of page) 297. 298. 299. 300. 301. Aware of heavy and/or irregular breathing Discomfort at high altitudes "Air hunger" or sigh frequently Compelled to open windows in a closed room Shortness of breath with moderate exertion Section 15 (See key at bottom of page) 307. 308. 309. Pain in mid-back region Puffy around the eyes, dark circles under eyes History of kidney stones (0=no, 1=yes) Section 16 (See key at bottom of page) 312. 313. 314. 315. 316. Runny or drippy nose Catch colds at the beginning of winter Mucus producing cough Frequent colds or flu (0=1 or less per year, 1=2 to 3 times per year, 2=4 to 5 times per year, 3=6 or more times per year) Other infections (sinus, ear, lung, skin, bladder, kidney, etc.) (0=1 or less per year, 1=2 to 3 times per year, 2=4 to 5 times per year, 3=6 or more times per year) 318. 319. 320. 321. NOTES: KEY: 0=No, symptom does not occur 1=Yes, minor or mild symptom, rarely occurs (monthly) 2=Moderate symptom, occurs occasionally (weekly) 3=Severe symptom, occurs frequently (daily)