here - Glaucoma Genetics Lab
advertisement

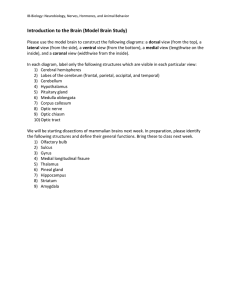
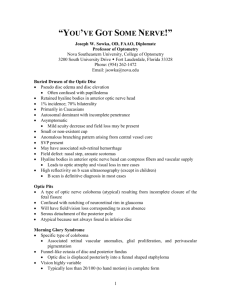
Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com BJO Online First, published on October 30, 2014 as 10.1136/bjophthalmol-2014-305722 Clinical science Enhanced depth imaging optical coherence tomography of congenital cavitary optic disc anomaly (CODA) Marion R Munk,1,2 Evica Simjanoski,1 John H Fingert,3 Lee M Jampol1 ▸ Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/ bjophthalmol-2014-305722). 1 Department of Ophthalmology, Northwestern University, Feinberg School of Medicine, Chicago, Illinois, USA 2 Department of Ophthalmology, Medical University of Vienna, Vienna, Austria 3 University of Iowa, Iowa City, Iowa, USA Correspondence to Dr Lee M Jampol, Department of Ophthalmology; Northwestern University, Feinberg School of Medicine, 645 N Michigan Avenue, Suite 440, Chicago IL 60611, USA; l-jampol@northwestern.edu Received 25 June 2014 Revised 22 September 2014 Accepted 9 October 2014 ABSTRACT Aim To report the finding of extension of the 4th hyper-reflective band and retinal tissue into the optic disc in patients with cavitary optic disc anomalies (CODAs). Methods In this observational study, 10 patients (18 eyes) with sporadic or autosomal dominant CODA were evaluated with enhanced depth imaging optical coherence tomography (EDI-OCT) and colour fundus images for the presence of 4th hyper-reflective band extension into the optic disc. Results Of 10 CODA patients (18 eyes), five patients (8 eyes) showed a definite 4th hyper-reflective band ( presumed retinal pigment epithelium (RPE)) extension into the optic disc. In these five patients (seven eyes), the inner retinal layers also extended with the 4th hyperreflective band into the optic disc. Best corrected visual acuity ranged from 20/20 to 20/200. In three patients (four eyes), retinal splitting/schisis was present and in two patients (two eyes), the macula was involved. In all cases, the 4th hyper-reflective band extended far beyond the termination of the choroid into the optic disc. The RPE extension was found either temporally or nasally in areas of optic nerve head excavation, most often adjacent to peripapillary pigment. Compared with eyes without RPE extension, eyes with RPE extension were more myopic (mean dioptres −0.9±2.6 vs −8.8±5, p=0.043). Conclusions The RPE usually stops near the optic nerve border separated by a border tissue. With CODA, extension of this hyper-reflective band and retinal tissue into the disc is possible and best evaluable using EDIOCT or analogous image modalities. Whether this is a finding specific for CODA, linked to specific gene loci or is also seen in patients with other optic disc abnormalities needs further evaluation. INTRODUCTION To cite: Munk MR, Simjanoski E, Fingert JH, et al. Br J Ophthalmol Published Online First: [please include Day Month Year] doi:10.1136/ bjophthalmol-2014-305722 Congenital cavitary optic disc anomalies (CODAs) is a term used to include various optic nerve defects ranging from large excavated discs to very subtle changes. This includes classic colobomas, optic pits, morning glory syndrome and other malformations.1 2 These malformations can be associated with visual-field defects, peripapillary pigmentary changes, retinal splitting/schisis and subretinal fluid (SRF).1 3 4 Classic colobomas result from a closure defect of the fetal fissure of the developing optic cup. Based on this pathogenesis, they are typically found inferotemporal and present as yellowish/greyish lesions.3 5 Optic pits are focal depressions in the optic nerve head (ONH).2 Histologically and with spectral domain optical coherence tomography (SD-OCT), herniation of dysplastic retina can be found.6–8 They are mostly located temporal in the ONH but also found centrally.2 Morning glory optic disc anomalies have a deeply excavated optic disc and cilioretinal vessels which radiate from the disk’s edge. It is a congenital funnel-shaped excavation of the posterior fundus that incorporates the optic disc.2 4 9 10 Previous studies using swept-source and enhanced depth