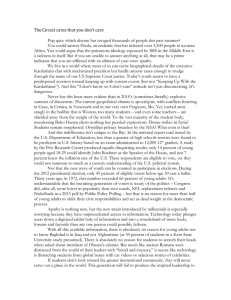
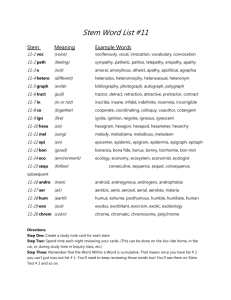
REVIEW Biba R Stanton,1 Alan Carson2 1 Department of Neurology, Royal Free Hospital, London, UK Departments of Clinical Neurosciences and Rehabilitation Medicine, NHS Lothian, and Centre for Clinical Brain Studies, University of Edinburgh, Edinburgh, UK 2 Correspondence to Dr Biba R Stanton, Department of Neurology, Royal Free Hospital, Pond St, London, NW3 2QG, UK; biba.stanton@nhs.net Accepted 20 September 2015 Published Online First 27 October 2015 ABSTRACT Apathy is an under-recognised and underestimated problem for people with chronic neurological disorders. Despite being common and disabling, it is seldom volunteered as a symptom by patients or even their caregivers. Yet apathy undoubtedly has an important impact on caregiver stress, functional disability and quality of life. A detailed clinical assessment can distinguish apathy from depression and allow clinicians to make practical suggestions to reduce the impact of symptoms on individual patients and their families. Pharmacological approaches to treatment include cholinesterase inhibitors, dopamine agonists and stimulants. CASE 1 To cite: Stanton BR, Carson A. Pract Neurol 2016;16:42–47. 42 A 66-year-old man with progressive supranuclear palsy returned to clinic for review. His wife was upset and finding it difficult to cope. She described him as ‘completely lazy’, as he just sat in his chair all day watching television, even though he could still do things for himself. She felt that he could not be bothered to speak to her anymore because he was ‘obsessed with TV’. He did not seem to engage with the visits to the grandchildren that she arranged. He said that he felt fine apart from the problems with his walking. The neurologist was confident that the patient was not depressed, and that the wife’s concerns reflected the apathy that is often very pronounced in progressive supranuclear palsy. By explaining to the man’s wife that these problems were due to his disease, their relationship improved and she felt more able to cope with caring for him. CASE 2 A 75-year-old man attended clinic with his wife. She had worried about him for over a year, as he had become increasingly withdrawn. He used to enjoy going to the local pub but now stayed at home all day. He seemed less concerned about his personal appearance, about which he used to be meticulous. More recently, she had noticed that he had become forgetful. On examination, he had a mild episodic memory deficit but no impairments in other domains. He was diagnosed with mild cognitive impairment but the presence of apathy suggested a high risk of him developing Alzheimer’s disease. He did not improve with a trial of antidepressant treatment but had useful input from an occupational therapist. His apathy improved after he started a cholinesterase inhibitor a year later, when his cognitive symptoms had progressed. INTRODUCTION The term apathy derives from the Greek ‘pathos’, meaning passions. Apathy as used by the stoic philosophers referred to a desirable state of ascendancy of reason over unwanted emotional influence (figure 1). In common use today, apathy means lack of interest, enthusiasm, concern or emotion and can refer to an aspect of normal experience. The clinical syndrome of apathy refers to a disorder of goal-directed behaviour, manifesting as reduced motivation compared with a previous level of functioning.1 APATHY IS COMMON The reported prevalence of apathy in different disorders inevitably depends on Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. Apathy: a practical guide for neurologists REVIEW Parkinson’s disease Progressive supranuclear palsy Stroke Alzheimer’s disease Mild cognitive impairment Frontotemporal dementia Traumatic brain injury 20–30%2 80%3 40%4 50%5 30%6 up to 90%7 50%8 Apathy generally becomes more common with more severe disease9 but can also be a very early symptom; apathy in the context of mild cognitive impairment suggests an increased risk of developing Alzheimer’s disease.6 THE IMPACT OF APATHY ON PATIENTS AND CAREGIVERS Patients themselves are rarely distressed by apathy: by definition, apathy is associated with lack of insight and lack of concern about symptoms. Despite this, it has a major impact on quality of life.10 More importantly, perhaps, there is good evidence that caregivers find apathy distressing. Carers of patients with traumatic brain injury rate lack of motivation as one of the three most distressing problems.11 In dementia, apathy significantly predicts carer burden, even after controlling