MAGNETIC RESONANCE IMAGING SAFETY: PRINCIPLES AND
advertisement

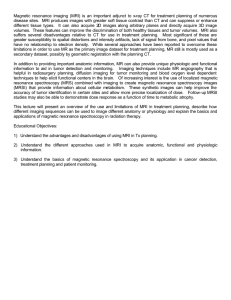
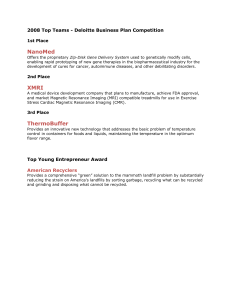
Prilozi, Odd. biol. med. nauki, MANU, XXXIII, 1, c. 441–472 (2012) Contributions, Sec. Biol. Med. Sci., MASA, XXXIII, 1, p. 441–472 (2012) ISSN 0351–3254 UDC: 616-073.763.5 MAGNETIC RESONANCE IMAGING SAFETY: PRINCIPLES AND GUIDELINES Stikova E Faculty of Medicine, Public Health Institute, Ss Cyril and Methodius University, Skopje, R. Macedonia A b s t r a c t: This paper provides an overview of the published literature regarding magnetic resonance imaging (MRI) safety. It gives basic information about the electromagnetic fields that are generated during the MRI diagnostic procedure, followed by a description of the biological effects of those fields on humans. It concludes with a discussion of the safety issues related to MRI use in clinical practice, highlighting the existing MRI standards and guidelines. Key words: magnetic resonance imaging, biological effects of electromagnetic radiation, MRI standards, safety guidelines. Introduction The 20th century saw an increase in the exposure of humans to electric and magnetic fields, due to the growing electricity demands of modern society. The widespread use of industrial equipment, communication devices and modern home appliances has resulted in increased levels of man-made electromagnetic radiation. According to its frequency (measured in Hertz, Hz) and its ability to ionize an atom or molecule in biological tissues, the electromagnetic (EM) radiation is classified in two categories – ionizing and non-ionizing (Hansson Mild, Alanko et al. 2009; Hartwig, Giovannetti et al. 2009). The ionizing radiation refers to X-rays and gamma rays, which have the ability to produce ionization of the biological tissues and cell damage. The non- 442 Stikova E ionizing part of the electromagnetic spectrum refers to static electromagnetic fields, radiofrequency and optical waves. Figure 1 illustrates the EM spectrum and the range of frequencies for different EM subclasses. (Hartwig, Giovannetti et al. 2009) Figure 1 – Electromagnetic spectrum and main application of different electromagnetic fields Medical diagnostic imaging is recognized as an important source of human exposure to ionizing and non-ionizing electromagnetic radiation (X-ray, CT, MRI, and ultrasound). While it is well established that ionizing radiation (X-ray, CT) poses risks to human health mainly because of the ionizing of tissues, the available data on possible effects of non-ionizing radition on patient and worker safety are not sufficient to draw firm conclusions (Hartwig, Giovannetti et al. 2009; International Commission on Non-Ionizing Radiation 2009). In the last decades the use of non-ionizing radiation in medical imaging has rapidly increased, mainly because of the more frequent use of magnetic resonance imaging – MRI (Picano 2004). MRI is an imaging technique designed to visualize internal structures of the body using electromagnetic fields to induce a resonance effect in hydrogen atoms. MRI provides a good contrast between the different soft tissues in the body, which makes it especially useful in imaging the brain, muscles, and the heart. MRI procedures have been utilized in clinical diagnostic practice for approximately 30 years. The use of MRI in the clinical setting started in the 1980s. Since then, more than 100,000,000 diagnostic procedures have been completed worldwide, with relatively few major incidents (Formica and Silvestri 2004). Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 443 Figures 2 and 3 show that the total number of MRI units in 27 OECD countries has increased from 811 in 1990 to more than 17,000 two decades later Source: OECD Health Data 2011 Statististics Figure 2 – Total number of MRI units in 27 OECD countries in the period 1980–2008 Source: OECD Health Data 2011 Statististics Figure 3 – MRI units in 27 OECD countries (in % of total number) Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 444 Stikova E with participation of US with 44% in total number of MRI units. The total number of MRI units varies from a few MRI units per one million populations in Hungary, the Netherlands, Poland, Slovenia to more than 20 in Iceland, Italy and the US. The biggest number of MRI units is registred in Japan with 43 units/one million population (Figure. 4). Source: OECD Health Data 2011 Statististics Figure 4 – Number of MRI units in 27 OECD countries per million population (by country) Source: OECD Health Data 2011 Statististics The number of examinations per 1000 population varies from 1.7/1000 in Chile to 67.2/1000 in Turkey, 73.9/1000 in Luxemburg and 75.5/1000 in Iceland., reaching highest values of 91.2/1000 population in United States and 97.9/1000 in Greece (OECD 2011). Magnetic Resonance Imaging is considered a safe technology due to its ability to change the position of atoms without altering their structure, composition, or properties. With the growing number of magnetic resonance systems, one concern related to the use of MRI is possible adverse biological effects, but there are also other concerns related to the effects of magnetic fields on patients, equipment and personnel (Dempsey, Condon et al. 2002; Coskun 2011; Boutin, Briggs et al. 1994; Colletti 2004).Therefore, it is necessary to evaluate the possible risks and various biological effects caused by the MRI fields on human Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 445 health (Abart and Ganssen 1995). It is also necessary to develop guidelines and protocols aimed at protecting the safety and health of staff and patients. The MRI practices and safety guidelines target different focus groups: MR physicists, research/academic radiologists, MR safety experts, electrical engineers and/or manufactures, legal counsellors and others (Shellock and Kanal 1991). There are also legislative issues that are country-specific, making it difficult to reach a consensus about safe MR practices. In the absence of such consensus, attempts should be made to observe the precautionary principle and to avoid unnecessary examinations (Hartwig, Vanello et al. 2011). This paper provides an overview of the published literature and the main existing safety guidelines, with focus on possible biological effects and safety issues relevant for the use of MRI as a medical diagnostic procedure. The aim of the paper is to give basic information about the electromagnetic fields that are generated during the MRI diagnostic procedure, their sources and physical characteristics, to briefly describe the potential biological effects and important safety issues related to MRI use in clinical practice, and to clarify the necessity of maintenance of an appropriate MRI safety policy including application of safety standards (required or voluntary) and good practices. To this effect, the paper is divided into three sections: I. Basic information about MRI, II. Biological effects of MRI, and III. Safety issues in MRI I. BASIC INFORMATION ABOUT MAGNETIC RESONANCE IMAGING The technology used for magnetic resonance (MR) procedures has evolved continuously during the past 40 years, yielding MR systems with stronger static magnetic fields, faster and stronger gradient magnetic fields, and more powerful radiofrequency transmission coils. The following three magnetic field types are produced by the basic components of an MRI system (Formica and Silvestri 2004; Hartwig, Giovannetti et al. 2009): • High static magnetic field (B0) – it generates a net magnetization in the human body and is responsible for alignment of nuclei; • Gradient magnetic fields (dB/dt) – caused by cycling of power through the gradient coils; they are used to localize aligned protons inside the body allowing spatial reconstruction of tissue sections into images; • Radio frequency magnetic fields (B1) (10 to 400 MHz) – responsible for exciting the patient's protons within the stable magnetic field and for positioning of nuclei during the imaging process. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 446 Stikova E The static magnetic field is the main magnetic field in MRI that is used to align the patient's protons in an organized and predictable fashion. It is usually generated by a strong superconducting magnet and is represented by the symbol B0. The static magnetic field is measured at the exact centre of the magnet at the intersection of the three orthogonal planes (X, Y, Z). This central point is called the isocentre. The strength of the static field (Bo) is measured in tesla (T), with one tesla equal to 10,000 gauss (G). Clinical imaging systems today typically have static field strengths up to 3T. Spectroscopic systems, usually used for research, are available with field strengths as high as 17.5T (Hartwig, Giovannetti et al. 2009; International Commission on Non-Ionizing Radiation 2009). The very powerful magnet in the centre of the scanner is always on even when the machine is not scanning, including all night, every weekend, and even holidays. This means that a very strong static magnetic field is always present in the MRI environment. The second type of magnetic field used in MRI is the gradient magnetic field. All MR imaging systems are equipped with a set of resistive wire windings known as gradient coils. Gradient magnetic fields are created by the cycling of power through the gradient coils and are called gradient or time varying magnetic fields (TVM). The gradient magnetic fields are used to control the selective excitation of the patient's protons. Time-varying magnetic fields are superimposed on the static magnetic field to obtain spatial information in MR imaging. These fields are of low magnitude compared with the static field. There are 3 sets of gradient coils capable of producing a TVMF in all three orthogonal directions (X, Y, and Z). For oblique imaging, gradient coils are used in combination. Figure 5 is an example of the gradient coils creating a varying magnetic field in the Z direction. Source: Roth R.T.C. (1996) Figure 5 – A representation of the magnet bore and the time-varying magnetic field in the Z-direction Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 447 The third type of magnetic field used in MRI is the radiofrequency (RF) magnetic field. During an MRI exam, the patient is exposed to RF radiation in the range of 10 to 400 MHz (Shellock 2000; Formica and Silvestri 2004). The source of this radiation is the radiofrequency coil that surrounds the patient inside the magnet bore. Radio waves are used to excite the patient's protons within the stable magnetic field. II. BIOLOGICAL EFFECTS OF MRI a) Biological effects of static magnetic fields Interest in the biological effects of static magnetic fields has increased with the invention of MRI. Several studies were carried out in order to understand the potential hazards associated with exposure to a strong static magnetic field. The majority of these studies did not report positive results, thus postulating no adverse effects for human health (Formica and Silvestri 2004). Static magnetic fields can interact with biological systems by exerting forces on molecules and cells having diamagnetic susceptibility. They can also affect enzyme kinetics and act on moving charges (including moving fluids). The metabolic functions of human tissues require a large quantity of chemical reactions, and it is therefore reasonable to suppose that a strong magnetic field might alter the rates or the equilibrium conditions of these reactions (Formica and Silvestri 2004). With regard to short-term exposure, investigations include studies on alteration in cell growth and morphology, cell reproduction and teratogenicity, DNA structure, blood-brain barrier permeability, nerve activity, cognitive function and behaviour, haematologic parameters, circadian rhythms and other biological changes. The majority of these studies concludes that static electromagnetic fields produce no substantial harmful biological effects (Abart and Ganssen 1995; Schwenzer, Bantleon et al. 2007). Only some sensory effects have been found associated with exposure to a static magnetic field. There was a statistically significant (p < 0.05) finding for sensations of nausea, vertigo, and metallic taste in subjects exposed to 1.5 and 4 T static magnetic fields, but no statistical significance was found for other effects such as headache, hiccups, tinnitus, vomiting, and numbness. A higher incidence of positive reports originated from those subjects exposed to a 4 T field. However there was no evidence that these effects were at all harmful (Schenck, Dumoulin et al. 1992; Formica and Silvestri 2004). Many studies have been carried out on the in vitro effects of static magnetic fields on cell growth, cell proliferation, cell cycle distribution pattern and apoptotic cell death. The cells were not affected by an exposure up to four days at field strengths up to 10T, while an exposure of 10–17T for 30–60 minuPrilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 448 Stikova E tes can reduce number and size, cell organization and vitality in cultured mammalian cells. These studies suggest that static magnetic fields might affect the process of cancer induction and/or progression by altering cellular responses to some known carcinogens (chemicals, radiation). However, the findings available in the literature are often not comparable and in some cases also not reproducible making a definitive conclusion premature (Karpowicz, Gryz et al. 2011). No changes in gene expression were found in exposed or sham-exposed cells at the end of a two-hour exposure for any of the 498 tested protein genes. The results suggest that MRI has no influence on protein-gene expression in eugenic human lung cells (Schwenzer, Bantleon et al. 2007). The results of other studies showed that the static magnetic field alone and MRI sequences at 3 Tesla have no effect on the induction of double–strand breaks (DSBs) in cells (Schwenzer, Bantleon et al. 2007; Simi, Ballardin et al. 2008; Hartwig, Giovan‐ netti et al. 2009). One phenomenon that has been observed is a magneto-hydrodynamic effect (Shellock and Crues 2004). When a conductor moves through a magnetic field, a current is induced in the conductor. This phenomenon is present during the blood flowing through the heart. The current induced in the blood can produce the change in an elevation of the S-T segment on the patient's electrocardiogram (Figure 6). The degree of change is directly related to the strength of the magnetic field. This change is present only when the patient is in the bore of the magnet, and it is not associated with any serious bio-effects. The effects are totally reversible by removing the patient from the magnet. However, because an elevated S-T segment can be indicative of myocardial infarction, ischaemia, or an electrolyte imbalance, it is imperative that any patient with compromised cardiovascular function should be closely monitored with an MRI-compatible pulse oximeter and/or blood pressure monitor (McKenna, Laxpati et al. 2008). Different studies, modelling and calculations of possible exposure dose and time, suggest three groups of adverse effects of the static magnetic field to the cardiovascular system as follows: • minor changes in the rate of heart beat, • induction of ectopic heart beats and • increase in the likelihood of re-entrant arrhythmia (possibly leading to ventricular fibrillation). The first two are thought to have thresholds in excess of 8 T, while the threshold values for increase in the likelihood of re-entrant arrhythmia is difficult to assess because of the modelling complexity. Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 449 Source: Roth, R.T.C. (1996) Figure 6 – Reversible increase in the amplitude of the T-wave noted on electrocardiograms inside the magnet bore In 2006, the World Health Organization stated that there is no evidence on the short- and long-term adverse effects of MRI static MF on human health. With regard to the long-term effects, there are interactions between tissues and static magnetic fields that could theoretically lead to pathologic changes in human subjects. There are no carefully controlled studies that demonstrate the absolute safety of chronic exposure to powerful magnetic fields. Considering the increased use of MR scanners with higher static MF values, there is aneed to perform more studies to provide assurance about their safety (Franco, Perduri et al. 2008). b) Biological effects of gradient fields During an MRI examination, the time-varying (gradient) magnetic fields are often switched on and off. The biological response is based on the opportunity of gradient fields to induce electrical currents in any conductor (so called "eddy currents") and the ability of some biological tissues to act as a conductor. The human body has several excellent conductors: nerves, muscles, and blood (So, Stuchly et al. 2004). The biological effects are related to the changes in the magnetic field that induces the current (Stuart, Trakic et al. 2007). The Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 450 Stikova E magnitude of the induced current depends on the strength and speed of the gradient fields and the resistance of the conductor. The most studied phenomenon that is produced by fast-varying gradient fields is peripheral nerve stimulation (PNS). The time-varying magnetic fields induce an electric field (current), which stimulates nerves and muscles, and this could result in involuntary twitching, especially in the periphery of the bore where the gradient variations are greatest. Direct stimulation of peripheral nerves could cause muscle contractions or sensations of tingling and itching, depending on whether the stimulated nerve is a sensory or motor nerve (Abart, Eberhardt et al. 1997). The peripheral nerve stimulation may cause discomfort to the subjects, resulting in the subject moving in the scanner or possibly requesting the operator to stop the examination (So, Stuchly et al. 2004). The stimulation threshold for nerves and muscles depends on the ratio between rheobase and chronaxie. The rheobase is the minimal electric current of infinite duration (practically, a few hundred milliseconds) that results in an action potential or the contraction of the muscle cell: 6–20 V/m for peripheral nerve and cardiac stimulation and 30–40 V/m for cortex. The calculated rheobase threshold for brain stimulation can be lower for patients with epilepsy, subjects with a family history of seizures, users of anti-depressants, and neuroleptics, making them more vulnerable for MRI examination. Chronaxie is the minimum time over which an electric current twice the strength of the rheobase needs to be applied, in order to stimulate a muscle fibre or nerve cell: 200–350 microseconds for peripheral nerve, 350–450 microseconds for cortex. Several studies in vivo have been performed to obtain gradient-induced stimulation thresholds in animals and in humans (Bourland, Nyenhuis et al. 1999; Bencsik, Bowtell et al. 2002; Formica and Silvestri 2004). The mean thresholds for peripheral stimulation in head and body are similar and the greatest frequency of reported peripheral stimulations occurs when the y-gradient is used (Bourland, Nyenhuis et al. 1999; Den Boer, Bourland et al. 2002). If the stimulation is in the cardiac muscle, it could theoretically disrupt the normal cardiac cycle and lead to an arrhythmia. The cardiac stimulation could cause ventricular fibrillation and it would be a very serious life-threatening condition (Glover 2009, Schaefer, Bourland et al. 2000). Direct stimulation of the retina and/or optic nerve can produce a phenomenon known as magnetophosphenes and it occurs when retinal phosphenes are stimulated by induction from TVMF. Magnetic phosphenes can cause a flashing sensation in the eyes that, together with disturbance of eyehand coordination, could affect the optimal working performances of the staff executing delicate interventional MRI procedures. Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 451 The time varying magnetic fields also produce acoustic noise, which can reach up to 140 dB for some sequences (Shellock, Ziarati et al. 1998). Levels greater than 100 dB may result in disturbance in microcirculation in the brain and produce mechanical damage (McJury 1995; McJury and Shellock 2000). In conclusion, MRI gradients can produce peripheral nerve stimulation, and even cardiac stimulation in extreme cases. With the advent of the new generation of MR systems characterized by higher static MF and faster gradient fields, their effects on human health should be the object of further and properly designed studies. c) Biological effects of radiofrequency fields The primary biological effects associated with exposure to RF radiation are related to the thermogenic qualities of electromagnetic fields. The interactions of RF fields with biological tissues depend on the field frequency, type of field (electric, magnetic, far-field, near-field) and the body size and shape. In the case of MR systems, the spatial distribution of RF energy depends on the design of the transmitter coils, the frequency, and the shape, size and tissue type of the imaged object (Grandolfo, Polichetti et al. 1992; Abart and Ganssen 1995). Fortunately, the human body has a very efficient thermoregulation system and can adequately respond to temperature increase by increasing the capillary flow. Several organs, such as eyes and testicles, cannot quickly respond to heating, mainly because of their very poor capillary network. Because of this they are under increased risk of thermal injury. The parameter used for quantification of the effects is called the specific absorption rate – SAR (Gandhi and Chen 1992; Grandolfo, Polichetti et al. 1992). The SAR is the dose rate, defined as the rate at which RF energy is imparted into a unit mass of the exposed biological body. SAR is measured in watts per kilogram, and its maximum value should be less than 2 W/Kg for the human head, according to the guidelines of the International Commission on Non-Ionizing Radiation Protection – ICNIRP (Ahlbom, Bergqvist et al. 1998). A whole-body averaged SAR of 6.0 W/kg can be physiologically tolerated by individuals with normal thermoregulatory function. Further studies were conducted on volunteers exposed to whole-body average SARs ranging from approximately 0.05 W/kg to 4.0 W/kg. These experiments document that body temperature changes were always less than 0.6°C, though there were statistically significant increases in skin temperature, but without serious physiological consequences (Shellock and Crues 1987; Shellock 2000; Shellock 2002). During a MR scan the patient’s temperature is not easy to measure, so SAR represents a convenient parameter to control any possible temperature increases. Generally, the MRI scanner software allows monitoring of the SAR Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 452 Stikova E for the whole body (Shellock and Crues 1987). If the SAR value exceeds the standard limits, the software stops the scanning process. Various underlying health conditions may affect an individual's ability to tolerate a thermal challenge, including cardiovascular disease, hypertension, diabetes, fever, old age, and obesity. In addition, medications such as diuretics, β-blockers, calcium blockers, amphetamines, muscle relaxants, and sedatives can also greatly alter thermoregulatory responses to a heat load (Shellock and Crues 1987; Shellock 2002). In conclusion, interactions between RF and biological tissues during MR procedures could be unsafe for patients (Formica and Silvestri 2004). Most of the reported accidents are burns due to hot spots in the presence of conducting materials close to the patient such as the leads of equipment for monitoring physiological parameters (heart rate, blood pressure, oxygen saturation and temperature). This kind of risk can be more serious in the case of internal biomedical implants (aneurism clips, stents, etc.) especially for implants that have elongated configurations and/or are electronically activated (neurostimulation systems, cardiac pacemakers) (Dempsey and Condon 2001; Kanal, Borgstede et al. 2004). III. SAFETY ISSUES IN MRI The technology used for magnetic resonance (MR) procedures has evolved continuously, yielding MR systems with stronger static magnetic fields, faster and stronger gradient magnetic fields, and more powerful radiofrequency transmission coils. Most reported cases of MR-related injuries and the few fatalities that have occurred have apparently been the result of failure to follow safety guidelines, or of use of inappropriate or outdated information related to the safety aspects of biomedical implants and devices. To prevent accidents in the MR environment, therefore, it is necessary to revise the information on biological effects and safety according to changes that have occurred in MR technology and with regard to current guidelines for biomedical implants and devices. All staff must be aware of and trained to eliminate the MR hazards. It is important to emphasize that many safety investigations have been carried out on 1.5T scanners, although in the last few years many centres install magnets of 3.0T and above. Because of this, further investigations will be regularly required to reassure staff and patients of their safety. The MR safety policy and procedure should be reviewed and adjusted to the newest scientific results and evidence-based information. This should apply to all segments of the MRI environment – equipment, working regime (e.g. adding faster or stronger gradient capabilities or higher RF duty cycle studies), hazard identification, measurement, workplace risk assessment and health Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 453 surveillance of exposed workers. The establishment of obligatory screening forms for all patient, staff, family members and other people who enter in appropriate MR’ zones is a very important part of safety practices. Finally, the appointment of a well-trained and experienced MR safety officer for all MRI suites is essential for the development, implementation and maintenance of the appropriate safety procedure. Along with these people-oriented strategies of policies and training, organizations also need to adopt the strategies of safety-oriented architectural and interior design (International Commission on Non-Ionizing Radiation 2009). Usually, MR equipment manufacturers provide design safety templates that meet the minimum technical sitting requirements for the specific equipment. However, appropriate procedures for design of patient/family waiting area, interview areas, physical screening/changing areas, access controls, storage, crash carts, induction, medical gas services, holding areas for patients after screening, infection control provisions, and interventional applications, are not usually addressed in a typical vendor-provided safety design template. a) Safety issues related to the static magnetic fields Most safety issues concerning strong static magnetic fields are related to the effects caused by the stray magnetic field (Baltisberger, Hediger et al. 2005). The portion of the stray static magnetic field that extends outside of the bore of the magnet is called the fringe field (Kok, Raaymakers et al. 2009); this field is measured in gauss (G) units. The fringe field should be less than or equal to 5 G at the outside perimeter of the room (Iwamiya and Sinton 1996; Kanal, Borgstede et al. 2002; Barbic and Scherer 2006). The extent of the fringe field depends on: • the main magnet field strength, • the design of the magnet (open versus tunnel bore), and • the shielding (active versus whole room shielding). Source: Roth, R.T.C. (1996) Figure 7 – Stray magnetic field – fringe field at the edges of the magnet bore Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 454 Stikova E Projectiles The strong static magnetic field can attract ferromagnetic metal