imaging (EDI)-OCT have described the appearance of optic disc colobomas, optic pits and morning glory syndromes. Herniation of dysplastic retina, abnormal communication between subarachnoidal- and subretinal spaces as well as detection of lamina cribrosa torn off of peripapillary sclera at the site of the excavation have been reported.8 10 11 These previous studies did not note unusual retinal pigment epithelium (RPE) configurations. The aim of this study is to report EDI-OCT finding of the 4th hyper-reflective band and retina extending into the optic disc in patients with sporadic and hereditary CODA. METHODS Patient selection and setting This study enrolled 10 patients (18 eyes) diagnosed with hereditary or sporadic CODA. They were evaluated based on their characteristic ophthalmoscopic ONH appearance that may include absent or poorly defined central retinal arteries, an ONH with roundish, yellow/greyish depression with steep walls and varying degrees of peripapillary pigment. The disc may be grossly excavated with absence of rim tissue and marked saucerisation associated with abnormal peripapillary pigment.3 ONHs of each enrolled eye are shown in figure 1A. These 10 patients (18 eyes) were assessed for the presence of definite extension of the 4th hyper-reflective band into the disc on EDI-OCT (figure 1B). Characteristics of eyes with RPE extension were described and a potential difference between eyes with and without RPE extension with respect to refraction and the presence of schisis was evaluated. This study adhered to the Declaration of Helsinki, was IRB approved and all patients gave written informed consent. Study variable and scan protocol Medical history was obtained and examination consisted of best corrected visual acuity (BCVA), intraocular pressure (IOP)-measurement, slit-lamp examination and dilated fundus exam. Colour fundus photographs (Topcon, USA) of the macula and the ONH were taken plus serial horizontal Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 Copyright Article author (or their employer) 2014. Produced by BMJ Publishing Group Ltd under licence. 1 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Figure 1 (A) Exhibits the 10 patients (18 eyes) examined and diagnosed with cavitary optic disc anomalies. R=right eye, L=left eye. (B) Exhibits corresponding enhanced depth imaging optical coherence tomography scans of the optic nerve heads: Patient Nr. 1, 3, 6, 8 and 10 reveal no 4th hyper-reflective band extension. Patient Nr. 2, 4 and 5 show 4th hyper-reflective band extension in both eyes and Nr. 7 and 9 in the left eye. cross-sectional SD-OCT and EDI-OCTs of the macula and ONH (HRA+OCT Spectralis; Heidelberg Engineering, Germany). Validity and reliability of EDI-OCT to assess optic disc anomalies have been previously shown.11 The scan protocol included a horizontal 20×20 25-line macular SD-OCT (scan distance 244 mm) and a horizontal 31-line EDI-OCT 30×25 raster scan (scan distance 244 mm) centred foveally, ranging from the macula to the nasal edge of the optic disc, a horizontal 25-line EDI-OCT 30×25 raster scan centred over the optic disc (scan distance 244 mm) and a horizontal 73-line EDI-OCT 15×15 raster scan (scan distance 60 mm) centred over the ONH. Each scan had 10 OCT frames (average real time (ART) mode) averaged. Image quality was assessed immediately after image acquisition. If the image was of insufficient quality to evaluate morphology especially with respect to the hyperreflective bands and the optic disc margin, the image acquisitions were repeated. In order to overcome bad image quality due to media opacities, the number of ART frames was 2 increased. Poor compliance was addressed by decreasing the number of scans in the raster scans. The central macular SD-OCT scans were carefully evaluated for retinal splitting/ schisis and SRF. The ONH EDI-OCTs were evaluated for subtle and discrete retinal splitting/schisis near the optic disc and for the course of the RPE. In cases of RPE extension, the appearance of the RPE at the border of the ONH was evaluated in relation to border tissue, retinal layers and the choroid.12 13 As Bruch’s membrane was not differentiable from the RPE, we suspect that Bruch’s membrane corresponds to the visible RPE course. The scans were individually assessed by two of the coauthors (LMJ and MRM). Discrepancies were resolved by a consensus reading. In order to assess the reliability of this finding, an intraobserver agreement analysis was performed. Therefore, two datasets of identical single EDI-OCT cross-sections scans of the 10 CODA patients were graded for the presence/absence of RPE extension by an initially uninvolved clinician (KE). Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Figure 1 Continued In order to evaluate the location of the RPE extension and corresponding peripapillary changes in respective eyes, the infra red (IR) image of the EDI-OCT cross-section B-scan with the deepest RPE extension was superimposed on a colour picture of the ONH using imaging software (Gimp, http://www.gimp.org; eg, see figure 2A). Therefore, the respective singular EDI-OCT scan with the corresponding IR image was extracted for each eye (in TIFF) from Heidelberg Eye Explorer (V.5.7.4.0). Then, the IR image displaying the region and level of the single EDI-OCT cross-section scan by a green line (figure 2A) was cut out and the IR image was overlaid on the colour fundus image by using vessels for alignment and matching vessel landmarks manually. RESULTS Of the 10 patients (18 eyes), five patients (eight eyes, mean age 45±14 years) presented with definite extension of the 4th hyperreflective band into the disc visible on EDI-OCT (figure 1B). Thus, five patients (10 eyes) did not show RPE extension. Demographic and baseline characteristics of all enrolled CODA patients are given in table 1. OCTs of all ONH are shown in figure 1B. In the following, findings of the five patients (eight eyes) with RPE extension are summarised; in these patients, BCVA ranged from 20/20 to 20/200. Three patients (six eyes) had autosomal dominant (AD) CODA and belonged to the family previously reported.2 3 The four patients (seven eyes) with visual field assessment showed defects. Three patients (four eyes) had retinal splitting/schisis and two (two eyes) presented additionally with foveal SRF. In all cases, RPE (and possibly Bruch’s Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 membrane) extended far beyond the termination of the choroid into the optic disc. In four eyes, the RPE extension was most prominent nasally, in four temporally (figure 1B). The RPE extension was most often adjacent to highly pigmented areas along the disc margin (eg, see figure 2A). In five patients (seven eyes), apparent inner retinal tissue also extended together with the presumed RPE into the ONH (figure 1B, Nr. 2, 4, 5 and 9). One patient (one eye) showed a membrane traversing the cup and another eye revealed a hyper-reflective strand, presumable rudimentary retinal tissue which traversed the cup (figure 1B, Nr. 2). The intraobserver agreement for presence/absence of RPE extension was 92%. There was no association between schisis and the presence of RPE extension (Fisher’s exact test: p=0.145). Frequency distribution of RPE extension and schisis can be found in online supplementary table S1. Eyes with RPE extension were more myopic than eyes without RPE extension (mean dioptres −8.8±5 vs −0.9±2.6; Mann–Whitney U test p=0.043). EXEMPLARY CASES Case 1: Pt. Nr. 5 This highly myopic (SE −9 both eyes (OU)) 42-year-old Caucasian woman belongs to a family with AD CODA.2 3 14 This family was found to carry a gene mutation on chromosome 12 responsible for this abnormality.2 3 BCVA was 20/100 right eye (OD); 20/200-1 left eye (OS). Her vision OS has been poor since childhood. She had been noted to have retinal splitting/ schisis with intraretinal cavities in the macula and serous retinal detachment OD in the past and had received barrier laser 3 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Figure 2 (A) Case 2: Cavitary optic disc anomaly of the left eye. Top left: Infrared of the enhanced depth imaging optical coherence tomography (EDI-OCT) line scan with the deepest retinal pigment epithelium (RPE) extension is superimposed on