for functional disability and caregiver depression.12 Apathy also increases patients’ functional disability because they fail to engage in activities that they could otherwise perform and need prompting to structure their daily life.13 It also presents a major barrier to engagement in rehabilitative activities. The negative impact of apathy on activities of daily living is likely to result in increased healthcare costs and need for care.14 DEFINING AND ASSESSING APATHY Current psychiatric classifications do not define apathy as an independent disorder but rather as a symptom; The International Classification of Diseases 10th Revision (ICD-10) does not mention it at all. The psychologists Robert Marin and Sergio Starkstein have done much to raise awareness of apathy as a clinical problem and to define it more rigorously for the purpose of research. Current criteria define apathy as reduced motivation, with symptoms in at least two of three domains of: ▸ reduced initiative (lack of effort, dependency on others to structure activity); ▸ reduced interest (lack of interest in learning new things or in new experiences, lack of concern about one’s personal problems); ▸ reduced emotional responsiveness (unchanging affect, lack of emotional responsivity to positive or negative events).15 Patients typically have poor insight into the symptoms, not recognising them at all or not perceiving them as problematic. Despite the burden it causes, caregivers may not volunteer apathy as a problem, because they often perceive the patient’s behaviour as laziness, or as an inevitable response to their illness, rather than a core part of the disease. It is therefore important to ask specific questions of carers to detect apathy symptoms as part of the routine assessment in any chronic neurological condition (box 1). Box 1 Questions to ask of carers to detect apathy Figure 1 Zeno of Citium (334–262 BC) was the founder of the Stoic school of philosophy and taught that the ‘pathe’ (emotions and passions) should be extirpated. Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 ▸ Does he seem more passive or withdrawn? ▸ Do you need to prompt or encourage her to get started with things? ▸ Has he lost interest in things that he used to enjoy? ▸ Does she seem less emotional than she used to be? 43 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. how it is defined and what population is assessed. The summary of evidence from different studies suggests the following rates of clinically important apathy symptoms in neurology clinic patients: REVIEW THE RELATIONSHIP BETWEEN APATHY AND DEPRESSION The symptoms of depression, as defined in ICD-10, include loss of interest and diminished activity in addition to low mood. However, the experience of anhedonia in depression (the inability to perceive pleasure) is characterised, even among those who describe it as an ‘emptiness’, as a highly negative affective experience. This contrasts with the neutral experience of apathy, which is essentially an emotionally deficit state. There is good evidence that while depression and apathy sometimes occur together in neurological disorders, they can also be present independently: depression without apathy is common in Parkinson’s disease, whereas apathy without depression is common in progressive supranuclear palsy.19 Scores on apathy and depression rating scales correlate modestly because of the overlap in symptoms included,20 but dysphoria and apathy do not correlate at all.21 This distinction is not always clear cut and perhaps some older people who meet criteria for a depressive illness might be better classified as apathetic (eg, due to small vessel disease). Alexopoulos described a group of older patients with ‘depression’ who have prominent apathy, little agitation or guilt, marked executive dysfunction, white matter disease on imaging, and a poor response to antidepressant treatment.22 In practical terms, it is crucial to consider underlying depression in any patient with apathy symptoms because depression is more amenable to treatment. It is essential to obtain a history from the caregiver as well as from the patient. Table 1 suggests some useful clues, from our clinical experience, to distinguish between apathy and depression in a patient with lack of interest or motivation. 