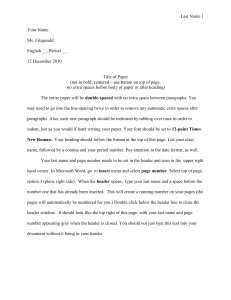
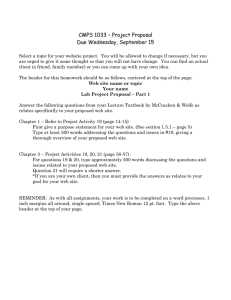
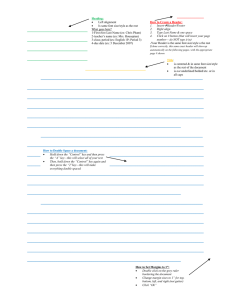
MODULE 04: BASIC PATHOLOGIES II Lecture Title (Font size 17, but adjust as needed) INSERT MD NAME HERE (All caps and bold; Name of lecturer followed by credentials, font size 8) MM/DD/YYYY (00:00-24:00) If the lecture is asynchronous, date will be the date of submission, and you may omit the time. SUBJECT (e.g. PATHOLOGY, PHARMACOLOGY, MICROBIOLOGY, PARASITOLOGY, PUBLIC HEALTH, RADIOLOGY, CLINICAL MEDICINE, FAMILY MEDICINE, etc. – if the lecture covers multiple subjects, separate with a comma) I. OVERVIEW OF MYCOSES A. NATURE OF HUMAN FUNGAL INFECTIONS More difficult to treat compared to bacterial and viral infections o Fungi invade when the the body is at its weakest state (i.e. immunocompromised) o Fungi have a thicker cell wall Have recently increased in incidence, severity, and susceptibility due to the following: o Advances in surgery o Cancer chemotherapy o Use of broad-spectrum antimicrobials in critically ill patients o Use of immunosuppressant drugs in transplant patients o HIV-AIDS epidemics May be classified as superficial or systemic o Systemic fungal infections are typically fatal for immunocompromised patients B. THE FUNGAL CELL Specific components of the fungal cell are targeted by different antifungal agents (04.44, 2023) o Cell Wall Targeted by echinocandins o Cell Membrane Targeted by amphotericin B, nystatin, azoles & terbinafine o Cytoskeleton Targeted by griseofulvin o Nucleus Targeted by flucytosine Table 1. Targets of Antifungal Agents FUNGAL CELL COMPONENT Cell Wall (w/ glucans) Cell Membrane (w/ ergosterol) Cytoskeleton (w/ microtubules) Nucleus (with nucleic acids) ANTIFUNGAL AGENTS Echinocandins Amphotericin B, Nystatin Azoles Terbinafine Griseofulvin Flucytosine ACTIVE RECALL 1. Antifungal agents target all of the following fungal cell components, except: a) Nucleus b) Mitochondria c) Cytoskeleton d) Plasma Membrane 2. True or False. Fungi have a thicker cell wall than gram positive bacteria ANSWERS: 1B, 2True Table 2. Overview of Different Organism Responsible for Fungal Infections CUTANEOUS MYCOSES Fungus Disease Dermatophytes Dermatophytosis Malassezia furfur Tinea Versicolor Cladosporium Tinea Nigra SUBCUTANEOUS MYCOSES Fungus Disease Sporothrix Sporotrichosis Cladosporium, etc. Chromomycosis (Various) Mycetoma SYSTEMIC MYCOSES Fungus Disease Coccidiodes Coccidioidomycosis Histoplasma Histoplasmosis Cryptococcus Blastomycosis Paracoccidiodes Paracoccidioidomycosis OPPORTUNISTIC MYCOSES Fungus Disease Candida Candidiasis Cryptococcus Cryptococcosis Aspergillus Aspergillosis Mucor & Rhizopus Mucormycosis Pneuomocystis Pneumonia II. DRUGS FOR SUBCUTANEOUS AND SYSTEMIC MYCOSES A. AMPHOTERICIN B The “penicillin of antifungal agents” (Cuenca, 2020) o First line, broad spectrum antifungal used in empiric antimicrobial therapy Remains the drug of choice in most cases despite its potential to be toxic o It has a tendency to harm host cell cholesterol instead of just fungal cell ergosterol o It has a very slow renal excretion, which can lead to nephrotoxicity An amphoteric polyene macrolide o Polyenes are compounds that attack ergosterol molecules Figure 1. Components of a fungal cell and the targets of antifungal drugs (Katzung, 14th ed) YL6: 04.LL MOA Binds to ergosterols in the fungal cell membrane, which leads to: o Pore formation Causing an increased cell permeability o Leakage of cellular content Majorly K+ ions Ionophores form complexes with ions and facilitate their transport across membranes o And then eventually, fungal cell death May be fungistatic or fungicidal, depending on: o The organism it is targeting Transcribed by TG [#]: [Surnames in alphabetic order, with TG police in bold] Checked by TG [#]: [Surnames in alphabetic order, with TG police in bold] 1 of 6 o The concentration of the drug Has a relative specificity o It usually targets ergosterols in the fungal cell membrane, but it can also bind to cholesterols in host cell membrane, which may cause harm to the host o To counter this potential toxicity, the drug is usually delivered via a lipid-associated delivery system (liposomal) rather than a colloid suspension Allows the drug to preferentially target fungal cell ergosterols rather than host cell cholesterols Reduces toxicity without sacrificing efficacy Allows its contents to be released