DARZALEX Reimbursement and Access Guide

DARZALEX
TM
REIMBURSEMENT
& ACCESS GUIDE
IMPORTANT INFORMATION TO SUPPORT
THE REIMBURSEMENT PROCESS
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
2
INTRODUCTION
Janssen Biotech, Inc., is committed to providing you and your office staff with detailed information to assist you in obtaining reimbursement for DARZALEX™ (daratumumab).
This Reimbursement and Access Guide has been developed to provide you with information regarding:
• Essential Coding Considerations
• Sample Claims Forms
• A list of Specialty Distributors
• Important Product Information
• Reimbursement Support Services
Information about access and reimbursement support services for DARZALEX™—for both providers and patients has been made available through Janssen CarePath.Please feel free to call 1-844-55-DARZA (553-2792) to speak with a Janssen CarePath Case Coordinator about any reimbursement-related questions or concerns.
Indication
DARZALEX™ is indicated for the treatment of patients with multiple myeloma who have received at least 3 prior lines of therapy, including a proteasome inhibitor (PI) and an immunomodulatory agent, or who are double refractory to a PI and immunomodulatory agent.
1 Please see Important Safety Information on page 30.
This indication is approved under accelerated approval based on response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
Disclaimer
• This document is presented for informational purposes only and is not intended to provide reimbursement or legal advice
• Laws, regulations, and policies concerning reimbursement are complex and are updated frequently
– While we have made an effort to be current as of the issue date of this document, the information may not be as current or comprehensive when you view it
– Similarly, all Current Procedural Terminology (CPT ® ) and Healthcare Common
Procedure Coding System (HCPCS) codes are supplied for informational purposes only, and this information does not represent any statement, promise, or guarantee by Janssen Biotech, Inc., about coverage, levels of reimbursement, payment, or charge
• Please consult your payer organization(s) for local or actual coverage and reimbursement policies and determination processes
• Please consult with your counsel or internal reimbursement specialist for any reimbursement or billing questions specific to your institution. CPT ® codes and descriptions are copyright 2015 American Medical Association. All rights reserved.
CPT ® is a registered trademark of the American Medical Association (AMA)
TABLE OF CONTENTS
DARZALEX™ (daratumumab) Dosing and Administration ...........................................................
4
Coding for DARZALEX™ .........................................................................................................................
7
NDC Numbers ......................................................................................................................................
7
Miscellaneous HCPCS Codes ..........................................................................................................
8
Transition to Temporary and Permanent HCPCS Codes .........................................................
9
CPT ® Codes .........................................................................................................................................
10
ICD-9-CM and ICD-10-CM Potential Diagnosis Codes ..........................................................
11
Other Coding Considerations ..........................................................................................................
12
Modifiers .............................................................................................................................................
12
CMS Discarded Drug Policies ........................................................................................................
14
Same-Day Evaluation and Management Services ................................................................
15
Partial Additional Hours of Infusion Time ....................................................................................
15
Sample Claim Forms for DARZALEX TM .............................................................................................
16
Physician Office Sample Claim Form: CMS 1500 ....................................................................
18
Hospital Outpatient Department Sample Claim Form: CMS 1450 (UB-04) ......................
20
Specialty Distributors ..........................................................................................................................
22
Janssen CarePath ................................................................................................................................
24
Potential Cost Support Options for DARZALEX™ ......................................................................
26
Appendix
Sample Letter of Medical Necessity ............................................................................................
28
Sample Letter of Formulary Exception Request .......................................................................
29
Important Safety Information ...........................................................................................................
30
References .............................................................................................................................................
31
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
3
4
DARZALEX™ (daratumumab) DOSING AND ADMINISTRATION
The recommended dose of DARZALEX™ is 16 mg/kg body weight administered as an intravenous infusion according to the dosing schedule shown in the chart below.
1
For example, a patient with a body weight of 75 kg would require 1200 mg dose of DARZALEX™.
Administer pre-infusion and post-infusion medications to reduce the risk of infusion-related reactions.
Pre-infusion Medication
Approximately 1 hour prior to every infusion of DARZALEX™ patients should receive:
• IV methylprednisolone 100 mg, or equivalent dose of an intermediate-acting or long-acting corticosteroid, plus
• Oral acetaminophen 650 to 1000 mg, plus
• Oral or IV diphenhydramine 25 to 50 mg or equivalent
Following the second infusion, the dose of methylprednisolone may be reduced to 60 mg IV.
Post-infusion Medication
Administer oral methylprednisolone 20 mg or equivalent dose of a corticosteroid to patients the first and second day after all infusions.
Following dilution with 0.9% sodium chloride USP, administer the DARZALEX™ infusion intravenously at the appropriate infusion rate as presented on the next page. Consider incremental escalation of the infusion rate only in the absence of infusion reactions with the previous infusion of DARZALEX™ as defined on the next page.
DARZALEX
TM
dosing schedule
1
Weeks 1–8 Weekly Weekly
Dose DARZALEX TM
16 mg/kg of body at weight as an intravenous
(IV) infusion, on a 28-day schedule.
Weeks 9–24 Every 2 Weeks Every 2 Weeks Every 2 Weeks Every 2 Weeks
Week 25+ Every 4 Weeks until disease progression alts
Preparation for adminstration
Adminstration
Infusion rates for DARZALEX
TM, 1
Dilution volume Initial infusion Increments of infusion rate
Maximum infusion rate
First infusion
Second infusion*
Subsequent infusions †
1000 mL
500 mL
500 mL
50 mL/hour
50 mL/hour
100 mL/hour
50 mL/hour every hour
50 mL/hour every hour
50 mL/hour every hour
200 mL/hour
200 mL/hour
200 mL/hour
* Escalate only if there were no Grade 1 (mild) or greater infusion reactions during the first 3 hours of the first infusion.
† Escalate only if there were no Grade 1 (mild) or greater infusion reactions during a final infusion rate of ≤100 mL/hr in the first two infusions.
Note: For infusion-related reactions of any grade/severity, immediately interrupt the
DARZALEX™ (daratumumab) infusion and manage symptoms. Management of infusion-related reactions may further require reduction in the rate of infusion or treatment discontinuation of
DARZALEX™.
Important Safety Information
CONTRAINDICATIONS
None
WARNINGS AND PRECAUTIONS
Infusion Reactions
DARZALEX™ can cause severe infusion reactions. Approximately half of all patients experienced a reaction, most during the first infusion. Infusion reactions can also occur with subsequent infusions.
Nearly all reactions occurred during infusion or within 4 hours of completing an infusion. Prior to the introduction of post-infusion medication in clinical trials, infusion reactions occurred up to 48 hours after infusion. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, and hypertension. Signs and symptoms may include respiratory symptoms, such as cough, wheezing, larynx and throat tightness and irritation, laryngeal edema, pulmonary edema, nasal congestion, and allergic rhinitis. Less common symptoms were hypotension, headache, rash, urticaria, pruritus, nausea, vomiting, and chills.
Pre-medicate patients with antihistamines, antipyretics, and corticosteroids. Frequently monitor patients during the entire infusion. Interrupt infusion for reactions of any severity and institute medical management as needed. Permanently discontinue therapy for life-threatening (Grade 4) reactions. For patients with Grade 1, 2, or 3 reactions, reduce the infusion rate when re-starting the infusion.
To reduce the risk of delayed infusion reactions, administer oral corticosteroids to all patients the first and second day after all infusions. Patients with a history of obstructive pulmonary disorders may require additional post-infusion medications to manage respiratory complications.
Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with obstructive pulmonary disorders.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
5
Average Length of DARZALEX™ Infusion in a Phase II Study
2
In a Phase II efficacy and safety study of DARZALEX™ (daratumumab), the median
(mean) length of infusion was as follows:
7.0
First
Infusion
Median Duration
7.0 hours
4.6
Second
Infusion
Median Duration
4.6 hours
3.4
Subsequent
Infusion
Median Duration
3.4 hours
CODING FOR DARZALEX™ (daratumumab)
NDC Numbers
1
In some cases, you may be required to include the National Drug Code (NDC) number in the appropriate location on a claim form, especially when reporting with a miscellaneous
Healthcare Common Procedure Coding System (HCPCS) code.
10-digit NDC
NDC Numbers for DARZALEX™
,1
11-digit NDC
(most commonly used)
Description
57894-502-05 57894-0502-05
100 mg/5 mL vial
Single-use vial containing
100 mg of daratumumab solution for intravenous infusion
Important Safety Information (cont’d)
WARNINGS AND PRECAUTIONS
Interference with Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive Indirect Antiglobulin
Test (Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to
6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum. The determination of a patient’s ABO and Rh blood type are not impacted. Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX™. Type and screen patients prior to starting DARZALEX™.
Interference with Determination of Complete Response
Daratumumab is a human IgG kappa monoclonal antibody that can be detected on both the serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for the clinical monitoring of endogenous M-protein. This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
Adverse Reactions
The most frequently reported adverse reactions (incidence ≥20%) were: infusion reactions, fatigue, nausea, back pain, pyrexia, cough, and upper respiratory tract infection.
Serious adverse reactions were reported in 51 (33%) patients. The most frequent serious adverse reactions were pneumonia (6%), general physical health deterioration (3%), and pyrexia (3%).
DRUG INTERACTIONS
No drug interaction studies have been performed.
6
57894-502-20 57894-0502-20
400 mg/20 mL vial
Single-use vial containing
400 mg of daratumumab solution for intravenous infusion
Note: Payer requirements regarding the use of the 10- or 11-digit NDC may vary. Electronic submission generally requires use of the 11-digit NDC. To convert the 10-digit NDC to the
11-digit format, insert a leading zero in the middle sequence, as illustrated in the table above.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
7
8
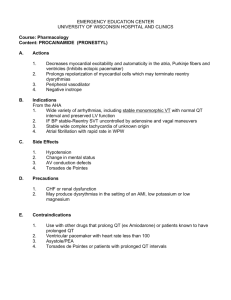
Miscellaneous HCPCS Codes
3
Drugs are typically reported using product-specific HCPCS codes (eg, J-code) assigned by the
Centers for Medicare & Medicaid Services (CMS). J-codes are a subset of the HCPCS Level II code set. Initially, as a new drug, DARZALEX TM (daratumumab) will be reported with a miscellaneous
HCPCS code that may vary by payer and treatment setting.
