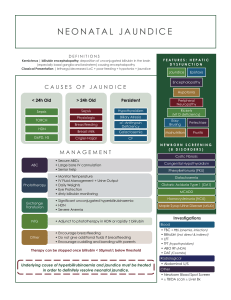
Semester 3X/4C Week 6-7 (H&L 2) Review 1. A 7-year-old boy presents to the ER with anemia and hemarthrosis. The boy has a sister with a similar bleeding disorder, one that involves a normal Platelet Count, BT, and PT. The only abnormality is a prolonged PTT. Wanting to correct the PTT, which treatment would be suggested for this patient? A. Transfusing the patient with recombinant vWF B. Administering a megakaryocyte precursor growth factor C. Transfusing normal plasma D. Administering recombinant ADAMTS-13 1. A 7-year-old boy presents to the ER with anemia and hemarthrosis. The boy has a sister with a similar bleeding disorder, one that involves a normal Platelet Count, BT, and PT. The only abnormality is a prolonged PTT. Wanting to correct the PTT, which treatment would be suggested for this patient? A. Transfusing the patient with recombinant vWF B. Administering a megakaryocyte precursor growth factor C. Transfusing normal plasma D. Administering recombinant ADAMTS-13 Given that the patient has hemarthrosis and a family history of a bleeding disorder, you should immediately be thinking that this is a familial bleeding disorder, likely either Hemophilia A or B. This is confirmed by all lab values being normal except for the prolong PTT. Given the question stem, you won’t be able to differentiate whether the patient has Hemophilia A or B, but this isn’t important in answering the question. Since Hemophilia A is a deficiency in Factor VIII and Hemophilia B is a deficiency in Factor IX, there will be an issue in the intrinsic coagulation pathway (aka PTT). So to correct the PTT, all you’ll need is normal of either Factor VIII or XI, which can be found in normal plasma. A. B. D. TTP. Treating with recombinant vWF won’t correct the PTT since the deficiency is either Factor VIII or XI. This would not work since the issue is not a thrombocytopenia, as told with the normal platelet count. This will not work since there is no deficiency in ADAMTS-13, as there is in 2. While on your pediatrics rotation, you come across an infant patient with the primary complaint of “Nutcracker Syndrome”. Which clinical finding should you immediately expect to find? A. B. C. D. E. F. Pale Infarct of the Left Kidney Red Infarct of the Left Testicle Red Infarct of the Right Kidney Pale Infarct of the Right Testicle Red Infarct of the Right Testicle Pale Infarct of the Left Testicle 2. While on your pediatrics rotation, you come across an infant patient with the primary complaint of “Nutcracker Syndrome”. Which clinical finding should you immediately expect to find? A. B. C. D. E. F. Pale Infarct of the Left Kidney Red Infarct of the Left Testicle Red Infarct of the Right Kidney Pale Infarct of the Right Testicle Red Infarct of the Right Testicle Pale Infarct of the Left Testicle You should already go into this question knowing what Nutcracker Syndrome is, but as a refresher, it’s when the left renal vein gets compressed between the Abdominal Aorta and the Superior Mesenteric Artery. Therefore, you should suspect there to be venous occlusion of the left renal vein. Typically, venous occlusions lead to red infarcts, as blood is able to reach the target organ, but has no exit out, thus allowing for blood to pool in the target organ, causing it to be engorged in blood (hence “red” infarct). So knowing that there’s venous occlusion on the left side, that should narrow down the choices to red infarcts on the left side, thus leaving Red Infarct of the Left Testis as the correct answer. 3. Which antimetabolite of purine nucleotides is NOT matched up with its proper analog? A: 6-Mercaptopurine(6-MP) to Hypoxanthine B: Azaserine (AS) to Glutamine (Gln) C: Aminopterin (AP) to Folic Acid D: Methotrexate (MTX) to Folic Acid E: 5-Fluorouracil (5-FU) to Thymine 3. Which antimetabolite of purine nucleotides is NOT matched up with its proper analog? A: 6-Mercaptopurine(6-MP) to Hypoxanthine B: Azaserine (AS) to Glutamine (Gln) C: Aminopterin (AP) to Folic Acid D: Methotrexate (MTX) to Folic Acid E: 5-Fluorouracil (5-FU) to Thymine Answer: E is a PYRIMIDINE Analog thus not the correct answer though it is the correct antimetabolite analog. A-D are all PURINE antimetabolites that match up with their analog. 