colour fundus image by manually matching retinal vessel landmarks. Based on the green line which displays the level and region of the selected EDI-OCT scans, the corresponding peripapillary changes can be evaluated. Colour photograph shows an anomalous large and deep cup. There is a temporal optic disc anomaly with peripapillary pigmentary changes and a cilioretinal artery. The image-overlay reveals that the RPE extension into the disc is found adjacent to a peripapillary pigmented area. Top right: Infrared: Note the anomaly and the localised circumscribed hyporeflectivity extending from the optic nerve head to the fovea corresponding to retinal thinning. Bottom right: Red-free: Note the peripapillary pigmentary changes and the cilioretinal artery. Bottom left: The fluorescein angiography shows early localised disc hypofluorescence. treatment OD 27 years ago. She had a large arch-shaped scotoma in the superior visual field OU. At presentation, IOP was 12/11 mm Hg OD/OS. Ophthalmoscopy showed deep cavitary defects of the optic nerve OU (figure 1A, Nr. 5). The central retinal arteries were missing and both eyes showed anomalous radial cilioretinal vessels. Pigment mottling along the temporal margin of the nerve was seen OD and along the inferotemporal vessels bone spicule pigment was found. OS showed temporal ONH crescent. EDI-OCT highlighted bilateral very deep cups. Nasally, both eyes revealed abnormal extension of the 4th hyperreflective band and the inner retinal layers into the nerve. Adjacent prominent peripapillary pigment was present. Border tissue, photoreceptors, outer retinal layers and choroid ceased before the RPE extension in both eyes (figure 1B, Nr. 5). Case 2: Pt. Nr. 9 A 37-year-old healthy man noticed a paracentral scotoma in the left lower quadrant of his visual field when covering his right eye. At presentation, BCVA was OD 20/15-1; OS 20/20+2 and IOP 13/13 mm Hg. OD showed a large, deep cup and peripapillary atrophy. OS presented with a similar abnormal large and deep cup. An inferotemporal CODA, peripapillary pigmentary 4 changes, localised temporal peripapillary retinal thinning and a cilioretinal artery were present (figure 2A). SD-OCT confirmed a deep cup and retinal thinning in the outer nasal Early Treatment Diabetic Retinopathy Study (ETDRS)-subgrid corresponding to an inferotemporal scotoma (figure 2B). Horizontal SD-OCT scans showed retinal nerve fibre layer thinning nasal to the fovea (figure 2B). Most strikingly, at the temporal side of the ONH adjacent to peripapillary hyperpigmentation near the cilioretinal artery, the RPE and the inner retinal layers extended into the disc beyond the termination of the choroid (figure 2B). The family history was negative for optic disc anomalies. Case 3: Pt. Nr. 2 This 33-year-old woman from the CODA family with the genetic aberration in the chromosome 12q locus2 3 had a history of retinal detachment OU and vitrectomy OU. Over the years, her visual fields revealed increasing scotomata and she was placed on timolol maleate, latanoprost and brimonidine. At presentation, IOP was 14/9 mm Hg; BCVA was stable at 20/ 200 OU. Indirect ophthalmoscopy revealed multiple peripheral retinal laser scars OS. The ONH showed deep cavitary defects OU (figure 1A, Nr. 2). The left ONH had a temporal crescent. Bilateral macular pigmentary changes were visible. Nasal to the Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Figure 2 (B) I: Early Treatment Diabetic Retinopathy Study (ETDRS) thickness map and a representative spectral domain optical coherence tomography (SD-OCT) B-scan, showing loss of retinal nerve fibre layer (RNFL) with thinning in the area corresponding to the visual field defect and the cavitary optic disc anomaly. II: Central SD-OCT B-scan shows RNFL loss and RPE and the inner retinal layers extending into the disc. The photoreceptors and the outer retinal layers end earlier than the Bruch’s membrane and the RPE. III+IV: The SD-OCT B-scans of the optic nerve head clearly shows a deep cup with the temporal RPE, border tissue and inner retina extending into the disc (white arrow). The photoreceptors seem to end earlier at the border tissue. There is also a membrane traversing the cup (red arrow). fovea schisis like changes not involving the fovea were visible OU in SD-OCT. EDI-OCT showed extension of presumable RPE into the disc OU, nasally OD and temporally OS (figure 1B, Nr. 2). The RPE extension was found in the area of deep excavation and peripapillary pigment. A strand assumed to be rudimentary retinal tissue traversed the right excavated cup. In the left eye, the presumable RPE and inner retinal layers extended beyond the end of the choroid. The border tissue configuration was internally oblique with a clear RPE overhang. Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 DISCUSSION This is the first clinical report of an optic disc anomaly with extension of the hyper-reflective band into the optic disc cavity.12 15 The respective eyes presented with 4th hyperreflective band extension far beyond the termination of the choroid. In all these eyes but one, the inner retinal layers also extended into the optic disc. The extension was usually adjacent to pigmented peripapillary areas. In normal eyes, the retinal layers as well as RPE and choroid end near the borders of the optic nerve are separated by a 5 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Table 1 Demographic characteristics of cavitary optic disc anomaly patients Pt. Nr Age Sex Inheritance BCVA RPE in cup Schisis VF defect Nr. 1 64 m Sporadic No OU OU Nr. 2 33 f AD OU OU OU Nr. 3 70 m AD No OU OU Nr. 4 45 f AD OU OS OU Nr. 5 42 f AD OU No OU Nr. 6 59 m Sporadic No OS OU Nr. 7 69 f Sporadic OS OD No VF available Nr. 8 73 m AD No OU OU Nr. 9 38 m Sporadic OS No OS Nr. 10 20 m Sporadic OD 20/20 OS 20/15 OD 20/200 OS 20/200 OD 20/20 OS 20/15 OD 20/40 OS 20/25 OD 20/100 OS 20/200 OD 20/20 OS 20/40 OD 20/50 OS 20/25 OD 20/70 OS CF OD 20/15 OS 20/20 OD 20/25 OS 20/20 No No No VF available Patients with retinal pigment epithelium (RPE) extending into the cup are shown in bold letters. Pt. Nr. resembles consecutive patient number visible in figure 1. AD, autosomal dominant; BCVA, best corrected visual acuity; CF, counting fingers; f, female; m, male; VF, visual field. border tissue from the ONH.12 15 The cessation of the retina is usually oblique with the inner layers ending before the outer layers. Photoreceptors become smaller and terminate before the RPE at the border tissue of Kuhnt and the choriocapillaries ends at variable distance at the border tissue of Elschnig.12 15 The RPE continues almost as far as Bruch’s membrane and terminates at the outer border of the ONH on the inner border of the choroid. Bruch’s membrane itself is the outermost retinal structure and defines the optic nerve canal opening.15 In our patients, we could not determine if Bruch’s membrane accompanied the RPE extension into the disc, but as the Bruch’s membrane is the basement membrane of the RPE, it is very likely that the Bruch’s membrane, too, extended into the ONH. The definition of the nerve canal opening is the end of Bruch’s membrane in normal eyes. The finding of this unusual extension of RPE (and possibly Bruch’s membrane) is anomalous.13 15–17 The anatomy of the optic disc margin in CODA patients is not comparable with normal eyes as CODA affects the integrity of the disc margin.8 18 A short Bruch’s membrane (and RPE) overhang with respect to the border tissue termination is common in healthy and glaucomatous eyes and in eyes with ONH drusen.11 13 However, in these eyes, the overhang is very short and does not extend into the disc. Congenital CODAs are rare with an incidence of 1/11 000.18 They can be sporadic or inherited.18 In our cases, RPE extension was found in sporadic as well as in AD CODA cases. Although this is the first study reporting in vivo images of the extension of the 4th hyper-reflective band into the disc, previous reports on morning glory syndrome and ONH colobomas using swept-source OCT demonstrated clear extension of the respective band in these presented figures. However, no comment on this alteration can be found in any of these reports.19 20 Previous histopathology case reports have described unusual forms of optic disc