Code
C9399
J9999
Potential Miscellaneous HCPCS Codes for DARZALEX™ 3
Description
Unclassified drugs or biologicals
Not otherwise classified, antineoplastic drugs
Relevant Payer Requirements 4
Office Setting Hospital Outpatient Setting n/a
For Medicare or commercial payer claims
For Medicare claims
For commercial payer claims
Note: Unclassified or miscellaneous HCPCS codes are used to allow suppliers to begin billing immediately for an item as soon as the FDA grants marketing approval for a new product, even though no existing national code adequately describes the item being billed. These miscellaneous
HCPCS codes can be used during the time when a new code is being considered for a specific product under the HCPCS review process.
5 When listing a miscellaneous HCPCS code, payers may require reporting the drug name, strength, NDC number, dose administered, and route of administration. In addition, for claims with a miscellaneous HCPCS code, some payers may request supplemental information such as the prescribing information, published clinical trials, and/or the purchase invoice. However, specific payer requirements may vary.
Transition to Temporary and Permanent HCPCS Codes
5
A temporary C-code for DARZALEX™ (daratumumab) is expected by April 2016. Once effective, the DARZALEX™ temporary C-code will replace the miscellaneous code C9399 when it is provided for billing Medicare in the hospital outpatient setting.
A permanent J-code for DARZALEX™ is expected by January 2017. The DARZALEX™ permanent
J-code will replace miscellaneous and/or temporary codes used across all settings of care.
Setting of Care
Expected Changes in HCPCS Codes for DARZALEX™
5
Miscellaneous Code
Office Setting J9999
Hospital Outpatient Setting C9399
Temporary Code n/a
April 2016
Permanent Code
January 2017
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
9
10
CPT
®
Codes
CPT codes (Current Procedural Terminology) are the most widely accepted medical nomenclature used to report medical procedures and services under public and private health insurance programs. CPT ® is a registered trademark of the American Medical Association.
6
Consider using the following CPT codes for the administration of the DARZALEX™ (daratumumab) infusion 7 :
Code
Potential CPT Codes for DARZALEX™ Administration 7
Description
96413
96415
Chemotherapy administration, intravenous infusion technique; up to 1 hour, single or initial substance/drug
Chemotherapy administration, intravenous infusion technique; each additional hour (list separately in addition to code for primary procedure)
Note: These chemotherapy administration codes apply to parenteral administration of non-radionuclide anti-neoplastic drugs. CMS policy for chemotherapy administration codes states that if performed to facilitate the chemotherapy infusion, professional services and items described by these CPT codes include use of local anesthesia, IV access, access to indwelling IV, flush at conclusion of infusion, standard tubing, syringes and supplies, and preparation of chemotherapy agent(s).
8
ICD-9-CM and ICD-10-CM Potential Diagnosis Codes
9
The Department of Health & Human Services requires all entities covered by the Health
Insurance Portability and Accountability Act (HIPAA) to transition from the ICD-9-CM diagnosis coding system to the ICD-10-CM diagnosis coding system for services performed on or after
October 1, 2015. The transition to the ICD-10 coding system does not affect CPT coding for outpatient procedures and physician services.
The table below lists the ICD-9-CM and ICD-10-CM potential diagnosis codes for multiple myeloma, which you can consider for patients treated with DARZALEX™ (daratumumab).
203.02
Multiple Myeloma Diagnosis Codes for Consideration
ICD-9-CM 10 ICD-10-CM 11
Multiple myeloma, in relapse C90.02
Multiple myeloma in relapse
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
11
12
OTHER CODING CONSIDERATIONS
When coding and billing for DARZALEX™ (daratumumab) and drug administration services, providers also may need to describe concomitant services or supplies, report discarded drug amount, or account for modification to a service. This section reviews some of those additional considerations.
Modifiers
4,12,13
Modifiers are used to report or indicate that a service or procedure has been altered by some specific circumstance but not changed in its definition or code. They provide additional information about a service or procedure and help to eliminate the appearance of duplicate billing and unbundling. This could include using modifiers to designate a specific site of service, or to document an interrupted procedure, wasted product, same-day procedure, etc.
Appropriately used, modifiers improve coding and reimbursement accuracy. The following table summarizes modifiers that may be applicable to the provision of DARZALEX™ in physician offices and hospital outpatient departments.
Modifier
25
Description Indication and Placement
CMS-1500
Item 24D
CMS-1450
Locator Box
44
Significant, separately identifiable evaluation and management service by the same physician or other qualified healthcare professional on the same day of the procedure or other service
• Patient requires distinct evaluation and management
(E/M) service in addition to the infusion procedure
• Must be substantiated with relevant documentation
• Append the modifier to the relevant E/M code
JW
Drug amount discarded/not administered to any patient
• Unused drug remains after applicable dose is administered from single-use vial
• CMS has issued a discarded drug policy; local maximum allowable cost (MAC)/other payer requirements may vary
• Append the modifier to the drug code on a line separate from that reporting the administered dose
If required by payer
If required by payer
PO
Services, procedures, and/or surgeries furnished at off-campus provider-based outpatient departments
• Outpatient hospital items and services furnished in an off-campus provider-based department of a hospital*
• CMS has issued a policy for off-campus outpatient hospital departments; other payer requirements may vary
• Append the modifier to the relevant HCPCS/CPT code(s)
Required by
Medicare in
2016 †
MAC (Maximum Allowable Cost)/other payer
* The PO modifier should not be reported for remote locations of a hospital satellite, facilities of a hospital, or for services furnished in an emergency department.
13
† In 2015, reporting of the PO modifier in Medicare claims is voluntary.
13
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
13
14
CMS Discarded Drug Policies
4
When it is necessary to discard the remainder of a single-use vial or other single-use package after administering a dose/quantity of the drug or biological to a Medicare patient, the program provides payment for the amount of drug or biological discarded as well as the dose administered, up to the amount of the drug or biological as indicated on the vial or package label.
When processing claims for drugs and biologicals, local contractors may require the use of the modifier JW to identify unused drug or biologicals from single-use vials or packages. This modifier, billed on a separate line, will provide payment for the amount of discarded drug or biological. For example, a single-use vial that is labeled to contain 100 units of a drug has 95 units administered to the patient and 5 units discarded. The 95-unit dose is billed on one line, while the discarded 5 units is billed on another line using the JW modifier. Both line items are processed for payment. The JW modifier is applied only to the amount of drug or biological that is discarded.
Summary
• Both the administered and discarded drug amounts should be clearly documented in the medical record
• Payment for discarded amounts of drug or biologics applies only to single-use vials or packages
• Multi-use vials are not subject to payment for discarded amounts of drug or biological
• Medicare contractors may choose to require the JW modifier on claims for discarded drug or biological.
Check with your local contractor for specific requirements
Same-Day Evaluation and Management Services
8,14
It may be necessary to provide evaluation and management (E/M) services on the same day as a drug administration procedure. Depending on the payer, E/M services that are medically necessary, separate, and distinct from the infusion procedure (CPT codes
99201-99205 and 99211-99215 in the physician office and HCPCS code G0463 in the hospital outpatient setting), and documented appropriately are generally covered. Please note that CMS has a specific policy regarding use of CPT code 99211 (level 1 medical visit for an established patient) in the physician office. The policy states:
For services furnished on or after January 1, 2004, do not allow payment for CPT code
99211, with or without modifier 25, if it is billed with a nonchemotherapy drug infusion code or a chemotherapy administration code.
Because Medicare payment for a chemotherapy infusion is assumed to already cover nursing services related to a Level 1 visit for an established patient, CPT code 99211 cannot be billed on the same day as an office-based infusion of DARZALEX™ (daratumumab).
Partial Additional Hours of Infusion Time
8
CMS has a policy for reporting add-on infusion codes when less than a full hour of service is provided. CPT code 96415 (for “each additional hour”) is to be used for “infusion intervals of greater than 30 minutes beyond 1-hour increments.” If the incremental amount of infusion time is 30 minutes or less, the time is not to be billed separately. Document infusion start and stop times in the medical record. Some payers may require reporting the actual number of minutes on claims. Time associated with interruptions in the infusion process (ie, when drug is not flowing, IV saline to keep a line open with no drug flowing) does not count toward billable infusion time.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
15
16
SAMPLE CLAIM FORMS FOR DARZALEX™ (daratumumab)
The Form CMS-1500 is prescribed by CMS for Medicare and Medicaid claims from noninstitutional providers and suppliers that qualify for a waiver submitted by the Administrative
Simplification Compliance Act (ASCA) requirement for electronic submission. This form is also used in the TRICARE Program. For detailed guidance on completing the CMS-1500 items, please see the Medicare Claims Processing Manual, Pub. 100-04, Chap 26, available at: www.cms.gov/Regulationsand-Guidance/Guidance/Manuals/index.html.
The 837P (Professional) is the standard format used by healthcare professionals and suppliers to transmit healthcare claims electronically. The American National Standards Institute (ANSI)
Accredited Standards Committee (ASC) X12N 837P (Professional) Version 5010A1 is the current electronic claim version. Data elements in the CMS uniform electronic billing specifications are consistent with the hard copy data set to the extent that one processing system can handle both. For more information on electronic claims, please see the ASC website at: www.x12.org.
To view a crosswalk between the electronic and hard copy claim form, please see: www.nucc.
org/images/stories/PDF/1500_form_map_to_837p_5010_v2-0_112011.pdf.
