Intrinsic positive end-expiratory pressure in
advertisement

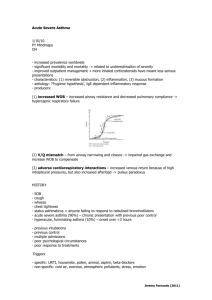
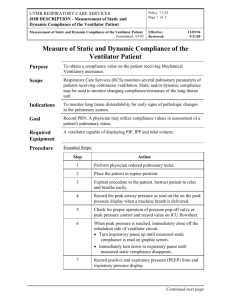
Intrinsic positive end-expiratory pressure in mechanically ventilated patients with and without tidal expiratory flow limitation Apostolos Armaganidis, MD; Krystallia Stavrakaki-Kallergi, MD; Antonia Koutsoukou, MD; Andreas Lymberis, PhD; Joseph Milic-Emili, MD; Charis Roussos, MD, PhD Objective: To assess static intrinsic positive end-expiratory pressure (PEEPi,st) and expiratory flow limitation (FL) in 32 consecutive mechanically ventilated patients with acute respiratory failure (ARF), using a commercial ventilator with an incorporated device that allows the application of a negative expiratory pressure (NEP). Design: Prospective clinical study. Setting: Multidisciplinary intensive care unit of a university hospital. Patients: Thirty-two consecutive ventilated patients with ARF of various etiologies. Interventions: Evaluation of respiratory mechanics, PEEPi,st, and FL from pressure, flow, and volume traces provided by the ventilator. Measurements: Peak airway pressure, PEEPi,st, dynamic elastance, and interrupter resistance were measured in relaxed patients in a supine position. Comparison of tidal flow–volume curves before and during the application of an NEP of 5 cm H2O was used to assess tidal expiratory FL. Results: Twelve of 32 patients studied exhibited tidal expiratory FL, which was detected by the absence of increase in A lthough static intrinsic positive end-expiratory pressure (PEEPi,st) and dynamic hyperinflation (DH) have been reported for patients with airway obstruction as early as 1975 (1), widespread From the Critical Care Department (Drs. Armaganidis, Stavrakaki, Koutsoukou, Lymberis, and Roussos), Evangelismos General Hospital, Medical School of Athens University, Greece; and the Meakins– Christie Laboratories (Dr. Milic–Emili), McGill University, Montreal, Quebec, Canada. Supported, in part, by a grant from the Thorax Foundation, Athens, Greece. Draegerwork A.G., Lübeck, Germany, and their distributor in Greece, N. Papapostolou LTD, provided the Draeger Evita 2 ventilator equipped with an NEP device for assessment of expiratory FL. Address reprint requests to: Apostolos Armaganidis, MD, Critical Care Department, Medical School of Athens University, Evangelismos General Hospital, Ipsilantou 45– 47, Athens 106 75, Greece. Copyright © 2000 by Lippincott Williams & Wilkins Crit Care Med 2000 Vol. 28, No. 12 expiratory flow despite application of an NEP over the entire or part of the baseline expiratory flow–volume curve. All patients exhibited PEEPi,st, which amounted to 1.2 ⴞ 0.9 cm H2O (mean ⴞ SD) in the 20 non-FL patients and 7.1 ⴞ 2.8 cm H2O in the 12 FL patients (p < 0.00001). The majority of patients with ARF resulting from underlying lung disease (11 of 13) had FL and a PEEPi,st > 4 cm H2O, whereas in patients with ARF of extrapulmonary origin, PEEPi,st was always < 4 cm H2O and only one grossly obese patient exhibited FL. Based on multiple regression analysis, in non-FL patients, PEEPi,st correlated significantly only with minute ventilation, whereas in FL patients PEEPi,st correlated significantly with peak airway pressure. Conclusions: Because all the patients exhibited PEEPi,st and 12 of 32 patients (38%) also had FL, the authors conclude that the assessment of these variables at the bedside could provide useful information concerning respiratory mechanics in mechanically ventilated patients. (Crit Care Med 2000; 28:3837–3842) KEY WORDS: expiratory flow limitation; mechanical ventilation; intrinsic positive end-expiratory pressure; respiratory mechanics; negative expiratory pressure; ventilator; flow–volume curves; dynamic hyperinflation; resistance; elastance interest in this topic started in the 1980s (2– 4). Since then it has been recognized that PEEPi,st (measured by an expiratory hold maneuver) and DH promote an increase in inspiratory work, impairment of inspiratory muscle function, and adverse effects on hemodynamics. DH and PEEPi,st contribute to dyspnea (5, 6), are the main cause of ventilatory failure (7, 8), and exercise limitation (9) in patients with chronic obstructive pulmonary disease (COPD). The fact that in COPD patients tidal expiratory flow limitation (FL) plays a major role in eliciting DH was first suggested by Hyatt (10). This was based on his observation that at-rest patients with severe COPD often breathe tidally along their maximal flow–volume curve. This approach to detect FL requires the use of a body plethysmograph (11) and hence it cannot be used in mechanically ventilated patients. Further- more, there are other factors that make assessment of tidal FL based on comparison of tidal and maximal flow–volume (V̇–V) curves problematic (12). Recently, however, an alternative technique, the negative expiratory pressure (NEP) method, has been introduced to detect FL during tidal breathing. This technique is reliable and does not require body plethysmography (13). Furthermore, this method can be used in mechanically ventilated patients (13). With NEP it has been documented that in both spontaneously breathing (6) and mechanically ventilated (13) COPD patients, PEEPi,st and DH are mainly the result of the presence of tidal FL. DH and PEEPi,st are also common in patients with adult respiratory distress syndrome (7, 14, 15) and cardiogenic pulmonary edema (CPE) (7). It is not known, however, if in these instances DH and 3837 PEEPi,st are associated with FL. Indeed, DH and PEEPi,st may also occur in the absence of FL: A high expiratory resistance (resulting from underlying disease and from the endotracheal tube and expiratory circuitry of the ventilator) may impede expiration such that the next mechanical inspiration occurs before complete exhalation to the elastic equilibrium (relaxation volume) of the respiratory system (16). The ventilatory settings of the ventilator (e.g., high inspiratory-toexpiratory time ratio, high ventilation) may also elicit PEEPi,st and DH in the absence of tidal FL (4, 17). In the current investigation we assessed PEEPi,st by occluding the airway at end-expiration and FL using the NEP technique (13) in 32 consecutive patients who required mechanical ventilation for different etiologies. Our hypothesis was (1) that we could demonstrate FL in most mechanically ventilated patients with underlying airway or parenchymal lung disease but not in patients without lung disease and (2) that PEEPi,st should be higher in patients with lung disease as a result of FL. MATERIALS AND METHODS Patients. Thirty-two consecutive patients admitted to the department of intensive care of Athens University Medical School and who required mechanical ventilation for different etiologies were recruited for the study. Their anthropometric characteristics, baseline blood gases, and etiology are presented in Table 1. Patients were studied within 48 hrs from admission, after respiratory and hemodynamic stability had been achieved. The research protocol was approved by the ethics committee of our institution, and informed consent was obtained from the patient or next of kin. Patients were intubated (Portex cuffed endotracheal tube with an internal diameter of 7.5–9 mm; Portex Limited, Kent, UK) and mechanically ventilated on control mode with constant inspiratory flow with a Draeger-Evita 2 respirator (Draeger, Lübeck, Germany) equipped with an NEP device attached to the distal end of the expiratory circuit of the ventilator (i.e., after the expiratory valve). During the experiments the humidifier was omitted from the ventilator circuit. The respirator set- tings (Table 2) and inspired oxygen fraction (FIO2) were selected by the primary physicians according to their clinical