44 Table 1 Clinical features suggesting apathy versus depression Suggesting apathy Suggesting depression ▸ Reduced experience of negative as well as positive emotions ▸ Marked executive dysfunction on cognitive testing ▸ ‘Frontal release’ signs, such as grasp reflex or utilisation behaviour ▸ Lack of concern about symptoms ▸ Displaying an emotional emptiness ▸ Feeling sad, tearful or guilty ▸ A sense of hopelessness about the future ▸ Agitation ▸ Diurnal variation in mood ▸ Negative cognitive bias (seeing the ‘bad or upsetting’ in everything) ▸ Feeling an emotional emptiness NOSOLOGY OF APATHY The nosological position of apathy is complicated by the use of other terms to describe similar clinical features. The concept of negative symptoms in schizophrenia overlaps with definitions of apathy in neurological disorders. Negative symptoms include: ▸ avolition (equivalent to the behavioural domain of apathy) ▸ alogia (poverty of speech, which may be another behavioural aspect of apathy) ▸ asociality (which overlaps with lack of interest as described in apathy) ▸ affective flattening (similar to the emotional domain of apathy) ▸ anhedonia (a more specific lack of pleasure, not part of definitions of apathy) The phenomenology of negative symptoms in schizophrenia has not been directly compared with that of apathy in neurological disorders, but the general view is that they represent a degenerative cognitive component to the illness23 and it seems likely that there will be considerable overlap in the neurobiological substrate. The term abulia has been used interchangeably with the term apathy, or to describe particularly severe impairment of initiation of purposeful behaviour in the context of organic brain disease. WHAT CAUSES APATHY? Although apathy can occur across a wide range of neurological disorders, the common factor in all of these is damage either to the frontal lobes or to the subcortical structures. Focal brain lesions in the frontal lobes, thalamus or basal ganglia can be sufficient to cause apathy, consistent with the role of these brain regions in normal goal-directed behaviour and emotional processing. Studies using structural brain imaging in clinical groups to explore the neuroanatomical correlates of apathy report an association with volume loss in regions including the frontal pole, orbitofrontal cortex, insula, anterior cingulate cortex, and dorsolateral prefrontal cortex (figure 2).24 Different apathy symptoms (reduced initiative and emotional blunting) may be associated with distinct patterns of Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. To some extent, apathy can be the understandable result of physical or cognitive limitations: patients with neurological disorders may lose interest or pleasure in things they used to enjoy because of difficulties in walking, speech, memory or concentration. Yet there is a psychopathological aspect to the absence of emotion in apathy that separates it from this mournful withdrawal as part of an illness response. There is good evidence that patients with neurological disorders have much more prominent apathy than equally disabled patients with nonneurological conditions.16 Apathy can be more formally assessed and quantified using several different rating scales. It is included in broader assessments of behavioural symptoms, such as the Neuropsychiatric Inventory,17 and can be assessed in more detail with instruments such as the Apathy Evaluation Scale.18 Clinician-rated or carerrated scales are usually more reliable than self-report questionnaires, because apathy is usually accompanied by a lack of insight. REVIEW Figure 2 Differences in regional grey matter volume between patients with and without apathy in Alzheimer’s disease and progressive supranuclear palsy. Red clusters show reduced grey matter volume in the cingulate gyrus and insula in apathetic patients (adapted from Stanton et al25). frontal atrophy.25 Many studies have used Single Photon Emission Computed Tomography (SPECT) or Positron Emission Tomography (PET) to examine the relationship between apathy and regional brain blood flow/metabolism. In Alzheimer’s disease, the anterior cingulate cortex and orbitofrontal cortex appear most consistently associated with apathy (figure 3).26 The brain regions implicated by these studies map well on to the ‘salience network’, a group of functionally linked brain regions thought to be crucial in motivation and readiness to act.27 Functional connectivity in the salience network, studied with resting state functional MRI, is reduced in elderly depressed patients with high apathy, compared with those without.28 MANAGEMENT OF APATHY The first step in managing apathy is to recognise it. ‘Has he become more passive or withdrawn?’ is a useful single screening question to ask a carer. If the answer is yes, then it is helpful to explore symptoms in more detail with the following questions in mind: If there is any suspicion of depression, a trial of an antidepressant is indicated but medication should be stopped if it is ineffective. There is some evidence that selective serotonin-reuptake inhibitors, which can cause extrapyramidal side effects, may actually worsen apathy symptoms.29 In theory, there might be a rationale for selecting a more ‘activating’ antidepressant (such as reboxetine or venlafaxine) but there is no evidence base for this. It is important to address any other reversible problems that could aggravate apathy symptoms, including visual or hearing impairment, motor or cognitive symptoms and medications. In particular, antidopaminergic drugs can certainly worsen apathy and should be stopped where possible. Should patients with apathy be encouraged to greater levels of activity, or should caregivers allow patients to withdraw if they choose? This question can only be answered for an individual, with an understanding of their particular psychosocial context. In some families, the main problem is the caregiver’s frustration with a patient’s behaviour. In this situation, explaining that apathy is a symptom of their illness and caused by a problem in the brain is a surprisingly useful intervention.30 Caregivers may find it upsetting to see their loved one more passive or withdrawn, but actually find apathetic behaviour easy to manage. Open discussion and reassurance from the patients themselves that they are not distressed may be all that is required in this situation. For others, the need for continuous prompting and their increasingly limited activities may have a hugely negative impact on daily life. Box 2 suggests some simple strategies that a couple or family might use to minimise the impact of apathy symptoms. For patients with dementia in nursing homes, there is some evidence for interventions designed to ‘increase the reward potential of the environment’. A randomised controlled trial of ‘activity therapy’ for Figure 3 Reduced metabolism in the anterior cingulate and medial orbitofrontal cortex in apathetic patients compared with non-apathetic patients with Alzheimer’s disease (adapted from Marshall et al26). Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 45 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. ▸ Are the symptoms out of proportion to what might be expected in someone with these physical symptoms or disability? ▸ Does the patient have awareness of the symptoms? ▸ Could there be significant depression? ▸ What specific problems are causing distress for that individual or family? REVIEW ▸ Create a regular daily routine with more varied activities but fewer choices for the patient to make ▸ Use frequent prompts to remind the patient start activities: these could be set as alarms on a mobile phone rather than always having to come verbally from a carer ▸ Get out of the house every day, even if only to the local shops ▸ If motor or cognitive symptoms limit participation in previous interests, think carefully about how these could be adapted with advice from an occupational therapist ▸ Encourage caregivers to take up regular respite care without guilt Key points apathy showed improvements in apathy with activity therapy and with the control intervention (one-to-one meetings with a therapist to give the same time and attention).31 A small controlled study of ‘validation therapy’ (designed to improve communication with patients with dementia) showed that this could improve apathy.32 Specialised cognitive rehabilitative approaches, for instance to enhance attention or performance speed, may help some people although there is no evidence for this approach. There are many pharmacological strategies suggested for managing apathy. In dementia, a meta-analysis suggested that cholinesterase inhibitors modestly benefited neuropsychiatric symptoms (as a secondary end point33). In a randomised study of 30 patients with Parkinson’s disease who were apathetic but free of depression and dementia, rivastigmine significantly improved apathy.34. Small open-label studies of cholinesterase inhibitors for apathy following traumatic brain injury have also suggested some benefits.35 Dopamine is the other neurotransmitter often implicated in apathy symptoms. Apathy can occur early in Parkinson’s disease, and can worsen with antidopaminergic drugs.36 Patients with idiopathic Parkinson’s disease and motor fluctuations may be more apathetic in their ‘off ’ state. Patients with Parkinson’s disease may become apathetic following deep brain stimulation surgery when their levodopa dose is reduced, and this may improve with dopamine agonist treatment.37 Pramipexole may be particularly useful because of its selective affinity for D3 dopamine receptors.38 There are two case reports of success in using dopamine agonists for apathy following stroke.39 40 There are also case reports of amantadine (with effects on dopamine and glutamate41), buproprion (a norepinephrine and dopamine reuptake inhibitor42) and selegiline (a monoamine oxidase inhibitor43) for apathy symptoms. 