gradually, which permits the use of larger doses o Very important for immunosuppressed and those with severe fungal infections Not used for chronic therapy or relapse prevention Can be taken on its own but it is suggested that it is combined with another drug to reduce its toxicity o Usually combined with flucytosine Empiric therapy for those with high risks of leaving a systemic fungal infection untreated (e.g. febrile neutropenic cancer patients on broad spectrum antibiotics) Intrathecal and local use o To treat mycotic corneal ulcers and keratitis Can also be used for as an antiprotozoal agent, specifically for: o Leishmania braziliensis o Naegleria fowleri Adverse Effects Figure 2. Mechanism of action of Amphotericin B Pharmacokinetics Absorption Most common route: parenteral o 90% protein-bound Other routes used: o Oral Poor absorption Effective only on the fungi along the GIT lumen o Intrathecal (through spinal canal) Adverse effects may happen such as arachnoiditis o Local Topical application Immediate (Infusion/IV) o Fever, chills, muscle spasms, vomiting, headache and hypotension Management: slow down infusion, decrease the daily dose, give premedication Premedication: Give other medication prior to starting the patient on anti-fungal e.g. give Acetaminophen first to lessen the effects of fever or chills before starting Amphotericin B Chronic/Cumulative o Nephrotoxicity (most significant toxic reaction) Characterized by renal tubular acidosis and severe K+ and Mg2+ wasting Managed with Na+ Loading and adequate hydration Dose-dependent and increased toxicity with concurrent therapy, specially with other nephrotoxic antibacterial agents such as aminoglycosides >3-4g cumulative o Hepatic dysfunction o Anemia due to decreased erythropoietin because of damaged renal tubular cells o Seizures and chemical arachnoiditis (if given intrathecally) o Thrombophlebitis B. FLUCYTOSINE Other names: 5-fluorocytosine or 5-FC A water-soluble, synthetic, fluorinated cytosine (pyrimidine) analog o Devoid of anticancer properties, but very potent The only antifungal agent that targets the nucleus of fungi Distribution Widely distributed o A reason for it being the first line antifungal o Inflammation favors penetration into various body fluids o However, only 2-3% reaches the CSF (poor distribution) o Can cross the placenta Metabolism & Excretion Mostly metabolized Renal excretion (very slow) o The reason for it being very nephrotoxic Therefore, it is only used in initial treatment (not chronic) The goal is to replace with a less toxic drug over time Antifungal Activity and Clinical Use Broadest spectrum of action Useful for any life-threatening fungal infections Drug of choice for systemic mycoses caused by: o Candida albicans o Cryptococcus neoformans o Histoplasma capsulatum o Blastomyces dermatitidis o Coccidioides immitis o Aspergillus fumigatus Initial Induction Regimen Therapy o Amphotericin B is the first-line treatment when a fungal infection is suspected based on signs and symptoms o Replaced after a while to prevent chronic use (nephrotoxicity) or when the specific fungus is already identified (by culture) Usually replaced with azoles YL6: 04.LL BASIC PATHOLOGIES II: Lecture Title MOA Inhibits nucleic acid synthesis o Flucytosine is converted to 5-fluorouracil, which is responsible for inhibiting DNA & RNA synthesis Several enzymes are involved in the action of Flucytosine o Cytosine permease - rarely found in human cells Allows 5-FC to be taken up inside the fungal cell o Cytosine deaminase – rarely found in human cells Allows 5-FC to be deaminated to 5-FU (fluorouracil) o Ribonucleotide reductase Converts 5-FU to 5-FUMP (5-fluorouridine monophosphate) 5-FUMP can then enter two pathways: o Interfering in protein synthesis (via RNA inhibition) 5-FUMP → 5-FUDP (fluorouridine diphosphate) → 5-FUTP (fluorouridine triphosphate) → leads to a faulty RNA o Inhibiting thymidylate synthetase 5-FUMP → 5-FdUMP (fluorodeoxyuridine monophosphate) → leads to inhibition of thymidylate synthetase 2 of 6 ACTIVE RECALL 2. 