Female Gender, Estrogen Loss, and Sub
advertisement

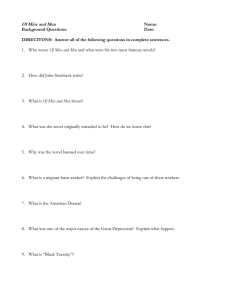
Female Gender, Estrogen Loss, and Sub-RPE Deposit Formation in Aged Mice Scott W. Cousins,1 Maria E. Marin-Castaño,1,2 Diego G. Espinosa-Heidmann,1,2 Anastassia Alexandridou,1 Liliane Striker,3 and Sharon Elliot 3 PURPOSE. Estrogen status influences the incidence and severity of many diseases in women. Because women with early menopause appear at risk for worse ARMD, estrogen deficiency may also contribute to the onset or severity of ARMD in women. It has been observed that aged male C57BL/6 mice fed a high-fat diet and briefly exposed to blue-green light exhibit development of significant sub-RPE deposits and mild Bruch’s membrane (BrM) thickening. This model was used in an attempt to delineate the role of gender and estrogen status in this model. METHODS. C57BL/6 male and female mice of 9 or 16 months were fed a high-fat diet for 4.5 months. Several groups of 9-month-old female mice underwent estrogen depletion by ovariectomy, with or without supplementation with exogenous 17-estradiol. After 4 weeks of a high-fat diet, the eyes were exposed to seven 5-second doses of nonphototoxic levels of blue-green light over 2 weeks. Three and a half months after cessation of blue light treatment, transmission electron microscopy was performed to assess severity of deposits, BrM changes, and choriocapillaris endothelial morphology. In some mice, gelatin zymography and Western blot analyses were performed on protein extracts of freshly isolated RPE to determine the effect of estrogen on matrix metalloproteinase (MMP)-2 activity in the RPE. RESULTS. Both male and female 16-month-old mice showed qualitatively similar basal laminar deposit morphology, but the severity of thickness, continuity, and content was significantly greater in female mice. Aged female mice also demonstrated a trend toward more severe endothelial changes and increased BrM thickening compared with age-matched male mice. Ovariectomized middle-aged mice showed more severe deposits than sham-surgery control animals. However, ovariectomized mice that received high-dose estrogen supplementation also showed significant deposits, although they had thinner BrMs than did the estrogen-deficient mice. Loss of RPE MMP-2 activity correlated with deposit severity, with estrogen-deficient mice expressing less MMP-2 than ovary-intact control mice. CONCLUSIONS. Female gender in aged mice and estrogen deficiency in middle-aged mice appears to increase the severity of sub-RPE deposit formation. Estrogen deficiency may increase From the 1Department of Ophthalmology, Bascom Palmer Eye Institute, Miami Florida; and the 3Vascular Biology Institute, University of Miami School of Medicine, Miami, Florida. 2 Joint 2nd authorship. Presented at the annual meetings of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, Florida, May 2001 and May 2002. Supported by National Eye Institute Grant EYAI13318. Submitted for publication March 21, 2002; revised August 13 and September 30, 2002; accepted October 10, 2002. Commercial relationships policy: N. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertisement” in accordance with 18 U.S.C. §1734 solely to indicate this fact. Corresponding author: Scott W. Cousins, Bascom Palmer Eye Institute, William L. McKnight Vision Research Center, 1638 NW 10th Avenue, Miami, FL 33136; scousins@med.miami.edu. Investigative Ophthalmology & Visual Science, March 2003, Vol. 44, No. 3 Copyright © Association for Research in Vision and Ophthalmology susceptibility to formation of sub-RPE deposits by dysregulating turnover of BrM, contributing to collagenous thickening and endothelial changes. Estrogen supplementation at the dosages used in this study does not appear to protect against formation of sub-RPE deposits. (Invest Ophthalmol Vis Sci. 2003;44:1221–1229) DOI:10.1167/iovs.02-0285 A ge-related macular degeneration (ARMD) is the most common cause of lost central vision in the elderly.1 The histopathology of early ARMD demonstrates accumulation of specific lipid-rich deposits under the retinal pigmented epithelium (RPE). During aging, deposits, called basal laminar deposits or BLDs, initially accumulate between the RPE and its basement membrane, but progression into ARMD requires additional formation of deposits within Bruch’s membrane (BrM, called basal linear deposit and drusen).1,2 The pathogenesis of deposits in ARMD is unknown, but the process is influenced by genetic, systemic health, and environmental risk factors. The incidence and severity of many diseases have been associated with the reduction of estrogen in women.3– 6 Although information is limited, several observational studies have suggested that estrogens may serve to protect women from the development or progression of ARMD. Early menopause may be associated with the development of ARMD in women,7,8 implying that estrogen deficiency may play a role in the pathogenesis of ARMD.9 Nonetheless, these few observational studies have provided the basis for a large clinical trial to evaluate estrogen-replacement therapy to prevent the onset or progression of ARMD. Among their many actions, estrogens regulate the expression of genes important for extracellular matrix (ECM) turnover, including collagen and matrix metalloproteinases (MMPs).10,11 For example, estrogens have been shown to increase both MMP-9 mRNA and activity in glomerular mesangial cells,12,13 and to increase MMP-2 activity and protein expression in human granulosa lutein cells.10 The effects of estrogen on the retina or RPE are unknown. Estrogen-mediated regulation of genes, which are expressed in RPE and are important for matrix turnover, may provide a pathogenic mechanism to explain the link between estrogen status and ARMD. In this regard, MMP-2 may be important since it preferentially degrades extracellular matrix components such as types IV and I collagen.14 –16 Dysregulation in the relative production of MMP-2 and collagen may lead to net deposition in BrM and contribute to formation of sub-RPE deposits. We have recently shown that normal human RPE contains functionally active estrogen receptors (ERs) of both subtypes and that those and MMP-2 are regulated by estrogens.17 A dose dependency was observed, with physiologic levels of estrogen causing upregulation (compared with RPE without estrogen) but superphysiologic concentrations revealed a paradoxical absence of effect. These data suggest that loss of estrogen and/or estrogen function is associated with downregulation of expression of MMP-2 and its activity in the RPE. In this study, we sought to determine whether gender and estrogen status affect formation of deposits and RPE expression of MMP-2 in vivo. We have recently developed a mouse model 1221 1222 