4) A 6 year old boy presents to the clinic with hyperuricemia, dystonia, and “sand” like crystals in his diaper. What molucule would you expect to see in excess leading to the patient’s symptoms? A: Ribose-5-Phosphatase B: PRPP (phosphoribosyl pyrophosphate) C: Thymidylate Synthase D: CSP-II (carbamoyl phosphate synthase II) E: UMP Synthase 4) A 6 year old boy presents to the clinic with hyperuricemia, dystonia, and “sand” like crystals in his diaper. What molecule would you expect to see in excess leading to the patient’s symptoms? A: Ribose-5-Phosphatase B: PRPP (phosphoribosyl pyrophosphate) C: Thymidylate Synthase D: CSP-II (carbamoyl phosphate synthase II) E: UMP Synthase Correct Answer is B: This patient has Lesch-Nyhan Syndrome based upon the hyperuricemia (which will lead to gout), the dystonia, and the uric acid crystals “sand”. Also, the fact that a 6yo is still in diapers displays a developmental development which is also seen in Lesch-Nyhan. Lesch-Nyhan will have defective purine salvaging due to an absent HGRT [hypoxanthine guanine phosphoribosyltransferase]. The precursor for HGRT is PRPP [phosphoribosyl pyrophosphate] and without HGRT the patient will have excess PRPP leading to an increase in Guanine, Hypoxanthine, Xanthine and thus Uric Acid. Answer A is what what’s used in De novo synthesis to make IMP which then later makes AMP & GMP. Answers C, D, and E are mechanisms in the Pyrimidine base production pathway and not a factor with Lesch-Nyhan syndrome. 5) A male patient, 40-50 yo presents to the clinic complaining of abdominal pain. He has been going to AA meetings for the last 2 years but hasn’t been attending lately due to the pandemic. He seems a bit fatigued and has red lesions on his hands. The attached image is his urine sample. What enzyme is most likely INCREASED in this patient? A: ALAS1 B: δ-aminolevulinate synthase C: Uroporphyrinogen decarboxylase D: Uroporphyrinogen III synthase E: ALA dehydratase 5) A male patient, 40-50 yo presents to the clinic complaining of abdominal pain. He has been going to AA meetings for the last 2 years but hasn’t been attending lately due to the pandemic. He seems a bit fatigued and has red lesions on his hands. The attached image is his urine sample. What enzyme is most likely INCREASED in this patient? A: ALAS1 B: δ-aminolevulinate synthase C: Uroporphyrinogen decarboxylase D: Uroporphyrinogen III synthase E: ALA dehydratase Answer: A. With ALL Porphyrias heme synthesis is decreased, because of this ALAS1 is not inhibited by hemin therefore it’s activity is increased. The Porphyria described is Porphyria Cutanea Tarda, clinical expression is described as red lesions on hands and red colored urine that has no RBCs. Clinical expression is influenced by alcohol, as well as Fe load, Sunlight exposure, Hep B/C, HIV, or Estrogen therapy. The enzyme deficient in this disease is C. 6) A infant is brought in for a general follow-up. You notice yellow tinge to his skin. In his chart, it states that the child had phototherapy when born. A certain type of bilirubin is increased in blood work that is ordered. Match the correct enzyme deficiency to the correct increase bilirubin. A: MRP2/Unconjugated B: OATP1B1/Conjugated C: UDP-glucuronyl transferase/Conjugated D: Bilirubin Glucuronyl Transferase/Unconjugated E: OATP1B1/Unconjugated 6) A infant is brought in for a general follow-up. You notice yellow tinge to his skin. In his chart, it states that the child had phototherapy when born. A certain type of bilirubin is increased in blood work that is ordered. Match the correct enzyme deficiency to the correct increase bilirubin. A: MRP2/Unconjugated B: OATP1B1/Conjugated C: UDP-glucuronyl transferase/Conjugated D: Bilirubin Glucuronyl Transferase/Unconjugated E: OATP1B1/Unconjugated Answer is D. Phototherapy is used to treat Neonatal jaundice which has incomplete maturation of Bilirubin Glucuronyl transferase, this produces Unconjugated Bilirubin because the Bilirubin is unable to be transferred into the liver. The child has Gilbert Syndrome the yellow tint to skin helps with this and Unconjugated Bilirubin is increased in this disease as well. B is the only correct match and is Rotor Syndrome. 