The Form CMS-1450, also known as the UB-04, is a uniform institutional provider bill suitable for use in billing multiple third-party payers. It is prescribed by CMS for the Medicare and
Medicaid claims from hospitals, including hospital outpatient departments. Because it serves many different types of payers, a particular payer may not need some data elements. For detailed guidance on completing the CMS-1450 items, please see the Medicare Claims Processing Manual, Pub. 100-04, Chap 25, available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/index.html.
__ __
1 2
CNTL # b. MED.
REC. #
5 FED. TAX NO.
6 STATEMENT COVERS PERIOD
FROM THROUGH
7
8 PATIENT NAME b
10 BIRTHDATE a
31
CODE
OCCURRENCE
DATE
11 SEX
12 DATE
32
CODE
OCCURRENCE
DATE
9 PATIENT ADDRESS b
16 DHR 17 STAT
18 19
33 OCCURRENCE
CODE DATE
34
CODE
OCCURRENCE
DATE a
35
CODE
24
OCCURRENCE SPAN
FROM THROUGH
36
CODE c
28 d
OCCURRENCE SPAN
FROM THROUGH
37
__
4 TYPE
OF BILL e
38 41
CODE
44 HCPCS / RATE / HIPPS CODE b c a
39 VALUE CODES
CODE AMOUNT d
45 SERV. DATE
40 VALUE CODES
CODE AMOUNT
46 SERV. UNITS 47 TOTAL CHARGES 48 NON-COVERED CHARGES
3
4
1
2
42 REV. CD. 43 DESCRIPTION
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
A
B
C
A
B
C
50 PAYER NAME
58 INSURED’S NAME
SAM
59 P.REL 60 INSURED’S UNIQUE ID
53 ASG.
BEN.
54 PRIOR PAYMENTS
PLE
TOTALS
55 EST. AMOUNT DUE
61 GROUP NAME
56 NPI
57
OTHER
PRV ID
62 INSURANCE GROUP NO.
VALUE CODES
AMOUNT
A
B
63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 65 EMPLOYER NAME
C
74 c.
67 A B C D E F G H
I J K L M a. a b b.
c
68
N O P Q
75
72
ECI
76 ATTENDING NPI QUAL
73
80 REMARKS
UB-04 CMS-1450 d.
CODE
APPROVED OMB NO.
81CC a b c d e.
LAST
77 OPERATING
LAST
78 OTHER
LAST
79 OTHER
NPI
NPI
FIRST
QUAL
FIRST
QUAL
FIRST
QUAL NPI
LAST FIRST
THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF.
NUBC ™
National Uniform
LIC9213257
C
A
B
A
B
C
49
A
B
C
19
20
21
22
23
15
16
17
18
11
12
13
14
7
8
9
10
3
4
1
2
5
6
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
17
18
Physician Office Sample Claim Form: CMS-1500
Time associated with interruptions in the infusion process (ie, when drug is not flowing, IV saline to keep a line open with no drug flowing) does not count toward billable infusion time.
A
B
C
D
Item 21 - Indicate diagnosis using appropriate ICD-10-CM code(s).
Potential codes for consideration 11 :
• C90.02 (Multiple myeloma, in relapse)
Item 24D - Indicate appropriate CPT and HCPCS codes and modifiers, if required.
Drug - Miscellaneous HCPCS code for consideration 3, *:
• J9999 (Not otherwise classified, antineoplastic drugs)
Infusion Services - Potential CPT codes for consideration 7 :
• 96413 (Chemotherapy administration, intravenous infusion technique; up to
1 hour, single or initial substance/drug)
• 96415 (Chemotherapy administration, intravenous infusion technique; each additional hour (list separately in addition to code for primary procedure)
Item 24G - Indicate appropriate billing units for the listed CPT and HCPCS codes.
Drug - Report 1 unit with a miscellaneous HCPCS code regardless of the dose and number of vials used.
Infusion Services - For the CPT code 96413, indicate 1 unit of service. For the
CPT code 96415, indicate appropriate units of service, based on the duration of
DARZALEX™ (daratumumab) infusion.
Item 19 - Report additional information required by the payer for claims with a miscellaneous HCPCS code.*
Potential information required by the payer may include drug name, NDC, dose administered, and route of administration.
†
NDC for DARZALEX™ (11-digit format) 1 :
• 57894-0502-05 (100 mg/5 mL vial)
• 57894-0502-20 (400 mg/20 mL vial)
†
*Specific payer requirements for DARZALEX™ may vary.
If the information exceeds the capacity of Item 19, attach additional documentation to the claim.
CMS 1500 Sample Claim Form (7-Hour Sample Infusion)
x
Doe, John B
123 Any Street
Any Town
12345 555 555-5555
AS
07 01 45 x x
000-00-1234
Doe, John B
Medicare
D
A
Dr. Jones 123-456-7890
Darzalex (daratumumab) 57894-0502-20, 1200 mg IV
C90.02
10 01 15
10 01 15
10 01 15
11
11
11
B 96413
96415
J9999
A
A
A
C
1
6
1
123-456-7890
123-456-7890
123-456-7890
Dr. Jones
555 Any Street
Anytown, AS 12345
123-456-7890
555 123-5555
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
19
20
Hospital Outpatient Department Sample Claim Form: CMS-1450 (UB-04)
A
B
C
D
Locator Box 67 - Indicate diagnosis using appropriate ICD-10-CM code(s).
Potential codes for consideration 11 :
• C90.02 (Multiple myeloma, in relapse)
Locator Box 44 - Indicate appropriate CPT and HCPCS codes and modifiers, if required.
Drug - Miscellaneous HCPCS codes for consideration 3 :
MEDICARE - C9399 (Unclassified drugs or biologicals)
COMMERCIAL PAYERS - J9999 (Not otherwise classified, antineoplastic drugs)
Infusion Services - Potential CPT codes for consideration 7, *:
• 96413 (Chemotherapy administration, intravenous infusion technique; up to
1 hour, single or initial substance/drug)
• 96415 (Chemotherapy administration, intravenous infusion technique; each additional hour (list separately in addition to code for primary procedure)
Locator Box 46 - Indicate appropriate billing units for the listed CPT and
HCPCS codes.
Drug - Report 1 unit with a miscellaneous HCPCS code regardless of the dose and number of vials used.
Infusion Services - For the CPT code 96413, indicate 1 unit of service. For the
CPT code 96415, indicate appropriate units of service, based on the duration of
DARZALEX™ (daratumumab) infusion.
Locator Box 80 - Report additional information required by the payer for claims with a miscellaneous HCPCS code.
†
Potential information required by the payer may include drug name, NDC, dose administered, and route of administration.
†
NDC for DARZALEX™ (11-digit format) 1 :
• 57894-0502-05 (100 mg/5 mL vial)
• 57894-0502-20 (400 mg/20 mL vial)
* For 2016, Medicare requires reporting the PO modifier for all outpatient hospital items and services furnished in an off-campus provider-based department of a hospital.
13
† Specific payer requirements for DARZALEX™ may vary.
‡ If the information exceeds the capacity of Locator Box 80, attach additional documentation to the claim.
1 Anytown Hospital
123 Any Street
Anytown, AS 12345
8 PATIENT NAME b
John B Doe
10 BIRTHDATE
07 01 45
31
CODE
OCCURRENCE
DATE a
11 SEX
John B Doe
12 DATE
M
32
CODE
OCCURRENCE
DATE
2
Pay-to-name
Pay-to-address
Pay-to-city/state
ADMISSION
13 HR 14 TYPE 15 SRC
16 DHR
33 OCCURRENCE
CODE DATE
9 PATIENT ADDRESS b
Any Town
17 STAT
34
CODE
18 19
OCCURRENCE
DATE a
3a PAT.
CNTL # b. MED.
REC. # xx-xxxx
DOE 1234-97
5 FED. TAX NO.
6 STATEMENT COVERS PERIOD
FROM THROUGH
010001010
123 Any Street
CONDITION CODES
20 21 22 23 24 c
28
AS d
12345
29 ACDT 30
STATE
35
CODE
OCCURRENCE SPAN
FROM THROUGH
36
CODE
OCCURRENCE SPAN
FROM THROUGH
7
37
__
4 TYPE
OF BILL e
US
D c.
38 41
CODE
1
42 REV. CD. 43 DESCRIPTION 44 HCPCS / RATE / HIPPS CODE a
39 VALUE CODES
CODE AMOUNT b c d
46 SERV. UNITS
40 VALUE CODES
CODE AMOUNT
47 TOTAL CHARGES 48 NON-COVERED CHARGES B
96413 10-01-15 1
2
3
96415 10-01-15 6
4
5
C9399 10-01-15 1
6
7
A
A
B
C
A
B
C
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
50 PAYER NAME
Medicare
58 INSURED’S NAME
SAM
59 P.REL 60 INSURED’S UNIQUE ID
53 ASG.
BEN.
54 PRIOR PAYMENTS
PLE
TOTALS
55 EST. AMOUNT DUE
61 GROUP NAME
56 NPI
57
OTHER
PRV ID
246 555 1234
62 INSURANCE GROUP NO.
63 TREATMENT AUTHORIZATION CODES 64 DOCUMENT CONTROL NUMBER 65 EMPLOYER NAME
VALUE CODES
AMOUNT
A
B
C
66
DX
69 ADMIT
DX
74
I J K L M
70 PATIENT
REASON DX
PRINCIPAL PROCEDURE
CODE DATE a. a b
OTHER PROCEDURE
CODE DATE b.
c
71 PPS
CODE
OTHER PROCEDURE
CODE DATE
68
49
OTHER PROCEDURE
CODE DATE d.
OTHER PROCEDURE
CODE DATE
80 REMARKS
Darzalex (daratumumab)
57894-0502-20, 1200 mg IV
UB-04 CMS-1450 APPROVED OMB NO.
81CC a b c d e.