46 ▸ Apathy is very common in patients with stroke, brain injury and neurodegenerative disorders and has a huge impact on caregiver distress. ▸ A useful screening question to ask caregivers is whether the patient seems more passive or withdrawn. ▸ Always assess whether the patient may be depressed, as this may be more amenable to treatment. ▸ Education about apathy and suggestions of practical strategies to reduce its impact on daily life can greatly help patients and families. Correction notice This paper has been corrected since it was published Online First. Figure 2 has been corrected. Contributors BRS drafted the article. AC provided comments and helped to make revisions. Competing interests None declared. Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Masud Husain, Oxford, UK. REFERENCES 1 Marin RS. Differential diagnosis and classification of apathy. Am J Psychiatry 1990;147:22–30. 2 Aarsland D, Larsen JP, Lim NG, et al. Range of neuropsychiatric disturbances in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 1999;67:492–6. 3 Aarsland D, Litvan I, Larsen JP. Neuropsychiatric symptoms of patients with progressive supranuclear palsy and Parkinson’s disease. J Neuropsychiatry Clin Neurosci 2001;13:42–9. 4 Brodaty H, Sachdev PS, Withall A, et al. Frequency and clinical, neuropsychological and neuroimaging correlates of apathy following stroke—the Sydney Stroke Study. Psychol Med 2005;35:1707–16. 5 Kuzis G, Sabe L, Tiberti C, et al. Neuropsychological correlates of apathy and depression in patients with dementia. Neurology 1999;52:1403–7. 6 Robert PH, Berr C, Volteau M, et al. Apathy in patients with mild cognitive impairment and the risk of developing dementia of Alzheimer’s disease: a one-year follow-up study. Clin Neurol Neurosurg 2006;108:733–6. 7 Jenner C, Reali G, Puopolo M, et al. Can cognitive and behavioural disorders differentiate frontal variant-frontotemporal dementia from Alzheimer’s disease at early stages? Behav Neurol 2006;17:89–95. Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. Stimulants are the other class of drug sometimes recommended for apathy, including methylphenidate (a potent norepinephrine and dopamine releaser) and modafinil. In a 6-week double-blind randomised controlled trial of methylphenidate in 60 patients with Alzheimer’s disease, there was improvement in two out of three apathy measures.44 Modafinil has been reported to help in case studies, but a small randomised trial in Alzheimer’s disease showed no significant effect.45 Box 2 Simple strategies for reducing the impact of apathy symptoms REVIEW 28 Yuen GS, Gunning-Dixon FM, Hoptman MJ, et al. The salience network in the apathy of late-life depression. Int J Geriatr Psychiatry 2014;29:1116–24. 29 Wongpakaran N, van Reekum R, Wongpakaran T, et al. Selective serotonin reuptake inhibitor use associates with apathy among depressed elderly: a case-control study. Ann Gen Psychiatry 2007;6:7. 30 Marin RS, Wilkosz PA. Disorders of diminished motivation. J Head Trauma Rehabil 2005;20:377–88. 31 Politis AM, Vozzella S, Mayer LS, et al. A randomized, controlled, clinical trial of activity therapy for apathy in patients with dementia residing in long-term care. Int J Geriatr Psychiatry 2004;19:1087–94. 32 Tondi L, Ribani L, Bottazzi M, et al. Validation therapy (VT) in nursing home: a case-control study. Arch Gerontol Geriatr 2007;44(Suppl 1):407–11. 33 Trinh NH, Hoblyn J, Mohanty S, et al. Efficacy of cholinesterase inhibitors in the treatment of neuropsychiatric symptoms and functional impairment in Alzheimer disease: a meta-analysis. JAMA 2003;289:210–16. 34 Devos D, Moreau C, Maltête D, et al. Rivastigmine in apathetic but dementia and depression-free patients with Parkinson’s disease: a double-blind, placebo-controlled, randomised clinical trial. J Neurol Neurosurg Psychiatry 2014;85:668–74. 35 Masanic CA, Bayley MT, VanReekum R, et al. Open-label study of donepezil in traumatic brain injury. Arch Phys Med Rehabil 2001;82:896–901. 36 Powell JH, al-Adawi S, Morgan J, et al. Motivational deficits after brain injury: effects of bromocriptine in 11 patients. J Neurol Neurosurg Psychiatry 1996;60:416–21. 