7) A 25 y/o female presents to the clinic complaining of morning joint stiffness for 30 minutes, a rash that comes and goes, and general feelings of malaise/feverish. Vitals are 110/70 mmHg, 24 breaths per min, and a pulse ox of 94%. Upon a general inspection, patient looks to be in respiratory distress with SOB. A complete heart and lung exam were performed with no abnormal findings. The patient states to have had a recent doctor’s appointment where she was diagnosed with Wolff-Parkinson-White syndrome (WPW), which she is on appropriate medications for. Being a wonderful physician, you already have a list of possible diagnoses for what this patient currently has, and order some lab work to confirm your top suspicion. What would you expect to see? A: Elevated anti ds-DNA and anti-Smith antibodies B: T cell mediated hypersensitivity response C: Positive Rheumatoid Factor D: Positive HLA-B27 antigen E: Elevated anti-histone antibodies 7) A 25 y/o female presents to the clinic complaining of morning joint stiffness for 30 minutes, a rash that comes and goes, and general feelings of malaise/feverish. Vitals are 110/70 mmHg, 24 breaths per min, and a pulse ox of 94%. Upon a general inspection, patient looks to be in respiratory distress with SOB. A complete heart and lung exam were performed with no abnormal findings. The patient states to have had a recent doctor’s appointment where she was diagnosed with Wolff-Parkinson-White syndrome (WPW), which she is on appropriate medications for. Being a wonderful physician, you already have a list of possible diagnoses for what this patient currently has, and order some lab work to confirm your top suspicion. What would you expect to see? A: Elevated anti ds-DNA and anti-Smith antibodies B: T cell mediated hypersensitivity response C: Positive Rheumatoid Factor D: Positive HLA-B27 antigen E: Elevated anti-histone antibodies This is a great example of how a Mini question may be worded for you. 2 of the above answer choices are slightly wrong as well, which makes for great discussion. Key points in this question stem are bolded for your review. Patient is experiencing a classic triad of fever, joint pain, and a rash, which points to SLE. Furthermore, the patient is a female in her 20-30’s, making her fit the ideal demographics for this autoimmune mediated disease. Low BP and tachypnea are most probably due to serositis. As the patient is on medications for a recent diagnosis WPW (procainamide!), and there is also no heart involvement in her current presentation, this points towards drug-induced lupus, with elevated anti histone Abs. A: Found in SLE (non drug induced) B. Lupus is a type III hypersensitivity response involving generation of immune complexes on affected tissue. These are not T cell mediated (that’s type IV). C. RF found in rheumatoid arthritis D. HLA B27 associated with ankylosing spondylitis in males 8) A 45 y/o male is currently on a drug regimen recommended by his physician in anticipation for a kidney transplant within a few weeks. He presents at your clinic with difficulty breathing and a really bad headache. Upon checking vitals, you see that the patient has a BP of 150/90 mmHg, 20 breaths per minute, 90 bpm, and a 98% O2 reading. Your patient is especially worried because he has been seeing red in his urine for the past two days. Based on the patient’s presentation, you deduce that the drug regimen prescribed to him is faulty, and correct the mistake. What’s the mechanism of action of the drug causing this current presentation? A: Inhibition of mTOR B: Increased nuclear transcription of NFAT C: Blockade of CTLA-4 interaction with B7 D: Inhibition of IL-2 gene expression E: Inhibition of TNFa 8) A 45 y/o male is currently on a drug regimen recommended by his physician in anticipation for a kidney transplant within a few weeks. He presents at your clinic with difficulty breathing and a really bad headache. Upon checking vitals, you see that the patient has a BP of 150/90 mmHg, 20 breaths per minute, 90 bpm, and a 98% O2 reading. Your patient is especially worried because he has been seeing red in his urine for the past two days. Based on the patient’s presentation, you deduce that the drug regimen prescribed to him is faulty, and correct the mistake. What’s the mechanism of action of the drug causing this current presentation? A: Inhibition of mTOR B: Increased nuclear transcription of NFAT C: Blockade of CTLA-4 interaction with B7 D: Inhibition of IL-2 gene expression E: Inhibition of TNFa The drug that is causing this patient’s symptoms is Cyclosporine. This is due to it’s BBW of nephrotoxicity (blood in urine) and hypertension (150/90). You would want to avoid giving this drug to patients that are at risk of renal impairment, such as this patient that is looking for a kidney transplant! A. Sirolimus inhibits mTOR. This is the correct drug that should have been given to this patient, considering his risk of renal toxicity B. Nuclear transcription of NFAT is inhibited, not increased, by calcineurin complexing with cyclosporin