objects, which can act as projectiles. The strength of attraction is inversely proportional to the square of the distance, which means that the force quadruples as the object's distance from the bore is halved. A ferromagnetic object can reach speeds of up to 45 miles per hour on its way into a 1.5-T magnet. Such iron-containing metal objects can become powerful projectiles and can cause serious injury or even death (Chaljub, Kramer et al. 2001). All equipment, regardless of its function, should be tested with a strong hand magnet of at least 3000 G before it is used in or around the MR scanner. If the equipment is found safe after testing, it should be labelled as MRI-safe and used only in the MRI suite (Gilk 2006; Gilk 2007; Gilk 2009; Gill and Shellock 2012). Torque Magnetically induced torque causes objects to rotate to align along the magnet’s field lines. Torque is a twisting force on objects and is greatest in the centre of the bore magnet, where it can cause ferromagnetic implants and foreign bodies to align with the magnetic field. The potential for an injury depends on the strength of the magnetic field, type and location of the implant, physical dimensions and orientation of the implant, and the length of time the implant has been in place (Becker, Norfray et al. 1988). The two greatest potential complications of implant-related torque are the eyes and brain. All patients with a history of metal-related eye injury and/or sheet metal work or welding that do not have positive confirmation of the absence of intra-ocular metal should be screened with conventional x-rays before undergoing MRI. Research has indicated that metal fragments too small to be seen on conventional radiographs (i.e. smaller than 0.1 × 0.1 × 0.1 mm) are too small to damage the ocular tissue. Also, because intracranial aneurysm clips can be ferromagnetic, implants in the brain should be approached with caution. All patients with intracranial aneurysm clips should be excluded from MRI unless the clip was tested before implantation. If the clip demonstrates no attraction, it is probably MRI-compatible and the patient's operative notes should be annotated accordingly (Shellock and Shellock 1999; Shellock and Spinazzi 2008). Other devicies that could produce implant-related torque effects are: • Heart valves, • Dental devices and materials (12 of 16 dental implants showed measurable deflection to the magnetic field), • Otological implants, Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 455 • Ocular implants, • Intra-ocular ferrous foreign bodies, • Orthopaedic implants, materials and devices, • Surgical clips and pins, • Electrically, magnetically or mechanically activated or electrically conductive implanted devices, • Pacemakers – cardiac pacemakers are an absolute contraindication for MRI. (Martin, Coman et al. 2004; Shinbane, Colletti et al. 2007; Shinbane, Colletti et al. 2011). Most forms of medical or biostimulation implants are generally considered contraindications for MRI scanning. These include pacemakers,vagus nerve stimulators, implantable cardioverter-defibrillators, loop recorders, insulin pumps, cochlear implants, deep brain stimulators and capsules retained from capsule endoscopy (Teitelbaum, Bradley et al. 1988). Patients are therefore always asked for complete information about all implants before entering the room for an MRI scan. Several deaths have been reported in patients with pacemakers who have undergone MRI scanning without appropriate precautions (Shinbane, Colletti et al. 2011). To reduce such risks, implants are increasingly being developed to make them MR safe, and specialized protocols have been developed to permit the safe scanning of selected implants and pacing devices. Cardiovascular stents are considered safe, as are titanium and its alloys (Teitelbaum, Bradley et al. 1988; Teitelbaum, Yee et al. 1990). Labelling In 1997, the FDA's Center for Devices and Radiological Health (CDRH) first proposed terms to be used to label MRI information for medical devices. At that time devices were classified as MR safe or MR compatible (Shellock, Woods et al. 2009). In 2005 the terminology was revised to adapt to the increasing variety of available MR scanners and to make it clearer that MR compatible devices are not necessarily MR safe. The current labelling categories are: • MR Safe – an item that poses no known hazards in all MRI environments. "MR Safe" items are non-conducting, non-metallic, and non-magnetic. The "MR Safe" icon consists of the letters ‛MR’ in green in a white square with a green border, or the letters ‛MR’ in white within a green square. • MR Conditional – an item that has been demonstrated to pose no known hazards in a specified MR environment with specified conditions of use. The special conditions for use are determined by listing the acceptable static magnetic field strength, spatial gradient magnetic field, slew rate (time rate of change of the magnetic field), radio frequency (RF) fields, and specific absorption rate (SAR). The "MR Conditional" icon consists of the letters ‛MR’ in Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 456 Stikova E black inside a yellow triangle with a black border. A device or implant would be MR conditional if it contains magnetic, electrically conductive or RF-reactive components that are safe for operations in proximity to the MRI, under the defined conditions for safe operation (such as 'tested safe up to 1.5 Tesla' or 'safe in magnetic fields below 500 Gauss') (Greenberg, Weinreb et al. 2011). • MR Unsafe – an item that is known to pose hazards in all MRI environments. MR Unsafe items include magnetic items. The "MR Unsafe" icon consists of the letters ‛MR’ in black on a white field inside a red circle with a diagonal red band. MR SAFE MR CONDITIONAL MR UNSAFE Source: Kanal, E., A. J. Barkovich, et al. (2007) Figure 8 – Safety labelling icons used in the MRI environment Signs should be posted to deter possible entry into the scan room with ferromagnetic objects and to prevent the occurrence of a possible dangerous event (Shellock, Woods et al. 2009). The very high strength of the magnetic field can also cause "missileeffect" accidents, where ferromagnetic objects are attracted to the centre of the magnet, and there have been incidences of injury and death. To reduce the risks of projectile accidents, ferromagnetic objects and devices are typically prohibited in proximity to the MRI scanner and patients undergoing MRI examinations are required to remove all metallic objects and fill out pre-screening forms for identification of risky issues (Sawyer-Glover and Shellock 2000). Zoning of MR facilities and working positions The MRI environment is the area within the 0.50 mT (5 Gauss) line of an MR system, which includes the entire three-dimensional volume of space surrounding the MR scanner. For cases where the 0.50 mT line is contained within the Faraday shielded volume, the entire room is considered to be the MR environment (Robitaille, Warner et al. 1999). The MRI related space is divided in two categories: Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 457 • A Controlled area is any area where the static magnetic field may exceed 0.5 mT, or where gradient or RF fields may interfere with electronic devices. This area should be controlled, by warning signs or some other means, in order to exclude people who may have pacemakers, or implanted defibrillators or neurostimulators. Any areas adjacent to the MRI equipment to which there is unrestricted access (corridors, adjacent rooms or outside areas) should have fields less than 0.5 mT and be shielded from RF fields. • A Restricted area is any area where the static magnetic fields may exceed 3 mT, and it should be restricted to qualified MRI staff, or people under the supervision of such staff. Qualified MRI staff are expected to be aware of precautions which must be taken inside such areas and the possible hazards that may arise. This would normally include MRI operating staff and maintenance engineers, and possibly trained cleaning staff. Ferromagnetic materials, and anything which has not been shown to be compatible with MRI equipment, should not be brought into the restricted area (Shellock and Crues 2004). The controlled and restricted areas of the MR site are conceptually divided into four zones (Kanal, Barkovich et al. 2007) and they are shown in Figure 9 below. Zone I: This area is freely accessible to the general public and typically is outside the MR environment itself. This is the place through which patients, health care personnel, and other employees of the MR site access the MR environment. Zone II: This area is the interface between the publicly accessible, uncontrolled Zone I and the strictly controlled Zones III and IV. Typically, patients’ movement in Zone II is not free and should be supervised by MR personnel. Zone III: This area is the region large enough to contain the 0.5 mT (5 Gauss) magnetic field contour and in which free access of unscreened non-MR personnel is not allowed. The use of any ferromagnetic objects or equipment can result in serious injury or death. All access to Zone III is strictly restricted, and all entrances should be controlled and supervised by MR personnel. The access to Zone III should be physically restricted by key locks, passkey locking systems, or any