Stroke
JULY-AUGUST
VOL. 10
1979
NO. 4
A Journal ofCerebral Circulation
Effect of STA-MCA Anastomosis
On the Course of Experimental
Acute MCA Embolic Occlusion
ROBERT LEVINTHAL, M.D.,
W. JANN B R O W N , M.D.,
JOHN I. MOSELEY, M.S.,
AND W. EUGENE STERN,
M.D.,
M.D.
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
SUMMARY The experiments in this report were designed to evaluate the effect of superficial temporalmiddle cerebral artery (STA-MCA) anastomosis on the course of middle cerebral artery (MCA) occlusion by
emboli while avoiding a vessel clipping technique as well as the use of long-acting barbiturate anesthesia. Dogs
were divided into 3 general groups: A) embolus placement 1 b following anastomosis; B) embolus placement 5
h prior to anastomosis; C) control group without anastomosis. Anastomosis prior to MCA occlusion has a
favorable clinical effect and reduces the size of an infarction. Anastomosis 5 h after embolus placement is
deleterious unless other therapeutic modalities can be shown to delay the course of infarction.
Stroke Vol 10, No 4, 1979
owing to aberrant emboli or other unforeseen
problems. Anesthesia was induced in all animals with
thiopental (20 mg/kg intravenous push). They were
maintained on methoxyfluorethane inhalation
anesthesia. The femoral artery was exposed and cannulated for continuous blood pressure recording and
random blood gas sampling. Three operative groups
were selected as follows:
Group A — STA-MCAA followed in 1 hr by embolic occlusion of the middle cerebral artery.
Group B — STA-MCAA performed 5 hr after
embolic occlusion of the MCA.
Group C — MCA embolus to the MCA with or
without control craniectomy.
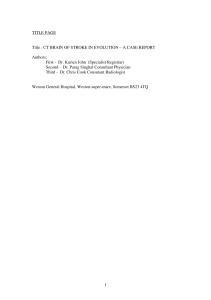
The technique previously described by Molinari13
was utilized for embolization (fig. 1). A silicon rubber
cylinder (1.8 X 8 mm) was inserted into an 18-gauge
medicut cannula and injected into the isolated internal
carotid artery. The cannula was removed and the ICA
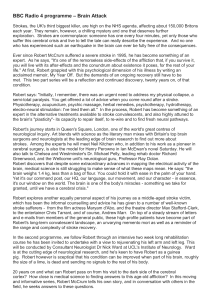
ligated. An extracranial-intracranial anastomosis
(EC-IC) was performed between the STA, which was
1.0-1.4 mm in diameter, and a MCA cortical branch
0.8-1.0 mm in diameter (fig. 2).
On the day following surgery, the animals were
clinically graded and this was continued daily until
sacrifice 2 to 5 days after operation (table 1). Grading
of all animals was done by 2 observers separately.
Immediately prior to death, the dogs received 50
milliliters of 2% Evans blue intravenously. In all
animals who had anastomosis, vessel patency was
evaluated by 2 methods: 1) observation of rapid Evans
blue discoloration of the STA and 2) cutting the STA
and observing blood flow.
The animals were killed by aortic perfusion with
gluteraldehyde or formalin. The brains were im-
SINCE the superficial temporal to middle cerebral
artery anastomosis (STA-MCA) was first described a
decade ago,21-22 the indications for the procedure have
remained controversial. The effect of a superficial
temporal to middle cerebral artery by-pass on the
course of acute occlusion of the middle cerebral artery
is of considerable importance in the prevention and
early therapy of stroke. Revascularization by carotid
endarterectomy in patients with acute stroke has
generally produced poor clinical results.3- "• "•16- lfl- 20
In the limited number of reports on extracranial to
intracranial by-pass following early vessel occlusion,
the outcome has also been discouraging.1-4-8-12-1S
Previous laboratory studies have utilized vessel clipping methods to produce occlusions or have failed to
direct their attention specifically to extracranialintracranial revascularization procedures.2' 6~7-18
This study was designed to evaluate the effect of an
extracranial to intracranial anastomosis on the course
of an acute embolic occlusion of the middle cerebral
artery, while avoiding clipping the vessel as well as
avoiding the use of long-acting barbiturate anesthesia.
