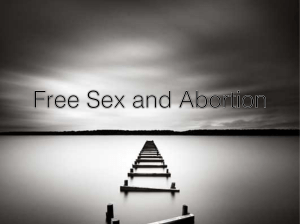
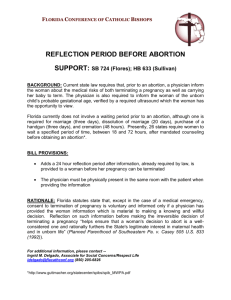
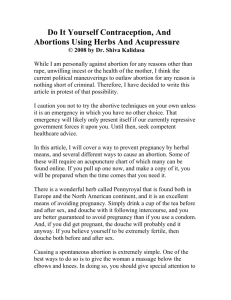
OBSTETRICS 2 BLEEDING IN THE FIRST HALF OF PREGNANCY Therese Beriña-Mallen, MD First Shift: August 15, 2018 Table of Contents REMEMBER G TEXTBOOK & EDITOR ! I. ABORTION ......................................................................... 1 A. Pathogenesis .............................................................. 1 Majority of the content are lifted from Dra. Mallen’s PPT with a little bit of handpicked items from Williams 25th ed. There are some changes in the latest edition so if you are using a previous trans, try to cross-reference it with Williams 25th ed. When in a rush, skip to the last page for the summary. Happy studying! B. Fetal Factors .............................................................. 1 C. Maternal Factors ........................................................ 2 D. Classification of Abortion ............................................ 2 E. Classification of Spontaneous Abortion ...................... 2 F. Early Pregnancy Loss ................................................. 3 G. Induced Abortion | & (not discussed) ....................... 3 H. Recurrent Abortion ..................................................... 4 I. Incompetent Cervix ...................................................... 4 J. Septic Abortion ............................................................ 4 I. ABORTION II. ECTOPIC PREGNANCY ................................................... 5 A. Heterotropic Pregnancy .............................................. 5 B. Risk Factors ............................................................... 5 C. Outcomes ................................................................... 5 D. Clinical Manifestations ............................................... 5 E. Differential Diagnosis for Abdominal Pain in Pregnancy F. Diagnosis .................................................................... 6 5 • Spontaneous or induced termination of pregnancy before fetal viability | & (new definition from Williams 25th ed) • Defined as spontaneous or induced termination of pregnancy (old definition from Williams 24th ed) o Prior to 20 weeks AOG or o With a fetus weighing <500g • Bleeding is most predictive risk factor for pregnancy loss | &G G. Threatened Abortion vs Ectopic Pregnancy............... 6 H. Dead fetus .................................................................. 6 I. Medical Management .................................................. 6 J. Surgical Management ................................................. 7 III. GESTATIONAL TROPHOBLASTIC DISEASE ................ 8 A. Classification .............................................................. 8 B. Strongest Risk Factors ............................................... 8 C. Racial Predilection ..................................................... 8 D. Epidemiology and Risk factors | & ........................... 8 E. Partial vs Complete Mole ........................................... 8 F. Clinical Manifestations ................................................ 8 G. Diagnosis ................................................................... 8 H. Sonography ................................................................ 8 I. Pathology | & ............................................................. 9 J. Management | & ........................................................ 9 K. Molar Pregnancy Termination .................................... 9 L. Gestational Trophoblastic Neoplasia .......................... 9 M. FIGO Staging for GTN ............................................. 10 N. Modified WHO Prognostic Scoring System .............. 10 O. HIGH YIELD SUMMARY ......................................... 