Cousins et al. for formation of sub-RPE deposits based on feeding C57BL/6 mice a diet high in polyunsaturated fats followed by exposure to blue light.18 Briefly, the results indicated that in aged mice (16 months) but not in younger mice, moderately severe subRPE deposits developed, consistent with BLD. Significant thickening and other changes occurred in BrM, but without definite drusen, and a variable degree of endothelial injury was present in the choriocapillaris without definite neovascularization. In this prior analysis of sub-RPE deposits and mild thickening of BrM, we did not analyze differences between male and female mice. We performed a study to better delineate the role of age, gender, and estrogen depletion or supplementation in this model. METHODS Mice C57BL/6 male or female mice of ages 9 or 16 months were purchased from the National Institute of Aging (Bethesda, MD). C57BL/6 were chosen because, compared with other strains of mice, they exhibit development of plasma hyperlipidemia when fed a high-fat diet.19 The guidelines of the ARVO Statement for the Use and of Animals in Ophthalmic and Vision Research were followed, and the Division of Veterinary Resources approved all experiments. Experimental Model for Sub-RPE Deposits In our recently developed model of formation of sub-RPE deposits based on feeding mice a high-fat diet followed by exposure to bluegreen light,18 experimental mice were switched from a regular diet (Diet 5001; PMI Nutrition International Test Diet, Richmond, IN) to high-fat chow (Diet 5015; PMI Nutrition International Test Diet) at the beginning of the experiments to allow tissue distribution of dietary lipid. The high-fat diet more than doubled the relative percentage of calories from fat but maintained the same number of calories per gram of food (by reducing the percentage of calories from carbohydrates). Dietary fat was increased from 11% of total calories to 25% of total calories, equally divided between increased saturated and unsaturated fat. The diets contained the following constituents: 64% carbohydrates, 30% protein, 6.5% total fat, 3.6% unsaturated fat, 1.2% linoleic acid, and 0.05 IU/g vitamin E for the regular chow versus 55% carbohydrates, 18% protein, 26% total fat, 8.2% unsaturated fat, 2.5% linoleic acid, and 0.04 IU/g vitamin E for the high-fat chow. In the right eye, a brief, repetitive exposure to nonphototoxic levels of argon laser 488 nm blue-green light (Model 910A Argon Laser; Coherent, Palo Alto, CA) was added to induce transient production of RPE oxidant,20 –24 4 weeks after starting the high-fat chow. After dilation of eyes with 0.5% tropicamide and 2.5% phenylephrine and with anesthesia induced in the animal by intramuscular injection of 0.1 mL of a cocktail of xylazine (8.5 mg/mL), acepromazine (1.5 mg/mL), and ketamine (42 mg/mL), seven 5-second exposures to 20 mJ (approximately one third the threshold intensity to produce a clinical lesion) of argon laser 488-nm blue-green light was administered 2 to 3 days apart over a 2-week period. Pilot experiments demonstrated that 60 to 80 mJ was required to produce a distinct retinal burn clinically visible as a light gray lesion, and that 120 mJ was needed to produce an intense white burn with BrM injury detectable by histologic examination 24 hours later. The delivery system used a probe producing a 200-m spot, and the energy intensity was calibrated before each application by a photometer (210 Power Meter; Coherent) held at a standardized distance from the probe. Retinal illumination required a specially designed biconcave contact lens (focal distance, ⫺6.5 mm at 670 nm; 153.8 dioptric power) to neutralize the optical power of the natural lens and to enlarge the retinal spot size. When threshold injury (i.e., visible retinal burns requiring 60 –100 mJ) were applied to characterize the actual area of retinal illumination, the retinal area of direct burn occurred in the superotemporal retina and appeared to be approximately 700 to 1000 m, or approximately three to six disc areas, IOVS, March 2003, Vol. 44, No. 3 accounting for approximately 5% to 8% of the retinal surface area. Runoff (spread from the edge of the burn) and significant scattering through the delivery system both occur. Thus, actual amount of energy delivered to the retina is impossible to calculate, and retinal illumination is uneven over its surface. All mice were maintained on 12-hour light– dark cycles with ambient light maintained by fluorescent lighting, and cages were kept on middle shelves of the cage rack. The high-fat chow diet was continued for three additional months, after the 2-week exposure to blue-green light. Mice were then killed and the eyes immediately removed for transmission electron microscopy (TEM) or recovery of RPE for MMP zymography and Western blot analysis. Experimental Protocol Studies were divided into three protocols: 1. To evaluate age-related gender differences, the deposit model described earlier was used in male and female mice aged 9 months (n ⫽ 5 of each gender) or 16 months (n ⫽ 5 male, 6 female). The nonexposed left eye was not evaluated in this study. 2. To evaluate the effect of estrogen status in middle-aged mice, 9-month-old female mice were divided into three groups: ovary intact (controls, n ⫽ 6), ovariectomy plus implantation of an empty pellet (n ⫽ 5), or ovariectomy followed by subcutaneous implantation of a sustained release pellet containing a 90-day supply of 17-estradiol (1.7 mg/pellet; (n ⫽ 7). Ovariectomies were performed with animals under general anesthesia in sterile conditions with a 1-cm laparotomy incision. The peritoneal cavity was entered, the ovaries identified, retracted, and excised bilaterally. The incision was closed with 6-0 interrupted sutures (Vicryl; Ethicon, Piscataway, NJ). Two weeks after ovariectomy, subcutaneous implantation of the empty or estrogen-containing pellet was performed, and the high-fat diet was initiated. The deposit model described previously was performed. Ninety days after implantation, the original pellet was removed and replaced with a fresh implant to ensure constant estrogen for 135 days of the experiment. The drug delivery pellet is a commercially available polylactide-containing polymer with well-defined pharmacokinetic and drug-release characteristics (Innovative Research of America, Sarasota, FL). The nonexposed left eye was not evaluated in this study. 