0013-7227/03/$15.00/0
Printed in U.S.A.
The Journal of Clinical Endocrinology & Metabolism 88(2):787–792
Copyright © 2003 by The Endocrine Society
doi: 10.1210/jc.2002-020889
The Role of Müllerian Inhibiting Substance in the
Evaluation of Phenotypic Female Patients with Mild
Degrees of Virilization
MADHUSMITA MISRA, DAVID T. MACLAUGHLIN, PATRICIA K. DONAHOE,
AND
MARY M. LEE
Pediatric Endocrine Unit (M.M.) and Pediatric Surgical Research Laboratory (D.T.M., P.K.D.), MassGeneral Hospital for
Children and Harvard Medical School, Boston, Massachusetts 02114; and Pediatric Endocrine Division (M.M.L.), Duke
University Medical Center, Durham, North Carolina 27710
Müllerian inhibiting substance (MIS) is a sexually dimorphic
gonadal hormone with proven efficacy in the evaluation of
boys with cryptorchidism and children with intersex conditions. We examined the role of MIS determination in the evaluation of 65 phenotypic females with mild virilization. Among
the 28 subjects with MIS values elevated above the normal
female range, all had abnormal gonadal tissue: ovotestes in 11,
testes in 7, dysgenetic gonads in 7, and MIS-secreting ovarian
tumors in 3. Among the 37 children with serum MIS in the
normal female range, 19 had detectable MIS and 18 had unmeasurable MIS. In the former group with measurable but
normal female MIS values, 16 subjects had ovaries, 1 had an
ovotestis, and 1 had dysgenetic gonads containing testicular
elements. Of 18 children with undetectable MIS values, 16 had
ovaries and 2 had ovarian dysgenesis. In this study, elevation
of serum MIS above the normal female range was consistently
associated with the presence of testicular tissue or MISsecreting tumors, mandating additional evaluation and surgical exploration. A value within the normal female range in
a virilized patient did not exclude dysgenetic testicular tissue
or ovotestis, whereas undetectable values were consistent
with the absence of testicular tissue. (J Clin Endocrinol Metab
88: 787–792, 2003)
M
ÜLLERIAN INHIBITING SUBSTANCE (MIS) also
known as anti-Müllerian hormone (AMH) (1) promotes involution of the Müllerian ducts during male sexual
differentiation and also exerts paracrine actions on postnatal
ovarian and testicular development (2–7). MIS is a member
of the TGF- family of peptide hormones that regulates cellular growth and differentiation (1, 8 –11). The expression of
MIS is sexually dimorphic in Sertoli cells of the testis and
granulosa cells of the ovary. Consequently, mean serum MIS
values are much higher in males than females, particularly
in prepubertal children. In girls, the expression of MIS is low
or undetectable at birth, then increases slightly, but remains
distinctly lower than the male range until 8 –10 yr of age (12,
13). At puberty, MIS values in females and males start to
overlap (12, 13). Serum MIS in women varies across the
menstrual cycle within a narrow range (mean values of 1.4 –
1.7 ng/ml) (14). In boys, serum MIS rises rapidly after birth,
peaks in late infancy, then decreases by puberty to low adult
values (12, 15–19). The abundant expression of MIS in the
prepubertal testis has proven useful for the evaluation of
boys with cryptorchidism and children with intersex conditions (19 –24). In boys with cryptorchidism, a measurable
serum MIS is highly predictive of testicular tissue, whereas
an undetectable value is consistent with anorchia (21–24). In
children with intersex conditions, MIS not only distinguishes
between testes and ovaries but also helps define the extent
of testicular parenchymal tissue (19 –23). Because serum MIS
in prepubertal girls is near the detection limit of the MIS
assays, its utility for the evaluation of gonadal disorders in
phenotypic females has not been systematically explored.
Although the role of MIS in the regression of Müllerian
ducts during male sexual differentiation is well understood,
its role in females is less clear. MIS induces follicular growth
and differentiation (4, 5, 7) and inhibits recruitment of primordial follicles (25) in animal studies. In women, MIS is
measurable in ovarian follicular fluid (26) and its concentration in serum fluctuates across the menstrual cycle, peaking in the late follicular phase (13, 14). Women with polycystic ovarian syndrome have higher serum MIS values,
which correlate inversely with serum estradiol, indicating
that MIS may play a role in regulating estradiol synthesis as
well as in the disordered folliculogenesis of polycystic ovarian syndrome (26).