37 Thobois S, Lhommée E, Klinger H, et al. Parkinsonian apathy responds to dopaminergic stimulation of D2/D3 receptors with piribedil. Brain 2013;136:1568–77. 38 Guttman M, Jaskolka J. The use of pramipexole in Parkinson’s disease: are its actions D3 mediated? Parkinsonism Relat Disord 2001;7:231–4. 39 Adam R, Leff A, Sinha N, et al. Dopamine reverses reward insensitivity in apathy following globus pallidus lesions. Cortex 2013;49:1292–303. 40 Kohno N, Abe S, Toyoda G, et al. Successful treatment of post-stroke apathy by the dopamine receptor agonist ropinirole. J Clin Neurosci 2010;17:804–6. 41 Van Reekum R, Bayley M, Garner S, et al. N of 1 study: amantadine for the amotivational syndrome in a patient with traumatic brain injury. Brain Inj 1995;9:49–54. 42 Corcoran C, Wong ML, O’Keane V. Bupropion in the management of apathy. J Psychopharmacol 2004;18:133–5. 43 Newburn G, Newburn D. Selegiline in the management of apathy following traumatic brain injury. Brain Inj 2005;19:149–54. 44 Rosenberg PB, Lanctôt KL, Drye LT, et al. MET Investigators. Safety and efficacy of methylphenidate for apathy in Alzheimer’s disease: a randomized, placebo-controlled trial. J Clin Psychiatry 2013;74:810–16. 45 Frakey LL, Salloway S, Buelow M, et al. A randomized, double-blind, placebo-controlled trial of modafinil for the treatment of apathy in individuals with mild-to-moderate Alzheimer’s disease. J Clin Psychiatry 2012;73:796–801. Stanton BR, Carson A. Pract Neurol 2016;16:42–47. doi:10.1136/practneurol-2015-001232 47 Pract Neurol: first published as 10.1136/practneurol-2015-001232 on 26 October 2015. Downloaded from http://pn.bmj.com/ on 15 July 2018 by guest. Protected by copyright. 8 Andersson S, Krogstad JM, Finset A. Apathy and depressed mood in acquired brain damage: relationship to lesion localization and psychophysiological reactivity. Psychol Med 1999;29:447–56. 9 Starkstein SE, Petracca G, Chemerinski E, et al. Syndromic validity of apathy in Alzheimer’s disease. Am J Psychiatry 2001;158:872–7. 10 Boström F, Jönsson L, Minthon L, et al. Patients with dementia with lewy bodies have more impaired quality of life than patients with Alzheimer disease. Alzheimer Dis Assoc Disord 2007;21:150–4. 11 Marsh NV, Kersel DA, Havill JH, et al. Caregiver burden at 1 year following severe traumatic brain injury. Brain Inj 1998;12:1045–59. 12 Davis JD, Tremont G. Impact of frontal systems behavioral functioning in dementia on caregiver burden. J Neuropsychiatry Clin Neurosci 2007;19:43–9. 13 Stout JC, Wyman MF, Johnson SA, et al. Frontal behavioral syndromes and functional status in probable Alzheimer disease. Am J Geriatr Psychiatry 2003;11:683–6. 14 Trabucchi M. An economic perspective on Alzheimer’s disease. J Geriatr Psychiatry Neurol 1999;12:29–38. 15 Starkstein SE, Leentjens AF. The nosological position of apathy in clinical practice. J Neurol Neurosurg Psychiatry 2008;79:1088–92. 16 Pluck GC, Brown RG. Apathy in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2002;73:636–42. 17 Cummings JL, Mega M, Gray K, et al. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 1994;44:2308–14. 18 Marin RS, Biedrzycki RC, Firinciogullari S. Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res 1991;38:143–62. 19 Levy ML, Cummings JL, Fairbanks LA, et al. Apathy is not depression. J Neuropsychiatry Clin Neurosci 1998;10:314–19. 20 Marin RS, Firinciogullari S, Biedrzycki RC. The sources of convergence between measures of apathy and depression. J Affect Disord 1993;28:117–24. 21 Landes AM, Sperry SD, Strauss ME. Prevalence of apathy, dysphoria, and depression in relation to dementia severity in Alzheimer’s disease. J Neuropsychiatry Clin Neurosci 2005;17:342–9. 22 Alexopoulos GS. Depression in the elderly. Lancet 2005;365:1961–70. 23 Joyce EM. Cognitive function in schizophrenia: insights from intelligence research. Br J Psychiatry 2013;203:161–2. 24 Apostolova LG, Akopyan GG, Partiali N, et al. Structural correlates of apathy in Alzheimer’s disease. Dement Geriatr Cogn Disord 2007;24:91–7. 25 Stanton BR, Leigh PN, Howard RJ, et al. Behavioural and emotional symptoms of apathy are associated with distinct patterns of brain atrophy in neurodegenerative disorders. J Neurol 2013;260:2481–90. 26 Marshall GA, Monserratt L, Harwood D, et al. Positron emission tomography metabolic correlates of apathy in Alzheimer disease. Arch Neurol 2007;64:1015–20. 27 Seeley WW, Menon V, Schatzberg AF, et al. Dissociable intrinsic connectivity networks for salience processing and executive control. J Neurosci 2007;27:2349–56.