3. To evaluate the effect of 17-estradiol on MMP-2 expression and activity in RPE, five additional groups of 9-month-old mice were evaluated: ovary intact (n ⫽ 7); ovariectomy (n ⫽ 7), ovariectomy plus high-dose (1.7 mg/pellet; n ⫽ 7), moderate-dose (0.36 mg/pellet; n ⫽ 7), or low-dose (0.18 mg/pellet; n ⫽ 7) estradiol implant (NE-121, Innovative Research of America). Surgery was conducted as explained previously. The deposit model was performed exposing both eyes to the blue-green light. Six weeks after the high-fat chow was started, the eyes were removed for analysis of MMP-2 in RPE. This time point was chosen to evaluate the physiologic effect of estrogen at the midpoint of deposit formation. RPE Isolation After enucleation, the eyes were rinsed with 10% gentamicin for sterilization and twice with PBS (1⫻). The eyes were then placed in a dish containing PBS (1⫻) and with the aid of a dissecting microscope, were opened by a circumferential incision at the ora serrata. The anterior segment was removed, and the vitreous-retina was separated from the RPE and choroid eyecup with a round-tipped disposable blade (K20-1504; Katena Products, Inc., Denville, NJ) and Tennant forceps (K5-5230; Katena Products, Inc.). The remaining eyecup was incubated with Dulbecco’s modified Eagle’s medium (DMEM)/F12 (1:1 vol/vol) supplemented with 10% fetal bovine serum (FBS) at 37°C for 10 minutes. Then, using a Barraquer spatula (K3-2310; Katena Products, Inc.) for blunt dissection and scraping, the RPE monolayer was Estrogen and Experimental BLD IOVS, March 2003, Vol. 44, No. 3 dissected from BrM and choroid. The RPE was aspirated with a micropipette and transferred into individual tubes (Eppendorf, Fremont, CA) containing 250 L cold lysis buffer or (1⫻) Earle’s balanced salt solution (EBSS) and homogenized on ice with a pestle. RPE samples of left and right eyes of individual mice from each group were pooled and stored at – 80°C until protein extraction and analysis. An aliquot from the isolated RPE cells were stained with mouse anti-cytokeratin-18 antibody (Sigma, St. Louis, MO) and with mouse anti-endothelial cell (CD146) monoclonal antibody (Chemicon International, Inc., Temecula, CA) to ensure that there was no contamination with endothelial cells. Western Blot Analysis Dissected RPE monolayer was homogenized with a pestle in lysis buffer and centrifuged for 30 minutes at 15,000g at 4°C. Supernatant was collected, and protein concentration was determined by bicinchoninic acid (BCA) protein assay.12 All samples were then diluted in Laemmli buffer and boiled. Twenty micrograms of the samples was loaded on a 10% polyacrylamide gel. Prestained markers were used to estimate molecular weight. Electrotransfer to nitrocellulose was performed by electroelution. Immunoblot analysis was performed with MMP-2 antibody (mAb 13405; Chemicon), and immunoreactive bands were determined by exposing the nitrocellulose blots to a chemiluminescence solution and exposure to autoradiographic film (Hyperfilm ECL; Amersham Pharmacia Biotech, Piscataway, NJ). Confluent cell layers were washed with PBS (1⫻) and collected in the presence of lysis buffer. RPE tissue and cell homogenates were centrifuged for 30 minutes at 15,000g at 4°C. Supernatant was collected, and protein concentration was determined by BCA protein assay. All samples were then diluted in Laemmli buffer and boiled. Ten milligrams of samples for ER type a and MMP-2 or 40 mg for ER type b were loaded on a 10% polyacrylamide gel. Prestained markers were used to estimate molecular weight. Electrotransfer to nitrocellulose was performed by electroelution. Immunoblot analysis was performed with each anti-ERa, -ERb, and -MMP-2 antibody (H-184 and N-19; Santa Cruz Biotechnology, Santa Cruz, CA; and mAb 13405; Chemicon), and immunoreactive bands were determined by exposing the nitrocellulose blots to a chemiluminescence solution and exposing to autoradiographic film (Hyperfilm ECL; Amersham Pharmacia Biotech). MMP-2 Activity The tissue homogenate supernatants were collected, and protein concentration was determined. MMP-2 activity was assessed with 10% zymogram gels (Invitrogen Corp., Carlsbad, CA), as described previously.25 Briefly, 20 g of proteins from RPE tissue were used. The medium was diluted to normalize for protein quantity before the addition of 5⫻ Laemmli buffer under nonreducing conditions. After electrophoresis, gels were washed for 1 hour in 2.5% Triton X-100 and incubated 24 hours in 50 mM Tris buffer. The gels were stained with Coomassie Blue and air dried. Densitometry, using NIH image ver. 1.6 (available by ftp from zippy.nimh.nih.gov/or from http://rsb.info.nih. gov/nih-image; developed by Wayne Rasband, National Institutes of Health, Bethesda, MD) was used to analyze relative MMP-2 activity. Each zymography assay was repeated at least three times. Serum Levels of 17-Estradiol Serum (50 L) was removed by cardiac puncture, and 17-estradiol was measured in triplicate for each group by a competitive enzyme immunoassay kit (Active Estradiol EIA kit DSL-10-4300; Diagnostic Systems Laboratories, Inc., Webster, TX). Histology and TEM Mice were killed by anesthetic overdose and perfused with saline followed by a mixture of 3% glutaraldehyde and 2% paraformaldehyde. Eyes were immediately enucleated and the corneas removed and fixed in 3% glutaraldehyde and 2% paraformaldehyde in PBS (0.1 M, pH 7.3) 1223 overnight. The lens was removed, and the posterior segment (retina, choroid, and sclera) was quadrisected to contain the perioptic nerve portion at the apex and the ciliary body at the base. The superotemporal quadrant of retina, choroid, and sclera was submitted for electron microscopic sectioning. The tissue was fixed in 1% osmium tetroxide for 1 hour, rinsed in PBS, dehydrated in EtOH, and then imbedded in Spur’s resin. Thick and ultrathin sections (0.7-1.0 m) were cut on a microtome (MT-2; Porter Blum, Hatfield, PA). Thick sections were stained with toluidine blue and examined by light microscopy. Ultrathin sections were stained with 4% uranyl acetate and lead citrate and examined with a transmission electron microscope (model CX-100; JEOL, Tokyo, Japan). Semiquantitative Grading System For each specimen, a single cross-section was examined, and lowpower transmission electron micrographs were made of the entire section from perioptic to ciliary body portion (usually approximately 10 micrographs). Then, two to four representative high-power micrographs were made from each low-power section, by an individual unaware of the experimental conditions, and were used for semiquantitative scoring. The high-power micrographs were graded by two independent examiners for the presence and severity of BLD. A severity score of 0 to 15 points was determined for each section by summation of the median scores of all the micrographs from a section on each of five different categories of abnormalities (from 0 to 3 points for each): continuity of BLD; maximal thickness of BLD; nature of deposit content (homogeneous, banded structures, membranous debris, granular material); presence of BrM abnormalities; and assessment of other choriocapillaris