11 A. Pathogenesis • More than 80% of spontaneous abortions occur within the first 12 weeks of gestation | & Bleeding into the decidua basalis following fetal death (recall that the decidua basalis is the deepest layer in the pregnant endometrium) ↓ Necrosis of adjacent tissues ↓ Uterine contractions initiated ↓ Expulsion B. Fetal Factors • Abortions due to fetal factors usually occur < 8-10 weeks • Most aneuploid abortions (95%) occur because of maternal gametogenesis errors • Incidence of euploid abortions increases after maternal age 35 | G o Euploid pregnancies abort later than aneuploid ones | & • Monosomy X (45, X) or Turner Syndrome o Single most frequent specific chromosomal abnormality 1 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE C. Maternal Factors • Abortions due to maternal factors occur at a later time > 810 weeks • Central factor is stress | G o Stress promotes the release of CRH which causes the uterus to lose its quiescent state | G • Age (>35) • Infections • Medical disorders (poorly controlled DM, thyroid disease, obesity, SLE) • Cancer and its treatment (radiotherapy, chemotherapy) • Surgical procedures o Uncomplicated procedures performed during early pregnancy are unlikely to increase abortion risk o Exception: early removal of corpus luteum or the ovary in which a tumor resides • Nutrition o Obesity raises pregnancy loss rates o Sole deficiency of one nutrient or moderate deficiency of all does NOT appear to increase risk o Underweight is NOT associated with greater risk • Social and behavioral factors o Regular and heavy alcohol intake o Cigarette smoking o > 5 cups of coffee/day • Occupational and environmental factors o Bisphenol A, phthalates, polychlorinated biphenyls, and dichlorodiphenyltrichloroethane or DDT; radiation exposure, nitrous oxide) • Uterine defects (eg. myoma) D. Classification of Abortion • Spontaneous - most occur prior to 12 weeks o Threatened o Inevitable o Incomplete o Complete o Missed • Induced • Recurrent • Septic - abortion complicated by infection E. Classification of Spontaneous Abortion • Remember the clinical presentation (uterine size, cervix closed/dilated) and management | ! 1. Threatened Abortion a. Clinical presentation § § § § § Lower abdominal/hypogastric crampy pain/discomfort Bloody vaginal discharge/vaginal bleeding Cervix closed | G Uterine size is compatible with AOG based on LMP | G Subchorionic hemorrhage may also be a sign | G b. Management § Bed rest | G * Why bed rest? Lying in a supine position may decrease the pressure of gravity on the uterus and implanted fetus. It is also important to address the other problems which may have caused the bleeding (eg. infection) | ! * In practice, they sometimes give tocolytics but the primary management is still BED REST | G § Acetaminophen-based analgesia will help relieve discomfort from cramping | & § Hematocrit and blood type is determined. if there is significant anemia or hypovolemia, perform evacuation (but if fetus is live, some opt for transfusion and further observation) 2. Inevitable Abortion o Preterm premature rupture of membranes (PPROM) at a previable gestational age a. Clinical presentation § § § § (+) bleeding, pain (±) fever (+) cervical dilatation | G Gross rupture of membranes | G b. Confirmation of membrane rupture § A gush of vaginal fluid seen pooling during sterile speculum examination confirms the diagnosis * May lumabas na fluid through the cervix after bearing down or Valsalva maneuver | ! § In suspected cases: * (+) ferning * pH > 7.0 * Oligohydramnios on sonography * AF Positive for proteins placental alpha microglobulin1 and insulin growth factor binding protein-1 § According to Dra. Mallen, in practice, the best measure is the physical evidence of the fluid pooling at the cul de sac | G c. Management § Uterine evacuation | G * No choice but to evacuate the uterus because the membranes have ruptured! This is a point of no return as membrane rupture puts the woman at risk for infection, specifically chorioamnionitis | ! 