other reliable, physically restricting method. Usually this zone is called a controlled area. The access restrictions should be displayed at all entrances in accordance with the IEC 60601-2-33 standard. Zone IV: This area is the magnet room where the MR scanner is located. This zone is laid out to contain the 3 mT (30 Gauss) magnetic field contour and the so-called inner controlled area. Zone IV, by definition, will always be located within Zone III. Zone IV should also be demarcated and clearly marked because of the presence of very strong magnetic fields. Zone IV should be clearly marked with a red light and lighted sign stating, "The Magnet is On". The movement of staff in this area is restricted, and exposure assessment should Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 458 Stikova E be observed in the scope of the usually measured and proposed values of magnetic strength near the bore of the magnet. Source: Kanal, E., A. J. Barkovich, et al. (2007) Figure 9 – Typical zone configuration in MRI facilities and strength of the static magnetic field The MRI activities of MRI staff level II in MRI room (zone IV) are performed in 4 typical areas (Stuart, Trakic et al. 2007) as folows: • Area A – whole body exposure, • Area B – exposure of hand and/or head if the worker is leaning towards the patient, • Area C – hand exposure, • Area D – hand and/or whole body exposure when the worker approaches very closely to the patient leaning against the magnet bore. Figures 10 shows the typical position and working operation of the MR staff in zone IV and the typical average strength of the static magnetic field. This Figure 10 – Clasification of the zone 4 regarding the strength of the static field Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 459 information would be very useful for estimation of occupational exposure, especially in a case of lack of nationally permitted total exposure and action levels and personal dosimeters. Classification of MR Personnel The classification of the MR personnel is made using the criteria for MRI environment zoning and in accordance with the risk of the general public, patients and staff. The main purpose for this classification is to determine the movement restriction and to prevent adverse health effects and dangerous events. The main criteria for this classification are justification of the need for entrance to the MRI environment based on education level, job activities and safety training (Kanal, Barkovich et al. 2007). Regarding these criteria, there are three categories of workers with permission to enter and move through the MRI environment zones: • Level 1 MR Personnel Individuals who have passed minimal safety educational efforts to ensure their own safety while working in Zone III will be referred to as level 1 MR personnel (e.g. MRI department office staff and patient aides). They are responsible for accompanying non-MRI personnel throughout zone III. • Level 2 MR Personnel Individuals who have been more extensively trained and educated in the broader aspects of MR safety issues, including issues related to the potential for thermal loading or burns and direct neuromuscular excitation from rapidly changing gradients, will be referred to as level 2 MR personnel (e.g., MRI technologists, radiologists, and radiology department nursing staff). They are permitted to move through all zones and they are responsible for the admission of patient and other non-MRI personnel to zone IV. • Non-MR Personnel Non-MR personnel are all patients, visitors, or facility staff who do not meet the criteria of level 1 or level 2 MR personnel. All non-MR personnel wishing to enter Zone III must first pass an MR safety screening process using the same screening form as patient, non-MRI and MRI personnel. Only MR personnel are authorized to perform an MR safety screen before permitting non-MR personnel into Zone III (Kanal, Borgstede et al. 2002; Kanal, Borgstede et al. 2004; Kanal, Barkovich et al. 2007). b) Safety issues related to the effects of MR time-varying fields Acoustic noise As current is passed through the gradient coils during image acquisition, a significant amount of acoustic noise is generated (Price, De Wilde et al. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 460 Stikova E 2001). the noise results from Lorentz forces in the gradient coils and the noise levels could be as high as 140 dB. As gradient amplitudes increase and rise times decrease, the acoustic noise becomes greater. MRI noise may cause the patient annoyance, anxiety, difficulties in verbal communication, distress, temporary hearing loss and even potential permanent hearing problems (Kanal, Borgstede et al. 2004; Kanal, Barkovich et al. 2007). Temporary hearing loss has been reported using conventional MRI sequences. Gradient noise may also interfere with patient communication or affect staff and visitors (McJury, Blug et al. 1994; McJury, Stewart et al. 1997; McJury and Shellock 2000). An acceptable and inexpensive means for the prevention of hearing loss is the regular use of disposable earplugs. Earplugs should be made available to anyone present in the imaging room during a scan, especially if noise levels exceed 94 dBA. Commercially available earplugs can reduce the noise levels associated with MRI by as much as 20 decibels (McJury, Stewart et al. 1997). There are also commercially available noise cancellation systems or anti-noise systems that reportedly can lower the noise levels by up to 70% (Price, De Wilde et al. 2001). Peripheral nerve stimulation (PNS) All commercial MRI scanners have a limit on the maximum slew rate (dB/dt) allowed, preventing the fast gradient switching that causes PNS. While most MRI sequences are well below the slew rate (dB/dt) limit, sequences that utilize echo-planar imaging (fMRI, diffusion) can sometimes result in peripheral nerve stimulation and cause the subject discomfort. In such cases, the subject should notify the operator, and the scan should be aborted. c) Safety issues related to the effects of RF electromagnetic fields Heating of implants and other medical devices RFelectromagnetic waves can cause heating in metallic implants and foreign bodies by inducing a current (Nitz, Brinker et al. 2005). Without a pathway to exit the body, the current builds up, and the implant gets warm. The degree of warming depends on the strength and rate of change of the magnetic field and the conductivity of the implant. Military shrapnel, metal slivers, and wires are all susceptible to heating. If these items are located in or around the eyes, spine, heart, or brain, serious and irreversible damage can occur (Schaefer, Bourland et al. 2000). Heat stress Pulses of radio-frequency (RF) energy heat the body. This heat can be dissipated by the body, provided that the rate of heating is not excessive(Nitz, Brinker et al. 2005). The human body has a very efficient thermoregulatory system and can handle reasonable changes in temperature. Even though the eyes Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 461 and testicles have a poor capilary network and cannot quickly dissipate the heat by increasing capillary flow, the risks are believed to be minimal. Some conditions (cardiovascular disease, hypertension, diabetes, fever, old age and obesity) and some medications (diuretics, beta-blockers, calcium blockers, amphetamines, muscle relaxants and sedatives) may impair the normal cooling mechanisms. There are no adverse effects in the case of whole body exposure if the rise in the core body temperature is less than 1oC for healthy adults and less than 0.5oC for infants and persons with cardio-circulatory impairment (Shellock 2000). Thermal burns While not very common, thermal burns can occur, especially in patients who are sedated during the scan. Tattoos and permanent cosmetics realized with iron oxide or other metal-based pigments can cause reactions or adverse events, including first and second-degree local burns. Certain types of underclothing with antimicrobial silver microfibres (usually worn under braces to prevent infection) have also resulted in local burns, so the best safety practice is to ask the subjects to change into a hospital supplied gown. Also, during the scan the subjects should be discouraged from crossing or forming loops with their arms, to prevent induction of currents in the extremities. d) Other MR related safety issues Quench – cryogen safety Currently, all superconducting magnets use liquid helium to maintain the magnet coils at a temperature enabling superconductivity. The helium and magnet coils are maintained in a vacuum. The temperature of liquid helium is approximately -269°C or 4.17 degrees K, close to the liquid helium boiling temperature. Any disruption to the temperature or loss of the vacuum will cause the liquid helium within the magnet to "boil off" causing an immediate and sudden loss of the magnetic field. This event is referred to as a "quench". When this occurs, the helium will expand and for every litre of liquid helium, 760 litres of gas will be produced. This marked expansion in volume causes the gas to rush out of the magnet and, under normal conditions, be vented outside the scan room and building. In the event of a quench, the patient should be removed from the scan room as quickly as possible. Although not immediate, asphyxiation can occur from breathing helium. Additionally, because of the extremely cold temperature of helium gas, frostbite is also a concern. The quench produces a marked increase in air pressure inside the scan room, which makes it difficult to open the scan room’s exit door immediately. In the event of a large change in room pressure, ruptured eardrums are also a possibility. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 462 Stikova E Every site should have a written policy establishing what to do in the event of a quench. MR equipment (including the examination room and any other areas where the coolant may be stored) should be installed with an appropriate exhaust system to vent gases to the outside in the event of a quench. As a precaution in a case of quenching, an emergency evacuation procedure should be established and rehearsed. Oxygen monitors with an alarm audible in the control room should be in the examination room and other areas where coolants are stored. It is recommended that emergency quench buttons be installed both inside and outside the examination room. Contrast agent safety Several Gadolinium-based contrast agents have been introduced, and more are in development. Adverse reactions have been relatively few and mostly minor, and cautionary notes are included with the packaging. Contrast agents should be administered with the same care and attention as any other pharmaceutical product (Kanal, Broome et al. 2008). Some agents have been shown to cross the placenta readily. When the rate of clearance from the amniotic fluid is not known, a careful assessment of the possible risks and benefits of contrast agents in pregnant women should be made. Caution should be exercised before administering contrast agents to lactating mothers, as some agents are excreted in breast milk. There are no well-defined policies for patients who are considered to be at increased risk for having an adverse reaction to MR contrast agents. However, patients who have previously reacted to one MR contrast agent, all patients with asthma or a history of allergic respiratory disorders are at higher risk of adverse reaction and they should be premedicated with corticosteroids and antihistamines (Kanal, Barkovich et al. 2007). Another contrast-based safety issue is the occurrence of a very rare disease known as nephrogenic systemic fibrosis (NSF). The disease is seen only in patients with severely impaired renal function. The first case was observed in 1997 and the disease was formally described in 2000 (Shellock, Parker et al. 2006; Kuo, Kanal et al. 2007). A few weeks or months prior to the onset of the disease the patients had been administered gadolinium-based MR contrast agents (GBMRCA). Literature data from Denmark suggest that 5% of patients with severely impaired renal function treated with GBMRCA developed NSF. The disease is characterized with increased tissue deposition of collagen (Boyd, Zic et al. 2007), often resulting in thickening and tightening of the skin, predominantly of the distal extremities but also of the trunk, as well as fibrosisof other parts of the body (heart, lungs, kidneys, periphery vasculaturesand skeletal muscles) (Boyd, Zic et al. 2007). The disease is progressive and can be fulminant in approximately 5% of cases and can even be associated with a fatal Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 463 outcome (Broome, Girguis et al. 2007). The disease predominantly affects middle-aged patients, with special predilection for patients with concurrent hepatic disease (Grobner and Prischl 2008). Based on the literature data, for patients with moderate to end-stage kidney disease, imaging methods other than MRI with a gadolinium-based contrast agent should be recomended whenever possible (Kanal, Broome et al. 2008). If these patients must receive a gadolinium-based contrast agent, prompt dialysis following the MRI or MRA should be considered because the average excretory rates of gadolinium is 78%, 96%, and 99% in the first to third haemodialysis sessions. Special recommendation and guidelines are developed for patients with kidney diseases (Grobner and Prischl 2007; Rosenkranz, Grobner et al. 2007). The ACR Contrast Committee and the Subcommittee for MR Safety recommends pre-screening of patients prior to the administration of Gadolinium-based MR Contrast Agents (GBMCA). It is recommended that prior to elective Gadolinium-based MR Contrast Agent (GBMCA) administration, a recent (e.g. last 6 weeks) Glomerular Filtration Rate (GFR) assessment be reviewed for patients with a history of: renal disease (including solitary kidney, renal transplant, renal tumour), age > 60, history of hypertension, history of diabetes, history of severe hepatic disease/liver transplant/pending liver transplant (Kanal, Borgstede et al. 2004; Kanal, Barkovich et al. 2007; Kuo, Kanal et al. 2007). Claustrophobia Some patients may experience claustrophobia, even if they have no personal or family history of the condition. This may be precipitated by the restricted space inside the MR bore, anxiety about the scan and the possible outcome, noise, and the duration of the examination (Kanal, Borgstede et al. 2002; Kanal, Borgstede et al. 2004; Kanal, Barkovich et al. 2007). Staff should be aware that claustrophobic reactions may occur, and of the techniques which may avert them. Although the majority of these effects are transient, it is important to have controllable air movement within the bore of the magnet to maintain a comfort zone for patients (Spouse and Gedroyc 2000). This, along with good patient contact and education, could help reduce claustrophobic reactions, which clearly are a safety concern (Kanal, Borgstede et al. 2004). Patient preparation and screening forms Patient preparation involves many steps. The patient should be instructted to wear loose, comfortable clothing without zippers, snaps, or buttons (Shellock and Spinazzi 2008; International Commission on Non-ionizing Radiation 2009) For most examinations, patients can wear elastic-waisted, cotton sweat Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 464 Stikova E pants and a plain T-shirt. Female patients should wear a sports bra without hooks or wires; any other type of bra should be removed before the patient enters the room. All accessories should be removed. Accessories include rings, bracelets, watches, earrings, and body piercings. Face and eye make-up should also be removed. If the patient arrives wearing clothes with zippers or other metal, he/she should change into an appropriate gown (Shellock and Spinazzi 2008). The gowns should have loose-fitting sleeves so that the technologist can check for watches and bracelets; loose sleeves are also an asset if the patient requires an injection of contrast agent. The patient gowns should not have pockets. It will be much more difficult for a patient to accidentally bring contraindicated materials into the room without pockets (Kanal, Borgstede et al. 2002; Kanal, Borgstede et al. 2004; Kanal, Barkovich et al. 2007). Occupational risk, standards and classification Many organizations are involved in MRI safety and health regulation and almost all of them are part of the World Health Organization’s framework. The leading organization for producing and implementation of MRI safety standards and guidelines is the International Commission of Non-ionizing Radiation Protection (ICNIRP). Usually their proposals and guidelines are incorporated in EU Directives and standards produced by the European Committee for Electrotechnical Standardization (CENELEC), International Technical Commission (IEC) and Institute of Electrical and Electronics Engineers (IEEE). How they are connected between them and how they can support the preparation and adoption of the national legislation is shown in the figure below. Figure 11 – Organizations involved in EMF Regulation and Standardization Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 465 The main document dealing with occupational exposure of workers in Europe is the physical agents directive (PAD) 2004/40/EC. In addition to protecting workers occupationally exposed to non-ionizing radiation, the implementation of this Directive into EU legislation would have limited the use of MRI, due to the restrictive exposure limits for MR staff. As a result of strong opposition from the MRI community, Directive 2004/40/EC was amended by Directive 2008/46/EC in April 2008, with the effect of postponing by four years the deadline for transposition of Directive 2004/40/EC. On June 14, 2011 the European Commision adopted a proposal to derogate the medical and research use of MRI from the exposure limit values. Workers using MRI will be protected through existing regulations, which ensure its safe use. The established MR safety standard IEC/EN 60601–2–33 defines criteria for minimizing physiological effects due to exposure to time-varying electromagnetic fields, thus aiming to eliminate danger to patients and workers. In the light of these recent proposals, many MR safety studies have been conducted since 2004. A 2008 review summarized the studies on the health effects of occupational exposure to static magnetic fields, and no firm conclusions were drawn about these effects (Perrin and Morris 2008). However, there are still concerns about workers repeatedly exposed to magnetic fields