endothelial damage or invasion. BrM thickness was also directly measured in three different standardized locations in each image and then averaged to provide a mean score for that micrograph. The mean of 10 high-power micrographs was used to assign and average BrM thickness for an individual specimen. Groups were compared by determining the mean ⫾ SD, and the t-test was used for statistical analysis of the differences. In addition, the frequency of BLD was determined using two different criteria. “Any BLD” was defined as the presence of any discrete focal nodule of homogenous material of intermediate electron density between the RPE cell membrane and BrM in at least one micrograph within a section. “Moderate BLD” was defined as the presence, in at least three micrographs, of the following: continuous BLD extending under two or more cells, deposit thickness equal to or greater than 20% of RPE cell cross-sectional thickness, or the presence of any banded structures within the BLD. Differences in the relative frequency were tested using 2 analysis. Data from statistical analysis of zymography, Western blot analysis, and estradiol levels are expressed as percentage of control (ovary intact) or as arbitrary densitometry units. One-way analysis of variance and the Dunnett multiple-comparison post hoc test or Student’s t-test were performed for the statistical analysis. RESULTS Gender Differences in Deposit Formation in Aged Mice Recently, we have shown that 16-month-old mice, fed a high-fat diet and exposed to blue light, develop morphologic changes consistent with early ARMD, including sub-RPE deposits, thickening of BrM, and morphologic changes in the choriocapillaris. However, young (2-month-old) mice did not exhibit the anatomic changes and 9-month-old developed infrequent but mild changes. We sought to determine the contribution of gender to the morphologic changes by comparing male and female aged mice. Lipid level determination confirmed previous results in which middle-aged and aged C57BL/6 mice fed high-fat chows developed a 1.4- to 2-fold elevated plasma triglycerides and 1224 Cousins et al. IOVS, March 2003, Vol. 44, No. 3 FIGURE 1. TEM of the outer retina and choroid from 16-month-old fatfed female or male mice exposed to blue-green light. Left: specimen from an aged female mouse revealed moderately thick sub-RPE deposits (under white dotted line) containing many banded structures (white asterisk) consistent with BLDs. BrM revealed marked collagenous thickening and scattered debris (black asterisk). Invasion by several cellular processes (black arrows) apparently emanating from the choriocapillaris (CC) was also evident. The endothelium revealed some loss of fenestrations with thickened basement membrane. Right: specimen from an aged male mouse revealed continuous, moderately thick sub-RPE deposits (under white dotted line) containing banded structures (white asterisk) similar to those observed in the female. However, BrM was only mildly and irregularly thickened. The endothelial morphology appears slightly abnormal, with mild reduplication of the basement membrane, but evidence of severe injury or invasion was not observed. Magnification, ⫻25,000. cholesterol compared with age-matched mice fed regular diets.18 Sixteen-month-old female and male mice exhibited qualitatively similar morphologic changes internal to the RPE basement membrane (Fig. 1). Mice of neither gender showed significant photoreceptor degeneration or morphologic changes in the RPE indicative of severe degeneration or injury. However, TEM revealed that mice of both genders had moderately severe basal laminar deposits. In general, deposits in both genders were multifocal and moderately thick, often containing oval-shaped banded structures (i.e., fibrous long-spaced collagen) and other debris embedded in a homogenous material of moderate electron density. These findings are typical of BLD observed in humans.1,2 Table 1 shows that semiquantitative scoring suggested that the deposits were more severe in female than in male mice (10.6 ⫾ 2.4 in females versus 7.4 ⫾ 1.8 in males), indicating a modest but significant increase in continuity, thickness, and the nature of the deposit content. Qualitative and quantitative differences between male and female mice were also observed within BrM and the choriocapillaris. In general, BrM of male mice demonstrated moderate collagenous thickening with accumulation of minimal amorphous debris (Fig. 1, right). The choriocapillaris endothelium revealed normal morphology or showed mild hypertrophy. Compared with male mice, female mice often demonstrated pronounced collagenous thickening of BrM with accumulation of various kinds of debris and deposits (Fig. 1 left, asterisk). In approximately half the specimens, prominent cellular processes were identified, suggesting cellular invasion from the choriocapillaris (possibly representing endothelial cells; Fig. 1, left, arrows; Fig. 2 right, arrowheads). The choriocapillaris endothelium often demonstrated morphologic changes suggestive of chronic injury, especially loss of fenestrations and hypertrophy when compared with normal aged female mice consuming a regular diet and not exposed to blue-green light (Fig. 2, left). However, no definite neovascularization or vascular lumen formation was identified within BrM. Measurement of BrM demonstrated increased thickness, although very high variability among specimens from aged females prevented statistical significance (Table 1). Neither male nor female 9-month-old mice had moderate or severe deposits, BrM thickening, or endothelial changes, and therefore the differences were not quantitatively analyzed. TABLE 1. Effect of Gender on sub-RPE Deposits in Aged Mice Group n Frequency of Any BLD (%) 16 mo male 16 mo female 5 6 100 100 Frequency of Moderate BLD (%) Mean Severity Score (15 max.) Mean BrM Thickness Frequency of Endothelial Invasion (%) 100 100 7.4 ⫾ 1.8 10.6 ⫾ 2.4* 15.6 ⫾ 3.3 30.0 ⫾ 21.0† 0 50‡ Any BLD, presence of any homogeneous deposit (focal or continuous) between the RPE cell membrane and its basement membrane in at least one (of five) transmission electron micrographs from an individual specimen (i.e., one micrograph with a score of at least 1 point). Moderate BLD, presence of continuous deposits underlying several cells, or presence of banded structures (fiber long-spaced collagen), or focal deposit thickness more than one quarter the cell height in at least three TEMs from an individual specimen (i.e., three micrographs with a minimum score of three or more). * P ⫽ 0.045. † P ⫽ NS. ‡ P ⫽ 0.02. Estrogen and Experimental BLD IOVS, March 2003, Vol. 44, No. 3 1225 FIGURE 2. TEM of the outer retina and choroid of 16-month-old female mice. Left: specimen from an aged female mouse consuming