Because MIS is a hormone restricted in expression to the
gonads and expressed at much higher levels in testicular than
ovarian tissue, we reasoned that MIS determination would
help differentiate between gonadal and nongonadal causes
of mild virilization. MIS values would be low in female
infants with a 46,XX karyotype and normal ovarian tissue
who are virilized from in utero exposure to maternal androgens or elevated adrenal androgens as with congenital adrenal hyperplasia (CAH). On the other hand, serum MIS
would be elevated above the normal female range if the
virilization is caused by testicular androgens in a child with
a 46,XY karyotype and male pseudohermaphroditism. With
acquired virilization, MIS determination might help distinguish between gonadal androgens and those from other
sources. For example, androgen-secreting ovarian tumors
such as Sertoli-Leydig cell tumors and selected virilizing
granulosa-theca cell tumors (27, 28) might express high levels
Abbreviations: AMH, Anti-Müllerian hormone; CAH, congenital adrenal hyperplasia; MIS, Müllerian inhibiting substance.
787
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.
788
J Clin Endocrinol Metab, February 2003, 88(2):787–792
Misra et al. • MIS in Mildly Virilized Phenotypic Females
of MIS (29, 30). Therefore, we examined serum MIS concentrations in relation to gonadal histology and cytogenetic findings in phenotypic girls with mild virilization (nonpalpable
gonads, clitoromegaly, and partial labial fusion).
Patients and Methods
Patient selection
We identified 65 phenotypic females who presented with virilization
between 1 d and 17 yr of age and had MIS measurements from December
1995 to April 2000. These patients were evaluated initially in the Pediatric Endocrine Unit or the Pediatric Surgical Unit of the MassGeneral
Hospital for Children (n ⫽ 20), or at other institutions (n ⫽ 45). At
Massachusetts General Hospital, the parents gave verbal consent for MIS
determination, in accordance with approved institutional guidelines.
However, because MIS determination is available as a standard diagnostic test, this was not uniformly obtained at other institutions. All
patients underwent surgical exploration, gonadal biopsy, or diagnostic
imaging. Clinical findings, cytogenetic analysis, operative details, and
pathologic details of the gonadal biopsies were obtained from chart
review and communications with the patients’ physicians.
Serum MIS assay
Serum MIS was measured by an ELISA as described in earlier studies
(12, 16, 22). This assay does not cross-react with other members of this
gene family, and is specific for primate MIS. The intraassay coefficient
of variation for the assay is 9%, and the interassay coefficient of variation
is 15%. The limit of sensitivity is 0.3 ng/ml. MIS values that fell below
this (⬍0.3 ng/ml) were considered undetectable. Values of MIS that fell
within the range for age-matched females were designated as normal,
and MIS values above the female range were designated as elevated. We
previously reported mean serum MIS values of 0.7 ng/ml (range, 0.2–1.9
ng/ml) in female infants, ages 2–12 months (12). By 18 months, MIS rises
minimally to prepubertal values of 0.9 ng/ml (range, 0.2–3.9 ng/ml),
then increases further to pubertal and adult values of 2.9 ng/ml (range,
0.2– 8.9 ng/ml) (12). All MIS measurements were made on specimens
that were freshly collected or stored for less than 2 yr.
Statistical analysis
The Student’s t test was used to compare means between groups.
Sensitivity, specificity, and positive and negative predictive values with
95% confidence intervals were calculated using two-way contingency
table analysis of Javastat, based on methods described by Fleiss (31), and
the program Matlab (binofit.m) produced by The Mathworks Inc. (Newton, MA), which uses methods described by Johnson et al. (32).
Results
Patient characteristics
The subjects included 65 phenotypic females with mild
degrees of virilization (Prader stages 1 and 2). All subjects
were considered to have clitoromegaly by the examining
physician. Some also had posterior labial fusion. The diagnoses, gonadal histology, karyotype, and MIS values are
elaborated in Table 1. Mean age was 2.4 ⫾ 0.5 yr (range of
1 d to 17 yr), and most were prepubertal (61/65).