5-FC belongs to which class of substances a) Folic acid analog b) Pyrimidine analog c) Purine analog d) Cytosol analog 3. True or False. Amphotericin B is generally advised to be taken in combination with other drugs to reduce its toxic effects ANSWERS: 1B, 2 True REVIEW QUESTIONS Figure 2. Mechanism of action of Flucytosine Pharmacokinetics Absorption Most common route: oral Well-absorbed o Serum concentrations peak 1-2 hours after oral dose Distribution Widely distributed o Poorly protein-bound o Penetrates well into body fluid compartments o Good CSF penetration Metabolism & Excretion Renal excretion o Rapid rise in levels may lead to renal impairment Antifungal Activity and Clinical Use Monotherapy o Rarely used (restricted) o For select cases of non-life-threatening infections o Generally not as effective due to resistance Combination Therapy o Flucytosine is known to have a high incidence of primary or acquired resistance To avoid flucytosine resistance, it is usually combined with other antifungals o Flucytosine + Itraconazole Used to treat chromoblastomycosis o Flucytosine + Amphotericin B Used to treat cryptococcis (cryptococcal meningitis) and candidiasis This combination leads to an enhanced penetration through amphotericin-damaged fungal cell membranes Amphotericin B increases cell permeability, thus allowing more flucytosine to penetrate the cell and affect nucleic acids 1. Amphotericin B is usually taken in a combination therapy. Flucytosine is commonly used in initial induction regimen therapy. a) Only Statement 1 is true b) Only Statement 2 is true c) Both statements are true d) Both statements are false 2. Which enzyme is responsible for converting 5-FC to 5-FU a) Cytosine kinase b) Cytosine deaminase c) Cytosine permase d) Ribonucleotide reductase 3. Amphotericin B is usually delivered via a lipid-associated delivery system because: a) It allows the drug to preferentially bind host cell cholesterol b) It reduces the drug’s toxicity and efficacy c) It allows its contents to be released gradually, which permits the use of larger doses d) All of the above ANSWERS: 1D, 2B, 3C EXPLANATIONS: 1. D. Both statements are false – It’s the other way around. 3. C. It allows its contents to be released gradually, which permits the use of larger doses – A is false because it preferentially binds fungal cell ergosterol. B is false because it only reduces the drugs toxicity, while allowing its efficacy to be unchanged. REFERENCES REQUIRED Katzung, 14th ed. 04.44, 2023 Adverse Effects Hematologic effects o Bone marrow suppression with pancytopenia Hepatic injury Renal failure Gastrointestinal distress o Toxic enterocolitis o Nausea o Vomiting o Diarrhea Contraindications: o Extreme caution in patients with renal impairment o Pregnancy and breastfeeding Has a narrow therapeutic window o Increased risk for toxicity o AIDS, Azotemia, increased drug concentrationsLess toxic than amphotericin B YL6: 04.LL BASIC PATHOLOGIES II: Lecture Title 3 of 6 Last Name, First Name>. <Book Title>. <City of Publication>, <Publisher>, <Publication Year>. <Last Name, First Name or Organization>. “<Webpage Title>.” <Website>, [<url>]. Accessed <Day Month Year>. <Last Name, First Name, et al.>. “<Title of the article>.” <Title of the journal>, vol. <volume #>, no. <issue #>, <year>, pp. <page numbers>. <Title of the database>, <URL or DOI>. <Contributor>. <Date>. <Video Title> [Video]. Retrieved from [<url>]. ASMPH <Batch>. <MM>.<LL>: <Lecture Title> by <Lecturer, Credentials>. (1) <Lecturer>. <Date>. <Lecture Title> [Lecture slides]. (2) <Owner of Photo>. “<Title or Description>.” <Website>, <url>. Accessed <Day Month Year>. NOTE: o Add references that were used by the lecturer and/or the trans group. o References are to be arranged according to their order of appearance in the trans. This is so that it would be easier to refer to it in the references section as one goes through the trans. o If sources not belonging to the above categories (e.g. lecture, book, webpage, video) are used, use the appropriate MLA citation format. o If the in-text citation of the source is not specified in the module template/usage guide, use the appropriate MLA in-text citation format. SUPPLEMENTARY (1) See REQUIRED for sample formats. NOTE: o Add helpful, but non-required, references that were suggested by the lecturer and/or the trans group. o If sources not belonging to the above categories (e.g. lecture, book, webpage, video) are used, use the appropriate MLA citation format. FREEDOM SPACE Content: This space may be used for jokes, memes, quotes, inspirational messages and other content. Length: This section must NOT contribute another page. REMINDER: DOUBLE CHECK Header and Footer o Update the header and footer accordingly. o Brackets: <Brackets> are meant to signify placeholders and should not be included in the submission. o Footers: The footer on the first page and the footer on all succeeding pages are not linked so that the header does not appear on all pages. Headings o Check the cases and numbering of each heading. o Case: 01 Heading 1 & 02 Heading 2 are in uppercase. 