OTHER PROCEDURE
CODE DATE
75
72
ECI
73
76 ATTENDING
LAST
Jones
123-456-7890
77 OPERATING NPI
QUAL
FIRST
John
QUAL
LAST
78 OTHER NPI
FIRST
QUAL
LAST
79 OTHER
FIRST
QUAL NPI
LAST FIRST
THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF.
NUBC ™
National Uniform
Billing Committee
LIC9213257
A
B
C
A
B
C
A
B
C
18
19
20
21
22
23
13
14
15
16
17
6
7
8
4
5
1
2
3
9
10
11
12
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
21
22
SPECIALTY DISTRIBUTORS
The following specialty distributors are authorized to sell
DARZALEX™ (daratumumab) and are able to service institutions and/or physician offices, and community oncology practices.
Specialty Distributor
ASD Healthcare
Phone
1-800-746-6273
Fax Website
1-800-547-9413 https://www.asdhealthcare.com
Cardinal Health
Specialty
Pharmaceutical
Distribution
Physician Offices:
1-877-453-3972 1-614-652-7043
Hospitals/All Other:
1-866-677-4844
1-614-652-7043 https://specialtyonline. cardinalhealth.com
https://orderexpress.
cardinalhealth.com
CuraScript
Specialty Distribution
(Priority Healthcare)
McKesson
Plasma & Biologics
1-877-599-7748
1-877-625-2566
McKesson
Specialty Health
Oncology Supply
Multispecialty:
1-855-477-9800
Oncology:
1-800-482-6700
1-800-633-7555
1-800-862-6208 https://www.curascriptonline.com
1-888-752-7626 https://connect.mckesson.com
Email: plasma@mckesson.com
Multispecialty:
1-800-800-5673
Oncology:
1-800-289-9285 https://www.
mckessonspecialtyhealth.com
1-800-248-8205 https://www.oncologysupply.com
Note: Janssen Biotech, Inc., does not endorse the use of any of the listed distributors in particular.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
23
24
One source for support...
Jassen CarePath is a single point of contact for comprehensive services and support for physicians, office staff, and patients treated with DARZALEX TM (daratumumab).
ACCESS tools
Help your patients start therapy by making treatment accessible with services and resources that include:
• Benefit investigation
• Prior authorization assistance
• Patient cost support options
• Dedicated Case Coordinators that work with you and your patient
• Billing and coding information
EDUCATION tools
Help keep your patients informed about the disease and their treatment with services and resources that include:
• Access to nurses who can answer questions about the disease and treatment with DARZALEX™
• Education about and referral to independent organizations that provide assistance with costs associated with travel to and from treatment
• A tool that connects patients and caregivers to national and/or state advocacy groups that offer resources relevant to their needs
• Personalized, live appointment reminders
Getting Started Is Easy
1
Complete the Business Associate
Agreement (BAA) one time only.
Available online at DARZALEX.com or by calling Janssen CarePath at
1-844-55DARZA (1-844-553-2792)
BAA
PEF
2
Complete the Patient Enrollment Form
(PEF) for each patient or complete online at oncologycarepathportal.com
3
Fax the completed forms to 1-844-553-2793
PEF
BAA
After receiving your completed PEF, Janssen CarePath will research your patient’s health coverage and return a Verification of Benefits within 48 hours. Janssen CarePath will also attempt to call your patient to review benefits and discuss potential cost support options.
For More Information
Please call Janssen CarePath at 1-844-55DARZA (1-844-553-2792), Monday-Friday,
8:00 am
-8:00 pm
ET, and speak to a Janssen CarePath Case Coordinator today.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
25
26
Important Documents
• Business Associate Agreement
• Janssen CarePath Patient Enrollment Form for DARZALEX™
• Janssen CarePath Savings Program Enrollment Form for DARZALEX™
• Sample Letter of Medical Necessity
• Sample Exception Letter
Potential Cost Support Options for DARZALEX™ (daratumumab)
Your patients may be eligible for programs that can help them afford their treatment with DARZALEX™.
For more information on these programs, please have your patients call Janssen CarePath at
1-844-55DARZA (1-844-553-2792), Monday-Friday, 8:00 am
-8:00 pm
ET, and speak to a Janssen Care-
Path Case Coordinator.
If your patient has commercial insurance
Janssen CarePath
Savings Program for
DARZALEX™
If eligible, patients pay no more than $10 for each infusion. Infusions 1-8 are $5 per infusion, and infusions 9+ are $10 per infusion. Subject to a $15,000 maximum annual program benefit for each calendar year. Not valid for patients enrolled in Medicare or Medicaid. Other restrictions may apply.
Rebates are determined by medication cost only, not the cost associated with IV infusion.
For additional details including complete eligibility and restrictions, please visit www.carepathsavingsprogram.com.
If your patient has Medicare
Janssen CarePath can refer patients to the Medicare Savings Program to discuss eligibility and program benefits. To learn more about eligibility and how the
Medicare Savings Program can help patients pay for Medicare Part B products:
• Visit www.medicare.gov/contacts
• Click on the link for “Medicare Savings Program (MSPs)” under
“Other Helpful Websites”
• Select the appropriate state
If your patient has Medicare, Medicaid, TRICARE, or commercial insurance
If eligible, patients may able be able to receive cost assistance through independent foundations:
• CancerCare | www.cancercare.org | 1-866-552-6729
• Good Days from CDF | www.gooddaysfromcdf.org | 1-877-968-7233
• Patient Advocate Foundation | www.copays.org | 1-800-532-5274
• Patient Access Network Foundation | www.panfoundation.org |
1-866-316-7263
• Leukemia & Lymphoma Society | www.lls.org | 1-877-557-2672
Other resources
The Johnson & Johnson Patient Assistance Foundation, Inc. (JJPAF) is committed to providing access to uninsured patients who lack the financial resources to pay for their medicines. If your patients need DARZALEX™ (daratumumab) and are uninsured and unable to pay for their medicine, please contact a JJPAF program specialist at 1-800-652-6227, 9:00 am
-6:00 pm
ET, or visit the foundation website at www.jjpaf.org to see if they may qualify for assistance.
1-800-652-6227, 9:00 am
-6:00 pm
ET www.jjpaf.org
For a comprehensive list of cost support programs related to DARZALEX™, visit www.JanssenPrescriptionAssistance.com/DARZALEX.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
27
28
APPENDIX
Sample Letter of Medical Necessity
Some payers and other formulary decision makers may require that treating physicians complete a Letter of Medical Necessity or request a formulary exception before patients can receive a specific therapy. We have provided a sample Letter of
Medical Necessity and a sample Letter of Formulary Exception Request below.*
[Insert Physician Letterhead]
[Insert Name of Medical Director]
[Insert Payer Name]
[Insert Address]
[Insert City, State Zip]
RE: Member Name:
Group Number:
[Insert Member Name]
Member Number: [Insert Member Number]
[Insert Group Number]
REQUEST: Authorization for treatment with DARZALEX™ (daratumumab)
DIAGNOSIS: [Insert Diagnosis] [Insert ICD]
DOSE AND FREQUENCY: [Insert Dose & Frequency]
REQUEST TYPE: Standard EXPEDITED
Dear [Insert Name of Medical Director] :
I am writing to support my request for an authorization for the above-mentioned patient to receive intravenous treatment with DARZALEX™, [insert indication] . This request is consistent with the indication statement for DARZALEX™. My request is supported by the following:
Summary of Patient’s Diagnosis
[Insert patient’s diagnosis, date of diagnosis, lab results and date, current condition]
Summary of Patient History
[Insert previous therapies/procedures, response to those interventions, description of patient's recent symptoms/condition.
Exercise your medical judgment and discretion when providing a diagnosis and characterization of the patient’s medical condition.]
Rationale for Treatment
Considering the patient’s history, condition, and the full Prescribing Information supporting uses of DARZALEX™, I believe treatment with DARZALEX™ at this time is warranted, appropriate, and medically necessary, and should be a covered and reimbursed service. The accompanying full Prescribing Information provides the approved clinical information for DARZALEX™.
Given the urgent nature of this request, please provide a timely authorization. Contact my office at [Insert Phone Number] if I can provide you with any additional information.
Sincerely,
[Insert Physician Name and Participating Provider Number]
P.S. – If this request is denied, I am requesting an expedited Exception reviewed by a “Like” specialist.
© Janssen Biotech, Inc. 2015 10/15 035903-150618
* PLEASE NOTE: These are sample letters.
Use of these letters does not guarantee reimbursement.
Sample Letter of Formulary Exception Request
[Insert Physician Letterhead]
[Insert Name of Medical Director]
[Insert Payer Name]
[Insert Address]
[Insert City, State Zip]
RE: Member Name:
Group Number:
[Insert Member Name]
Member Number: [Insert Member Number]
[Insert Group Number]
REQUEST: Authorization for treatment with DARZALEX™ (daratumumab)
DIAGNOSIS: [Insert Diagnosis] [Insert ICD]
DOSE AND FREQUENCY: [Insert Dose & Frequency]
REQUEST TYPE: Standard EXPEDITED
Dear [Insert Name of Medical Director] :
I am writing to request a formulary exception for the above-mentioned patient to receive intravenous treatment with
DARZALEX™, [indication] . This request is consistent with the indication statement for DARZALEX™. My request is supported by the following:
Summary of Patient’s Diagnosis
[Insert patient’s diagnosis, date of diagnosis, lab results and date, current condition]
Summary of Patient History
[Insert previous therapies/procedures, response to those interventions, description of patient's recent symptoms/condition.
Exercise your medical judgment and discretion when providing a diagnosis and characterization of the patient’s medical condition.]
Rationale for Treatment
Considering the patient’s history, condition, and the full Prescribing Information supporting uses of DARZALEX™, I believe treatment with DARZALEX™ at this time is warranted, appropriate, and medically necessary, and should be a covered and reimbursed service. The accompanying full Prescribing Information provides the approved clinical information for DARZALEX™.