Of the 65 subjects studied, 28 had elevated MIS values with
a mean ⫾ sem of 18.9 ⫾ 5.1 ng/ml and individual values of
5.0 to 92.5 ng/ml (Table 2). Thirty-seven subjects had MIS in
the female range with a mean ⫾ sem of 0.6 ⫾ 0.1 ng/ml and
individual values ranging from undetectable to 3.3 ng/ml. Of
the latter group, MIS was measurable in 19 and undetectable
in 18 subjects. Cytogenetic analysis was available in all but
two patients, and all subjects underwent surgical exploration, gonadal biopsy, and/or imaging studies. Gonads were
not biopsied in thirteen 46,XX girls diagnosed with CAH and
in twenty 46,XX Prader 1 girls with low or undetectable
testosterone and normal imaging.
MIS and gonadal histology
All subjects with ovarian tissue had individual MIS values
that fell within the normal female range. The lowest mean
MIS value was found in this gonadal category (Fig. 1). The
highest MIS values were found in 46,XX females with MISsecreting ovarian tumors, followed by patients with bilateral
testes. The individual MIS values in both of these categories
were clearly above the female range but within the normal
male range (Fig. 2). Subjects with bilateral or unilateral testes
(n ⫽ 7) had higher MIS values than those with dysgenetic
gonads or ovotestes (n ⫽ 22) (23.6 ⫾ 11.1 ng/ml vs. 7.3 ⫾ 1.6
ng/ml, P ⬍ 0.05, Fig. 1). In this latter group with abnormal
gonads, a number of individual MIS values fell within the
normal female range, although the mean value was significantly higher than that of girls with ovaries (7.3 ⫾ 1.6 ng/ml
vs. 0.7 ⫾ 0.1 ng/ml, P ⬍ 0.0001). Among those with an
TABLE 1. Gonadal status, mean MIS, and karyotype of study population (n ⫽ 65)
Group
Diagnosis
n
1
13
Ovaries
2
3
Congenital adrenal
hyperplasia
Idiopathic virilization
True hermaphrodite
20
14
Ovaries
Bilateral ovotestes (6)
Ovotestis and ovary (6)
Testis and ovary (2)
4
Gonadal dysgenesis
10
Dysgenetic
5
Partial androgen
insensitivity
Virilizing ovarian
tumor
6
a
b
c
Gonadal status (n)
MIS (ng/ml)
0.8 ⫾ 0.3
0.6 ⫾ 0.1
10.5 ⫾ 2.8a,b,c
Karyotype
All 46,XX
5
Bilateral testes
25.3 ⫾ 15.1a,b
All 46,XX
10-46,XX
1-46,XX/46,XY
1-45,X/46,XY
1-46,XY
1-unknown
4-45,X/46,XY
2-45,X/46,XX
3-46,XY
1-unknown
All 46,XY
3
Sertoli-Leydig cell tumor
69.0 ⫾ 25.2a,b
All 46,XX
5.2 ⫾ 1.8a,b,c
Significantly greater than group 1. Groups 3, 4, and 5, P ⱕ 0.01; group 6, P ⱕ 0.0001.
Significantly greater than group 2. Groups 3 and 4, P ⱕ 0.001; group 5, P ⱕ 0.01; group 6, P ⱕ 0.0001.
Significantly lower than group 6. Groups 3 and 4, P ⱕ 0.001.
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.
Misra et al. • MIS in Mildly Virilized Phenotypic Females
J Clin Endocrinol Metab, February 2003, 88(2):787–792 789
TABLE 2. Gonadal status and karyotype according to elevated or normal MIS values
MIS
Karyotype
Gonadal status
46,XX
46,XY
2 (U/L)
7
5 (B/L)
1
Mosaic
Unknown
2 (45,X/46,XY)
(46,XX/46,XY)
1
3 (45,X/46,XY)
1
Elevated (n ⫽ 28)
Testis
Ovotestis
Normal (n ⫽ 37)
Detectable (n ⫽ 19)
Undetectable (n ⫽ 18)
Dysgenetic gonad
Testicular elements ⫹
Testicular elements ⫺
MIS-secreting ovarian tumor
Ovotestis
Dysgenetic gonad
Testicular elements
Testicular elements
Ovaries
Dysgenetic gonad
Testicular elements
Testicular elements
Ovaries
3
3
1
⫹
⫺
1 (45,X/46,XY)
17
⫹
⫺
2 (45,X/46,XX)
16
U/L Unilateral; B/L bilateral.
