A&P 2 lecture 1
advertisement

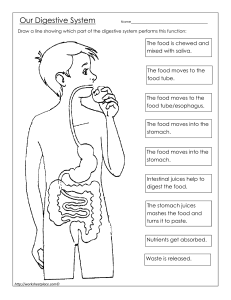
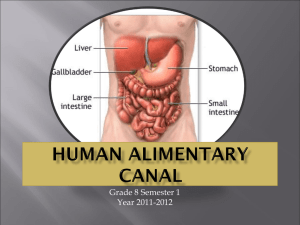
BSC2086 LECTURE 1 THE DIGESTIVE SYSTEM Hernan Aviles Main topics • General anatomy and digestive processes • Mouth through esophagus • Stomach • Liver, gallbladder and pancreas • Small intestine • Chemical digestion and absorption • Large intestine 1 Overview • nutrients that we eat must be broken into smaller components (amino acids, sugars) • proteins such as myosin (beef) and others can not be absorbed and incorporated into your muscles, it must be broken down into amino acids before it can be used to make human proteins • digestive system is a disassembly line that breaks food into molecules that can be used by the body, it also absorbs and distribute those molecules to tissues • Gastroenterology: study of digestive system and its disorders 2 Digestive Functions • ingestion: intake of food • digestion: breakdown – mechanical (teeth, contractions): physical breakdown (cutting, grinding) that expose more food to digestive enzymes – chemical (enzymes from saliva, stomach, pancreas, intestines ): break macromolecules into their monomers (poly into monosaccharides, proteins into amino acids, fats into glycerol and fatty acids • absorption: uptake nutrients into blood/lymph • defecation: elimination of undigested material 3 Anatomy of the Digestive System • two subdivisions and is open in both ends – most material like feces never go inside the body • digestive tract: 30 foot long tube extending from mouth to anus – mouth, esophagus, stomach, small and large intestines – gastrointestinal (GI) tract: stomach and intestines • accessory organs: teeth, tongue, liver, gallbladder, pancreas, salivary glands 4 Tissue Layers of GI Tract • mucosa: epithelium (simple columnar in all GI except in mouth, esophagus and anus that have stratified squamous), lamina propria, muscularis mucosae) • submucosa • muscularis externa: inner circular layer, outer longitudinal layer • adventitia or serosa: areolar tissue or mesothelium 5 Enteric Nervous Control • regulates moltility, secretion and blood flow • function independently of CNS, two nerve networks – submucosal plexus • glandular secretion of mucosa & contractions of muscularis mucosae – myenteric plexus • peristalsis & contractions of muscularis externa 6 Relationship to Peritoneum • organs are covered by peritoneum, because of contractions, organs need freedom to move (suspended by sheets of connective tissue called mesenteries) • dorsal mesentery suspends GI tract and forms serosa (visceral peritoneum) of stomach and intestines • ventral mesentery forms lesser and greater omentum (contains lymph nodes, lymphatic vessels, blood vessels) • duodenum, pancreas and parts of large intestine are retroperitoneal 7 Lesser and Greater Omentum • Lesser: attaches stomach to liver • Greater: covers small intestines like an apron, extends from greater curvature of stomach to transverse colon 8 Mesentery and Mesocolon • Mesentery of small intestines holds many blood vessels • Mesocolon anchors colon to posterior body wall 9 Regulation of Digestive Tract • digestive processes such as motility (contractions that break up food, mix it with enzymes and move it along), secretion, membrane transport (absorption of nutrients) are controlled by 3 mechanisms • neural control: short myenteric (swallowing) & long vagovagal reflexes (motility and secretion) • hormones (gastrin, secretin): messengers diffuse into bloodstream, distant targets • paracrine secretions (histamine, protaglandins): messengers diffuse to nearby target cells 10 Features of Oral Cavity • cheeks and lips: keep food between teeth for chewing; essential for speech and suckling in infants – vestibule: space between teeth and cheeks – lips: cutaneous (mustache) and red area or vermilion (lipstick) • tongue is