coloboma that included abnormal extension of sclera, choroid, retinal tissue and hyperplastic RPE with prolapse into the optic disc.6 21 In hypoplastic 6 optic discs, abnormal extension of retina and RPE over the outer portion of the lamina cribrosa can be found.4 Other histological studies have reported RPE cells in an optic pit and a coloboma with a membrane consisting of rudimentary retinal tissue and RPE, which traversed the cavity.22 23 Five patients (seven eyes) presented with additional inner retinal extension, one also had a membrane traversing the cavity and one showed a traversing hyper-reflective strand in OCT which we presume is rudimentary retinal tissue (figure 1B, Nr. 2). Embryologically, the ectoderm folds into itself, creating a double-layer of neural ectoderm which ultimately differentiates into the neurosensory retina and the RPE. Extension and prolapse of retinal tissue into the cavity may represent faulty development at this embryological phase. However, the main event leading to this respective morphological alteration may be also found during scleral canal formation, developing long before the axons of the ganglion cells of the neurosensory retina form the optic disc. A previous study found disruption of intermediary tissue of Kuhnt in a patient with coloboma.4 24 RPE (and possibly Bruch’s membrane) extension may be therefore caused by disruption or absence of border tissue, impeding normal development and normal cessation of the RPE and Bruch’s membrane. Yet, based on our EDI-OCT findings, we can only speculate that the extension of the 4th hyper-reflective band is actual RPE; it could also be dysplastic outer retinoblasts or proliferative gliosis. Further histological or electron-microscopic evaluation or image modalities like polarisation sensitive-OCT are warranted to further address this issue. Also, further studies are warranted to determine whether this finding is seen specifically with certain genetic changes, like the recently detected candidate genes in chromosome 12q2 or PAX6 and PAX2 genes,25 26 or whether it may be also found in patients with other congenital and even acquired disc abnormalities. Myopia as a potential contributing factor needs also further evaluation. Limitation of this study includes the relatively small patient population, its qualitative design and the fact that no star scan or vertical raster scans were included. Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Clinical science Acknowledgements The authors want to thank Ronil Shah for his help to overlay the images and Dr Katharina Eibenberger for grading the images of the intraobserver agreement study. The authors have obtained written permission from the person named in the acknowledgement. Contributors Study concept and design: MRM, LMJ; Acquisition of data: ES, MRM, LMJ, JHF; Analysis and interpretation of the data: MRM, LMJ; Drafting the manuscript: MRM; Critical revision of the manuscript: LMJ, JHF; Obtaining funding: LMJ; Administrative, technical, material support: ES; Study supervision: LMJ. Funding This work was supported in part by an unrestricted grant from the Macula Foundation, New York City and by Research to Prevent Blindness, New York. Competing interests None. Patient consent Obtained. Ethics approval Northwestern University IRB. Provenance and peer review Not commissioned; externally peer reviewed. REFERENCES 1 2 3 4 5 6 7 8 9 10 Corbett JJ, Savino PJ, Schatz NJ, et al. Cavitary developmental defects of the optic disc. Visual loss associated with optic pits and colobomas. Arch Neurol 1980;37:210–13. Fingert JH, Honkanen RA, Shankar SP, et al. Familial cavitary optic disk anomalies: identification of a novel genetic locus. Am J Ophthalmol 2007;143:795–800. Honkanen RA, Jampol LM, Fingert JH, et al. Familial cavitary optic disk anomalies: clinical features of a large family with examples of progressive optic nerve head cupping. Am J Ophthalmol 2007;143:788–94. Brodsky MC. Congenital optic disk anomalies. Surv Ophthalmol 1994;39:89–112. Brown GC, Shields JA, Goldberg RE. Congenital pits of the optic nerve head. II. Clinical studies in humans. Ophthalmology 