C. Immunostimulant (not correct in this case). MOA of Ipilimumab E. Inflixifmab 9) A 46 year old man reports to the ED with a blistering rash on his face and arms for 2 weeks. The rash occurs in sun-exposed areas. He also notices that his urine is darker than normal. Examination of the skin reveals multiple fluid-filled blisters and erosions. What is the most appropriate pharmacotherapy? A) B) C) D) Hemin Prednisone Acyclovir hydroxychloroquine A 46 year old man reports to the ED with a blistering rash on his face and arms for 2 weeks. The rash occurs in sun-exposed areas. He also notices that his urine is darker than normal. Examination of the skin reveals multiple fluid-filled blisters and erosions. What is the most appropriate pharmacotherapy? A) B) C) D) Hemin Prednisone Acyclovir hydroxychloroquine Hydroxycholroquine- treatment of PCT is avoidance of known triggers and administration of hydoxycholoroquine or choloroquine which form water-soluble complexes with porphyrin rings. Phlebotomy is also an option in patients with iron overload or contraindications to hydroxycholorquine. Hemin is an iron-containing protein that blocks heme synthesis and is used to treat AIP. AIP is associated with upregulation of ALAS activity due to decreased activity of porphobilinogen deaminase. It is important to distinguish acute porphyrias from chronic porphyrias because treatment of acute porphyrias will actually exacerbate chronic porphyrias. Acute porphyrias are typically accompanied by neuro and abdominal symptoms. 10) A 62 year old post-menopausal woman reports to her PCP for a 2 month history of fatigability and dyspnea on exertion. PE shows conjunctival palor and peripheral blood smear shows small, pale rbcs. Further evaluation is likely to show which of the following? A)Dry bone marrow tap B)Decreased serum haptoglobin C)Increased serum methylmalonic acid concentration D) Positive stool guaiac test A 62 year old post-menopausal woman reports to her PCP for a 2 month history of fatigability and dyspnea on exertion. PE shows conjunctival palor and peripheral blood smear shows small, pale rbcs. Further evaluation is likely to show which of the following? A)Dry bone marrow tap B)Decreased serum haptoglobin C)Increased serum methylmalonic acid concentration D) Positive stool guaiac test Correct answer: Positive stool guaiac test- MCC of iron deficiency anemia in adult males and post-menopausal woman is chronic iron loss 2/2 GI bleeding. Haptoglobin can be thought of as like a scavenger that searches the blood for broken/damaged heme. Broken/damaged heme is usually found in hemolytic anemias, so when you have a hemolytic anemia, all the haptoglobin in being used up since there’s lots of broken heme to scavenge, which is why you’d see decreased haptoglobin usually in the hemolytic anemias, not the anemia due to iron deficiency. In Iron-Deficient Anemia vs the Hemolytic Anemia, the reason Haptoglobin is decreased in Hemolytic is because the Hematocrit is low due to RBC DESTRUCTION. Whereas in Iron-Deficient Anemia, the Hematocrit is low due to DECREASED RBC PRODUCTION. A 62 year old post-menopausal woman reports to her PCP for a 2 month history of fatigability and dyspnea on exertion. PE shows conjunctival palor and peripheral blood smear shows small, pale rbcs. Further evaluation is likely to show which of the following? A)Dry bone marrow tap B)Decreased serum haptoglobin C)Increased serum methylmalonic acid concentration D) Positive stool guaiac test Correct answer: Positive stool guaiac test- MCC of iron deficiency anemia in adult males and post-menopausal woman is chronic iron loss 2/2 GI bleeding. A 62 year old post-menopausal woman reports to her PCP for a 2 month history of fatigability and dyspnea on exertion. PE shows conjunctival palor and peripheral blood smear shows small, pale rbcs. Further evaluation is likely to show which of the following? A)Dry bone marrow tap B)Decreased serum haptoglobin C)Increased serum methylmalonic acid concentration D) Positive stool guaiac test Correct answer: Positive stool guaiac test- MCC of iron deficiency anemia in adult males and post-menopausal woman is chronic iron loss 2/2 GI bleeding. Resources 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Hemodynamic Disorders 1 Hemodynamic Disorders 2 Metabolism of Purine & Pyrimidines Metabolism of Purine & Pyrimidines Heme Metabolism Heme Metabolism Autoimmune Diseases Immunomodulators TBL Hemodynamic Disorders Heme Metabolism Questions? Comments? Rossiereview@gmail.com