Given the urgent nature of this request, please provide a timely authorization. Contact my office at [Insert Phone Number] if I can provide you with any additional information.
Sincerely,
[Insert Physician Name and Participating Provider Number]
P.S. – If this request is denied, I am requesting an expedited Exception reviewed by a “Like” specialist.
© Janssen Biotech, Inc. 2015 6/15
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
035901-150618
29
30
Important Safety Information
CONTRAINDICATIONS
None
WARNINGS AND PRECAUTIONS
Infusion Reactions
DARZALEX™ can cause severe infusion reactions. Approximately half of all patients experienced a reaction, most during the first infusion. Infusion reactions can also occur with subsequent infusions.
Nearly all reactions occurred during infusion or within 4 hours of completing an infusion. Prior to the introduction of post-infusion medication in clinical trials, infusion reactions occurred up to 48 hours after infusion. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, and hypertension. Signs and symptoms may include respiratory symptoms, such as cough, wheezing, larynx and throat tightness and irritation, laryngeal edema, pulmonary edema, nasal congestion, and allergic rhinitis. Less common symptoms were hypotension, headache, rash, urticaria, pruritus, nausea, vomiting, and chills.
Pre-medicate patients with antihistamines, antipyretics, and corticosteroids. Frequently monitor patients during the entire infusion. Interrupt infusion for reactions of any severity and institute medical management as needed. Permanently discontinue therapy for life-threatening (Grade 4) reactions.
For patients with Grade 1, 2, or 3 reactions, reduce the infusion rate when re-starting the infusion.
To reduce the risk of delayed infusion reactions, administer oral corticosteroids to all patients the first and second day after all infusions. Patients with a history of obstructive pulmonary disorders may require additional post-infusion medications to manage respiratory complications.
Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with obstructive pulmonary disorders.
Interference with Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive Indirect Antiglobulin
Test (Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to
6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum. The determination of a patient’s ABO and Rh blood type are not impacted. Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX™. Type and screen patients prior to starting DARZALEX™.
Interference with Determination of Complete Response
Daratumumab is a human IgG kappa monoclonal antibody that can be detected on both the serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for the clinical monitoring of endogenous M-protein. This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
Adverse Reactions
The most frequently reported adverse reactions (incidence ≥20%) were: infusion reactions, fatigue, nausea, back pain, pyrexia, cough, and upper respiratory tract infection.
Serious adverse reactions were reported in 51 (33%) patients. The most frequent serious adverse reactions were pneumonia (6%), general physical health deterioration (3%), and pyrexia (3%).
DRUG INTERACTIONS
No drug interaction studies have been performed.
References:
1. DARZALEX™ (daratumumab) [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc. 2. Data on file,
Janssen Biotech. 3. 2015 alpha-numeric HCPCS file. Centers for Medicare & Medicaid Services website. http:// www.cms.gov/Medicare/Coding/HCPCSReleaseCodeSets/Alpha-Numeric-HCPCS-Items/ 2015-Alpha-Numeric-
HCPCS-File-%C2%A0.html. Accessed August 26, 2015. 4. Centers for Medicare & Medicaid Services. Medicare
Claims Processing Manual. Chapter 17. July 2015. https://www.cms.gov/ Regulations-and-Guidance/Guidance/
Manuals/Downloads/clm104c17.pdf. Accessed August 31, 2015. 5. Healthcare common procedure coding system (HCPCS) level II coding procedures. Centers for Medicare & Medicaid Services website. http://www.cms.
gov/Medicare/Coding/MedHCPCSGenInfo/downloads/HCPCSLevelIICodingProcedures7-2011.pdf. Accessed
August 26, 2015. 6. About CPT ® . American Medical Association website. http://www.ama-assn.org/ama/pub/ physician-resources/solutions-managing-your- practice/coding-billing-insurance/cpt/about-cpt.page. Accessed
August 26, 2015. 7. CodeManager ® . American Medical Association website. https://ocm.ama-assn.org/OCM/
CPTRelativeValueSearch.do? submitbutton=accept. Accessed August 5, 2015. 8. Centers for Medicare & Medicaid
Services. Medicare Claims Processing Manual. Chapter 12. October 2014. https://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/clm104c12.pdf. Accessed August 31, 2015. 9. ICD-10-CM/PCS myths and facts. Centers for Medicare & Medicaid Services website. http://www.cms.gov/Medicare/Coding/ICD10/ downloads/icd-10mythsandfacts.pdf. Accessed August 5, 2015. 10. 203 codes. ICD9 data website. http://www.
icd9data. com/2015/Volume1/140-239/200-209/203/default.htm. Accessed August 31, 2015. 11. ICD-10-CM tabular list of diseases and injuries. Centers for Medicare & Medicaid Services website. http://www.cms.gov/Medicare/
Coding/ICD10/2015-ICD-10-CM-and-GEMs.html. Accessed August 5, 2015. 12. CodeManager: Current Procedural
Terminology. Appendix A. 2015. American Medical Association website. https://ocm.ama-assn.org/OCM/ codemanager/CPT. Accessed August 12, 2015. 13. Centers for Medicare & Medicaid Services. Medicare Claims
Processing Manual. Chapter 4. June 2015. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/
Downloads/clm104c04.pdf. Accessed August 31, 2015. 14. Centers for Medicare & Medicaid Services. Medicare
Claims Processing Manual. Transmittal 2845. December 2013. https://www.cms.gov/Regulations-and-Guidance/
Guidance/Transmittals/Downloads/R2845CP.pdf. Accessed August 31, 2015.
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
31
Contact Janssen CarePath at 1-844-55DARZA (1-844-553-2792),
Monday to Friday, 8:00 am
to 8:00 pm
ET, to learn about cost support options.
To contact JanssenMD ®
Phone: Call 1-800-JANSSEN (1-800-526-7736)
E-mail: Submit questions via www.askjanssenmedinfo.com
Please see Important Safety Information on page 30 and accompanying full Prescribing Information in pocket.
© Janssen Biotech, Inc. 2015 8/15 038447-150810
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use
DARZALEX™ safely and effectively. See full prescribing information for
DARZALEX.
DARZALEX (daratumumab) injection, for intravenous use
Initial U.S. Approval – 2015
------------------------------INDICATIONS AND USAGE-----------------------------
DARZALEX is a human CD38-directed monoclonal antibody indicated for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent. (1)
This indication is approved under accelerated approval based on response rate (14). Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
--------------------------DOSAGE AND ADMINISTRATION-------------------------
Pre-medicate with corticosteroids, antipyretics and antihistamines. (2.2)
Dilute and administer as an intravenous infusion. (2.3, 2.4)
Recommended dose is 16 mg/kg body weight:
Weekly Weeks 1 to 8
Every two weeks
Every four weeks
Weeks 9 to 24
Week 25 onwards until disease progression
Administer post-infusion medications. (2.2)
DARZALEX™ (daratumumab) injection
-------------------------DOSAGE FORMS AND STRENGTHS------------------------
Injection:
• 100 mg/5 mL solution in a single-dose vial (3)
• 400 mg/20 mL solution in a single-dose vial (3)
--------------------------------CONTRAINDICATIONS--------------------------------
None. (4)
---------------------------WARNINGS AND PRECAUTIONS-------------------------
• Infusion reactions: Interrupt DARZALEX infusion for infusion reactions of any severity. Permanently discontinue the infusion in case of lifethreatening infusion reactions. (2.1, 5.1)
• Interference with cross-matching and red blood cell antibody screening:
Type and screen patients prior to starting treatment. Inform blood banks that a patient has received DARZALEX. (5.2, 7.1)
--------------------------------ADVERSE REACTIONS--------------------------------
The most frequently reported adverse reactions (incidence ≥20%) were: infusion reactions, fatigue, nausea, back pain, pyrexia, cough, and upper respiratory tract infection. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Janssen Biotech, Inc. at 1-800-526-7736 (1-800-JANSSEN) or FDA at 1-800-FDA-1088 or www.fda. gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and Patient Information.
Revised: 11/2015
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose and Schedule
2.2 Recommended Concomitant Medications
2.3 Preparation for Administration
2.4 Administration
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS
5.1 Infusion Reactions
5.2 Interference with Serological Testing
5.3 Interference with Determination of Complete Response
6 ADVERSE REACTIONS
6.1 Adverse Reactions in Clinical Trials
6.2 Immunogenicity
7 DRUG INTERACTIONS
7.1 Effects of Daratumumab on Laboratory Tests
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
8.2 Lactation
8.3 Females and Males of Reproductive Potential
8.4 Pediatric Use
8.5 Geriatric Use
8.6 Renal Impairment
8.7 Hepatic Impairment
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
12.2 Pharmacodynamics
12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
16.2 Storage and Stability
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
DARZALEX is indicated for the treatment of patients with multiple myeloma who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent.
This indication is approved under accelerated approval based on response rate [see Clinical Studies (14)] . Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
2 DOSAGE AND ADMINISTRATION
2.1 Recommended Dose and Schedule
• Administer pre-infusion and post-infusion medications [see Dosage and
Administration (2.2)].
• Administer only as an intravenous infusion after dilution [see Dosage and
Administration (2.4)].
• DARZALEX should be administered by a healthcare professional, with immediate access to emergency equipment and appropriate medical support to manage infusion reactions if they occur [see Warnings and
Precautions (5.1)].
The recommended dose of DARZALEX is 16 mg/kg body weight administered as an intravenous infusion according to the following dosing schedule.
Table 1: DARZALEX dosing schedule
Schedule
Weekly
Every two weeks
Every four weeks
Weeks
Weeks 1 to 8
Weeks 9 to 24
Week 25 onwards until disease progression
If a planned dose of DARZALEX is missed, administer the dose as soon as possible and adjust the dosing schedule accordingly, maintaining the treatment interval.
Administer DARZALEX infusion intravenously at the appropriate infusion rate. Consider incremental escalation of the infusion rate only in the absence of infusion reactions with the previous infusion of DARZALEX as defined in
Table 2.