exceeding regulatory limits with respect to modern MRI. There is a proposal for a mandatory ambulatory magnetic field dosimeter capable of measuring the fields in and around an MRI scanner in order to evaluate the regulatory guidelines and determine any underlying exposure risks. The numerical analysis shows that at certain positions surrounding the MRI scanner edges, such fields may induce current densities and electric fields that may exceed the relevant EU, ICNIRP, and IEEE standards (Fuentes, Trakic et al. 2008; International Commission on Non-ionizing Radiation 2009). Usually, the time-weighted average magnetic field exposures in 1.5 T, 2 T, and 4 T were all within the regulatory limits but the peak limits for the exposure of the head to static magnetic field measurements can be exceeded in some circumstances, especially when workers are standing close to the gradient coils and when all three gradients are switched on simultaneously (Gilk 2007; Fuentes, Trakic et al. 2008). Conclusion As the number of MRI scanners rises and the MRI technology advances, there is a growing need for understanding the biological effects of MRI and for maintaining the safety of the patients and the MR personnel. While the effects of exposure to MRI fields remain an active research area, clinical experience shows that MRI is a safe imaging modality, and that most of the risks are preventable by obeying the safety guidelines listed above. Coordination betPrilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 466 Stikova E ween local regulatory bodies and the organizations involved in EMF regulation and standardization is essential for keeping the guidelines current and for ensuring that MRI remains a safe diagnostic procedure. REFERENCES Abart J, Eberhardt K. et al. "Peripheral nerve stimulation by time-varying magnetic fields." J Comput Assist Tomogr. 1997; 21(4): 532–538. Abart J. and Ganssen A. "[Safety aspects in MR imaging]." Aktuelle Radiol. 1995; 5(6): 376–384. Ahlbom A, Bergqvist U, et al. "Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (up to 300 GHz). International Commission on Non-Ionizing Radiation Protection." Health Phys. 1998 ; 74(4): 494–522. Baltisberger JH, Hediger S. et al. "Multi-dimensional magnetic resonance imaging in a stray magnetic field." J Magn Reson. 2005; 172(1): 79–84. Barbic M. and Scherer A. "Stray field magnetic resonance tomography using ferromagnetic spheres." J Magn Reson. 2006; 181(2): 223–228. Becker RL, Norfray JF. et al. "MR imaging in patients with intracranial aneurysm clips." AJNR Am J Neuroradiol. 1988; 9(5): 885–889. Bencsik M, Bowtell R. et al. "Electric fields induced in the human body by time-varying magnetic field gradients in MRI: numerical calculations and correlation analysis." Phys Med Biol. 2007; 52(9): 2337–2353. Bencsik M, Bowtell R. et al. "Electric fields induced in a spherical volume conductor by temporally varying magnetic field gradients." Phys Med Biol. 2002; 47(4): 557–576. Bourland JD, Nyenhuis JA. et al. "Physiologic effects of intense MR imaging gradient fields." Neuroimaging Clin N Am. 1999; 9(2): 363–377. Boutin RD, Briggs JE. et al. "Injuries associated with MR imaging: survey of safety records and methods used to screen patients for metallic foreign bodies before imaging." AJR Am J Roentgenol. 1994 ; 162(1): 189–194. Boyd AS, Zic JA. et al. "Gadolinium deposition in nephrogenic fibrosing dermopathy." J Am Acad Dermatol. 2007; 56(1): 27–30. Broome DR, Girguis MS. et al. "Gadodiamide-associated nephrogenic systemic fibrosis: why radiologists should be concerned." AJR Am J Roentgenol. 2007; 188(2): 586–592. Chaljub G, Kramer LA. et al. "Projectile cylinder accidents resulting from the presence of ferromagnetic nitrous oxide or oxygen tanks in the MR suite." AJR Am J Roentgenol. 2001; 177(1): 27–30. Colletti PM. "Size "H" oxygen cylinder: accidental MR projectile at 1.5 Tesla." J Magn Reson Imaging. 2004; 19(1): 141–143. Colletti PM, Shinbane JS. et al. "MR-conditional" pacemakers: the radiologist's role in multidisciplinary management." AJR Am J Roentgenol. 2011; 197(3): W457– 459. Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 467 Coskun O. "Magnetic resonance imaging and safety aspects." Toxicol Ind Health. 2011; 27(4): 307–313. Crozier S, Wang H. et al. "Exposure of workers to pulsed gradients in MRI." J Magn Reson Imaging. 2007; 26(5): 1236–1254. Dempsey MF. and Condon B. "Thermal injuries associated with MRI." Clin Radiol. 2001; 56(6): 457–465. Dempsey MF, Condon B. et al. "MRI safety review." Semin Ultrasound CT MR. 2002; 23(5): 392–401. Den Boer JA, Bourland JD. et al. "Comparison of the threshold for peripheral nerve stimulation during gradient switching in whole body MR systems." J Magn Reson Imaging. 2002; 15(5): 520–525. Formica D. and Silvestri S. "Biological effects of exposure to magnetic resonance imaging: an overview." Biomed Eng Online. 2004; 3: 11. Franco G, Mora E. et al. "Focusing ethical dilemmas of evidence-based practice in SMF-exposed MRI-workers: a qualitative analysis." Int Arch Occup Environ Health. 2010; 83(4): 417–421. Franco G, Perduri R. et al. "[Health effects of occupational exposure to static magnetic fields used in magnetic resonance imaging: a review]." Med Lav. 2008; 99(1): 16–28. Fuentes MA, Trakic A. et al. "Analysis and measurements of magnetic field exposures for healthcare workers in selected MR environments." IEEE Trans Biomed Eng. 2008; 55(4): 1355–1364. Gandhi OP. and Chen JY. "Absorption and distribution patterns of RF fields." Ann N Y Acad Sci. 1992; 649: 131–143. Gilk T. "Dangerous attraction. MRI equipment siting should not be taken lightly." Health Facil Manage. 2006; 19(5): 33–37. Gilk T. "Safety first: 'MR facility design guidelines' takes planners through the process." Health Facil Manage. 2007; 20(5): 41–43. Gilk T. "Magnetic attraction. Joint Commission turns its attention to MRI safety." Health Facil Manage. 2009; 22(5): 33–34. Gill A. and Shellock FG. "Assessment of MRI issues at 3-Tesla for metallic surgical implants: findings applied to 61 additional skin closure staples and vessel ligation clips." J Cardiovasc Magn Reson. 2012; 14: 3. Glover PM. "Interaction of MRI field gradients with the human body." Phys Med Biol. 2009; 54(21): R99–R115. Grandolfo M, Polichetti A. et al. "Spatial distribution of RF power in critical organs during magnetic resonance imaging." Ann N Y Acad Sci. 1992; 649: 176–187. Greenberg KL, Weinreb J. et al. "MR conditional" respiratory ventilator system incident in a 3-T MRI environment." Magn Reson Imaging. 2011; 29(8): 1150–1154. Grobner T. and Prischl FC. "Gadolinium and nephrogenic systemic fibrosis." Kidney Int. 2007; 72(3): 260–264. Grobner T. and Prischl FC. "Patient characteristics and risk factors for nephrogenic systemic fibrosis following gadolinium exposure." Semin Dial. 2008; 21(2): 135–139. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 468 Stikova E Gryz K. and Karpowicz J. "[Measurements of electromagnetic fields and evaluation of occupational exposure: PN-T-06580:2002 requirements and principles adopted in the European Union]." Med Pr. 2003; 54(3): 279–284. Hansson Mild K, Alanko T. et al. "Exposure of workers to electromagnetic fields. A review of open questions on exposure assessment techniques." Int J Occup Saf Ergon. 2009; 15(1): 3–33. Hartwig V, Giovannetti G. et al. "Biological effects and safety in magnetic resonance imaging: a review." Int J Environ Res Public Health. 2009; 6(6): 1778–1798. Hartwig V, Vanello N. et al. "A novel tool for estimation of magnetic resonance occupational exposure to spatially varying magnetic fields". MAGMA. 2011; 24(6): 323–330. International Commission on Non-Ionizing Radiation, P. "Amendment to the ICNIRP "Statement on medical magnetic resonance (MR) procedures: protection of patients". Health Phys. 2009; 97(3): 259–261. International Commission on Non-Ionizing Radiation, P. "Guidelines on limits of exposure to static magnetic fields. Health Phys. 2009; 96(4): 504–514. Iwamiya JH. and Sinton SW. "Stray-field magnetic resonance imaging of solid materials". Solid State Nucl Magn Reson. 1996; 6(4): 333–345. Kanal E, Barkovich AJ. et al. "ACR guidance document for safe MR practices: 2007." AJR Am J Roentgenol. 2007; 188(6): 1447–1474. Kanal E, Borgstede JP. et al. "American College of Radiology White Paper on MR Safety: 2004 update and revisions." AJR Am J Roentgenol. 2004; 182(5): 1111– 1114. Kanal E, Borgstede JP. et al. "American College of Radiology White Paper on MR Safety." AJR Am J Roentgenol. 2002; 178(6): 1335–1347. Kanal E, Broome DR. et al. "Response to the FDA's May 23, 2007, nephrogenic systemic fibrosis update." Radiology. 2008; 246(1): 11–14. Kanal E. and Shellock FG. "Burns associated with clinical MR examinations". Radiology. 1990; 175(2): 585. Kanal E, Shellock FG. et al. "Safety considerations in MR imaging." Radiology. 1990; 176(3): 593–606. Kangarlu A, Burgess RE. et al. "Cognitive, cardiac, and physiological safety studies in ultra high field magnetic resonance imaging." Magn Reson Imaging. 1999; 17(10): 1407–1416. Karpowicz J. and Gryz K. "[Limitations of occupational exposure to electromagnetic fields adopted by Polish law from the perspectives of international documents with particular reference to fields of low and medium frequencies]." Med Pr. 2003; 54(3): 269–278. Karpowicz J. and Gryz K. "Health risk assessment of occupational exposure to a magnetic field from magnetic resonance imaging devices." Int J Occup Saf Ergon. 