sensitive, muscular manipulator of food – papillae and taste buds on dorsal surface (vallate, foliate, filiform, fungiform) – lingual glands secrete saliva, tonsils in root • hard and soft palate: allow breathing and chewing at same time – palatoglossal and palatopharyngeal arches 11 The teeth (Dentition) • Baby or milk or deciduous teeth erupt from 6-30 months and by 2 years (20); Adult or permanent (32) between 6 and 25 years, third molars (wisdom) erupt 17-25 years, because of evolution, jaws become shorter (no space for them, become impacted) – incisors: cutting teeth – canines: puncture and shred food – premolars and molars: crushing and grinding • oclussion: meeting of teeth when mouth closes • cusps: rounded bumps located in the occlusal surfaces (premolars have 2, bicuspids; molars have 4-5 cusps) 12 Tooth Structure • each tooth anchors into a cavity alveolus • periodontal ligament anchors teeth into alveolus • dentin: tissue of teeth (material) – cementum covers root and neck – enamel covers crown – damaged dentin and cementum can regenerate, enamel does not • root canal leads into pulp cavity – nerves and blood vessels • gingiva or gum covers the alveolar bone – crown: above the gum; root: below the gum and neck: place where crown, root and gum meet – gingival sulcus: space between tooth and gum 13 Tooth & gum disease, mastication or chewing • mouth has ~700 species (bacteria), bacteria and sugars form plaque, if not removed bacteria acts on sugars to produce lactic acid (dissolve minerals and form cavities) • If penetrate the pulp cavity (either remove or root canal therapy to remove pulp and replace with inert material) • periodontal disease (~90% of tooth loss): plaque calcifies (tartar) which separates tooth and gum followed by bacterial infection • mastication: breaks food into smaller pieces to be swallowed – ↑ surface area exposed to digestive enzymes – contact of food with sensory receptors triggers chewing reflex – tongue, buccinator and orbicularis oris manipulate food – masseter and temporalis elevate the teeth to crush food – medial and lateral pterygoids swing teeth in side-to-side (grinding action of molars) 14 Saliva and Salivary Glands • functions: moisten, begins starch and fat digestion, cleanse teeth, inhibit bacteria, bind food together into bolus, pH 6.8 to 7.0 • components: 97-99.5% water and solutes such as amylase (starch digestion); lipase (digests fat, activated by stomach acid); mucus (aids in swallowing); lysozyme (kills bacteria); immunoglobulin A (inhibits bacterial growth); electrolytes such as Na+, K+, Cl-, phosphate and bicarbonate • salivary glands: (intrinsic and extrinsic) – intrinsic: small glands (lingual, tongue; labial, lips; buccal, cheeks), small amounts of saliva – extrinsic: 3 pairs connected to oral cavity by ducts • parotid: anterior to earlobe, duct empties in the upper second molar (mumps, virus) • submandibular: duct empties close to the lower incisors • sublingual: floor of the mouth, multiple ducts empty posterior to submandibular duct 15 Salivation • total of 1 to 1.5 L of saliva per day • cells filter water from blood and add other substances (amylase, mucin, lysozyme) • food stimulates receptors in mouth that signal salivatory nuclei in medulla and pons, nuclei send signals to glands using facial and glossopharyngeal nerves – parasympathetic stimulation → salivary glands produce thin saliva, rich in enzymes – sympathetic stimulation → produce less abundant, thicker saliva, with more mucus – stress and dehydration reduce salivation • higher brain centers also stimulate salivatory nuclei so sight, smell and thought of food cause salivation 16 Pharynx • skeletal muscle – deep layer: longitudinal – superficial layer: circular • superior, middle and inferior pharyngeal constrictors • inferior constrictor (upper esophageal sphincter) remains