judgment, and no changes were made before or during the study. The inspiratory flow amounted to 0.85 ⫾ 0.13 L/sec (mean ⫾ SD) and the duty cycle (inspiratory time/total cycle duration [TI/TTOT]) was 0.33 (ratio of inspiration to expiration, 1:2) in all but two patients (0.44 L/sec and 0.50 L/sec in Patients 8 and 23 respectively). All patients were sedated with midazolam, and some of them were paralyzed with pancuronium bromide at the discretion of their primary physician. No patient was sedated or paralyzed because of our protocol. Airway pressure (Paw), flow (V̇), and volume (V) were measured with the pressure transducers and flowmeters built into the ventilator used. Built-in software was used to monitor these variables on an Evita Screen (Draeger) and to obtain on-line records of the time course of Paw, V̇, and V, as well as the V̇–V loops before and during the application of NEP. The Paw, V̇, and V signals were also stored at 125 Hz on an IBM-compatible personal computer (Turbo X; Plaisio Computers, Athens, Greece) interfaced with a homemade data acquisition program based on Test Point Table 1. Anthropometric characteristics, blood gases, tidal expiratory flow limitation, static PEEPi, and diagnosis of patients Patient No. Age yr Sex Height cm Weight kg PaO2 mm Hg PaCO2 mm Hg FIO2 FL % VT PEEPi,st cm H2O Diagnosis 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 65 73 78 65 78 63 75 20 84 70 70 58 83 55 18 30 77 30 25 26 21 63 30 55 70 68 77 75 69 70 67 58 F F M M F F M M M F M M M M M M M F M M F F F M F M M M M M M M 162 162 175 170 160 162 175 180 178 153 170 168 175 178 170 175 180 160 170 175 160 158 158 175 158 175 168 170 175 170 170 170 78 80 78 130 85 80 90 90 80 60 70 70 85 130 70 88 78 60 75 75 68 55 60 78 55 80 70 75 80 75 75 75 83 151 107 80 111 60 69 215 162 93 119 99 99 188 124 193 130 203 180 251 254 135 102 168 89 88 107 165 94 140 144 124 32 63 39 55 36 38 44 42 55 39 40 42 36 29 30 26 35 25 25 29 25 34 22 42 39 35 32 34 33 40 37 31 0.55 0.45 0.70 0.75 0.45 0.80 0.70 0.60 0.60 0.60 0.60 0.60 0.55 0.50 0.60 0.50 0.55 0.40 0.60 0.50 0.50 0.40 0.35 0.50 0.50 0.55 0.70 0.60 0.55 0.45 0.65 0.60 52 48 75 57 68 11 14 23 28 51 84 0 0 17 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 5.2 7.7 8.7 4.3 12.6 8.8 5.0 7.7 8.3 9.3 4.4 1.6 2.5 2.8 3.3 1.2 0.9 0.2 0.5 0.4 0.4 0.2 1.0 0.9 1.2 1.0 2.7 1.7 2.2 0.5 0.9 0.4 COPD COPD COPD COPD, obesity, sleep apnea Pulmonary embolism, asthma Pneumonia, asthma Aspiration pneumonia, atelectasis Aspiration pneumonia, head trauma Myasthenia, pneumonia Pulmonary edema, pleural effusions Cardiosurgery, pneumonia Pneumonia, diabetic coma Cardiogenic pulmonary edema Obesity, sepsis, abdominal surgery Head trauma, atelectasis Head trauma Head trauma Head trauma Head trauma Head trauma Head trauma Brain tumor Brain tumor Intracerebral hematoma Polyneuropathy Myasthenia Septic shock Ketoacidosis, renal failure Abdominal surgery, sepsis Abdominal surgery Thoracic empyema Hemothorax F, female; M, male; FL, tidal expiratory flow limitation; PEEPi,st, intrinsic static positive end-expiratory pressure; COPD, chronic obstructive pulmonary disease. 3838 Crit Care Med 2000 Vol. 28, No. 12 software (version 3, Capital Equipment, Billerica, MA) for subsequent replay and assessment of respiratory mechanics. Arterial blood gases were measured with an ABL System 610 blood gas analyzer (Radiometer, Copenhagen, Denmark) during baseline ventilation. Heart rate, systemic arterial blood pressure, and arterial O2 saturation were monitored continuously (Life Scope 14; Nihon Kohden, Tokyo, Japan). Patients were studied in the supine position at a zero positive end-expiratory pressure (PEEP) setting on the ventilator. At this setting the ventilator actually applies a PEEP of 0.8 cm H2O. The latter was subtracted from total PEEP to obtain PEEPi,st. Patient relaxation during the experiments was evidenced