1
DARZALEX™ (daratumumab) injection
Table 2: Infusion rates for DARZALEX administration
Dilution volume
Initial rate
(first hour)
Rate increment
Maximum rate
First infusion 1000 mL 50 mL/hour 50 mL/hour every hour
200 mL/hour
Second infusion a 500 mL 50 mL/hour 50 mL/hour every hour
200 mL/hour
Subsequent infusions b
500 mL 100 mL/hour 50 mL/hour every hour
200 mL/hour a Escalate only if there were no Grade 1 (mild) or greater infusion reactions b during the first 3 hours of the first infusion.
Escalate only if there were no Grade 1 (mild) or greater infusion reactions during a final infusion rate of ≥100 mL/hr in the first two infusions.
For infusion reactions of any grade/severity, immediately interrupt the
DARZALEX infusion and manage symptoms. Management of infusion reactions may further require reduction in the rate of infusion, or treatment discontinuation of DARZALEX as outlined below [see Warnings and
Precautions (5.1)].
• Grade 1-2 (mild to moderate): Once reaction symptoms resolve, resume the infusion at no more than half the rate at which the reaction occurred.
If the patient does not experience any further reaction symptoms, infusion rate escalation may resume at increments and intervals as appropriate
(Table 2).
• Grade 3 (severe): If the intensity of the reaction decreases to Grade 2 or lower, consider restarting the infusion at no more than half the rate at which the reaction occurred. If the patient does not experience additional symptoms, resume infusion rate escalation at increments and intervals as outlined in Table 2. Repeat the procedure above in the event of recurrence of Grade 3 symptoms. Permanently discontinue DARZALEX upon the third occurrence of a Grade 3 or greater infusion reaction.
• Grade 4 (life threatening): Permanently discontinue DARZALEX treatment.
2.2 Recommended Concomitant Medications
Pre-infusion Medication
Administer pre-infusion medications to reduce the risk of infusion reactions to all patients approximately 1 hour prior to every infusion of DARZALEX as follows:
• intravenous corticosteroid (methylprednisolone 100 mg, or equivalent dose of an intermediate-acting or long-acting corticosteroid), plus
• oral antipyretics (acetaminophen 650 to 1000 mg), plus
• oral or intravenous antihistamine (diphenhydramine 25 to 50 mg or equivalent).
Following the second infusion, the dose of corticosteroid may be reduced
(methylprednisolone 60 mg intravenously).
Post-infusion Medication
Administer post-infusion medication to reduce the risk of delayed infusion reactions to all patients as follows:
• oral corticosteroid (20 mg methylprednisolone or equivalent dose of a corticosteroid in accordance with local standards) on the first and second day after all infusions.
For patients with a history of obstructive pulmonary disorder, consider prescribing post-infusion medications such as short and long-acting bronchodilators, and inhaled corticosteroids. Following the first four infusions, if the patient experiences no major infusion reactions, these additional inhaled post-infusion medications may be discontinued.
Prophylaxis for Herpes Zoster Reactivation
Initiate antiviral prophylaxis to prevent herpes zoster reactivation within
1 week of starting DARZALEX and continue for 3 months following treatment
[see Adverse Reactions (6.1)] .
2.3 Preparation for Administration
DARZALEX is for single use only.
Prepare the solution for infusion using aseptic technique as follows:
• Calculate the dose (mg), total volume (mL) of DARZALEX solution required and the number of DARZALEX vials needed based on patient actual body weight.
• Check that the DARZALEX solution is colorless to pale yellow. Do not use if opaque particles, discoloration or other foreign particles are present.
• Using aseptic technique, remove a volume of 0.9% Sodium Chloride
Injection, USP from the infusion bag/container that is equal to the required volume of DARZALEX solution.
DARZALEX™ (daratumumab) injection
• Withdraw the necessary amount of DARZALEX solution and dilute to the appropriate volume by adding to the infusion bag/container containing 0.9% Sodium Chloride Injection, USP as specified in Table 2
[see Dosage and Administration (2.1)] . Infusion bags/containers must be made of polyvinylchloride (PVC), polypropylene (PP), polyethylene (PE) or polyolefin blend (PP+PE). Dilute under appropriate aseptic conditions.
Discard any unused portion left in the vial.
• Gently invert the bag/container to mix the solution. Do not shake.
• Following dilution the infusion bag/container may be stored for up to
24 hours in a refrigerator at 2ºC to 8ºC (36ºF to 46ºF), protected from light. Do not freeze. After allowing the bag/container to come to room temperature, use immediately since DARZALEX solutions do not contain a preservative.
• Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. The diluted solution may develop very small, translucent to white proteinaceous particles, as daratumumab is a protein. Do not use if visibly opaque particles, discoloration or foreign particles are observed.
2.4 Administration
• Administer the diluted solution by intravenous infusion using an infusion set fitted with a flow regulator and with an in-line, sterile, non-pyrogenic, low protein-binding polyethersulfone (PES) filter (pore size 0.22 or
0.2 micrometer). Polyurethane (PU), polybutadiene (PBD), PVC, PP or PE administration sets must be used.
• Infusion should be completed within 15 hours.
• Do not store any unused portion of the infusion solution for reuse. Any unused product or waste material should be disposed of in accordance with local requirements.
• Do not infuse DARZALEX concomitantly in the same intravenous line with other agents.
3 DOSAGE FORMS AND STRENGTHS
DARZALEX is a colorless to pale yellow, preservative-free solution available as:
Injection:
• 100 mg/5 mL (20 mg/mL) in a single-dose vial.
• 400 mg/20 mL (20 mg/mL) in a single-dose vial.
4 CONTRAINDICATIONS
None.
5 WARNINGS AND PRECAUTIONS
5.1 Infusion Reactions
DARZALEX can cause severe infusion reactions. Approximately half of all patients experienced a reaction, most during the first infusion.
Infusion reactions can also occur with subsequent infusions. Nearly all reactions occurred during infusion or within 4 hours of completing
DARZALEX. Prior to the introduction of post-infusion medication in clinical trials, infusion reactions occurred up to 48 hours after infusion.
Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, and hypertension. Signs and symptoms may include respiratory symptoms, such as cough, wheezing, larynx and throat tightness and irritation, laryngeal edema, pulmonary edema, nasal congestion, and allergic rhinitis. Less common symptoms were hypotension, headache, rash, urticaria, pruritus, nausea, vomiting, and chills [see Adverse Reactions (6.1)].
Pre-medicate patients with antihistamines, antipyretics and corticosteroids.
Frequently monitor patients during the entire infusion. Interrupt
DARZALEX infusion for reactions of any severity and institute medical management as needed. Permanently discontinue DARZALEX therapy for life-threatening (Grade 4) reactions. For patients with Grade 1, 2, or
3 reactions, reduce the infusion rate when re-starting the infusion [see
Dosage and Administration (2.1)].
To reduce the risk of delayed infusion reactions, administer oral corticosteroids to all patients the first and second day after all infusions.
Patients with a history of obstructive pulmonary disorders may require additional post-infusion medications to manage respiratory complications.
Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with obstructive pulmonary disorders.
5.2 Interference with Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive Indirect Antiglobulin Test (Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to 6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum 1 [see References (15)] .
The determination of a patient’s ABO and Rh blood type are not impacted
[see Drug Interactions (7.1)] .
Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX. Type and screen patients prior to starting DARZALEX.
2
DARZALEX™ (daratumumab) injection DARZALEX™ (daratumumab) injection
5.3 Interference with Determination of Complete Response
Daratumumab is a human IgG kappa monoclonal antibody that can be detected on both, the serum protein electrophoresis (SPE) and immunofixation
(IFE) assays used for the clinical monitoring of endogenous M-protein [see
Drug Interactions (7.1)] . This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
6 ADVERSE REACTIONS
The following serious adverse reactions are also described elsewhere in the labeling:
• Infusion reactions [see Warning and Precautions (5.1)] .
6.1 Adverse Reactions in Clinical Trials
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety data reflect exposure to DARZALEX in 156 adult patients with relapsed and refractory multiple myeloma treated with DARZALEX at
16 mg/kg in three open-label, clinical trials. The median duration of exposure was 3.3 months (range: 0.03 to 20.4 months).
Serious adverse reactions were reported in 51 (33%) patients. The most frequent serious adverse reactions were pneumonia (6%), general physical health deterioration (3%), and pyrexia (3%).
Adverse reactions resulted in treatment delay for 24 (15%) patients, most frequently for infections. Adverse reactions resulted in discontinuations for
6 (4%) patients.
Adverse reactions occurring in at least 10% of patients are presented in
Table 3. Table 4 describes Grade 3–4 laboratory abnormalities reported at a rate of ≥10%.
Table 3: Adverse reactions with incidence ≥10% in patients with multiple myeloma treated with DARZALEX 16 mg/kg
DARZALEX 16 mg/kg
N=156
System Organ Class
Adverse Reaction
Infusion reaction a
Pyrexia
Chills
Incidence (%)
Any Grade Grade 3 Grade 4
48
General disorders and administration site conditions
Fatigue 39
21
10
3
2
1
0
0
0
0
0
Respiratory, thoracic and mediastinal disorders
Cough 21
Nasal congestion
Dyspnea
17
15
0
0
1
0
0
0
Musculoskeletal and connective tissue disorders
Back pain
Arthralgia
23
17
Pain in extremity
Musculoskeletal chest pain
15
12
2
0
1
1
0
0
0
0
Infections and infestations
Upper respiratory tract infection
Nasopharyngitis
Pneumonia b
Gastrointestinal disorders
Nausea
Diarrhea
Constipation
Vomiting
Metabolism and nutrition disorders
Decreased appetite
Nervous system disorders
Headache
Vascular disorders
Hypertension
20
15
11
27
16
15
14
15
12
10
1
0
5
6
0
1
0
0
1
1
0
0
0
0
0
0
0
0
0
0 a Infusion reaction includes terms determined by investigators to be related b to infusion, see below
Pneumonia also includes the terms streptococcal pneumonia and lobar pneumonia
3
Table 4: Treatment Emergent Grade 3-4 laboratory abnormalities (≥10%)
Anemia
Thrombocytopenia
Neutropenia
Lymphopenia
Daratumumab 16 mg/kg (N=156)
All Grade (%)
45
Grade 3 (%)
19
Grade 4 (%)
0
48
60
72
10
17
30
8
3
10
Infusion Reactions
The incidence of any grade infusion reactions was 46% with the first infusion of DARZALEX, 5% with the second infusion, and 4% with subsequent infusions. None of the reactions with second or subsequent infusions were
Grade 3 or higher.