regular chow and not exposed to blue light revealed normal RPE without deposits and minimally thickened BrM. The choriocapillaris (CC) appeared normal. Right: specimen from an aged female mouse fed high-fat chow and exposed to blue-green light revealed moderately thick sub-RPE deposits (under white dotted line) containing banded structures (white arrow). There was irregular thickening of BrM. The endothelium revealed thickening (white asterisk) with some loss of fenestrations (black arrows) and reduplication of the basement membrane (black asterisks). Invasion by several cellular processes (black arrowheads), apparently emanating from the choriocapillaris, was also evident. Abbreviations as in Figure 1. Magnification, ⫻25,000. Effect of Estrogen Depletion and Supplementation on Deposit Severity To better determine the role of estrogen depletion as a mechanism for the gender differences in aged mice, we compared the effect of ovariectomy on severity of deposits in 9-month-old female mice. Reduction of estrogen is among the most important hormonal deficiencies induced by ovariectomy. We confirmed that ovariectomy caused a reduction in plasma estradiol (Table 2). Compared with aged-matched females (97 pg/mL) ovariectomized females demonstrated approximately 30 pg/ mL. Male mice had approximately 47.5 pg/mL, resulting from metabolism of normal testosterone and other sex hormones. We examined the subretinal morphologic changes in the ovariectomized mice. As expected, sham-surgery control animals had minimal changes in RPE morphology (Fig. 3, top left). Minor, focal homogenous nodular deposits under the RPE were observed, and minimal changes in BrM or choriocapillaris were present. In contrast, ovariectomy induced significant morphologic changes (Fig. 3, top right). Moderately severe BLD were observed with typical morphologic features including banded structures and other heterogeneous debris. Also, moderate collagenous thickening of BrM was present in most eyes, although intra-BrM debris or cellular invasion was not observed. However, significant morphologic choriocapillaris changes were often apparent, especially hypertrophy and loss of fenestration (Fig. 3, bottom left). These qualitative differences were TABLE 2. Effect of Estrogen Depletion or Supplementation on Blood Levels of 17-Estradiol Group 9-month male 9-month female (Ovary intact) 18.5-month female (ovary intact but postmenopausal) 9-month female (ovariectomized) 9-month female (ovariectomized ⫹ supplemental estrogen [1.7 mg/pellet]) 9-month female (ovariectomized ⫹ supplemental estrogen [0.36 mg/pellet]) 9-month female (ovariectomized ⫹ supplemental estrogen [0.18 mg/pellet]) Plasma 17-Estradiol Concentration (pg/ml) 47.5 ⫾ 1.9 97 ⫾ 3.4 36.1 ⫾ 0.2 30.8 ⫾ 0.8 545 ⫾ 5.3 175 ⫾ 2.9 82 ⫾ 1.4 Data are expressed as mean picograms per milliliter ⫾ SEM. n ⫽ 7 for all groups except 9-month male, where n ⫽ 5. reflected in quantitative measures of BLD severity score and BrM thickness (Table 3). Because estrogen depletion was associated with more severe sub-RPE deposits, we investigated the ability of estrogen replacement therapy with subcutaneous implantation of pellets containing a sustained release formulation of estradiol. Three different dosages were evaluated in preliminary experiments. As expected, pellets containing different estradiol dosages were associated with predictable plasma levels 6 weeks after implantation (Table 2). Ovariectomized mice implanted with the 1.7-mg/pellet showed blood estradiol levels of 545 ⫾ 5.3 pg/mL, whereas mice implanted with the 0.18-mg/pellet dose showed blood estradiol at the physiological level of 82 ⫾ 1.4 pg/mL. Based on the presumption that a higher concentration of estradiol would provide better regulation of MMP-2 in the RPE and vascular protective effects, we evaluated the capacity of a 1.7-mg dose in preventing sub-RPE deposits. Mice receiving implantation of high-dose pellets unexpectedly showed development of BLDs that were only slightly less severe than those in ovariectomized mice without estrogen (4.9 ⫾ 3.6 in estrogen-supplemented mice versus 5.6 ⫾ 3.2 in estrogen-depleted mice; Fig. 3, bottom right). In general, the qualitative features were identical. However, BrM appeared thinner in estrogensupplemented mice (12.7 ⫾ 7.5 in supplemented mice versus 20.7 ⫾ 4.1 in ovariectomized mice; Table 3). Effect of Estrogen Depletion and Supplementation in RPE Expression of MMP-2 Estrogen replacement may have failed to protect against formation of deposits after ovariectomy for at least two reasons: First, estrogen replacement alone may not be sufficient, because other ovarian hormones contribute to protection from deposit accumulation. Second, estrogen may demonstrate a paradoxical bimodal dose effect on RPE production of molecules that may influence the turnover of the RPE basement membrane and other extracellular matrix molecules. Previously, we have shown that superphysiologic concentrations of estradiol failed to increase production of MMP-2 in cultured human RPE compared with the two- to threefold increase in activity induced by physiologic concentrations.17 We sought to determine whether a bimodal response in the regulation of MMP-2 activity was evident in RPE of ovariectomized mice, with and without estrogen replacement. RPE were isolated from eyecups of mouse eyes in five groups of 9-month-old female mice: ovary intact, after ovariectomy, or after estrogen replacement with low-, moderate-, or 1226 Cousins et al. IOVS, March 2003, Vol. 44, No. 3 FIGURE 3. TEM of the outer retina and choroid from fat-fed, blue-green light– exposed 9-month-old female mice undergoing sham surgery (ovary-intact), ovariectomy alone, or ovariectomy with estrogen replacement. Top left: specimen from a middle-aged sham-surgery (ovary-intact) female mouse revealed minimal subRPE deposits and minimally thickened BrM. The choriocapillaris (CC) appeared normal. Top right: specimen from a middle-aged ovariectomized mouse reveals moderately thick continuous BLD (under white dotted line) with banded structure (white asterisk), irregular thickening of BrM, and normal choriocapillaris. Marked thickening and reduplication of the basement membrane was evident (black asterisks). Bottom left: another specimen from an ovariectomized mouse revealed nodular BLDs and irregularly thickened BrM. The endothelium appeared hypertrophied (white asterisk) with irregular protrusions into BrM, loss of fenestrations (open white arrowheads), and reduplication of the basement membrane (black asterisk). No invasive processes were observed. Bottom right: specimen from an ovariectomized mouse with estrogen replacement revealed moderately thick BLD (under white dotted line) of severity similar to that in the ovariectomized mice with banded structures (white