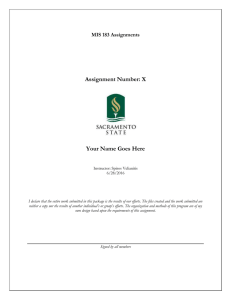
FIG. 1. Mean serum MIS concentrations in 65 mildly virilized phenotypic females according to gonadal status. The groups of subjects
with testes, ovotestes, dysgenetic gonads, or MIS-secreting ovarian
tumors all had significantly higher MIS values than the group of girls
with ovaries (*, P ⬍ 0.0001).
ovotestis, the presence or absence of Y chromosomal material
did not alter the mean MIS value (7.5 ⫾ 1.4 ng/ml vs. 8.1 ⫾
3.2 ng/ml).
MIS and karyotype
All 28 subjects with elevated serum MIS had gonads containing testicular tissue or MIS-secreting ovarian tumors (Table 2). Five of the seven subjects with testes were subsequently diagnosed with partial androgen insensitivity. The
other two had 46,XX true hermaphroditism with unilateral
testes. Eleven subjects had ovotestes, defined by the presence
of both ovarian follicles and seminiferous tubules containing
germ cells. Seven of these children had a 46,XX karyotype.
The karyotype was unknown in one. The other three had the
following karyotypes: 46,XY, 46,XX/46,XY, and 45,X/46,XY.
The presence of ovarian follicles was unexpected in the patient with a 45,X/46,XY karyotype, raising the possibility of
a gonadal 46,XX cell line. Seven subjects had dysgenetic
testes, defined by the presence of dense fibrosis between
tubules and absence of germ cells. Of these, the karyotype
was 46,XY in three, 45,X/46,XY in three, and unknown in
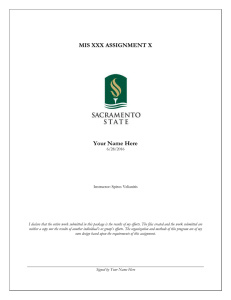
FIG. 2. Individual MIS values by gonadal status in relation to normal
female MIS values for age. Normal MIS values in girls (broken black
lines) and boys (solid black lines) with the mean and lower and upper
limits depicted. Individual serum MIS concentrations of girls are
plotted according to gonadal status. Subjects with testes, ovotestes, or
MIS-secreting ovarian tumors had values above the female range,
whereas those with dysgenetic testes (open triangles) had MIS values
that ranged from the low normal female to above the normal range.
All subjects with ovaries had values within the normal female range
for age.
one. All three subjects with virilizing ovarian tumors had
46,XX karyotypes.
Among the 37 virilized subjects with MIS values in the
normal female range, 19 had measurable values, whereas 18
had undetectable serum MIS (Table 2). Among those with
measurable MIS values, one 8 yr old with a 46,XX karyotype
and an MIS value of 0.7 ng/ml had an ovotestis, and a 7
month old with a 45,X/46,XY karyotype and low MIS of 0.3
ng/ml had dysgenetic testicular tissue. The rest had presumably normal ovaries. None of the subjects in the group
with undetectable MIS values had testicular tissue or dysgenetic gonads with testicular elements. Sixteen had ovaries,
whereas two patients aged 2.5 and 4 yr with 45,X/46,XX
karyotypes and clitoromegaly had ovarian dysgenesis without any testicular elements identified.
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.
790
J Clin Endocrinol Metab, February 2003, 88(2):787–792
Misra et al. • MIS in Mildly Virilized Phenotypic Females
All 33 subjects with presumptive ovarian tissue (no testicular elements or dysgenetic gonads detected by imaging
studies) had 46,XX karyotypes. Thirteen of these subjects
were confirmed to have 46,XX CAH, whereas the remaining
20 girls had mild idiopathic virilization of unidentified etiology and low neonatal testosterone values. Further work-up
was advised in these 20 girls, all of whom were classified as
Prader 1 with clitoromegaly ⫾ minimal posterior labial
fusion.
Comparison of MIS and karyotype determination
Testicular tissue was found in all subjects in this series with
Y chromosomal material (nine with a 46,XY karyotype and
six with sex chromosome mosaicism). As anticipated from
previous clinical observations, the presence of an Y chromosome was associated with the presence of testicular tissue (33,
34). The absence of Y chromosomal material in the peripheral
karyotype, however, was not predictive of absent testicular
tissue. In this series, 10 subjects with a 46,XX karyotype had
testes or ovotestes. Therefore, MIS determination was compared with cytogenetic analysis for discerning the presence
of testicular tissue (Table 3). This analysis indicated that an
elevated MIS value and Y chromosomal material were both
highly specific and predictive for testicular tissue (Table 3).