by uniform sequential recordings of Paw, V̇, and V, and absence of negative deflections in Paw or other visible signs of spontaneous breathing efforts. In each subject respiratory mechanics, PEEPi,st, and expiratory FL were assessed as described in the following sections. Respiratory Mechanics and PEEPi,st. The total interrupter resistance (Rint) was measured by occluding the airway at end-inspiration, as described previously in detail (7, 18). Briefly, Rint was obtained using the following equation: Rint ⫽ (Ppeak ⫺ P1)/V̇I (1) where Ppeak ⫺ P1 is the immediate drop in P aw from peak value (Ppeak) to P1 on cessa- tion of inspiratory flow and V̇I is the flow immediately preceding the airway occlusion (Fig. 1). The dynamic elastance of the respiratory system (Edyn,rs), which reflects the pressure dissipation resulting from elastic recoil, viscoelastic behavior, and time constant inequality (17, 18), was obtained by the following equation: Edyn,rs ⫽ (P1 ⫺ PEEPi,dyn)/VT (2) where dynamic instrinsic PEEP (PEEPi,dyn) was the Paw indicated on the Evita Screen (Fig. 1) when the cursor was placed at the onset of inspiratory flow. Respiratory mechanics variables were measured on three subsequent breaths, and the mean values were used for subsequent analysis. PEEPi,st was obtained by occluding the airway at end-expiration using the endexpiratory hold button of the respirator (2, 4, 7). When this button is activated, both inspiratory and expiratory valves are closed for a time corresponding to the inspiratory time set on the ventilator. Because 3 sec of end-expiratory occlusion are required for accurate measurement of PEEPi,st (8), 3 to 4-sec occlusions were achieved by decreasing the frequency of the respirator to 6 cpm immediately after activation of the end-expiratory hold button (Fig. 1). At least two end-expiratory occlusion maneuvers were performed, and the mean PEEPi,st value was used for subsequent analysis. The total inspiratory work (WI) per breath was obtained by integration of Paw with respect to inspiratory volume during baseline ventilation. The WI included the total work done on the respiratory system and the resistive work resulting from the endotracheal tube. The work resulting from PEEPi,st was obtained as a product of PEEPi,st and VT. Work was also expressed per liter of inspired volume (WI/VT). With constant flow inflation, WI/VT corresponds to mean inspiratory pressure (8). Flow Limitation. Expiratory FL was assessed using the NEP technique (13). The NEP device incorporated into the Evita 2 ventilator applies an NEP of ⫺5 cm H2O 8 msec after the onset of expiratory flow, and maintains it throughout the expiratory time set on the ventilator. However, NEP is discontinued automatically if there is occurrence of spontaneous inspiratory efforts, as evidenced by inspiratory flow during the expiratory time of the ventilator. The NEP device is activated by pressing a special button on the ventilator during inspiration—a maneuver not seen by the patient. Using the built-in software in the Evita Screen, the V̇–V loop of the breath with NEP was superimposed on that of the preceding control breath. The end-expiratory volume was reset automatically after each expiration, Table 2. Anthropometric characteristics, blood gases, ventilatory settings, and respiratory mechanics data of FL and non-FL patients Parameter Sex, M/F Age, yr Height, cm Weight, kg FIO2 PaO2, mm Hg PaCO2, mm Hg pH V̇E, L/min VT, mL fR, breaths/min TI, sec TP, sec TE, sec TL:TTOT Ppeak, cm H2O PEEPi,st, cm H2O Edyn,rs, cm H2O/mL Rint,rs, cm H2O/L/sec WI,rs, cm H2O/L WI,rs/VT, cm H2O FL (n ⫽ 12) Non-FL (n ⫽ 20) p Value 7/5 66 ⫾ 16 169 ⫾ 8 88 ⫾ 21 0.61 ⫾ 0.11 120 ⫾ 49 43 ⫾ 10 7.40 ⫾ 0.9 9.99 ⫾ 2.70 638 ⫾ 80 15.7 ⫾ 3.7 1.40 ⫾ 0.39 0.58 ⫾ 0.36 2.67 ⫾ 0.86 0.35 ⫾ 0.04 41.6 ⫾ 6.4 7.1 ⫾ 2.8 47.3 ⫾ 17.2 18.3 ⫾ 7.1 20.7 ⫾ 4.6 33.1 ⫾ 7.4 15/5 52 ⫾ 21 169 ⫾ 7 72 ⫾ 9 0.53 ⫾ 