3. Incomplete Abortion o If <10 weeks, fetal and placental parts expelled together o If >10 weeks, separately (thus, tissue may remain entirely within the uterus or partially extrude through the cervix) a. Clinical presentation § (+) bleeding, pain § (+) cervical dilatation | G * The cervix remains dilated because there are still some tissues left in the uterus. The uterus is not yet done with its job of expelling its contents and may ilalabas pa so the ‘door’ (cervix) remains open | ! § (+) passage of placental (“meaty”) tissues | G § Uterine size usually smaller than expected based on LMP * Because some of its contents have already been expelled | ! b. Management § Completion curettage | G * Completion curettage is preferred because it may take time for the uterus to respond to the uterotonics eventually making the woman prone to infection | ! § Medical (Misoprostol) § Expectant 2 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE c. Disadvantages of medical and expectant management § Unpredictable bleeding (anemia due to blood loss) § May eventually end up doing curettage § Deferred in clinically unstable women or those with uterine infection 4. Complete Abortion a. Clinical presentation § (+) heavy bleeding, pain § (+) cervix closed | G * The cervix is now closed because ALL of the fetus has been expelled. :( The uterus has fulfilled its job and wala na siyang mabubuga so the ‘door’ (cervix) is now closed § (+) passage of placental (“meaty”) tissues | G § Uterine size either normal or slightly enlarged b. To confirm diagnosis § Patient presents to you the expelled placental tissues or collapsed sac § On TVS, minimally thickened endometrium without a gestational sac | G § Serial B-hCG levels drop quickly with complete abortion Table 1| Percentage decline following complete spontaneous abortion (nice to know only) Initial ß-HCG (mIU/ml) By Day 2 By Day 4 By Day 7 50 68 78 88 100 68 80 90 300 70 83 93 500 71 84 94 1000 72 86 95 2000 74 88 96 3000 74 88 96 4000 75 89 97 5000 75 89 97 c. Management § Reassurance/Observe | G 5. Missed Abortion o Dead products of conception retained for days to months in utero, with a closed cervical os * According to Dra. Mallen, basically, tinamad yung uterus. Ideally, the uterus expels the fetus when it dies. But since tinamad yung uterus, it DID NOT contract and the dead fetus remained in uterus with a CLOSED cervix. If left untreated, the woman may have an infection or worse, progress into DIC | ! o Currently, missed abortion is used interchangeably with early pregnancy loss/wastage b. Diagnosis § Diagnosis is imperative prior to intervention and avoids interruption of a potentially live IUP | & § Rapid confirmation of fetal death is possible with VS and serial ß-HCG * Primary tool: transvaginal ultrasound | & * Check via UTZ for fetal heart tone | G § Mean death-to-abortion interval is 6 weeks c. Management § Dilation & curettage | G * Mechanical dilators (eg. laminaria) or PGE may be used to dilate the cervix | ! * Mechanical is faster acc. to Dra. Mallen | ! F. Early Pregnancy Loss • A nonviable, intrauterine pregnancy (IUP) with either: o An empty gestational sac or o A gestational sac containing an embryo or fetus without fetal heart activity within the first 12 6/7 weeks of gestation 1. Criteria for diagnosis of early pregnancy loss o Acc. To Dra. Mallen, no need to study this daw, pang- fellow level na daw ito | ! a. Sonographic findings § CRL ≥ 7 mm and no heartbeat § MSD ≥ 25 mm and no embryo § An initial US scan shows a gestational sac with yolk sac, and after ≥ 11 days no embryo with heartbeat is seen § An initial US scan shows a gestational sac without yolk sac, and after ≥ 2 weeks no embryo with heartbeat is seen G. Induced Abortion | & (not discussed) • Medical or surgical termination of pregnancy before the time of fetal viability 1. Types of Induced Abortion a. Therapeutic abortion § Termination for medical indications (most frequent: prevent birth of fetus with significant anatomical, metabolic, or mental deformity) § Based on our med ethics class: NOT ETHICAL b. Elective/voluntary abortion § Interruption of pregnancy before viability at the request of the woman, but not for medical reasons § Also NOT ETHICAL a. Clinical presentation § Early part of pregnancy appeared to be normal (with signs and symptoms related to intrauterine pregnancy) § After embryonic death, spontaneous miscarriage will eventually ensue § Cervix closed | G § If kamamatay lang ng fetus, the uterine size may still be compatible with AOG. If there is a longer interval, mas maliit na ang uterus | ! 