03 Heading 3 & 04 Heading 4 are capitalized. All headings are in bold. o Alignment: 01 Heading 1 & 02 Heading 2 are centered. 03 Heading 3 & 04 Heading 4 are aligned left. o Numbering: Roman numerals for 01 Heading 1 and capital letters for 02 Heading 2. Figures and Tables o Check the numbering and formatting. Use Style 12 and 13. o Formatting: Tables MUST be encoded using the prescribed table format. Make sure that they are labeled accordingly. o Resolution: High enough for use as both a digital and physical reference. o Size: Figures must not exceed a total width of 3.5”. Table of Contents o Make sure that the contents reflect the trans outline. Update it one last time by going to the References tab of the Ribbon, and clicking “Update Table” and then selecting “Update entire table”. o Do NOT edit the table of contents directly. LAST NOTES: o Remove the references for trans format and MLA citation. o Remove the formatting “NOTE:” and examples of information (for layout purposes) within the trans. o Delete this REMINDER box. o If you have any questions, message Giana Barredo on Workplace. YL6: 04.LL BASIC PATHOLOGIES II: Lecture Title 4 of 6 MASTER TABLES Table A. Sample Master Table with multiple columns HEADER A HEADER B HEADER C Info Info Info Info Info Info HEADER D HEADER E Info Info Info Info Table B. Sample Master Table with 2 topics TOPIC A HEADER Info Info HEADER Info Info HEADER Info Info HEADER Info Info TOPIC B HEADER Info Info HEADER Info Info HEADER Info Info HEADER Info Info Table C. Sample Matrix Master Table TOPIC A HEADER Type Type Type HEADER Info Info Info HEADER Type Type Type HEADER Info Info Info TOPIC B HEADER Info Info Info HEADER Info Info Info HEADER Info Info Info HEADER Info Info Info Table D. Sample Master Table with 2 subtopics for each topic TOPIC A SUBTOPIC A HEADER Info Info HEADER Info Info HEADER Info Info HEADER Info Info HEADER Info Info HEADER HEADER HEADER Info Info HEADER Info Info SUBTOPIC B HEADER Info Info HEADER Info Info Info Info TOPIC B SUBTOPIC A Info Info HEADER Info Info HEADER Info Info SUBTOPIC B HEADER Info Info HEADER Info Info HEADER Info Info NOTE: o Purpose: A summary of important tables or a compilation of details in table form that would aid in reviewing and memorizing important concepts within the trans. o Master Tables are NOT part of the appendix. They are part of the QUICK REVIEW. o Label: Use letters to label the master tables. (i.e. start from Table A) o Hex color code: Topic: 9AAC9D Subtopic: C3D4CA Header (except Table A sample): BFBFBF Type: E7E6E6 o You may add bullet notes under the tables if needed (use 06 Bulleted List). o ALL tables should be continuous as much as possible. In the case that the table is too long, make sure to add the table headers where the table was cut. o If not applicable, you may omit this section. How to REMOVE the Master Tables page (without removing the Appendix page)? o Select from the “Master Tables” heading until the end of the page. o Click Format Columns Set as two (2) columns o Set the width to 3.5”, and tick the box for Equal column width. o Delete How to REMOVE Master Tables and Appendix page? o Command-A to select the entire document. o Click Format Columns Set as two (2) columns o Set the width to 3.5”, and tick the box for Equal column width. o Select from the last line of the page prior to the Master Tables page until the end of the appendix page Delete. YL6: 04.LL BASIC PATHOLOGIES II: Lecture Title 5 of 6 APPENDIX APPENDIX A: <Table Label> or <Figure Label> (i.e. Figure 2. Label) <Table or Figure> APPENDIX B: <Table Label> or <Figure Label> (i.e. Table 4. Label) <Table or Figure> NOTE: o Include the nice-to-know or supplementary tables and important figures referenced in the trans proper. (i.e. see Figure 2 and Table 4 example) o This space and beyond is set as a single column for formatting purposes. o If not needed, you may omit this part. How to REMOVE the appendix page? o Select the last line of the Master Tables page until the last line of the Appendix page. o Delete. YL6: 04.LL BASIC PATHOLOGIES II: Lecture Title 6 of 6