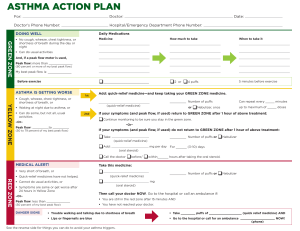
ASTHMA ACTION PLAN Personal Best Peak Flow___________ Jessica NAME_____________________DOCTOR______________________ph#__________ ◊ ◊ ◊ ◊ ◊ AVOID YOUR TRIGGERS POLLEN ◊ COLD/FLU ◊ ANIMALS, PET DANDER EXERCISE ◊ DUST MITES ◊ AIR POLLUTION MOLD ◊ WEATHER ◊ SMOKE PLANTS, FLOWERS, GRASS, POLLEN STRONG ODORS, PERFUMES ◊OTHER___________________ THE GREEN ZONE (also known as the Safety Zone) SYMPTOMS ◘ ◘ ◘ ◘ ◘ Use these controller medicines as listed Breathing is easy No cough or wheeze Can sleep through the night Can sleep through the night Able to exercise MEDICATION HOW MUCH WHEN Albuterol 1 puff Q 2x/day Singular 1 tab Daily Peak flow from ____to____ 214 (pt’s over 5 yrs old) THE YELLOW ZONE (also known as the CAUTION ZONE) SYMPTOMS ◘ ◘ ◘ ◘ ◘ Continue with controller medicines as above Some shortness of breath Cough, wheeze, or chest tightness Some difficulty doing usual activities Sleep disturbed by symptoms Symptoms of a cold or flu 107 and ADD rescue medicines MEDICATION HOW MUCH WHEN Atrovent 4-8 puffs Q 20 min Prednisone 5mg/5mL PO BID Montelurast 5 mg PO Q PM 171 Peak flow from____to____ (pts over 5 years old) THE RED ZONE (also known as the DANGER ZONE) SYMPTOMS ◘ Severe breathing problems ◘ Cannot do usual activities ◘ Difficulty walking and talking ◘ Rescue medicine is not helping Take this medicine and call the doctor NOW MEDICATION HOW MUCH WHEN Albuterol 4 puffs Immediately 1 puff in ER Immediately via nebulizer <107 Peak flow from_____to_____ (pts over 5 years old)_ IF SYMPTOMS DO NOT IMPROVE AND YOU CANNOT CONTACT THE DOCTOR GO TO THE HOSPITAL OR DIAL 911 FOLLOWUP APPOINTMENT SCHEDULED 1 Week WITH DR. PCP PHYSICIAN SIGNATURE___________________________________DATE_________________________ Renown logo Patient stamp