Clinical Material and Methods
Thirty-one mongrel dogs underwent operative
procedures, but only 17 were available for this report,
From the Department of Surgery, Division of Neurosurgery,
School of Medicine, UCLA, Los Angeles, CA 90024. Dr. Levinthal
is Assistant Professor of Neurosurgery, Baylor College of
Medicine. Dr. Moseley is Chief Resident Neurosurgery, Dr. Brown
is Professor of Pathology (Neuropathology), and Dr. Stern is
Professor and Chairman, Division of Neurosurgery, University of
California, Los Angeles.
Reprints: Dr. Levinthal, 6410 Fannin, 1531 Houston, TX 77030.
371
3T2
STROKE
VOL
10, No
4, JULY-AUGUST
1979
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
FIGURE 2. Superficial temporal artery (arrow) lying above
cortical branch of middle cerebral artery. Rectangular object below the middle cerebral artery is 1-cm rule.
Clinical Observations
The following results were obtained: arterial blood
gas (ABG), blood pressure (BP) and operative times
did not differ significantly among 3 groups. The
TABLE 1 Clinical Grades
FIGURE 1. A) Silicone rubber cylinder 1.8 X 8 mm with
18-gauge polyethylene cannula. B) Silk sutures around
origin of the internal carotid artery. Cannula containing the
silicone rubber cylinder is placed into internal carotid artery
and injected into intracranial circulation.
mediately removed and placed in the appropriate fixative. Two weeks after perfusion, the brains were examined and photographed. Beginning immediately
anterior to the distribution of the MCA in the brain, 1
cm coronal sections were made. The 1 cm thick slices
were photographed and then the 20th and 220th sections of each slice were stained with H & E and Luxor
blue. The slides were projected afixeddistance with a
photographic enlarger and the hemispheric and infarcted areas were traced from their projected images,
after which the traced images were examined with a
compensating planimeter and the ratios of infarcted
area to the whole hemisphere were computed for each
slice. The amount of infarction present in each cut was
averaged and that figure was accepted as the percent
infarction for that animal.
A Strength
1. stands with no weakness—no dysfunction
2. stands well but with slight weakness—mild
dysfunction
3. marked weakness and/or unable to stand—marked
dysfunction
B
Gait
1. walks with no deficit—no dysfunction
2. mild limp—mild dysfunction
3. marked limp or unable to walk—marked dysfunction
C
Sensation
1. withdraws briskly to pain—no dysfunction
2. slow withdrawal—mild dysfunction
3. no withdrawal—marked dysfunction
D Level of consciousness
1. awake, active—no dysfunction
2. lethargic—mild dysfunction
3. comatose—marked dysfunction
E
Field cut
absent —
marked +
EFFECT OF STA-MCA ANASTOMOSIS ON MCA OCCLUSION/Lev/n/Aa/ et al.
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
MCAflowby clip removal in cats and monkeys within
6 h of clip placement will prevent significant infarction.18 Utilizing a similar technique in monkeys,
Crowell and co-workers could demonstrate moderate
to severe deficits after 6 to 8 h of clipping. Occlusion
for 2 h after clipping produced mild neurologic deficits
or none at all, and 4 h after clip occlusion produced
results that were intermediate between these extremes.8 Although these reports have contributed to
our understanding of the course of ischemic infarction, other variables need to be considered in their interpretation. Recent experimental work suggests a
beneficial effect of barbiturates on the course of infarction10- "•23 and anatomic studies introduce a consideration of the activity of autonomic nerve supply to
the cerebral vessels.9 These variables were examined
more closely.
Except for Dujovnoy, the investigators used a
vessel-clipping technique which might affect the
vascular autonomic supply and which produces only a
"point" occlusion of blood flow in contrast to an embolus in a segment of vessel. All of the animals in the
reported series were anesthetized for the entire experiment with medium- or long-acting barbiturates. Only
in a study by Crowell and Olsson was the effect of
revascularization through an EC-IC bypass evaluated
(performed 2 h subsequent to MCA clipping).