3 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE H. Recurrent Abortion • Aka Recurrent Pregnancy Loss/Habitual Abortion • Defined as 2 or more consecutive abortions confirmed by sonographic or histopathological examination | G& (new definition from Williams 25th ed) 1. Types of Recurrent Abortion a. Primary RPL § Multiple losses in a patient who has never delivered a liveborn b. Secondary RPL § Multiple losses in a patient with prior live birth 2. Etiology o Three widely accepted causes of RPL | & § Parental chromosomal abnormalities § Antiphospholipid antibody syndrome § Structural uterine abnormalities o Genetic factors usually result in early embryonic losses | & o Autoimmune or uterine anatomical abnormalities are more likely cause 2nd trimester losses | & Table 2| Factors implicated in recurrent pregnancy losses ETIOLOGY EXAMPLES • Balanced Translocation Chromosomal • Robertsonian Translocation abnormalities • Mosaicism • Asherman’s Syndrome Anatomical • Myomas | G factors • Congenital malformations Immunological • APAS (Antiphospholipid Antibody Syndrome) factors • Alloimmune factors • Uncontrolled DM Endocrine • Hypothyroidism factors • Luteal phase defect I. Incompetent Cervix • Aka Cervical Insufficiency | & • Painless cervical dilatation in the second trimester | G & • Can be followed by prolapse and ballooning of membranes into the vagina and expulsion of an immature fetus | & 1. Risk factors o Previous cervical trauma § Dilatation and curettage § Conization (excision of cervical tissue) § Cauterization 2. Diagnosis o TVS § Cervical length < 2.5 cm § Funneling (ballooning of the membranes into a dilated internal os but with closed external os) Figure 1 | Cervical funnel shapes 3. Management o Cerclage (ideally between the 12th-14th week AOG) o Surgical indications: § Unequivocal hx of 2nd trimester painless delivery (prophylactic cerclage) § Physical finding of early dilation of the internal cervical os (may be an indicator of insufficiency) § Funneling on TVS o With imminent abortion or delivery, the suture should be removed at once because uterine contractions can tear through the uterus or cervix Figure 2 | Cerclage for incompetent cervix J. Septic Abortion • Acc. to Dra. Mallen, septic abortion may complicate all the other types of abortion discussed above. However, this is more common in induced abortions (esp. in unsterile settings), and inevitable abortions. • Abortion complicated by infection (uterine, parametrial, peritoneal, sepsis, endocardial) o Most bacteria causing septic abortion are part of the normal vaginal flora | & o Particularly worrisome are severe necrotizing infections and toxic shock syndrome caused by group A streptococcus (S. pyogenes) | & 1. Clinical presentation and diagnosis • (+) post-abortal fever, foul smelling discharge/bleeding • Cervix dilated; (+) uterine and/or adnexal tenderness • Ancillary: TVS, CBC, C/S 2. Management o Curettage, if there are retained products of conception o Broad-spectrum IV antibiotics o Intensive care, if necessary (septic shock) 3. Prophylaxis o Doxycycline, 100mg 1 hour prior to evacuation; 200 mg post evacuation § Doxcycline is used because it covers Chlamydia | G 4 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE II. ECTOPIC PREGNANCY • Implantation of the blastocyst in areas other than the endometrial lining • Sites: o Tubal (fimbrial, ampullary, isthmic, interstitial) – 95% § Ampulla (70%) is the most frequent site § Followed by isthmic (12%), fimbrial (11%), and interstitial tubal pregnancy (2%) | & o Abdominal o Intraligamentous o Ovarian o Cervical o Cesarean Scar D. Clinical Manifestations • Classic triad o Missed menses o Pain (sharp, stabbing, or tearing) | & o MINIMAL vaginal bleeding or spotting • (±) Passage of decidual cast o Sloughed endometrium that takes the shape of the endometrial cavity | & 1. Unruptured Ectopic Pregnancy o Uterus slightly enlarged due to hormonal stimulation o Adnexal mass o Tenderness on palpation of the lower abdomen and adnexa o Cervical motion tenderness 2. Ruptured Ectopic Pregnancy o Severe lower abdominal pain o Direct/rebound tenderness, board-like rigidity all point to an acute abdomen secondary to a tubal rupture | G o On PE: Figure 3 | Sites of ectopic pregnancy Generalized tenderness on palpation of the abdomen Cervical motion tenderness (“wiggling tenderness”) Bulging cul de sac (because of hemoperitoneum) Pain in the