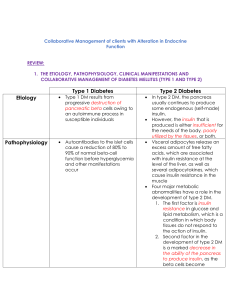
1. Type 1 diabetes is caused by the autoimmune destruction of the B cells in the pancreas, and the damaged pancreas doesn’t make insulin, so insulin injection is necessary for life. The initial onset of type 1 diabetes occurs rapidly among children and adolescents, and individuals have often experienced weight loss and have at higher risk for acidosis. In diet management, it is important to have regular daily intake of kilocalories from carbohydrate, protein and fat; in addition, extra food or snacks are needed to prevent hypoglycemia. Type 2 diabetes results from an insulin that not being produced enough or produced cannot be used. The individuals usually do not need exogenous insulin. Age of onset is generally older than 40 years old, and the genetic predisposition and obesity may be the main reasons. The diet therapy need built regular daily intake and decrease calories if weight loss is needed. 2. Retinopathy is a long-term complication associated with diabetes, and it involves damage to the small blood vessels in the retina. It often leads to small hemorrhages in the retina that involve yellow, waxy discharge or retinal detachment, even blindness. The tight control of the blood glucose level and intensive intervention can reduce retinopathy progression. Nephropathy means the hyperglycemia damages the small vessels within the kidneys, and its primary symptom is microalbuminuria. The blood glucose control and antihypertensive therapy can slow down its progression. Neuropathy indicates the highly sensitive nature of the small nerves to chronically elevated blood glucose levels. Damage to the nerves most commonly involves injury in the peripheral nervous system, especially in the legs and feet. The loss of nerve sensation can lead to further tissue damage and infection from unfelt foot injuries, so amputation and foot ulcerations are the most common results of severe neuropathy. Diabetic neuropathy is also linked to chronic problems such as motor deficits, cardiac ischemia, hypotension, bladder dysfunction. 3. Family history and race may be main risk factor for type 1 diabetes. It is more common in Northern European heritage. Overweight, physical inactivity, high-risk race like African American, Latino, Native American, these people have more risk for type 2 diabetes; in additional, women with a history of gestational diabetes or who have delivered an infant weighing over than 9 pounds, or hypertension, high cholesterol level, history of cardiovascular disease, and age older than 45 years are the risk factors for developing type 2 diabetes. 4. The consistent control of blood glucose levels helps to reduce the risks of chronic complication like hyperglycemia, hypoglycemia, and glycosuria, which indicate poor glycemic control, so monitoring blood glucose levels can identify when changes in insulin or food intake are necessary, and learn the glycemic response to different physical activity condition. 5. The diabetic patient should keep nutrition in balance, and daily food intake: 45% to 65% from CHO, 20% to 35% from fat, and 10% to 35% from protein. The basic food plan should be rich in complex carbohydrates and dietary fiber, low in simple sugars, saturated fats, and cholesterol. Moderate protein can increase the insulin response. Sodium should be reduced to less than 2300mg/day from the diet. Alcohol intake should be limited to a moderate amount. Food should be distributed throughout the day in fairly regular amounts and at regular times,