However, the absence of Y chromosomal material was less
sensitive and predictive for the absence of testicular tissue
than MIS determination (negative predictive value of 72.9%
vs. 94.6% (Table 3).
Discussion
We have shown that MIS determination distinguishes gonadal from nongonadal causes of mild virilization in phenotypic females. If Y chromosomal material is present in a
virilized child, testicular tissue is likely, and MIS would
likewise be elevated. In the absence of Y chromosomal material, an elevated MIS suggests that either testicular tissue or
a virilizing ovarian tumor is present. In this study, all of the
18 subjects with undetectable MIS values had apparently
normal or dysgenetic ovaries: no testicular tissue or gonadal
tumors were identified. In 16 of these 18 cases, the karyotype
was 46,XX. The most frequent diagnosis was CAH with virilization caused by elevated adrenal rather than gonadal
androgens. Conversely, an MIS above the normal female
range in these subjects was uniformly associated with gonadal pathology, either testicular tissue or ovarian tumor.
Across species, the expression of MIS is limited to the
gonads, making it a highly specific marker of gonadal tissue.
During early childhood, MIS expression is much higher in
the testis than the ovary, with no overlap in mean serum
concentrations (12). These characteristics of MIS expression,
i.e. its sexual dimorphism and specificity for gonadal tissue,
have facilitated the use of the MIS assay for evaluating children with diverse gonadal disorders (19 –24, 35). In boys with
cryptorchidism, MIS determination reliably distinguishes
between anorchia and undescended testes (22, 24), with the
rare exception of a patient with the persistent Müllerian duct
syndrome caused by an MIS gene defect (36 –38). In children
with intersex conditions, MIS determination helps ascertain
the presence of testicular tissue and aids differential diagnosis (19, 21, 23, 35). This study extends these findings by
focusing on a subgroup of patients with lesser degrees of
genital ambiguity who were deemed to be phenotypic females with virilization.
The evaluation of virilized girls can be challenging, particularly in the prepubertal years when gonadotropins and
sex steroids are nondiagnostic (39, 40). Cytogenetic analysis,
although not indicative of a specific condition, can help direct
further evaluation. If Y chromosomal material is detected,
quantitative assessment of MIS secretion may help distinguish between conditions primarily affecting androgen synthesis or action (such as androgen insensitivity) from those
due to abnormal formation and structure of the gonad such
as a dysgenetic testes or anorchia (19, 21, 23). A normal or
high normal MIS value is consistent with a structurally normal testis, whereas a low value may indicate an abnormality
of testicular formation. One caveat must be kept in mind,
however. In children with dysgenetic testes, serum MIS can
fall either within the normal female range or above the female
norms to the low normal male range (19, 22). Therefore, an
MIS value within the normal female range in a virilized
female does not exclude dysgenetic testicular tissue or
ovotestis and cannot be used as confirmation of normal ovaries. In this situation, more extensive evaluation including
assessment of basal or stimulated testosterone levels or imaging studies may help establish the diagnosis.
In virilized girls, it is not uncommon to find a 46,XX karyotype or a mosaic karyotype without Y chromosomal material.
Only 15 of our subjects had Y material detected, whereas 48
had a 46,XX karyotype and 2 had mosaicism (45,X/46,XX).
In this study, 13 of the 48 virilized patients with a 46,XX
TABLE 3. Test parameters for MIS determination vs. cytogenetic analysis (n ⫽ 63)a
Testicular tissue
Elevated MIS
Normal MIS
Present
Absent
26
2
0
35
Sensitivity
Specificity
Positive predictive value
Negative predictive value
Karyotype
Y material present
Y material absent
Testicular tissue
Present
Absent
15
13
0
35
MIS
Y material
92.9% (76.5–99.1%)
100.0% (90.0 –100.0%)
100.0% (86.8 –100.0%)
94.6% (81.8 –99.3%)
53.6% (33.9 –72.5%)
100.0% (90.0 –100.0%)
100.0% (78.2–100.0%)
72.9% (58.2– 84.7%)
Numbers in parentheses represent confidence intervals.