closed when not swallowing, it is physiological sphincter (disappears in dead people) 17 Esophagus • muscular tube of 25-30 cm long – skeletal muscle in upper part, mixed in the middle and smooth in bottom – nonkeratinized stratified squamous epithelium – glands in submucosa • extends from pharynx, passes through esophageal hiatus in diaphragm and finishes in stomach (cardiac sphincter) • upper sphincter (inferior pharyngeal constrictor) excludes air from esophagus • lower sphincter closes orifice helping diaphragm to avoid reflux • heartburn: nothing to do with heart (acid reflux) 18 Esophagus 19 Swallowing (Deglutition) • series of muscular contractions (22 muscles) coordinated by the swallowing center (medulla and pons), center send signals using cranial nerves V, VII, IX and XII • buccal phase: tongue collects food, presses it against palate (bolus) and pushes it back into oropharynx • pharyngeal-esophageal phase: 3 actions avoid food going to mouth, nose or larynx – tongue (blocks mouth), soft palate rises (blocks nasopharynx), infrahyoid muscles lift larynx; epiglottis folds back (block larynx) – pharyngeal constrictors push bolus down and triggers peristalsis (wave of contractions that pushes bolus ahead of it) – food uses gravity to swallow when standing, peristalsis can swallow in any position, liquids 1-2 sec, bolus 4-8 sec – lower esophageal sphincter relaxes to let food pass into stomach 20 Swallowing 21 Stomach • food storage, empty: 50 mL, after meal: 1-1.5 L, extremely full: 4 L • mechanically breaks up food, liquefies it and begins chemical digestion of protein and fat resulting in a soupy or pasty mixture (chyme) • absorbs only small amount of nutrients, absorbs aspirin and some drugs • gross anatomy: curvatures: greater and lesser; regions: cardia (small area inside cardiac orifice); fundus (dome-shaped area on top); body (greatest part); pyloric region subdivided into antrum and pyloric canal, which finishes in the pylorus (narrow passage into duodenum); pylorus surrounded by a muscle (pyloric sphincter) Esophagus Pyloric Antrum Cardia Pyloric Canal Fundus Pyloric Orifice Body Duodenum 25-23 Stomach Esophag us Cardia Fundus Body Pylorus Duodenu m 23 Innervation and Circulation • innervation by parasympathetic (vagus); sympathetic fibers (celiac plexus) • blood is supplied by arterial branches of celiac trunk, used blood from stomach enters hepatic portal circulation and is filtered through liver before returning to heart 24 Unique Features of Stomach Wall & Cells • mucosa: simple columnar epithelium, pocked with depressions (gastric pits) • mucosa and submucosa (empty stomach) form wrinkles (rugae) • lamina propria: tubular glands • muscularis externa: 3 layers (outer longitudinal, middle circular and inner oblique) • 2 or 3 glands open in bottom of each gastric pit (cardiac, pyloric or gastric glands), cells of glands are: – mucous: secrete mucus – regenerative: divide fast, produce new cells that migrate to surface – parietal: HCl and intrinsic factor – chief (greater #): pepsinogen, and chymosin and lipase in infancy – enteroendocrine (G): hormones and paracrine messengers – cardiac and pyloric (mucus); gastric (acids & enzymes); both (hormones) 25 Gastric Secretions • 2 to 3L juice/day (H2O, HCl, pepsin) • HCl functions: activates enzymes, breaks up tissue, converts ferric (Fe3+) to ferrous ions (Fe2+) used for Hb synthesis, destroys bacteria and pathogens • HCl production: parietal cells contain carbonic anhydrase (CAH) CAH – CO2 + H2O → H2CO3 → HCO3- + H+ – H+ is pumped into stomach lumen by H+K+ ATPase, antiporter uses ATP to pump H+ out and K+ in – HCO3- goes to blood and is exchanged for Cl- (chloride shift), Clpumped out joins H+ forming HCl, ↑ HCO3- in blood causes blood pH ↑ (alkaline tide) • pepsin: protein digestion (partial), secreted by chief cells as pepsinogen (inactive), HCl converts it to pepsin (active) 27 Other Enzymes, Intrinsic Factor, Chemicals • gastric lipase and chymosin (infants’s chief cells), lipase digests butterfat of milk, chymosin curdles milk by coagulating proteins • intrinsic factor (parietal): essential for B12 absorption by small intestine; if not B12, Hb can not be produced (pernicious anemia) • chemical messengers (gastrin, serotonin, histamine, somatostatin): many produced by enteroendocrine (G) cells – hormones enter blood → distant cells – paracrine secretions → neighboring cells • gut-brain peptides: signaling molecules produced in digestive tract and CNS – substance P, vasoactive intestinal peptide (VIP), gastric inhibitory peptide (GIP), cholecystokinin, neuropeptide Y (NPY) 27 28 Gastric Motility & Vomiting • motility: swallowing center signals stomach to relax • food stretches stomach activating a receptive-relaxation response – resists stretching briefly, but relaxes to hold more food • soon, stomach shows a rhythm of peristalsis controlled by pacemaker cells in longitudinal muscle layer – gentle ripple of contraction happens every 20 seconds, churns and mixes food with gastric juice, after 30 mins it becomes strong – stronger contraction at pyloric region; ejects 3 ml of chyme at a time (this give time to duodenum to neutralize and digest nutrients) – typical meal emptied from stomach in 4 hours (less if liquid and ~ 6 hours if high in fat) • vomiting: excessive stretching of stomach, psychological stimuli, chemical irritants (alcohol, bacterial toxins), diaphragm and abdominal muscles and not stomach are involved – emetic center in medulla causes lower esophageal sphincter to relax while diaphragm and abdominal muscles are stimulated to contract • most digestion and nutrient absorption occur when chyme passes into small intestine (alcohol is absorbed in small intestine) 29 Healthy Mucosa and Peptic Ulcer • protection: living stomach is protected in 3 ways: thick mucus resists acids and enzymes, cell replacement every 3-6 days and tight junctions • peptic ulcer: breakdown of protection can lead to inflammation and ulcer (if untreated, ulcer can perforate organ causing bleeding or peritonitis) • causes: no evidence of stress, many involve Helicobacter pylori, other risk factors are smoking and nonsteroidal anti-inflammatory drugs (aspirin), they block prostaglandin production (mucus and bicarbonate) • treatment: cimetidine (tagamet) which reduces acid secretion (20-30% success) • it is an H2 receptor blocker, histamine stimulates acid secretion in parietal cells by binding to H2 receptors • lately, antibiotics against H. pylori + Pepto-Bismol (90% success) 30 Regulation of Gastric Function • cephalic phase: sight, smell, taste or thought of food; vagus stimulates secretion and motility • gastric phase: food or semidigested protein activate gastric activity by stretch and ↑ in pH – stretch: activates short (myoenteric) and long reflexes (vagus) – secretion is stimulated by ACh (parasympathetic from both, short and long), histamine (enteroendocrine cells) and gastrin (pyloric G cells) – 3 have receptors on parietal (HCl & intrinsic factor) and chief cells (pepsinogen, mucus) 31 Regulation of Gastric Function • intestinal phase: duodenum regulates gastric activity through hormones and nervous reflexes – at first gastric activity increases (if duodenum is stretched or amino acids in chyme cause gastrin release) – enterogastric reflex: duodenum inhibits activity • caused by acid and semi-digested fats in duodenum – chyme stimulates duodenal cells to release secretin, cholecystokinin (CCK) and gastric inhibitory peptide (GIP) • all 3 suppress gastric secretion and motility • gastrin decreases, pyloric sphincter contracts (no more food passes) 32 Regulation of Gastric Secretion 33 Positive Feedback Control- Gastric Secretion 34