neck or shoulder, especially on inspiration (indicates diaphragmatic irritation secondary to sizable hemoperitoneum) § Hypotension, tachycardia and pallor may present only when hypovolemia becomes significant § § § § A. Heterotropic Pregnancy • A multifetal pregnancy composed of one conceptus with normal uterine implantation coexisting with one implanted ectopically B. Risk Factors • • • • • • Prior tubal surgery - greatest risk factor! | G Tubal infection (PID/STD) Salpingitis Previous tubal pregnancy Peritubal adhesions (appendicitis, endometriosis) Smoking (has an effect that reduces the peristaltic movement of the fallopian tubes, slowing down the travel of the fertilized egg to the uterus) | G • Infertility and ART use • Salpingitis isthmica nodosa - epithelium-lined diverticula extend into a hypertrophied muscularis layer | & • Congenital fallopian tube anomalies, secondary to in utero diethylstilbestrol exposure | & E. Differential Diagnosis for Abdominal Pain in Pregnancy UTERINE • • • • Miscarriage Abortion Infection Enlarging or degenerating myoma [leiomyomas] • Molar pregnancy • Round-ligament pain ADNEXAL • Ectopic pregnancy • Complicated ovarian mass (ruptured, torsed, hemorrhagic) NON-GYNE • • • • Appendicitis Cystitis Gastroenteritis Urolithiasis C. Outcomes • Tubal Rupture o Early rupture – isthmic (narrowest portion) | G o Late rupture – interstitial | G • Tubal Abortion o Common in fimbrial and ampullary tubal pregnancies o According to Dra. Mallen, this type may subside on its own o Uncommonly, an aborted fetus will implant on a peritoneal surface and become an abdominal pregnancy | & • Pregnancy Failure with Resolution 5 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE F. Diagnosis • Clinical findings • CBC o For ruptured ectopic pregnancy, Hgb and Hct levels do not usually reflect the hemodynamic status of the patient until after several hours later • TVS • B-hCG if TVS results are nonconclusive • Laparoscopy Figure 5 | Ring of fire 1. Interpreting B-hCG levels o Discriminatory zone – 1500 mIU/mL § ABOVE the discriminatory zone * Plus failure to visualize an intrauterine pregnancy on ultrasound = ECTOPIC pregnancy (or a non-viable pregnancy) § BELOW the discriminatory zone * Do serial B-hCG determinations (every 2 days) * If values double every 2 days: live intrauterine pregnancy * If values decrease according to anticipated patterns: failing intrauterine pregnancy * Otherwise, it is ectopic pregnancy G. Threatened Abortion vs Ectopic Pregnancy • Both may present with missed menses, pain and vaginal bleeding • PROMPT diagnosis of ectopic pregnancy is of utmost importance • Means of ascertaining an INTRAUTERINE pregnancy: o TVS: demonstration of intrauterine gestational sac rules out ectopic pregnancy o Serial B-hCG: doubling time every 48 hours o Serum progesterone level § < 5 ng/mL: dying pregnancy/ectopic pregnancy § > 20 ng/mL: healthy pregnancy • TVS o Gestational sac 4.5 weeks B-hCG 1500-2000 mIU/mL o Yolk sac 5.5 weeks 10mm GS diameter o Embryo 5-6 weeks embryonic length 1-2mm o Fetal ❤ activity 6-6.5 weeks embryonic length 1-5mm MSD 13-18mm H. Dead fetus Figure 4 | Expected rate of decline in B-hCG levels for failing pregnancies 2. TVS Findings in Ectopic Pregnancy a. Endometrial findings o Thickened endometrium, usually trilaminar o Decidual cyst o Pseudogestational sac b. Adnexal findings o Visualization of an inhomogenous complex adnexal mass separate from the ovary; or an extrauterine gestational sac/yolk sac with or without an embryo o With Doppler imaging, “ring of fire” is demonstrated (representing placental blood flow at the periphery of the mass) | G c. Cul de sac o Anechoic or hypoechoic fluid in the cul de sac may signify hemoperitoneum (as little as 50ml can be detected by TVS) • No embryo within a sac with a mean sac diameter (MSD) of 16-20mm (>20mm) • No cardiac activity in a 5-mm embryo (>10mm) • Be wary of a pseudogestional sac which may be seen in ectopic pregnancies o Intrauterine fluid accumulation (possibly blood) I. Medical Management • Methotrexate (folic acid antagonist) | G • For UNRUPTURED ectopic pregnancy | G • Patient should be asymptomatic, compliant, motivated 1. Criteria for patient selection | o Initial B-hCG level < 1000 mIU/mL § Single best prognostic indicator of successful treatment with single-dose MTX | & o Ectopic mass size < 3.5cm o Absent fetal cardiac activity (for ethical reasons) o Rationale: The larger the size or the higher is the hCG level, the longer it may take for treatment to be successful. That’s why a low hCG and a size of <3.5 cm is preferred. | ! 