asterisk). However, BrM appeared to be normally compact and the endothelium was normal. Magnification, ⫻25,000. high-dose estrogen-containing pellets for 6 weeks. Protein was extracted and gelatin zymography for MMP-2 activity and Western blot for detection of latent MMP-2 protein was performed. Female 9-month mice demonstrated significant MMP-2 activity and expression of latent protein (Figs. 4, 5). By comparison, ovariectomized mice demonstrated 70% loss of MMP-2 activity. TABLE 3. Effect of Estrogen Depletion or Supplementation on Deposit Severity in 9-Month-Old Mice Group n Frequency of Any BLD (%) Ovary intact Ovariectomized Supplemental estrogen 6 5 7 100 100 71 Frequency of “Moderate” BLD (%) Mean Severity Score (15 max.) Mean Bruch’s Membrane Thickness 0 60* 71† 1.8 ⫾ 1.3 5.6 ⫾ 3.2‡ 4.9 ⫾ 3.6§ 16.5 ⫾ 3.4 20.7 ⫾ 4.1㛳 12.7 ⫾ 2.5¶ Frequencies of BLD are as described in Table 1. * P ⫽ 0.02 versus ovary intact (2 test). † P ⫽ 0.008 versus ovary intact (2 test). ‡ P ⫽ 0.023 versus ovary intact. § P ⫽ 0.07 versus ovary intact; P ⫽ NS versus ovariectomy. 㛳 P ⫽ ns versus ovary intact. ¶ P ⫽ 0.039 versus ovary intact; P ⫽ 0.002 versus ovariectomy. IOVS, March 2003, Vol. 44, No. 3 FIGURE 4. RPE-derived MMP-2 activity. Protein was extracted from RPE of seven pairs of eyes in each group and the left and right eye pooled from groups of mice treated by sham ovariectomy (ovary intact), ovariectomy (O) without estrogen, or ovariectomy with 17estradiol replacement: high (1.7 mg/pellet), moderate (0.36 mg/pellet), or low (0.18 mg/pellet) dose. Top: gelatin zymogram from a representative experiment. Bottom: data are the average of results in seven pairs of eyes. **Significant difference (P ⬍ 0.01) compared with the sham-surgery control. A striking dose effect on activity of MMP-2 was observed in the estrogen-supplemented groups. Mice receiving the high-dose supplement demonstrated low MMP-2 activity with similar levels as observed in the ovariectomized mice without supplement. However, mice receiving the lowest-dose implants (reproducing physiologic blood estrogen concentration) demonstrated MMP-2 levels similar to the ovary-intact mice. DISCUSSION Estrogens are a large family of chemically related steroid compounds produced mainly by the ovary but can also result from testosterone metabolism and extragonadal production. 17Estradiol is the main estrogen produced by the ovary. Since the discovery of ERs in nearly every tissue, estrogen has been considered to be a powerful regulator of many biological processes. In particular, estrogen has been implicated as a regulatory factor in many chronic degenerative and vascular diseases, including Alzheimer’s disease,26 atherosclerosis, 27,28 and renal glomerulosclerosis.12 A large body of literature of retrospective and observational research has suggested that estrogen status influences progression of disease: Female gender and late onset of menopause are beneficial, estrogen depletion by menopause or oophorectomy is associated with increased risk of disease progression, and hormone replacement therapy (HRT) seems to be protective. ARMD is characterized by the accumulation of various lipidrich deposits and progressive thickening in BrM.29 Several observational studies have suggested that estrogens protect women from the development of ARMD,3 and estrogen replacement therapy is currently being studied in a large clinical trial for the prevention of ARMD. However, our knowledge regarding the actions of estrogens in RPE, a crucial target tissue in the progression of ARMD is limited. In these experiments, we evaluated the effect of age, gender, and estrogen status in the regulation of severity of sub-RPE Estrogen and Experimental BLD 1227 deposits and in RPE expression of MMP-2. These studies confirm our previous findings that older age renders mice susceptible to high-fat diet-induced formation of deposits, especially in response to blue-green laser light. The changes include sub-RPE deposits (i.e., BLD), thickening of BrM and endothelial invasion. In the current study, old (16 months) female mice had more severe sub-RPE deposits and endothelial changes to the choriocapillaris than did age-matched male mice. Certainly other factors associated with ovariectomy and postmenopause, other than estrogen depletion, could contribute to the formation of BLD. We also showed that estrogen deficiency may increase the susceptibility of middle-aged (9 months) female mice to formation of sub-RPE deposits, because ovariectomy was associated with more severe collagenous thickening, accumulation of deposits, and endothelial changes than were observed in ovaryintact control animals. High-dose estrogen replacement did not prevent the onset of formation of deposits, although less BrM thickening was observed. The explanation for this lack of protection against formation of deposits may be that estrogen exerts a bimodal dose response on RPE MMP-2 activity and protein expression, as we observed in vitro in cultured human RPE cells. Ovariectomy to cause subphysiologic blood estrogen levels or high-dose replacement to induce superphysiologic estrogen concentration was associated with diminished activity of MMP-2 in the RPE. Normal estrogen levels in 9-month-old mice or replacement with exogenous estradiol to reproduce physiologic blood estrogen concentrations, correlated with higher RPE MMP-2 activity. Thus, loss of MMP-2 activity in the RPE correlated with development of deposits, suggesting that regulation of the extracellular matrix by MMP-2 may play a role in the pathogenesis of deposits. In the mouse model, choriocapillaris endothelial changes, including hypertrophy, loss of fenestration, reduplication of the endothelial basement membrane, and possible cellular invasion into BrM, were an important feature in some aged and ovariectomized female mice. Abnormal regulation of ECM turnover by “injured” endothelial cells in the absence of estrogen is possibly another component in this model. In a preliminary experiment not shown, the choroidal MMP-2 response to estrogen depletion and replacement appeared to be similar to FIGURE 5. RPE-derived MMP-2 protein. Protein was extracted from RPE as described in Figure 4. Top: Western blot from a representative experiment. Bottom: data are the average of results in seven pairs of eyes. **Significant difference (P ⬍ 0.01) compared with the shamsurgery control. 1228 Cousins et al. that observed in the RPE. Nevertheless, the choroidal specimens processed for this study contained a wide range of heterogeneous cell types in addition to the choriocapillaris endothelial cells, including pericytes, macrophages, melanocytes, and others. Thus, much more thorough analysis of regulation of choroidal ECM is required to draw any meaningful conclusions. 