0.09 145 ⫾ 50 33 ⫾ 9 7.45 ⫾ 0.6 10.02 ⫾ 2.10 607 ⫾ 86 16.6 ⫾ 3.1 1.29 ⫾ 0.32 0.49 ⫾ 0.33 2.47 ⫾ 0.56 0.34 ⫾ 0.04 31.0 ⫾ 6.5 1.2 ⫾ 0.9 31.8 ⫾ 7.1 13.9 ⫾ 2.8 13.3 ⫾ 5.4 21.6 ⫾ 7.0 — NS NS ⬍0.01 NS NS ⬍0.002 NS NS NS NS NS NS NS NS ⬍0.0001 ⬍0.00001 ⬍0.002 ⬍0.02 ⬍0.0004 ⬍0.0002 FL, flow limited; Non-FL, nonflow limited; M, male; F, female; V̇E, minute ventilation; VT, tidal volume; fR, respiratory frequency; TI, inspiratory time; TP, end-inspiratory pause time; TE, expiratory time; TTOT, total cycle duration; Ppeak, peak airway pressure; PEEPi,st, intrinsic static positive end-expiratory pressure; Edyn,rs, dynamic elastance; Rint,rs, interrupter resistance; WI,rs, total inspiratory work per breath; WI,rs/VT, total inspiratory work per liter of ventilation. Values are mean ⫾ SD. Crit Care Med 2000 Vol. 28, No. 12 Figure 1. Recordings of pressure at airway opening (Paw), flow, and volume provided by the Evita screen. During the end-inspiratory pause there was a rapid drop in Paw from a peak value (Ppeak) to P1. Static, intrinsic positive end-expiratory pressure was obtained by occluding the airway at end-expiration and decreasing the frequency of the respirator to 6 cpm to obtain an occlusion time ⬎ 3 sec. Dynamic, intrinsic positive endexpiratory pressure (PEEPi,dyn) was the Paw value at the onset of inspiratory flow. PEEPi, static, intrinsic positive end-expiratory pressure; TI, inspiratory time; TP, end-inspiratory pause time; TE, expiratory time; s, seconds. 3839 and negative values of volume were not displayed by the ventilator’s software. Patients were categorized as non-FL if NEP elicited an increased flow over the entire range of the control VT, as shown in Figure 2A. In contrast, if part or the entire V̇–V curve with NEP was superimposed on the control V̇–V curve, FL was present (Fig. 2B). The extent of FL (i.e., the volume over which the flow with NEP was the same as in the preceding control expiration) was expressed as a percent of the control expired VT (FL, %VT) (13). Because all measurements were made on relaxed subjects, the mechanics data and the NEP tests were highly reproducible in repeated measurements. Statistical Analysis. Results are reported as mean ⫾ SD. The conventional level of significance (p ⬍ 0.05) was used for all analyses. Patients were divided into two groups according to the presence or absence of expiratory FL: FL and non-FL. Differences between the two groups were evaluated using the unpaired Student’s t-test. In each group, regression analysis was carried out using the least squares method, with PEEPi,st as the dependent variable, whereas the independent variables included the anthropometric characteristics, ventilator settings, and blood gas and respiratory mechanics data. The strongest significant contributors to PEEPi,st were selected by forward stepwise regression analysis to form predictive equations. All statistical analyses were performed with STATISTICA software (version 6.0, Statsoft, Tulsa, OK). RESULTS The use of NEP revealed that 20 patients were non-FL and 12 were FL. Of the latter group of patients, the FL portion of the expired volume amounted to 44 ⫾ 25% of the control VT (range, 11– 85%). PEEPi,st was present in all patients (Fig. 3), but values were significantly higher (p ⬍ 0.00001) in the FL patients (7.1 ⫾ 2.8 cm H2O; range, 2.8 –12.6 cm H2O) than in the non-FL patients (1.2 ⫾ 0.9 cm H2O; range, 0.2–3.3 cm H2O). The individual values of FL (%VT) and PEEPi,st are provided in Table 1. The anthropometric characteristics, arterial blood gases, ventilatory settings used, and respiratory mechanics data of FL and non-FL patients are shown in Table 2. Body weight, PaCO2, and all respiratory mechanics data were significantly lower in the non-FL patients. Half of the latter population had head trauma, which required therapeutic hyperventilation. According to the results of multiple regression