3. Culdocentesis o Has been largely replaced by TVS o Used to diagnose presence of hemoperitoneum o Fragments of old clots or non-clotting blood indicate a hemoperitoneum 6 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE J. Surgical Management • Either via Laparoscopy or Laparotomy o Laparoscopy is the preferred surgical treatment for ectopic pregnancy unless the patient is hemodynamically unstable | & 1. Salpingostomy § Size < 2cm * Preserving that portion of the tube if the size is > 2 cm will only predispose the woman to future ectopic pregnancies! | G § Location: distal third of the fallopian tube § Linear incision made on the antimesenteric border, contents evacuated, and incision is left unsutured to heal by secondary intention | G 2. Salpingotomy § Same as salpingostomy except that the incision is closed by suturing 3. Salpingectomy § For ruptured and unruptured cases * Primarily for ruptured ectopic pregnancies | G § Entire length of the affected tube is removed § Complete excision to minimize recurrence of pregnancy in the tubal stump SALPINGECTOMY • Ruptured • Live ectopic, even if unruptured SALPINGOTOMY/ SALPINGOSTOMY • Unruptured • Distal third of FT • < 2 cm size LAPAROSCOPY • Unruptured 7 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE III. GESTATIONAL TROPHOBLASTIC DISEASE A. Classification 1. Hydatidiform mole (+) villi F. Clinical Manifestations • Missed menses, irregular bleeding, passage of grape-like molar tissues o Complete mole o Partial mole o Invasive mole (GTN) 2. Non-molar trophoblastic neoplasm (-) villi o Choriocarcinoma (GTN) o Placental site trophoblastic tumor (GTN) o Epithelioid trophoblastic tumor (GTN) • Hydatidiform moles: excessively edematous immature placentas | & • Invasive mole: deemed malignant due to marked penetration and destruction of the myometrium and its ability to metastasize | & • Histological confirmation is not used to diagnose and treat GTNs. Instead, measurement of serum hCG levels combined with clinical findings are utilized. They are effectively treated as a group. | & B. Strongest Risk Factors • Both extremes of reproductive age o Adolescents o Women >40 (10-fold risk) • History of molar pregnancy C. Racial Predilection • Asians, Hispanics, American Indians D. Epidemiology and Risk factors | • Adolescents, and women aged 36-40 y/o → two-fold risk • > 40 y/o → almost 10x risk E. Partial vs Complete Mole • One difference is that in a PARTIAL mole, there may still be some embryonal tissue, hence may show fetal heart tones on UTZ | G Figure 6 | Grape-like appearance • Symptoms tend to be more pronounced with complete mole than partial moles | G& o High hCG levels account for possible HPN and tachycardia (because of the thyrotropin like effects of HCG) | G • Complete mole o Uterus soft/boggy consistency; usually larger than dates o No FHT appreciated o Cystic ovarian masses may be palpated (theca-lutein cysts) o Medical complications include thyrotoxicosis, early-onset pre-eclampsia, hyperemesis o Complete moles have a greater chance to develop into a malignancy | G G. Diagnosis • Clinical findings • B-hCG o High values can lead to erroneous false-negative urine pregnancy test results, termed a “hook effect,” wherein excessive b-hCG hormone levels oversaturate the assay’s targeting antibody and create a falsely low reading (this is especially true for complete moles) | & • Sonography • Histopathology H. Sonography • Mainstay of trophoblastic disease diagnosis • Complete mole o Echogenic uterine masses with numerous anechoic cystic spaces (“snowstorm appearance”) | G o NO fetus or amniotic sac • Partial mole o Thickened multi-cystic placenta along with a fetus or fetal tissue | G • Most common mimics: incomplete or missed abortion | & • Molar pregnancy may be confused for a multifetal pregnancy