2006; 12(2): 155–167. Karpowicz J, Gryz K. et al. "[Exposure to static magnetic field and health hazards during the operation of magnetic resonance scanners]." Med Pr. 2011; 62(3): 309–321. Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 469 Karpowicz J, Hietanen M. et al. "EU Directive, ICNIRP guidelines and Polish legislation on electromagnetic fields." Int J Occup Saf Ergon. 2006; 12(2): 125–136. Kavet R, Stuchly MA. et al. "Evaluation of biological effects, dosimetric models, and exposure assessment related to ELF electric- and magnetic-field guidelines." Appl Occup Environ Hyg. 2001; 16(12): 1118–1138. Kok JG, Raaymakers BW. et al. "Installation of the 1.5 T MRI accelerator next to clinical accelerators: impact of the fringe field." Phys Med Biol. 2009; 54(18): N409– 415. Kuo PH, Kanal E. et al. "Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis." Radiology. 2007; 242(3): 647–649. Martin ET, Coman JA. et al. "Magnetic resonance imaging and cardiac pacemaker safety at 1.5-Tesla." J Am Coll Cardiol. 2004; 43(7): 1315–1324. McJury M, Blug A. et al. "Short communication: acoustic noise levels during magnetic resonance imaging scanning at 1.5 T." Br J Radiol. 1994; 67(796): 413–415. McJury M. and Shellock FG. "Auditory noise associated with MR procedures: a review." J Magn Reson Imaging. 2000; 12(1): 37–45. McJury M, Stewart RW. et al. "The use of active noise control (ANC) to reduce acoustic noise generated during MRI scanning: some initial results." Magn Reson Imaging. 1997; 15(3): 319–322. McJury MJ. "Acoustic noise levels generated during high field MR imaging." Clin Radiol. 1995; 50(5): 331–334. McKenna, DA, Laxpati M. et al. "The prevalence of incidental findings at cardiac MRI." Open Cardiovasc Med. 2008; J 2: 20–25. Moratal D, Marti-Bonmati L. et al. "[European Directive 2004/40/EC on workers' exposure to electromagnetic fields from MRI]". Radiologia. 2009; 51(1): 30–37; quiz 120–121. Nitz WR, Brinker G. et al. "Specific absorption rate as a poor indicator of magnetic resonance-related implant heating." Invest Radiol. 2005; 40(12): 773–776. OECD Health Data 2011. OECD StatExtracts. Available at: http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT#. Accessed on: March 30, 2012. OECD Health data 2011. OECD StatExtracts. Available at: http://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_PROC#. Accessed on: March, 30, 2012. Perrin NM. and Morris CJ. "A survey of the potential impact of the European Union Physical Agents Directive (EU PAD) on electromagnetic fields (EMF) on MRI research practice in the United Kingdom." J Magn Reson Imaging. 2008; 28(2): 486– 492. Picano E. "Sustainability of medical imaging." BMJ. 2004; 328(7439): 578– 580. Price DL, JP. De Wilde, et al. "Investigation of acoustic noise on 15 MRI scanners from 0.2 T to 3 T." J Magn Reson Imaging. 2001; 13(2): 288–293. Reilly JP. "Magnetic field excitation of peripheral nerves and the heart: a comparison of thresholds." Med Biol Eng Comput. 1991; 29(6): 571–579. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 470 Stikova E Robitaille P. M, Warner R. et al. "Design and assembly of an 8 tesla wholebody MR scanner." J Comput Assist Tomogr. 1999; 23(6): 808–820. Rosen AD. "Mechanism of action of moderate-intensity static magnetic fields on biological systems." Cell Biochem Biophys. 2003; 39(2): 163–173. Rosenkranz AR, Grobner T. et al. "Conventional or Gadolinium containing contrast media: the choice between acute renal failure or Nephrogenic Systemic Fibrosis?" Wien Klin Wochenschr. 2007; 119(9–10): 271–275. Roth RTC. "MR Safety". OutSorce, Inc . Available at: http://www.e-radiography.net/mrict/MR_Safety.pdf. Accessed on: March 30, 2012, (1996). Sawyer-Glover AM. and Shellock FG.. "Pre-MRI procedure screening: recommendations and safety considerations for biomedical implants and devices." J Magn Reson Imaging. 2000; 12(1): 92–106. Schaefer DJ, Bourland JD. et al. "Review of patient safety in time-varying gradient fields." J Magn Reson Imaging. 2000; 12(1): 20–29. Schenck JF, Dumoulin CL. et al. "Human exposure to 4.0-Tesla magnetic fields in a whole-body scanner." Med Phys. 1992; 19(4): 1089–1098. Schwenzer NF, Bantleon R. et al. "In vitro evaluation of magnetic resonance imaging at 3.0 tesla on clonogenic ability, proliferation, and cell cycle in human embryonic lung fibroblasts". Invest Radiol. 2007; 42(4): 212–217. Schwenzer NF, Bantleon R. et al. "Detection of DNA double-strand breaks using gammaH2AX after MRI exposure at 3 Tesla: an in vitro study." J Magn Reson Imaging. 2007; 26(5): 1308–1314. Shellock FG. "Radiofrequency energy-induced heating during MR procedures: a review". J Magn Reson Imaging. 2000; 12(1): 30–36. Shellock FG. "Magnetic resonance safety update 2002: implants and devices". J Magn Reson Imaging. 2002; 16(5): 485–496. Shellock FG. "Radiofrequency energy induced heating of bovine capsular tissue: in vitro assessment of newly developed, temperature-controlled monopolar and bipolar radiofrequency electrodes". Knee Surg Sports Traumatol Arthrosc. 2002; 10(4): 254–259. Shellock FG. and Crues JV. "Temperature, heart rate, and blood pressure changes associated with clinical MR imaging at 1.5 T." Radiology. 1987; 163(1): 259– 262. Shellock FG. and Crues JV. "Thermoregulatory consequences of NMR imaging." Magn Reson Imaging. 1987; 5(6): 505,507. Shellock FG. and Crues JV. "MR procedures: biologic effects, safety, and patient care". Radiology. 2004; 232(3): 635–652. Shellock FG. and Kanal E. "Policies, guidelines, and recommendations for MR imaging safety and patient management. SMRI Safety Committee." J Magn Reson Imaging. 1991; 1(1): 97–101. Shellock FG, Kanal E. et al. "Regarding the value reported for the term "spatial gradient magnetic field" and how this information is applied to labeling of medical implants and devices." AJR Am J Roentgenol 196(1): 142–145. Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472 Magnetic resonance imaging safety: principles and guidelines 471 Shellock, FG, Parker JR. et al. (2006). "Safety of gadobenate dimeglumine (MultiHance): Summary of findings from clinical studies and postmarketing surveillance." Invest Radiol. 2011; 41(6): 500–509. Shellock FG. and Shellock VJ. "Metallic stents: evaluation of MR imaging safety." AJR Am J Roentgenol. 1999; 173(3): 543–547. Shellock FG. and Spinazzi A. "MRI safety update 2008: part 2, screening patients for MRI." AJR Am J Roentgenol. 2008; 191(4): 1140–1149. Shellock FG, Woods TO. et al. "MR labeling information for implants and devices: explanation of terminology." Radiology. 2009; 253(1): 26–30. Shellock FG, Ziarati M. et al. "Determination of gradient magnetic fieldinduced acoustic noise associated with the use of echo planar and three-dimensional, fast spin echo techniques." J Magn Reson Imaging. 1998; 8(5): 1154–1157. Shinbane JS, Colletti PM. et al. "MR in patients with pacemakers and ICDs: Defining the issues." J Cardiovasc Magn Reson. 2007; 9(1): 5–13. Shinbane JS, Colletti PM. et al. "Magnetic resonance imaging in patients with cardiac pacemakers: era of "MR Conditional" designs." J Cardiovasc Magn Reson. 2011; 13: 63. Simi S, Ballardin M. et al. "Is the genotoxic effect of magnetic resonance negligible? Low persistence of micronucleus frequency in lymphocytes of individuals after cardiac scan." Mutat Res. 2008; 645(1–2): 39–43. So PP, Stuchly MA. et al. "Peripheral nerve stimulation by gradient switching fields in magnetic resonance imaging." IEEE Trans Biomed Eng. 2004; 51(11): 1907– 1914. Spouse E. and Gedroyc WM. "MRI of the claustrophobic patient: interventionally configured magnets." Br J Radiol. 2000; 73(866): 146–151. Stuart C, Trakic A. et al. "Numerical study of currents in workers induced by body-motion around high-ultrahigh field MRI magnets." J Magn Reson Imaging. 2007; 26(5): 1261–1277. Teitelbaum GP, Bradley Jr. WG, et al. "MR imaging artifacts, ferromagnetism, and magnetic torque of intravascular filters, stents, and coils." Radiology. 1988; 166(3): 657–664. Teitelbaum GP, Yee CA. et al. "Metallic ballistic fragments: MR imaging safety and artifacts." Radiology. 1990; 175(3): 855–859. Prilozi, Odd. biol. med. nauki, XXXIII/1 (2012), 441–472 472 Stikova E Резиме БЕЗБЕДНОСТ ПРИ ИМИЏИНГ СО МАГНЕТНА РЕЗОНАНСА: ПРИНЦИПИ И ПРЕПОРАКИ Stikova E Медицински факулtеt, Инсtиtуt за јавно здравје, Универзиtеt Св. Кирил и Меtодиј, Скоpје, Р. Македонија А п с т р а к т: Овој труд е преглед на постоечката литература за безбедност при имиџинг со магнетна резонанса (ИМР). Трудот ги систематизира основните информации за електромагнетните полиња што се создаваат при дијагностичката процедура, а потоа дава опис на биолошките ефекти на овие полиња врз човекот. Прегледот завршува со дискусија за безбедноста при употребата на ИМР во клиничка практика, со посебен акцент на безбедносните процедури и стандарди. Клучни зборови: имиџинг со магнетна резонанса, биолошки ефекти на електромагнетно зрачење, ИМР стандарди, безбедносна процедура. Corresponding Author: Prof. Elisaveta Stikova MD, PhD University "Ss. Cyril and Methodius" Faculty of Medicine National Public Health Institute Skopje, R. Macedonia E-mail: elisaveta.stikova@fulbrightmail.org Contributions, Sec. Biol. Med. Sci., XXXIII/1 (2012), 441–472