17-Estradiol can influence cell biology in several important areas, especially as gene regulators through activation of two nuclear receptors and as antioxidants.26,30 –33 Extracellular estrogen directly permeates cell membranes to enter the cytosol. Estrogen mediates its actions through two nuclear receptors ER␣ and ER, which on binding their ligand in the cytoplasm, translocate into the nucleus, becoming transcription factors to modulate gene expression.26,34,35 ERs can influence AP-1– dependent, NF-– dependent, and other transcriptional regulation.30,31,33 Although ERs generally inhibit transcriptional functions, many cell-specific differences have been noted, and each cell type must be independently evaluated. Additional complexity is introduced by injury-dependent and concentration-dependent changes in expression of ER, as well as interactions between ER␣ and ER, all of which can lead to positive or negative feedback that profoundly alters estrogen activity.26,36,37 In general, ER activation usually prevents dysregulated production of matrix molecule expression in response to injury or hormonal stimulation (e.g., in vascular smooth muscle cells within the glomerulus or coronary artery), but many cellspecific exceptions have been noted. In several tissues, estrogens have been shown to modulate the expression and activity of molecules important for turnover of ECM, including MMP2.8,10,11,38 MMP-2 has type IV collagenolytic activity but also cleaves type I, V, VII, and XI collagens as well as laminin. Because many of these molecules are part of BrM39 – 41 and BLD,42 altered production or activity of MMP-2 may influence accumulation of deposits, collagenous thickening, and biochemical function of BrM. Estrogen-mediated regulation of RPE genes important for matrix turnover may be a potential mechanism by which estrogens exert their protective effects against ARMD. Estrogens can also function as antioxidants,27 a property not investigated in this study. Two recent prospective studies evaluating the putative protective benefit of HRT in coronary artery disease in women have raised the issue of an “estrogen paradox.”43,44 Estrogen depletion has been confirmed to increase risk for cardiovascular events, but estrogen replacement therapy with conventional modalities (sustained levels of high physiologic concentrations rather than the natural cyclic, fluctuating levels) was not found to be protective.43– 46 Prospective studies are currently ongoing in other diseases as well. However, at least in coronary artery disease, the paradox presented is that estrogen depletion is harmful, but conventional replacement is not necessarily beneficial to those women predisposed to cardiac disease.46 Our results may reflect on this paradox by suggesting a strong concentration-dependent difference in the regulation of MMP expression: Physiologic concentrations of estrogen, but not sub- or superphysiologic levels, upregulated MMP-2 activity (and probably many other molecules). Studies are underway to confirm and extend these observations in vitro.17 Also, we intend to perform in vivo studies to evaluate different doses of estrogen and their impact on RPE and choriocapillaris ECM production. We expect that these and similar studies will assist in testing a hypothetical model for early formation of deposits in ARMD. We propose that initial oxidant injury to the RPE causes the formation of extruded RPE cell membrane blebs, which in association with downregulation of MMP-2, accumulate between the RPE and its basement membrane as part of BLDs. IOVS, March 2003, Vol. 44, No. 3 Estrogen reduction may promote this process by loss of estrogen signaling through the ERs, which may lead to downregulation of MMP-2, a major gelatinase responsible for degradation of type IV collagen, to cause thickening of the RPE basement membrane as well as collagenous thickening of BrM. In support of this model, we have observed that cultured human RPE, exposed to mild, sublethal oxidant injury, develop cell membrane blebs and downregulation of MMP-2 activity.47,48 Similar mechanisms may be responsible for choriocapillaris endothelial injury as well. Studies are under way to confirm these observations in vitro and in vivo. References 1. Berger JW, Fine SL, Maguire MG. Age-Related Macular Degeneration. St. Louis: Mosby; 1999. 2. Green WR. Histopathology of age-related macular degeneration. Mol Vis. 1999;5:27. 3. Risk factors for neovascular age-related macular degeneration. The Eye Disease Case-Control Study Group. Arch Ophthalmol. 1992; 110:1701–1708. 4. U. S. Renal Date System: USRDS 1997 Annual Data Report. Bethesda, MD: The National Institute of Health, Diabetes and Digestive and Kidney Disease; 1997. 5. Nathan L, Chaudhuri G. Estrogens and atherosclerosis. Annu Rev Pharmacol Toxicol. 1997;37:477–515. 6. Snow KK, Seddon JM. Age-related eye diseases: impact of hormone replacement therapy, and reproductive and other risk factors. Int J Fertil Women Med. 2000;45:301–313. 7. Klein BE, Klein R, Lee KE. Reproductive exposures, incident agerelated cataracts, and age-related maculopathy in women: the Beaver Dam Eye Study. Am J Ophthalmol. 2000;130:322–326. 8. Vingerling JR, Dielemans I, Witteman JC, Hofman A, Grobbee DE, De Jong PT. Macular degeneration and early menopause: a casecontrol study. BMJ. 1995;310:1570 –1571. 9. Smith W, Mitchell P, Wang JJ. Gender, oestrogen, hormone replacement and age-related macular degeneration: results from the Blue Mountains Eye Study. Aust NZ J Ophthalmol. 1997;25(suppl 1):S13–S15. 10. Puistola U, Westerlund A, Kauppila A, Turpeenniemi-Hujanen T. Regulation of 72-kd type IV collagenase-matrix metalloproteinase-2 by estradiol and gonadotropin-releasing hormone agonist in human granulosa-lutein cells. Fertil Steril. 1995;64:81– 87. 11. Sato T, Ito A, Mori Y, Yamashita K, Hayakawa T, Nagase H. Hormonal regulation of collagenolysis in uterine cervical fibroblasts: modulation of synthesis of procollagenase, prostromelysin and tissue inhibitor of metalloproteinases (TIMP) by progesterone and oestradiol-17 beta. Biochem J. 1991;275:645– 650. 12. Potier M, Elliot SJ, Tack I, et al. Expression and regulation of estrogen receptors in mesangial cells: influence on matrix metalloproteinase-9. J Am Soc Nephrol. 2001;12:241–251. 13. Silbiger S, Lei J, Neugarten J. Estradiol suppresses type I collagen synthesis in mesangial cells via activation of activator protein-1. Kidney Int. 1999;55:1268 –1276. 14. Atkinson SJ, Patterson ML, Butler MJ, Murphy G. Membrane type 1 matrix metalloproteinase and gelatinase A synergistically degrade type 1 collagen in a cell model. FEBS Lett. 2001;491:222–226. 15. Deryugina EI, Bourdon MA, Reisfeld RA, Strongin A. Remodeling of collagen matrix by human tumor cells requires activation and cell surface association of matrix metalloproteinase-2. Cancer Res. 1998;58:3743–3750. 