or uterine leiomyoma w/ cystic degeneration | & Figure 7| L: Sagittal view of complete hydatidiform mole, with ‘snowstorm’ appearance; R: Partial hydatidiform mole 8 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE I. Pathology | & • Surveillance for subsequent neoplasia following molar pregnancy is crucial • Before 10 weeks, villi may still not be enlarged • Molar stroma may not yet be edematous and avascular • Immunohistochemical staining for p57 expression enhances histopathological evaluation • p57(KIP2): nuclear protein whose gene is paternally imprinted and maternally expressed • Strongly expressed in normal placentas, pregnancy losses with hydropic degeneration, and partial hydatidiform moles (the three can be distinguished by molecular genotyping) • Complete moles: contain only paternal genes; does not take up the stain J. Management | • Preoperative evaluation attempts to identify known potential complications such as: o Preeclampsia, o hyperthyroidism, o anemia, o electrolyte depletions from hyperemesis, and o Metastatic disease • Chest radiography: most recommended K. Molar Pregnancy Termination 1. Evacuation of uterine contents by suction curettage o Preferred treatment since it’s faster | G o Cervix must be dilated to accommodate the suction curette (hygroscopic dilator/laminaria is frequently used) (typically 10-14mm diameter) o As evacuation is begun, oxytocin is infused to limit bleeding o If bleeding continues, other uterotonic agents are given (methylergonovine, misoprostol) | & 2. Hysterectomy with ovarian preservation o For women > 40 (completed childbearing) § The ovaries are preserved to prevent unwanted effects of “surgical menopause” due to low estrogen levels (eg. cardiovascular diseases, osteoporosis) | G o Theca-lutein cysts seen at the time of hysterectomy do not require removal; they spontaneously regress following molar termination 3. Post-evacuation surveillance for GTN (serial B-hCG) o Post-evacuation prophylactic chemotherapy to prevent persistent GTD is NOT recommended o Initial B-hCG within 48 hrs after evacuation as baseline for further tests o Subsequent determinations done at 1-2 week intervals until b-hCG levels are undetected § After 7 weeks for PARTIAL moles § After 9 weeks for COMPLETE moles o Monthly B-hCG for 6 months thereafter o Prevent new pregnancy during this period. It will interfere with B-hCG monitoring • If a woman has not become pregnant but B-hCG levels increase or remain persistently plateaued at high levels, this signify increasing trophoblastic proliferation that is most likely malignant. | & • L. Gestational Trophoblastic Neoplasia • Aka Malignant GTD or Persistent GTD • Follows o H moles in 50% o Abortion or ectopic pregnancy in 25% o Term or preterm pregnancy in 25% • Invades the myometrium; metastasizes 1. Risk Factors for GTN o Prior Complete mole § Hydatidiform mole > Ectopic > Term/Preterm pregnancy o Older age o B-hCG > 100,000 mIU/mL o Theca-lutein cysts >6 cm o Slow decline in b-hCG 2. Examples of GTN a. Invasive mole § Most common GTN that follows an H-mole | G § Characterized by extensive tissue invasion trophoblast and whole villi | & § Locally aggressive but less prone to metastasize by b. Gestational Choriocarcinoma § Most common GTN that follows an abortion or a term pregnancy | G § Contains no villi § Most common sites of metastasis: vagina, lungs § Metastases often develop early and generally bloodborne | & c. Placenta site trophoblastic tumor § Associated with only moderately elevated B-hCG § Preferred treatment is hysterectomy because tumor is usually resistant to chemotherapy | & d. Epithelioid trophoblastic tumor § Main site: uterus § Typical findings: low hCG levels and bleeding | & 3. Clinical Findings o Irregular bleeding (continuous or intermittent) associated with uterine subinvolution o May present with massive intraperitoneal hemorrhage following myometrial perforation from trophoblastic growth 4. Diagnosis o Plateau of serum B-hCG level (+10%) for four measurements during a period of 3 weeks or longer – days 1,7,14,21 o Rise of serum b-hCG level > 10% during 3 weekly consecutive measurements or longer, during a period of 2 weeks or more days 1,7,14 o Serum