analysis, in the non-FL patients there was a significant relation (p ⬍ 0.01) only between PEEPi,st and minute ventilation VE (Fig. 4). In the FL patients, the only significant relation was between PEEPi,st and Ppeak (Fig. 5). The linear regression equation was PEEPi,st ⫽ ⫺7.4 ⫹ 0.35 Ppeak (3) with a standard error of regression amounting to 1.6 cm H2O. DISCUSSION The main finding of the current study is that 11 of 13 patients with acute respiratory failure (ARF) resulting from pulmonary disease (Patients 1–11 in Table 1) exhibited tidal FL with PEEPi,st ⬎ 4 cm H2O. In contrast, in all 19 patients in whom ARF was of extrapulmonary origin (Patients 14 –32 in Table 1), PEEPi,st was ⬍ 4 cm H2O and tidal FL was absent, except in Patient 14, who was grossly obese. In the non-FL group of patients, a significant correlation was only found between PEEPi,st and VE (Fig. 4). In the absence of FL, the rate of passive lung deflation is determined by the elastic recoil pressure stored during the preceding lung inflation and the opposing flow resistance offered by the respiratory system (including the endotracheal tube and the expiratory circuit of the ventilator). In non-FL patients Rint,rs, which included the resistance of the endotracheal tube, was high (13.9 ⫾ 2.8 cm H2O/L/sec). Furthermore, the resistance of the expiratory circuit of ventilators is also high (13). With high resistance, the next mechanical inflation may occur before complete exhalation to the elastic equilibrium (relaxation volume) of the respiratory system with ensuing DH and PEEPi,st (4, 14). The latter is enhanced by a high VE (17). Accordingly, the finding of a significant correlation of PEEPi,st to VE is not surprising. In this connection it should be noted that our non-FL group included 10 patients with severe brain damage who were therapeutically hyperventilated (PaCO2 ⫽ 29 ⫾ 6 mm Hg) to produce cerebral vasoconstriction to decrease Figure 4. Relationship of static, intrinsic positive end-expiratory pressure (PEEPi) to minute ventilation (V E ) in nonflow-limited patients. PEEPi ⫽ ⫺1.2 ⫹ 0.24 V̇E; r ⫽ 0.56; p ⬍0.01. Figure 2. Tidal flow–volume loops of breath with negative expiratory pressure (thick lines) and preceding control breath (thin lines) in a nonflow-limited (non-FL) patient (A) and an FL (B) patient. Arrow indicates onset of FL in Patient 3. See text for further explanation. FL, flow limitation; L, liter. 3840 Figure 3. Individual and mean values of static, intrinsic positive end-expiratory pressure (PEEPi) in flow-limited (FL) and non-FL patients. Figure 5. Relationship of static intrinsic positive end-expiratory pressure (PEEPi) to peak airway pressure (Ppeak) in flow-limited patients. PEEPi ⫽ ⫺7.4 ⫹0.35 Ppeak; r ⫽ 0.82; p ⬍0.001. Crit Care Med 2000 Vol. 28, No. 12 M odern ventilators allowing on-line assess- ment of flow limitation and static intrinsic positive endexpiratory pressure could provide useful information concerning respiratory mechanics in mechanically ventilated patients. blood flow and brain water (19). In five patients with severe brain damage who were hyperventilated (PaCO2 ⫽ 30 ⫾ 4 mm Hg), Tantucci et al. (20) also observed a high flow resistance, which they attributed to bronchoconstriction. In our 10 patients with brain damage, Rint,rs amounted to 13.1 ⫾ 3.3 cm H2O/L/sec. In the other 10 non-FL patients, PaCO2 was 36 ⫾ 4 mm Hg but Rint,rs was also high (14.8 ⫾ 1.9 cm H2O/L/sec). Thus, in the non-FL patients, PEEPi,st was the result of the association of high Rint,rs and relatively high V̇E (Table 2). Based on the multiple regression analysis, in the FL patients PEEPi,st correlated significantly only with Ppeak (Fig. 5). Because in our FL patients no external PEEP was added and the ventilatory settings were relatively homogeneous (Table 2), Ppeak reflects the combined pressure dissipation resulting from flow resistance, elastic