The median time to onset of a reaction was 1.5 hours (range: 0.02 to
9.3 hours). The incidence of infusion interruptions due to reactions was 37%.
Median durations of infusion for the 1st, 2nd and subsequent infusions were
7.0, 4.6 and 3.4 hours respectively.
Severe infusion reactions included bronchospasm, dyspnea, hypoxia, and hypertension (<2% each). Common any grade adverse infusion reactions
(≥5%) were nasal congestion, cough, chills, rhinitis allergic, throat irritation, dyspnea, and nausea.
Herpes Zoster Virus Reactivation
Prophylaxis for Herpes Zoster Virus reactivation was recommended for patients in some clinical trials of DARZALEX. Systemic anti-viral medications were used in 73% of patients. Herpes zoster was reported in 3% of patients.
6.2 Immunogenicity
As with all therapeutic proteins, there is the potential for immunogenicity. In an open-label, clinical trial of patients with relapsed or refractory multiple myeloma treated with DARZALEX, 111 patients were evaluated for antitherapeutic antibody (ATA) responses to daratumumab at multiple time points during treatment and up to 8 weeks following the end of treatment using an electrochemiluminescence-based immunoassay. Following the start of DARZALEX treatment, none of the patients tested positive for antidaratumumab antibodies. However, this assay has limitations in detecting anti-daratumumab antibodies in the presence of high concentrations of daratumumab; therefore, the incidence of antibody development might not have been reliably determined.
Immunogenicity data are highly dependent on the sensitivity and specificity of the test methods used. Additionally, the observed incidence of a positive result in a test method may be influenced by several factors, including sample handling, timing of sample collection, drug interference, concomitant medication and the underlying disease. Therefore, comparison of the incidence of antibodies to daratumumab with the incidence of antibodies to other products may be misleading.
7 DRUG INTERACTIONS
No drug interaction studies have been performed.
7.1 Effects of Daratumumab on Laboratory Tests
Interference with Indirect Antiglobulin Tests (Coombs Test)
Daratumumab binds to CD38 on RBCs and interferes with compatibility testing, including antibody screening and cross matching. Daratumumab interference mitigation methods include treating reagent RBCs with dithiothreitol (DTT) to disrupt daratumumab binding 1 [see References (15)] or genotyping. Since the Kell blood group system is also sensitive to DTT treatment, K-negative units should be supplied after ruling out or identifying alloantibodies using DTT-treated RBCs.
If an emergency transfusion is required, non-cross-matched ABO/RhDcompatible RBCs can be given per local blood bank practices.
Interference with Serum Protein Electrophoresis and Immunofixation Tests
Daratumumab may be detected on serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for monitoring disease monoclonal immunoglobulins (M protein). This can lead to false positive SPE and IFE assay results for patients with IgG kappa myeloma protein impacting initial assessment of complete responses by International Myeloma Working
Group (IMWG) criteria. In patients with persistent very good partial response, consider other methods to evaluate the depth of response.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk Summary
There are no human data to inform a risk with use of DARZALEX during pregnancy. Animal studies have not been conducted. However, there are clinical considerations [see Clinical Considerations] . The estimated background risk of major birth defects and miscarriage for the indicated
DARZALEX™ (daratumumab) injection population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
Immunoglobulin G1 (IgG1) monoclonal antibodies are transferred across the placenta. Based on its mechanism of action, DARZALEX may cause fetal myeloid or lymphoid-cell depletion and decreased bone density. Defer administering live vaccines to neonates and infants exposed to DARZALEX in utero until a hematology evaluation is completed.
Data
Animal Data
Mice that were genetically modified to eliminate all CD38 expression
(CD38 knockout mice) had reduced bone density at birth that recovered by
5 months of age. In cynomolgus monkeys exposed during pregnancy to other monoclonal antibodies that affect leukocyte populations, infant monkeys had a reversible reduction in leukocytes.
8.2 Lactation
Risk Summary
There is no information regarding the presence of daratumumab in human milk, the effects on the breastfed infant, or the effects on milk production.
Human IgG is known to be present in human milk. Published data suggest that antibodies in breast milk do not enter the neonatal and infant circulations in substantial amounts.
The developmental and health benefits of breast-feeding should be considered along with the mother’s clinical need for DARZALEX and any potential adverse effects on the breast-fed child from DARZALEX or from the underlying maternal condition.
8.3 Females and Males of Reproductive Potential
Contraception
To avoid exposure to the fetus, women of reproductive potential should use effective contraception during treatment and for 3 months after cessation of
DARZALEX treatment.
8.4 Pediatric Use
Safety and effectiveness of DARZALEX in pediatric patients have not been established.
8.5 Geriatric Use
Of the 156 patients on the recommended dose, 45% were 65 years of age or older, and 10% were 75 years of age or older. No overall differences in safety or effectiveness were observed between these patients and younger patients [see Clinical Studies (14)] .
8.6 Renal Impairment
Based on a population pharmacokinetic (PK) analysis no dosage adjustment is necessary for patients with pre-existing renal impairment [see Clinical
Pharmacology (12.3)].
8.7 Hepatic Impairment
Based on a population PK analysis, no dosage adjustments are necessary for patients with mild hepatic impairment (Total Bilirubin [TB] 1.0× to
1.5× upper limit of normal [ULN] or aspartate aminotransferase [AST] >ULN).
Daratumumab has not been studied in patients with moderate to severe hepatic impairment (TB >1.5× ULN and any AST) [see Clinical Pharmacology
(12.3)].
10 OVERDOSAGE
The dose of DARZALEX at which severe toxicity occurs is not known.
In the event of an overdose, monitor patients for any signs or symptoms of adverse effects and provide appropriate supportive treatment.
11 DESCRIPTION
Daratumumab is an immunoglobulin G1 kappa (IgG1 κ ) human monoclonal antibody against CD38 antigen, produced in a mammalian cell line (Chinese
Hamster Ovary [CHO]) using recombinant DNA technology. The molecular weight of daratumumab is approximately 148 kDa.
DARZALEX is supplied as a colorless to pale yellow preservative-free solution for intravenous infusion in single-dose vials. The pH is 5.5. DARZALEX must be diluted with 0.9% Sodium Chloride Injection, USP [see Dosage and
Administration (2.3, 2.4)].
Each DARZALEX single-dose 20 mL vial contains 400 mg daratumumab, glacial acetic acid (3.7 mg), mannitol (510 mg), polysorbate 20 (8 mg), sodium acetate trihydrate (59.3 mg), sodium chloride (70.1 mg), and water for injection.
Each DARZALEX single-dose 5 mL vial contains 100 mg daratumumab, glacial acetic acid (0.9 mg), mannitol (127.5 mg), polysorbate 20 (2 mg), sodium acetate trihydrate (14.8 mg), sodium chloride (17.5 mg), and water for injection.
DARZALEX™ (daratumumab) injection
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
CD38 is a transmembrane glycoprotein (48 kDa) expressed on the surface of hematopoietic cells, including multiple myeloma and other cell types and tissues and has multiple functions, such as receptor mediated adhesion, signaling, and modulation of cyclase and hydrolase activity. Daratumumab is an IgG1 κ human monoclonal antibody (mAb) that binds to CD38 and inhibits the growth of CD38 expressing tumor cells by inducing apoptosis directly through Fc mediated cross linking as well as by immune-mediated tumor cell lysis through complement dependent cytotoxicity (CDC), antibody dependent cell mediated cytotoxicity (ADCC) and antibody dependent cellular phagocytosis (ADCP). Myeloid derived suppressor cells (MDSCs) and a subset of regulatory T cells (CD38+T daratumumab mediated cell lysis.
regs
) express CD38 and are susceptible to
12.2 Pharmacodynamics
NK cells express CD38 and are susceptible to daratumumab mediated cell lysis. Decreases in absolute counts and percentages of total NK cells
(CD16+CD56+) and activated (CD16+CD56 dim ) NK cells in peripheral whole blood and bone marrow were observed with DARZALEX treatment.
CD4+ and CD8+ T cell absolute counts, as well as their percentage of total lymphocytes, increased with DARZALEX treatment in both the peripheral blood and bone marrow.
Cardiac Electrophysiology
DARZALEX as a large protein has a low likelihood of direct ion channel interactions. There is no evidence from non-clinical or clinical data to suggest that DARZALEX has the potential to delay ventricular repolarization.
12.3 Pharmacokinetics
The pharmacokinetics (PK) of daratumumab following intravenous administration were evaluated in patients with relapsed and refractory multiple myeloma at dose levels from 0.1 mg/kg to 24 mg/kg, and included the recommended 16 mg/kg dose and regimen. The population PK analysis included 223 patients with multiple myeloma receiving DARZALEX in two clinical trials (150 subjects received 16 mg/kg).
Over the dose range from 1 to 24 mg/kg, increases in area under the concentration-time curve (AUC) were more than dose-proportional.
Clearance decreased with increasing dose and repeated dosing, indicating target-mediated pharmacokinetics.
Following the recommended schedule and dose of 16 mg/kg, the mean
[standard deviation (SD)] serum C max
value was 915 (410) µg/mL at the end of weekly dosing, approximately 2.9-fold higher than following the first infusion.