Karyotype was unknown in two subjects.
a
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.
Misra et al. • MIS in Mildly Virilized Phenotypic Females
karyotype had a diagnosis of CAH, the predominant cause
of virilization in 46,XX individuals. For this subset of patients, MIS determination would not provide additional useful information. In the remaining subjects, cytogenetic analysis is not discriminatory for gonadal pathology; for
example, a 46,XX karyotype can be associated with normal
ovaries, true hermaphroditism (41) or even 46,XX sex reversal (males with intact testes) (42). In a virilized patient with
no Y sequences detected peripherally, however, MIS determination would help identify testicular tissue or ovarian
tumors. Of the 12 patients with a 46,XX karyotype and elevated MIS in this study, 9 had either testes or ovotestes (all
with diagnoses of true hermaphroditism) and 3 had ovarian
tumors. In these subjects, the cytogenetic analysis was nondiagnostic, whereas MIS determination reliably predicted
testicular tissue or a virilizing tumor.
Our data demonstrate that MIS has a high sensitivity,
specificity, and positive and negative predictive values for
detecting testicular tissue or an MIS-secreting virilizing ovarian tumor in phenotypic females with virilization. MIS determination is especially valuable during late infancy and the
prepubertal years when gonadotropins and testosterone are
nondiagnostic (42, 43). MIS values that are elevated to the
male range are consistent with the presence of testicular
tissue or MIS secreting tumors, mandating additional evaluation and surgical exploration to verify the gonadal histology and resect testicular or tumor tissue. MIS can then be
measured postoperatively to document complete removal of
testicular tissue or tumor. Our study confirms the value of
MIS determination in conjunction with cytogenetic, steroid,
and radiologic studies in the evaluation of phenotypic females with virilization.
J Clin Endocrinol Metab, February 2003, 88(2):787–792 791
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Acknowledgments
We thank Dr. Hang Lee of the Biostatistics Unit of Massachusetts
General Hospital for his help with the statistical section of this paper.
Received June 7, 2002. Accepted November 12, 2002.
Address all correspondence and requests for reprints to: Mary M. Lee,
M.D., Pediatric Endocrine Division, Box 3080, 308 Bell Building, Duke
University Medical Center, Durham, North Carolina 27710. E-mail:
Lee00140@mc.duke.edu.
This work was supported in part by National Institute of Child Health
and Human Development (NICHD) Grants HD-10367 and HD-36768 (to
M.M.L.), NIH Nutrition Training Grant DK-07703 (to M.M.), National
Cancer Institute Grant CA-17393 (to P.K.D. and D.T.M.), and NICHD
Grant HD-31223 (to P.K.D.).
20.
21.
22.
23.
24.
25.
References
1. Josso N, Cate RL, Picard JY, Vigier B, di Clemente N, Wilson C, Imbeaud S,
Pepinsky RB, Guerrier D, Boussin L 1993 Anti-mullerian hormone: the Jost
factor. Recent Prog Horm Res 48:1–59
2. Racine C, Rey R, Forest MG, Louis F, Ferre A, Huhtaniemi I, Josso N, di
Clemente N 1998 Receptors for anti-Mullerian hormone on Leydig cells are
responsible for its effects on steroidogenesis and cell differentiation. Proc Natl
Acad Sci USA 95:594 –599
3. Lee MM, Seah CC, Masiakos PT, Sottas CM, Preffer FI, Donahoe PK,
MacLaughlin DT, Hardy MP 1999 Mullerian inhibiting substance type II
receptor expression and function in purified rat Leydig cells. Endocrinology
140:2819 –2827
4. McGee EA, Smith R, Spears N, Nachtigal MW, Ingraham H, Hsueh AJ 2001
Mullerian inhibitory substance induces growth of rat preantral ovarian follicles. Biol Reprod 64:293–298
5. Durlinger AL, Gruijters MJ, Kramer P, Karels B, Kumar TR, Matzuk MM,
Rose UM, de Jong FH, Uilenbroek JT, Grootegoed JA, Themmen AP 2001
26.
27.
28.
29.
30.