recoil, viscoelastic behavior, and PEEPi,st (15) (i.e., the overall severity of lung disease). Accordingly, equation 3 can be taken as an indication that in FL patients, PEEPi,st increases with the severity of lung disease, as reflected by Ppeak. It should be noted, however, that the significant correlation of PEEPi,st to Ppeak may simply reflect the fact that PEEPi,st, which is included in Ppeak, is actually a major determinant of Ppeak. Tidal FL and PEEPi,st, which have been previously reported in mechanically ventilated patients with chronic obstructive lung disease (6, 13), were also observed in our six patients with COPD or asthma. One of these patients (Patient 4) as well as a patient with sepsis and abdominal surgery (Patient 14) were grossly Crit Care Med 2000 Vol. 28, No. 12 obese (130 kg; Table 1): Tidal FL and PEEPi,st have recently been demonstrated in healthy, supine obese patients by Pankow et al. (21), who attributed this to breathing at low lung volume with concomitant reduction in expiratory flow reserve and air trapping. Decreased expiratory flow reserve resulting from a reduction in functional lung units may also explain the presence of tidal FL and PEEPi,st in the four patients with pneumonia (Patients 7–9 and 11). Tidal FL and PEEPi,st were also found in Patient 10, who had CPE. Although PEEPi,st has been reported previously in patients with CPE (7), expiratory FL was not assessed in those patients. There are several mechanisms that could induce FL in CPE. In patients with heart disease, there is a reduction in maximal expiratory flows, which has been attributed to competition for space between the airways and the pulmonary vessels (22–24). With alveolar flooding, functional residual capacity may be reduced (25), with a concomitant decrease in expiratory flow reserve in the tidal volume range. Breathing at low lung volume caused by CPE should also promote small-airway closure and gas trapping, particularly in the supine position (26). Furthermore, Patient 10 was 70 yrs old, and old age promotes small-airway closure (26). Increased closing volume and gas trapping have been reported in pulmonary edema (27, 28). By reducing the number of lung units with patent airways, enhanced small-airway closure should further decrease expiratory flow reserve in CPE. In conclusion, using a new Evita 2 ventilator equipped with an NEP device, we were able to assess tidal expiratory FL and PEEPi,st in 32 consecutive mechanically ventilated patients. Most patients with ARF of pulmonary origin were FL and had a PEEPi,st ⬎ 4 cm H2O. In contrast, all patients with ARF of extrapulmonary origin were non-FL and had a PEEPi,st ⬍ 4 cm H2O. Modern ventilators allowing on-line assessment of FL and PEEPi,st could provide useful information concerning respiratory mechanics in mechanically ventilated patients. ACKNOWLEDGMENTS The authors especially thank Dr. J. Manigel from Draeger for his kind advice and support in the construction of the NEP device. They also thank Mrs. C. Sotiropoulou for advice on the statistical analysis of the data, as well as the nurses and staff of the intensive care unit of their hospital for support and cooperation during the study. REFERENCES 1. Jonson B, Nordstrom L, Olson SG, et al: Monitoring of ventilation and lung mechanics during automatic ventilation: A new device. Bull Physiopath Resp 1975; 11:729 –743 2. Pepe PE, Marini J: Occult positive endexpiratory pressure in mechanically ventilated patients with airflow obstruction. Am Rev Respir Dis 1982; 126:166 –170 3. Kimball WR, Leith DE, Robins AG: Dynamic hyperinflation and ventilator dependance in chronic obstructive pulmonary disease. Am Rev Respir Dis 1982; 126:991–995 4. Rossi A, Gottfried SB, Zocchi L, et al: Measurement of static compliance of the total respiratory system in patients with acute respiratory failure during mechanical ventilation. Am Rev Respir