Children's Hospital and Regional Medical Center
(Clinical Policy/Procedure: C )
Critical Test Result/Value Reporting Requiring Read-Back
POLICY:
Critical results reported verbally or by telephone will be read back to the person
reporting the results, thus providing verification of the test result heard. These
results will be reported immediately. Audit documentation will support that the
communication has occurred within one hour of confirmation.
PURPOSE:
To promote accurate and timely communication of critical test results.
PROCEDURE:
I.
Definition of Critical Test Result/Value:
A.
II.
A critical test result/value is one that deviates from defined medical and analytic
criteria and which has not been present on an immediate preceding examination
and whose value reflects a potential life threatening situation and may necessitate
an urgent response.
Communicating Critical Test Results/Values:
A.
B.
C.
D.
Critical test results will be verbally provided to a licensed care provider responsible
for the care of the patient whose result is being reported. To verify accurate
transfer of verbal information, staff reporting a critical test result(s) will first
confirm the care provider / patient assignment, and then ask the patient’s care
provider to write down and read back the patient’s name, medical record number
and test result. The reporting staff will use the following script:
I have a critical result to report. You will need to write down and read the
information back to me to verify accuracy.
Any person receiving a critical test result will write down and read back for
verification.
The receiver of the critical test information will communicate the result as
appropriate to the responsible provider or follow an existing guideline of care for
action.
To ensure timely communication of critical test results/values, the following
escalation will occur in rapid succession if initial contact is not available:
1.
Inpatients: Patient’s Nurse → Charge Nurse → Responsible House Staff
Officer → Patient’s Attending Physician or covering physician
2.
Outpatient (Children’s Clinics): Patient’s Clinic Nurse → If no nurse or
after hours, patient’s Attending Physician or covering physician
3.
Community Outpatient: Patient’s Community Provider or covering
physician
4.
Children’s Emergency Department Patient: Patient’s Nurse → E.D.
Communication Specialist Nurse → E.D. Attending Physician
5.
In all cases, failure to reach a responsible house officer, attending physician
or community physician will lead to contact with the pediatric chief
resident. Failure to reach the pediatric chief resident will lead to contact
with the Medical Director or designee.
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
Children’s Hospital and Regional Medical Center
All Rights Reserved
© 2006
Page 2: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
E.
III.
Note: The most common practice is to report critical Radiology or
Cardiology findings directly to the Ordering/Attending Physician/Provider.
When that provider is unavailable, the reporting provider would follow the
reporting department escalation process as outlined to expedite
communication of the critical result to another provider associated with the
patient’s care.
In highly emergent cases where read-back would be impractical or impede patient
care, repeat-back is allowable. In this situation, the write down step may be
eliminated.
Department Specific Critical Test Results:
A.
B.
C.
D.
APPENDIX I:
APPENDIX II:
APPENDIX III:
APPENDIX IV:
Radiology
Laboratory
Cardiology
EEG
Originated by: Jennifer Abermanis, M.S., Administrator, Clinical Systems and Logistics
Reviewed by:
John Salyer, RRT, MBA, Director Respiratory Care
QI Coaches
National Patient Safety Goal #2 Workgroup (Jennifer Abermanis, Chair)
Revised by:
Approved by Medical Executive Committee: 2/05
APPROVED BY:
Richard Molteni, MD
Vice President & Medical Director
ORIGINATED:
REVIEWED:
REVISED:
Susan Heath, RN, MN
Nurse Executive
2/05
6/06
Additional Key Words: Patient Safety, Patient Safety Goal, Sentinel Event, Radiology
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
©
Page 3: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
APPENDIX I: Radiology
I.
Specific Critical Read-Back Findings:
A.
Central nervous system:
1.
Brain herniation or impending herniation.
2.
Acute ventricular dilation.
3.
Unsuspected intracranial hemorrhage, infarction or edema.
4.
Spinal cord transection or compression.
B.
Chest:
1.
Pneumothorax.
2.
Pneumopericardium.
3.
Unsuspected airway or esophageal foreign body.
4.
Tracheal narrowing of greater than 50%.
5.
Aortic rupture and/or dissection.
C.
Abdomen:
1.
Pneumoperitoneum.
2.
Pneumatosis.
3.
Portal venous gas.
D.
Musculoskeletal system:
1.
Gas in soft tissues.
2.
Signs of child abuse.