Anti-Mullerian hormone attenuates the effects of FSH on follicle development
in the mouse ovary. Endocrinology 142:4891– 4899
Sriraman V, Niu E, Matias JR, Donahoe PK, MacLaughlin DT, Hardy MP,
Lee MM 2001 Mullerian inhibiting substance inhibits testosterone synthesis in
adult rats. J Androl 22:750 –758
Ikeda Y, Nagai A, Ikeda MA, Hayashi S 2002 Increased expression of
Mullerian inhibiting substance correlates with inhibition of follicular growth
in the developing ovary of rats treated with E2 benzoate. Endocrinology
143:304 –312
Lee MM, Donahoe PK 1993 Mullerian inhibiting substance: a gonadal hormone with multiple functions. Endocr Rev 14:152–164
Lane AH, Donahoe PK 1998 New insights into Mullerian inhibiting substance
and its mechanism of action. J Endocrinol 158:1– 6
Teixeira JT, Maheswaran S and Donahoe PK 2001 Mullerian inhibiting substance: an instructive developmental hormone with diagnostic and possible
therapeutic applications. Endocr Rev 22:657– 674
Josso N, di Clemente N, Gouedard L 2001 Anti-Mullerian hormone and its
receptors. Mol Cell Endocrinol 179:25–32
Lee MM, Donahoe PK, Hasegawa T, Silverman B, Crist GB, Best S, Hasegawa Y, Noto RA, Schoenfeld D, MacLaughlin DT 1996 Mullerian inhibiting
substance in humans: normal levels from infancy to adulthood. J Clin Endocrinol Metab 81:571–576
Long WQ, Ranchin V, Pautier P, Belville C, Denizot P, Cailla H, Lhomme
C, Picard JY, Bidart JM, Rey R 2000 Detection of minimal levels of serum
anti-Mullerian hormone during follow-up of patients with ovarian granulosa
cell tumor by means of a highly sensitive enzyme-linked immunosorbent
assay. J Clin Endocrinol Metab 85:540 –544
Cook CL, Siow Y, Taylor S, Fallat ME 2000 Serum Mullerian inhibiting
substance levels during normal menstrual cycles. Fertil Steril 73:859 – 861
Josso N, Legeai L, Forest MG, Chaussain JL, Brauner R 1990 An enzyme
linked immunoassay for anti-Mullerian hormone: a new tool for the evaluation
of testicular function in infants and children. J Clin Endocrinol Metab 70:23–27
Hudson PL, Dougas I, Donahoe PK, Cate RL, Epstein J, Pepinsky RB,
MacLaughlin DT 1990 An immunoassay to detect human Mullerian inhibiting
substance in males and females during normal development. J Clin Endocrinol
Metab 70:16 –22
Baker ML, Metcalfe SA, Hutson JM 1990 Serum levels of Mullerian inhibiting
substance in boys from birth to 18 years, as determined by enzyme immunoassay. J Clin Endocrinol Metab 70:11–15
Schwindt B, Doyle LW, Hutson JM 1997 Serum levels of Mullerian inhibiting
substance in preterm and term male neonates. J Urol 158:610 – 612
Rey RA, Belville C, Nihoul-Fekete C, Michel-Calemard L, Forest MG, Lahlou
N, Jaubert F, Mowszowicz I, David M, Saka N, Bouvattier C, Bertrand AM,
Lecointre C, Soskin S, Cabrol S, Crosnier H, Leger J, Lortat-Jacob S, Nicolino
M, Rabl W, Toledo SP, Bas F, Gompel A, Czernichow P, Josso N 1999
Evaluation of gonadal function in 107 intersex patients by means of serum
anti-mullerian hormone measurement. J Clin Endocrinol Metab 84:627– 631
Josso N, Boussin L, Knebelmann B, Nihoul-Fekete C, Picard JY 1991 AntiMullerian hormone and intersex states. Trends Endocrinol Metab 2:227–233
Josso N 1995 Paediatric applications of anti-Mullerian hormone research. 1992
Andrea Prader Lecture. Horm Res 43:243–248
Lee MM, Donahoe PK, Silverman BL, Hasegawa T, Hasegawa Y, Gustafson
ML, Chang YC, MacLaughlin DT 1997 Measurement of serum Mullerian
inhibiting substance in the evaluation of children with nonpalpable gonads.