B-hCG level remains detectable for 6 months or more o Histological criteria for choriocarcinoma o It is stressed that diagnosis is usually made by persistently elevated serum B-hCG levels without confirmation of tissue study | & o Additional laboratory procedures ff diagnosis of GTN: § CBC, SGPT, SGOT, BUN, Crea § TVS § CXR or Chest CT § Cranial CT or MRI § Abdominal CT 9 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE 5. Treatment N. Modified WHO Prognostic Scoring System a. Chemotherapy § Single-agent * Methotrexate or Actinomycin-D * For low-risk, non-metastatic neoplasia § Multi-agent * EMA-CO (Etoposide, Methotrexate, Actinomycin-D, Cyclophosphamide, Oncovicin/Vincristine) * For high-risk disease b. Hysterectomy * For PSTT and ETT, which are generally resistant to chemotherapy o Serosurveillance should be done for 1 year following undetectable B-hCG levels o Women who have completed GTN chemotherapy are advised to delay pregnancy for 12 months | & M. FIGO Staging for GTN o FIGO=International Federation of Gynecology and Obstetrics STAGE STAGE 1 STAGE 2 STAGE 3 STAGE 4 DESCRIPTION Disease confined to the uterus GTN extends outside of the uterus but is limited to the genital structures (adnexa, vagina, broad ligament) GTN extends to the lungs, with or without known genital tract involvement All other metastatic sites SCORES Age Antecedent pregnancy Interval after index pregnancy (mo.) Pretreatment serum b-hCG (mIU/mL) Largest tumor size incl. uterus Size of metastases Number of metastases Previously failed chemotherapy drugs STAGE 1 0 <40 1 > 40 2 - 4 - Mole Abortion Term - <4 4-6 7-12 >12 <103 103 – 104 104– 105 > 105 <3cm 3-4cm >5cm - - Spleen, kidney GI Liver, brain - 1-4 5-8 >8 - 1 >2 Disease confined to the uterus GTN extends outside of the uterus but is limited STAGE 2 to the genital structures (adnexa, vagina, broad ligament) GTN extends to the lungs, with or without known STAGE 3 genital tract involvement STAGE 4 All other metastatic sites • LOW RISK = WHO score of 0-6 • HIGH RISK = WHO score of >7 10 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE POSTPARTUM HEMORRHAGE O. HIGH YIELD SUMMARY TYPE CLINICAL PRESENTATION PE FINDINGS Threatened Vaginal bleeding with or without hypogastric pain “Spotting” Closed cervix Uterus enlarged to AOG Inevitable Incomplete Complete Missed Septic Unruptured ectopic Ruptured ectopic Molar Gross rupture of membranes No passage of products of conception History of watery vaginal discharge Passage of meaty tissues Vaginal bleeding Hypogastric pain Passage of “meaty” tissues Vaginal bleeding Hypogastric pain No passage of “meaty” tissues +/- Vaginal bleeding +/- Hypogastric pain May symptoms then nawala | ! Fever Foul vaginal discharge History of instrumentation Stable BP Wiggling tenderness Lower abdomen & adnexal tenderness Hypotension (hypovolemia) Wiggling tenderness Generalized tenderness Passage of “grape-like” tissues Dilated cervix Uterus enlarged to AOG Dilated cervix Uterus smaller to AOG Closed cervix Uterus normal-sized Closed cervix Uterus enlarged to AOG or smaller than AOG ULTRASOUND FINDINGS Live, intrauterine pregnancy (fetal pole, gestational sac within the endometrial cavity) Subchorionic hemorrhage Live, intrauterine pregnancy Products of conception/ Placental tissues still seen within the endometrial cavity Minimally-thickened endometrial lining without gestational sac Dead fetus within the endometrial cavity MANAGEMENT Bed rest Expectant management → Curettage Antibiotic coverage Completion curettage Reassurance Dilatation and curettage Curettage, IV antibiotics, Intensive care Doxy prophylaxis Methotrexate or Laparoscopy or Salpingostomy or Salpingotomy Dilated cervix Uterine and/or adnexal tenderness - Closed cervix Uterus slightly enlarged Adnexal mass Pseudogestional sac “Ring of fire” Fluid in the culdesac (hemoperitoneum) - Salpingectomy “Snowstorm” appearance, no fetus (complete) Suction curettage or Hysterectomy with ovarian preservation for >40 y/o Uterus enlarged, soft/boggy Thickened multicystic placenta with fetus (incomplete) - END - REFERENCES • PPT from Dra. Mallen • Williams 25th ed 11 CONTRERAS • CORPUZ | CID • CLAVIO • CO • CO • CORRALES • CORTEZ • COSARE