Our experimental design utilizing an embolization
technique and incorporating only short-acting barbiturate induction has shown that anastomosis
between the STA and MCA 5 h after an embolus is
deleterious both clinically and pathologically.
For a revascularization procedure to be beneficial
during an acute ischemic period, it must be performed
before irreversible brain damage takes place. Our experiment indicates that this is earlier than 5 h after
vascular occlusion. Because of the small number of
animals involved, no significant difference could be
demonstrated between the percent of infarction in
control dogs and those that had a STA-MCA performed 1 h prior to embolization. However, clinically
and by gross pathologic examination, there appeared
to be a reproducible and consistent beneficial effect of
anastomosis was patent in all animals in Groups A
and B. All group A & B dogs had emboli lodged in the
proximal MCA.
The Group A animals (STA-MCA prior to embolus
placement), in 4 out of 5 dogs, demonstrated no abnormality of strength, gait, sensation or level of consciousness. But all of these dogs had evidence of a
visualfielddeficit. The one animal which had evidence
of marked dysfunction in all clinical categories had an
intracerebral hemorrhage (the only animal to
demonstrate gross hemorrhage).
The Group B dogs (embolus placement 5 h prior to
anastomosis) fared less well, and had either mild or
marked dysfunction in each clinical neurologic
category tested. Visual field cuts were consistently
demonstrated in all animals.
Group C animals (embolus only in the MCA) fell
into 2 separate clinical groups. Three animals with
emboli resting in the proximal MCA had mild visual
field defects. Two animals with emboli in the
peripheral MCA had no neurologic deficit (table 2).
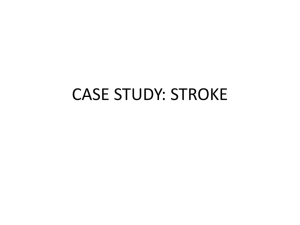
On postmortem examination, 4 of the 5 Group A
dogs had scattered microscopic hemorrhage; the one
with intracerebral hematoma was the exception. The
percentage of infarction was 33.3. In Group B animals
all had gross evidence of hemorrhage and 77.2% had
cerebral infarction, and the Group C dogs had slight
hemorrhage with 55.2% infarction (fig. 3).
There was a significant deleterious effect of arterial
anastomosis on the percent of infarction in animals
that had an operation 5 h after embolization (p 0.01)
(Student's /-test).
Discussion
Dujovnoy and associates showed that embolectomy
in dogs is safe if performed up to and including 5 h
subsequent to MCA embolization.7 After 5 h the
animals developed massive cerebral infarction with
gross neurologic impairment. Crowell and Olsson
demonstrated a favorable effect of EC-IC bypass performed 2 h after MCA clip occlusion in the dog.6
Sundt and co-workers have reported that reinstituting
TABLE 2 Clinical Results
Marked dysfunction
000
000
0
0
0000
*0
0
0
00000
*••
(hem)
Mild dysfunction
00
**•
No deficit
-
Group A 0
Group B 0
Group C *
(prox) (hem)
(hem)
(hem)
0
000
000
(proximal)
(proximal)
(proximal)
00**
00**
**o
**o
00
00
000
000
Gait
(prox)
•**
•*
(proximal)
Strength
373
Sensations
Level of
Consciousness
**
Field Deficit
374
STROKE
VOL 10, No 4, JULY-AUGUST
1979
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
of acute infarction. If therapy could be shown to delay
the course of infarction and thereby lengthen the grace
period in which a bypass procedure could be done, it
might substantially improve the treatment of acute
vascular occlusion.
References
FIGURE 3. A) Coronal serial sections of animal with embolus placement I h after extracranial-intracranial
anastomosis. Small area of visible hemorrhage and edema.
B) Coronal serial sections of animal with embalm placement
5 h before extracranial-intracranial anastomosis. Marked
areas of hemorrhage and edema are visible. C) Coronal
serial sections of animal with embolus placement only.