N Engl J Med 336:1480 –1486
Lane AH, Lee MM 2001 Mullerian inhibiting substance: a sensitive marker of
gonadal function. Curr Opin Endocrinol Diabetes 8:296 –300
Misra M, McLaughlin D, Donahoe P, Lee MM 2002 Measurement of MIS
facilitates management of boys with microphallus and cryptorchidism. J Clin
Endocrinol Metab 87:3598 –3602
Durlinger ALL, Kramer P, Karles B, deJong FH, Uilenbroek JTJ, Grootegoed
JA, Themmen AP 1999 Control of primordial follicle recruitment by antimullerian hormone in the mouse ovary. Endocrinology 140:5789 –5796
Cook CL, Siow Y, Brenner AG, Fallat ME 2002 Relationship between serum
Mullerian inhibiting substance and other reproductive hormones in untreated
women with polycystic ovary syndrome and normal women. Fertil Steril
77:141–146
Sayegh RA, DeLellis R, Alroy J, Lechan R, Ball HG 1999 Masculinizing
granulosa cell tumor of the ovary in a postmenopausal woman. A case report.
J Reprod Med 44:821– 825
Betta P, Bellingeri D 1985 Androgenic juvenile granulosa cell tumour. Case
Report. Eur J Gynaecol Oncol 6:71–74
Lane AH, Lee MM, Fuller Jr AF, Kehas DJ, Donahoe PK, MacLaughlin DT
1999 Diagnostic utility of Mullerian inhibiting substance determination in
patients with primary and recurrent granulosa cell tumors. Gynecol Oncol
73:51–55
Rey R, Sabourin JC, Venara M, Long WQ, Jaubert F, Zeller WP, Duvillard
P, Chemes H, Bidart JM 2000 Anti-Mullerian hormone is a specific marker of
Sertoli- and granulosa-cell origin in gonadal tumors. Hum Pathol 31:1202–1208
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.
792
J Clin Endocrinol Metab, February 2003, 88(2):787–792
31. Fleiss JL 1981 Statistical methods for rates and proportions. 2nd ed. New York:
John Wiley and Sons; 4 – 8
32. Johnson NL, Kotz S, Kemp AW 1992 Univariate discrete distributions. 2nd ed.
New York: John Wiley and Sons; 124 –130
33. Donahoe PK, Crawford JD, Hendren WH 1978 True hermaphroditism: a
clinical description and a proposed function for the long arm of the Y chromosome. J Pediatr Surg 13:293–301
34. Rutgers JL, Scully RE 1987 Pathology of the testis in intersex syndromes.
Semin Diagn Pathol 4:275–291
35. Gustafson ML, Lee MM, Asmundson L, MacLaughlin DT, Donahoe PK 1993
Mullerian inhibiting substance in the diagnosis and management of intersex
and gonadal abnormalities. J Pediatr Surg 28:439 – 444
36. Guerrier D, Tran D, Vanderwinden JM, Hideux S, Van Outryve L, Legeai
L, Bouchard M, Van Vliet G, De Laet MH, Picard JY 1989 The persistent
Mullerian duct syndrome: a molecular approach. J Clin Endocrinol Metab
68:46 –52
37. Imbeaud S, Carre-Eusebe D, Rey R, Belville C, Josso N, Picard JY 1994
Misra et al. • MIS in Mildly Virilized Phenotypic Females
38.
39.
40.
41.
42.
Molecular genetics of the persistent Mullerian duct syndrome: a study of 19
families. Hum Mol Genet 3:125–131
Belville C, Josso N, Picard JY 1999 Persistence of Mullerian derivatives in
males. Am J Med Genet 89:218 –223
Lustig RH, Conte FA, Kogan BA, Grumbach MM 1987 The ontogeny of
gonadotropin secretion in congenital anorchism: sexual dimorphism versus
syndrome of gonadal dysgenesis and diagnostic considerations. J Urol 138:
587–591
Lee PA 2000 Appropriate use and interpretation of human chorionic
gonadotropin stimulation in prepubertal male patients. Endocr Prac 6:112–
114
Krob G, Braun A, Kuhnle U 1994 True hermaphroditism: geographical distribution, clinical findings, chromosomes and gonadal histology. Eur J Pediatr
153:2–10
Kadandale JS, Wachtel SS, Tunca Y, Wilroy Jr RS, Martens PR, Tharapel AT
2000 localization of SRY by primed in situ labeling in XX and XY sex reversal.
Am J Med Genet 95:71–74
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 02 October 2016. at 06:51 For personal use only. No other uses without permission. . All rights reserved.