(Approved 02/05; Revised 06/06)
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
Page 4: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
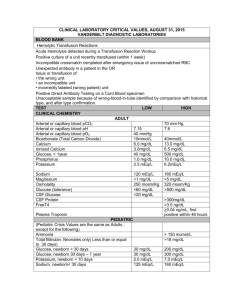
APPENDIX II: Laboratory
Hematology Critical Values:
Platelet Count
WBC
HCT
Low
< 30,000/CMM
< 1000/CMM
15%
Coagulation Critical Values:
PT
INR
PTT
Fibrinogen
> 30 sec
> 2.8
> 120 sec
< 50 mg/dL
High
> 1,000,000/CMM
> 50,000/CMM
68%
Chemistry Critical Values:
Sodium
Potassium
< 2 days
> 2 days
Chloride
CO2
Phosphorus
Serum Osmolality
Glucose
Newborn (0 – 1 month)
Infant (I month) - Adult
Calcium
Low
115 meq/L
High
160 meq/L
≤ 3.0 meq/L
≤ 3.0 meq/L
70 meq/L
10 meq/L
1.0 mg/dL
< 265 mOsm/kg
≥ 6.5 meq/L
≥ 6.0 meq/L
130 meq/L
40 meq/L
12 mg/dL
> 320 mOsm/kg
<40 mg/dL
<50 mg/dL
6 mg/dL
> 300 mg/dL
> 700 mg/dL
14 mg/dL
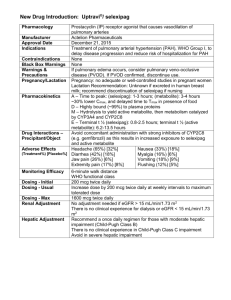
Ionized Calcium
Bilirubin
BUN
Magnesium
pH (blood)
pCO2
pO2
0 - 3 months
3 mo. - Adult
all ages
< 0.75mmol/L
1.75 mmol/L
20 mg/dL
100 mg/dL
> 5.0 mg/dL
> 7.60
> 70 mmHg
< 1.0 mg/dL
< 7.20
< 20 mmHg
< 30 arterial mmHg
< 50 arterial mmHg
< 30 capillary mmHg
< 20 venous mmHg
TSH
Birth – 3 days
3 days – 1 month
TDM Critical Values:
Amikacin
Caffeine
Carbamazepine
(Tegretol)
Chloramphenicol
25.0 uIU/mL
10.0 uIU/mL
High Result
> 35 mcg/mL
> 30 mcg/mL
> 13 mcg/mL
> 25 mcg/mL
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
Page 5: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
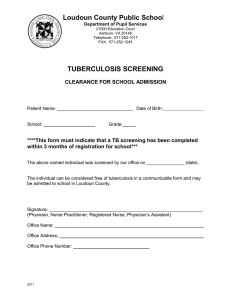
TDM Critical Values:
Cyclosporin A
Digoxin
Gentamicin
Lamictal
Lithium
Phenobarbitol
Phenytoin (Dilantin)
Salicylate
Theophylline
Tobramycin
Vancomycin
Zonisamide
High Result
> 600 ng/mL
> 2.5 ng/mL
> 12 mcg/L
>20 mcg/mL
> 2.0 mmol/L
> 50 mcg/mL
> 25 mcg/mL
> 40 mg/dL
> 25 mcg/mL
> 12 mcg/mL
> 50 mcg/mL
> 45mcg/mL
Microbiology:
Positive Blood and CSF Cultures and CSF gram stains will be called to the patient’s nurse, or
if unavailable, the charge nurse. The nurse is responsible for notifying the physician.
1. The first positive blood culture vial(s) of the day is to be given a telephone report. Any
subsequent positive vials showing the same organism from the same day or the same patient
(24-hour period) will be referred to the first reported vial with no additional telephone report.
2. Any new positive vial(s) of different date after 24-hour period of initial phoned report is to be
given an independent telephone report of the day regardless of organism identification.
3. Any new findings of a second organism different from the initial telephone report is to be
given an independent telephoned report immediately as soon as the difference is determined.
Reference Laboratory Results
Laboratory test results defined as critical (alert) by a Reference Laboratory will be called to the
care provider.
(Approved 02/05; Revised 06/06)
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
Page 6: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
APPENDIX III: Cardiology
I.
ECG / Holter:
A.
Ventricular fibrillation, Torsades de Pointe, bi-directional ventricular tachycardia,
severe 3rd degree AV block or long QTC or sinus node dysfunction or ventricular
tachycardia or wide QRS tachycardia.
II.
ECHO:
A.
Severe conditions of aortic, pulmonary and truncal valves, including aortic
insufficiency, aortic stenosis, dysplastic pulmonary valve, homograft
insufficiency or stenosis, pulmonary insufficiency or stenosis, truncal valve
stenosis.
B.
Severe conditions of the aortic, systemic artery, pulmonary and coronary
circulation, including absent pulmonary or coronary artery, left coronary from
pulmonary artery, A-P window, abnormal origin of coronary artery, coarctation of
aorta, interrupted aortic arch, myocardial ischemia/infarction, pulmonary embolus
or thrombosis, primary or secondary pulmonary hypertension, systemic A-V
malformation (large).
C.
Severe restrictive, dilated or hypertrophic cardiomyopathy.
D.
Pericardial effusion (large), pericarditis (acute, severe), cardiac tumor.
E.
Total anomalous pulmonary venous return (cardiac, infracardiac or supracardiac,
severe pulmonary vein stenosis or obstruction.
F.
Arrhythmogenic right ventricular dysplasia, hypoplastic ventricle, single
ventricle, severe ventricular dilation or dysfunction or hypertrophy.
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
Page 7: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
(Approved 02/05; Revised 06/06)
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved
Page 8: Clinical Policy/Procedure: Critical Test Result/Value Reporting Requiring Read-Back
APPENDIX IV: EEG
I.
Specific Critical Read-Back Findings:
A.
An electrographic seizure recorded on EEG, with or without clinical correlate, for
all inpatients and for outpatients not on anticonvulsant medication.
(Approved 02/05; Revised 06/06)
C:\Documents and Settings\shalse\Desktop\TEMP FILES\pdfs\Critical Test Results_Value Reporting_Read Back 153-04.doc (sh:jjcm)
© 2006 Children’s Hospital and Regional Medical Center
All Rights Reserved