The mean (SD) predose (trough) serum concentration at the end of weekly dosing was 573 (332) µg/mL.
Based on the population PK analysis, daratumumab steady state is achieved approximately 5 months into the every 4-week dosing period (by the 21 st infusion), and the mean (SD) ratio of C max
at steady-state to C max
after the first dose was 1.6 (0.5). The mean (SD) linear clearance and mean (SD) central volume of distribution are estimated to be 171.4 (95.3) mL/day and 4.7
(1.3 L), respectively. The mean (SD) estimated terminal half-life associated with linear clearance was approximately 18 (9) days.
Population PK analyses indicated that the central volume of distribution and clearance of daratumumab increase with increasing body weight, supporting the body weight-based dosing regimen. Population PK analyses also showed that age (31 to 84 years) and gender do not have clinically important effects on the pharmacokinetics of daratumumab.
Special Populations
Renal Impairment
The population PK analysis included 71 patients with normal renal function
(creatinine clearance [CrCL] ≥90 mL/min), 78 patients with mild renal impairment
(CrCL <90 and ≥60 mL/min), 68 patients with moderate renal impairment (CrCL
<60 and ≥30 mL/min), and 6 patients with severe renal impairment or end stage renal disease (CrCL <30 mL/min). No clinical differences in exposure to daratumumab were observed between patients with renal impairment and those with normal renal function [see Use in Specific Populations (8.6)].
Hepatic Impairment
The population PK analysis included 189 patients with normal hepatic function (TB and AST ≤ULN) and 34 with mild hepatic impairment
(TB 1.0× to 1.5× ULN or AST>ULN) patients. No clinical differences in the exposure to daratumumab were observed between patients with mild hepatic impairment and those with normal hepatic function. Daratumumab has not been studied in patients with moderate (TB>1.5× to 3× ULN and any
AST) or severe (TB>3× ULN and any AST) hepatic impairment.
4
DARZALEX™ (daratumumab) injection
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No carcinogenicity or genotoxicity studies have been conducted with daratumumab. No animal studies have been performed to evaluate the potential effects of daratumumab on reproduction or development, or to determine potential effects on fertility in males or females.
14 CLINICAL STUDIES
Study 1, was an open-label trial evaluating DARZALEX monotherapy in patients with relapsed or refractory multiple myeloma who had received at least 3 prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent or who were double-refractory to a proteasome inhibitor and an immunomodulatory agent. In 106 patients, DARZALEX
16 mg/kg was administered with pre- and post-infusion medication. Treatment continued until unacceptable toxicity or disease progression.
The median patient age was 63.5 years (range: 31 to 84 years), 49% were male and 79% were Caucasian. Patients had received a median of 5 prior lines of therapy. Eighty percent of patients had received prior autologous stem cell transplantation (ASCT). Prior therapies included bortezomib (99%), lenalidomide (99%), pomalidomide (63%) and carfilzomib (50%). At baseline,
97% of patients were refractory to the last line of treatment, 95% were refractory to both, a proteasome inhibitor (PI) and immunomodulatory agent, and 77% were refractory to alkylating agents.
Efficacy results were based on overall response rate as determined by the Independent Review Committee assessment using IMWG criteria (see
Table 5).
Table 5: Efficacy results for Study 1
Overall response rate (ORR)
95% CI (%)
Stringent complete response (sCR)
Complete response (CR)
Very good partial response (VGPR)
Partial response (PR)
ORR = sCR+CR+VGPR+PR
CI = confidence interval
N=106
31 (29.2%)
(20.8, 38.9)
3 (2.8%)
0
10 (9.4%)
18 (17.0%)
The median time to response was 1 month (range: 0.9 to 5.6 months). The median duration of response was 7.4 months (range: 1.2 to 13.1+ months).
Study 2 was an open-label dose escalation trial evaluating DARZALEX monotherapy in patients with relapsed or refractory multiple myeloma who had received at least 2 different cytoreductive therapies. In 42 patients,
DARZALEX 16 mg/kg was administered with pre- and post-infusion medication. Treatment continued until unacceptable toxicity or disease progression.
The median patient age was 64 years (range: 44 to 76 years), 64% were male and 76% were Caucasian. Patients in the study had received a median of
4 prior lines of therapy. Seventy-four percent of patients had received prior
ASCT. Prior therapies included bortezomib (100%), lenalidomide (95%), pomalidomide (36%) and carfilzomib (19%). At baseline, 76% of patients were refractory to the last line of treatment, 64% of patients were refractory to both, a PI and an immunomodulatory agent, and 60% of patients were refractory to alkylating agents.
Overall response rate was 36% (95% CI: 21.6, 52.0%) with 1 CR and 3 VGPR.
The median time to response was 1 month (range: 0.5 to 3.2 months). The median duration of response was not estimable (range: 2.2 to 13.1+ months).
15 REFERENCES
1. Chapuy, CI, RT Nicholson, MD Aguad, et al., 2015, Resolving the daratumumab interference with blood compatibility testing, Transfusion,
55:1545-1554 (accessible at http://onlinelibrary.wiley.com/doi/10.1111/trf.13069/ epdf).
DARZALEX™ (daratumumab) injection
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
DARZALEX is a colorless to pale yellow, preservative-free solution for intravenous infusion supplied as:
NDC 57894-502-05 contains one 100 mg/5 mL single-dose vial
NDC 57894-502-20 contains one 400 mg/20 mL single-dose vial
16.2 Storage and Stability
Store in a refrigerator at 2ºC to 8ºC (36ºF to 46ºF).
Do not freeze or shake. Protect from light. This product contains no preservative.
17 PATIENT COUNSELING INFORMATION
Advise the patient to read the FDA-approved patient labeling (Patient
Information).
Infusion Reactions
Advise patients to seek immediate medical attention for any of the following signs and symptoms of infusion reactions:
• itchy, runny or blocked nose; chills, nausea, throat irritation, cough, headache, shortness of breath or difficulty breathing [see Warnings and
Precautions (5.1) and Adverse Reactions (6.1)] .
Interference with Laboratory Tests
Advise patients to inform healthcare providers including blood transfusion centers/personnel that they are taking DARZALEX, in the event of a planned transfusion.
Advise patients that DARZALEX can affect the results of some tests used to determine complete response in some patients and additional tests may be needed to evaluate response.
Manufactured by:
Janssen Biotech, Inc.
Horsham, PA 19044
U.S. License Number 1864
© Janssen Biotech, Inc., 2015
5
PATIENT INFORMATION
DARZALEX™ (Dar'-zah-lex)
(daratumumab) injection, for intravenous use
What is DARZALEX?
DARZALEX is a prescription medicine used to treat a type of cancer called multiple myeloma in people who:
• have received at least three prior medicines to treat multiple myeloma, including a proteasome inhibitor and an immunomodulatory agent, or
• did not respond to a proteasome inhibitor and an immunomodulatory agent
It is not known if DARZALEX is safe and effective in children.
Before you receive DARZALEX, tell your healthcare provider about all of your medical conditions, including if you:
• have a history of breathing problems
• have had shingles (herpes zoster)
• are pregnant or plan to become pregnant. DARZALEX may harm your unborn baby.
°
Females who are able to become pregnant should use an effective method of birth control during treatment and for at least 3 months after your final dose of DARZALEX. Talk to your healthcare provider about birth control methods that you can use during this time.
• are breastfeeding or plan to breastfeed. It is not known if DARZALEX passes into your breast milk.
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
How will I receive DARZALEX?
• DARZALEX will be given to you by intravenous (IV) infusion into your vein. The infusion should be completed within 15 hours.
• DARZALEX is usually given weekly for the first 8 weeks, then every 2 weeks for 16 weeks, and then every
4 weeks after that.
• Your healthcare provider will decide how many treatments you will receive.
• Your healthcare provider will give you medicines before each dose of DARZALEX and on the first and second day after each dose of DARZALEX to help reduce the risk of infusion reactions.
• If you miss any appointments, call your healthcare provider as soon as possible to reschedule your appointment.
6
DARZALEX™ (daratumumab) injection
What are the possible side effects of DARZALEX?
DARZALEX may cause serious reactions, including:
• Infusion reactions are common with DARZALEX and can be severe. Your healthcare provider may temporarily stop your infusion or completely stop treatment with DARZALEX if you have infusion reactions. Tell your healthcare provider right away if you get any of the following symptoms:
• shortness of breath or trouble breathing
• dizziness or lightheadedness (hypotension)
• cough
• wheezing
• headache
• rash or hives
• itching
• nausea
• throat tightness
• runny or stuffy nose
• vomiting
• chills
• DARZALEX can affect the results of blood tests to match your blood type. These changes can last for up to 6 months after your final dose of DARZALEX. Your healthcare provider will do blood tests to match your blood type before you start treatment with DARZALEX. Tell all of your healthcare providers that you are being treated with DARZALEX before receiving blood transfusions.
The most common side effects of DARZALEX include:
• tiredness
• nausea
• back pain
• fever
• cough
• cold-like symptoms (upper respiratory infection)
Tell your healthcare provider if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of DARZALEX. Call your doctor for medical advice about side effects.
You may report side effects to FDA at 1-800-FDA-1088.
General information about the safe and effective use of DARZALEX
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. You can ask your healthcare provider or pharmacist for information about DARZALEX that is written for health professionals.
What are the ingredients in DARZALEX?
Active ingredient: daratumumab
Inactive ingredients: glacial acetic acid, mannitol, polysorbate 20, sodium acetate trihydrate, sodium chloride, and water for injection
Manufactured by: Janssen Biotech, Inc., Horsham, PA 19044 U.S. License Number 1864
For more information, call 1-800-526-7736 or go to www.DARZALEX.com.
This Patient Information has been approved by the U.S. Food and Drug Administration. Issued: November/2015
040925-150923
7