1980;87:51–65. Cogan DG. Coloboma of optic nerve with overlay of peripapillary retina. Br J Ophthalmol 1978;62:347–50. Ohno-Matsui K, Hirakata A, Inoue M, et al. Evaluation of congenital optic disc pits and optic disc colobomas by swept-source optical coherence tomography. Invest Ophthalmol Vis Sci 2013;54:7769–78. Onwochei BC, Simon JW, Bateman JB, et al. Ocular colobomata. Surv Ophthalmol 2000;45:175–94. Knape RM, Motamarry SP, Clark CL III, et al. Morning glory disc anomaly and optic nerve coloboma. Clin Pediatr (Phila) 2012;51:991–3. Cennamo G, de Crecchio G, Iaccarino G, et al. Evaluation of morning glory syndrome with spectral optical coherence tomography and echography. Ophthalmology 2010;117:1269–73. Munk MR, et al. Br J Ophthalmol 2014;0:1–7. doi:10.1136/bjophthalmol-2014-305722 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 Merchant KY, Su D, Park SC, et al. Enhanced depth imaging optical coherence tomography of optic nerve head drusen. Ophthalmology 2013;120:1409–14. Woff E. Anatomy of the eye and orbit, Chapter 7 The visual pathway. 6th edn. Philadelphia: W.B. Saunders Company, 1968. Reis AS, O’Leary N, Yang H, et al. Influence of clinically invisible, but optical coherence tomography detected, optic disc margin anatomy on neuroretinal rim evaluation. Invest Ophthalmol Vis Sci 2012;53:1852–60. Moore M, Salles D, Jampol LM. Progressive optic nerve cupping and neural rim decrease in a patient with bilateral autosomal dominant optic nerve colobomas. Am J Ophthalmol 2000;129:517–20. Anderson DR, Hoyt WF. Ultrastructure of intraorbital portion of human and monkey optic nerve. Arch Ophthalmol 1969;82:506–30. Strouthidis NG, Yang H, Reynaud JF, et al. Comparison of clinical and spectral domain optical coherence tomography optic disc margin anatomy. Invest Ophthalmol Vis Sci 2009;50:4709–18. Mwanza JC, Oakley JD, Budenz DL, et al. Ability of cirrus HD-OCT optic nerve head parameters to discriminate normal from glaucomatous eyes. Ophthalmology 2011;118:241–8 e1. Georgalas I, Ladas I, Georgopoulos G, et al. Optic disc pit: a review. Graefes Arch Clin Exp Ophthalmol 2011;249:1113–22. Nagasawa T, Mitamura Y, Katome T, et al. Swept-Source Optical Coherence Tomographic Findings in Morning Glory Syndrome. Retina 2014;34:206–8. Chang S, Gregory-Roberts E, Chen R. Retinal detachment associated with optic disc colobomas and morning glory syndrome. Eye (Lond) 2012; 26:494–500. Pedler C. Unusual Coloboma of the Optic Nerve Entrance. Br J Ophthalmol 1961;45:803–7. Poulson AV, Snead DR, Jacobs PM, et al. Intraocular surgery for optic nerve disorders. Eye (Lond) 2004;18:1056–65. Ferry AP. Macular Detachment Associated with Congenital Pit of the Optic Nerve Head. Pathologic Findings in Two Cases Simulating Malignant Melanoma of the Choroid. Arch Ophthalmol 1963;70:346–57. Lin CC, Tso MO, Vygantas CM. Coloboma of optic nerve associated with serous maculopathy. A clinicopathologic correlative study. Arch Ophthalmol 1984;102:1651–4. Sanyanusin P, Schimmenti LA, McNoe LA, et al. Mutation of the PAX2 gene in a family with optic nerve colobomas, renal anomalies and vesicoureteral reflux. Nat Genet 1995;9:358–64. Holme RH, Thomson SJ, Davidson DR. Ectopic expression of Msx2 in chick retinal pigmented epithelium cultures suggests a role in patterning the optic vesicle. Mech Dev 2000;91:175–87. 7 Downloaded from http://bjo.bmj.com/ on November 3, 2014 - Published by group.bmj.com Enhanced depth imaging optical coherence tomography of congenital cavitary optic disc anomaly (CODA) Marion R Munk, Evica Simjanoski, John H Fingert and Lee M Jampol Br J Ophthalmol published online October 30, 2014 Updated information and services can be found at: http://bjo.bmj.com/content/early/2014/10/30/bjophthalmol-2014-30572 2 Supplementary Material Supplementary material can be found at: http://bjo.bmj.com/content/suppl/2014/10/30/bjophthalmol-2014-3057 22.DC1.html These include: References This article cites 25 articles, 6 of which you can access for free at: http://bjo.bmj.com/content/early/2014/10/30/bjophthalmol-2014-30572 2#BIBL Email alerting service Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/