Moderate hemorrhage is visible.
revascularization when performed as soon as 1 h
before embolic MCA occlusion. This experimental
model may lend itself to further evaluation of the
effects of various therapeutic modalities on the course
1. Austin G, Hayward W, Laffin D: Modification of cerebral
ischemia by microsurgical intracranial anastomosis. In
Anastomosis for Cerebral Ischemia. Springfield, CC Thomas,
1977, pp 281-294
2. Branston NM, Symon L, Crockard HA: Recovery of the cortical evoked response following temporary-middle cerebral
artery occlusion in baboons: relation to local blood flow and
pO,. Stroke 2: 151-157, 1976
3. Brateman NE, Reids WS, Crawford ES, De Bakey ME:
Cerebral hemorrhage in carotid artery surgery. Arch Neurol 9:
458-467, 1963
4. Chater N: Patient selection and results of extra to intracranial
anastomosis in selected cases of cerebrovascular disease. In
Clinical Neurosurgery Vol 23. Baltimore, Williams and
Wilkins, 1976, pp 287-309
5. Crowell RM, Olsson Y: Effect of extracranial-intracranial
vascular bypass graft on experimental acute stroke in dogs. J
Neurosurg 38: 26-31, 1976
6. Crowell RM, Olsson Y, Klatzo I, Ommaya A: Temporary
occlusion of the middle cerebral artery in the monkey: clinical
and pathological observations. Stroke 1: 439-448, 1970
7. Dujovnoy M, Marrinuevo BS, Ranjit KL, De Castro S,
Maroon JC: Experimental middle cerebral artery embolectomy. Surg Fonim 27: 495-496, 1976
8 Gratzlo O, Schmeidek P, Spetzler R, Steinhoff H, Marguth F:
Clinical experience with extra-intracranial arterial anastomosis
in 65 cases. J Neurosurg 44: 313-325, 1976
EFFECT OF STA-MCA ANASTOMOSIS ON MCA OCCLUSION/Levj/zf/w/ et al.
9. Harper MA, Deshmukh VK, Rowan JO, Jennett WB: The influence of sympathetic nervous activity on cerebral blood flow.
Arch Neurol 27: 1-6, 1972
10. Hoff JT, Smith AL, Hankison HL, Nielsen SL: Barbiturate
protections from cerebral infarction in primates. Stroke 6:
28-33, 1975
11. Hunter JA, Julian OC, Dye WS, Javid H: Emergency operation
for acute cerebral ischemia due to carotid artery obstruction:
review of 26 cases. Ann Surg 162: 901-904, 1965
12. Lazar M, Clark K: Microsurgical cerebral revascularization
concepts and practice. Surg Neurol 1: 355-359, 1973
13. Molinari GF: Experimental cerebral infarction. I. Selective
segmental occlusion of intracranial arteries in the dog. Stroke
1: 224-231, 1970
14. Ojemann RG, Crowell RM, Roberson GH, Fisher CM:
Surgical treatment of extracranial carotid occlusive disease. In
Clinical Neurosurgery Vol 22. Baltimore, Williams and
Wilkins, 1975, pp 214-263
15. Reichman OH: Selection of patients and clinical results following STA-cortical MCA anastomosis. In Anastomosis for
Cerebral Ischemia. Springfield, CC Thomas, 1977, pp 275-280
16. Rob CG: Operation for acute completed stroke due to thrombosis of the internal carotid artery. Surgery 65: 862-865, 1969
375
17. Smith AC, Hoff JT, Nielsen SL, Larson CP: Barbiturate
protection in acute focal cerebral ischemia. Stroke 5: 1-7, 1974
18. Sundt TM, Grant WC, Garcia JH: Restoration of middle
cerebral artery flow in experimental infarction. J Neurosurg31:
311-323, 1969
19. Thompson JE, Austin DJ, Patman RD: Endarterectomy for the
totally occluded carotid artery for stroke. Arch Surg 95:
795-801, 1967
20. Wylie EJ, Hein MF, Adams JE: Intracranial hemorrhage
following surgical revascularization for treatment of acute
strokes. J Neurosurg 21: 212-215, 1964
21. Yasargil MG: Experimental small vessel surgery in the dog including patching and grafting of cerebral vessels and the formation of functional extra-intracranial shunts. In Microvascular