Dis 1985; 131:672– 677 5. Killian KJ, Cambell EJM: Dyspnea. In: The Thorax. Roussos C, Macklem PT (Eds). Basel, Marcel Dekker, 1985, pp 787– 828 6. Eltayara L, Becklake MR, Volta CA, et al: Relationship between chronic dyspnea and expiratory flow limitation in patients with chronic obstructive lung disease. Am J Respir Crit Care Med 1996; 154:1726 –1734 7. Broseghini D, Brandolese R, Poggi R, et al: Respiratory mechanics during the first day of mechanical ventilation in patients with pulmonary edema and chronic airway obstruction. Am Rev Respir Dis 1988; 138:355–361 8. Coussa ML, Guérin C, Eissa NT, et al: Partitioning of work of breathing in mechanically ventilated COPD patients. J Appl Physiol 1993; 75:1711–1719 9. Obdrzalek J, O’Donnell DE, Webb KA: Exertional breathlessness in patients with chronic airflow limitation: The role of lung hyperinflation. Am Rev Respir Dis 1993; 148: 1351–1357 10. Hyatt RE: The interrelationship of pressure, flow and volume during various respiratory maneuvers in normal and emphysematous patients. Am Rev Respir Dis 1981; 83: 676 – 683 11. Ingram RH Jr, Shilder DP: Effect of gas compression on pulmonary pressure, flow and volume relationship. J Appl Physiol 1966; 21:1821–1826 12. Milic–Emili J: Recent advances in spirometry and flow–volume loop. Semin Respir Crit Care Med 1998; 19:309 –316 13. Valta P, Corbeil C, Lavoie A, et al: Detection of expiratory flow limitation during mechanical ventilation. Am J Respir Crit Care Med 1994; 150:1311–1317 14. Eissa NT, Ranieri VM, Corbeil C, et al: Analysis of behavior of the respiratory system in ARDS patients: Effects of flow, volume and time. J Appl Physiol 1991; 70:2719 –2729 3841 15. Pesenti A, Pelosi P, Rossi N, et al: Respiratory mechanics and bronchodilator responsiveness in patients with the adult respiratory distress syndrome. Crit Care Med 1993; 21: 78 – 83 16. Gottfried SB: The role of PEEP in the mechanically ventilated COPD patient. In: Ventilatory Failure. Roussos X, Marini J (Eds). Berlin, Springer–Verlag, 1991, pp 392– 418 17. Rossi A, Ranieri M: Positive end-expiratory pressure. In: Principles and Practice of Mechanical Ventilation. Tobin JM (Ed). New York, McGraw Hill, 1998, pp 155–189 18. Bates JH, Rossi A, Milic–Emili J: Analysis of the behavior of the respiratory system with constant inspiratory flow. J Appl Physiol 1985; 58:1840 –1848 19. Aires SM, Schlichtig R, Sterling MJ: The central nervous system. In: Care of the critically 3842 20. 21. 22. 23. 24. ill. Tinker J, Zapol WM (Eds). Chicago, Year Book Medical Publishers, 1988, pp 320 –322 Tantucci C, Corbeil C, Chassé C, et al: Flow resistance in mechanically ventilated patients with severe neurological injury. J Crit Care 1993; 8:133–139 Pankow W, Podszus T, Gutheil T, et al: Expiratory flow limitation and intrinsic positive end-expiratory pressure in obesity. J Appl Physiol 1998; 85:1236 –1243 Wood TE, McLeod P, Antonisen NR, et al: Mechanics of breathing in mitral stenosis. Am Rev Respir Dis 1971; 104:52– 60 Hogg JC, Agarawal JB, Gardiner AJ, et al: Distribution of airway resistance with developing pulmonary edema in dogs. J Appl Physiol 1998; 85:1236 –1243 De Troyer AD, Yernault JC, Englert M: Me- 25. 26. 27. 28. chanics of breathing in patients with atrial septal defect. Am Rev Respir Dis 1977; 115: 413– 421 Noble WH, Kay JC, Obdrzalek J: Lung mechanics in hypervolemic pulmonary edema. J Appl Physiol 1975; 38:681– 687 Leblanc P, Ruff F, Milic–Emili J: Effect of age and body position on airway closure in man. J Appl Physiol 1970; 28:448 – 451 Demets M, Sniderman F, Utz G, et al: Lung volumes including closing volume, and arterial blood gas measurements in acute ischaemic left heart failure. Bull Physiopath Resp 1974; 10:11–25 Hughes JMB: Pulmonary edema. In: Regional Differences in the Lung. West JB (Ed). New York, Academic Press, 1977, pp 381– 418 Crit Care Med 2000 Vol. 28, No. 12