16. Zhuge Y, Xu J. Rac1 mediates type I collagen-dependent MMP-2 activation: role in cell invasion across collagen barrier. J Biol Chem. 2001;276:16248 –16256. 17. Marin-Castaño ME, Elliot SJ, Potier M, et al. Regulation of estrogen receptors and MMP-2 expression by estrogens in human retinal pigment epithelium. Invest Ophthalmol Vis Sci. 2003;44:50 –59. 18. Cousins SW, Espinosa-Heidmann DG, Alexandridou A, Sall J, Dubovy S, Csaki K. The role of aging, high fat diet and blue light exposure in an experimental mouse model for basal laminar deposit formation. Exp Eye Res. 2002;75:543–553. IOVS, March 2003, Vol. 44, No. 3 19. Hernandez E, Alexandridou A, Sall J, Csaky KG, Cousins SW. Relationship between plasma lipidemia and basal laminar deposit (BLD) formation in the mouse [ARVO Abstract]. Invest Ophthalmol Vis Sci. 2000;41(4):S160. Abstract nr 826. 20. Hernandez E, Morales P, Sierra P, Rubsamen P, Csaky KG, Cousins SW. A mouse model for RPE injury based on blue light exposure [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1998;39(4):S392. Abstract nr 1829. 21. Alexandridou A, Sall J, Hernandez E, Dix R, Csaky KG, Cousins SW. Age increases susceptibility of normal mice to polyunsaturated fat induced RPE injury [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1999;40(4):S921. Abstract nr 4829. 22. Hernandez E, Sall J, Alexandridou A, Dix R, Csaky KG, Cousins SW. Polyunsaturated fat increases RPE susceptibility to lipid peroxidation: a mechanism for BLD formation [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1999;40(4):S927. Abstract nr 4893. 23. Alexandridou A, Sall J, Hernandez E, Csaky KG, Cousins SW. Susceptibility of mice to basal laminar deposit (BLD) formation: role of aging and blue light exposure [ARVO Abstract]. Invest Ophthalmol Vis Sci. 2000;41(4):S160. Abstract nr 827. 24. Dithmar S, Sharara N, Curcio C, et al. Murine high-fat diet and laser photochemical model of basal deposits in Bruch’s membrane. Arch Ophthalmol. 2001;119:1643–1649. 25. Elliot SJ, Striker LJ, Stetler-Stevenson WG, Jacot TA, Striker GE. Pentosan polysulfate decreases proliferation and net extracellular matrix production in mouse mesangial cells. J Am Soc Nephrol. 1999;10:62– 68. 26. Behl C, Skutella T, Lezoualc’h F, et al. Neuroprotection against oxidative stress by estrogens: structure-activity relationship. Mol Pharmacol. 1997;51:535–541. 27. Speir E, Yu ZX, Takeda K, Ferrans VJ, Cannon RO, III. Antioxidant effect of estrogen on cytomegalovirus-induced gene expression in coronary artery smooth muscle cells. Circulation. 2000;102: 2990 –2996. 28. Buko VU, Lukivskaya O, Naruta E, et al. Antiatherogenic effects of 17 beta-estradiol and 17 alpha-estradiol and its derivative J811 in cholesterol-fed rabbits with thyroid inhibition. Climacteric. 2001; 4:49 –57. 29. Abdelsalam A, Del Priore L, Zarbin MA. Drusen in age-related macular degeneration: pathogenesis, natural course, and laser photocoagulation-induced regression. Surv Ophthalmol. 1999;44:1– 29. 30. Evans MJ, Eckert A, Lai K, Adelman SJ, Harnish DC. Reciprocal antagonism between estrogen receptor and NF-kappaB activity in vivo. Circ Res. 2001;89:823– 830. 31. Guccione M, Silbiger S, Lei J, Neugarten J. Estradiol upregulates mesangial cell MMP-2 activity via the transcription factor AP-2. Am J Physiol Renal Physiol. 2002;282:F164 –F169. 32. Hsu SM, Chen YC, Jiang MC. 17 beta-estradiol inhibits tumor necrosis factor-alpha-induced nuclear factor-kappa B activation by increasing nuclear factor-kappa B p105 level in MCF-7 breast cancer cells. Biochem Biophys Res Commun. 2000;279:47–52. 33. Maruyama S, Fujimoto N, Asano K, Ito A. Suppression by estrogen receptor beta of AP-1 mediated transactivation through estrogen receptor alpha. J Steroid Biochem Mol Biol. 2001;78:177–184. Estrogen and Experimental BLD 1229 34. Tremblay GB, Tremblay A, Copeland NG, et al. Cloning, chromosomal localization, and functional analysis of the murine estrogen receptor beta. Mol Endocrinol. 1997;11:353–365. 35. White R, Lees JA, Needham M, Ham J, Parker M. Structural organization and expression of the mouse estrogen receptor. Mol Endocrinol. 1987;1:735–744. 36. Borras M, Hardy L, Lempereur F, et al. Estradiol-induced downregulation of estrogen receptor: effect of various modulators of protein synthesis and expression. J Steroid Biochem Mol Biol. 1994;48:325–336. 37. Vladusic EA, Hornby AE, Guerra-Vladusic FK, Lakins J, Lupu R. Expression and regulation of estrogen receptor beta in human breast tumors and cell lines. Oncol Rep. 2000;7:157–167. 38 Miyamoto N, Mandai M, Suzuma I, Suzuma K, Kobayashi K, Honda Y. Estrogen protects against cellular infiltration by reducing the expressions of E-selectin and IL-6 in endotoxin-induced uveitis. J Immunol. 1999;163:374 –379. 39. Campochiaro PA, Jerdon JA, Glaser BM. The extracellular matrix of human retinal pigment cells in vivo and its synthesis in vitro. Invest Ophthalmol Vis Sci. 1986;27:1615–1621. 40. Karwatowski WS, Jeffries TE, Duance VC, Albon J, Bailey AJ, Easty DL. Preparation of Bruch’s membrane and analysis of the agerelated changes in the structural collagens. Br J Ophthalmol. 1995;79:944 –952. 41. Newsome DA, Pfeffer BA, Hewitt AT, Robey PG, Hassel JR. Detection of extracellular matrix molecules synthesized in vitro by monkey and human retinal pigment epithelium: influence of donor age and multiple passages. Exp Eye Res. 1988;46:305–321. 42. Van der Schaft TL, Mooy CM, de Bruijin WC, Bosman FT, de Jong PT. Immunohistochemical light and electron microscopy of basal laminar deposit. Graefes Arch Clin Exp Ophthalmol. 1994;232: 40 – 46. 43. Herrington DM, Reboussin DM, Klein KP, et al. The estrogen replacement and atherosclerosis (ERA) study: study design and baseline characteristics of the cohort. Control Clin Trials. 2000; 21:257–285. 44. Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women: Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA. 1998;280:605– 613. 45. Herrington DM, Fong J, Sempos CT, et al. Comparison of the Heart and Estrogen/Progestin Replacement Study (HERS) cohort with women with coronary disease from the National Health and Nutrition Examination Survey III (NHANES III). Am Heart J. 1998; 136:115–124. 46. Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288:321–333. 47. Csaky KG, Cousins SW. Membrane blebbing in retinal pigment epithelial (RPE) cells: differentiating between injury stimuli and regulatory cofactors [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1999;40(4):S223. Abstract nr 1180. 48. Monroy D, Marin-Castaño ME, Striker LJ,et al. RPE expression of matrix metalloproteinase (MMP-2) and MCP-1 after different kinds of injury [ARVO Abstract]. Invest Ophthalmol Vis Sci. 2001;42(4): S758. Abstract nr 4060.