Surgery. St Louis, CV Mosby, 1967, pp 87-126
22. Yasargil MG: Diagnosis and indications for operations in
cerebrovascular occlusive disease. In Microneurosurgery
Applied to Neurosurgery. Stuttgart, Georg Thieme Verlag,
1969, pp 95-119
23. Yatsu FM, Diamond I, Graziano C, Linguist P: Experimental
brain ischemia: protection from irreversible damage with a
rapid acting barbiturate (methohexital). Stroke 3: 726-732,
1972
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
Role of Adrenergic Nerves in Blood-Induced
Cerebral Vasospasm
F R E D E R I C K A . S I M E O N E , M . D . , PHILLIP E. V I N A L L ,
A.B.,
J. L. A L D E R M A N , P H . D . , A N D J O H N D . I R V I N , M . D . , P H . D .
SUMMARY Cerebral arteries have an abundant supply of adrenergic nerve fibers which are believed to
release vasoactive substances responsible for the induction of cerebral vasospasm. To assess the importance of
adrenergic nerves in this phenomenon, high doses (600 Mg/ml) of 6-hydroxydopamine (6-OHDA) were used to
produce in vitro chemical sympathectomy in bovine middle cerebral artery. 6-OHDA reduced catecholamine
fluorescence to undectable limits. H3-norepinephrine re-uptake was reduced to 1.5% of intact controls. Arterial
norepinephrine content was reduced by 92%.
Contractile responses to norepinephrine, serotonin, and fresh human whole blood were modestly reduced
after denervation. This reduction was probably due to alpha receptor inactivation by 6-OHDA, because after
protection of the alpha receptors with phentolamine the vessel response was the same as in untreated controls.
Contractions in response to aged human whole blood were not affected by denervation. The results suggest that
the endogenous release of catecholamines does not play a major role in the initiation or spread of bloodinduced vasospasm in large cerebral arteries.
Stroke Vol 10, No 4, 1979
THE P H E N O M E N O N of cerebral vasospasm
following aneurysm rupture and the clinical problems
associated -with it are well documented. 14 (Study of
the responses of bovine middle cerebral artery has
been made in vitro to define some of the underlying
mechanisms of the phenomenon of vasospasm in
previous work from this laboratory.6) The results implicate serotonin (5-HT), released from whole blood,
as a primary agent responsible for the initiation of
early (first phase) vessel contraction. Studies reported
From the Department of Neurosurgery of the Pennsylvania
Hospital and the University of Pennsylvania School of Medicine
(Dr. Simeone and Mr. Vinall) and the Department of Neurosurgery
of the Thomas Jefferson University School of Medicine (Drs. Alderman and Irvin), Philadelphia, PA.
Supported by NINDS Grant 11186.
recently indicated that breakdown products of
erythrocytes in aged whole blood6 are important factors in prolongation of spasm and the initiation of
delayed spasm (second phase). An event not readily
explicable by a vasoactive agent released in whole
blood is the occurrence of diffuse spasm remote from
the local accumulation of blood. One explanation is
that the adrenergic innervation of these larger cerebral
vessels plays a role in the pathogenesis and spread of
spasm, that a spasmogenic agent or agents trigger
release of the catecholamine (CA) norepinephrine
(NE) from adrenergic nerves, or that the adrenergic
nerves may spontaneously release NE which initiates
the spasm. The presence of adrenergic nerve terminals
in the cerebral artery of many species is well
documented. 711 By using 6-hydroxydopamine (6OHDA), a substance known to produce functional
Effect of STA-MCA anastomosis on the course of experimental acute MCA embolic
occlusion.
R Levinthal, J I Moseley, W J Brown and W E Stern
Stroke. 1979;10:371-375
doi: 10.1161/01.STR.10.4.371
Downloaded from http://stroke.ahajournals.org/ by guest on October 2, 2016
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1979 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/10/4/371
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click Request
Permissions in the middle column of the Web page under Services. Further information about this process is
available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/